Orthopedic Board Review MCQs: Arthroplasty, Fracture & Spine | Practice Part 230

Key Takeaway
This page offers Part 230 of a comprehensive, interactive MCQ bank for orthopedic surgeons and residents. It features 100 verified, high-yield questions, modeled on OITE/AAOS/ABOS exams, with detailed clinical explanations and two learning modes to optimize board certification preparation.
About This Board Review Set
This is Part 230 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 230
This module focuses heavily on: Arthroplasty, Elbow, Fracture, Shoulder, Spine.
Sample Questions from This Set
Sample Question 1: Six weeks after open reduction internal fixation of a closed tibial pilon fracture, a patient has a draining wound with surrounding erythema and swelling. Radiographs show lucency around screws. What is the most appropriate treatment sequen...
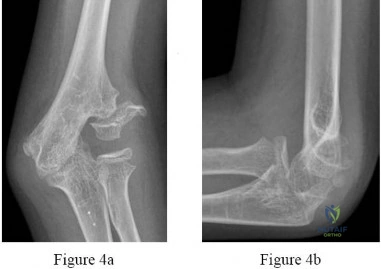
Sample Question 2: Figure 42 shows the radiograph of a 70-year-old woman who has had a painful near ankylosis of her dominant elbow for 1 year. Treatment should consist of...
Sample Question 3: A 63-year-old man has a feeling of generalized clumsiness in his arms and hands, difficulty buttoning his shirt, and gradually worsening gait instability. During examination, his neck is gently passively flexed to end range while he is seat...
Sample Question 4: A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had...
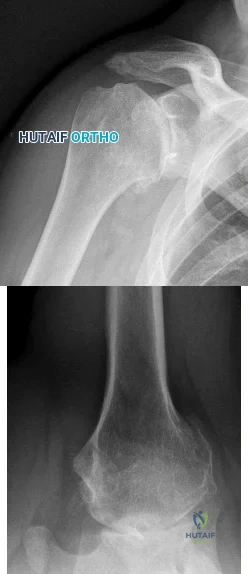
Sample Question 5: A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, an...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Six weeks after open reduction internal fixation of a closed tibial pilon fracture, a patient has a draining wound with surrounding erythema and swelling. Radiographs show lucency around screws. What is the most appropriate treatment sequence?
Explanation
Question 2
Figure 42 shows the radiograph of a 70-year-old woman who has had a painful near ankylosis of her dominant elbow for 1 year. Treatment should consist of
Explanation
REFERENCES: Ramsey ML, Morrey BF: Total elbow arthroplasty for nonunion and dysfunctional instability, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
Sim FH, Morrey BF: Nonunion and delayed union of distal humeral fractures, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
Question 3
A 63-year-old man has a feeling of generalized clumsiness in his arms and hands, difficulty buttoning his shirt, and gradually worsening gait instability. During examination, his neck is gently passively flexed to end range while he is seated. The patient describes an electric shock-like sensation that radiates down the spine and into the extremities. This describes which of the following? Review Topic
Explanation
Question 4
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had
Explanation
Question 5
A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, and has internal rotation to the fifth lumbar vertebra. At 6 months, his motion fails to improve. Radiographs are shown in Figures 18a and 18b. What is the best course of action?
Explanation
REFERENCES: Cuomo F, Checroun A: Avoiding pitfalls and complication in total shoulder arthroplasty. Orthop Clin North Am 1998;29:507-518.
Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 6
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5?
Explanation
REFERENCE: McCullouch JA, Transfeldt EE: Macnab’s Backache, ed 3. Philadelphia, PA, Williams and Wilkins, 1997, pp 569-608.
Question 7
What proteinaceous compound binds to hyaluronic acid to function as an effective boundary molecular layer in articular cartilage?
Explanation
Question 8
A 10-year-old girl has been referred for evaluation of a prominence at the lower cervical spine. The patient is asymptomatic, and the examination reveals no evidence of neurologic abnormality. A radiograph and CT scans are shown in Figures 12a through 12c. What is the most likely diagnosis?
Explanation
REFERENCES: Hsu LC, Leong JC: Tuberculosis of the lower cervical spine (C2 to C7): A report on 40 cases. J Bone Joint Surg Br 1984;66:1-5.
Loder RT: The cervical spine, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 739-789.
Question 9
Which of the following factors has been shown to increase mortality in poly-trauma patients with severe head injuries?

Explanation
Chesnut et al demonstrated that hypotension (SBP <90mmHg) was profoundly detrimental, occurring in 35% of these patients and associated with 150% increase in mortality.
Pietropaoli et al reviewed 53 patients with severe head injuries and required early surgical intervention (surgery within 72 hours of injury). All patients were initially normotensive on arrival. There were 17 patients (32%) who developed intra-operative hypotension and 36 (68%) who remained normotensive throughout surgery. The mortality rate was 82% in the IH group and 25% in the normotensive group.
Question 10
A 23-year-old man cut the dorsal and ulnar aspects of his long finger on a table saw. The dorsal and ulnar skin over the middle phalanx is missing, with a 2-cm x 2-cm area of loss. There is a 50% loss of the extensor tendon (ulnar), and the remaining tendon has no tenosynovium. The physician should recommend irrigation and debridement and
Explanation
The patient has exposed bone and tendon and a partial tendon injury. The remaining radial tendon is satisfactory and no tendon repair is required. The exposed bone and tendon necessitate vascularized tissue coverage. A reversed cross-finger flap from the ring finger is suitable for coverage of the dorsal surface of an adjacent digit.
Question 11
Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?
Explanation
to 18 hours. This is greater than the 1 hour half-life of unfractionated heparin.
Low-molecular-weight heparin offers an advantage over unfractionated heparin by selectively targeting Factor Xa while having a lesser effect on circulating thrombin (Factor IIa). Circulating thrombin Factor IIa is needed for local hemostasis at the site of the surgical wound. Clinical studies have shown a reduction by one third in the incidence of thrombocytopenia with the use of low-molecular-weight heparin. Low-molecular-weight heparin has been shown to demonstrate similar clinical results compared to warfarin with respect to preventing thromboembolic disease after total hip arthroplasty and complications such as bleeding.
REFERENCES: Zimlich RH, Fulbright BM, Friedman RJ: Current status of anticoagulation therapy after total hip and total knee arthroplasty. J Am Acad Orthop Surg 1996;4:54-62.
Colwell CW Jr, Spiro TE, Trowbridge AA, et al: Use of enoxaparin, a low-molecular-weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Torholm C, Broeng L, Jorgensen PS, et al: Thromboprophylaxis by low-molecular-weight heparin in elective hip surgery: A placebo controlled study. J Bone Joint Surg Br 1991;73:434-438.
Question 12
A 26-year-old weight lifter has had increasing pain in his left shoulder for 4 months. His symptoms do not improve with nonsurgical treatment that included activity modification, anti-inflammatory medication, and corticosteroid injections. He undergoes arthroscopic distal clavicle excision with resection of the distal 2.5 cm of clavicle. Three months after surgery, he reports persistent pain and popping in his shoulder. An examination demonstrates anterior and posterior instability of the distal clavicle without gross deformity. Radiographs are unremarkable. What is the most likely cause of distal clavicle instability after surgery?
Explanation
Overresection of the distal clavicle can result in disruption of the acromioclavicular ligamentous complex, which inserts at an average of 22.9 mm from the distal clavicle. A comparison of arthroscopic and open distal clavicle excision demonstrated less pain in the arthroscopic group, with no difference in patient satisfaction or shoulder function between groups. Injuries to the conoid and trapezoid ligaments occur with high-grade acromioclavicular separations, resulting in superior migration of the distal clavicle relative to the acromion. Release of the coracoacromial ligament typically is not performed during distal clavicle excision.

Question 13
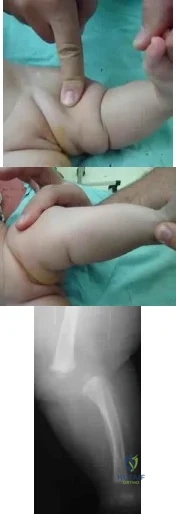
A mother brings in her 6-month-old infant with a knee deformity. The child had previously been treated with serial casting in flexion for 3 month at an outside facility. Examination reveals passive hyperextension to 25° and passive flexion to 15° as shown in Figures A and B respectively. A lateral radiograph of the knee is shown in Figure C. What is the most appropriate next step in treatment? Review Topic
Explanation
Congenital knee dislocation is rare. The etiology is thought to be quadriceps contracture. It is associated with developmental dysplasia of the hip (DDH) and clubfoot (CTEV). In newborn infant, casting or bracing with the knee in flexion
should be performed. If this fails, percutaneous or open VY quadricepsplasty, followed by above-knee casting, is indicated.
Abdelaziz et al. proposed a new grading system (Tarek CDK grading system-see Illustrations A and B) and treatment protocol as follows: (1) Serial casting for Grade 1 regardless of age and in neonates with grade 2 <1mth. If flexion to >90° is achieved within 4 weeks, then serial casting is continued; if range remains <90°, percutaneous quadriceps recession (PQR) is performed. (2) PQR is performed in Grade 2 CDK in infants >1 month of age upon presentation. (3) VY quadricepsplasty is indicated in patients with Grade 3 CDK or in recurrent cases.
Klingele et al. describe ACL shortening and reinforcement in 2 patients with congenital knee dislocation who developed ACL incompetence due to elongation. They conclude that stabilizing and reinforcing the ACL may prevent long-term anterior instability, hyperextension and recurrent deformity.
Figures A and B show the range of motion of the knee (25deg hyperextension to 15deg flexion). Figure C is a lateral radiograph showing congenital dislocation of the knee. Illustrations A and B show the Tarek grading system. Illustration C shows the different techniques of quadricepsplasty (upper row, structures divided and skin incisions used; lower row, how lengthening of the quadriceps mechanism is achieved). The most common PQR is the Roy-Crawford technique. The most common VYQ is the Curtis-Fisher technique.
Incorrect Answers:
Question 14
A 66-year-old male sustains an open crush injury to his right lower leg with significant skin loss. His history is significant for COPD, diabetes controlled with an insluin pump, and testicular cancer treated with bleomycin twenty years ago. A radiograph of the chest shows a pneumothorax which is treated with a thoracostomy tube. Which of the following is not a contraindication to hyperbaric oxygen treatment for this patient?

Explanation
Hyperbaric oxygen therapy potentially can provide enhanced oxygen delivery to peripheral tissues affected by vascular disruption, cytogenic and vasogenic edema, and cellular hypoxia caused by extremity trauma. The idea behind HBO is to provide enhanced oxygen delivery to peripheral tissues affected by vascular disruption, cytogenic and vasogenic edema, and cellular hypoxia caused by extremity trauma.
Greensmith et al provide a review of HBO therapy and discuss the relative and absolute contraindications and indications for this treatment. They report in patients with crush injury or early compartment syndrome, hyperbaric oxygen therapy may reduce the penumbra of cells at risk for delayed necrosis and secondary ischemia. They report that both animal studies and prospective human clinical trials suggest the benefits of such therapy.
Buettner et al found that based on clinical evidence and cost analysis, medical institutions that treat open fractures and crush injuries are justified in incorporating HBO theray as a standard of care.
Illustration A shows an example of a hyperbaric oxygen(HBO) chamber. Incorrect Answers:
Question 15
03 Which of the following findings is one of the diagnostic criteria for diffuse idiopathic skeletal hyperostosis?
Explanation
Diffuse idiopathic skeletal hyperostosis is a common disease, most prevalent in those over 50 years of age. The usual presentation is a middle-aged or older patient with chronic mild pain in the middle to lower back, spinal stiffness, and typical radiographic changes in the thoracic spine. Diffuse idiopathic skeletal hyperostosis is predominantly a radiographic diagnosis with 3 major diagnostic criteria. 1. Flowing ossification along the anterolateral aspect of at least four contiguous vertebrae. 2. Preservation of disk height in the involved vertebral segment; the relative absence of significant degenterative changes, such as marginal sclerosis in vertebral bodies or vacuum phenomenon. 3.
Absence of facet-joint ankylosis; absence of sacroiliac erosion, sclerosis, or intra-articular osseous fusion. Treatment is typically non-operative, with anti-inflammatories, activity modification and PT.
back to this question next question
Question 16
A 72-year-old woman with diabetes mellitus who underwent a total shoulder arthroplasty for degenerative arthritis 5 years ago now reports the sudden onset of shoulder pain following recent hospitalization for pneumonia. Laboratory values show a WBC count of 11,400/mm3 and an erythrocyte sedimentation rate of 52mm/h. What is the most appropriate action?
Explanation
REFERENCES: Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 953-954.
Stinchfield FE, Bigliani LU, Neu HC, et al: Late hematogenous infection of total joint replacement. J Bone Joint Surg Am 1980;62:1345-1350.
Question 17
A year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the
aspiration and proceed to a revision TKA with possible augments on standby.
Question 18
In a polytraumatized patient with a high lactate level, large base deficit, and pulmonary injury, what is the best initial treatment for a femoral shaft fracture?
Explanation
intramedullary nails in the acute setting is to be avoided because of the possibility of increasing the patient's morbidity. Plating is time consuming and leads to blood loss which should be avoided in the severely injured patient. Skeletal traction and supine positioning are detrimental in the trauma patient. Expedient external fixation, resuscitation, and later definitive treatment with an intramedullary nail is considered to be the best choice for the polytraumatized patient with a femoral shaft fracture.
Question 19
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal.
Explanation
Question 20
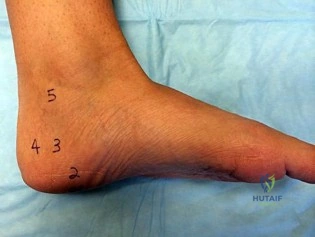
A 30-year-old man who sustained a tibial fracture with a peroneal nerve palsy 2 years ago now has a drop foot and weak eversion of the foot. He reports success with stretching exercises, but he catches his toes when his foot tires. Examination reveals that the foot is plantigrade and supple. What is the next most appropriate step in management?
Explanation
REFERENCES: Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Santi MD, Botte MJ: Nerve injury and repair in the foot and ankle. Foot Ankle Int
1996;17:425-439.
Question 21
A 55-year-old male sustained a Sanders IV intra-articular calcaneus fracture two years ago that was treated nonoperatively. He presents to your office with a mechanical block preventing his ankle from dorsiflexing to neutral, continued severe pain and a widened heel. Radiographs show significant loss of calcaneal height and an incongruous subtalar joint. What is the most appropriate surgical treatment at this time?

Explanation
difficulties, and foot deformity. Foot deformity (collapse of the talus into the posterior facet) can result in tibiotalar neck impingement. Carr et al described a subtalar fusion technique for late complications of calcaneus fractures that were treated conservatively. The subtalar fusion technique involves distraction of the subtalar joint, insertion of a bone block, and rigid screw fixation. The distraction allows correction of the talocalcaneal relationship and regains lost hindfoot height. (A subtalar fusion would address the pain issue but not the other factors.) Chandler et al states that distraction arthrodesis should be considered only if findings of anterior ankle impingement are present, as is true in this case.
Question 22
A B Figures 82a and 82b are the clinical photograph and radiograph of a 60-year-old man with a 30-year history of diabetes complicated by borderline chronic renal failure, heart failure controlled by medication, and bilateral lower extremity neuropathy. He is currently wheelchair bound because of his cardiopulmonary limitations, but uses his legs for transfers. He has had a progressive left ankle deformity that has progressed to the point at which he cannot use his leg for pivot transfers. He is adamant that something should be done to improve his living situation. Which surgical option can best achieve his goal of using the leg for transfers?

Explanation
The indications for surgery in a Charcot joint are an unbraceable deformity or recurrent ulceration despite use of adequate bracing. Any significant varus/valgus deformity of the ankle or hindfoot (as in this patient) is unbraceable, whereas midfoot Charcot deformities usually can be treated nonsurgically. The goal of surgery is to provide a stable aligned foot and ankle to permit activities and reduce risk for recurrent ulceration. This does not mean that there has to be a radiographic fusion because many patients with diabetes achieve a stable nonunion without pain. The only surgical construct that will provide long-term inherent stability and alignment in this situation is use of a hindfoot fusion rod. It provides better stability and purchase than screw fixation and can be left in indefinitely (unlike an external fixator).
RECOMMENDED READINGS
Dalla Paola L, Volpe A, Varotto D, Postorino A, Brocco E, Senesi A, Merico M, De Vido D, Da Ros R, Assaloni R. Use of a retrograde nail for ankle arthrodesis in Charcot neuroarthropathy: a limb salvage procedure. Foot Ankle Int. 2007 Sep;28(9):967-70. PubMed PMID: 17880869. View Abstract at PubMed
Pinzur MS. Benchmark analysis of diabetic patients with neuropathic (Charcot) foot deformity. Foot Ankle Int. 1999 Sep;20(9):564-7. PubMed PMID: 10509683. View Abstract at PubMed Pinzur M. Surgical versus accommodative treatment for Charcot arthropathy of the midfoot. Foot Ankle Int. 2004 Aug;25(8):545-9. PubMed PMID: 15363375. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 87

Figures 83a and 83b are the clinical photographs of a 42-year-old woman with a BMI of 31 who has had a 1-year history of right heel pain.
A
B
Question 23
Which statement is true with respect to acetabular fracture surgery as the time between injury and surgery increases?

