Orthopedic Board Review MCQs: Foot, Fracture, Knee, Pediatric, Wrist | Part 207

Key Takeaway
This page offers Part 207 of an interactive OITE/AAOS Orthopedic Surgery Board Review quiz. Designed for orthopedic residents and surgeons, it features 100 high-yield, verified MCQs covering Foot, Fracture, Knee, Pediatric, and Wrist. Prepare for your board certification with study and exam modes.
About This Board Review Set
This is Part 207 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 207
This module focuses heavily on: Foot, Fracture, Knee, Pediatric, Wrist.
Sample Questions from This Set
Sample Question 1: A 12½-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full...
Sample Question 2: A 70-year-old male with longstanding diabetic neuropathy sustains a fall down a flight of stairs and sustains the injury shown in Figures A and B. In the operating room, direct reduction of the fracture is performed. The syndesmosis is asse...
Sample Question 3: Figures 1 and 2 show the postreduction radiographs obtained from a 32-year-old man who fell from a ladder onto his outstretched right arm. He reports right wrist pain and dense numbness in his radial digits. What is the most appropriate tre...
Sample Question 4: A cortisone injection in the subacromial space will most likely result in...
Sample Question 5: Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
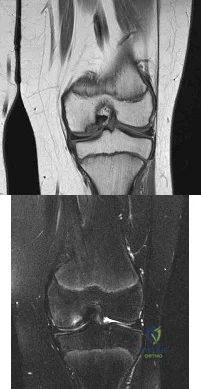
A 12½-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full range of motion without effusion. Radiographs reveal an osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. MRI scans are shown in Figures 14a and 14b. Initial treatment should consist of Review Topic
Explanation
Cessation of sport activities for 4 to 6 months may allow healing of the lesion. Surgical treatment of juvenile OCD lesions is reserved for unstable lesions, patients
who have not shown radiographic evidence of healing and are still symptomatic after
6 months of nonsurgical management, or patients who are approaching skeletal maturity. Good results with stable in situ lesions that have failed to respond to nonsurgical management have been reported with both transarticular and retroarticular drilling. Results after excision alone are poor at 5-year follow-up, and it is unclear if microfracture will improve the long-term outcome. Mosaicplasty may be the next best option for patients who remain or become symptomatic after excision of the fragment and microfracture.
Wall et al. reviewed juvenile OCD. They state that JOCD has better potential for healing than adult OCD, but several series have shown up to a 50% failure to heal with nonsurgical techniques. The presence of a loose body is an indication for surgical fixation, drilling or regenerative procedures, depending on the presence/extent of subchondral bone sclerosis and the surgeon's experience.
Figure A and B are coronal MRI images showing a stable appearing JOCD lesion of the medial femoral condyle.
Incorrect
in the first
(SBQ13PE.9) A 6-year-old boy complains of a 'clunking' sensation in his left knee. He has no associated pain and denies trauma. He can elicit the sensation when moving his knee from flexion into full extension. He is otherwise healthy, with no birth or developmental issues. On examination, there is a palpable clunk felt over the anterior knee through range of motion. There is no obvious instability or tenderness and he had normal patellar tracking. An AP radiograph of the knee is shown in Figure A. What would be the most likely diagnosis? Review Topic

Agenesis of the anterior cruciate ligament
Thickened medial plica
Grade IV chondral flap
Pigmented villonodular synovitis
Abnormal meniscal morphology
This child presents with an asymptomatic click in the knee. It is associated with widening of the lateral joint space of the knee on X-ray. These features are highly suggestive of a discoid lateral meniscus in this age category.
The principal diagnostic feature of a discoid meniscus is the complaint of snapping or clicking in the knee. Children are usually asymptomatic. Although, less frequently, children may present with pain that is largely secondary to an underlying meniscal tear. MRI scans of the knee have show to have the greatest sensitivity for identifying discoid menisci. The presence of a contiguous central meniscus on three consecutive slices is usually indicative of the diagnosis. Treatment is mostly focused on conservative modalities. Surgical intervention is reserved for symptomatic cases with recurrent locking, swelling or persistent pain is present in older children.
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Figure A shows an AP radiograph of a pediatric knee. There is an increased lateral joint space suggestive of a discoid meniscus.
Illustrations A-C show an MRI of the knee with 3 consecutive coronal cuts showing an abnormal appearing discoid meniscus.
Incorrect Answers:
Question 2
A 70-year-old male with longstanding diabetic neuropathy sustains a fall down a flight of stairs and sustains the injury shown in Figures A and B. In the operating room, direct reduction of the fracture is performed. The syndesmosis is assessed and found to be intact. The fibula is fixed with a small fragment locking plate and the medial malleolus is fixed with screws. What is the next best step? Review Topic

Explanation
Diabetics with ankle fractures are prone to complications. Nonoperatively treated cases have up to a 50% incidence of skin breakdown in a cast. Surgically treated patients have up to 40% complication rate. Supplemental fixation can include include multiple syndesmotic screws, spanning external fixation, tibio-talar Steinmann pins, more rigid fibular plates, supplemental intramedulary fibular pinning. Weightbearing after surgery should be delayed (8-12weeks).
McCormack and Leith reviewed the complications in 26 diabetic ankle fractures. 19 patients had surgery. The incidence of complications was 42%. Two required amputation and died. None of the non-diabetic control group had complications. They concluded that in the older, diabetic patient with lower demands, especially if insulin-dependent, it may be preferable to accept a loss of reduction and malunion rather than risk the potentially devastating complications associated with operative intervention. If surgery is necessary, the results of this study provides a more accurate prognosis and allows for better discussion of surgical risks with the patient.
Roseunbaum et al polled AOFAS members on the treatment of diabetic ankle fractures. (1) For nondisplaced bimalleolar fracture with diabetic neuropathy, respondents preferred casting and nonweightbearing (NWB) for 8-12 weeks. (2) For Weber B fracture dislocation without neuropathy, without syndesmotic injury,
respondents preferred either 1/3 tubular or small fragment locking plates with syndesmotic screws and NWB for 8-12 weeks. (3) For bimalleolar fracture dislocation with neuropathy, without syndesmotic injury, respondents preferred small fragment locking plates with syndesmotic screws and NWB for 8-12 weeks.
Wukich and Kline reviewed the management of ankle fractures in diabetics. They found that neuropathy is more prevalent in patients with ankle fractures than without. They stress that 1% reduction in HbA1C results in 30% reduction in complication rate. Fracture healing is slower, callus is smaller, with less stiffness, tensile strength and collagen content. Amputation rate is up to 5% for patients treated operatively or nonoperatively. Complications are higher in patients with vasculopathy, neuropathy, or Charcot arthropathy.
Incorrect Answers:
Question 3
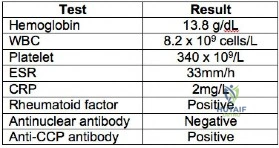
Figures 1 and 2 show the postreduction radiographs obtained from a 32-year-old man who fell from a ladder onto his outstretched right arm. He reports right wrist pain and dense numbness in his radial digits. What is the most appropriate treatment option?

Explanation
This patient sustained a lesser-arc perilunate dislocation. As a result of the injury, he also developed acute carpal tunnel syndrome. The closed reduction attempt was unsuccessful; therefore, this injury is best managed with emergent surgery, an open carpal tunnel release, an open reduction of the perilunate dislocation, scapholunate ligament repair, and intercarpal pinning. Outpatient surgery in a delayed fashion is not advised because of the acuity and severity of the carpal tunnel syndrome. Closed reduction and casting is not advised, because it commonly leads to continued carpal instability with subsequent dorsal
intercalated segment instability deformity and scaphoid lunate advanced collapse wrist arthritis.
Question 4
A cortisone injection in the subacromial space will most likely result in
Explanation
REFERENCES: Matsen FA III, Arntz CT: Subacromial impingement, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 623-646.
Koehler BE, Urowitz MB, Killinger DW: The systemic effects of intra-articular corticosteroid. J Rheumatol 1974;1:117-125.
Question 5
Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of
Explanation
REFERENCE: O’Reilly R, Link M, Fletcher B, et al: NCCN pediatric osteosarcoma practice guidelines: The National Comprehensive Cancer Network. Oncology (Huntingt) 1996;10:1799-1806, 1812.
Question 6
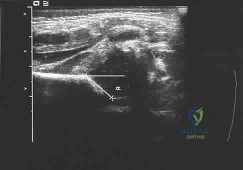
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management? Review Topic
Explanation
not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness.
Question 7
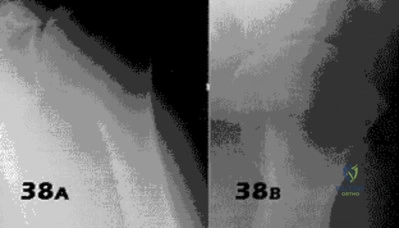
- Figures 38a & 38b show radiographs of a 40 year old man who underwent a Putti-Platt repair for recurrent dislocations at age 22. He reports increasing pain in the shoulder and limited motion for five years. Examination reveals 130 degrees of elevation and 15 degrees of external rotation. Non-surgical treatment has failed. Treatment should now consist of what?
Explanation
Late onset of pain (average 13 years) was noted following this procedure in a small number of patients. The pain is attributed to excessive G-H compressive forces due to limited external rotation. NSAIDS and PT are first line treatments. If these fail, the authors demonstrated good results with release of the anterior structures. Choices 3 & 4 would probably be reserved for patients older than 50 with more advanced signs of degenerative disease.
Question 8
A 54-year-old woman sustains the injury seen in Figures 71a and 71b. The injury involves her nondominant extremity. What should the patient be told regarding her expected outcome?

