OITE & ABOS Orthopedic Board Prep MCQs: Deformity, Fracture, & Nerve Part 190

Key Takeaway
This page offers Part 190 of a comprehensive orthopedic board review. It features 100 high-yield MCQs, formatted like OITE/AAOS exams, for orthopedic residents and surgeons. Use Study or Exam Mode to prepare for your board certification, covering key topics like Deformity, Fracture, and Nerve. Essential for success.
About This Board Review Set
This is Part 190 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 190
This module focuses heavily on: Deformity, Fracture, Nerve.
Sample Questions from This Set
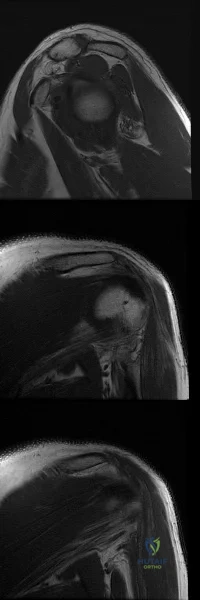
Sample Question 1: Figure 46 shows the MRI scan of a patient who has a mass in the calf that has been fluctuating in size. Radiographs are negative. Which of the following procedures will most quickly aid in confirming the diagnosis?...
Sample Question 2: Figures A-C are images of a 37-year-old man who presents with isolated muscle atrophy due to a compressed nerve. Which of the following sequences correctly describes the pathway of this nerve through the brachial plexus, before it innervate...
Sample Question 3: A 53-year-old man is involved in a motor vehicle collision and sustains the closed distal femur fracture seen in Figures 54a and 54b. A precontoured distal femoral locking plate is selected for fixation. A locking construct should be used t...
Sample Question 4: -Posterior cruciate insufficiency diagnosed using the quadriceps active test is confirmed with tibial translation...
Sample Question 5: A 17-year-old girl with a history of Scheuermann's kyphosis has a fixed thoracic deformity of 80 degrees. There was no correction of her deformity on supine hyperextension radiographs. What is the most appropriate treatment? Review Topic...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 46 shows the MRI scan of a patient who has a mass in the calf that has been fluctuating in size. Radiographs are negative. Which of the following procedures will most quickly aid in confirming the diagnosis?
Explanation
REFERENCES: Bianchi S, Abdelwahab IF, Kenan S, Zwass A, Ricci G, Palomba G: Intramuscular ganglia arising from the superior tibiofibular joint: CT and MR evaluation. Skeletal Radiol 1995;24:253-256.
Feldman F, Singson RD, Staron RB: Magnetic resonance imaging of para-articular and ectopic ganglia. Skeletal Radiol 1989;18:353-358.
Question 2
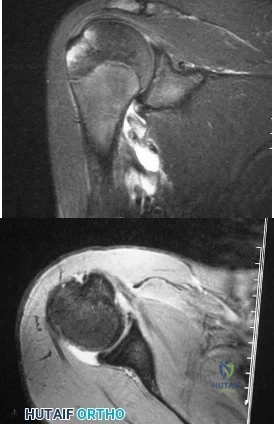
Figures A-C are images of a 37-year-old man who presents with isolated muscle atrophy due to a compressed nerve. Which of the following sequences correctly describes the pathway of this nerve through the brachial plexus, before it innervates the affected muscles?
Explanation
Quadrilateral space syndrome is a condition defined by axillary nerve, +/- posterior humeral circumflex artery compression in the quadrilateral space. It most commonly affects the dominant shoulder in overhead movement athletes (e.g. basketball players) or other throwing athletes. Physical examination may reveal weakness with the arm positioned in abduction and external rotation. In situations of long-standing compression, there may also be atrophy of the teres minor and deltoid muscle.
Chafik et al. dissected thirty-one cadaveric human shoulders to describe the neuromuscular anatomy of teres minor. They showed that the primary nerve branch to teres minor travelled in a fascial sling 44 mm medial to the muscular insertion. This
area may be the potential site of greatest compression and tethering of this nerve in patients with isolated teres minor atrophy.
Friend et al. performed a cadaveric dissection of nine shoulder specimens to look at the anatomical variability in course, length and branching pattern of both the teres minor nerve and the axillary nerve. These were compared to a case-based study of these two male patients with isolated atrophy of teres minor. They concluded that there is no good anatomical predictor of nerve compression outside the quadrilateral space as there is considerable anatomical variation in its origin and course, as well as potential site of compression.
Figure A-C are MRI images that show atrophy of the teres minor muscle and possibly deltoid muscle. The rotator cuff muscles are labeled in Illustration A. The teres minor muscle is labeled in Illustration B. Illustration C shows a diagram of the brachial plexus.
Incorrect
1:
This
describes
the
musculocutaneous
nerve.
3:
This
describes
the
suprascapular
nerve.
4:
This
describes
the
long thoracic
nerve.
Question 3
A 53-year-old man is involved in a motor vehicle collision and sustains the closed distal femur fracture seen in Figures 54a and 54b. A precontoured distal femoral locking plate is selected for fixation. A locking construct should be used to A B

Explanation
This patient has a comminuted distal femur fracture. A fixed-angle device such as a locking plate is preferred to confer angular stability to the construct and prevent varus collapse. The strategy to promote union of the fracture is to provide a low-strain environment to allow bone healing. Strain is determined by the amount of motion over the length of a fracture. In the case of a noncomminuted fracture, the fracture surfaces can be compressed and rigid fixation applied to abolish strain and promote primary bone healing without callus. In the case of a comminuted fracture, the preferred fixation strategy
focuses on distributing motion along the length of the fracture to provide a low-strain environment that will promote secondary bone healing and callus formation.
RECOMMENDED READINGS
Gardner MJ, Evans JM, Dunbar RP. Failure of fracture plate fixation. J Am Acad Orthop Surg. 2009 Oct;17(10):647-57. Review. PubMed PMID: 19794222.View Abstract at PubMed
Lujan TJ, Henderson CE, Madey SM, Fitzpatrick DC, Marsh JL, Bottlang M. Locked plating of distal femur fractures leads to inconsistent and asymmetric callus formation. J Orthop Trauma. 2010 Mar;24(3):156-62. doi: 10.1097/BOT.0b013e3181be6720. PubMed PMID:
Question 4
- Posterior cruciate insufficiency diagnosed using the quadriceps active test is confirmed with tibial translation
Explanation
Question 5
A 17-year-old girl with a history of Scheuermann's kyphosis has a fixed thoracic deformity of 80 degrees. There was no correction of her deformity on supine hyperextension radiographs. What is the most appropriate treatment? Review Topic
Explanation
Question 6
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ,
Ciba-Geigy, 1991, vol 8, p 53.
Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA,
Harper and Row, 1982, vol 3, pp 428-429.
Question 7
A 14-year-old girl reports hip pain that is exacerbated by weight bearing. A radiograph and biopsy specimen are shown in Figures 16a and 16b. The best course of management should be
Explanation
REFERENCES: Azouz EM, Karamitsos C, Reed MH, Baker L, Kozlowski K, Hoeffel JC: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420.
Hecht AC, Gebhardt MC: Diagnosis and treatment of unicameral and aneurysmal bone cysts in children. Curr Opin Pediatr 1998;10:87-94.
Question 8
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared to a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.

