Orthopedic Board Review MCQs: Hip & Knee Arthroplasty & Oncology | Part 89

Key Takeaway
This Orthopedic Surgery Board Review features 100 verified, high-yield MCQs, strictly modeled on OITE and AAOS exams. Designed for orthopedic surgeons and residents, it covers critical topics including Arthroplasty, Hip, and Knee. This interactive quiz provides essential preparation for your board certification.
About This Board Review Set
This is Part 89 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 89
This module focuses heavily on: Arthroplasty, Dislocation, Hip, Knee, Revision, Tumor.
Sample Questions from This Set
Sample Question 1: A 25-year-old male professional lacrosse player collides with another player, with injury resulting from a knee impacting the athlete’s thigh. He has immediate pain in the mid-thigh area and is unable to return to the game because of diffic...
Sample Question 2: Which of the following clinical scenarios represents the strongest indication for locked plating technique in a 70-year-old woman?...
Sample Question 3: Figure 18 shows the radiograph of a patient with a total hip arthroplasty dislocation. During revision, increasing the diameter of the femoral head while maintaining the ratio of head-to-neck diameter constant has the effect of...
Sample Question 4: -What factor is most commonly associated with malignant transformation of a giant cell tumor?...
Sample Question 5: An operating room intervention that should be undertaken by anesthesia staff during the cementing of a femoral stem is to...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 25-year-old male professional lacrosse player collides with another player, with injury resulting from a knee impacting the athlete’s thigh. He has immediate pain in the mid-thigh area and is unable to return to the game because of difficulty with running. Examination reveals developing swelling in the anterior mid-thigh area. The thigh compartments are soft, and he is able to extend his knee against gravity. Knee flexion at 90° gives him discomfort in the thigh but no knee pain. The knee and hip examinations are otherwise unremarkable. Plain films of the femur are negative. What is the best next step?
Explanation
A. only type 1 collagen.
B. only type 2 collagen.
C. type 1 and type 2 collagen.
D. neither type 1 or type 2 collagen.
The MRI scan shows a full-thickness cartilage defect. When treated with a marrow stimulation technique, such as a microfracture, the reparative tissue is fibrocartilage. Unlike hyaline cartilage, which is composed of only type 2 collagen, fibrocartilage is composed of both type 1 and type 2 collagen.
15- Figures 1 and 2 are the radiographs of a 58-year-old retired laborer who has had many years of right shoulder pain. He initially experienced relief with anti-inflammatory medication over the past year, but this no longer provides him pain relief. He has pain with overhead activities and is dissatisfied with his shoulder function. Examination indicates active and passive forward elevation to 130°, full strength with external rotation, and a negative belly press test. MRI demonstrates an intact rotator cuff. What is the best next step in treatment?
A. Anatomic total shoulder arthroplasty (TSA)
B. Hemiarthroplasty
C. Reverse shoulder arthroplasty
D. Arthroscopy with debridement and biceps tenodesis
The patient has glenohumeral osteoarthritis based on the radiograph. His examination demonstrates limited motion and no significant rotator cuff pathology – full strength with external rotation, negative belly press, and no pseudoparalysis. Of all the answer choices, an anatomic TSA would be the most appropriate treatment option. Hemiarthroplasty does not address glenoid pathology and provides inferior pain relief and function, compared with TSA. A reverse shoulder arthroplasty is utilized for patients with degenerative shoulder changes in conjunction with irreparable rotator cuff pathology. Shoulder arthroscopy with debridement and biceps tenodesis is not appropriate for those with severe degenerative changes of the shoulder.
16- According to the MRI scan shown in Figure 1, which pathologic finding is expected to be encountered during arthroscopy?
A. Figure 2
B. Figure 3
C. Figure 4
D. Figure 5
The sagittal MRI scan is a clear example of a double posterior cruciate ligament (PCL) sign. This sign has a high specificity for a displaced bucket handle tear of the medial meniscus as seen in Figure 4. The other arthroscopic
images show a flap tear of the medial meniscus (Figure 2), anterior cruciate ligament tear (Figure 3), and a full thickness articular cartilage defect (Figure 5). Other less likely causes of a double PCL sign include intermeniscal ligament, meniscofemoral ligaments, loose bodies, osteophytes, and fracture fragments. Correct answer : C 13
17- Figures 1 and 2 are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test, trace effusion, and range of motion from 0 to 85° of knee flexion. Which factor is most contributory to his examination findings?
A. Incorrect graft choice
B. Improper tunnel position
C. Tibial graft-tunnel mismatch
D. Femoral fixation at 80° flexion
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario.
Question 2
Which of the following clinical scenarios represents the strongest indication for locked plating technique in a 70-year-old woman?
Explanation
Question 3
Figure 18 shows the radiograph of a patient with a total hip arthroplasty dislocation. During revision, increasing the diameter of the femoral head while maintaining the ratio of head-to-neck diameter constant has the effect of
Explanation
Scifert and associates used a three-dimensional finite element model to study various combinations of femoral head size and neck ratios. They found that increasing the diameter of the femoral head while maintaining a constant head-to-neck diameter had the effect of significantly increasing the resisting moment necessary to induce a dislocation. The higher the head-to-neck ratio, the greater the range of motion until impingement and the greater the range of motion to dislocation.
REFERENCE: Scifert CF, Brown TD, Pedersen DR, Callaghan JJ: A finite element analysis of factors influencing total hip dislocation. Clin Orthop 1998;355:152-162.
Question 4
- What factor is most commonly associated with malignant transformation of a giant cell tumor?
Explanation
Question 5
An operating room intervention that should be undertaken by anesthesia staff during the cementing of a femoral stem is to
Explanation
Young age is a risk factor for early failure of cementless femoral components. Surgeons could consider cementing for patients older than 80 years of age. The Dorr classification has been shown to favor a cemented femoral stem in Dorr type C bone. Dorr type B bone can potentially sustain a proximally porous ingrowth stem. Osteoporosis is a risk factor for early failure of cementless femoral components.
Earlier designs for cemented femoral stems used microtexture to interlock the stem into the cement mantle. If these stems became loose, they would abrade the cement and loosen the stem further. Successful cemented femoral components are polished and have smooth edges with tapered bodies. Collars do not add to the design of femoral stems.
Patients are at risk for hypotension during the femoral pressurization process. With that in mind, the surgeon should make sure the anesthesiologist is ready to respond to hypotension. The FiO2 should be increased. The IV fluid rate also should be increased, and the anesthesiologist should be prepared with phenylephrine to support the patient’s blood pressure if he or she becomes hypotensive.

Question 6
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as
Explanation
REFERENCE: O’Rourke M, Callaghan J, Goetz D, Sullivan P, Johnson R: Osteolysis associated with a cemented modular posterior cruciate substituting total knee design. J Bone Joint Surgery Am 2002;84:1362-1371.
Question 7
Management of a grade IV osteochondritis dissecans lesion of the capitellum should consist of
Explanation
Lesions are graded I through V based on radiographic and arthroscopic appearance. Grade I lesions show intact but soft cartilage. Grade II lesions show fissuring of the overlying cartilage. Grade III lesions show exposed bone or an attached osteoarticular flap that is not loose. Grade IV lesions show a loose but nondisplaced osteoarticular flap. Grade V lesions show a displaced fragment.
Simple excision of the loose osteoarticular flap is the treatment of choice for grade IV and V lesions. More complex procedures such as drilling of the in situ lesion, bone grafting, or internal fixation are associated with significantly worse results. While some authors advocate abrasion chondroplasty, the long-term benefits of the procedure are yet to be proven.
REFERENCES: Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Shaughnessy WJ, Bianco AJ: Osteochondritis dissecans, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 282-287.
Question 8
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Green DP, Anderson JR: Closed reduction and percutaneous pin fixation of fractured phalanges. J Bone Joint Surg Am 1973;55:1651-1653.
Question 9
A patient competing in a professional motocross race sustained a direct blow to the knee after falling off his bike at high speed. He sustained several lacerations as shown in Figure 60. He is able to actively extend his knee painlessly and his Lachman examination is negative. What is the most likely injury? Review Topic

Explanation
Question 10
A 25-year-old patient who sustained multiple bilateral rib fractures, a pulmonary contusion, a left nondisplaced transtectal acetabular fracture, and a closed humerus fracture in a motor vehicle accident 2 weeks ago is transferred from another hospital. The humerus fracture has been surgically treated. There are no signs of infection, and the trauma surgeon wants to mobilize the patient as soon as possible. Radiographs are shown in Figures 15a and 15b. Management of the humerus fracture should consist of
Explanation
REFERENCE: Tingstad EM, Wolinsky PR, Shyr Y, Johnson KD: Effect of immediate weightbearing on plated fractures of the humeral shaft. J Trauma 2000;49:278-280.
Question 11
A 66-year-old man who underwent shoulder arthroplasty 7 years ago reports progressively worsening shoulder pain for the past 4 weeks after hospital discharge for community-acquired pneumonia. He is afebrile and reports no chills or night sweats. Laboratory studies show a white blood cell count of 11,200/mm3 and an erythrocyte sedimentation rate of 25/h. Shoulder radiographs are negative for fracture, dislocation, or signs of implant loosening. What is the most appropriate management? Review Topic
Explanation
Question 12
A year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 13
A 30-year-old man undergoes arthroscopic Bankart repair for recurrent anterior dislocation. He continues to experience instability postoperatively. Examination reveals a positive apprehension test. Radiographs of both shoulders are seen in Figure A. CT scan of his left shoulder is seen in Figure B. What is the best treatment option? Review Topic
Explanation
Patients with glenoid bone defects >20-30% have a high recurrence rate (>60%) after Bankart repair alone. Bone grafting is necessary to offer containment. Autograft options include coracoid transfer (such as the Latarjet procedure which extends the articular arc and creates a conjoined tendon sling) and iliac crest bone grafting.
Burkhart et al. addressed glenohumeral bone defects. They advise that significant bone deficits cannot be adequately addressed via arthroscopic Bankart repair alone. The Latarjet transfer creates an extra-articular platform to extend the articular arc of the glenoid.
Hantes et al. assessed Latarjet repairs using CT. They found that there is almost
complete repair of a 25% to 30% glenoid defect when using the Latarjet procedure.
Figure A comprises comparison Bernageau view glenoid profile radiographs of both shoulders. Figure B is a 3D reconstruction CT with showing glenoid bone deficiency (inverted pear deformity) with a large bony Bankart lesion. Illustration A shows the method of obtaining a Bernageau glenoid profile view. Illustration B shows the "cliff sign" of anterior glenoid bone loss. Illustration C depicts the Latarjet procedure. Illustration D depicts reduction in the articular arc with anterior glenoid loss.
Incorrect Answers:
Question 14
Which of the following is not a characteristic of synovial sarcomas?
Explanation
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1109-1126.
Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Question 15
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.
Kwon BK, Vaccaro AR, Grauer JN, et al: Subaxial cervical spine trauma. J Am Acad Orthop Surg 2006;14:78-89.
Question 16
A 28-year-old man was shot in the foot with a .22 caliber handgun approximately 2 hours ago. Examination reveals an entrance wound dorsally and a plantar exit wound. The foot is neurovascularly intact. Radiographs reveal a nondisplaced fracture of the third metatarsal. Soft-tissue management for this injury should consist of
Explanation
REFERENCES: Brettler D, Sedlin ED, Mendes DG: Conservative treatment of low velocity gunshot wounds. Clin Orthop 1979;140:26-31.
Hampton OD: The indications for debridement of gunshot bullet wounds of the extremities in civilian practice. J Trauma 1961;1:368-372.
Marcus NA, Blair WF, Shuck JM, Omer GE Jr: Low-velocity gunshot wounds to extremities. J Trauma 1980;20:1061-1064.
Question 17
A 25-year-old male is involved in an high-speed motor vehicle collision and sustains a closed femoral shaft fracture. During further evaluation, a CT scan of the chest/abdomen/pelvis reveals a non-displaced ipsilateral femoral neck fracture. Which of the following treatment options will most likely achieve anatomic healing of both fractures, mobilize the patient, and minimize the risk of complications?

Explanation
Question 18
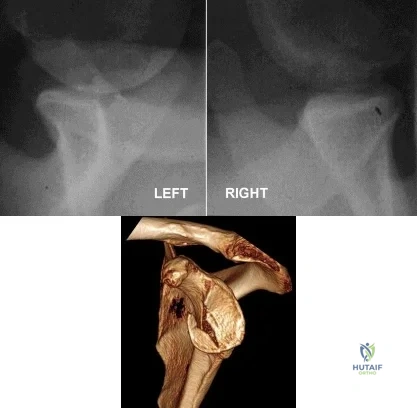
9 degress Celsius, serum WBC is 14,000, and his C-reactive protein is elevated. He reports that he uses IV heroin. A coronal 3D CT scan of the left clavicle is shown in Figure B. Joint aspiration shows many grams stain positive organisms. Which of the following organisms is the most likely pathogen?

Explanation
Ross et al states "Staphylococcus aureus is now the major cause of
sternoclavicular septic arthritis in intravenous drug users. Pseudomonas aeruginosa infection in injection drug users declined dramatically with the end of an epidemic of pentazocine abuse in the 1980s."
The referenced article by Goldin et al is from the New England Journal of Medicine reports that all of their cases of SC joint septic arthritis were in intravenous drug abusers and that P. aeruginosa grew out of 3 patients and S. aureus grew out of 1 patient.
A more recent article by Abu Arab et al reported that Staph aureus was most common even in IV drug users. The review article by Higginbotham and Kuhn note that risk factors for SC joint septic arthritis include hemodialysis, immunocompromise, alcoholism, and HIV. Neisseria gonorrhoeae, fungal, and candida present in HIV patients.
Treatment is I&D and appropriate antibiotics, although aspiration and abx have shown some success too. CT and MRI are useful in diagnosis, and open biopsy or aspiration is recommended for definitive diagnosis.
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?
Degenerative lumbar spine changes
Ipsilateral ankle pain and stiffness
Ipsilateral hip joint degenerative changes
Contralateral hip joint degenerative changes
Ipsilateral medial knee degenerative changes Correct answer: 2
A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted
that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
A 33-year-old man sustains a femur fracture in a motorcycle accident. AP and lateral radiographs are provided in Figure A. Prior to surgery, a CT scan of the knee is ordered for preoperative planning. Which of the following additional findings is most likely to be discovered?

Tibial eminence fracture
Sagittal plane fracture of the medial femoral condyle
Schatzker I tibia plateau fracture
Coronal plane fracture of the lateral femoral condyle
Axial plane fracture through the medial femoral condyle Correct answer: 4
The "Hoffa fracture" is a coronal plane fracture of the femoral condyle that is often missed on plain radiographs of supracondylar and intercondylar femur fractures. It involves the lateral condyle more frequently than the medial.
Identification is important as it may impact operative planning and likely require screw fixation in the anteroposterior plane.
Nork et al. reviewed 202 supracondylar-intercondylar distal femoral fractures and found a 38% prevalence of associated coronal plane fractures. The authors recommend CT scan imaging of all supracondylar and intercondylar fractures.
Ostermann et al reported on 24 unicondylar fractures of the distal femur treated with open reduction internal fixation with a screw construct. Twenty-
three patients acheived satisfactory results at 5 year follow-up. Illustrations A and B are another example of a supracondylar femur fracture with an associated Hoffa fracture identified on CT scan.

