Orthopedic MCQ Exam: Arthroplasty, Elbow, Foot, Fracture, Hip | Part 263
Key Takeaway
This page offers Part 263 of a comprehensive Orthopedic Surgery Board Review. It features 100 verified, high-yield MCQs tailored to OITE and AAOS exam formats. Designed for orthopedic residents and surgeons, it provides essential practice with detailed explanations to achieve board certification.
About This Board Review Set
This is Part 263 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 263
This module focuses heavily on: Arthroplasty, Elbow, Foot, Fracture, Hip.
Sample Questions from This Set
Sample Question 1: Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgica...
Sample Question 2: A 5-year-old boy has had pain in the right foot for the past month. Examination reveals tenderness and mild swelling in the region of the tarsal navicular. Radiographs are shown in Figure 30. Management should consist of...
Sample Question 3: Which of the following clinical tests is used to diagnose medial instability of the elbow? Review Topic...
Sample Question 4: A 23-year-old man is injured in a motorcycle accident and has a Glasgow Coma Scale (GCS) score of 10. His fiance arrives shortly after he does. He has an open, IIIc tibial fracture. The patient's parents are on the way but are not expected ...
Sample Question 5: A 72-year-old patient fell 3 weeks after undergoing a total hip arthroplasty using cementless fixation ofthe femoral component. She sustained a comminuted Vancouver type B-2 fracture with displacement of the calcar fragment. What is the bes...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 2
A 5-year-old boy has had pain in the right foot for the past month. Examination reveals tenderness and mild swelling in the region of the tarsal navicular. Radiographs are shown in Figure 30. Management should consist of
Explanation
REFERENCES: Karp M: Kohler’s disease of the tarsal scaphoid. J Bone Joint Surg
1937;19:84-96.
Borges JL, Guille JT, Bowen JR: Kohler’s bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-598.
Question 3
Which of the following clinical tests is used to diagnose medial instability of the elbow? Review Topic
Explanation
Question 4
A 23-year-old man is injured in a motorcycle accident and has a Glasgow Coma Scale (GCS) score of 10. His fiance arrives shortly after he does. He has an open, IIIc tibial fracture. The patient's parents are on the way but are not expected to arrive for some time. Who should be asked to provide informed consent?
Explanation
Question 5
A 72-year-old patient fell 3 weeks after undergoing a total hip arthroplasty using cementless fixation of the femoral component. She sustained a comminuted Vancouver type B-2 fracture with displacement of the calcar fragment. What is the best treatment option?
Explanation
The patient has an acute postoperative fracture of the proximal femur with subsidence. It is also common that the stem retroverts relative to the femur. It is most often seen in proximally porous coated stems within 90 days of surgery, one paper found it to occur 0.7% of the time in modern implants. There is always a debate whether this is a missed intraoperative fracture, or a new fracture that has resulted from an event of increased hoop stresses. Removal of the primary stem, placement of a diaphyseal engaging
stem (most frequently a tapered-fluted stem), and cabling of the fracture is the most successful treatment.
Question 6
Following resection of malignant tumors, complications related to endoprosthetic reconstruction are most common in what anatomic location?
Explanation
REFERENCE: Horowitz SM, Glasser DB, Lane JM, Healey JH: Prosthetic and extremity survivorship after limb salvage for sarcoma: How long do the reconstructions last? Clin Orthop 1993;293:280-286.
Question 7
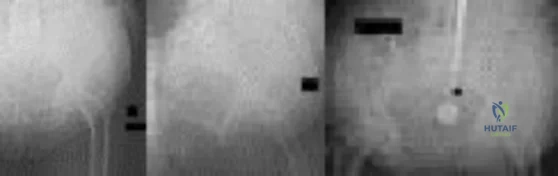
What is the heaviest weight that can be safely applied to the adult cervical spine via Gardner-Wells tong traction?
Explanation
REFERENCES: Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Anderson DG, Vacccaro AR, Gavin K: Cervical orthoses and cranioskeletal traction, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005,
pp 110-121.
Question 8
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.
Question 9
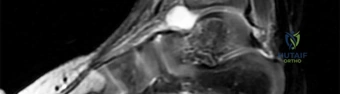
The patient undergoes hip arthroscopy and the image of the right hip is shown in Figure 39. Repair of the injured structure would be expected to improve
Explanation
The radiographic studies reveal both acetabular dysplasia and cam-type femoroacetabular impingement. The MR image shows an acetabular labral tear. Structural abnormalities of the hip, including femoroacetabular impingement, have commonly been identified in association with labral tears. Disruption of the ligamentum teres is not associated with impingement conditions in the absence of trauma.
The patient has acetabular dysplasia with a decreased lateral center-edge angle and also has visible cam-type femoroacetabular impingement. The common pathway for joint degeneration in hips with cam-type femoral head anatomy includes the development of cartilage damage in the anterior or superolateral aspects of the acetabular cartilage. Paralabral cysts may be seen more commonly in association with acetabular dysplasia, although the patient’s radiographs did not demonstrate substantial cystic changes. Osteochondral loose bodies and ligamentum teres ruptures can be seen at arthroscopy in a small number of cases.
There are several proposed roles of the acetabular labrum. It can increase the depth of the acetabular socket by as much as 21% to 28%. Roles of the acetabular labrum include joint lubrication, shock absorption, and pressure distribution. Recent studies assessing the effects of loading on joint stability for both normal and dysplastic hips did not demonstrate a substantial role of the labrum in differences in loading. Although joint stability might be improved following surgical repair, acetabular dysplasia is not likely to be resolved with acetabular labral repair alone.
RECOMMENDED READINGS
Tibor LM, Leunig M. The pathoanatomy and arthroscopic management of femoroacetabular impingement. Bone Joint Res. 2012 Oct 1;1(10):245-57. doi: 10.1302/2046-3758.110.2000105.PubMed: 23610655. View Abstract at PubMed
Peelle MW, Della Rocca GJ, Maloney WJ, Curry MC, Clohisy JC. Acetabular and femoral radiographic abnormalities associated with labral tears. Clin Orthop Relat Res. 2005 Dec;441:327-33. PubMed PMID: 16331022. View Abstract at PubMed
Ross JR, Zaltz I, Nepple JJ, Schoenecker PL, Clohisy JC. Arthroscopic disease classification and interventions as an adjunct in the treatment of acetabular dysplasia. Am J Sports Med. 2011 Jul;39 Suppl:72S-8S. doi: 10.1177/0363546511412320.
PubMed PMID: 21709035. View Abstract at PubMed
James SL, Ali K, Malara F, Young D, O'Donnell J, Connell DA. MRI findings of 37
femoroacetabular impingement. AJR Am J Roentgenol. 2006 Dec;187(6):1412-9. PubMed PMID: 17114529. View Abstract at PubMed
Groh MM, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskelet Med. 2009 Jun;2(2):105-17. doi: 10.1007/s12178-009-9052-9. Epub 2009 Apr 7. PubMed PMID: 19468871. View Abstract at PubMed
Henak CR, Ellis BJ, Harris MD, Anderson AE, Peters CL, Weiss JA. Role of the acetabular labrum in load support across the hip joint. J Biomech. 2011 Aug 11;44(12):2201-6. doi: 10.1016/j.jbiomech.2011.06.011. Epub 2011 Jul 14. PubMed PMID: 21757198. View Abstract at PubMed
Question 10
A 33-year-old man had his foot run over by a forklift 1 hour ago. Examination reveals that the head of the fifth metatarsal is extruded through the plantar aspect of the foot. The foot is severely swollen and pale, there is no sensation in the toes, and the pulses are not palpable. Radiographs are shown in Figures 42a and 42b. Emergent management should consist of
Explanation
REFERENCES: Fakhouri AJ, Manoli A II: Acute foot compartment syndromes. J Orthop Trauma 1992;6:223-228.
Myerson MS: Management of compartment syndromes of the foot. Clin Orthop 1991;271:239-248.
Ziv I, Mosheiff R, Zeligowski A, Liebergal M, Lowe J, Segal D: Crush injuries of the foot with compartment syndrome: Immediate one-stage management. Foot Ankle 1989;9:185-189.
Question 11
A 24-year-old professional basketball player reports the gradual onset of pain that is poorly localized to the left midfoot for the past 2 months. Examination reveals diffuse tenderness to palpation, full range of motion of the ankle and subtalar joint, and a normal neurovascular examination to the foot. An AP radiograph is shown in Figure 10. Definitive treatment should include
Explanation
REFERENCES: Torg JS, Pavlov H, Cooley JH, et al: Stress fractures of the tarsal navicular.
J Bone Joint Surg Am 1982;64:700-712.
Brodsky JW, Krause JO: Stress fractures of the foot and ankle, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2391-2409.
Question 12
Second-impact syndrome following a concussion
Explanation
According to several consensus statements, no child or adolescent athlete with a concussion should be allowed to return to play on the same day, regardless of severity. Second-impact syndrome refers to a second traumatic head injury that occurs while an athlete is still experiencing symptoms from the first injury. Young athletes are particularly vulnerable to second-impact syndrome. The mechanism by which this syndrome occurs likely is disruption of cerebral autoregulation, which may result in cerebral vascular congestion, diffuse brain swelling, and death.