RESPONSES FOR QUESTIONS 58 THROUGH 62
Nerve palsy
Skin necrosis
Flexion instability
Patellar instability
Anterior knee pain
Malalignment
Total knee arthroplasty (TKA) is performed to address each condition shown in Figures 58 through 62b. Which complication is most commonly associated with each image?
Question 9
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis. J Bone Joint Surg Am 2005;87:725-730.
Question 10
A 7-year-old sustains the isolated injury shown in Figures A and B. On physical examination there is no evidence of soft tissue compromise and he is able to make an okay sign, give a thumbs up sign and cross his fingers. Which treatment will minimize complications? Review Topic

Explanation
Supracondylar fractures are common pediatric elbow injuries. Extension type injuries account for 95-98% of all cases. Non-displaced injuries may be treated conservatively. Displaced fractures are treated with closed reduction and percutaneous pinning. Use of laterally divergent pin constructs avoids risk of ulnar nerve injury, while maintaining satisfactory fracture alignment.
Slobogean et al. retrospectively reviewed pediatric supracondylar fractures to identify if there was an increased risk of ulnar nerve injury with crossed pin configurations. They found a higher incidence of ulnar nerve injury with crossed pinning constructs. For every 28 crossed pin constructs, there was one ulnar nerve injury identified.
Woratanarat et al. retrospectively reviewed supracondylar fractures to identify differences in the outcomes between lateral pinning versus crossed pinning constructs. No difference was found for loss of fixation or development of late deformity between the two groups. Crossed pin constructs were associated with a 4.3 times higher risk of iatrogenic ulnar nerve injury.
Omid et al. review pediatric supracondaylar humerus fractures. They note that lateral pinning is as stable as crossed pinning when appropriately spread-out at the fracture line. This also avoids the risk of ulnar nerve injury.
Figures A and B show AP and lateral radiographs of a pediatric supracondylar fracture. This would be classified as a Gartland Type 3.
Incorrect Answers:
Question 11
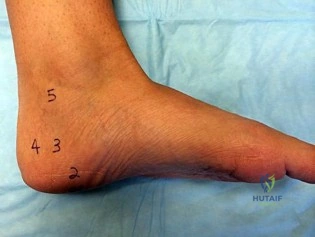
A B Figures 82a and 82b are the clinical photograph and radiograph of a 60-year-old man with a 30-year history of diabetes complicated by borderline chronic renal failure, heart failure controlled by medication, and bilateral lower extremity neuropathy. He is currently wheelchair bound because of his cardiopulmonary limitations, but uses his legs for transfers. He has had a progressive left ankle deformity that has progressed to the point at which he cannot use his leg for pivot transfers. He is adamant that something should be done to improve his living situation. Which surgical option can best achieve his goal of using the leg for transfers?

Explanation
The indications for surgery in a Charcot joint are an unbraceable deformity or recurrent ulceration despite use of adequate bracing. Any significant varus/valgus deformity of the ankle or hindfoot (as in this patient) is unbraceable, whereas midfoot Charcot deformities usually can be treated nonsurgically. The goal of surgery is to provide a stable aligned foot and ankle to permit activities and reduce risk for recurrent ulceration. This does not mean that there has to be a radiographic fusion because many patients with diabetes achieve a stable nonunion without pain. The only surgical construct that will provide long-term inherent stability and alignment in this situation is use of a hindfoot fusion rod. It provides better stability and purchase than screw fixation and can be left in indefinitely (unlike an external fixator).
RECOMMENDED READINGS
Dalla Paola L, Volpe A, Varotto D, Postorino A, Brocco E, Senesi A, Merico M, De Vido D, Da Ros R, Assaloni R. Use of a retrograde nail for ankle arthrodesis in Charcot neuroarthropathy: a limb salvage procedure. Foot Ankle Int. 2007 Sep;28(9):967-70. PubMed PMID: 17880869. View Abstract at PubMed
Pinzur MS. Benchmark analysis of diabetic patients with neuropathic (Charcot) foot deformity. Foot Ankle Int. 1999 Sep;20(9):564-7. PubMed PMID: 10509683. View Abstract at PubMed Pinzur M. Surgical versus accommodative treatment for Charcot arthropathy of the midfoot. Foot Ankle Int. 2004 Aug;25(8):545-9. PubMed PMID: 15363375. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 87

