Orthopedic MCQ Exam: Trauma, Arthroplasty, Foot & Ankle | Part 38

Key Takeaway
This interactive quiz is for orthopedic surgeons and residents preparing for OITE & ABOS board exams. It features 100 high-yield, verified MCQs, mirroring AAOS exam formats. Benefit from study/exam modes and detailed clinical explanations to ace your certification.
About This Board Review Set
This is Part 38 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 38
This module focuses heavily on: Ankle, Arthroplasty, Foot, Fracture, Hip, Infection, Trauma.
Sample Questions from This Set
Sample Question 1: Figure 14 is a sagittal-cut MR image from the hindfoot of a 54-year-old woman who has had plantar heel pain for 3 months. There is no history of trauma. Her pain is worse when she rises and at the end of the day. Upon examination she has lo...
Sample Question 2: A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion,...
Sample Question 3: A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?...
Sample Question 4: A patient with a grade 2 L5-S1 isthmic spondylolisthesis reports low back pain and bilateral lower extremity pain. Nonsurgical management has failed to provide relief, and the patient is now a candidate for surgical intervention. The...
Sample Question 5: Hip pain of 1-month duration has developed in a 72-year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
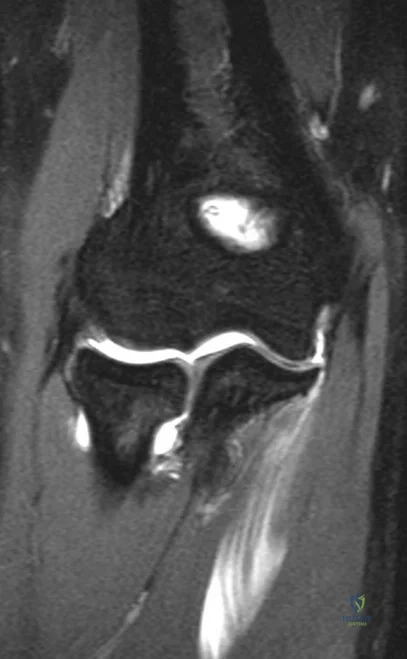
Figure 14 is a sagittal-cut MR image from the hindfoot of a 54-year-old woman who has had plantar heel pain for 3 months. There is no history of trauma. Her pain is worse when she rises and at the end of the day. Upon examination she has localizable tenderness over the plantar medial tubercle of the calcaneus. The Achilles is intact and nontender, and subtalar joint motion is full and painless. A Tinel test result is negative. What is the most likely diagnosis?

Explanation
Plantar fasciitis is inflammation of the plantar fascia at its insertion onto the medial calcaneus. The T2-weighted sagittal MR image reveals thickening of the plantar fascia with no evidence of a calcaneal stress fracture, coalition, or inflammation of the insertion of the Achilles tendon.
RECOMMENDED READINGS
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
Question 2
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?
Explanation
REFERENCES: Calvert E, Younger A, Penner M: Post talus neck fracture reconstruction.
Foot Ankle Clin 2007;12:137-151.
Migues A, Solari G, Carrasco NM, et al: Repair of talar neck nonunion with indirect corticocancellous graft technique: A case report and review of the literature. Foot Ankle Int 1996;17:690-694.
Question 3
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?
Explanation
REFERENCES: Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
Question 4
A patient with a grade 2 L5-S1 isthmic spondylolisthesis reports low back pain and bilateral lower extremity pain. Nonsurgical management has failed to provide relief, and the patient is now a candidate for surgical intervention. The
Explanation
Question 5
Hip pain of 1-month duration has developed in a 72-year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's prognosis for infection resolution?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin-resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was 21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 6
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle?
Explanation
REFERENCES: Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop Relat Res 1999;368:17 -27.
Warner JJ, Navarro RA: Serratus anterior dysfunction: Recognition and treatment. Clin Orthop Relat Res 1998;349:139-148.
Question 7
A 14-year-old gymnast presents after a fall from the balance beam with a hyperextension injury to her left knee. She could ambulate with pain but was unable to continue exercise due to pain. On examination she has a swollen knee with painful

Explanation
Tibial eminence fractures are rare but occur more often in pediatric populations, often in the setting of sports-related injuries. Debate continues over operative vs nonoperative treatment, as well as fixation type (screw vs suture) for openly treated fractures. Past evidence suggested closed treatment was adequate but there has been an increase in operative management. Closed treatment is suggested for minimally displaced fractures (Type I and reducible Type II) and open treatment for completely displaced fractures (non-reducible Type II and Type III).
Wilfinger et al provide the results of a closed reduction protocol at their institution including 38 patients with long term followup. All patients underwent aspiration and closed reduction in the OR under fluoroscopic guidance followed by long leg casting in hyperextension and graduated weight bearing over weeks. No patients complained of persistent pain, swelling, giving way, or disability at follow up.
However, Edmonds et al in a retrospective review compare open reduction internal fixation (ORIF), arthroscopic-assisted internal fixation (AAIF), and closed reduction with casting (CRC) for pediatric patients with displaced tibial spine fractures. They report improved reduction but also increased arthrofibrosis in ORIF and AAIF groups
compared to CRC, but of the 24% of patients with long term followup results, there was no difference in functional outcomes across all 3 groups. There was a 17% rate of later operation for the CRC group patients. They suggest closed treatment for fractures with <5mm displacement, otherwise ORIF or AAIF.
Gans et al conducted a systematic review focused on the questions of open vs closed reduction, and screw vs suture fixation. The 26-article review found insufficient evidence to have any clear recommendations. They did find reduced laxity and improved range of motion for minimally displaced fractures that had an open reduction, and that completely displaced fractures treated nonoperative had higher rates of nonunion.
Figures A and B are AP and lateral knee radiographs demonstrating a moderately displaced (Meyers and McKeever Type II) tibial spine fracture in a skeletally immature patient.
Incorrect Responses
Question 8
A 10-year-old boy reports a gradual onset of weakness; however, he is fully ambulatory. History reveals that he has a 17-year-old brother who has just stopped walking because of a similar condition. Laboratory studies show a creatine kinase level of 5,480 IU/L (normal 25 to 232 IU/L), and examination shows a slightly positive Gower sign. What is the most likely diagnosis?
Explanation
REFERENCES: Matsuo M: From molecular diagnosis to gene therapy. Brain Dev 1996;18:167-172.
Darras BT: Molecular genetics of Duchenne and Becker muscular dystrophy. J Pediatr 1990;117:1-15.
Gutmann DH, Fischbeck KH: Molecular biology of Duchenne and Becker’s muscular dystrophy: Clinical applications. Ann Neurol 1989;26:189-194.
Question 9
An otherwise healthy year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?
Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 10
A patient who underwent primary total hip arthroplasty 7 years ago that resulted in excellent pain relief and a normal gait now reports pain and a limp. Postoperative and current AP radiographs are shown in Figures 2a and 2b. What is the most likely cause of the pathology seen?
Explanation
REFERENCES: Claus MC, Hopper RH, Engh CA: Fractures of the greater trochanter induced by osteolysis with the anatomic medullary locking prosthesis. J Arthroplasty 2002;17:706-712.
Heekin RD, Engh CA, Herzwurm MF: Fractures through cystic lesions of the greater trochanter: A cause of late pain after cementless total hip arthroplasty. J Arthroplasty 1996;11:757-760.
Question 11
A 70-year-old healthy man had total knee arthroplasty 18 years ago, and it now is painful. Radiographs reveal aseptic loosening and the range of motion before surgery is 15 to 85 degrees. The strongest indication for performing a tibial tubercle osteotomy to aid in exposure in his knee would be
Explanation