Explanation
Question 24
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle?
Explanation
REFERENCES: Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop Relat Res 1999;368:17 -27.
Warner JJ, Navarro RA: Serratus anterior dysfunction: Recognition and treatment. Clin Orthop Relat Res 1998;349:139-148.
Question 25
-T1-weighted, fat-saturated MRI scans are shown in Figures 37a and 37b. What is the next step intreatment?
Explanation
Examination findings of posterior glenohumeral tenderness, decreased internal rotation, and reproduction of symptoms with a posterior stress test indicate a posterior shoulder injury or instability. The jerk test,with the patient seated, positions the arm in forward flexion and internal rotation with elbow flexion. One hand of the examiner is placed on the patient’s distal clavicle and scapular spine and the other hand grasps the elbow. The arm is jerked posteriorly while the shoulder girdle is jerked anteriorly, which creates pain as the posteriorly subluxated humeral head relocates into the glenoid fossa. During the Kim test, the patient is seated with the arm in 90 degrees of abduction. While the arm is elevated 45 degrees diagonally (forward flexion and adduction), the examiner applies an axial load to the elbow and a downward and posterior force to the upper arm. A positive result causes a sudden onset of posterior shoulder pain. A positive jerk test combined with a positive Kim test has a 97% sensitivity for posterior instability. After extensive PT, the patient continues to have examination findings consistent with posterior shoulder injury or instability, so an MRI scan or MRI arthrography would be helpful to assess for any pathology.A subacromial injection is not indicated by this examination, which shows a strong rotator cuff and no demonstrated bursal-sided symptoms. A CT scan can be helpful in scenarios involving bony pathology,but an MRI is indicated at this stage in the evaluation of soft tissue. Although continuing PT may help to abate symptoms, the patient was continuing to have symptoms with PT. The MRI arthrogram shows a complex posterior labrum tear at the inferior to mid glenoid with separation of labrum from the glenoid. Because the examination findings are consistent with the MRI findings and nonsurgical treatment has failed to resolve symptoms, the next step is to recommend surgical treatment with labrum debridement and/or repair. No examination or MRI findings indicate a need for injection, rotator cuff repair, ORIF, or chondroplasty unless incidental intrasurgical findings are found.
Question 26
A 6-year-old boy with severe spastic quadriplegic cerebral palsy is nonambulatory. Examination reveals 10° of hip abduction on the left and 30° on the right with the hips and knees extended. The Thomas test shows 20° of flexion bilaterally, and Ely test results are 3+/4 bilaterally. Radiographs show a center edge angle of 0° on the left and -10° on the right. The neck shaft angles are 170° bilaterally. Which of the following procedures would offer the best results?
Explanation
REFERENCES: Tylkowski CM, Rosenthal RK, Simon SR: Proximal femoral osteotomy in cerebral palsy. Clin Orthop 1980;151:183-192.
Brunner R, Baumann JU: Long-term effects of intertrochanteric varus-derotation osteotomy on femur and acetabulum in spastic cerebral palsy: An 11- to 18-year follow-up study. J Pediatr Orthop 1997;17:585-591.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 27
A 17-year-old girl is involved in a motor vehicle collision and sustains the injury shown in Figures 46a through 46c. She is neurologically intact in her bilateral lower extremities. Definitive treatment should consist of A B C

Explanation
The figures reveal a fracture-dislocation at L1-2. Proper treatment consists of posterior reduction, stabilization, and fusion 2 levels above and below the level of injury. Short-segment stabilization schemes do not stabilize the injury properly, and longer-segment constructs are not necessary. Anterior treatment is not indicated in fracture-dislocations.
RECOMMENDED READINGS
Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. View Abstract at PubMed
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Question 28
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. What is the UKA survivorship for a 55- year-old patient, compared with the survivorship for total knee arthroplasty?
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress
faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 29
When performing a Green transfer for cerebral palsy—flexor carpi ulnaris (FCU) to extensor carpi radialis brevis (ECRB)—in addition to improving wrist extension, what other motion may be improved if the FCU is routed around the ulna instead of through the interosseous membrane?
Explanation
The typical upper extremity deformity in spastic hemiplegic cerebral palsy consists of shoulder internal rotation, elbow flexion, forearm pronation and wrist flexion, and ulnar deviation. The pronation position of the forearm can make bimanual activities more challenging for the child. The wrist flexion and ulnar deviation deformity interferes with finger function and therefore with grasp and release patterns. By transferring the FCU tendon to the ECRB, the deforming force is released, and central wrist extension is augmented. This transfer can lead to a supination moment when it is routed around the ulna to the ECRB insertion on the dorsum of the wrist. Thumb and finger extension are not affected by an FCU-to-ECRB tendon transfer. Forearm supination, not pronation, is potentially improved with this tendon transfer.
Question 30
A 67-year-old woman has a painful, arthritic proximal interphalangeal (PIP) joint, and nonsurgical measures have failed to improve the pain. What implant and joint replacement approach combination has been demonstrated to have the lowest rate of revision surgery?
Explanation
A recent systematic review compared silicone replacement, pyrocarbon replacement, and surface replacement arthroplasty for PIP arthritis. Silicone arthroplasty through a volar approach showed the greatest gains in arc of motion and had the lowest rate of revision surgeries. The rates of revision surgeries from low to high for each type of arthroplasty were 6% for silicone volar, 10% for silicone lateral, 11%
Surface replacement arthroplasty through a volar
for silicone dorsal, 18% for surface replacement dorsal, and 37% for surface replacement volar. Revision surgeries include implant replacement (to silicone or maintaining the surface replacement), arthrodesis, explantation, amputation, and other procedures.
approach showed the highest revision rate, the worst gain in arc of motion, and the greatest extension lag. However, substantial pain relief and higher satisfaction still were reported after surface replacement arthroplasty, regardless of the complications.
Question 31
Steroids are thought to prevent neurologic deterioration after traumatic spinal cord injury by which of the following mechanisms? Review Topic
Explanation
Question 32
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel’s sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Styf J: Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165-169.
Sridhara CR, Izzo KL: Terminal sensory branches of the superficial peroneal nerve: An entrapment syndrome. Arch Phys Med Rehabil 1985;66:789-791.
Styf J: Entrapment of the superficial peroneal nerve: Diagnosis and results of decompression.
J Bone Joint Surg Br 1989;71:131-135.
Question 33
A 68-year-old man with no significant medical history underwent a total knee arthroplasty 4 years ago. A radiograph is shown in Figure 55. He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm 3 . Management should consist of
Explanation
REFERENCES: Swanson KC, Windsor RE: Diagnosis of infection after total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1485-1491.
Hanssen AD, Rand JA, Osmon DR: Management of the infected total knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 1070-1089.
Question 34
A 36-year-old woman with familial neurofibromatosis has an enlarging mass in the posterior thigh. The lesion has slowly increased in size and is now constantly painful. Pressure on the mass causes dysesthesias in the foot. Figures 44a through 44c show T 1 -weighted, STIR, and T 1 -weighted fat-saturated gadolinium scans, respectively. Figure 44d shows a PET scan. What does this lesion most likely represent?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 225-230.
Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4218-4235.
Question 35
A 10-year-old child was referred for spinal curvature and a 2-year history of back pain. She has pain during the day and pain at night that wakes her from sleep and is temporarily relieved with nonsteroidal anti-inflammatory drugs. Examination shows very tight hamstrings and an irritative spinal curvature. Figures 71a through 7Id show radiographs, a bone scan, and a CT scan. What is the most appropriate treatment?
Explanation
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, et al: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-
Question 36
The bone avulsion shown in Figure 32 has a high correlation with tearing of the
Explanation
REFERENCES: Bach BR, Warren RF: Radiographic indicators of anterior cruciate ligament injury, in Feagin JA (ed): The Crucial Ligaments. New York, NY, Churchill Livingston, 1988, pp 301-327.
Segond P: Recherches cliniques et experimentales sur les epanchements sanguins du genou par entorse. Prog Med (Paris) 1987;7:297.
Johnson LL: Lateral capsular ligament complex: Anatomical and surgical considerations. Am J Sports Med 1979;7:156-160.
Question 37
What risk factor is most associated with progression of idiopathic scoliosis to a curve requiring surgery? Review Topic
Explanation
Question 38
All of the following are true statements regarding compartment syndrome in the pediatric patient EXCEPT:

Explanation
Level 4 evidence by Bae et al reviewed 33 children with compartment syndrome. They found that all 10 compartment syndrome patients that had access to nurse or patient controlled analgesia (PCAs), during their initial evaluation, demonstrated an increasing requirement for pain medication.
Matsen et al reviewed 24 children with compartment syndrome with the most common causes being fracture, vascular injury, and tibial osteotomy. The study concluded that is imperative that a compartment syndrome be identified and treated as promptly as possible.
Question 39
Stability at the atlanto-occipital joint is provided mainly by
Explanation
REFERENCES: Werne S: Studies in spontaneous atlas dislocation. Acta Orthopaedica Scandinavica 1977;23(supplement).
Jarrett PJ, Whitesides TE Jr: Injuries of the cervicocranium, in Browner BD, Jupiter JB, Levine AM, Trafton PG (eds): Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 665-697.
Question 40
A 58-year-old man has a painful, warm, erythematous and fluctuant area over his left olecranon. An aspiration would be most likely to reveal
Explanation
Question 41
Figure 99 is the radiograph of an 18-year-old National Collegiate Athletic Association Division I basketball player who jumped for a basket. After landing, he was unable to put weight on his left great toe. He developed pain, swelling, and ecchymosis maximally around the sesamoids. When assessing stability of the first metatarsophalangeal joint, he appears to have more laxity on the left. What is the best next step?

Explanation
This patient jumped on his forefoot and landed with pain in his great toe. His radiograph shows possible increased space between the sesamoids and the base of the phalanx. A comparison radiograph on the other side will reveal if this position is normal for this patient. If findings are asymmetric, turf toe injury is a possibility based on this patient's symptoms and mechanism of injury.
RECOMMENDED READINGS
Waldrop NE 3rd, Zirker CA, Wijdicks CA, Laprade RF, Clanton TO. Radiographic evaluation of plantar plate injury: an in vitro biomechanical study. Foot Ankle Int. 2013 Mar;34(3):403-8. doi: 10.1177/1071100712464953. Epub 2013 Jan 14. PubMed PMID: 23520299. View
Abstract at PubMed
McCormick JJ, Anderson RB. The great toe: failed turf toe, chronic turf toe, and complicated sesamoid injuries. Foot Ankle Clin. 2009 Jun;14(2):135-50. doi: 10.1016/j.fcl.2009.01.001. Review. PubMed PMID: 19501799. View Abstract at PubMed
Question 42
Ulnohumeral distraction interposition arthroplasty is considered the most appropriate treatment for which of the following patients?
Explanation
REFERENCES: Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Mansat P: Surgical treatment of the rheumatoid elbow. Joint Bone Spine 2001;68:198-210.
Question 43
-Video 3 shows the physical examination of the right hip of a 14-day-old full-term female infant. There is no history of breech presentation, she was born vaginally, and is the second child born to her mother. She is otherwise healthy and has been eating and gaining weight appropriately. What is the most appropriate course of action at this time?
Explanation
Question 44
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
REFERENCES: Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JS (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 45
An 18-year-old collegiate football player injures his right shoulder during a tackle. He reports pain and numbness in the shoulder and numbness radiating to his fingers. His symptoms improve within 15 minutes and he has no residual symptoms. This condition is best known as
Explanation
REFERENCES: Safran MR: Nerve injury about the shoulder in athletes. Part 2: Long thoracic nerve, spinal accessory nerve, burners/stingers, thoracic outlet syndrome. Am J Sports Med 2004;32:1063-1076. Aval SM, Durand P Jr, Shankwiler JA: Neurovascular injuries to the athlete’s shoulder: Part I. J Am Acad Orthop Surg 2007;15:249-256.
Question 46
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
REFERENCE: Herring JA (ed): Tachjians Pediatric Orthopedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 2, p 984.
Question 47
Figure 11 shows the radiograph of a 3-year-old girl who sustained a proximal radius injury. Appropriate initial management should include
Explanation
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39.
Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Gonzalez-Herranz P, Alvarez-Romera A, Burgos J, et al: Displaced radial neck fractures in children treated by closed intramedullary pinning (Metaizeau technique). J Pediatr Orthop 1997;17:325-331.
Question 48
When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral base of the proximal phalanx of the great toe. This conjoined tendon is made up of what two muscles?
Explanation
REFERENCES: Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983, chapter 5.
Question 49
Refers to the effectiveness of various antibiotics against a particular microorganism.
Explanation
Knowledge of the basic nomenclature of antibiotic use is important to effectively treat patients and communicate with colleagues. The effectiveness of an antimicrobial against an infecting organism is measured by the MIC, which refers to the concentration needed to prevent growth of a microorganism on culture medium, and MBC, which is the smallest concentration of the antibiotic necessary to kill the microorganism in culture. Typically, an antibiotic is considered bactericidal if the MBC is no more than 4 times the MIC. The spectrum of antimicrobial coverage refers to an agent’s effectiveness against a range of bacteria. An antibiogram refers to the tabulation of prevalence of different bacteria in a specific setting or specific patient population. Antibiotic susceptibility and resistance refers to the bacteria’s ability to be affected or unaffected by a given antibiotic.

Question 50
Figures 1 and 2 are the radiographs of a 55-year-old man who has a 3-year history of right shoulder pain. He has maximized nonoperative management and is interested in operative treatment. He had an open Bankart repair 20 years ago and did well until a few years ago. What is most important to know when deciding on the best surgical treatment for this patient?
Explanation
Although the radiographs do not reveal any obvious signs of rotator cuff failure, the patient had had an open Bankart 20 years ago. The integrity of the subscapularis tendon following a previous open shoulder procedure is crucial in deciding which type of arthroplasty to consider. Range of motion and infraspinatus strength do not affect the decision-making process, assuming the rotator cuff is intact. Activity level can be important when deciding whether to proceed with an arthroplasty, but it is not as important as the rotator cuff integrity when choosing which
arthroplasty to use.
Question 51
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of Review Topic

Explanation
Question 52
During a transperitoneal approach to the L5-S1 interspace, care must be taken to protect the superior hypogastric plexus from injury. Which of the following techniques reduces the risk of neurologic injury?
Explanation
REFERENCE: Transperitoneal midline approach to L4-S1, in Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer Verlag, 1983, pp 123-129.
Question 53
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?
Explanation
REFERENCES: Brodsky AE, Khalil MA: Talar compression syndrome. Am J Sports Med 1986;14:472-476.
Wredmark T, Carlstedt CA, Bauer H, Saartok T: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Question 54
A 62-year-old active man returns for routine follow-up 16 years after hip replacement. He has no hip pain. Radiographs reveal a well-circumscribed osteolytic lesion around a single acetabular screw. All hip components are perfectly positioned. Comparison radiographs obtained 6 months later show an increase in the size of the osteolytic lesion. CT depicts a well-described lesion that is 3 cm at its largest diameter and is localized around one screw hole with an eccentric femoral head. What treatment is appropriate, assuming that well-fixed cementless total hip components are in place?
Explanation
Given a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected from liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings arise during revision surgery. Here, complete cup revision is not warranted, considering the appropriate implant position. Beaulé and associates reviewed 83 consecutive patients (90 hips) in whom a well-fixed acetabular component was retained in a clinical scenario such as the one described. No hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, acetabular component revision may be indicated.
Question 55
A 44-year-old man sustains the injury shown in Figures 1 through 3. What is the most appropriate treatment?

Explanation
Reduction, either open or closed, with internal fixation (pinning) is the recommended treatment for the majority of these injuries. Closed reduction with pinning is most often performed for acute injuries. Open reduction with pinning is performed for those injuries that cannot be reduced by closed means or those with a delayed presentation. Four cases of successful closed reduction and splinting, all performed upon presentation in the emergency department, have been described by Storken and associates, but the authors note that their review of three prior reports uncovered cases of secondary dislocation, which required surgical stabilization. One of the dislocations occurred 4 months after the reduction. They assert that an indication for primary ORIF is a CMC dislocation associated with major fractures. Primary arthrodesis can be considered in cases with severe intra-articular comminution, but this procedure substantially limits the ability of the hand to increase and decrease the transverse metacarpal arch, which is an important functional movement. It can also lead to osteoarthritis of the triquetrohamate joint. Suspension arthroplasty has been described for old fracture-dislocations of the fifth CMC joint, using a partial slip of the extensor carpi ulnaris.




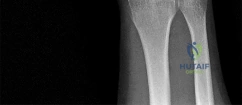




Question 56
Figures 1 and 2 show the intraoperative photographs obtained from a man who is undergoing open reduction and internal fixation of a fifth carpometacarpal joint fracture dislocation. If the structure marked with an arrow in Figure 2 is cut, the patient can expect to experience
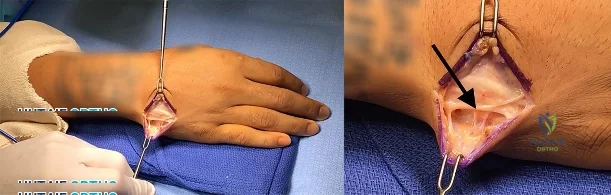
Explanation
The arrow in Figure 2 marks the dorsal sensory branch of the ulnar nerve. Injury to this nerve results in sensory loss of the dorsal ulnar palm and the dorsal small and ring finger digits. The dorsal sensory branch of the ulnar nerve exits the main ulnar nerve at an average distance of 8.3 cm from the proximal border of the pisiform. It becomes subcutaneous on the ulnar aspect of the forearm at an average distance of 5
cm from the proximal edge of the pisiform. It then travels dorsal to the extensor carpi ulnaris tendon to innervate the dorsal ulnar hand and the dorsal ring and small digits. Injuries to this nerve can occur from open and arthroscopic procedures (such as triangular fibrocartilage complex repair) as well as from procedures requiring percutaneous pinning. Care must be taken to identify and protect this nerve to avoid the complications of numbness and possible neuroma formation. The inability to extend the small finger would be caused by an injury to the extensor tendon(s) in this area, and the inability to abduct the small finger would require an injury to the abductor digiti minimi muscle/tendon unit or the ulnar nerve motor branch, which is located on the volar aspect of the proximal palm. Clawing of the small and ring fingers would be caused by absent intrinsic function due to an injury to the ulnar motor nerve branch located on the volar proximal palm.
Question 57
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?
Explanation
REFERENCES: Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Warner JJ, Higgins L, Parsons IM, et al: Diagnosis and treatment of anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2001;10:37-46.
Question 58
An 82-year-old man is seen in consultation after being admitted for a fall from ground level. There was no loss of consciousness and the patient recalls striking his head and sustaining a hyperextension-type injury to the cervical spine. Examination reveals an 8-cm head laceration with only mild axial neck tenderness. He has generalized weakness throughout the upper extremities and maintained motor function of the lower extremities. There are no obvious sensory deficits, and the bulbocavernous reflex and deep tendon reflexes are maintained. What is the most appropriate diagnosis at this time?
Explanation
REFERENCES: Penrod LE, Hegde SK, Ditunno JF: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Harrop JS, Sharan A, Ratliff J: Central cord injury: Pathophysiology, management, and outcomes. Spine J 2006;6:198S-206S.
Question 59
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?
Explanation
REFERENCE: Leffert RD: Anatomy of the Brachial Plexus in Brachial Plexus Injuries. Churchill Livingstone, New York, NY, 1985.
Question 60
Hamstring lengthening and posterior transfer of the rectus femoris will be most successful in a patient with cerebral palsy who has which of the following gait abnormalities?
Explanation
REFERENCES: Gage JR, Perry J, Hicks RR, Koop S, Werntz JR: Rectus femoris transfer to improve knee function of children with cerebral palsy. Dev Med Child Neurol 1987;29:159-166.
Sutherland DH, Santi M, Abel MF: Treatment of stiff-knee gait in cerebral palsy: A comparison by gait analysis of distal rectus femoris transfer versus proximal rectus release. J Pediatr Orthop 1990;10:433-441.
Question 61
A B C Figures 91a through 91c are CT images of a 76-year-old man who was involved in a motor vehicle collision. Which of the following scenarios would pose a contraindication to closed reduction of this injury prior to MR imaging?

