Orthopedic Surgery Board Review MCQs: Hip, Arthroplasty, Foot, Trauma | Part 231

Key Takeaway
This page offers Part 231 of a comprehensive orthopedic surgery board review quiz. Featuring 100 high-yield MCQs, it's designed for orthopedic surgeons and residents preparing for AAOS, ABOS, and OITE certification exams. Utilize interactive study and exam modes with detailed explanations for optimal preparation.
About This Board Review Set
This is Part 231 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 231
This module focuses heavily on: Arthroplasty, Foot, Fracture, Hip.
Sample Questions from This Set
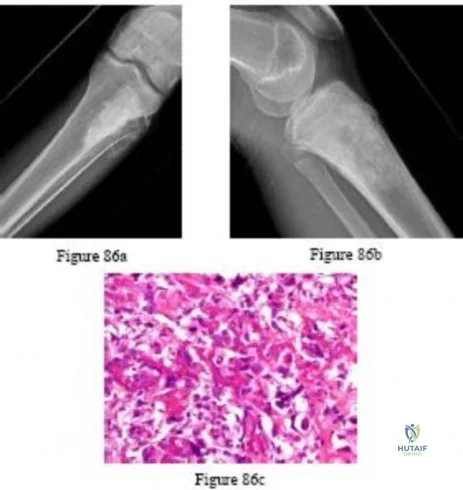
Sample Question 1: Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage s...
Sample Question 2: -The Injury Severity Score (ISS), using point scores from five different body systems, is a method that aids in predicting the chances of mortality in a patient with multiple injuries by...
Sample Question 3: Which of the following acetabular cup designs has shown the greatest survivorship at 10 years in patients younger than age 60 years?...
Sample Question 4: An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?...
Sample Question 5: Figures 51a through 51c show the radiographs of a 7-year-old soccer player who reports a gradual onset of midfoot pain that began shortly after the start of soccer season. He states that the pain is worse with activity and is partially alle...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?
Explanation
REFERENCES: Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642
Question 2
- The Injury Severity Score (ISS), using point scores from five different body systems, is a method that aids in predicting the chances of mortality in a patient with multiple injuries by
Explanation
Question 3
Which of the following acetabular cup designs has shown the greatest survivorship at 10 years in patients younger than age 60 years?
Explanation
REFERENCES: Smith SE, Harris WH: Total hip arthroplasty performed with insertion of the femoral component with cement and the acetabular component without cement: Ten to thirteen-year study. J Bone Joint Surg Am 1997;79:1827-1833.
Pellicci PM, Tria AJ Jr, Garvin KL, (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 195-206.
Question 4
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
REFERENCES: Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 5
Figures 51a through 51c show the radiographs of a 7-year-old soccer player who reports a gradual onset of midfoot pain that began shortly after the start of soccer season. He states that the pain is worse with activity and is partially alleviated by rest. Examination reveals soft-tissue swelling, and tenderness and warmth in the region of the talonavicular and navicular cunieform joints. Management should consist of
Explanation
REFERENCE: Lutter LD: Sports-related injuries, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992.
Question 6
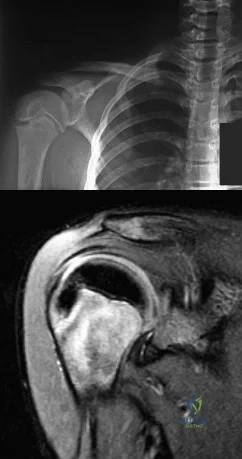
A 12-year-old boy has severe left shoulder pain after being struck by an automobile. A chest radiograph, AP and lateral radiographs, and a CT scan with three-dimensional reconstruction of the scapula are shown in Figures 38a through 38d. Management should consist of
Explanation
REFERENCES: Green N, Swiontkowski M: Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 3, pp 319-341.
Curtis RJ Jr, Rockwood CA Jr: Fractures and dislocations of the shoulder in children, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 991-1032.
Question 7
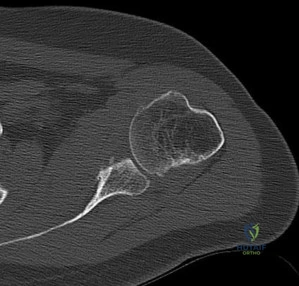
Figures 79a through 79d are the plain radiographs and axial CT scans of an 80-year-old woman with severe dementia and a newly noted thigh mass. Examination reveals a large, nonmobile anterior thigh mass that is minimally tender. What is the best next treatment step?
Explanation
Question 8
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty?
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Question 9
A 62-year-old man has a severe pes planus and pain in the hindfoot. Radiographs show advanced degenerative changes at the talonavicular and subtalar joints with good preservation of the ankle joint. What is the most appropriate surgical procedure to alleviate his pain?
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 269-282.
Graves SC, Stephenson K: The use of subtalar and triple arthrodesis in the treatment of posterior tibial tendon dysfunction. Foot Ankle Clin 1997;2:319.
Question 10
Total hip arthroplasty in a patient with a long-standing hip fusion on the contralateral side is most likely to result in
Explanation
REFERENCES: Garvin KL, Pellicci PM, Windsor RE, et al: Contralateral total hip arthroplasty or ipsilateral total hip arthroplasty in patients who have long-standing fusion of the hip. J Bone Joint Surg Am 1989;71:1355-1362.
Gore DR, Murray MP, et al: Walking patterns of men with unilateral surgical hip fusion. J Bone Joint Surg Am 1975;57:759-765.
Romness DW, Morrey BF: Total knee arthroplasty in patients with prior ipsilateral hip fusion. J Arthroplasty 1992;7:63-70.
Question 11
Which of the following structures may help maintain radial length after a radial head fracture?
Explanation
REFERENCES: Morrey BF, Chao EY, Hui FC: Biomechanical study of the elbow following excision of the radial head. J Bone Joint Surg Am 1979;61:63-68.
Coleman DA, Blair WF, Shurr D: Resection of the radial head for fracture of the radial head: Long-term follow-up of seventeen cases. J Bone Joint Surg Am 1987;69:385-392.
Question 12
In the anterior cruciate ligament-deficient knee, what structure provides an important secondary restraint to anterior tibial translation?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 200.
Allen CR, Wong EK, Livesay GA, et al: Importance of the medial meniscus in the anterior cruciate ligament-deficient knee. J Orthop Res 2000;18:109-115.
Levy IM, Torzilli PA, Warren RF: The effect of medial meniscectomy on anterior-posterior motion of the knee. J Bone Joint Surg Am 1982;64:883-888.
0 •v. .
jfp
JM w
!i
1 mf
m
Question 13
In a patient who has had low back pain for less than 2 weeks, which of the following findings is an indication for continued observation and symptomatic treatment rather than more aggressive evaluation and/or treatment?
Explanation
REFERENCES: Frymoyer JW: Back pain and sciatica. N Engl J Med 1988;318:291-300.
McCullough JA, Transfeldt EE: Macnab’s Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 240-357.
Question 14
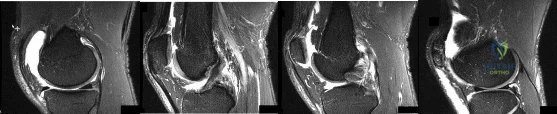
Figures 1 through 4 are selected sagittal MR images of an otherwise healthy 20-year-old collegiate football running back who was tackled during a game and has immediate onset of right knee pain. Video analysis of the injury shows that his flexed knee impacted the field. He is not able to return to play. On examination in the training room the following morning, he has a moderate effusion, no patellar instability, minimal joint line tenderness, and is stable to varus and valgus stress at 30° of knee flexion. A dial test is also negative. He has increased laxity in the anterior to posterior direction. What is the most appropriate next step in treatment?
Explanation
This athlete sustained an isolated PCL injury. The mechanism of injury is typical for a PCL injury. When a PCL injury is identified, one must rule out other ligamentous injuries to the knee. The patient has a stable examination to varus and valgus and a negative dial test, so the lateral collateral, medial collateral, and posterolateral corner (respectively) are intact. It is common to have increased anterior to posterior translation in isolated PCL injuries, even with an intact ACL, as the tibia will rest posterior to the medial femoral condyle. Treatment of isolated PCL injuries is typically nonoperative, with an initial focus on quadriceps strengthening. Hamstring strengthening and rehabilitation is added at a later time, as this places increased stress on the healing PCL. The images reveal an isolated PCL injury with intact menisci and ACL, ruling out ACL reconstruction using autograft tissue and PCL reconstruction using autograft tissue.
Question 15
A 3-year-old girl has had wrist pain, a fever, and has refused to move her right wrist for the past 10 days. She has an oral temperature of 102 degrees F (38.7 degree C). Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h, a WBC count of 11,000/mm 3 , and a left shift. AP and lateral radiographs are shown in Figures 57a and 57b. What is the most likely diagnosis?
Explanation
REFERENCES: Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Song KM, Sloboda JF: Acute hematogenous osteomyelitis in children. J Am Acad Orthop Surg 2001;9:166-175.
Question 16
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
REFERENCES: Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Conn RA, Colfield RH, Byer DE, Lindstromberg JW: Interscalene block anesthesia for shoulder surgery. Clin Orthop 1987;216:94-98.
Question 17
A 56-year-old woman sustains a type IIIB open tibial shaft fracture. She undergoes irrigation and debridement and intramedullary nailing with flap coverage 24 hours later. Cultures are taken pre-debridement and post-debridement. She develops a surgical site infection at 6 weeks, which requires removing the hardware and placing show Commented [1]: an external fixator. Deep cultures are most likely to pathogens found in
Explanation
In another study, before any interventions were performed, initial aerobic and anaerobic cultures of the wounds of 117 consecutive open extremity fractures grades I through III were obtained. The results of these cultures were correlated with the development of a wound infection. If an infection occurred, the organism grown from the infected wound was compared with any organism grown from the primary wound cultures. Of the initial cultures, 76% (89/117) did not demonstrate any growth, while the other 24% (28/117) only grew skin flora. There were only 7 (6%) wound infections, and 71% (5/7) initially did not grow any organisms. Of the isolates that grew from the initial cultures, none were the organisms that eventually led to
Question 18
Which examination finding points toward a brachial plexus injury rather than root avulsion?
Explanation
A brachial plexus injury distal to the root level should leave the rhomboid muscle with intact function. Root avulsions of C5-6 will cause weakness of the rhomboids. The branching of the dorsal scapular nerve is proximal and often spared with upper brachial plexus injuries. Winging and biceps weakness may occur
with either injury, and an ipsilateral fracture does not differentiate an avulsion from a brachial plexus injury.
Question 19
During the approach to the lumbar spine for an L4-L5 anterior lumbar interbody fusion, which structure generally is found overlying the anterior surface of the L4 vertebra?
Explanation
During an anterior approach to the L4-L5 disk space for anterior lumbar interbody fusion, meticulous exposure is paramount to allow for safe preparation of the disk space and subsequent arthrodesis. Although all of these structures can come into play during the exposure, the aorta lies anterior to the L4 vertebral body and bifurcates at this level. The vena cava bifurcates just distal to this. The ureters lie to both sides of the anterior spine. The right common iliac artery and the left common iliac vein originate after the bifurcation of the great vessels and lie caudal to the L4 vertebra.
RECOMMENDED READINGS
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:226-235.
Agur AMR, Lee MJ, eds. Grant's Atlas of Anatomy. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:89.
Question 20
A 17-year-old high school football linebacker sustains an injury while making a tackle. His initial symptoms are right shoulder pain, bilateral biceps weakness, and right arm numbness. The symptoms only last a few minutes, and he continues to play in the game. He tells his parents after the game, and they bring him to your office for evaluation the next day. He no longer has any symptoms, and his examination findings and cervical spine radiographs are normal. What is the best next step?
Explanation
Question 21
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Lucas DR, Nascimento AG, Sim FH: Clear cell sarcoma of soft tissues: Mayo Clinic experience with 35 cases. Am J Surg Pathol 1992;16:1197-1204.
Question 22
Which of the following associated type acetabular fracture patterns is defined based on the fact that all articular segments are detached from the intact portion of the ilium, which remains attached to the sacrum through the sacroiliac joint?

