Orthopedic Board Review MCQs: Spine, Trauma, Hip & Shoulder | Part 104

Key Takeaway
This interactive MCQ set (Part 104) aids orthopedic surgeons preparing for OITE/AAOS & ABOS board exams. Authored by Dr. Hutaif, it features 100 high-yield, verified questions covering Dislocation, Hip, Shoulder, Spine, Trauma. Utilize Study/Exam Modes for comprehensive exam preparation.
About This Board Review Set
This is Part 104 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 104
This module focuses heavily on: Dislocation, Hip, Shoulder, Spine, Trauma.
Sample Questions from This Set
Sample Question 1: An 83-year-old man is seen in the emergency department for evaluation of neck pain after a motor vehicle accident. The patient has no neurologic deficits. The patient has a history significant for late stage ankylosing spondylitis with cerv...
Sample Question 2: A 6-year-old boy has leg pain. A radiograph, MRI, CT, and bone scans, and a biopsy specimen are shown in Figures 14a through 14e. What is the most likely diagnosis?...
Sample Question 3: Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management s...
Sample Question 4: A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination...
Sample Question 5: Within the intervertebral disk, aggrecan is primarily responsible for: Review Topic...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An 83-year-old man is seen in the emergency department for evaluation of neck pain after a motor vehicle accident. The patient has no neurologic deficits. The patient has a history significant for late stage ankylosing spondylitis with cervicothoracic kyphosis. What is the most appropriate method of immobilization for the cervical spine while diagnostic testing is performed? Review Topic
Explanation
(SBQ12SP.43) The right vertebral artery sustains a complex injury during a occipitocervical (C3-O) fusion. Bleeding cannot be controlled with local tamponade and a hemostatic agent. After clamping the vessel a segmental defect is noted in the vessel. The patient undergoes urgent angiography, which reveals adequate collateral circulation. What is the next step in the management of this injury? Review Topic
Addition of a systemic antifibrolytic solution
Direct repair
Contralateral vetebral artery anastomosis
Acute synthetic grafting
Embolization treatment
When (1) vetebral artery [VA] bleeding cannot be controlled with local tamponade and a local hemostatic agent, and (2) collateral circulation is maintained in the non-dominant artery (left vertebral artery is usually dominant), the next best step would be to achieve local control with an intraoperative endovascular procedure such as embolization, stenting or clipping.
The management of VA injury is difficult. If local tamponade can be achieved, the next best step would be to consider direct repair of the artery. If tamponade fails to achieve proper hemostasis, additional procedures may be considered, such as intraoperative endovascular embolization, or clipping and ligation. When considering these intraoperative endovascular treatments, the collateral circulation should be assessed. If collateral circulation is inadequate, direct repair or stenting should be reconsidered.
Peng et al. reviewed the anatomical considerations, management, and preventive measures of vertebral artery injury in cervical spine surgery. They showed that
ligation-associated morbidities such as cerebellar infarction, cranial nerve palsies, or hemiplegia can occur in up to 12% of cases. They suggest direct repair should be considered as first-line treatment when local hemostasis can be controlled.
Lall et al. reviewed the perioperative complications associated with occipitocervical fusion. The most commonly encountered complications were related to instrumentation failure after nonunion (6-7%). Other complications included vertebral artery injury (1.3%-4.1% during placement of C1-C2 transarticular screws, most commonly in the case of high-riding vertebral artery), dural tears, and wound infections.
Illustration A shows the treatment algorithm of VA injuries as suggested by Peng et al.
Incorrect Answers:
Question 2
A 6-year-old boy has leg pain. A radiograph, MRI, CT, and bone scans, and a biopsy specimen are shown in Figures 14a through 14e. What is the most likely diagnosis?
Explanation
REFERENCES: Fletcher BD, Hanna SL: Pediatric musculoskeletal lesions simulating neoplasms. Magn Reson Imaging Clin N Am 1996;4:721-747.
Hanna SL, Fletcher BD, Kaste SC, Fairclough DL, Parham DM: Increased confidence of diagnosis of Ewing sarcoma using T2-weighted MR images. Magn Reson Imaging 1994;12:559-568.
Question 3
Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management should consist of
Explanation
REFERENCES: Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Pemberton PA: Pericapsular osteotomy of the ilium for the treatment of congenital subluxation and dislocation of the hip. J Bone Joint Surg Am 1965;47:65-86.
Question 4
A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management?
Explanation
REFERENCES: Stayner LR, Cumming J, Andersen J, et al: Shoulder dislocations in patients older than 40 years of age. Orthop Clin North Am 2000;31:231-239.
Neviaser RJ, Neviaser TJ, Neviaser JS: Concurrent rupture of the rotator cuff and anterior dislocation of the shoulder in the older patient. J Bone Joint Surg Am 1988;70:1308-1311.
Question 5
Within the intervertebral disk, aggrecan is primarily responsible for: Review Topic
Explanation
Aggrecan, the most abundant proteoglycan within the intervertebral disk, is a hydrophillic molecule which helps attract and maintain water within the disc. This is important to maintain compressive strength. Early in life aggrecan has a high percentage of chondroitin sulfate chains. With aging this gradually changes to higher percentage of keratin sulfate. Other proteoglycans include decorin and versican. Decorin is believed to regulate cell cycles and influence fibrillogensis. Versican is a large extra-cellular matrix proteoglycan involved in cell adhesion and migration.
Roughley et al. provide a review of biologic changes within the intervertebral disc during development, maturation, and degeneration. They note that aggrecan works to maintain water content within the disc, thus improving its compressive strength. Aggrecan content decreases with age leading to a loss of compressive strength.
Illustration A shows the structure of aggrecan.
Incorrect answers:
Question 6
A healthy, active year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in A radiograph taken after the fall is shown in He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?
Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 7
An 11-year-old child has Ewing’s sarcoma of the femoral diaphysis with a small soft-tissue mass. Staging studies show no evidence of metastases. Treatment should consist of
Explanation
REFERENCES: Toni A, Neff JR, Sudanese A, et al: The role of surgical therapy in patients with non-metastatic Ewing’s sarcoma of the limbs. Clin Orthop 1991;286:225.
Picci P, Rougraff BT, Bacci G, et al: Prognostic significance of histopathologic response to chemotherapy in non-metastatic Ewing’s sarcoma of the extremities. J Clin Oncol 1993;11:1763.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant Bone Tumors. Instr Course Lect 2002;51:413-428.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 8
Figure 12 shows a lateral radiograph of the elbow. What is the most likely diagnosis?
Explanation
REFERENCE: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 132-133.
Keats TE, Anderson MW: Atlas of Normal Roentgen Variants That May Simulate Disease, ed 7. St Louis, MO, Mosby Inc, 2001, p 497.
Question 9
Figure 30 shows the MRI scan of a 68-year-old woman who has left hip pain. What is the most appropriate treatment?
Explanation
REFERENCES: Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 213-223.
Watson RM, Roach NA, Dalinka MK: Avascular necrosis and bone marrow edema syndrome. Radiol Clin North Am 2004;42:207-219.
Question 10
A 12-year-old girl has had right knee pain for the past 3 months. Radiographs and a coronal T 2 -weighted MRI scan are shown in Figures 10a through 10c. A biopsy specimen is shown in Figure 10d. What is the most appropriate treatment for this lesion?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 11
A 45-year-old tennis player undergoes surgery for chronic lateral epicondylitis. After returning to play, he notes increasing lateral elbow pain with mechanical catching and locking. Examination shows positive supine posterolateral rotatory instability. What ligament has been injured? Review Topic
Explanation
Question 12
Which of the following medications has been shown to improve skeletal muscle regeneration and decrease fibrosis following muscle injury in an animal model? Review Topic
Explanation
Skeletal muscle undergoes a natural process of healing and regeneration after injury. The formation of fibrous tissue in place of normal muscle is also part of this process. However, fibrous tissue in place of muscle can predispose the area to re-injury and impaired function. Administration of angiotensin II receptor blockade medications (e.g. losartan) after skeletal muscle injury has been shown to decrease the apoptotic cascade response and the formation of fibrous tissue. The mechanism of benefit is thought to be associated with blockade of insulin-like growth factor.
Terada et al. looked at the affect of platelet-rich plasma (PRP) and losartan on muscle healing after contusion injuries. They showed that PRP plus losartan combination
therapy improved overall skeletal muscle healing by enhancing angiogenesis and follistatin expression as well as reducing the expression of phosphorylated Smad2/3 and the development of fibrosis.
Bedair et al. used a rat model to investigate the effect of angiotensin receptor blockade on muscle fibrosis after injury. They found that angiotensin receptor blockade therapy significantly reduced fibrosis and led to an increase in the number of regenerating myofibers in acutely injured skeletal muscle.
Incorrect
Question 13
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling’s test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis?
Explanation
REFERENCES: Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
McCarty EC, Tsairis P, Warren RF: Brachial neuritis. Clin Orthop Relat Res 1999;368:37-43.
Question 14
Which of the following deformities is most common after the amputation shown in Figure A?

Explanation
Ng et al. review foot and ankle amputations, and review the issues inherent with each amputation level, including prosthesis fitting and use. They also mention that careful repair of all released or transected tendons is needed to maintain a plantigrade foot.
Early reviews the importance of soft tissue balancing with midfoot amputations. They note that the attachment of the resected tendons into the more proximal retained bones is critical for success in restoration of foot position and ambulation capabilities.
Figure A shows a midfoot amputation as the result of trauma. Illustration A shows the lateral view of the amputation, with an obvious equinus deformity.
Incorrect Answers:
Question 15
5 g/dL and his base deficit is 10mEq/L. What is the most appropriate next step in management?
Explanation
Of all of the reported values, the most important predictor of morbidity and mortality is the base deficit (normal range -2 to +2mEq/L), which represents overall resuscitation status. Another representative parameter of resuscitation status is lactate (normal <2mg/dL). Heart rate, blood pressure and hematocrit are not reliable predictors of normalized resuscitation status, morbidity or mortality.
Callaway et al. retrospectively reviewed a large cohort of blunt trauma patients over a 6 year period. Only base deficit and lactate levels were directly correlated with and were reliable predictors of mortality.
Paladino et al. retrospectively reviewed a prospective database of over 1400 patients. Base deficit and lactate were significant and useful predictors of triage upon initial presentation to denote severe versus non-severe injury.
Martin et al. retrospectively analyzed over 2000 sets of laboratory data in 427 ICU patients. Base deficit (anion status), even in ICU patients with normal lactate levels, were predictive of decreased survival.
Incorrect Answers:
OrthoCash 2020
A 26-year-old male sustains an elbow injury after a fall from a skateboard resulting in valgus and supination forces across the left elbow. A CT scan of the left elbow is shown in Figures A through D. This fracture pattern is most commonly associated with what other traumatic elbow pathology?
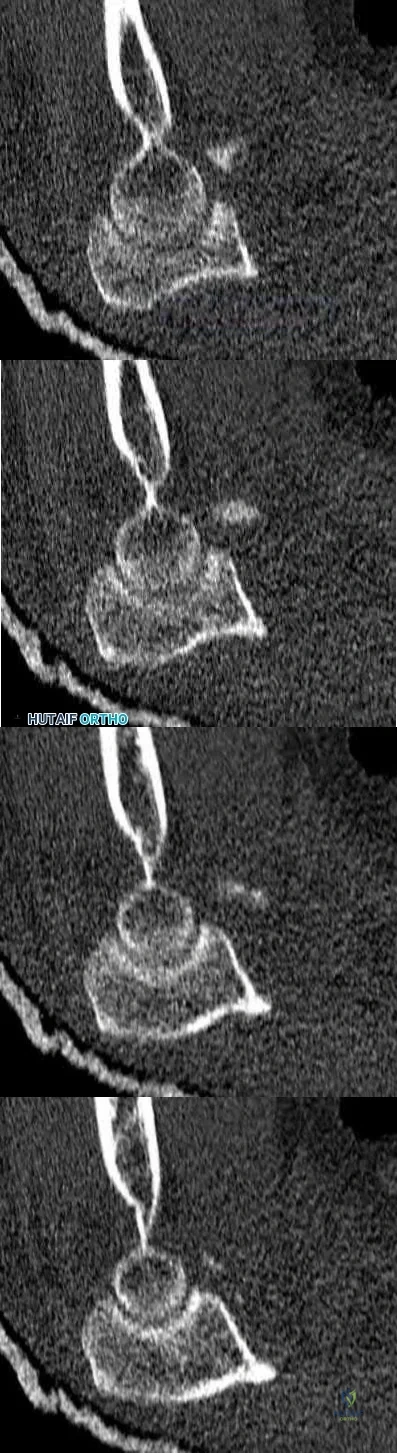
Posteromedial rotatory instability
Capitellum fracture
Radial head fracture and posterolateral ulnohumeral dislocation
Trans-olecranon fracture dislocation
Medial (ulnar) collateral ligament rupture Corrent answer: 3
The clinical presentation is consistent with a coronoid tip fracture. This fracture pattern is associated with a radial head fracture and posterolateral ulnohumeral dislocation - together making up the terrible triad injury.
A terrible triad injury is the result of a valgus and supination injury and involves posterolateral elbow dislocation or lateral collateral ligament injury, radial head fracture, and fracture of the coronoid process. The elbow may dislocate postero-laterally with the anterior bundle of the MCL intact, but if the MCL is injured it is typically the last structure to fail. The coronoid fracture is typically a small fragment isolated to the tip. This is a result of a posteriorly directed force driving the coronoid into the trochlea prior to posterior elbow dislocation. CT scan is a useful modality when small or comminuted fragments are difficult to visualize on plain radiographs.
Steinmann reviews the anatomy, diagnosis, classification and treatment of coronoid fractures with a focus on surgical exposures and fixation techniques.
Doornberg et al. reviewed 67 coronoid fractures to determine whether type of coronoid fracture correlated with pattern of instability. They found strong associations between (1) large coronoid fractures and trans-olecranon fracture-dislocations, (2) small fractures and terrible-triad injuries, and (3) anteromedial facet fractures and varus posteromedial rotational injury mechanisms.
Doornberg et al. evaluated 18 patients with a fracture of the anteromedial facet of the coronoid. They found that malalignment of the anteromedial facet fragment was associated with arthrosis and a fair or poor result.
Figures A through D show consecutive 2.00 mm sagittal CT reformats demonstrating a small coronoid fracture fragment which was addressed with suture fixation.
Incorrect Answers:
OrthoCash 2020
A 62-year-old right-hand-dominant school teacher sustains a mechanical fall at home and presents with right shoulder pain. Plain
radiographs of the right shoulder are pictured in Figures A and B. The patient asks you what she can expect in terms of recovery following this injury. Which of the following is the most appropriate statement?
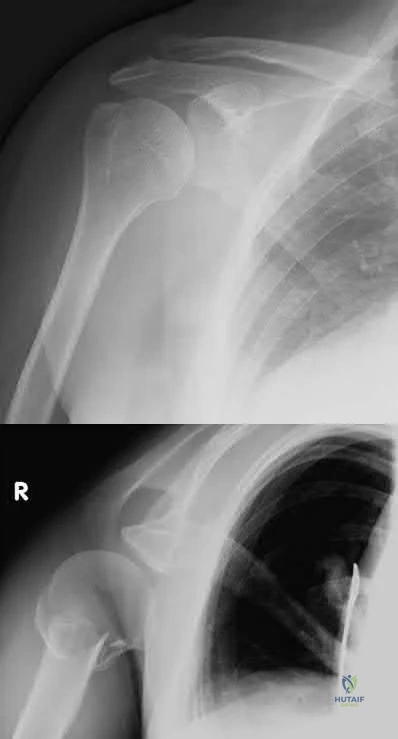
At 1-year post-injury, the right shoulder range of motion will most likely be equal to the contralateral extremity.
At 1-year post-injury, you will most likely have returned to your baseline functional status.
Early range of motion exercises risk fracture displacement and should be avoided until at least 4 weeks post-injury.
Most patients do not return to work following this injury.
One in 5 patients with this fracture go on to nonunion and you may benefit from surgery in the future to address this.
This patient has a minimally displaced (1-part) proximal humerus fracture involving the humeral neck and greater tuberosity. This injury pattern is most commonly managed nonoperatively with the majority of patients returning to their baseline functional status by 1 year.
Proximal humerus fractures (PHF) can be classified by number of parts (Neer classification), with a part defined as a fracture fragment displaced > 1cm (> 5mm for greater tuberosity) or angulated > 45°. One-part PHF comprise ~80% of all PHF and are treated nonoperatively with a sling and early range of motion (ROM).
Tejwani et al performed a prospective study of 67 patients with 1-part PHF. At 1-year follow up the ASES score and functional status was similar to pre-injury status. However, ROM of the affected shoulder was diminished in both external and internal rotation. Forward flexion was preserved.
Hanson et al prospectively analyzed 160 patients with PHF of all types (1-4 parts and head-splitting) managed nonoperatively. At 1-year follow up, 93% showed solid union. Constant and DASH scores improved steadily over time but were still lower compared to the contralateral extremity. Of employed patients, 97.6% returned to work with a median time off of 10 weeks and no difference between manual and nonmanual workers.
Figures A and B are the AP and axillary radiographs of the right shoulder, respectively, demonstrating a 1-part PHF involving the humeral neck and greater tuberosity.
Incorrect Responses:
OrthoCash 2020
A 44-year-old male presents with the isolated injury seen in Figure A after a motor vehicle accident and underwent the operative treatment seen in Figure B within 8 hours from the time of incident. Which of the following complications is this patient at highest risk of developing?