Explanation
(SBQ12TR.101) An otherwise healthy young adult male sustains a transverse radial shaft and ulna fracture. He undergoes definitive surgical fixation with two nonlocking compression plates (LCPs) as shown in Figure A. What is the principle of this fixation technique on bone healing?

Absolute stability with direct healing by callus formation
Relative stability with indirect healing by callus formation
Absolute stability with direct healing by internal remodeling
Relative stability with indirect healing by internal remodeling
Absolute stability with endochondral bone formation
Definitive surgical fixation for a simple transverse both bone forearm fracture would include open reduction and internal fixation with absolute stability with direct healing by internal remodelling (i.e., primary bone healing). The radius is fixed with a 7-hole
Question 9
What is the most likely long-term sequela of the injury shown in Figures 47a and 47b?
Explanation
REFERENCES: Tucker DJ, Feder JM, Boylan JP: Fractures of the lateral process of the talus: Two case reports and a comprehensive literature review. Foot Ankle Int 1998;19:641-646.
Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1465-1518.
Question 10
A patient undergoes a proximal tibial resection that is reconstructed with a fresh frozen osteoarticular allograft. Eleven months later, the graft is retrieved. Histologically, the articular cartilage and subchondral bone retrieved would be expected to show evidence of
Explanation
REFERENCES: Enneking WF, Campanacci DA: Retrieved human allografts:
A clinicopathological study. J Bone Joint Surg Am 2001;83:971-986.
Enneking WF, Mindell ER: Observations on massive retrieved human allografts.
J Bone Joint Surg Am 1991;73:1123-1142.
Question 11
-Postsurgically, the patient recovers well and is fully rehabilitated. He demonstrates full motion with no instability or pain and is cleared to return to play 12 months after the surgery. He asks for your advice regarding use of a functional brace for playing basketball following his reconstruction. What is the most appropriate recommendation?
Explanation
The athlete most likely suffered an acute ACL rupture however the presence of a lipohemarthrosis is concerning for the possibility of an intraarticular fracture. Because of this, the patient should not be allowed full weight bearing until a fracture is ruled out with radiographs. Given the athlete’s inability to perform a straight leg raise, the extensor mechanism is not functioning and a telescoping knee brace locked in extension should be utilized. A neoprene knee sleeve does not have a role in the
treatment of this acute injury.The radiographs reveal a lateral avulsion fracture off of the proximal tibial epiphysis which is known as a Segond fracture. It is indicative of an ACL injury and the fracture fragment seen is the consequence of the lateral capsule injury sustained during the pivot-shift mechanism. There is no radiographic evidence of a medial tibial plateau fracture. A radiographic sign of a chronic MCL injury is known as a Pellegrini-Stieda lesion and this is seen as calcification of the femoral origin of the MCL. A radiographic sign of an acute LCL rupture would be an avulsion fracture of the tip of the fibula.The MRI shows kissing contusions of the posterolateral tibial plateau and the midpoint of the lateral femoral condyle. These “kissing lesions” are seen as a result of a pivot shift mechanism of injury and are diagnostic for an ACL rupture. The most common associated injury in an acute ACL rupture is a lateral meniscus tear. Medial meniscus tears are more common in chronic ACL injuries. PCL rupture and PLC injury are all associated injuries seen in acute ACL rupture; however, these are much less common than meniscal tears. The team physician has a role in encouraging, but
not demanding, the athlete to report the injury andtreatment to the scholarship school’s coaching staff. What the athlete decides to do is his decision; the physician would be violating the athlete’s HIPAA rights as well as their confidence by reporting it directly to the scholarship school. Clearly the physician should not discourage the athlete from reporting the injury. The athlete is 18 years old and, as such, the physician would need the athlete’s permission to discuss any medical issues with the family in keeping with HIPAA.
The athlete’s exam demonstrates incompetence of both bundles of the ACL as demonstrated by the loss of stability with anterior translation of the tibia (Lachman test) as well as with rotation (pivot shift). The external rotation stress with the knee in 30 degrees of flexion tests the competence of the posterolateral corner while rotation at 90 degrees of flexion tests the PCL. Since the athlete’s knee is stable to posterior drawer testing demonstrating an intact PCL and the external rotation at 30 degrees is equivalent to that at 90 degrees, the posterolateral corner in intact.
The ACL has two separate and distinct bundles, the AM and PL. Each bundle takes on tension at varying degrees of knee flexion and therefore each bundle is thought to have a varying contribution to the stability of the knee. The AM bundle takes on tension with the knee in flexion and the PL bundle is tight in extension. Neither bundle is isometric during knee range of motion. Both bundles have contributions to rotational stability of the knee throughout the range of motion.
The success of traditional trans-tibial single-bundle ACL reconstruction has recently been called into question given the demonstration of persistent rotational instability following reconstruction. The persistence of rotational instability in trans-tibial single bundle ACL reconstruction has been attributed to the location of the graft in a vertically malpositioned femoral tunnel. The goal of double-bundle ACL reconstruction is to more accurately reproduce the native ACL and provide grafts that contribute to anteroposterior stability as well as rotational stability by placing the grafts in more anatomic locations not central in the knee axis. There is an increased cost and surgical time associated with double-bundle reconstruction.
The use of functional braces following ACL reconstruction is a surgeon’s preference because there is no difference in retear rate with or without a brace. Some authors recommend brace use for one to two years following ACL reconstruction for all athletic activities, but this is not supported by the literature. No literature exists showing a higher rate of reinjury with a functional brace and off-the shelf and custom braces have been found to be equivalent leading those who advocate for braces to recommend off-theshelf braces given their significantly lower cost.
Question 12
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Warner JJ, Johnson D, Miller M, Caborn DN: Technique for selecting capsular tightness in repair of anterior-inferior shoulder instability. J Shoulder Elbow Surg 1995;4:352-364.
Question 13
A 38-year-old man is being considered for medial meniscus transplantation following an arthroscopic subtotal meniscectomy performed at the time of ACL reconstruction. His body mass index (BMI) is 28kg/m2. Laboratory tests are shown in Figure A. Standing long-leg radiographs reveal a 4 degree valgus deformity compared with the contralateral side, with the weightbearing line running through the lateral tibial spine. His arthroscopic photos also revealed a 1.7cm wide Outerbridge II chondral lesion over the lateral femoral condyle and synovitis. What factor in this patient is an absolute contraindication to meniscal transplantation? Review Topic
Explanation
Besides inflammatory arthritis, other absolute contraindications include diffuse arthritis, Outerbridge grade IV changes, untreated tibiofemoral subluxation, synovial disease, previous joint infection, skeletal immaturity, or marked obesity.
Lee et al. reviewed meniscal transplantation. They recommend meniscal transplantation only after nonoperative measures (unloading braces, weight loss, activity modification, analgesia) have failed. Indications include young patients (<50yo) with symptoms referable to a meniscus-deficient tibiofemoral compartment, with a stable knee with normal alignment, with intact articular surfaces (grade I or II).
Figure A is a table showing this patient's lab results. He has positive RF and anti-CCP antibody. In addition, he has synovial changes on arthroscopy. These findings are significant for active RA.
Incorrect Answers:
Meniscus transplantation can be attempted if cruciate ligament deficiency was addressed, or there are plans for concurrent or staged reconstruction. Answer 3: Varus/valgus malalignment is not an absolute contraindication although concurrent/staged treatment is necessary to correct alignment. Answer 4: Outerbridge Grade I and II chondral defects are not contraindications. Knees with Outerbridge III lesions may still be considered if defects are focal and concomitant treatment is performed. Answer 5: Marked obesity is a contraindication. This is not present in this individual.
Question 14
What root is most commonly involved with a segmental root level palsy after laminoplasty?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-249.
Uematsu Y, Tokuhashi Y, Matsuzaki H: Radiculopathy after laminoplasty of the cervical spine. Spine 1998;23:2057-2062.
Question 15
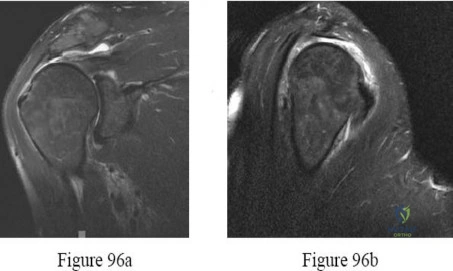
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. A large intra-articular and intrapelvic pseudotumor has developed. What predominant histological feature(s) is/are present in such a lesion?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic
feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 16
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
REFERENCES: Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of twenty cases. J Pediatr Orthop 1990;10:442-444.
Hoffer MM, Wickenden R, Roper S: Brachial plexus birth palsies. J Bone Joint Surgery Am 1978;60:692-695.
Question 17
Which radiographic abnormality most accurately serves as a predictor of ankle syndesmosis disruption?
Explanation
Normal syndesmotic relationships include a tibiofibular clear space smaller than 6 mm on both AP and mortise views. In a 1989 cadaveric study by Harper and Keller, a tibiofibular clear space exceeding 6 mm on both the AP and mortise views was the most reliable predictor of early syndesmotic widening. Tibiofibular overlap is measured 1 cm proximal to the plafond. Normal values exceed 6 mm or 42% of the width of the fibula on the AP view, or 1 mm on the mortise view. Proximal fibula fracture can occur in isolation without syndesmotic injury, frequently after direct trauma. The medial clear space is the distance between the lateral border of the medial malleolus and the medial border of the talus and is measured at the level of the talar dome. In the mortise view with the ankle in neutral dorsiflexion, the medial clear space should be equal to or smaller than the superior clear space between the talar dome and the tibial plafond. ?A normal medial clear space may be present with syndesmotic injury and consequently lacks sensitivity and specificity.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. View Abstract at PubMed
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
Question 18
A polytrauma patient sustains a right bicondylar tibial plateau fracture and a right humeral shaft fracture both treated with open reduction and internal fixation. He also underwent statically locked intramedullary nailing of a left femoral shaft fracture. What is the appropriate weightbearing status?
Explanation
Tingstad et al found favorable results of immediate weightbearing on humeral shaft fractures treated with plating and full weightbearing did not have any effect on the union or malunion rates.
Brumback et al evaluated the feasibility, safety and efficacy of immediate
weightbearing after treatment of femoral shaft fractures with statically locked IM nail. All the patients went on to union and no loss of fixation occurred.
OrthoCash 2020
Question 19
A 10-lb, 2-oz infant who was born via a difficult breech delivery 12 hours ago is now being evaluated for hip pain. Although the infant is resting comfortably, examination reveals that the patient is not moving the right lower extremity and manipulation of the right hip causes the infant to cry. The Galeazzi sign is positive. An AP radiograph of the pelvis shows proximal and superior migration of the right proximal femoral metaphysis. What is the most likely diagnosis?
Explanation
REFERENCES: Weinstein JN, Kuo KN, Millar EA: Congenital coxa vara: A retrospective review. J Pediatr Orthop 1984;4:70-77.
Beaty JH: Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 409-425.
Question 20
A 52-year-old, right hand dominant man comes for evaluation of right shoulder pain that has been intermittently bothering him for three months. The pain is worse with overhead activities. He denies any history of trauma. His range of forward elevation in the plane of the scapula is painful and is limited to 145 degrees, compared to 170 degrees on his unaffected side. A radiograph is shown in Figure A. He saw another orthopedist a month ago, who ordered an MRI, which showed a small, partial thickness supraspinatus tendon tear. He received a subacromial injection of lidocaine at that time which temporarily relieved 90 percent of the pain he felt with passive forward elevation of his shoulder past 90 degrees. Today he is requesting a subacromial injection of platelet rich plasma (PRP). You tell him that with regard to pain, function and range of motion, subacromial injection of PRP: Review Topic