Explanation
Question 23
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
Explanation
ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Paletta GA Jr, Laskins RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
Question 24
A 15-year-old boy has hindfoot pain and very limited subtalar motion. A CT scan reveals a talocalcaneal coalition involving 40% of the middle facet. He has no degeneration of the posterior subtalar facet. Following failure of nonsurgical management, treatment should consist of
Explanation
REFERENCES: Sullivan JA: The child’s foot, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1077-1135.
Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
Question 25
A 9-year-old girl reports progressive right knee pain. Radiographs are shown in Figures 59a and 59b. Work-up reveals no other sites of disease. Low- and high-power photomicrographs are shown in Figures 59c and 59d. What is the most appropriate treatment?
Explanation
REFERENCES: Bacci G, Ferrari S, Bertoni F, et al: Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the Instituto Ortopedico Rizzoli according to the Instituto Ortopedico Rizzoli/osteosarcoma-2 protocol: An updated report. J Clin Oncol 2000;18:4016-4037.
Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790.
Mankin HJ, Hornicek FJ, Rosenberg AE, et al: Survival data for 648 patients with osteosarcoma treated at one institution. Clin Orthop Relat Res 2004;429:286-291.
Question 26
A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?
Explanation
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
Harris MB, Banta JV: Cost of skin care in the myelomeningocele population. J Pediatr Orthop 1990;10:355:361.
Question 27
A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
Explanation
REFERENCES: Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am
2006;88:113-120.
Iannotti JP, Hennigan S, Herzog R, et al: Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am 2006;88:342-348.
Question 28
A 14-year-old boy has an asymptomatic mass on the right arm. MRI scans and biopsy specimens are shown in Figures 51a through 51d. Immunostaining is positive for desmin. Additional staging studies should include
Explanation
REFERENCES: Lawrence W, Jr., Hays DM, Heyn R, Tefft M, Crist W, Beltangady M, et al: Lymphatic metastases with childhood rhabdomyosarcoma: A report from the Intergroup Rhabdomyosarcoma Study. Cancer 1987;60:910-915.
Schleiermacher G, Peter M, Oberlin O, et al: Increased risk of systemic relapses associated with bone marrow micrometastasis and circulating tumor cells in localized ewing tumor. J Clin Oncol 2003;21:85-91.
Question 29
A 43-year-old woman has a 2-week history of right shoulder pain. She denies any injury to initiate her symptoms but states that she has shoulder pain with range of motion and lifting objects. Examination reveals mild pain with abduction, empty can testing, and with the Neer and Hawkins impingement tests. Her range of motion with the right shoulder reveals passive forward flexion to 90 degrees, abduction to 90 degrees, external rotation at the side to 15 degrees, and internal rotation to her buttock. The uninvolved left shoulder has forward flexion to 160 degrees, abduction to 150 degrees, external rotation at the side to 60 degrees, and internal rotation to T6. Radiographs of the shoulder are normal. What is the next most appropriate step in management? Review Topic
Explanation
Question 30
Figure 11 shows the radiograph of a 2-year-old child with marked genu varum and tibial bowing. Based on these findings, what is the best initial course of action?