RESPONSES FOR QUESTIONS 2 THROUGH 6
Curettage and/or grafting
Radiofrequency ablation
Intravenous (IV) antibiotics
Incision, drainage, and IV antibiotics
Neoadjuvant chemotherapy followed by surgical reconstruction
Observation alone
For each clinical vignette seen in the figures, select the best initial treatment from the list above.
Question 13
During a transperitoneal approach to the L5-S1 interspace, care must be taken to protect the superior hypogastric plexus from injury. Which of the following techniques reduces the risk of neurologic injury?
Explanation
REFERENCE: Transperitoneal midline approach to L4-S1, in Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer Verlag, 1983, pp 123-129.
Question 14
A 42-year-old woman sustains a closed posterior elbow dislocation. A closed reduction is performed, and the elbow appears stable under fluoroscopic examination. Initial treatment should consist of
Explanation
application of a hinged external fixator may be considered.
Question 15
A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management? Review Topic
Explanation
in management should be MRI. If the findings are negative, suspicion of nerve injury should lead to electromyography.
Question 16
Figures A and B show routine postoperative radiographs obtained 2 weeks after anterior cruciate ligament (ACL) reconstruction with autologous patellar tendon graft. Based on these findings, what is the next most appropriate action? Review Topic

Explanation
Question 17
The best definitive treatment for this patient’s left knee is
Explanation
This patient now has a major fixed flexion contracture and severe varus alignment and instability. Infection of the knee joint has to be ruled out. The radiograph shows all the hallmarks of Charcot arthropathy, including disintegration and fragmentation of the joint with major deformity. Infection of the knee joint and contiguous osteomyelitis still have to be ruled out. The clinical and radiographic findings are highly suggestive of a Charcot neurogenic arthropathy associated with uncontrolled diabetes. This patient is an unsuitable candidate for total knee arthroplasty (TKA) because he is noncompliant regarding his diabetes and has had a previously infected native joint that now is associated with Charcot arthropathy. He is nonambulatory. The failure rate of TKA or knee arthrodesis is extremely high in this setting. He will best be served with observation or amputation depending upon his symptom severity.
Question 18
A 15-year-old boy has had pain in the right shoulder for the past 3 months. He denies any history of trauma and has no constitutional symptoms. Examination reveals a large firm mass in the proximal arm. A radiograph and MRI scan are shown in Figures 27a and 27b. Biopsy specimens are shown in Figures 27c and 27d. Management should consist of
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 232-233.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-196.
Question 19
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?
Explanation
of displacement.
REFERENCES: Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603.
Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Brandser E, Marsh JL: Acetabular fractures: Easier classification with a systematic approach. Am J Roentgenol 1998;171:1217-1228.
Question 20
A 47-year-old landscaper presents with worsening left shoulder pain and weakness. Three years ago, he injured the left shoulder in a fall and elected for nonoperative management to minimize time off from work. Physical therapy was effective until 6 months ago when his shoulder function worsened to the point that he is now unable to work. Examination of his active range of motion reveals forward elevation 120° with pain, abduction 100°, IR at neutral to T8 and ER at neutral 5°. He has a positive ER lag sign and Hornblower's sign. Belly press and lift-off tests are normal. A recent radiograph is shown in Figures A. MRI images are shown in Figures B and C. Which of the following is the best treatment option? Review Topic
Explanation
Irreparable rotator cuff tears are marked by: (1) Superior displacement of the humeral head (AHI < 5-7mm), (2) Fatty infiltration of the rotator cuff muscles (Goutallier stage 3-4), (3) Increased duration of the tendon tear and (4) Profound external rotation weakness. These findings are predictive of poor-quality tissue and stiffness of the muscle-tendon unit, not amenable to primary repair. In this setting, a latissimus dorsi
transfer can be utilized to restore shoulder strength, function and improve pain. Relative contraindications include subscapularis deficiency, deltoid deficiency, pseudoparalysis of the shoulder and advanced glenohumeral arthritis.
Gerber et al. performed a case series analysis of 67 patients with irreparable rotator cuff tears managed with latissimus dorsi transfer. Patients with an intact subscapularis demonstrated improvement in pain, range of motion and strength postoperatively, while no improvement was noted in patients with subscapularis deficiency. The authors conclude that latissimus dorsi transfer should not be performed in the setting of poor subscapularis function.
Iannotti et al. found that better clinical results following latissimus dorsi transfer were associated with: preserved active shoulder range of motion and strength (specifically forward elevation > 90° and external rotation > 20°), synchronous firing of the transferred latissimus dorsi muscle and male gender.
Figure A is an AP radiograph of the left shoulder with superior migration of the humeral head (AHI < 5mm) and no evidence of glenohumeral arthritis. Figures B and C show a retracted posterosuperior rotator cuff tear and Goutallier stage 4 atrophy (more fat than muscle) of the supraspinatus, infraspinatus and teres minor, rendering this tear irreparable. Illustration A shows a latissimus dorsi transfer. The latissimus dorsi tendon is positioned over the top of the humeral head, covering most of the rotator cuff defect. The tendon is then secured to the subscapularis tendon edge and lesser tuberosity anteriorly, the remnant supraspinatus and infraspinatus tendons medially, and the greater tuberosity laterally.
Incorrect Answers:
Question 21
A 70-year-old man is experiencing neck pain, progressive weakness, and numbness in his arms and legs without bowel or bladder dysfunction or dysphagia. Upon examination, he has atrophy of his upper extremities but normal muscle bulk in his legs. Strength is diffusely 4/5 throughout. Cervical spine radiographs show spondylosis. Electromyography (EMG) reveals fibrillations with increased amplitude in the extensor carpi radialis and pronator teres. Nerve conduction studies demonstrate slowing conduction diffusely in the sural, peroneal, and ulnar nerves, and severe slowing in the median nerve. Testing of the tongue and thoracic paraspinal muscles does not show fibrillations or positive short waves. What is the most likely diagnosis? Review Topic
Explanation
Question 22
- Which of the following advantages does the use of a vascularized fibula graft have over a nonvascularized fibula graft?
Explanation
And a vascularized graft requires greater technical skills and a larger dissection to isolate the vascular pedicle with associated increased donor site morbidity.
Question 23
A 45-year-old woman with grade II adult-acquired flatfoot deformity has pain on the lateral side of her foot just distal to the tip of the fibula. Which component of a comprehensive flatfoot reconstruction most likely will address the deformity responsible for this pain?
Explanation
Patients develop lateral ankle pain with progression of adult-acquired flatfoot deformity. This is associated with increased hindfoot valgus deformity. Calcaneal fibular impingement has been considered the primary cause of this pain. Studies demonstrate that arthrosis of the posterior facet of the subtalar joint strongly correlates with lateral pain in adult-acquired flatfoot deformity. Both conditions are related to hindfoot valgus deformity. Although lateral column lengthening is a powerful tool for correction of flatfoot deformity, its effect on hindfoot deformity is less defined. Lateral column lengthening provides better correction of the longitudinal arch of the midfoot and realignment of the medial column than other osteotomies. A medializing calcaneal osteotomy has a significant linear effect on hindfoot valgus alignment. Spring ligament reconstruction and medial cuneiform opening-wedge osteotomies have less effect on hindfoot alignment than the medial calcaneal slide.
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
Question 24
With respect to the structure identified by the arrow in Figure 22b, the meniscofemoral 25 ligaments are
Explanation
The stress radiographs demonstrate posterior instability of the right knee in flexion. The MR images demonstrate injury to both the anterior and posterior cruciate ligament (PCL), with the stump identified with the arrow on the MR image (Figure 22b). The PCL has 2 functional bands. The anterolateral bundle originates from the roof of the intercondylar notch. It runs in a posterolateral direction onto the tibial crest between the posterior attachment of the medial and lateral menisci. During a double-bundled posterior ligament reconstruction, the
anterolateral bundle is tensioned with the knee in a position of mid flexion. The posteromedial bundle has a variable pattern of tension both in extension and in high flexion. Tensioning of the posteromedial bundle in extension may contribute to resistance against knee hyperextension.
The meniscofemoral ligaments are variably present. Although 93% of knees have been reported to have at least 1 meniscofemoral ligament present, both ligaments are simultaneously present in approximately 50% of knees. The ligament of Humphrey (anterior meniscofemoral ligament) and ligament of Wrisberg (posterior meniscofemoral ligament) are delineated by their anatomic relationship to the posterior cruciate.
RECOMMENDED READINGS
Amis AA, Bull AM, Gupte CM, Hijazi I, Race A, Robinson JR. Biomechanics of the PCL and related structures: posterolateral, posteromedial and meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2003 Sep;11(5):271-81. Epub 2003 Sep 5. Review. PubMed PMID: 12961064.View Abstract at PubMed
Amis AA, Gupte CM, Bull AM, Edwards A. Anatomy of the posterior cruciate ligament and the meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):257-63. Epub 2005 Oct 14. Review. PubMed PMID: 16228178.
View Abstract at PubMed . 26
Question 25
Figures 65a and 65b show the MRI scans of a 33-year-old man with severe left leg pain. He has had symptoms for 3 months with progressive worsening pain and function. Examination reveals ankle plantar-flexor weakness and diminished light touch sensation on the plantar surface of the foot. What treatment provides the best outcome? Review Topic
Explanation
Question 26
A 52-year-old man has had groin and deep buttock pain for the past 2 months. Examination reveals that hip range of motion is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 28. Management should consist of
Explanation
REFERENCES: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Urbanski SR, de Lange EE, Eschenroeder HC Jr: Magnetic resonance imaging of transient osteoporosis of the hip:. A case report. J Bone Joint Surg Am 1991;73:451-455.
Question 27
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of
Explanation
REFERENCES: Simon S, Whiffen J, Shapiro F: Leg-length discrepancies in monoarticular and pauciarticular juvenile rheumatoid arthritis. J Bone Joint Surg Am 1981;63:209-215.
Ansell BM, Bywaters EGL: Growth in Still’s disease. Ann Rheum Dis 1956;15:295-319.
Question 28
A 45-year-old man who has had recurrent pain and swelling of the left Achilles tendon insertion for the past 10 years reports that physical therapy and activity modification have provided relief in the past. He now has continued pain despite these efforts. He also reports occasional bouts of dysuria that he attributes to a history of prostatitis. He also notes recent eye irritation that he attributes to allergies. A lateral heel radiograph is shown in Figure 33. Which of the following laboratory studies would best aid in diagnosis?
Explanation
REFERENCE: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 560-650.
Question 29
Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment?
Explanation
REFERENCES: Favard L, Lautmann S, Sirveaux F, et al: Hemiarthroplasty versus reverse arthroplasty in the treatment of osteoarthritis with massive rotator cuff tear, in Walch G, Boileau P, Mole D (eds): 2000 Shoulder Prosthesis Two to Ten Year Follow-Up. Montpellier, France, Sauramps Medical, 2001, pp 261-268.
Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Werner CM, Steinmann PA, Gilbart M, et al: Treatment of painful pseudoparesis due to irreparable rotator cuff dysfunction with the Delta III reverse-ball-and-socket total shoulder prosthesis. J Bone Joint Surg Am 2005;87:1476-1486.
Question 30
Which of the following is considered a contraindication to functional bracing for the treatment of humeral shaft fractures?
Explanation
1) massive soft-tissue or bone loss; 2) an unreliable or noncompliant patient; and 3) an inability to maintain acceptable fracture alignment of up to 20 degrees of anterior or posterior angulation, 30 degrees of varus or valgus angulation, and greater than 3 cm of shortening.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Sarmiento A. Zagorski JB, Zych GA, et al: Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am 2000;82:478-486.
Question 31
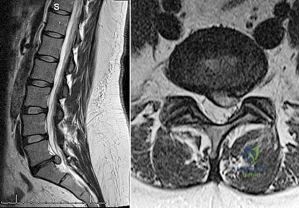
A 75-year-old man presents with worsening low back and bilateral leg pain. The pain worsens with ambulation and improves with sitting. On exam, he has strong DP and PT pulses. Straight leg raise is negative. A MRI of the lumbar spine is performed and is pictured in Figure A. On further questioning, which of the following is the patient also likely to report? Review Topic

