OITE & ABOS Orthopedic MCQ Exam: Arthroplasty, Trauma & Sports Medicine - Part 52

Key Takeaway
This page offers Part 52 of an interactive MCQ set for orthopedic residents and surgeons preparing for their AAOS and ABOS board certification exams. It features 100 high-yield questions, mirroring OITE and AAOS exam formats, focusing on arthroplasty, fracture, hip, and knee. Utilize study and exam modes for comprehensive board exam preparation.
About This Board Review Set
This is Part 52 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 52
This module focuses heavily on: Arthroplasty, Fracture, Hip, Infection, Knee, Ligament, Tendon.
Sample Questions from This Set
Sample Question 1: An otherwise healthy 25-year-old man underwent a right anterior cruciate ligament reconstruction with a bone-patellar tendon-bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-...
Sample Question 2: A 72-year-old woman falls onto her left hip after tripping over a curb during her daily 3-mile walk. An injury radiograph is shown in Figure A. What is the best long term solution?...
Sample Question 3: Following an episode of transient quadriplegia in contact sports, an athlete’s return to play is absolutely contraindicated when...
Sample Question 4: Which of the following treatment regimens for thromboembolic prophylaxis meets the American College of Chest Physicians Guidelines for 10-day treatment after total hip arthroplasty and total knee arthroplasty?...
Sample Question 5: What is the incidence and significance of anterior cruciate ligament laxity following tibial eminence fractures in skeletally immature individuals?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An otherwise healthy 25-year-old man underwent a right anterior cruciate ligament reconstruction with a bone-patellar tendon-bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-negative Staphylococcus 5 days postoperatively. The patient has exhibited no evidence of clinical infection and his postoperative course has been uncomplicated during this time. What is the ideal management of this patient?
Explanation
implanted with a "contaminated" graft develop a clinical infection. The results of the current literature suggest that the treatment of low-virulence organisms is unnecessary if no evidence of clinical infection exists. Preimplantation cultures do not appear to correlate with clinical infection. Therefore, the routine culture of allograft tissue is not recommended.
Question 2
A 72-year-old woman falls onto her left hip after tripping over a curb during her daily 3-mile walk. An injury radiograph is shown in Figure A. What is the best long term solution?

Explanation
The aims of surgery for FNF in elderly patients are immediate pain relief, rapid mobilization, and low complications and revision. THA has best pain relief, fewer reoperations, best survivorship and is most cost-effective but has longer operative/anesthetic time, blood loss, higher infection rate, and potential instability compared with HA.
Healy and Iorio examined the optimal treatment for elderly FNF. They compared internal fixation (120 patients) with arthroplasty (HA, 43 patients; THA, 23 patients). There was no different in reoperation or mortality rates between the 2 groups, but arthroplasty was more cost effective, had independent living, and longer interval to reoperation/death. THA had less pain, better function, and lower rates of reoperation than HA, and was most cost-effective. They concluded that THA was the best treatment.
Yu et al. performed a meta-analysis of randomized controlled trials to determine whether THA or hemiarthroplasty (HA) was superior. They found that THA had lower risk of reoperation (RR = 0.53), higher risk of dislocation (RR = 1.99), and
higher functional scores at 1 and 4 years. There was no difference in mortality, infection and complication rates.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Question 3
Following an episode of transient quadriplegia in contact sports, an athlete’s return to play is absolutely contraindicated when
Explanation
REFERENCES: Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146.
Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Bailes JE, Hadley MN, Quigley MR, Sonntag VK, Cerullo LJ: Management of athletic injuries of the cervical spine and spinal cord. Neurosurgery 1991;29:491-497.
Question 4
Which of the following treatment regimens for thromboembolic prophylaxis meets the American College of Chest Physicians Guidelines for 10-day treatment after total hip arthroplasty and total knee arthroplasty?
Explanation
Low-molecular-weight heparin and fondaparinox are also acceptable treatment options. Aspirin, adjusted dose unfractionated heparin, and elastic compressive stockings are not recommended as stand-alone options.
REFERENCES: Colwell C: Evidence based guidelines for prevention of venous thromboembolism: Symposia. Proceedings of the 2005 AAOS Annual Meeting. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 15-18.
Freedman KB, Brookenthal KR, Fitzgerald RH, et al: A meta-analysis of thromboembolic prophylaxis following elective total hip arthroplasty. J Bone Joint Surg Am 2000;82:929-938.
Question 5
What is the incidence and significance of anterior cruciate ligament laxity following tibial eminence fractures in skeletally immature individuals?
Explanation
REFERENCES: Willis R, Blokker C, Stall TM, et al: Long-term follow-up of anterior
eminence fractures. J Pediatr Orthop 1993;13:361-364.
Smith JB: Knee instability after fracture of the intercondylar eminence of the tibia.
J Pediatr Orthop 1984;4:462-464.
Question 6
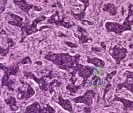
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. View Abstract at PubMed
Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. Enzinger & Weiss’s Soft Tissue Tumors. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. View Abstract at PubMed
Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. View Abstract at PubMed
Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.View Abstract at PubMed
Question 7
A 29-year-old female has sustained the acute injury shown in Figure A. Which of the following is an indication for open reduction internal fixation in this patient?

Explanation
In patients who present with no medial widening on standard ankle radiographs and no clinical symptoms of deltoid ligament injury, the integrity of the deltoid ligament remains unknown. The gravity stress radiograph may be used to help identify a deltoid ligament injury in association with an isolated distal fibular fracture. Stage-IV supination-external rotation fractures, which involve the deltoid ligament, are more likely to be treated operatively as they are often considered unstable ankle fractures.
Egol et al. reviewed 101 patients with isolated fibular fracture and an intact mortise. They found that medial tenderness, swelling, and ecchymosis were not sensitive with regard to predicting widening of the medial clear space on stress radiographs. Interestingly, they report that good functional results can be obtained in patients with widening of the medial clear space on a stress radiograph in the absence of medial signs.
Gill et al. compared the effectiveness of gravity stress radiograph as compared to manual stress radiograph for the detection of deltoid ligament injury in isolated fibular fracture. A total of twenty-five patients with SER type-II fracture and SER Type IV-equivalent fractures were enrolled. They found the gravity stress radiograph was equivalent to the manual stress radiograph for determining deltoid ligament injury.
Figure A shows a mortise radiograph displaying a minimally displaced Weber B ankle fracture. Illustration A shows the positioning for a gravity stress radiograph. The patient is in the lateral decubitus position with the injured leg dependent and off the end of the table, a mortise view is taken in 10° of internal rotation of the tibia.
Incorrect Answers:
Question 8
-Figures 3a and 3b are the clinical photographs of a 35-year-old man seen 3 months after repair of an acute Achilles tendon rupture. He has no constitutional symptoms and is unable to perform a single heelrise test. The most appropriate treatment is

Explanation
Question 9
Which of the following radiographic findings indicates that the injury to the great toe shown in Figures 60a and 60b should be reducible by closed manipulation?