A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
closed reduction and early range of motion
radial head resection and lateral collateral ligament reconstruction
radial head resection and coronoid open reduction internal fixation
radial head arthroplasty and coronoid open reduction internal fixation
radial head arthroplasty, coronoid open reduction internal fixation, and lateral collateral ligament repair
A terrible triad of the elbow includes dislocation of the elbow with associated fractures of the radial head and the coronoid process. Ring et al. stressed that these injuries are prone to complications and advised against resection of the radial head due to instability, and instead recommended a radial head replacement if too comminuted for ORIF. Coronoid fractures compromise elbow stability as well and require open reduction and internal fixation as with the lateral collateral ligament. McKee et al. showed stable elbows in 34/36 with mean Mayo elbow score of 88 when the standard protocol of coronoid ORIF, radial head repair/replacement, and LCL repair were employed.
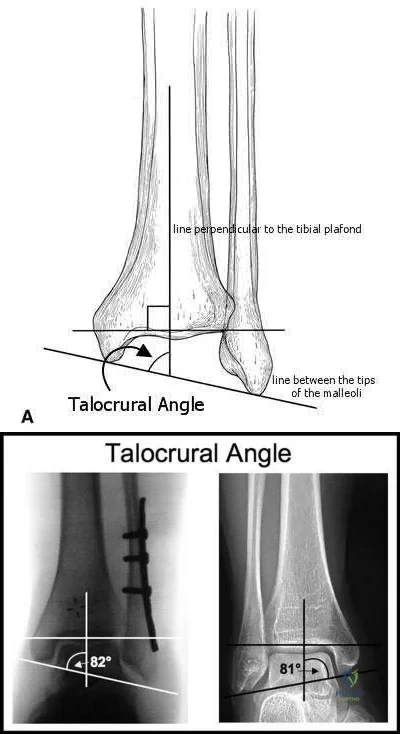
The talocrural angle of an ankle mortise x-ray is formed between a line perpendicular to the tibial plafond and a line drawn:
perpendicular to the medial clear space
parallel to the talar body
between the tips of the malleoli
perpendicular to the shaft of the fibular
parallel to the subtalar joint Correct answer: 3
The talocrural angle is formed by the intersection of a line perpendicular to the plafond with a line drawn between the malleoli (average = 83+/-4deg). When the lateral malleolus is shortened secondary to fracture, this can lead to increased talocrural angle. This malunion leads to lateral tilt of the talus.
Phillips et al looked at 138 patients with a closed grade-4 supination-external rotation or pronation-external rotation ankle fracture. Although the conclusions were limited due to poor follow up, they found the difference in the talocrural angle between the injured and normal sides was a statistically significant radiographic indicator of a good prognosis.
Pettrone et al looked at a series of 146 displaced ankle fractures, and the effect of open or closed treatment, and internal fixation of one or both malleoli. They found open reduction proved superior to closed reduction, and in bimalleolar fractures open reduction of both malleoli was better than fixing only the medial side.
Illustrations A and B are demonstrations of the talocrural angle.
A 33-year-old male sustains the injury shown in Figure A. He is initially treated with a spanning external fixator followed by definitive open reduction internal fixation of the tibia and fibula. His wounds healed without infection or other complications. Two years following surgery, which of the following parameters will most likely predict a poor clinical outcome and inability to return to work?

Joint line restoration
Degree of fracture displacement
Time before definitive ORIF
Open fracture
Lower level of education Correct answer: 5
Lower level of education is the parameter that correlated most closely with a poor clinical outcome and inability to return to work.
To determine what fracture- and patient-specific variables affect outcome, Williams et al evaluated 29 patients with 32 tibial plafond fractures at a minimum of 2 years from the time of injury. Outcome was assessed by four independent measures: a radiographic arthrosis score, a subjective ankle score, the Short Form-36 (SF-36), and the patient’s ability to return to work. The four outcome measures did not correlate with each other. Radiographic arthrosis was predicted best by severity of injury and accuracy of reduction. However, these variables did not show any significant relationship to the clinical ankle score, the SF-36, or return to work. These outcome measures were more influenced by patient-specific socioeconomic factors. Higher ankle
scores were seen in patients with college degrees and lower scores were seen in patients with a work-related injury. The ability to return to work was affected by the patient’s level of education.
Pollak et al performed a retrospective cohort analysis of pilon fractures. Patient, injury, and treatment characteristics were recorded. The primary outcomes that were measured included general health, walking ability, limitation of range of motion, pain, and stair-climbing ability. A secondary outcome measure was employment status. Multivariate analyses revealed that presence of two or more comorbidities, being married, having an annual personal income of less than $25,000, not having attained a high-school diploma, and having been treated with external fixation with or without limited internal fixation were significantly related to poorer results as reflected by at least two of the five primary outcome measures.
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?
Irrigation and local wound care in the emergency department
Emergent irrigation and debridement in the operating room with vacuum-assisted wound closure
Emergent irrigation and debridement in the operating room with 7 days of intravenous antibiotics
Wound closure in the emergency department with follow-up wound check in 1 week
Exploration and removal of all bullet fragments in the emergency department and 10 day course of oral antibiotics
The question refers to appropriate management of a gunshot wound to the forearm. The first question that must be answered when evaluating gunshot injuries is whether the gunshot is low velocity or high velocity. Low-velocity wounds are less severe, are more common in the civilian population, and are typically attributed to bullets with muzzle velocities below 1,000 to 2,000 feet per second. Tissue damage is usually more substantial with higher-velocity (greater than 2,000 to 3,000 fps) military and hunting weapons. In this question, a muzzle velocity of 1,000 ft/sec is provided. Low velocity injuries with stable, non-operative fractures can be treated with local wound care.
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds.
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?
pulselessness
pallor
paresthesia
paralysis
increasing analgesia requirement Correct answer: 5
Although pain, pallor, paresthesia, paralysis, and pulselessness are all possible signs and symptoms of compartment syndrome in children with fractures, studies have shown increasing analgesia requirement is more sensitive.
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of
compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
A 45-year-old man sustains the injury seen in Figures A and B following a motor vehicle accident. Postoperative radiographs are seen in Figures C and D. Which of the following is the most accurate when comparing outcomes between intramedullary nailing (IMN) and open reduction internal fixation (ORIF) for this injury?

Union rates at one year are higher with ORIF
Infection rates are higher with IMN
Functional shoulder outcomes at one year are equivalent with IMN and ORIF
Iatrogenic radial nerve injury rate is higher with ORIF
Shoulder stiffness rates at one year are equivalent with IMN and ORIF Correct answer: 3
Although shoulder pain and stiffness is increased following IMN compared to ORIF, functional outcome scores at one year have been shown to be equivalent
in both treatment groups.
Diaphyseal humeral shaft fractures outcomes following IMN and ORIF are under further investigation. Diaphyseal humeral shaft fractures have historically been treated with ORIF, however proponents for IMN cite benefits of less periosteal stripping and soft tissue dissection. Recent investigations have shown outcomes with regard to nonunion, infection, re-operation, and nerve palsy appear equivalent between both groups. Rates of shoulder stiffness and shoulder pain have been demonstrated to be higher in IMN compared to ORIF. American Shoulder and Elbow Scores (ASES) have shown no difference at one year post-operatively.
Bhandari et al. performed a meta-anaylsis of 3 prospective randomized trials. They found lower rates of re-operation and shoulder impingement with ORIF of humeral shaft fractures.
Wali et al. performed a prospective randomized study of IMN or ORIF on 50 patients with mid-diaphyseal humeral shaft fractures. They found IMN had shorter operative time, shorter hospital stay, and lower blood loss. They found no difference in union rates, complication, or shoulder functional outcomes scores. They conclude IMN to be an effective option for treating mid-diaphyseal humeral shaft fractures.
Heineman et al. have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF. The authors found no significant difference between the two treatment modalities for the secondary outcomes (nonunion, infection, nerve palsy, re-operation).
Figures A and B show a diaphyseal humeral shaft fracture. Figure C and D show postoperative radiographs following intramedullary nailing of a humeral shaft fracture.
Incorrect Answers:
A 25-year-old female presents complaining of progressive anteromedial pain in her left ankle. She underwent operative fixation 5 months prior at an outside hospital. The operative report indicated that, due to anterior fracture blisters, a direct medial incision was utilized, centered over the posterior colliculus of the medial malleolus, without violation of the deltoid ligament. A radiograph and computed tomographic scan of her initial injury are shown in Figures A and B, respectively. On exam, she has well-healed incisions, exhibits no tenderness to palpation over her hardware, but does endorse pain with deep palpation along the anteromedial joint line. Figure C shows an anteroposterior left ankle radiograph taken today. Labs are obtained and reveal a white blood cell count of 9.0 k/uL (reference range 4.5-11.0 k/uL) and a C-reactive protein value of 0.8 mg/dL (<0.9 mg/dL). What is the next best step in managing her problem?

Syndesmotic fixation
Intra-articular corticosteroid injection
Referral to physical therapy
Surgical correction of malunion
Removal of hardware Correct answer: 4
This patient sustained a supination-adduction (SAD) injury with a vertical shear fracture of her medial malleolus and a fibular avulsion fracture. She sustained a medial plafond articular impaction injury that was not addressed at the time of surgery.
In SAD injuries, supination of the foot is combined with inward rotation at the ankle, adduction of the hindfoot, and inversion of the forefoot. This results in the following sequence of events: 1. Talofibular sprain or distal fibular avulsion (equivalent to Weber A). 2. Vertical medial malleolus fracture as the talus strikes the tibia. Associated injuries may include osteochondral damage to the talus and marginal impaction of the medial plafond. It is important to evaluate the medial plafond for articular impaction. When present, an arthrotomy must be performed, typically utilizing an anteromedial incision, with direct visualization of the articular surface to restore the joint line appropriately.
Weber et al. provided a review article on corrective osteotomies for malleolar fracture malunions. They stress that malunions can lead to ankle instability, abnormal load transfer, and post-traumatic arthritis. They conclude that corrective osteotomies that restore anatomical alignment show good results in long-term follow-up.
Perera et al. provided additional commentary on the surgical reconstruction of malunited ankle fractures. The authors emphasize the link between malunion and poor outcomes. They state that successful salvage procedures involve a clear understanding of the deformity, careful preoperative planning, and a solid understanding of reconstructive techniques. They provide several instructive case examples in their review.
McConnell et al. provided a discussion on SAD ankle fractures at their institution and emphasized the importance of recognizing marginal impaction of the tibial plafond when treating these injuries. Of 800 ankle fractures identified over a 5-year period, 44 were SAD injuries, 19 of the 44 displayed a vertical shear fracture of the medial malleolus, and 8 of the 19 demonstrated marginal impaction of the tibial plafond. These 8 impaction injuries were treated with open reduction internal fixation with elevation of the articular impaction; all had good to excellent outcomes without arthritic changes at last
follow-up.
Figure A is an anteroposterior left ankle radiograph demonstrating a SAD injury with a vertical shear fracture of the medial malleolus, a fibular avulsion fracture, and articular impaction of the medial tibial plafond. Figure B is a coronal CT demonstrating articular impaction of the medial plafond. Illustration A is an intra-operative photograph with the medial malleolus retracted allowing inspection of the articular surface; mild anteromedial plafond impaction is present.
Incorrect Answers:

A 90-year-old female slips and falls at home. She is a community ambulator and has no medical problems. She reports right hip pain at this time. Injury radiographs are shown in Figures A & B. Delay of more than 48 hours may result in:

Increased intraoperative time
Increased 30-day mortality
No impact on the rate of postoperative pneumonia
Higher rates of blood transfusion
Increased risk of post-operative infection Correct answer: 2
Figures A & B demonstrate a right, unstable intertrochanteric femur fracture. Surgical stabilization within 48 hours improves short-term and 30-day mortality.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:

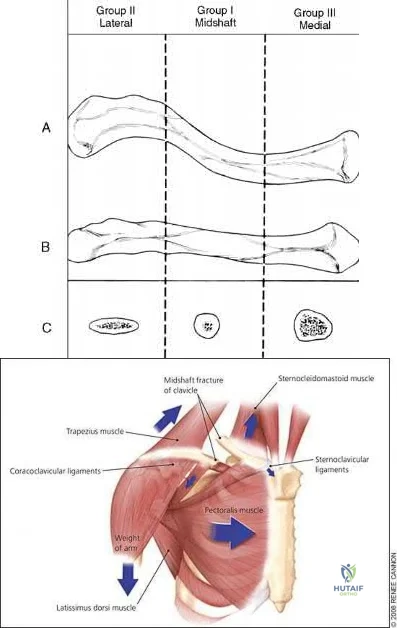
A 22-year-old healthy left hand dominant male presents to the ED with left shoulder pain after falling from an ATV. Figure A is the radiograph of his left clavicle. He is neurovascularly intact and there is no evidence of skin tenting or open fracture. Which of the following most predisposes this patient to nonunion?

Diaphyseal fracture
Fracture displacement
Age
Male Gender
Injury involving the dominant extremity Correct answer: 2
Displaced clavicle fractures are associated with higher rates of nonunion.
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
A 24-year-old male presents with ankle pain after being involved in a motor vehicle accident. His injury radiograph is shown in Figure A. Which of the following has been shown to contribute to the development of post-traumatic arthritis in this injury pattern?

Initial superficial zone cartilage cell death via apoptosis at the fracture margins
Initial superficial zone cartilage cell death via apoptosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis at the fracture margins
Delayed superficial zone cartilage cell death via necrosis at the fracture margins
Figure A demonstrates a tibial plafond fracture. Initial superficial zone cartilage cell death via necrosis at the fracture margins has been shown to contribute to post-traumatic arthritis.
Post-traumatic osteoarthritis typically occurs after an intra-articular fracture. Impacted chondrocytes die by either necrosis or apoptosis, which have both been implicated in post-traumatic osteoarthritis. Initial cell death in the superficial cartilage zones at the fracture margins occurs by necrosis. Apoptosis occurs in a delayed fashion and is mitigated by several bioactive agents.
Apoptosis also affects the superficial cartilage zones near the fracture margins. Deep cartilaginous zones and areas away from the fracture margins do not seem to be involved in these processes.
McKinley et al. performed a review of the basic science of intra-articular fractures and posttraumatic osteoarthritis. They report that initial damage to the cartilage in combination with the ensuing pathomechanical and pathobiologic response of the cartilage after a fracture contribute to posttraumatic arthritis. Chronic abnormal joint loading is also thought to contribute to this process as well. They conclude that the relative contribution of each is unknown.
Tochigi et al. performed a study to determine the distribution and progression of chondrocyte damage after intra-articular ankle fractures. They harvested 7 normal human ankles and subjected them to impaction. They found that immediate superficial zone chondrocyte death was greater in fracture-edge regions than on-fracture regions. Subsequent cell death over the next 48 hours was significantly higher in fracture-edge regions as well. They conclude that cartilage damage in intra-articular fractures was characterized by chondrocyte death at fracture margins.
Figure A is an ankle mortise radiograph demonstrating an intra-articular tibial plafond fracture.
Incorrect Answers:
A 35-year-old male presents with left knee pain after sustaining the injury seen in Figure A. He is neurovascularly intact and can perform a straight leg raise, but has pain with passive range of motion. Figures B and C show an anteroposterior and lateral radiograph of the left knee, respectively. 175 cc of saline is injected into the superolateral quadrant with no egress of fluid from the inferolateral
laceration. What percentage of traumatic arthrotomies would be detected with this test?

Question 19
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful total knee arthroplasty.
Question 20
Which of the following is most associated with local recurrence of the lesion seen in the radiograph and MRI scan shown in Figures 27a and 27b?
Explanation
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Vergel De Dios AM, Bond JR, Shives TC, et al: Aneurysmal bone cyst: A clinicopathologic study of 238 cases. Cancer 1992;69:2921-2931.
Question 21
A left-handed 23-year-old man who fell 5 feet from a ladder onto his left elbow sustained the closed injury shown in Figure 26. Management should consist of
Explanation
REFERENCES: Hotchkiss RN: Fractures and dislocations of the elbow, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 929-1024.
Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
Hume MC, Wiss DA: Olecranon fractures: A clinical and radiographic comparison of tension band wiring and plate fixation. Clin Orthop 1992;285:229-235.
Question 22
A 14-year-old male sustains the injuries shown in Figures A and B after a fall off the roof of his house. What is the most appropriate management? Review Topic

Explanation
Pediatric femoral neck fractures are classified into transphyseal, transcervical, cervicotrochanteric and intertrochanteric (Delbets I-IV) respectively. Fixation type varies by author, but generally speaking, Types I-III can be treated with smooth wires for patients 0-3yrs of age, 4.5-6.5 mm cannulated screws 4-10yrs of age, or l 6.5-
Question 23
A year-old man who underwent right total knee replacement surgery 2 and a half years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3° and 120°. Radiographs show well-fixed and well-aligned implants. What is the most appropriate initial treatment?
Explanation
This patient's history and physical findings are concerning for deep infection. Inflammatory markers, including ESR and CRP, should be obtained first. If the levels are elevated, knee aspiration should be performed for the synovial cell count and culture. A bone scan is not indicated in an initial investigation for deep infection; it is rarely helpful and is not cost effective. CT to assess implant rotation is an appropriate investigation for knee pain when the clinical scenario is not suspicious for a deep infection
and when infection has been excluded.
Question 24
You design a research study in which you ask patients who have a nonunion of the tibia to fill out a questionnaire in which they report on a variety of medical conditions and social/behavioral practices. You compare these findings to a similar group who did not develop a nonunion in order to identify medical and/or social conditions that might be risk factors for the development of tibial nonunions. This would be an example of what type of study?
Explanation
Question 25
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
REFERENCES: Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its affects on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Question 26
The term anorexia athletica refers to a problem whose criteria include all of the following, EXCEPT Review Topic
Explanation
Question 27
- A patient sustained a joint depression-type fracture of the calcaneus that healed despite lack of treatment. The loss of dorsiflexion the patient is now experiencing is most likely the result of
Explanation
Question 28
What structure is located at the tip of the arrow in Figure 18? Review Topic

Explanation
Question 29
A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
Explanation
REFERENCES: Luhmann SJ, Gordon JE, Schoenecker PL: Intramedullary fixation of unstable both-bone forearm fractures in children. J Pediatr Orthop 1998;18:451-456.
Mehlman CT, Wall EJ: Injuries to the shafts of the radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 430-436.
Question 30
What antithrombotic agent is a selective factor I0a inhibitor? Review Topic
Explanation
Question 31
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Henry A: Extensile Exposure, ed 3. Edinburgh, UK, Churchill Livingstone, 1995, pp 100-107.
Question 32
What is the primary advantage of two incisions compared to one for open reduction internal fixation of a both bones forearm fracture?