Pulmonary embolus
Periprosthetic fracture
Contralateral hip fracture
Osteonecrosis
Infection
This young male patient has sustained a displaced femoral neck fracture and underwent open reduction internal fixation with 3 cannulated screws. Based on the available options, the patient is most at risk of developing osteonecrosis of the femoral head.
Femoral neck fractures in young patients typically are the result of a high-energy trauma. Fracture displacement has been shown to disrupt vascular supply to the femoral head by interrupting retinacular vessels and ligament teres vascularization, as well as increasing intracapsular pressure, producing a tamponade effect. The incidence of osteonecrosis in patients younger than 60 years with displaced femoral neck fractures has been shown to be between 15-30%. Quality of reduction is one key factor that has been shown to influence outcomes postoperatively.
Loizou et al. prospectively studied 1,023 patients who sustained an intracapsular hip fracture that was treated with internal fixation using standard fixation modalities. They showed that osteonecrosis was less common for undisplaced (4.0%) than for displaced fractures (9.5%). The population at greatest risk were women younger than the age of 60 with displaced fractures.
Barnes et al. review subcapital hip fractures. They found that late segmental collapse was more common in displaced fractures in women younger than age 75 years than in those older than age 75 years treated with internal fixation.
Figure A shows a displaced, Garden 3/Pauwels III hip fracture. Figure B shows anatomical fixation with 3 cannulated screws.
Incorrect Answers:
OrthoCash 2020
A 58-year-old male is involved in a motor vehicle collision and sustains the injury shown in Figure A in addition to right 5th and 6th rib fractures. Upon evaluation in the emergency department, he is noted to have a 2 centimeter laceration over the anterior aspect of his left leg with visible bone. Vitals and labs are normal. Which of the following statements is most accurate regarding surgical management for this patient?

Reamed intramedullary nailing is favored due to increased rates of union
Unreamed intramedullary nailing is favored due to presence of concomitant rib fractures
Reamed intramedullary nailing is favored due to decreased rates of infection
Unreamed intramedullary nailing is favored due to less local trauma
Both unreamed and reamed intramedullary nailing are equivalent Corrent answer: 5
Both unreamed and reamed intramedullary nailing are equivalent treatments in patients with open tibia fractures. Intramedullary nailing is the treatment of choice for stable patients with tibial shaft fractures.
Tibial shaft fractures can be the result of low energy twisting injuries or higher energy axial loads. Closed fractures with acceptable alignment can be often be treated with closed reduction and casting. Intramedullary nailing, unreamed or reamed, is the treatment of choice for open fractures except in the setting of damage control orthopaedics when an external fixator may be more appropriate.
Bhandari et al. investigated reamed and unreamed intramedullary nailing for tibial shaft fractures in a randomized trial ("SPRINT" Trial - Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures Investigators). They concluded that reamed nailing was more beneficial (decreased rate of primary outcome event: need for bone grafting, implant exchange or removal for infection, debridement for infection) for closed fractures, but had no benefit in open fractures.
Finkemeier et al. evaluated consecutive patients treated with unreamed and reamed intramedullary nailing and found similar rates of union in both open and closed tibial shaft fractures at six and twelve months.
Figures A shows AP and lateral xrays of the left tibia showing a tibial shaft fracture.
Incorrect Answers:
OrthoCash 2020
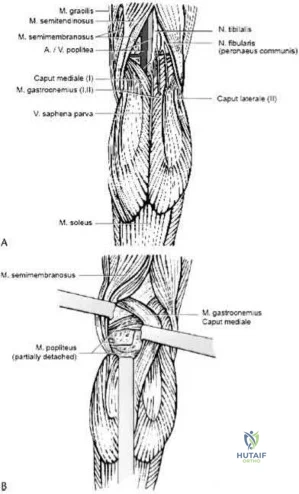
A 36-year-old male falls from a 10-ft scaffold and suffers the injuries shown in Figures A and B. The patient is placed in a spanning external fixator and brought back to the operating room once his soft tissues are amenable. Planning to use a dual-incision approach, what is the correct interval to use when approaching the medial side?
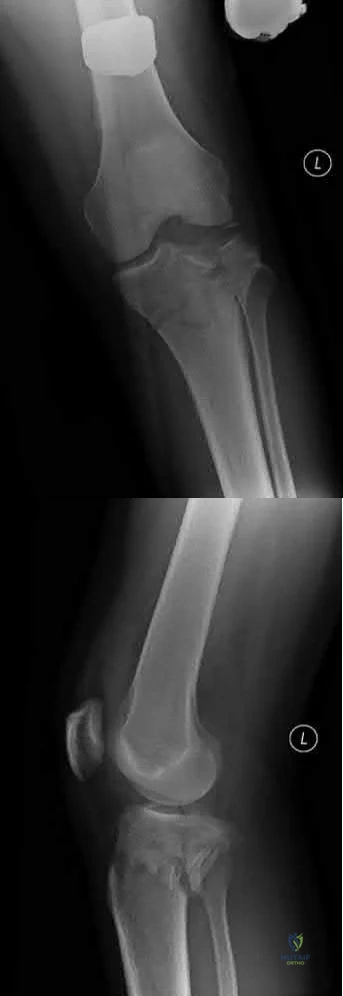
Popliteus and pes anserine
Lateral head of the gastrocnemius and pes anserine
Politeus and lateral head of the gastrocnemius
Iliotibial band and medial head of the gastrocnemius
Pes anserine and medial head of the gastrocnemius Corrent answer: 5
The posteromedial approach to the tibial plateau is between the the pes anserine tendons and the medial head of the gastrocnemius.
A dual-incision approach is often utilized to optimally place definitive fixation for bicondylar tibial plateau fractures. For fractures that require posterior or posteromedial fixation, the correct interval is between the pes anserine and the medial head of the gastrocnemius.
Higgins et al. in a large cohort morphological review, noted a high incidence of a posteromedial fragment in bicondylar fractures. Occurring at a high frequency, the authors recommended direct visualization and reduction via a dual approach rather than using indirect reduction techniques.
Falker et al. describes a step-by-step approach to utilizing the posteromedial approach for the tibial plateau and placing an anti-glide plate.
Figure A and B exhibit a bicondylar tibial plateau fracture with a posteromedial fragment noted on the lateral x-ray. Illustration A exhibits the surrounding anatomy and interval in between the medial head of the gastrocnemius and the pes anserine.
Incorrect answers:
OrthoCash 2020
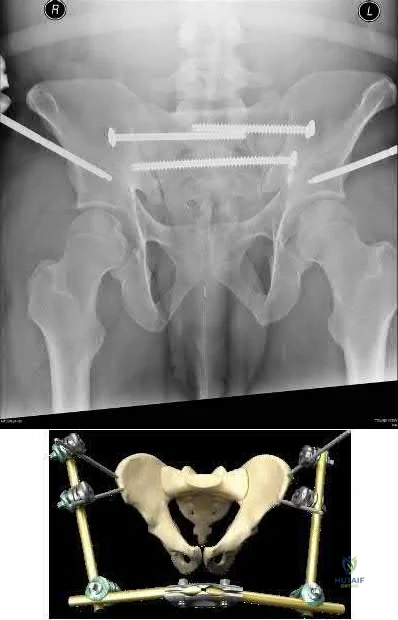
A 25-year-old male presents to the emergency department with the injury seen in Figure A after a motorcycle collision. The patient has a blood pressure of 70 systolic, elevated lactate and a tense abdomen with positive FAST examination. Trauma surgery will be performing an emergent laparotomy. Orthopaedic surgery is consulted and places a pelvic external fixator intraoperatvely to assist with resuscitation. What is an advantage of supra-acetabular external fixator pins as compared with iliac crest pins?

Less interference with pelvic surgical incisions
Less risk of pin tract infection
Less risk of malreduction
Less control of posterior pelvic ring
No interference with laparotomy Corrent answer: 1
One advantage of supra-acetabular external fixator pins is that they do not interfere or contaminate future approaches to the pelvis or acetabulum involving the lateral window.
In multiply injured patients with pelvic trauma external fixation of the pelvic ring is a valuable tool to assist with resuscitation. Pelvic external fixation should be applied rapidly and allow full access to the abdomen for general surgery intervention. Regardless of the technique used, a pelvic external fixator should form a stable construct that minimizes motion of fracture surfaces and allows for clot formation.
Haidukewych et al evaluated the safety of supra-acetabular pin placement in a cadaveric study. The authors found that the lateral femoral cutaneous nerve (LFCN) was most at risk during pin placement.
Figure A demonstrates a widely displaced symphyseal dislocation with associated bilateral sacroiliac (SI) dislocations (APC 3). Illustration A demonstrates an outlet radiograph of a supra-acetabular external fixtator in conjunction with posterior pelvic ring fixation for an LC3 pelvic ring injury.
Illustration B is an illustration of iliac crest external fixation. The video demonstrates techniques for application of both supra-acetabular and iliac
crest external fixation pins.
Incorrect Answers:
OrthoCash 2020
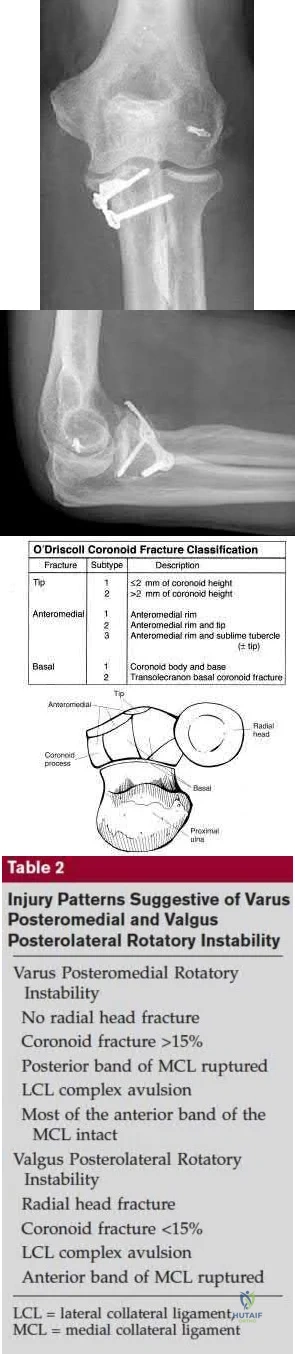
What physical exam finding is most likely to be found in association with the injury shown in Figures A and B?

Numbness in the small finger and ulnar side of the ring finger
No elbow instability
Varus posteromedial rotatory instability
Valgus posterolateral rotatory instability
An anterior open wound Corrent answer: 3
The x-ray shows a fracture of the anteromedial facet of the coronoid with an intact radial head. Large anteromedial facet fractures are associated with varus posteromedial rotatory instability.
The anteromedial facet of the coronoid provides support to the medial elbow against varus stress. Varus and posteromedial force applied to the elbow results in disruption of the lateral collateral ligament (LCL) from its proximal origin. The coronoid is fractured as it is forced against the medial trochlea.
Coronoid fractures of significant size involving the sublime tubercle (insertion of medial collateral ligament) result in varus instability.
Steinmann reviews the anatomy, diagnosis, classification and treatment of coronoid fractures with a focus on surgical exposures and fixation techniques. He states that when a coronoid fracture is associated with a pattern of varus instability, it requires fixation with either suture, buttress plating or screw fixation. Concomitant LCL repair or reconstruction will also be necessary.
Doornberg et al. reviewed 67 coronoid fractures to determine whether type of coronoid fracture correlated with pattern of instability. They found strong
associations between (1) large coronoid fractures and trans-olecranon fracture-dislocations, (2) small fractures and terrible-triad injuries, and (3) anteromedial facet fractures and varus posteromedial rotational injury mechanisms.
Doornberg et al. evaluated 18 patients with a fracture of the anteromedial facet of the coronoid. They found that malalignment of the anteromedial facet fragment was associated with arthrosis and a fair or poor result.
Figure A is an AP view of an elbow with an anteromedial facet of the coronoid fractured. The lateral joint space is widened due to injury to the LCL. The medial joint space is narrowed and collapsed. A lateral view is shown in Figure
B. Illustrations A and B show AP and lateral views of a coronoid fracture fixed with buttress plating. The LCL origin was fixed with a suture anchor. Illustration C shows the O'Driscoll classification of coronoid fractures. Illustration D lists injury patterns that suggest posteromedial versus posterolateral rotatory instability.
Incorrect Answers:
OrthoCash 2020
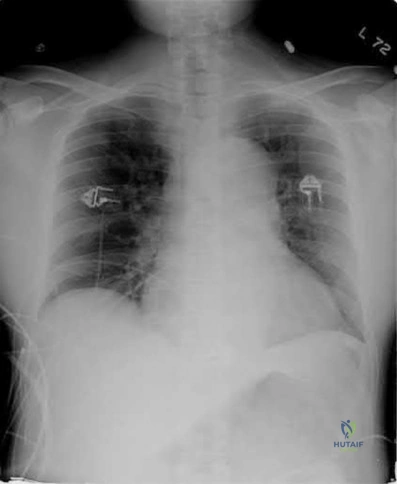
A 35-year-old man presents to the ED as the restrained driver of a high speed motor vehicle collision complaining of hip, chest, and abdominal pain. He becomes diaphoretic, tachycardic, and hypotensive in the trauma bay and is noted to have diminished lower extremity pulses. He is found on ATLS workup to have mediastinal widening.
Which of the following injuries is most associated with thoracic aortic injury?