Explanation
Question 31
The patient in Figure 55 is actively attempting to make a fist. This clinical scenario suggests which of the following anatomic lesions?
Explanation
REFERENCE: Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, p 189.
Question 32
The most appropriate treatment for this fracture is
Explanation
Tibial fractures are classified on the basis of their anatomical location and the status of the prosthesis fixation. Type I fractures involve the tibial plateau, type II fractures occur adjacent to the stem of the tibial component, type III fractures are distal to the tibial stem, and type IV fractures involve the tibial tubercle. Subclassifications include A with a well-fixed implant; B with a loose implant; and C, which occur intraoperatively.
Treatment of periprosthetic tibial fractures is based on the location of the fracture and the status of the component fixation. Types II or III fractures associated with prosthetic loosening or instability are best managed with revision arthroplasty, usually with a diaphyseal-engaging intramedullary tibial stem. Supplemental internal fixation may be necessary. Type III fractures with well-fixed and stable implants are treated using the standard principles of tibial fracture management.
Question 33
A 17-year-old male football player is seen 1 week after developing symptoms of infectious mononucleosis in the middle of the season. Examination reveals evidence of splenomegaly. He and his parents want to know if he can play in a game the following day. What is the most appropriate recommendation? Review Topic
Explanation
Question 34
Figures 18a and 18b show the radiographs of a 13-year-old baseball player who sustained a patellar dislocation with an associated lateral femoral condyle fracture. What ligament is attached to this fragment?
Explanation
REFERENCES: Jobe CM, Wright M: Anatomy of the knee, in Fu FH, Harner CD, Vince KG (eds): Knee Surgery. Baltimore, MD, Williams & Wilkins, 1994, pp 1-54.
Moore KL, Dalley AF: Lower limb, in Moore KL, Dalley AF (eds): Clinically Oriented Anatomy, ed 4. Philadelphia, PA, Lippincott, Williams & Wilkins, 1999, pp 503-664.
Question 35
Limited weight bearing usually is recommended following open reduction and internal fixation of intra-articular lower extremity fractures. A bone graft, or bone graft substitute is often placed in the metaphyseal void beneath the reduced articular fragments. Which of the following bone grafts or bone graft substitutes will most likely permit earlier weight bearing without subsidence of the articular reduction?
Explanation
Question 36
A 21-year-old man has had posterior neck discomfort for the past 6 months. A whole-body bone scan and a cervical single-photon emission CT reveal increased activity at the C7 spinous process. MRI reveals multifocal involvement of the spinous process lamina and facet of C7. A CT-directed needle biopsy reveals osteoblastoma. What is the best course of action?
Explanation
REFERENCES: Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1143-1174.
Ozaki T, Liljenquist U, Hillmann A, et al: Osteoid osteoma and osteoblastoma of the spine: Experience with 22 patients. Clin Orthop 2002;397:394-402.
Question 37
The arrow in Figure 39 is pointing to which of the following ligaments?
Explanation
REFERENCES: Berger RA: Ligament anatomy, in Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist, Diagnosis and Operative Management. St Louis, MO, Mosby, 1998,
pp 73-105.
Adams BD, Divelbiss BJ: Anatomy of the wrist ligaments, in Trumble TE (ed): Carpal Fracture-Dislocatons. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 1-5.
Question 38
A 68-year-old patient undergoes total knee arthroplasty for end-stage degenerative joint disease. Two years later, she trips and falls at home and sustains a fracture seen in Figures A and B. Before her fall, she was a community ambulator and had no knee pain. The component is determined to be stable and the surgeon decides to treat this fracture with closed reduction and retrograde intramedullary fixation with a supracondylar nail. Which of the following statements is true?

Explanation
Periprosthetic femur fractures above total knee implants occur in 2% of patients. It is important to note: (1) pre-injury function, to determine if the prosthesis was loose, (2) the type of implant (CR vs posterior stabilized, PS) as a PS implant with a closed box would make retrograde intramedullary nailing more difficult (the surgeon has to consider the size of the box vs size of the nail, and if the box is smaller than the nail,
must be prepared to enlarge the box with a metal-cutting burr, which has inherent problems of introducing wear debris into the joint), (3) pre-fracture radiographs help determine the position of the implants (flexion-extension, varus-valgus). These fractures can be treated with non-locking condylar buttress plates (not recommended today), fixed angle devices and intramedullary nailing.
McLaren et al. describe 7 osteopenic patients (mean age, 61yrs, range 47-84yrs) treated with retrograde supracondylar nailing. They suggest not reaming, and placing 2-3 screws in the distal fragment. This may require leaving the nail protruding by 1cm. They then suggest removing the protruding segment with a burr at the end of the procedure.
Haidukewych et al. debate plating vs nailing in a 80yr old osteopenic patient. It may be difficult to introduce retrograde intramedullary nails through the same incision if dense scar tissue is present. On the other hand, most plates require extensive dissection and do not respect the soft tissues and fracture biology, except for LISS plates and nails.
Figures A and B show a displaced Lewis and Rorabeck type II periprosthetic fracture. Illustration A shows the technique of retrograde supracondylar nailing. With the knee flexed, the fracture is reduced and the entry point is in the intercondylar notch. Illustration B shows a comparison between PS and CR implants. Note the "box" in the PS implant. This is absent in the CR implant. Illustration C shows the Lewis and Rorabeck classification.
Incorrect Answers:
1 (at most 2) point of fixation in the distal segment. Answer 5: The backup plan should include devices that resist varus collapse (especially in cases with medial comminution), such as angle-stable devices (ABP, DCS and locking plates). Non-locking condylar buttress plates will not resist varus collapse.
Question 39
Figure 7 shows the radiograph of an 18-year-old hockey player who sustained a shoulder injury during a fall into the side boards. Examination reveals a significant prominence at the acromioclavicular joint. Management should consist of
Explanation
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 1995;23:324-331.
Question 40
Augmentation of a Broström repair with the mobilized lateral portion of the extensor retinaculum (Gould modification) is expected to produce
Explanation
Question 41
Figures 1 and 2 depict the postoperative radiographs obtained from a 22-year-old man who was involved in a motor vehicle accident. The most likely limitation in motion arising from this treatment is