Figures 83a and 83b are the clinical photographs of a 42-year-old woman with a BMI of 31 who has had a 1-year history of right heel pain.
A
B
Question 12
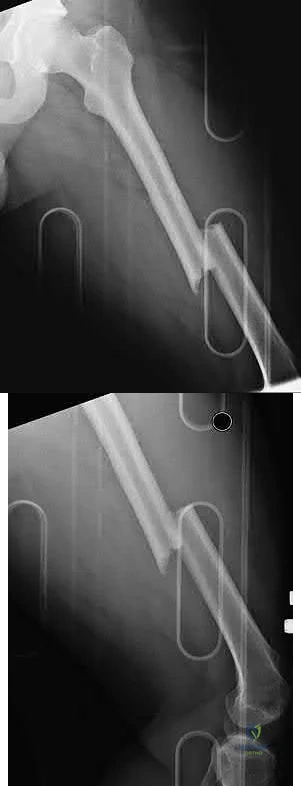
A 32-year-old man is brought to the emergency department after being involved in an MVC. He is found to have a closed left femoral shaft fracture (Figures A and B) and a Glasgow Coma Scale (GCS) score of 13. A CT scan of the head is performed and demonstrates no significant bleeding. He has no other injuries and is hemodynamically stable. Which of the following statements is true?
Explanation
Treatment of patients with a closed head injury and a femoral fracture remains controversial but recent data suggests that intramedullary nails done acutely
leads to decreased pulmonary complications, decreased thromboembolic events, improved rehabilitation, decreased length of stay and cost of hospitalization, and improved GCS scores on discharge. However, it is important to note that intraoperative hypotension should be avoided in these patients, as it has been associated with worsening outcomes following acute intramedullary nailing of the femur.
Starr et al. performed a retrospective study to determine if the timing of treatment of femur fractures in patients with an associated head injury had an effect on the risk of pulmonary and CNS complications. They found that delaying fracture stabilization (> 24 hours) made pulmonary complications 45 times more likely, while early fracture stabilization had no effect on the risk of CNS complications.
McKee et al. performed a retrospective case-control study to determine the effect of early intramedullary nailing of femoral shaft fractures on the neurologic outcome of patients with multiple injuries and a concomitant head injury. They found no significant differences between the two groups in terms of early mortality, length of hospital/ICU stay, level of neurologic disability, or results of cognitive testing. Their results support the continued early intramedullary nailing of femoral fractures for patients with a concomitant head injury.
Richards et al. performed a retrospective study evaluating lactate levels before reamed intramedullary nailing (IMN) of femur fractures treated with early fixation (< 24 hours) and its effects on pulmonary complications (defined as mechanical ventilation lasting ≥ 5 days). They found that a median admission lactate of 3.7 mmol/L was associated with duration of mechanical ventilation ≥ 5 days, whereas a median preoperative lactate of 2.8 mmol/L was not.
Figures A and B are radiographs demonstrating a transverse femoral shaft fracture.
Incorrect Answers:
OrthoCash 2020
Question 13
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals no other injuries. Radiographs are shown in Figures 35a and 35b. Initial management of this fracture should consist of
Explanation
REFERENCES: Meyers MH, McKeever FM: Fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60
Janarv PM, Westblad P, Johansson C, Hirsch G: Long-term follow-up of anterior tibial spine fractures in children. J Pediatr Orthop 1995;15:63-68.
Kuhn JE, Sailer MJ, Sterett WI, Hawkins RJ: Arthroscopic technique for the treatment of tibial spine fractures in the skeletally immature patient. J Ortho Tech 1995;3:7-12.
Question 14
A 35-year-old woman who runs long distance has had posterior calf tenderness for the past 3 months. A clinical photograph is shown in Figure 10a, and MRI scans are shown in Figures 10b and 10c. Management at this point should consist of
Explanation
REFERENCES: Alfredson H, Pietila T, Jansson P, Lorentzon R: Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med 1998;26:360-366.
Angermann P, Hougaard D: Chronic Achilles tendinopathy in athletic individuals: Results of nonsurgical treatment. Foot Ankle Int 1999;20:304-306.
Question 15
A patient sustains an injury to the pelvis as a result of high-energy trauma. A radiographic and clinical assessment is performed. A lateral view of the pelvis will best identify
Explanation
Question 16
The so-called high ankle sprain from an external rotation mechanism of injury typically involves injury to which of the following structures?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 182.
Kaye RA: Stabilization of ankle syndesmosis injuries with a syndesmosis screw. Foot Ankle 1989;9:290-293.
Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
Pfeffer GB (ed): Chronic Ankle Pain in the Athlete. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 11.
Question 17
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Explanation
REFERENCES: Braddom RL (ed): Physical Medicine and Rehabilitation, ed 2. Philadelphia, PA, Saunders, 2000, pp 975-976.
Childs DC, Irrang JJ: The language of exercise and rehabilitation, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 329.
Question 18
A 68-year-old man underwent a primary total hip arthroplasty 2 years ago for a femoral neck fracture. His early postoperative course was unremarkable, but he notes some aching in the thigh since surgery. His symptoms have gotten worse over the last year, such that he now has activity-related thigh pain that limits his walking ability. An AP hip radiograph is shown in Figure 9. What is the most appropriate surgical management?
Explanation
There is a reactive radiolucent line around the fiber mesh portion of the implant, hypertrophy of the bone under the collar, and a pedestal formation at the distal tip of the implant, all of which indicate failure of bone ingrowth. If
bone ingrowth had occurred, there would be stress shielding of bone under the collar.
REFERENCES: Engh CA, Massin P, Suthers KE: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop Relat Res 1990;257:107-128.
Lieberman JR, Huo MH, Schneider R, et al: Evaluation of painful hip arthroplasties: Are technetium bone scans necessary? J Bone Joint Surg Br 1993;75:475-478.
Vresilovic EJ, Hozack WJ, Rothman RH: Radiographic assessment of cementless femoral components: Correlation with intraoperative mechanical stability. J Arthroplasty 1994;9:137-141.
Question 19
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of
Explanation
REFERENCES: Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996,
pp 83-95.
Heinrich SD, Drvaric DM, Darr K, MacEwen GD: The operative stabilization of pediatric diaphyseal femur fractures with flexible intramedullary nails: A prospective analysis. J Pediatr Orthop 1994;14:501-507.
Question 20
A 40-year-old man reports an enlarging soft-tissue mass in his right shoulder. Based on the MRI scan and biopsy specimens shown in Figures 40a through 40c, what is the most likely diagnosis?
Explanation
are arranged in short, irregular bundles and fascicles and are adjacent to collagen and reticulin. The lesions can appear to be more myxoid or more fibrotic in nature and this correlates to the duration of symptoms. The lesions with a short duration of symptoms have a more myxoid appearance in contrast to those of longer duration characterized by hyaline fibrosis.
REFERENCES: Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 250-266.
Wang XL, De Schepper AM, Vanhoenacker F, et al: Nodular fasciitis: Correlation of MRI findings and histopathology. Skeletal Radiol 2002;31;155-161.
Question 21
Which of the following changes to heart rate, blood pressure, and bulbocavernosus reflex are typical of spinal shock?
Explanation
REFERENCE: Ditunno JF, Little JW, Tessler A, et al: Spinal shock revisited: A four-phase model. Spinal Cord 2004;42:383-395.
Question 22
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of
Explanation
REFERENCES: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Asnis SE, Wanek-Sgaglione L: Intracapsular fractures of the femoral neck: Results of cannulated screw fixation. J Bone Joint Surg 1994;76A:1793-1803.
Question 23
- The primary effect of deep freezing on musculoskeletal allografts is a reduction of
Explanation
Question 24
A 28-year-old woman who is training for the New York Marathon reports pain in the posteromedial aspect of her right ankle. Examination reveals tenderness just posterior to the medial malleolus. Radiographs are normal. An MRI scan is shown in Figure 3. What is the most likely diagnosis?
Explanation
REFERENCES: Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Lee JK, Yao L: Stress fractures: MR imaging. Radiology 1988;169:217-220.