Thoracic aortic rupture is associated with posterior hip dislocation in deceleration trauma mechanism of injuries.
Posterior hip dislocations are infrequently associated with local vascular injuries. With bilateral perfusion deficits, more proximal large vessel trauma should be considered, and in this situation, thoracic surgery should be involved emergently. Screening chest x-ray in the trauma bay should be reviewed for widened mediastinum, suggestive of aortic injury, as shown in illustration A. Given the high energy mechanism associated with these injuries, a full ATLS trauma survey must be done for every patient.
Marymont et al. studies the association between posterior hip dislocation and thoracic aortic injury. They performed a retrospective chart review of 89 posterior hip dislocations and found 8% had an aortic injury. Although not statistically significant, they note the importance of evaluation for aortic injury in patients with posterior hip dislocations given its emergent life-threatening nature.
In addition to associated chest injuries, Schmidt et al. highlight the importance of evaluating the ipsilateral knee after high-energy traumatic hip dislocation. In a prospective study, they identified a 93% rate of ipsilateral knee injury on MRI including effusion (37%), bone bruising (33%), and meniscal tear (30%) as the most common. They recommend a thorough exam but also expanded use of knee MRI after hip dislocation.
Illustration A shows an example of chest x-ray with a widened mediastinum, suggestive of thoracic aortic injury.
OrthoCash 2020
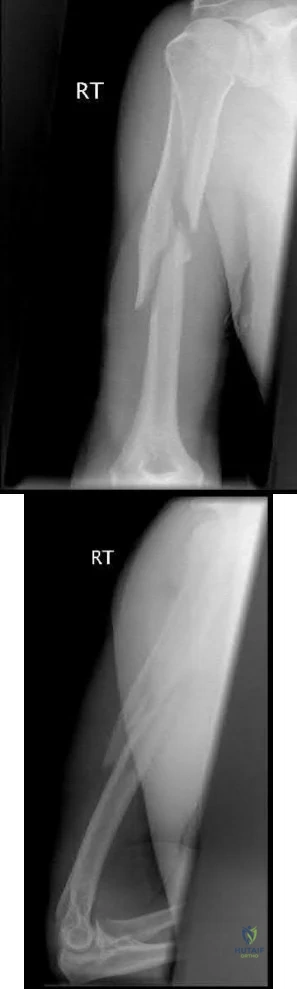
A 31-year-old female smoker was involved in a skiing accident approximately 9 months ago and underwent open reduction internal fixation of the radius and ulna at the time of injury. She now returns to the clinic complaining of increasing pain with range of motion and activity. Radiographs from her most recent follow-up can be seen in Figure A. Laboratory tests show ESR, CRP and WBC count to be within normal limits. Which of the following options is the most appropriate next step in management?

Bone scan
Above elbow cast
Removable splint
Reamed intramedullary nail
Iliac crest bone grafting + compression plating Corrent answer: 5
This patient is presenting with an atrophic non-union of the ulna after open reduction internal fixation for a both bone forearm fracture 9 months ago. The most appropriate next step in management would be iliac crest bone grafting and compression plating of the ulna.
The primary issue with an atrophic nonunion is biological. The blood supply is poor and therefore incapable of purposeful fracture healing. Smokers, as in this vignette, are at high risk for nonunion. The treatment of an atrophic nonunion involves improving biology at the fracture site through use of autologous bone graft (e.g. iliac crest) and providing mechanical stability by means of compression plating (e.g. 3.5 mm LC-DCP).
dos Reis et al. reports excellent results of 31 cases of diaphyseal forearm fracture non-unions treated with autologous bone grafting and compression
plating. Thirty of thirty-one patients went on to bony union within 3.5 months of revision surgery.
Nadkarni et al. presented a case series of 11 patients with non-unions of various long bones initially managed with intradmedullary (IM) nail fixation. The authors successfully used locking compression plates while retaining the IM nails in the treatment of the nonunion in all cases.
Figure A shows an AP radiograph of a both bone forearm fracture. Figure B shows an AP and lateral radiograph of an atrophic non-union of the ulnar shaft. Illustration A shows a lateral x-ray of a fully healed radius and ulna after hardware removal 1 year after revision surgery.
Incorrect Answers:

OrthoCash 2020
A 27 year-old patient sustains a fracture-dislocation of the acetabulum. Pelvic radiographs (Figures A and B) are taken at initial presentation and a CT scan (Figures C and D) is performed after reduction of the hip in the emergency room. What is the importance of the finding highlighted in the CT scan cuts?

Comminution indicates a better result with non-operative management
Significant marginal impaction could compromise the results of the surgical reduction if the joint surface is not properly restored
The impacted fracture segment will heal without fixation because it is not gapped or translated
The CT scan finding highlighted indicates osteochondral defects to the femoral head, which can be addressed arthroscopically
Intraarticular fracture fragments should be discarded from the surgical field, as incorporation of the fragments into the fixation construct leads to a high rate of avascular necrosis
The CT images shown in Figures C and D display significant marginal impaction of the joint surface.
Marginal impaction is common in posterior wall fractures and fracture-dislocations. Critical review of CT imaging of posterior wall fractures can help with preoperative planning for identifying impaction of the articular surface of the acetabulum. Restoration of the sphericity of the acetabulum to match that of the femoral head is important for successful outcome following ORIF of posterior wall fractures. A common surgical technique to accomplish joint surface restoration includes freeing the impacted articular segments, bone grafting of the void created to support the articular segments, and buttress plating of the posterior wall fracture fragments.
Patel et al. discuss the challenge of interpreting imaging of the acetabulum for assessing fracture characteristics that may significantly impact success or surgical intervention. These characteristics include: articular displacement, marginal impaction, incongruity of the joint surface, intra-articular fragments, and osteochondral injury to the femoral head. Based on expert review of images, determination of significant marginal impaction had a poor intraobserver reliability, as did each of the other modifiers listed.
Figures A and B are radiographs of the posterior wall fracture and hip dislocation. They do not show the large amount of marginal impaction of the acetabular surface. Figure C (coronal reconstruction) and Figure D (sagittal reconstruction) point out a large a amount of marginal impaction of the acetabular. Note the disruption of the joint surface on the intact portion of the acetabulum.
Incorrect answers:
Comminuted posterior wall fractures still should be surgically stabilized if the joint is unstable
This impacted fragment on the margin of the main fracture line will likely heal regardless of restoration of the articular surface; however, this malreduction will lead to a incongruent joint surface
These CT cuts do not show any osteochondral defects of the femoral head; however if found in other CT cuts or intraoperatively, they should be appropriately addressed
Intraarticular fracture fragments should be removed from the joint, but if they make up a substantial portion of the joint surface, they should be incorporated in the fixation construct to obtain the goal of anatomic reduction of the joint surface
OrthoCash 2020
A 32-year-old female is involved in a motor vehicle collision and suffers a right hip dislocation. She is in the twelfth week of pregnancy.
Evaluation in the emergency department reveals no other injuries and ultrasound reveals a strong fetal heart rate and no abnormalities. She undergoes emergent closed reduction but the hip remains unstable and a traction pin is placed. Post-reduction films are shown in Figure
What is the most appropriate next step in management?

Acute open reduction internal fixation
Exam under anesthesia
Skeletal traction for 6-8 weeks
Fetal monitoring until 15 weeks followed by open reduction internal fixation
Percutaneous pinning
This patient has a large posterior wall fracture of the right acetabulum with an unstable hip. The most appropriate next step in treatment is open reduction and internal fixation.
Fixation of acetabular fractures during pregnancy is not contraindicated in the setting of stable fetal heart rate and no abnormalities on pelvic ultrasound.
There is, however, an increased risk of complications for the mother and fetus. Injury severity and mechanism are most closely associated with increased rate of fetal complications. The trimester of pregnancy is not associated with increased risk of complications.
Leggon et al. reviewed 101 cases of pelvic and acetabular fractures in pregnant patients and found mechanism of injury and injury severity were associated with higher mortality for both mother and fetus. Trimester of pregnancy was not associated with increased mortality.
Flik et al. reviewed orthopaedic trauma in a pregnant patients and recommended fetal ultrasound for assessment of fetal well-being in all pregnant patients.
Desai et al. investigated orthopaedic trauma during pregnancy and reported minimal radiation risk to the fetus when obtaining x-rays. They also advocate for LMWH as one of the safest choices for anticoagulation.
Figure A is an x-ray showing a right posterior wall acetabular fracture. Figures B and C are Judet views of the pelvis focusing on the right hip. A large posterior wall fragment is visible in Figure B.
Incorrect Answers:
OrthoCash 2020
Figure A is radiograph of a 50-year-old male science teacher that was involved in a motor vehicle accident. He underwent closed reduction as seen in Figure B and C. What would be the most appropriate treatment?
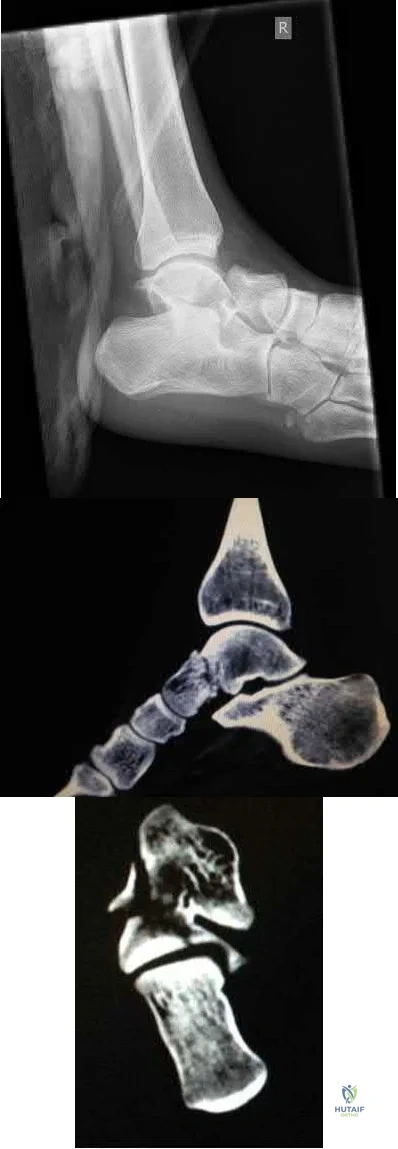
Open reduction and internal fixation with medial bridge plate and lateral screw in non-lagging mode
Tibiotalocalcaneal arthrodesis
Open reduction and internal fixation with lateral and medial screw in lagging mode
Closed reduction and internal fixation with medial and lateral screw in non-lagging mode
Closed reduction with percutaneous pins Corrent answer: 1
This patient is presenting with a Hawkins II talar neck fracture with medial wall comminution. The most appropriate treatment of this patient would be open reduction internal fixation with medial plate and lateral screw in non-lagging mode.
The treatment of talar fractures is based on the severity of the fracture, soft-tissues, and patient factors. The fracture and subluxation of the subtalar joint should be reduced and stable anatomical fixation should be obtained. When there is comminution of either the superior, lateral or medial aspects of the talus, one should avoid shortening the medial wall as this will cause a varus malunion. The use of a medial or lateral plate can help to re-establish column length, which can often prevent this potential complication.
Sanders et al. showed significant complications after fixation of talar neck fractures. They showed the incidence of secondary reconstructive procedures following talar neck fractures increased from 24% +/- 5% at 1 year to 48%
+/- 10% at 10 years post-injury.
Vallier et al. retrospectively reviewed the records of 39 fractures of the talar neck treated with open reduction and internal fixation. Twenty-one (54%) of thirty-nine patients had development of posttraumatic arthritis, which was more common after comminuted fractures (p < 0.07) and open fractures (p = 0.09).
Vallier et al. reviewed 81 talar neck fractures to revisit the rate of osteonecrosis and post-traumatic arthritis based on the Hawkins Classification. They found that delaying definitive internal fixation does not increase the risk of developing osteonecrosis. Thirty-five patients (54%) developed posttraumatic arthritis, including 83% of those with an associated talar body fracture (p < 0.0001) and 59% of those with Hawkins type-III injuries (p < 0.01).
Figure A shows a Hawkins II talar neck fracture. Figures B and C are saggital and coronal CT images, respectively, of the foot. There is significant comminution of the medial wall of the talus with extension into the subtalar joint.
Incorrect Answers:
There is some research to suggest primarily subtalar arthrodesis with these injuries. However, to date, there is no high level evidence that has conclusively shown subtalar arthrodesis to be better than ORIF.
OrthoCash 2020
A 28-year-old male college student sustains a severe foot injury from gunshot-related violence, and subsequently undergoes a lower-extremity amputation as shown in Figure A. At long-term follow-up, which of the following is the strongest predictor of patient satisfaction as related to his injury?

Age less than 30
Marijuana use
Use of negative pressure wound therapy
Male gender
Ability to return to work Corrent answer: 5
The strongest factor to predict patient-reported outcomes after trauma-related lower extremity amputations is the patient's ability to return to work. This is likely due to the effect of the return to work on the physical, emotional, and financial aspects of the patient's life.
The LEAP study is a multicenter, prospective study evaluating multiple aspects of reconstruction versus amputation in the treatment of mangled extremity injuries. With regard to patient satisfaction, treatment variables such as decision for reconstruction versus amputation, or initial presence or absence of plantar sensation have little impact. In addition, demographic factors such as age, gender, socioeconomic status, and education level do not predict patient satisfaction. Instead, the most important predictors of patient satisfaction at 2 years after injury include the ability to return to work, absence of depression, faster walking speed, and decreased pain.
O'Toole et al reviewed 463 patients treated for limb-threatening lower-extremity injuries and identified factors associated with patient reported outcomes two years after surgery. They found that return to work was the most associated with outcomes, but that physical functioning, walking speed, pain levels, and presence of depression were also associated to a lesser extent with outcomes.
Bosse et al performed a multicenter, prospective study to assess outcomes of 569 patients with severe lower extremity limb injuries that resulted in either amputation or limb salvage procedures. They found that at two years postoperatively, no significant differences were seen between groups in patient-reported outcome. Worse outcomes were associated with rehospitalization for a major complication, a low educational level, nonwhite race, poverty, lack of private health insurance, poor social-support network, low self-efficacy (the patient's confidence in being able to resume life activities), and involvement in disability-compensation litigation.
Figure A shows a clinical photograph of a Pirigoff amputation at early follow-up. This amputation is an end-bearing amputation that utilizes the plantar heel pad for weightbearing, and relies on a tibiocalcaneal arthrodesis.
Incorrect Answers:
4: These options are not as strong of a factor of patient satisfaction in longterm follow up after trauma-induced lower extremity amputation.
OrthoCash 2020
A 34 year-old male falls off of motorcycle on an outstretched hand suffering the injuries shown in Figures A and B. He is brought to the operating room and undergoes radial head replacement and fixation and repair of the coronoid and the lateral collateral ligament (LCL). Prior to closing, the elbow is still unstable upon testing range of motion. What is the next best step in management?

Exchange radial head for larger implant
Complete resection of radial head
Cast at 90 degrees of flexion for 6-8 weeks
Reinforce LCL repair with non-absorbable suture
Repair the ulnar collateral ligament Corrent answer: 5
Following complete fixation and repair of a terrible triad, a final range of motion test should be performed prior to closure. If still unstable, the next step should be to assess and repair the ulnar collateral ligament. Another option
would be to placed a hinged external fixator.
Operative reconstruction of a terrible triad injury should be performed in a systematic fashion, working from deep to superficial. Working through a lateral incision and through the radial head fracture, the coronoid should be fixed first, followed by radial head fixation or replacement and then repair/reconstruction of the LCL. If still unstable, the medial side should be addressed, or the patient placed in a hinged external fixator.
Mathew et al review the anatomic, biomechanic, and operative principles (why the above step-by-step method works) to achieving appropriate stability in order to obtain early range of motion to maximize clinical outcome.
Pugh et al. in this retrospective, multi-center study report outcomes on 36 terrible triad injuries fixed with the standard protocol described above. The authors recommend following this systematic approach to achieve the best results.
Figures A and B are AP and lateral radiographs exhibiting a terrible triad elbow fracture-dislocation.
Incorrect answers:
OrthoCash 2020
When treating the pathology depicted in Figures A through D, which of the following is necessary to preserve the blood supply to the femoral head?