Explanation
This patient has bilateral jumped facet joints at C6-7. Although MR imaging is useful for revealing disk herniations, cord injuries, and bony fragments, early closed reduction to restore anatomic alignment may be attempted prior to MR imaging because reduction will decrease pressure on the cord. There have been reports of catastrophic outcomes with closed reduction in patients who are intubated when disk fragments are pushed into the spinal cord. Consequently, closed reduction should be attempted only in awake and cooperative patients for whom neurologic status monitoring is possible. MR imaging is generally performed after reduction is attempted (successful or not).
RECOMMENDED READINGS
Initial closed reduction of cervical spine fracture-dislocation injuries. Neurosurgery. 2002 Mar;50(3 Suppl):S44-50. Review. PubMed PMID: 12431286. View Abstract at PubMed Radcliff K, Sonagli MA, Delasotta L, Singh N, Morrison E, Levine AM, Vaccaro AR. Cervical facet fractures and dislocations. In: Zigler JE, Eismont FJ, Garfin SR, Vaccaro AR, eds. Spine Trauma. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2011:441-464.
Vaccaro AR, Falatyn SP, Flanders AE, Balderston RA, Northrup BE, Cotler JM. Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine (Phila Pa 1976). 1999 Jun 15;24(12):1210-7. PubMed PMID: 10382247. View Abstract at PubMed
Wimberley DW, Vaccaro AR, Goyal N, Harrop JS, Anderson DG, Albert TJ, Hilibrand AS. Acute quadriplegia following closed traction reduction of a cervical facet dislocation in the setting of ossification of the posterior longitudinal ligament: case report. Spine (Phila Pa 1976). 2005 Aug 1;30(15):E433-8. PubMed PMID: 16094262. View Abstract at PubMed
Question 62
The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the
Explanation
REFERENCES: Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F: Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577-583.
Moser RP Jr, Madewell JE: An approach to primary bone tumors. Radiol Clin North Am 1987;25:1049-1093.
Question 63
Botulinum toxin is used to treat vasospastic disorders of the hand such as the Raynaud phenomenon to improve digital perfusion and reduce pain. Botulinum toxin enables which transmitter to be unopposed, resulting in vasodilation?
Explanation
Nitric oxide is the only transmitter listed that is not inhibited by botulinum toxin. Substance P and glutamate are inhibited by botulinum toxin from release by pain nociceptors, thus reducing pain. Fonseca and associates have postulated that botulinum toxin inhibits the RhoA kinase pathway by blocking reactive oxygen species, which in turn does not allow actin/myosin to activate, thus preventing vasoconstriction of smooth muscle. Blocking the RhoA kinase pathway allows the action of nitric oxide to be unopposed, causing vasodilation. Nitric oxide is a potent vasodilator. Thus, botulinum toxin promotes nitric oxide activity to increase vasodilation.
Question 64
below show the radiographs, MRI, and MR arthrogram obtained from a year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. What is the primary cause of a cam deformity?
Explanation
Question 65
A 50-year-old patient underwent multiple débridements for an open radial shaft fracture with bone loss. The bed currently shows no evidence of infection but has a 14-cm diaphyseal bone defect. The most appropriate treatment includes open reduction and internal fixation along with
Explanation
The patient developed a large bone defect after undergoing multiple débridements for an open fracture. The most appropriate graft in this setting is a vascularized bone graft. Considering the length of the defect, a free vascularized fibular graft would be a suitable graft. The indications for a vascularized bone graft include infection, inadequate vascularity of the surrounding tissues, bone defects larger than 6 centimeters, and previous failed bone grafts. The osteocytes survive in the vascularized graft, allowing primary bone healing and thereby limiting a loss of graft strength. In contrast, nonvascularized bone graft heals by creeping substitution with a loss of its initial strength. Calcium sulfate pellets and calcium phosphate cement are synthetic bone substitutes with osteoconductive properties. Their role in fracture healing is limited. Demineralized bone matrix is the matrix remaining after allograft undergoes decalcification processing. These products alone would not be optimal in the treatment of such a large bone defect.
Question 66
A 45-year-old woman with a history of rheumatoid arthritis has C1-C2 instability with neurologic deterioration. Her posterior atlanto-dens interval is 10 mm. Which fixation technique will be the most biomechanically sound to facilitate fusion across the atlanto-axial junction?
Explanation
C1-C2 transarticular screw fixation is 10-fold stiffer than wiring constructs, particularly in rotation; eliminates the need for postsurgical halo use; and is associated with reported fusion rates to a maximum of 100% for bilateral screws and 95% for unilateral fixation. All of the other fusion techniques mentioned are associated with a pseudarthrosis rate of at least 30%.
RECOMMENDED READINGS
Stock GH, Vaccaro AR, Brown AK, Anderson PA. Contemporary posterior occipital fixation. J Bone Joint Surg Am. 2006 Jul;88(7):1642-9. PubMed PMID: 16841419. View Abstract at PubMed
Sim HB, Lee JW, Park JT, Mindea SA, Lim J, Park J. Biomechanical evaluations of various c1-c2 posterior fixation techniques. Spine (Phila Pa 1976). 2011 Mar 15;36(6):E401-7. doi: 10.1097/BRS.0b013e31820611ba. PubMed PMID: 21372651. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 43
Figure 37 is the lateral radiograph of a 71-year-old woman who has pain with ambulation that improves when she sits down. She had similar symptoms 2 years earlier when she underwent an L3-L5 posterior spinal fusion. Upon examination she has good range of hip and knee motion, 5/5 motor function, and normal sensation of her lower extremities. She has negative bilateral straight-leg raise findings and her knees slightly flex to stand upright
Question 67
When comparing arthroscopic lavage and knee debridement with placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?
Explanation
Excluding a diagnosis of meniscal tear, loose body, or mechanical derangement, treating knee osteoarthritis of indeterminate cause with arthroscopic lavage and debridement has been found to provide no discernable benefit to offset the risk of surgery. The effects of arthroscopy have not been clinically significant in the vast majority of patient-oriented outcomes measures for pain and function at multiple
times between 1 week and 2 years after surgery.
Question 68
Limited weight bearing usually is recommended following open reduction and internal fixation of intra-articular lower extremity fractures. A bone graft, or bone graft substitute is often placed in the metaphyseal void beneath the reduced articular fragments. Which of the following bone grafts or bone graft substitutes will most likely permit earlier weight bearing without subsidence of the articular reduction?
Explanation
Question 69
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10°. Initial management should consist of
Explanation
REFERENCES: Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
Franco AH: Pes cavus and pes planus: Analyses and treatment. Phys Ther 1987;67:688-694.
Question 70
An axial T 1 -weighted MRI scan of the pelvis is shown in Figure 35. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, et al (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System,
ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 71
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?
Explanation
REFERENCE: Perlik PC, Guilford WB: Magnetic resonance imaging to assess vascularity of scaphoid nonunions. J Hand Surg Am 1991;16:479-484.
Question 72
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
REFERENCES: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: How do these ankles function over time? J Bone Joint Surg Am 2003;85:287-295.
Question 73
What is the preferred treatment of a symptomatic curly toe deformity in a 6-year-old child?
Explanation
REFERENCES: Hamer A, Stanley D, Smith TW: Surgery for curly toe deformity: A
double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood.
J Bone Joint Surg Br 1984;66:770-771.
Question 74
Figures 1 through 5 are the MR images of a 12-year-old boy with left lateral-sided knee pain following a football injury. He has a several-year history of recurrent knee pain that improves with rest. An examination reveals a moderate effusion. Range of motion is 0° to 90° and is limited by pain in deep flexion. He has tenderness to palpation along the lateral joint line, and no instability is noted. What other finding may be noted in patients with this diagnosis?

Explanation
discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.
Question 75
Figure 88 is the radiograph of a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?
Explanation
Based on the fact that the fracture is occurring around the stem (type B) and the stem is clearly loose (type B2), the appropriate treatment is removal of the in situ stem (which is loose), ORIF of the femur (cerclage wires, cables, or a plate would be acceptable), and insertion of a longer revision stem (a tapered fluted modular titanium or fully porous coated cylindrical stem) to bypass the fracture. All other responses are incorrect because they provide inappropriate treatment options for a Vancouver B2 fracture.
Question 76
A 68-year-old man reports a 4-week history of progressive left-sided lower back and hip pain. The pain is in the posterior buttock region with radiation to the groin and to the left anterior knee region. The pain is aggravated with walking and improves with rest. There is no history of previous trauma. Radiographs are seen in Figures 14a and 14b, and MRI scans are seen in Figures 14c through 14e. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2007, pp 339-361.
Spivak JM, Connolly PJ (ed): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 43-56.
Question 77
A 27-year-old male competitive soccer player reports a 1-year history of pain in the adductor region that has prevented him from playing. Examination reveals tenderness about the adductor attachment to the pelvis, and pain at the same site with resisted contraction of the adductors. There is no tenderness over the hip joint and no signs of a sports hernia. Radiographs are normal. MRI does not show any evidence of enthesopathy. What is the next best step in management?
Explanation
REFERENCES: Schilders E, Bismil Q, Robinson P, et al: Adductor-related groin pain in competitive athletes: Role of adductor enthesis, magnetic resonance imaging, and entheseal pubic cleft injections. J Bone Joint Surg Am 2007;89:2173-2178.
Robinson P, Barron DA, Parsons W, et al: Adductor-related groin pain in athletes: Correlation of MR imaging with clinical findings. Skelet Radiol 2004;33:451-457.
Question 78
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior knee pain, a trace effusion, a 2+ posterior drawer, a grade 1A Lachman, no valgus laxity, and negative dial tests at 30° and 90°. What is the best treatment strategy at this time?
Explanation
A. Biceps tenotomy
B. Loose body removal
C. Latissimus dorsi transfer
D. Reverse total shoulder arthroplasty
Question 79
A year-old patient fell 3 weeks after undergoing a total hip arthroplasty using cementless fixation of the femoral component. She sustained a comminuted Vancouver type B-2 fracture with displacement of the calcar fragment. What is the best treatment option?
Explanation
The patient has an acute postoperative fracture of the proximal femur with subsidence. It is also common that the stem retroverts relative to the femur. It is most often seen in proximally porous coated stems within 90 days of surgery, one paper found it to occur 0.7% of the time in modern implants. There is always a debate whether this is a missed intraoperative fracture, or a new fracture that has resulted from an event of increased hoop stresses. Removal of the primary stem, placement of a diaphyseal engaging
stem (most frequently a tapered-fluted stem), and cabling of the fracture is the most successful treatment.
Question 80
An otherwise healthy 32-year-old man who underwent an uneventful L5-S1 lumbar microdiskectomy 6 weeks ago now reports increasing and severe back pain that awakens him from sleep. Examination reveals a benign-appearing wound, and the neurologic examination is normal. Laboratory studies show an erythrocyte sedimentation rate (ESR) of 90 mm/h and a WBC of 9,000/mm3. Plain radiographs are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 81
A 5-year-old boy reports intermittent left elbow pain. History reveals that he injured his elbow 4 months ago, but had no treatment. He is now using his arm normally but reports pain almost daily. Examination reveals tenderness over the lateral epicondyle and a prominence is evident. Range of motion is from -5 degrees to 120 degrees. Radiographs are shown in Figure 67. Management should include
Explanation
REFERENCES: Wattenbarger JM, Gerardi J, Johnson CE: Late open reduction internal fixation of lateral condyle fractures. J Pediatr Orthop 2002;223:94-398.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 82
…The patient underwent an uneventful arthroscopic repair and did well until 1 year later when she crashed during a race. She tore her anterior cruciate ligament (ACL) and underwent reconstruction. Followup after her successful ACL reconstruction reveals complaints of new shoulder pain and posterior instability from using crutches after her ACL surgery. A new MRI scan is shown in Figure 24. What factors are most likely associated with this patient’s recurrence?
Explanation
Question 83
A 27-year-old runner training for his first marathon reports lateral knee pain after an unusually long training run. He states that the most significant pain occurs while running downhill. Examination of the patient while he is laying on the unaffected side reveals increased pain when manual pressure is applied to the lateral femoral epicondylar area during knee range of motion of 30° to 45°. What is the most likely diagnosis?
Explanation
REFERENCES: Noble CA: The treatment of iliotibial band friction syndrome. Br J Sports Med 1979;13:51-54.
James SL: Running injuries to the knee. J Am Acad Orthop Surg 1995;3:309-318.
James SL, Jones DV: Biomechanical aspects of distance running, in Cavanagh PR (ed): Biomechanics of Distance Running. Champaign, IL, Human Kinetic Books, 1990, pp 249-269.
Question 84
A 45-year-old man reports a history of a popping sensation and pain in the right shoulder while lifting boxes 6 months ago. The pain has persisted with loss of motion of the shoulder. Radiographs and MRI scans are shown in Figures 47a through 47d. Which of the following studies is likely to produce a significant positive result? Review Topic

Explanation
Question 85
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?
Explanation
REFERENCES: Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.
Question 86
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509.
Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Vaccaro AR, Watkins B, Albert TJ, et al: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-703.
Question 87
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow. Which type of contraction of the involved muscle most likely resulted in this lineman's injury?
Explanation
followed by the ECU, EDQ, and, finally, the EIP.
Question 88
A 28-year-old woman has had pain in her hand and mild swelling of the little finger for the past 2 months. A radiograph is shown in Figure 41a, and the biopsy specimen is shown in Figures 41b and 41c. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 225.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 227.
Question 89
Reconstruction of the injured structure is performed. After surgery, the patient initially notes limitation in motion, and later develops recurrent instability of the knee. Which factor most likely contributed to the development of instability?
Explanation
The anteromedial bundle originates on the anterior and proximal aspect of the lateral femoral condyle and inserts on the anteromedial aspect of the anterior cruciate ligament (ACL) footprint on the proximal tibia. The posterolateral bundle originates posterior and distal to 63 the anteromedial bundle and inserts on the posterolateral aspect of the tibial footprint. The fibers are parallel when the knee is in an extended position. As the knee moves into flexion,
the fibers of the anteromedial bundle rotate externally with respect to the posterolateral bundle. The anteromedial bundle is tensioned in both flexion and extension. The posteromedial bundle is tensioned in extension, but relaxes as the knee moves into flexion.
The lateral meniscus is more commonly injured with an acute injury to the ACL. The medial meniscus is injured more commonly when the ACL is chronically unstable.
The ACL is an intra-articular and intrasynovial structure. It is innervated by posterior articular branches from the tibial nerve. Innervation of the ACL involves several types of mechanoreceptors (Ruffini, Pacini, Golgi tendon, and free-nerve endings) that may contribute to proprioceptive function of the knee and modulation of quadriceps function.
Injury to the ACL is predominantly associated with instability to anterior translation of the tibia in extension. The ACL plays a secondary role to limit internal rotation of the tibia, and a loss of ACL stability is confirmed by the reduction of the tibia from a position of anterior translation and internal rotation (pivot shift). The radiographs demonstrate anterior placement of the femoral tunnel. The convex shape of the lateral femoral condyle can make it more difficult to visualize the anatomic femoral origin of the ACL. Failure to identify the
anatomic footprint can result in anterior placement of the femoral tunnel. Anterior ACL graft placement can result in its impingement against the posterior cruciate ligament and early limitation of knee flexion. Over time, impingement on the graft may result in stretching of the graft and recurrent knee instability symptoms.
RECOMMENDED READINGS
Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. Epub 2005 Oct 19. Review. PubMed PMID: 16235056. View Abstract at PubMed
Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Oct;14(10):982-92. Epub 2006 Aug 5. Review. PubMed PMID: 16897068. View Abstract at PubMed
Question 90
An MRI scan
Explanation
Question 91
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
REFERENCES: Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 92
A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management? Review Topic
Explanation
in management should be MRI. If the findings are negative, suspicion of nerve injury should lead to electromyography.
Question 93
The mother of a 2-year-old boy reports that he had pain in the right hip all night and refuses to walk on the leg this morning. He is afebrile. Examination reveals pain on hip extension and adduction, but he is able to internally and externally rotate the hip approximately 20 degrees in each direction without pain. Laboratory studies reveal a WBC count of 7,400/mm 3 , with 62% polymorphonuclear neutrophil leukocytes. The AP radiograph shown in Figure 15 reveals a left teardrop distance of 8 mm, while the right side measures 10 mm. Which of the following diagnostic studies will best help confirm the diagnosis?
Explanation
REFERENCE: Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990, pp 1415-1435.
Question 94
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
Explanation
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
Question 95
1mg/L (normal 1-3mg/L). Knee aspiration yields WBC of 673 cells/mm(3) with 30% polymorphonucleocytes, and a negative gram stain. There is no surrounding erythema but there is a 1cm area at the inferior aspect of the wound that has a large amount of serous drainage able to be expressed. She has a painless range of motion is 0° to 117°. What would be the next most appropriate step in management?
Explanation
Malinzak et al performed a Level 4 review of 8494 patients undergoing a total knee arthroplasty. They found that patients with a body mass index greater
than 50 had an increased odds ratio of infection of 21.3 (P < .0001). Diabetic patients were 3 times as likely to become infected compared to nondiabetic patients (P = .0027).
Rasul et al performed a Level 4 review of 24 patients for a duration of 2 years with total knee arthroplasty infections. They found that patients with chronic (>1 month) deep infections were successfully treated 75% with debridement, intravenous antibiotics, tobramycin-impregnated polymethylmethacrylate beads, and delayed exchange arthroplasty with mean interval of staged reimplantation being 8 weeks.
OrthoCash 2020
A 47-year-old man presents with 1 week of left leg pain. 6 months prior he underwent a vascularized free-fibula bone graft from his left leg to his right hip for avascular necrosis. The pain is located at the level of his donor site and is worse with weight-bearing and relieved by rest. Physical exam shows focal tenderness over his tibia. A lateral radiograph from the day of presentation is shown in Figure A. WBC, ESR, and CRP are all within normal limits. What is the next best step in management to confirm the diagnosis?

Compartment pressure measurements
CT scan
MRI scan
Ultrasound to rule out deep abscess
Bone biopsy
The clinical presentation is suspicious for a stress fracture of the tibia following free-fibula bone grafting. If plain radiographs are negative, more sensitive imaging such as a MRI or bone scan should be performed.
Tibial stress fractures are a known complication following free-fibula bone grafting. Radiographs may be normal (as is the case in figure A), or might show the "dreaded black line" and/or new periosteal bone formation. If a stress fracture is confirmed with imaging, appropriate management would then consist of protective weight bearing until symptoms subside.
Pacifico et al detail a case report of tibial stress fractures after vascularised free-fibula graft to the mandible. They report non-traumatic stress fracture to the tibia following a vascularised free-fibula graft is an uncommon but important complication.
Ivey et al detail a case report of a tibial stress fracture after vascularised free-fibula graft for repair of non-union of the humerus.
Emery et al report a case-series of 5 patients who sustained tibial stress fractures after a graft had been obtained from the ipsilateral fibula for use in anterior reconstruction of the spine. They theorize that the increased load the tibia bears as a result of the missing fibular graft may result in stress fractures.
Illustration A shows new periosteal bone formation on the lateral cortex of the tibia consistent with a stress fracture.
Incorrect Answer Choices:
1: While compartment syndrome is on the differential diagnosis, his signs and symptoms are not most consistent with that diagnosis.
2: While CT scan may show evidence of a stress fracture, MRI/bone scans have been shown to be superior methods for detection.
4: As infectious laboratories are normal, an ultrasound to rule out a deep abscess would likely be negative.
5: Bone biopsy is not appropriate without evidence of a lesion or concern for
osteomyelitis.

OrthoCash 2020
A 65-year-old female with a history of developmental dysplasia of the hip (DDH) undergoes a total hip arthroplasty (THA) utlizing a posterior approach. Following THA, she notices an inability to dorsiflex the ankle of her operative extremity. Her pre-operative and postoperative radiographs are seen in figues A and B. Which of the following intra-operative techniques could have avoided this complication in this patient?

