Orthopedic Board Review MCQs: Shoulder, Arthroplasty & Foot | Part 243

Key Takeaway
This page offers Part 243 of a high-yield orthopedic surgery board review quiz. Featuring 100 verified MCQs mirroring AAOS and OITE exam formats, it's designed for residents and surgeons. Focus on Arthroplasty, Foot, Infection, Shoulder to master crucial topics for certification exams.
About This Board Review Set
This is Part 243 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 243
This module focuses heavily on: Arthroplasty, Foot, Infection, Shoulder.
Sample Questions from This Set
Sample Question 1: An obese 4-year-old boy has infantile Blount’s disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of...
Sample Question 2: A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side, but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear nor...
Sample Question 3: An active 66-year-old man who underwent total shoulder arthroplasty 3 years ago now reports pain. Laboratory studies reveal an elevated erythrocyte sedimentation rate and C-reactive protein. Intraoperative frozen section reveals greater tha...
Sample Question 4: A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsu...
Sample Question 5: Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory stud...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An obese 4-year-old boy has infantile Blount’s disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of
Explanation
REFERENCES: Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Loder RT, Johnston CE: Infantile tibia vara. J Pediatr Orthop 1987;7:639-646.
Question 2
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side, but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
Explanation
This clinical scenario describes a patient with an isolated injury affecting the infraspinatus muscle. The anatomic location of such a lesion would be at the spinoglenoid notch, at which the suprascapular nerve may be compressed distal to its innervation of the supraspinatus but proximal to the infraspinatus innervation. A calcified transverse scapular ligament would also affect the suprascapular nerve but is proximal to the innervation of both muscles. Quadrilateral space syndrome would affect innervation of the deltoid (and teres minor). Parsonage-Turner syndrome is a more diffuse, and often severely painful, brachial plexus neuropathy.
Question 3
An active 66-year-old man who underwent total shoulder arthroplasty 3 years ago now reports pain. Laboratory studies reveal an elevated erythrocyte sedimentation rate and C-reactive protein. Intraoperative frozen section reveals greater than 10 white blood cells per high power field on two slides and the Gram stain reveals gram-positive cocci in clusters. What is the most appropriate surgical treatment to eradicate the infection and maintain function? Review Topic
Explanation
Question 4
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time? Review Topic
Explanation
Question 5
Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory study would be most helpful in confirming the diagnosis?
Explanation
REFERENCES: Calin A: Ankylosing spondylitis. Clin Rheum Dis 1985;11:41-60.
Booth R, Simpson J, Herkowitz H: Arthritis of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 431.
van der Linden S, Valkenburg H, Cats A: The risk of developing ankylosing spondylitis in HLA-B27 positive individuals: A family and population study. Br J Rheumatol 1983;22:18-19.
Question 6
After full healing from this injury, which option most likely will help to optimize this patient's activities?
Explanation
Midfoot fracture dislocations typically occur after a fall from a height or a motor vehicle collision involving severe dorsiflexion loading of the foot from a brake pedal or the floorboards. The deformity that results may be subtle because the subluxation may be a valgus or varus rotation around the midfoot rather than pure dorsiflexion. Early recognition and reduction is indicated to minimize secondary complications such as nerve injury or vascular compromise. Closed reduction usually necessitates formal anesthesia in an operating room to permit adequate relaxation and reduction. In many cases, satisfactory reduction can be accomplished closed, but the surgeon must be prepared to perform an open reduction if needed. The most common reason for failed closed reduction is that the talar head is caught by the tibialis posterior tendon (under which the talar head has protruded). This acts as a Chinese finger trap, preventing relocation by the usual distraction followed by
a plantar flexion maneuver. In these cases, open reduction is performed through a dorsomedial incision through which the tibialis posterior is retracted medially, allowing reduction of the talonavicular joint. The joints usually require pinning to maintain stability during healing. The long-term prognosis for these injuries is guarded because many patients develop degenerative changes in the Chopart joint. If symptomatic arthritis develops, helpful external supports are designed to limit sagittal motion at the joint (for example, carbon fiber inserts or rocker-bottom soles).
RECOMMENDED READINGS
Swords MP, Schramski M, Switzer K, Nemec S. Chopart fractures and dislocations. Foot Ankle Clin. 2008 Dec;13(4):679-93, viii. Doi: 10.1016/j.fcl.2008.08.004. Review. PubMed PMID: 19013402.View Abstract at PubMed
Richter M, Thermann H, Huefner T, Schmidt U, Goesling T, Krettek C. Chopart joint fracture-dislocation: initial open reduction provides better outcome than closed reduction. Foot Ankle Int. 2004 May;25(5):340-8. PubMed PMID: 15134617. View Abstract at PubMed
Question 7
A 21-year-old woman is struck by a car and sustains a Gustillo IIIB fracture of the tibia. The wound was debrided and immobilized with an external fixator. Radiographs are shown in Figure A. The soft tissue defect was covered with a free flap. Her recovery was complicated by wound infection with Klebsiella pneumoniae and Escherichia coli. One month after her injury, she underwent intramedullary nailing and placement of an antibiotic spacer measuring 15cm in length. Radiographs are shown in Figure B. At the next stage of surgery 6 weeks later, the surgeon should plan to do all of the following:

Explanation
The Masquelet staged technique of induced membranes is an option for filling large bone defects up to 25cm in length. This technique protects against autograft resorption, stimulates mesenchymal cell-to-osteoblast differentiation, maintains graft position, and prevents soft tissue interposition. Cement impregnation achieves high local antibiotic concentration without risk of systemic toxicity.
Ashman et al. discussed the techniques of addressing bone defects. Options include:
(1) acute limb shortening (up to 4cm in the tibia and humerus, and 7cm in the femur);
(2) distraction osteogenesis for defects up to 10cm long (at 1mm/day with consolidation period of 5days per mm, or total treatment time of up to 60days/cm), (3) autograft (up to 25cm of vascularized fibula, or 3cm of nonvascularized iliac crest),
and (4) Masquelet technique.
Taylor et al. reviewed the induced membranes technique. They found that the membrane is well vascularized and composed of type I collagen with fibroblasts with an inner epithelial cell layer. There is a high concentration of VEGF, RUNX2 (CBFA1), TGFß1, and BMP2. The membrane is sutured over bone graft to create a closed pouch. When a nail is present, they note a second internal membrane around the nail, potentially increasing local vascularity and osteoinductive factor concentration.
Figure A shows a Gustillo IIIB tibia fracture with a large bone defect held in a temporizing external fixator. Figure B shows the same defect following intramedullary nailing and with a cement spacer placed circumferentially around the nail in the defect.
Incorrect Answers
Question 8
Moderate distance running has what effect on knee articular cartilage in asymptomatic distance runners?
Explanation
Question 9
A 19-year-old male collegiate rower has a 3-month history of right shoulder pain. There was no inciting trauma prior to the onset of his pain. He also complains of weakness, particularly in abduction and overhead activity. Examination reveals no range-of-motion deficits. Strength testing of the right shoulder demonstrates 4/5 motor strength in forward elevation and abduction. His Beighton hypermobility score is 3/9. Figure 1 shows his scapular position during a wall pushup maneuver. An EMG would likely reveal damage to what nerve?