Explanation
Question 33
A 25-year-old male presents to the emergency department with a mangled lower extremity that is not salvageable. He undergoes transfemoral amputation. Three months later the patient presents to the office with the limb sitting in an abducted position. What important step was forgotten during the amputation?

Explanation
Question 34
A still active 86-year-old pastry chef falls in her kitchen and notes pain and deformity of her little finger. There are no open wounds. Radiographs are shown in Figures 49a and 49b. What is the most appropriate management?
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.
Question 35
Which of the following is an advantage of computer-assisted navigation used to place medullary nail interlocking screws compared to a freehand techinque?

Explanation
Ricci et al compared two fluoroscopic navigation tracking technologies, optical and electromagnetic versus standard freehand fluoroscopic targeting, in a standardized foam block model for placement of interlocking screws. They found that fluoroscopy time (seconds) and number of fluoroscopy images were significantly less when using the computer-guided systems than for freehand-unguided insertion. Average distance of pin placement from the target in the foam blocks was significantly greater for controls than for each of the navigated systems.
Suhm et al performed a prospective controlled clinical study to compare fluoroscopic guidance with fluoroscopy-based surgical navigation for distal locking of intramedullary implants. The surgical navigation group showed increased procedure time, but equivalent precision with reduced radiation exposure. There was no significant difference in the technical reliability between both groups.
Question 36
What is the most likely cause of the lesion shown in Figures 35a and 35b?
Explanation
REFERENCES: Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Jarvinen TA, Jarvinen TL, Kaariainen M, et al: Muscle injuries: Biology and treatment. Am J Sports Med 2005;33:745-764.
Question 37
A posterolateral approach to the tibial plafond proceeds between what two muscles?
Explanation
lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most
medially within the lateral compartment, and the flexor hallucis longus lies most laterally
in the deep posterior compartment.
REFERENCES: Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 515.
Question 38
An otherwise healthy 57-year-old woman has limited range of motion and moderate effusion after undergoing total knee arthroplasty 6 months ago. One of two cultures of joint aspirate reveals methicillin-resistant Staphylococcus epidermidis. Management should now consist of
Explanation
REFERENCES: Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218.
Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993;24:751-759.
Oyen WJ, Claessens RA, van Horn JR, et al: Scintiographic detection of bone and joint infections with indium-111-labeled nonspecifonal human immunoglobulin G. J Nucl Med 1990;31:403-412.
Question 39
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Omer GE Jr: Osteotomy of the clavicle in surgical reduction of anterior sternoclavicular dislocation. J Trauma 1967;7:584-590.
Question 40
-Figures 7a through 7c are the radiograph and MRI scans of a 72-year-old woman who has had back and leg pain for 3 months. Her pain is worse with prolonged walking and relieved with bending forward.Examination reveals normal strength and sensation in her legs with intact pedal pulses. She has persistent pain despite physical therapy, medications, and epidural injections. What is the most appropriate treatment option?
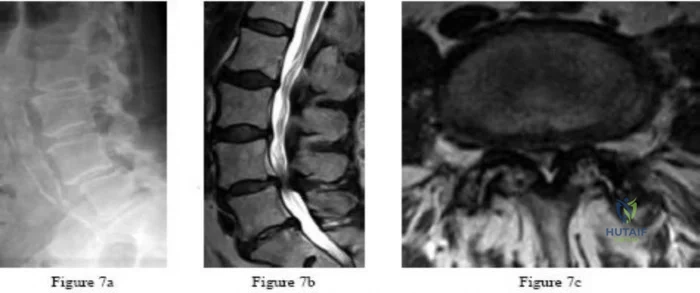
Explanation

Question 41
Preservation or reconstruction of which of the following structures is essential to minimize the risk of hallux valgus developing after removal of part or all of the medial sesamoid?
Explanation
REFERENCES: Dedmond BT, Cory JW, McBryde A Jr: The hallucal sesamoid complex. J Am Acad Orthop Surg 2006;14:745-753.
Lee S, James WC, Cohen BE, et al: Evaluation of hallux alignment and functional outcome after isolated tibial sesamoidectomy. Foot Ankle Int 2005;26:803-809.
Question 42
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of Review Topic

Explanation
Question 43
5 units PRBCs. The estimated blood loss was 1276cc and not affected by the fracture pattern or high/low energy pattern. They concluded that preoperative hemorrhage contributed to transfusion needs more than intraoperative blood loss.
Explanation
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?
Decreased joint penetration of distal screws
Increased rigidity
Decreased need for delayed hardware removal
Decreased peroneal irritation
Improved distal fixation Corrent answer: 4
Posterior antiglide plating is a technique that involves placement of a plate on the posterior aspect of the distal fibula, using the plate as a reduction tool and direct buttress against distal fracture fragment displacement.
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
OrthoCash 2020
A 24-year-old female sustains a surgical neck proximal humerus fracture in a motor-vehicle collision. She undergoes open reduction and internal fixation but heals in 45 degrees of varus and has significant limitation of shoulder range of motion despite 9 months of conservative treatments. What is the most appropriate treatment at this time?
Manipulation under anesthesia
Humeral head resurfacing
Shoulder hemiarthroplasty
Revision open reduction internal fixation with osteotomy
Reverse total shoulder arthroplasty Corrent answer: 4
Malunions of the proximal humerus typically result in significant restrictions in range of motion. This young patient has sustained a proximal humeral malunion, and treatment should include a corrective osteotomy for improved outcomes, as she has failed conservative treatment.
The cited reference by Williams et al as well as the referenced article by Siegel et al explain various techniques in management of proximal humerus malunions. They state that the two primary indications for surgical management of proximal humerus malunion include 1) pain and 2) diminished function resulting from limited range of motion. Because this patient is young, you would attempt revision ORIF/osteotomy as opposed to humeral head arthroplasty.
OrthoCash 2020
A 6-year-old boy with progressive bilateral genu varum undergoes the surgeries shown in Figure A. On postoperative rounds later that day, the patient appears sedated after several doses of pain medication. His toes are pink with brisk capillary refill however, passive motion of his toes causes pain. Among the answer choices listed, what is the best management strategy for this child?

Elevate his legs and reevaluate on morning rounds
Adjust his pain medication to accommodate for his increasing pain
Administer a muscle relaxant for leg spasms
Cast removal and measurement of compartment pressures with a standard device
Examine the cast for areas of constriction and reevaluate in the morning Corrent answer: 4
Intracompartmental pressure measurements should be performed when pain with passive motion of the toes is found in young patients with insufficient clinical data to establish a definitive diagnosis of compartment syndrome. The child in this clinical vignette has Blount’s disease which was treated with bilateral tibial osteotomies, a procedure commonly associated with compartment syndrome.
Pain with passive stretch is the most sensitive clinical sign of elevated compartment pressures prior to the onset of ischemia in compartment syndrome. Pain is difficult to assess in children at baseline, therefore, a high level of suspicion should exist and compartment pressure monitoring should be performed in unreliable patients.
Mubarak et al. reported on a series of 27 patients subjected to intracompartmental pressure monitoring for a clinical suspicion of acute compartment syndrome. The wick catheter technique was employed not only to aid in the diagnosis of compartment syndrome at an early stage but also to indicate the effectiveness of the decompressions when used intraoperatively during fasciotomies.
Matsen et al. reported on 24 children with compartment syndrome following injuries and surgery. The most common etiologies identified were fractures, vascular injuries, and tibial osteotomies. Compartment pressure measurements were helpful in establishing the diagnosis of compartment syndrome in young patients and in those with neurologic or vascular injuries with ambiguous clinical findings.
Figure A reveals an AP radiograph of bilateral knees status post valgus-producing tibial osteotomies and epiphysiolyses of the medial tibial physes in a 6-year-old male with Blount’s disease.
Incorrect Answers:
OrthoCash 2020
A 16-year-old male was struck by an automobile while riding his bicycle. He sustained the injuries in Figure A. Which of the following orthopedic injuries is MOST associated with this injury?

Brachial plexus injury
Ipsilateral clavicle fracture
Pelvic ring injury
Rib fracture
Spine fracture
Figure A demonstrates a scapula body fracture. Rib fractures are the most common orthopedic injury associated with these high-energy fractures, with a 52% incidence.
Scapula fractures are associated with high-energy trauma and have a reported mortality rate of 2-5%. Approximately 50% of high-energy scapular fractures involve the body and spine. Most scapular fractures may be treated conservatively with sling immobilization followed by early motion with no expected functional deficits. Indications for operative management of scapular fractures include glenohumeral instability with >25% of glenoid involvement or
>5mm of articular step-off, excessive medialization of the glenoid, displaced scapular neck or coracoid fractures, and open fractures.
Baldwin et al. retrospectively reviewed 9,543 scapular fractures utilizing the US National Trauma Database. They reported that the most commonly associated fractures were rib fractures (52.9%), followed by fractures of the spine (29.2%), clavicle (25.2%), and pelvis (15.3%). They concluded that lung and head injuries occurred in 47.1% and 39.1% of the cases, respectively.
Brown et al. retrospectively reviewed the association between scapular fractures (SF) and blunt thoracic aortic injury (BTAI). They found that in 35,541 blunt trauma admissions, SF and BTAI occurred in 1.1% and 0.6% of patients, respectively. They noted that most of the patients with SF had associated injuries (99%), but only four patients with SF had BTAI. The most common injuries associated with SF were rib (43%), lower extremity (36%), and upper extremity (33%) fractures. They concluded that SF is uncommon after blunt trauma, but patients with SF almost always have significant associated injuries and indicates a high amount of energy.
Figure A demonstrates a high-energy scapular body fracture which may benefit from surgical intervention
Incorrect Answers:
OrthoCash 2020
Which of the following amputations will lead to the greatest oxygen requirement per meter walked following prosthesis fitting?
Above-knee-amputation (transfemoral)
Below-knee-amputation (transtibial)
Through Knee
Syme
Midfoot
The general trend is increasing energy requirement for more proximal amputations. Amputation should be performed at the lowest possible level in order to preserve the most function.
Pinzur compared 5 patients with amputations at midfoot, Syme’s, BKA, through knee, and AKA with five controls. Walking speed and cadence decreased while oxygen consumption per meter walked increased with each more proximal amputation.
The only exception is the Syme which was the most energy efficient even though it is more proximal to the midfoot amputation.
OrthoCash 2020
An otherwise healthy 30-year-old male sustains a left forearm injury as a result of a fall from a ladder. Initial examination in the emergency room reveals a clean 2 centimeter laceration over the volar forearm associated with the radiographs shown in Figures A and B. Treatment should consist of irrigation and debridement of the wound followed by which of the following?

Closed reduction and casting of left radius and ulna
Temporary external fixation of the left radius and ulna
Definitive external fixation of the left radius and ulna
Open reduction and internal fixation of the left radius and ulna with delayed skin closure
Open reduction and internal fixation of the left radius and ulna with immediate skin closure
The clinical scenario is consistent with an open fractures of the distal radial and ulnar shafts. Literature shows that definitive plating of an open forearm fracture followed by primary closure of the wound is acceptable treatment at the time of injury.
Chapman et al performed a retrospective review of 50 patients with immediate internal plate fixation of an open diaphyseal fracture of the forearm. The functional results were excellent or good in 85%.
The review by Levin is a comprehensive review of the literature on early versus delayed closure of open fractures, and covers the change in thought from previous literature, including change in technology, surgical techniques, and a more critical review of previous literature.
OrthoCash 2020
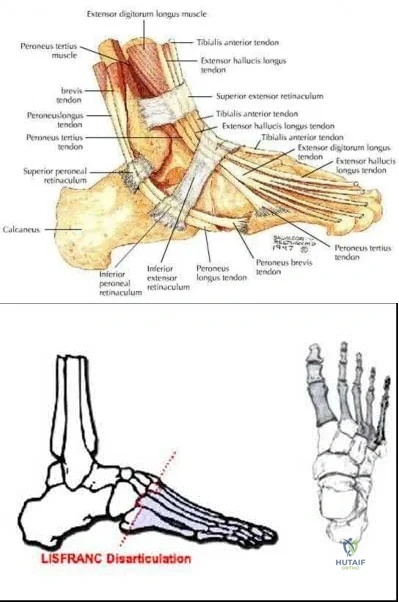
During a Lisfranc (tarsometatarsal) amputation of the foot, which of the following is crucial to prevent the patient from having a supinated foot during gait.
Releasing the posterior tibialis tendon
Preserving the soft-tissue envelope (peroneus brevis, tertius and plantar fascia) around the fifth metatarsal base
Myodesis of the anterior tibialis to the medial and middle cuneiforms
Lengthening of the gastrocsoleus (achilles tendon)
Osteotomy through 1st metatarsal Corrent answer: 2
A Lisfranc amputation is through the tarsometatarsal joints, except the 2nd metatarsal, which is osteotomized to preserve the stability of the medial cuneiform. To prevent the patient from supinating the foot following this amputation, the evertors on the foot must be maintained. The principal evertors are the peroneus brevis and longus (Illustration A). Therefore, the function of the peroneus brevis must be preserved. Technically this is done preserving the soft-tissue envelope (peroneus brevis, tertius and plantar fascia) around the fifth metatarsal base.
Illustration B depicts the level of a Lisfranc amputation of the foot. Incorrect Answers:
The posterior tibialis is the primary supinator of the foot, and releasing it
would lead to an eversion deformity. The tibialis posterior tendon attachment to the bases of the second and third metatarsals will actually be released with this amputation, but the main attachment to the navicular preserved.
The anterior tibialis dorsiflexes and inverts the foot, but transferring it to the medial and middle cuneiforms would mimick its native function to dorsiflex and invert the foot.
A lengthened Achilles would lead to increased dorsiflexion, not supination.
Osteotomy of 2nd MT is crucial to preserve the medial cuneiform and midfoot stable.
OrthoCash 2020
A 39-year-old male is thrown from his motorcycle into a fast-food restaurant and sustains a closed pelvic ring injury. During placement of percutaneous iliosacral screws, the outlet radiograph in Figure A is obtained. What purpose does this view serve?
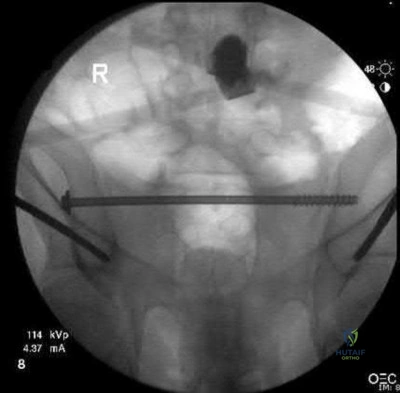
Evaluation of possible injury to L5 nerve root
Evaluation of anterior-posterior position of screw(s)
Best visualization of sagittal curvature of sacral ala
Best visualization of spinal canal
Best visualization of sacral neural foramina Corrent answer: 5
Figure A shows an intraoperative outlet view, which provides the best visualization of the neural foramina (and possible screw placement into these foramina). This view provides information regarding cephalad-caudad placement of the screw, whereas the inlet view provides information regarding the anterior-posterior position of the screw. The lateral sacral view provides information regarding the sagittal curvature of the sacral ala and gives information regarding possible iatrogenic L5 nerve injury as it goes over the sacral ala.
The referenced article by Routt et al is a review article regarding the safety and techniques of percutaneous pelvic ring fixation.
OrthoCash 2020
A 35-year-old male sustains a closed Schatzker VI tibial plateau fracture. Two weeks following external fixation, examination reveals intact sensation, palpable pulses and no soft tissue compromise. An axial CT image is shown in Figure A. What is the optimal surgical plan?
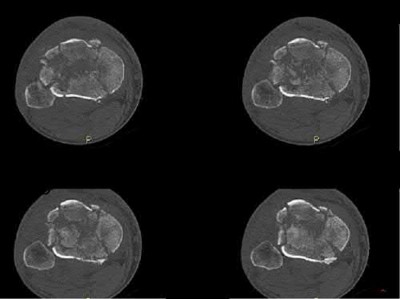
Medial and lateral plate fixation through two approaches
Medial and lateral plate fixation through a single anterior approach
Lateral locking plate fixation
Continued external fixation until union
Multiplanar transarticular external fixator Corrent answer: 1
The Figure shows a bicondylar tibial plateau fracture. The goals that need to be met when treating tibial plateau fractures are the following: restoration of mechanical axis alignment, restoration of condylar width, articular reduction, and restoration of knee stability. Since the soft tissue envelope is favorable, open reduction internal fixation with dual incisions and dual plates will provide the best probablity of achieving those goals.
Gosling et al did a biomechanical evaluation in cadavers comparing lateral locked plating with a combined medial and lateral plate and found no difference in resistance to vertical subsidence even with loads exceeding the average body weight. However, this was a cadaveric study with no mention and capability of analyzing articular reduction. Lateral locked plating only allows for indirect reduction of the medial plateau.
Barei et al in a retrospective review found that comminuted bicondylar tibial plateau fractures can be successfully treated with open reduction and medial and lateral plate fixation using 2 incisions, and postulate that the use of 2 incisions may contribute to a lower wound complication rate. A two incision approach allows not necessarily for a stronger construct as some studies are controversial, but for a more accurate reduction and restoration of alignment.
OrthoCash 2020
Which of the following is true regarding the use of the saline injection load test to diagnose traumatic knee arthrotomies?
Addition of methylene blue to the saline load test increases the sensitivity of the test
Injection of 110ml of saline will diagnose 95% of knee arthrotomies
Injection of 175ml of saline will diagnose 99% of knee arthrotomies
A superomedial injection location requires significantly less fluid than a inferoeromedial injection location
A history and physical exam by an orthopaedic surgeon has equivalent sensitivity to saline load test at detecting a traumatic arthrotomy
Injection of 175ml of saline will diagnose 99% of knee arthrotomies.
Clinical evaluation alone to determine if a periarticular laceration has penetrated the joint can often be incorrect. A Saline Load Test (SLT) is an effective methods to detect intraarticular penetration. New studies have shown addition of methylene blue does not improve the diagnostic value of the saline load test. The use of a CT scan can be helpful, especially in the presence of intra-articular air.
Voit et al. investigated the sensitivity of the clinical exam and a saline load test in 50 consecutive patients with periarticular lacerations suggestive of joint penetration. In 14 there was leakage of fluid on saline load test. In six of these patients, the clinician had judged there was no traumatic arthrotomy based on physical exam and clinical history. They therefore concluded performing a saline load test is important adjunct and the clinical exam alone can not be relied on to detect traumatic arthrotomies.
Nord et al. found that the volumes of saline that were needed in order to effectively diagnose 75%, 90%, 95%, and 99% of the knee arthrotomies were
110, 145, 155, and 175 mL, respectively. They also found that an inferomedial injection location required significantly less fluid than a superomedial injection location did.
Metzger et al. studied 58 patients that underwent saline load test with about 100ml of saline injected (methylene blue 29, normal saline 29). They found that the false-negative rate was 67% (methylene blue 69%, normal saline 66%). They concluded the addition of methylene blue does not improve the diagnostic value of the saline load test.
Konda et al. performed a study evaluationg the role of CT scan versus saline load test. They found that the sensitivity and specificity of the CT scan to detect traumatic arthrotomy was 100%. In a subgroup of 37 patients that received both a CT scan and the conventional saline load test, the sensitivity and specificity of the CT scan was 100% compared to 92% for the saline load test (p<0.001).
Incorrect Answers:
OrthoCash 2020
A 36-year-old rancher is involved in a tractor roll-over accident and sustains the injury shown in Figure A to his dominant right arm. After undergoing rigid anatomic fixation of the fracture, the distal radio-ulnar joint (DRUJ) remains incongruent. What is the next step in management?