Dissection of the gluteal musculature off the iliac crest
Ligation of the ascending branches of the lateral femoral circumflex artery
Greater trochanteric osteotomy
Identification and detachment of the piriformis tendon
Supine positioning
Figures A-D show a femoral head with associated acetabular fracture (Pipkin IV). Both the posterior wall fracture and the femoral head fracture can be addressed through a surgical dislocation via greater trochanteric osteotomy.
Pipkin IV femoral head fracture (with associated acetabular fractures) are somewhat problematic in that the femoral head fracture is usually anterior, while the acetabular fracture usually involves the posterior wall. A Kocher-Langenbeck approach gives good access to the posterior wall but limited access to the articular surface and femoral head avascular necrosis (AVN) is a concern. A Smith-Peterson approach provides good access to the femoral head
but not to the posterior wall. Combined approaches significantly increase the amount of surgical dissection. Surgical dislocation with trochanteric flip osteotomy provides access to the femoral head and posterior wall while preserving blood supply to the femoral head.
Solberg et al. retrospectively reviewed 12 patients with Pipkin IV injuries treated via a trochanteric flip osteotomy. All patients healed their acetabular fractures. Eleven of 12 patients healed their femoral head fractures and one patient (8.3%) developed osteonecrosis.
Henle et al. likewise treated 12 patients with Pipkin IV injuries through a trochanteric flip osteotomy. Two of 12 patients (16.7%) developed osteonecrosis. The remaining 10 patients (83.3%) had good or excellent results. Heterotopic ossification occurred in five patients, causing significant range of motion loss in four of these.
Figure A is a pre-reduction AP pelvis in which the posterior wall fracture is apparent. Figure B is a post-reduction AP pelvis in which an infra-foveal femoral head fracture is apparent (Pipkin IV). Figure C is an axial CT cut which further characterizes the posterior wall fracture. Figure D is an obturator oblique showing femoral head dislocation and posterior wall fracture. The video shows a surgical hip dislocation technique.
Incorrect Answers:
OrthoCash 2020
A 42-year-old male presents to your clinic for the first time with the radiographs seen in Figure A. He sustained the injury 4 weeks ago while skiing overseas and treatment was provided by the local orthopaedic surgeon. The operative note states that he sustained an Gustilo Type I open fracture. After surgical fixation of this type of injury, what is the most common complication requiring reoperation?

Chronic elbow instability
Post-traumatic arthritis
Infection
Heterotopic ossification
Loss of elbow range of motion Corrent answer: 5
This patient sustained a terrible triad elbow fracture-dislocation. Reduced range of motion of the elbow joint is the most common complication REQUIRING reoperation with these injuries.
Terrible triad elbow fracture-dislocations are characterized by posterolateral dislocation/lateral collateral ligament (LCL) injury, radial head fracture and coronoid fracture. Displaced fractures result in elbow instability. Acute radial head stabilization, coronoid open reduction and internal fixation, and LCL +/-medial collateral ligament (MCL) repair/reconstruction is considered the most appropriate treatment for displaced fractures. Operative complications include elbow stiffness, recurrent instability, arthritis, failure of hardware, heterotopic ossification, posterior interosseous nerve palsy and infection.
Egol et al. looked at the functional outcomes of 27 patients that underwent fixation of terrible triad injuries. At one year follow-up, the average flexion-extension arc of elbow motion was 109 degrees +/- 27 degrees, and the average pronation-supination arc was 128 degrees +/- 44 degrees. Grip strength averaged 72% of the contralateral extremity. Although operative fixation led to functional elbow stability, results were poor.
They included a reference to McKee et al. to highlight that intra-articular fractures of the elbow have high rates of stiffness. While not specific to terrible
triads, they looked at the effectiveness of the posterior elbow approach in 25 patients that underwent internal fixation of intra-articular distal humerus fractures. They showed poor outcomes at a mean follow-up of 36 months with reduced range-of-motion, decreased strength and high re-operation rates.
Figure A shows AP fluoroscopic image of a terrible triad injury that has undergone operative fixation. The radial head and coronoid have undergone open reduction internal fixation, and the MCL bony avulsion has been repaired.
Incorrect Answers:
OrthoCash 2020
Figure A is a radiograph from a 59-year-old male that was transferred to a Level I trauma center five hours after a motor vehicle accident. Closed reduction and skeletal traction was successfully performed in the trauma bay. Which of the following factors has been shown to increase the risk of unsatisfactory clinical outcome for this patient?

Need for skeletal traction
Mechanism of injury
Gender
Age
Time to reduction Corrent answer: 4
Age greater than 55-years-old has been found to be an independent risk factor for inferior clinical outcome in patients with combined acetabular fractures and hip dislocations.
The most important initial step in management following resuscitation involves urgent reduction of the dislocated hip. This should be followed by a preoperative CT scan and ultimately surgical fixation of the combined acetabular fracture. Hip dislocations should be reduced within 6-12 hours for optimal outcome, although different critical times have been cited, particularly for dislocations with concomitant acetabular fractures. Skeletal traction may be required to maintain hip reduction.
Moed et. al. present a Level 3 retrospective review of 100 patients who had been treated with open reduction internal fixation of an acetabular fracture. The authors found that factors associated with unsatisfactory clinical outcomes included age greater than 55, intra-articular comminution, osteonecrosis, and delay of greater than 12 hours for reduction of an associated hip dislocation.
Additionally, they showed that there was a strong association of clinical outcome and final radiographic grade.
Figure A demonstrates an acetabular fracture with concomitant hip dislocation. Incorrect Answers:
injury, male gender, and time to reduction <6 hours have not been shown to be related to unsatisfactory outcomes.
OrthoCash 2020
A 37-year-old male cashier is shot in the leg. He sustains the injury shown in Figures A and B, and is subsequently taken to the operating room for intramedullary nailing. Figure C shows a radiograph of the nail starting point (*). What complication is most likely to result?

Varus malunion
Nonunion
Valgus malunion
Malrotation
Superficial peroneal nerve injury Corrent answer: 3
This patient is presenting with a comminuted fracture of the proximal third of the tibia. He is appropriately undergoing intramedullary nail fixation, however, the start point illustrated in Figure C is too medial and often leads to a valgus malunion.
Intramedullary nail fixation is more technically demanding in proximal tibial fractures than diaphyseal fractures. The valgus deformity is due to imbalanced muscle forces on the proximal fragment, which are then accentuated by a start point that is too medial. An apex anterior (procurvatum) deformity can also occur and results from the pull of the patellar tendon or a posteriorly directed nail that deflects off the posterior tibial cortex and rotates the proximal fragment. The ideal starting point for proximal tibial fractures is slightly lateral to the medial aspect of the lateral tibial spine on a true AP x-ray and very proximal and just anterior to the anterior margin of the articular surface.
Nork et al. reported the results of intramedullary nailing of proximal tibial fractures with emphasis on techniques of reduction. Various techniques were found to be successful including attention to the proper starting point, the use of unicortical plates, and the use of a femoral distractor applied to the tibia.
Lowe et al. describe surgical techniques for complex proximal tibial fractures. They describe the extended leg position, use of a femoral distractor, temporary plate fixation, blocking (Poller) screws, and use of percutaneous clamps as means to achieve reduction during fixation.
Figure A and B show an AP and lateral radiograph of a comminuted extra-articular fracture through the proximal third of the tibia. Figure C demonstrates a start point that is too medial (represented by the asterisk) for intramedullary nail fixation. Illustration A and B show the ideal start point for intramedullary nail fixation of the tibia on AP and lateral radiographs.
Incorrect Answers:
Varus malunion is more likely to occur in midshaft tibia fractures with an intact fibula.
Nonunion after a proximal tibial fracture treated with intramedullary nailing is less common than malunion.
Malrotation occurs most commonly after IM nailing of fractures through the distal third of the tibia.
The superficial peroneal nerve is at risk during distal screw fixation using a LISS plating technique for fracture fixation.

OrthoCash 2020
A 24-year-old motorcyclist is brought in as a polytrauma after striking a tree at 65 mph. He is found to have injuries involving the chest, abdomen, pelvis, as well as a left open femoral shaft fracture. He undergoes resuscitation in the trauma bay. Which of the following parameters best supports proceeding with irrigation, debridement and external fixation as opposed to immediate reamed intramedullary nailing?
Temperature = 35.5°C (95.9°F)
Fractures of ribs 2-3 with left apical pneumothorax
Grade IV liver laceration with SBP = 85 mmHg
Left superior and inferior pubic ramus fractures
Lactate = 2.3 mg/dL
Significant abdominal trauma with evidence of hemorrhagic shock (SBP < 90 mmHg) following resuscitation is an unstable parameter and therefore is an indication to proceed with damage control orthopaedics (irrigation and debridement of open fractures and temporizing external fixation) in a polytraumatized patient.
The management of orthopaedic injuries in a polytrauma patient depends on the physiological stability of the patient. In an unstable patient, damage control orthopaedics (DCO) is preferred over early total care (ETC) to avoid an iatrogenic second hit with development of adult respiratory distress syndrome (ARDS) and/or multiple organ failure. Clinical parameters indicative of instability include shock (BP < 90 mmHg, refractory to blood products, lactate
> 2.5 mg/dL), coagulopathy (platelet count < 90,000 mm3, fibrinogen < 1 g/L), hypothermia (< 35°C), and significant chest, abdomen or pelvis injuries (pulmonary contusions, severe liver/spleen lacerations, pelvic ring disruption).
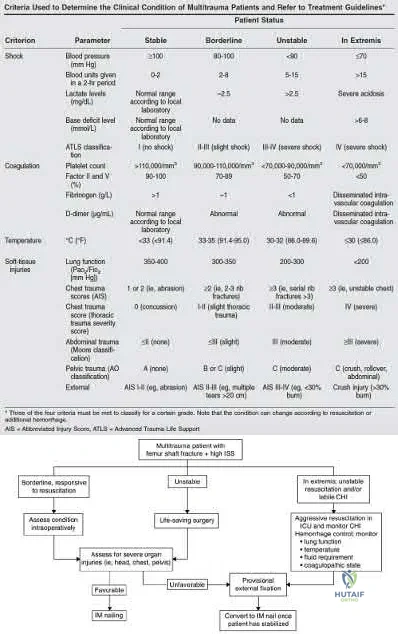
Pape et al. (2009) authored a review article detailing the management of a multitrauma patient. Polytrauma patients can be classified as stable, borderline, unstable or in extremis using a variety of criteria pertaining to hemodynamic stability, coagulation, temperature and soft tissue injury.
Patients who are stable or borderline can undergo ETC, while patients who are unstable or in extremis should be managed with DCO.
Pape et al. (2008) concluded that all patients who underwent early femoral nailing demonstrated increased systemic inflammatory response compared to external fixation, regardless of clinical stability. However, unstable patients
with a preexisting elevation of inflammatory status are likely more impacted by this additional increase. Improved postoperative clinical status coincided with a less vigorous inflammatory response.
Illustration A is a table from Pape et al (2009) depicting the criteria used to determine clinical condition of a polytraumatized patient. Illustration B is an algorithm from Pape et al (2009) detailing management of the multitrauma patient.
Incorrect Responses:
OrthoCash 2020
A 92-year-old female sustains the injury shown in Figure A to her nondominant extremity as the result of a non-syncopal ground-level fall. She denies any previous injury or pain of the elbow, and her medical history is significant only for osteoporosis and hypothyroidism. What is the most appropriate treatment for her injury?

Immediate range of motion as tolerated with a sling for comfort
Long arm cast for 3 weeks, then physical therapy for motion
Open reduction and internal fixation
Radiocapitellar arthroplasty
Total elbow arthroplasty Corrent answer: 5
Use of total elbow arthroplasty (TEA) in the elderly is a well-recognized method of treatment of complex distal humerus fractures. This procedure allows for improved ROM, improved patient-reported outcomes, and decreased revision rates as compared to fixation.
TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation. Elderly patients appear to accommodate to objective limitations in function with time, which is important, as most recommendations list restrictions of lifting no more than 5-10 pounds postoperatively.
McKee et al conducted a prospective, randomized, controlled trial to compare functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with open reduction-internal fixation (ORIF) or primary semiconstrained total elbow arthroplasty (TEA). Patients who underwent TEA had a quicker procedure, improved DASH scores at 6 months, improved elbow ROM, and decreased revision rates.
Athwal et al review TEA and the options available at the time of publication. They also report on the techniques and purported advantages of arthroplasty as compared to fixation of complex distal humerus fractures.
Frankle et al reviewed patients >65 years old with distal humerus fractures at a minimum of 2 years follow-up. Outcomes were excellent in 33% of cases undergoing ORIF and 92% excellent with TEA. They recommend TEA in instances of arthritis, osteoporosis, or other diagnoses requiring steroids.
Figure A shows a significantly comminuted distal humerus fracture in an osteoporotic patient. Illustration A shows the same patient after undergoing total elbow arthroplasty.
Incorrect Answers:
1:Immediate range of motion is not recommended for this injury, even with the "bag of bones" treatment method. A brief period of immobilization is generally recommended for this technique.
2: Casting is not indicated for this injury.
3: ORIF of this injury will lead to worse outcomes as compared to arthroplasty. 4: Isolated radiocapitellar replacement is not indicated for this injury.

OrthoCash 2020
A 56-year-old right hand dominant attorney falls from standing and sustains the closed injury shown in Figure A. The treating surgeon elects to fix her fracture using a plate and screw construct. Based on
the available imaging, which of the following fracture characteristics best justifies this fixation choice?

Fracture displacement
Intra-articular fracture extension
The fracture extends distal to the coronoid
Oblique fracture line
Fracture comminution
This patient has a displaced, intra-articular, comminuted olecranon fracture. Comminution is an indication for plate fixation.
Most displaced olecranon fractures are treated operatively. Options include tension band constructs, intramedullary screws, plate and screw fixation or fragment excision with triceps advancement. Any construct relying on interfragmentary compression (tension band, intramedullary screws) requires a non-comminuted fracture pattern. Plate fixation is indicated in the setting of comminution, extension past the coronoid, or in the setting of associated instability.
Bailey et al. retrospectively reviewed 25 patients who underwent plate fixation of displaced olecranon fractures. Twenty-two of 25 patients had good or excellent outcomes. Five of 25 patients (20%) of patients required plate removal for symptomatic hardware. The authors concluded that plate fixation
was an effective treatment for displaced olecranon fractures, with good functional outcomes.
Figure A shows a displaced, comminuted olecranon fracture without evidence of propagation past the coronoid.
Incorrect answers:
OrthoCash 2020
A 35-year-old male was involved in a high speed motorcycle accident. He has a closed head injury, bilateral pulmonary contusions and splenic rupture. His orthopaedic injuries are shown in Figure A. He has a blood pressure of 90/50 mm Hg and a heart rate of 115, despite aggressive resuscitation. An arterial blood gas reveals that his blood lactate is 3.5 and base deficit is -6 mmol/L. Following successful closed reduction of the right hip in the operating room with a percutaneous inserted Schantz pin, what is the next most appropriate treatment for his orthopaedic injuries?

Bilateral open reduction and internal fixation
Open reduction internal fixation on the right, reamed intramedullary nailing on the left
Temporizing external fixation on the right, open reduction and internal fixation on the left
Bilateral reamed intramedullary nailing
Bilateral temporizing external fixation Corrent answer: 5
This patient presents with features of hemodynamic instability and a high injury severity score. The next most appropriate treatment would be temporizing external fixation bilaterally. This patient meets the criteria for damage control orthopaedics.
Damage control orthopaedics is an approach that contains and stabilizes orthopaedic injuries so that the patient's overall physiology does not undergo further inflammatory insult. As a result, external fixation of femoral shaft fracture and pelvic stabilization is an effective treatment under this strategy. Other indications include vascular injury and severe open fracture.
Pallister et al. reviewed the effects of surgical fracture fixation on the systemic inflammatory response to major trauma. They show that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure. However, early fracture surgery increases the post-traumatic inflammatory response, which
carries a higher complication rate compared to temporary fixation.
Tisherman et al. created clinical guidelines for the endpoints of resuscitation. Level I data found that standard hemodynamic parameters do not adequately quantify the degree of physiologic derangement in trauma patients. The initial base deficit, lactate level, or gastric pH should be used to stratify patients with regard to the need for ongoing fluid resuscitation.
Pape et al. retrospectively reviewed the impact of early total care vs. damage control orthopaedics in the treatment of femoral shaft fractures in polytrauma patients. They found a significantly higher incidence of acute respiratory distress syndrome (ARDS) with intramedullary nailing (15.1%) compared to external fixation (9.1%) when DCO subgroups were compared.
Figure A is a pelvic AP radiograph showing a right hip fracture-dislocation with an ipsilateral femoral shaft fracture. On the left side there is a displaced pertrochanteric hip fracture.
Incorrect Answers:
OrthoCash 2020
Which of the following has been shown to be the greatest risk factor for refracture after implant removal from a radial shaft?
Removal of locking screws
Removal of small fragment plates
Removal of metaphyseal implants
Removal of implants less than 1 year after insertion
Removal of protective splinting from limb earlier than 10 weeks postoperatively
Removal of implants earlier than 1 year after insertion is a risk factor for refracture of the bone after implant removal.
The risk of refracture after hardware removal is multifactorial. Multiple
variables have been studied such as protective splinting for 6 weeks after hardware removal, waiting 12 months or more prior to hardware removal, and the location of the fracture. The variable that seems to correlate most with the risk of refracture is a diaphyseal location of the initial fracture. Large fragment plates (4.5 mm), when removed, are also at higher risk for refracture in the forearm.
Deluca et. al reported on a case series of patients who sustained a refracture of a forearm after implant removal. They noted that radiolucency at the site of the original fracture was seen in most refractured patients when the plate was removed. They also recommend delaying implant removal to two years after insertion to minimize risk.
Rumball et. al reported that the incidence of refracture after forearm implant removal is 6% in their series. They found that early removal, lack of postoperative immobilization, and plate size are the most critical risk factors for refracture.
Illustration A shows a forearm with evidence of refracture after implant removal.
Incorrect Answers:

OrthoCash 2020
A 23-year-old male arrives to the trauma bay after a motorcycle crash caused by a drive-by shooting. The patient is awake and alert and following commands. Vital signs include a blood pressure of 145/90 and a heart rate of 117bpm. Initial lactate is reported as 2.4 mmol/L. The patient has 2 rib fractures on the right with a clear chest radiograph. The patient is neurovascularly intact with a 4cm transverse wound over the medial ankle. Figures A, B and C exhibit his orthopaedic injuries. What is the most appropriate management?