Explanation
Question 10
Closure of the rotator cuff interval results in elimination of which direction of shoulder instability?
Explanation
REFERENCES: Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
O’Brien SJ, Schwartz RS, Warren RF, et al: Capsular restraints to anterior-posterior motion of the abducted shoulder: A biomechanical study. J Shoulder Elbow Surg 1995;4:298-308.
Warner JJ, Deng XH, Warren RF, et al: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Question 11
What is the main benefit of using metal-backed tibial components in total knee arthroplasty?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Question 12
A 64-year-old man who underwent an L4-5 decompression approximately 1 year ago reported relief of his claudicatory leg pain initially, but he now has increasing low back pain and recurrent neurogenic claudication despite nonsurgical management. Radiographs show new asymmetric collapse and spondylolisthesis at the decompressed segment, and MRI scans show lateral recess stenosis. The next most appropriate step in management should consist of
Explanation
REFERENCES: Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.
Hansraj KK, O’Leary PF, Cammisa FP Jr, et al: Decompression, fusion, and instrumentation surgery for complex lumbar spinal stenosis. Clin Orthop 2001;384:18-25.
Question 13
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior knee pain, a trace effusion, a 2+ posterior drawer, a grade 1+ stable Lachman, no valgus laxity, and negative dial tests at 30° and 90°. What is the best treatment strategy at this time?
Explanation
Question 14
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Explanation
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 15
A patient with a below-the-knee amputation is being evaluated for a new prosthesis. He wants to improve his ability to walk on uneven surfaces. What modification to the prosthesis can be made to accommodate this request?
Explanation
REFERENCES: Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 31-45.
Goldberg B (ed): Atlas of Orthoses and Assistive Devices, ed 3. St Louis, MO, Mosby-Year Book, 1997.
Question 16
A Trendelenburg gait is most likely to be seen in association with
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Andersson GB, Deyo RA: History and physical examination in patients with herniated lumbar discs. Spine 1996;21:10S-18S.
Question 17
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal.
Explanation
Question 18
Figures below show the radiographs, and the CT obtained from a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?

Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 19
A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness? Review Topic
Explanation
Question 20
Figures 4a and 4b show the radiographs of a 53-year-old woman who was injured in a fall. After initial closed reduction, what is the preferred treatment for this fracture?
Explanation
REFERENCES: Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Pugh DM, Wild LM, Schemitsch EH, et al: Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures. J Bone Joint Surg Am 2004;86:1122-1130.
Question 21
…Figure 53 is the emergency department radiograph of a 7-year-old boy who has pain and is unwilling to use his right arm after a fall on the playground. What is the most appropriate initial treatment?
Explanation

Question 22
All of the following have been shown to negatively affect clinical outcomes in treating displaced acetabular fractures, EXCEPT:

Explanation
The referenced study by Matta evaluated outcomes of displaced acetabular fractures. The overall clinical result was excellent for 104 hips (40 per cent), good for ninety-five (36 per cent), fair for twenty-one (8 per cent), and poor for forty-two (16 per cent). The clinical result was related closely to the radiographic result. These findings indicate that in many patients who have a complex acetabular fracture the hip joint can be preserved and post-traumatic osteoarthrosis can be avoided if an anatomical reduction is achieved.
Question 23
Which of the following has been associated with a decreased rate of glenoid component radiolucent lines?
Explanation
REFERENCES: Gartsman GM, Elkousy HA, Warnock KM, et al: Radiographic comparison of pegged and keeled glenoid components. J Shoulder Elbow Surg 2005;14:252-257.
Szabo I, Buscayret F, Edwards TB, et al: Radiographic comparison of flat-back and convex-back glenoid components in total shoulder arthroplasty. J Shoulder Elbow Surg 2005;14:636-642.
Mileti J, Boardman ND III, Sperling JW, et al: Radiographic analysis of polyethylene glenoid components using modern cementing techniques. J Shoulder Elbow Surg 2004;13:492-498.
Question 24
A 29-year-old woman reports shoulder pain after sustaining a minor fall 6 weeks ago. She has a history of celiac sprue. Radiographs of the forearm and shoulder are shown in Figures 53a and 53b. Which of the following serum abnormalities would be expected?
Explanation
REFERENCES: Potts JT: Parathyroid hormone: Past and present. J Endocrinol 2005;187:311-325.
Corazza GR, Di Stefano M, Maurino E, et al: Bones in coeliac disease: Diagnosis and treatment. Best Pract Res Clin Gastroenterol 2005;19:453-465.
Mankin HJ, Mankin CJ: Metabolic bone disease: An update. Instr Course Lect 2003;52:769-784.
Question 25
When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral base of the proximal phalanx of the great toe. This conjoined tendon is made up of what two muscles?
Explanation
REFERENCES: Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983, chapter 5.
Question 26
Figures 31a and 31b are the radiographs of a 5-year-old boy with an elbow injury.
Explanation
Figure 26 shows lucent areas of both femoral condyles. This may represent a variation of ossification, in which case this boy’s knee pain is coincidental. Another possibility is atypical osteochondritis dissecans. An MRI will distinguish between the 2 entities and will guide treatment.
Figures 27a and 27b show healing rib and distal tibia fractures. These fractures likely are attributable to child abuse. A plain radiographic skeletal survey is sufficient for orthopaedic needs.
A triplane fracture of the distal tibia is revealed in Figure 28. A CT scan will quantify displacement and identify fracture fragments for planning of screw trajectories if open reduction and internal fixation is indicated (displacement > 2 mm).
In Figure 29, the linear lucency of the capitellum indicates an early osteochondritis dissecans. An MRI will allow staging of the lesion.
Figure 30 shows that the left radius and ulna do not align with the humerus; this is the likely result of a transphyseal fracture of the distal humerus. An arthrogram will outline the unossified distal humerus and allow for reduction. For an unstable neonate, this likely can be performed in the NICU.
Figures 31a and 31b reveal a widely displaced lateral condyle fracture for which open reduction and internal fixation is required. No advanced imaging is necessary.