Explanation
Question 10
A 42-year-old man with a history of renal cell carcinoma has progressive weakness in the lower extremities for the past 3 weeks. The patient desires intervention. A sagittal T 2 -weighted MRI scan is shown in Figure 9a, and a sagittal contrast enhanced T 1 -weighted MRI scan is shown in Figure 9b. He currently ambulates minimal distances with a walker. His life expectancy is 8 months. Treatment of the spine lesion should consist of
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
White AP, Kwon BK, Lindskog DM, et al: Metastatic disease of the spine. J Am Acad Orthop Surg 2006;14:587-598.
Question 11
In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?
Explanation
require surgery.
REFERENCES: Little DG, Song KM, Katz D, Herring JA: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am
2000;82:685-693.
Anderson M, Hwang SC, Green WT: Growth of the normal trunk in boys and girls during the second decade of life; related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 1965;47:1554-1564.
Question 12
A 40-year-old man has had hip pain with increased activity over the past year. Examination reveals restriction of motion and tenderness with combined hip flexion, adduction, and internal rotation. An AP radiograph is shown in Figure 34. What is the most likely diagnosis?
Explanation
REFERENCES: Beall DP, Sweet CF, Martin HD, et al: Imaging findings of femoraoacetabular impingement syndrome. Skeletal Radiol 2005;34:691-701.
Mardones RM, Gonzalez C, Chen Q, et al: Surgical treatment of femoroacetabular impingement: Evaluation of the effect of the size of the resection. J Bone Joint Surg Am 2006;88:84-91.
Question 13
Figure 52 shows the MRI scan of a 28-year-old baseball pitcher. Examination will most likely reveal which of the following findings?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi V: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7:223-227.
Question 14
Examination of the shoulder seen in Figure 52 shows atrophy and tenderness of the infraspinous fossa and profound weakness in external rotation. The supraspinous fossa shows normal muscle bulk. What is the most likely cause of this condition?
Explanation
REFERENCES: Schickendantz MS, Ho CP: Suprascapular nerve compression by a ganglion cyst: Diagnosis by magnetic resonance imaging. J Shoulder Elbow Surg 1993;2:110-114.
Thompson RC, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop 1982;166:185-187.
Iannotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Question 15
A patient undergoes the procedure shown in Figure 19. An important part of this procedure is preservation of what wrist ligament?
Explanation
REFERENCE: Jebson PJ, Engber WD: Proximal row carpectomy. Tech Hand Up Extrem Surg 1999;3:32-36.
Question 16
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?
Explanation
REFERENCES: Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Kelley SS: Periprosthetic femoral fractures. J Am Acad Orthop Surg 1994;2:164-172.
Question 17
Acetaminophen is an antipyretic medication. It exerts its pharmacologic effects by inhibiting which of the following enzymes?
Explanation
REFERENCE: Mancini F, Landolfi C, Muzio M, et al: Acetaminophen down-regulates interleukin-1beta-induced nuclear factor-kappaB nuclear translocation in a human astrocytic cell line. Neurosci Lett 2003;353:79-82.
Question 18
What is the most appropriate way to communicate instructions to a family when there is a language barrier?
Explanation
Ideally, professional medical interpreters should be used in situations involving language difficulties. Printed instructions are helpful, but, if there is a language barrier, these instructions cannot substitute for conversing and answering questions. Asking the child to translate (no matter how fluent he or she may be) is suboptimal. Nonmedical staff may not be fluent enough to adequately translate medical terms.

RESPONSES FOR QUESTIONS 14 THROUGH 16
Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
Aspiration, cultures, Lyme serology, and oral amoxicillin
Biopsy, culture, curettage, bone graft, and possible internal fixation
Physical therapy, ibuprofen, and an antinuclear antibody test
Select the most appropriate treatment above to address each clinical scenario below.
Question 19
Which of the following is associated with increased fetal morbidity and mortality in acetabular fractures during pregnancy?
Explanation
Question 20
What is the most serious complication that may occur with a ceramic-on-ceramic bearing in a total hip prosthesis?
Explanation
Question 21
Which of the following findings is a contraindication to isolated percutaneous pinning of a distal radius fracture?
Explanation
REFERENCES: Trumble TE, Wagner W, Hanel DP, et al: Intrafocal (Kapandji) pinning of distal radius fractures with and without external fixation. J Hand Surg Am 1998;23:381-394.
Choi KY, Chan WS, Lam TP, et al: Percutaneous Kirschner-wire pinning for severely displaced distal radial fractures in children: A report of 157 cases. J Bone Joint Surg Br 1995;77:797-801.
Weil WM, Trumble TE: Treatment of distal radius fractures with intrafocal (Kapandji) pinning and supplemental skeletal stabilization. Hand Clin 2005;21:317-328.
Question 22
A 21-year-old football player reports increasing pain and a deformity involving his chest after colliding with another player during a scrimmage. Imaging studies confirm an anterior sternoclavicular dislocation. Management should consist of
Explanation
REFERENCES: Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 477-525.
Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Question 23
Figures 81a through 81c show the MRI scans of a 53-year-old man who has experienced a long history of progressively worsening right-sided back pain with radiation to the buttocks and right lower extremity. Examination reveals weakness and hyperreflexia in the right lower extremity. He reports intermittent episodes of urinary incontinence. What is the most appropriate surgical approach? Review Topic

Explanation
Question 24
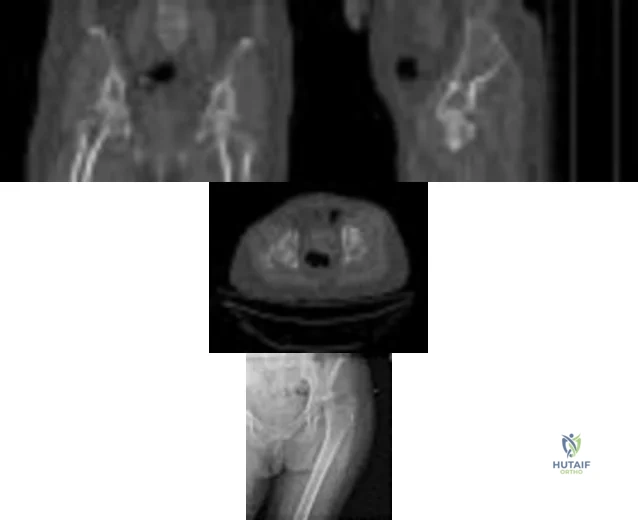
Figures below show the radiographs, and the CT obtained from a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?
Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 25
A 29-year-old female has sustained the acute injury shown in Figure A. Which of the following is an indication for open reduction internal fixation in this patient?

Explanation
In patients who present with no medial widening on standard ankle radiographs and no clinical symptoms of deltoid ligament injury, the integrity of the deltoid ligament remains unknown. The gravity stress radiograph may be used to help identify a deltoid ligament injury in association with an isolated distal fibular fracture. Stage-IV supination-external rotation fractures, which involve the deltoid ligament, are more likely to be treated operatively as they are often considered unstable ankle fractures.
Egol et al. reviewed 101 patients with isolated fibular fracture and an intact mortise. They found that medial tenderness, swelling, and ecchymosis were not sensitive with regard to predicting widening of the medial clear space on stress radiographs. Interestingly, they report that good functional results can be obtained in patients with widening of the medial clear space on a stress radiograph in the absence of medial signs.
Gill et al. compared the effectiveness of gravity stress radiograph as compared to manual stress radiograph for the detection of deltoid ligament injury in isolated fibular fracture. A total of twenty-five patients with SER type-II fracture and SER Type IV-equivalent fractures were enrolled. They found the gravity stress radiograph was equivalent to the manual stress radiograph for determining deltoid ligament injury.
Figure A shows a mortise radiograph displaying a minimally displaced Weber B ankle fracture. Illustration A shows the positioning for a gravity stress radiograph. The patient is in the lateral decubitus position with the injured leg dependent and off the end of the table, a mortise view is taken in 10° of internal rotation of the tibia.
Incorrect Answers:
Question 26
- A 12-year-old Little League pitcher has had pain in the dominant shoulder for the past week that prevents him from pitching. Examination reveals normal strength, full range of motion, normal stability, and mild tenderness about the proximal humerus. Radiographs with comparison views of the opposite shoulder show widening of the proximal humerus physis. Management should include
Explanation
Treatment requires cessation of repetitive physeal stress. There is no long-term sequelae. The athlete can return to same sports in the following season with emphasis on preseason conditioning.
Question 27
The initiating cellular event in development of posttraumatic osteoarthritis is attributed to which of the following?
Explanation
Question 28
A 59-year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Figure 1. Postreduction CT is shown in Figures 2 through 4. What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 29
Figure 11 shows the radiograph of a 2-year-old child with marked genu varum and tibial bowing. Based on these findings, what is the best initial course of action?

Explanation
Question 30
What nerve is most likely to be injured during the anterior exposure of C2-3?
Explanation
REFERENCES: Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-54.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 31
A 20-year-old collegiate pitcher has had a 5-month history of shoulder pain while throwing, decreased velocity, and difficulty with location of his pitches despite multiple attempts at rest. He reports no traumatic event. Examination with his throwing arm abducted at 90 degrees reveals external rotation to 110 degrees and internal rotation to 70 degrees when compared with his nonthrowing shoulder which has external rotation to 95 degrees and internal rotation to 85 degrees. He has a positive O'Brien's sign, positive modified Jobe's relocation test, full rotator cuff strength, no obvious muscular atrophy, and no scapular winging. Radiographs of the affected shoulder show no abnormalities. What is the next most appropriate step in management? Review Topic
Explanation
Question 32
A 13-year-old girl has had increasing left hip pain for the past 4 months. A radiograph, bone scan, MRI scan, and photomicrograph are shown in Figures 1a through 1d. Which of the following immunohistochemistry results would confirm the most likely diagnosis?
Explanation
REFERENCES: Halliday BE, Slagel DD, Elsheikh TE, et al: Diagnostic utility of MIC-2 immunocytochemical staining in the differential diagnosis of small blue cell tumors. Diagn Cytopathol 1998;19:410-416.
Llombart-Bosch A, Navarro S: Immunohistochemical detection of EWS and FLI-1 proteins is Ewing sarcoma and primitive neuroectodermal tumors: Comparative analysis with CD99
(MIC-2) expression. Appl Immunohistochem Mol Morphol 2001;9:255-260.
Question 33
Which group experiences the highest rate of anterior cruciate ligament (ACL) tears?
Explanation
ACL tears are several times more common among women than men. Women who land from jumps in increased valgus and external rotation are at particularly increased risk for ACL tears. Women have smaller notch widths and a smaller ACL cross-sectional area than men, but these factors have not been proven to increase risk for ACL tears.

CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 67
Figure 64 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain.
Question 34
What is the most common behavioral effect of anabolic steroid use in athletes? Review Topic
Explanation
Question 35
-A collegiate offensive football lineman has decreased bench-press strength and shoulder pain as off-season workouts begin. Examination revealed no atrophy, and deltoid and rotator cuff strength testing findings were normal. Translational testing was difficult to achieve because of his large size.Apprehension and relocation test findings were negative. An O’Brien’s active compression test result was negative. Jerk testing was positive on the affected side. Which diagnosis is most likely revealed on an MRI arthrogram?
Explanation
Question 36
You are counseling a 55-year-old woman for a right carpal tunnel release. What can you tell her about the treatment benefit (grip strength and paresthesia relief) 1 year after surgery compared with continued splinting, NSAID use, physical therapy, and a single steroid injection?
Explanation
Gerritsen and associates, Hui and associates, and Jarvik and associates compared the effectiveness of surgical versus nonsurgical treatment for the relief of carpal tunnel symptoms. All three studies showed that surgery was superior for the relief of paresthesias and the improvement of grip strength. According to the American Academy of Orthopaedic Surgeons Clinical Guidelines on the Treatment of Carpal Tunnel Syndrome, strong evidence supports the assertion that surgical treatment of carpal tunnel syndrome should have a greater treatment benefit at 6 and 12 months than splinting, NSAIDs, physical therapy, and a single steroid injection. The other choices, including no change in grip strength and
paresthesias, decrease in grip strength and increase in paresthesias, and increase in grip strength and paresthesias, are not supported by the evidence.
Question 37
An 80-year-old right-hand dominant male presents to clinic with 1 month of left shoulder pain. He has crepitance as well as a positive drop arm test on exam. Radiographs are significant for moderate glenohumeral arthritis and MRI demonstrates Goutallier Stage IV fatty infiltration of the rotator cuff. Which of the following is NOT an appropriate option for treatment of this condition? Review Topic
Explanation
The optimal management of patients with irreparable rotator cuff tears with glenohumeral osteoarthritis is not well defined in literature. Initial management should involve conservative measures, including injection of corticosteroids, physical therapy, activity modification, and NSAIDs, with consideration of operative intervention in those that fail a trial of nonoperative management.
Laudicina et al review the management of irreparable rotator cuff tears in the setting of glenohumeral osteoarthritis(OA). NSAIDs, corticosteroid injection, activity modification, and physical therapy are mainstays of nonoperative treatment. Failure of conservative management may lead to operative intervention. The authors endorse that hemiarthroplasty is currently the procedure of choice for patients with moderate to severe glenohumeral OA and irreparable cuff tears.
Izquierdo et al provide a clinical practice guideline of the treatment of glenohumeral osteoarthritis based on systematic review. Nine of 16 addressed recommendations were inconclusive, illustrating that the management of glenohumeral osteoarthritis remains controversial. The single moderate-rated recommendation was for the use of total shoulder arthroplasty (TSA) rather than hemiarthroplasty. The two recommendations reached by consensus include use of perioperative mechanical and/or chemical DVT prophylaxis for shoulder arthroplasty patients and that TSA should be avoided in patients with glenohumeral OA with irreparable rotator cuff tear.
Illustration A demonstrates the Goutallier staging system of rotator cuff tears.
Incorrect Answers:
Question 38
A skeletally mature 15-year-old girl who was thrown from the car in a rollover accident sustained the injuries shown in Figures 23a through 23d. Examination reveals no neurologic deficit, but the patient has moderate posterior spinal tenderness at the level of the injury. What is the most appropriate treatment?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Question 39
What structure is located at the tip of the arrow in Figure 18? Review Topic

Explanation
Question 40
Decreased risk of shoulder and elbow injury in a throwing athlete has been demonstrated with which of the following? Review Topic
Explanation
Question 41
A 55-year-old man who runs on the weekends reports a 1-year history of continued pain directly posteriorly in the heel. Management consisting of anti-inflammatory drugs, icing techniques, a heel-counter in his shoe split, and physical therapy consisting of stretching, contrast baths, custom orthotics, and iontophoresis has failed to provide relief. Not only is his lifestyle disrupted with respect to running, but he now has pain with normal ambulation with all forms of shoe wear. He is not necessarily concerned with returning to running; he is primarily seeking pain relief. A lateral radiograph and clinical photograph are shown in Figures 32a and 32b. Treatment should now consist of
Explanation
REFERENCES: Clain M, Baxter D: Achilles tendinitis. Foot Ankle 1992;13:482-487.
Schepsis A, Wagner C, Leach R: Surgical management of Achilles tendon overuse injuries: A long-term follow-up study. Am J Sports Med 1994;22:611-619.
Schepsis A, Leach R: Surgical management of Achilles tendinitis. Am J Sports Med 1987;15:308-315.
Keck S, Kelly P: Bursitis of the posterior part of the heel: Evaluation of surgical treatment of eighteen patients. J Bone Joint Surg Am 1965;47:267-273.
Question 42
Figure 61 shows the current radiograph of a 69-year-old woman who fell getting out of bed 10 months ago. At the time of injury she was diagnosed with a nondisplaced humeral surgical neck fracture. After 2 weeks of sling immobilization, physical therapy was started for range of motion. She continues to have pain and is unable to elevate her arm. What is the most likely diagnosis?

Explanation
(SBQ12TR.96) Interleukin-6 levels have been shown to be a reliable measure of which of the following?
Osteoporosis
Severity of injury
Sarcomatous tumor burden
Bone turnover
Hyperparathyroidism
Interleukin-6 (IL-6) is a proinflammatory cytokine that is increased according to the level of injury sustained and acts to activate the host immune system. In addition, new literature exists to indicate its high sensitivity and specificity for detecting infection in total joint arthroplasty.
Overactivation of the immune system and cytokines can lead to systemic inflammatory response syndrome (SIRS), which results in end-organ damage, including small-vessel vascular damage; this would lead to parenchymal cell death from hypoxic insult.
Keel et al. report that immediate and early trauma deaths are determined by brain injuries or significant blood loss, while late mortality is caused by secondary brain injuries and host defense failure. The secondary effects are characterized by local and systemic release of pro-inflammatory cytokines, arachidonic acid metabolites, proteins of the contact phase and coagulation systems, complement factors and acute phase proteins, as well as hormonal mediators.
Pape et al. investigated the effect of surgeries as a "second-hit" phenomenon. They found that surgery on days 2-4 was associated with a greater amount of postoperative organ dysfunction than if the secondary surgery was done on days 5-8. They also found a significant association between IL-6 values above 500pg/dL at the time of surgery and development of multiple organ failure.
Sears et al. review the effect of the inflammatory response to trauma and the development of complications (death, multiple organ failure). They report that IL-6 and the HLA-DR2 molecules currently appear to have the most potential for use in predicting outcomes in trauma patients.
Illustration A is a diagram that shows some of the effects of IL-6 production. Incorrect Answers:
1,3-5: IL-6 levels are not known to be reliably altered by these factors.
Question 43
A 36-year-old woman sustained a tarsometatarsal joint fracture-dislocation in a motor vehicle accident. The patient is treated with open reduction and internal fixation. What is the most common complication?
Explanation
REFERENCES: Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Arntz CT, Veith RG, Hansen ST Jr: Fractures and fracture-dislocations of the tarsometatarsal joint. J Bone Joint Surg Am 1988;70:173-181.
Thompson MC, Mormino MA: Injury to the tarsometatarsal joint complex. J Am Acad Orthop Surg 2003;11:260-267.
Question 44
A 45-year-old man reports a history of a popping sensation and pain in the right shoulder while lifting boxes 6 months ago. The pain has persisted with loss of motion of the shoulder. Radiographs and MRI scans are shown in Figures 47a through 47d. Which of the following studies is likely to produce a significant positive result? Review Topic