Irrigation, debridement and placement external fixator right ankle, external fixation femur and intramedullary fixation tibia
Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and tibia
Irrigation, debridement and placement external fixator right ankle, intramedullary fixation femur and external fixation tibia
Irrigation, debridement and placement external fixator right ankle, femur and tibia
Irrigation, debridement and external fixation right ankle and skeletal traction
The patient is relatively hemodynamically stable. In this case the femur and tibia should be definitively fixed while the open ankle fracture can be irrigated and debrided and placed in a spanning external fixator, temporizing for later definitive fixation.
Aside from an elevated heart rate and mildly elevated lactate (normal < 2.5 mmol/L), the patient is relatively stable making him a good candidate for long bone stabilization and temporizing external fixation of the right ankle. Gross contamination of the open injury also supports temporizing fixation, which can be brought back for repeat I&D and possible fixation.
Pape et al. compared outcomes for intramedullary nailing (IMN) versus staged fixation for femur fractures in stable versus borderline patients. Borderline patients were defined as those with multi-system injury (especially to lungs) and exhibited higher lung complications following acute IMN when compared to stable patients with isolated orthopaedic injuries.
O'Brien reviewed the literature regarding early total care in regards to IMN stabilization of femur fractures. Summarized data noted isolated injuries treated with early IMN had good outcomes, whereas those with head or lung injury had worse outcomes and pulmonary complications.
Figure A exhibits a right open ankle fracture dislocation. Figure B exhibits a mid-shaft tibia fracture. Figure C exhibits a ballistic mid-shaft femur fracture.
Incorrect Answers:
OrthoCash 2020
Figure A is an anterior-posterior (AP) radiograph of a 27-year-old male who was a bicyclist struck by a motor vehicle. He was intubated in the field and unresponsive in the trauma slot. Ultrasound of his abdomen is positive for blood and he is brought to the operating room emergently for an exploratory laparotomy. He is found to have ischemic bowel and a grade 4 liver laceration. His lactate is 9.0 mg/dL. Which figure represents the next appropriate step in regard to his pelvic ring injury?
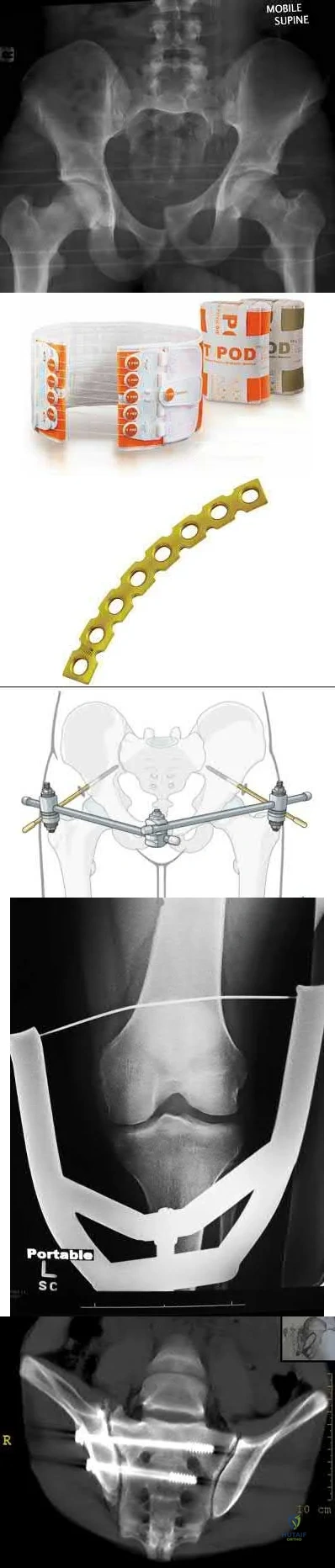
The radiograph exhibits an elevated left hemipelvis with complete sacroiliac disruption, which can be temporized with placement in skeletal traction.
The patient is unstable, as indicated by an elevated lactate level. The most appropriate next step is temporizing skeletal traction to reduce the left hemipelvis.
Langford et al. review the initial diagnosis, evaluation and resuscitation in the management of pelvic fractures. Reduction of pelvic volume can be achieved with pelvic binders and temporizing external fixation for anterior posterior compression (APC) and/or lateral compression (LC) fracture patterns, while skeletal traction can help do the same in vertical shear patterns.
Matullo et al. review the uses of skeletal traction in orthopaedic trauma, where lower extremity skeletal traction can be an efficient, fast, easy way to help reduce pelvic volume in vertical shear injuries, especially when the patient is unstable and not cleared for definitive fixation.
Figure A exhibits an elevated left hemipelvis indicative of a vertical shear injury and complete SI disruption. Figure B is an example of a pelvic binder. Figure C is a pelvic reconstruction plate. Figure D is a schematic of an anterior pelvic external fixator. Figure E is a schematic drawing of a patient in lower extremity
skeletal traction. Figure F is a radiograph exhibiting S1 and S2 sacroiliac (SI) screws.
Incorrect answers:
OrthoCash 2020
A 38-year-old man is involved in a motor vehicle collision and suffers the grossly open injury shown in Figure A. He subsequently undergoes irrigation and debridement and placement of an external fixator. In Figure B, if the proximal pin is placed at the red circle as compared to the black circle, the patient is at increased risk for which of the following?

Foot drop
Injury to the anterior tibial artery
Septic arthritis
Flexion contracture of the knee
Patellar tendon rupture Corrent answer: 3
The patient is at increased risk of septic arthritis when placing the proximal tibial pin too proximal due to penetration of the joint capsule. Pin site flora can track into the joint and lead to a septic knee.
Tibial external fixators can be used to temporize tibial shaft, pilon, and ankle fractures not ready for definitive management due to soft tissue concerns and/or practice of damage control orthopaedics. Intracapsular placement of fixator pins can lead to septic arthritis. The capsular reflection typically extends 14 mm distal to the subchondral line.
DeCoster et al. reported a cadaveric dissection study for safe placement of proximal tibia pins and determined that the capsule inserts 14 mm below the articular surface along the posteromedial and posterolateral surfaces. For fractures requiring extremely proximal pin placement, they recommend
anterior cortex penetration only at least 6 mm distal to articular surface.
Reid et al. investigated safe transtibial pin placement using MRI and cadaveric and volunteer knees. They found that pin placement 14 mm distal to subchondral bone will result in low likelihood of capsular penetration.
Figure A is an AP radiograph showing a segmental middle third tibia/fibula fracture. Figure B is a lateral diagram of the tibia showing potential sites of proximal pin placement.
Incorrect Answers:
OrthoCash 2020
Figures A and B are radiographs of a 43-year-old, right-hand dominant, male that injured his arm in a motor vehicle accident. What would be an absolute indication for surgical fixation of his injury?
Radial nerve palsy
Intra-articular extension
2mm fracture distraction, 5 degrees of rotational malignment
Ipsilateral proximal both bone forearm fracture
Bilateral fracture
This patient has a humeral shaft fracture. An absolute indication for surgery would include a floating elbow, i.e. ipsilateral both bone forearm fracture.
The primary causes of humeral fractures include motor vehicle accidents, falls, or violent injury. Almost all cases are treated non-operatively with functional bracing. The absolute indications for surgical management include: ipsilateral vascular injury, severe soft-tissue injury, open fracture, compartment syndrome, and associated ipsilateral forearm fracture, ie, floating elbow. The relative indications for surgical management include: segmental fracture, intraarticular extension, significant fracture distraction, bilateral humeral fracture, inability to maintain acceptable alignment, and polytrauma.
Klenerman et al. reviewed non-operative treatment of humeral shaft fractures. They showed that acceptable results could be achieved even after 20° of
anterior bowing, 30° of varus angulation, 15° of malrotation, and 3 cm of shortening.
Carroll et al. reviewed the management of humeral shaft fractures. They state the indications for operative fixation to be polytraumatic injuries, open fractures, vascular injury, ipsilateral articular fractures, floating elbow injuries, and fractures that fail nonsurgical management. Surgical techniques include external fixation, open reduction and internal fixation, minimally invasive percutaneous osteosynthesis, and antegrade or retrograde intramedullary nailing
Figure A and B shows a comminuted mid-shaft humeral fracture with intraarticular extension.
Incorrect Answers:
OrthoCash 2020
Which of the following findings is a contraindication in retrograde nailing of a periprosthetic distal femur fracture around a total knee arthroplasty?
Posterior-stabilized total knee implant
Cruciate retaining total knee implant
Spiral fracture pattern
Distal femoral replacement
Knee flexion contracture of 15 degrees Corrent answer: 4
A distal femoral replacement (TKA) implant will generally preclude placement of a retrograde nail due to the long stem on the femoral component.
Supracondylar femur fractures above a well-fixed TKA component are increasingly common. These fractures are often treated with a lateral locking plate, but can also be treated with a retrograde nail in certain circumstances. An important factor in determining if nailing is a viable option are knowing the TKA implant and it's design. In addition, if the TKA component is known, the maximum size of reamer head and nail can be determined preoperatively from the size of the femoral 'box'.
Schutz et al report on a prospective multicenter study of 112 patients who underwent fixation of a distal femur fracture with the LISS system. They report that 90% of fractures went on to union and they attribute all of the failures to either the high-energy nature of particular fractures or a lack of experience in applying the plate in an appropriate pattern. They also note that primary grafting of these fractures is not necessary.
Illustration A shows a periprosthetic femur fracture treated with a retrograde nail.
Incorrect Answers:
1: A posterior-stabilized implant can be treated with an intramedullary nail in many circumstances but can be technically challenging, depending on the components.
2: A cruciate retaining TKA is not a contraindication to use of a retrograde nail. 3: A spiral pattern periprosthetic supracondylar femur fracture can be treated with a femoral nail.
5: A knee flexion contracture will often provide the flexion necessary for access to the box of the femoral component. A knee extension contracture, however, can preclude access to this box for placement of a nail.

OrthoCash 2020
A patient falls and sustains the isolated injury seen in Figures A and B. The surgical plan includes open reduction and internal fixation with a small mini-fragment plate using a direct lateral approach. During the approach, the forearm was placed in a fully pronated position. What would be the correct position of the forearm during plate application?

Full pronation
25 degrees pronation
Neutral
25 degrees supination
Full supination
Using the lateral approach (Kocher or Kaplan), the correct placement of the arm should be in a neutral position so that the plate can be placed on the bare area of the proximal radius.
Displaced radial head fractures with less than 3 fragments can be amendable to open reduction internal fixation. The methods of fixation include buried or headless screws, if placed at the articular surface, or posterolateral plating, if placed in the bare area. The safe zone for plating is located at a 90-110 arc from the radial styloid to Lister's tubercle with the arm in neutral rotation. This position helps to avoid impingement of ulna against the plate with forearm rotation. It should be noted that during the approach, that the forearm should be fully pronated to avoid injury to the posterior interosseous nerve.
Mathew et al. reviewed the concepts of terrible triad injuries of the elbow. Radial head fractures are treated conservatively when there is an isolated minimally displaced (less than 2mm) fracture with no mechanical block to motion. Open reduction internal fixation is used for Mason II or III fractures with < 3 fragments. Radial head replacement is considered for comminuted
fractures (Mason Type III) with 3 or more fragments.
Cheung et al. reviewed the surgical approaches to the elbow. The lateral approach (Kocher or Kaplan) is most commonly used with these injuries. The Kocher approach utilizes the intramuscular plane between anconeus and extensor carpi ulnaris. Kaplan utilizes the plane between extensor digitorum commons and extensor carpi radialis brevis.
Figure A and B show AP and lateral radiographs of the left elbow. There is a displaced radial head fracture. Illustration A shows a schematic diagram of the radial head "safe zone" between the radial styloid to Lister's tubercle.
Incorrect Answers:
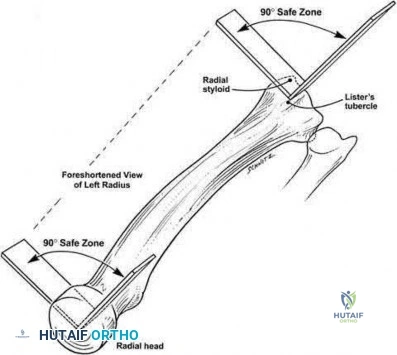
OrthoCash 2020
A 38-year-old male is involved in a high speed motor vehicle collision. He has a Glasgow Coma Scale of 13 and receives 2 liters of fluid en route to the emergency department. Upon evaluation in the emergency department, he is found to have a bilateral femoral shaft fractures, a right ankle fracture, and a left both bone forearm fracture. He also has 2 left sided rib fracture and a grade II liver laceration. His heart rate is 130 and blood pressure is 85/50. All of the following
would be indications to practice damage control orthopaedics in this patient except:
Bilateral femur fractures
Rib fractures
Lactate of 5.2
Urine output of 20 cc/hr
Heart rate and blood pressure Corrent answer: 2
Rib fractures without evidence of further thoracic trauma would not be an indication to practice damage control orthopaedics. This patient is underresuscitated based on his lactate level, urine output, and vital signs and definitive management should be delayed.
Damage control orthopaedics is the practice of delaying definitive management of fractures and utilizing temporary stabilization (such as an external fixator) until a patient has recovered from the initial physiologic insult of trauma.
Patients are at increased risk for perioperative complications such as ARDS and multi-system organ failure during the acute period after polytrauma. In addition to underresuscitation, other indications to practice damage control orthopaedics include: injury severity score>40 (or >20 with thoracic trauma), bilateral femoral fractures, hypothermia below 35 degrees Celsius, and pulmonary contusions.
Pape et al. (2007) studied the incidence of acute lung injuries in polytrauma patients undergoing either intramedullary nailing or external fixation and later definitive fixation of femoral shaft fractures. They found that patients undergoing immediate intramedullary nailing were nearly 6.7 times more likely to have acute lung injury
The Canadian Orthopedic Trauma Society studied the effect of reamed versus unreamed femoral nailing on incidence of ARDS for femoral shaft fractures in trauma patients using a randomized controlled study. They found no difference between the groups.
Pape et al. also examined the pathophysiological cascades that accompany soft tissue injuries of the extremities, abdomen, and pelvis and recommend a more comprehensive for evaluation of patients with these injuries.
Incorrect Answers:
OrthoCash 2020
The anterior intrapelvic (modified Stoppa) approach is most appropriate for which of the following fractures?
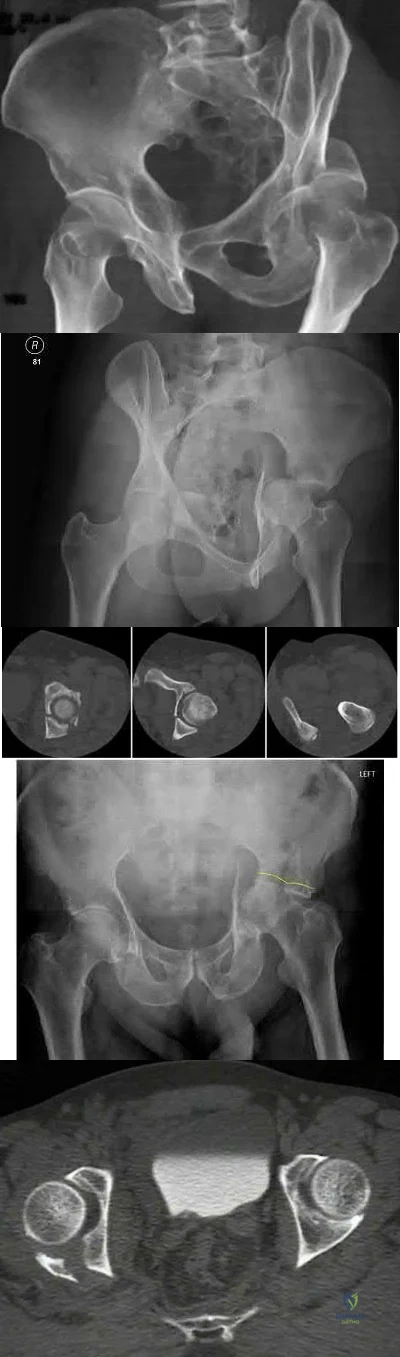
The anterior intrapelvic (AIP) or modified Stoppa approach provides access to the quadrilateral plate, which is a common location for fracture displacement in associated both column acetabulum fractures as seen in Figure D.
Compared to the traditional ilioinguinal approach, the modified Stoppa with a lateral window can offer comparable access to the quadrilateral plate, which can allow for its use in associated both column fracture patterns.
de Peretti et al. prospectively followed 25 patients with both column fractures
treated via an iliofemoral approach. Results led the authors to not recommend the extensile approach for both column fractures due to lack of efficiency and high complication rates.
Alonso et al. compared the extensile iliofemoral and triradiate approaches, and both reported acceptable results. However, concerning were the relatively high rates of heterotopic ossification, despite prophylaxis.
Bible al. performed a cadaver study to quantify the amount of access provided by the modified Stoppa approach. This approach provides access to approximately 80% of both the inner pelvis, and the quadrilateral plate, however, comparison to the ilioinguinal approach was not performed.
Shazar et al., in a cohort comparison between the ilioguinal and Stoppa approaches, noted better visualization and potential improve fracture reduction via the Stoppa approach for both column fractures. However, this study was limited in its retrospective and relative observer bias.
Figure A depicts a posterior wall fracture dislocation with concomitant femoral neck fracture. Figure B is an iliac oblique view which depicts a posterior column fracture. Figure C exhibits a posterior column + posterior wall fracture. Figure D depicts acetabular fracture with protrusio. Figure E exhibits a posterior wall fracture.
Incorrect answers:
OrthoCash 2020
Figure A is a radiograph of a 75-year-old woman that fell onto her non-dominant shoulder from a standing height. She was treated nonoperatively for 9 months but continues to complain of pain when she elevates her arm. In patients with this type of fracture pattern, what factor has the greatest impact on fracture healing?