Revision plating of the fracture
Revision reduction and intramedullary fixation
Reduction of interposed extensor carpi ulnaris tendon
Reduction of interposed pronator quadratus tendon
Reduction of interposed flexor carpi ulnaris tendon Corrent answer: 3
The most likely cause of persistent DRUJ incongruity after anatomic reduction and fixation of the radial shaft fracture of the answers above is interposition of the extensor carpi ulnaris (ECU) tendon. The tendon must be extricated from the joint to permit DRUJ reduction.
Gaeleazzi fracture-dislocations, such as that seen in Figure A, are typically stable once the radial shaft fracture is anatomically reduced. After fixation, the DRUJ is translated in pronation, supination, and in a neutral position to test for stability. A “clunk” during passive motion of the DRUJ is further evidence of gross instability. Gross laxity can be treated by splinting in supination or by pinning the DRUJ. However, ECU tendon interposition has been reported as a possible cause of a persistently irreducible DRUJ. Radiographic findings typically demonstrate a dorsally displaced ulnar head and a widened DRUJ. The interposed tendon must be removed from the joint, often through a separate dorsal approach to permit DRUJ reduction.
Bruckner et al. review the evaluation and management of complex dislocations of the DRUJ. The authors note that these injuries are associated with frequent irreducibility, recurrent subluxation, or soft reduction of the DRUJ secondary to interposed tissue. In their institutional series, four of the 11 cases of Galeazzi fractures were associated with complex DRUJ dislocations, most commonly due to displacement of the ECU tendon volar to the ulna, necessitating open reduction. They cautioned that unobtainable or unconvincing reductions should warrant surgical exploration.
Paley et al. reported two cases of an irreducible DRUJ after radial shaft fracture fixation. The authors describe an empty ECU tendon sulcus on the dorsum of the wrist in both cases. One case was noted and addressed intraoperatively.
However, the second case was not identified and this patient went on to endure persistent subluxation and diastasis of the DRUJ, ultimately experiencing a poor result. The authors advocate a separate dorsal exposure to reduce the ECU.
Hanel and Scheid reported a case of entrapment of the ECU in the DRUJ in a skeletal immature 12 year old boy. They noted that intraoperative radiographic analysis was significant for a widened DRUJ and dorsally displaced ulnar head. These authors too advocated a separate dorsal exposure to approach and extricate the ECU tendon.
Incorrect answers
OrthoCash 2020
A 58-year-old right-hand-dominant computer programmer trips and falls onto his right arm. He reports right arm pain and that his elbow felt "sloppy". His initial lateral radiograph is shown in Figure A. The orthopedic junior resident counsels him that he will likely need a radial head arthroplasty, ligament repair, and possible fixation of the ulna. What factor would most significantly affect the decision to surgically address the ulna fracture?

Degree of radial head comminution
The deforming force acting on the avulsed fracture fragment
Size of fragment and elbow stability after radial head replacement
The degree of fracture displacement
Patient age and bone quality Corrent answer: 3
The size of the fragment and degree of elbow instability following radial head fixation or replacement most often determines the intraoperative decision on coronoid fragment fixation.
The radial head is a secondary restraint to posterolateral rotatory instability (PLRI) of the elbow, while the coronoid provides an anterior and varus buttress to the ulnohumeral joint, resisting posterior dislocation. The medial ulnar collateral ligament attaches to the anteromedial facet of the coronoid, so large medial facet fractures may displace and cause varus posteromedial instability (PMRI). However, in terrible triad injuries (causing PLRI), small coronoid tip fractures are more common. These are typically left as they most often do not contribute to elbow instability. Therefore in most cases, radial head replacement and lateral ligamentous repair are sufficient to restore stability.
However larger coronoid base fractures may require fixation in order to stabilize the elbow. In these cases, the coronoid fracture may be addressed through the lateral window after radial head resection and before the trial implant is assessed. The anterior capsule can be tied down to the ulna or if the fracture is large enough, it may sometimes tolerate internal fixation.
Conversely, a buttress plate for the coronoid may be applied via a medial approach in the setting of a large coronoid base fracture as in PMRI.
Ring et al. reviewed 11 terrible triad injuries including 7 of which had the radial head surgically addressed and 4 of which had undergone radial head excision. The authors found that all four patients who underwent radial head excision dislocated after surgery. Only four patients had a satisfactory result, and all of these had fixation of the radial head, two requiring concomitant repair of the lateral ulnar collateral ligament (LUCL). The authors concluded that terrible triad injuries were unstable, prone to redislocation and that radiocapitellar contact is critical for ulnohumeral stability.
Pugh et al. reviewed 36 cases of terrible triad injuries in which all coronoid fractures were addressed, either with screw fixation or suture repair of the anterior capsule. The authors reported that the average arc of motion postoperatively was 112 degrees, Mayo score was 88, and concentric stability was restored in 34/36. There were 8 complications requiring re-operation. They concluded that coronoid fixation with radial head fixation or replacement yields a stable elbow suitable for early motion.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They found that radial head excision even in the setting of an intact LUCL lead to posterolateral laxity. Furthermore, if 30% of the coronoid tip was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement. However, if 50% of the coronoid was
excised, even with a radial head replacement dislocation occurred. They concluded that so long as the radial head is replaced, small coronoid fractures may not need to be repaired.
Figure A demonstrates a comminuted radial head fracture, a small coronoid fracture, and subluxation of the ulnohumeral joint.
Incorrect answers:
OrthoCash 2020
What is the most appropriate plating technique utilized for the medial malleolus fracture typically seen in a displaced supination-adduction ankle fracture?
Tension band plating
Antiglide plating
Bridge plating
Neutralization plating
Submuscular plating
A supination-adduction ankle fracture leads to a vertical fracture of the medial malleolus. Traditional fixation of the medial malleolus with oblique screws from the tip of the malleolus directed proximally will ineffectively protect against shear forces at the fracture site; these also are directed quite obliquely to the vertical fracture line, and therefore have poor biomechanical resistance to failure. An antiglide plate is used medially to prevent displacement of the fracture segment due to shear forces.
According to the referenced article by Toolan et al, placement of two horizontal (perpendicular to the fracture line) lag screws from medial to lateral are
biomechanically the most important aspect of the construct whether a plate is used or not.
OrthoCash 2020
A 25-year-old Norwegian amateur curler slips on the ice, falling onto an outstretched right elbow. He is taken to the local teaching hospital and radiographs demonstrate a significantly comminuted radial head fracture and coronoid base fracture. His elbow is reduced and splinted. To restore stability and allow early range of motion, which of the following will most likely need to be performed in most cases?
Radial head fixation or replacement
Radial head fixation or replacement and coronoid fixation
Radial head fixation or replacement, coronoid fixation, and lateral ulnar collateral ligament (LUCL) repair
Radial head fixation or replacement, coronoid fixation, LUCL and medial ulnar collateral ligament (MUCL) repair
Radial head fixation or replacement, coronoid fixation, LUCL and MUCL repair, and application of a hinged fixator
The patient has sustained a "terrible triad" injury, classically involving a radial head fracture, coronoid fracture, and elbow dislocation. These often involve LUCL injuries and a traumatic injury in the radiocapitellar joint. Stability is achieved with radial head replacement (or fixation), coronoid fixation (in cases with a large coronoid fracture), and lateral soft tissue repair.
Posterolateral rotatory instability (PLRI) following a terrible triad injury is usually caused by a fall on an extended arm that produces a valgus, axial, and rotatory force. The mechanism of injury begins laterally and moves medially.
Hence, the LUCL fails first, followed by the anterior capsule (or coronoid), and lastly the MUCL. Even following fixation, patients often lose some degree of their flexion-extension arc, may develop post-traumatic arthritis, or most commonly may have persistent instability. The radial head is a primary restraint to PLRI and must be either replaced with a prosthesis or fixed in the setting of a terrible triad injury. Replacement is typically chosen when the radial head is in more than 3 fragments. Coronoid fractures should be fixed when they involve >30-50% of the coronoid base. However, the best way to determine if coronoid fixation is necessary is with an intraoperative fluoroscopic examination.
Forthman et al. reviewed outcomes following the management of 34 elbow fracture-dislocations. In all cases, the radial head was replaced or underwent fixation. The MUCL was not repaired in any case. The authors noted only 2 cases of post-operative instability, one terrible triad, and one combined capitellum and trochlea fracture. The authors noted that both cases were related to non-compliance. The remaining 32 averaged 120 degrees of flexion-extension and 74% had good-excellent outcomes. The authors concluded that MUCL repair is not required for elbow dislocations so long as the radial head, large coronoid fractures, and LUCL are addressed.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They found that radial head excision even in the setting of an intact LCL leads to posterolateral laxity. If 30% of the coronoid was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement. However, if 50% of the coronoid was excised, even with a radial head replacement, dislocation occurred. This led the authors to conclude that long as the radial head was replaced, small coronoid fractures may not need to be repaired.
Papatheodorou et al. reviewed 14 terrible triad injuries (all of which had Regan-Morrey type 1 or 2 coronoid fractures) that underwent surgical fixation or replacement of the radial head combined with LUCL repair. The authors noted that intraoperative stability was confirmed in all cases without coronoid fixation, MCL repair, or an external fixator. The authors concluded that coronoid fixation is not required in fractures up to 50% the height of the coronoid and that MCL repair is not necessary.
Incorrect answers:
OrthoCash 2020
A 32-year-old female sustains the injury shown in Video A. The right-sided pelvic injury is best classified as which of the following?
Lateral compression 1
Lateral compression 2
Vertical shear
Anterior-posterior compression 2
Anterior-posterior compression 3
The injury shown in Video V reveals a right sided posterior ilium fracture, which is known as a crescent fracture. The presence of a crescent fracture is consistent with a lateral compression type 2 injury; this differentiates this from a type I injury. The ipsilateral anterior sacrum has a small impaction injury anteriorly while the contralateral SI joint has a minor amount of anterior sacral impaction indicative of a lateral compression type I injury.
The reference by Burgess et al is the primary source of the mechanism classification of pelvic ring injuries. Overall blood replacement averaged 5.9 units (lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units). Overall mortality was 8.6% (lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear,
0%; combined mechanical, 18.0%).
Incorrect answers:
1: The presence of a crescent fracture means this is at least a LC-2 injury. The left-sided fracture pattern is consistent with an LC-1 pattern.
3: A vertical shear fracture pattern would exhibit some vertical displacement and does not typically exhibit the crescent fragment.
4: The fracture pattern does not match an anterior-posterior compression pattern.
5: The fracture pattern does not match an anterior-posterior compression pattern.
OrthoCash 2020
A 35-year-old zookeeper fell 10 feet while preparing an exhibit for a grand reopening, landing on his left arm. The patient is then evaluated by a keen orthopedic resident in the emergency room who describes the zookeeper's injuries to his chief. He describes a comminuted radial head fracture and posterolateral ulnohumeral dislocation. The chief resident orders a CT scan which demonstrates a coronoid fracture involving 50% the height with no involvement of the anteromedial facet. During surgery, the trauma surgeon replaces the radial head and repairs the lateral collateral ligament complex. The
elbow is splinted in elbow flexion and pronation. The patient begins range of motion exercises with her occupational therapist 3 days after surgery, and her elbow dislocates. What is the most likely reason for her instability?
Length of immobilization
Position of immobilization
Lack of coronoid fixation with medial buttress plate
Lack of coronoid fixation from lateral approach
Lack of medial collateral ligament repair Corrent answer: 4
The zookeeper sustained a "terrible triad" injury with resulting posterolateral rotatory instability (PLRI). To prevent post-operative instability, large coronoid fractures should be fixed, and this would be performed through a lateral approach given that the radial head will be replaced.
The coronoid serves as an anterior and varus buttress to the ulnohumeral joint, resisting posterior dislocation. Though the coronoid tip has no soft tissue attachments, the medial ulnar collateral ligament attaches to the anteromedial facet of the coronoid. A coronoid fracture through the anteromedial facet, such as in the setting of posteroMEDIAL rotatory instability, would require a medial buttress plate to restore varus stability. In a coronoid base fracture involving 50% of the coronoid, fixation is required even when a radial head arthroplasty is performed. This can be done with suture fixation via a bone tunnel through the ulna or with screws from dorsal to volar. Failure to fix a large coronoid base fracture would result in persistent instability, as with the patient in this vignette.
Ring et al. reviewed 11 terrible triad injuries - including 7 of which had the radial head surgically addressed and 4 of which underwent radial head excision. They noted that all four patients who underwent radial head excision dislocated after surgery. Moreover, only four patients had a satisfactory result, and all of these had fixation of the radial head, with two requiring concomitant repair of the lateral ulnar collateral ligament (LUCL). The authors concluded that terrible triad injuries are unstable, prone to redislocation and that radiocapitellar contact is critical for ulnohumeral stability.
Schneeberger et al. evaluated elbow instability after simulated terrible triad injuries. They showed that radial head excision even with an intact LUCL resulted in persistent posterolateral laxity. If 30% of the coronoid was excised, the elbow dislocated at 60 degrees of flexion, but stability was restored with a radial head replacement alone. If 50% of the coronoid was excised, even with
a radial head replacement, dislocation occurred. The authors concluded that so long as the radial head was replaced, small coronoid fractures may not need to be repaired, but large fractures involving 50% or more would require fixation even if the radial head and LUCL were addressed.
Moro et al. treated 25 unreconstructible radial head fractures with a metal radial head arthroplasty. The authors reported a DASH score of 17, PRWE of 17, and Mayo elbow score of 80. Poor outcomes were seen in those with psychiatric disorders or those involved in a worker's compensation claim. The authors reported that radial head arthroplasty resulted in stable elbows with mild-moderate physical impairment.
Ring, Quintero, and Jupiter reviewed 56 patients with radial head fractures who underwent surgical fixation. Of the comminuted Mason type-3 fractures that underwent ORIF, they found that 13/14 had a poor result. The authors recommend that fractures with 3 or fewer fragments are amenable to fixation while those with 4 or more articular fragments are not.
Incorrect answers:
OrthoCash 2020
Which of the following injuries would require plating of the radius along with closed reduction and evaluation of the distal radioulnar joint (DRUJ)?
Nightstick fracture
Galeazzi fracture
Monteggia fracture
Rolando fracture
Smith fracture
A Galeazzi fracture is a fracture of the distal third of the radius with dislocation of the distal radioulnar joint. It commonly results from a fall onto an outstretched hand with the forearm in pronation.
A Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction and fixation of the radial shaft, and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. Otherwise, either open or closed reduction with pinning can be undertaken to stabilize the joint. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
Acute intervention results in improved outcomes as compared to delayed reconstruction.
Rettig et al. retrospectively analyzed 40 patients with Galeazzi fracture-dislocations that were treated with open reduction and internal fixation of the radial shaft fracture. They noted that a radial shaft fracture located within
Question 44
A study was conducted in 500 patients to measure the effectiveness of a new growth factor in reducing healing time of distal radial fractures. The authors reported that average healing time was reduced from 9.2 to 8.9 weeks (P < 0.0001). Because the difference was highly statistically significant, they recommended routine clinical use of this drug despite its high cost. A more appropriate interpretation of these results is that they are
Explanation
REFERENCE: Ebramzadeh E, McKellop H, Dorey F, et al: Challenging the validity of conclusions based on P-values alone: A critique of contemporary clinical research design and methods. Instr Course Lect 1994;43:587-600.
Question 45
The afferent pain innervation of the L3-L4 facet joint arises from the medial branch nerve of
Explanation
REFERENCES: Nade SL, Bell E, Wyke BD: The innervation of the lumbar spinal joint and its significance. J Bone Joint Surg Br 1980;62:255-261
Kornick C, Kramarich SS, Lamer TJ, et al: Complications of lumbar facet radiofrequency denervation. Spine 2004;29:1352-1354.
Question 46
Figure 6 shows the lateral radiograph of a 22-year-old woman who has painful Scheuermanns’s kyphosis in the middle and lower thoracic spine. When planning surgical correction using instrumentation, the distal aspect of the instrumentation should ideally extend to the
Explanation
REFERENCES: Lowe TG: Scheuermann’s disease. Orthop Clin North Am 1999;30:475-487.
Lenke LG: Kyphosis of the thoracic and thoracolumbar spine in the pediatric patients: Prevention and treatment of surgical complications. Instr Course Lect 2004;53:501-510.
Question 47
A 2-year-old girl has had a 2-day history of fever and refuses to move her left shoulder following varicella. Laboratory studies show an erythrocyte sedimentation rate of 75 mm/h and a peripheral WBC count of 18,000/mm P 3 P . What is the most common organism in this scenario?
Explanation
REFERENCES: Schreck P, Schreck P, Bradley J, et al: Musculoskeletal complications of varicella. J Bone Joint Surg Am 1996;78:1713-1719.
Mills WJ, Mosca VS, Nizet V: Orthopaedic manifestations of invasive group A streptococcal infections complicating primary varicella. J Pediatr Orthop 1996;16:522-528.
Question 48
Performance parameters developed by the Centers for Medicare and Medicaid Services and the Centers for Disease Control and Prevention regarding prophylactic antibiotics include
Explanation
Question 49
Compact bone, titanium, stainless steel, cobalt-chrome
Explanation
In a patient with a previous compression hip screw in place at the time of total hip arthroplasty, what precautionary measures should be undertaken after hardware removal to prevent a periprosthetic fracture:
Question 50
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient?
Explanation
REFERENCES: Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 51
What is the most common reason an individual with a malignant soft-tissue tumor in the extremities seeks medical attention?
Explanation
REFERENCES: Brouns F, Stas M, De Wever I: Delay in diagnosis of soft tissue sarcomas. Eur J Surg Oncol 2003;29:440-445.
Rougraff B: The diagnosis and management of soft tissue sarcomas of the extremities in the adult. Curr Probl Cancer 1999;23:1-50.
Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 52
Staphylococcus aureus develops methicillin resistance through production of which of the following agents?
Explanation
REFERENCES: Fuda C, Suvorov M, Vakulenko SB, et al: The basis for resistance to beta-lactam antibiotics by penicillin-binding protein 2a (PBP2a) of methicillin-resistant staphylococcus aureus. J Biol Chem 2004;279:40802-40806.
Lim D, Strynadka NC: Structural basis for the beta lactam resistance of PBP2a from methicillin-resistant Staphylococcus aureus. Nat Struct Biol 2002;9:870-876.
Schwarz EM: Infections in orthopaedics, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 53
A 58-year-old man with type 1 diabetes mellitus is seen in the emergency department and he reports a 3-day history of a red swollen foot but no history of trauma. Examination reveals that the skin is intact, and the patient has discomfort with passive range of motion at the ankle, hindfoot, and midfoot joints. He denies any fever. Laboratory studies show a WBC count of 7,800/mm 3 , an erythrocyte sedimentation rate of 40 mm/h, a C-reactive protein level of 23, and a serum glucose of 100. A radiograph and MRI scans are shown in Figures 16a through 16c. What is the next most appropriate step in management?
Explanation
REFERENCES: Trepman E, Nihal A, Pinzur MS: Current topics review: Charcot neuropathy of the foot and ankle. Foot Ankle Int 2005;26:46-63.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 123-134.
Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Question 54
A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?
Explanation
REFERENCES: Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA,
JB Lippincott, 2003, vol 2, pp 1265-1271.
Meding JB, Keating EM, Ritter MA, et al: Total knee arthroplasty after high tibial osteotomy:
A comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am 2000;82:1252-1259.
Question 55
-are the anteroposterior (AP) and lateral radiographs of the right elbow of a 7-yearold boy who fell off the monkey bars onto his outstretched right hand. Immediate pain and swelling were noted around his elbow; there were no other injuries. His hand was neurovascularly intact. What is the best treatment for this fracture?