Question 25
Figure 45 shows the lateral radiograph of a 19-year-old swimmer who has had back pain for the past 2 months. What is the most likely diagnosis?
Explanation
REFERENCES: Papanicolaou N, Wilkinson RH, Emmans JB, Treves S, Micheli LJ: Bone scintigraphy and radiography in young athletes with low back pain. Am J Roentgenol 1985;145:1039-1044.
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 291-302.
Question 26
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of
Explanation
REFERENCES: Jakob RP, Miniaci A, Anson PS, et al: Four-part valgus impacted fractures of the proximal humerus. J Bone Joint Surg Br 1991;73:295-298.
Resch H, Povacz P, Frohlich R, et al: Percutaneous fixation of three- and four-part fractures of the proximal humerus. J Bone Joint Surg Br 1997;79:295-300.
Question 27
What is the most common organism found following a nail puncture wound through tennis shoes in a host without immunocompromise?
Explanation
REFERENCES: Green NE, Bruno J III: Pseudomonas infections of the foot after puncture wounds. South Med J 1980;73:146-149.
Riegler HF, Routson GW: Complications of deep puncture wounds of the foot. J Trauma 1979;19:18-22.
Question 28
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty? i. Infection
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
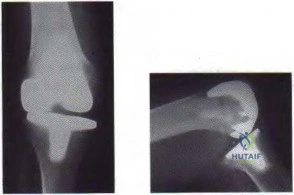
Figure 59a Figure 59b
Question 29
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Explanation
REFERENCES: Miller MD: Review of Orthopaedics, ed 3. Philadelphia PA, WB Saunders, 2000, p 116.
Guanche CA, Kozin SH, Levy AS, et al: The use of MRI in the diagnosis of occult hip fractures in the elderly: A preliminary review. Orthopedics 1994;17:327-330.
Question 30
A 60-year-old woman has a mass in the right scapula. Figures 25a and 25b show a CT scan and a biopsy specimen. The cells are lymphocyte common antigen positive, Ewing’s specific antigen (CD99) negative, and keratin negative. What is the next step in management?
Explanation
REFERENCES: Finiewicz K, van Biesen K: Non-Hodgkins lymphoma, in Golomb H, Vokes E (eds): Oncologic Therapies, ed 2. Berlin, Germany, Springer, 2003, pp 295-318.
Lems P, Primus G, Anastas J, Doherty D, Montag AG, Peabody TD, Simon MA: Oncologic outcomes of primary lymphoma of bone in adults. Clin Orthop 2003;415:90-97.
Question 31
Which of the following surgical devices employed for stabilization of the sternoclavicular joint is associated with the highest incidence of life-threatening complications?
Explanation
REFERENCES: Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.
Lyons FA, Rockwood CA Jr: Migration of pins used in operations of the shoulder. J Bone Joint Surg Am 1990;72:1262-1267.
Question 32
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
Explanation
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity
= 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Question 33
A 30-year-old woman has had pain in her right leg for the past 6 months. A lytic lesion is noted in the anterior cortex of the midtibia, extending 5 cm in length without a soft-tissue mass. A radiograph and a biopsy specimen are shown in Figures 35a and 35b. What is the preferred treatment?
Explanation
REFERENCES: McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 263.
Moon NF, Mori H: Adamantinoma of the appendicular skeleton: Updated. Clin Orthop Relat Res 1986;204:215-237.
Question 34
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with Review Topic
Explanation
Question 35
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
D’Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up.
Am J Sports Med 2004;32:21-33.
Levine WN, Clark AM Jr, D’Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 278-279.
Question 36
A 25-year-old man has an isolated flexor digitorum profundus laceration just proximal to the distal interphalangeal (DIP) flexion crease of his ring finger. The tendon ends are trimmed, removing 10 mm from each end (secondary to fraying) and the tendon repaired. Four months later, he reports limited finger motion of the long, ring, and small fingers. He cannot fully extend his wrist and all joints of the 3 fingers simultaneously. He has full passive flexion but cannot actively completely close his fingers into a fist. What is the most likely cause?
Explanation
If a single flexor digitorum profundus (FDP) tendon is debrided more than 1 cm prior to repair, the tendon is advanced too far distally, essentially shortening the musculotendon unit. The finger will likely develop a flexion posture. Because of the common muscle belly and interconnections of the profundi, the long and small fingers adjacent to the injured finger will be affected because of loss of some of their normal proximal excursion. The result is an inability of the adjacent fingers to completely flex. This condition, known as quadrigia, is named after the Roman chariot driver who held control of the reins of 4 horses, forcing them to move as 1. Quadrigia occurs when the FDP tendon is advanced too far distally, when a tendon graft is too short, or when the profundus is sutured over the end of an amputated digit. Intrinsic muscles of the hand flex the metacarpophalangeal (MP) joints and extend the PIP joint. Intrinsic tightness causes decreased PIP flexion when the MP joint is in extension. The lumbrical muscle modulates tension on the flexor profundus tendon. When a tendon graft to repair the profundus tendon is too long, a lumbrical plus deformity occurs. This is a paradoxical PIP extension as the finger is flexed. Disruption of the tendon
repair causes limited flexion of the injured finger.
Question 37
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-247.
Question 38
When a patient has recurrent anterior shoulder instability, a bony glenoid reconstructive procedure should be considered in which clinical setting?
Explanation
in collision athletes.
Question 39
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to
Explanation
REFERENCES: Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Question 40
An investigation studying whether physical therapy or subacromial injection can be successfully used to treat shoulder pain is conducted. Two groups are identified. One group is prescribed physical therapy, while the other receives a subacromial injection. The groups have similar baseline demographics and shoulder pathologies. Ten patients are randomized in each group and findings show that there is no significant difference in any patient-reported outcome measure. An increase in sample size would reduce the risk of what parameter?
Explanation
Question 41
A 68-year-old woman with metastatic breast carcinoma is seen in the emergency department. She appears lethargic, and she reports abdominal pain, nausea, and constipation. An EKG reveals a shortened QT interval. The only physical finding on examination is diffuse hyporeflexia. What is the most appropriate step in management?
Explanation
REFERENCE: Stewart AF: Clinical practice: Hypercalcemia associated with cancer. N Engl J of Med 2005;352:373-379.
Question 42
Free flap coverage for severe trauma to the upper extremity has the fewest complications when performed within what time period after injury?
Explanation
REFERENCES: Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
Manske PR (ed): Hand Surgery Update. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 31-37.
Question 43
A 14-year-old girl reports bilateral patellofemoral symptoms. Based on the radiograph and MRI scans shown in Figures 23a through 23d, what is the next most appropriate step in management of the lesion?
Explanation
REFERENCES: Dunham WK, Marcus NW, Enneking WF, et al: Developmental defects of the distal femoral metaphysis. J Bone Joint Surg Am 1980;62:801-806.
Verdonk PC, Verstraete K, Verdonk R: Distal femoral cortical irregularity in a 13-year old boy: A case report. Acta Orthop Belg 2003;69:377-381.
Question 44
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. A large intra-articular and intrapelvic pseudotumor has developed. What predominant histological feature(s) is/are present in such a lesion?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross-sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 45
A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment? Review Topic