Question 27
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with Review Topic
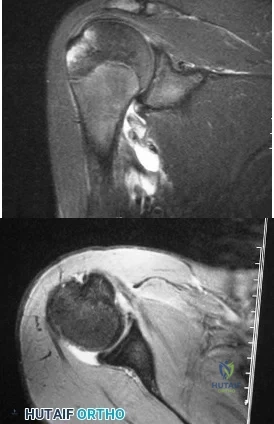
Explanation
Question 28
-Six weeks later the boy remains uncomfortable and continues to use crutches for all ambulation. What do the new radiographs seen in Figures 78a and 78b reveal?
Explanation
It has been demonstrated on a cadaver model that screw fixation of moderate and severe slipped capital femoral epiphyses may result in screw impingement upon the acetabulum and labrum. This is likely when the screw head on the anteroposterior view is seen to lie medial to the intertrochanteric line. Femoral artery pseudoaneurysm has been reported when the screws are left long (projecting far from the bone) to ease removal. Chondrolysis is associated with persistent penetration into the hip joint; both screws stop well short of the articular surface. Many in vitro studies of slip models have demonstrated increased strength of construct of two screws compared to one, although the clinical relevance can be questioned.
The radiographs show the screw heads firmly in the femoral head, with loss of fixation in the femoral neck. Sanders and associates reported a series of 7 such failures and hypothesized that acute-on-chronic slips may develop osteopenia of the femoral neck. All patients reported continued pain postoperatively rather than the relief typically seen following surgical stabilization of the epiphysis.
There is no radiographic evidence of osteonecrosis or chondrolysis.
Question 29
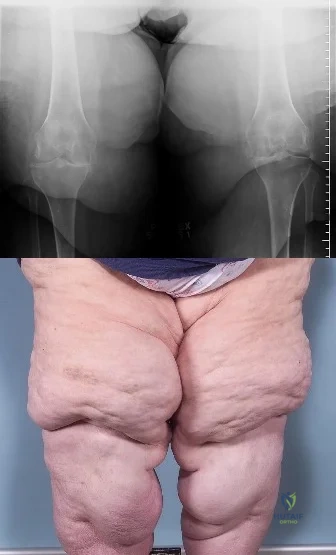
An 18-year-old high school football player sustains a thigh injury that results in the findings shown in Figure 1. Initial management should consist of
Explanation
REFERENCES: Anderson JE (ed): Grant’s Atlas of Anatomy. Baltimore, MD, Williams & Wilkins, 1978, pp 4.39-4.49.
Brumet ME, Hontas RB: The thigh, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Antao NA: Myositis of the hip in a professional soccer player: A case report. Am J Sports Med 1988;16:82-83.
Jackson DW, Feagin JA: Quadriceps contusions in young athletes: Relation of severity of injury to treatment and prognosis. J Bone Joint Surg Am 1973;55:95-105.
Question 30
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study results fits the definition of chronic prosthetic joint infection?
Explanation
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
Question 31
Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment?
Explanation
REFERENCES: Favard L, Lautmann S, Sirveaux F, et al: Hemiarthroplasty versus reverse arthroplasty in the treatment of osteoarthritis with massive rotator cuff tear, in Walch G, Boileau P, Mole D (eds): 2000 Shoulder Prosthesis Two to Ten Year Follow-Up. Montpellier, France, Sauramps Medical, 2001, pp 261-268.
Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 32
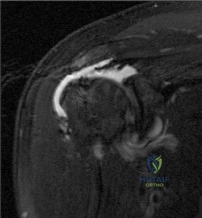
A 67-year-old female presents with shoulder pain for 3 months after falling down stairs. Imaging demonstrates a large rotator cuff tear involving multiple tendons. You perform an arthroscopic rotator cuff repair and biceps tenodesis. At her 2 month follow up, she reports worsening shoulder pain and decreased range of motion. Examination reveals active forward flexion to 80°. Passive range of motion is full. There is a positive external rotation lag sign. An MRI is performed and is pictured in Figure A. Which is the best treatment for this patient? Review Topic
Explanation
Failed rotator cuff repair is multifactorial. Structural failure of repair is the result of both intrinsic and extrinsic factors. Intrinsic factors include advancing patient age, increasing tear size, poor tendon and muscle quality, systemic disease and smoking history. Extrinsic factors include inadequate biomechanical construct or repair configuration and overaggressive postoperative rehabilitation.
Denard et al authored a review article on revision rotator cuff repair. Indications for revision repair are persistent symptoms despite nonoperative management in whom infection and advanced degenerative changes have been ruled out. Satisfactory results have been reported following revision repair of recurrent rotator cuff tears, particularly with arthroscopic techniques. Female sex and preoperative forward flexion < 135° is associated with poorer outcomes.
Lambers Heerspink et al found that increasing age, larger tear size and additional biceps or acromioclavicular (AC) joint procedures have a negative influence on cuff integrity at follow up. Smoking, duration of symptoms, obesity and medical comorbidities were not found to influence cuff integrity in this study. Only AC procedures and workers’ compensation status were associated with worse functional outcomes.
Figure A is a coronal T2 MRI demonstrating a failed rotator cuff repair with retear. Incorrect Responses:
Question 33
In a patient with a major head injury and a femoral shaft fracture, intraoperative hypotension during femoral fixation has been associated with which of the following?