Explanation
PRP injection.
Platelet rich plasma has been used for the treatment of chronic tendinopathy in different areas with mixed results. No benefit to patients with symptoms of subacromial impingement has been demonstrated for subacromial injection of PRP, when added to a standard therapy program.
Kesikburun et al. conducted a randomized controlled trial in which patients with rotator cuff tendinopathy or partial rotator cuff tears were randomized to receive ultrasound-guided subacromial injection of either PRP or lidocaine, followed by a standard six-week therapy program. The authors found no difference in pain, range of motion or validated outcome scores at one year follow up.
Hall et al. reviewed sports medicine applications for PRP. At that time (2009), with regard to PRP, they concluded that there was "little clinical evidence for its use."
Ketola et al. sought to determine the effectiveness of subacromial decompression for the treatment of subacromial impingement syndrome. They randomized 140 patients to a supervised exercise program or arthroscopic subacromial decompression followed by a supervised exercise program. They found no clinically important differences between the two groups at 24 months follow up.
Figure A shows a right shoulder radiograph without osseous pathology. Incorrect answers:
Question 21
The structure that runs just beneath the peroneal tubercle of the calcaneus is the
Explanation
The peroneal tubercle is often a good landmark at which to identify the peroneus longus tendon surgically, and a hypertrophic tubercle has been associated with peroneus longus tendinopathy. Both peroneal tendons curve anteriorly around the tip of the fibula, with the peroneal tubercle separating the 2 tendons at the level of the calcaneus. The peroneus brevis runs in front of the tubercle and the longus behind. The flexor hallucis longus runs through a fibro-osseus tunnel posterior to the hindfoot formed by the posterolateral (os trigonum) and posteromedial tubercle of the talus. The calcaneal fibular ligament attaches to the calcaneus below the posterior facet of the subtalar joint and deep to the peroneal tendons.
RECOMMENDED READINGS
Hyer CF, Dawson JM, Philbin TM, Berlet GC, Lee TH. The peroneal tubercle: description, classification, and relevance to peroneus longus tendon pathology. Foot Ankle Int. 2005 Nov;26(11):947-50. Pub PMID: 16309609.View Abstract at PubMed
Bruce WD, Christofersen MR, Phillips DL. Stenosing tenosynovitis and impingement
of the peroneal tendons associated with hypertrophy of the peroneal tubercle. Foot Ankle Int. 1999 Jul;20(7):464-7. PubMed PMID: 10437932.View Abstract at PubMed
Question 22
Figures 38a and 38b
Explanation
Inversion of the ankle can cause various injuries about the foot and ankle, all via the same mechanism. Fifth metatarsal base avulsion (Figure 35) fractures can be treated with use of a walking boot until pain subsides. Jones fractures (Figure 36) can be treated with surgical or nonsurgical treatment, although young, active patients are perhaps better treated with ORIF, which can decrease disability time. Treatment of an anterior process calcaneus fracture (Figure 37) is similar to that for a fifth metatarsal base avulsion fracture. Figures 38a and 38b show a calcaneal fracture-dislocation, which necessitates ORIF.
RECOMMENDED READINGS
Schepers T, Backes M, Schep NW, Carel Goslings J, Luitse JS. Functional outcome following a locked fracture-dislocation of the calcaneus. Int Orthop. 2013 Sep;37(9):1833-8. PubMed PMID: 23959223. View Abstract at PubMed
Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. View Abstract at PubMed
Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. View Abstract at PubMed
Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. View Abstract at PubMed
Question 23
During a Lisfranc (tarsometatarsal) amputation of the foot, which of the following is crucial to prevent the patient from having a supinated foot during gait.

Explanation
Illustration B depicts the level of a Lisfranc amputation of the foot. Incorrect Answers:
The posterior tibialis is the primary supinator of the foot, and releasing it would lead to an eversion deformity. The tibialis posterior tendon attachment to the bases of the second and third metatarsals will actually be released with this amputation, but the main attachment to the navicular preserved. 3-The anterior tibialis dorsiflexes and inverts the foot, but transferring it to the medial and middle cuneiforms would mimick its native function to dorsiflex and invert the foot. 4-A lengthened Achilles would lead to increased dorsiflexion, not supination. 5-Osteotomy of 2nd MT is crucial to preserve the medial cuneiform and midfoot stable.
Question 24
An active 23-year-old man has right groin pain that increases with sports activity. Examination reveals decreased internal rotation of the affected hip. He has a positive impingement test and radiographs reveal no crossover sign. An MRI scan is most likely to reveal which of the following? Review Topic
Explanation
Question 25
-Figures 14a through 14d are the radiographs and sagittal T1- and T2-weighted MRI scans of an otherwise healthy 10-year-old girl who has experienced 3 weeks of worsening pain with weight bearing and is now refusing to bear weight to either of her lower extremities. She denies any history of injury or trauma.She has not had any fevers or recent illnesses. She denies any numbness or parasthesias. She has had no bowel or bladder incontinence. In the emergency department she is afebrile and tender to palpation over the midlumbar spine. She has pain with hyperextension and flexion of her back. Her white blood cell count is 11.4 (reference range, 4.5-11.0 x109/L), erythrocyte sedimentation rate is 40 mm/h (reference range, 0-20 mm/h), and C-reactive protein is 2.6 mg/L (reference range, 0.08-3.1 mg/L). What is the most appropriate course of action at this time?

Explanation

Question 26
An 80-year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 27
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
Explanation
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Baker CL, Uribe JW, Whitman C: Arthroscopic evaluation of acute initial anterior shoulder dislocations. Am J Sports Med 1990;18:25-28.
Question 28
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of
Explanation
shown some healing response with callus formation, but these techniques are not successful
in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions
of the clavicle.
REFERENCES: Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 29
When performing a Weil osteotomy of a lesser metatarsal, the desired angle of the saw cut should be approximately
Explanation
REFERENCES: Trnka H, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Grimes J, Coughlin M: Geometric analysis of the Weil osteotomy. Foot Ankle Int 2006;27:985-992.
Question 30
A Canale view best visualizes which of the following structures?
Explanation
REFERENCES: Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Bruden B: Roentgen examination of the subtaloid joint in fractures of the calcaneus. Acta Radiol 1949;31:85-91.
Question 31
A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches
Explanation
REFERENCES: Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements and outcome. J Trauma 1989;29:981-1000.
Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center. J Trauma 1997;42:695-700.
Gilliland MD, Ward RE, Barton RM, et al: Factors affecting mortality in pelvic fractures.
J Trauma 1982;22:691-693.
Question 32
A 55-year-old woman is referred for evaluation of a painful knee replacement. She underwent total knee arthroplasty (TKA) more than 1 year ago without perioperative complications but has had consistent pain since the surgery. The patient’s preoperative radiographs and postoperative radiographs are shown in Figures below. Examination reveals medial laxity during valgus stress testing and range of motion of 0° to 70°. Her erythrocyte sedimentation rate and C-reactive protein level are normal. What is the best next step?