Hand dominance
Angulation of fracture
Smoking
Early physical therapy
Diet
This patient has an impacted varus proximal humerus fracture. Smoking has been shown to increase the nonunion risk up to 5.5 times with these fractures.
Impacted varus proximal humerus fractures can be managed effectively with non-operative care. The major factors that influence non-union are age and smoking. Solid bony union can be seen in 93-98% of patients at 1 year, with more than 97% of people returning to pre-injury level of function. The angulation of fracture, hand dominance and physical therapy does not seem to influence bone union or functional outcomes with this fracture pattern.
Court-Brown et al. looked at the outcomes of impacted varus fractures. They determined that the age of the patient was the major factor in overall outcome. They showed that the best results occurred in younger patients, but results deteriorate with advancing age. Physical therapy was not found to
impact outcome.
Hanson et al. showed that impacted varus fractures can be successfully managed with non-operative care. They found that overall fracture displacement had a minor impact of fracture healing and functional outcome. The predicted risk of delayed union and nonunion was 7% with patients that smoke. This was 5.5 times greater than non-smokers.
Figure A shows an AP radiograph of a varus angulated proximal humerus fracture. This radiograph shows delayed atrophic union.
Incorrect Answers:
OrthoCash 2020
A 26-year-old male epileptic patients presents with right shoulder pain and deformity after a grand mal seizure. After medical stabilization, he denies previous injury to his shoulder. Pre-reduction and post-reduction radiographs of the shoulder are shown in Figures A-C, respectively; physical examination reveals a normal upper extremity neurovascular examination. After shoulder immobilization, what would be the next most appropriate step in management of this patient?

Abduction brace for three weeks, followed by therapy
Right shoulder MR arthrogram
Open reduction and internal fixation
Hemiarthroplasty
Early range of motion Corrent answer: 3
This patient has presented with a fracture dislocation of the right shoulder. After urgent closed reduction, this patient requires open reduction internal fixation of the proximal humerus, and greater tuberosity fracture fragment in particular.
Isolated greater tuberosity fractures may be associated with shoulder dislocations. Careful review of imaging is critical to identify fracture lines that may extend into the humeral neck and head. If these extensions go undetected, catastrophic propagating fractures may occur during closed reduction maneuvers. Treatment is usually with open reduction internal fixation (ORIF). Young patients with proximal humerus fractures should be treated more aggressively with ORIF as compared to elderly patients. Another example would be a severely impacted valgus proximal humeral fracture in a young patient.
Erasmo et al. examined of 82 cases of humerus fracture dislocations treated with the lateral locking plates. Overall outcomes were excellent to good based on standard scoring systems. Complications included avascular necrosis (12%), varus positioning of the head (4.8%), impingement syndrome (3.6%), secondary screw perforation (3.6%), non-union (2.4%) and infection (1.2%).
Robinson et al. looked at severely impacted valgus proximal humeral fractures treated with open reduction internal fixation in young patients. Anatomic reduction is required with lateral plating to re-establish the normal head/neck angle. Good to excellent results can be achieved with fixation methods.
Figure A shows an anterior fracture-dislocation of the right shoulder. Figure B and C show post-reduction radiographs with a congruent glenohumeral joint. Displacement of the greater tuberosity (GT) fragment is greater than 5mm.
Incorrect Answers:
OrthoCash 2020
Pelvic packing can be performed to temporarily treat a hemodynamically unstable patient with a pelvic ring fracture. Which of the following is the preferred location of the skin incision to perform pelvic packing?
Right anterior superior iliac spine (ASIS) to mid-symphysis, left lateral window incision
Left ASIS to mid-symphysis, right lateral window incision
Subumbilical incision
ASIS to ASIS bilaterally
Pararectus incision
The preferred skin incision location is a subumbilical incision, 6-8cm extending upwards from the pubic symphysis towards the umbilicus; this allows access to all of the appropriate areas for pelvic packing.
Following skin incision, the rectus fascia is then divided in the midline which allows for access to both sides of the bladder for packing deep in the pelvic
brim. On each side, 3 lap pads are placed from sacroiliac joint to the retropubic space, all placed below the level of the pelvic brim.
Hak et al. review the options for emergent treatment in life threatening hemorrhage secondary to pelvic fractures. The authors offer several options for emergent treatment, which includes the use of pelvic binders, the placement of external fixators, pelvic packing and interventional angiography. Goals include reduction of pelvic volume and stopping rapid hemorrhage to save a patient's life. Pelvic packing, properly performed, is done through a subumbilical incision, as described above.
Osborn et al. retrospectively reviewed and compared emergent pelvic packing to angiography in hemorrhagic pelvic fracture clinical scenarios. The authors noted comparable results in mortality with a noted decrease in need for post-procedure transfusions in the pelvic packing group.
Cothren et al. reported their outcomes following an institutional algorithmic change from pelvic ex-fix/angiography to pelvic packing and ex-fix. Since their institutional change, the authors noted a significant decrease in transfusions, need for angiography and mortality.
Incorrect answers:
OrthoCash 2020
A 28-year-old man is brought by ambulance to the emergency department after falling from the roof of his home four hours ago. Upon initial evaluation, he has visible deformities of his bilateral lower extremities and a positive FAST exam. Heart rate is 135, blood pressure 85/58, and urine output is 40 cc over 3 hours. According to ATLS guidelines, what percentage of his blood volume has this patient likely lost?
Question 16
No fractures were identified and the patient was treated nonsurgically in a range-of-motion brace. Two months later, he continued to experience elbow pain and was unable to return to sports. He regained motion and strength with physical therapy, there was no gross instability with varus or valgus testing, and he had a negative moving-valgus stress test. The orthopaedic surgeon performed an examination under anesthesia in the operating room (Video 54). Which anatomic structure is injured?
Explanation
Ninety percent of elbow dislocations occur in a posterolateral direction. O’Driscoll and associates described the mechanism of injury in posterolateral elbow dislocations in 1992, reporting that they occur most typically after a fall onto an outstretched arm. As the arm hits the ground it causes axial compression, forearm supination, and valgus load across the elbow. The triceps fires, pulling the olecranon posterior; the forearm supinates while simultaneous shoulder internal rotators fire; and the elbow falls into valgus. These 3 mechanisms cause the elbow to subluxate and dislocate posterolaterally. The elbow is most stable following posterolateral dislocation in a flexed and pronated position. The elbow is least stable in extension and supination. Simple dislocation often can be treated nonsurgically, while fracture dislocation will usually necessitate surgical intervention. The video shows the elbow pivot-shift test, which evaluates for posterolateral rotatory instability. A positive test finding elicits apprehension and, in this case, radial head subluxation and confirms an insufficient lateral UCL.
Question 17
Optimal management of the injury shown in Figure 31 should include which of the following?
Explanation
REFERENCES: Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.
Question 18
Figures 1 and 2 show the postreduction radiographs obtained from a 32-year-old man who fell from a ladder onto his outstretched right arm. He reports right wrist pain and dense numbness in his radial digits. What is the most appropriate treatment option?

Explanation
This patient sustained a lesser-arc perilunate dislocation. As a result of the injury, he also developed acute carpal tunnel syndrome. The closed reduction attempt was unsuccessful; therefore, this injury is best managed with emergent surgery, an open carpal tunnel release, an open reduction of the perilunate dislocation, scapholunate ligament repair, and intercarpal pinning. Outpatient surgery in a delayed fashion is not advised because of the acuity and severity of the carpal tunnel syndrome. Closed reduction and casting is not advised, because it commonly leads to continued carpal instability with subsequent dorsal
intercalated segment instability deformity and scaphoid lunate advanced collapse wrist arthritis.
Question 19
Which of the following statements describing chordomas is false?
Explanation
REFERENCE: Casali PG, Stacchiotti S, Sangalli C, et al: Chordoma. Curr Opin Oncol 2007;19:367-370.
Question 20
- Which of the following acetabular/femoral head components would be expected to show an optimal combination of linear and volumetric wear?
Explanation
Question 21
A 2-year-old girl has had a swollen right knee for the past 7 weeks. There is no history of significant trauma, and she has not had a fever or been ill. Her parents report that she is stiff in the morning but otherwise does not report pain. A CBC count and erythrocyte sedimentation rate are normal. Treatment with naproxen at appropriate doses for the past 2 weeks has resulted in some improvement. Radiographs show only soft-tissue swelling. Examination reveals a healthy-appearing child with a warm and swollen right knee that is only slightly tender but lacks full extension by 20 degrees. What is the next most appropriate step in management?
Explanation
REFERENCES: Wolf MD, Lichter PR, Ragsdale CG: Prognostic factors in the uveitis of juvenile rheumatoid arthritis. Ophthalmology 1987;94:1242.
Cassidy JT, Petty RE: Textbook of Pediatric Rheumatology. Philadelphia, PA, WB Saunders, 2001, p 220.
Chalom ED, Goldsmith DP, Koehler MA, et al: Prevalence and outcome of uveitis in a regional cohort of patients with juvenile rheumatoid arthritis. J Rheumatol 1997;24:2031-2034.
Question 22
A 25-year-old semiprofessional football player sustains a hyperextension injury to the left foot. He is unable to bear weight. Examination reveals tenderness along the midfoot with swelling and plantar ecchymosis. Radiographs are negative. What is the next step in evaluation of this patient?
Explanation
REFERENCES: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Hunt SA, Ropiak C, Tejwani NC: Lisfranc joint injuries: Diagnosis and treatment. Am J Orthop 2006;35:376-385.
Question 23
Which of the following findings is considered a poor prognostic factor for postoperative neurologic recovery in patients with rheumatoid arthritis?
Explanation
REFERENCES: Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Casey AT, Crockard HA, Bland JM, et al: Predictors of outcome in the quadriparetic nonambulatory myelopathic patient with rheumatoid arthritis: A prospective study of 55 surgically treated Ranawat Class IIIb patients. J Neurosurg 1996;85:574-581.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 24
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?
Explanation
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79:1653-1662.
Question 25
In a locking plate screw construct, axial forces are borne by which of the following?
Explanation
Question 26
Complications following a reverse shoulder prosthesis occur most frequently when performed for what diagnosis? Review Topic
Explanation
Question 27
Figure 31 is the abdominal radiograph of a 70-year-old woman who experiences nausea and abdominal tightness 48 hours following left total knee arthroplasty performed under general anesthesia. She received 24 hours of cefazolin antibiotic prophylaxis and a patient-controlled analgesia narcotic pump for pain management. She has been receiving warfarin for thromboembolic prophylaxis. Her severe abdominal distension and markedly decreased bowel sounds are most likely secondary to
Explanation
The radiograph reveals severe intestinal dilatation, which has occurred as the result of acute colonic pseudo-obstruction and is associated with excessive narcotic administration following total joint arthroplasty. Anesthetic type, antibiotic administration, and warfarin have not been associated with this obstruction. Electrolyte imbalances such as hypokalemia have been associated with postsurgical acute colonic pseudo-obstruction.

CLINICAL SITUATION FOR QUESTIONS 32 THROUGH 35
Figures 32a through 32c are the radiographs of a 30-year old man who is experiencing right hip pain. He has no current medical problems, but, with a body mass index of 41, he is morbidly obese. He was previously treated for leukemia with chemotherapy that included
high-dose steroids. He undergoes total hip arthroplasty (THA) with a ceramic-on-ceramic bearing.
Question 28
A unilateral "piano key" sign, indicates
Explanation
The piano key sign is a demonstration of instability at the DRUJ, typically seen after healing from a distal radius fracture with an associated ulnar styloid fracture (as in this case) or other wrist injury. The hand is pushed down against a table top, and the distal radius translates dorsally (with the distal ulna apparently moving volarly). In fact, the distal radius is the mobile segment, while the distal ulna is fixed in space. Treatment involves repair or reconstruction of the foveal insertion of the triangular fibrocartilage complex (TFCC) and distal radioulnar ligaments. This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ. Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
Question 29
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Explanation
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 30
In infantile idiopathic scoliosis, which of the following factors suggests progression?
Explanation
REFERENCES: Mehta MH: The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J Bone Joint Surg Br 1972;54:230-243.
Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 697.
Question 31
A 26-year-old man is involved in a high-speed motorcycle accident. He sustains a grade IIIB open tibia fracture. Examination reveals a large soft-tissue defect and an insensate foot. What is the expected outcome in this scenario? Review Topic
Explanation
Question 32
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 33
Which of the following is an advantage of computer-assisted navigation used to place medullary nail interlocking screws compared to a freehand techinque?