Explanation
appears to be helpful. A hindfoot arthrodesis (usually triple) would be reserved if coalition resection proves to be unsuccessful. Achilles tendon lengthening and orthotic support, as well as debridement of the sinus tarsi, are not expected to result in a satisfactory outcome. The patient does not have a flatfoot deformity.
(SBQ13PE.64) A 5-year-old boy presents to clinic for evaluation of bilateral foot deformities shown in Figure 1. He is fully active and has no pain. The feet appear normal when he is sitting on the examination table, and there is supple passive motion at the subtalar joint. Passive ankle dorsiflexion is to neutral with knee in extension and 15 degrees with knee in flexion. What is the most appropriate next step? Review Topic

Spine MRI
Standing radiographs of the bilateral feet
Gastrocnemius stretching and nightime use of ankle foot orthosis
Gastrocnemius stretching and use of UCBL orthotic when ambulating
Gastrocnemius stretching
The patient is presenting with bilateral flexible pes planovalgus (or flexbile flatfoot). The most appropriate treatment in patients with a tight heel cord and no pain is gastrocnemius stretching
A flexible flatfoot in a child typically resolves spontaneously. Radiographs are typically indicated when there is pain to rule out other conditions. Treatment for patients without pain includes observation and gastrocnemius stretching. If there is pain, soft arch support or a more rigid UCBL can be used, but orthotics do not change the natural history. In patients with continued tightness in the heel cord despite aggressive stretching, gastrocnemius lengthening may be necessary.
Mosca reviews the management of flexible flatfeet in children and adolescents. He reports that there is no compelling evidence that an arch can be created with use of
orthotics. He proposes the following algorithm: patients with asymptomatic flatfeet are observed; symptomatic flatfeet with tight heel cords undergoing stretching until they become asymptomatic; symptomatic flatfeet with tight heel cords that do not respond to stretching (rare cases) are considered for surgery.
Figure A shows a young a patient with bilateral flatfeet when standing. Incorrect Answers:
abnormalities can seen in patients with cavovarus deformity Answer 2: Radiographs are indicated when there is pain to rule out other conditions. Answer 3: Ankle foot orthoses are not used for pes planovalgus Answer 4: UCBL would be indicated if the patient was having pain.
(SBQ13PE.42) Submuscular bridge plating is appropriate treatment for which of the following? Review Topic
A 2-month-old female with displaced, spiral, mid-diaphyseal femur fracture
A 26-month-old boy with a displaced spiral mid-diaphyseal femur fracture with
<2cm shortening
A 7-year old boy with a transverse, non-comminuted mid-diaphyseal femur fracture
A 7-year-old boy with a highly comminuted mid-diaphyseal femur fracture
A 15-year-old girl with a displaced butterfly fragmented mid-diaphyseal femur fracture
Submuscular bridge plating is appropriate for length-unstable femur fractures in skeletally immature patients ages 6 years and older.
Traditional plating of diaphyseal femur fractures in children has been abandoned due to the large incision and significant periosteal stripping involved. Submuscular plating with limited incisions and percutaneously applied fixation is a more biologically friendly way to achieve rigid internal fixation in length-unstable fracture patterns. External fixation is another acceptable option for these fractures. Locked plating, on the other hand, provides an 'internal external fixator,' avoids pin site issues and allows rapid mobilization while providing a biologically favorable environment for healing.
Kocher et al. provide the AAOS Clinical Practice Guideline for the treatment of pediatric diaphyseal femur fractures. They concluded that there was insufficient evidence regarding submuscular bridge plating to include it in the guideline.
Flynn et al. review the management of pediatric femoral shaft fractures. The note that
the narrow indications for plating of pediatric femoral fractures are open fractures, multiple trauma, head injury or compartment syndrome in patients less than 12 years old. Plating allows rigid fixation with readily available equipment and allows for rapid mobilization.
Hedequist et al. present a Technical Tricks paper in which they detail their surgical technique for submuscular bridge plating. They recommend this fixation strategy for patients between age 6 and skeletal maturity with comminuted diaphyseal femur fractures that are not easily treated by other methods.
Illustration A shows a preoperative and postoperative radiograph of a comminuted pediatric femur fracture treated with submuscular plating.
Incorrect answers:
(SBQ13PE.88) A 12-month-old boy attends a government regulated childcare center. His parents are called after a fall. Non-accidental trauma has been ruled out. On physical examination the right elbow is swollen and tender. He is unwilling to allow you to move the arm. Radiographs of the elbow are shown in Figure A. What is the orthopaedic management of this injury? Review Topic

Observation only
Elbow sling for 3 to 4 weeks
Rigid elbow immobilisation for 4 to 5 weeks
Admit for 24-48 hours for continuous intracompartmental pressure measurements
Operative fixation with percutaneous pinning PREFERRED RESPONSE 5
This patient presents with a distal humeral physeal separation. The most appropriate treatment would be closed reduction with internal fixation with percutaneous pins.
Displaced distal humerus physeal separation is typically seen in children under the age of 3 and has a high association with child abuse. The diagnosis can be a difficult as radiographs of a distal humeral physeal separation may be subtle. Often, radiographs show no obvious fracture, but can appear like an elbow dislocation since the secondary ossification centers have not yet developed. MRI or arthrogram can be used to aid in diagnosis.
Shrader et al. reviewed pediatric supracondylar fractures and pediatric physeal elbow fractures. They state the key to diagnosis of distal humerus physeal separation is the assessment is the radial head–capitellum relationship. These injuries should be fixed with closed reduction and smooth wire pinning. An elbow arthrogram may be considered intraoperatively for these patients because of the difficulty visualizing the distal humeral anatomy in children so young.
Skaggs et al. reviewed the diagnosis and management of pediatric elbow fractures. He states that child abuse should be suspected in all cases of elbow fracture when the child is less than 3 years of age and/or the injury pattern occur from a shearing mechanism. The displacement of physeal elbow fractures is almost always posteromedial.
Figure A shows AP and lateral radiographs with posteromedial displacement of the radial and ulnar shafts relative to the distal humerus. This is consistent with distal humeral physeal separation.
Incorrect Answers:
Question 46
What ligament is the primary restraint to applied valgus loading of the knee?
Explanation
REFERENCE: Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 767.
Question 47
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
Explanation
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Baker CL, Uribe JW, Whitman C: Arthroscopic evaluation of acute initial anterior shoulder dislocations. Am J Sports Med 1990;18:25-28.
Question 48
Figures 1a and 1b are the recent radiographs of an 82-year-old man with rheumatoid arthritis who underwent total knee arthroplasty (TKA) 18 years ago. These radiographs reveal osteolysis with loosening of the tibial component. Aspiration and laboratory study findings for infection are negative. During the revision TKA, treatment of tibial bone loss should consist of
Explanation

Video 1 for reference
For severe tibial defects (Anderson Orthopaedic Research Institute [AORI] types 2 and 3), metaphyseal fixation is necessary to achieve construct fixation during revision TKA. Metaphyseal fixation may be achieved with cement, structural allograft, or conical metallic implants. The major concerns regarding structural allograft are graft resorption and mechanical failure and technical issues related to fashioning the graft and obtaining a good host-allograft interface. In a systematic review, porous metal cones were associated with a decreased loosening rate in AORI 2 and 3 defects compared to structural allografts. Metallic trabecular metal cones and metaphyseal porous coated sleeves provide a stable construct with which to support the tibial component during revision TKA. Clinical results with these devices include good metaphyseal fixation for severe tibial bone defects.
Question 49
A neurologic injury at T11-L2 with loss of bowel and bladder control is best described as what syndrome?
Explanation
REFERENCES: Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Weisberg LA: Neurologic localization: Lesions below foramen magnum, in Weisberg LA, Strub RL, Garcia CA (eds): Adult Neurology, ed 2. St. Louis, MO, Mosby, 1993.
Question 50
A 9-month-old nonambulatory girl is seen in the emergency department with a fracture of her right forearm. The mother says she fell from the changing table yesterday and continues to cry and not use her right arm. Radiographs are shown in Figure 31. Treatment should consist of which of the following? Review Topic