Explanation
The radiographs show substantial valgus malalignment of the femoral component, with lateral mechanical axis deviation. Clinically, by examination she displays instability and stiffness as a result. Revision knee replacement is appropriate and should consist of total revision to stemmed femoral and tibial components with a varus-valgus constrained insert, given the likely attenuation of the medial collateral ligament. Open debridement with ligament balancing and polyethylene exchange do not address the underlying cause and are inappropriate. Distal femoral osteotomy is not useful in the setting of previous total knee replacement. Nonsurgical treatment with an unloader brace would be ineffective in correcting the alignment.
Question 33
A 12-year-old boy reports knee discomfort after prolonged strenuous activities. He denies knee swelling or catching and has no pain with activities of daily living. A radiograph is shown in Figure 4. Prognosis for the pathology shown is most influenced by
Explanation
REFERENCES: Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
Question 34
A 53-year-old woman reports a 4-month history of gradual onset diffuse shoulder pain and limited function. She has had no prior treatment, and her medical history is unremarkable. Examination reveals globally painful active range of motion to 120 degrees forward elevation, 25 degrees external rotation with the arm at the side, and internal rotation to the sacrum. Passive range of motion is also limited in comparison with the contralateral shoulder. Radiographs are shown in Figures 31a through 31c. What is the most appropriate management? Review Topic

Explanation
Question 35
A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of 25 degrees. The O’Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management? Review Topic
Explanation
Question 36
An 18-year-old football player reports acute pain and swelling after a direct injury to his plantar flexed foot. Examination reveals midfoot swelling and tenderness. Nonstanding radiographs are normal. What is the next most appropriate step in management?
Explanation
to activity.
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries with the transmetatarsal joint. Orthop Clin North Am 2001;32:11-20.
Question 37
Cell signaling through the activation of a transmembrane receptor complex formed by serine/threonine kinase receptors occurs with which of the following growth factors?
Explanation
REFERENCES: Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
Schmitt JM, Hwang K, Winn SR, et al: Bone morphogenetic proteins: An update on basic biology and clinical relevance. J Orthop Res 1999;17:269-278.
Question 38
During a posterior approach to the right Achilles tendon, the surgeon encounters a nerve running with the small saphenous vein as shown in Figure 22. This nerve innervates what part of the foot?
Explanation
REFERENCES: Aktan Ikiz ZA, Ucerler H, Bilge O: The anatomic features of the sural nerve with an emphasis on its clinical importance. Foot Ankle Int 2005;26:560-567.
Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 39
Survival rates for children with soft-tissue sarcoma other than rhabdomyosarcoma are best correlated with
Explanation
REFERENCES: Rao BN: Nonrhabdomyosarcoma in children: Prognostic factors influencing survival. Semin Surg Oncol 1993;9:524-531.
Andrassy R, et al: Non-rhabdomyosarcoma Soft-Tissue Sarcomas: Pediatric Surgical Oncology. Philadelphia, PA, WB Saunders, p 221.
Question 40
A 70-year-old healthy man had total knee arthroplasty 18 years ago, and it now is painful. Radiographs reveal aseptic loosening and the range of motion before surgery is 15 to 85 degrees. The strongest indication for performing a tibial tubercle osteotomy to aid in exposure in his knee would be
Explanation

Question 41
A 65-year-old man has a painful and often audible crepitus after undergoing a total knee arthroplasty 8 months ago. His symptoms are reproduced with active extension of about 30°. Examination reveals no effusion or localized tenderness, a stable knee, and a range of motion of 5° to 120°. Radiographs are shown in Figures 37a and 37b. Management should consist of
Explanation
REFERENCES: Beight JL, Yao B, Hozack WJ, Hearn SL, Booth RE Jr: The patellar “clunk” syndrome after posterior stabilized total knee arthroplasty. Clin Orthop 1994;299:139-142.
Lintner DM, Bocell JR, Tullos HS: Arthroscopic treatment of intra-articular fibrous bands after total knee arthroplasty: A follow-up note. Clin Orthop 1994;309:230-233.
Question 42
82 • American Academy of Orthopaedic Surgeons A 12-year-old girl is seen for left ankle pain. Radiographs reveal osteochondritis dissecans (OCD) involving the talus. What should the parents be told regarding management?
Explanation
REFERENCES: Perumal V, Wall E, Babekir N: Juvenile osteochondritis dissecans of the talus. J Pediat Orthop 2007;27:821-825.
Letts M, Davidson D, Ahmer A: Osteochondritis dissecans of the talus in children. J Pediatr Orthop 2003;23:617-625.
Question 43
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 44
- Which of the following procedures is associated with the highest risk of osteonecrosis of the metatarsal head?
Explanation
Question 45
Figure 3 shows the radiographs of a 32-year-old man who fell 12 feet onto his outstretched arm and sustained a fracture-dislocation of the elbow. Initial management consisted of closed reduction of the dislocation. Surgical treatment should now include repair or reduction and fixation of the
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
O’Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Question 46
A 27-year-old professional rugby player is sprinting down the field during a game and sustains a twisting injury to his right knee with immediate onset of swelling, pain, and difficulty with ambulation. Imaging of his right knee is demonstrated in Figures A, B, and C. Which of the following structures has most likely been injured? Review Topic

Explanation
The ACL is the most commonly injured knee ligament, with an incidence of between
100,000 and 200,000 ruptures per year in the United States. The majority of ACL tears occur from non-contact athletic injuries. Acute ACL tears are associated with lateral meniscal tears. Physical examination findings include positive Lachman and Pivot shift tests. Imaging includes radiographs which are usually normal; however, the presence of a Segond fracture (avulsion fracture of the proximal lateral tibia) is pathognomonic for an ACL rupture and represents bony avulsion by the anterolateral ligament (ALL). MRI demonstrates bone bruising of the middle third of the lateral femoral condyle (sulcus terminalis) and posterior third of the lateral tibial plateau in more than 50% of acute ACL tears.. Bone bruise patterns correlate with the direction of the abnormal anterior translation and abutment of the posterolateral tibia against the middle third of the lateral femur during the injury. Treatment options include nonoperative management with physical therapy and lifestyle modification or operative intervention if failure of conservative measures.
Bathala et al present a radiologic case study of a Segond fracture visualized on AP radiograph of the knee of a patient who sustained an ACL rupture. They discuss the critical nature of this finding and the need for further imaging, as it is associated with ACL tears, meniscal tears, and damage to structures in the posterolateral corner.
Viskontas et al discuss different patterns of bone bruising demonstrated on MRI in acute anterior cruciate ligament ruptures of 100 patients, 86 with non-contact and 14 with contact injuries. They found that the non-contact mechanism correlates with more severe bone bruising in both the medial and lateral compartments as demonstrated on MRI.
Figures:
Figure A - AP radiograph of the knee that demonstrates a Segond fracture Figures B and C - coronal T1 and T2 MRI slices that demonstrate bone bruising of the middle third of the lateral femoral condyle and posterior third of the lateral tibial plateau
INCORRECT ANSWERS:
Question 47
A 17-year-old high school gymnast who has peripatellar knee pain has been unable to practice on a consistent basis for the past 3 years. She denies any specific injury events. Physical therapy for modalities, quadriceps strengthening, and hamstring stretching provide temporary relief. A trial of patellar taping significantly reduces her pain. Examination reveals an 15-degree Q angle, moderate lateral facet tenderness, negative patellar apprehension, and the inability to evert the patella. Radiographs show a moderate lateral patellar tilt. Treatment should now consist of
Explanation
REFERENCES: Gambardella RA: Techical pitfalls of patellofemoral surgery. Clin Sports Med 1999;18:897-903.
Post WR: Clinical evaluation of patients with patellofemoral disorders. Arthroscopy 1999;15:841-851.
Question 48
A 27-year-old man has had pain in the right index finger for the past 9 months. The pain is completely relieved with ibuprofen. An AP radiograph and CT scan are shown in Figures 80a and 80b. What is the most likely diagnosis?
Explanation
radiolucent nidus. A small area of calcification may be present within the center of the nidus. The radiolucent nidus is surrounded by a thick rim of sclerotic bone. These diagnostic
features are frequently better seen on CT. An increase in cyclooxygenase activity has been demonstrated within osteoid osteomas, which may explain why aspirin and other nonsteroidal anti-inflammatory drugs classically relieve the pain associated with these lesions.
REFERENCES: Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 121-130.
Question 49
A 31-year-old man sustained an unstable closed left posterior hip dislocation in a motorcycle accident. A postreduction radiograph is shown in Figure 51a. 3-D CT scans are shown in Figures 51b and 51c. What is the optimal surgical approach that will allow for the most appropriate treatment?