Explanation
This patient sustained fractures of his radius and ulna; both were treated with plate and screw fixation. The plate used on the radius was straight, resulting in loss of the radial bow, which is critical for enabling the radius to curve around the ulna during pronation. This patient is unable to pronate beyond 20°. Schemitsch and Richards correlated a good functional outcome, defined as more than 80% of normal rotation of the forearm, with restoration of the normal amount and location of the radial bow. Additionally, they related the restoration of grip strength with appropriate restoration of the radial bow. Matthews and associates reported little significant loss of rotation with 10° of angulation; however, 20° of angulation resulted in a statistically and clinically significant loss of forearm rotation.
Question 42
A 15-year-old baseball pitcher who reports increasing pain in his right shoulder over the past 3 weeks states that the pain increases the more he pitches. Radiographs of both shoulders are shown in Figures 35a and 35b. What is the next most appropriate step in management?
Explanation
REFERENCES: Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in the adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Cahill BR, Tullos HS, Fain RH: Little league shoulder: Lesions of the proximal humeral epiphyseal plate. J Sports Med 1974;2:150-152.
Question 43
A 15-year-old boy has a fracture of the proximal tibia extending from the apophysis of the tubercle up through the posterior part of the proximal tibial epiphysis and into the joint. What is the most likely mechanism of injury?
Explanation
Question 44
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Explanation
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 45
Design factors that enhance the long-term survival of proximally coated cementless hip implants include both initial stability and
Explanation
REFERENCES: Mont MA, Hungerford DS: Proximally coated ingrowth prostheses: A review. Clin Orthop 1997;344:139-149.
Engh CA, Hooten JP Jr, Zettl-Schaffer KF, Ghaffarpour M, McGovern TF, Bobyn JD: Evaluation of bone ingrowth in proximally and extensively porous-coated anatomic medullary locking prostheses retrieved at autopsy. J Bone Joint Surg Am 1995;77:903-910.
Urban RM, Jacobs JJ, Sumner DR, Peters CL, Voss FR, Galante JO: The bone-implant interface of femoral stems with non-circumferential porous coating. J Bone Joint Surg Am 1996;78:1068-1081.
Question 46
Figures 65a and 65b show the MRI scans of a 33-year-old man with severe left leg pain. He has had symptoms for 3 months with progressive worsening pain and function. Examination reveals ankle plantar-flexor weakness and diminished light touch sensation on the plantar surface of the foot. What treatment provides the best outcome? Review Topic
Explanation
Question 47
The sartorius muscle is innervated by which of the following nerves?
Explanation
REFERENCES: Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 404.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 139.
Question 48
Cortical bone demonstrates viscoelastic behavior as its mechanical properties are sensitive to strain rate and duration of applied load. Regarding longitudinal strain in cortical bone, which of the following statements regarding this characteristic is true?
Explanation
For LOW strain rates typical of normal activity (physiological strain rates of <0.1/s), bone is ELASTIC and DUCTILE (increasing ultimate strain with increasing strain rate). There is a ductile-to-brittle transition with increasing strain rate from normal to
supranormal rates. For EXTREMELY HIGH supranormal strain rates (>0.1/s, high impact trauma), bone is VISCOELASTIC and BRITTLE (low ultimate strain with increasing strain rate). Bone also becomes stronger and stiffer (higher modulus, steeper slope of stress-strain plot) as strain rate increases. This viscoelastic property helps in damping muscle contracture.
Natali and Meroi reviewed studies examining mechanical properties of bone. Mechanical properties are correlated with moisture, deformation rate, density and region of bone. Mechanical adaptation of bone is affected by strain rate (rate at which bone is deformed), strain mode (tension, compression, shear), strain direction (direction of strain relative to bone surface), strain frequency (cycles/second), stimulus duration (period over which deformation cycles are applied), strain distribution (pattern of strain magnitude across bone section) and strain energy (energy stored during deformation).
Illustration A shows the mechanical properties of bone with increasing strain rates. Incorrect Answers:
increase. During normal activity, as strain rate increases, bone is more ductile. With high impact trauma, bone is more brittle.
Question 49
A 57-year-old man has had right ankle pain for the past 10 months following an injury that went untreated. Radiographs are shown in Figures 30a through 30c. Management should consist of
Explanation
REFERENCES: Marti RK, Raaymakers EL, Nolte PA: Malunited ankle fractures: The late results of reconstruction. J Bone Joint Surg Br 1990;72:709-713.
Geissler W, Tsao A, Hughes J: Fractures and injuries of the ankle, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2201-2206.
Yablon IG, Leach RE: Reconstruction of malunited fractures of the lateral malleolus. J Bone Joint Surg Am 1989;71:521-527.
Question 50
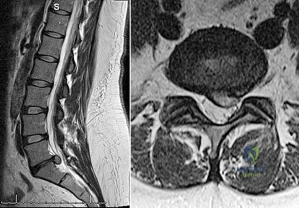
Figure 35 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?

Explanation
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-a, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-ß, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
RECOMMENDED READINGS
Kim HT, Yoon ST, Jarrett C. Articular cartilage and intervertebral disk. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:23-33.
Hoyland JA, Le Maitre C, Freemont AJ. Investigation of the role of IL-1 and TNF in matrix degradation in the intervertebral disc. Rheumatology (Oxford). 2008 Jun;47(6):809-14. doi: 10.1093/rheumatology/ken056. Epub 2008 Apr 8. PubMed PMID: 18397957. View Abstract at PubMed
Gruber HE, Ingram JA, Hanley EN Jr. Immunolocalization of MMP-19 in the human intervertebral disc: implications for disc aging and degeneration. Biotech Histochem. 2005 May-Aug;80(3-4):157-62. PubMed PMID: 16298901. View Abstract at PubMed
Question 51
Figure 74 shows the radiograph of an 84-year-old woman who reports severe right knee pain. At the time of total knee arthroplasty, she is found to have gross insufficiency and attenuation of the medial collateral ligament (MCL) complex. Optimal management should consist of
Explanation
REFERENCES: Lachiewicz PF, Soileau ES: Ten-year survival and clinical results of constrained components in primary total knee arthroplasty. J Arthroplasty 2006;21:803-808.
Anderson JA, Baldini A, MacDonald JH, et al: Primary constrained condylar knee arthroplasty without stem extensions for the valgus knee. Clin Orthop Relat Res 2006;442:199-203.