Explanation
Lumbar spinal stenosis often results from degenerative changes of the intervertebral disc and facet joints which ultimately narrows the space available for the thecal sac and exiting nerve roots. Patients can present with neurogenic claudication, reported as worsening leg and/or back pain with ambulation and diminished walking capacity. MRI may demonstrate disc degeneration/bulging, hypertrophy of the ligamentum flavum and facet capsule, and narrowing of the central canal. Nonoperative management includes NSAIDs, PT and epidural steroid injections (ESI). Surgery is reserved for patients who have failed nonoperative measures and includes decompressive laminectomy with or without fusion depending on presence of instability.
Issack et al reviewed degenerative lumbar spinal stenosis. Unlike patients with vascular claudication, patients with neurogenic claudication are able to improve walking tolerance with postural changes, specifically with flexed-forward posture (such as leaning forward on a shopping cart). They are unable to improve their symptoms simply by cessation of walking. Patients with neurogenic claudication tend to lack the trophic changes of the skin on the legs/feet as well as diminished pulses characteristic of vascular disease.
Young et al reviewed the utilization of lumbar ESI for low back and leg pain. The authors concluded that lumbar ESI are a reasonable nonsurgical option to provide temporary symptomatic relief. Fluoroscopic guidance facilitates accurate placement of the injection into the epidural space, while its nonuse may lead to higher percentage of technical failures. Lastly, the transforaminal approach is more selective
than the interlaminar approach and can provide diagnostic information as well as symptom relief.
Figures A and B are T1 sagittal and T2 axial MR images, respectively, of the lumbar spine demonstrating significant central canal stenosis most notable at L4-L5 with broad disc protrusion, facet degeneration and infolding of the ligamentum flavum.
Incorrect
Responses:
Question 32
A 47-year-old woman underwent a bunionectomy and hallux valgus correction a few years ago. She now has the complication shown in Figures 38a and 38b. She has no pain with motion of the metatarsophalangeal or interphalangeal joints. What is the best reconstructive option in this setting?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 27-32.
Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 345-351.
Question 33
During total hip arthroplasty, what characteristic of irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene should provide a more wear-resistant construct than traditional gamma-irradiated (2.5-4 Mrad)-in-air polyethylene mated with the same head?
Explanation
Highly cross-linked polyethylene makes material resistant to adhesive wear. Abrasive wear from third bodies does not decrease wear. The fatigue strength of such material is inferior to that of traditional polyethylene, and its resistance to creep is the same, if not lower, than that of traditional polyethylene.
Question 34
The Lisfranc ligament connects the base of the
Explanation
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Solan MC, Moorman CT III, Miyamoto RG, et al: Ligamentous restraints of the second tarsometatarsal joint: A biomechanical evaluation. Foot Ankle Int 2001;22:637-641.
Question 35
A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, and has internal rotation to the fifth lumbar vertebra. At 6 months, his motion fails to improve. Radiographs are shown in Figures 18a and 18b. What is the best course of action?
Explanation
REFERENCES: Cuomo F, Checroun A: Avoiding pitfalls and complication in total shoulder arthroplasty. Orthop Clin North Am 1998;29:507-518.
Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 36
Figure 62 shows the radiograph of a 46-year-old man who has had increasing shoulder pain and diminishing motion over the last 10 years. Because his difficulties are severely impacting his quality of life, he is seeking advice and treatment options. Twenty five years ago, he underwent a shoulder stabilization procedure for recurrent shoulder dislocations. Examination reveals he can only elevate his arm to less than shoulder level and his external rotation is no more than 10 degrees. Management consisting of nonsteroidal anti-inflammatory drugs and intra-articular steroid injections has failed to provide relief. What is the most appropriate treatment recommendation? Review Topic

