Orthopedic Surgery Board Review MCQs: Hip & Spine | Part 169

Key Takeaway
This page presents Part 169 of an interactive orthopedic surgery board review quiz. Targeting orthopedic residents and surgeons, it offers 100 high-yield MCQs mirroring OITE and AAOS exam formats. Prepare confidently with verified questions, clinical explanations, and two learning modes to achieve board certification.
About This Board Review Set
This is Part 169 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 169
This module focuses heavily on: Hip.
Sample Questions from This Set
Sample Question 1: If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?...
Sample Question 2: Which gene correlates with severity of disease in spinal muscular atrophy (SMA)? Review Topic...
Sample Question 3: What is the most common location of osteosarcoma?...
Sample Question 4: Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in...
Sample Question 5: Which clinical signs are consistent with the diagnosis of cauda equina syndrome?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?
Explanation
REFERENCES: Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-807.
Garfin SR, Rauschning W: Spinal stenosis. Instr Course Lect 2001;50:145-152.
Question 2
Which gene correlates with severity of disease in spinal muscular atrophy (SMA)? Review Topic
Explanation
Question 3
What is the most common location of osteosarcoma?
Explanation
REFERENCES: Malawer MM, Sugarbaker PH, Malawer M: Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Kluwer Academic Publishers, 2001.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 4
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Robinson RP, Lovell TP, Green TM, Bailey GA: Early femoral component loosening in DF-80 total hip arthroplasty. J Arthroplasty 1989;4:55-64.
Question 5
Which clinical signs are consistent with the diagnosis of cauda equina syndrome?
Explanation
Cauda equina syndrome is a lower-motor neuron deficit. Hyperreflexia, clonus, and other upper-motor neuron findings would not be seen. Saddle anesthesia, motor weakness, and neurogenic bladder are elements critical to the diagnosis of cauda equina syndrome.
RECOMMENDED READINGS
Kostuik JP, Harrington I, Alexander D, Rand W, Evans D. Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am. 1986 Mar;68(3):386-91. PubMed PMID: 2936744. View Abstract at PubMed
Spector LR, Madigan L, Rhyne A, Darden B 2nd, Kim D. Cauda equina syndrome. J Am Acad Orthop Surg. 2008 Aug;16(8):471-9. Review. PubMed PMID: 18664636. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 78 THROUGH 80
Figures 78a and 78b are the axial and sagittal MR images of an otherwise healthy 24-year-old woman who has had 8 weeks of severe leg pain without weakness.
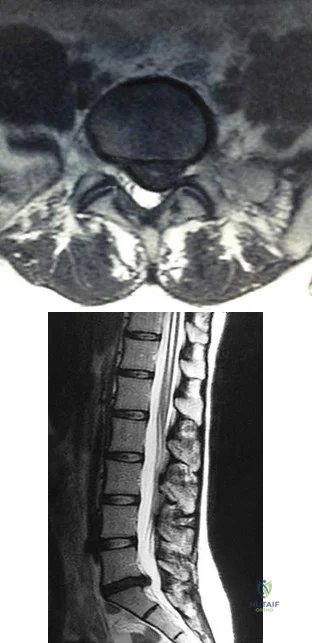
A B
Question 6
For patients undergoing a surgical procedure where the risk of requiring a transfusion is less than 10%, the International Committee of Effective Blood Usage suggests
Explanation
REFERENCES: Toy P, Beattie C, Gould S, et al: Transfusion alert: Use of autologous blood. National Heart, Lung, and Blood Institute Expert Panel on the use of autologous blood. Transfusion 1992;35:703-711.
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 7
A 54-year-old woman undergoes an interposition arthroplasty that fails and requires conversion to a total elbow arthroplasty. She has progressive elbow pain and radiographic loosening. Erythrocyte sedimentation rate and C-reactive protein are normal. Joint aspiration is positive for Staphylococcus epidermidis. What surgical treatment would best optimize function and decrease risk of recurrence?
Explanation
is best reserved for low-demand or infirm patients.
Question 8
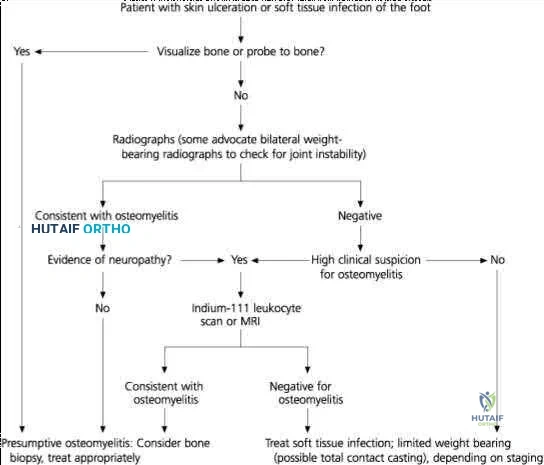
Figures 1 through 4 show the radiographs and MRI obtained from a 40-year-old man who has a 6-week history of ring finger pain, redness, and swelling after puncturing the finger with a toothpick. Purulent drainage from the puncture wound site grew Eikenella corrodens . The patient was initially treated with oral antibiotics for 10 days and then intravenous (IV) antibiotics for 3 weeks. What is the best next step in treatment?

Explanation
This patient has a septic distal interphalangeal joint, which was treated with antibiotics alone. As a result, the patient developed osteomyelitis with bone destruction and abscess. The best way to treat this problem is to perform surgical débridement of bone and soft tissue, along with abscess drainage and an appropriate antibiotic regimen. Antibiotic treatment without surgery would not be successful in eliminating this particular infection. Bone scan with biopsy is not the correct option, because this problem is an infection and not a tumor, and MRI already has provided enough diagnostic information.
Question 9
03 A 23 year old sustains an isolated right knee dislocation in an MVA. A closed reduction is performed and confirmed with radiographs. What is the next appropriate study?
Explanation
OKU Truama 2 says “the use of ABI with the blood pressure cuff and Doppler evaluation of the distal circulation has been proposed as effective in determining any occult vascular injury. A ratio > 0.9indicates a normal study.”[1] The referenced article confirms this. “Confirmation of the safety and accuracy of physical exam in the evaluation of knee dislocation for injury of the popliteal artery.” J. Trauma2002; 52: 247-252
back to this question next question
[1] OKU Trauma 2 pg 151-153
Question 10
A 30-year-old farmer undergoes replantation of an above-the-elbow amputation. What form of management is most important following this surgery?
Explanation
REFERENCES: Wood MB: Replantations about the elbow, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1985, pp 472-480.
Goldner RD, Nunley JA: Replantation proximal to the wrist, in Wood MD (ed) Hand Clinics: Microsurgery. Philadelphia, PA, WB Saunders, 1992, pp 413-425.
Question 11
The lateral arm flap is based on what arterial supply?
Explanation
REFERENCES: Katsaros J, Tan E, Zoltie N: The use of the lateral arm flap in upper limb surgery. J Hand Surg 1991;16:598-604.
Katsaros J, Schusterman M, Beppu M, et al: The lateral upper arm flap: Anatomy and clinical applications. Ann Plast Surg 1984;12:489-499.
Question 12
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include
Explanation
REFERENCES: Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Fisher SE, Shelbourne KD: Arthroscopic treatment of symptomatic extension block complicating anterior cruciate ligament reconstruction. Am J Sports Med 1993;4:558-564.
Question 13
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management? Review Topic

Explanation
Question 14
A 13-year-old girl with hallux valgus reports pain after playing basketball. Radiographs show a hallux valgus angle of 20 degrees, an intermetatarsal angle of 11 degrees, a distal metatarsal articular angle of 10 degrees, and a congruent joint. Management should consist of
Explanation
REFERENCES: Stephens HM: Bunions, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1510-1519.
Donley BG, Richardson GE: Disorders of the first ray, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1718-1731.
Question 15
A 58-year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 16
Which of the following tendons is found in the same dorsal compartment of the wrist as the posterior interosseous nerve?
Explanation
1st Compartment: Abductor pollicis longus, extensor pollis brevis
2nd Compartment: Extensor carpi radialis brevis, extensor carpi radialis longus
3rd Compartment: Extensor pollicis longus
4th Compartment: Extensor digitorum comminus, extensor indicus proprius, posterior interosseous nerve
5th Compartment: Extensor digiti minimi
6th Compartment: Extensor carpi ulnaris
The extensor indicis proprius is also contained in the fourth dorsal compartment. The extensor digiti minimi is located in the fifth dorsal compartment. The extensor carpi radialis brevis is located in the second dorsal compartment. The extensor pollicis longus is located in the third dorsal compartment, and the abductor pollicis longus is located in the first dorsal compartment.
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 150-151.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 60.
Question 17
A year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 18
A 14-year-old gymnast presents after a fall from the balance beam with a hyperextension injury to her left knee. She could ambulate with pain but was unable to continue exercise due to pain. On examination she has a swollen knee with painful