Utilization of an anterior approach
Modular components
Use of a larger femoral head
Femoral shortening osteotomy
Acetabular osteotomy
Patients with DDH undergoing THA are at risk for post-operative sciatic nerve palsy due to intra-operative limb lengthening which increases tension on the sciatic nerve. Appropriate management after discovering a sciatic nerve palsy
after surgery should include immediate knee flexion and hip extension to decrease tension on the sciatic nerve. Sciatic nerve palsy following THA most commonly only affects the common peroneal nerve branch, and spares the tibial nerve and can present as an inability to dorsiflex and evert the ankle.
Farrell et al retrospectively looked at the risk factors for motor nerve palsy after THA. They found while motor nerve palsy is uncommon following primary THA, it can be a devastating complication. Some risk factors include: preoperative diagnosis of developmental dysplasia of the hip, posttraumatic arthritis, the use of a posterior approach, lengthening of the extremity, and use of an uncemented femoral implant. In their review, many of the motor nerve deficits did not fully resolve.
Barrack et al reviewed neurovascular complications following THA. They stated that sciatic nerve injury is the most common nerve injury following THA utilizing a posterior approach. In comparison, femoral nerve injury is much less common and is usually from an anterior approach.
OrthoCash 2020
A cane held in the contralateral hand reduces joint reactive forces through the affected hip approximately 50% by which of the following mechanisms?
Reducing hip abductor muscle pull
Increasing hip flexor muscle pull
Moving the center of rotation for the femoroacetabular joint
Increasing joint congruence at the femoroacetabular joint
Moving the center of gravity posterior to the second sacral vertebra Corrent answer: 1
A cane held in the contralateral hand reduces joint reactive forces through the affected hip up to 50% by reducing abductor muscle pull.
A cane create an additional force that keeps the pelvis level in the face of gravity's tendency to adduct the hip during unilateral stance. The cane's force must substitute for the hip abductors of the affected hip and creates a moment arm that is relatively long and originates on the side opposite the hip whose abductor muscles are weak. Additionally, the person needs adequate strength in the muscles of the wrist, elbow, shoulder girdle, and trunk.
Brand and Crowninshield performed a 3-dimensional hip joint reactive force evaluation of 4 different groups of patients. The groups included normal
subjects, preoperative THA subjects walking without a cane, preoperative THA subjects walking with a cane, and subjects following total hip reconstruction. Each of the 3 groups evaluated without the cane had statistically similar hip joint reactive forces. The preoperative THA subjects walking with a cane and significantly lower joint reactive forces (approximately 60%).
The article by Blount was named by JBJS as a "Classics in JBJS" in 2003. It is a commentary encouraging the use of canes by describing how the biomechanics of the hip joint are altered while using a cane.
Illustration A shows some of the mathematics behind cane use.
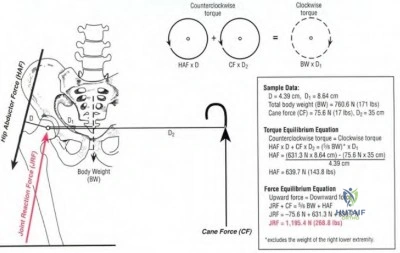
OrthoCash 2020
Which of the following is an example of an antalgic gait pattern not typically seen in clinical practice?
Patient's knee is maintained in slight flexion throughout the stance period for ipsilateral knee arthritis
Patient's contralateral step length is shortened with ipsilateral ankle arthritis
Patient leans their trunk laterally over the painful leg during stance phase with ipsilateral hip arthritis
Patient ambulates on their toes with an ipsilateral calcaneal stress fracture
Patient ambulates predominately through the heel for ipsilateral knee arthritis
The term antalgic gait is non-specific and describes any gait abnormality resulting from pain. A patient with knee arthritis maintains slight flexion throughout the gait cycle. This compensatory knee flexion is exacerbated if the patient has a concomitant effusion in the knee as flexion reduces tension on
the knee joint capsule. Gait compensation for knee arthritis also involves toe walking on the affected side, reducing the stride length, and reducing time of weight bearing on the painful leg.
Gok et al performed a case-control gait analysis study of 13 patients with OA and 13 normal patients. They found that walking velocity, cadence and stride length were reduced in the OA group and that the overall stance phase was prolonged in the OA group. They concluded that computerized gait analysis can be used to reveal various mechanical abnormalities accompanying arthrosis of the knee joint at an early stage.
Cole and Harner present Level 5 evidence about knee arthritis in the active patient. They stress that weightbearing radiographs are important in the diagnosis of arthritis. They also discuss the importance of looking for medial or lateral thrusts during gait and dynamic gait changes such as quadriceps avoidance or out-toeing.
Incorrect Answers:
OrthoCash 2020
A 78-year-old male falls at home four months following a right total hip arthroplasty. Right leg deformity, pain, and inability to bear weight are present on physical exam. An injury radiograph is provided in Figure A, while radiographs taken immediately following the initial total hip arthroplasty are provided in Figures B and C. The patient denies any prodromal groin pain prior to his fall. Which of the following is the best treatment option?
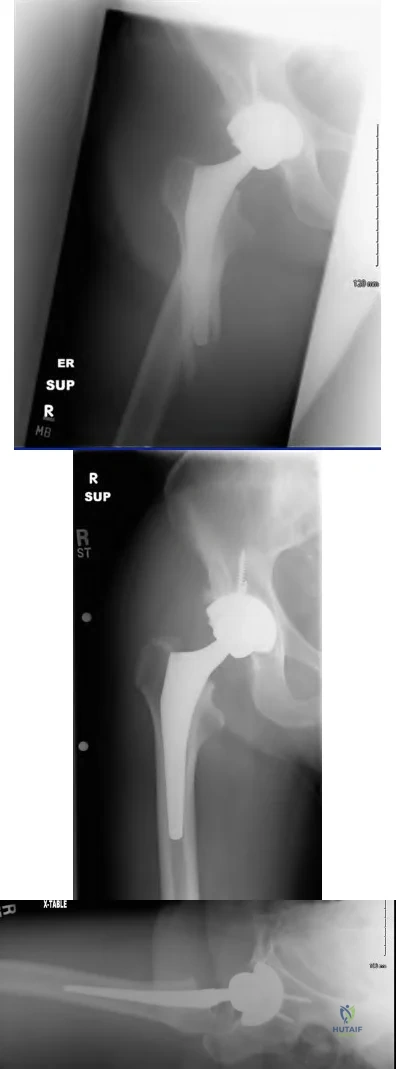
Traction for 6 weeks followed by slow return to weight bearing
Open reduction and internal fixation
Revision to a long, cementless femoral stem
Revision to a long, cementless stem with strut allograft
Revision to a long, cemented stem Corrent answer: 2
The clinical presentation and radiograph are consistent with a Vancouver B1 periprosthetic femur fracture. The stem appears stable within the femur, and there is no evidence of subsidence with comparison to the initial post-THA radiographs. This fracture pattern is best treated with internal fixation.
Illustrations A and B are radiographs of this patient following fixation. Illustrations C and D show bone healing at 2 years following the fracture.
Duwelius et al report on 33 periprosthetic femur fractures. All fractures that demonstrated a stable stem at the time of surgery were treated with internal fixation, while those that were unstable were treated with a long, cementless revision femoral stem. At 2.5 years complications were minimal and the patients had regained their pre-fracture level of function.
The review article by Kelley outlines the evaluation, classification, and treatment of periprosthetic femur fractures reinforcing the importance of stem stability within the femur. Periprosthetic fractures around a hemiarthroplasty should be treated with the same algorithm. However, if the patient had antecedent groin pain, then conversion to a total hip arthroplasty should be considered to prevent continued groin pain.

OrthoCash 2020
A 64-year-old male underwent the procedure shown in Figures A and B 7 weeks ago. He complains of difficulty with going down stairs. He reports no pain and denies constitutional symptoms. On examination the incision is well healed and no effusion is present. He is able to perform a straight leg raise with 5/5 strength. He lacks 2 degrees of terminal extension and has 80 degrees of active flexion. The knee is stable to varus and valgus stress testing at extension and mid flexion. His C-reactive protein and erythrocyte sedimentation rate are normal. What is the next most appropriate step in management?

Manipulation under anesthesia
Cortisone injection followed by physical therapy for quadriceps strengthening
Aspiration to evaluate for septic arthritis
Revise femoral component by downsizing A-P diameter
Revise tibial component and add 5 degrees of posterior tibial slope Corrent answer: 1
The history, physical examination, laboratory studies, and imaging are consistent with a total knee arthroplasty patient with arthrofibrosis. The next most appropriate option includes a manipulation under anesthesia to increase the patient's flexion.
Maloney presents Level 4 evidence discussing TKA postoperative arthrofibrosis. They report that manipulation under anesthesia was successful in improving flexion from an average of 67 degrees premanipulation to 111 degrees
postmanipulation.
Keating et al report Level 4 evidence of 113 patients that underwent manipulation following TKA. They found that 90% of the patients achieved improvement of ultimate knee flexion following manipulation. The average improvement in flexion from the measurement made before manipulation to that recorded at the five-year follow-up was 35 degrees.
OrthoCash 2020
Which of the following total hip arthroplasty patients appropriately meets the criteria for a surgical debridement with isolated femoral head and polyethylene liner exchange?
Prosthesis infection of 4 months duration
Prosthesis infection 8 weeks following implantation
Prosthesis infection 3 days following a systemic infection
Acetabular component loosening due to osteolysis
Vancouver Type A periprosthetic fracture.
Femoral head and polyethylene liner exchange is an appropriate treatment for the acutely infected arthroplasty. Acute infection has been defined as 3-6 weeks following surgery or following a systemic infection depending on the literature source. Subacute and chronic infections must be treated with a complete explant and exchange of all components. (One-stage or two-stage is controversial).
Salvati et al review the management of total hip arthroplasty infection. Most importantly, the pathogen must be isolated to direct antibiotic treatment. The acuity of the infection must also be recognized to direct surgical management.
OrthoCash 2020
A 54-year-old woman is at physical therapy 3 months after a total knee arthroplasty when she feels a pop and develops increased pain in her knee. She continues therapy for another 3 months but reports weakness and frequent buckling. On exam, she has full passive extension but a 60 degree extensor lag. A lateral radiograph is shown in Figure A. What is the treatment of choice?

Reconstruction with a bone-tendon allograft
Repair augmented with hamstring autograft
Continued therapy and strengthening
Arthrodesis
Treatment with orthotics for support Corrent answer: 1
The patient has a chronic patellar tendon rupture following a TKA with marked extensor lag and patella alta on radiograph. A study by Barrack et al concluded that allograft reconstruction for the chronically-disrupted extensor mechanism after TKA could restore active extension and improve ambulatory function. In chronic cases, primary repair with or without local tissue augmentation have had disappointing results. Extensor mechanism injuries after TKA was reviewed by Parker et al. Patellar tendon ruptures are rare complications after TKA with an incidence reported <2.5%. Quadriceps tendon ruptures are even more rare with an incidence ~1%.
OrthoCash 2020
When compared to the standard medial parapatellar approach for revision total knee arthroplasties, the oblique rectus snip approach
showed impairment in which of the following post-operative outcomes?
range-of-motion
patient satisfaction
pain
WOMAC function score
no difference in outcomes Corrent answer: 5
Meek et al compared the rectus snip to a standard medial parapatellar approach for revision total knee arthroplasty. The WOMAC function, pain, stiffness and satisfaction scores demonstrated no statistical difference. They concluded that use of a rectus snip as an extensile procedure had no adverse effect on outcome.
OrthoCash 2020
What is the range of pore size of cementless porous implants to allow for optimal bony ingrowth?
Less than 1 micron
50 to 400 microns
1,000 to 5,000 microns
10,000 to 50,000 microns
100,000 to 500,000 microns
The range of 50 to 400 microns is the optimal pore size for cementless porous implants to allow for optimal bony ingrowth.
Bobyn et al looked at the optimum pore size for fixation of porous surfaced metallic implants. Four different pore sizes were examined and placed in canine femurs for 4, 8, and 12 weeks and tested to measure the shear strength based on pore sizes. A pore size of 50 to 400 microns provided the maximum fixation strength in the shortest time period (8 weeks), implying maximal bony ingrowth.
Pilliar et al discussed two independent canine studies which showed that initial implant movement relative to host bone can result in attachment by a nonmineralized fibrous connective tissue layer. They state that implant movement of greater than 150 microns leads to fibrous ingrowth.
Jasty et al implanted porous-coated implants in the distal femoral metaphyses of twenty dogs and subjected them to zero, twenty, forty, or 150 micrometers of oscillatory motion. They found that that the implants that had been subjected to 150 micrometers of motion were surrounded by dense fibrous tissue.
OrthoCash 2020
An active 73-year-old male presents with progressive pain and instability 15 years after undergoing a left total knee arthroplasty. He denies any recent trauma. A comprehensive workup for infection is negative. What is the most appropriate management of this patient?

Protected weight bearing for 6 weeks
Revision total knee arthroplasty
Bisphosphonate therapy
Routine follow-up in 1 year
Polyethylene liner exchange and bone grafting Corrent answer: 2
This patient has evidence of periarticular osteolysis and component loosening around a previous total knee arthroplasty. He is symptomatic and would benefit from revision total knee arthroplasty (TKA).
Osteolysis is one of the leading causes for late reoperation in patients who undergo TKA. Osteolysis occurs as the result of a foreign body response to particulate wear debris from the prosthetic joint. These particles consist of polyethylene, polymethylmethacrylate cement, and metal, all of which have been shown to elicit a distinct inflammatory response. Once the particles are generated from and around the implant, they become phagocytosed by macrophages and giant cells in the synovial or periprosthetic tissue. These cells, in turn, become activated and can directly or indirectly cause osteolysis. The femur is prone to osteolysis in the region of the femoral condyles and near the attachments of the collateral ligaments of the femur. Osteolysis around the tibia tends to occur along the periphery of the component or along the access channels to the cancellous bone.
Maloney & Rosenberg reviewed the management and outcome of periprosthetic osteolysis around hip and knee implants. They recommended surgical intervention for periprosthetic osteolysis around a TKA with (1) first-time presentation of advanced osteolysis in the presence of an identifiable cause of wear particle production or in the presence of associated bone loss that places the structural integrity of the bone or fixation of the components at risk, (2) bearing surface wear in the presence of impending wear-through or related mechanical symptoms, (3) progressive osteolysis in an active individual, and (4) symptoms of wear debris-related synovitis that are refractory to conservative treatment.
Griffin et al. evaluated the results of isolated polyethylene exchange for wear and/or osteolysis in 68 press-fit condylar TKAs from four centers. At a minimum of 24 months after polyethylene exchange surgery, there were 11 failures (16.2%).
Gupta et al. discuss the etiology, diagnosis, contributing factors, and management of osteolysis as it relates to TKAs. They recommend that if the patient is asymptomatic with minimal osteolysis on plain radiographs, regular
follow-up at 6 months to 1 year with medical management including calcium and bisphosphonates would be adequate. If the patient becomes symptomatic or the osteolysis is progressive, then early liner exchange with or without tibial baseplate exchange is considered.
Figure A & B are AP and lateral radiographs of periarticular osteolysis and component loosening. Illustration A is an AP and lateral radiograph of the revision TKA.
Incorrect Answers:

OrthoCash 2020
Which of the following statements is true regarding the thirty-year follow-up data obtained from the Charnley "low-friction" total hip arthroplasty?
Acetabular component failure was the least common reason for revision surgery
The number of revisions required for periprosthetic fractures was higher than that for deep infections
Acetabular component failure was a more common reason for revision than deep infection
Femoral component failure was a more common reason for revision than acetabular component failure
Deep infection was the most common reason for revision Corrent answer: 3
Failure of the acetabular component was the most common reason for revision at thirty-years for the Charnley "low-friction" total hip arthroplasty.
The Charnley low-friction torque arthroplasty was introduced in 1962. It consisted of a 22mm diameter metal head, a cemented femoral component, and a cemented ultra-high-molecular-weight polyethylene acetabular component. Overall, the results were very good at thirty years with only 11.8% requiring revision.
Charnley et al. in 1972 reported the 4-7 year results of 379 "low-friction" total hip arthroplasties. Overall, their short-term results were very good with only 2 loose acetabular components, 0 loose femoral components, and 1 late dislocation.
Wroblewski et al. in 2009 reported the 30 year follow-up of 110 patients who underwent the "low-friction" total hip arthroplasty. 13 hips (11.8%) had to be revised. Of these, 5 were for problems with the acetabular component, 4 were for loosening of both components, 2 were for deep infection, 1 was from a loose femoral component, and 1 was from a fractured femoral component.
Illustration A shows a radiograph after a Charnley low-friction total hip arthroplasty. Note the all poly-ethylene acetabular component. Illustration B shows the components used for the operation.
Incorrect Answers:

OrthoCash 2020
A 71 year old gentleman underwent left total hip arthroplasty 10 years ago. Eighteen months ago he began having hip and thigh pain. Over the past 6 weeks, the pain has become excruciating and he has been unable to ambulate, even with the aid of a walker. He has mild pain with passive internal and external rotation of the hip. He is unable to ambulate in the office. Laboratory values are notable for a WBC of 10,300, CRP of 0.2, and ESR of 13. A radiograph is provided in figure A. Which of the following is the best treatment option?

Radionuclide bone scan and MRI
Open reduction internal fixation with a cable plate and allograft strut
Revision arthroplasty with a fully coated cementless stem, cable wiring, and bone graft
Revision arthroplasty with a modular, tapered stem and bone grafting of the diaphyseal fixation
Revision arthroplasty with a total femur prosthesis Corrent answer: 3
The radiograph is consistent with a periprosthetic femur fracture, with a loose femoral stem, and a Paprosky IIIA femoral defect. This is best treated with a fully-coated cementless stem with metaphyseal onlay allograft.
Paprosky devised a classification for femoral bone loss following THA. The classification is as follows:
Type I: minimal metaphyseal bone loss and intact diaphyseal fixation Type II: extensive metaphyseal bone loss with intact diaphyseal fixation
Type IIIA: severe metaphyseal bone loss with greater than 4 cm of diaphyseal bone preservation for distal fixation.
Type IIIB: severe metaphyseal bone loss and less than 4 cm of diaphyseal
bone preservation for distal fixation
Type IV: extensive metaphyseal and diaphyseal bone loss.
Type IIIA may be treated with a fully coated stem. Type IIIB should consider a tapered, modular stem and/or bone grafting. Type IV likely needs a megaprosthesis. In this patient, given the preserved diaphyseal bone, revision arthroplasty with a fully coated femoral stem is the most appropriate treatment.
The Sporer article reviews a case series of patients undergoing revision hip arthroplasty for femoral bone loss. Type IIIB defects with a femoral canal less than 19 mm may be treated with a fully porous-coated stem. However, patients with Type IIIB defect and a cavernous canal greater than 19 mm or a Type IV defect may need a modular tapered stem or a bone grafting procedure.
The Paprosky article summarizes his classification of femoral bone loss in revision hip arthroplasty and provides an algorithm for treatment. Extensively porous-coated, diaphyseal filling femoral components showed excellent results in Paprosky IIIA defects.
Radiograph A shows a total hip arthroplasty with severe metaphyseal bone loss and a supportive diaphysis.
Incorrect Answers:
OrthoCash 2020
A 74-year-old man presents with start-up thigh pain following a total hip replacement 10 years ago. Immediate post-operative radiograph is shown in Figure A. A current radiograph is shown in Figure B. Aspiration of the hip yields 1,005 white blood cells/ml. ESR is 12 (normal <40) and CRP is 0.4 (normal <1.2). Which of the following is the most appropriate management at this time?
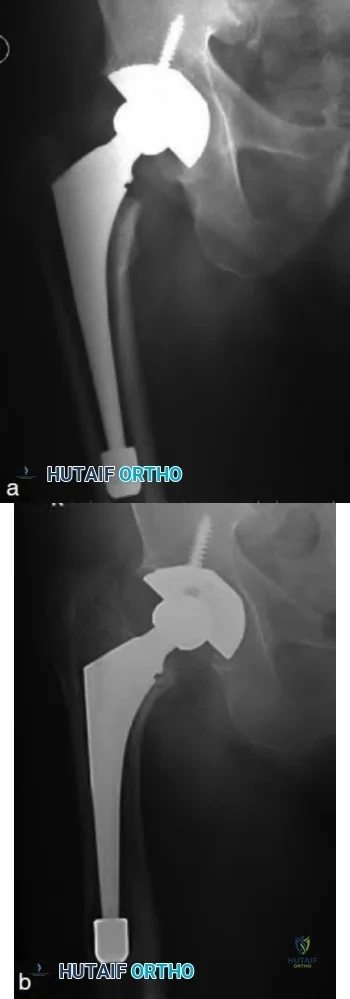
Revision of the femoral component to an uncemented, long, fully porous-coated stem
Revision of the femoral component to a cemented stem
Revision of the femoral component to an allograft prosthetic composite
Revision of the femoral component to a proximal femoral replacement
Removal of prosthesis with insertion of antibiotic spacer Corrent answer: 1
The clinical presentation is consistent with symptomatic, aseptic femoral component loosening with no evidence of femoral bone defects. Appropriate management consists of revision of the femoral component to an uncemented, fully porous-coated stem.
Aseptic loosening remains one of the most common indications for revision total hip arthroplasty. After infection has been ruled-out, management is determined by gauging the patients symptoms, the rate of progression of the subsidence, and the amount of femoral bone loss. Uncemented revision femoral components have shown superior results to cemented revision femoral components in the long-term. In the setting of Paprosky Type I, II, and IIIA defects of the femur, revision to an uncemented, fully porous-coated stem is advised.
Moreland et al. review the results of 134 patients (137 hips) who underwent revision arthroplasty with an extensively porous-coated cobalt chrome femoral prosthesis. At a mean follow-up of 9.3 years, only 10 (7%) had to removed for any reason.
Sporer et al. review the results of fully porous-coated stems, impaction bone grafting, and modular tapered stems for Paprosky III and IV femoral defects. They found a high rate of failure with fully porous-coated stems when used in patients with Type IIIB defects >19mm and Type IV defects. They attribute these failures to instability and the inability to eliminate micromotion.
Figure A shows a cementless, metaphyseal engaging femoral component in good alignment. Figure B is a post-operative radiograph from 10 years later showing significant subsidence of the femoral component.
Incorrect Answers:
OrthoCash 2020
A 72-year old female who underwent an uncemented right total hip arthroplasty 2 years ago complains of right hip pain after a fall. Figure A shows her current radiograph. Which acetabular bone defect classification and treatment option best describes this scenario?