Explanation
efficient way to evaluate for other fractures. A MRI of the brain is not indicated unless fundoscopic examination reveals an abnormality.
Question 51
Which of the following methods most reliably detects mechanical loosening of the hip?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Miniaci A, Bailey WH, Bourne RB, McLaren AC, Rorabeck CH: Analysis of radionuclide arthrograms, radiographic arthrograms, and sequential plain radiographs in the assessment of painful hip arthroplasty. J Arthroplasty 1990;5:143-149.
Question 52
A 25-year-old man has had an insidious onset of left hip pain over the past 11 months. A radiograph, coronal MRI scan, and histopathologic specimens are seen in Figures 2a through 2d. What is the most likely diagnosis?
Explanation
REFERENCE: Sucato DJ, Rougraff B, McGrath BE, et al: Ewing’s sarcoma of the pelvis: Long-term survival and functional outcome. Clin Orthop 2000;373:193-201.
Question 53
A 25-year-old man injured his dominant shoulder after falling on his outstretched arm 4 months ago. Examination reveals that he cannot lift his arm above 90 degrees, and he has pronounced medial scapular winging. Management should consist of
Explanation
REFERENCES: Post M: Pectoralis major transfer for winging of the scapula. J Shoulder Elbow Surg 1995;4:1-9.
Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 54
-A 42-year-old patient with a right distal radius fracture underwent open reduction and internal fixation. To reduce the likelihood of complex regional pain syndrome, the most appropriate medication is
Explanation

Question 55
An 8-year-old boy has had pain and swelling around the right knee for the past 4 weeks. He recalls bumping it about 4 weeks ago. He has no pain in other joints, and denies any fevers, chills, or other symptoms. A radiograph is shown in Figure 13. Laboratory studies show a WBC count of 9,700/mm P 3 P , an erythrocyte sedimentation rate of 18 mm/h, and a C-reactive protein level of 3.7 mg/L. What is the next most appropriate step in management?
Explanation
REFERENCES: Morrisy RT: Bone and joint sepsis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 466-470.
Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis, and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 56
A year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the
aspiration and proceed to a revision TKA with possible augments on standby.
Question 57
Figures 1 through 3 are the weight-bearing radiograph and MRI scans of a 27-year-old man who twisted his knee coming down awkwardly from a lay-up during a basketball game. He felt a sharp stabbing pain in the posterior aspect of his knee at the time of the injury. Physical examination reveals a trace effusion, full range of motion but pain with hyperflexion >90° degrees and tenderness over the affected joint line. What is the most appropriate treatment at this time?