Explanation
Tibial eminence fractures are rare but occur more often in pediatric populations, often in the setting of sports-related injuries. Debate continues over operative vs nonoperative treatment, as well as fixation type (screw vs suture) for openly treated fractures. Past evidence suggested closed treatment was adequate but there has been an increase in operative management. Closed treatment is suggested for minimally displaced fractures (Type I and reducible Type II) and open treatment for completely displaced fractures (non-reducible Type II and Type III).
Wilfinger et al provide the results of a closed reduction protocol at their institution including 38 patients with long term followup. All patients underwent aspiration and closed reduction in the OR under fluoroscopic guidance followed by long leg casting in hyperextension and graduated weight bearing over weeks. No patients complained of persistent pain, swelling, giving way, or disability at follow up.
However, Edmonds et al in a retrospective review compare open reduction internal fixation (ORIF), arthroscopic-assisted internal fixation (AAIF), and closed reduction with casting (CRC) for pediatric patients with displaced tibial spine fractures. They report improved reduction but also increased arthrofibrosis in ORIF and AAIF groups
compared to CRC, but of the 24% of patients with long term followup results, there was no difference in functional outcomes across all 3 groups. There was a 17% rate of later operation for the CRC group patients. They suggest closed treatment for fractures with <5mm displacement, otherwise ORIF or AAIF.
Gans et al conducted a systematic review focused on the questions of open vs closed reduction, and screw vs suture fixation. The 26-article review found insufficient evidence to have any clear recommendations. They did find reduced laxity and improved range of motion for minimally displaced fractures that had an open reduction, and that completely displaced fractures treated nonoperative had higher rates of nonunion.
Figures A and B are AP and lateral knee radiographs demonstrating a moderately displaced (Meyers and McKeever Type II) tibial spine fracture in a skeletally immature patient.
Incorrect Responses
Question 19
Figure 1 is an MRI scan of the right hip of a 19-year-old woman with a 6-month history of right groin pain. She was diagnosed with a stress fracture and was treated with 3 months of limited weight bearing. Figure 2 is a repeat MRI scan in which the edema pattern changed minimally but the pain worsened. Ibuprofen alleviates most of her pain. What is the best next step?

Explanation
cells, forms the nidus of the tumor, which is easily identified on CT scans.
Question 20
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi Y: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7;223-227.
Question 21
A 25-year-old man has a mass on the medial aspect of the left knee. He reports that the mass has been present for several years, but a recent increase in physical activity has resulted in periodic tenderness. Radiographs are shown in Figures 13a and 13b. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 22
Thermal capsulorrhaphy of the inferior glenohumeral ligament can cause iatrogenic injury to which of the following nerves?
Explanation
REFERENCES: Wong KL, Williams GR: Complications of thermal capsulorrhaphy of the shoulder. J Bone Joint Surg Am 2001;83:151-155.
Bryan WJ, Schauder K, Tullos HS: The axillary nerve and its relationship to common sports medicine shoulder procedures. Am J Sports Med 1986;15:113-116.
Question 23
A 58-year-old woman who underwent a successful total hip replacement for degenerative arthritis 8 years ago reports groin pain for the past 6 months. A radiograph of the hip is shown in Figure 32. At revision, severe deficiency of the posterior column is noted. What reconstructive option would be most appropriate for the acetabulum?
Explanation
REFERENCES: Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 24
Figure 30 shows the radiograph of a 38-year-old man who reports persistent pain laterally and plantarly about the fifth metatarsal head. Examination reveals calluses dorsolaterally and plantarly about the fifth metatarsal head. Nonsurgical management has failed to provide relief. Surgical treatment should include
Explanation
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Moran MM, Claridge RJ: Chevron osteotomy for bunionette. Foot Ankle Int 1994;15:684-688.
Question 25
What is the most common non-anesthetic-related reversible cause of sustained changes in intraoperative neurophysiologic monitoring signals during spinal surgery? Review Topic
Explanation
Question 26
A 67-year-old woman has had pain in the area of the metatarsal heads and toes bilaterally for the past 18 months. She describes a diffuse discomfort and a constant burning sensation. She notes that the area feels swollen. Examination reveals that her pulses are normal, and there is no frank swelling or focal tenderness. What is the most likely diagnosis?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-121.
Gorson KC, Ropper AH: Idiopathic distal small fiber neuropathy. Acta Neurol Scand 1995;92:376-382.
Question 27
-A collegiate offensive football lineman has decreased bench-press strength and shoulder pain as off-season workouts begin. Examination revealed no atrophy, and deltoid and rotator cuff strength testing findings were normal. Translational testing was difficult to achieve because of his large size.Apprehension and relocation test findings were negative. An O’Brien’s active compression test result was negative. Jerk testing was positive on the affected side. Which diagnosis is most likely revealed on an MRI arthrogram?
Explanation
Question 28
A 21-year-old male is brought to the emergency department after being involved in gang-related violence. A radiograph of his pelvis is shown in Figure A. The patient is hemodynamically stable. Which of the following imaging modalities is the next best step in evaluating this patient for the most common associated injury? Review Topic

Explanation
The incidence of GSW is increasing and it is the 2nd leading cause of death in young males in the US after motor vehicle accidents. The incidence of a GSW to the buttock is approximately 8% of all GSW to the extremities. Potential complications of pelvic and acetabular GSW include septic arthritis, enterocutaneous, enteroacetabular, and vesicoacetabular fistulas, infected nonunion, malunion, and injuries to the iliac vessels. The presence or absence of intra-abdominal injuries affects treatment and outcome.
Bartkiw et al. reviewed 2808 GSW and found 1235 associated fractures including 42 fractures of the hip and pelvis. Ten orthopaedic operative procedures were performed in 7 patients. Associated nonorthopaedic injuries included 15 small/large bowel perforations (36%), 7 vessel lacerations (17%), and 2 urogenital injuries (5%) that required surgery.
Najibi et al. reviewed 39 GSW to acetabulum. They found 32 simple and 7 associated fracture patterns. The most common simple and associated patterns were anterior column and both column, respectively. Bowel injuries were the most common associated injures (42%). Predictors of poor outcome include high-velocity missile, involvement of acetabular dome, abdominal injury, nerve injury, vascular injury, and male gender. Deep infection was associated with primary anastomosis of bowel injury and an associated fracture pattern.
Figure A shows a GSW to the right hip with acetabular fracture and visible bullet fragment.
Incorrect Answers:
Question 29
use of a true lateral to assess the DRUJ, 4) beginning early range of motion of the wrist after stable fixation and 5) use vitamin C to help mitigate intractable pain.
Explanation
A 26-year-old male sustains a fall from a ladder onto his outstretched right hand. He is evaluated in the emergency room and is found to have a closed injury to his elbow without evidence of neurovascular compromise. Plain radiographs are obtained and are shown in Figures A and B. During surgery a sequential approach is used to treat each element of this injury. Which part of the procedure is felt to add the most to rotatory stability?