Explanation
Question 34
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?
Explanation
REFERENCES: Hartsock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29:467-475.
Hughes M, Neer CS: Glenohumeral joint replacement and postoperative rehabilitation.
Phys Ther 1975;55:850-858.
Compito CA, Self EB, Bigliani LU: Arthroplasty and acute shoulder trauma. Clin Orthop 1994;307:27-36.
Question 35
A 66-year-old woman was a restrained passenger in an automobile accident. She sustained a direct blow to her nondominant left hand as the airbag in her automobile deployed and she now reports pain, swelling, and difficulty moving her fingers. Radiographs are shown in Figures 58a and 58b. Appropriate definitive treatment should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 286.
Faraj AA, Davis TR: Percutaneous intramedullary fixation of metacarpal shaft fractures. J Hand Surg Br 1999;24:76-79.
Question 36
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 37
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis in the setting of reaction to metal debris?
Explanation
Question 38
A 17-year-old football player is injured during a play and reports abdominal pain that is soon followed by nausea and vomiting. What organ has most likely been injured?
Explanation
REFERENCES: Green GA: Gastrointestinal disorders in the athlete. Clin Sports Med 1992;11:453-470.
Kibler WB (ed): ACSM’s Handbook for Team Physician. Philadelphia, PA,
Williams & Wilkins, 1996, p 151.
Question 39
Acral metastases are most commonly seen in what type of carcinoma?
Explanation
REFERENCES: Hayden RJ, Sullivan LG, Jebson PJ: The hand in metastatic disease and acral manifestations of paraneoplastic syndromes. Hand Clin 2004;20:335-343.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 313.
Question 40
Which of the following best describes heat stroke? Review Topic
Explanation
Question 41
A 54-year-old woman undergoes an interposition arthroplasty that fails and requires conversion to a total elbow arthroplasty. She has progressive elbow pain and radiographic loosening. Erythrocyte sedimentation rate and C-reactive protein are normal. Joint aspiration is positive for Staphylococcus epidermidis. What surgical treatment would best optimize function and decrease risk of recurrence?
Explanation
is best reserved for low-demand or infirm patients.
Question 42
An 18-year-old girl with quadriplegic cerebral palsy underwent posterior spinal fusion from T2 to the pelvis 3 weeks ago. She now has a low-grade fever and mild midline erythema in a 1-cm area from which there is slight clear yellowish drainage. What is the next most appropriate step in management?
Explanation
REFERENCES: Theiss SM, Lonstein JE, Winter RB: Wound infections in reconstructive spine surgery. Orthop Clin North Am 1996;27:105-110.
Richards BS: Delayed infections following posterior spinal instrumentation for the treatment of idiopathic scoliosis. J Bone Joint Surg Am 1995;77:524-529.
Question 43
What is the best initial screening test for a patient with a limb-length discrepancy?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 1041-1045.
Schoenecker PL, Rich MM: The lower extremity, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1120-1122.
Stanitski DF: Limb-length inequality: Assessment and treatment options. J Am Acad Orthop Surg 1999;7:143-153.
Aaron A, Weinstein D, Thickman D, Eilert R: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Question 44
A 7-year-old boy sustained a head contusion and small bowel injuries in a motor vehicle accident in which he was wearing a lap belt. He subsequently required a bowel resection. Six weeks after the accident, his parents note a painful mass in his lower back. His neurologic examination is normal. A radiograph and CT scans are shown in Figures 47a through 47c. Definitive management should now consist of
Explanation
REFERENCES: Ebraheim NA, Savolain ER, Southworth SR, et al: Pediatric lumbar seat belt injuries. Orthopedics 1991;14:1010-1013.
Taylor JA, Eggli KD: Lap belt inhuries of the lumbar spine in children: A pitfall in CT diagnosis. Am J Rad 1988;150:1355-1358.
Question 45
Following spinal cord injury (SCI), methylprednisolone (a bolus of 30 mg/kg plus 5.4 mg/kg per hour over 24 hours) initiated within 8 hours of injury has been associated with which of the following MRI findings? Review Topic
Explanation
Question 46
.A patient is unable to actively externally rotate the shoulder when the arm is placed into 90 degrees of abduction and neutral rotation. This finding is most consistent with a tear of the
Explanation
Question 47
Which structure(s) is/are most at risk with surgical treatment of displaced clavicle fractures with ORIF?
Explanation
Complications associated with nonsurgical treatment of displaced midshaft clavicle fractures are uncommon. Although intrathoracic and local vascular complications have been reported with clavicle fracture, subclavian artery aneurysm and pneumothorax are rare. Malunion to some degree is inevitable with nonsurgical treatment of displaced clavicle fractures, but only about 9% of patients develop symptomatic malunion. Nonunion occurs in about 15% of patients.
Previously identified risk factors for nonunion of clavicle fractures include female gender, displacement exceeding 100%, comminution, and advanced age. Research demonstrates the strongest risk factors are smoking, comminution, and fracture displacement. Rate of nonunion in 1 study was approximately 13%. Murray and associates showed that by estimating the risk of nonunion using their model and operating only on fractures with at least a 40% chance of nonunion, they would only need to operate on 1.7 patients to prevent 1 nonunion (decreased from 7.5 procedures per nonunion if operating on all displaced midshaft fractures). This data could potentially be used to limit unnecessary procedures and decrease costs associated with treatment of clavicle fractures.
Hardware removal is the most common reason for revision surgery. Symptomatic malunion and supraclavicular nerve entrapment are rare after surgery. Nonunion is uncommon (in fewer than 2% of cases). The main reason for revision surgery is hardware removal to address local irritation/prominent hardware or infection.
An anatomical study demonstrated that in 97% of clavicles, 2 to 3 branches of the supraclavicular nerve were crossing the clavicle with wide location variability in the zone in which most clavicle fractures occur and surgery would take place. The subclavian vein and artery and brachial are rarely injured,
although there are case reports of injury to all either by the displaced fracture fragments or errant hardware.
RECOMMENDED READINGS
McKee RC, Whelan DB, Schemitsch EH, McKee MD. Operative versus nonoperative care of displaced midshaft clavicular fractures: a meta-analysis of randomized clinical trials. J Bone Joint Surg Am. 2012 Apr 18;94(8):675-84. doi: 10.2106/JBJS.J.01364. Review. PubMed PMID: 22419410.View Abstract at PubMed
Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am. 2004 Jul;86-A(7):1359-65. PubMed PMID: 15252081.View Abstract at PubMed
Murray IR, Foster CJ, Eros A, Robinson CM. Risk factors for nonunion after nonoperative treatment of displaced midshaft fractures of the clavicle. J Bone Joint Surg Am. 2013 Jul 3;95(13):1153-8. doi: 10.2106/JBJS.K.01275. PubMed PMID: 23824382.View Abstract at
PubMed
Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am. 2007 Jan;89(1):1-10. PubMed PMID: 17200303.View Abstract at PubMed
Nathe T, Tseng S, Yoo B. The anatomy of the supraclavicular nerve during surgical approach to the clavicular shaft. Clin Orthop Relat Res. 2011 Mar;469(3):890-4. doi: 10.1007/s11999-010-1608-x. Epub 2010 Oct 9. PubMed PMID: 20936387.View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 26 AND 27

A

B

C

D
Figures 26a through 26c are the radiographs of a 50-year-old athlete who sustained an injury to his right foot; the foot was plantar flexed and another player landed on the posterior aspect of his heel. After sustaining the injury he was unable to bear weight, and 3 days later he was seen in the emergency department because of persistent pain and tenderness over his midfoot.
Question 48
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals no other injuries. Radiographs are shown in Figures 35a and 35b. Initial management of this fracture should consist of
Explanation
REFERENCES: Meyers MH, McKeever FM: Fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60
Janarv PM, Westblad P, Johansson C, Hirsch G: Long-term follow-up of anterior tibial spine fractures in children. J Pediatr Orthop 1995;15:63-68.
Kuhn JE, Sailer MJ, Sterett WI, Hawkins RJ: Arthroscopic technique for the treatment of tibial spine fractures in the skeletally immature patient. J Ortho Tech 1995;3:7-12.
Question 49
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, p 1550.
Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 212-214.
Kaplan FS, August CS, Fallon MD, et al: Successful treatment of infantile malignant osteopetrosis by bone-marrow transplantation: A case report. J Bone Joint Surg Am 1988;70:617-623.
Question 50
What is the best approach to reduce and stabilize a displaced volar lunate facet fracture of the wrist?
Explanation
REFERENCES: Hanel DP, Jones MD, Trumble TE: Wrist fractures. Orthop Clin North Am 2002;33:35-57.
Trumble TE, Culp RW, Hanel DP, et al: Intra-articular fractures of the distal aspect of the radius. Instr Course Lect 1999;48:465-480.
Question 51
A 26-year-old man with chronic lateral ankle instability underwent a modified Broström procedure 8 months ago. He reports persistent pain and swelling of the lateral ankle. Examination reveals lateral ankle tenderness and swelling and a negative anterior drawer test. Laboratory studies show a WBC count of 6,500/mm 3 and an erythrocyte sedimentation rate of 15 mm/h. Radiographs of the ankle are normal. What is the most likely cause of this problem?
Explanation
REFERENCES: Bonnin M, Tavernier T, Bouysset M: Split lesions of the peroneus brevis tendon in chronic ankle laxity. Am J Sports Med 1997;25:699-703.
Sobel M, Geppert MJ, Warren RF: Chronic ankle instability as a cause of peroneal tendon injury. Clin Orthop Relat Res 1993;296:187-191.
Question 52
Figures 1 and 2 are the radiographs of a 35-year-old right-hand-dominant man who has had progressive right wrist pain for 1 year. There is no history of trauma, and he has had no treatment to date. He reports some pain at rest with limited motion and substantial pain with use. He is currently out of work on short-term disability because of this wrist problem. An examination reveals mild dorsal wrist swelling, decrease wrist range of motion, and decreased grip strength. Contralateral wrist examination findings are normal. What is the most appropriate course of treatment?