Question 52
Figures below show the AP and lateral radiographs obtained from a 54-year-old woman who has worsening groin pain 18 months after a primary left total hip arthroplasty. The pain is worst when climbing stairs, when rising from a seated position, and during resisted hip flexion. Her pain improved early after surgery but did not completely resolve. Her C-reactive protein and erythrocyte sedimentation rate results of less than 1 mg/dL and 10 mm/hr, respectively, were obtained in the office. What is the best next step?
Explanation
Iliopsoas impingement is a potential cause of persistent groin pain after a total hip arthroplasty. This patient’s history gives groin pain with resisted hip flexion and during activities that require this level of function. The radiographs depict an acetabular component with substantial retroversion. Typical options for the management of iliopsoas tendon impingement include injections, tenotomy, and acetabular revision. Recently, Chalmers and associates reported more predictable groin pain resolution with 8 mm or more of anterior acetabular component when overhang was revised. The radiographs clearly show more retroversion, with a cup prominence of more than 8 mm anteriorly. MRI with MARS could potentially help in the diagnosis of this impingement but would not help in management (option A). An ultrasound- guided injection would need to be administered into the iliopsoas tendon sheath to be of help and, in this case, would likely be performed for diagnostic purposes due to the extreme anterior overhang (option C). Option D would be useful for mild cases of iliopsoas impingement but likely would not help much in this more extreme case.
Question 53
Figure 20 shows the clinical photograph of a man who has had diabetes mellitus controlled with oral medication for the past 10 years. He wears soft-soled shoes and only uses leather-soled shoes for important business meetings. Examination reveals palpable dorsalis pedis and posterior tibial pulses, although they are somewhat diminished. He is insensate to pressure with the Semmes-Weinstein 5.07 monofilament. The ulcer heals after treatment with a full contact cast. What is the best course of action at this time?
Explanation
REFERENCES: Pinzur MS, Kernan-Schroeder D, Emmanuele NV, et al: Development of a nurse-provided health system strategy for diabetic foot care. Foot Ank Int 2001;22:744-746.
Pinzur MS, Shields N, Goelitz B, et al: American Orthopaedic Foot & Ankle Society shoe survey of diabetic patients. Foot & Ankle Int 1999;20:703-707.
Reiber GE, Smith DG, Wallace CM, et al: Effect of therapeutic footwear on foot reulceration in patients with diabetes: A randomized controlled trial. JAMA 2002;287:2552-2558.
Question 54
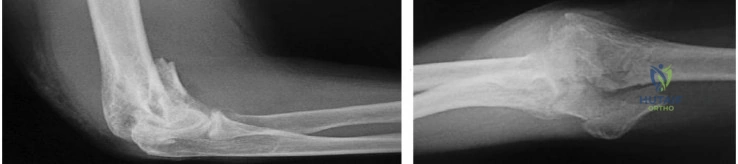
..Figures 83a and 83b are the radiographs of a 53-year-old otherwise healthy homemaker who had a syncopal episode and sustained a ground-level fall and injury to her right elbow. She presently admits to right elbow pain, swelling, and an inability to bend her elbow. What is the best initial treatment for this injury?
Explanation
Figure 84 is the glenoid CT scan of a 20-year-old man who dislocated his shoulder anteriorly while playing football. He had persistent instability 2 months after the injury, but he did not have a sulcus sign or posterior instability. He underwent an arthroscopic Bankart repair with 4 bioabsorbable anchors with simple sutures through the labrum and capsule.
He did not have an engaging Hill-Sachs lesion, the rotator cuff was unremarkable, and the capsule was not torn from the humerus. After surgery, he did well for 6 months until he jumped into a lake and again dislocated his shoulder anteriorly. He says his shoulder no longer felt stable after his reduction.
Question 55
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 56
What root is most commonly involved with a segmental root level palsy after laminoplasty?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-249.
Uematsu Y, Tokuhashi Y, Matsuzaki H: Radiculopathy after laminoplasty of the cervical spine. Spine 1998;23:2057-2062.
Question 57
Figure 30a is the anteroposterior radiograph of a 20-year-old woman with mild right groin pain and intermittent “catching” in the hip region. What is the most appropriate next step? tear
Explanation
Because this patient is young, substantial bilateral acetabular dysplasia is present, and the joint space is well preserved, periacetabular osteotomy is the treatment of choice (Figure 30b). Arthroscopic evaluation and treatment is insufficient to address the mechanical deformity. Although a hip injection can be diagnostically helpful, it would not alter the treatment plan in this scenario. The patient’s young age would make observation and subsequent THA less desirable. Femoral osteotomies also were performed to address rotational deformity.

Question 58
A B Figures 19a and 19b are the CT scans of an 18-year-old man who was a restrained driver in a rollover motor vehicle collision. What was the primary mechanism of injury?
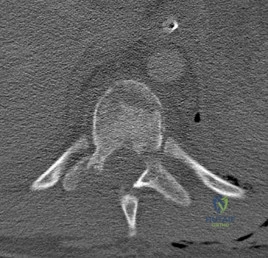
Explanation
This injury pattern represents a flexion distraction injury, or a Chance fracture. The imaging hallmark of this injury is the axial split of the pedicle seen on the sagittal CT scan. This injury necessitates surgical intervention to prevent progressive deformity and pain. A rotation mechanism results in a dislocation with a rotational deformity at the level of injury. An extension force causes failure of the anterior column in tension with compression of the posterior column. An axial load force would result in a burst fracture.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Vaccaro AR, Baron EM, Sanfilippo J, Jacoby S, Steuve J, Grossman E, DiPaola M, Ranier P, Austin L, Ropiak R, Ciminello M, Okafor C, Eichenbaum M, Rapuri V, Smith E, Orozco F, Ugolini P, Fletcher M, Minnich J, Goldberg G, Wilsey J, Lee JY, Lim MR, Burns A, Marino R, DiPaola C, Zeiller L, Zeiler SC, Harrop J, Anderson DG, Albert TJ, Hilibrand AS. Reliability of a novel classification system for thoracolumbar injuries: the Thoracolumbar Injury Severity Score. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S62-9; discussion S104. PubMed PMID:16685239.View Abstract at PubMed
Question 59
Which of the following zones of articular cartilage has the highest concentration of proteoglycans?
Explanation
Question 60
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?
Explanation
REFERENCES: Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Johnson T, Steinbach L (eds): Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, p 44.
Question 61
A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of Review Topic
Explanation
Question 62
A 21-year-old male is brought to the emergency department after being involved in gang-related violence. A radiograph of his pelvis is shown in Figure A. The patient is hemodynamically stable. Which of the following imaging modalities is the next best step in evaluating this patient for the most common associated injury? Review Topic