Radial head replacement
Radial head ORIF
Capsular plication
Lateral collateral ligament complex repair or reconstruction
Medial collateral ligament complex reconstruction Corrent answer: 4
The essential lesion that results in the most instability in a terrible triad injury of the elbow is rupture of the lateral collateral ligament. Repair of this lesion
results in the greatest increase in elbow rotatory stability.
The key components of a terrible triad injury are a radial head fracture, coronoid fracture, dislocation of the ulnohumeral joint and disruption of the lateral collateral ligament complex. While restoration of the bony anatomy is important for static stability, the key primary stabilizer that needs to be addressed is the lateral collateral ligament complex. In acute injuries LCL repair may be possible. In chronic injury, LCL reconstruction would need to be considered.
Forthman et al. reviewed 34 patients with an elbow dislocation, 22 of 34 of which were terrible triad injuries. Open reduction internal fixation or radial head replacement (as appropriate) along with LCL repair was completed; the MCL was not surgically addressed. Seventeen of 22 had good or excellent results, indicating that MCL repair is not necessary.
Pugh et al. discuss their surgical protocol for addressing terrible triad injuries with 28/36 of their patients obtaining good or excellent results. Their inside out protocol is described as follows: 1) coronoid fracture ORIF (capsular repair), 2) radial head fracture ORIF or replacement 3) LCL complex repair (isometric point is center of capitellum), 4) reevaluation of stability; MCL repair or hinged fixator application
Jensen et.al in cadaveric studies have demonstrated that radial head replacement alone decreases varus laxity and external rotatory laxity to 14.6 &
Question 30
Radiographs of the femur are unremarkable. A radionuclide bone scan demonstrates abnormal uptake in the mid-femur. A radionuclide bone marrow scan demonstrates decreased uptake within the marrow. Which of the following is the best step in management?
Explanation
Skaggs et al reviewed 79 cases of acute extremity pain in sickle cell patients. Radionuclide bone marrow and bone scan was used to differentiate osteomyelitis from bone infarct. Four cases of infection were diagnosed by normal uptake on the bone marrow scan and abnormal uptake on the bone scan. These cases were confirmed osteomyelitis by positive culture. Seventy cases were diagnosed as bone infarct by decreased uptake on the bone marrow scan and abnormal uptake bone scan.
Chambers et al reviewed the charts of 2000 known sickle cell patients. Fourteen patients had an episode of osteomyelitis or septic arthritis. Radiographs and bone scans were not helpful in differentiating infection from an acute bone infarct. Salmonella was the most frequent organism cultured from the osteomyelitis cases. The authors recommend bone aspiration or biopsy in an sickle cell patient with extremity pain, swelling, and a fever greater than 38.2 degrees C.
An otherwise healthy, 65-year-old male undergoes a right total knee arthroplasty without complications. Which of the following statements is recommended by the American Academy of Orthopaedic Surgeons Clinical Practice Guidelines for preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty?
Administer aspirin one week pre-operatively
Use elastic compressive stockings for 10 days pre-operatively
Obtain a post-operative duplex ultrasound of the patient for screening purposes
Administer Coumadin to maintain the patient’s INR between 1.5 and 2.5 during the post-perative period
Use mechanical compressive devices in the postoperative period
Use of mechanical compressive devices and aspirin during the postoperative period is
recommended by the American Academy of Orthopaedic Surgeons Clinical Practice Guidelines.
In 2011, the American Academy of Orthopaedic Surgeons published their Clinical Practice Guidelines for preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. A summary of those guidelines provide general recommendations for venous thromboembolic disease in patients with and without bleeding disorders. These recommendations range from strong (recommending against the use of routine post-operative duplex ultrasonography), to moderate (using mechanical compressive devices or a pharmacologic agent for prophylaxis in the post- operative period), to inconclusive (they are unable to recommend for or against specific pharmacologic prophylaxis agents). Additionally, there are recommendations based on consensus agreement of the authors (the recommendation of early mobilization in the post-operative period).
These guidelines are now much closer to in agreement with the American College of Chest Surgeons (ACCS) 2012 guidelines for VTE prophylaxis. One of the differences between the guidelines is that the AAOS guidelines do not state a specific amount of time that a pharmacologic agent should be given post- operatively while the ACCS recommends such agents for a minimum of 10-14 days.
Incorrect answers:
The definition of effect size is best described as which of the following?
Likelihood that a statistically significant difference would be found between 2 groups given that a difference truly did exist
Estimated magnitude of the difference in the means between two groups
Average of the squares of each value's deviation from the mean
Range within which it is probable that the true value lies for the whole population of patients
Probability of obtaining a result equal to or more extreme than what was actually observed assuming the null hypothesis is true
The effect size is best defined as the magnitude of the difference in the means of the control and experimental groups in a study with respect to the pooled standard deviation. Effect sizes are normally used for continuous variables in contrast to relative risk reduction which is used for dichotomous variables. Power (1), variance (3), confidence interval (4), and P value (5) are the other options provided.
Which of the following patients are at greatest risk of having a future vertebral fragility fracture?
Elderly female with prior hip fragility fracture
Elderly female with prior distal radius fragility fracture
Elderly female with prior T6 compression fragility fracture
Elderly female with a T-score of -3.0
Elderly female currently on hormone replacement therapy
History of a prior vertebral fragility fracture is the strongest predictor of a future fragility fracture. A meta-analysis by Klotzbuecher et al examined risk factors for fragility fractures and found an association between prior and subsequent fragility fractures. The strongest associations were observed between prior and subsequent vertebral fractures. They found women with preexisting vertebral fractures had an approximately 4 times greater risk of subsequent vertebral fractures than those without prior fractures. They also found this risk increases with the number of prior vertebral fractures. Other combinations of prior and future fracture sites, such as the hip or wrist, were also strongly associated, but none so high as vertebral fractures.
A 79-year-old female falls onto her right hip at home and sustains the injury shown in Figure A. She undergoes an uncemented unipolar hemiarthroplasty. During insertion of the stem into the femoral canal, the patient becomes hypotensive and hypoxic. Which of the following has most likely occurred?
Femoral shaft fracture
Inadequate fluid resuscitation during surgery
Acute myocardial infarction
Pulmonary embolism caused by dislodging of deep venous thrombosis during hip exposure
Intramedullary fat and marrow embolization
During insertion of the femoral stem, the intramedullary pressures are increased. Fat and marrow elements can become embolized into the bloodstream at this point resulting in ventilation perfusion mismatch in the lungs.
Kim et al prospectively followed 156 total hip arthroplasties including bilateral and unilateral procedures as well as cemented and uncemented procedures. They found no difference in fat embolization amongst any of the groups. However, they did find that if patients had evidence of bone marrow cells in the right atrium on the first postoperative day, they developed diffuse encephalopathy with confusion and agitation that lasted for about twenty-four hours.
Which of the following investigative studies is most useful in the definitive diagnosis of Amyotrophic Lateral Sclerosis (ALS)?
Genetic testing
MRI brain and spinal cord
Muscle biopsy
Serum protein electrophoresis and immunoelectrophoresis
Electrodiagnostic studies
The diagnosis of ALS requires a period of clinical observation to document the progressive loss of upper and lower motor function. Electrodiagnositic studies are required to make a definitive diagnosis.
Amyotrophic lateral sclerosis (ALS) is the most common degenerative disease of the motor neuron system. Nerve conduction studies and needle electromyography (EMG) are useful for confirming the diagnosis of ALS and for excluding peripheral conditions that resemble ALS. Hallmark findings in the electrodiagnosis of ALS are abnormal motor nerve conduction studies, with normal sensory nerve conduction studies. UMN signs are mild weakness, spasticity, and abnormally brisk reflexes; LMN signs are progressive weakness, wasting, and loss of reflexes and muscle tone.
Brooks et al. developed a diagnostic algorithm for the diagnosis of ALS. The algorithm is based on the degree of certainty of diagnosis, which is increased by the number of body segments that demonstrate upper motor neuron (UMN) and lower motor neuron (LMN) abnormalities. Clinical and electrophysiologic findings in 3 or more body segments is definitive of the diagnosis.
Incorrect Answers:
Radiographic changes suggestive of osteopetrosis in children are a known complication of which of the following types of medications?
TNF-alpha inhibitors
Bone morphogenic proteins
Bisphosphonates
Fluoroquinolones
RANKL antibiodies
Radiographic changes suggestive of osteopetrosis (marble bone disease) are a known complication of bisphosphonate usage. The common cellular pathway in this process is the osteoclast. Bisphosphonates target and inhibit the osteoclast, and these cells are not functioning in patients with osteopetrosis.
Whyte et al describe a case report of a 12-year-old child with idiopathic hyperphosphatasia treated with bisphosphonates who developed osteopetrosis.
Falk et al report on their small case series which showed the beneficial effects and known complications in the treatment of osteogenesis imperfecta with bisphosphonate therapy.
Marini presents a perspective article describing the off-label use of bisphosphonates in children.
What function does computerized physician order entry have on medication monitoring?
Reduces the rate of medication errors
Improves physician satisfaction
Decreases narcotic requirements by patients
Increases rates of allergy related medication errors
Improves physician knowledge about the drugs they are prescribing
Computerized physician order entry has greatest impact on reducing medication errors.
Bobb et al. studied medication errors averted by pharmacists at a 700-bed academic center and concluded that 65% of them would likely have been prevented with computerized physician order entry.
Upperman et al. reviewed medication errors at a pediatric hospital before and after implementation of a computerized physician order entry system. They found a significant decrease in adverse drug events following establishment of the computerized system.
Incorrect Answers:
2: Physician satisfaction has not been correlated with computer entry for medications.
3: Narcotic requirements are related to injury or patient characteristics, not computerized entry.
4: Allergy-related errors are decreased with use of computerized entry.
5: Physician knowledge is not necessarily increased with computerized entry.
What is the cellular mechanism of action for non-nitrogen containing bisphosphonates (such as clodronate and etidronate) to induce osteoclast apoptosis?
Inhibiting caspase
Inhibiting matrix metalloprotease
Inhibiting reverse transcriptase
Targeting of farnesyl diphosphate synthase
Creating toxic analog of adenosine triphosphate that targets mitochondria
Bisphosphonates work by one of two mechanisms. Non-nitrogren containing bisphosphonates (such as etidronate and clodronate) work by creating a toxic analog of ATP which inhibits ATP and leads to osteoclast apoptosis. Nitrogen containing bisphosphonates (such as alendronate, risedronate, and zoledronate) inhibit the enzyme farnesyl diphosphate synthase which prevents protein geranylgeranylation and prevents osteoclastic bone resorption.
Reska et. al. specifically discuss the difference between the two pathways. Non-nitrogen containing compounds inhibit ATP production and cause osteoclast apoptosis. Nitrogen containing bisphophonates inhibit protein synthesis by interrupting the cholesterol biosynthetic pathway, which prevents osteoclastic resorption.
Which class of antibiotics inhibit early fracture healing through toxic effects on chondrocytes?
cephalosporins
quinolones
penicillins
macrolides
sulfonamides
Animal models have shown that quinolones inhibit early fracture healing through a toxic effect on chondrocytes. The study by Perry et al demonstrated that fracture calluses in the animals treated with quinolones showed a lower histologic grade as compared with control animals representing a less mature callus with the presence of more cartilage and less woven bone. The study by Huddleston et al demonstrated fracture calluses in the animals treated with ciprofloxacin showed abnormalities in cartilage morphology and endochondral bone formation and a significant decrease in the number of chondrocytes compared with the controls. None of the other antibiotics listed are known to have toxic effects on chondrocytes.
A mutation of the retinoblastoma gene RB-1 leads to the development of malignancies such as retinoblastoma and osteosarcoma. Which term best characterizes the RB-1 gene?
growth factor
retro-oncogene
proto-oncogene
oncogene
tumor suppressor
A tumor suppressor is a gene whose presence normally prevents neoplasia and whose absence leads to unregulated cell growth. Two well-studied tumor suppressor genes include p53 and RB-1. P53 normally suppresses cell division by blocking the cell cycle if genetic damage is present. If it is absent or mutated, the p53 suppressing effect no longer regulates cell growth and neoplasm results. In a similar fashion, a mutation in RB-1, or the retinoblastoma gene, may leads to retinoblastoma and osteosarcoma.
Youarecounseling ayoungfemalepatientabout herfuturerisk of osteoporosis. Which of the following regarding peak bone mass (PBM) is true?
PBM is consistently attained by the end of the second decade of life in both men and women.
PBM is independent from environmental factors.
PBM correlates strongly with post-menopausal bone mineral density
Timing of PBM varies based on anatomic site.
Women attain PBM prior to men, regardless of anatomic site. Corrent answer: 4
The timing and magnitude of PBM varies based on anatomic site. PBM is often reached in the appendicular skeleton earlier than in the axial skeleton.
PBM is defined as the greatest amount of bone an individual will attain in his or her lifetime. Controversy has surrounded the timing of PBM due to significant anatomical variations as well as strong gender-based, genetic, geographic, environmental, and mechanical influences. While women may reach PBM
earlier than men in the hip, the converse has been found to be true of the spine. Furthermore, the age at which each is obtained varies widely. Though the PBM of the hip is most often achieved by the end of the second decade of life, PBM of the spine may not occur until the third or fourth decade of life. Interestingly, PBM has been found to correlate poorly with post-menopausal bone mineral density, likely a result of these strong confounding influences.
Bonjour et al. reviewed the controversy behind peak bone mass. The authors note that the gender-based difference in bone mass becomes expressed during puberty and that there is a large variability in normal values of bone mineral density between anatomic sites.
They conclude that bone mass accumulation can be completed by the end of the second decade at both the lumbar spine and femoral neck, but that this may be significantly influenced by a number of variables during growth such as genetics, diet, endocrine and mechanical factors.
Berger et al. more recently evaluated trends in peak bone mass from longitudinal data in the Canadian Multicentre Osteoporosis Study (CaMos). The authors found that peak bone mass was highly variable between the axial and appendicular skeleton. Specifically, lumbar spine PBM was reached in women
at 33-40 years, but much earlier in men at 19-33 years. Conversely, hip PBM was reached earlier in women at 16-19 years and later in men at 19-21 years. Furthermore, there was a lack of concordance between PBM and BMD over age
Question 31
0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C). What is the most appropriate management for the femoral shaft fracture at this point?
Explanation
Question 32
A 72-year-old man with a history of Parkinson’s disease, stable coronary artery disease, and mild renal insufficiency is seen for hip arthroplasty. Which of the following is considered the most appropriate bearing of choice?
Explanation
REFERENCES: Bragdon CR, Greene ME, Freiberg AA, et al: Radiostereometric analysis comparison of wear of highly cross-linked polyethylene against 36- vs 28-mm femoral heads. J Arthroplasty 2007;22:125-129.
MacDonald SJ: Metal-on-metal total hip arthroplasty: The concerns. Clin Orthop Relat Res 2004;429:86- 93.
Question 33
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?

Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the osteoarthritis.
Question 34
A 16-year-old competitive female swimmer has a 1-year history of left shoulder pain. She denies any specific injury to her shoulder. She reports that the pain is worse with swimming but also has pain with daily activities. She also notes similar occasional symptoms in her right shoulder. Examination reveals symmetric range of motion and rotator cuff strength. Examination of the left shoulder reveals 2+ anterior and posterior translation with pain in both directions and a 2-cm sulcus sign. The right shoulder also has 2+ anterior and posterior translation and a 2-cm sulcus sign with no pain. She also has hyperextension of the elbows and the ability to touch the radial border of her thumb to her forearm. What is the next step in management? Review Topic
Explanation
Question 35
A 22-year-old professional ballet dancer reports a 3-month history of posterior ankle pain that occurs when she changes from a flat foot to pointe (hyperplantar flexed position). Examination does not elicit the pain with forced passive plantar flexion. A radiograph is shown in Figure 8. What is the most likely cause of the pain?
Explanation
REFERENCES: Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
Khan K, Brown J, Way S, et al: Overuse injuries in classical ballet. Sports Med
1995;19:341-357.
Question 36
Figures 94a and 94b show T1 sagittal and coronal MR images of the right shoulder of a 45-year-old woman. She has insidious onset of dull, aching right shoulder pain localized at the superior aspect of her shoulder. The nerve that supplies the atrophied muscle arises from the upper trunk from contributions of which nerve roots? A B