Explanation
root tears lead to progressive degenerative changes as a result of the altered tibiofemoral contact pressures and areas. Nonsurgical treatment including injections, physical therapy, and unloader braces are more appropriate in the older patient with pre-existing advanced degenerative changes.
Question 58
What is the most appropriate treatment for a chordoma involving the sacrum?
Explanation
REFERENCES: Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133.
Stener B, Gunterberg B: High amputation of the sacrum for extirpation of tumors: Principles and technique. Spine 1978;3:351-366.
Stener B: Resection of the sacrum for tumors. Chir Organi Mov 1990;75:S108-S110.
Question 59
Which of the following bones is most frequently involved in stress fractures in athletes? Review Topic
Explanation
Question 60
Based on the findings seen at C5-6 in Figure 30, the most likely deficit for this patient will be weakness of the
Explanation
REFERENCE: Hoppenfeld S: Evaluation of nerve root lesions involving the upper extremity, in Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-23.
Question 61
In overhead athletic activities, the kinetic chain generates what percentage of force from the leg and trunk segments of the chain?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 47.
McClure PW, Michener LA, Sennett BJ, et al: Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg 2001;10:269-277.
Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 2003;19:641-661.
Question 62
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
(type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive.
REFERENCES: Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Zerres K, Wirth B, Rudnik-Schoneborn S: Spinal muscular atrophy: Clinical and genetic correlations. Neuromuscul Disord 1997;7:202-207.
Question 63
A teenager is undergoing a correction of deformity and lengthening of the femur. Distractions are proceeding as expected; however, during his 6-week follow-up examination, the patient reports that the distraction motors have become harder to turn over for the past 2 to 3 days. Figures 37a and 37b show current radiographs. What is the most likely complication being encountered?
Explanation
REFERENCES: Paley D: Problems, obstacles and complications of limb lengthening, in Maiocchi AB, Aronson J (eds): Operative Principles of Ilizarov. Baltimore, MD, Williams & Wilkins, 1991, p 360.
Herring JA: Limb length discrepancy, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics,
ed 3. Philadelphia, PA, WB Saunders, 2002, p 1088.
Question 64
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern? Review Topic
Explanation
Question 65
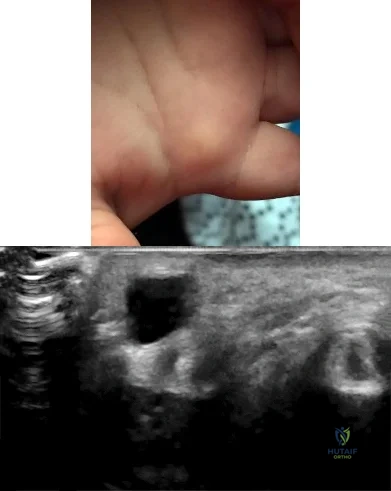
Figures 1 and 2 show the clinical photograph and ultrasonography image obtained from an 8-month-old boy who has a 2-month history of a well-circumscribed mass in the palm, just proximal to the palmar digital crease of the index finger. The mass has not changed in size and does not seem to cause pain. What is the best next step in treatment?
Explanation
The history, clinical photograph, and ultrasonography evaluation point to a diagnosis of ganglion cyst. The likelihood of resolution of ganglion cysts without intervention in pediatric patients ranges from 66-79%. Therefore the most appropriate treatment at this time is observation. Because the diagnosis is confirmed with the information provided, excisional biopsy and further imaging are not necessary.
Question 66
A 38-year-old man who is an avid runner reports a several month history of right hip pain. Based on the radiograph and cross-sectional CT scan shown in Figures 33a and 33b, what is the most likely diagnosis for the lesions seen on the femoral neck?
Explanation
REFERENCES: Pitt MJ, Graham AR, Shipman JH, et al: Herniation pit of the femoral neck. Am J Roentgenol 1982;138:1115-1121.
Daenen B, Preidler KW, Padmanabhan S, et al: Symptomatic herniation pits of the femoral neck: Anatomic and clinical study. Am J Roentgenol 1997;168:149-153.
Question 67
Consider the theoretic articulation shown in Figure 11 as femoral and tibial components of a total knee prosthesis in which the components fit like a “roller in trough.” Which of the following best describes the articulation?
Explanation
REFERENCE: Alicea J: Scoring systems and their validation for the arthritic knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1507-1515.
Question 68
Which of the following procedures is not part of the routine evaluation of a patient with suspected metastatic disease to bone?
Explanation
REFERENCES: Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
Frassica FJ, Gitelis S, Sim FH: Metastic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 69
below show the radiographs obtained from a year-old woman with a year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?
Explanation
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 70
A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root. You suggest a left-sided L5-S1 microdiskectomy and tell her that when comparing tubular diskectomy and open procedures
Explanation
Several comparative studies have reported no difference in functional outcomes between tubular diskectomy and microsurgical lumbar diskectomy. A recent systematic review by Kamper and associates in which conventional microdiskectomy and minimally invasive approaches were compared revealed that there was no difference between the procedures in terms of clinical outcomes, complication risk, or rate of revision surgery.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183.View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 71
What antithrombotic agent is a selective factor I0a inhibitor? Review Topic
Explanation
Question 72
A 15-year-old boy falls from his bicycle and sustains an injury to his elbow. Prereduction radiographs are shown in Figure 12a. Closed reduction is performed without difficulty and postreduction radiographs are shown in Figure 12b. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Rasool MN: Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-1058.
Beaty JH: Fractures and dislocations about the elbow in children. Instr Course Lect 1992;41:373-384.
Question 73
Figure 9 shows a cross-sectional view of the spinal cord at the lower cervical level. Injury to the structure indicated by the black arrow will lead to what neurologic deficit?
Explanation
REFERENCES: Bohlman H, Ducker T, Levine A: Spine trauma in adults, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 911.
Northrup B: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 545.
Question 74
Which of the following is considered an advantage of the tibial inlay fixation compared to transtibial tunnel technique when used in posterior cruciate ligament reconstruction? Review Topic
Explanation
Question 75
A patient in the recovery room has weakness of the extensor hallucis longus and tibialis anterior muscles following a total knee replacement. Initial management should consist of
Explanation
This is a rare
complication of TKA, and when conservative nonoperative measures do not lead to sufficient improvement in nerve function, consideration may be given to operative decompression of the peroneal nerve.
Question 76
A 46-year-old male construction worker has right hip pain that has failed to respond to nonsurgical management. His body mass index (BMI) is 32, he is 6’2” tall, and he has no other medical comorbidities. AP and lateral radiographs of the right hip are shown in Figures 23a and 23b. The patient inquires about his suitability for metal-on-metal hip resurfacing. The patient should be educated that he is at higher risk for failure secondary to which of the following?
Explanation
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
distal femoral varus osteotomy.
osteoarticular transplant to the lateral femoral condyle.
unicondylar arthroplasty.
high tibial osteotomy.
Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
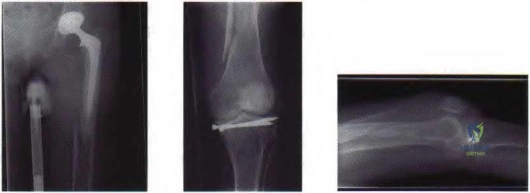
Figure 25a Figure 25b Figure 25c
Question 77
A 21-year-old basketball player inverts his foot during practice. Examination reveals obvious deformity of the hindfoot with a prominence of the talar head dorsolaterally and medial displacement of the forefoot. A radiograph is shown in Figure 17. What is the most likely obstacle to closed reduction?
Explanation
REFERENCES: Mulroy RD: The tibialis posterior tendon as an obstacle to reduction of a lateral anterior subtalar dislocation. J Bone Joint Surg Am 1953;37:859-863.
Heckman JD: Fractures and dislocations of the foot, in Rockwood CA, Green DP, Bucholz RW (eds): Fractures in Adults. Philadelphia, PA, JB Lippincott, 1991, pp 2093-2100.
Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
Question 78
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
Explanation
REFERENCES: Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.
Question 79
A 67-year-old woman has a painful, arthritic proximal interphalangeal (PIP) joint, and nonsurgical measures have failed to improve the pain. What implant and joint replacement approach combination has been demonstrated to have the lowest rate of revision surgery?
Explanation
A recent systematic review compared silicone replacement, pyrocarbon replacement, and surface replacement arthroplasty for PIP arthritis. Silicone arthroplasty through a volar approach showed the greatest gains in arc of motion and had the lowest rate of revision surgeries. The rates of revision surgeries from low to high for each type of arthroplasty were 6% for silicone volar, 10% for silicone lateral, 11%
Surface replacement arthroplasty through a volar
for silicone dorsal, 18% for surface replacement dorsal, and 37% for surface replacement volar. Revision surgeries include implant replacement (to silicone or maintaining the surface replacement), arthrodesis, explantation, amputation, and other procedures.
approach showed the highest revision rate, the worst gain in arc of motion, and the greatest extension lag. However, substantial pain relief and higher satisfaction still were reported after surface replacement arthroplasty, regardless of the complications.
Question 80
- Demyelination diseases as multiple sclerosis and Guillain-Barre $ create neurologic symptoms by
Explanation
Question 81
A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Chan KW, McAdams TR: Central screw placement in percutaneous screw scaphoid fixation: A cadaveric comparison of proximal and distal techniques. J Hand Surg Am 2004;29:74-79.
Bedi A, Jebson PJ, Hayden RJ, et al: Internal fixation of acute non-displaced scaphoid waist fractures via a limited dorsal approach: An assessment or radiographic and functional outcomes. J Hand Surg Am 2007;32:326-333.
McCallister WV, Knight J, Kaliappan R, et al: Central placement of the screw in simulated fractures of the scaphoid waist: A biomechanical study. J Bone Joint Surg Am 2003;85:72-77.
Question 82
A 42-year-old man sustained a burst fracture at L2 in a motor vehicle accident. Examination reveals that he is neurologically intact. Figure 18 shows a cross-sectional CT scan through the fracture. If the fracture is managed nonsurgically for the next 2 years, the retained fragments can be expected to
Explanation
REFERENCES: Mumford J, Weinstein JN, Spratt KF, et al: Thoracolumbar burst fractures: The clinical efficacy and outcome of nonoperative management. Spine 1993;18:955-970.
Wood KB, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurologic deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Question 83
A new composite material is being evaluated for potential use as a prosthetic ligament. In measuring the tensile strength of this material, why is it important to consider and accurately control the loading rate?
Explanation
Question 84
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of
Explanation
REFERENCES: Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Wredmark T, Carlstedt CA, Bauer H, et al: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Question 85
A 17-year-old patient sustained a closed calcaneal fracture when he jumped off of a roof 2 years ago, and he underwent nonsurgical management at the time of injury. The patient now reports lateral hindfoot pain that is worse with weight-bearing activities. Anti-inflammatory drugs and orthoses have failed to provide relief. Coronal and sagittal CT scans are shown in Figures 36a and 36b. What is the best course of action?
Explanation
REFERENCES: Chandler JT, Bonar SK, Anderson RB, et al: Results of in situ subtalar arthrodesis for late sequelae of calcaneus fractures. Foot Ankle Int 1999;20:18-24.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, p 52.
Question 86
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury? Review Topic