Explanation
Question 50
A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals
Explanation
REFERENCES: Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Iannotti JP, Zlatkin MB, Esterhai JL, et al: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29.
Question 51
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral Review Topic
Explanation
Question 52
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle?
Explanation
REFERENCES: Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop Relat Res 1999;368:17 -27.
Warner JJ, Navarro RA: Serratus anterior dysfunction: Recognition and treatment. Clin Orthop Relat Res 1998;349:139-148.
Question 53
A 53-year-old woman has severe neck and left shoulder pain after a rollover motor vehicle accident. Radiographs and a CT scan of the cervical spine are shown in Figures 34a through 34c. Management should consist of
Explanation
REFERENCES: Levine AM, Mazel C, Roy-Camille R: Management of fracture separations of the articular mass using posterior cervical plating. Spine 1992;17:S447-S454.
Levine AM: Facet fractures and dislocations, in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 360-362.
Whitehill R, Richman JA, Glaser JA: Failure of immobilization of the cervical spine by the halo vest: A report of five cases. J Bone Joint Surg Am 1986;68:326-332.
Garvey TA, Eismont FJ, Roberti LJ: Anterior decompression, structural bone grafting, and Caspar plate stabilization for unstable cervical spine fractures and/or dislocations. Spine 1992;17:S431-S435.
Question 54
A displaced pediatric supracondylar humerus fracture is treated with closed manipulation and placement of 2 Kirschner wires placed from the lateral side. What would be the effect of adding a third pin from the lateral side? Review Topic
Explanation
Question 55
Which of the following treatments for osteoporosis is a direct inhibitor of RANK ligand (RANK-L)?
Explanation
RANKL (Receptor activator of nuclear factor kappa-B ligand) is a key molecule for osteoclast differentiation and activation. Inhibition of RANKL activity with anti-RANKL antibody reduces osteoclastogenesis, resulting in inhibition of bone resorption.
Capozzi et al. author a review article on denosumab. They state the medication confers improved bone mineral density and prevents new fragility fractures similar to alendronate. However, denosumab presents less risk of atypical femoral fractures and
osteonecrosis of the jaw.
Yasuda et al. present a review that details the creation of three elegant animal models to mimic metabolic bone disease and how the animal models can create a template to help cure human metabolic bone disease. These enable modeling of osteoporosis, hypercalcemia, and osteopetrosis by treating normal mice with soluble RANKL (sRANKL), adenovirus expressing sRANKL, and anti-mouse RANKL neutralizing antibody, respectively. They report that these animal models can be established in about 14 days using normal mice.
Illustration A demonstrates the mechanism of action of bisphosphonates and denosumab.
Incorrect Answers:
1: Romosozumab is the first humanized anti-sclerostin monoclonal antibody that has been demonstrated to increase bone formation. 2: Zoledronic acid (Reclast) is a nitrogen containing bisphosphonates that inhibits osteoclast resorption by inhibiting the enzyme farnesyl diphosphate synthase. 4: Teriparatide (Forteo) comprises the first 34 amino acids of the 84 amino acid parathyroid hormone (PTH) and can reproduce the primary effects of PTH by activating adenyl cyclase. 5: Blosozumab is an investigational monoclonal anti-sclerostin antibody showing osteoanabolic properties with the potential to improve clinical outcomes in patients with osteoporosis.
Question 56
Figure 1 shows the radiograph of an 11-year-old boy who stubbed his great toe while playing soccer barefoot. He is able to walk home despite a small amount of bleeding at the nail fold. Management should consist of
Explanation
the fracture.
REFERENCES: Noonan KJ, Saltzman CL, Dietz FR: Open physeal fractures of the distal phalanx of the great toe: A case report. J Bone Joint Surg Am 1994;76:122-125.
Banks AS, Cain TD, Ruch JA: Physeal fractures of the distal phalanx of the hallux. J Am Podiatr Med Assoc 1988;78:310-313.
Question 57
You perform an ACL reconstruction with bone-patella tendon-bone (BTB) autograft and are explaining the postoperative rehabilitation protocol to your patient. Which of the following is associated with increased quadriceps volume and improved quadriceps strength at 1 year without a higher risk of knee instability? Review Topic
Explanation
Proper rehabilitation following ACL reconstruction is vital to a successful outcome. The cornerstone of ACL rehabilitation is range of motion, strengthening and functional exercises without risk of destabilizing the knee. There are a variety of rehabilitation protocols and recently an effort has been made to standardize the approach to postoperative ACL care. An accelerated protocol starting at 3 weeks postoperatively has been deemed safe and may enhance the speed and safety with which an athlete returns to play.
Kruse et al completed a meta-analysis of 29 Level I and II studies focused on the ACL rehabilitation process. The authors concluded that immediate postoperative weightbearing and knee range of motion 0-90 is safe. Early eccentric strengthening appears to accelerate and improve strength gains at 1 year as compared to delayed eccentric strengthening. Home-based rehabilitation programs can be as effective as formal physical therapy. Postoperative bracing and CPM use is neither necessary nor beneficial.
Van Grinsven et al conducted a systematic review of ACL rehabilitation programs and physical therapy modalities to develop an evidence-based rehabilitation protocol. The authors demonstrated that an accelerated protocol without postoperative bracing focused on reduction of pain, swelling and inflammation and regaining range of motion, strength and neuromuscular control has significant advantages and does not lead to stability problems.
Gerber et al performed a randomized trial comparing two accelerated postoperative rehabilitation protocols – early eccentric (ECC) rehabilitation versus traditional (TRAD) rehabilitation starting at 3 weeks. There were no significant differences in knee pain, effusion or stability. However, quadriceps strength, hopping distance and activity level improved by a significantly greater amount in the ECC group versus the TRAD group at 26 weeks postoperatively. In a separate analysis of these patients, quadriceps and gluteus muscle cross-sectional area and volume in ECC patients were more than twice those in the TRAD group.
Illustration A depicts two eccentric ergometers that can be used in postoperative ACL rehabilitation.
Incorrect Responses:
another Answer
type of brace,
2:
There
duration is
of
bracing or no bracing at all.
no
advantage
to
CPM
use.
Question 58
Figure 3 shows the clinical photograph of a wrestler who has an acute mass in his ear. He does not wear protective headgear. The area is mildly tender and without erythema. Management should consist of
Explanation
REFERENCES: Kaufman BR, Heckler FR: Sports-related facial injuries. Clin Sports Med 1997;16:543-562.
Griffin CS: Wrestler’s ear: Pathophysiology and treatment. Ann Plastic Surg 1992;28:131-139.
Question 59
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and
Explanation
REFERENCES: Smith CS, Nork SE, Sangeorzan BJ: The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-2424.
Brewster NT, Maffulli N: Reimplantation of the totally extruded talus. J Orthop Trauma 1997;11:42-45.
Question 60
-A 23-year-old man had a laparotomy and splenectomy with packing of the abdomen after a motorcycle collision. Laboratory studies show a hemoglobin level of 7.1 g/dL (reference range [rr], 14.0-17.5 g/dL) and a lactate level of 8.0 mmol/L (rr, 0.6-1.7 mmol/L). He also has a left humeral fracture,an anteroposterior compression I pelvic fracture, bilateral distal third femur fractures, and an open GustilotypeIIIA tibial diaphysis fracture with moderate contamination. What is the most appropriate treatment to administer before leaving the operating room?
Explanation