Explanation
Ricci et al compared two fluoroscopic navigation tracking technologies, optical and electromagnetic versus standard freehand fluoroscopic targeting, in a standardized foam block model for placement of interlocking screws. They found that fluoroscopy time (seconds) and number of fluoroscopy images were significantly less when using the computer-guided systems than for freehand-unguided insertion. Average distance of pin placement from the target in the foam blocks was significantly greater for controls than for each of the navigated systems.
Suhm et al performed a prospective controlled clinical study to compare fluoroscopic guidance with fluoroscopy-based surgical navigation for distal locking of intramedullary implants. The surgical navigation group showed increased procedure time, but equivalent precision with reduced radiation exposure. There was no significant difference in the technical reliability between both groups.
Question 34
- Which of the following events is most likely to occur following a complete transection of a peripheral nerve?
Explanation
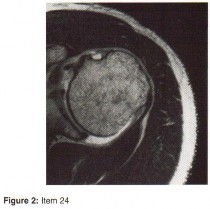
Question 35
The best candidate for a reverse total shoulder arthroplasty is a patient with rotator cuff tear arthropathy with Review Topic
Explanation
Question 36
Tension band wire fixation is best indicated for which of the following types of olecranon fractures?
Explanation
Question 37
03 Figure 9 shows the radiograph of a patient who has anterior knee pain and range of motion from 0-of the tibial tubercle. Treatment should consist of

Explanation
The picture shows a laterally subluxed and a relatively-externally rotated patella on a femoral component. The question tells us that the femoral component is internally rotated and the tibial component is perfectly placed. If we know that the femoral component should be externally
rotated about 3 degrees, we know that in this patient, that’s where the problem is. So, we don’t have to do anything to the quads, tubercle or tibial component. We need to revise the femur. Besides, a lateral retinacular release may damage the lateral geniculates; since this patient most likely had a medial arthrotomy, this may devascularize the patella and lead to patellar AVN. A lateral retinacular release will not address the malpositioned components )
back to this question next question
Question 38
An 82-year-old man is seen in consultation after being admitted for a fall from ground level. There was no loss of consciousness and the patient recalls striking his head and sustaining a hyperextension-type injury to the cervical spine. Examination reveals an 8-cm head laceration with only mild axial neck tenderness. He has generalized weakness throughout the upper extremities and maintained motor function of the lower extremities. There are no obvious sensory deficits, and the bulbocavernous reflex and deep tendon reflexes are maintained. What is the most appropriate diagnosis at this time?
Explanation
REFERENCES: Penrod LE, Hegde SK, Ditunno JF: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Harrop JS, Sharan A, Ratliff J: Central cord injury: Pathophysiology, management, and outcomes. Spine J 2006;6:198S-206S.
Question 39
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show
Explanation
REFERENCES: Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin
Bernhardt DT, Landry GL: Sports injuries in young athletes. Adv Pediatr 1995;42:465- Sports Med 1999;18:109-171.
Brown HR, Indelicato PA: Complications of anterior cruciate ligament reconstruction. Op Tech Orthop 1992;2:125-135.
Question 40
Vertebral fractures are common in the thoracolumbar spine. What is the most important factor that determines the strength of the cancellous bone in the vertebral body?
Explanation
REFERENCES: Carter DR, Hayes WC: The compressive behavior of bone as a two-phase porous structure. J Bone Joint Surg Am 1977;59:954-962.
Keaveny TM: Strength of trabecular bone, in Cowin SC (ed): Bone Mechanics Handbook. Boca Raton, FL, CRC Press, 2001, pp 16-1-16-8.
Question 41
What is the most common complication requiring reoperation after dorsal plating for a distal radius fracture?
Explanation
REFERENCES: Rozental TD, Beredjiklian PK, Bozentka DJ: Functional outcome and complications following two types of dorsal plating for unstable fractures of the distal part of the radius. J Bone Joint Surg Am 2003;85:1956-1960.
Kambouroglou GK, Axelrod TS: Complications of the AO/ASIF titanium distal radius plate system (pi plate) in internal fixation of the distal radius: A brief report. J Hand Surg Am 1998;23:737-741.
Question 42
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management? Review Topic

Explanation
Question 43
An orthopaedic surgeon frequently uses hip and knee prostheses from a specific manufacturer. The surgeon becomes acquainted with the manufacturer’s representative who provides the support for these prostheses in the hospital. They develop a personal relationship outside of work through a common interest in sailing. Together they become interested in buying a sailboat. The manufacture’s representative suggests a partnership in a boat costing $200,000. The manufacture’s representative would purchase a 90% interest and the surgeon a 10% interest in the boat. There would be no restrictions on use of the boat by the surgeon. What should the orthopaedic surgeon do?
Explanation
partnership seems completely outside of the orthopaedic business relationship does not excuse it. Conflicts of interest should always be resolved and in the best interest of patient care, and in this case the best course clearly is to avoid the conflict of interest totally. An equal interest in the boat does not eliminate the conflict of interest.
Question 44
An otherwise healthy 25-year-old man with an isolated closed mid-diaphyseal femoral fracture undergoes intramedullary nailing. Compared with nonreamed nailing, reamed femoral nailing is associated with a higher rate of Review Topic
Explanation
Question 45
When compared with a conventional ultra-high molecular weight polyethylene (UHMWPE) -bearing surface in total hip arthroplasty, a highly cross-linked polyethylene (XLPE) -bearing surface is associated with
Explanation
A. a functional result for at least 20 years.
B. a functional result that deteriorates within the first 10 years.
C. an eventual conversion to a constrained knee arthroplasty.
D. an eventual need for arthrodesis.
Distal femoral varus osteotomy (DFVO) is intended for patients younger than age 50, more active patients with isolated lateral compartment arthritis and valgus malalignment. Although the knee functional score improves at 1-year follow-up, the function scores significantly deteriorate at 10-year follow-up. At 15-year follow-up, the knee function further declines, resulting in an overall failure rate of 48.5%. DFVO provides longer lasting benefit in patients with better presurgical knee function.
Total knee arthroplasty following DFVO provides improved function and successful outcomes. Standard posterior stabilized components provide satisfactory stability after appropriate ligament balancing without the need for stemmed or highly constrained implants for most patients.
Question 46
A 59-year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Figure 1. Postreduction CT is shown in Figures 2 through 4. What is the most appropriate definitive surgical treatment?
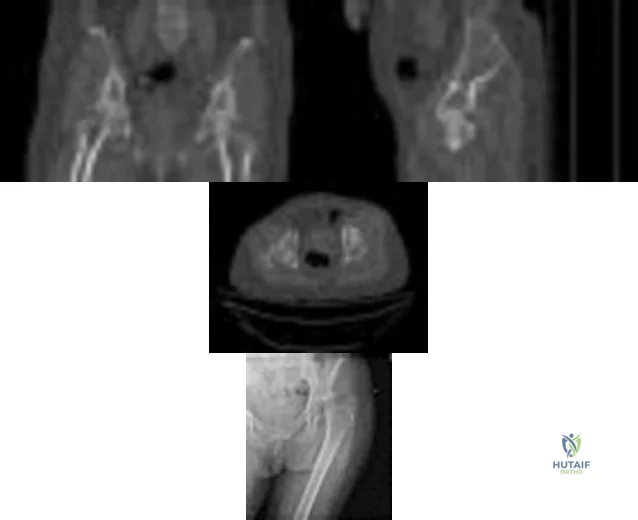
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 47
Internal impingement of the shoulder and posterosuperior labral pathology in throwers has been most clearly associated with which of the following? Review Topic
Explanation
Coracoacromial arch stenosis is associated with subacromial impingement and unrelated to internal impingement. Bennett's lesion refers to exostosis or calcification at the posterior capsule and while potentially associated with overhead throwing athletes who may have internal impingement, a causal link between the two has not been established and therefore posterior capsular contracture is the preferred response.
Question 48
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?

Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 49
Figures 163a through 163c show the radiograph and MRI scans of a 45-year-old woman with severe right arm pain. She has had symptoms for 6 months without resolution despite multiple nonsurgical treatments. Examination reveals weakness in the right triceps and wrist flexors with decreased sensation in the middle finger and a positive Spurling's sign. What is the most appropriate treatment for the patient's symptoms? Review Topic

Explanation
Question 50
below show the radiograph and the MRI scan obtained from a year-old woman with a month history of left hip pain. Which presurgical factor is most commonly associated with a poor outcome after a hip joint salvage procedure?
Explanation
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the
Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge
score cannot be determined presurgically.
Question 51
The hallucal sesamoids are held together by which of the following structures?
Explanation
REFERENCES: Lewis WH (ed): Gray’s Anatomy of the Human Body, ed 20. Philadelphia, PA, Lea & Febiger, 2000.
Richardson EG: Hallucal sesamoid pain: Causes and surgical treatment. J Am Acad Orthop Surg 1999;7:270-278.
Question 52
Figure 61 shows the radiograph of a 28-year-old professional football player who sustained a hyperextension injury to the great toe. He continued to play with pain and loss of push-off strength. What is the most likely diagnosis?

Explanation
Question 53
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?
Explanation
REFERENCES: Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.
Question 54
Physiologic bowing of the lower extremities should spontaneously correct by what age?
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 7.
Salenius P, Vankka E: The development of the tibiofemoral angle in children. J Bone Joint Surg Am
J V :
Question 55
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal? Review Topic
Explanation
Question 56
Compared with retention of the native patella in primary total knee arthroplasty, routine patellar resurfacing is associated with
Explanation
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in
large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate in patients with anterior knee pain.
Question 57
A 43-year-old woman has had pain in the left hip for the past 2 months. A radiograph, CT scan, MRI scan, and biopsy specimens are shown in Figures 16a through 16e. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra JM, Gold R, Downs J, Eckardt JJ: A new histologic approach to the differentiation of enchondroma and chondrosarcoma of the bones: A clinicopathologic analysis of 51 cases. Clin Orthop 1985;201:214-237.
Question 58
- A 20-year-old college football player sustains a forceful hyperextension injury to his shoulder 4 months after undergoing an anterior capsular shift. Examination 2 weeks later reveals anterior tenderness. He is unable to lift the dorsum of his hand away from his back. What is the most likely diagnosis?
Explanation
Question 59
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?
Explanation
REFERENCES: Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Posner MA: Flexor superficialis tendon transfers to the thumb: An alternative to the free tendon graft for treatment of chronic injuries within the digital sheath. J Hand Surg Am 1983;8:876-881.
Question 60
Figure 46 shows the AP radiograph of an active 80-year-old patient with an acetabular fracture. The fracture was initially managed nonsurgically; however, the patient is now scheduled to undergo total hip arthroplasty. What is the treatment of choice for the contained acetabular bone defect?
Explanation
REFERENCES: Mears DC: Surgical treatment of acetabular fractures in elderly patients with osteoporotic bone. J Am Acad Orthop Surg 1999;7:128-141.
Bellabarba C, Berger RA, Bentley CD, et al: Cementless acetabular reconstruction after acetabular fracture. J Bone Joint Surg Am 2001;83:868-876.
Question 61
What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?
Explanation
REFERENCES: Cantu RC: Head and spine injuries in youth sports. Clin Sports Med 1995;14:517-532.
Proctor MR, Cantu RC: Head and neck injuries in young athletes. Clin Sports Med 2000;19:693-715.
Torg JS: Epidemiology, pathomechanics, and prevention of athletic injuries to the cervical spine. Med Sci Sports Exerc 1985;17:295-303.
Question 62
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?
Explanation
REFERENCES: Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214.
McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Ouzounian TJ: Metatarsophalangeal arthrodesis for salvage of failed hallux valgus surgery. Foot Ankle Clin 1997;2:741-752.
Question 63
A 13-year-old boy is comatose and has irregular breathing after being struck by a car while riding his bicycle. Auscultation suggests a pneumothorax on the right side and swelling about the right arm and leg. Initial management should consist of
Explanation
REFERENCES: American College of Surgeons Committee on Trauma. Advanced Trauma Life Support Course. Instructor’s Manual. Chicago, IL, American College of Surgeons, 1984.
Eichelberger MR, Randolph JG: Pediatric trauma: An algorithm for diagnosis and therapy. J Trauma 1983;23:91-97.
Question 64
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?
Explanation
REFERENCES: Hartsock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29:467-475.
Hughes M, Neer CS: Glenohumeral joint replacement and postoperative rehabilitation.
Phys Ther 1975;55:850-858.
Compito CA, Self EB, Bigliani LU: Arthroplasty and acute shoulder trauma. Clin Orthop 1994;307:27-36.
Question 65
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints?
Explanation
After activity, pain persists longer with tibial stress fractures.
DISCUSSION: Anterior tibial pain can often be difficult to diagnose. A bone scan showing the tibial cortex in a diffuse, longitudinal orientation is consistent with shin splints compared to a more discreet, localized uptake more commonly seen with a stress fracture. Bone stress injuries are due to cyclical overuse of the bone. They are relatively common in athletes and military recruits but are also seem in otherwise healthy people who have recently started new or intensive physical activity. Diagnosis of bone stress injuries is based on the patient’s history of increased physical activity and on imaging findings.
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
REFERENCES: Mubarak SJ, Gould RN, Lee YF, et al: The medial tibial stress syndrome: A cause of shin splints. Am J Sports Med 1982;10:201-205.
Knobloch K, Yoon U, Vogt PM: Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int 2008:29:671-676.
Kiuru MJ, Pihlajamaki HK, Ahovuo JA: Bone stress injuries. Acta Radiol 2004;45:317-326.
Question 66
A 35-year-old man who has had a 6-month history of low back pain and tenderness now reports worsening pain and stiffness in the hips and entire back. An AP radiograph of the pelvis demonstrates fusion of the sacroiliac joints bilaterally. What is the next most appropriate step in management? Review Topic
Explanation
disease, further work-up in a patient with potential ankylosing spondylitis is not warranted. Sacroiliac joint anesthetic injections and sacroiliac fusion are not recommended treatments for early ankylosing spondylitis. Aspiration of the sacroiliac joints can be done if sacroiliac joint infection is suspected; however, in the absence of fever or other constitutional symptoms, infection is unlikely.
Question 67
An 8-year-old boy with severe hemophilia A (factor VIII) and no inhibitor is averaging eight transfusions per month for bleeding into the right ankle. Examination shows synovial hypertrophy; range of motion consists of 0° of dorsiflexion and 20° of plantar flexion. The patient’s knees, elbows, and left ankle have no restriction of motion. Standing radiographs of the right ankle are shown in Figure 18. Management should consist of
Explanation
REFERENCES: Greene WB: Synovectomy of the ankle for hemophilic arthropathy. J Bone Joint Surg Am 1994;76:812-819.
Greene WB: Chronic inflammatory arthridities and diseases related to the hematopoietic system, in Drennan JC (ed): The Child’s Foot and Ankle, New York, NY, Raven Press, 1992, pp 461-482.
Question 68
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management? L Intensive physiotherapy
Explanation
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Question 69
An 18-year-old man sustained a knife injury to his midback, with the entry wound 2 cm to the left of the midline. He has been diagnosed with a hemicord transection. Neurologic examination will most likely reveal left-sided loss of
Explanation
REFERENCES: Northrup BE, Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 541-549.
Collins RD: Illustrated Manual of Neurologic Diagnosis. Philadelphia, PA, JB Lippincott, 1962, p 71.
Question 70
An Asian 45-year-old man has bilateral upper extremity dysfunction. Figure 35a shows a T2-weighted sagittal MRI scan of the cervical spine, and Figure 35b shows a T2-weighted axial MRI scan at the level of the C3 vertebral body. What is the most likely pathologic process?
Explanation
REFERENCES: McAfee PC, Regan JJ, Bohlman HH: Cervical cord compression from ossification of the posterior longitudinal ligament in non-orientals. J Bone Joint Surg Br 1987;69:569-575.
Kricun R, Kricun ME: MRI and CT of the Spine. New York, NY, Raven Press, 1994,
pp 126-130.
Question 71
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child’s ability to walk in the future?
Explanation
REFERENCES: Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Tachdjian MO: The neuromuscular system: Cerebral palsy, in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 2, p 1621.
Question 72
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future?
Explanation
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Dearolf WW III, Betz RR. Vogl LC, et al: Scoliosis in pediatric spinal cord-injured patients. J Pediatr Orthop 1990;10:214-218.
Mehta S, Betz RR. Mulcahey MJ, et al: Effect of bracing on paralytic scoliosis secondary to spinal cord injury. J Spinal Cord Med 2004;27:S88-S92.
Question 73
A 21-year-old woman with scoliosis reports no pain, and her examination is unremarkable except for the scoliosis. Preoperative radiographs, including bending views, are shown in Figures 14a through 14e. The thoracic curve measures 62 degrees. Treatment should consist of
Explanation
REFERENCES: King HA, Moe JH, Bradford DS, Winter RB: The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg Am 1983;65:1302-1313.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 161-171.
Question 74
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?
Explanation
REFERENCE: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, pp 98-100.
Question 75
Which of the following have been found to affect the rate of perioperative infections or wound complication rates in foot and ankle surgery?
Explanation
REFERENCES: Bibbo C, Anderson RB, Davis WH, et al: The influence of rheumatoid chemotherapy, age, and presence of rheumatoid nodules on postoperative complications in rheumatoid foot and ankle surgery: Analysis of 725 procedures in 104 patients. Foot Ankle Int 2003;24:40-44.
Bibbo C, Goldberg JW: Infections and healing complications after elective orthopaedic foot and ankle surgery during tumor necrosis factor-alpha inhibition therapy. Foot Ankle Int
2004;25:331-335.
Sorensen LT, Karlsmark T, Gottrup F: Abstinence from smoking reduces incisional wound infection: A randomized controlled trial. Ann Surg 2003;238:1-5.
Question 76
Which clinical finding most strongly suggests that nonsurgical care should be discontinued and surgical intervention is necessary?
Explanation
Epidural abscesses are potentially devastating. Nonsurgical care may be chosen for select patients. A baseline failure rate of 8.3% increases based on patient risk factors, which include a history of IV drug abuse, diabetes, age older than 65, CRP level higher than 115, WBC level higher than 12.5, and Staphylococcus aureus as the causative organism. Immunosuppression and abscess size are not significant risk factors for failure of nonsurgical care. Nonsurgical care may be regarded as "failed" if there is worsening of a patient's neurologic status. When nonsurgical care fails, delayed surgery is less successful at restoring motor function (vs early surgery).
RECOMMENDED READINGS
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 77
A 55-year-old man has had progressive right shoulder pain for the past 2 years. Examination reveals active elevation to 120 degrees, external rotation to 20 degrees, and internal rotation to the sacrum. AP and axillary radiographs are shown in Figures 23a and 23b. Which of the following procedures would result in the most predictable long-term pain relief?
Explanation
REFERENCES: Cofield RH, Frankle MA, Zuckerman JD: Humeral head replacement for glenohumeral arthritis. Semin Arthroplasty 1995;6:214-221.
Levine WN, Djurasovic M, Glasson JM, Pollock RG, Flatow EL, Bigliani LU: Hemiarthroplasty for glenohumeral osteoarthritis: Results correlated to degree of glenoid wear. J Shoulder Elbow Surg 1997;6:449-454.
Matsen FA III: Early effectiveness of shoulder arthroplasty for patients who have primary glenohumeral degenerative joint disease. J Bone Joint Surg Am 1996;78:260-264.
Question 78
In patients who have undergone nonsurgical management for idiopathic adhesive capsulitis, long-term follow-up studies have shown which of the following results?
Explanation
REFERENCES: Griggs SM, Ahn A, Green A: Idiopathic adhesive capsulitis: A prospective functional outcome study of nonoperative treatment. J Bone Joint Surg Am 2000;82:1398-1407.
Shaffer B, Tibone JE, Kerlan RK: Frozen shoulder: A long-term follow-up. J Bone Joint Surg Am 1992;74:738-746.
Question 79
A 65-year-old woman sustained an axial load on the arm followed by an abduction injury after falling on ice. Treatment in the emergency department consisted of reduction of an anterior dislocation. She now has a positive drop arm sign and a positive lift-off test. An MRI scan is shown in Figure 9. Based on these findings, management should consist of
Explanation
REFERENCES: Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes.
J Am Acad Orthop Surg 1999;7:300-310.
Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Walch G, Boileau P: Subluxations and dislocations of the tendon of the long head of the biceps. J Shoulder Elbow Surg 1998;7:100-108.
Question 80
A 23-year-old man cut the dorsal and ulnar aspects of his long finger on a table saw. The dorsal and ulnar skin over the middle phalanx is missing, with a 2-cm x 2-cm area of loss. There is a 50% loss of the extensor tendon (ulnar), and the remaining tendon has no tenosynovium. The physician should recommend irrigation and debridement and
Explanation
The patient has exposed bone and tendon and a partial tendon injury. The remaining radial tendon is satisfactory and no tendon repair is required. The exposed bone and tendon necessitate vascularized tissue coverage. A reversed cross-finger flap from the ring finger is suitable for coverage of the dorsal surface of an adjacent digit.
Question 81
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92? Review Topic