Explanation
Question 45
An active 55-year-old man who felt a sudden pop in the left heel while playing tennis 6 months ago was diagnosed with an ankle sprain around the time of injury. He now reports calf atrophy and severe weakness with running. Examination reveals a palpable defect in the Achilles tendon and only trace passive ankle flexion when the calf is squeezed. At the time of surgery, an Achilles tendon defect of 6 cm cannot be approximated. Surgical management of the Achilles tendon should include
Explanation
REFERENCES: Myerson M: Achilles tendon ruptures. Instr Course Lect 1999;48:219-230.
Mandelbaum BR, Myerson MS, Forster R: Achilles tendon ruptures: A new method of repair, early range of motion, and functional rehabilitation. Am J Sports Med 1995;23:392-395.
Question 46
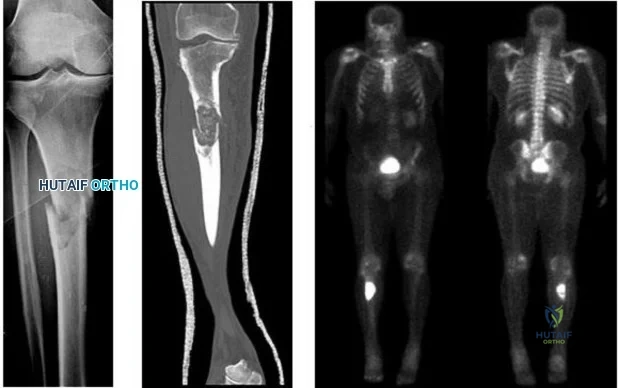
..Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man. While walking, he collapsed and was unable to ambulate because of pain and deformity in his right leg. What is the most appropriate next step?
Explanation
Glomus tumor
Diffuse pigmented villonodular synovitis (PVNS)
Extra-abdominal fibromatosis
Schwannoma
Hemangioma
Please match the characteristics below to the condition listed above.
Question 47
A 30-year-old patient has wrist pain. A radiograph and biopsy specimen are shown in Figures 34a and 34b. What is the most likely diagnosis?
Explanation
REFERENCES: Bieselker JL, Marcove RC, Huvos AG, Mike V: Aneurysmal bone cyst: A Clinico-pathologic study of 66 cases. Cancer 1973;26:615.
Martinez V, Sissons HA: A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291.
Question 48
A college athlete on a scholarship has a medical condition that you feel presents a life-threatening risk to him with participation in athletics. Because of the gravity of this decision and the potential effect it can have on the student/athlete's future, the college asks for your guidance. As the team physician for the college, what is your ethical obligation?
Explanation
Question 49
In patients without spondylolisthesis or scoliosis undergoing laminectomy for lumbar spinal stenosis, spinal fusion is generally recommended if Review Topic
Explanation
Question 50
An 18-year-old football player reports acute pain and swelling after a direct injury to his plantar flexed foot. Examination reveals midfoot swelling and tenderness. Nonstanding radiographs are normal. What is the next most appropriate step in management?
Explanation
to activity.
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries with the transmetatarsal joint. Orthop Clin North Am 2001;32:11-20.
Question 51
50%
Explanation
Enneking et al. conducted both radiographic and histologic studies of sixteen massive retrieved human allografts four to sixty-five months after implantation. Analysis of the articular cartilage revealed no evidence that any chondrocytes had survived, even when the graft had been cryoprotected before it was preserved by freezing.
A 64-year-old woman with a longstanding history of rheumatoid arthritis complains of finger dysfunction for the past 6 months. Figure A displays her hand during active extension of all fingers. Figure B displays her hand maintaining her fingers extended following passive extension. What is the next most appropriate treatment for the ring finger?
Spiral oblique retinacular ligament reconstruction
Sagittal band reconstruction
Lateral band reconstruction
Central slip reconstruction
Triangular ligament and transverse retinacular ligament reconstruction
Sagittal band disruption is often associated with rheumatoid arthritis. When this patient attempts to actively extend the affected digit, the extensor tendon
subluxates ulnarly as a result of the sagittal band rupture, and is left with an extensor lag. If one passively extends the finger fully, the patient is able to maintain this position, as the tendon is intact.
Sagittal band reconstruction can be performed with Watson's technique of creating a distally based tendon graft harvested from the central third of the extensor tendon, passed deep to the intermetacarpal ligament and sutured back to itself. Illustration A depicts an intraoperative view of the tendon before reconstruction and Illustration B displays tendon following sagittal band reconstruction. Illustration C displays all of the anatomic locations
of the options listed above.
A splenectomy is performed in a 7-year-old boy following a motor vehicle accident. All of the following are recommended for long-term management EXCEPT:
Pneumococcal vaccination
Haemophilus influenza type B vaccination
Meningococcal group C vaccination
Lifelong prophylactic antibiotics
Hepatitis A vaccination
All of the responses are correct except the need for Hepatitis A vaccine. Hepatitis A is a virus with tropism for hepatocytes which causes infection from fecal-oral contaminated food/water, and shows no increased rate of either infectivity or morbidity in patients with hyposplenism.
Basic recommendations for splenectomized patients include:
All splenectomized patients and those with functional hyposplenism should receive pneumococcal immunization.
Patients not previously immunized should receive haemophilus influenza type B vaccine.
Patients not previously immunized should receive meningococcal group C conjugate vaccine.
Influenza immunization should be given.
Lifelong prophylactic antibiotics are still recommended (oral phenoxymethylpenicillin or erythromycin). This is seemingly despite lack of good data demonstrating a role for lifelong chemoprophylaxis and the acknowledgement that long-term compliance may be problematic.
Davies et al review the current level of evidence supporting these guidelines
for infection prevention in patients with hyposplenism. New to these guidelines are issues regarding occupational exposure and the use of the meningococcal group C and the seven-valent pneumococcal vaccine in non-immunized hyposplenic patients.
Gandhi et al evaluated their nonoperative management of blunt splenic injury in pediatric trauma care. They found compared to historical controls, children with blunt splenic injuries who were hemodynamically stable could be safely monitored with a protocol which required 4 days of inpatient care, 3 weeks of quiet home activities, and 3 months of light activity. This protocol seems to allow for safe return to unrestricted activity.
Incorrect Answer:
Ligaments attach to bone by both direct insertion and indirect insertion. Which of the following most accurately describes the order of the four transition zones of direct insertion?
Ligament > fibrocartilage > mineralized fibrocartilage > bone
Ligament > mineralized fibrocartilage > fibrocartilage > bone
Ligament > mineralized fibrocartilage > periosteum > bone
Ligament > Sharpey's fiber > periosteum > bone
Ligament > periosteum > fibrocartilage > bone
There are two types of tendon/ligament insertion into bone: direct and indirect insertion. The more common, indirect insertion, occurs when the superficial ligament fibers insert into the periosteum. Direct insertion of tendon/ligaments
into bone occurs through a transition of 4 distinct phases: 1) ligament, 2) fibrocartilage, 3) mineralized fibrocartilage, and 4) bone.
While flexing the elbow to perform a biceps curl, what type of muscle contraction is occuring?
Isometric
Isokinetic
Plyometric
Eccentric
Concentric
Concentric muscle contractions occur when a muscle shortens during contraction, as in the upward motion when performing a biceps curl. An eccentric contraction occurs when a muscle lengthens with contraction, as in the "negative" or lowering motion of a biceps curl. An example of an isometric (muscle contracts while maintaining constant length) contraction would be pushing against an immovable object. An example of an isokinetic (muscle has constant speed of contraction) occurs with specialized equipment like Cybex machines. Plyometric contractions occur when a muscle rapidly lengthens just prior to contraction - like during repetitive box jumping.
Woo and Buckwalter describe the mechanisms, barriers, and molecular processes involved in ligament and tendon injury and repair.
A 34-year-old laborer has her left foot crushed in a piece of farming equipment as shown in Figure A. All of the following are reasons for a poor outcome following a crush injury to the foot EXCEPT:
Workers compensation injury
Development of reflex sympathetic dystrophy (complex regional pain syndrome)
Delayed soft-tissue coverage in mangled extremities
Immediate skeletal stabilization
Ongoing litigation
This patient has a mangled extremity. Rigid skeletal stabilization is recommended to enhance soft-tissue healing.
Level 4 evidence from Myerson et al found that delayed soft-tissue coverage in mangled extremities correlated with poor outcome. Poor results also occurred
if treatment was not immediately initiated (immediate debridement shown in Illustration A), if patients subsequently had neuritis or reflex sympathetic dystrophy, or if patients were involved in ongoing workers' compensation and litigation. Neuroischemia following substantial soft-tissue injury likely plays a role in the development of chronic pain after crush injuries to the foot, either through direct trauma to the peripheral nerves or by intraneural or extraneural fibrosis. This trauma to the nerve may cause chronic neuritis, which then triggers a sympathetically mediated reflex sympathetic dystrophy (complex regional pain syndrome).
A 65-year-old man undergoes total knee replacement and is found to have deep vein thrombosis two days later. What molecule is
thought to be involved in this process when it is released during surgical dissection?
Prothrombin
RANKL
IL-1b
Thromboplastin
Factor XI Corrent answer: 4
Thromboplastin is also known more commonly as Tissue Factor (TF), which is involved in the Extrinsic Pathology of the coagulation cascade.
During surgical dissection, insults occur to the endothelial walls of blood vessels. There are three ways in which the body reacts to form a clot so that the patient does not bleed excessively. One is via vessel contraction, another is by collagen release, and a third is by tissue thromboplastin release. Thromboplastin release is part of the extrinsic coagulation pathway (see
Illustration A). Thromboplastin release activates Factor VII which activates Factor X which converts prothrombin to thrombin. Thrombin is the catalyst for converting fibrinogen to fibrin which induces clot formation. While this is useful for decreasing bleeding, it is the same mechanism by which a deep venous thrombosis (DVT) develops.
Which of the following materials has a Young's modulus of elasticity that is most similar to cortical bone
Titanium
Zirconia
Stainless steel
Ceramic (Al2O3)
Alloy (Co-Cr-Mo)
Of the materials listed Titanium has an elastic moduli closest to cortical bone. Titanium is extra-ordinarily light, strong, highly ductile, and corrosion resistant. Titanium is however very notch sensitive and has poor wear resistance.
Young Modulus of Elasticity is defined as the stiffness (ability to maintain
shape under external loading) of a material. On the stress vs. strain curve it is defined as the slope of the line in the elastic zone (see Illustration A). Young’s modulus is constant and different for each material. The relevant moduli (unit GPa) are approximated below:
Question 52
A 32-year-old patient reports progressively increasing pain and stiffness after undergoing arthroscopic shoulder stabilization 1 year ago. The stabilization procedure was a Bankart repair with anchor fixation and supplemented with the heat probe. Radiographs are shown in Figures 45a and 45b. What is the most likely diagnosis?
Explanation
REFERENCES: Levine WN, Clark AM Jr, D’Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
Petty DH, Jazrawi LM, Estrada LS, et al: Glenohumeral chondrolysis after shoulder arthroscopy: Case reports and review of the literature. Am J Sports Med 2004;32:509-515.
Question 53
Which of the following factors is most critical to the success of a meniscal allograft transplantation?
Explanation
cryopreservation of the graft to ensure cell viability is not necessary. There is a limited immune response to musculoskeletal allografts; therefore, immunosuppression, as is required for visceral organ transplantation, is not indicated.
Question 54
03 A 64 year old man who underwent revision total knee arthroplasty 6 months ago has leg pain after walking. AP and lateral radiographs are shown in Figures 39a and 39b. The cause of pain is most likely related to