Explanation
Question 87
A 23-year-old woman has had vague left knee pain for the past 6 months. A radiograph and CT scan are shown in Figures 50a and 50b. What is the most likely diagnosis?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 185-196.
Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK: Parosteal osteosarcoma. A clinicopathological study. J Bone Joint Surg Am 1994;76:366-378.
Question 88
A 45-year-old construction worker sees a surgeon 23 days after sustaining an eccentric injury to his dominant right elbow. An MRI demonstrates a distal biceps tendon rupture with 5 cm of proximal retraction. In the operating room, the surgeon encounters good tissue quality but finds that primary repair can only be performed with the elbow hyperflexed to 70°. What is the best next step?
Explanation
strength. Isolated debridement of the distal tendon would not be an appropriate treatment.
Question 89
A 73-year-old man reports increasing back and lower extremity pain. A bone scan is shown in Figure 31. What is the most likely diagnosis?
Explanation
REFERENCES: Roudier MP, Vesselle H, True LD, Higano CS, Ott SM, King SH, Vessella RL: Bone histology at autopsy and matched bone scintigraphy findings in patients with hormone refractory prostate cancer: The effect of bisphosphonate therapy on bone scintigraphy results. Clin Exp Metastasis 2003;20:171-180.
Sartor O: Radioisotopic treatment of bone pain from metastatic prostate cancer. Curr Oncol Rep 2003;5:258-262.
Question 90
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
REFERENCES: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: How do these ankles function over time? J Bone Joint Surg Am 2003;85:287-295.
Question 91
- Which of the following factors is most likely to predispose a patient to dislocation of the patellar component following total knee arthoplasty?
Explanation
Internally rotating the femoral component produced abnormal laxity seen at 30, 60, and 90 degrees of flexion. There was no gapping noted in the neutral or externally rotated specimens.
The normal pattern for patellar tracking was a gentle curve with maximal deflection at 15 and 60 degrees of flexion. The maximal medial displacement were lowest for the externally rotated specimens.
Although contact areas could not be quantitatively measured accurately, the contact areas were more evenly distributed between the medial and lateral sides of the patella in the externally rotated specimens than they were in either the internally rotated or neutral specimens.
You have to be careful interpreting this data at least in reference to knee stability. In this study a perpendicular tibial cut was made. The normal tibia has a 30 degree varus slope and thus more bone is resected from the lateral surface. External rotation of the femoral component compensates for this.
No tests were done with lateral placement of the femoral component or medial placement of the patellar component.
Question 92
Which of the following structures is most vulnerable during a medial sesamoidectomy of the hallux?
Explanation
REFERENCE: Sarrafian SK: Anatomy of the Foot and Ankle, Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, p 377.
Question 93
What root is most commonly involved with a segmental root level palsy after laminoplasty?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-249.
Uematsu Y, Tokuhashi Y, Matsuzaki H: Radiculopathy after laminoplasty of the cervical spine. Spine 1998;23:2057-2062.
Question 94
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?

Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 95
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
Explanation
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Nonarthroplasty), level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1,500 mg/day and chondroitin sulfate 800 mg/day as well as
arthroscopic debridement and lavage).
Question 96
Which of the following is associated with increased fetal morbidity and mortality in acetabular fractures during pregnancy?
Explanation
Question 97
Treatment should now include
Explanation
Extensive laminectomy in patients with degenerative spondylolisthesis does result in postoperative instability. In the study by White and Wiltse, further subluxation did occur in 66 percent of patients who were operated on for degenerative spondylolisthesis , whereas it was observed in only 2 percent of the spondylolisthesis or disc patients who did not have
spondylolisthesis postoperatively. The extent of decompression and facet removal must be limited in the patient with degenerative spondylolisthesis or a fusion of the transverse processes included as part of the treatment. Internal fixation devices have been used in these circumstances to prevent further subluxation while the fusion is consolidating. Wiltse outlined some guidelines for spinal fusion in spinal stenosis: (1) the patient who is less than sixty years old and had degenerative spondylolisthesis with a total loss of posterior stability due to removal of the articular processes (a one-level fusion of the transverse processes); (2) the patient who is less than fifty-five and had a midline decompression for degenerative spondylolisthesis with facet preservation; and
(3) the patient who is less than fifty years old with isthmic spondylolisthesis, if the posterior elements have been removed. Simple degenerative spinal stenosis seldom requires a fusion, even if all posterior stability has been lost. The problem with obtaining a successful spinal fusion is real and conditions are less than optimum in these instances.
Question 98
Metal-on-metal lumbar disk arthroplasty devices may generate cobalt and chromium ions into the serum of patients after implantation into the lumbar spine. Which of the following statements best represents the levels of the serum ion levels in these patients? Review Topic
Explanation
Question 99
A 75-year-old man has persistent radial sided hand and wrist pain. Radiographs demonstrate severe scaphotrapezial trapezoidal arthritis. His basal joint is unaffected. His pain has failed to improve with bracing, activity modification, and image-guided corticosteroid injection. He has elected surgical treatment. What longterm complication can arise from a distal scaphoid resection?
Explanation
Resection of the distal pole of the scaphoid eliminates the arthritic contact at the scaphotrapeziotrapezoid joint; however, it functionally shortens the scaphoid. Theoretically, the lunate is at equilibrium between the extension moment of the capitate and the triquetrum and the flexion moment of the scaphoid. Shortening the scaphoid allows the extension moment of the triquetrum to predominate, pulling the lunate into extension and creating a DISI deformity. Concomitant capsulodesis or interposition is recommended by some authors to prevent this complication.
Question 100
-Figures 156a and 156b are the radiographs of a 38-year-old man with diabetes mellitus who fell 8 feet from a ladder and sustained an isolated closed injury of his leg. Examination revealed swollen but soft compartments. His neurovascular examination was unremarkable. A damage-control fixator was initially applied, and his soft-tissue envelope is now amenable to further intervention. What is the most appropriate treatment?
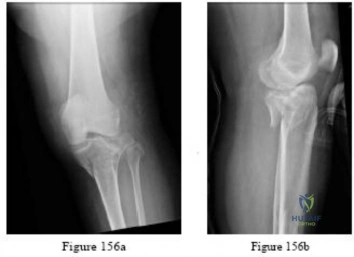
Explanation