Explanation
Question 82
-This boy’s parents are eager to get him back on the field as soon as possible. What is the most appropriate treatment option?
Explanation
Although a recent increase in the number of pitches may have contributed to this patient’s development of little leaguer’s shoulder, the most significant overall factor is age. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress, and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Genetic factors and gender have not been studied in association with little leaguer’s shoulder. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms.Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to baseline pitching is implemented until the patient is back to baseline. This protocol has a long-term success rate exceeding 90%.

Question 83
An otherwise healthy 76-year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in Figures below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?
Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 84
You design a research study in which you ask patients who have a nonunion of the tibia to fill out a questionnaire in which they report on a variety of medical conditions and social/behavioral practices. You compare these findings to a similar group who did not develop a nonunion in order to identify medical and/or social conditions that might be risk factors for the development of tibial nonunions. This would be an example of what type of study?
Explanation
Question 85
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?
Explanation
REFERENCES: Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Bellier G, Dupont JY, Larrain M, et al: Lateral discoid menisci in children. Arthroscopy 1989;5:52-56.
Question 86
Figures 48a through 48c show the lateral radiograph and MRI scans of a 60-year-old man who has had pain in his thigh for 1 month. The next most appropriate step in management should consist of
Explanation
REFERENCES: Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Question 87
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of
Explanation
REFERENCES: Cain JE Jr, Major MR, Lauerman WC, et al: The morbidity of heparin therapy after development of pulmonary embolus in patients undergoing thoracolumbar or lumbar spinal fusion. Spine 1995;20:1600-1603.
Roberts AC: Venous imaging and inferior vena cava filters. Curr Opin Radiol 1992;4:88-96.
Becker DM, Philbrick JT, Selby JB: Inferior vena cava filters. Arch Intern Med
1992;152:1985-1994.
Question 88
Anterior penetration of an iliosacral screw through the sacral ala would most likely lead to weakness of which of the following movements?

Explanation
The referenced study by Routt et al reviewed 177 patients with pelvic ring injuries treated with these screws and found that quality triplanar imaging decreased intraoperative and postoperative complications. They also recommend supplemental fixation of iliosacral screws with posterior plating in noncompliant patients.
Question 89
If a percutaneous iliosacral screw is placed too anteriorly, and the screw exits anterior to the sacral ala before re-entering the sacral body, what will be the most likely finding postoperatively?

Explanation
Question 90
Following a partial muscle laceration, keeping the affected extremity immobilized for 2 weeks before starting an exercise program will likely lead to: Review Topic
Explanation
Healing a muscle injury involves two competing processes: regeneration of muscle fibers and formation of granulation tissue. Starting motion too soon after injury may increase the area of fibrous scar, and limit the ability of new muscle fibers to penetrate this area. Prolonged immobilization limits scar production but penetrating muscle fibers will lack appropriate orientation, and the muscle as whole begins to atrophy. Three to 5 days of immobilization has been shown to limit scar tissue production
while the early motion helps generate appropriately organized muscle fibers and maintain strength and range of motion.
Järvinen et al. present a review of muscle injury and healing. They found that immediate mobilization led to a large area of dense scar tissue that regenerating muscle fibers could not adequately penetrate. Prolonged immobilization allowed muscle fibers to regenerate but they lacked appropriate morphology. Following 3-5 days of immobilization they found less scar tissue, better penetration of regenerated muscle fibers, and the regenerated fibers were more well aligned with the uninjured fibers surrounding them.
Menetrey et al. present a mouse model of muscle laceration comparing a short period of immobilization (5 days) to suture repair of the muscle. They found quicker healing and greater strength in the suture repair group. Tetanus strength at one month after injury was (compared to an uninjured control) 81% for sutured muscle, 35% for the early mobilization only group, and 18% for the prolonged immobilization group.
Illustration A is a histology section of lacerated muscle after 7 days of immobilization. The area is infiltrated with granulation tissue and few regenerating myofibers. Illustration B is a histology section of lacerated muscle after 14 days of immobilization. Further infiltration with granulation tissue and mononuclear cells can be seen with regenerating myofibers only at the periphery.
Incorrect answers:
Question 91
A 27-year-old man was struck by a taxi cab and sustained comminuted right distal third tibia and fibula fractures; treatment consisted of placement of an intramedullary nail in the tibia the following morning. At his 6-month follow-up, he has clawing of all five toes. Examination reveals flexion deformities of the distal and proximal interphalangeal joints that are flexible with plantar flexion and rigid with dorsiflexion. Calluses are present on the dorsum and tip of the toes. Single heel rise is normal. He has a mild equinus contracture (relative to the left leg) that is not relieved with knee flexion. What is the most appropriate treatment option?
Explanation
REFERENCES: Feeny MS, Williams RL, Stephens MM: Selective lengthening of the proximal flexor tendon in the management of acquired claw toes. J Bone Joint Surg Br 2001;83:335-338.
Clawson DK: Claw toes following tibial fracture. Clin Orthop Relat Res 1974;103:47-48.
Question 92
A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis?
Explanation
REFERENCES: Guanche CA, Sikka RS: Acetabular labral tears with underlying chondralmalacia: A possible association with high-level running. Arthroscopy 2005;21:580-585.
McCarthy JC: The diagnosis and treatment of labral and chondral injuries. Instr Course Lect 2004;53:573-577.
Question 93
During a revision total knee arthroplasty (TKA), there is difficulty gaining exposure and a tibial tubercle osteotomy (TTO) is performed. The final components are stable and include a stemmed tibial component that bypasses the osteotomy site. The tibial tubercle is reattached to the osteotomy site with multiple cerclage wires. Following closure of the arthrotomy, the knee is flexed to 90 degrees, and there is no observed displacement of the TTO. What is the best next step in postsurgical rehabilitation?
Explanation
TTO is a recognized technique for improving exposure when performing TKA in a stiff knee. TTO has been reported to enhance surgical exposure and not adversely affect outcomes after TKA, but there is a 5% complication rate. The postsurgical routine following TTO
includes full weight-bearing activity and range of motion as tolerated. Caution should be exercised when manipulation is performed to improve knee flexion following a TTO.
Question 94
Risk for vascular injury during transtibial drilling for reconstruction of this injury is increased by
Explanation
The clinical description and MR image point to an injury to the posterior cruciate ligament (PCL). This ligament is thought to be primarily composed of anterolateral and posteromedial bundles, with the former tightening in flexion and the latter in extension. Because of alterations in knee kinematics and increased varus alignment in PCL insufficiency, contact stresses and cartilage loads increase in the patellofemoral and medial compartments. Although good outcomes may be obtained with transtibial, open inlay, and arthroscopic inlay techniques, 1 major difference is the creation of the “killer-turn” during the transtibial approach. This sharp turn in the graft as it emerges from the tibia appears to lead to more pronounced attenuation and thinning of the graft during cyclic loading.
In Question 12, the scenario describes a patient with chronic PCL and posterolateral corner (PLC) injury, as evidenced by the varus thrust and abnormal Dial test finding. A valgus-
producing osteotomy may be effective, and, in fact, may be the only treatment necessary to address chronic PLC injury. Accordingly, an opening lateral osteotomy would not be appropriate. Of the remaining responses, an osteotomy that increases tibial slope would also address the PCL deficiency by reducing posterior tibial sag.
Vascular injury is an uncommon, but potentially devastating, complication associated with PCL surgery and may occur regardless of the technique used. Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 95
Figures 45a and 45b show the CT scans of a 41-year-old man who was ejected from a vehicle after a high-speed collision. Examination reveals weak (2/5) toe flexion on the right side, but otherwise he has no voluntary motor function in his lower extremities and no sensation. He has some perianal sensation. He has no other associated injuries and his upper extremities are neurologically intact. Which of the following represents the best treatment option? Review Topic
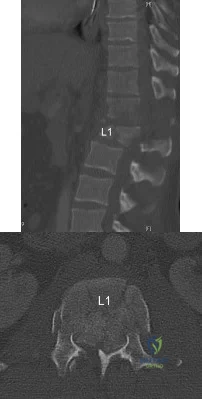
Explanation
(SBQ12SP.25) A 63-year-old female undergoes lumbar decompression and instrumented fusion for the condition shown in Figure A and B. Which of the following factors are associated with increased risk of early post-operative complications? Review Topic

Increasing Age
Intraoperative blood loss
Number of levels fused
All of the above
Age, intraoperative blood loss, and number of spinal levels fused are associated with increased rates of inpatient complication following lumbar decompression and fusion for degenerative spondylolisthesis. Older age correlates with the highest risk for complications.
Lumbar decompression and fusion is well supported in the literature to be effective in the treatment of degenerative spondylolithesis when nonoperative modalities fail. Common complications associated with lumbar decompression and fusion include asymptomatic or symptomatic pseudarthroses (estimated 5-30%), surgical site infection (0.10-2%),and adjacent level degeneration (2-3%). Age, intraoperative blood loss, longer operative times, number of levels fused are associated with increased risk of complication. Smoking is associated with worse outcome after surgery.
Kalanithi et al. reviewed the Nationwide Inpatient Sample adminstrative data on sixty six thousand patients undergoing lumbar laminectomy and fusion. They found the increased age and having 3 or more medical comorbidities was associated with increased risk of complication.
Carreon et al. reviewed cases of ninety eight patients who underwent laminectomy and fusion for lumbar degenerative disease. They found that rates of major and minor complication increased with older age, increased blood loss, longer operative time, number of levels fused.
Figure A is a AP lumbar spine radiograph. Figure B is a lateral lumbar spine radiograph showing degenerative spondylolisthesis at L4-L5. Illustration A shows the postoperative images of the patient treated with an L4-5 fusion with an interbody device.
Incorrect
Question 96
Figures 1 and 2 are the radiographs of a 55-year-old man who has a 3-year history of right shoulder pain. He has maximized nonoperative management and is interested in operative treatment. He had an open Bankart repair 20 years ago and did well until a few years ago. What is most important to know when deciding on the best surgical treatment for this patient?
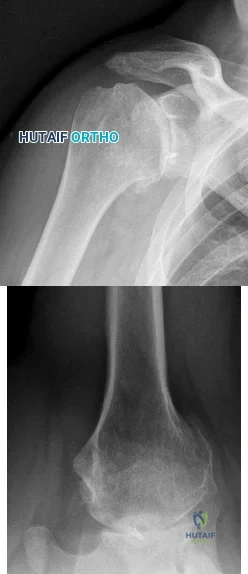
Explanation
Although the radiographs do not reveal any obvious signs of rotator cuff failure, the patient had had an open Bankart 20 years ago. The integrity of the subscapularis tendon following a previous open shoulder procedure is crucial in deciding which type of arthroplasty to consider. Range of motion and infraspinatus strength do not affect the decision-making process, assuming the rotator cuff is intact. Activity level can be important when deciding whether to proceed with an arthroplasty, but it is not as important as the rotator cuff integrity when choosing which
arthroplasty to use.
Question 97
A 25-year-old carpenter falls on his outstretched arm. What physical finding best correlates with the lesion seen on the MRI scan shown in Figure 3?
Explanation
REFERENCES: Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Greis PE, Kuhn JE, Schultheis J, et al: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 98
Porous hydroxyapatite is placed into a bone defect. Incorporation of this bone graft substitute is expected to follow which of the following patterns?
Explanation
Question 99
Figures 155a and 155b are the plain radiographs of a 17-year-old boy who recently noted painless swelling in his distal thigh. Examination reveals a firm, fixed, deep distal thigh mass. There is no associated tenderness. What is the best next treatment step?

Explanation
Question 100
What is the primary problem in rickets osteomalacia?
Explanation