Explanation
arthritis of dislocation is 45 years old. Despite the young age of these patients, total shoulder arthroplasty offers the most predictable improvement in pain and function. However, the patient must be made aware of the need to protect the arm from excessive loads to protect the glenoid implant. Because there is complete loss of articular cartilage and incongruent joint surfaces, there is no role for arthroscopic debridement and capsular release. Injections offer little, if any, chance of improvement with the prior history of nonresponse. Physical therapy predictably makes patients worse because loading the arthritic joint generates more pain. Reverse shoulder arthroplasty is reserved for elderly patients with severe rotator cuff deficiency. A humeral head arthroplasty, while potentially more ideal than a total shoulder arthroplasty because of glenoid concerns, would likely not offer pain relief in the face of the significant glenoid involvement and incongruity.
Question 37
Osteopenia is defined by the World Health Organization (WHO) as a bone mineral density (BMD) that is
Explanation
The T-score represents a comparison to young normals or optimum peak density. The Z-score represents a comparison of BMD to age-matched normals. Measurements of bone mineral density (BMD) at various skeletal sites help in predicting fracture risk. Hip BMD best predicts fracture of the hip, as well as fractures at other sites.
REFERENCE: Kanis JA, Johnell O, Oden A, et al: Risk of hip fracture according to the World Health Organization criteria for osteopenia and osteoporosis. Bone 2000;27:585-590.
Question 38
- Which of the following types of sarcoma of the bone is most sensitive to external beam radiation?
Explanation
Question 39
A 68-year-old woman had advanced right knee arthritis and total knee replacement was planned. She learned she had primary biliary cirrhosis at age 41 and now has advancing liver failure. Preoperative coagulation tests show a baseline International Normalized Ratio (INR) of 1.36. Appropriate methods to prevent thromboembolic disease as recommended by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty , include
Explanation
Question 40
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
REFERENCES: Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
Question 41
A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
Explanation
Question 42
A 38-year-old man reports a 6-week history of shoulder pain and stiffness after falling on the stairs and landing onto the affected side. Radiographs are shown in Figures 54a and 54b. What is the most appropriate treatment? Review Topic

Explanation
Question 43
A 52-year-old man underwent arthroscopic repair of a 1-cm supraspinatus tendon tear 3 weeks ago. He was doing well until he fell down three stairs. One week after the fall he continues to report pain similar to his preoperative pain. An MRI scan reveals a minimally retracted 1-cm supraspinatus tendon tear in the same location as his original tear. Management should now consist of Review Topic
Explanation
Question 44
-Figures 56a and 56b are the MRI scans of a 2-year-old girl who has a fever of 39°C and inability to move her left arm. She has not had any recent injury and is otherwise healthy. Radiograph findings of her left upper extremity are normal. What is the most appropriate treatment?
Explanation

Question 45
A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment? Review Topic

Explanation
appears to be helpful. A hindfoot arthrodesis (usually triple) would be reserved if coalition resection proves to be unsuccessful. Achilles tendon lengthening and orthotic support, as well as debridement of the sinus tarsi, are not expected to result in a satisfactory outcome. The patient does not have a flatfoot deformity.
(SBQ13PE.64) A 5-year-old boy presents to clinic for evaluation of bilateral foot deformities shown in Figure 1. He is fully active and has no pain. The feet appear normal when he is sitting on the examination table, and there is supple passive motion at the subtalar joint. Passive ankle dorsiflexion is to neutral with knee in extension and 15 degrees with knee in flexion. What is the most appropriate next step? Review Topic

Spine MRI
Standing radiographs of the bilateral feet
Gastrocnemius stretching and nightime use of ankle foot orthosis
Gastrocnemius stretching and use of UCBL orthotic when ambulating
Gastrocnemius stretching
The patient is presenting with bilateral flexible pes planovalgus (or flexbile flatfoot). The most appropriate treatment in patients with a tight heel cord and no pain is gastrocnemius stretching
A flexible flatfoot in a child typically resolves spontaneously. Radiographs are typically indicated when there is pain to rule out other conditions. Treatment for patients without pain includes observation and gastrocnemius stretching. If there is pain, soft arch support or a more rigid UCBL can be used, but orthotics do not change the natural history. In patients with continued tightness in the heel cord despite aggressive stretching, gastrocnemius lengthening may be necessary.
Mosca reviews the management of flexible flatfeet in children and adolescents. He reports that there is no compelling evidence that an arch can be created with use of
orthotics. He proposes the following algorithm: patients with asymptomatic flatfeet are observed; symptomatic flatfeet with tight heel cords undergoing stretching until they become asymptomatic; symptomatic flatfeet with tight heel cords that do not respond to stretching (rare cases) are considered for surgery.
Figure A shows a young a patient with bilateral flatfeet when standing. Incorrect Answers:
abnormalities can seen in patients with cavovarus deformity Answer 2: Radiographs are indicated when there is pain to rule out other conditions. Answer 3: Ankle foot orthoses are not used for pes planovalgus Answer 4: UCBL would be indicated if the patient was having pain.
(SBQ13PE.42) Submuscular bridge plating is appropriate treatment for which of the following? Review Topic
A 2-month-old female with displaced, spiral, mid-diaphyseal femur fracture
A 26-month-old boy with a displaced spiral mid-diaphyseal femur fracture with
<2cm shortening
A 7-year old boy with a transverse, non-comminuted mid-diaphyseal femur fracture
A 7-year-old boy with a highly comminuted mid-diaphyseal femur fracture
A 15-year-old girl with a displaced butterfly fragmented mid-diaphyseal femur fracture
Submuscular bridge plating is appropriate for length-unstable femur fractures in skeletally immature patients ages 6 years and older.
Traditional plating of diaphyseal femur fractures in children has been abandoned due to the large incision and significant periosteal stripping involved. Submuscular plating with limited incisions and percutaneously applied fixation is a more biologically friendly way to achieve rigid internal fixation in length-unstable fracture patterns. External fixation is another acceptable option for these fractures. Locked plating, on the other hand, provides an 'internal external fixator,' avoids pin site issues and allows rapid mobilization while providing a biologically favorable environment for healing.
Kocher et al. provide the AAOS Clinical Practice Guideline for the treatment of pediatric diaphyseal femur fractures. They concluded that there was insufficient evidence regarding submuscular bridge plating to include it in the guideline.
Flynn et al. review the management of pediatric femoral shaft fractures. The note that
the narrow indications for plating of pediatric femoral fractures are open fractures, multiple trauma, head injury or compartment syndrome in patients less than 12 years old. Plating allows rigid fixation with readily available equipment and allows for rapid mobilization.
Hedequist et al. present a Technical Tricks paper in which they detail their surgical technique for submuscular bridge plating. They recommend this fixation strategy for patients between age 6 and skeletal maturity with comminuted diaphyseal femur fractures that are not easily treated by other methods.
Illustration A shows a preoperative and postoperative radiograph of a comminuted pediatric femur fracture treated with submuscular plating.
Incorrect answers:
(SBQ13PE.88) A 12-month-old boy attends a government regulated childcare center. His parents are called after a fall. Non-accidental trauma has been ruled out. On physical examination the right elbow is swollen and tender. He is unwilling to allow you to move the arm. Radiographs of the elbow are shown in Figure A. What is the orthopaedic management of this injury? Review Topic

Observation only
Elbow sling for 3 to 4 weeks
Rigid elbow immobilisation for 4 to 5 weeks
Admit for 24-48 hours for continuous intracompartmental pressure measurements
Operative fixation with percutaneous pinning PREFERRED RESPONSE 5
This patient presents with a distal humeral physeal separation. The most appropriate treatment would be closed reduction with internal fixation with percutaneous pins.
Displaced distal humerus physeal separation is typically seen in children under the age of 3 and has a high association with child abuse. The diagnosis can be a difficult as radiographs of a distal humeral physeal separation may be subtle. Often, radiographs show no obvious fracture, but can appear like an elbow dislocation since the secondary ossification centers have not yet developed. MRI or arthrogram can be used to aid in diagnosis.
Shrader et al. reviewed pediatric supracondylar fractures and pediatric physeal elbow fractures. They state the key to diagnosis of distal humerus physeal separation is the assessment is the radial head–capitellum relationship. These injuries should be fixed with closed reduction and smooth wire pinning. An elbow arthrogram may be considered intraoperatively for these patients because of the difficulty visualizing the distal humeral anatomy in children so young.
Skaggs et al. reviewed the diagnosis and management of pediatric elbow fractures. He states that child abuse should be suspected in all cases of elbow fracture when the child is less than 3 years of age and/or the injury pattern occur from a shearing mechanism. The displacement of physeal elbow fractures is almost always posteromedial.
Figure A shows AP and lateral radiographs with posteromedial displacement of the radial and ulnar shafts relative to the distal humerus. This is consistent with distal humeral physeal separation.
Incorrect Answers:
Question 46
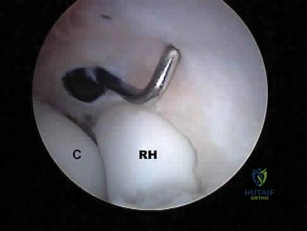
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50? Review Topic
Explanation
Question 47
A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?