AAOS Type III - anti-protrusio cage with augmentation and a posterior column plate
AAOS Type IV - anti-protrusio cage with screw fixation and a posterior column plate
AAOS Type II - jumbo cup with augmentation and a posterior column plate
AAOS Type I - total acetabular allograft with a cemented cup
AAOS Type II - custom triflange acetabular component Corrent answer: 2
Figure A shows pelvic discontinuity, which is consistent with a AAOS Type IV defect. Acetabular antiprotrusio cage with screw fixation and a posterior column plate is a reasonable treatment option for this condition.
Acetabular bone loss following total hip arthroplasty is a challenging problem with a wide variety of treatment options available. The two most widely accepted classification systems are the AAOS and Paprosky classifications.
AAOS type I defects are segmental, type II are cavitary, type III are combined cavitary and segmental, type IV is discontinuity, and type V is arthrodesis. All of the treatment options listed above are described for pelvic discontinuity,
with none being described as superior.
DeBoer et al. describe the results of 28 patients with pelvic discontinuity treated with a custom-made porous-coated triflange acetabular prosthesis. 20 of these patients were followed for 10 years. There were no re-operations, 5 hip dislocations, 1 sciatic nerve palsy, and an average improvement in the Harris hip score from 41 to 80.
Paprosky et al. retrospectively reviewed patients who had an acetabular revision using a trabecular metal acetabular component for a pelvic discontinuity and compared these patients with a cohort of patients who had a previous reconstruction for a pelvic discontinuity using an acetabular cage.
They found a decreased incidence of pain and need for walking aids in those patients who had revision with a trabecular metal acetabular component.
Figure A shows pelvic discontinuity, likely acute given the lack of associated bony defects and recent fall. Illustration A details the AAOS hip acetabular defect classification and Illustration B is the often cited Paprosky classification.
Incorrect Answers:

OrthoCash 2020
Which of the following is indicative of type 1 collagen breakdown and can be utilized as a marker of bone turnover?
Increased urinary N-telopeptide
Increased urinary cAMP and phosphate
Increased urinary phosphoethanolamine
Increased urinary Bence Jones proteins
Increased serum bone sialoprotein Corrent answer: 1
Urinary N-telopeptide is a marker of increased bone turnover and is a breakdown product of Type 1 collagen.
Increased serum alkaline phosphatase level and increased urinary markers of N-telopeptide, hydroxylproline, deoxypyridinoline indicate high bone turnover and can be seen in metabolic bone diseases such as Paget's disease.
von Schewelov et al. reviewed 160 patients that underwent total hip replacements and examined their urine specimens to see if N-telopeptide levels correlated to periprosthetic osteolysis. They found that n-telopeptide levels were 1/3 higher in the patients that had evidence of osteolysis. N-
telopeptide release and annual wear were both associated with increased prevalence of osteolysis in the study.
Illustration A shows a radiograph of Pagets disease of the femur, an example of a condition where there is an increased level of N-telopeptide in the urine. Illustration B is a radiograph showing periprosthetic osteolysis, another condition where there is an increased level of N-telopeptide in the urine.
Incorrect Answers:
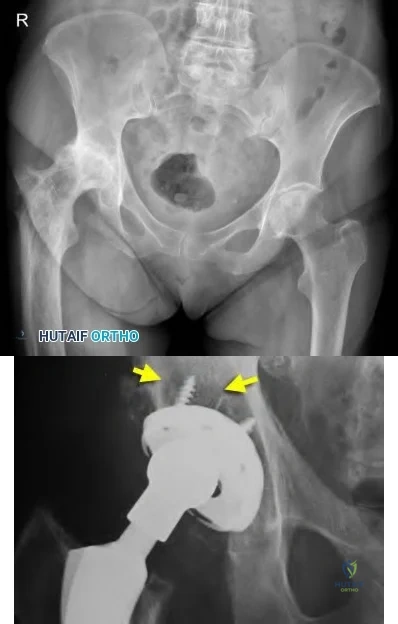
OrthoCash 2020
A 78-year-old female undergoes total hip arthroplasty through a minimally invasive surgical approach. During insertion of a metaphyseal fixation stem with a cementless press-fit technique, a crack in the calcar is identified. The stem is removed, two cable wires are passed around the calcar, and the same stem is reinserted. Which of the following statements is true?
The patient should be advised she is at greater risk of stem subsidence and early revision
Female sex is a risk factor for intraoperative calcar fracture
A better outcome would be expected if a long-stem diaphyseal fixation stem had been inserted after recognition of the calcar fracture
Cementless press-fit technique is not a risk factor for intraoperative fracture
Minimally invasive surgical approach is not a risk factor for intraoperative fracture
Of the statements listed, the only true statement is that female gender is a risk factor for intraoperative calcar fracture.
Calcar fractures are a documented complication of total hip arthroplasty. Studies have shown that successful outcomes can be achieved with stem removal, cable wiring of the calcar, and re-insertion of the primary stem.
Berend et al. reviewed a series of 58 total hip arthroplasties who sustained an intraoperative calcar fracture. All were treated with cable wiring of the calcar and stem insertion. The authors report no femoral component subsidence or failure otherwise at 16 year follow-up.
Graw et al. review a series of 46 revision THA's. Of the 46, fifteen underwent primary THA through a minimally invasive technique. The average length of time from primary THA to revision was 1.4 years for the minimally invasive group versus 14.7 years for the traditional exposure THA's. The authors conclude minimally invasive THA is a risk for early revision.
Davidson et al. review intraoperative periprosthetic hip fractures. "Risk factors for intraoperative periprosthetic fractures include the use of minimally invasive techniques; the use of press-fit cementless stems; revision operations, especially when a long cementless stem is used or when a short stem with impaction allografting is used; female sex; metabolic bone disease; bone diseases leading to altered morphology such as Paget disease; and technical errors at the time of the operation." The authors summarize techniques for treatment and postulate that long term outcome is unaffected when the intraoperative fracture is identified and treated appropriately.
Illustration A shows a nondisplaced calcar crack that was treated with a single Luque wire.
Incorrect Answers:

OrthoCash 2020
Which of the following types of prosthetic designs, seen in figures A-E, has been shown to have a high rate of loosening secondary to overconstraint?

Figure C shows an example of an Walldius hinge total knee prosthesis. This design had a higher rate of aseptic loosening (up to 20%) secondary to a high-degree of constraint.
Constraint is defined as the effect of the elements of knee implant design that provides the stability needed to counteract forces about the knee after arthroplasty in the presence of a deficient soft-tissue envelope. While increasing component constraint increases the stability of the knee, it also transmits forces to the fixation and implant interfaces, which may lead to premature aseptic loosening. First-generation total knee hinged prostheses were highly constrained devices that only allowed a single axis of rotation.
Lombardi et al. provide an Instructional Course Lecture on the different prosthetic designs in total knee arthroplasty. They argue that PCL sacrificing implants are more appropriate than cruciate-retaining implants in rheumatoid arthritis, previous patellectomy, previous high tibial osteotomy or distal femoral osteotomy, and in cases where the PCL is absent secondary to trauma.
Morgan et al. discuss constraint in primary total knee arthroplasty. They argue that a hinge total knee arthroplasty should be reserved for severe instability, elderly patients with comminuted distal femur fractures, patients with
extensor-mechanism disruption and unstable knees, and those with substantial bone loss not amenable to augmentation.
Figure C shows an example of a Walldius hinged prosthesis.
Illustration A shows an intra-operative example of a constrained-hinged knee prosthesis. Note the link between the tibial and femoral components, which differentiates it from a constrained, non-hinged prosthesis.
Incorrect Answers: The following responses are incorrect as they all have lower rates of aseptic loosening than than varus/valgus constrained prostheses or hinged designs.

OrthoCash 2020
A 28-year-old football player sustains a contact knee injury while being tackled. On physical exam, he has a 1A Lachman, and a normal McMurray test. His posterior drawer, dial, and varus stress tests are normal. He has pain and 5mm opening on valgus stress at 30 degrees of flexion. Which statement is true regarding the injured structure?
Resides between layers 1 and 2 on medial side of knee
Inserts onto Gerdy's tubercle
Originates slightly posterior and proximal to the medial epicondyle
Courses intraarticularly thru hiatus of lateral meniscus
Has an attachment between adductor tubercle and medial epicondyle at Schöttle's point
The clinical presentation is consistent with an injury to the superficial medial collateral ligament (MCL) of the knee, which originates slightly posterior and proximal to the medial epicondyle.
The superficial portion of the MCL is the primary stabilizer to valgus stress at all angles, contributing 57% and 78% of medial stability at 5 degrees and 25 degrees of knee flexion, respectively. Anatomic studies have shown that the superficial MCL originates approximately 3.2 mm proximal and 4.8 mm posterior from the medial femoral epicondyle and inserts into the periosteum of the proximal tibia (deep to pes anserinus). The superficial MCL lies in layer 2, just deep to gracilis and semitendinosus tendons.
Wijdicks et al. (2009) looked at radiographic identification of the primary medial knee structures including the superficial MCL. On the lateral radiograph, they found that the attachment of the superficial MCL was an average of 6.0 mm from the medial epicondyle.
Wijdicks et al. (2010) reviewed injuries to the MCL and associated medial structures of the knee. They state that physical examination is the initial method of choice for the diagnosis of medial knee injuries through the application of a valgus load both at full knee extension and between 20 degrees and 30 degrees of knee flexion. Treatment of isolated grade-III injuries to the MCL, or such injuries combined with an anterior cruciate ligament tear, should start with nonoperative treatment of the MCL due to high rates of success with nonoperative treatment. If operative treatment is required, an anatomic repair or reconstruction is recommended.
Illustration A shows the femoral and tibial attachments of the superficial MCL. Illustration B shows the osseous landmarks and attachments of medial knee structures (AT, adductor tubercle; GT, gastrocnemius tubercle; ME, medial epicondyle; AMT, adductor magnus tubercle; MGT, medial gastrocnemius tendon; sMCL, superficial MCL; MPFL, medial patellofemoral ligament; POL, posterior oblique ligament).
Incorrect Answers:
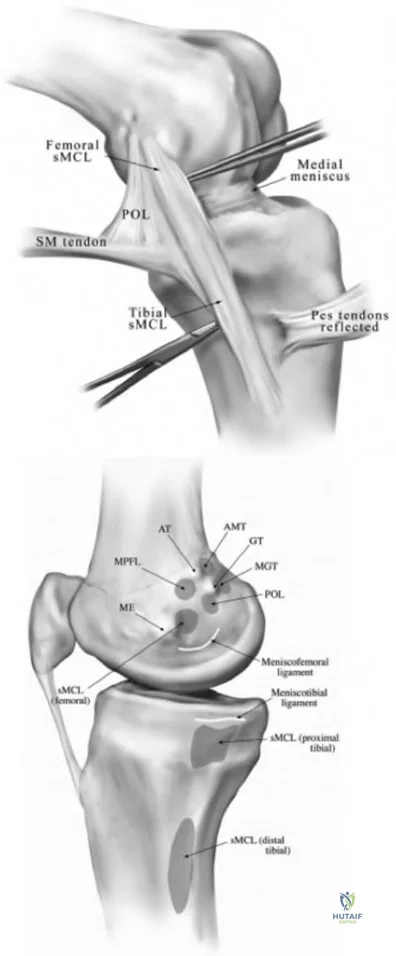
OrthoCash 2020
Which of the following best describes normal tibio-femoral joint kinematics ?
The femur undergoes internal rotation with knee flexion
The lateral femoral condyle remains stationary on the lateral tibia plateau during knee flexion from 0 to 120 degrees
The tibia undergoes internal rotation with knee flexion
The medial femoral condyle moves posteriorly on the medial tibial plateau during knee flexion from 0 to 120 degrees
Beyond 120 degrees of flexion only the lateral femoral condyle participates in femoral rollback
Tibia is subjected to internal rotation with knee flexion and the tibia EXternally rotates on femur as the knee EXtends.
The axis of rotation shifts posterior on the lateral condyle with knee flexion. Flexion and extension at the knee occur about a constantly changing center of rotation (polycentric rotation).
Freeman et al. conducted a biomechanical experiment and found that the medial femoral condyle does not move much from 0 to 120 degrees of flexion. They also found that the lateral femoral condyle and the contact area between that condyle and the tibia move posteriorly and tibial internal rotation occurs with knee flexion. They found that from 120 degrees to full flexion both condyles participate in "roll back".
Illustration A shows why the screw-home mechanism occurs. The medial tibial plateau is longer than the lateral tibial plateau, leading to external rotation of the tibia during extension as the femoral condyle rotates about the tibia. Video V shows an example of external tibial rotation during extension.
Incorrect Answers:
OrthoCash 2020
Which of the following molecules is associated with macrophage induced osteolysis surrounding orthopaedic implants?
BMP-7
IL-10
SOX-9
Osteoprotegrin
IL-1
Of the options provided, IL-1 is most associated with macrophage induced osteolysis surrounding orthopaedic implants.
Macrophages initiate the inflammatory cascade associated with aseptic loosening of orthopaedic implants by secreting platelet-derived growth factor (PDGF), prostaglandin E2 (PGE2), TNF-alpha, IL-1, and IL-6.
Archibeck et al. state the primary cells involved in the process of periprosthetic loosening include the macrophage, osteoblast, fibroblast, and osteoclast. They report the chemical mediators that are responsible for the cellular interactions and effects on bone primarily include PGE2, TNF-alpha, IL-1, and IL-6.
Drees et al. discuss the molecular pathway of aseptic loosening of orthopedic implants. They describe the following steps: 1) Wear debris particles released at the cement–bone interface attract macrophages, which, in turn, are stimulated to produce proinflammatory mediators and proteolytic enzymes; 2) RANKL, TNF-alpha, IL-1, IL-6, IL-17, and M-CSF mediate the differentiation of myeloid precursor cells into multinucleated osteoclasts, which release cathepsin K and acid and cause resorption lacunae; 3) Mesenchymal cells (prosthesis-loosening fibroblasts) present at the bone surface contribute actively to bone resorption.
Illustration A shows the pathway described by Drees et al.
Incorrect Answers
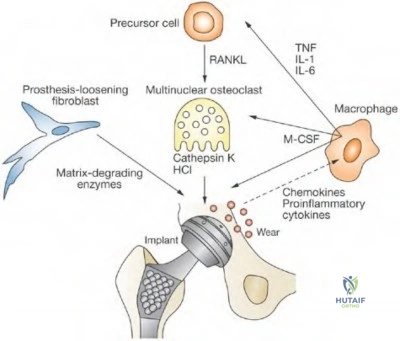
OrthoCash 2020
Which of the following templates, seen in Figures A-E, will increase the offset while keeping the leg lengths the same?

If the total hip prosthesis is inserted according to the template in Figure E, the offset will be increased, while the leg lengths will remain unchanged.
Restoration of limb length is essential following total hip arthroplasty. The amount of limb-length change will be the vertical distance between the center of rotation of the femoral component and the center of rotation of the acetabular component. Thus, when the femoral center of rotation on templating is inferior to that of the acetabular component, the limb will be shortened. Restoring femoral offset is also important. If the center of rotation of the prosthetic head lies lateral to that of the cup on templating, the reconstruction will produce decreased offset.
Scheerlinck et al. present a stepwise approach to hip templating through four steps. Step 1 involves identifying landmarks, step 2 involves assessing the
quality of the radiograph, step 3 identifies mechanical references, and step 4 optimizes implant positioning.
Tripuraneni et al. discuss the common errors encountered when templating for total hip arthroplasty. They found the most common error was excessive limb lengthening and incomplete medialization of the acetabular component.
Della Valle et al. review hip templating. They stress the importance of preoperative planning, but also discuss the importance of tactile feedback during the surgery in choosing the correct implants.
Illustration A shows a table of how offset and leg lengths can be changed through positioning and selection of components.
Incorrect Answers:
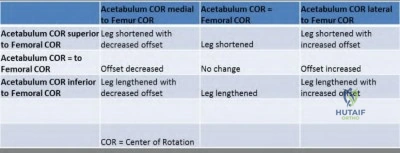
OrthoCash 2020
A 91-year-old male with a history of chronic leukemia and dementia falls and sustains the hip fracture shown in Figure A. He undergoes a hemiarthroplasty through a posterior approach. A postoperative radiograph is shown in Figure B. Three weeks later he dislocates the hip arising from the toilet seat. A radiograph is shown in Figure C. The patient undergoes a closed reduction and is placed in a hip abduction brace. Post reduction radiograph is shown in Figure D. One month later he returns to clinic complaining of pain and inability to bear weight through the leg. A radiograph of the hip is included in Figure E. Which of the following factors has MOST likely contributed to the instability of the hip hemiarthroplasty?

Femoral stem subsidence
Increased offset
Inadequate femoral stem neck length
Patient's dementia status
Patient's gender
The most likely contributing factor to the instability include the patient's dementia.
Sultan et al use a basic science model to show liners with elevated rims placed in the posterior superior quadrant allow greater range of motion to dislocation than standard liners. They also show that 32 mm heads have greater range of motion to dislocation compared to 28 mm heads.
Morrey et al reviewed a series of 19,680 primary THA's for late dislocation (first dislocation greater than 5 years after surgery). 165 hips (0.8%) had a late dislocation. Factors associated with late dislocation include implant malposition, neurologic decline, trauma, and polyethylene wear.
Figure A shows a femoral neck fracture. Figures B and D show a hip hemiarthroplasty in appropriate position. Figure C and E show a dislocated hip hemiarthroplasty
This patient's instability was managed by converting the hip hemiarthroplasty to a total hip arthroplasty with a constrained liner as shown in illustration A. No further instability episodes occurred following the revision.
Incorrect Answers:

OrthoCash 2020
What surgeon is credited for designing the prosthesis seen in Figure A?
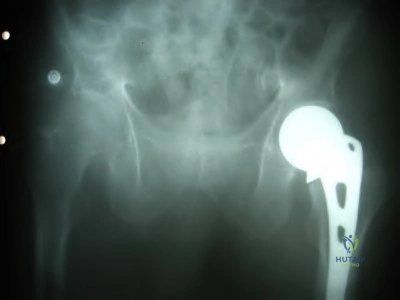
John Charnley
San Baw
Sir Harry Platt
Austin T. Moore
Charles Frederick Thackray Corrent answer: 4
Figure A shows an example of an Austin-Moore hemiarthroplasty.
Austin Moore developed the most popular long-stemmed prosthesis in the 1950s. The Austin-Moore prosthesis was a large, uncemented femoral stem that didn't use polyethylene. The Austin-Moore prosthesis had fenestrations for self-locking which later became the impetus for biological fixation. These implants were originally used to treat hip fractures and certain cases of degenerative arthritis. Later, in the 1960s, John Charnley introduced the idea of replacing the eroded acetabulum with a Teflon component.
Moore et al. describe the first metallic hip replacement surgery in 1940. The patient had a proximal femoral resection for a giant cell tumor. The original prosthesis he designed was a proximal femoral replacement, with a large fixed head, made of the Cobalt-Chrome alloy Vitallium.
Charnley et al. discuss the long-term results (up to 7 years) of the "low-friction" total hip arthroplasty. Infection rate was 3.8%, late mechanical failure was 1.3%, and most patients had excellent pain relief.
Figure A shows a radiograph of an Austin-Moore hemiarthroplasty. Illustration A shows an Austin-Moore prosthesis. Illustration B shows an example of Charnley's "low-friction" total hip arthroplasty, with a stainless steel head and
stem and a polyethylene acetabular component.
Incorrect Answers:
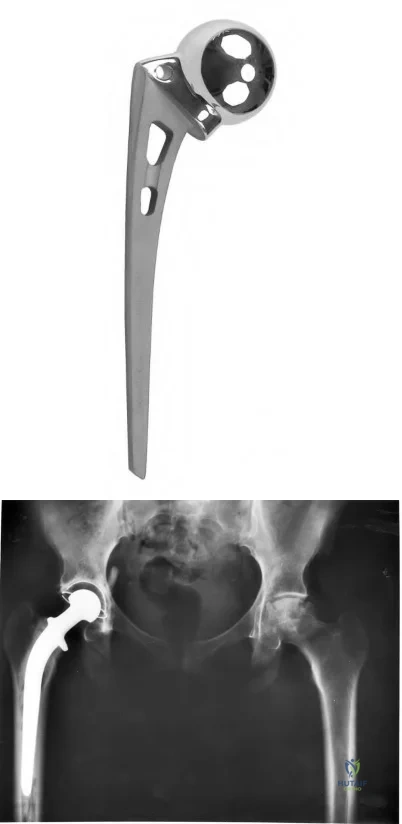
OrthoCash 2020
A 45-year-old man has had the gait disturbance shown in Video A ever since a total hip replacement two years ago. Since then he has undergone physical therapy and nerve exploration without any clinical improvement. Extensive AFO bracing was attempted but was not tolerated by the patient. A recent ankle radiograph is shown in Figure
A. The Silfverskiold test reveals dorsiflexion of 20 degrees with knee flexion, and 10 degrees with full knee extension. The results of muscle
testing using a Cybex dynamometer are shown in Figure B. What is the most appropriate next step in in treatment.
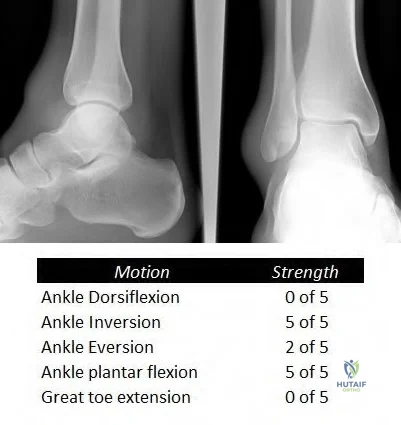
Ankle arthrodesis in 30 degrees of dorsiflexion
Posterior tibial tendon transfer to the lateral cuneiform through the interosseous membrane
Split anterior tibial tendon transfer to the cuboid
Peroneus longus transfer to the navicular and gastrocnemius recession
Flexor hallucis transfer to the navicular and tendo Achilles lengthening (TAL) Corrent answer: 2
The clinical presentation is consistent with a sciatic neuropathy following THA in a patient that does not tolerate AFO bracing. Posterior tibialis tendon transfer is the next most appropriate step in treatment.
Sciatic neuropathy, especially involving the common peroneal branch, is a known complication of total hip arthroplasty. Typically a patient is adequately treated with an AFO. In some clinical situations an AFO is not tolerated, and a tendon transfer is required. The posterior tibial tendon is the most commonly used donor muscle. A tendon transfer is feasible only if the tendon possesses at least 4/5 power. There is a loss of 1 MRC grade of strength following transfer.
Rodriguez et al. retrospectively reviewed the results of the Bridle procedure 10 patients (11 feet) with a foot drop. The Bridle procedure consists of a posterior tibial tendon transfer through the interosseous membrane to the dorsum of the foot with a dual anastomosis to the tendon of the anterior tibial and a rerouted peroneus longus in front of the lateral malleolus. In their study all 11 feet were brace-free at final followup at 6.68 years.
Yeap et al. retrospectively reviewed 12 patients who were treated with tibialis posterior tendon transfer for footdrop. They found good/excellent patient satisfaction in 10/12 patients. Additionally they found favorable variables for a good outcome include common peroneal nerve palsy over sciatic nerve palsy, male gender less than 30 years of age.
Figure V is a Video that shows a right footdrop with high steppage gait. Figure A shows normal ankle radiographs. Figure B shows the results of dynamometer testing described above. Illustration A shows the Bridle procedure. The left panel shows how the tibialis posterior tendon (C) is tunneled through the interosseous membrane and through a slit in the tibialis anterior tendon (A) and inserted into the second cuneiform. The peroneus longus (B) is also transected and the distal stump is routed anterior the lateral malleolus and anastomosed to the tibialis anterior and tibialis posterior (at the slit where it passes through the tibialis anterior). The right panel shows retrieval of the tibialis posterior tendon above the ankle and passage through a window in the interosseous membrane.
Incorrect Answers:
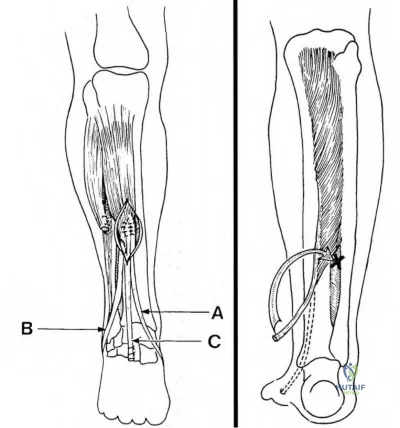
OrthoCash 2020
Which of the following variables is associated with elevated serum metal ion levels following metal-on-metal hip resurfacing arthroplasty?
Smaller implant diameter
Smaller acetabular cup abduction angle
Higher postoperative functional scores
Severe preoperative osteoarthritis
Anteversion of acetabular cup between 10 and 20 degrees Corrent answer: 1
Smaller femoral head diameter is associated with elevated serum metal ion levels with metal-on-metal hip resurfacing arthroplasty.
Metal-on-metal (MOM) hip resurfacing arthroplasty has the advantage of better wear properties (lower linear wear rate and volume of particles) than metal on polyethylene. However, elevated serum metal ion levels is one of the negatives which has received much attention recently. Studies have found smaller implant diameter and acetabular cup abduction angle >55 degrees are associated with elevated serum metal ion levels. Cup abduction angles of greater than 55 degrees lead to a more vertical cup and edge loading.
Desy et al. found that smaller implant diameter, larger cup inclination, and lower postoperative functional scores are associated with increased cobalt and chromium levels after metal-on-metal hip resurfacing. They found that severity of preoperative osteoarthritis, acetabular version, femoral stem-shaft and valgus angle, and anterior orientation of the femoral component had no effect on the circulating metal ion levels.
DeHaan et al. obtained serum ion levels in 214 MOM resurfacing patients at least 1 year following surgery. They found that cup abduction angles greater than 55 degrees combined with smaller component sizes led to edge loading and elevated ion levels.
Illustration A shows how a metal-on-metal prosthesis design allows you to have a larger femoral head as opposed to a metal on polyethylene design (example in THA). Illustrations B and C show a photo of a metal on metal resurfacing implant and radiographs of the implant.
Incorrect Answers:
2: Elevated cup abduction angle leads to elevated serum metal ions.
3: Higher postoperative functional scores have not been shown to increase serum metal ions.
4: Severity of pre-operative arthritis has not been associated with increased serum metal ions.
5: Anteversion of the acetabular cup between 10 and 20 degrees has not been shown to increase serum metal ions.

OrthoCash 2020
Which of the following intra-operative steps would put a patient at risk for lateral patellar maltracking during total knee arthroplasty (TKA)?
External rotation of the femoral component
Medial placement of the patellar component
Internal rotation of the tibial component
Lateral translation of the femoral component
Superior placement of the patellar component Corrent answer: 3
Internal rotation of the tibial component increases the Q angle and causes an increased risk of lateral patellar maltracking.
During TKA, useful techniques that help prevent patellar maltracking include: external rotation of the femoral and tibial components, lateral translation of the femoral component, and medial placement of the patellar component.
In an instructional course lecture, McPherson looked at patellar tracking in primary TKA. He reviews the concept of patellofemoral maltracking, the importance of the Q angle, mechanical alignment, femoral component rotation, tibial component positioning, patellar component positioning, patellar height, and patellar resurfacing as factors related to patellofemoral tracking.
Bengs et al. studied the effect of patellar thickness on intra-operative knee flexion and patellar tracking during PCL retaining TKAs. Using 2mm increments (2-8 mm), passive knee flexion was recorded and gross mechanics of patellofemoral tracking were assessed. On average, passive knee flexion decreased 3 degrees for every 2-mm increment of patellar thickness, there was no gross effect on patellar subluxation or tilt.
Illustration A shows how internal rotation of the tibial component would increase the Q angle, and thus be more likely to have lateral patellar maltracking.
Incorrect answers:
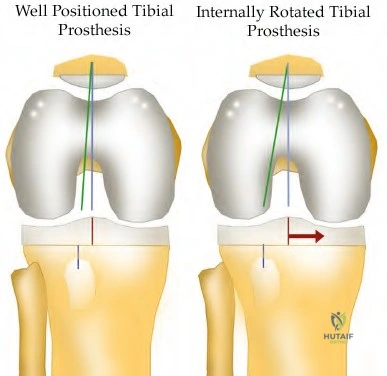
OrthoCash 2020
A patient undergoes a primary total hip arthroplasty with a highly cross-linked ultra-high molecular weight (UHMW) polyethylene acetabular liner. In comparison to a 28mm femoral head, a 32mm femoral head will provide which of the following?
Increased risk of dislocation
Decreased range of motion
Decreased risk of osteolysis
Equivalent wear rate of the polyethylene acetabular liner
Increased risk of periprosthetic fracture Corrent answer: 4
Wear rates of highly cross-linked UHMW polyethylene liners are independent of femoral head size between 22 and 46 mm in diameter.
While the wear rates of old polyethylene liners increased with increasing femoral head size, wear rates of the new highly cross-linked UHMW polyethylene liners have shown to be independent of head size. This is extremely advantageous, as increasing the femoral head size improves range of motion and increases jump distance, thereby decreasing dislocation rates.
Geller et al. report a prospective series of 42 patients that had a total hip arthroplasty with a highly cross-linked UHMW polyethylene liner and a femoral head >32 mm in diameter. After three years, there were no cases of osteolysis or failure due to aseptic loosening.
Muratoglu et al. studied the wear rates of several polyethylene liners with varying femoral head sizes. In the highly cross-linked UHMW polyethylene group, wear rates were independent of femoral head size.
Illustration A shows how increasing femoral head size increases the jump distance required for dislocation.
Incorrect Answers:
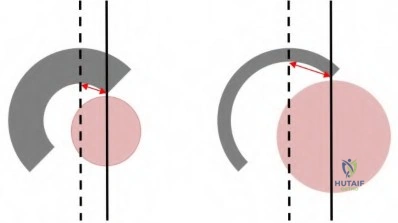
OrthoCash 2020
A 56-year-old male undergoes an uncomplicated revision total knee arthroplasty. Post-operatively, he is noted to have a foot drop that has persisted despite conservative management including bracing and physical therapy. At two months, the patient undergoes external neurolysis with no improvement in function. At 18 months follow-up, he demonstrates passive ankle dorsiflexion 10 degrees past neutral, complete absence of active dorsiflexion, and 5/5 inversion strength. Which of the following is the most appropriate treatment at this time?
Continue Ankle-foot orthosis (AFO) and physical therapy
Repeat neurolysis with possible nerve repair
Peroneus tertius transfer
Peroneus tertius transfer with achilles tendon lengthening
Posterior tibial tendon transfer to dorsum of foot Corrent answer: 5
A peroneal nerve palsy (with intact posterior tibial tendon strength) that has failed conservative management is best treated with a posterior tibial tendon transfer to the dorsum of the foot.
Peroneal nerve palsy following total knee arthroplasty or knee dislocation is a potentially devastating complication that may lead to lack of active dorsiflexion and a compensatory steppage gait pattern. Initial management consists of an ankle-foot orthosis (AFO) and physical therapy to maintain passive ankle dorsiflexion. If nerve function fails to return during the course of conservative management and the patient demonstrates intact posterior tibialis muscle strength, posterior tibial tendon transfer to the dorsum of the foot has been shown to improve functional outcomes and eliminate the need for continued bracing. The most common procedure for posterior tibial tendon transfer involves transferring the tendon through the interosseous membrane and inserting the tendon onto the lateral cuneiform.
Prahinski et al. review the results of 10 patients at 61 months' follow-up who underwent the Bridle transfer (posterior tibialis transfer through interosseous membrane and peroneus longus to front of lateral malleolus) for peroneal nerve palsies. They conclude the Bridle procedure is adequate for return to function in low-demand individuals, but may fail over time in those who return to vigorous physical activity.
Rodriguez et al. review the results of 10 patients who underwent the Bridle procedure for peroneal nerve palsy in an attempt to balance their foot and
provide dorsiflexion. All of their patients were brace free at an average followup of 6.8 years.
Video V shows the clinical results 10 weeks after transfer of the tibialis posterior tendon for a drop foot.
Incorrect Answers:
OrthoCash 2020
An 82-year-old male sustains a ground level fall and sustains the injury shown in Figure A. Which of the following treatment methods is most appropriate for treating this injury?

Closed reduction and functional bracing
Open reduction and fixation with a plate with screws and cerclage cables
Open reduction and fixation with a cortical allograft strut and cerclage cables
Revision hip arthroplasty with bridging of the fracture with a plate with screws and cerclage cables
Total femoral replacement Corrent answer: 2
This fracture pattern is typically referred to as an interprosthetic fracture; this is increasing in incidence due to increasing numbers of patients with ipsilateral hip and knee arthroplasty.
The first reference by Ricci et al reviewed 50 Vancouver B1 fractures treated with a lateral plate without allograft. They reported 100% union rate at a mean of 12 weeks and only one deep infection. Nearly 75% of patients were able to return to their baseline ambulatory status.
The second reference by Ricci et al reviewed 59 patients with periprosthetic femur fractures (THA or TKA) treated with ORIF without bone grafting. They report 58/59 patients healed after the index procedure and 49/59 were able to
return to their baseline functional level.
The reference by Fulkerson et al reported on 24 patients who underwent LISS plate fixation of periprosthetic femur fractures around well-fixed THA or TKA. They reported union in 21/24 at a mean of 6.2 months, with only one failure of fixation. They note that percutaneous fixation is effective although technically demanding.
Figure A shows an interprosthetic femur fracture between well-fixed hip and knee arthroplasties.
Incorrect Answers:
OrthoCash 2020
A 62-year-old female undergoes an uncomplicated primary total knee replacement. Her knee range-of-motion pre-operatively was 0-135 degrees of flexion. Which of the following is true regarding the immediate post-operative use of a continuous passive motion machine in this patient?
Reduced risk of venous thromboembolism
No long-term difference in ROM compared to patients not using CPM
Increased passive knee flexion at 6 months
Increased length of hospitalization
Decreased risk of surgical site infection Corrent answer: 2
The use of a continuous passive motion (CPM) machine following primary total knee arthroplasty has not shown any long-term benefits with regards to
range-of-motion.
The concept of CPM was created by Dr. Robert Salter in 1970 and is currently being used in select patients following total knee replacement, ACL
reconstruction, and a variety of other procedures about the knee. In theory, the CPM allows for movement of synovial fluid to allow for better diffusion of nutrients into damaged cartilage. Additionally, it has been thought to prevent fibrous scar tissue formation about the joint. While some studies have shown increased early active knee flexion at two weeks, these results were not significant at later follow-up. Controversy exists as to whether these small benefits offset the patient inconvenience and expense of the CPM.
Lotke et al. expolre the effects of tourniquets and CPM machines in 121 patients undergoing total knee arthroplasty. They found that immediate CPM combined with intraoperative release of the tourniquet increased blood loss. The patients with the least amount of blood loss had the tourniquet released after a compressive dressing was applied and in whom CPM was delayed for a few days.
Bourne et al. perform a meta-analysis on the effectiveness of CPM following total knee arthroplasty. They found the CPM plus physical therapy increased active knee flexion more than physical therapy alone 2 weeks after surgery with a decreased length of hospitalization. The benefits of increased active knee flexion were not maintained after 2 weeks.
Illustration A shows an example of a CPM machine. Incorrect Answers:
from available RCTs to conclude that CPM reduces the risk of venous thromboembolism following total knee arthroplasty.

OrthoCash 2020
A 67-year-old female complains of anterior groin pain one year following a primary, uncemented total hip arthroplasty. The pain is exacerbated when she tries to climb stairs or get up from a seated position. She denies any recent fevers or chills. On physical exam, the pain is reproduced with resisted seated hip flexion. Laboratory analysis, including WBC, ESR, and CRP are within normal limits. Radiographs reveal that the components are appropriately positioned without evidence of loosening or fracture. Which of the following is the most appropriate at this time?
Revision of the acetabular component
Image-guided diagnostic injection of lidocaine into the iliopsoas tendon sheath
Hip aspiration
Bone scan
Conservative management including activity modifications, NSAIDs, and physical therapy
The patients history and physical exam are most consistent with iliopsoas impingement. This diagnosis is most reliably confirmed with a diagnostic/therapeutic injection of steroid or lidocaine into the iliopsoas tendon sheath.
Iliopsoas tendinitis following total hip arthroplasty is an uncommon but treatable cause of anterior groin pain following total hip arthroplasty. The true incidence is unknown, but some studies suggest it is the cause of a painful
total hip arthroplasty in up to 4.3% of cases. Potential causes include a malpositioned acetabular component, excessively long screws, limb length discrepancy, or retained cement. Diagnosis is confirmed by injecting the iliopsoas tendon sheath. Most cases are refractory to conservative management and often require surgical intervention. In the case of a malpositioned acetabular component, revision to a more agreeable position is advisable. In the absence of a defined etiology, iliopsoas tendon release offers adequate pain relief and return to function in a majority of patients.
Lachiewicz et al. review anterior iliopsoas impingement after total hip arthroplasty. They state that most patients with iliopsoas impingement often require surgical treatment, with options including iliopsoas tendon release or resection, removal of protruding cement or screws, and acetabular revision.
O' Sullivan et al. review 16 cases of iliopsoas impingement following primary total hip arthroplasty. Only 1 of the cases was secondary to a malpositioned acetabular component, with the other 15 cases being attributed to altered anatomy of the iliopsoas tendon as a result of the surgery. These 15 patients underwent iliopsoas tendon release, and all had improvement in pain and function following surgery.
Nunley et al. review 27 patients with a presumed diagnosis of iliopsoas impingement following total hip arthroplasty who were treated with fluoroscopically guided injections of the iliopsoas bursa. The average modified Harris hip score in the patients who underwent injection improved, however, 30% required an additional injection and 22% underwent surgical release for continued pain.
Illustration A shows a flouroscopic injection into the iliopsoas tendon sheath. Incorrect Answers:
revision of the acetabular component without a confirmed diagnosis is not advisable.
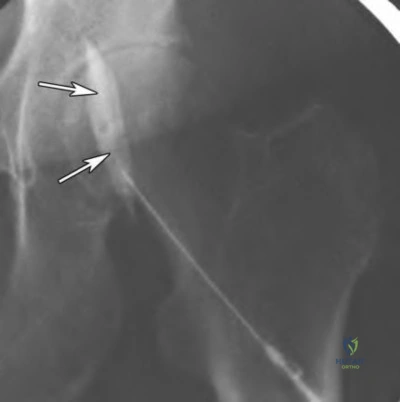
OrthoCash 2020
A 72-year-old female underwent an uncomplicated primary total hip replacement 18 years ago. Current radiographs reveal the abnormality shown in Figure A. Which of the following cell types (Figures B-F) is implicated in the process shown by the arrow?

Figure F shows an example of a macrophage, which is a key mediator in the osteolytic process shown in Figure A.
Osteolysis is the end result of a biologic process that begins when the number of wear particles following a joint replacement overwhelms the body's capacity to clear them from circulation. The residual particles are phagocytosed by macrophages, which then release an array of cytokines and other inflammatory mediators that recruit osteoclasts to resorb bone.
Gupta et al. review osteolysis following total knee arthroplasty, including etiology, diagnosis, and management. Amongst other things, they highlight the importance of design changes to minimize osteolysis including highly cross-linked polyethylene and alternative bearing materials.
Ren et al. performed a study where they implanted a hollow titanium rod into the distal femur and pumped polyethylene particles into the femoral bone marrow cavity. They found that macrophage migration occurs at a systemic (rather than local) level, and that the recruitment of macrophages led to localized osteolysis.
Holt et al. review the biology behind aseptic osteolysis. Specifically, they highlight the importance of the RANK-RANKL-OPG pathway as the final
common pathway to osteoclastogenesis, and the possibility of eliminating osteolysis by blocking this pathway. AMG-162 is a human immunoglobulin monoclonal antibody with a high affinity for RANKL, and studies are currently being undertaken to determine its safety and efficacy.
Figure F shows an example of a macrophage, which may be identified by its irregular shape and phagocytic inclusions. Illustration A shows the pathway by which marcrophages induce osteolysis following a joint replacement surgery.
Incorrect Answers:
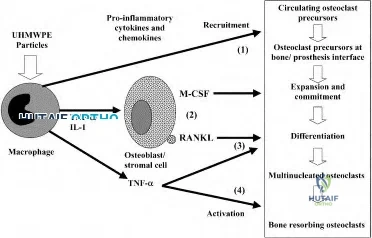
OrthoCash 2020
A 45-year-old with a history of sickle cell anemia reports hip pain for the past 6 months. A radiograph of the affected hip is shown in Figure A. Which of the following interventions has been shown to have the best outcomes in this patient population?