Explanation
This patient has late-stage Kienböck disease. According to the Lichtman classification for Kienböck disease, this would represent stage IIIB, with lunate collapse/fragmentation, loss of carpal height secondary to proximal capitate migration, and a flexed scaphoid. The lateral radiograph reveals a radioscaphoid angle exceeding 60 degrees, so disease stage is IIIB. According to Condit and associates, when the presurgical radioscaphoid angle exceeds 60 degrees, results are poor when an attempt to maintain the lunate is made. As a result, the procedure with the most predictable outcome is a proximal row carpectomy. A radial-shortening osteotomy could be performed because the ulnar variance is negative. Considering the marked lunate fragmentation and collapse, a vascularized bone graft likely is contraindicated and associated with less predictable results than a proximal row carpectomy. There is no role for supervised hand therapy and splinting in the setting of advanced Kienböck disease. Similarly, there is no role for maintenance of the lunate in the setting of advanced collapse and fragmentation.
Question 53
Plate fixation of olecranon fractures is recommended over tension band wire fixation when
Explanation
Question 54
A metal-on-metal bearing used for total hip arthroplasty shows which of the following properties?
Explanation
REFERENCE: Heisel C, Silva M, Skipor AK, et al: The relationship between activity and ions in patients with metal-on-metal bearing hip prostheses. J Bone Joint Surg Am 2005;87:781-787.
Question 55
A 58-year-old man has had increasing midback pain for 8 weeks. Radiographs reveal mild osteopenia and mild disk degeneration but no fractures or lesions. An MRI of the spine reveals diskitis with a small-intensity signal within the spinal canal that is consistent with an epidural abscess at T11-12. The patient is neurologically intact but in significant pain. CT-guided biopsy of the disk space is positive for methicillin-sensitive Staphylococcus aureus. What is the most appropriate treatment?
Explanation
The treatment of spinal infections is variable. A diskitis in a patient with a mechanically stable spine without neurologic compromise is typically treated with needle biopsy/culture and appropriate IV antibiotics. Epidural abscess often is considered one of the true orthopaedic emergencies that necessitates surgical intervention. However, there is growing evidence that medical management can be appropriate to treat epidural abscesses in certain cases. In cases involving neurologic deterioration, surgical decompression, drainage, and systemic IV antibiotics is the treatment of choice. Medical management of spinal abscesses can be considered when a patient refuses surgical decompression; surgery is contraindicated because of high risk, pain, or
infection; or paralysis lasting longer than 24 to 36 hours results in a likely inability to reverse the paralysis. Patients who are neurologically intact may also be treated with medical management alone if they are stable and have an identifiable microorganism that can be observed closely to assess for neurologic deterioration. If neurologic changes are noted, surgical decompression and debridement and continued IV antibiotic therapy are appropriate.
RECOMMENDED READINGS
Darouiche RO. Spinal epidural abscess. N Engl J Med. 2006 Nov 9;355(19):2012-20. Review. PubMed PMID: 17093252.View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 56
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to
Explanation
REFERENCES: Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Question 57
A 44-year-old man sustains the injury shown in Figures 1 through 3. What is the most appropriate treatment?

Explanation
Reduction, either open or closed, with internal fixation (pinning) is the recommended treatment for the majority of these injuries. Closed reduction with pinning is most often performed for acute injuries. Open reduction with pinning is performed for those injuries that cannot be reduced by closed means or those with a delayed presentation. Four cases of successful closed reduction and splinting, all performed upon presentation in the emergency department, have been described by Storken and associates, but the authors note that their review of three prior reports uncovered cases of secondary dislocation, which required surgical stabilization. One of the dislocations occurred 4 months after the reduction. They assert that an indication for primary ORIF is a CMC dislocation associated with major fractures. Primary arthrodesis can be considered in cases with severe intra-articular comminution, but this procedure substantially limits the ability of the hand to increase and decrease the transverse metacarpal arch, which is an important functional movement. It can also lead to osteoarthritis of the triquetrohamate joint. Suspension arthroplasty has been described for old fracture-dislocations of the fifth CMC joint, using a partial slip of the extensor carpi ulnaris.