Question 12
A 19-year-old collegiate lacrosse player has bilateral lower extremity pain during training runs and practice sessions. She says her pain is only associated with activity, always begins 4 to 5 minutes into an activity, and resolves within 10 minutes after activity cessation. She reports a feeling of numbness and tingling in her first- and second-toe web space with continued activity. She has no pain while at rest and has tried nonsteroidal anti-inflammatory drugs, ice baths, and rehabilitation techniques with her athletic trainers without experiencing noticeable changes. Which test has the highest specificity and sensitivity for the pathology suspected?
Explanation
Chronic exertional compartment syndrome (CECS) is an uncommon cause of pain that is most often encountered in athletes or military populations. The diagnosis is suggested by pain after the start of the activity with resolution of symptoms when the activity stops. Traditionally, the diagnosis was established by measuring intracompartment pressures at 1 and 5 minutes of
activity. Roscoe and associates have shown that using continuous pressure monitoring during the activity until pain forces subjects to stop provides higher sensitivity and specificity than the traditional diagnostic technique. Palpating the leg is not as sensitive or specific as direct pressure monitoring. Although certain changes can be seen on MRI in CECS, this is not the diagnostic study of choice.
Question 13
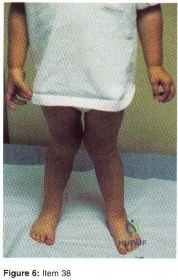
- Item Deleted by AAOS Question 38 - Figure 6 shows the clinical photograph of a 3-year-old boy who started to walk at the age of 10 months and has a gait that is appropriate for his age. His height is in the 40th percentile for his age. Management should consist of
Explanation
The correct treatment for children with physiologic genu valgum up to six years of life is OBSERVATION, if the condition persists past six years standing AP radiographs and a metabolic work-up are indicated. Because response (1) is the only answer not including x-rays, this is the one you should have selected.
Question 14
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
Explanation
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 115-140.
Beaule PE, Dorey FJ, Matta JM: Letournel classification of acetabular fractures: Assessment of interobserver and intraobserver reliability. J Bone Joint Surg Am 2003;85:1704-1709.
Question 15
A 72-year-old woman with rheumatoid arthritis who underwent primary total knee arthroplasty 2 years ago has had diffuse knee pain that developed shortly after the surgery. The patient has difficulty with stair descent and arising from chairs. Evaluation for infection is negative. AP and lateral radiographs are shown in Figure 26. Management should now consist of
Explanation
REFERENCES: Pagnano MW, Hanssen AD, Lewallen DG, Stuart MJ: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.
Fehring TK, Odum S, Griffin WL, Mason B, Nadaud M: Early failures of total knee arthroplasty. Clin Orthop 2001;392:315-318.
Question 16
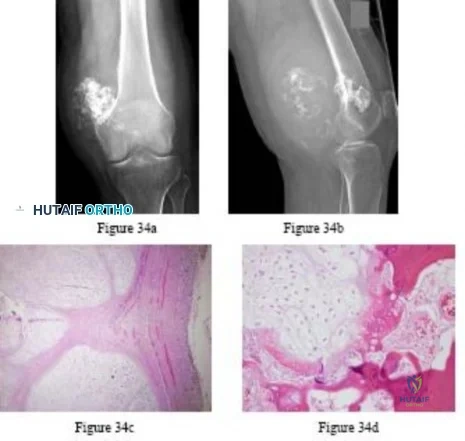
A 30-year-old patient has wrist pain. A radiograph and biopsy specimen are shown in Figures 34a and 34b. What is the most likely diagnosis?
Explanation
REFERENCES: Bieselker JL, Marcove RC, Huvos AG, Mike V: Aneurysmal bone cyst: A Clinico-pathologic study of 66 cases. Cancer 1973;26:615.
Martinez V, Sissons HA: A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291.
Question 17
A 72-year-old female presents to your office with a 24-month old painful nonunion of a 3-part fracture of the proximal humerus. She has been treated conservatively with range of motion exercises but continues to complain of debilitating pain and dysfunction. Operative management should include:

Explanation
The referenced article by Cheung et al reviews treatment options for proximal humeral nonunions and reports successful use of arthroplasty in treating elderly osteoporotic proximal humeral nonunions as a pain relieving procedure.
Dines reported a case series of 20 chronic post-traumatic proximal humerus fractures including nonunions that were treated with shoulder arthroplasty achieving fair to excellent results in 90% at mid-term follow-up
Question 18
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show
Explanation
REFERENCES: Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin
Bernhardt DT, Landry GL: Sports injuries in young athletes. Adv Pediatr 1995;42:465- Sports Med 1999;18:109-171.
Brown HR, Indelicato PA: Complications of anterior cruciate ligament reconstruction. Op Tech Orthop 1992;2:125-135.
Question 19
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
REFERENCES: Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393.
Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Kostuik JP, Valdevit A, Chang HG, et al: Biomechanical testing of the lumbosacral spine. Spine 1998;23:1721-1728.
Question 20
Which of the following clinical findings is commonly associated with symptomatic partial-thickness rotator cuff tears?
Explanation
REFERENCES: Hertel R, Ballmer FT, Lambert SM, Gerber C: Lag signs in the diagnosis of rotator cuff rupture. J Shoulder Elbow Surg 1996;5:307-313.
McConville OR, Iannotti JP: Partial thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43.
Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Fukuda H: Partial-thickness rotator cuff tears: A modern view on Codman’s classic. J Shoulder Elbow Surg 2000;9:163-168.
Question 21
The difference between vitamin D-dependent rickets type I (VDDR I) and vitamin D-dependent rickets type II (VDDR II) is
Explanation
VDDR I is a deficiency of 1a-hydroxylase [converts 25(OH)D to 1a,25(OH)2D3].
Lab tests show hypocalcemia, secondary hyperparathyroidism, elevated alkaline phosphatase (ALP) and low or undetectable calcitriol in the presence of adequate 25(OH)D levels. VDDR II or hereditary vitamin D resistant rickets (HVDRR) (autosomal recessive) is an inactivating mutation in the vitamin D receptor (VDR). Lab tests show low serum calcium and phosphate, elevated ALP and secondary hyperparathyroidism. Serum 25(OH)D values are normal and the 1,25(OH)2D levels are elevated (key difference from VDDR I).
Malloy et al. reviewed genetic disorders in vitamin D action. They state that VDDR I is an inborn error of vitamin D metabolism coded by the gene CYP27B1. Children with VDDR I present with joint pain/deformity, hypotonia, muscle weakness, growth failure, and hypocalcemic seizures or fractures in early infancy. Treatment is with calcitriol or 1a-hydroxyvitamin D (NOT cholecalciferol). Children with VDDR II present with bone pain, muscle weakness, hypotonia, hypocalcemic convulsions, growth retardation, severe dental caries or teeth hypoplasia. Affected children are resistant to therapy and supra-physiologic doses of all forms of vitamin D.
Illustration A shows the differences between VDDR I and VDDR II. Incorrect Answers
in the kidney). The liver enzyme vitamin D 25-hydroxylase (found in hepatocytes) is not responsible for VDDR. VDDR II is caused by an inactivating mutation (rather than an activating mutation).
Question 22
An 18-year-old football player sustains a contact injury to his right lower leg, and radiographs show a closed transverse fracture of the middle third of the tibia. Based on the clinical examination, a compartment syndrome is suspected. When measuring compartment pressures, the highest tissue pressure is recorded how many centimeters proximal or distal to the fracture site?
Explanation
REFERENCES: Heckman MM, Whitesides TE Jr, Grewe SR, Rooks MD: Compartment pressure in association with closed tibial fractures: The relationship between tissue pressure, compartment, and the distance from the site of the fracture. J Bone Joint Surg Am 1994;76:1285-1292.
Whitesides TE Jr, Heckman MM: Acute compartment syndrome: Update on diagnosis and treatment. J Am Acad Orthop Surg 1996;4:209-218.
Question 23
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of
Explanation
REFERENCES: Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 24
An elderly woman with radiographic evidence of spinal stenosis reports difficulty walking and calf pain that is relieved by rest and a change of position. The most likely cause of pain is ischemia of the
Explanation
Question 25
Figures 18a and 18b show the radiographs of a 13-year-old baseball player who sustained a patellar dislocation with an associated lateral femoral condyle fracture. What ligament is attached to this fragment?
Explanation
REFERENCES: Jobe CM, Wright M: Anatomy of the knee, in Fu FH, Harner CD, Vince KG (eds): Knee Surgery. Baltimore, MD, Williams & Wilkins, 1994, pp 1-54.
Moore KL, Dalley AF: Lower limb, in Moore KL, Dalley AF (eds): Clinically Oriented Anatomy, ed 4. Philadelphia, PA, Lippincott, Williams & Wilkins, 1999, pp 503-664.
Question 26
03 A 28-year-old man underwent surgical fixation for an intra-articular distal humeral fracture 8 weeks ago now reports progressively restricted elbow motion. Radiographs at the time of union are shown in Figures 13a and 13b. Management should now consist of
Explanation
delayed until the heterotopic ossification was “mature”. This was signified by a cold bone scan and normal serum alk phos, as well as a mature appearance on xray. It was thought that by waiting until the HO was mature, recurrence would be avoided. However, in the cited reference, out of the widely read Journal of Hand Surgery, the authors obtained good results with increased range of motion, resolution of cubital tunnel syndrome and no recurrence of contractures or loss of motion with excision of ectopic bone and elbow release that was performed once bony union of fracture was obtained. They also used a 5 day course of indomethacin post-op.
back to this question next question
Question 27
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245.
Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Thometz JG, Gould JS: Cavus deformity, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 28
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?
Explanation
REFERENCES: Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Lemos MJ, Albert J, Simon T, et al: Radiographic analysis of femoral interference screw placement during ACL reconstruction: Endoscopic versus open technique. Arthroscopy 1993;9:154-158.
Question 29
A 30-year-old man who sustained a work-related injury 6 weeks ago reports persistent back and left-sided buttock pain that has been attributed to lumbar transverse process fractures. A pelvic radiograph and CT scans obtained 2 days ago are seen in Figures 17a through 17c. What is the best treatment for his injury?
Explanation
REFERENCES: Mears DC: Management of pelvic pseudarthroses and pelvic malunion. Orthopade 1996;25:441-448.
Matta JM, Dickson KF, Markovich GD: Surgical treatment of pelvic nonunions and malunions. Clin Orthop Relat Res 1996;329:199-206.
McLaren AC, Rorabeck CH, Halpenny J: Long-term pain and disability in relation to residual deformity after displaced pelvic ring fractures. Can J Surg 1990;33:492-494.
Question 30
A 23-year-old national team rower reports pain over the radial dorsum of the forearm that is made worse with flexion and extension of the wrist during competition. His primary physician initially diagnosed de Quervain’s tenosynovitis, and a subsequent corticosteroid injection into the first dorsal compartment at the wrist provided no relief. The patient continues to report pain and audible crepitus that is noted 5 cm proximal to the wrist joint, on the radial aspect. What structures are involved in the continued pathology?
Explanation
REFERENCES: Grundberg AB, Reagan DS: Pathologic anatomy of the forearm: Intersection syndrome. J Hand Surg Am 1985; 10:299-302.
Thorson E, Szabo RM: Common tendinitis problems in the hand and forearm. Orthop Clin North Am 1992;23:65-74.
Williams JG: Surgical management of traumatic non-infective tenosynovitis of the wrist extensors. J Bone Joint Surg Br 1977;59:408-410.
Wood MB, Dobyns JH: Sports-related extraarticular wrist syndromes. Clin Orthop Relat Res 1986;202:93-102.
Question 31
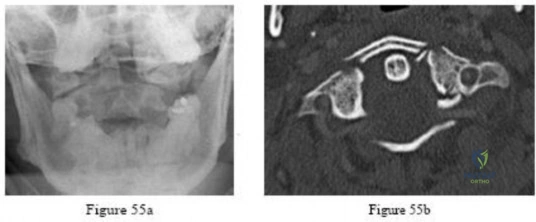
-Figures 55a and 55b are the radiograph and CT scan of a 61-year-old woman who has had neck pain after being involved in a high-speed motor vehicle collision. Examination reveals normal strength and sensation in both upper and lower extremities, normal rectal tone, and no other injuries. The C1-C2 lateral mass overhang measures 8.5 mm. What is the most appropriate treatment option?
Explanation