Explanation
The incidence of GSW is increasing and it is the 2nd leading cause of death in young males in the US after motor vehicle accidents. The incidence of a GSW to the buttock is approximately 8% of all GSW to the extremities. Potential complications of pelvic and acetabular GSW include septic arthritis, enterocutaneous, enteroacetabular, and vesicoacetabular fistulas, infected nonunion, malunion, and injuries to the iliac vessels. The presence or absence of intra-abdominal injuries affects treatment and outcome.
Bartkiw et al. reviewed 2808 GSW and found 1235 associated fractures including 42 fractures of the hip and pelvis. Ten orthopaedic operative procedures were performed in 7 patients. Associated nonorthopaedic injuries included 15 small/large bowel perforations (36%), 7 vessel lacerations (17%), and 2 urogenital injuries (5%) that required surgery.
Najibi et al. reviewed 39 GSW to acetabulum. They found 32 simple and 7 associated fracture patterns. The most common simple and associated patterns were anterior column and both column, respectively. Bowel injuries were the most common associated injures (42%). Predictors of poor outcome include high-velocity missile, involvement of acetabular dome, abdominal injury, nerve injury, vascular injury, and male gender. Deep infection was associated with primary anastomosis of bowel injury and an associated fracture pattern.
Figure A shows a GSW to the right hip with acetabular fracture and visible bullet fragment.
Incorrect Answers:
Question 63
Figures 15a and 15b are intrasurgical photographs from the posterolateral viewing portal that were taken at the beginning and end of a right shoulder arthroscopic procedure performed on a 54-year-old man. This technique demonstrates superior results compared to traditional arthroscopic techniques when evaluating which outcome?
Explanation
The images reveal a medium-sized tear of the rotator cuff. As more clinical studies are published comparing double-row with single-row rotator cuff repair, it has become clear that the retear rate is lower with a double-row construct for small and medium-sized tears. This may be attributable to the stronger time-zero repair construct that double-row repair provides. No study to date has demonstrated a significant difference in clinical outcomes (functional and pain scores at any time) or time to healing between the 2 techniques.

CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 17
Figure 16 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop," and then he needed help walking off the field. His knee is visibly swollen.
Question 64
In providing culturally competent care to a Muslim woman with a cervical spine injury, which of the following most accurately describes the steps a male orthopaedist should take to respect her religious beliefs during his examination?
Explanation
REFERENCE: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 65
The most common complication associated with corticosteroid injection for the treatment of interdigital neuroma is
Explanation
Interdigital neuromas represent perineural fibrosis of the intermetatarsal nerve most commonly seen in the second and third web spaces. The photographs depict a neuroma in the second web space, which is less common than in the third space. Its hypoechoic appearance is characteristic on ultrasound. PVNS occurs in joints. Lipomas are fatty tumors. A ganglion cyst can occasionally occur adjacent to a nerve, but it has a cystic appearance.
The most popular theory on the etiology of interdigital neuromas is compression neuropathy by the intermetatarsal ligament. The plantar approach for the resection of interdigital neuromas has become more popular, especially for recurrent neuromas. The major advantage is better visualization and access to the neuromas.
Infection and allergic reactions such as hives are rare after steroid injection. CRPS is not known to occur in this setting. Hammertoe formation can occur, especially after multiple steroid injections into an interdigital neuroma.
RECOMMENDED READINGS
Schon LC, Reed MA. Disorder of the nerves. In: Coughlin MJ, Saltzman CL, Anderson RB, eds. Mann's Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Elsevier-Saunders; 2014:622-641.
Gauthier G. Thomas Morton's disease: a nerve entrapment syndrome. A new surgical technique. Clin Orthop Relat Res. 1979 Jul-Aug;(142):90-2. PubMed PMID: 498653. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 96 THROUGH 98
Figure 96 is the anteroposterior projection foot radiograph of a 35-year-old woman who is injured in a high-speed motorcycle collision. Her assessment reveals an isolated injury. Her pulses are palpable and her neuromotor examination is intact. There is tenting of skin with ecchymosis over the second metatarsal. The foot is extremely swollen but not tense. Passive toe range of motion is painless.

Question 66
A 26-year-old rugby player injured his foot when tackled from behind. Radiographs are seen in Figures 35a through 35c. What is the most appropriate treatment?
Explanation
REFERENCES: Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries of the tarsometatarsal joint. Orthop Clin North Am 2001;32:11-20.
Hunt SA, Ropiak C, Tejwani NC: Lisfranc joint injuries: Diagnosis and treatment. Am J Orthop 2006;35:376-385.
Question 67
During the first stage of osteoarthritis, which of the following processes predominates?
Explanation
aggrecan concentration are both decreased. Increased water content tends to decrease the stiffness of the matrix, rendering cartilage tissue more susceptible to further mechanical damage. In the second stage, chondrocytes detect tissue damage and respond by releasing mediators to increase proliferation. Clusters or clones of proliferating chondrocytes are hallmark of the response to articular degeneration. In the third stage, both the proliferative response and anabolic activity are decreased. In this stage, the loss of articular cartilage is more evident and leads to clinical signs of degenerative joint disease.
Question 68
A sagittal T1-weighted MRI scan of the knee joint is shown in Figure 23. What structure is identified by the arrow?
Explanation
REFERENCES: Gross ML, Grover JS, Bassett LW, Seeger LL, Finerman GA: Magnetic resonance imaging of the posterior cruciate ligament: Clinical use to improve diagnostic accuracy. Am J Sports Med 1992;20:732-737.
Sonin AH, Fitzgerald SW, Friedman H, Hoff FL, Hendrix RW, Rogers LF: Posterior cruciate ligament injury: MR imaging diagnosis and patterns of injury. Radiology 1994;190:455-458.
Question 69
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
REFERENCES: Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Shin AY, Moran ME, Wenger DR: Superior gluteal artery injury secondary to posterior iliac crest bone graft harvesting: A surgical technique to control hemorrhage. Spine 1996;21:1371-1374.
Question 70
03 Which of the following findings is the best indication for the use of temporary external fixation of a femoral shaft fracture?

Explanation

These days, femoral shaft fractures at Tulane / Charity are commonly encountered by orthopaedic residents on the night-float team.
Despite the presence of a well-rested 4th year surgeon, definitive orthopaedic fixation is not always the correct answer for each trauma patient.

Tulane defines “Orthopaedic Tunnel Vision” as a condition commonly associated with a young MD at the Bulldog without a proper wing-man, trying to make advances on the wrong patron due to his relatively easy 80-hour work week schedule and a few too many refined hops.
Skeletal Trauma (p. 1967) describes “Orthopaedic Tunnel Vision” as looking at the orthopaedic injury without considering the patient’s injury in general. Femoral shaft fractures are typically high energy injuries which often do not occur in isolation. In these fractures, it is particularly important to not have tunnel vision.

Indications for temporary bridging external fixation includes hemodynamic instability
(ans. 2), acidosis, hypothermjia, hypoxemia, coagulopathy, sepsis or severely contaminated soft tissues that cannot be adequately debrided. Definitive fixation is performed after the general surgical and medical issues have resolved.