Observation
Bisphosphonates
Hemi-arthroplasty
Uncemented metal on polyethylene total hip arthroplasty
Cemented metal on polyethylene total hip arthroplasty Corrent answer: 4
Based on the radiographs and current literature, the best intervention is an uncemented metal on polyethylene total hip arthroplasty.
Avascular necrosis of the hip may be idiopathic in nature or associated with alcoholism, steroid use, or as in this case, sickle cell anemia. The Ficat staging system is used to classify avascular necrosis of the hip. Changes in treatment are driven by development of symptoms as well as the development of subchondral bone collapse (Ficat Stage 3). In those with with femoral head flattening (Ficat Stage 4) and acetabular degenerative changes (Ficat Stage 5), total hip replacement has good to excellent outcomes.
Mont et al. review surgical options for avascular necrosis of the hip. Head preserving procedures are generally reserved for those patients where the femoral head has not collapsed. Collapse and associated arthritis warrant utilization of arthroplasty procedures.
Mont et al. conducted a systematic review to better delineate the symptomatic progression of asymptomatic avascular necrosis of the hip. They found that patients with sickle cell disease have the highest rate of progression to
collapse. Medium sized, laterally located lesions were associated with a higher frequency of collapse and joint preserving procedures are recommended for these.
Figure A shows radiograph of a patient with avascular necrosis; note the femoral head flattening, narrowing of the joint space and acetabular sclerosis.
Incorrect Answers:
OrthoCash 2020
The function of which of the following structures is to resist internal tibial rotation with the knee in full extension?
Anterior cruciate ligament
Iliotibial band
Popliteus tendon
Popliteofibular ligament
Posterior oblique ligament Corrent answer: 5
The primary function of the posterior oblique ligament is to resist internal tibial rotation with the knee in full extension.
The posterior oblique ligament is a structure within the posteromedial corner of the knee, with attachments proximally to the adductor tubercle of the femur and distally to the tibia/posterior knee capsule. The posterior oblique ligament and posteromedial capsule play a significant role in the prevention of additional posterior tibial translation in the knee in the setting of posterior cruciate ligament injury. They also act to resist internal tibial rotation with the knee in full extension.
Griffith et al. reports that the posterior oblique ligament provides significant resistance to valgus and internal rotation forces with knee extension. They used a cadaver model and demonstrated that the superficial MCL resists valgus and external rotation forces more than the posterior oblique ligament, while the posterior oblique ligament is more involved in resisting internal rotation.
Tibor et al. reviews the anatomy of the posteromedial corner of the knee. They report that failing to recognize injury to these structures may cause failure of cruciate ligament reconstruction surgery, and that reconstruction or repair of the posteromedial corner may be indicated in the face of multiple ligament injuries.
Illustration A shows the posteromedial corner of the knee, including the posterior oblique ligament.
Incorrect answers:
4: These structures are not primary restraints to internal tibial rotation in full extension.
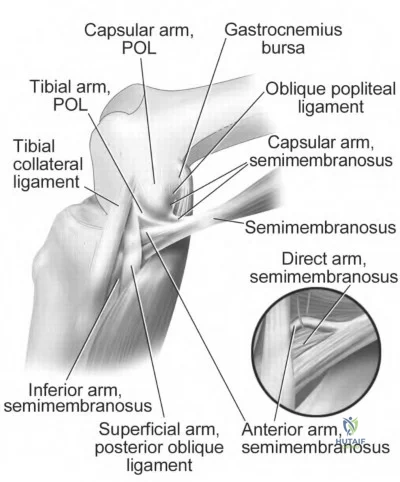
OrthoCash 2020
Increasing the porosity of a cement spacer for an infected total knee arthroplasty leads to which of the following?
Increased strength
Increased elution of antibiotics
Increased cement density
Improved cement-prosthesis bonding
Increased reinfection rate Corrent answer: 2
Elution of an antibiotic is increased with increased porosity of a cement spacer. This porosity increase can be obtained with hand mixing and avoiding the use of a vacuum-type mixing device.
Joseph et al. reviews antibiotic-impregnated cement in hip arthroplasty. They note that use of this cement in one- or two-stage revisions has lowered reinfection rates, with the spacers acting to reduce dead space while stabilizing the joint.
Cui et al. reviews antibiotic impregnated cement for TKA and THA. They report that use of greater than 2 grams of antibiotic per 40 gram unit of cement weakens the cement and that use of two antibiotics in conjunction may potentially increase elution.
The reference by Stevens et al compared Simplex and Palacos bone cement in regards to elution in a TKA mold model. They found that initial as well as weekly (9 weeks total) elution rates were greater in the Palacos spacers than the Simplex models. They recommend use of the Palacos cement in TKA model to target antimicrobial delivery while limiting the potential for systemic antibiotic-related toxicity.
Illustrations A and B show an antibiotic spacer in a two-stage revision TKA. Illustration C shows a PROSTALAC in a two-stage revision THA.
Incorrect Answers:

OrthoCash 2020
A 65-year-old patient was treated with an open reduction/internal fixation for a left femoral neck fracture sustained 25 years ago. Five years ago he developed hip pain and was converted to a left hip hemiarthroplasty. He presents with complaints of groin pain for the past 6 weeks. A recent radiograph is shown in Figure A. The patient’s physical exam is limited secondary to pain. Serum laboratory values are WBC-8.0, ESR-20, CRP-0.5. A synovial fluid aspirate of the hip demonstrates < 500 cells (60% PMN). What is the most likely cause of this patient's symptoms?

Acetabular protrusio
Infected hip hemiarthroplasty
Lumbar radiculopathy
Impingement of the hip hemiarthroplasty
Iliopsoas tendinitis
Based on the history, radiographs, and laboratory values, the patient has developed failure of his hip hemiarthroplasty. At this point in time he warrants a conversion to a total hip arthroplasty.
Avascular necrosis (AVN) of the femoral head after traumatic injury to the femoral neck occurs at an incidence of 10-45%. Although the risk increases with failure to anatomically reduce the fractue, it can still occur in non displaced settings. Treatment of avascular necrosis in older patients includes hip hemiarthroplasty or a total hip replacement. With the former, development of acetabular protrusio can contribute to groin symptoms. Functional outcomes have been reported to be higher in those receiving total hip replacement for AVN of the femoral head.
Lee et al. prospectively compared the use of bipolar hip hemiarthroplasty versus total hip arthroplasty for advanced stages of AVN of the femoral head (Ficat Stage 3). Total hip scores were most improved in the total hip arthroplasty group. Migration of the outer head in the hemiarthroplasty group was seen in 23% of patients. They recommend use of a total hip arthroplasty in patients with Ficat Stage 3 AVN of the femoral head
Ito et al. evaluated the outcomes of patients who underwent bipolar hemiarthroplasties for femoral head avascular necrosis. They found that proximal migration and acetabular degeneration were risk factors for groin symptoms. They also found that outcomes were inferior to patients who had undergone total hip arthroplasty for AVN of the femoral head. They recommend use of total hip arthroplasty in advanced osteonecrosis of the femoral head
Diwanji et al. evaluated outcomes of patients who underwent a conversion from a bipolar hip arthroplasty to total hip arthroplasty in 25 patients. Thirteen (52%) patients were revised to THA because of acetabular erosions. Follow up was completed for an average of 7.2 years. At final follow-up, they found improvement of the Harris Hip Scores and improvement of the pain portion of the WOMAC index. They recommend use of total hip replacement as an option to salvage failed bipolar hip hemiarthroplasty
Figure A shows the radiograph of a hip hemiarthroplasty where acetabular protrusion has developed.
Incorrect Answers
OrthoCash 2020
A 38-year-old female patient presents to your office three years after a hip resurfacing. She complains of worsening left hip discomfort for the last 6 months. Her ESR is 12 (normal 0-20) and CRP is 1.2 (0-5). A radiograph and axial and coronal MRI scans are shown in Figures A, B, and C. What is the most likely diagnosis?
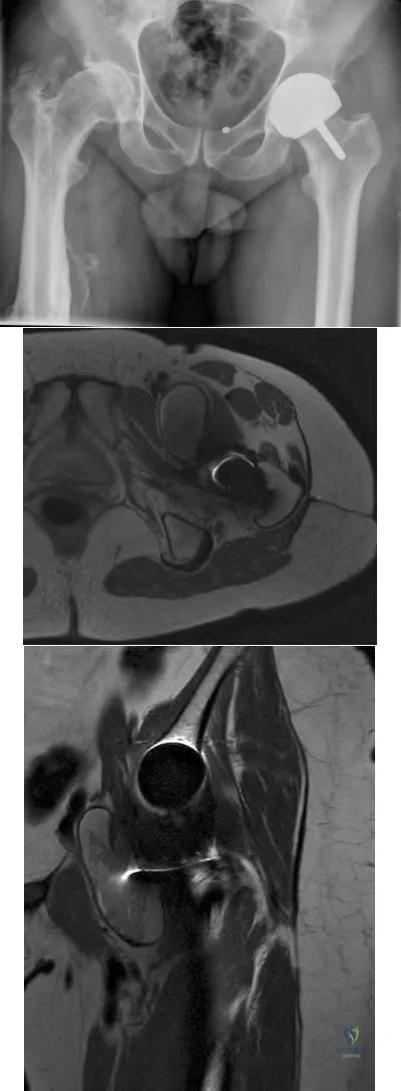
Infection
Type I Hypersensitivity reaction
Femoral neck fracture
Prosthesis Loosening
Pseudotumor
The clinical presentation is consistent with a young woman who has developed a symptomatic pseudotumor following hip resurfacing. Her hip discomfort is related to a mass that has developed around the left hip.
Pseudotumors, also referred to as Aseptic Lymphocyte-Dominated Vascular-Associated Lesions (ALVAL), are sterile inflammatory lesions that most commonly occur from metal-on-metal articulations. They occur at an incidence of 0-39% with metal-on-metal resurfacing hip components. The exact mechanishm of formation is unclear, however excessive wear is considered the initiating process, leading to the release of microscopic metal particles. These are cytotoxic to macrophages once phagozytised, leading to necrosis within the lesions and the development of semi-solid or fluid-filled masses around the implant. Lymphocytes are thought to be responsible for the tissue reaction.
Patients often do not complain of pain, but present with a mass around the hip that causes discomfort.
Hart et al. performed a case-control study comparing patients with well-functioning metal-on-metal hip resurfacing to those who have painful prostheses. They found no significant difference between the painfree and painful groups with MRI diagnosed pseudtumors (61% vs. 57%). They concluded that the presence of a pseudotumor should not automatically necessitate revision surgery.
Daniel et al. reviewed the current concepts surrounding pseudotumor. Risk factors associated with pseudotumor formation and failure are female gender, age under 40, hip dysplasia, metal hypersensitivity, and small components.
Larger components have been found to decrease the risk of failure.
Figure A is an AP pelvis radiograph of a patient following a left hip resurfacing surgery. Figures B and C are axial and coronal MR images demonstrating a large pseudotumor around the left hip resurfacing. Illustrations A and B identify the large pseudotumor as outlined in red.
Incorrect Answers:
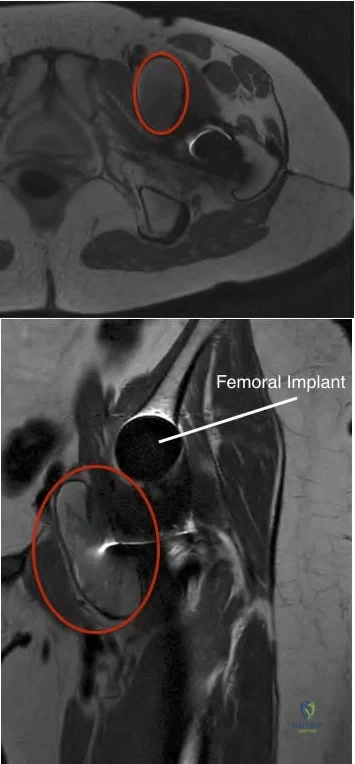
OrthoCash 2020
After total hip arthroplasty (THA) for osteoarthritis a patient is unable to dorsiflex her ankle or extend her great toe. She is treated conservatively with an orthosis and after 3 months on physical therapy she ambulates with a "slapping gait." What is the most appropriate next treatment option?
MRI of her spine
Ankle Fusion
Continue Ankle-Foot Orthosis
Revision total hip arthroplasty
Sural nerve grafting Corrent answer: 3
The patient has suffered from a peroneal nerve injury most likely from errant retractor placement during the hip replacement resulting in a foot drop. The most appropriate next treatment is an ankle-foot orthosis.
The ankle joint of an ankle-foot orthoses (AFOs) should restrict plantarflexion to prevent foot drop during the swing phase. In a patient who can not actively dorsiflex the foot the AFO keeps the foot in a neutral position during gait allowing for uninterrupted swing during ambulation.
Park et al reviewed common peroneal nerve injury after THA. Only one-half of the patients in the study who developed common peroneal nerve palsy following total hip arthroplasty recovered fully. The mean time to recovery was approximately one year for partial peroneal palsy and one and one-half years for complete palsy. Obesity adversely influenced the nerve recovery. Thus, at 3 months, the nerve should continue to be monitored and the use of an AFO would assist in ambulation.
Yokoyama et al. developed an AFO with an oil damper to adjust the plantarflexion resistive moment as excessive plantarflexion resistance will cause excessive knee flexion during the stance phase. They found the AFO with the oil damper achieved sufficient plantarflexion of the ankle and mild flexion of the knee by adjusting a proper plantarflexion resistive moment during initial stance phase, and provided a more comfortable gait than did the traditional AFOs.
Illustration A shows the location of the sciatic nerve relative to the short external rotators when performing a posterior approach to the hip.
Incorrect Answers:
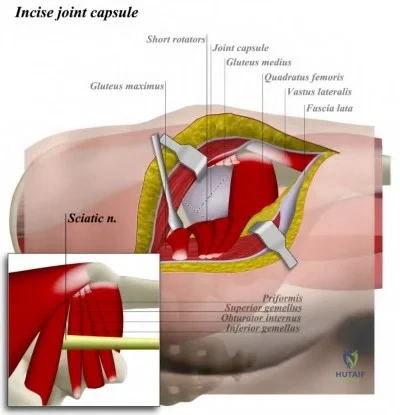
OrthoCash 2020
Which of the following statements is true about racial disparities in total joint arthroplasty?
The rate of surgical intervention for African American males is lower than white or Hispanic males
The rate of surgical intervention for Hispanics is higher than that for whites
The rate of surgical intervention for white males is lower than for African American males
There is no difference in the rate of surgical intervention between whites, Hispanics, or African Americans
The rate of surgical intervention is equal for Hispanic and white males Corrent answer: 1
The rate of surgical intervention for African American males is lower than either white or Hispanic males.
Numerous studies have shown clear racial disparities in the utilization of total joint arthroplasty for the treatment of osteoarthritis. African American and Hispanic patients undergo total joint arthroplasty at a rate much lower than
white patients, even in areas where insurance coverage is more equitable. Currently, little is known about the reasons for such disparities.
Skinner et al. reviewed the Medicare claims between 1998 through 2000 to determine any racial or ethnic disparities amongst patients undergoing total knee arthroplasty. Amongst other things, they showed that the arthroplasty rates for black men were consistently lower than white men in nearly every region.
Nelson reviews health disparities in orthopaedic surgery. Amongst other things, they discuss how African American patients and white patients perceive the same pain and functional limitations for similar radiographic disease. Thus, ethnic differences in perception of symptoms cannot explan the racial disparities noted in total joint arthroplasty.
Incorrect Answers:
OrthoCash 2020
A 65-year-old man presents with aseptic loosening 3 years after total knee arthroplasty. The surgeon reviews radiographs of his knee and takes him to the operating room for revision total knee arthroplasty. During surgery, the exposure technique shown in Figure A is used. Which of the following radiographs (Figures B-F) has the greatest likelihood of needing this exposure technique?

Figure A shows a tibial tubercle osteotomy (TTO). Patella baja (Figure D) is an indication for a TTO.
In revision total knee arthroplasty (TKA), surgical exposure should be extensile. Different exposure techniques have been described (see below). Patella baja may indicate that there is patellar tendon contracture. In this instance, a TTO can be used to prevent inadvertent patellar tendon avulsion which is difficult to repair and may lead to loss of function. Further, proximal transfer of the osteotomized tibial tubercle may be used to correct patella baja, bearing in mind that excessive superior translation alters the mechanics of the knee by making the quadriceps less efficient.
Younger et al. reviewed surgical approaches in revision TKA. They include quadriceps snip, patellar turndown, TTO, femoral peel, medial epicondylar osteotomy and quadriceps myocutaneous approach.
Mendes et al. reviewed the results of TTO in revision TKA. They advocate TTO for cases where the patellar cannot be retracted laterally with knee in 90deg of flexion. Complications include nonunion, tubercle fragment fracture and displacement, and tibial metaphyseal fracture (at the level of the distal cut of the osteotomy).
Della Valle et al. reviewed surgical approaches for revision TKA. They advocate TTO because repair is stronger than patellar turndown, there is less tension on the tibial tubercle in flexion than on the quadriceps tendon, and where multiple operations are required (as multiple VY approaches lead to excessive scar, making the approach difficult) or where stemmed tibial components need to be removed.
Illustration A shows tibial tubercle osteotomy hinged on a lateral periosteal flap. Illustration B shows quadriceps snip. Illustration C shows patellar turndown. Illustration D shows medial epicondyle osteotomy.
Incorrect Answers
situation.
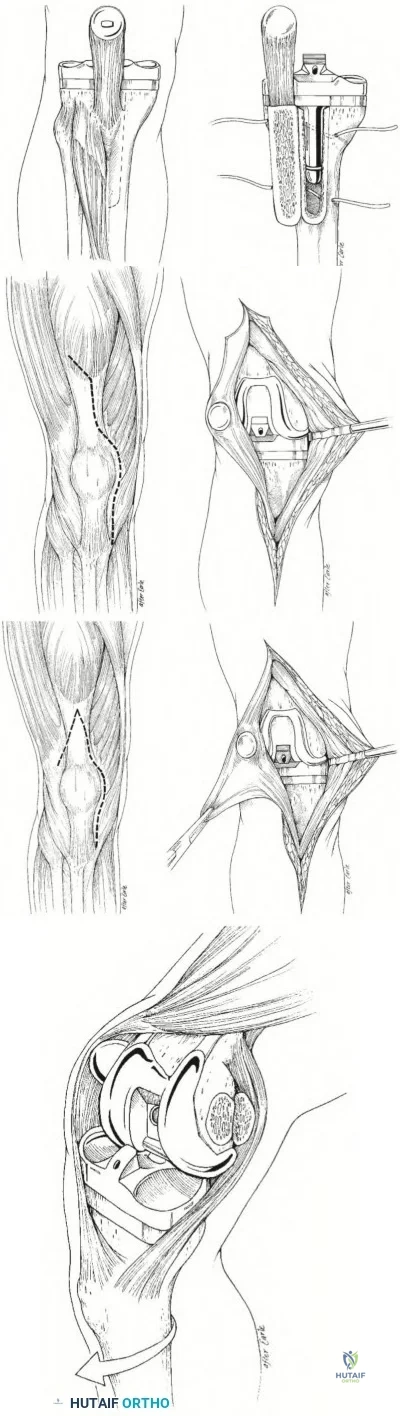
OrthoCash 2020
Which of the following is the most common intraoperative complication in a patient with sickle cell disease undergoing a total hip arthroplasty?
Periprosthetic fracture distal to the implant
Iatrogenic fracture causing pelvic discontinuity
Perforation of the femoral canal
Cardiac arrest from fat embolization to lungs
Injury to the sciatic nerve Corrent answer: 3
Perforation of the femoral canal during preparation of the femur is not an uncommon complication, with rates ranging from 4.9-18.2%.
While total hip arthroplasty is extremely effective for pain relief in patients with osteonecrosis of the hip secondary to sickle cell disease, the procedure carries a higher rate of complications compared with non-sickle cell disease patients. Particular attention should be given to the preparation of the femur as femoral medullary widening from chronic marrow hyperplasia adjacent to patchy areas of dense sclerosis can make preparation of the canal difficult.
Some surgeons prefer to ream over a guide-wire to avoid perforation.
Jeong et al. reviewed total hip arthroplasty in patients with sickle cell disease. Amongst other things, they discuss the difficulties associated with preparation of the femoral canal, quoting a perforation rate between 4.9-18.2%. They also state there are no prospective studies comparing cementless to cemented THA, but retrospective data has shown promising results with cementless components.
Hernigou et al. retrospectively reviewed 244 patients with sickle cell disease that underwent cemented total hip arthroplasty. They had a 3% infection rate, a relatively low rate of revision for aseptic loosening, and a 27% rate of medical complications. Overall, they viewed their results as favorable.
Illustration A shows a patient with bilateral AVN secondary to sickle cell disease. Note the areas of patchy dense sclerosis in the metaphyseal region of the proximal femur.
Incorrect Answers:
to be more common in this patient population. The rate of post-operative hematoma causing sciatic nerve dysfunction may be higher in this patient population.