Explanation
back to this question next question
Question 55
A B C Figures 63a through 63c are the radiographs of a 19-year-old woman who sustained injuries in a motorcycle collision. Which initial treatment will result in the best functional outcome and lowest pain scores at 2 years?

Explanation
Ligamentous injuries to the tarsometatarsal and intermetatarsal joints are commonly a result of high-energy mechanisms. These injuries have resulted in worse outcomes following ORIF than Lisfranc injuries, which involve fractures. Multiple injury patterns may occur, with some injuries involving mostly the ligamentous structures. Ligamentous Lisfranc injuries treated with primary arthrodesis have been shown to result in improved American Orthopaedic Foot & Ankle Society scores and lower Visual Analog Scale pain scores at 2-year follow-up than injuries treated with ORIF. ORIF with either plate or screw fixation has resulted in higher rates of secondary surgeries and lower functional scores. Nonsurgical management is not recommended for displaced injuries. Cast placement is recommended for patients with midfoot sprains with displacement of less than 2 mm. Nonanatomic reductions have been associated with poor results. Closed reduction and percutaneous pinning is unlikely to achieve an anatomic reduction and stable fixation.
RECOMMENDED READINGS
Henning JA, Jones CB, Sietsema DL, Bohay DR, Anderson JG. Open reduction internal fixation versus primary arthrodesis for lisfranc injuries: a prospective randomized study. Foot Ankle Int. 2009 Oct;30(10):913-22. doi: 10.3113/FAI.2009.0913. PubMed PMID: 19796583.View
Abstract at PubMed
Ly TV, Coetzee JC. Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation. A prospective, randomized study. J Bone Joint Surg Am. 2006 Mar;88(3):514-20. PubMed PMID: 16510816. View Abstract at PubMed
Kuo RS, Tejwani NC, Digiovanni CW, Holt SK, Benirschke SK, Hansen ST Jr, Sangeorzan BJ. Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am. 2000 Nov;82-A(11):1609-18. PubMed PMID: 11097452. View Abstract at PubMed Nunley JA, Vertullo CJ. Classification, investigation, and management of midfoot sprains: Lisfranc injuries in the athlete. Am J Sports Med. 2002 Nov-Dec;30(6):871-8. PubMed PMID: 12435655. View Abstract at PubMed
Question 56
Figures 15a through 15c show the radiographs of a 23-year-old football player who was injured when another player fell on his flexed and planted foot. He reports severe pain in the midfoot with a feeling of numbness on the dorsum of the foot, and he is unable to bear weight on the limb. Examination reveals mild swelling. Management should consist of
Explanation
REFERENCES: Baxter DE: The Foot and Ankle in Sport, ed 1. St Louis, MO, Mosby, 1995,
pp 107-123.
Curtis MJ, Myerson M, Szura B: Tarsometatarsal joint injuries in the athlete. Am J Sports Med 1993;21:497-502.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Thompson MC, Mormino MA: Injury to the tarsometatarsal joint complex. J Am Acad Orthop Surg 2003;11:260-267.
Question 57
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?
Explanation
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Ciccotti MG, Jobe FW: Medial collateral ligament instability and ulnar neuritis in the athlete’s elbow. Instr Course Lect 1999;48:383-391.
Question 58
- A 40-year-old woman has had pain in the metatarsophal joint of the second toe for the past 6 months despite nonsurgical treatment. A dorsalplantar stress test reproduces the pain, and there is 10 mm of dorsal subluxation of the toe. Radiographs show a normal second metatarsophalangeal joint. Surgical treatment should consist of synovectomy and
Explanation
Question 59
A 47-year-old man comes for evaluation of his dominant right elbow, which has been bothering him with activity for the past 3 months, especially with activities requiring wrist extension. He is an active squash player and has been unable to continue this sport. Examination shows tenderness at the common extensor origin. What is the next best step? Review Topic
Explanation
Lateral epicondylitis is a common problem with numerous non-operative treatments available. There is little scientific evidence to support any of these treatments however and the quality of most reports is low and their conclusions limited by bias and/or study design. Tennis elbow often resolves with time regardless of which conservative treatment is chosen.
Coombes et al. randomized patients with unilateral tennis elbow to receive either (1) corticosteroid injection, (2) placebo injection, (3) corticosteroid injection plus physical therapy or (4) placebo injection plus physical therapy. They found that
corticosteroid resulted in worse clinical outcome and recurrence rate compared to placebo injection. Use of physical therapy did not produce any significant differences.
Dines et al. review the diagnosis and of tennis injuries, including lateral epicondylitis. Although they acknowledge that there is "no long term benefit with regard to tendon healing," they note that steroid injection may be useful to control acute symptoms.
Boyer et al. review the myths surrounding lateral epicondylitis. They note that despite widespread use, corticosteroid injection has repeatedly been shown to have no long term benefit. They conclude based on their review of the literature that if there is any benefit to steroid injection, it is of short duration, and in patients whose symptoms have been of short duration, without any previous treatment.
Incorrect answers:
Question 60
A 40-year-old woman who is an avid tennis player reports the insidious onset of progressive left shoulder pain for the past 2 months. Examination reveals full range of motion with a positive impingement sign. Strength in the supraspinatus and infraspinatus muscles is normal, although stress testing is painful. An earlier subacromial cortisone injection provided good, but only temporary relief. An AP radiograph of the left shoulder is shown in Figure 10. Management should now consist of
Explanation
REFERENCES: Jerosch J, Strauss JM, Schmiel S: Arthroscopic treatment of calcific tendinitis of the shoulder. J Shoulder Elbow Surg 1998;7:30-37.
Ark JW, Flock TJ, Flatow EL, Bigliani LU: Arthroscopic treatment of calcific tendinitis of the shoulder. Arthroscopy 1992;8:183-188.
Question 61
below depict the radiographs obtained from a year-old woman with a painful total knee arthroplasty. She describes an uneventful recovery with no wound-healing issues and was pain free for the first 10 years. Although reporting no trauma or inciting event, she now describes pain in the entire knee that is most severe with her first few steps. She has begun to notice night pain and, more recently, constant swelling. What is the most appropriate work-up at this time?
Explanation
An evaluation of the painful total knee must be supported by an understanding of the potential etiologies of pain. They may include, aseptic loosening, infection, osteolysis, gap imbalance, referred pain, stiffness, and complex regional pain syndrome. In this case, the patient demonstrates start-up pain and had no prior history of infections. Her radiographs show subsidence of the tibia, indicating a loose prosthesis. Knowing that the prosthesis is already loose precludes the need for a bone scan. It is, however, important to rule out infection in this case; therefore, CRP and ESR testing is essential. Aspiration is also recommended when going into knee arthroplasty, and infection is a concern.
Question 62
A 40-year-old man with an acetabular chondrosarcoma has a small soft-tissue mass. Treatment should consist of
Explanation
REFERENCES: Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 63
03