Question 61
Figures 34a and 34b show the clinical photograph and a weight-bearing radiograph of a patient with diabetes mellitus who has had recurrent ulcers under the head of the talus that have previously resolved with a series of non-weight-bearing total contact casts. The deformity does not correct passively. Dorsalis pedis and posterior tibial pulses are palpable. The patient is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. The ulcer is currently healed. What is the best option to prevent recurrent ulceration and infection?
Explanation
REFERENCES: Bevan WP, Tomlinson MP: Radiographic measures as a predictor of ulcer formation in diabetic charcot midfoot. Foot Ank Int 2008;29:568-573.
Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Pinzur M: Surgical versus accommodative treatment for Charcot arthropathy of the midfoot.
Foot Ankle Int 2004;25:545-549.
Question 62
What muscle attaches to the site shown by the arrow in Figure 2?
Explanation
REFERENCES: Williams PL, Warwick R, Dyson M, Bannister LH: Neurology, in Gray’s Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 1131-1132.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 131-132.
Question 63
Which of the following statements is correct regarding Vitamin D?
Explanation
Vitamin D is paramount to proper calcium homeostasis and has important clinical implications in the orthopaedic patient. Vitamin D3 is synthesized in the skin and is converted to 25-hydroxycholecalciferol in the liver. 25-hydroxycholecalciferol is then converted in the kidney into 1,25-dihydroxycholecalciferol, the active form of vitamin
D. The best test to determine Vitamin D deficiency is the measurement of 25-hydroxycholecalciferol, as it has a longer half-life and circulating levels are 1,000x more than 1,25-dihydrocholecalciferol.
Patton et al. review the importance of Vitamin D in the orthopaedic patient. They discuss the implications of Vitamin D deficiency, and urge orthopaedic surgeons to be proficient in both the diagnosis and treatment of the condition.
Bogunovic et al. measured the levels of 25-hydroxycholecalciferol in 723 patients who were to undergo orthopaedic surgery. 40% of these patients were noted to be deficient in Vitamin D, with the highest rates in patients scheduled to undergo trauma and sports surgery.
Illustration A reviews Vitamin D metabolism. 24,25-dihydroxycholecalciferol is referred to as pre-Vitamin D.
Incorrect Answers:
Question 64
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
in intestinal absorption and an increase in urinary calcium loss. The reduction of
intestinal absorption is accompanied by reduced circulating concentrations of total, but
not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial.
REFERENCES: Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Reid IR: Menopause, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 55-57.
Question 65
A 38-year-old man who is an avid tennis player has had persistent pain over the medial aspect of his knee for the past 6 years. He notes that the pain occurs on a daily basis with any significant activity. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 22a and 22b. What is the best course of action?
Explanation
REFERENCES: Nagel A, Insall JN, Scuderi GR: Proximal tibial osteotomy: A subjective outcome study. J Bone Joint Surg Am 1996;78:1353-1358.
Rinonapoli E, Mancini GB, Corvaglia A, et al: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Manifold SG, Kelly MA, Richardson L, et al: Osteotomies about the knee, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 947-961.
Question 66
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of
Explanation
REFERENCES: Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 67
Contracture of which structure causes hammertoe deformity?
Explanation
A patient with a flexible hammertoe deformity has the deformity while standing, but practically no deformity when seated with the foot in equinus. The metatarsophalangeal joint is not involved. The deformity is created by contracture of the flexor digitorum longus tendon.
RECOMMENDED READINGS
Coughlin MJ. Lesser toe abnormalities. Instr Course Lect. 2003;52:421-44. Review. PubMed PMID: 12690869.View Abstract at PubMed
Couglin MJ. Lesser toe deformities. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 1. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:363-464.
Question 68
Haversian canals are found in the center of an osteon in compact bone. They contain blood vessels and nerves.
Explanation
amputations have several options to optimize ambulation including solid, energy storing, and multi-axial prothesis.
Aaron et al. reviews the important considerations for patient specific prostheses and new developments on the horizon to maximize ambulation in prosthesis users.
Mesenchymal stem cells have the capacity to differentiate into all the following cell types EXCEPT?
Osteoclasts
Chondrocytes
Adipocytes
Osteoblasts
Fibroblasts
Mesenchymal stem cells are multipotent stem cells which retain the ability to self-renew and to form cells of the mesenchymal lineage. They can therefore form muscle, fat, tendon (made from fibroblasts), bone, cartilage, and the marrow stromal cells. Mesenchymal stem cells do not however form osteoclasts, which are formed from the monocyte lineage - from hematopoietic stem cells.
Caterson et al review the use of mesenchymal stem cells in tissue engineering and regeneration of musculoskeletal tissue.
A 60 year-old male was brought into the operating room for total hip replacement. Before making the incision, what precautionary procedure must be performed by the entire staff to minimize surgical error?
Mark the word "No" on the nonoperative extremities
Use intraoperative fluoroscopic imaging
Perform "timeout"
Have blood products ready in the operating room
Use the newest prosthesis
Surgical "timeout" is now part of the standard procedure which must be performed before starting surgery to minimize surgical error such as wrong site surgery.
Which of the following statements regarding articular cartilage is TRUE?
Cartilage is an isotropic material
Most of the water in articular cartilage exists in the deep layer next to the calcified cartilage
Cartilage only heals if the injury does not pass through the tidemark
Calcified cartilage is the only place that type IV collagen is found
Cartilage exhibits stress shielding of the solid matrix components
Cartilage exhibits significant stress shielding of the solid matrix components due to its high water content, the non-compressibility of water, and the structural organization of collagen and proteoglycans. Cartilage is composed of a permeable porous matrix and 65 to 80% of the total weight of articular cartilage is made up of water. A pressure gradient causes the water to flow through the porous-permeable solid matrix. Significant flow of fluid through the solid matrix requires high hydrodynamic pressures because of the low
permeability of the solid matrix.
The other answers are incorrect because cartilage is anisotropic, most of the water is located in the superficial layers, it only heals if the injury does pass through the tidemark, type X collagen is found in calcified cartilage and is thought to be involved in mineralization. Type IV collagen is found in the basal lamina.
A 38-year-old patient presents 6 months after intramedullary nailing of a distal third tibia fracture with symptoms consistent with complex regional pain syndrome. During the early stage of the disease he was treated with intermittent splinting, elevation and massage, contrast baths, and transcutaneous electrical nerve stimulation. Despite these modalities, he continues to have severe and debilitating symptoms. Which of the following treatment options is indicated as a second line of treatment?
Long leg cast immobilization for 3 months
Walking boot with non weight bearing for three months
Exchange nailing to stimulate healing response to the limb
Epidural spinal cord stimulator
Surgical sympathectomy of the affected limb
Complex regional pain syndrome is a chronic progressive disease of unknown etiology characterized by pain, swelling and skin changes. If nonoperative modalities fail, a surgical sympathectomy of the affected limb is indicated.
The first line of treatment is physical therapy including intermittent splinting, elevation and massage, contrast baths, and transcutaneous electrical nerve stimulation. Aggressive passive range-of-motion exercises should be avoided. If nonoperative modalites fail and symptoms remain severe, a surgical sympathectomy of the affected limb is indicated.
Keys to successful treatment include early clinical suspicion and treatment. Late CRPS is highly refractory to treatment and often results in permanent disability.
Two forms of Complex regional pain syndrome exist: 1) Reflex sympathetic dystrophy
- which does not demonstrate nerve lesions, and 2) Causalgia - which is associated with damage to peripheral nerves. Diagnostic criteria include:
Major criteria: intense and prolonged pain, swelling, stiffness, and discoloration (vasomotor disturbances).
Minor criteria: trophic changes, osseous demineralization, temperature changes, and palmar fibromatosis.
Tran et al present their systemic review of 41 RCTs of the research regarding treatment of CRPS. Their data suggest that only bisphosphonates offer clear medicinal benefits in the treatment of CRPS. Evidence regarding a beneficial effect of lumbar sympathetic blocks, gabapentin, and physical therapy is lacking. As such, these authors advocate for further study thru well-designed RCTs to better evaluate appropriate and effective treatment strategies.
You are planning an intramedullary nail to treat a geriatric patient with a peritrochanteric femur fracture. Which of the following preoperative considerations is correct regarding your implant?
The radius of curvature of an intramedullary nail is generally greater than the radius of curvature of the femur
Closed section nails have less stiffness than slotted nails
The medial/lateral nail starting point relative to the greater trochanter does not affect varus/valgus position in the fracture
The bending stiffness of your nail is proportional to the second power of the radius
Intramedullary nails allow for mostly direct intramembranous bone healing
The radius of curvature of an intramedullary nail is generally greater than the radius of curvature of the femur, which is why anterior distal femur
penetration is a known complication of intramedullary nailing procedures.
Egol et al. evaluated the radius of curvature of 948 femurs (474 matched pairs) and compared those data with current intramedullary nails. He found the average femoral anterior radius of curvature was 120 cm (± 36 cm)
whereas the radius of curvature of the intramedullary nails ranged from 186 to 300 cm.
The other answers are incorrect because closed section nails have more stiffness than slotted nails. The starting position on the greater trochanter greatly affects the post- operative varus/valgus of the fracture. Intramedullary nails allow for mostly indirect enchondral bone healing due to relative motion at the fracture site.
All of the following antibiotics function by interfering with protein synthesis by inhibiting ribosomes EXCEPT
gentamicin
tobramycin
vancomycin
erythromycin
linezolid
Gentamicin and tobramycin are aminoglycosides that function by inhibition of bacterial protein synthesis via irreversible binding to ribosomal subunits. Erythromycin functions by binding to the 50s subunit of the bacterial 70s rRNA complex and thereby inhibits protein synthesis. Linezolid binds to the 23s portion of the ribosomal subunit and inhibits protein synthesis. In contrast, Vancomycin acts by inhibiting proper cell wall synthesis and does not inhibit the ribosome.
The bending rigidity of the implant shown in Figure A is proportional to what power of the measured radius of the implant?
Question 69
A patient was treated with a revision reamed intramedullary nail for a nonunion 6 months ago. A current radiograph is shown in Figure 62. Based on these findings, what is the most appropriate treatment?
Explanation
REFERENCES: Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nails for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Bellabarba C, Ricci WM, Bolhofner BR: Results of indirect reduction and plating of femoral shaft nonunions after intramedullary nailing. J Orthop Trauma 2001;15:254-263.
Question 70
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be
Explanation
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Martin SD, Warren RF, Martin TL, Kennedy K, O’Brien SJ, Wickiewicz TL: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 71
Figure 37 shows a coronal T2-weighted MRI scan. What is the name of the labeled torn structure?
Explanation
are intact.
REFERENCES: Potter HG, Weiland AJ, Schatz JA, et al: Posterolateral rotatory instability of the elbow: Usefulness of MR imaging in diagnosis. Radiology 1997;204:185-189.
King JC, Spencer EE: Lateral ligamentous instability: Techniques of repair and reconstruction. Techniques in Orthopaedics 2000;8:93-104.
Question 72
In a pilon fracture, the Chaput fragment typically maintains soft tissue attachment via which of the following structures?

Explanation
Question 73
A 45-year-old man is seeking evaluation of an injury sustained in a motor vehicle accident 10 weeks ago. Current radiographs are shown in Figures 2a and 2b. Based on the radiographic findings, what is the most likely diagnosis?
Explanation
REFERENCES: Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J: Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-1029.
Berlet GC, Lee TH, Massa EG: Talar neck fractures. Orthop Clin North Am 2001;32:53-64.
Question 74
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?
Explanation
REFERENCES: Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 75
The use of radiation therapy is most effective in metastatic bone disease from which of the following tumors?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
Riley LH III, Frassica DA, Kostuik JP, Frassica FJ: Metastatic disease to the spine: Diagnosis and treatment. Instr Course Lect 2000;49:471-477.
Question 76
A 13-year-old girl has had right groin pain for the past 3 weeks. She denies any history of trauma. Examination of the hip reveals no palpable soft-tissue mass or lymphadenopathy, and there is full range of motion. A plain radiograph and MRI scan are shown in Figures 15a and 15b. Biopsy specimens are shown in Figures 15c and 15d. What is the most likely diagnosis?
Explanation
REFERENCES: Enneking WF, Gearen PF: Fibrous dysplasia of the femoral neck: Treatment by cortical bone grafting. J Bone Joint Surg Am 1986;68:1415-1422.
Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
Question 77
A 43-year-old woman has a 2-week history of right shoulder pain. She denies any injury to initiate her symptoms but states that she has shoulder pain with range of motion and lifting objects. Examination reveals mild pain with abduction, empty can testing, and with the Neer and Hawkins impingement tests. Her range of motion with the right shoulder reveals passive forward flexion to 90 degrees, abduction to 90 degrees, external rotation at the side to 15 degrees, and internal rotation to her buttock. The uninvolved left shoulder has forward flexion to 160 degrees, abduction to 150 degrees, external rotation at the side to 60 degrees, and internal rotation to T6. Radiographs of the shoulder are normal. What is the next most appropriate step in management? Review Topic
Explanation
Question 78
A 7-year-old girl is hit by a motor vehicle and sustains the isolated ipsilateral injuries shown in Figures 16a and 16b. What is the optimal definitive method of treatment? Review Topic