Explanation
The suprascapular nerve innervates the supraspinatus muscle. Patients with suprascapular neuropathy usually have insidious onset of dull, aching shoulder pain at the superior or posterior aspect of the shoulder. There can be several causes of nerve compression, and the nerve is susceptible to compression at the suprascapular and spinoglenoid notches. Extrinsic compression can be secondary to joint-related fluid filled cysts of soft-tissue masses. Traction neuropathy may occur as the result of excessive nerve excursion during athletic activity (usually overhead sports) or after a massive, retracted rotator cuff tear. The suprascapular nerve originates from the upper trunk from predominantly the C5 and C6 nerve roots, with an occasional contribution from the C4 nerve root.
RECOMMENDED READINGS
Boykin RE, Friedman DJ, Higgins LD, Warner JJ. Suprascapular neuropathy. J Bone Joint Surg Am. 2010 Oct 6;92(13):2348-64. doi: 10.2106/JBJS.I.01743. Review. 81
PubMed PMID: 20926731. View Abstract at PubMed
Piasecki DP, Romeo AA, Bach BR Jr, Nicholson GP. Suprascapular neuropathy. J Am Acad Orthop Surg. 2009 Nov;17(11):665-76. Review. PubMed PMID: 19880677 View Abstract at PubMed
Question 37
A 2-year-old child has refused to bear weight on his leg for the past 2 days. His parents report that he will crawl, has no fever, and has painless full range of motion of his hip and knee. Examination reveals no deformity or bruising, but there is mild swelling and tenderness over the anterior tibia. C-reactive protein, WBC count, and erythrocyte sedimentation rate studies are normal. Radiographs are negative. What is the best course of action?
Explanation
REFERENCES: Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, et al: Toddler’s fracture: Presumptive diagnosis and treatment. J Pediatr Orthop 2001;21:152-156.
Oudjihane K, Newman B, Oh KS, et al: Occult fractures in preschool children. Trauma 1988;28:858-860.
Question 38
Figures 4a and 4b show the radiographs of a 32-year-old man who has right groin pain with activity or prolonged standing. Which of the following factors would not prohibit consideration of acetabular liner exchange and grafting of the defects?
Explanation
REFERENCES: Maloney WJ, Herzwurm P, Paprosky W, Rubash HE, Engh CA: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 39
Which of the following medications has been shown to improve skeletal muscle regeneration and decrease fibrosis following muscle injury in an animal model? Review Topic
Explanation
Skeletal muscle undergoes a natural process of healing and regeneration after injury. The formation of fibrous tissue in place of normal muscle is also part of this process. However, fibrous tissue in place of muscle can predispose the area to re-injury and impaired function. Administration of angiotensin II receptor blockade medications (e.g. losartan) after skeletal muscle injury has been shown to decrease the apoptotic cascade response and the formation of fibrous tissue. The mechanism of benefit is thought to be associated with blockade of insulin-like growth factor.
Terada et al. looked at the affect of platelet-rich plasma (PRP) and losartan on muscle healing after contusion injuries. They showed that PRP plus losartan combination
therapy improved overall skeletal muscle healing by enhancing angiogenesis and follistatin expression as well as reducing the expression of phosphorylated Smad2/3 and the development of fibrosis.
Bedair et al. used a rat model to investigate the effect of angiotensin receptor blockade on muscle fibrosis after injury. They found that angiotensin receptor blockade therapy significantly reduced fibrosis and led to an increase in the number of regenerating myofibers in acutely injured skeletal muscle.
Incorrect
Question 40
A 24-year-old man who was involved in a high speed motor vehicle accident is transferred for definitive care after having been diagnosed with an acute spinal cord injury from a fracture-dislocation at C6-7. He has a complete C6 neurologic level and it is now approximately 10 hours from his injury. What is the most appropriate pharmacologic treatment at this time?
Explanation
48 hours. In this patient, who is outside the 8-hour treatment window, no studies have supported starting the methylprednisolone protocol at this time.
REFERENCES: Braken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Kwon BK, Tetzlaff W, Grauer JN, et al: Pathophysiology and pharmacologic treatment of acute spinal cord injury. Spine J 2004;4:451-464.
Question 41
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?
Explanation
REFERENCES: Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Cannon LB, Hackney RG: Anterior tibiotalar impingement associated with chronic ankle instability. J Foot Ankle Surg 2000;39:383-386.
Question 42
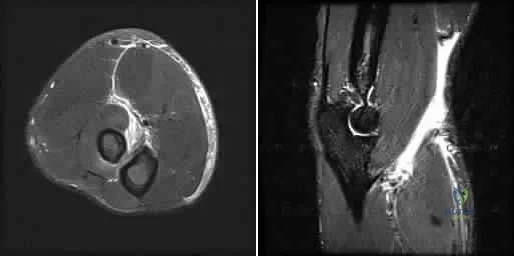
Surgical arthroscopy performed 1 week after injury presents increased risk for
Explanation
The MR images show injuries to the ACL, PCL, and PLC consistent with a knee dislocation. The optimal timing of surgery after multiligament knee injury remains unclear. Two systematic reviews demonstrated superior clinical outcome scores after early treatment, including higher mean Lysholm scores and a higher percentage of good/excellent International
Knee Documentation Committee scores. Early treatment was associated with increased residual anterior knee instability but no difference in posterior instability, varus laxity, or valgus laxity. Although numbers were limited, the average range of motion and rate of extension loss of at least 5 degrees was similar between groups. More patients in the early-treatment group demonstrated a higher rate of flexion loss of 10 or more degrees and an increased need to undergo a second procedure to address arthrofibrosis, including manipulation under anesthesia and arthrolysis. Return to work did not significantly differ between groups, but return to sports was lower in the early-treatment group. Evidence demonstrates a higher rate of low-energy mechanisms resulting in multiligament knee injury and an increased odds ratio for complications among obese (= 30 degrees kg/m2 patients, including wound complications and neurovascular injury. The complication rate increased 9.2% for every 1-point increase in body mass index. There is no association between complication rate and age, injury mechanism, or timing of surgery. Orthopaedic surgeons performing arthroscopy during the early postinjury period must be mindful of the extensive soft-tissue damage present in these patients, including potential capsular defects. Use of high-pressure irrigation can lead to substantial fluid extravasation into the thigh or lower leg compartments, placing patients at increased risk for compartment syndrome. In addition to avoiding high-pressure irrigation, some orthopaedic surgeons have advocated the creation of generous capsular incisions during portal establishment to allow for ready egress of irrigation fluid from the portal sites rather than into soft tissues.
RESPONSES FOR QUESTIONS 85 THROUGH 88
Excessive medial placement of coracoid autograft
Excessive lateral placement of coracoid autograft
Excessive inferior dissection during the procedure
Excessive retraction and dissection of the medial portion of the conjoint tendon
A 20-year-old right-hand-dominant football player sustained a traumatic shoulder dislocation during a tackle. He has had multiple recurrent dislocations, and radiographs reveal anterior glenoid bone loss. He underwent a Latarjet procedure. Match the most likely complication described below with the surgical error listed above.
Question 43
A patient wakes up with a foot drop following open reduction internal fixation of a posterior wall/posterior column acetabular fracture. What position of the leg causes the highest intraneural pressure in the sciatic nerve?

Explanation
Question 44
An active 55-year-old man who felt a sudden pop in the left heel while playing tennis 6 months ago was diagnosed with an ankle sprain around the time of injury. He now reports calf atrophy and severe weakness with running. Examination reveals a palpable defect in the Achilles tendon and only trace passive ankle flexion when the calf is squeezed. At the time of surgery, an Achilles tendon defect of 6 cm cannot be approximated. Surgical management of the Achilles tendon should include
Explanation
REFERENCES: Myerson M: Achilles tendon ruptures. Instr Course Lect 1999;48:219-230.
Mandelbaum BR, Myerson MS, Forster R: Achilles tendon ruptures: A new method of repair, early range of motion, and functional rehabilitation. Am J Sports Med 1995;23:392-395.
Question 45
A 20-year-old man with fascioscapulohumeral dystrophy has severe scapular winging of both shoulders. He can no longer abduct above 80 degrees, and it affects his activities of daily living. A clinical photograph is shown in Figure 26. Definitive management should consist of
Explanation
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
Question 46
A 20-year-old patient has foot pain. A radiograph and T 1 -weighted MRI scan are shown in Figures 8a and 8b. A biopsy specimen is shown in Figure 8c. Treatment should consist of
Explanation
REFERENCES: Dahlin DC, Unni KK: Bone Tumors: General Aspects and Data on 8,542 Cases. Springfield, IL, Charles C. Thomas, 1986.
Gitelis S, Mallin BA, Piasecki P, Turner F: Intralesional excision compared with en bloc resection for giant cell tumor of bone. J Bone Joint Surg Am 1993;75:1648-1655.
Question 47
A 19-year-old college football player reports persistent weakness, tingling, and numbness of both upper extremities at half time. He states that these symptoms initially occurred after tackling an opposing player with his head early in the game. History reveals that he has had “burners” in the past that typically resolved within 15 to 30 minutes. Examination reveals pain-free cervical motion, weakness to shoulder abduction testing bilaterally, normal upper extremity reflexes, and decreased sensation over both shoulders and the upper arms. Appropriate initial management should consist of
Explanation
REFERENCES: Torg JS, Sennett B, Pavlov H, et al: Spear tackler’s spine: An entity precluding participation in tackle football and collision activities that expose the cervical spine to axial energy inputs. Am J Sports Med 1993;21:640-649.
Torg JS: Cervical spinal stenosis with cord neurapraxia and transient quadriplegia. Sports Med 1995;20:429-434.
Torg JS, Guille JT, Jaffe S: Injuries to the cervical spine in American football players. J Bone Joint Surg Am 2002;84:112-122.
Question 48
A 2-year-old boy has complete absence of the sacrum and lower lumbar spine. What is the most likely long-term outcome if no spinal pelvic stabilization is performed?
Explanation
REFERENCES: Tachdjian MO: The spine: Congenital absence of the sacrum and lumbosacral vertebrae (lumbosacral agenesis), in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 3, p 2228.
Renshaw TS: Sacral agenesis: A classification and review of twenty-three cases. J Bone Joint Surg Am 1978;60:373-383.
Question 49
Which of the following tumors is most likely to present with a pathologic fracture in a child?
Explanation
REFERENCES: Wilkins RM: Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-224.
Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Hecht AC, Gebhardt MC: Diagnosis and treatment of unicameral and aneurysmal bone cysts in children. Curr Opin Pediatr 1998;10:87-94.
Question 50
An 18-year-old man sustained closed humeral shaft and forearm fractures of his dominant arm in a motor vehicle accident. Neurovascular examination is intact, and his condition is stable. The best course of action for management of the injuries should be
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Bell MJ, Beachamp CG, Kellam JK, McMurtry RY: The results of plating humeral shaft fractures in patients with multiple injuries: The Sunnybrook experience. J Bone Joint Surg Br 1985;67:293-296.
Question 51
A 5-year-old boy is seen in the emergency department with a 2-day history of refusing to walk. Examination shows that he has a temperature of 102.2 degrees F (39 degrees C) and limited range ot motion of the right hip. The AP pelvic radiograph is normal. The WBC count is normal but the C-reactive protein and erythrocyte sedimentation rate (ESR) are elevated. What is the next step in management?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 52
A 42-year-old woman has a history of nontraumatic ankle swelling with tenderness over the Achilles tendon and plantar fascia. She reports that while vacationing in Connecticut 2 months ago she noted the presence of a “red bull’s eye” rash. Management should consist of
Explanation
REFERENCES: Neu HC: A perspective on therapy of Lyme infection. Ann NY Acad Sci 1988;539:314-316.
Faller J, Thompson F, Hamilton W: Foot and ankle disorders resulting from Lyme disease. Foot Ankle 1991;11:236-238.
Question 53
A 26-year-old man falls off a motorcycle and injures his left wrist. There are no open wounds and the neurovascular examination is normal. Radiographs are shown in Figures 10a and 10b. Definitive management should consist of
Explanation
REFERENCES: May MM, Lawton JN, Blazar PE: Ulnar styloid fractures associated with distal radius fractures: Incidence and implications for distal radioulnar joint instability. J Hand Surg Am 2002;27:965-971.
Nana AD, Joshi A, Lichtman DM: Plating of the distal radius. J Am Acad Orthop Surg 2005;13:159-171.
Question 54
What neurovascular structure is most at risk when performing an inside-out repair of the posterior horn of the medial meniscus?
Explanation
REFERENCES: Cannon WD Jr, Morgan CD: Meniscal repair: Arthroscopic repair techniques. Instr Course Lect 1994;43:77-96.
Scott GA, Jolly BL, Henning CE: Combined posterior incision and arthroscopic intra-articular repair of the meniscus: An examination of factors affecting healing. J Bone Joint Surg Am 1986;68:847-861.
Question 55
A 53-year-old man reports acute, severe left shoulder pain after undergoing abdominal surgery 10 days ago. Initial management, consisting of anti-inflammatory drugs, physical therapy, and a subacromial injection of corticosteroid, fails to provide relief. Reexamination of the shoulder 2 months after the onset of symptoms reveals atrophy of the infraspinous and supraspinous fossa and profound weakness of active abduction and external rotation. His neck is supple with a full range of motion. Plain radiographs and an MRI scan of the shoulder are normal. What diagnostic study should be performed next in the evaluation of this patient?
Explanation
In this patient, the injury is most likely caused by traction or compression of the nerve in the suprascapular notch as the result of positioning during abdominal surgery; therefore, the studies of choice are electromyography and nerve conduction velocity studies. While MRI of the cervical spine may be of some value in ruling out a radiculopathy, the clinical history does not support such a cause for this condition.
REFERENCES: Rengachary SS, Neff JP, Singer PA, Brackett CE: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 1: Clinical study. Neurosurgery 1979;5:441-446.
Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H: Suprascapular entrapment neuropathy: A clinical, anatomical and comparative study. Part 2: Anatomical study. Neurosurgery 1979;5:447-451.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthoscopy 1990;6:301-305.
Question 56
A 20-year-old unrestrained driver sustained a midshaft femur fracture in a high-speed motor vehicle accident. The femoral neck was evaluated with a CT scan with 2-mm cuts through the hip; no fracture was identified. What additional studies (if any) should be performed to minimize the risk of having an undiagnosed femoral neck fracture?
Explanation
Question 57
The most appropriate treatment for this fracture is
Explanation
Tibial fractures are classified on the basis of their anatomical location and the status of the prosthesis fixation. Type I fractures involve the tibial plateau, type II fractures occur adjacent to the stem of the tibial component, type III fractures are distal to the tibial stem, and type IV fractures involve the tibial tubercle. Subclassifications include A with a well-fixed implant; B with a loose implant; and C, which occur intraoperatively.
Treatment of periprosthetic tibial fractures is based on the location of the fracture and the status of the component fixation. Types II or III fractures associated with prosthetic loosening or instability are best managed with revision arthroplasty, usually with a diaphyseal-engaging intramedullary tibial stem. Supplemental internal fixation may be necessary. Type III fractures with well-fixed and stable implants are treated using the standard principles of tibial fracture management.
Question 58
A 70-year old woman undergoes revision total knee arthroplasty for tibial component aseptic loosening. She is concerned about recurrent loosening, and tibial stem fixation options during revision are reviewed. Figure below displays a radiograph of the revision technique used for this patient. What is the incidence of intraoperative tibial shaft fracture that is associated with this type of revision surgery?

Explanation
Using press-fit tibial stems during a hybrid revision total knee arthroplasty is associated with a 3% to 5% incidence of intraoperative tibial shaft fracture. Diaphyseal fixation of press-fit stems has the advantage of setting component alignment, dispersing forces on the proximal tibia, and offers excellent clinical results. The disadvantages include proximal and distal tibia anatomic mismatch and tibial shaft fracture. Cipriano and associates reported a tibial shaft fracture incidence of 4.9% in a series of 420 consecutive
knee revisions. All fractures healed with nonsurgical management, and none led to implant loosening. In this patient, it is important to recognize on the radiograph that this technique is a hybrid method of revision total knee arthroplasty, with cementation along the tibial tray and metaphysis and with press-fit fixation of the diaphyseal engaging stem. Then, it is important to know the risk and management of intraoperative diaphyseal tibial fractures. Cemented tibial stems are associated with a low rate of intraoperative fracture, because the implant is typically undersized to allow for an appropriate cement mantle. Option C is incorrect, because this revision is not cemented. Option A underestimates the incidence of fracture, whereas D overestimates the rate of fracture.
Question 59
-Which type of cells has been implicated in the process shown inFigure?
Explanation

Question 60
The space available for the cord is an important determinant in neurologic recovery. Recent analysis suggests that the most reliable radiographic predictor for neurologic recovery after surgery in patients with rheumatoid arthritis and paralysis is a preoperative
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 273-279.
Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Wattenmaker I, Concepcion M, Hibberd P, Lipson S: Upper airway obstruction and perioperative management of the airway in patients managed with posterior operations on the cervical spine for rheumatoid arthritis. J Bone Joint Surg Am 1994;76:360-365.
Question 61
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T 1 - and T 2 -weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?
Explanation
REFERENCES: Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Kausch T, Rutt J: Subcutaneous rupture of the tibialis anterior tendon: Review of the literature and case report. Arch Orthop Traum Surg 1998;117:290-293.
Question 62
What procedure can eliminate a sulcus sign? Review Topic
Explanation
Question 63
An obese 4-year-old boy has infantile Blount’s disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of
Explanation
REFERENCES: Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Loder RT, Johnston CE: Infantile tibia vara. J Pediatr Orthop 1987;7:639-646.
Question 64
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
(range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon’s finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle.
REFERENCES: Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804.
Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
Question 65
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
REFERENCE: Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.
Question 66
A 47-year-old obese man with a body mass index of 42 comes in with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of his UKA secondary to poor patient selection. This young, heavy man likely loosened his component secondary to the ongoing varus alignment of the knee and his elevated weight. Despite this likely scenario, the next step is to determine if an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order an ESR and CRP to determine if aspiration is warranted. If laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.

CLINICAL SITUATION FOR QUESTIONS 69 THROUGH 72
Figures 69a through 69c are the radiograph and MR images of a 37-year-old woman who has had a 2-month history of left hip pain.
Question 67
A 22-year-old volleyball player reports the insidious onset of superior and posterior shoulder pain. Radiographs are normal. An MRI scan is shown in Figure 25. What is the most specific physical examination finding?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR Jr: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Question 68
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
REFERENCES: Colwell CW Jr, Collis DK, Paulson R, et al: Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty:. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999;81:932-940.
Salvati EA, Pelligrini VD Jr, Sharrock NE, et al: Recent advances in venous thromboembolic prophylaxis during and after total hip replacement. J Bone Joint Surg Am 2000;82:252-270.
Question 69
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 505-520.
Question 70
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by
Explanation
REFERENCE: Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 71
A 30-year-old man has had a slowly enlarging mass on the plantar medial aspect of the foot for the past 6 months. The mass is now 1 cm in diameter, adherent to the plantar fascia, and painful with weightbearing. The overlying skin is mobile. Management at this time should consist of
Explanation
Question 72
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Findlay JM: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;39:210.
Dickman CA, Mamourian A, Sonntag VK, et al: Magnetic resonance imaging of the transverse atlantal ligament for the evaluation of atlantoaxial instability. J Neurosurgery 1991;75:221-227.
Question 73
An otherwise healthy 76-year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in Figures below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?
Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 74
A 45-year-old male laborer injured his right elbow trying to catch a heavy object. He has antecubital pain and forearm ecchymosis. MRI scans are shown in Figures 4a and 4b. Nonsurgical management of this injury is most associated with the loss of Review Topic
Explanation
Question 75
What term in statistics defines rejecting the null hypothesis when it is in fact true?
Explanation
Type-I errors, to put it simply, detect an effect that is not present. In contrast, a type-II error fails to detect an effect that is present. In simple studies, the rate of a type-I error is denoted by a (alpha). For a 95% confidence level, the value of alpha is 0.05. This means that there is a 5% probability that we will reject a true null hypothesis.
Illustration A shows the difference between type-I and type-II errors. Incorrect Answers;
not technically considered "errors," but instead are variables that properly constructed studies attempt to avoid. Answer 4: Variance is an estimate of the variability of each individual data point from the mean.
Question 76
A 30-year-old man sustains a head injury as well as a femur and pelvis fractures as the result of a rollover motor vehicle accident. He is initially comatosed, but recovers cognitive function after 10 days in the hospital. Soon after awakening he complains of wrist pain and an x-ray demonstrates a distal radius fracture. What is the most likely explanation for this delayed diagnosis?

Explanation
Question 77
A 26-year-old weightlifter had increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication,
Explanation
Question 78
A 17-year-old boy is shot in the left side of the neck at the C5-6 level and sustains an incomplete spinal cord injury that is called a Brown-Sequard syndrome. Which of the following best describes the expected deficits? Review Topic
Explanation
Question 79
Figures 114a and 114b are the radiographs of a 5-year-old girl who fell from monkey bars. What is the first consideration regarding treatment for this injury? Review Topic

Explanation
Question 80
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Explanation
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 81
A 73-year-old man presents to your clinic many years after undergoing total shoulder arthroplasty with pain and the radiographic findings demonstrated in Figure 56. The most likely cause of this patient’s pain is

Explanation
The radiograph shows proximal humeral migration and loosening of the glenoid component. Proximal migration of the humeral head may represent rotator cuff dysfunction and can lead to progressive failure of the glenoid component. Stress shielding will not cause lysis or loosening of the glenoid component. Humeral osteolysis is an uncommon finding and is not shown. Progressive glenoid arthrosis is not possible with a resurfaced glenoid.
RECOMMENDED READINGS
Hill JM, Norris TR. Long-term results of total shoulder arthroplasty following bone-grafting of the glenoid. J Bone Joint Surg Am. 2001 Jun;83-A(6):877-83. PubMed PMID: 11407796.View Abstract at PubMed
Fox TJ, Cil A, Sperling JW, Sanchez-Sotelo J, Schleck CD, Cofield RH. Survival of the glenoid component in shoulder arthroplasty. J Shoulder Elbow Surg. 2009 Nov-Dec;18(6):859-63. doi: 10.1016/j.jse.2008.11.020. Epub 2009 Mar 17. PubMed
PMID: 19297199.View Abstract at PubMed
Question 82
-A 75-year-old woman fell at home and sustained the injury seen in Figures 249a through 249c. What is the most appropriate treatment option?
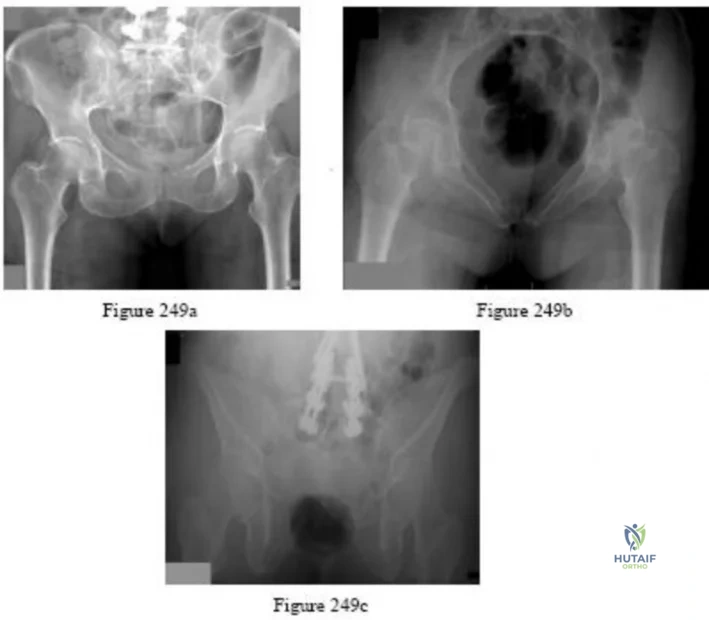
Explanation