Explanation

The Essex-Lopresti reduction technique is a useful method for the treatment of tongue type calcaneal fractures. With this technique, a steinman pin is inserted percutaneously into the posterior facet fragment. This pin is then used to disimpact the fragment and reduce the fracture.
Question 64
You are studying a single continuous variable after administration of a defined treatment intervention. Your statistician informs you the data are not normally distributed. What is the best test to analyze the data?
Explanation
Question 65
A 67-year-old retired steelworker was involved in a motor vehicle accident and sustained a midcervical spinal cord injury. Radiographs and MRI scans reveal severe cervical stenosis and spondylosis without fractures or dislocations. Neurologic examination reveals an ASIA C spinal cord impairment with greater motor involvement of the upper extremities than the lower extremities. What is the probability that the patient eventually will become ambulatory?
Explanation
(ASIA C and D) ultimately walked. The poorest prognosis, however, was in ASIA C patients older than age 50, in which only 40% walked.
REFERENCES: Penrod LE, Hegde SK, Ditunno JF Jr: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Northrup BE: Acute injuries to the spine and spinal cord: Evaluation and early treatment, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, p 735.
Question 66
- Figure 16 shoes the AP radiograph of a 32-year-old man with a fracture cephalad to the fovea of the femoral head. A CT scan shows a single head fragment. After closed reduction of the hip, there is 5 mm of residual articular incongruity. Management should now include
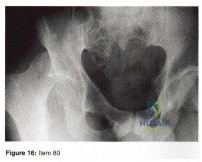
Explanation
Question 67
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal. Radiographs confirm a 2-cm discrepancy in the lengths of the lower extremities. Additional imaging studies should include
Explanation
REFERENCES: DeBaun MR, Tucker MA: Risk of cancer during the first four years of life in children from The Beckwith-Wiedemann Syndrome Registry. J Pediatr 1998;132:398-400.
Ballock RT, Wiesner GL, Myers MT, et al: Hemihypertrophy concepts and controversies.
J Bone Joint Surg Am 1997;79:1731-1738.
Carpenter CT, Lester EL: Skeletal age determination in young children: Analysis of three regions of the hand/wrist film. J Pediatr Orthop 1993;13:76-79.
Question 68
Which of the following nutraceuticals has been associated with perioperative bleeding?
Explanation
REFERENCES: Rowin J, Lewis SL: Spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Neurology 1996;46:1775-1776.
Vale S: Subarachnoid hemorrhage associated with ginkgo biloba. Lancet 1998;352:36.
Bebbington A, Kulkarni R, Roberts P: Ginkgo biloba: Persistent bleeding after total hip arthroplasty caused by herbal self-medication. J Arthroplasty 2005;20:125-126.
Question 69
A right-handed 24-year-old woman underwent an arthroscopic Bankart repair for recurrent anterior dislocations 9 months ago. Despite extensive physical therapy for 8 months, the patient has very limited range of motion (elevation to 130 degrees and external rotation to 10 degrees with the arm at the side). Shoulder radiographs are normal. The next step in management should consist of
Explanation
REFERENCES: Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
Question 70
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should
Explanation
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
Question 71
A 26-year-old right hand-dominant man has had right shoulder pain for the past 6 months. History reveals that he was the starting pitcher for his high school team. Activity modification, physical therapy, cortisone injection, and anti-inflammatory drugs have failed to improve his symptoms. He has a positive O’Brien’s active compression test. What is the next most appropriate step in the diagnosis of this patient?
Explanation
REFERENCES: Applegate GR, Hewitt M, Snyder SJ, et al: Chronic labral tears: Value of magnetic resonance arthrography in evaluating the glenoid labrum and labral-bicipital complex. Arthroscopy 2004;20:959-963.
Bencardino JT, Beltran J, Rosenberg ZS, et al: Superior labrum anterior-posterior lesions: Diagnosis with MR arthrography of the shoulder. Radiology 2000;214:267-271.
Nam EK, Snyder SJ: The diagnosis and treatment of superior labrum, anterior and posterior (SLAP) lesions. Am J Sports Med 2003;31:798-810.
Question 72
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
Explanation
REFERENCES: Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265.
Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 175-180.
Question 73
When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more than the extension space?
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point,
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 74
Which component is most common to both simple and complex elbow dislocations?

Explanation
Question 75
What type of muscle contraction occurs while the muscle is lengthening?
Explanation
REFERENCES: Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000,
pp 12-13.
Lieber RL: Form and function of skeletal muscle, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 76
A hip compression screw is placed in a test jig and a bending load is applied to the tip of the screw. After the load is released, the screw returns completely to its original shape. What is this type of deformation called?
Explanation
Question 77
Figure 26 shows the radiograph of a 48-year-old woman who has right arm pain and hematuria. A bone scan reveals increased uptake in the left ribs and thoracic spine. A needle biopsy specimen shows that the lesion is highly keratin positive and composed primarily of clear cells. What is the best course of action?
Explanation
REFERENCES: Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1054.
Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Katzner M, Schvingt E: Operative treatment of bone metastases secondary to renal carcinoma: Basic research and treatment of renal cell carcinoma metastasis. Prog Clin Biol Res EORTC 1990;348:151-168.
Question 78
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
Question 79
A 21-year-old man has had right groin pain for the past year. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 50a through 50e. What is the most likely diagnosis?
Explanation
REFERENCES: Terek RM: Recent advances in the basic science of chondrosarcoma. Orthop Clin North Am 2006;37:9-14.
Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530.
Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 80
Examination of a 12-year-old girl with a painful flatfoot deformity reveals tenderness in the region of the sinus tarsi and no appreciable subtalar motion. Radiographs are shown in Figures 48a through 48c. Two attempts to relieve her symptoms by cast immobilization fail to relieve the pain. Management should now consist of
Explanation
REFERENCES: Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interpostion of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 211-218.
Question 81
Initial management should consist of Review Topic