Explanation
Question 79
For the athlete performing heavy exercise, the magnitude of core temperature and heart rate increase is most proportional to
Explanation
REFERENCES: Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524.
Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Sawka MN, Young AJ, Francesconi RP, et al: Thermoregulatory and blood responses during exercise at graded hypohydration levels. J Appl Physiol 1985;59:1394-1401.
Question 80
During fracture healing, granulation tissue tolerates the greatest strain before failure so that mature bone can eventually bridge the fracture gap during healing. What is the definition of strain?
Explanation
The mechanical environment at the fracture site has a major influence on fracture healing. Granulation tissue can withstand higher strain, which stabilizes the mechanical environment and forms a scaffold on which cartilage and bone eventually form; this occurs after strain decreases incrementally. Optimal healing, however, depends on duration, rate, timing and type of mechanical influence. Bone is formed by osteoblasts that are adapted to the very low strains of over 1% change in length. Osteoblast synthesis and proliferation is stimulated at uniaxial strain of between 0.3% and 2.8%. It is known that limited inter-fragmentary movement of 0.2 mm to 1 mm is optimal for fracture healing, resulting in promotion of callus and increase in rigidity. Excessive movement, on the other hand, prolongs fracture healing. Researchers have identified that tissue strain of 2% is suitable for primary bone healing and secondary bone healing takes place at tissue strain of 2-10%. Strain of 10-100% results in fibrous tissue formation and 100% strain to non-union. This is known as Perren's theory.
Stokes published a review article on the effects of stress on bone healing and growth, and notes the importance of the 'Hueter-Volkmann Law' (growth is retarded by increased mechanical compression, and accelerated by reduced loading in comparison with normal values) in bone growth. Stokes also notes that sustained compression of physiological magnitude inhibits growth by 40% or more, while distraction increases growth rate by a much smaller amount.
Illustration A shows an example of a stress-strain curve, with several key definitions labeled on the diagram.
Incorrect Answers:
Question 81
Which of the following is considered the most appropriate shoe modification following transmetatarsal amputation?
Explanation
REFERENCES: Philbin TM, Leyes M, Sferra JJ, Donley BG: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Marks RM: Mid-foot/mid-tarsus amputations. Foot Ankle Clin 1999;4:1-16.
Question 82
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Explanation
Question 83
Figure 57a and 57b show the radiographs of a 57-year-old man who has pain in the ulnar side of the wrist and hand. Examination shows tenderness at the base of the hypothenar area. Additional diagnostic testing should include
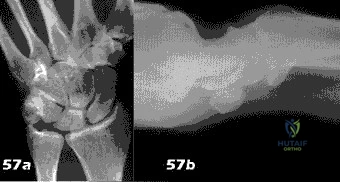
Explanation
Question 84
A 25-year-old man underwent a Putti-Platt repair for recurrent anterior dislocation of his right shoulder 9 months ago. He reports no further episodes of instability but continues to have severely restricted motion, with external rotation limited to less than 0 degrees with the arm at the side. He has pain at the ends of range of motion and restricted activities of daily living despite undergoing nearly 9 months of physical therapy. Radiographs of the shoulder show no arthritic changes. Management should now consist of
Explanation
REFERENCES: Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
Warner JJ: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg 1997;5:130-140.
Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
MacDonald PB, Hawkins RJ, Fowler PJ, Miniaci A: Release of the subscapularis for internal rotation contracture and pain after anterior repair for recurrent anterior dislocation of the shoulder. J Bone Joint Surg Am 1992;74:734-737.
Question 85
Which of the following anatomic structures is often difficult to visualize during elbow arthroscopy?
Explanation
REFERENCES: Johnson LL: Arthroscopic Surgery: Principles and Practice. St Louis, MO, CV Mosby, 1988.
Morrey BF: Arthroscopy of the elbow. Instr Course Lect 1986;35:102-107.
Question 86
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in
Explanation
REFERENCES: Shelton WR, Barrett GR, Dukes A: Early season anterior cruciate ligament tears: A treatment dilemma. Am J Sports Med 1997;25:656-658.
Snyder-Mackler L, Fitzgerald GK, Bartolozzi AR III, Ciccotti MG: The relationship between passive joint laxity and functional outcome after anterior cruciate ligament injury. Am J Sports Med 1997;25:191-195.
Question 87
A 75-year-old man has persistent radial sided hand and wrist pain. Radiographs demonstrate severe scaphotrapezial trapezoidal arthritis. His basal joint is unaffected. His pain has failed to improve with bracing, activity modification, and image-guided corticosteroid injection. He has elected surgical treatment. What longterm complication can arise from a distal scaphoid resection?
Explanation
Resection of the distal pole of the scaphoid eliminates the arthritic contact at the scaphotrapeziotrapezoid joint; however, it functionally shortens the scaphoid. Theoretically, the lunate is at equilibrium between the extension moment of the capitate and the triquetrum and the flexion moment of the scaphoid. Shortening the scaphoid allows the extension moment of the triquetrum to predominate, pulling the lunate into extension and creating a DISI deformity. Concomitant capsulodesis or interposition is recommended by some authors to prevent this complication.
Question 88
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints? Review Topic
Explanation
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
Question 89
In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?
Explanation
require surgery.
REFERENCES: Little DG, Song KM, Katz D, Herring JA: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am
2000;82:685-693.
Anderson M, Hwang SC, Green WT: Growth of the normal trunk in boys and girls during the second decade of life; related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 1965;47:1554-1564.
Question 90
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. The surgical approach for definitive reduction and stabilization of this pattern is

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally
stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 91
Figures below show the radiographs, and the CT obtained from a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?
Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 92
Increased hip intracapusular pressures can lead to diminished femoral head perfusion. What leg position has been shown to create the lowest intracapsular hip pressures after femoral neck fracture?

Explanation
Question 93
A 69-year-old man has nonpainful weakness in the upper and lower extremities. He also notes progressive instability in his gait and increasing difficulty ambulating, as well as manipulating small objects with his hands. MRI scans of his cervical spine are shown in Figures 85a and 85b. When would be the most appropriate time to proceed with surgical treatment? Review Topic