The other answer choices, including the type IIIA open fracture are not contraindications to definitive fixation in themselves (typically IM nailing—antegrade or retrograde).
Question 71
An 18-year-old male soccer player sustains a knee injury during a game. Examination is notable for a positive pivot shift test. What other physical examination finding is most likely to be present? Review Topic
Explanation
ACL tears usually occur as a result of a non-contact pivoting injury. Abnormal anterior translation results in bone contusions of mid-lateral femoral condyle and posterolateral tibia, which can be seen on MRI. Other concomitant intraarticular injuries include meniscal tears (lateral > medial), chondral damage and other ligamentous injury (MCL, LCL, PLC) usually found in cases of higher energy trauma such as a knee dislocation.
Piasecki et al prospectively analyzed intraarticular injuries associated with ACL tears in high school athletes by gender and sport. There was no significant difference in mechanism of injury between sexes. Female basketball and soccer players had fewer intraarticular injuries (medial femoral condyle lesions, medial and lateral meniscus tears) compared to male athletes. The authors hypothesized that women may therefore enjoy a better prognosis following reconstruction.
Spindler et al performed a prospective cohort study investigating concomitant intraarticular injuries in patients who underwent ACL reconstruction. Eighty percent of patients had a bone bruise on MRI, 68% involving the lateral condyle. At time of arthroscopic reconstruction, meniscal tears were identified in 56% of lateral menisci and 37% of medial menisci.
Incorrect Responses:
Question 72
What is the most important muscle adaptation resulting from endurance training? Review Topic
Explanation
Question 73
- A skeletal survey is more accurate than a bone scan for detecting skeletal involvement in which of the following neoplastic diseases?
Explanation
Question 74
A 59-year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Figure 1. Postreduction CT is shown in Figures 2 through 4. What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 75
Osteoporosis is best diagnosed by
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 141-154.
Question 76
A 35-year-old woman dislocated her right shoulder in a fall from a step stool several months ago. She now reports several painful recurrences. Examination reveals anterior and inferior apprehension that reproduces her symptoms. An MRI scan is shown in Figure 17. Management should consist of
Explanation
REFERENCES: Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Bokor DJ. Conboy VB. Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br
1999;81:93-96.
Coates MH, Breidahl W: Humeral avulsion of the anterior band of the inferior glenohumeral ligament with associated subscapularis bony avulsion in skeletally immature patients. Skeletal Radiol 2001;30:661-666.
Question 77
Figure 1 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder with loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in
Explanation
A. better glenoid exposure than with stemmed prostheses.
B. reliable use in four-part proximal humerus fracture reconstruction.
C. use in proximal humeral malunion without the need for an osteotomy.
D. improved long-term survivorship profile.
Question 78
A 25-year-old woman has had pain and stiffness in her knee following a motor vehicle accident 9 months ago. The radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 53a through 53d. What is the most likely diagnosis?
Explanation
REFERENCES: Horne LT, Blue BA: Intra-articular heterotopic ossification in the knee following intramedullary nailing of the fractured femur using a retrograde method. J Orthop Trauma 1999;13:385-388.
Stannard JP, Wilson TC, Sheils TM, McGwin G Jr, Volgas DA, Alonso JE: Heterotopic ossification associated with knee dislocation. Arthroscopy 2002;18:835-839.
Mills WJ, Tejwani N: Heterotopic ossification after knee dislocation: The predictive value of the injury severity score. J Orthop Trauma 2003;17:338-345.
Question 79
What is the most common type of malalignment after intramedullary nailing of distal 1/3 tibia fractures?