Question 32
Accurate evaluation of the upper portion of the subscapularis muscle is best accomplished with active internal rotation
Explanation
REFERENCES: Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ: Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 1998;26:210-220.
Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 33
below depict the radiographs obtained from a year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 34
Osteoporotic vertebral compression fractures are associated with
Explanation
REFERENCES: Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Lindsay R, Silverman SL, Cooper C, et al: Risk of new vertebral fracture in the year following a fracture. JAMA 2001;285:320-323.
Kado DM, Duong T, Stone KL, et al: Incident vertebral fractures and mortality in older women: A prospective study. Osteoporos Int 2003;14:589-594.
Question 35
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?
Explanation
inlay reconstruction.
REFERENCES: Berg EE: Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy 1995;8:95-99.
Burks RT, Schaffer JJ: A simplified approach to the tibial attachment of the posterior cruciate ligament. Clin Orthop 1990;254:216-219.
Question 36
Figures below show the radiographs obtained from a 90-year-old woman who is seen in the emergency department after a fall from a height. She has right hip and thigh pain and is unable to bear weight. Based on this patient's history and imaging, what is the best next step?

Explanation
Periprosthetic fracture is the third most common reason (after loosening and infection) for revision surgery after total hip arthroplasty (THA). Late periprosthetic fracture risk is 0.4% to 1.1% after primary
THA and 2.1% to 4% after revision THA. Risk factors for periprosthetic fracture include age over 70 years, decreasing bone mass, and loosening of implants and osteolysis. The risk of concomitant infection in the presence of a periprosthetic fracture is 11%, according to Chevillotte and associates. Obtaining presurgical aspiration or intrasurgical tissue for culture is recommended if concomitant infection is suspected.
Question 37
A 24-year-old female soccer player has had lateral joint line pain and a recurrent effusion in the left knee after sustaining a twisting injury 6 weeks ago. She reports that symptoms worsen with athletic activities. MRI scans are shown in Figures 2a through 2c. What is the most likely diagnosis?
Explanation
REFERENCES: Jordan MR: Lateral meniscal variants: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:191-200.
Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 625-630.
Question 38
In revision total hip arthroplasty, an acetabular reconstruction cage is best indicated for which of the following patterns of bone loss?
Explanation
REFERENCES: Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 39
A 45-year-old woman with grade II adult-acquired flatfoot deformity has pain on the lateral side of her foot just distal to the tip of the fibula. Which component of a comprehensive flatfoot reconstruction most likely will address the deformity responsible for this pain?
Explanation
Patients develop lateral ankle pain with progression of adult-acquired flatfoot deformity. This is associated with increased hindfoot valgus deformity. Calcaneal fibular impingement has been considered the primary cause of this pain. Studies demonstrate that arthrosis of the posterior facet of the subtalar joint strongly correlates with lateral pain in adult-acquired flatfoot deformity. Both conditions are related to hindfoot valgus deformity. Although lateral column lengthening is a powerful tool for correction of flatfoot deformity, its effect on hindfoot deformity is less defined. Lateral column lengthening provides better correction of the longitudinal arch of the midfoot and realignment of the medial column than other osteotomies. A medializing calcaneal osteotomy has a significant linear effect on hindfoot valgus alignment. Spring ligament reconstruction and medial cuneiform opening-wedge osteotomies have less effect on hindfoot alignment than the medial calcaneal slide.
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
Question 40
An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?
Explanation
REFERENCES: Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
Modabber M, Jupiter JB: Operative management of diaphyseal fractures of the humerus: Plate versus nail. Clin Orthop 1998;347:93-104.
Question 41
A 52-year-old woman has right hip pain and obvious swelling 3 years after undergoing a resurfacing arthroplasty. Her implant consists of a 42-mm femoral component and 48-mm socket. Her components are well positioned, and her metal ion levels are slightly elevated (less than 4 ppm) with a normal erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level. What is the most likely cause of her discomfort?
Explanation
This patient likely has a soft-tissue reaction (pseudotumor) related to metal-on-metal articulation. Although the components are well positioned, patient gender and small head size are both known risk factors for failure of hip resurfacing arthroplasties. Metal ion levels are elevated but are not always markedly increased in the setting of a problematic metal-on-metal articulation. The patient should have a metal artifact reduction sequence MR imaging study to confirm the presence of a pseudotumor. Chronic infection is very unlikely in the setting of normal ESR and CRP findings. Impingement and lumbar disk disease would not explain the swelling around the hip.
Question 42
Figure 6 shows the radiograph of a 14-year-old baseball player who felt a pop and had an immediate onset of pain in his elbow after a hard throw from the outfield. The best course of action should be to
Explanation
REFERENCES: Case SL, Hennrikus WL: Surgical treatment of displaced medial epicondyle fractures in adolescent athletes. Am J Sports Med 1997;25:682-686.
Woods GW, Tullos HS: Elbow instability and medial epicondyle fractures. Am J Sports Med 1977;5:23-30.
Question 43
What is a common clinical finding in patients with severe hypercalcemia secondary to bony metastasis?
Explanation
REFERENCE: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 44
In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of
Explanation
REFERENCES: Zeitlin L, Fassier F, Glorieux FH: Modern approach to children with osteogenesis imperfecta. J Pediatr Orthop B 2003;12:77-87.
Falk MJ, Heeger S, Lynch KA, et al: Intravenous bisphosphonate therapy in children with osteogenesis imperfecta. Pediatrics 2003;111:573-578.
Glorieux FH, Bishop NJ, Plotkin H, et al: Cyclic administration of pamidronate in children with severe osteogenesis imperfecta. N Engl J Med 1998;339:947-952.
Question 45
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
REFERENCES: Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 46
A 45-year-old male falls off his motorcycle and injures his arm. AP and lateral radiographs reveal an ulnar shaft fracture, 30 degrees apex anterior, and a radial head dislocation. Which direction is the radial head most likely dislocated?