Explanation
Question 94
Which of the following is most likely to decrease surgical mortality and inpatient morbidity while simultaneously increasing surgical team adherence to life-saving steps in operating room crisis situations?
Explanation
The World Health Organization concept of a surgical safety checklist concept was validated in 2009 as a way of improving surgical outcomes. Successful implementation of a surgical checklist relies upon surgeon leadership to educate staff on its rationale and the practical components of implementation in the operating room.
Haynes et al. evaluated a 19-item surgical safety checklist and evaluated its ability to reduce complications and deaths associated with surgery in a global population. Across 8 diverse hospitals in 8 cities around the world, their study demonstrated that implementation of a pre-surgical checklist resulted in a 50% reduction in mortality (1.5% to 0.8%) and a 37% reduction in inpatient complications (11% to 7%). The patients in the study were over the age of 16 and undergoing non-cardiac surgery.
Conley et al. evaluated the effectiveness of implementation of surgical safety checklists in five hospitals using a series of interviews conducted with surgeons. Analysis of the survey results demonstrated that effective implementation relied upon surgeon leadership to explain the necessity of the checklist and how to effectively implement its use. When surgeon leadership failed in these functions, hospital staff failed to comprehend the utility of the checklist and were not able to appropriately use it. These failures eventually led to institutional abandonment of the safety checklist.
Arriaga et al. evaluated the utility of checklists to guide the surgical team through intraoperative crisis situations (e.g., massive hemorrhage, cardiac arrest). Their study of 17 surgical teams undergoing 106 simulated surgical-crises demonstrated that use of a crisis checklist led to greater adherence to life-saving steps of a care plan. 97% of participants agreed that they desired a checklist to be present if a crisis were to occur while they themselves were undergoing surgery.
Incorrect answers:
Question 95
What is the most common mechanism of injury that produces turf toe?
Explanation
REFERENCES: Clanton TO, Ford JJ: Turf toe injury. Clin Sports Med 1994;13:731-741.
Rodeo SA, O’Brien S, Warren RF, et al: Turf toe: An analysis of metatarsophalangeal joint sprains in professional football players. Am J Sports Med 1990;18:280-285.
Question 96
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
Explanation
REFERENCE: Radke HM: Arterial circulation of the upper extremity, in Strandness DE Jr (ed): Collateral Circulation in Clinical Surgery. Philadelphia, PA, WB Saunders, 1969, pp 294-307.
Question 97
Which of the following methods most reliably detects mechanical loosening of the hip?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Miniaci A, Bailey WH, Bourne RB, McLaren AC, Rorabeck CH: Analysis of radionuclide arthrograms, radiographic arthrograms, and sequential plain radiographs in the assessment of painful hip arthroplasty. J Arthroplasty 1990;5:143-149.
Question 98
15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot's skin temperature), erythema, joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective sensation, are often pathognomonic of acute Charcot arthropathy. Cellulitis is an infection of the skin. Examination would reveal erythema, edema, and pain. Osteomyelitis is an infection of the bone. Examination may reveal edema, drainage, and pain.
Explanation
Which of the following clinical scenarios represents the strongest indication for locked plating technique in a 70-year-old woman?
Segmentally comminuted ulnar fracture
Simple diaphyseal fracture of the humerus
Transverse midshaft displaced clavicle fracture
Periprosthetic femur fracture distal to a well-fixed total hip arthroplasty
Schatzker 2 fracture of the tibia with severe joint depression and comminution
Locking screw fixation is a relatively new option in the armamentarium of orthopaedic surgeons treating fractures. The understanding of the biomechanics, implications to healing, and optimal indications and surgical techniques is still in evolution. A periprosthetic proximal femur fracture with a stable prosthesis is best treated with open reduction and internal fixation with locking proximal fixation with or without cerclage cables. Diaphyseal fractures treated with compression plating or bridge plating can be treated well with conventional implants unless osteoporosis is severe. An AO/OTA B-type partial articular fracture is also better suited to standard buttress plating with periarticular rafting lag screws. Locking fixation is not always required for a transverse displaced midshaft clavicle fracture.
What is the post-amplification product of reverse transcription polymerase chain reaction (RT-PCR)?
RNA
DNA
Protein
Mitochondria
Immunoglobulins
Reverse transcription polymerase chain reaction (RT-PCR) is a variant of polymerase chain reaction (PCR) used in molecular biology to generate many copies of a DNA sequence from fragments of RNA. The RNA strand is first reverse transcribed into its DNA complement, followed by amplification of the resulting DNA using polymerase chain reaction. Polymerase chain reaction amplifies short segments of DNA by using the temperature stable DNA polymerase enzyme.
A 63-year-old woman falls from standing and lands on her right hand. She complains of deformity and wrist pain. Radiographs are provided in Figure A. Following closed reduction, the patient inquires whether she has osteoporosis and if she is likely to have another fracture. In counselling the patient, which of the following is the strongest predictor for a future fracture from low energy trauma?
Bone mineral density T-score < -2.5
Low vitamin D levels
Family history of osteoporosis
History of a prior fragility fracture
Ten year history of oral prednisone use
Each of the answer choices is a risk factor for subsequent fragility fracture, but patient history of a prior fragility fracture is the strongest predictor.
Bouxsein et al reviews the proper care, diagnosis, and prevention of fragility fractures. History of a fragility fracture is the greatest predictor of a future fracture from low energy trauma. Appropriate care includes not only treatment of the fracture itself, but also proper evaluation to identify the etiology of the fracture and appropriate intervention to rectify the underlying pathology. Evaluation includes bone densitometry, lab testing of Vitamin D and calcium.
A T-score compares your bone density to the optimal peak bone density for your gender. It is reported as number of standard deviations below the average. A T-score of -1 to -2.5 is considered osteopenia, and a risk for developing osteoporosis. A T- score of less than -2.5 is diagnostic of osteoporosis.
Long-term alendronate (Fosamax) use for osteoporosis has been associated
with which of the following?
Scurvy
Detached retina
Uterine carcinoma
Osteonecrosis of the femoral head
Diaphyseal femoral insufficiency fractures
Alendronate is a bisphosphonate that inhibits the ruffled border of the osteoclast. When used long term, this class of medication prevents the normal bone remodeling process. Long-term use has recently been shown to be associated with insufficiency fractures of the femur. Osteonecrosis of the jaw has been described but not in other anatomic locations. Scurvy occurs because of a lack of vitamin C and use of bisphosphonates is not associated with
uterine cancer or a detached retina.
Implants composed of polylactic acid are excreted by what system after they are absorbed?
Hepatic
Renal
Respiratory
Gastrointestinal
Polylactic acid suture and suture anchors are popular bioabsorbable orthopaedic implants. This material undergoes hydrolysis of the ester background in vivo. Resulting lactic acid enters the tricarboxylic acid (Krebs)
cycle and is excreted as carbon dioxide by the lungs. Polyglycolic acid and poly(p- dioxanone) may also be excreted by the kidneys.
A patient sustains a grade III medial collateral ligament injury. One year later, when compared to collagen in an uninjured ligament, an increase is likely in the
gross number of fibers.
proportion of type III fibers.
cross-linking.
mass and diameter of fibers.
Studies on animal models have shown that there is a change in collagen fiber type and distribution early in the healing process. There is a higher portion of type III fibers than in
normal ligament initially, but this ratio returns to normal about 1 year after the injury occurs. Healing ligaments show an increased number of collagen fibers, but the number of mature collagen cross-links is
45% of predicted value after 1 year. There is also a decrease in the mass and diameter of the collagen fibers.
Sclerostin and dickkopf-1 (Dkk-1) are direct inhibitors of what pathway related to bone and/or cartilage regulation?
Bone morphogenetic protein (BMP)/SMAD pathway
Receptor activator of nuclear factor kappa beta (RANK)/RANK ligand (RANKL) pathway
Wnt/Beta-catenin (ß-catenin) pathway
Parathyroid hormone (PTH) pathway
Dkk-1 and sclerostin are proteins that inhibit the binding of the Wnt molecule to receptors LRP5/6. In the absence of sclerostin and Dkk-1, Wnt binds to its receptor, which in turn inhibits phosphorylation of the ß-catenin. The unphosphorylated ß-catenin then builds up in the cytoplasm of the cell, allowing it to be transported to the nucleus of the cell. Once in the nucleus, ß- catenin will lead to upregulation of a series of proteins involved in osteoblast formation differentiation. Knocking out or inhibiting sclerostin or Dkk-1 results in increased bone mass secondary to constitutive activation of the Wnt/ß- catenin pathway. The other responses are not directly affected by Dkk-1 or sclerostin. RANKL and RANK are expressed on osteoblasts and osteoclasts, respectively, and are involved in osteoblast-mediated osteoclast activation. BMPs work through SMADs to cause osteoblastic differentiation, and there is reported crosstalk between the Wnt and BMP pathways (but this is an indirect link). Finally, PTH at physiologic levels binds to osteoblasts, causing a series of events that lead to osteoblast-mediated osteoclast activation and subsequent increased bone resorption.
During endochondral ossification of the growth plate, the process that most contributes to the longitudinal growth of long bones is
chondrocyte apoptosis.
chondrocyte hypertrophy.
chondrocyte proliferation.
growth plate matrix synthesis.
The growth plate is divided into 5 distinct zones: reserve, proliferative, maturation, hypertrophy, and vascular invasion. During growth-plate chondrocyte hypertrophy, intracellular volume and an increase in chondrocyte height are responsible for most growth of long bones. Other factors that contribute to bone growth are chondrocyte proliferation and matrix synthesis, but to a lesser degree than chondrocyte hypertrophy. Growth plate chondrocytes undergo programmed cell death (apoptosis) after hypertrophy
takes place.
Bacterial resistance to tetracycline is confirmed by ribosome protection, tetracycline modification, and
altered RNA polymerase.
altered membrane binding protein.
increased drug efflux.
DNA gyrase mutation.
Mutations of bacterial DNA gyrase can decrease the effectiveness of quinolones. Altered membrane-binding protein is observed with resistance to ?
-lactam antibiotics. Tetracyclines are antibiotics that inhibit bacterial growth by stopping protein synthesis. Three specific mechanisms of tetracycline
resistance have been identified: increased tetracycline efflux, ribosome protection, and tetracycline modification. Alteration of RNA polymerase is found in resistance to rifampin.
A 14-year-old boy has failed physical therapy management for Scheuermann kyphosis, and an extension thoracolumbosacral orthosis brace is recommended. The boy and his parents are told that the brace will force his thoracic spine into normal sagittal alignment and put the anterior vertebral bodies of the thoracic segment into tension, which will induce bone growth and normalization of wedge- shaped
vertebrae. What name is associated with this process?
Hooke's law
Kirchhoff's law
Wolff's law
Heuter-Volkmann principle
The Heuter-Volkmann principle shows that bone placed in longitudinal tension will tend to stimulate longitudinal growth, and that compressive longitudinal forces inhibit longitudinal growth, making this response the best choice. Hooke's law relates to stress being proportional to strain and is not directly related to bone growth. Kirchhoff's laws apply to electrical circuit design. Wolff's law states that bone remodels in response to mechanical stress, with the correlate that increased stress causes increased growth, and decreased stress leads to bone loss.
A tendon repair is thought to be weakest during which phase of tendon healing?
Inflammatory
Proliferation
Maturation
Remodeling
Healing after a tendon repair or rupture has the following stages: inflammatory, cellular proliferation, and remodeling. During the inflammatory phase, neutrophils and macrophages migrate into the injury site and release chemotactic factors that recruit fibroblasts. A tendon is thought to be weakest
5 to 21 days after repair, which coincides with the inflammatory phase. During the proliferative phase, inflammatory cells secrete cytokines and growth
factors (platelet-derived growth factor, insulin-like growth factor, bone morphogenetic protein (BMP)-12 and BMP 13, and transforming growth factor- beta) that promote differentiation of fibroblasts. Fibrosis and decreased cellularity are the hallmarks of the remodeling stage.
A 4-year-old boy has bilateral genu varum and is in the fifth percentile for height for his age. A younger sister has less severe genu varum. Radiographs reveal physeal cupping and widening on both the distal femur and proximal tibia. Laboratory studies show sodium 145 mEq/L (reference range, 136-142 mEq/L), potassium 4.0 mEq/L (reference range, 3.5-5.0 mEq/L), calcium 9.0 mg/dL (reference range, 8.2-10.2 mg/dL), phosphorous 2 mg/dL (reference range, 4-
Question 99
Figure 27 shows the radiograph of a 68-year-old woman with a history of rheumatoid arthritis who was injured in a fall. History reveals that she has been asymptomatic since undergoing a left total knee arthroplasty 9 years ago. Management should consist of
Explanation
REFERENCE: Ayers DC: Supracondylar fracture of the distal femur proximal to a total knee replacement, in Springfield DS (ed): Instructional Course Lectures 46. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-203.
Question 100
A 35-year-old patient is involved in a motor vehicle accident and sustains multiple fractures including a closed comminuted proximal meta-diaphyseal tibia fracture. The surgeon is considering bridge plating the fracture using a minimally invasive approach. Which of the following is true regarding bridge plating? Review Topic
Explanation
Bridge plating is applicable to all long-bone fractures with complex fragmentation and where intramedullary nailing or conventional plate fixation is not suitable. The construct preserves the blood supply to the fracture fragments as the fracture site is undisturbed during the operative procedure. It provides RELATIVE stability, allowing for some motion at the fracture site, leading to callus formation and secondary bone healing. The construct is FLEXIBLE because of increased distance between the 2 screws closest to the fracture (long working length), allowing for stress distribution and permitting more motion at the fracture site. The construct is also
AXIALLY STABLE because the plate acts as an extramedullary splint and resists axial compression.
Livani et al. advocate using an anterior or antero-lateral approach for minimally invasive plating of the humerus. They recommend that distal access is obtained first, allowing identification of the lateral antebrachial cutaneous nerve. For distal fractures, they recommend extending the plate down to the lateral column.
Apivatthakakul et al. defined minimally-invasive plate osteosynthesis (MIPO) danger zones from the lateral epicondyle. They found the musculocutaneous nerve averaged 18-43% of the humeral length, the danger zone for the radial nerve averaged 36-59% of the humeral length, and the most dangerous screws that penetrated or touched the radial nerve lay 47-53% of the humeral length.
Illustration A shows a distal tibia fracture. Illustration B shows radiographs 5 months after bridge plating of this fracture. There is callus formation, characteristic of indirect bone healing.