Question 58
Figures below show the radiographs obtained from a 19-year-old woman with a 3-year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?
Explanation
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 59
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?
Explanation
REFERENCES: Smith GR, Hotchkiss RN: Radial head and neck fractures: Anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg 1996;5:113-117.
Caputo AE, Mazzocca AD, Santoro VM: The nonarticulating portion of the radial head: Anatomic and clinical correlations for internal fixation. J Hand Surg Am 1998;23:1082-1090.
Question 60
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?
Explanation
REFERENCES: Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
Burroughs PL, Gearen PF, Petty WR, et al: Shoulder arthroplasty in the young patient.
J Arthroplasty 2003;18:792-798.
Question 61
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to
surgery.
Question 62
When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively?
Explanation
REFERENCE: Glassman SD, Anagnost SC, Parker A, et al: The effect of cigarette smoking and smoking cessation on spinal fusion. Spine 2000;25:2608-2615.
Question 63
A 19-year-old wrestler has numbness along the radial aspect of the forearm after undergoing an open Bankart repair through an anterior deltopectoral approach. Motor weakness would be expected along with what other finding?
Explanation
REFERENCES: Bach BR, O’Brien SJ, Warren RF, et al: An unusual neurologic complication of the Bristow procedure. J Bone Joint Surg Am 1988;70:458-460.
McIlveen SJ, Duralde XA: Isolated nerve injuries about the shoulder, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993, pp 214-239.
Question 64
When planning pin placement for external fixation of the tibia, what is the maximum extent of the knee capsular reflection from the subchondral joint line?
Explanation
Question 65
What is the main biologic effect of aggrecan in cartilage? Review Topic
Explanation
Aggrecan is the predominant proteoglycan in cartilage. It contains a large number of negatively charged sequences that attract water called sulfated glycosaminoglycan (GAG) chains. Its the N-terminal globular domain of aggrecan that binds hyaluronan to form huge aggregates. Together with its chondroitin sulfate chains, they help to create a hydrophilic viscous gel that decreases the coefficient of friction as well as to help absorb compressive loads.
Ulrich-Vinthe et al. reviewed the biology of articular cartilage. They report that matrix metalloproteinases and aggrecanases play a major role in aggrecan degradation and their production is upregulated by mediators associated with joint inflammation and overloading.
Illustration A shows a depiction of the function of aggrecan in articular cartilage. In the relaxed state, the aggregates draw water into cartilage. With compressive loads, the water is displaced to cushion the load. Upon removal of the load, the water content is restored.
Incorrect Answers:
Question 66
A 66-year-old female presents to your clinic complaining of back pain, difficulty standing-up straight, weakness in her legs, and neurogenic claudication. On upright thoracolumbar radiographs, there is a 75 degree thoracolumbar curve with the apex at L2, and the C7 plumb line falls 12 cm anterior to the posterosuperior corner of S1. Aside from a decompression of the stenotic levels, which of the following choices will lead to the MOST reliable decrease in overall disability? Review Topic
Explanation
Spinal malalignment in Adult Spinal Deformity (ASD) challenges balance mechanisms used for maintenance of an upright posture to achieve the basic human needs of preserving level visual gaze and retaining the head over the pelvis. Severe malalignment can result in greater muscular effort and energy expenditure to maintain the erect posture as well as use of compensatory mechanisms. As such, surgical correction of these deformities are aimed at achieving proper spinopelvic alignment.
Glassman et al. performed a multi-center retrospective study of 298 adults with spinal deformity. Regardless of operative (129 patients) or non-operative care (172 patients) a positive sagittal balance was the found to be the most reliable predictor of clinical symptoms in both patient groups.
Schwab et al. published a current concepts review on operative management for adult spinal deformities and identified three major goals of surgery: (1) Correct the SVA to
within 5 cm of neutral, (2) Ensure the pelvic tilt is less than 20 degrees, (3) Ensure the lumbar lordosis is within 9 degrees of the pelvic incidence.
Illustration A demonstrates how to measure the SVA. Illustration B depicts the realignment objectives in the saggital plane as described by Schwab et al.
Incorrect
Question 67
A radiograph of a 12-year-old boy who has had an insidious onset of pain in the right hip for the past 6 weeks shows diffuse narrowing of the joint space. Examination reveals that he is afrebile, and the range of motion of the hip is less than 50% of normal in all planes. Laboratory studies show an erythrocyte sedimentation rate of 21 mm/hr and a WBC of 11,000/mm3. What is the most likely diagnosis?
Explanation
This patient has no history of hemophilia given. Hemophilic arthropathy begins with a hemarthrosis.
In osteoid osteoma the pain is typically unrelenting, sharp, boring, worse at night, and relieved with aspirin. It is not associated with joint space narrowing.
The most common age for Legg-Calve-Perthes disease is 4-8 years. It causes AVN of the femoral head and widening of the medial joint space is an early radiographic finding.
In Bleck’s report on Idiopathic Chondrolysis JBJS 1983 nine cases were seen at the reporting institution between 1973 and 1978. The average age was 11.5 years. All the patients were otherwise healthy and had no history of systemic illness of previous trauma. All the patients reported the insidious onset of pain in the anterior part of the hip. All had a decreased passive ROM. Radiographic examination showed regional osteoporosis, premature closure of the femoral capital physis, narrowing of the joint space, and lateral overgrowth of the femoral head on the neck. All laboratory examinations were negative for evidence of infection or rheumatoid arthritis. Treatment consists of administration of aspirin, active non-loading exercise of the hip, and protected weight-bearing with crutches.
Question 68
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient’s history is significant for smoking. The most immediate appropriate postoperative management for this patient should include
Explanation
REFERENCES: Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953.
Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multi-level cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
Question 69
Patient outcomes can be improved and early post-injury management errors decreased by adhering to the Advanced Trauma Life Support (ATLS) protocol. This protocol includes criteria for inter-hospital transfer when the patient's needs exceed the resources available. Which of the following would it be acceptable to manage without interfacility transfer to a trauma center?
Explanation
While most patients can receive all their definitive care at any hospital to which they present, early recognition of those that require transfer to a trauma center is essential to maximizing outcomes. Inherent in such identification is physician's' assessment of their own and their institutions' abilities and the limits thereof.
Van Olden et al. prospectively studied severely injured patients consecutively presenting to two community hospitals in the Netherlands. Comparison was made between patients treated prior to and after introduction of ATLS training to physicians at the studied hospitals. There was no difference in overall mortality between the two groups. however, there was a significant reduction in mortality in the first 60 minutes after admission, from 24.2% pre-ATLS to 0.0% post-ATLS.
Ali et al. studied trauma outcomes and mortality in patients presenting to the largest hospital in Trinidad and Tobago for the four years prior to and after introduction of ATLS training for physicians in the emergency department. Trauma mortality decreased to 33.5% from 67.5% after introduction of ATLS. Post-injury functional outcomes were also improved.
Illustration A shows the ATLS guidelines for interfacility transfer in table format. Incorrect answers:
Question 70
Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 145-150, 324.
Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Wilkins, 1978, plate 4-46.
Question 71
A 67-year-old woman has a painful, arthritic proximal interphalangeal (PIP) joint, and nonsurgical measures have failed to improve the pain. What implant and joint replacement approach combination has been demonstrated to have the lowest rate of revision surgery?
Explanation
A recent systematic review compared silicone replacement, pyrocarbon replacement, and surface replacement arthroplasty for PIP arthritis. Silicone arthroplasty through a volar approach showed the greatest gains in arc of motion and had the lowest rate of revision surgeries. The rates of revision surgeries from low to high for each type of arthroplasty were 6% for silicone volar, 10% for silicone lateral, 11%
Surface replacement arthroplasty through a volar
for silicone dorsal, 18% for surface replacement dorsal, and 37% for surface replacement volar. Revision surgeries include implant replacement (to silicone or maintaining the surface replacement), arthrodesis, explantation, amputation, and other procedures.
approach showed the highest revision rate, the worst gain in arc of motion, and the greatest extension lag. However, substantial pain relief and higher satisfaction still were reported after surface replacement arthroplasty, regardless of the complications.
Question 72
What percentage of bone weight is collagen?
Explanation
Question 73
Figures below depict the radiographs obtained from a 76-year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?

Explanation
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a concern.
Question 74
Figure 68 is the radiograph of a 33-year-old runner who recently decided to begin running barefoot on trails. Since his transition to running without shoes 3 months ago, he has been having pain in the second metatarsophalangeal (MTP) joint. He feels like he is walking on a stone, notes edema in the ball of his foot, and has started to see a deviation of the second toe. What is the most likely etiology of these symptoms and findings?