Explanation
Myerson reported 3/43 patients in his series below had chronic foot compartment syndrome. There are 9 compartments in the foot: (1) medial, (2) superficial, (3) lateral, (4) adductor, (5-8) four interossei, and (9) calcaneal. The plantar fascia limits the space available for hematoma and swelling, causing damage to the intrinsic flexors of the foot (particularly the lumbricals and interossei), resulting in clawtoes.
Question 48
Cortical bone demonstrates viscoelastic behavior as its mechanical properties are sensitive to strain rate and duration of applied load. Regarding longitudinal strain in cortical bone, which of the following statements regarding this characteristic is true?
Explanation
For LOW strain rates typical of normal activity (physiological strain rates of <0.1/s), bone is ELASTIC and DUCTILE (increasing ultimate strain with increasing strain rate). There is a ductile-to-brittle transition with increasing strain rate from normal to
supranormal rates. For EXTREMELY HIGH supranormal strain rates (>0.1/s, high impact trauma), bone is VISCOELASTIC and BRITTLE (low ultimate strain with increasing strain rate). Bone also becomes stronger and stiffer (higher modulus, steeper slope of stress-strain plot) as strain rate increases. This viscoelastic property helps in damping muscle contracture.
Natali and Meroi reviewed studies examining mechanical properties of bone. Mechanical properties are correlated with moisture, deformation rate, density and region of bone. Mechanical adaptation of bone is affected by strain rate (rate at which bone is deformed), strain mode (tension, compression, shear), strain direction (direction of strain relative to bone surface), strain frequency (cycles/second), stimulus duration (period over which deformation cycles are applied), strain distribution (pattern of strain magnitude across bone section) and strain energy (energy stored during deformation).
Illustration A shows the mechanical properties of bone with increasing strain rates. Incorrect Answers:
increase. During normal activity, as strain rate increases, bone is more ductile. With high impact trauma, bone is more brittle.
Question 49
The therapeutic effect of etanercept in the treatment of rheumatoid arthritis is primarily mediated through
Explanation
REFERENCES: Weinblatt ME, Kremer JM, Bankhurst AD, et al: A trial of etanercept, a recombinant tumor necrosis factor receptor: Fc fusion protein, in patients with rheumatoid arthritis receiving methotrexate. N Engl J Med 1999;340:253-259.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 489-530.
Question 50
A 34-year-old woman has had painful snapping and popping in the elbow since falling while in-line skating 6 months ago. The popping also occurs when she pushes off with her hands to rise from a seated position. Initial radiographs were normal, and she was told that she had sprained her elbow. Examination reveals few findings except that she is very apprehensive when the forearm is forcefully supinated with the elbow extended or partially flexed. A radiograph taken in that position is shown in Figure 24. Treatment should consist of
Explanation
REFERENCES: O’Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Burgess RC, Sprague HH: Post-traumatic posterior radial head subluxation: Two case reports. Clin Orthop 1984;186:192-194.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 51
Figures 25a and 25b show the radiograph and MRI scan of a 7 1/2-year-old boy who has been limping for 1 year. His pain has worsened over the past 2 weeks, and his parents note swelling over the dorsum of the foot for the past 4 days. Examination reveals no fever, and laboratory studies show a WBC of 6,700/mm 3 , an erythrocyte sedimentation rate of 26 mm/h, and a normal C-reactive protein level. What is the most likely diagnosis?
Explanation
REFERENCES: Wang MN, Chen WM, Lee KS, Chin LS, Lo WH: Tuberculous osteomyelitis in young children. J Pediatr Orthop 1999;19:151-155.
Watts HG, Lifeso RM: Tuberculosis of the bones and joints. J Bone Joint Surg Am 1996;78:288-298.
Question 52
An otherwise healthy 33-year-old man who works in construction reports a 3-month history of knee pain. Radiographs are shown in Figures 9a and 9b. An axial T 1 -weighted MRI scan with contrast, an angiogram, and histologies are shown in Figures 9c through 9f. What is the most likely diagnosis?
Explanation
REFERENCES: Sheth DS, Yasko AW, Raymond AK, et al: Conventional and dedifferentiated parosteal osteosarcoma: Diagnosis, treatment, and outcome. Cancer 1996;78:2136-2145.
Lewis VO, Gebhardt MC, Springfield DS: Parosteal osteosarcoma of the posterior aspect of the distal part of the femur: Oncological and functional results following a new resection technique. J Bone Joint Surg Am 2000;82:1083-1088.
Question 53
A 47-year-old man is seen in consultation in the ICU after being admitted and treated emergently for a dissecting aortic aneurysm. Current examination reveals generalized weakness of the lower extremities with a significant decrease in pain and temperature sensation from approximately the waist down. Proprioception is maintained. What is the most likely diagnosis at this time? Review Topic
Explanation
Question 54
below show the radiographs, and the MRIs obtained from a year-old man with worsening left knee pain. A foot hip-to-ankle radiograph shows a degree varus knee deformity. The patient sustained a major left knee injury 5 years ago and a confirmed complete anterior cruciate ligament (ACL) tear. He managed this injury nonsurgically with a functional brace but experienced worsening pain. He was seen by an orthopaedic surgeon 18 months ago, and a medial meniscus tear was diagnosed; the tear was treated with an arthroscopic partial medial meniscectomy. Since then, his knee has been giving way more often, and he no longer feels safe working on a pitched roof. The patient received 6 months of formal physical therapy and was fitted for a new functional ACL brace, but he still has pain and instability. He believes he has exhausted his nonsurgical options and would like to undergo surgery. What is the most appropriate treatment at this time?
Explanation
Proximal tibial osteotomy is the most appropriate intervention to correct varus malalignment and to reduce stress on the ACL. In some cases, proximal tibial osteotomy alone may address both pain and instability, but if instability persists, particularly in the setting in which instability can be dangerous, subsequent ACL reconstruction can further stabilize the knee with less stress on the graft after the correction of malalignment. Varus alignment places increased stress on the native or reconstructed ACL. ACL reconstruction should be performed only at the same time as or following proximal tibial osteotomy to correct alignment in the setting of varus malalignment. It is not appropriate to perform ACL reconstruction prior to proximal tibial osteotomy in this setting. Distal femoral osteotomy is not indicated to correct varus malalignment. Varus alignment places increased stress on the native or reconstructed ACL, and ACL
reconstruction alone is not indicated for this patient.
Question 55
What is the most important stabilizing mechanism in the midrange of motion of the glenohumeral joint? Review Topic
Explanation
Question 56
Figure 16 shows the radiograph of a 56-year-old man who has neck pain after a rollover accident on his lawnmower. The injury appears to be isolated, and he is neurologically intact. Management of the fracture should consist of
Explanation
REFERENCES: Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries. J Am Acad Orthop Surg 2002;10:271-280.
Question 57
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of
Explanation
REFERENCES: Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Warner JJ, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 58
Receptor activator of nuclear factor kappa b (RANKL) and macrophage colony stimulating factor (MCSF) signaling pathways are necessary for the formation of multinucleated osteoclasts that resorb bone. Which of the following cells are known to produce RANKL?
Explanation
Question 59
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty? i. Infection
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
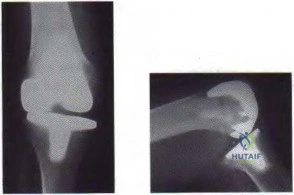
Figure 59a Figure 59b
Question 60
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure A. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion? Review Topic