Explanation
Question 82
A 54-year-old laborer has a 6-month history of lateral elbow pain. An elbow examination reveals full range of motion, tenderness over the lateral epicondyle, and pain with resisted wrist extension with the elbow in extension. Elbow radiograph findings are normal. You perform a steroid injection and the patient's symptoms are decreased 6 weeks later. One year after receiving the injection, this patient—when compared to a patient who did not have a steroid injection—is likely to
Explanation
This patient has signs and symptoms of lateral epicondylitis. Treatments include various forms of physical therapy, iontophoresis, corticosteroid injection, nitroglycerin patch treatment, blood injections, prolotherapy, and surgical intervention. No single treatment is superior to other treatments for this common problem. Several studies have demonstrated a short-term decrease in symptoms following steroid injection (6 weeks) but an increased likelihood of persistent symptoms 1 year after treatment. Steroid injection at this site has not been associated with increased risk for tendon rupture or need for surgical intervention.
Question 83
What factor highly correlates with poor outcomes after surgery for femoroacetabular impingement? Review Topic
Explanation
Question 84
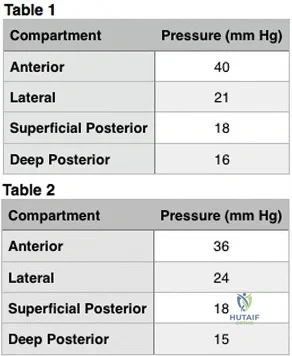
15% to 2.5%. Acute Charcot arthropathy almost always appears with signs of inflammation. Profound unilateral swelling, an increase in local skin temperature (generally, an increase of 3° to 7° above the nonaffected foot's skin temperature), erythema, joint effusion, and bone resorption in an insensate foot are present. These characteristics, in the presence of intact skin and a loss of protective sensation, are often pathognomonic of acute Charcot arthropathy. Cellulitis is an infection of the skin. Examination would reveal erythema, edema, and pain. Osteomyelitis is an infection of the bone. Examination may reveal edema, drainage, and pain.
Explanation
Which of the following clinical scenarios represents the strongest indication for locked plating technique in a 70-year-old woman?
Segmentally comminuted ulnar fracture
Simple diaphyseal fracture of the humerus
Transverse midshaft displaced clavicle fracture
Periprosthetic femur fracture distal to a well-fixed total hip arthroplasty
Schatzker 2 fracture of the tibia with severe joint depression and comminution
Locking screw fixation is a relatively new option in the armamentarium of orthopaedic surgeons treating fractures. The understanding of the biomechanics, implications to healing, and optimal indications and surgical techniques is still in evolution. A periprosthetic proximal femur fracture with a stable prosthesis is best treated with open reduction and internal fixation with locking proximal fixation with or without cerclage cables. Diaphyseal fractures treated with compression plating or bridge plating can be treated well with conventional implants unless osteoporosis is severe. An AO/OTA B-type partial articular fracture is also better suited to standard buttress plating with periarticular rafting lag screws. Locking fixation is not always required for a transverse displaced midshaft clavicle fracture.
What is the post-amplification product of reverse transcription polymerase chain reaction (RT-PCR)?
RNA
DNA
Protein
Mitochondria
Immunoglobulins
Reverse transcription polymerase chain reaction (RT-PCR) is a variant of polymerase chain reaction (PCR) used in molecular biology to generate many copies of a DNA sequence from fragments of RNA. The RNA strand is first reverse transcribed into its DNA complement, followed by amplification of the resulting DNA using polymerase chain reaction. Polymerase chain reaction amplifies short segments of DNA by using the temperature stable DNA polymerase enzyme.
A 63-year-old woman falls from standing and lands on her right hand. She complains of deformity and wrist pain. Radiographs are provided in Figure A. Following closed reduction, the patient inquires whether she has osteoporosis and if she is likely to have another fracture. In counselling the patient, which of the following is the strongest predictor for a future fracture from low energy trauma?
Bone mineral density T-score < -2.5
Low vitamin D levels
Family history of osteoporosis
History of a prior fragility fracture
Ten year history of oral prednisone use
Each of the answer choices is a risk factor for subsequent fragility fracture, but patient history of a prior fragility fracture is the strongest predictor.
Bouxsein et al reviews the proper care, diagnosis, and prevention of fragility fractures. History of a fragility fracture is the greatest predictor of a future fracture from low energy trauma. Appropriate care includes not only treatment of the fracture itself, but also proper evaluation to identify the etiology of the fracture and appropriate intervention to rectify the underlying pathology. Evaluation includes bone densitometry, lab testing of Vitamin D and calcium.
A T-score compares your bone density to the optimal peak bone density for your gender. It is reported as number of standard deviations below the average. A T-score of -1 to -2.5 is considered osteopenia, and a risk for developing osteoporosis. A T- score of less than -2.5 is diagnostic of osteoporosis.
Long-term alendronate (Fosamax) use for osteoporosis has been associated
with which of the following?
Scurvy
Detached retina
Uterine carcinoma
Osteonecrosis of the femoral head
Diaphyseal femoral insufficiency fractures
Alendronate is a bisphosphonate that inhibits the ruffled border of the osteoclast. When used long term, this class of medication prevents the normal bone remodeling process. Long-term use has recently been shown to be associated with insufficiency fractures of the femur. Osteonecrosis of the jaw has been described but not in other anatomic locations. Scurvy occurs because of a lack of vitamin C and use of bisphosphonates is not associated with
uterine cancer or a detached retina.
Implants composed of polylactic acid are excreted by what system after they are absorbed?
Hepatic
Renal
Respiratory
Gastrointestinal
Polylactic acid suture and suture anchors are popular bioabsorbable orthopaedic implants. This material undergoes hydrolysis of the ester background in vivo. Resulting lactic acid enters the tricarboxylic acid (Krebs)
cycle and is excreted as carbon dioxide by the lungs. Polyglycolic acid and poly(p- dioxanone) may also be excreted by the kidneys.
A patient sustains a grade III medial collateral ligament injury. One year later, when compared to collagen in an uninjured ligament, an increase is likely in the
gross number of fibers.
proportion of type III fibers.
cross-linking.
mass and diameter of fibers.
Studies on animal models have shown that there is a change in collagen fiber type and distribution early in the healing process. There is a higher portion of type III fibers than in
normal ligament initially, but this ratio returns to normal about 1 year after the injury occurs. Healing ligaments show an increased number of collagen fibers, but the number of mature collagen cross-links is
45% of predicted value after 1 year. There is also a decrease in the mass and diameter of the collagen fibers.
Sclerostin and dickkopf-1 (Dkk-1) are direct inhibitors of what pathway related to bone and/or cartilage regulation?
Bone morphogenetic protein (BMP)/SMAD pathway
Receptor activator of nuclear factor kappa beta (RANK)/RANK ligand (RANKL) pathway
Wnt/Beta-catenin (ß-catenin) pathway
Parathyroid hormone (PTH) pathway
Dkk-1 and sclerostin are proteins that inhibit the binding of the Wnt molecule to receptors LRP5/6. In the absence of sclerostin and Dkk-1, Wnt binds to its receptor, which in turn inhibits phosphorylation of the ß-catenin. The unphosphorylated ß-catenin then builds up in the cytoplasm of the cell, allowing it to be transported to the nucleus of the cell. Once in the nucleus, ß- catenin will lead to upregulation of a series of proteins involved in osteoblast formation differentiation. Knocking out or inhibiting sclerostin or Dkk-1 results in increased bone mass secondary to constitutive activation of the Wnt/ß- catenin pathway. The other responses are not directly affected by Dkk-1 or sclerostin. RANKL and RANK are expressed on osteoblasts and osteoclasts, respectively, and are involved in osteoblast-mediated osteoclast activation. BMPs work through SMADs to cause osteoblastic differentiation, and there is reported crosstalk between the Wnt and BMP pathways (but this is an indirect link). Finally, PTH at physiologic levels binds to osteoblasts, causing a series of events that lead to osteoblast-mediated osteoclast activation and subsequent increased bone resorption.
During endochondral ossification of the growth plate, the process that most contributes to the longitudinal growth of long bones is
chondrocyte apoptosis.
chondrocyte hypertrophy.
chondrocyte proliferation.
growth plate matrix synthesis.
The growth plate is divided into 5 distinct zones: reserve, proliferative, maturation, hypertrophy, and vascular invasion. During growth-plate chondrocyte hypertrophy, intracellular volume and an increase in chondrocyte height are responsible for most growth of long bones. Other factors that contribute to bone growth are chondrocyte proliferation and matrix synthesis, but to a lesser degree than chondrocyte hypertrophy. Growth plate chondrocytes undergo programmed cell death (apoptosis) after hypertrophy
takes place.
Bacterial resistance to tetracycline is confirmed by ribosome protection, tetracycline modification, and
altered RNA polymerase.
altered membrane binding protein.
increased drug efflux.
DNA gyrase mutation.
Mutations of bacterial DNA gyrase can decrease the effectiveness of quinolones. Altered membrane-binding protein is observed with resistance to ?
-lactam antibiotics. Tetracyclines are antibiotics that inhibit bacterial growth by stopping protein synthesis. Three specific mechanisms of tetracycline
resistance have been identified: increased tetracycline efflux, ribosome protection, and tetracycline modification. Alteration of RNA polymerase is found in resistance to rifampin.
A 14-year-old boy has failed physical therapy management for Scheuermann kyphosis, and an extension thoracolumbosacral orthosis brace is recommended. The boy and his parents are told that the brace will force his thoracic spine into normal sagittal alignment and put the anterior vertebral bodies of the thoracic segment into tension, which will induce bone growth and normalization of wedge- shaped
vertebrae. What name is associated with this process?
Hooke's law
Kirchhoff's law
Wolff's law
Heuter-Volkmann principle
The Heuter-Volkmann principle shows that bone placed in longitudinal tension will tend to stimulate longitudinal growth, and that compressive longitudinal forces inhibit longitudinal growth, making this response the best choice. Hooke's law relates to stress being proportional to strain and is not directly related to bone growth. Kirchhoff's laws apply to electrical circuit design. Wolff's law states that bone remodels in response to mechanical stress, with the correlate that increased stress causes increased growth, and decreased stress leads to bone loss.
A tendon repair is thought to be weakest during which phase of tendon healing?
Inflammatory
Proliferation
Maturation
Remodeling
Healing after a tendon repair or rupture has the following stages: inflammatory, cellular proliferation, and remodeling. During the inflammatory phase, neutrophils and macrophages migrate into the injury site and release chemotactic factors that recruit fibroblasts. A tendon is thought to be weakest
5 to 21 days after repair, which coincides with the inflammatory phase. During the proliferative phase, inflammatory cells secrete cytokines and growth
factors (platelet-derived growth factor, insulin-like growth factor, bone morphogenetic protein (BMP)-12 and BMP 13, and transforming growth factor- beta) that promote differentiation of fibroblasts. Fibrosis and decreased cellularity are the hallmarks of the remodeling stage.
A 4-year-old boy has bilateral genu varum and is in the fifth percentile for height for his age. A younger sister has less severe genu varum. Radiographs reveal physeal cupping and widening on both the distal femur and proximal tibia. Laboratory studies show sodium 145 mEq/L (reference range, 136-142 mEq/L), potassium 4.0 mEq/L (reference range, 3.5-5.0 mEq/L), calcium 9.0 mg/dL (reference range, 8.2-10.2 mg/dL), phosphorous 2 mg/dL (reference range, 4-
Question 85
An otherwise healthy adolescent girl was treated for left slipped capital femoral epiphysis. The contralateral hip had not slipped, but was stabilized prophylactically with a single cannulated screw. The implants were removed after 1 year. The pelvic radiographs (Figures 215a and 215b) and the MRI scans of the hip that had not originally slipped (Figures 215c through 215e) were obtained 10 months after screw removal (22 months after the original fixation). Which findings are shown in these studies?
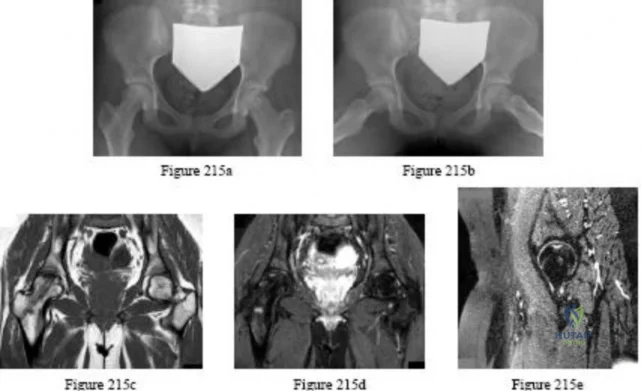
Explanation
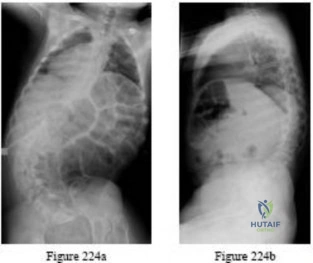
Question 86
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals no other injuries. Radiographs are shown in Figures 35a and 35b. Initial management of this fracture should consist of
Explanation
REFERENCES: Meyers MH, McKeever FM: Fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60
Janarv PM, Westblad P, Johansson C, Hirsch G: Long-term follow-up of anterior tibial spine fractures in children. J Pediatr Orthop 1995;15:63-68.
Kuhn JE, Sailer MJ, Sterett WI, Hawkins RJ: Arthroscopic technique for the treatment of tibial spine fractures in the skeletally immature patient. J Ortho Tech 1995;3:7-12.
Question 87
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?
Explanation
REFERENCES: Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 88
A 34-year-old man sustained a gunshot wound to the knee 18 months ago and was treated with bullet removal and a 10 day course of oral antibiotics. He now complains of 12 months duration of pain in the thigh and recent ulceration and drainage of the skin near the site of his gunshot wound. Physical exam is notable for a draining sinus tract, erythema and tenderness of the mid-thigh. He is afebrile. An MRI image of this patient is shown in Figure A. Which of the following is the most appropriate management?