Explanation
Question 47
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study results fits the definition of chronic prosthetic joint infection?
Explanation
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
Question 48
What is the most common complication following surgery for a "terrible triad" elbow fracture-dislocation?
Explanation
Question 49
When considering a flexor digitorum longus tendon transfer as part of the surgical treatment in patients with symptomatic flatfoot deformity caused by posterior tibial tendon insufficiency, which of the following patients is the most appropriate candidate?
Explanation
REFERENCES: Pedowitz WJ, Kovatis P: Flatfoot in the adult. J Am Acad Orthop Surg 1995;3:293-302.
Mann RA: Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 167-296.
Question 50
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
REFERENCES: Montgomery DM, Brower RS: Cervical spondylotic myelopathy: Clinical syndrome and natural history. Orthop Clin North Am 1992;23:487-493.
Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K: Myelopathy hand: New clinical signs of cervical cord damage. J Bone Joint Surg Br 1987;69:215-219.
An HS, Simpson JM: Surgery of the Cervical Spine. Baltimore, MD, Williams and
Wilkins, 1994.
Question 51
Which surgical procedure should be considered for treatment of chronic plantar fasciitis?
Explanation
Imaging studies in the evaluation of plantar fasciitis should always include weight-bearing foot radiographs to reveal alignment and exclude calcaneal stress fracture, tumor, subtalar arthritis, and insertional posterior spurs. MRI is occasionally indicated in problematic cases. Ultrasound can be helpful to evaluate thickening and disease in the proximal plantar fascia. Ultrasound is quick and much more cost effective than MRI. Laboratory screenings to evaluate inflammatory arthritis are indicated only for patients with bilateral heel pain who may be more likely to have systemic disease.
In the nonsurgical treatment of plantar fasciitis, high-impact loading exercises may make the condition worse. Corticosteroid injections may provide short-term relief only and can occasionally cause plantar fascia rupture. They should be used with caution. PRP injections are expensive and currently not covered by insurance. Studies have not demonstrated long-term pain relief with PRP. Plantar fascia-specific stretching has been shown more effective than Achilles tendon stretching alone.
Surgical treatment is indicated for fewer than 5% of patients. It is not necessary to resect the heel spur because the spur is not attached to the plantar fascia and rarely contributes to a patient's pain. The open extensile approach is associated with a much longer recovery than the open or endoscopic approaches and is no longer justified. Multiple studies have demonstrated the efficacy of endoscopic and open plantar fasciotomy techniques.
RECOMMENDED READINGS
Bader L, Park K, Gu Y, O'Malley MJ. Functional outcome of endoscopic plantar fasciotomy. Foot Ankle Int. 2012 Jan;33(1):37-43. doi: 10.3113/FAI.2012.0037. PubMed PMID:
Question 52
A 51-year-old woman who underwent a total knee arthroplasty 14 months ago for severe degenerative arthritis now reports progressive pain, swelling, and buckling of the knee. She must use crutches and is unable to negotiate stairs. Laboratory testing reveals a normal erythrocyte sedimentation rate and C-reactive protein. Radiographs of the patient are shown in Figures 17a through 17c. What is the most important test to further evaluate this problem?
Explanation
REFERENCES: Stiehl JB: Patellar instability in total knee arthroplasty. J Knee Surg 2003;16:229-235. Berger RA, Crossett LS, Jacobs JJ, et al: Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res 1998;356:144-153.
Question 53
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 3-23.
Question 54
Which of the following is considered a specific advantage of using COX-2 inhibitors over COX-1 inhibitors?
Explanation
REFERENCES: Lane JM: Anti-inflammatory medications: Selective COX-2 inhibitors. J Am Acad Orthop Surg 2002;10:75-78.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000.
Question 55
Figure 1 is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence?

Explanation
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision (Figures below) is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.

Question 56
Tension band wire fixation is best indicated for which of the following types of olecranon fractures?
Explanation
Question 57
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?
Explanation
REFERENCES: Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-807.
Garfin SR, Rauschning W: Spinal stenosis. Instr Course Lect 2001;50:145-152.
Question 58
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Explanation
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Question 59
A 56-year-old man who tripped and fell out of his golf cart onto his right shoulder 4 days ago now reports mild pain while chipping. Examination reveals mild bruising over the lateral clavicle but good shoulder range of motion and strength. A radiograph is shown in Figure 9. Appropriate treatment at this time should include which of the following?