Explanation

Question 56
A 14-year-old boy is seen for back pain. Radiographic evaluation reveals a grade III isthmic spondylolisthesis. What measurement is most useful in predicting the likelihood of progression? Review Topic
Explanation
Question 57
A 57-year-old man who plays recreational sports reports pain in his dominant shoulder. An MR arthrogram is shown in Figure 57. During arthroscopy of the shoulder, what pathology is most likely to be found? Review Topic
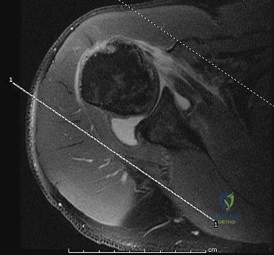
Explanation
Question 58
What is the average version of the humeral head (with respect to the transepicondylar axis)? Review Topic
Explanation
One of the goals of primary anatomic total shoulder arthroplasty (TSA) is recreation and reconstruction of proximal humeral anatomy. Modular prostheses have evolved to provide surgeons with better capability to recreate proximal humeral morphology based on humeral head inclination, retroversion, offset, height and size. In terms of size, humeral head thickness has been found in cadaver studies to be 70% of its radius of curvature. This can be helpful to avoid 'over-stuffing' the joint or leaving it too loose.
Boileau and Walch took digitized measurements of 65 humeri in order to create a computer model for proximal humeral morphology. They found that retroversion varied from -6.7 to 47.5 degrees, with a mean of 17.9. They advocate for prosthetic adaptability to recreate proximal humeral anatomy in a way that earlier generations of more geometrically constrained TSA implants could not.
Robertson et al. made 3D computed tomographic models of 60 humeri (30 pairs) to study proximal humeral morphology. They found mean retroversion to be 19 degrees, with a range of 9 to 31 degrees. They found that proximal canal version was similar to head version but that canal version in the middle and distal sections of the canal was variable.
Illustration A shows key proximal humeral morphologic parameters found by Robertson et al. in comparison with earlier studies (including Boileau's).
Incorrect Answers:
Question 59
What type of brace is shown in Figures 22a and 22b?
Explanation
REFERENCES: Mehta JA, Brown C, Sargeant N: Charcot restraint orthotic walker. Foot Ankle Int 1998;19:619-623.
Morgan JM, Biehl WC III, Wagner FW Jr: Management of neuropathic arthropathy with the Charcot restraint orthotic walker. Clin Orthop 1993;296:58-63.
Question 60
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
REFERENCES: Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 61
A radiograph of a 12-year-old boy who has had an insidious onset of pain in the right hip for the past 6 weeks shows diffuse narrowing of the joint space. Examination reveals that he is afrebile, and the range of motion of the hip is less than 50% of normal in all planes. Laboratory studies show an erythrocyte sedimentation rate of 21 mm/hr and a WBC of 11,000/mm3. What is the most likely diagnosis?
Explanation
This patient has no history of hemophilia given. Hemophilic arthropathy begins with a hemarthrosis.
In osteoid osteoma the pain is typically unrelenting, sharp, boring, worse at night, and relieved with aspirin. It is not associated with joint space narrowing.
The most common age for Legg-Calve-Perthes disease is 4-8 years. It causes AVN of the femoral head and widening of the medial joint space is an early radiographic finding.
In Bleck’s report on Idiopathic Chondrolysis JBJS 1983 nine cases were seen at the reporting institution between 1973 and 1978. The average age was 11.5 years. All the patients were otherwise healthy and had no history of systemic illness of previous trauma. All the patients reported the insidious onset of pain in the anterior part of the hip. All had a decreased passive ROM. Radiographic examination showed regional osteoporosis, premature closure of the femoral capital physis, narrowing of the joint space, and lateral overgrowth of the femoral head on the neck. All laboratory examinations were negative for evidence of infection or rheumatoid arthritis. Treatment consists of administration of aspirin, active non-loading exercise of the hip, and protected weight-bearing with crutches.
Question 62
For the athlete performing heavy exercise, the magnitude of core temperature and heart rate increase is most proportional to
Explanation
REFERENCES: Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524.
Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Sawka MN, Young AJ, Francesconi RP, et al: Thermoregulatory and blood responses during exercise at graded hypohydration levels. J Appl Physiol 1985;59:1394-1401.
Question 63
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
Explanation
REFERENCES: Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fixation: Techniques of application and prevention of complications. J Am Acad Orthop Surg 1996;4:44-53.
Garfin SR, Botte MJ, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1987;69:954.
Question 64
A 22-year-old patient has had severe groin pain for many months and is unable to engage in any physical activity. The AP radiograph of the pelvis shows minimal arthritis. The lateral radiograph of the hip is shown in Figure 33a. An MR-arthrogram is shown in Figure 33b. What is the most appropriate treatment at this stage? Review Topic

Explanation
Question 65
Figure 199 is the clinical photograph of a 68-year-old man with a history of atrial fibrillation who was treated with warfarin. Nine days after undergoing elective total hip arthroplasty, he has a swollen left thigh. His wound remains dry and he is afebrile. His erythrocyte sedimentation rate (ESR) is 25 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein (CRP) level is 6.1 mg/L (rr, 0.08-3.1 mg/L). Aspiration reveals 3246 white blood cells (WBCs)/µL with 47% polymorphonucleocytes. Treatment at this time should consist of
Explanation
This patient has a large postsurgical hematoma. Although his ESR and CRP level are elevated, they are not considered elevated given his recent surgery. Additionally, the hip aspiration reveals a synovial cell count lower than 10000 WBC/µL along with a low percentage of polymorphonucleocytes. Treatment at this time should consist of observation. The hematoma is likely attributable to postsurgical anticoagulation, considering his history of atrial fibrillation.
Question 66
Tendon fibroblasts detect applied strain through what mechanism?
Explanation
Question 67
What is the most common complication following reverse total shoulder arthroplasty?
Explanation
A. Open reduction internal fixation (ORIF) with parallel plates
B. ORIF with orthogonal plates and iliac crest bone grafting
C. Total elbow arthroplasty (TEA)
D. Closed reduction and percutaneous pinning
TEA is the best surgical option. McKee and associates published a multicenter randomized controlled trial comparing ORIF with TEA in elderly patients. TEA resulted in better 2-year clinical functional scores and more predictable outcomes compared with ORIF. TEA was also likely to result in a lower reoperation rate; one-quarter of patients with fractures randomized to ORIF could not achieve stable fixation. Further, Frankle and associates reported a comparative study of TEA versus ORIF in 24 elderly women. TEA outcomes were again superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed reduction and percutaneous pinning studies have not been published on the adult population. Correct answer : C
Question 68
A 24-year-old professional male soccer player has lower abdominal pain on exertion. He has pain with resisted hip adduction and with sit-ups. There is no palpable inguinal hernia with a Valsalva maneuver. Nonsurgical management has failed to provide relief. After ruling out malignancies, what is the next most appropriate step in management?
Explanation
REFERENCES: Meyers WC, Foley DP, Garrett WE, et al: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Biedert RM, Wamke K, Meyer S: Symphysis syndrome in athletes: Surgical treatment for chronic lower abdominal, groin, and adductor pain in athletes. Clin J Sport Med 2003;13:278-284.
Question 69
A 48-year-old man who is scheduled to undergo total knee replacement has an X-linked clotting disorder that leads to abnormal bleeding and recurrent, spontaneous hemarthrosis. Before undergoing surgery, he should have replacement therapy of
Explanation
Question 70
Radiotherapy for palliative pain control as the risk for pathological fracture is very small
Explanation
some centers, this procedure may contaminate the entire bone with tumor and make limb salvage nearly impossible if this is a sarcoma. If the incisional biopsy shows carcinoma, then intramedullary nailing with adjuvant radiotherapy would be completely appropriate.
Question 71
Which of the following statements best describes the instantaneous axis of rotation (IAR) for the functional spinal unit? Review Topic
Explanation
Question 72
A 20-year-old basketball player sustains a knee injury during a game and is seen in the orthopaedic clinic 3 days after injury. Examination reveals a positive Lachman, pivot shift, joint line tenderness, and moderate effusion. Which of the following tissue injuries is most likely causing the jointline tenderness? Review Topic
Explanation
Question 73
A concern when choosing irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene rather than lower dose–irradiated (4 Mrad) polyethylene is related to its inferior resistance to
Explanation
The higher the dose of radiation to the polyethylene, the higher the amount of cross-linking. Adhesive and abrasive wear resistance increases with an increase in cross-linking. However, fatigue properties of the material are decreased when polyethylene is melted (to remove free radicals) during the cross-linking process. Creep (deformation without wear) is also slightly increased with cross-linking of polyethylene.
Question 74
A patient with Charcot-Marie-Tooth disease has a progressively rigid cavovarus foot deformity. The patient states that the pain is restricted to the forefoot, where rigid claw toe deformities have developed. Which of the following structures is primarily involved in creation of a claw toe deformity?
Explanation
REFERENCES: Keenan MA, Gorai AP, Smith CW, Garland DE: Intrinsic toe flexion deformity following correction of spastic equinovarus deformity in adults. Foot Ankle 1987;7:333-337.
Pichney GA, Derner R, Lauf E: Digital “V” arthrodesis. J Foot Ankle Surg 1993;32:473-479.
Mizel MS, Michelson JD: Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint. Foot Ankle Int 1997;18:424-426.
Question 75
Figure 47 shows a transverse MRI scan of a patient’s left shoulder. The findings reveal which of the following abnormalities?
Explanation
REFERENCES: Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Cofield RH: Arthroscopy of the shoulder. Mayo Clin Proc 1983;58:501-508.
Question 76
An 83-year-old woman reports pain in her left middle finger after a minor injury. Laboratory studies show a WBC count of 7,000/mm 3 , an erythrocyte sedimentation rate of 3 mm/h, a uric acid of 10.4 mg/dL, and a normal serum protein electrophoresis. Radiographs are shown in Figures 49a and 49b. A core biopsy specimen is shown is Figure 49c. In addition to treatment of the finger fracture, treatment should include
Explanation
REFERENCES: Wise CM: Crystal-associated arthritis in the elderly. Clin Geriatr Med 2005;21:491-511.
Mudgal CS: Management of tophaceous gout of the distal interphalangeal joint. J Hand Surg Br 2006;31:101-103.
Question 77
When performing hip arthroscopy, the hip should be placed in neutral to slight internal rotation to protect which of the following structures? Review Topic
Explanation
Question 78
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
REFERENCES: Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Hoppenfeld S: Orthopaedic Neurology: A Diagnostic Guide to Neurologic Levels. Philadelphia, PA, JB Lippincott, 1977, pp 7-43.
Question 79
A year-old woman underwent an uncemented medial/lateral tapered femoral placement during a total hip arthroplasty. The orthopaedic surgeon noticed a nondisplaced vertical fracture in the calcar region of the femoral neck during final implant insertion. What is the most appropriate treatment?
Explanation
The recognized treatment for a proximal periprosthetic fracture is to first identify the extent and then optimize the correction of the fracture. Several studies indicate that proximal cerclage wiring is adequate to create "barrel hoop" stability of the proximal femur. Braided cables offer superior stability compared with twisted wires or Luque wires. Finally, the appropriate postoperative treatment is protected
weight bearing for 6 weeks, with periodic radiographs taken at 2-week intervals. Other options such as
cementing the femoral stem and using a revision arthroplasty device are indicated for unstable fractures.
Question 80
A 72-year-old female presents to your office with a 24-month old painful nonunion of a 3-part fracture of the proximal humerus. She has been treated conservatively with range of motion exercises but continues to complain of debilitating pain and dysfunction. Operative management should include:

Explanation
The referenced article by Cheung et al reviews treatment options for proximal humeral nonunions and reports successful use of arthroplasty in treating elderly osteoporotic proximal humeral nonunions as a pain relieving procedure.
Dines reported a case series of 20 chronic post-traumatic proximal humerus fractures including nonunions that were treated with shoulder arthroplasty achieving fair to excellent results in 90% at mid-term follow-up
Question 81
In either a ceramic-on-highly-cross-linked polyethylene (HXPE) or metal-on-HXPE component, increasing the ball head size leads to
Explanation
Increasing the size of the ball head increases the primary arc of motion prior to impingement and the jump distance prior to dislocation, assuming an acetabular component abduction of less than 90 degrees. Although HXPE has demonstrated decreases in linear wear rates even with ball head sizes larger than 28 mm, volumetric wear remains a concern. A larger ball head size does not significantly change offset, and larger metal ball heads are not associated with decreased risk for corrosion.
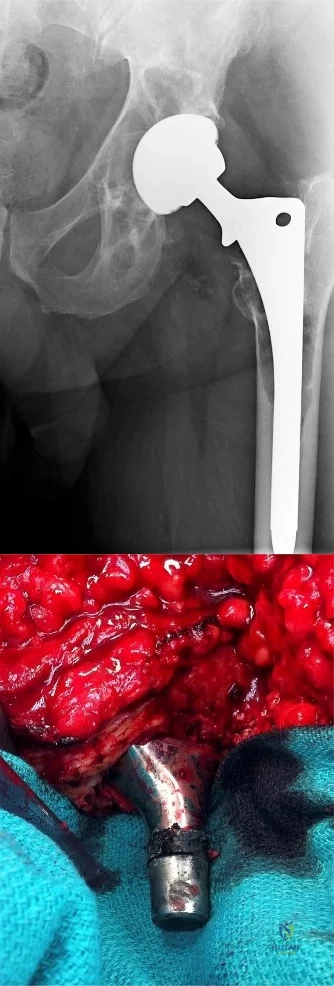
Question 82
Figures 4a and 4b show the radiographs of a 32-year-old man who has right groin pain with activity or prolonged standing. Which of the following factors would not prohibit consideration of acetabular liner exchange and grafting of the defects?
Explanation
REFERENCES: Maloney WJ, Herzwurm P, Paprosky W, Rubash HE, Engh CA: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 83
A 78-year-old male presents to clinic 4 weeks after left total shoulder arthroplasty. He has not been wearing his sling and reports that he developed increased pain after slipping in the shower. He used the arm to catch himself from falling. On examination, he can flex the shoulder to 70 degrees, limited by pain. Active external rotation with arm at the side is 50 degrees and active internal rotation is 5 degrees. Passive external rotation is to 80 degrees. A radiograph of the left shoulder is shown below in Figure A. What other complaint is the patient most likely to have? Review Topic

Explanation
Total shoulder arthroplasty is the preferred treatment for glenohumeral arthritis in patients with intact rotator cuff and good glenoid bone stock. The surgical approach involves detaching the subscapularis and capsule from the anterior humerus and dislocating the humeral head anteriorly. Post operatively, external rotation is limited to protect the subscapularis repair. If there is suspicion of a postoperative subscapularis tear, and ultrasound can be performed to confirm the diagnosis.
Miller et al. reported 7 cases of subscapularis tendon rupture after total shoulder arthroplasty, all of which were subsequently repaired. Decreased functional outcomes were observed in these patients, with lengthening techniques to address internal rotation contractures and prior surgery involving the subscapularis tendon as risk factors for rupture
Westoff et al. performed static and dynamic ultrasounds on 22 patients after total shoulder arthroplasty evaluating for numerous periarticular pathologies. The authors concluded that sonography is a useful tool for evaluation of peri-implant tissues after TSA.
Figure A shows an intact left total shoulder arthroplasty without evidence of fracture, dislocation, or hardware loosening. Illustration A shows the incision for the subscapularis tendon during TSA.
Incorrect Answers:
Question 84
A 72-year-old woman has had progressively increasing pain in the right knee for the past 6 months. She denies any trauma and has no pain in any other joints, but she notes occasional swelling in the knee and a catching sensation. Figures 31a and 31b show the plain radiographs and Figure 31c shows the MRI scan. Treatment should consist of
Explanation
REFERENCES: Lotke PA, Ecker ML: Osteonecrosis of the knee. J Bone Joint Surg Am 1988;70:470-473.
Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.
Question 85
Stiffness can occur following total knee arthroplasty. What is the most appropriate management for a patient who has deteriorating arc of motion after undergoing a revision knee arthroplasty 9 months ago?
Explanation
REFERENCES: Kim J, Nelson CL, Lotke PA: Stiffness after total knee arthroplasty: Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479-1484.
Gonzalez MH, Mekhail AO: The failed total knee arthroplasty: Evaluation and etiology. J Am Acad Orthop Surg 2004;12:436-446.
Question 86
What procedure can eliminate a sulcus sign? Review Topic
Explanation
Question 87
A 14-year-old patient has anterior knee pain. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 6a through 6e. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 18.
Question 88
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of
Explanation
shown some healing response with callus formation, but these techniques are not successful
in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions
of the clavicle.
REFERENCES: Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 89
A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment? Review Topic

Explanation
appears to be helpful. A hindfoot arthrodesis (usually triple) would be reserved if coalition resection proves to be unsuccessful. Achilles tendon lengthening and orthotic support, as well as debridement of the sinus tarsi, are not expected to result in a satisfactory outcome. The patient does not have a flatfoot deformity.
(SBQ13PE.64) A 5-year-old boy presents to clinic for evaluation of bilateral foot deformities shown in Figure 1. He is fully active and has no pain. The feet appear normal when he is sitting on the examination table, and there is supple passive motion at the subtalar joint. Passive ankle dorsiflexion is to neutral with knee in extension and 15 degrees with knee in flexion. What is the most appropriate next step? Review Topic

Spine MRI
Standing radiographs of the bilateral feet
Gastrocnemius stretching and nightime use of ankle foot orthosis
Gastrocnemius stretching and use of UCBL orthotic when ambulating
Gastrocnemius stretching
The patient is presenting with bilateral flexible pes planovalgus (or flexbile flatfoot). The most appropriate treatment in patients with a tight heel cord and no pain is gastrocnemius stretching
A flexible flatfoot in a child typically resolves spontaneously. Radiographs are typically indicated when there is pain to rule out other conditions. Treatment for patients without pain includes observation and gastrocnemius stretching. If there is pain, soft arch support or a more rigid UCBL can be used, but orthotics do not change the natural history. In patients with continued tightness in the heel cord despite aggressive stretching, gastrocnemius lengthening may be necessary.
Mosca reviews the management of flexible flatfeet in children and adolescents. He reports that there is no compelling evidence that an arch can be created with use of
orthotics. He proposes the following algorithm: patients with asymptomatic flatfeet are observed; symptomatic flatfeet with tight heel cords undergoing stretching until they become asymptomatic; symptomatic flatfeet with tight heel cords that do not respond to stretching (rare cases) are considered for surgery.
Figure A shows a young a patient with bilateral flatfeet when standing. Incorrect Answers:
abnormalities can seen in patients with cavovarus deformity Answer 2: Radiographs are indicated when there is pain to rule out other conditions. Answer 3: Ankle foot orthoses are not used for pes planovalgus Answer 4: UCBL would be indicated if the patient was having pain.
(SBQ13PE.42) Submuscular bridge plating is appropriate treatment for which of the following? Review Topic
A 2-month-old female with displaced, spiral, mid-diaphyseal femur fracture
A 26-month-old boy with a displaced spiral mid-diaphyseal femur fracture with
<2cm shortening
A 7-year old boy with a transverse, non-comminuted mid-diaphyseal femur fracture
A 7-year-old boy with a highly comminuted mid-diaphyseal femur fracture
A 15-year-old girl with a displaced butterfly fragmented mid-diaphyseal femur fracture
Submuscular bridge plating is appropriate for length-unstable femur fractures in skeletally immature patients ages 6 years and older.
Traditional plating of diaphyseal femur fractures in children has been abandoned due to the large incision and significant periosteal stripping involved. Submuscular plating with limited incisions and percutaneously applied fixation is a more biologically friendly way to achieve rigid internal fixation in length-unstable fracture patterns. External fixation is another acceptable option for these fractures. Locked plating, on the other hand, provides an 'internal external fixator,' avoids pin site issues and allows rapid mobilization while providing a biologically favorable environment for healing.
Kocher et al. provide the AAOS Clinical Practice Guideline for the treatment of pediatric diaphyseal femur fractures. They concluded that there was insufficient evidence regarding submuscular bridge plating to include it in the guideline.
Flynn et al. review the management of pediatric femoral shaft fractures. The note that
the narrow indications for plating of pediatric femoral fractures are open fractures, multiple trauma, head injury or compartment syndrome in patients less than 12 years old. Plating allows rigid fixation with readily available equipment and allows for rapid mobilization.
Hedequist et al. present a Technical Tricks paper in which they detail their surgical technique for submuscular bridge plating. They recommend this fixation strategy for patients between age 6 and skeletal maturity with comminuted diaphyseal femur fractures that are not easily treated by other methods.
Illustration A shows a preoperative and postoperative radiograph of a comminuted pediatric femur fracture treated with submuscular plating.
Incorrect answers:
(SBQ13PE.88) A 12-month-old boy attends a government regulated childcare center. His parents are called after a fall. Non-accidental trauma has been ruled out. On physical examination the right elbow is swollen and tender. He is unwilling to allow you to move the arm. Radiographs of the elbow are shown in Figure A. What is the orthopaedic management of this injury? Review Topic

Observation only
Elbow sling for 3 to 4 weeks
Rigid elbow immobilisation for 4 to 5 weeks
Admit for 24-48 hours for continuous intracompartmental pressure measurements
Operative fixation with percutaneous pinning PREFERRED RESPONSE 5
This patient presents with a distal humeral physeal separation. The most appropriate treatment would be closed reduction with internal fixation with percutaneous pins.
Displaced distal humerus physeal separation is typically seen in children under the age of 3 and has a high association with child abuse. The diagnosis can be a difficult as radiographs of a distal humeral physeal separation may be subtle. Often, radiographs show no obvious fracture, but can appear like an elbow dislocation since the secondary ossification centers have not yet developed. MRI or arthrogram can be used to aid in diagnosis.
Shrader et al. reviewed pediatric supracondylar fractures and pediatric physeal elbow fractures. They state the key to diagnosis of distal humerus physeal separation is the assessment is the radial head–capitellum relationship. These injuries should be fixed with closed reduction and smooth wire pinning. An elbow arthrogram may be considered intraoperatively for these patients because of the difficulty visualizing the distal humeral anatomy in children so young.
Skaggs et al. reviewed the diagnosis and management of pediatric elbow fractures. He states that child abuse should be suspected in all cases of elbow fracture when the child is less than 3 years of age and/or the injury pattern occur from a shearing mechanism. The displacement of physeal elbow fractures is almost always posteromedial.
Figure A shows AP and lateral radiographs with posteromedial displacement of the radial and ulnar shafts relative to the distal humerus. This is consistent with distal humeral physeal separation.
Incorrect Answers:
Question 90
- Analysis of which of the following proteins is used to establish the diagnosis of Becker muscular dystrophy?
Explanation
A 25-year-old woman with spastic diplegia has a painful progressive bunion deformity that has failed to respond to nonsurgical treatment. Examination reveals tenderness and erythema over the bunion prominence; however, the hallux metatarsophalangeal joint has full range of motion. A standing AP radiograph shows a hallux valgus angle of 30 degrees and a 1-2 intermetatarsal angle of 13 degrees. Treatment should now consist of
arthrodesis of the hallux metatarsophalangeal joint.
arthrodesis of the first tarsometatarsal joint.
excision of the medial eminence and medial capsular reefing of the metatarsophalangeal joint.
osteotomy of the distal first metatarsal.
proximal metatarsal osteotomy with distal soft-tissue realignment.
Treatment of hallux valgus in a patient with cerebral palsy is largely dependent on the degree of spasticity and the pattern of gait. The only way to adequately eliminate spastic deforming forces is with an arthrodesis of the MTP joint. Any other procedure will most likely lead to a high incidence of either hallux varus or recurrent hallux valgus.
The optimal arthrodesis angle is 25-30 degrees, and the metatarsal inclination angle should be 25-30 degrees also. Sagittal plane position should be checked intraoperatively and the proximal phalanx should clear the table by 5-10mm with simulated WB
Question 91
A 13-year-old girl has had a firm mass and pain in her right shoulder for the past several weeks. She denies any history of trauma. A radiograph and MRI scan are shown in Figures 31a and 31b. Biopsy specimens are shown in Figures 31c and 31d. What is the most likely diagnosis?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 92
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
REFERENCES: Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Fahrer H, Rentsch HU, Gerber NJ, et al: Knee effusion and reflex inhibition of the quadriceps: A bar to effective retraining. J Bone Joint Surg Br 1988;70:635-638.
Question 93
A 62-year-old patient is seen for routine follow-up after undergoing cementless total hip arthroplasty 2 years ago. The patient reports limited range of motion that severely affects daily activities. A radiograph is shown in Figure 51. Management should now consist of
Explanation
REFERENCES: Ayers DC, Evarts CM, Parkinson JR: The prevention of heterotopic ossification in high-risk patients by low-dose radiation therapy after total hip arthroplasty. J Bone Joint Surg Am 1986;68:1423-1430.
Healy WL, Lo TC, DeSimone AA, et al: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595.
Question 94
Figure 35 shows the AP radiograph of a patient who underwent a previous upper tibial osteotomy (UTO). The patient may be at risk for which of the following during total knee arthroplasty (TKA)?
Explanation
REFERENCES: Parvizi J, Hanssen AD, Spangehl MJ: Total knee arthroplasty following proximal tibial osteotomy: Risk factors for failure. J Bone Joint Surg Am 2004;86:474-479.
Meding JB, Keating EM, Ritter MA, et al: Total knee arthroplasty after high tibial osteotomy: A comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am 2000;82:1252-1259.
Question 95
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of
Explanation
REFERENCE: Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801.
Question 96
A 54-year-old woman sustains the injury seen in Figures 71a and 71b. The injury involves her nondominant extremity. What should the patient be told regarding her expected outcome?

Explanation
(SBQ12TR.101) An otherwise healthy young adult male sustains a transverse radial shaft and ulna fracture. He undergoes definitive surgical fixation with two nonlocking compression plates (LCPs) as shown in Figure A. What is the principle of this fixation technique on bone healing?

Absolute stability with direct healing by callus formation
Relative stability with indirect healing by callus formation
Absolute stability with direct healing by internal remodeling
Relative stability with indirect healing by internal remodeling
Absolute stability with endochondral bone formation
Definitive surgical fixation for a simple transverse both bone forearm fracture would include open reduction and internal fixation with absolute stability with direct healing by internal remodelling (i.e., primary bone healing). The radius is fixed with a 7-hole
Question 97
A complication unique to computer navigation of total knee arthroplasty (TKA) is
Explanation
Threaded pins are frequently inserted into the femoral shaft and tibial shafts or proximal tibia to attach arrays for tracking devices. There have been case reports of fractures propagating through the pin tracks, which is a complication unique to computer navigation. Intercondylar fractures can occur following posterior stabilized TKA. Vascular injury, ligament disruption, and nerve palsy are rare complications following TKA performed with or without computer navigation.