Explanation
In the referenced article by Parsons and Strauss, the management of chronic osteomyelitis is reviewed.
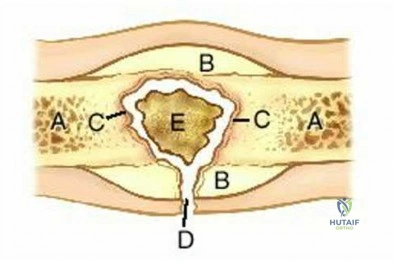
OrthoCash 2020
Question 89
When performing a revision total knee arthroplasty, trial components are inserted and the knee is stable in extension and loose in flexion. Which step should be taken to create a stable construct?
Explanation
The surgeon is facing a common scenario that occurs in revision knee surgery: a loose flexion gap with an appropriate extension gap. A flexion gap can be tightened by translating the femoral component more posteriorly and using an oversized femoral component. Insertion of a thicker tibial component changes both the flexion and extension gap. Augmentation of the distal femur tightens only the extension gap. A constrained insert would only be indicated if oversizing of the femoral component did not adequately tension the flexion gap.
Question 90
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms? Review Topic
Explanation
Question 91
What clinical finding is associated with the least favorable prognosis in an adolescent patient who has been diagnosed with a high-grade osteosarcoma of the distal femur?
Explanation
REFERENCE: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlation. Philadelphia, PA, Lea and Febiger, 1989, pp 344-350.
Question 92
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should consist of
Explanation
REFERENCES: Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Schepsis AA, Grafe MW, Jones HP, Lemos MJ: Rupture of the pectoralis major muscle: Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
Question 93
Nutritional rickets in the US occurs more frequently in infants older than 6 months of age who do not receive vitamin D supplementation and are Review Topic
Explanation
Question 94
The posterior cord of the brachial plexus terminates into what two main branches?
Explanation
REFERENCE: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 228-236.
Question 95
-A 16-year-old girl was seen after a motor vehicle collision. Imaging studies including plain radiographs,MRI scans, and CT scans confirm bilateral jumped facets at C5-6 without disk herniation. She is alert,oriented, and neurologically intact. What is the most appropriate next step?
Explanation
Question 96
Closed chain kinetic exercises are differentiated from open chain exercises by which of the following? Review Topic
Explanation
Question 97
A 32-year-old man sustains a forceful inversion injury while playing soccer. Examination reveals tenderness in the lateral hindfoot and midfoot region with associated ecchymosis and swelling. Radiographs show proximal migration of the os peroneum. Active eversion is still present. These findings indicate disruption of the
Explanation
REFERENCES: Thompson FM, Patterson AH: Rupture of the peroneus longus tendon: Report of three cases. J Bone Joint Surg Am 1989;71:293-295.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
Question 98
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient’s symptoms at this time?
Explanation
REFERENCES: Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
Mundy GR: Hypercalcemia of malignancy revisited. J Clin Invest 1988;82:1-6.
Question 99
03 A 35 year old man sustains a dislocation of his dominant shoulder in a fall. The shoulder is reduced and placed in a sling, but returns 6 hours later with shoulder dislocated again, despite use of a sling. A CT scan is shown in figure 36. Management should now consist of
Explanation
back to this question go to explanation
Question 100
Which of the following is the strongest contraindication to unicompartmental knee arthroplasty (UKA)?
Explanation
REFERENCES: Lotke PA (ed): Knee Arthroplasty: Master Techniques in Orthopaedic Surgery. New York, NY, Raven Press, 1995, pp 275-293.
Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 805-814.
Tabor OB Jr, Tabor OB: Unicompartmental arthroplasty: A long-term follow-up study.
J Arthroplasty 1998;13:373-379.