Explanation
Question 60
Figure 10 shows the radiograph of a 7-year-old patient who has a bilateral Trendelenburg limp and limited range of hip motion but no pain. His work-up should include
Explanation
REFERENCES: Crossan JF, Wynne-Davies R, Fulford GE: Bilateral failure of the capital femoral epiphysis: Bilateral Perthes disease, multiple epiphyseal dysplasia, pseudoachondroplasia, and spondyloepiphyseal dysplasia congenita and tarda. J Pediatr Orthop 1983;3:297-301.
Sponseller PD: The skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 269-270.
Question 61
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of
Explanation
REFERENCES: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Asnis SE, Wanek-Sgaglione L: Intracapsular fractures of the femoral neck: Results of cannulated screw fixation. J Bone Joint Surg 1994;76A:1793-1803.
Question 62
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following? Review Topic
Explanation
the restraints to medial translations of the biceps have been disrupted. Attempts at recentering the biceps have not been successful, and clinical results appear to be improved when tenodesis or tenotomy is employed in the treatment of the unstable biceps associated with subscapularis tears.
Question 63
A 24-year-old woman was struck by a mini van in a parking lot and sustained a closed segmental tibia fracture that was treated with an intramedullary nail the following morning. Follow-up examinations reveal a slowly progressive clawing of all five toes, a progressive equinocavovarus contracture, and the patient is unable to perform a single heel rise on the affected limb. At 1 year after surgery, the patient now has a 10-degree equinus contracture that is not relieved with knee flexion. Treatment should now consist of
Explanation
REFERENCES: Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 212-213.
Manoli A II, Smith DG, Hansen ST Jr: Scarred muscle excision for the treatment of established ischemic contracture of the lower extremity. Clin Orthop Relat Res 1993;292:309-314.
Early JS, Ricketts DS, Hansen ST: Treatment of compartmental liquefaction as a late sequelae of a lower limb compartment syndrome. J Orthop Trauma 1994;8:445-448.
Question 64
A 78-year-old woman underwent total hip arthroplasty 15 years ago. She reports a recent history of increasing thigh pain prior to a fall and is now unable to ambulate. Radiographs are shown in Figures 87a and 87b. What is the best treatment for this condition?
Explanation
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Kwong LM, Miller AJ, Lubinus P: A modular distal fixation option for proximal bone loss in revision total hip
arthroplasty: A 2- to 6-year follow-up study. J Arthroplasty 2003;18:94-97.
Question 65
Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?
Explanation
REFERENCES: Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.
Kim YH, Kim JS, Oh SW: Total knee arthroplasty in neuropathic arthropathy. J Bone Joint
Surg Br 2002;84:216-219.
Question 66
A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the clavicle distal to a line drawn vertically to the coracoid process. Management should consist of
Explanation
REFERENCES: Robinson CM, Cairns DA: Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-782.
Deafenbaugh MK, Dugdale TW, Staeheli JW, et al: Nonoperative treatment of Neer type II distal clavicle fractures: A prospective study. Contemp Orthop 1990;20:405-413.
Question 67
A 15-year-old girl has had a painful mass on the medial aspect of her left thigh for the past 5 years. The pain is present only when she is performing athletic activities and is completely relieved with rest. A radiograph and MRI scan are shown in Figures 29a and 29b. The patient and her parents would like to have the mass removed. What further diagnostic studies are required prior to considering surgical resection?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Murphey MD, Choi JJ, Kransdorf, MJ, et al: Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-1434.
Question 68
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient? Review Topic
Explanation
Question 69
Based on the radiographic findings shown in Figure 41, which of the following wrist ligaments is most likely disrupted?
Explanation
REFERENCES: Linscheid RL, Dobyns JH, Beabout JW, et al: Traumatic instability of the wrist: Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632.
Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Berger RA: Ligament anatomy, in Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist, Diagnosis and Operative Management. St Louis, MO, Mosby, 1998, pp 73-105.
Question 70
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
REFERENCE: CA, January/February 2000, vol 50, no. 1 (Cancer Statistics).
Question 71
What range of motion parameters are required for a patient with posttraumatic elbow stiffness to accomplish all the normal activities of daily living?
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Morrey BF, Askew LJ, Chao EY: A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 1981;63:872-877.
Question 72
Figures 28a and 28b show the sagittal and axial lumbar MRI scans of a 72-year-old man who reports dull aching back pain that spreads to his legs, calves, and buttocks. He has had the pain for several years and it is precipitated by standing and walking and relieved by sitting. His symptoms have been worsening over the past year and he notes that he is leaning forward while walking to help relieve his symptoms. He has had no treatment to date. What is his prognosis if he chooses to pursue nonsurgical management for this condition?
Explanation
REFERENCES: Amundsen T, Weber H, Nordal HJ, et al: Lumbar spinal stenosis: Conservative or surgical management? A prospective 10-year study. Spine 2000;25:1424-1435.
Hilibrand AS, Rand N: Degenerative lumbar stenosis: Diagnosis and management. J Am Acad Orthop Surg 1999;7:239-249.
Tadokoro K, Miyamoto H, Sumi M, et al: The prognosis of conservative treatments for lumbar spinal stenosis: Analysis of patients over 70 years of age. Spine 2005;30:2458-2463.
Question 73
A 62-year-old man has cervical myelopathy with no evidence of cervical radiculopathy. MRI reveals stenosis at C4-5 and C5-6 with severe cord compression. Examination will most likely reveal which of the following findings?
Explanation
REFERENCES: Sachs BL: Differential diagnosis of neck pain, arm pain and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 741-742.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 673-680.
Question 74
An 18-year-old man underwent open reduction and internal fixation of a tibial spine avulsion and a posterolateral corner repair. Two years later, he underwent lateral collateral ligament (LCL) and posterolateral corner reconstruction because of instability. Examination reveals a pronounced lateral varus knee thrust when ambulating. Varus stress in 30 degrees of flexion produces a 10-mm opening that is eliminated in extension. The Lachman’s test is 2 mm with a firm end point, and the posterior drawer test is negative. Standing radiographs show widening of the lateral joint space and a 5-degree mechanical varus alignment. What is the most effective course of treatment?
Explanation
REFERENCES: Naudie DD, Amendola A, Fowler PJ: Opening wedge high tibial osteotomy for symptomatic hyperextension-varus thrust. Am J Sports Med 2004;32:60-70.
Covey DC: Injuries of the posterolateral corner of the knee. J Bone Joint Surg Am
2001;83:106-118.
Question 75
A 47-year-old man who is right-hand dominant reports lateral-sided elbow pain after playing golf. His symptoms developed gradually and without trauma, and he has pain with gripping and repetitive movements with the hand and wrist. Examination reveals his shoulder and wrist to be normal, and the elbow has no effusion and normal range of movement. He is tender near the lateral epicondyle, and symptoms are exacerbated with resisted wrist extension. Radiographs are shown in Figures 104a and 104b. What is the next most appropriate step in management? Review Topic

Explanation
Question 76
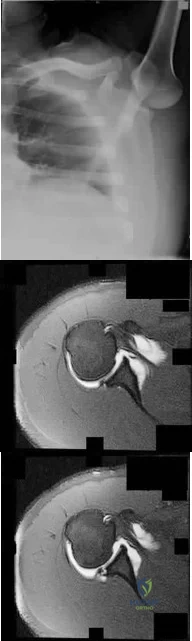
Figure 83a shows an axillary radiograph and Figures 83b and 83c show axial MR arthrograms of a 20-year-old collegiate offensive lineman who has shoulder pain while pass-blocking. He sustained a shoulder injury 3 months earlier when he "jammed it." Prior to this injury, he denies any pain or instability in either shoulder. Despite undergoing rehabilitation with a physical therapist and trainer and abstaining from playing for 6 weeks, he is currently unable to play because of his symptoms. Examination reveals full active range of motion, a positive jerk test which reproduces his symptoms, and a grade 2 posterior translation of the humeral head with load and shift testing which also reproduces his symptoms. What is the best management option to allow him to return to his pre-injury function next season? Review Topic
Explanation
Question 77
A 45-year-old male presented to the trauma department 10 hours after sustaining a fracture-dislocation of his ankle. The patient underwent an attempted closed reduction of his ankle which can be seen in Figures A and B. The splint was removed, and the appearance of the leg is shown in Figure C. Regarding the best next step in management and the intended goals, which of the following is most accurate?