Explanation
Question 61
--The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
Explanation
This patient has a classic presentation of postmeniscectomy medial compartment arthritis. The appropriate diagnostic study is weight-bearing radiographs to confirm the diagnosis. An MRI scan will reveal medial compartment arthritis but will not provide information about alignment. A CT scan would be appropriate to detect an occult fracture; however, this condition is not suspected in this clinical scenario. An ultrasound can provide information about fluid collection around the knee or a deep vein thrombosis; however, these conditions also are not suspected in this clinical scenario.
Because the patient has a correctable deformity (gaps 3 mm with valgus stress) and his symptoms are localized to the involved compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgicalplanning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient.A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation,examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result,current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 is an indication for HTO but does not influence technique.
Question 62
What is the most likely type of pathology seen in Figure 16?
Explanation
REFERENCES: McLain R, Weinstein J: Tumors of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1173.
Charlton OP, Martinez S, Gehweiler JA Jr: Pedicle thinning at the thoracolumbar junction: A normal variant. Am J Roentgenol 1980;134:825-826.
Question 63
When compared with reamed intramedullary nailing for an unstable diaphyseal tibia fracture, unreamed nailing is associated with which of the following?
Explanation
Question 64
Which component position is associated with poor patellar tracking during total knee arthroplasty (TKA)?
Explanation
Internal malrotation of the femoral or tibial component is associated with lateral tracking of the patella in TKA. Lateral placement of the femoral component and medial placement of the patella component can aid in preventing lateral tracking of the patella. Varus alignment of the proximal tibia has not been associated with patella maltracking.







RESPONSES FOR QUESTIONS 106 THROUGH 109
Immobilization/nonsurgical management
Irrigation and debridement
stage reimplantation total knee arthroplasty (TKA)
Increased constraint/polyethylene exchange
Revision of the femoral component only
Revision of the tibial component only
Revision of both components
Revision of the patellar component
Select the treatment listed above that most appropriately addresses each scenario described below.
Question 65
A 63-year-old woman is seen 10 weeks after sustaining a closed minimally displaced distal radius fracture. She has been in a short-arm cast and reports minimal pain but notes that she is having difficulty using her thumb. An extensor pollicis longus (EPL) tendon rupture is suspected. Which examination finding would confirm lack of EPL function?
Explanation
As many as to 5% of patients with a nondisplaced distal radius fracture experience EPL rupture. The extensor pollicis brevis (EPB) tendon often attaches to the extensor hood and sometimes continues more distally, providing weak metacarpophalangeal extension even in the setting of EPL disruption. However, because of the vector of its pull, the EPB cannot extend the thumb dorsal to the plane of the palm. A positive Froment sign is noted when flexion of the thumb interphalangeal joint with an attempted key pinch is caused by adductor pollicis weakness from ulnar nerve dysfunction. Compression of the median nerve in the carpal tunnel affects the recurrent motor branch of the abductor pollicis brevis, leading to thenar atrophy. The flexor pollicis longus tendon (FPL) is intact so the patient would not have difficulty flexing the thumb with the palm flat.
Question 66
Which of the following is considered the most common complication of the impaction grafting technique for femoral revision surgery?
Explanation
REFERENCES: Gie GA, Linder L, Ling RS, Simon JP, Slooff TH, Timperley AJ: Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br 1993;75:14-21.
Meding JB, Ritter MA, Keating ME, Faris PM: Impaction bone-grafting before insertion of a femoral stem with cement in revision total hip arthroplasty: A minimum two-year follow-up study. J Bone Joint Surg Am 1998;79:1834-1841.
Question 67
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
REFERENCES: Montgomery DM, Brower RS: Cervical spondylotic myelopathy: Clinical syndrome and natural history. Orthop Clin North Am 1992;23:487-493.
Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K: Myelopathy hand: New clinical signs of cervical cord damage. J Bone Joint Surg Br 1987;69:215-219.
An HS, Simpson JM: Surgery of the Cervical Spine. Baltimore, MD, Williams and
Wilkins, 1994.
Question 68
A 32 yr old man with oxalosis is scheduled for a surgical treatment of spinal stenosis. Which of the following organs is most likely to show signs of systemic oxalosis during a preoperative assessment?
Explanation
Question 69
A patient underwent an open reduction and internal fixation of a calcaneus fracture 6 months ago via an extensile lateral approach. He now reports burning pain on the lateral side of his ankle and foot. A local cortisone injection at the site of the tenderness, about 7 cm above the lateral heel, provided temporary relief of the pain. What is the recommended course of management for the persistent burning pain?
Explanation
Question 70
Which of the following is considered a contraindication to the use of a reverse total shoulder arthroplasty? Review Topic
Explanation
Question 71
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of
Explanation
REFERENCE: Callahan BC, Georgopoulos G, Eilert RE: Hemivertebral excision for congenital scoliosis. J Pediatr Orthop 1997;17:96-99.
Question 72
A 59-year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 73
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCE: Dorfman HD, Bodgan C: Immunohematopoietic tumors, in Dorfman HD, Bogdan C (eds): Bone Tumors. St Louis, MO, Mosby, 1998, Chapter 12.
Question 74
Figures below depict the radiographs obtained from a 60-year-old man with instability and pain 1 year after primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to 3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1% neutrophils. No growth of organisms is seen on routine culture. What is the best next step?

Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results show no signs of infection, so a single-stage procedure is preferred.
Question 75
Atraumatic suprascapular nerve compression usually occurs at which of the following anatomic locations if it develops atraumatically? Review Topic
Explanation
Question 76
A 27-year-old man has had pain in the right index finger for the past 9 months. The pain is completely relieved with ibuprofen. An AP radiograph and CT scan are shown in Figures 80a and 80b. What is the most likely diagnosis?
Explanation
radiolucent nidus. A small area of calcification may be present within the center of the nidus. The radiolucent nidus is surrounded by a thick rim of sclerotic bone. These diagnostic
features are frequently better seen on CT. An increase in cyclooxygenase activity has been demonstrated within osteoid osteomas, which may explain why aspirin and other nonsteroidal anti-inflammatory drugs classically relieve the pain associated with these lesions.
REFERENCES: Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 121-130.
Question 77
A 9-year-old girl has pain over the fifth toe that is aggravated by shoe wear. Clinical photographs are shown in Figures 28a and 28b. Treatment of this deformity should consist of
Explanation
REFERENCES: Black GB, Grogan DP, Bobechko WP: Butler arthroplasty for correction of adducted fifth toe: A retrospective study of 36 operations between 1968 and 1982. J Pediatr Orthop 1985;5:439-441.
Paton RW: V-Y plasty for correction of varus fifth toe. J Pediatr Orthop 1990;10:248-249.
Coughlin MJ, Mann RA: Lesser toe deformities, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 5. St Louis, MO, Mosby, 1986, pp 132-157.
Question 78
The most appropriate next surgical procedure is
Explanation
This patient’s arthritis likely has progressed to the lateral compartment. The location and degree of local pain and tenderness are the most important physical findings. History and physical findings indicate arthritis progression to the lateral and anterior compartments. This scenario suggests the need for conversion of the unicompartmental arthroplasty to TKA.