CLINICAL SITUATION FOR QUESTIONS 111 THROUGH 113
Figure 111 is the anteroposterior radiograph of a 79-year-old woman with a presurgical diagnosis of osteonecrosis who sustained a periprosthetic tibia fracture following her total knee arthroplasty (TKA).
Question 98
Synovitis of the MTP joints with eventual hyperextension deformity of the MTP is a common toe deformity seen with RA.
Explanation
Jin et al conducted a meta-analysis regarding polymorphisms in the 5' flank of COL1A1 gene and the conflicting results relating to osteoporosis. They found that the COL1A1 Sp1 polymorphism is associated with a modest reduction in BMD and an increased risk of fracture.
The attached review by Huang and Kung discusses the multiple genetic and environmental determinants of osteoporosis and illustration A (from a different review by these same authors) lists the known genes currently associated with osteoporosis.
The greatest biomechanical difference between unicortical and bicortical locking screws is seen when what force is applied?
Compression
Torsion
Distraction
Bending on the side of the plate
Bending on the surface perpendicular to the plate
Torsion force has the largest biomechanical difference between unicortical locked screws and bicortical locked screws.
The first referenced article by Roberts et al noted that by replacing the farthest unicortical
screws (3 per side of the fracture) with bicortical locking screws, torsion resistance was increased by over 50%.
The second referenced article by Fulkerson et al noted decreased resistance to all applied forces with unicortical screws in a comminuted fracture model, and recommended against their use in such a fracture.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
You are planning surgery on a 54-year-old female with the tibial plateau fracture seen in figures A and B. After reduction of the joint surface you plan to fill the void with a bone-graft substitute to prevent joint collapse. Which of the following bone-graft substitutes
disappears most quickly in vivo?
Collagen-based matrices
Calcium phosphate
Calcium sulfate
Synthetic calcium sulfate and tri-phosphate mixture
Coraline hydroxyapatite
Calcium sulfate disappears in vivo quickly, usually within 4-12 weeks. Calcium phosphate and coraline hydroxyapatite are resorbed slowly, somewhere between 1-10 years, depending on the manufacturer. Synthetics that combine calcium sulfate and phosphate
resorb quicker than calcium phosphate but slower than calcium sulfate. Collagen-based matrices show quick resorption of the collegen but slow resorption of their hydroxyapatite coating. Walsh et al. examined the in vivo response of calcium sulfate pellets alone or in combination with autogenous bone graft in a sheep model. They found excellent bone formation in defects filled with calcium sulfate pellets. Immunostaining for various cytokines (BMP-2, BMP-7, PDGF, or TGF-beta)
showed elevated levels in the newly formed bone. They proposed that the local environment acidity was responsible for breakdown of the calcium sulfate. Watson evaluated 8 patients with comminuted tibial metaphyseal fractures treated with an injectable calcium sulfate. They found that bone regrowth was observed in all patients and the bone substitute almost completely resorbed by
months. Bucholz reviewed the biochemical, biomechanical, and longevity characteristics of the common bone substitutes.
Which of the following Figures shows a fixation construct achieving absolute stability?
Figure A shows percutaneous pinning, Figure B shows locked bridge plating, Figure C shows intramedullary nailing, Figure D shows lag fixation and neutralization plating, and Figure E shows external fixation. All except Figure D show relative stability constructs.
Absolute stability is a construct seen in Figure D, where lag screws and a neutralization plate are shown in a postoperative clavicle. No micromotion is seen with this technique, and healing is by primary (Haversian) healing, as opposed to the other four constructs, which have relative stability and heal via callus formation. The first reference, the AO Principles textbook, covers this in depth.
The second reference by Claes et al notes that bone can still heal with bone (as opposed to fibrous union) with strain rates up to 15%.
Which immunoglobulin subtype does the rheumatoid factor target?
IgA
IgE
IgM
IgG
Rheumatoid factor does not target an immunoglobulin
Rheumatoid factor is an auto-antibody most commonly seen with rheumatoid arthritis. The presence of rheumatoid factor can also indicate generalized autoimmune activity unrelated to rheumatoid arthritis (e.g. tissue or organ rejection). Rheumatoid factor is itself an IgM antibody that is directed against the Fc portion of IgG antibody. Rheumatoid factor (IgM) attaches to IgG to form immune complexes which are deposited in tissues like the kidney and contribute to the overall disease process in rheumatoid arthritis.
James et al. assessed the occurrence and predictive factors for orthopaedic surgery in an cohort of patients with rheumatoid arthritis. Risk factors for surgery varied but the authors found that decreased inflammatory markers during the first year after diagnosis decreased the risk for subsequent surgery.
The positive predictive value is defined as which of the following?
True positives / (true positives + true negatives)
False negatives / (false negatives + true positives)
False positives / (false positives + false negatives)
(True positives + false positives) / (true negatives + false negatives)
True positives / (true positives + false positives) Corrent answer: 5
The positive predictive value is defined as the true positives divided by the sum of the positive results (true positive and false positive). It is also defined as the probability that a patient with a positive test actually has the disease; it is dependent on prevalence of disease.
The referenced articles by Wojtys and Kuhn et al are two of a series of medical statistics review papers.
An 85-year-old woman undergoes the treatment seen in Figure A for a displaced left femoral neck fracture. During wound closure, the patient becomes hypoxic and hypotensive. Despite aggressive resuscitation efforts, she passes away three hours later in the intensive care unit. The autopsy findings seen in
Figure B from the patient's lungs are most likely the result of which of the following
Reaming for the femoral component
Insertion of a femoral component after cement pressurization
Utilization of undersized broaches during canal preparation
Inadequate beta blockade
Use of spinal anesthesia
The clinical scenario is consistent with fat emboli syndrome. Figure A, shows a cemented bipolar hemiarthroplasty while Figure B shows marrow embolization into the lungs.
Studies have shown that intramedullary pressure and fat embolization are greatest during pressurization of cement and implant insertion.
Intramedullary pressure is influenced by size, shape, sharpness and insertion rate of an implant. Pressurization during cementing of a femoral component generates a large degree of pressure over a much wider surface area than in the other methods described of femoral canal instrumentation or preparation, as the entire femoral canal is
pressurized at one time. This results in the highest degree of marrow embolization to the lungs resulting in hypoxia.
Dobrjanski et al studied which variables affected intramedullary pressurization and found that lower implant insertion speed, lower hammering force, a
rubber- compared with steel-tipped hammer and a larger synthetic bone-to- implant radial gap reduced intramedullary pressure generated in a femur module.
Sustained compression applied to a growth plate under experimental conditions has what effect?
No effect
Accelerated longitudinal growth
Decelerated longitudinal growth
Decelerated apposition growth
Decreased bending strength of the bone
The Heuter-Volkmann Law states that compression across the growth plate slows longitudinal growth.
Stokes et al demonstrated that sustained compression across the growth plate can decrease longitudinal growth by 40%. Tension across the physis increases growth, but to a lesser degree.
A 13-year-old girl with a displaced proximal tibia fracture is brought into the emergency department by her adult cousin. The
fracture needs surgical management. The child is living with her cousin's family while her parents are in Germany. While the child speaks fluent English, her cousin and her parents are German-only speaking. How should you consent this patient?
No consent is needed given the urgent nature of the injury, proceed with surgery
Talk with the cousin, using the child as a translator
Talk with the cousin, using a German-translator
Call the parents in Germany, using the child as a translator over the phone
Call the parents in Germany, using a German-translator over the phone
This is an urgent (not emergent) clinical senario, and as such, the child needs to have
formal consent by speaking with her parents using a German- translator.
Wenger and Lieberman discuss the problems and potential solutions surrounding the process of informed consent in patients who either personally lack capacity to make decisions or in patients who require surrogates (like minors) to make treatment decisions.
Lindseth reviews the ethical issues encountered in pediatric orthopaedics and the problems associated with these decisions. Specifically pediatric consent is confounded because the person giving the consent is not the person who will bear the consequences of the treatment.
What is the primary mode of bisphosphonate excretion?
Renal
Gastrointestinal
Liver
Skin
Pulmonary
Bisphosphonates are a broad class of medicines used to treat osteoporosis and Paget's disease. They work by inhibiting osteoclast-mediated resorption after being absorbed into the inorganic phase of bone and taken up by osteoclasts. The paper by Lin et al provides a nice review of bisphosphonates and describe their appropriate use in enhancing bone density in patients with structurally
flawed bone. They describe the mechanism of action of bisphosphonates as pyrophosphate analogues and their renal mechanism of excretion, thus, prohibiting their use in patients with renal insufficiency. Rosier discusses the role of the orthopaedic surgeon in the diagnosis and treatment of patients with osteoporosis, now referred to as the "own the bone" initiative. Central to the treatment of osteoporosis are bisphosphonates and the anti-RANKL
monoclonal antibody, Denosumab.
The 2009 AAOS Clinical Guideline on prevention of pulmonary embolism in patients undergoing total hip or knee arthroplasty recommends classifying patients as having either a "standard" or "elevated" risk of bleeding complications. The presence of all of the following qualify a patient as having an "elevated" risk of major bleeding EXCEPT?
History of hemophilia
History of protein C deficiency
History of a recent gastrointestinal bleed
History of a recent hemorrhagic stroke
History of Von Willebrand's Disease
The 2009 AAOS Clinical Guideline on prevention of pulmonary embolism in patients undergoing total hip or knee arthroplasty recommends that all patients pre-operatively should be classified as either having an elevated or standard risk of bleeding and either an elevated or standard risk of pulmonary embolism.
A history of a bleeding disorder (e.g., hemophilia, Von Willebrand's Disease), recent GI bleed, or hemorrhagic stroke qualifies a patient as having an elevated risk of major bleeding.
A history of hypercoagulable state (such as protein C deficiency) or previous documented pulmonary embolism qualifies a patient as having an elevated risk of pulmonary embolism. Type of thromboembolism prophylaxis is recommended by weighing risk of major bleeding vs risk of PE. For those patients with a known contraindication to anticoagulation an IVC filter is considered. Mechanical prophylaxis is recommended across all risk (low to
high risk of either bleeding or pulmonary embolism) groups undergoing total hip or total knee arthroplasty. The detailed AAOS guidelines can be found on the AAOS website.
The evidence based clinical recommendations are presented in the reference by Johanson et al.
In consideration of a prosthetic knee, each of the following are advantages of choosing a polycentric knee with fluid control over a constant friction knee EXCEPT:
Allows variations in cadence
Flexes in a more controlled manner
Lighter in weight
Improved stance control allows less energy expenditure
Overall length of the limb is shortened during initiation of a step reducing the risk of stumbling
Single axis, constant friction knees function as a simple hinge. They are light, durable, and much cheaper prostheses making them ideal for growing children who will need multiple prostheses before reaching adulthood. This prosthesis allows only a single speed of walking, and relies solely on alignment for stance phase stability. Polycentric knees offer each of the advantages stated above making it a more ideal prosthesis for the active adult. Disadvantages of the polycentric knee include cost, weight, and more sophisticated maintenance.
Tang et al reviews the current prosthetic options for leg and foot amputees. Illustration A demonstrates a single axis knee prosthesis.
Illustration B demonstrates a polycentric knee prosthesis.
Which of the following biologic agents commonly used to treat rheumatoid arthritis (RA) DOES NOT target tumor necrosis factor- alpha (TNF-alpha)?
Infliximab
Rituximab
Etanercept
Golimumab
Adalimumab
Rituximab is a chimeric monoclonal antibody against the protein CD20, which is primarily found on the surface of immune system B cells. Rituximab is used in combination with methotrexate to treat RA that has not responded to one or more types of treatment, including anti-tumor necrosis factor (TNF) blockers.
In rheumatoid arthritis, and other chronic inflammatory conditions, cytokines produced by activated T-cells/macrophages contribute to the pro-inflammatory state. TNF-alpha is thought to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat RA are directed towards blocking TNF-alpha or its receptors. These drugs are able to reduce inflammation and stop disease progression.
Elliot et al. evaluated the safety and efficacy of infliximab in 20 patients with active RA in an open phase I/II trial lasting 8 weeks. They found that treatment with anti-TNFa was safe, well tolerated and resulted in significant clinical and laboratory improvements.
Illustration A depicts five commonly used anti-TNF alpha biologic agents for the treatment of rheumatoid arhtirits with their usual dosing regimens.
Incorrect Answers:
Receptor activator of nuclear-factor kappa-B ligand (RANKL) is
an important regulator of bone resorption. Which of the following cells is the MAJOR source of RANKL in bone remodelling?
Osteoclasts
Osteoblasts
Integrins
T cells
Macrophages
RANKL, a key osteoclastogenic protein, is expressed by osteoblasts and binds to the RANK receptor on osteoclast precursor cells.
The binding of RANKL to RANK on osteoclast precursor cells drives their differentiation into mature osteoclasts (multinucleated giant cells). Mature osteoclasts bind to the bone surfaces via integrins and resorb bone via their ruffled border within Howship's lacunae. Osteocytes orchestrate bone resorption and bone deposition by controlling osteoclast and osteoblast activity. Osteoblasts release RANKL to induce osteoclast differentiation, while
osteoblasts release osteoprotegerin (OPG) to downregulate osteoclastogenesis. Osteocytes also release fibroblast growth factor-23 (FGF-23), BMPs and sclerostin to regulate osteoblast activity. Antibodies to RANKL and Sclerostin have both been shown to increase bone density.
Compton et al. reviewed osteocyte function and the emerging importance of sclerostin, which is a glycoprotein. Sclerostin is predominantly secreted by osteocytes under physiologic conditions to act as an important negative regulator of bone mass through inhibition of bone formation by osteoblasts.
Illustration A demonstrates local bone milieu. It depicts the interplay between osteocytes, osteoblasts, and osteoclasts via the factors described above.
Incorrect answers:
A 45-year-old woman with rheumatoid arthritis is being scheduled for a total knee athroplasty in 2 weeks. She is currently taking sulfasalazine, Penicillamine, and etanercept, a tumor necrosis factor inhibitor (aTNF-a). What changes should be made to her medication regimen prior to surgery?
Discontinuation of all three medications 1 weeks prior to surgery
Discontinuation of sulfasalazine 1 weeks prior to surgery, continuation of etanercept and penicillamine
Continuation of sulfasalazine, penicillamine, and etanercept
Continuation of sulfasalazine and penicillamine, discontinuation of etanercept 1 week prior to surgery
Continuation of penicillamine, discontinuation of sulfasalazine and etanercept 1 week prior to surgery
Anticytokine disease-modifying antirheumatic drugs (DMARD) have become increasingly popular in the treatment of RA. Immunosuppression and the risk of infection are potential complications for all anti-TNF-alpha medications. Current recommendations for cessation of immunosuppressive therapy are when the drug concentrations are at their lowest levels which include the following: 3 days after etanercept injection; 2 weeks prior to infliximab infusion; 10 days after adalimumab injection. Medications such as sulfasalazine and penicillamine may be continued during the pre and post- operative period. Recent evidence and guidelines such as those reviewed by Keith's paper, suggest that anti-TNF-alpha medications should be stopped 4 weeks prior to surgery.
Giles et al report in their case control series an increased infection rate of RA patients undergoing an orthopaedic procedure who were on TNF-a inhibitors as opposed to patients on more traditional treatment regimens like methotrexate and prednisone.
Which of the following supplements affects blood clotting through its effect on platelets?
Ginkgo
Vitamin D
Ephedra
St. John's Wort
Selenium
Ginkgo and ginseng are two common supplements used in the general population that have inhibitory effects of platelet function. Adverse peri- operative complications consisting of increased bleeding and hematoma formation have been reported with the use of these two herbal supplements. The most commonly used supplements that could have an effect in the peri- operative period include echinacea, ephedra, garlic, ginkgo, ginseng, kava, St John's wort, and valerian. Bleeding has been shown to be effected by garlic, ginkgo, and ginseng; cardiovascular instability from ephedra; and hypoglycemia from ginseng. Kava and valerian have pharmacodynamic herb- drug interactions that can increase the sedative effect of anesthetics. St John's wort has been shown to alter the metabolism of certain drugs used in the perioperative period.
Ang-Lee et al review common supplements used today and their potential anesthesia/operative effects. The article places emphasis on proper history taking of not only medications but also supplements which is often times left out of documentation.
The femur radiograph of a healthy 25-year-old female is compared to the femur radiograph of a healthy 85-year-old female. Which of the following best describes the 25-year-old's femur?
Increased cortical thickness and a smaller medullary canal volume
Decreased cortical thickness and a larger medullary canal volume
Equivalent cortical thickness and medullary canal volume
Increased cortical thickness and larger medullary canal volume
Decreased cortical thickness and a smaller medullary canal volume
As the human body ages the cortical thickness/area decreases and subsequently the diameter/volume of the medullary canal increases. Therefore, a young healthy 25- year-old woman should have thicker cortices and a smaller medullary canal volume than her counterpart at 85 years. A decreased cortical bone area is linked to increased fracture risk.
Stein et al studied femurs from subjects aged 21-92 years of age. They found that a reduction in cortical area was seen in older specimens and this change was more
pronounced in female specimens.
Wrong Answers:
Which of the following is NOT a described complication of corticosteroid injections?
Local flare in surrounding tissues
Apoptosis of myocytes
Skin pigmentation changes
Fat atrophy
Facial flushing
Corticosteroids have not been shown to cause apoptosis of myocytes when injected extra-articularly. Each of the other answers have been described.
Cole and Schumacher provide a review of current uses of corticosteroid injections, and emphasize that how accurately the injection is placed affects the outcome.
Kumar and Newman report prospectively on 672 patients who received 1147 intra- and extra-articular injections. Their overall complication rate was low (16%) with injection site pain (mild) and bleeding constituting the majority of cases. There were 4 instances of fat atrophy in the extra-articular group, and
cases of syncope or dizziness in the intra-articular group. They did not discuss the efficacy of their injections.
A surgeon chooses a periarticular locking plate with unicortical proximal locking screws for an extra-articular distal femur fracture as seen in Figure A. Compared to an identical construct with bicortical unlocked proximal screw fixation, the periarticular locking plate with unicortical locking screws has which biomechanical properties?
Greater torsional and axial fixation strength
Less torsional but greater axial fixation strength
Equal torsional and axial fixation strength
Greater torsional but less axial fixation strength
Less torsional and axial fixation strength
Unicortical locking plates have characteristically less torsional strength than bicortical locking plates and bicortical non-locking plates. Axial strength is improved with locking plate fixation.
Zlowodzki et al studied the LISS periarticular locking plate with unicortical proximal fixation in a distal femur model and found superior axial fixation strength (134%) but worse torsional strength (68%) compared to a fixed angle blade plate with non- locking bicortical screw fixation.
Locked plating was reviewed by Haidukewych and Ricci which highlighted the added cost, unique complications, and they recommended the use of locked plating only in situations when unlocked constructs have demonstrated poor outcomes.
In rat models looking at the effect of malnutrition on fracture healing, amino acid supplementation in a nutritionally deprived rat increases all of the following EXCEPT
Serum albumin
Body mass
Quadriceps total protein content
Fracture callus mineralization
Insulin-like growth factor 1 (IGF-1) mRNA expression
The study by Hughes et al found that essential amino acid supplementation (glutamine, arginine, and taurine) following femoral fracture in a protein- malnourished rat model increases serum albumin, body mass, quadriceps total protein content, and fracture callus mineralization. Expression of IGF-1 and
IGF-2, myosin, actin, and VEGF mRNA were all significantly decreased in the amino acid supplemented group compared to the malnourished group. The malnourished group is thought to have upregulation of mRNA expression in attempt to increase the amount of protein product that is translated, however the lack of amino acid building blocks in the malnutrition group was a barrier to appropriate protein synthesis.
The study by Day et al created a malnourished rat femur fracture model by administering a 6% protein diet. They found that administering a 20% protein diet in the post-fracture period yielded a greater cross-sectional area of the
fracture callus and callus stiffness compared to the 6% protein malnourished group.
The statistical power of a study is best defined by?
1 - probability of type-II (beta) error
True positive/(true positive + false negative)
True negative/(false positive + true negative)
1 - probability of type-I (alpha) error
[True positive/(true positive + false negative)] / false-positive rate
The power of a study is an estimate of the probability of finding a significant association in a research study when one truly exists. The power is defined by
1 - probability of type-II (beta) error, and is often set at 80%. For example, a power of 80% means that if the intervention works, the study has an 80% chance of detecting this and a 20% chance of randomly missing it. A type-II or beta error occurs when one falsely concludes that there is no significant association when there actually is an association (resulting in a false-negative study that rejects a true alternative hypothesis). The type-II or beta error can be determined if Type I error rate and sample size are known. A type-I or alpha error occurs when a significant association is found when there is no true association (resulting in a false-positive study that rejects a true null hypothesis). The alpha level refers to the probability of a type-I (alpha) error and is usually set for most studies at 0.05. Answer 2 is the formula for sensitivity. Answer 3 is the formula for specificity. Answer 5 is the formula for the positive likelihood ratio. The references by
Kocher and Wojtys are excellent reviews of basic biostatistic principles.
A 55-year-old female with a history of metastatic breast cancer develops shoulder pain without any trauma. Which of the following is involved with the findings shown in Figures A and B?
IL-4
RANK
TNF-alpha
OPG
Sox-9
Osteoclastic bone resorption is the final common mechanism for osteolysis, whether due to a pathologic lytic lesion, macrophage activation in particle wear, or normal remodeling. The RANK-RANKL mechanism controls the coupling of osteoblast and osteoclast activation. Figures A and B show an osteolytic lesion in the humerus in a patient with known metastatic breast carcinoma.
RANKL is expressed from osteoblasts and bone-marrow stromal cells. When RANKL binds to the RANK receptor (receptor/activator of NF-[kappa]B) on the cell membrane of osteoclasts it stimulates differentiation from osteoclast progenitor cells to mature osteoclasts. Mature osteoclasts proceed with osteoclastic bone resporption.
Osteoprotegerin (OPG) acts as a decoy receptor by binding to RANKL and blocking the interaction between RANKL and the RANK-receptor and consequently inhibiting osteoclast formation and
activation.
Illustration A depicts the RANK/RANKL involvement in tumor metastatic spread.
Laboratory values of a normal serum calcium and parathyroid hormone can be found in which of the following disease states?
Primary hyperparathyroidism
Type I vitamin D deficient rickets
Type II vitamin D deficient rickets
X-linked hypophosphatemic rickets
Nutritional rickets
Hypophosphatemic rickets is caused by the inability of kidney proximal tubules to reabsorb phosphate due to a mutated PHEX gene, found on the X chromosome. PHEX is thought to protect extracellular matrix glycoproteins from proteolysis. Hypophosphatemic rickets shares many clinical similarities with nutritional rickets but shows PTH levels that are not elevated, even with calcium and phosphate abnormalities.
Pettifor reviews the advances in molecular genetics in the understanding and possible treatments in tumour-induced osteomalacia/rickets.
The review article by Carpenter discusses the X-linked disorder including its clinical manifestations, the wide spectrum of disease severity, and complications of the disease in adult patients.
Illustration A is a table that details the laboratory values associated with each type of rickets.
An 80 year-old female undergoes ORIF of her hip fracture without any complications. A hospitalist consult was obtained for medical clearance pre- operatively, and she was diagnosed with osteoporosis. Which of the following treatment scenarios will lead to the best management of the patient's osteoporosis?
Schedule a follow-up appointment with the patients primary care physician to initiate therapy
Order a physical therapy consult and initiate an exercise plan
Have the patient meet with a nutritionist to increase her calcium and vitamin D intake
Start bisphosphonates, and have the patient follow-up with her primary care physician
Perform a metabolic work-up as an inpatient, and set-up an appointment in an osteoporosis clinic
The initiation of appropriate osteoporosis treatment following hip fractures occurs at a surprisingly low rate. Physical therapy and dietary changes are not appropriate initial treatments for osteoporosis, and bisphosphonate therapy should be prescribed by the physician who will be following and managing the patient's osteoporosis.
Miki et al performed a prospective randomized trial where they compared the rates of osteoporosis treatment initiation. The percentage of patients who were on pharmacologic treatment at 6 months post-injury was 58% in the group whose treatment was directed by the orthopedic surgeon and osteoporosis clinic, and 29% when managed by the primary care physician alone.
The elements chromium, molybdenum, and cobalt are basic components of which of the following implant materials?
Aluminum oxide
Cobalt alloy
Stainless steel
PMMA
Tantalum
Cobalt alloys are extremely strong and are well-suited to applications requiring longevity. Strength of the implant is improved by the addition of molybdenum. Corrosion resistance is addressed by the addition of chromium, which also increases the hardness of the implant.
Incorrect Answers:
Which of the following scenarios of treatment of a humerus fracture best achieves low strain at the fracture site and high stiffness of the treatment construct?
Functional bracing of a transverse midshaft fracture
Comminuted midshaft fracture with locked bridge plating
Short oblique fracture with interfragmentary lag screw and locked neutralization plate
Uniplane external fixation of a spiral open fracture
Oblique fracture with intramedullary nail fixation
Strain in fractures is calculated by dividing the interfragmentary movement by the size of the fracture gap. Strain must be very low (2%) for primary bone healing to occur, and should be less than 10% for secondary bone healing to occur. Stiffness refers the ability of the construct to resist movement under applied loads. Answer 3 describes a situation where primary bone healing is
the goal. For this to occur, there must be no significant gapping at the fracture site, there must be low strain between fracture fragments, and the construct must be stiff.
None of the other answers would accomplish this. Functional bracing and intramedullary fixation both accomplish healing through formation of fracture callus, or secondary healing. A comminuted fracture treated with locked bridge plating relies on less stiffness to allow for secondary healing between fragments. However, since there are many fracture fragments, the strain is distributed among them and therefore remains low. A uniplane external fixator is very unlikely to accomplish low strain and high stiffness in this setting.
A 67-year-old man complains of low-grade fevers and calf pain 2 weeks following a total knee arthroplasty. What is the next appropriate step in management of this patient?
Plethysmography of lower extremity
MRI of lower extremity
CT angiography of lower extremity
Venous ultrasonography
Knee aspiration to evaluate for septic joint
Venous ultrasonography is the next best step in this patient's management, due to the clinical picture of a deep venous thrombosis. The most sensitive and specific recommended diagnostic procedure is a venous ultrasonography.
In their multi-center study, Haut et al. hypothesized that admission to trauma centers that use duplex ultrasound more frequently would independently predict increased DVT reporting for individual patients. They indeed found that trauma centers ultrasound practice was an independent predictor of DVT diagnosis for individual patients, controlling for patient-level risk factors, but concluded the elevated DVT rates at these centers were due to surveillance bias. As such, they recommend that surveillance for DVT should not be considered as a quality control measure in the care of trauma patients.
A patient undergoes closed reduction of a bimalleolar ankle fracture dislocation by the ER physician and is sent to your clinic for evaluation. You evaluate the patient and schedule him for surgery. According to the 2009 guidelines, which of the following scenarios would meet criteria for coding the encounter as a new patient?
You injected his knee in the office almost 3 years ago for osteoarthritis, and have not seen him since
He had an arthroscopic operation by your partner 4 years ago
You were consulted 1 year ago for shoulder pain when he was hospitalized for chronic renal failure
He was seen by your partner in clinic for a herniated disk 2 years ago, but had no procedures performed
You performed a hip replacement on him 12 years ago, and his last follow- up was 18 months ago at which time he was doing well
Only answer two is correct. The 2009 guidlines clarify that the patient can be defined as new only if he has not been seen by anyone in the physician's same group practice and of the same specialty in the past 3 years. Hand and sports medicine specialists with a CAQ, however, are an exception and are allowed to bill for patients already seen by other orthopedists in the same group as new
patients. This scenario would not qualify as a consultation, since the orthopedic surgeon
is taking over care of the patient's problem and is not merely offering advice to another physician who is already caring for the patient. Consultations do not have the same 3 year time qualification. However, Medicare and many other insurers no longer recognize consultation codes.
All the following medications binds reversibly to the enzyme COX-1 EXCEPT
Meloxicam
Diclofenac
Indomethacin
Naproxen sodium
Aspirin
Aspirin binds irreversibly to the cyclooxygenase enzyme. Aspirin acetylates platelet cyclooxygenase and permanently inhibits thromboxane (TX) A2 production leading to its antiplatelet effects. The other NSAID's listed above bind reversibly with COX-1.
Patrono et al discuss the pharmokinetics and platelet effect of both low dose and regular dose aspirin. Nonsteroidal anti-inflammatory drugs compete dose- dependently with arachidonate for binding to platelet cyclooxygenase.
In the treatment of patients with rheumatoid arthritis, TNF-alpha is blocked by which of the following agents?
Tocilizumab
Anakinra
Etanercept
Abatacept
Rituximab
Etanercept is a biochemically designed soluble p75 tumor necrosis factor receptor immunoglobulin G fusion protein, which blocks the downstream
effects of TNF.
Methotrexate is a chemotherapy agent used to inhibit lymphocytes. Gold inhibits monocytes, while sulfasalazine is an anti-inflammatory decreasing the production of
prostaglandins and leukotrienes. Rituximab inhibits B-cells as it
is a monoclonal antibody to CD20 antigen. Anakinra (Kineret) is a recombinant IL-1 receptor antagonist. Abatacept (Orencia) is a selective costimulation modulator that binds to CD-80 and CD-86 (inhibits T cells). Tocilizumab (Actemra)is an IL-6 receptor inhibitor (2nd line treatment for poor response to TNF-antagonist therapy).
Pisetsky wrote an editorial in NEJM discussing the development of TNF blockers through research, and the potential for the use of Etanercept in patients with juvenile RA through its inhibition of lymphotoxin-alpha.
Which of the following medications when combined with methotrexate has been shown to be more effective than methotrexate alone in the treatment of rheumatoid arthritis?
Nitrofurantoin
Rifampin
Azithromycin
Erythromycin
Doxycycline
Tetracycline was initially used in the treatment of rheumatoid arthritis (RA) because Mycoplasma was thought to be the causative agent. It was later found that tetracyclines have biologic effects on the inflammatory and immunologic cascade by inhibiting collagenase activity. Collagenase is an enzyme involved
in breaking down macromolecules in the connective tissue, contributing to the pathologic changes of RA.
In a prospective study, O'Dell et al found that initial therapy with methotrexate plus doxycycline was superior to treatment with methotrexate alone. Furthermore, similar results for low-dose and high-dose doxycycline suggested that antimetalloproteinase effects were more important than the antibacterial effects.
When using C-arm fluorocopy, patient radiation exposure will be increased with which of the following?
The extremity is positioned closer to the image intensifier
A larger body part is imaged compared to a smaller body part
Use of radiation beam collimation
Mini C-arm fluroscopy is used instead of large C-arm fluroscopy
Decreased duration of imaging
Patient radiation exposure will be increased if a larger body part is imaged compared to a smaller body part.
The first study by Giordano et al used radiation dosimeters for large and mini c-arm machines. They found that elevated exposure levels can be expected when larger body parts are imaged, when the extremity is positioned closer to the x-ray source, and when the large c-arm is used over the mini c-arm.
The second study by Giordano et al also used dosimeters for a mini c-arm and found that the surgical team is exposed to minimal radiation during routine
use of mini-c-arm fluoroscopy, except when they are in the direct path of the radiation beam. They list factors to decrease radiation exposure to patient and surgeon including: minimizing exposure time, reducing exposure factors, manipulating the x-ray beam with collimation, orienting the fluoroscopic beam in an inverted position relative to the patient, strategic positioning of the surgeon within the operative field, judicious use of protective shielding during imaging, and maximizing the distance of the surgeon from the radiation beam.
Illustration A shows that arrangement #1 has the body part half-way between the radiation source and image intensifier. Arrangement #2 has the the image intensifier acting as an arm table for the body part with the radiation source further away. Arrangement #1 has more radiation exposure than #2. The distance between the x-ray tube and the body part is doubled in arrangement
#2 compared to arrangement #1. This increased distance correlates to a reduction in exposure according to the inverse square law (reduction in radiation intensity with greater distance from the x-ray source).
You are seeing a 13-year-old girl for asymptomatic flat feet and recommend observation. In educating this patient/family about general bone health, you recommend what amount of daily dietary calcium for your patient?
Question 99
Which of the following processes does not account for decreased hematopoiesis in patients with metastatic disease?
Explanation
REFERENCE: Frassica FJ, Gitelis S, Sim FH: Metastic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 100
A 20-year-old collegiate pitcher sustains a medial collateral ligament (MCL) rupture of his throwing elbow for which surgical reconstruction is necessary. The goal of surgery is anatomic restoration of the MCL. Which statement best describes the kinematics of the native MCL?
Explanation
full extension and full flexion. True lateral radiographs reveal that the flexion-extension axis, or center of rotation, of the elbow lies in the center of the trochlea and capitellum. The origin of the anterior bundle of the MCL lies slightly posterior to the rotational center of the elbow. The anterior bundle is further divided into an anterior band and a posterior band. The eccentric origin of these anterior bundle components in relation to the rotational center through the trochlea creates a CAM effect during flexion and extension. The anterior band tightens during extension, and the posterior band tightens during flexion. This reciprocal tightening of the two functional components of the anterior bundle allows the ligament to remain taut throughout the full range of flexion. Cadaver dissection studies have identified the origin and insertion of both the medial and lateral stabilizing elbow ligaments. The anterior bundle of the MCL is isometric throughout the flexion/extension arc of motion, making Response C incorrect. The posterior bundle of the MCL elongates with elbow flexion, so Responses B and D are incorrect. The posterior bundle of the MCL also demonstrates the most change in
length from extension to flexion of all the elbow ligaments.