Explanation
Patients with high-energy periarticular fractures in the lower extremity are at risk for surgical wound complications due to compromised soft tissues. As in this case, joint dislocations can place harmful tension on the skin that leads to blistering and/or skin necrosis. An urgent reduction is indicated, and if it cannot be obtained with a closed manipulation alone, percutaneous or open treatment is indicated. Staged joint-spanning external fixation can both hold a reduction and allow access for skin or wound care prior to a definitive open reduction of an articular fracture. Fracture healing during external fixation occurs by enchondral ossification by way of the relative stability.
Strauss et al. developed a treatment protocol for the treatment of fracture blisters. They used silver sulfadine to minimize soft tissue complications by promoting re-epithelialization. After providone-iodine prep, each blister was unroofed by removing the overlying epithelium of the fracture. Once the blister was unroofed, silver sulfadiazine was applied and covered with dry gauze. They would then perform bid dressing changes. Extremities were deemed operable when skin wrinkles were visible on the overlying skin of the injured extremity.
Anglen et al. in a review of external fixation, report that fractures of the lower extremity are frequently associated with soft tissue trauma that precludes safe surgical treatment in the early period. They present a technique of temporary joint-spanning external fixation which allows stabilization of length and alignment while awaiting resolution of soft tissue swelling. They report no differences between patients who had a temporary external fixator and those who did not with respect to healing time, time to partial or full weight bearing, or clinical score.
Figures A and B demonstrate a pronation-external rotation type fracture with disruption of the syndesmosis. Figure C demonstrates fracture blisters.
Illustration A demonstrates an ankle-spanning external fixator. Illustration B demonstrates skin wrinkling to indicate that the skin is safe to incise.
Incorrect Answers:

OrthoCash 2020
Question 78
During an anterior approach to the bicipital 53 tuberosity, you encounter a nerve overlying the brachioradialis fascia (Figure 58). It provides innervation to the

Explanation
The structure shown is the lateral antebrachial cutaneous nerve (LABC). It is the terminal sensory branch of the musculocutaneous nerve and runs superficial to the brachioradialis. It supplies sensation to the anterolateral surface of the forearm. The flexor pollicis longus is innervated by the anterior interosseous nerve. The extensor indicis proprius is innervated by the radial nerve. The LABC does not innervate the skin of the anteromedial forearm. Careful
identification and protection of this nerve is critical to prevent the most common nerve injury during distal biceps repair.
RECOMMENDED READINGS
Agur AM. Grant's Atlas of Human Anatomy. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:460.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1994:118-125.
RESPONSES FOR QUESTIONS 59 THROUGH 61

Please select the image that represents the most appropriate response to the question or statement below.
Question 79
Figures 25a through 25c are the axial T1 and postcontrast MRI scans and biopsy specimen of a 35-yearold man with a painless right thigh mass. He noticed the mass about 2 weeks ago and is unsure if it has changed in size. Which translocation most commonly is associated with this type of tumor?
Explanation
Question 80
Which of the following conditions is associated with palmoplantar pustulosis?
Explanation
REFERENCES: Wirth MA, Rockwood CA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.
Sonozaki H, Azuma A, Okai K, et al: Clinical features of 22 cases with inter-sterno-costo-clavicular ossification: A new rheumatic syndrome. Arch Orthop Trauma Surg 1979;95:13-22.
Question 81
Which of the following fluoroscopic views is used to assess intra-articular screw penetration during volar fixation of a distal radius fracture?
Explanation
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
check for long distal screws.
OrthoCash 2020
Question 82
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
REFERENCES: Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Eaton RG, Crowe JF, Parkes JC III: Anterior transposition of the ulnar nerve using a non-compressing fasciodermal sling. J Bone Joint Surg Am 1980;62:820-825.
Question 83
An orthotic that provides laterally based hindfoot posting support would be most useful for which of the following conditions? Review Topic
Explanation
Cavovarus feet may be seen in multiple conditions, including Charcot-Marie-Tooth disease. The initial deformity is plantarflexion of the first ray, which is often followed by compensatory hindfoot varus. In flexible deformities, orthotics that post the lateral forefoot and lateral heel should be utilized.
Schwend et al. review the etiology, diagnosis and management of the cavus foot in children. They note that shoe inserts with lateral support can be used in patients when there is flexibility to the hindfoot. Recession of the orthotic to accommodate a plantarflexed first ray is also beneficial.
Illustration A shows an orthotic with lateral foot posting and a recessed area for the first metatarsal head. Illustration B shows an AP radiograph of the left foot demonstrative of an accessory navicular. This may be associated with a flatfoot deformity. Illustration C shows a lateral radiograph of a right foot with a middle facet coalition. This may give rise to a rigid, painful flatfoot deformity. Illustration D shows a lateral radiograph of a right foot with collapse of the medial longitudinal arch. This patient had a flexible flatfoot that was painful. Illustration E shows an AP radiograph of a left foot with evidence of metatarsus adductus. Note the alignment of the 2nd metatarsal axis relative to the proximal articular surface of the middle cuneiform. In this case, the metatarsus adductus angle (MAA) was 24 degrees (normal is < 20 degrees).
Incorrect Answers:
Question 84
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Explanation
REFERENCES: Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
O’Hara LJ, Marshall RW: Far lateral lumbar disc herniation: The key to the intertransverse approach. J Bone Joint Surg Br 1997;79:943-947.
Question 85
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
(range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon’s finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle.
REFERENCES: Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804.
Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 86
You are evaluating a patient with recurrent patellar instability who has failed conservative management. MRI demonstrates articular cartilage loss in the patella. In addition to a cartilage restoration procedure, you recommend the procedure depicted in Figures A and B. Which of the following imaging findings best supports your decision? Review Topic

Explanation
Recurrent patellar instability is often associated with chondral lesions of the patellofemoral joint. In addition to managing the cartilage injury, the underlying etiology of the instability must also be addressed to ensure a successful outcome. Patellar instability may arise from coronal or rotational malalignment, patella alta, trochlear dysplasia or damage to soft tissue restraints including the medial patellofemoral ligament (MPFL). Rotational malalignment, defined by a TT-TG distance > 20mm, can be addressed by AMZ. Medialization of the tubercle restores a normal TT-TG distance while anteriorization of the tubercle unloads patellofemoral contact forces.
Beck et al performed a cadaveric study measuring patellofemoral contact pressures on the trochlear surface following AMZ. They found that anteromedialization decreased the mean contact pressures and shifted contact pressures to the medial trochlea. The authors concluded that while this procedure successfully unloads the lateral trochlea, it likely has minimal benefit for central chondral defects and may be detrimental for medial chondral defects where contact pressures are increased.
Strauss et al authored a review article detailing the surgical treatment options for patellofemoral cartilage lesions, including concomitant realignment/unloading procedures. AMZ is designed to correct rotational malalignment while unloading the patellofemoral compartment in the setting of cartilage restoration surgery. While AMZ has demonstrated good outcomes for lesions located in the lateral facet or distal
pole of the patella, poor outcomes have been seen with medial facet or central trochlear lesions.
Figures A and B are the AP and lateral radiographs, respectively, of a knee s/p AMZ, also know as a Fulkerson procedure. Illustration A is an algorithm detailing the approach to recurrent patellar instability in both skeletally immature and mature patients. Illustration B demonstrates how to measure the TT-TG distance, the distance between two lines drawn perpendicular to the posterior condylar axis to the tibial tubercle and deepest portion of the trochlear groove (normal 8-10mm). Illustration C depicts the measurement of the femoral trochlear angle or sulcus angle (normal 137°
+/- 8°). Illustration D shows how to measure lateral patellar tilt (normal < 5°). Illustration E is a postoperative radiograph after AMZ. A long (> 5cm) and thick (> 0.75cm) osteotomy cut is required to allow adequate fixation with two screws.
Incorrect Responses:
Question 87
Figure 61 shows the radiograph of a 28-year-old professional football player who sustained a hyperextension injury to the great toe. He continued to play with pain and loss of push-off strength. What is the most likely diagnosis?