Question 79
Which of the following abnormalities has been observed in a higher than expected frequency in patients with metal-on-metal hip bearings?
Explanation
REFERENCES: Dunstan E, Ladon D, Whittingham-Jones P, et al: Chromosomal aberrations in the peripheral blood of patients with metal-on-metal hip bearings. J Bone Joint Surg Am 2008;90:517-522. Ladon D, Doherty A, Newson R, et al: Changes in metal levels and chromosome aberrations in the peripheral blood of patients after metal-on-metal hip arthroplasty. J Arthroplasty 2004:19:78-83.
Visuri T, Pukkala E, Paavolainen P, et al: Cancer risk after metal on metal and polyethylene on metal total hip
arthroplasty. Clin Orthop Relat Res 1996:329:S280-S289. Question 61
A 73-year-old woman with a history of type II diabetes mellitus undergoes a total hip arthroplasty for osteoarthritis. She continues to have serosanguinous wound drainage from the midportion of the incision 12 days after surgery. What is the most appropriate treatment at this time?
Return to the operating room for debridement and irrigation with removal of all implants and immediate reimplantation
Return to the operating room for open debridement and irrigation, exchange of the polyethylene
insert, followed by appropriate antibiotics based on intraoperative culture results
Hip spica pressure dressing and a 2-week course of oral antibiotics
Hip aspiration for culture, followed by a 2-week course of appropriate IV antibiotics based on
culture results
Hip aspiration for culture, followed by a 6-week course of appropriate IV antibiotics based on culture results
DISCUSSION: This patient has an acute postoperative deep infection, with prolonged drainage at 12 days postoperatively. Even without other signs or symptoms of infection, the prolonged drainage this far out after surgery is concerning for an acute postoperative infection. The most appropriate treatment at this point is open debridement with retention of the implants. Modular parts, if present, are exchanged. Oral or IV antibiotics alone are generally inadequate to treat the infection, and this form of management alone would result in a missed opportunity to potentially cure the infection. Removal of all implants at this point is not required because early aggressive debridement within the first 2 weeks after surgery offers a reasonable outcome. After 4 to 6 weeks of symptoms, results of debridement are less favorable and removal of the implants is usually required.
REFERENCES: Crockarell JR, Hanssen AD, Osmon DR, et al: Treatment of infection with debridement and retention of the components following hip arthroplasty. J Bone Joint Surg Am 1998;80:1306-1313. Hanssen AD, Osmon DR: Assessment of patient selection criteria for treatment of the infected hip arthroplasty. Clin Orthop Relat Res 2000;381:91 -100.
Question 80
During placement of an external fixator for a distal radius fracture, the most commonly injured nerve is a branch of which of the following nerves? Review Topic
Explanation
(SBQ12TR.106) A 67-year-old female sustains the injury shown in Figure A after a trip and fall. When discussing the outcomes of surgery with the patient, which of the following statements is true?

Post-surgical mortality rates are significantly lower after total hip arthroplasty compared to hemiarthroplasty
Internal fixation shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to arthroplasty
Bipolar hemiarthroplasty shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to unipolar hemiarthroplasty
A delay in surgery greater than 48 hours is recommended if the patient has multiple medical comorbiditiesm which are not fully optimized
Dislocation rates are equivalent between total hip arthroplasty and hemiarthroplasty
Moderate evidence supports that hip fracture surgery within 48 hours of admission is associated with better outcomes. However, patients with significant medical comorbidity should be fully optimized before surgery.
Although several studies have shown a benefit to surgery within 48 hours, no definitive time frame has been elucidated. The majority of literature has shown improved outcomes in regards to pain, complications, and length of stay with early surgery. Patients with significant medical comorbidities have been shown to have the highest mortality rates.
Moran et al. aimed to determine whether a delay in surgery for hip fractures had an affect on postoperative mortality among elderly patients. In an observational study of 2660 patients, they showed that mortality following hip fracture surgery was 9% at 30-days, 19% at 90-days, and 30% at 12-months. Patients with medical comorbidities had 2.5 times the risk of death within 30-days of surgery. In addition, individuals who had surgery delayed beyond 4 days had increased mortality at 90-days and 12-months.
Papakostidis et al. examined the timing of internal fixation of intracapsular fractures of the neck of femur on the development of late complications, particularly osteonecrosis of femoral head (ONFH) and non-union. They showed no benefit of
early surgery on incidence of AVN. However, delay of internal fixation of more than
24 hours showed increased rates of non-union.
Figure A shows a displaced right femoral neck fracture. Incorrect Answers:
Question 81
A 12-month-old boy has right congenital fibular intercalary hemimelia with a normal contralateral limb. A radiograph of the lower extremities shows a limb-length discrepancy of 2 cm. All of the shortening is in the right tibia. Assuming that no treatment is rendered prior to skeletal maturity, the limb-length discrepancy will most likely
Explanation
REFERENCES: Paley D, Bhave A, Herzenberg JE, et al: Multiplier method for predicting
limb-length discrepancy. J Bone Joint Surg Am 2000;82:1432-1446.
Moseley CF: A straight-line graph for leg length discrepancies. Clin Orthop 1978;136:33-40.
Question 82
The knee arthroplasty type associated with the highest 5-year revision rate is
Explanation
Revision rates for UKA at 10 years are lower than 5% at specialty centers. However, the 10-year revision rate associated with UKA in registries such as the National Joint Registry for England and Wales is 2 to 3 times that of TKA. Among partial knee replacements, patellofemoral arthroplasty is associated with the highest revision rate at every time interval.

CLINICAL SITUATION QUESTIONS 167 THROUGH 169
Figures 167a and 167b are the radiographs of a middle-age man. He is a noncompliant patient who has severe insulin-dependent diabetes and a below-knee amputation on the right side. He is usually in a wheelchair, does not use a prosthesis, transfers using a walker, and resides in an institution. He had an infection in the left leg years ago, which was treated successfully with intravenous antibiotics (the details are unknown). His left knee is mildly painful, swollen but not warm, has limited range of motion (40-140 degrees), and is grossly unstable.
Question 83
An otherwise healthy 25-year-old man with an isolated closed mid-diaphyseal femoral fracture undergoes intramedullary nailing. Compared with nonreamed nailing, reamed femoral nailing is associated with a higher rate of Review Topic
Explanation
Question 84
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology?
Explanation
REFERENCES: Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, p 23.
Sammarco VJ: Os acromiale: Frequency, anatomy, and clinical implications. J Bone Joint Surg Am 2000;82:394-400.
Question 85
After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office with continued pain 2 years after surgery. He describes instability, particularly when descending stairs. Upon examination, there is range of motion from 0 to 120 degrees with no extensor lag. The knee is stable to varus and valgus stress in extension, but there is flexion instability in both the anterior-posterior direction and in the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection workup is negative. What is the most appropriate surgical intervention at this time?
Explanation