Explanation
McKee et al randomized 85 patients undergoing intramedullary tibial nailing using manual traction with the leg draped free versus standard fracture table positioning and traction. They found that manual traction is an effective technique that can save a significant amount of time without sacrificing the quality of reduction or fixation of tibial shaft fractures.
Question 80
The comparative outcomes of needle aponeurotomy (NA) and collagenase Clostridium histolyticum (CCH) use in the treatment of Dupuytren contracture indicate that patients treated with CCH have
Explanation
A. Proximal row carpectomy
B. Vascularized bone graft
C. Radial shortening osteotomy
D. Capitate shortening osteotomy
Osteonecrosis of the capitate is a rare condition that presents with an insidious onset of dorsal wrist pain. When nonsurgical treatment fails to alleviate symptoms, surgical intervention is appropriate. When collapse of the capitate is present, partial excision of the capitate with interposition, partial wrist arthrodesis, or wrist denervation can be considered. In the absence of collapse, capitate-preserving options are available. Vascularized grafting is a mainstay of treatment. Grafting with distal radius vascularized grafts based on the 1,2 intercompartmental supraretinacular artery or the 4 + 5 extensor compartment artery and second metacarpal graft based on the first dorsal metacarpal artery have been described.
Question 81
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?
Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 82
New painful paresthesias near the site of the incision after an ulnar nerve transposition is the result of injury to what nerve?
Explanation
REFERENCE: Dellon AL, Mackinnon SE: Injury to the medial antebrachial cutaneous nerve during cubital tunnel surgery. J Hand Surg Br 1985;10:33-36.
Question 83
What is the most appropriate orthotic management for the lesion shown in Figure 6?
Explanation
REFERENCE: Rudicel SA: Intractable plantar keratoses, in Gould J (ed): Operative Foot Surgery. Philadelphia, PA, WB Saunders, 1994, p 70.
Question 84
What is the structure indicated by the letter “A” in Figure A? Review Topic
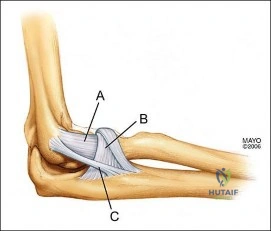
Explanation
Question 85
Figure 28 shows the postoperative radiograph of a 36-year-old patient. The cerclage cable was placed for a minimal medial calcar fracture seen during femoral preparation. In the immediate postoperative period, what is the highest level of activity that would be safely permitted?
Explanation
REFERENCES: Berend KR, Lombardi AV Jr, Mallory TH, et al: Cerclage wires or cables for the management of intraoperative fracture associated with a cementless, tapered femoral prosthesis: Results at 2 to 16 years. J Arthroplasty 2004;19:17-21.
Schmidt AH, Kyle RF: Periprosthetic fractures of the femur. Orthop Clin North Am 2002;33:143-152.
Greidanus NV, Mitchell PA, Masri BA, et al: Principles of management and results of treating the fractured femur during and after total hip arthroplasty. Instr Course Lect 2003;52:309-322.
Question 86
repair of the rotator cuff
Explanation
Question 87
A 12-year-old girl with juvenile rheumatoid arthritis (JRA) has had chronic pain and synovitis about the knee that is now well-controlled medically. Examination reveals 20° of valgus at the knee. Knee range of motion shows 10° to 90° of flexion. Treatment should consist of
Explanation
REFERENCE: Rydholm U, Brattstrom H, Bylander B, Lidgren L: Stapling of the knee in juvenile chronic arthritis. J Pediatr Orthop 1987;7:63-68.
Question 88
A patient with Pott's disease, tuberculosis of the spine, is more likely to have which of the following early findings? Review Topic
Explanation
Question 89
A 21-year-old female college athlete sustained a stress fracture of the fifth metatarsal 1 year ago which was treated successfully with surgical stabilization and she returned to normal activities. She now has a tension-sided femoral neck fracture. Along with surgical fixation of the fracture, what is the next step in management? Review Topic
Explanation
Question 90
A 17-year-old football player is tackled with an opposing player's helmet hitting him hard in the abdomen. He is knocked backwards and suffers a diaphyseal femur fracture. He denies any loss of consciousness. Vital signs reveal a heart rate of 118, mean arterial pressure (MAP) of 68, and a respiration rate of 32 per minute. A FAST ultrasound study shows trace free fluid in the perisplenic space. A CBC taken prior to bolus IV fluids reveals a hematocrit of 48%, and a blood gas shows a lactate level of 1.8 and a base excess of -2.0. Which of the follow statements regarding the patient's hemodynamic status is correct?
Explanation
Hypovolemic shock leads to poor tissue perfusion due to inadequate flow or oxygenation. If a patient is in compensated shock (i.e. normal vital signs), there may be ongoing inadequate perfusion of some end-organs. Elevated lactate or a base deficit are markers of poor end-organ perfusion, thus when normalized indicate appropriate end-organ perfusion even if vital sign derangements persist.
Rossaint et al. wrote a comprehensive review article in 2006 in which they discuss principles of fluid management, coagulopathy, hypothermia and tissue oxygenation in hypovolemic shock. In addition to prolonged elevated lactate levels correlating to mortality, lactate levels (or base deficits) can be used to evaluate for compensated shock in the setting of normal hemodynamic status.
Illustration A shows the classification of hypovolemic shock. Note the percent of blood loss required for vital sign abnormalities.
Incorrect Answers:
setting of massive blood loss. The hematocrit only changes once the patient has physiologic or iatrogenic fluid shifts in response to the blood loss. Answer 3: Vital sign derangements indicate uncompensated shock, but do not directly measure tissue perfusion or end-organ damage Answer 5: Though uncommon, bleeding from isolated femur fractures can lead to Class II shock (blood loss 15-30%)
Question 91
In Ewing’s sarcoma, neoplastic properties are thought to be related to a
Explanation
tumor cell proliferation include inactivation of tumor suppressor genes, or activation of proto-oncogenes.
REFERENCES: Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Pierz KA, Womer RB, Dormans JP: Pediatric bone tumors: Osteosarcoma Ewing’s sarcoma, and chondrosarcoma associated with multiple hereditary osteochondromatosis. J Pediatr Orthop 2001
;21:412- 418.
Question 92
Figures below depict the radiographs obtained from a 53-year-old man who has had swelling in his right knee for 2 years, with minimal pain. He did not note an injury to the knee but has been unable to ambulate without crutches during this period. His past history is unremarkable, and he denies a history of diabetes or back problems. The social history reveals that he emigrated from China, and he works at a desk job. Physical examination shows a healthy man in no acute distress. Range of motion of the right knee is 5° to 120° actively and 0° to 120° passively, without pain. Sensation is decreased on the bottom of both feet, but otherwise the neurologic examination is unremarkable. Laboratory testing reveals a positive rapid plasma reagin (RPR) test. What is the best next step?
Explanation
This patient has a neuropathic knee caused by neurosyphilis, as shown by the joint destruction on the radiographs, with a lack of pain and a positive RPR test. He has a low-demand job and would be best treated with a hinged knee arthroplasty to provide stability for his knee.
Question 93
Complications following a reverse shoulder prosthesis occur most frequently when performed for what diagnosis? Review Topic
Explanation
Question 94
An elderly woman with radiographic evidence of spinal stenosis reports difficulty walking and calf pain that is relieved by rest and a change of position. The most likely cause of pain is ischemia of the
Explanation
Question 95
-The Coleman block test is used to test for
Explanation

Question 96
During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?
Explanation
REFERENCES: Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
Wapner K, Pavlock GS, Hecht PJ, Naselli F, Walther R: Repair of chronic Achilles tendon rupture with flexor hallucis longus tendon transfer. Foot Ankle Int 1993;14:443-449.
Question 97
Avascular necrosis
Explanation
A 9-year-old girl sustains an injury (Slide) as a result of a fall. What is her risk of avascular necrosis:
Question 98
A 30-year-old accountant and recreational softball player, who is seen at the end of his baseball season, reports a several month history of pain along the medial side of his dominant elbow. He cannot identify a specific injury and notes it only hurts when he throws the ball in from the outfield. Besides the pain, he remarks that his speed and distance while throwing have diminished considerably. Examination reveals tenderness along the medial elbow but no weakness or gross instability is found. Radiographs are normal. Based on the history, what is the most likely diagnosis? Review Topic
Explanation
the forearm during resisted forearm pronation and is not associated with the throwing motion in particular. Valgus extension overload may mimic medial collateral ligament injury, not varus extension injuries. Medial epicondylitis may be confused with ligament insufficiency but the examination and a history of pain only while throwing make this an unlikely diagnosis.
Question 99
-Figures 156a and 156b are the radiographs of a 38-year-old man with diabetes mellitus who fell 8 feet from a ladder and sustained an isolated closed injury of his leg. Examination revealed swollen but soft compartments. His neurovascular examination was unremarkable. A damage-control fixator was initially applied, and his soft-tissue envelope is now amenable to further intervention. What is the most appropriate treatment?
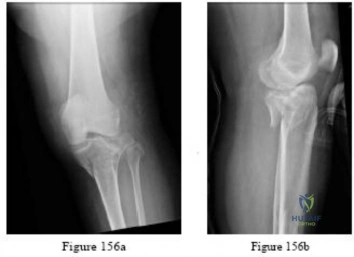
Explanation

Question 100
The dominant arterial blood supply to the patella enters at which anatomical location?
Explanation
The arterial blood supply to the patella is made up of branches of six main arteries: the descending genicular, the superior medial and lateral genicular, the inferior medial and lateral genicular, and the anterior genicular. Several of these branches contribute to the anastomotic network that surround the patella. From the ring, there are two main interosseous blood supply systems to enter the patella, known as the midpatellar and polar vessel systems. The distal pole of the patella is considered to be the largest arterial contribution to the peripatellar ring and the polar vessel system.
Lazaro et al. used twenty matched pairs of fresh-frozen cadaveric knees to isolate the dominant blood supply to the patella. After cannulating the superficial femoral artery, anterior tibialis artery, and posterior tibialis artery and performing magnetic resonance imaging, they found that the largest arterial contribution to the patella entered at the inferior pole in 100% of the specimens. In sixteen specimens (80%), the dominant artery entered the medial aspect of the distal pole. In three specimens (15%), it entered the lateral aspect of the distal pole.
Illustation A shows the arterial supply system to the patella. The dominant arterial supply enters at the distal (inferior) pole of the patella, with the dominant geniculate arteries entering inferomedially (labelled with a green star). Illustration B shows an anatomical illustration of the patellar blood supply. Note the dominant distal pole blood supply (arrow).
Incorrect Answers:
