OITE & ABOS Orthopedic Board Prep: Arthroplasty, Hip, Knee & Spine | Part 248

Key Takeaway
This page offers Part 248 of a comprehensive orthopedic board review. Featuring 100 verified, high-yield MCQs in OITE/AAOS format, it's designed for orthopedic surgeons and residents preparing for their certification exams. Utilize interactive study and exam modes to master topics like Arthroplasty, Cartilage, Hip, and Knee, ensuring exam readiness.
About This Board Review Set
This is Part 248 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 248
This module focuses heavily on: Arthroplasty, Cartilage, Hip, Knee.
Sample Questions from This Set
Sample Question 1: Which of the following is a true statement regarding thoracic disk herniations?...
Sample Question 2: Figure 50 shows the MRI scan of a 20-year-old female college soccer player with knee pain. What is the most likely diagnosis?...
Sample Question 3: What is the primary concern for arthrodesis of a failed infected total knee arthroplasty using internal fixation?...
Sample Question 4: During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this ath...
Sample Question 5: Which of the following properties apply to the human meniscus when compared with articular cartilage?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following is a true statement regarding thoracic disk herniations?
Explanation
REFERENCES: Shah RP, Grauer JN: Thoracoscopic excision of thoracic herniated disc, in Vaccaro AR, Bono CM (eds): Minimally Invasive Spine Surgery. New York, NY, Informa Healthcare, 2007, pp 73-80.
Bohlman HH, Zdeblick TA: Anterior excision of herniated thoracic discs. J Bone Joint Surg Am 1988;70:1038-1047.
Question 2
Figure 50 shows the MRI scan of a 20-year-old female college soccer player with knee pain. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 3
What is the primary concern for arthrodesis of a failed infected total knee arthroplasty using internal fixation?
Explanation
REFERENCE: Windsor RE: Knee arthrodesis, in Insall JN, Windsor R, Kelly M, et al (eds): Surgery of the Knee. New York, NY, Churchill Livingstone, 1993, pp 1103-1116.
Question 4
During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this athlete be managed? Review Topic
Explanation
Question 5
Which of the following properties apply to the human meniscus when compared with articular cartilage?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 3-23.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, AAOS, 1999, pp 349-354.
Question 6
A 30-year-old man who sustained a work-related injury 6 weeks ago reports persistent back and left-sided buttock pain that has been attributed to lumbar transverse process fractures. A pelvic radiograph and CT scans obtained 2 days ago are seen in Figures 17a through 17c. What is the best treatment for his injury?
Explanation
REFERENCES: Mears DC: Management of pelvic pseudarthroses and pelvic malunion. Orthopade 1996;25:441-448.
Matta JM, Dickson KF, Markovich GD: Surgical treatment of pelvic nonunions and malunions. Clin Orthop Relat Res 1996;329:199-206.
McLaren AC, Rorabeck CH, Halpenny J: Long-term pain and disability in relation to residual deformity after displaced pelvic ring fractures. Can J Surg 1990;33:492-494.
Question 7
A patient has a displaced complex intra-articular distal humeral fracture. What factor is considered most important when deciding on what surgical approach to use?
Explanation
REFERENCES: McKee MD, Mehne DK, Jupiter JP: Fractures of the distal humerus: Part II, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1483-1522
McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Patterson SD, Bain GI, Mehta JA: Surgical approaches to the elbow. Clin Orthop
2000;370:19-33.
Bryan RS, Morrey BF: Extensive posterior exposure of the elbow: A triceps-sparing approach. Clin Orthop 1982;166:188-192.
Question 8
A patient reports pain in the hip with functional positioning. With the patient supine, pain in which of the following positions would be typical for femoral acetabular impingement? Review Topic
Explanation
(SBQ13PE.10) Which statement is true regarding discoid menisci? Review Topic
Most commonly involves the medial meniscus
Bilateral in >75% of cases
Asymptomatic discoid meniscus should undergo saucerization
Radiographs will commonly show a hyperplastic lateral intercondylar spine
Radiographs will commonly show squaring of affected condyle with cupping of tibial plateau
Radiographs of knees with discoid menisci will commonly show squaring of affected condyle (lateral>medial) with cupping of tibial plateau.
Discoid meniscus refers to the abnormal development of a hypertrophic and discoid shaped meniscus. It occurs in 3-5% of the population and it is considered the most common cause of a symptomatic clicking or clunking in a childs knee. The lateral meniscus is most commonly affected and it will occur bilaterally in 25% of affected
people. The Watanabe Classification describes the 3 types of discoid menisci. Type 1
= Incomplete, Type 2 = Complete, Type 3 = Wrisberg (lack of posterior meniscotibial attachment to tibia)
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Lee et al. retrospectively reviewed 36 patients aged less than 15 years who underwent arthroscopic procedures for torn discoid menisci. The mean patient age at the time of surgery was 9.5 years. They showed that partial meniscectomy yielded better radiologic results than subtotal/total meniscectomy for torn discoid menisci in this population.
Illustration A shows the 3 classifications of discoid menisus as originally described by Watanabe. Type 4 is a ring type discoid that was not originally described by Watanabe in his 1978 paper. Illustration B shows an AP and lateral radiograph of a discoid meniscus knee. Note squaring of affected lateral condyle in the presence of a lateral discoid meniscus. Illustration C shows 4 consecutive sagittal MRI images with meniscus continuity. It is important to note that the diagnosis of discoid menisci can be made when 3 or more 5mm sagittal images show meniscal continuity.
Incorrect Answers:
Question 9
A 45-year-old man sustains an acute closed posterolateral elbow dislocation. The elbow is reduced, and examination reveals that the elbow dislocates posteriorly at 35 degrees with the forearm placed in supination. What is the best course of action?
Explanation
REFERENCE: O’Driscoll SW, Morrey BF, Korinek S, et al: Elbow subluxation and dislocation: A spectrum of instability. Clin Orthop 1992;280:186-197.
Question 10
Figure 91 shows the radiograph of a 57-year-old man who fell 6 feet off a ladder. He is neurovascularly intact but reports shoulder pain. What is the most appropriate acute treatment for this patient?

Explanation
Question 11
A 45-year-old man underwent a fingertip amputation through the distal phalanx after his ring finger was caught in a garage door. He was treated in the emergency department with a revision amputation by advancement of the flexor digitorum profundus (FDP) tendon to the extensor mechanism. Three months following the injury, he is able to fully flex his injured ring finger to touch his palm, but he reports that it is difficult for him to make a tight fist due to decreased flexion of his other fingers. What is this complication called?
Explanation
The quadrigia effect can occur due to over-advancement of the FDP tendon during repair (usually greater than 1 cm), development of FDP tendon adhesions, and (as in this case) "over the top" repair of the FDP tendon to the extensor tendon after amputation at the distal phalanx level. All of these conditions result in a functionally shortened FDP tendon of the injured digit. Because the FDP tendons of the long, ring, and small digits share a common muscle belly, excursion of the combined tendons is equal to the shortest tendon. Therefore, the uninjured digits will not have full excursion of their respective FDP tendons and will not be able to close into a full fisting position. Treatment of this condition is most commonly release
of the injured FDP tendon. A lumbrical plus deformity can occur in amputations distal to the flexor digitorum superficialis insertion through the middle phalanx. The FDP tendon retracts and increases tension on the lumbrical muscle, which leads to paradoxical interphalangeal (IP) joint extension with attempted flexion. Intrinsic tightness and interphalangeal joint contractures can be caused by hand trauma but would not lead to the clinical condition this patient has.
Question 12
A 50-year-old woman with a 2-part surgical neck proximal humerus fracture and metaphyseal comminution
Explanation
Proximal humerus fractures account for approximately 5% of all fractures, with incidence increasing to reflect an aging population and related osteoporosis. Treatment is dependent upon the mechanism of injury, the patient’s physiologic age and activity level, the fracture pattern, and rotator cuff integrity. Most of these injuries are nondisplaced or minimally displaced and are associated with a good overall prognosis with nonsurgical treatment and temporary impairment. A patient with a nondisplaced surgical neck fracture should be treated without surgery. K-wire stabilization, although technically difficult to achieve, is an option for compliant patients with 2-part, 3-part, and valgus-impacted 4-part fractures who have adequate bone stock. Valgus-impacted 4-part fractures pose reduced risk for osteonecrosis because of the preserved blood supply through the medial hinge, which allows for this technique. For displaced 2-part fractures accompanied by
metaphyseal comminution, K-wire fixation cannot provide adequate stability to initiate a graduated home exercise or outpatient physical therapy program. Formal open reduction with intramedullary or plate fixation in addition to bone grafting (fibular strut allograft) is the best surgical option for the clinical scenario involving a displaced surgical neck fracture with comminution. Osteosynthesis of 3-part fractures may be feasible for physiologically young and active patients without humeral head involvement and osteoporosis.
Current indications for primary hemiarthroplasty include most 4-part fractures, 3-part fractures and dislocations in elderly patients with osteoporotic bone, head-splitting articular segment fractures, and chronic anterior or posterior humeral head dislocations with more than 40% of articular surface involvement. Because of the intra-articular nature of this patient’s 4-part injury in this scenario, hemiarthroplasty with anatomic reconstruction of the greater and lesser tuberosities is most appropriate. Relative indications for hemiarthroplasty also include fractures with more than 20 degrees of varus, associated moderate to severe osteopenia, and revision surgery for failed osteosynthesis. Currently accepted indications for rTSA include scenarios in which the fracture pattern, level of comminution, bone quality, and rotator cuff deficiency preclude plate fixation or hemiarthroplasty. Scenarios involving 4-part fractures and associated rotator cuff tears and tuberosity comminution are best served with a reverse shoulder prosthesis. One of the positive attributes of this implant is the ability to achieve functional forward flexion and abduction regardless of tuberosity healing, position, and degree of comminution. Caution is warranted with this surgical technique because complication rates are higher than for hemiarthroplasty reconstruction. Acute, irreducible 2-part fracture-dislocations of the proximal humerus necessitate open reduction and internal fixation of the affected tuberosities (posterior, lesser tuberosity; anterior, greater tuberosity) through screw, anchor, and/or suture fixation. These fracture-dislocations can be managed with this technique because of the integrity of the vascular supply, which is maintained by the soft-tissue attachments to the intact tuberosities. Repeated attempts at a closed reduction in the 37-year-old with the posterior fracture-dislocation could result in neurovascular injury and myositis ossificans and should be avoided. Arthroplasty reconstruction in this scenario should not be the index procedure in light of concerns regarding implant survivorship in patients of this age and their assumed elevated activity levels.
RECOMMENDED READINGS
Harrison AK, Gruson KI, Zmistowski B, Keener J, Galatz L, Williams G, Parsons BO, Flatow EL. Intermediate outcomes following percutaneous fixation of proximal humeral fractures. J Bone Joint Surg Am. 2012 Jul 3;94(13):1223-8. doi: 10.2106/JBJS.J.01371. View Abstract at PubMed
Iannotti JP, Ramsey ML, Williams GR Jr, Warner JJ. Nonprosthetic management of proximal humeral fractures. Instr Course Lect. 2004;53:403-16. Review. View Abstract at PubMed
Mata-Fink A, Meinke M, Jones C, Kim B, Bell JE. Reverse shoulder arthroplasty for treatment of proximal humeral fractures in older adults: a systematic review. J Shoulder Elbow Surg. 2013 Dec;22(12):1737-48. doi: 10.1016/j.jse.2013.08.021. Review. View Abstract at PubMed
Jobin CM, Galdi B, Anakwenze OA, Ahmad CS, Levine WN. Reverse shoulder arthroplasty for the management of proximal humerus fractures. J Am Acad Orthop Surg. 2015 Mar;23(3):190-201. doi: 10.5435/JAAOS-D-13-00190. Epub 2015 Jan 28. Review. View Abstract at PubMed
Bae JH, Oh JK, Chon CS, Oh CW, Hwang JH, Yoon YC. The biomechanical performance of locking plate fixation with intramedullary fibular strut graft augmentation in the treatment of unstable fractures of the proximal humerus. J Bone Joint Surg Br. 2011 Jul;93(7):937-41. View Abstract at PubMed
Kontakis G, Koutras C, Tosounidis T, Giannoudis P. Early management of proximal humeral fractures with hemiarthroplasty: a systematic review. J Bone Joint Surg Br. 2008 Nov;90(11):1407-13. doi: 10.1302/0301-620X.90B11.21070. Review. PubMed PMID: 18978256. View Abstract at PubMed
Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg. 2004 Jul-Aug;13(4):427-33. PubMed PMID: 15220884. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 67 THROUGH 70
Figure 67 is the radiograph of a right-hand-dominant 70-year-old woman who arrives at the emergency department with acute left shoulder pain following a fall down a flight of stairs. She expresses acute diffuse left shoulder pain and swelling. Prior to her injury, she had full active painless shoulder range of motion.

Question 13
A 19-year-old college cross-country runner is amenorrheic and has recurrent stress fractures. Long-term management should consist of
Explanation
REFERENCES: Nattiv A, Armsey TD Jr: Stress injury to bone in the female athlete. Clin Sports Med 1997;16:197-224.
Drinkwater BL: Exercise and bones: Lessons learned from female athletes. Am J Sports Med 1996;24:S33-S35.
Question 14
A patient sustained a puncture wound to the plantar aspect of his foot. He was wearing shoes and socks at the time of the injury. Systemic antibiotic administration with specific coverage for which bacterial species (in addition to Staphylococcus aureus) should be instituted?
Explanation
Puncture wounds sustained through a shoe and sock increase risk for Pseudomonas infection. Clostridium are associated with soil-contaminated wounds. Mycobacterium marinum is associated with injuries sustained within water.
RECOMMENDED READINGS
DeCoster TA, Miller RA. Management of Traumatic Foot Wounds. J Am Acad Orthop Surg. 1994 Jul;2(4):226-230. PubMed PMID: 10709013. View Abstract at PubMed
Raikin SM. Common infections of the foot. In: Richardson EG, ed. Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2004:199-205.
Question 15
Figures 29a and 29b show the radiographs of a 13-year-old competitive gymnast who has had elbow pain for the past 2 weeks. The pain is worse with tumbling activities. Examination reveals a mild effusion and slight limitation of extension and forearm rotation with no locking. Initial management should consist of
Explanation
REFERENCES: Maffulli N, Chan D, Aldridge MJ: Derangement of the articular surfaces of the elbow in young gymnasts. J Pediatr Orthop 1992;12:344-350.
Bauer M, Jonsson K, Josefsson PO, Linden B: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160.
Tivnon MC, Anzel SH, Waugh TR: Surgical management of osteochondritis dissecans of the capitellum. Am J Sports Med 1976;4:121-128.
Question 16
A Trendelenburg gait is most likely to be seen in association with
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Andersson GB, Deyo RA: History and physical examination in patients with herniated lumbar discs. Spine 1996;21:10S-18S.
Question 17
A 25-year-old woman undergoes surgical treatment of a displaced proximal humeral fracture via a deltopectoral approach. At the first postoperative visit, she reports a tingling numbness along the anterolateral aspect of the forearm. What structure is most likely injured?
Explanation
REFERENCES: McIlveen SJ, Duralde XA, D’Alessandro DF, et al: Isolated nerve injuries about the shoulder. Clin Orthop 1994;306:54-63.
Warner JP: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg
1997;5:130-140.
Question 18
After trial placement of components in a primary total knee arthroplasty, the knee is unable to come to full extension, but the flexion gap is appropriately balanced. After adequate soft-tissue releases have been performed, what is the next most appropriate action to balance the reconstruction?
Explanation
REFERENCES: Ayers DC, Dennis DA, Johanson NA, et al: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 281-286.
Question 19
Which is the best initial study for the diagnostic evaluation of diskogenic low back pain? Review Topic
Explanation
Question 20
A 40-year-old man has a painful mass on his anterior ankle joint with limited range of motion. A radiograph, MRI scan, a gross specimen, and a hematoxylin/eosin biopsy specimen are shown in Figures 5a through 5d. What is the most likely diagnosis?
Explanation
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Hocking R, Negrine J: Primary synovial chondromatosis of the subtalar joint affecting two brothers. Foot Ankle Int 2003;24:865-867.
Question 21
An elderly woman with osteoporosis falls from a standing height, sustaining a low-energy fracture of the acetabulum. What structures are most likely fractured?
Explanation
may present as atypical fracture patterns not always conforming to classic injury patterns described by Judet and associates. This fracture pattern seen commonly in geriatric patients results from low-energy falls with force directly applied to the greater trochanter. Fractures involving the posterior column and/or wall and transverse fracture patterns involving both the anterior and posterior columns occur infrequently in this age group. They are, however, more commonly encountered in younger age groups as a result of higher energy trauma.
Question 22
An 80-year-old man has had increasing shoulder pain for the past 4 months. He reports that it began with soreness and stiffness after chopping some wood. A coronal MRI scan is shown in Figure 16. Initial management should consist of
Explanation
REFERENCES: Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr: Debridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-866.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 299-312.
Question 23
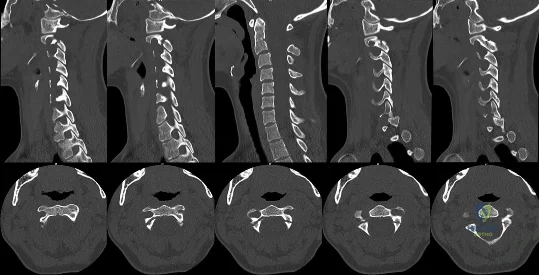
A 32-year-old woman is ejected from her vehicle in a motor vehicle accident. She has a distant history of pacemaker implantation for an unknown arrthymia. She complains of neck pain. Examination reveals midline cervical tenderness but no neurological deficit. CT scans of her cervical spine are shown in Figures A and B. She requires an emergency laparotomy for a splenic injury. Regarding her cervical spine, what is the next best step? Review Topic
Explanation
Traditional hangman's fractures (execution by hanging) are hyperextension-distraction injuries, severing the spinal cord. Motor vehicle accidents/falls are caused by hyperextension-compression, and neurologic injury is uncommon because the fracture fragments separate, decompressing the spinal canal. The Levine-Edwards classification is most commonly used. Type II fractures have disruption of the posterior longitudinal ligament, and Type III have bilateral facet joint dislocation.
Pryputniewicz et al. reviewed axis fractures. They advocate rigid collar or halo immobilization as initial treatment for hangman's fractures, and surgery for fusion failures or irreducible fractures or repeatedly unstable fractures during initial bracing. For unstable fractures or failure of external immobilization, surgical options include C2-C3 ACDF and dorsal C1-C3 fusion.
Jackson et al. reviewed upper cervical spine injuries. They advocate collar immobilization for Types I and IA fractures, gentle reduction and halo vest immobilization for 6-8weeks for Types II and IIA fractures, and open reduction and wiring/plating (depending on the integrity of the facets/lamina) for Type III fractures.
Li et al. performed a systematic review of hangman fractures. They advocate nonrigid external immobilization for stable Type I and Type II injuries, rigid immobilization for Type IIa and III fractures, and surgery for Levine-Edwards Type IIA and III fractures with significant dislocation or possibility for late instability.
Figure A is a composite of sagittal CT scan images through left facet and pars, dens, and right facet and pars. There is no facet dislocation. Figure B is a composite of sequential axial CT scan images showing bilateral pars interarticularis fracture. Illustration A is the Effendi classification. Illustration B is the Levine-Edwards classification.
Incorrect Answers:
Question 24
A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of
Explanation
REFERENCE: Tasdemiroglu E, Tibbs PA: Long-term follow-up results of thoracolumbar fractures after posterior instrumentation. Spine 1995;20:1704-1708.
Question 25
Figures 1 and 2 are of a 51-year-old man who underwent open reduction and internal fixation of a right proximal humerus fracture with concomitant rotator cuff repair. Within 1 year, he develops heterotopic ossification, for which he undergoes excision and hardware removal. Postoperatively, he was noted to have progressive atrophy in the shoulder and anterior humeral head subluxation with attempted shoulder abduction. What nerve was damaged during the most recent procedure?

Explanation
This patient has a deficiency of the anterior deltoid muscle, resulting in inferior subluxation of the humerus with associated glenohumeral instability. Axillary nerve injury during shoulder surgery accounts for 6% to 10% of brachial plexus injuries. In the posterior scapular region, the axillary nerve terminates by dividing into two main branches: the posterior terminal branch, which provides motor innervation to the teres minor and posterior deltoid muscles, and the anterior terminal branch, which provides motor innervation to the anterior and middle portions of the deltoid muscle. The deltoid determines the silhouette of the shoulder and is a stabilizer of the humeral head.
Question 26
What is the most likely type of pathology seen in Figure 16?
Explanation
REFERENCES: McLain R, Weinstein J: Tumors of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1173.
Charlton OP, Martinez S, Gehweiler JA Jr: Pedicle thinning at the thoracolumbar junction: A normal variant. Am J Roentgenol 1980;134:825-826.
Question 27
A 35-year-old man who is involved in an improvised explosive device attack is hit by a piece 57 of shrapnel. He has a solitary penetrating wound in his left tibia. Radiographs show no fracture. He has significant pain and his calf is grossly swollen. He has good sensation and palpable dorsalis pedis and tibialis posterior pulses. He has elevated pressure in all 4 compartments. When performing a 4-compartment fasciotomy using the 2-incision technique, which structure is at risk when opening the deep posterior compartment?
Explanation
Compartment syndrome is commonly seen in lower-extremity trauma, especially in blast injuries or high-energy trauma to the lower extremity. It is important to recall the neurovascular structures present in each of the 4 compartments. The posterior tibial artery is in the deep posterior compartment along with the tibial nerve, the peroneal artery and vein, and the posterior tibial vein. The lateral compartment contains the superficial peroneal nerve.
The anterior compartment contains the deep peroneal nerve and the anterior tibial artery and vein. The superficial posterior compartment does not have any neurovascular structures. The saphenous nerve is superficial.
RECOMMENDED READINGS
Thompson JC, ed. Netter’s Concise Atlas of Orthopaedic Anatomy. Teterboro: NJ: Icon Learning Systems; 2002.
Mubarak SJ, Owen CA. Double-incision fasciotomy of the leg for decompression in compartment syndromes. J Bone Joint Surg Am. 1977 Mar;59(2):184-7. PubMed PMID: 15455478.View Abstract at PubMed
Question 28
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with Review Topic
Explanation
Question 29
What part of the glenoid labrum has the least vascularity?
Explanation
REFERENCE: Cooper DE, Arnoczky SP, O’Brien SJ, et al: Anatomy, histology and vascularity of the glenoid labrum: An anatomical study. J Bone Joint Surg Am 1992;74:46-52.
Question 30
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
REFERENCES: Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.
Question 31
A 75-year-old man presents with a displaced femoral neck fracture. During your surgical exposure for a hemiarthroplasty, the femoral neck has fractured through a pathologic lesion which is diagnosed as a lymphoma on frozen section. The lesion is located in the center of the femoral neck and the calcar femorale is not involved. Your treatment should include:
Explanation
The clinical and radiographic features specific to lymphoma of bone are outlined by Dürr but on the whole are not diagnostic.
Vose describes the current treatment protocols for patients with non-Hodgkin's lymphoma including patients with impending/sustained pathologic fractures.
Question 32
Figures 9a and 9b show the radiographs of a 12-year-old girl who has had right hip pain for the past 4 months. She reports that the pain is so severe that she is unable to walk and is now using a wheelchair. Examination reveals pain with any attempted range of motion. Management should include
Explanation
REFERENCES: Springfield DS, Gebhardt MC: Bone and soft tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 507-518, 542-544.
Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002,
p 2030.
Question 33
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?
Explanation
REFERENCES: Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, pp 632-635.
Question 34
A 6-year-old boy is being treated for acute hematogeneous osteomyelitis of the distal femur with intravenous antibiotics. The best method to determine the success or failure of initial treatment is by serial evaluations of which of the following studies?
Explanation
REFERENCES: Unkila-Kallio L. Kallio MJ, Eskola J, et al: Serum C-reactive protein, erythrocyte sedimentation rate, and white blood cell count in acute hematogenous osteomyelitis of children. Pediatrics 1994;93:59-62.
Herring JA(ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia. PA. WB Saunders, 2008, pp 2090-2100.
AL-Madena Copy
Question 35
A 20-year-old man reports painless snapping about the lateral aspect of the right hip. He denies any history of trauma. Examination reveals no limp or tenderness. Hip range of motion is full, and there is good strength. Radiographs are normal. What anatomic structure is most likely causing these symptoms?
Explanation
REFERENCES: White RA, Hughes MS, Burd T, et al: A new operative approach in the correction of external coxa saltans: The snapping hip. Am J Sports Med 2004;32:1504-1508.
Faraj AA, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Choi YS, Lee SM, Song BY, et al: Dynamic sonography of external snapping hip syndrome.
J Ultrasound Med 2002;21:753-758.
Question 36
A patient with a transverse femur fracture undergoes statically locked antegrade intramedullary nailing. Postoperatively, the patient appears to have a
Explanation
Question 37
Figures 113a and 113b are the radiographs of a 7-year-old girl who was evaluated for a visible elbow deformity by a foster parent. She thought the child fell, but her history was vague. On physical examination, a large prominence was seen over the posterolateral elbow, and the girl lacks the terminal 20 degrees of elbow extension. She has 75 degrees of elbow pronation and supination. She was nontender on examination. What is the most appropriate next treatment step? Review Topic

Explanation
Question 38
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
Explanation
REFERENCES: Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 39
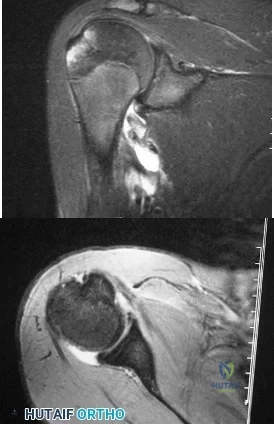
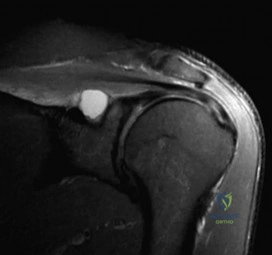
A 24-year-old avid volleyball player has noted gradual onset of shoulder fatigue and weakness limiting his game. Radiographs done by his primary care physician were normal and he has failed to improve with 6 weeks of physical therapy. Given the MRI image shown in Figure A, this patients physical exam may reveal weakness with which of the following actions? Review Topic
Explanation
Extrinsic compression or traction on the suprascapular nerve can result in suprascapular neuropathy. Compression of the nerve may occur at two distinct locations: the suprascapular notch and the spinoglenoid notch. Extrinsic compression of the suprascapular nerve by ganglion cysts can occur at the spinoglenoid notch or, less commonly, at the suprascapular notch. These cysts may originate from the transverse scapular ligament, the fibrous tissue of the scapula, or the glenohumeral joint.
Mittal et al. reviewed the literature and found that the formation of ganglionic cysts in the spinoglenoid fossa occurs with cumulative trauma and leads to entrapment neuropathy of the suprascapular nerve and denervation of the infraspinatus muscle.
Romeo et al. reported on various etiologies of suprascapular neuropathy including traction injury at the level of the transverse scapular ligament or the spinoglenoid ligament and direct trauma to the nerve. They noted that sports involving overhead motion, such as tennis, swimming, and weight lifting, may result in traction injury to the suprascapular nerve, leading to dysfunction. They also reported that the onset of weakness can be subtle and must be differentiated from cervical radiculopathy and degenerative disease of the shoulder.
Figure A depicts a T2 coronal MRI of the shoulder with a cyst easily visualized occupying the suprascapular notch. Illustration A is an algorithm for the management of suprascapular neuropathy. Illustration B is a sagittal MRI from the same patient depicting the ganglion cyst within the suprascapular notch once again leading to atrophy of both the supraspinatus and infraspinatus (asterisks).
Incorrect Answers:
Question 40
Flow cytometry of tumors measures the
Explanation
Question 41
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with
Explanation
REFERENCES: Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96.
Wolf EM, Cheng JC, Dickson K: Humeral avulsion of the inferior glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Question 42
Figure 12 shows the radiograph of a patient who has anterior knee pain. History reveals a femoral fracture at age 5 years. What is the most likely cause of the deformity?
Explanation
REFERENCES: Hresko MT, Kasser JR: Physeal arrest about the knee associated with non-physeal injuries of the lower extremity. J Bone Joint Surg Am 1989;71:698-703.
Bowler JR, Mubarak SJ, Wenger DR: Tibial physeal closure and genu recurvatum after femoral fracture: Occurrence without a tibial traction pin. J Pediatric Orthop 1990;10:653-657.
Question 43
Which of the following is considered a reasonable goal for arthroplasty surgery in rotator cuff arthropathy?
Explanation
REFERENCES: Zeman CA, Arcand MA, Cantrell JS, Skedros JG, Burkhead WZ Jr: The rotator cuff-deficient arthritic shoulder: Diagnosis and surgical management. J Am Acad Orthop Surg 1998;6:337-348.
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for the treatment of defects in the rotator cuff and the surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Williams GR Jr, Rockwood CA Jr: Hemiarthroplasty in rotator cuff-deficient shoulders. J Shoulder Elbow Surg 1996;5:362-367.
Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
Question 44
A young active patient with a complete isolated posterior cruciate ligament (PCL) tear undergoes a double bundle PCL reconstruction. The tensioning pattern of the anterolateral (AL) and posteromedial (PM) bundles most likely to reproduce the most normal knee kinematics would be to tension
Explanation
REFERENCES: Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin T, Woo SL: Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 2000;28:144-151.
Mannor DA, Shearn JT, Grood ES, Noyes FR, Levy MS: Two-bundle posterior cruciate ligament reconstruction: An in vitro analysis of graft placement and tension. Am J Sports Med 2000;28:833-845.
Question 45
Figure 5 is a T2-weighted MR image of a 26-year-old man who has had left leg pain for 3 months that has failed nonsurgical treatment. Surgical decompression is planned. Which approach would provide the most direct ability to perform surgical decompression?

Explanation
The MR image shows a far lateral disk herniation impinging on the exiting nerve root lateral to the exiting foramen. This is reached most directly with a far lateral (Wiltse) approach. This is a posterior paramedian approach that uses the interval between the paraspinal muscles (multifidus and longissimus) and arrives onto the facet joints. The intertransverse membrane can then be released, exposing the far lateral disk herniation. A posterior midline approach will allow easy access to the spinal canal, which is medial to the disk herniation, and will not allow for easy disk removal without the need for a facetectomy, which would destabilize the level. An anterior approach would not allow for access to the far lateral disk herniation, nor would a traditional retroperitoneal or newer transpsoas approach.
RECOMMENDED READINGS
Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988 Jun;13(6):696-706. PubMed PMID: 3175760. View Abstract at PubMed
Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: indications and results. J Neurosurg. 1995 Oct;83(4):648-56. PubMed PMID: 7674015. View Abstract at PubMed
Question 46
A 68-year-old man reports a 4-week history of progressive left-sided lower back and hip pain. The pain is in the posterior buttock region with radiation to the groin and to the left anterior knee region. The pain is aggravated with walking and improves with rest. There is no history of previous trauma. Radiographs are seen in Figures 14a and 14b, and MRI scans are seen in Figures 14c through 14e. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2007, pp 339-361.
Spivak JM, Connolly PJ (ed): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 43-56.
Question 47
Which of the following statements best describes the typical early presentation of osteochondritis dissecans of the elbow? Review Topic
Explanation
Question 48
Triple arthrodesis in a reduced position
Explanation
Question 49
Among patients with lumbar degenerative disk disease and low back pain, what factor is most predictive of clinical outcomes after surgical management? Review Topic
Explanation
Question 50
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
REFERENCE: Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.
Question 51
Which of the following medications may have a negative effect on bone healing following fracture?
Explanation
REFERENCES: Gerstenfeld LC, Thiede M, Seibert K, et al: Differential inhibition of fracture healing by non-selective and cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs. J Orthop Res 2003;21:670-675.
Harder AT, An YH: The mechanisms of the inhibitory effects of nonsteroidal anti-inflammatory drugs on bone healing: A concise review. J Clin Pharmacol 2003;43:807-815.
Question 52
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
Explanation
REFERENCES: Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273.
Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Kim WY, Hearn TC, Seleem O, et al: Effect of pin location on stability of pelvic external fixation. Clin Orthop Relat Res 1999;361:237-244.
Question 53
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. If present, what is the most likely complication after surgical treatment in this scenario?
Explanation
and degenerative joint disease.
Question 54
Figure 17 shows the AP radiograph of a 5-year old child who has mild short stature and a painless bilateral gluteus medius lurch. Initial work-up should include
Explanation
REFERENCES: Sponseller PD: Skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 269-270.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 689-691.
Question 55
-An absolute contraindication for closed management of a humeral shaft fracture in a fracture brace is
Explanation

Question 56
Figure 53 shows the MRI scan of a 53-year-old carnival worker who has pain and swelling in the left shoulder as a result of attempting to stop a roller coaster car with his arm. Examination reveals decreased ROM, apprehension, and inability to move the dorsum of his hand away from his back. Treatment should consist of
Explanation
Question 57
A 21-year-old collegiate female cross-country athlete reports right hip pain that begins about 12 miles into a run, followed by pain resolution when she discontinues running. However, each time she tries to resume a running program, she experiences recurrence of pain deep in the anterior groin. A plain radiograph and MRI scan are shown in Figures 8a and 8b. Management should consist of
Explanation
REFERENCES: Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Lynch SA, Renstrom PA: Groin injuries in sport: Treatment strategies. Sports Med 1999;28:137-144.
Question 58
- A 7-year old boy has a painless abductor limp and limited hip abduction. Radiographs show varus of the proximal femur, with a narrow upper femoral epiphysis that has the shape of an inverted "Y". Which of the following factors best predicts the risk that the deformity will become worse?
Explanation
Question 59
An 18-year-old high school football player exits the field after making a tackle on the opening kickoff. He reports "feeling out of it" and states that he has a headache. He does not recall any loss of consciousness and has no amnesia. He is unable to list the months of the year in reverse order on questioning. He does not return to the game and feels normal at the completion of the game. What is the most sensitive test in assessing deficits after mild traumatic brain injury? Review Topic
Explanation
Question 60
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
REFERENCES: Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 61
All of the following are advantages of supine over lateral positioning during intramedullary nailing of subtrochanteric femur fractures EXCEPT:

Explanation
Advantages of the supine position include: may help protect a potentially unstable spine, facilitates access to sites other than the injured femur, shorter setup time, rotational and angulatory deformities may be more easily appreciated. Disadvantages of the supine position include: starting point localization may be more difficult.
Question 62
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
REFERENCES: Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
D’Antonio J, Capello W, Manley M, et al: New experience with alumina-on-alumina ceramic bearings for total hip arthroplasty. J Arthroplasty 2002;17:390-397.
Question 63
Which of the following patients has the highest risk of developing recurrent instability after an arthroscopic Bankart procedure for anterior shoulder instability? Review Topic
Explanation
The surgical management of anterior shoulder instability consists of both arthroscopic and open approaches. The guiding principles for treatment are the restoration of the normal glenoid labrum anatomy and retensioning of the inferior glenohumeral ligament which is achieved via soft-tissue reconstructions (repair of any labral detachment +/- capsular shift) or bony procedures (such as transfer of the coracoid process).
Ahmed et al. reviewed 302 patients who had undergone arthroscopic Bankart repair and capsular shift for the treatment of recurrent anterior glenohumeral instability. The prevalence of patient and injury-related risk factors for recurrence was assessed. The rate of recurrent glenohumeral instability after arthroscopic Bankart repair and capsular shift was 13.2%. The risk of recurrence was independently predicted by the patient’s age at surgery, the severity of glenoid bone loss, and the presence of an engaging Hill-Sachs lesion.
Balg et al. identified risk factors for recurrent instability after arthroscopic Bankart procedure in 131 consecutive patients. Age under 20 years at the time of surgery; involvement in competitive or contact sports or those involving forced overhead activity; shoulder hyperlaxity; a Hill-Sachs lesion present on an AP radiograph of the shoulder in external rotation and/or loss of the sclerotic inferior glenoid contour were all identified as risk factors. These factors were integrated into a 10-point preoperative instability severity index score (ISIS). Patients with a score over 6 points had an unacceptable recurrence risk of 70%.
Illustration A summarizes the components of the ISIS as developed by Balg and Boileau.
Incorrect Answers:
Question 64
..The optimal method to treat a recurrent presentation of pigmented villonodular synovitis (PVNS) with diffuse joint involvement in a 24-year-old woman with pain and symptomatic effusions is
Explanation

Question 65
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future?
Explanation
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Dearolf WW III, Betz RR. Vogl LC, et al: Scoliosis in pediatric spinal cord-injured patients. J Pediatr Orthop 1990;10:214-218.
Mehta S, Betz RR. Mulcahey MJ, et al: Effect of bracing on paralytic scoliosis secondary to spinal cord injury. J Spinal Cord Med 2004;27:S88-S92.
Question 66
Which of the following radiographic parameters is most predictive of a poor result following multilevel fusion surgery for adult degenerative scoliosis? Review Topic
Explanation
Question 67
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?
Explanation
REFERENCES: Albert MJ, Drvaric DM: Little League shoulder: Case report. Orthopedics 1990;13:779-781.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 68
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?
Explanation
REFERENCES: Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
Sugano N, Noble PC, Kamaric E, et al: The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-719.
Question 69
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 70
A large circumferential proximal femoral allograft is to be used in the reconstruction of a failed femoral component in a total hip arthroplasty. To enhance fixation of the graft to the implant, which of the following strategies should be used?
Explanation
REFERENCES: Allan DG, Lavoie GJ, Rudan JF, et al: The use of allograft bone in revision total hip arthroplasty, in Friedlaender GE, Goldberg VM (eds): Bone and Cartilage Allografts: Biology and Clinical Applications. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1991, pp 263-264.
Gross AE, Lavoie MV, McDermott P, Marks P: The use of allograft bone in revision of total hip arthroplasty. Clin Orthop 1985;197:115-122.
Head WC, Berklacich FM, Malinin TI, Emerson RH Jr: Proximal femoral allografts in revision total hip arthroplasty. Clin Orthop 1987;225:22-36.
Question 71
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?
Explanation
REFERENCES: Fanton GS: Arthroscopic electrothermal surgery of the shoulder. Op Tech Sports Med 1998;6:157-160.
David TS, Drez DJ Jr: Electrothermally-assisted capsular shift. IEEE Eng Med Biol Mag 1998;17:102-104.
Question 72
What are the five major compartments of the foot?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 262-264.
Shereff MJ: Compartment syndromes of the foot. Instr Course Lect 1990;39:127-132.
Question 73
The flexor hallucis longus tendon is at greatest risk of injury with a lateral-to-medial drill or screw during fixation of what structure?

Explanation
Question 74
Hip pain of month duration has developed in a year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. The patient has a final culture that reveals methicillin-resistant Staphylococcus aureus (MRSA). If the attending physician recommends the two-stage protocol, including the use of an antibiotic-cement spacer, what is the most likely prognosis for this patient?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California
Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 75
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior knee pain, a trace effusion, a 2+ posterior drawer, a grade 1+ stable Lachman, no valgus laxity, and negative dial tests at 30 degrees and 90 degrees. What is the best treatment strategy at this time? Review Topic
Explanation
Question 76
Serum parathyroid hormone level The plain radiograph of the shoulder shows lytic lesions in the scapular spine, distal clavicle, and the proximal third of the clavicle. There is an elliptical erosion in the proximal clavicle. These three lesions suggest a diagnosis of metastatic bone disease or multiple myeloma. The biopsy specimen shows plasma cells. The plasma cells have these characteristic features: Eccentrically placed nucleus Peripheral clumping of the nuclear chromatin A perinuclear halo The diagnosis is multiple myeloma. Staging is important and is performed with a skeletal survey, bone marrow biopsy, hemoglobin level, and chemistry studies including kidney function and serum calcium determination. Serum protein electrophoresis is performed to assess the amount of abnormal gammaglobulin in the serum. There are three major criteria in the diagnosis of multiple myeloma:
Explanation
A 55-year old man presents with a 4-month history of shoulder discomfort. The plain radiographs are shown in Slide 1 and a biopsy in Slide 2. Which of the following tests will probably be abnormal:
Question 77
Figures 87a and 87b are the radiographs of an 18-year-old pedestrian who was struck by a car. During intramedullary nailing, it is difficult to maintain proper alignment. Poller blocking screws placed in the proximal fragment at which position(s) relative to the nail can help prevent the typical deformity?

Explanation
Question 78
All of the following are characteristic of synovium affected by rheumatoid arthritis (RA) EXCEPT:
Explanation
Normal synovium consists of two layers, the intimal and the sublining, and two types of cells, type A and B. In RA, the following changes to the synovium are seen: 1) hyperplasia, with the intimal lining increasing from two cell layers to 10-20 layers 2) decreased apoptosis of the lining 3) increased angiogenesis and 4) abundant lymphocytes around vessels, forming lymphoid follicles.
The synovial pannus is invasive granulation tissue that contains fibroblast-like synoviocytes, but few inflammatory cells. The synovial cells in the pannus have anchorage-independent growth and invasive capabilities, allowing them to directly attack and destroy articular cartilage.
Koch et al. note that the possible contributions of angiogenesis to the proliferation of the inflammatory synovial pannus and the ingress of inflammatory leukocytes into the synovial tissue in RA have been extensively studied. Relevant angiogenesis inducers seen in RA include FGF-2, VEGF, TGFß, TNFa, IL-1, IL-8, VCAM-1, among others. Modulation of angiogenesis may be a viable therapeutic option for RA in the future.
Incorrect Answers:
Question 79
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?

Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on-metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of childbearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 80
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to
Explanation
REFERENCES: Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Question 81
..First-line treatment recommendations include
Explanation
Ultrasound
MRI scan of the thigh
Chest CT scan and whole-body bone scan
Positron emission tomography (PET) scan
Presurgical radiation therapy
Marginal resection
Radical resection and postsurgical radiation
Transverse incision centered over the mass
Incision centered over the mass in line with long axis of limb
Sentinel node biopsy
Core needle biopsy
For each soft-tissue mass clinical scenario or question below, match the most appropriate next evaluation or treatment step listed above.
Question 82
A previously healthy 35-year-old man was involved in a rollover motor vehicle accident 2 days ago. He was placed in a semi-rigid cervical orthosis. He now reports mostly axial neck pain with attempted range of motion. Examination reveals the mechanical neck pain but no obvious neurologic deficits. AP, flexion, and extension radiographs are shown in Figures 10a through 10c, and sagittal and coronal CT scans are shown in Figures 10d and 10e. What is the most appropriate management at this time?
Explanation
REFERENCES: Shilpakar S, McLaughlin MR, Haid RW Jr, et al: Management of acute odontoid fractures: Operative techniques and complication avoidance. Neurosurg Focus 2000;8:e3.
Subach BR, Morone MA, Haid RW Jr, et al: Management of acute odontoid fractures with single-screw anterior fixation. Neurosurgery 1999;45:812-819.
Fountas KN, Kapsalaki EZ, Karampelas I, et al: Results of long-term follow-up in patients undergoing anterior screw fixation for type II and rostral type III odontoid fractures. Spine 2005;30:661-669.
Question 83
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. Examination reveals symmetric knee flexion, extension, and frontal alignment compared to the contralateral knee. She has 1-cm of shortening of the right femur. History reveals that she has always been in the 50th percentile for height, and her skeletal age matches her chronologic age. Radiographs are shown in Figure 9. What is the expected consequence at maturity?
Explanation
REFERENCES: Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Moseley CF: Assessment and prediction in leg-length discrepancy. Instr Course Lect 1989;38:325-330.
Question 84
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?
Explanation
REFERENCES: Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
McCarty DJ, Halverson PB, Carrera GF, Brewer BJ, Kozin F: Milwaukee shoulder: Association of microspheroids containing hydroxyapatite crystals, active collagenase, and neutral protease with rotator cuff defects. I: Clinical aspects. Arthritis Rheum 1981;24:464-473.
Question 85
--The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
Explanation
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. An ultrasound can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario.
Because the patient has a correctable deformity (gaps 3 mm with valgus stress) and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgicalplanning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient.A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation,examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result,current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 is an indication for HTO but does not influence technique.
Question 86
A still active 86-year-old pastry chef falls in her kitchen and notes pain and deformity of her little finger. There are no open wounds. Radiographs are shown in Figures 49a and 49b. What is the most appropriate management?
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.
Question 87
A collegiate lacrosse player is struck on the head by an opposing player’s stick. She is initially unresponsive. She regains consciousness within 2 minutes but remains confused and uncooperative, complaining of head and neck pain. This is her second concussion of the calendar year. Initial management should consist of
Explanation
Question 88
Progressive paralysis is most likely to be seen in association with what type of congenital vertebral abnormality?
Explanation
REFERENCES: McMaster MJ, Singh H: Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-1383.
Dubousset J: Congenital kyphosis and lordosis, in Weinstein SL (ed): The Pediatric Spine: Principles and Practice, ed 1. New York, NY, Raven Press, 1994, pp 245-258.
Question 89
Following its exit from the sciatic notch, the sciatic nerve passes between what two muscles?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 335-348.
Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Williams,
1978, Figure 4-34.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 90
A man who weighs 75 kg (165 pounds) is scheduled for elective total hip arthroplasty. He reports a history consistent with anaphylaxis from penicillin. Within 1 hour of the incision the patient should receive 1000 mg of
Explanation
Question 91
A 30-year-old man sustains a head injury as well as a femur and pelvis fractures as the result of a rollover motor vehicle accident. He is initially comatosed, but recovers cognitive function after 10 days in the hospital. Soon after awakening he complains of wrist pain and an x-ray demonstrates a distal radius fracture. What is the most likely explanation for this delayed diagnosis?

Explanation
Question 92
A 28-year-old woman undergoes a closing-wedge high tibial osteotomy (HTO) for medial compartment overload after medial meniscectomy. Postsurgically, she reports improvement in her medial pain and resumes normal activities. About 9 months after her surgery, however, she reports burning pain in the front of her knee with running. Her examination reveals no joint line tenderness, mild pain with patellar compression, and limited patellar glides. What is the most likely cause of her symptoms?
Explanation
Question 93
Figures 23a and 23b show the MRI scans of a 50-year-old woman who has increasing gait disturbance. She reports three falls in the past week. Examination reveals hyperreflexia, motor weakness in the biceps and triceps, and a positive Hoffman’s sign. What is the most appropriate treatment plan? Review Topic

Explanation
(SBQ12SP.77) A 68-year-old is undergoing lateral lumbar interbody fusion using the tranpsoas approach. Which of the following statements is true regarding the safe approach zone for this procedure as you move cranial to caudal in the lumbar spine? Review Topic
Safe approach zone increases due to vessels moving more ventral
Safe approach zone increases due to lumbar plexus moving more dorsal
Safe approach zone decreases due to vessels moving more dorsal
Safe approach zone decreases due to lumbar plexus moving more ventral
Safe approach zone remains the same throughout the lumbar spine
As you move cranial to caudal in the lumbar spine, the safe approach zone for the lateral transpsoas approach decreases due to the more ventral position of the lumbar plexus.
Lateral lumbar interbody fusion has become more common for degenerative spine disorders and adjacent segment degeneration. This transpsoas approach is typically useful for pathology from L1-L2 disc space to the L4-L5 disc space and places the lumbar plexus at risk. Working at the more caudal disc spaces is especially difficult given the more ventral position of the plexus, but the use of triggered EMG retractors and probes can help prevent nerve injuries. Surgical approach can be especially difficult in patients with rotational deformities.
Benglis et al. did a cadaver study with specimens placed lateral to trace the course of the lumbar plexus. They found that the plexus move more ventral with respect to the disc space moving more caudal in the lumbar spine.
Park et al. used 10 cadaver specimens to measure the distance of the lumbar nerve roots from the center of the disc space in the lateral approach. While disc space access was generally safe, there was less distance to the nerve root for more caudal disc levels.
Regev et al. did a MRI study to evaluate the safe working corridor for the lateral approach. The safe zone narrows considerably in the L4-L5 disc space due to more
ventral position of the nerve roots, and they recommend careful monitoring when addressing this level.
Incorrect
Question 94
-Which treatment approach for acetabular fractures carries the highest risk for heterotopic ossification?
Explanation
Question 95
Immediately after undergoing lumbar instrumentation, a patient reports severe right leg pain and has 4+/5 weakness. Figure 24 shows an axial CT scan of L5. Exploratory surgery will most likely reveal
Explanation
REFERENCES: Esses SI, Sachs BL, Dreyzin V: Complications associated with the technique of pedicle screw fixation: A selected survey of ABS members. Spine 1993;18:2231-2238.
Laine T, Lund T, Ylikoski M, et al: Accuracy of pedicle screw insertion with and without computer assistance: A randomised controlled clinical study in 100 consecutive patients. Eur Spine J 2000;9:235-240.
Lonstein JE, Denis F, Perra JH, et al: Complications associated with pedicle screws. J Bone Joint Surg Am 1999;81:1519-1528.
Question 96
An 18-year-old male soccer player sustains a knee injury during a game. Examination is notable for a positive pivot shift test. What other physical examination finding is most likely to be present? Review Topic
Explanation
ACL tears usually occur as a result of a non-contact pivoting injury. Abnormal anterior translation results in bone contusions of mid-lateral femoral condyle and posterolateral tibia, which can be seen on MRI. Other concomitant intraarticular injuries include meniscal tears (lateral > medial), chondral damage and other ligamentous injury (MCL, LCL, PLC) usually found in cases of higher energy trauma such as a knee dislocation.
Piasecki et al prospectively analyzed intraarticular injuries associated with ACL tears in high school athletes by gender and sport. There was no significant difference in mechanism of injury between sexes. Female basketball and soccer players had fewer intraarticular injuries (medial femoral condyle lesions, medial and lateral meniscus tears) compared to male athletes. The authors hypothesized that women may therefore enjoy a better prognosis following reconstruction.
Spindler et al performed a prospective cohort study investigating concomitant intraarticular injuries in patients who underwent ACL reconstruction. Eighty percent of patients had a bone bruise on MRI, 68% involving the lateral condyle. At time of arthroscopic reconstruction, meniscal tears were identified in 56% of lateral menisci and 37% of medial menisci.
Incorrect Responses:
Question 97
Figure 12a shows the clinical photograph of a 36-year-old man who has left shoulder pain and dysfunction after undergoing a lymph node biopsy 2 years ago. The appearance of the shoulder during abduction and a wall push-up maneuver is shown in Figures 12b and 12c, respectively. Which of the following procedures provides the best pain relief and function?
Explanation
REFERENCES: Steinman SP, Spinner RJ: Nerve problems in the shoulder, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1013-1015.
Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop Relat Res 1999;368:5-16.
Question 98
The patient does not improve with 1 year of rehabilitation exercises. MR arthrography reveals a normal glenoid labrum and rotator cuff. Surgical treatment should consist of
Explanation
This patient has multidirectional instability (MDI). Symptoms are typically of insidious onset with nonspecific sports-related pain during the second or third decade of life. The etiology of MDI involves a patulous inferior capsular complex, but, in isolation, this lesion may not produce symptoms. Patients with MDI have abnormal patterns of rotator cuff muscle activity that is not restored with nonsurgical treatment. Symptomatic patients with MDI also demonstrate increased rates of abnormal scapular kinematics. The prevalence of MDI is higher among overhead athletes. The sulcus sign is an examination finding that produces a visible dimple inferior to the lateral border of the acromion with application of inferior traction on the arm. Generalized hyperlaxity or a connective tissue disorder may be present. Physical therapy for strengthening of the rotator cuff and scapular stabilizers remains the recommended initial treatment. Rehabilitation should continue for at least 6 months (and possibly much longer). Motivated patients frequently report diminished pain and improved stability with strengthening exercises. If nonsurgical measures fail to provide adequate relief, arthroscopic capsular plication is a viable treatment option, with high rates of return to play among properly selected patients. Thermal capsulorrhaphy has a high failure rate and poses potential for serious complications, including chondrolysis and thermal injury to the axillary nerve. Closure of the rotator interval has not been definitively shown to enhance stability or improve outcomes for patients with MDI.

Question 99
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Explanation
REFERENCES: Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 100
A surgeon desires to use an implant that will be able to absorb as much energy as possible before it fails. The implant should be made of a material that has which of the following properties?
Explanation