Explanation
Lesser-toe plantar plate injuries are becoming increasingly recognized. Patients typically have an increase in pain, a positive Lachman test result upon examination, and deviation of the MTP joint. On radiograph, MTP subluxation can be appreciated. Nonsurgical treatment with a metatarsal pad may be attempted. Many patients who have surgery will have a partial or full tear of the plantar plate. The repair necessitates reinsertion of the plantar plate to the base of the proximal phalanx.
RECOMMENDED READINGS
Doty JF, Coughlin MJ, Weil L Jr, Nery C. Etiology and management of lesser toe metatarsophalangeal joint instability. Foot Ankle Clin. 2014 Sep;19(3):385-405. doi: 10.1016/j.fcl.2014.06.013. Epub 2014 Jul 10. PubMed PMID: 25129351. View Abstract at PubMed
Nery C, Coughlin MJ, Baumfeld D, Raduan FC, Mann TS, Catena F. Prospective evaluation of protocol for surgical treatment of lesser MTP joint plantar plate tears. Foot Ankle Int. 2014 Sep;35(9):876-85. doi: 10.1177/1071100714539659. Epub 2014 Jun 23. PubMed PMID:
Question 75
The primary purpose of obtaining the radiograph shown in Figure 9 is to assess
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Lequesne M, deSez S: Le faux profil du bassin: Nouvelle incidence radiographique pour l’etude de la hance. Son utilite dans les dysplasies et les differentes coxopathies. Rev Rhum Mal Osteoartic 1961;28:643.
Question 76
Figures 9a and 9b show the radiographs of a 75-year-old man who underwent a revision total knee arthroplasty with a long-stemmed tibial component. In rehabilitation, he reports fullness and tenderness in the proximal medial leg (at the knee). The strategy that would best limit this postoperative problem is use of
Explanation
REFERENCE: Gustke K: Cemented tibial stems are not requisite in revision. Orthopedics 2004;27:991-992.
Question 77
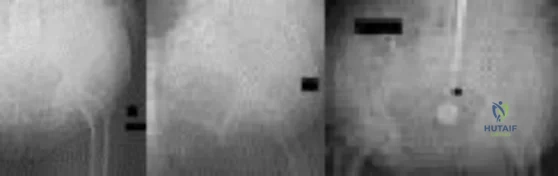
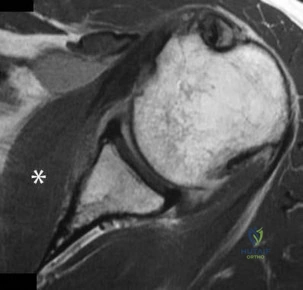
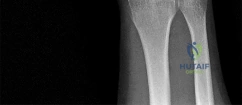
Chondrosarcoma The plain radiographs show a purely lytic destructive lesion that is poorly marginated. The technetium bone scan does not show any major uptake. The computerized tomography scan shows purely lytic bone destruction with breakthrough of the cortical bone. Complete destruction of the cortical bone is suggestive of a malignancy. The magnetic resonance image shows a lesion that is homogenously low on T1-weighted images and high on T2-weighted images. Surgeons cannot make a definitive diagnosis based upon the radiographic features. The most common malignancies in this age group are:
Explanation
Slide 5 Slide 6
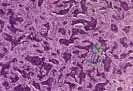
A 50-year-old woman has had severe hip pain for 4 months. Her plain radiographs (Slide 1), technetium bone scan (Slide 2), computerized tomography scan (Slide 3), and coronal T1- and T2-weighted magnetic resonance images (Slide 4) are presented. A needle biopsy is also performed (Slides 5 and 6). Which of the following treatment regimens would be the most appropriate:
Question 78
A 23-year-old national team rower reports pain over the radial dorsum of the forearm that is made worse with flexion and extension of the wrist during competition. His primary physician initially diagnosed de Quervain’s tenosynovitis, and a subsequent corticosteroid injection into the first dorsal compartment at the wrist provided no relief. The patient continues to report pain and audible crepitus that is noted 5 cm proximal to the wrist joint, on the radial aspect. What structures are involved in the continued pathology?
Explanation
REFERENCES: Grundberg AB, Reagan DS: Pathologic anatomy of the forearm: Intersection syndrome. J Hand Surg Am 1985; 10:299-302.
Thorson E, Szabo RM: Common tendinitis problems in the hand and forearm. Orthop Clin North Am 1992;23:65-74.
Williams JG: Surgical management of traumatic non-infective tenosynovitis of the wrist extensors. J Bone Joint Surg Br 1977;59:408-410.
Wood MB, Dobyns JH: Sports-related extraarticular wrist syndromes. Clin Orthop Relat Res 1986;202:93-102.
Question 79
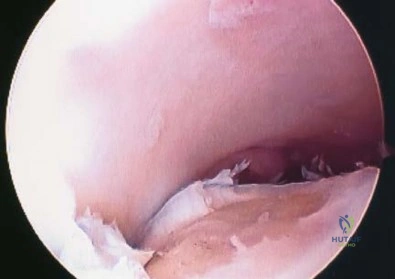
Figure 24 shows the arthroscopic view of a patient with ankle impingement syndrome. This is commonly seen after high ankle sprains and represents fibrotic granulation thickening of what structure?
Explanation
REFERENCES: Hopkinson WJ, St Pierre P, Ryan JB, Wheeler JH: Syndesmosis sprains of the ankle. Foot Ankle 1990;10:325-330.
Amendola A: Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle 1992;13:44-50.
Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
Pfeffer GB (ed): Chronic Ankle Pain in the Athlete. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 11.
Question 80
Figure 21 shows the tomogram of a 26-year-old woman who sustained an axial load injury to her neck in a fall off a horse. What ligament is injured?
Explanation
REFERENCES: Levine AM, Edwards CC: Fractures of the atlas. J Bone Joint Surg Am 1991;73:680-691.
Kurz LT: Fractures of the first cervical vertebra, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 409-413.
Question 81
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?
Explanation
REFERENCES: Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment.
J Am Acad Orthop Surg 2001;9:268-278.
Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Duchesneau S, Fallat LM: The Tillaux fracture. J Foot Ankle Surg 1996;35:127-133.
Question 82
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?
Explanation
REFERENCES: Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 83
A 35-year-old man has a brachial plexus injury affecting the lateral cord. He partially improves with observation and now has complete return of median nerve function and pectoral muscle function. What nerve transfer is most likely to restore the motor function he is lacking?
Explanation
The lateral cord of the brachial plexus gives off the lateral pectoral nerve, the musculocutaneous nerve, and then contributes to the median nerve. The patient has had recovery of function of these components except for the musculocutaneous nerve. The musculocutaneous nerve innervates the biceps and the brachialis, which provide elbow flexion. To restore motor function, a nerve transfer would have to provide reinnervation of the biceps and brachialis.
Question 84
Which of the following factors has the greatest effect on the pull-out strength of a lumbar pedicle screw?
Explanation
REFERENCES: Wittenberg RH, Shea M, Swartz DE, et al: Importance of bone mineral density in instrumented spine fusions. Spine 1991;16:647-652.
Zindrick MR, Wiltse LL, Widell EH, et al: A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop 1986;203:99-112.
Question 85
Figures below show the radiographs, and the MRIs obtained from a 32-year-old man with worsening left knee pain. A 3-foot hip-to-ankle radiograph shows a 13-degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago, and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often, and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to reduce stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after the correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL
reconstruction alone is not indicated for this patient.
Question 86
A 14-year-old girl with a right thoracic curve from T4 through L2 measuring 78 degrees is scheduled to undergo posterior spinal fusion for scoliosis. The surgical plan is to fuse from T3 through L2, using pedicle screws at L2 and about the apex at T8. What neural monitoring modality is most likely to identify a reversible neurologic deficit during surgery?
Explanation
REFERENCES: Padberg AM, Wilson-Holden TJ, Lenke LG, Bridwell KH: Somatosensory- and motor-evoked potential monitoring without wake-up test during idiopathic scoliosis surgery: An accepted standard of care. Spine 1998;23:1392-1400.
Schwartz DM, Drummond DS, Hahn M, Ecker MI, Dormans JP: Prevention of positional brachial plexopathy during surgical correction of scoliosis. J Spinal Disord 2000;13:178-182.
Question 87
A 17-year-old boy is shot in the left side of the neck at the C5-6 level and sustains an incomplete spinal cord injury that is called a Brown-Sequard syndrome. Which of the following best describes the expected deficits? Review Topic
Explanation
Question 88
A 66-year-old man who underwent shoulder arthroplasty 7 years ago reports progressively worsening shoulder pain for the past 4 weeks after hospital discharge for community-acquired pneumonia. He is afebrile and reports no chills or night sweats. Laboratory studies show a white blood cell count of 11,200/mm3 and an erythrocyte sedimentation rate of 25/h. Shoulder radiographs are negative for fracture, dislocation, or signs of implant loosening. What is the most appropriate management? Review Topic
Explanation
Question 89
When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more than the extension space?
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point,
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 90
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?
Explanation
REFERENCES: Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Crockett HC, Gross LB, Wilk KE, et al: Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med 2002;30:20-26.
Question 91
A 13-year-old girl has had increasing left hip pain for the past 4 months. A radiograph, bone scan, MRI scan, and photomicrograph are shown in Figures 1a through 1d. Which of the following immunohistochemistry results would confirm the most likely diagnosis?
Explanation
REFERENCES: Halliday BE, Slagel DD, Elsheikh TE, et al: Diagnostic utility of MIC-2 immunocytochemical staining in the differential diagnosis of small blue cell tumors. Diagn Cytopathol 1998;19:410-416.
Llombart-Bosch A, Navarro S: Immunohistochemical detection of EWS and FLI-1 proteins is Ewing sarcoma and primitive neuroectodermal tumors: Comparative analysis with CD99
(MIC-2) expression. Appl Immunohistochem Mol Morphol 2001;9:255-260.
Question 92
Which of the following factors are considered prognostic of survival in patients with soft-tissue sarcomas?
Explanation
REFERENCES: Cheng EY, Thompson RC Jr: New developments in the staging and imaging of soft-tissue sarcomas. Instr Course Lect 2000;49:443-451.
Fleming ID, et al: Manual for Staging of Cancer/American Joint Committee on Cancer, ed 5. Philadelphia, PA, Lippincott Raven, 1997, pp 149-156.
Question 93
.Figures 59a and 59b are the axial T2 and T1 with contrast MRI scans of a 32-year-old woman who has a 10-year history of pain and a 1-year history of progressive swelling in her right leg. The histopathology is shown in Figure 59c. A radiograph of her leg showed no mineralizations or osseous erosions. The chromosomal abnormality that is associated with this disease is
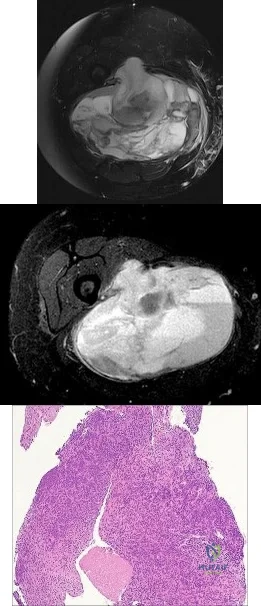
Explanation
A 45-year-old woman has an enlarging buttock mass. The mass is 12 cm and nonpainful. The patient first noticed it about 6 months after she had a low-impact fall. The general surgeon evaluating the patient felt this mass could be either a lipoma or a hematoma. The patient underwent a surgical procedure to remove the mass.
Question 94
A 65-year-old woman sustained an axial load on the arm followed by an abduction injury after falling on ice. Treatment in the emergency department consisted of reduction of an anterior dislocation. She now has a positive drop arm sign and a positive lift-off test. An MRI scan is shown in Figure 9. Based on these findings, management should consist of
Explanation
REFERENCES: Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes.
J Am Acad Orthop Surg 1999;7:300-310.
Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Walch G, Boileau P: Subluxations and dislocations of the tendon of the long head of the biceps. J Shoulder Elbow Surg 1998;7:100-108.
Question 95
Which of the following amputations will lead to the greatest oxygen requirement per meter walked following prosthesis fitting?