Explanation
Question 88
What is the most important preoperative factor predicting conversion to total hip arthroplasty after arthroscopic surgery of the hip?
Explanation
The authors cited in the references examined large databases to determine the risk factors for conversion to total hip arthroplasty after arthroscopic surgery of the hip. In the study by Kester and associates, obesity had an odds ratio (OR) of 5.6 for conversion to hip arthroplasty, whereas age over 60 years had an OR of 3.4, osteoarthritis had an OR of 2.4, and tobacco use had an OR of 1.9.
Question 89
A 30-year-old man has had a 3-day history of severe, incapacitating lower back pain without radiation. He reports improvement with rest. He denies any history of trauma, has no constitutional symptoms, and his neurologic examination is normal. What is the best course of action?
Explanation
REFERENCE: Deyo RA, Diehl AK, Rosenthal M: How many days of bed rest for acute low back pain? A randomized clinical trial. N Engl J Med 1986;315:1064-1070.
Question 90
Figures 233a through 233c are the radiographs and biopsy specimen of a 32-year-old woman who has had progressive ankle pain for 6 months. What is the most appropriate treatment option?

Explanation

Question 91
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-247.
Question 92
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear? Review Topic
Explanation
Question 93
Figure 69 is the radiograph of a 9-year-old who has posterior hindfoot pain while running. What is the most likely diagnosis?

Explanation
Sever disease is a traction apophysitis at the Achilles tendon insertion on the calcaneus. Plain radiographs may be unremarkable for this condition. Other osteochondroses of the foot include Kohler disease (tarsal navicular), Freiberg infraction (lesser metatarsal head), and Thiemann disease (great toe phalanx).
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
Schantz K, Rasmussen F. Thiemann's finger or toe disease. Follow-up of seven cases. Acta Orthop Scand. 1986 Feb;57(1):91-3. PubMed PMID: 3962642. View Abstract at PubMed
Question 94
Which of the following is an important factor in performing a proper biopsy?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 29-34.
Question 95
01 (left). What is the most appropriate next step?

Explanation
Knee dislocations are associated with popliteal artery injury in 18-45% of cases and range from intimal tears to complete transection. Amputation rates of 85% have been reported if revascularization is delayed greater than 6 to 8 hours. Neurologic injury occurs in 15-40% of cases and is most common after posterolateral dislocation. The peroneal nerve is more commonly injured.
Rihn et al. reviewed the acutely dislocated knee. They recommend a vascular consult if pulses are weak, or ABI is compromised. They warn that in arterial injury, pulses, temperature and capillary refill can be normal. If the limb remains ischemic, surgical exploration and revascularization is indicated.
Medina et al. systematically reviewed neurovascular injury after knee dislocation in 862 patients. Vascular injury rate was 18%, and nerve injury rate was 25%. Repair was performed in 80% of vascular injuries, and amputation in 12%. The most vascular injury was seen in KDIIIL injuries (32%) and posterior dislocation (25%).
Figure A is an AP radiograph of a posterior knee dislocation. Figure B is a lateral showing the same injury.
Incorrect Answers:
Question 96
A 52-year-old man has had right shoulder pain in the deltoid region that increases at night for the past 2 months. He denies any history of trauma. Examination reveals mild tenderness over the greater tuberosity, and the Neer and Hawkins impingement signs are positive. AP and outlet lateral radiographs are shown in Figures 24a and 24b. Initial management should consist of
Explanation
REFERENCES: Morrison DS, Frogameni AD, Woodworth P: Non-operative treatment of subacromial impingement syndrome. J Bone Joint Surg Am 1997;79:732-737.
Neer CS: Impingement lesions. Clin Orthop 1983;173:70-77.
Blair B, Rokito AS, Cuomo F, et al: Efficacy of injections of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am 1996;78:1685-1689.
Question 97
When the elbow is extended and an axial load is applied, what percent of stress distribution occurs across the ulnohumeral and radiohumeral articular surface, respectively?
Explanation
REFERENCES: Halls AA, Travill R: Transmission of pressure across the elbow joint. Anat Rec 1964;150:243.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000.
Question 98
Figure 30 shows the radiograph of a 38-year-old man who reports persistent pain laterally and plantarly about the fifth metatarsal head. Examination reveals calluses dorsolaterally and plantarly about the fifth metatarsal head. Nonsurgical management has failed to provide relief. Surgical treatment should include
Explanation
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Moran MM, Claridge RJ: Chevron osteotomy for bunionette. Foot Ankle Int 1994;15:684-688.
Question 99
Induction coupling stimulates bone growth through all of the following direct effects EXCEPT:
Explanation
In basic science studies, electrical stimulation (i.e. induction coupling), has been shown to promote bone healing via release of growth factors that induce osteoblast differentiation/proliferation. Electrical current can be placed around bone in various ways, creating a current to stimulate growth factor release and subsequent osteoblast proliferation.
Aaron et al. summarized, in a systematic review, the effects of various types of electrical stimulation on bone and bone healing. Regardless of type (i.e. inductive coupling, capacitive coupling, direct current), they report electricity and/or electromagnetic fields promote gene expression of growth factors that promote an osteogenic environment.
Illustration A depicts a cathode placed directly to allograft with a subcutaneously placed electrical stimulator. Illustration B depicts cathodes placed anteriorly and posteriorly around the hip, connected to an outside power source to create the necessary current. Illustration C depicts an inductive coil placed laterally on the skin in order to create an electrical current.
Incorrect answers:
Question 100
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful total knee arthroplasty.