Question 83
A farmer is seen in the emergency department after falling out of a hay loft onto the barn floor below. He is unable to bear weight. Exploration of a 0.5 cm laceration over the anterior tibia reveals bone. Radiographs reveal oblique displaced midshaft tibial and fibular fractures. Based on these findings, what is the most appropriate antibiotic prophylaxis?
Explanation
REFERENCES: Okike K, Bhattacharyya T: Trends in the management of open fractures: A critical analysis. J Bone Joint Surg Am 2006;88:2739-2748.
Holtom PD: Antibiotic prophylaxis: Current recommendations. J Am Acad Orthop Surg 2006:14:S98-S100.
Question 84
A 66-year-old female presents to your clinic complaining of back pain, difficulty standing-up straight, weakness in her legs, and neurogenic claudication. On upright thoracolumbar radiographs, there is a 75 degree thoracolumbar curve with the apex at L2, and the C7 plumb line falls 12 cm anterior to the posterosuperior corner of S1. Aside from a decompression of the stenotic levels, which of the following choices will lead to the MOST reliable decrease in overall disability? Review Topic
Explanation
Spinal malalignment in Adult Spinal Deformity (ASD) challenges balance mechanisms used for maintenance of an upright posture to achieve the basic human needs of preserving level visual gaze and retaining the head over the pelvis. Severe malalignment can result in greater muscular effort and energy expenditure to maintain the erect posture as well as use of compensatory mechanisms. As such, surgical correction of these deformities are aimed at achieving proper spinopelvic alignment.
Glassman et al. performed a multi-center retrospective study of 298 adults with spinal deformity. Regardless of operative (129 patients) or non-operative care (172 patients) a positive sagittal balance was the found to be the most reliable predictor of clinical symptoms in both patient groups.
Schwab et al. published a current concepts review on operative management for adult spinal deformities and identified three major goals of surgery: (1) Correct the SVA to
within 5 cm of neutral, (2) Ensure the pelvic tilt is less than 20 degrees, (3) Ensure the lumbar lordosis is within 9 degrees of the pelvic incidence.
Illustration A demonstrates how to measure the SVA. Illustration B depicts the realignment objectives in the saggital plane as described by Schwab et al.
Incorrect
Question 85
An operating room intervention that should be undertaken by anesthesia staff during the cementing of a femoral stem is to
Explanation
Young age is a risk factor for early failure of cementless femoral components. Surgeons could consider cementing for patients older than 80 years of age. The Dorr classification has been shown to favor a cemented femoral stem in Dorr type C bone. Dorr type B bone can potentially sustain a proximally porous ingrowth stem. Osteoporosis is a risk factor for early failure of cementless femoral components.
Earlier designs for cemented femoral stems used microtexture to interlock the stem into the cement mantle. If these stems became loose, they would abrade the cement and loosen the stem further. Successful cemented femoral components are polished and have smooth edges with tapered bodies. Collars do not add to the design of femoral stems.
Patients are at risk for hypotension during the femoral pressurization process. With that in mind, the surgeon should make sure the anesthesiologist is ready to respond to hypotension. The FiO2 should be increased. The IV fluid rate also should be increased, and the anesthesiologist should be prepared with phenylephrine to support the patient’s blood pressure if he or she becomes hypotensive.

Question 86
- A patient reports persistent pain in the wrist 6 months after undergoing open reduction and internal fixation of a Galleazi fracture. Radiographs of the wrist in a neutral position are normal. Which of the following studies would best evaluate the reduction of the distal radioulnar joint?
Explanation
Question 87
A patient sustained the injuries shown in the radiographs and clinical photograph seen in Figures 10a through 10c. The neurovascular examination is normal. The first step in emergent management of the extremity injuries should consist of
Explanation
REFERENCES: Sahin V, Karakas ES, Aksu S, et al: Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-529.
Moed BR, WillsonCarr SE, Watson JT: Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am 2002;84:752-758.
Question 88
At the level of tibial bone resection in total knee arthroplasty, where does the common peroneal nerve lie?
Explanation
REFERENCES: Clarke HD, Schwartz JB, Math KR, et al: Anatomic risk of peroneal nerve injury with the “pie crust” technique for valgus release in total knee arthroplasty. J Arthroplasty 2004;19:40-44.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-52, 4-53.
Question 89
A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of
Explanation
REFERENCES: Cooney WP, Linscheid RL, Dobyns JH, Wood MB: Scaphoid nonunion: Role of anterior interpositional bone grafts. J Hand Surg Am 1988;13:635-650.
Fernandez DL: A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-737.
Stark HH, Rickard TA, Zemel NP, Ashworth CR: Treatment of ununited fractures of the scaphoid by illiac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am
1988;70:982-991.
Feldman MD, Manske PR, Welch RL, Szerzinski JM: Evaluation of Herbert screw fixation for the treatment of displaced scaphoid nonunions. Orthopedics 1997;20:325-328.
Question 90
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time?
Explanation
REFERENCES: Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217.
Hart RA: Cervical facet dislocation: When is magnetic resonance imaging indicated? Spine 2002;27:116-117.
Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 91
A 68-year-old man embarks on a 24-week strength training program. He trains at 80% of his single repetition maximum for both the upper and lower extremities. Which of the following changes can be anticipated?
Explanation
REFERENCES: Kirkendall DT, Garrett WE Jr: The effects of aging and training on skeletal muscle. Am J Sports Med 1998;26:598-602.
Frontera WR, Meredith CN, O’Reilly KP, Knuttgen HG, Evans WJ: Strength conditioning in older men: Skeletal muscle hypertrophy and improved function. J Appl Physiol 1988;64:1038-1044.
Question 92
A 23-year-old man who was the restrained driver in a car involved in a high-speed motor vehicle accident sustained the closed injury shown in Figures 32a through 32c. Which of the following factors has the greatest impact on the risk of osteonecrosis?
Explanation
REFERENCES: Lindvall E, Haidukewych G, Dipasquale T, et al: Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am 2004;86:2229-2234.
Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.
Question 93
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?
Explanation
REFERENCE: Waters RL, Keenan ME: Surgical treatment of the upper extremity after stroke, in Chapman MW (ed): Operative Orthopedics. Philadelphia, PA, JB Lippincott, 1988, vol 2,
pp 1449-1450.
Question 94
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Explanation
Question 95
Examination of the shoulder seen in Figure 52 shows atrophy and tenderness of the infraspinous fossa and profound weakness in external rotation. The supraspinous fossa shows normal muscle bulk. What is the most likely cause of this condition?
Explanation
REFERENCES: Schickendantz MS, Ho CP: Suprascapular nerve compression by a ganglion cyst: Diagnosis by magnetic resonance imaging. J Shoulder Elbow Surg 1993;2:110-114.
Thompson RC, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982;166:185-187.
Iannotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Question 96
A 28-year-old man underwent open reduction and internal fixation of a closed, displaced, intra-articular calcaneal fracture 8 weeks ago. Examination now reveals that the lateral wound is red and draining purulent material. Cultures obtained from the wound grow out Staphylococcus aureus. Radiographs show early healing of the fracture. What is the next most appropriate step in management?
Explanation
REFERENCES: Benirschke SK, Kramer PA: Wound healing complications in closed and open calcaneal fractures. J Orthop Trauma 2004;18:1-6.
Lim EV, Leung JP: Complications of intra-articular calcaneal fractures. Clin Orthop
2001;391:7-16.
Folk JW, Starr AJ, Early JS: Early wound complications of operative treatment of calcaneus fractures: Analysis of 190 fractures. J Orthop Trauma 1999;13:369-372.
Question 97
-Use of the shorter, anterior screw may result in
Explanation
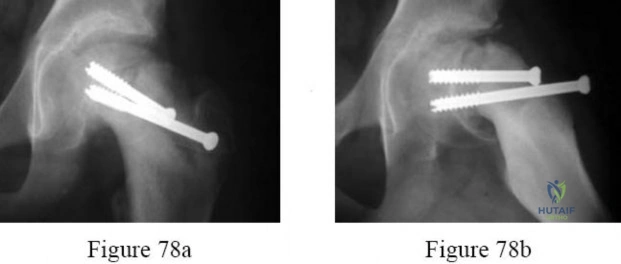
Question 98
-A 42-year-old woman has had right wrist pain for 2 years. She tried splint wear and naproxen and has had 3 steroid injections, each time experiencing less relief.
Explanation

Question 99
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraneural and intraneural arterial anatomy of the ulnar nerve at the elbow. J Shoulder Elbow Surg 1999;8:17-21.
Question 100
Item Deleted by AAOS Question 40 - Figure 8 shows the AP radiograph of a 38-yea-old woman who has constant pain in her shoulder as the results of a motor vehicle accident. Examination reveals marked restriction in external rotation. Which of the following studies should be ordered to aid in making a diagnosis?
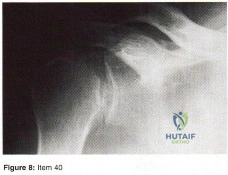
Explanation