Explanation
Question 96
- Which of the following factors is used to determine torsional rigidity of a long bone fracture under internal or external fixation?
Explanation
quantity having a magnitude and direction. Torsion involves shear and tensile stresses that cause deformation. Thus torsional rigidity is related to bone rotation and the torque applied to it.
Question 97
What mechanism is most likely responsible for the initiation of mechanical failure seen at the midstem modular junction of modular revision hip stems?
Explanation
Question 98
A 27-year-old woman with Down syndrome has a severe bunion with pain and deformity in the left forefoot. Nonsurgical management has failed to provide relief. She does not use any assistive ambulatory devices. A radiograph is shown in Figure 21. Treatment should now consist of
Explanation
REFERENCES: Coughlin MJ, Abdo RV: Arthodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
Mann RA: Disorders of the first metatarsophalangeal joint. J Am Acad Orthop Surg 1995;3:34-43.
Question 99
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?
Explanation
REFERENCES: Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Cannon LB, Hackney RG: Anterior tibiotalar impingement associated with chronic ankle instability. J Foot Ankle Surg 2000;39:383-386.
Question 100
Following insertion of a cementless femoral component into the total hip arthroplasty construct, the amount of femoral stress shielding is most associated with
Explanation
Although material modulus, characteristics of surface, and extent of coating all contribute to stress shielding, poor bone quality is the most important factor associated with stress shielding.