Video 99 for reference
This patient has valgus knee alignment, and, after undergoing appropriate bone resections and soft-tissue balancing, has demonstrated a tight PCL on trial reduction as evidenced by lift-off of the trial insert as described by Scott and Chmell. The appropriate maneuver is PCL recession with partial release of tight (usually anterolateral) PCL fibers. However, for this patient, instability resulted in increased anterior translation. At this stage, the options are to convert to either a deeper-dish insert with increased sagittal conformity or a posterior stabilized insert. The only appropriate choice among the responses is use of an insert with increased sagittal conformity to prevent excessive anterior translation. Increasing the polyethylene could improve stability in flexion, but, considering there is good stability in extension, this likely would lead to an inability to achieve full extension. The patient’s valgus deformity, flexion contracture, correction with release of the iliotibial band, and posterolateral capsule predispose him to increased risk for peroneal nerve palsy. His symptoms at follow-up suggest knee flexion
instability with pain, swelling, and difficulty descending stairs. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant depending on the condition of the ligaments likely is needed to address his symptoms. The difference in extension vs flexion stability makes polyethylene exchange a poor option. There is no reason to believe a constrained rotating hinge design is necessary. Repeat use of a PCL-retaining insert is not recommended.
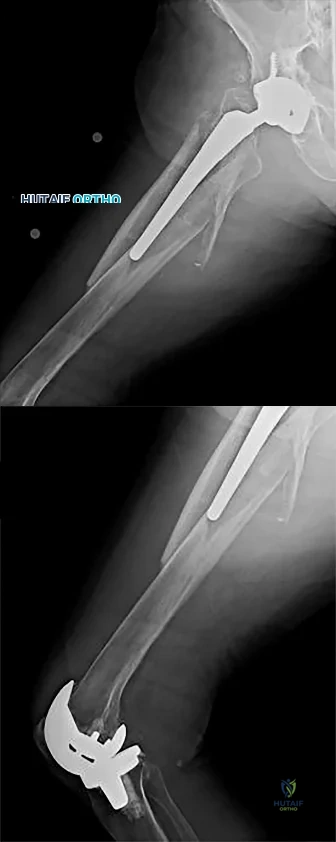
Question 86
A 20-year-old man has activity-related deep-seated shoulder pain in his dominant right shoulder. He has taken 3 months off training as a college javelin thrower, and management consisting of physical therapy has failed to provide relief. Shoulder arthroscopic views are shown in Figures 16a through 16c. What is the underlying association with this condition? Review Topic
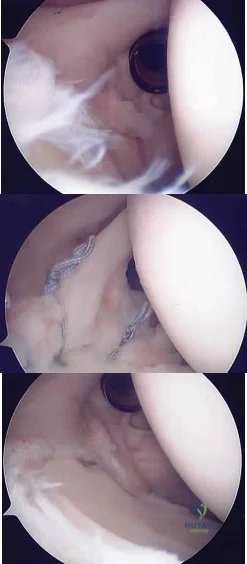
Explanation
Question 87
What is the most common causative bacteria in septic arthritis in children? Review Topic
Explanation
Question 88
Figures 136a through 136c are the weight-bearing anteroposterior and lateral radiographs of a 28-year-old construction worker who has had 6 months of progressive knee pain isolated to the medial aspect of his right knee. The pain has not responded to nonsurgical treatment. His body mass index is 26. He has knee range of motion from 0 to 125 degrees, and his knee is stable to ligament examination. What is the most appropriate surgical treatment?
Explanation
Proximal tibial osteotomy is the best option for this young patient who has good range of motion and arthritis isolated to the medial compartment. Distal femoral osteotomy is more appropriate for correction of valgus deformity. In the setting of most varus deformities as shown in this patient’s radiographs, there is varus angulation of the proximal tibial. Correction of alignment at the femur results in obliquity of the joint line and abnormal loading. Medial
unicompartmental knee arthroplasty and TKA are less optimal in this setting because of this patient’s young age and high demands as a laborer. Unicompartmental knee arthroplasty and TKA are not preferred options for this patient because risk for premature failure is high.
Question 89
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings? Review Topic
Explanation
Question 90
A 25-year-old male professional lacrosse player collides with another player, with injury resulting from a knee impacting the athlete’s thigh. He has immediate pain in the mid-thigh area and is unable to return to the game because of difficulty with running. Examination reveals developing swelling in the anterior mid-thigh area. The thigh compartments are soft, and he is able to extend his knee against gravity. Knee flexion at 90° gives him discomfort in the thigh but no knee pain. The knee and hip examinations are otherwise unremarkable. Plain films of the femur are negative. What is the best next step?
Explanation
A. only type 1 collagen.
B. only type 2 collagen.
C. type 1 and type 2 collagen.
D. neither type 1 or type 2 collagen.
The MRI scan shows a full-thickness cartilage defect. When treated with a marrow stimulation technique, such as a microfracture, the reparative tissue is fibrocartilage. Unlike hyaline cartilage, which is composed of only type 2 collagen, fibrocartilage is composed of both type 1 and type 2 collagen.
15- Figures 1 and 2 are the radiographs of a 58-year-old retired laborer who has had many years of right shoulder pain. He initially experienced relief with anti-inflammatory medication over the past year, but this no longer provides him pain relief. He has pain with overhead activities and is dissatisfied with his shoulder function. Examination indicates active and passive forward elevation to 130°, full strength with external rotation, and a negative belly press test. MRI demonstrates an intact rotator cuff. What is the best next step in treatment?
A. Anatomic total shoulder arthroplasty (TSA)
B. Hemiarthroplasty
C. Reverse shoulder arthroplasty
D. Arthroscopy with debridement and biceps tenodesis
The patient has glenohumeral osteoarthritis based on the radiograph. His examination demonstrates limited motion and no significant rotator cuff pathology – full strength with external rotation, negative belly press, and no pseudoparalysis. Of all the answer choices, an anatomic TSA would be the most appropriate treatment option. Hemiarthroplasty does not address glenoid pathology and provides inferior pain relief and function, compared with TSA. A reverse shoulder arthroplasty is utilized for patients with degenerative shoulder changes in conjunction with irreparable rotator cuff pathology. Shoulder arthroscopy with debridement and biceps tenodesis is not appropriate for those with severe degenerative changes of the shoulder.
16- According to the MRI scan shown in Figure 1, which pathologic finding is expected to be encountered during arthroscopy?
A. Figure 2
B. Figure 3
C. Figure 4
D. Figure 5
The sagittal MRI scan is a clear example of a double posterior cruciate ligament (PCL) sign. This sign has a high specificity for a displaced bucket handle tear of the medial meniscus as seen in Figure 4. The other arthroscopic
images show a flap tear of the medial meniscus (Figure 2), anterior cruciate ligament tear (Figure 3), and a full thickness articular cartilage defect (Figure 5). Other less likely causes of a double PCL sign include intermeniscal ligament, meniscofemoral ligaments, loose bodies, osteophytes, and fracture fragments. Correct answer : C 13
17- Figures 1 and 2 are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test, trace effusion, and range of motion from 0 to 85° of knee flexion. Which factor is most contributory to his examination findings?
A. Incorrect graft choice
B. Improper tunnel position
C. Tibial graft-tunnel mismatch
D. Femoral fixation at 80° flexion
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario.
Question 91
Implants composed of polylactic acid are excreted by what system after they are absorbed?
Explanation
Question 92
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?
Explanation
REFERENCES: Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637.
Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423.
Question 93
Figures 42a and 42b show the radiographs of a 52-year-old man who sustained a fall from a motorcycle 6 months ago and now reports pain and stiffness in his left shoulder. What is the most reliable treatment to improve function and comfort of the shoulder?
Explanation
REFERENCES: Gerber C, Lambert SM: Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1996;78:376-382.
Spencer EE Jr, Brems JJ: A simple technique for management of locked posterior shoulder dislocations: Report of two cases. J Shoulder Elbow Surg 2005;14:650-652.
Sperling JW, Pring M, Antuna SA, et al: Shoulder arthroplasty for locked posterior dislocation of the shoulder. J Shoulder Elbow Surg 2004;13:522-527.
Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;34:584-590.
Question 94
Which of the following tendons is the primary antagonist of the posterior tibialis tendon?
Explanation
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
Mann RA: Biomechanics of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 2-36.
Question 95
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
Explanation
Question 96
Figures 1 and 2 are the most recent radiographs of an 18-year-old high school student who sustains an anterior shoulder dislocation playing recreational football. He has a low Beighton score on physical examination. He was closed reduced and underwent a course of physical therapy but had a second dislocation playing recreational basketball. What is the most appropriate course of treatment, with the lowest complication rate, to prevent further dislocation?

Explanation
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
Question 97
- In revision hip arthroplasty, which of the following is the 5- to 10-year reported graft failure rate when using structural acetabular allografts in the repair of acetabular deficiencies?
Explanation
Question 98
A 17-year-old high school athlete comes in with a 6-month history of right midfoot pain. She has been treated with cast immobilization, crutches, and physical therapy. She still has significant pain with activities and cannot participate in sports. Her radiograph is shown in Figure 93a, and MR images are shown in Figures 93b and 93c. What is the most appropriate 79 next step? A B C
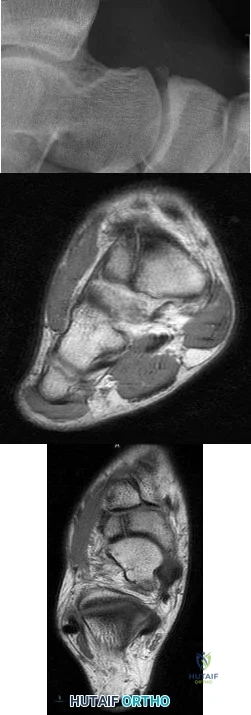
Explanation
RECOMMENDED READINGS
Lee S, Anderson RB. Stress fractures of the tarsal navicular. Foot Ankle Clin. 2004 Mar;9(1):85-104. Review. PubMed PMID: 15062216. View Abstract at PubMed
Anderson RB, Cohen BE. Stress fractures of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 2. 8th ed. Philadelphia, PA: Mosby; 2007:1590-1597.
Question 99
Figures below demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. A further work-up reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MRI with MARS. Revision THA is recommended. The most common complication following revision of a failed metal-on- metal hip arthroplasty is
Explanation
Question 100
An 11-year-old boy reports the acute onset of elbow pain and swelling after pushing his brother. The patient's mother and a younger sibling have experienced numerous fractures. You note that the patient and his mother have blue sclera and normal-appearing teeth. A radiograph of the elbow is shown in Figure 60. This patient's disorder is most likely the result of Review Topic

Explanation
Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). These individuals have blue sclerae, and although the initial fracture usually occurs in the preschool years, it may occur at any age. Furthermore, olecranon apophyseal fractures that occur after relatively minor trauma have been associated with type I OI. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. In this patient, there are no indications that the child has been subjected to abuse. Radiographs of the elbow show no evidence of osteopetrosis (due to abnormal osteoclast function) or rickets (due to a deficiency of vitamin D). Morquio syndrome (characterized by a defect of the enzyme N-Ac-Gal-6 sulfate sulfatase) is not associated with blue sclera.