OrthoCash 2020
A 63-year-old patient presents with periprosthetic joint infection 3 years after primary total knee arthroplasty. A radiograph of her knee is seen in Figure A. She undergoes 2-stage revision total knee arthroplasty. Radiographs taken at the time of explantation are seen in Figure B. An articulating antibiotic spacer is placed. Two months later, she is deemed to be free of infection and is taken to the operating room for the second stage operation. Intraoperatively, it is noted that the collaterals are intact and the previous tibial tubercle osteotomy had healed. What is the most appropriate surgical strategy at this point?

Address epiphyseal defects with impaction particulate bone grafting
Address metaphyseal defects with structural allograft and uncemented, unstemmed implants
Address metaphyseal defects with uncemented, porous metaphyseal
sleeves and uncemented, stemmed implants
Address diaphyseal defects with porous metal cones and uncemented, stemmed implants
Address diaphyseal defects with cemented stemmed implants Corrent answer: 3
This patient has massive metaphyseal defects following resection of primary TKA implants. Metaphyseal defects may be addressed with uncemented, porous metaphyseal sleeves and uncemented stemmed implants.
In revision settings, metaphyseal bone is often deficient. The Anderson Orthopaedic Research Institute classification (AORI) is most commonly used to classify defects. Stemmed implants are necessary to divert stress away from deficient metaphyseal defects to structurally sound cortical bone. These may be cemented or uncemented.
Haidukewych et al. reviewed metaphyseal fixation in revision TKA. For large defects, they advocate structural allograft, porous metal cones, and stepped metaphyseal sleeves.
Bush et al. reviewed managing bone loss in TKA. They cautioned that joint line elevation, distal femoral bone loss, and femoral prosthesis downsizing leads to flexion instability. They advocate cement filling for Type I defects, modular augments for Type 2, impaction grafting for Type 1 or 3, structural allograft for Types 2 and 3, metaphyseal filling or megaprosthesis for Type 3, including porous metal implants.
Figure A shows an infected primary TKA with a stemmed tibial component with medial augments. This suggests that the revision implant will require at least a stemmed, augmented component. Figure B shows massive metaphyseal defects (AORI Type 2) at the time of explantation. Illustration A comprises postop images of osseointegrated metaphyseal sleeves and stemmed implants. Illustration B depicts the AORI classification (see Review Topic for detailed description). Images courtesy of Haidukewych et al (Ref 1).
Incorrect Answers:
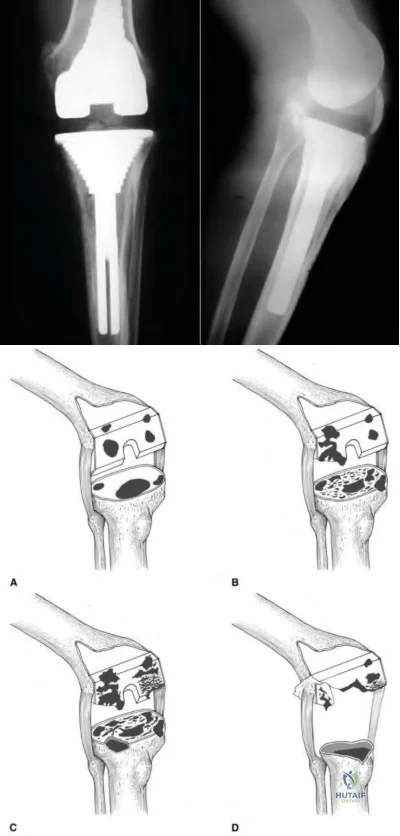
OrthoCash 2020
During templating for a total hip arthroplasty, placing the femoral head center of rotation directly superior to the center of rotation of the acetabular component will have which of the following effects?
Increase offset
Decrease limb length
Decrease offset
Increase limb length
No change in length or offset Corrent answer: 4
Placing the femoral head center of rotation directly superior (above) the acetabular center of rotation will lengthen the limb without changing offset.
When templating the femoral component for a total hip arthroplasty, it is imperative to restore limb length and offset. To change limb length, the femoral component center of rotation (COR) can be adjusted in a superior or inferior direction. If the femoral component COR is superior to the acetabular component COR, the limb will be lengthened (as in the example above).
Conversely, if the femoral component COR is inferior to the acetabular component COR, the hip will be shortened. A change in offset will be determined by the medial/lateral relationship between the acetabular and femoral components. In the example above, the COR of the femoral component is directly above the COR of the acetabular component. In this situation, there is no change in offset.
Merle et al. performed a retrospective cohort study to identify differences in femoral offset as measured on an AP pelvis radiograph, AP hip radiograph, and a CT scan. They found that femoral offset is significantly underestimated on AP radiographs of the pelvis. In contrast, AP radiographs of the hip are much more accurate in representing true offset.
Della Valle et al. review the importance of preoperative planning prior to total hip arthroplasty. While they mention that templating can be very accurate, determination of stem and cup size should also be determined by tactile feedback during broaching and reaming.
Illustration A shows the femoral head COR inferior to the acetabular COR. This will result in a decreased limb length.
Incorrect Answers:

OrthoCash 2020
Which of the following intra-operative errors most commonly leads to patellar maltracking during a total knee arthroplasty?
Using the gap balancing technique instead of measured resection technique
Internal rotation of the femoral component
External rotation of the tibial component
Lateralization of the femoral prosthesis
Overresection of the patella
Internal rotation of the femoral component increases the Q-angle and will increase the likelihood of patellar maltracking.
Patellar maltracking is one of the most common complications following a total knee arthroplasty. Any alteration that results in increased lateral retinaculum tension or an increased Q-angle may lead to patellofemoral instability.
Common causes include internal rotation of the femoral or tibial components, medialization of the femoral component, and placement of the patellar prosthesis on the lateral border of the patella. If a patient presents with postoperative maltracking and component rotation is thought to be the cause, a CT scan is the diagnostic study of choice.
Rhoads et al. analyze 7 cadaveric specimens to define the kinematics of the intact knee and to evaluate the effects of prosthetic replacement on those kinematics. Amongst other things, they showed that lateralization of the femoral component improved patellar tracking and prevented dislocation.
Malo et al. review patellar maltracking following a total knee replacement. They discuss the importance of externally rotating the femoral component on the femur relative to the posterior articular condyles to establish a rectangular and balanced flexion gap and to accommodate central patellar tracking.
Illustration A shows how an internally rotated femoral component displaces the patella medially. The blue line is a straight line upwards from the tibial tubercle, and the green line represents a line from the tibial tubercle to the center of the patella. The difference between the blue and green lines in the internally rotated prosthesis is the amount the patella has displaced medially. If you deviate the patella medially, this increases the Q-angle and could lead to patellar maltracking in a total knee replacement.
Incorrect Answers:
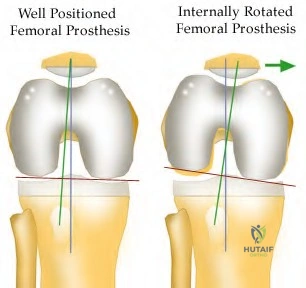
OrthoCash 2020
When performing a total knee arthroplasty on a 60-year-old female patient, a surgeon chooses not to resurface the patella. Instead, he performs a patelloplasty by excising the marginal osteophytes and reshaping the patella. All of the following statements comparing the results of patelloplasty to patella resurfacing are true EXCEPT:
There is no difference in relative risk of anterior knee pain.
There is no difference in relative risk for revision surgery involving the tibial and femoral components.
There is an increased risk that she will need secondary resurfacing.
No difference in rates of patellar avascular necrosis or patellar tendon injury.
Total knee arthroplasty improved function regardless of whether the patella was resurfaced.
In TKA with an unresurfaced patella, there is an increased risk of anterior knee pain and secondary resurfacing.
Surgeons can choose to resurface or not resurface all patellae, or selectively resurface patellae. In unresurfaced patellae, they may perform a patelloplasty (excise marginal osteophytes and reshape the patella). Unresurfaced patellae have increased risk of anterior knee pain requiring secondary resurfacing.
Indications for resurfacing include inflammatory arthritis, patella maltracking, patellofemoral osteoarthritis as the main indication for TKA.
Meneghini et al. reviewed the literature on patellar resurfacing. Prospective, randomized studies show conflicting results with regards to satisfaction rates between groups. Meta-analyses show increased risk of re-operation and anterior knee pain in the unresurfaced group.
Parvizi et al. performed meta-analysis on 1519 knees. They found there was
(1) lower relative risk of re-operation (resurfaced group), (2) lower relative risk of anterior knee pain (resurfaced group), (3) increased rate of secondary resurfacing (unresurfaced group), (4) no difference in patient satisfaction, (5) TKA improved function regardless of whether the patella was resurfaced, (6) no difference in complications.
Incorrect Answers:
OrthoCash 2020
A 55-year-old patient returns for followup 2 years after a left ceramic-on-ceramic total hip arthroplasty. He has no pain or symptoms of instability. The video in Figure V shows him ascending stairs. All of the following factors may contribute to this phenomenon EXCEPT
Impingement
Edge-loading
Loss of fluid film lubrication.
Third-body particles
Subclinical infection
The clinical presentation is consistent for prosthesis squeaking following a THA. Squeaking is multifactorial and may include impingement, edge-loading, loss of fluid film lubrication, and third-body particles. Subclinical infection does not play a role in squeaking.
Squeaking is defined as a high-pitched, audible sound occurring during movement of the hip. In ceramic-on-ceramic (COC) hips, the incidence is 0.5-10%. The incidence of revision because of squeaking is 0.5%. Squeaking is less common in metal-on-metal bearing surfaces (4-5%).
Chevilotte et al. reviewed COC bearing surfaces. They found that without lubrication, squeaking occurred with normal gait, high load, stripe wear, material transfer, edge wear and microfractures. In contrast, with lubrication, squeaking only occurred with material transfer.
Finkbone et al. reviewed COC total hip arthroplasty in patients <20-years-old after 52-month (average) follow-up. They found that survival rate was 96% with 1 revision for a loose acetabular component (failure of bone ingrowth). They found no cases of osteolysis, which can theoretically occur because of stripe wear, or femoral neck-on-liner impingement.
Walter et al. reviewed squeaking hips. They found that this phenomenon is associated with (1) walking, bending, rising (cyclical gait movements or extreme flexion), (2) maloriented acetabular components, (3) impingement,
(4) third-body particles, (5) edge loading, (6) loss of fluid film lubrication and
(7) thin, flexible (titanium) stem.
The video shows squeaking of a left total hip arthroplasty during hip extension from a flexed position. This is consistent with edge loading. Illustration A shows superior edge loading in the walking position. The arrow represents the loading force. The superolateral edge of the liner is in contact with the superior surface of the head. The dark area (area of edge loading) is anteverted with respect to a line of latitude (dark line) on the head. Illustration B shows posterior edge loading in the bending position. The arrow represents the loading force. The posterior edge of the liner is in contact with the superior surface of the head. The shaded area represents the area of edge loading and the dark stripe indicates wear on the femoral head.
Incorrect Answers:
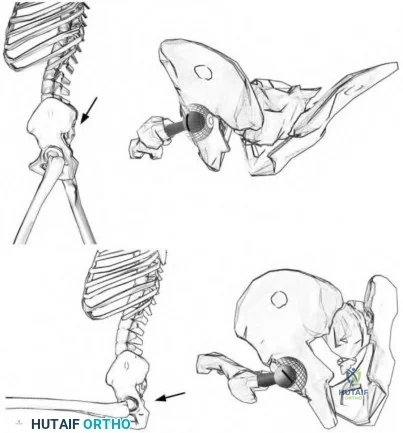
OrthoCash 2020
Figure A shows the image of a 72-year-old male who sustained a fall from standing. Past medical history is significant for hypertension. He was a community ambulator without the use of a cane or walker prior to the fall. During the operation, he is noted to have a well-fixed acetabular component without significant wear of his polyethylene liner, but his femoral component is easily extractable. Which of the following correctly pairs his Vancouver classification and appropriate surgical intervention?
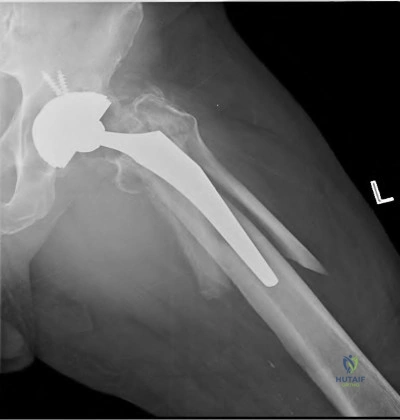
Vancouver A, Revision of femoral component to cemented stem with fixation of the fracture
Vancouver B1, Revision of femoral component to cemented stem with fixation of the fracture
Vanvouver B1, Revision of femoral component to a long, porous-coated, cementless stem with fixation of the fracture
Vancouver B2, Fixation of the fracture with a plate and cerclage wires
Vancouver B2, Revision of femoral component to a long, porous-coated, cementless stem with fixation of the fracture
Figure A shows a Vancouver B fracture around the femoral prosthesis. Because the prosthesis is noted to be loose during the operation, it is classified as a Vancouver B2 fracture. The most appropriate operation would be revision of the femoral component to a long, porous-coated, cementless stem in addition to fixation of fracture with a plate and cerclage wires.
According to the Vancouver classification, a type B2 fracture occurs around or just distal to a loose femoral stem with adequate proximal bone. Revision of the femoral component is necessary, with uncemented stems showing superior clinical results to cemented stems in most studies. The revision prosthesis should bypass the distal fracture by 2 cortical widths.
Corten et al. reviewed thirty-one patients with Vancouver B2 fractures that
were treated with a long cemented stem with additional allograft or plate fixation. At 46 months, none of the implants had to be revised, but it should be noted that 43% of the patients died within the first year.
Mulay et al. reviewed 24 patients with Vancouver B2 and B3 fractures managed with a cementless, tapered, fluted, and distally fixed stem. 91% of fractures united uneventfully. Complications included dislocations (5), nonunions (2), and infection (1).
Springer et al. review 116 patients with Vanvouver B fractures treated with revision of the femoral component. The uncemented, extensively porous-coated implants had the highest likelihood of stable fixation and were not associated with any nonunions.
Illustration A reviews the Vancouver classification for periprosthetic femur fractures. Illustration B shows a post-operative radiograph following a Vancouver B2 fracture. In this case, a trochanteric plate with cerclage wires was used to fix the fracture. A long-stemmed, porous-coated, cementless femoral prosthesis was used for the revision.
Incorrect Answers:
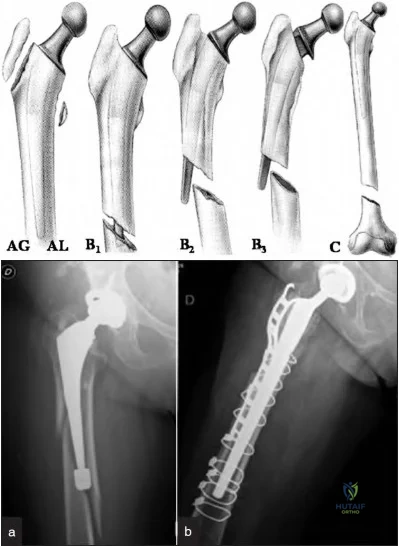
OrthoCash 2020
A 56-year-old male undergoes revision of his right hip arthroplasty for acute pain and radiographs suggestive of ceramic femoral head fracture. At the time of the revision, multiple fragments of the ceramic femoral head were seen in the joint and soft tissues. The components were noted to be in good position. He was copiously irrigated and the ceramic head was exchanged with a metallic femoral head. 12 months later, the patient presents with insidious onset right groin pain. Radiographs show no gross abnormalities without signs of loosening. Which of the following is the most likely cause of the patient's pain?
Periprosthetic infection
Massive third body wear
Pseudotumor formation
Soft tissue metallosis
Iliopsoas tendonitis
The most likely cause of the patient's pain is massive third body wear caused by retained ceramic fragments.
Cermamic femoral head fractures create many fragments that are difficult to extract at the time of revision surgery. During the revision surgery, it is imperative to remove all fragments that can be visualized. Despite a thorough debridement, microscopic fragments will still remain. These particles may cause pain through the creation of an inflammatory response in the tissues.
Exchange of the femoral head should be performed with another ceramic head, as opposed to a metal head. If a metal head is used, abrasive wear will ensue as the microscopic fragments will scratch the femoral head due to differences in hardness.
Traina et al. describe their experiences with revision of ceramic components. Most commonly, fractures of ceramic components occur as a result of trauma, dislocation, or errors in operative technique. These include head-neck taper mismatch, impacting the ceramic head with too much force, debris, and intraoperative damage to the metal neck taper.
Hannouche et al. review ceramics in total hip replacement. They state that if the ceramic is properly manufactured, it can be a highly effective, low-wear solution for the young patient in need of a total hip replacement.
Illustration A shows the typical ceramic femoral head used for a total hip arthroplasty. Illustration B shows a fractured ceramic head in many pieces.
Incorrect Answers:

OrthoCash 2020
Figure A and B are radiographs of a 77-year-old patient presenting with right hip and upper thigh pain for the past 3 months. He is an avid golfer and plans to travel south for 6 months on a golf tour. He denies fever, chills or weight loss. His past medical history includes hypertension and a right total hip replacement 15 years ago. Physical examination reveals minimal pain with range of motion. ESR=10 (normal range 0-20) and CRP=4 (normal range 0-10). He does not want any further surgery. The patient is at the highest risk of which complication with non-operative care?

Infection
Pseudotumour formation
Periprosthetic femoral fracture
Periprosthetic acetabular fracture
Dislocation
This patient has presented with significant osteolysis and aseptic loosening of his femoral THA component. If untreated, he is at an increased risk of a periprosthetic femur fracture.
Indications for surgery for periprosthetic osteolysis include: pathological fracture, impending pathological fracture, symptomatic THA with evidence of osteolysis, and extensive osteolysis that would compromise revision surgery in the future. The goal of surgery is to remove the loose component, repair/bypass/replace bone deficiency, and obtain stable component fixation.
Robbins et al. reviewed the causes of pain in THA. They report that hip pain can originate from the implant, soft tissue, or bone. The use of laboratory tests (e.g. ESR/CRP), radiographic and fluoroscopic imaging, hip aspirate, contrast arthrography and local anesthetic injections can help to determine the origin of pain.
Ollivere et al. report that the most frequent cause of failure after total hip replacement in all reported arthroplasty registries is periprosthetic osteolysis. Osteolysis occurs with the activation of macrophages and a complex biological cascade that results in bone loss.
Hirakawa et al. analyzed the circumstances around retrieved failed THA components. They showed that cement mantle defects, noncircumferential porous coatings, and screw holes are risk factors for osteolysis. They conclude by saying that the formation of a granulomatous tissue that ultimately invades the bone-implant interface is the final step in the pathogenesis of aseptic loosening.
Figure A and B show AP and lateral views of a right THA. The femoral stem shows gross loosening in all zones. Subsidence is obvious with a high-riding greater trochanter. The lateral cement mantle is fractured. There is endosteal erosion distally with the tip of the stem showing radiographic toggle.
Incorrect Answers:
osteolysis, but it remains well fixed. Acetabular fractures are less likely when there is minimal osteolysis.
OrthoCash 2020
A 60-year-old woman undergoes a total knee arthroplasty for end-stage osteoarthritis. Preoperative knee range of motion is 5 to 100 degrees. Postoperatively, she experiences reduced range of motion. She is scheduled to undergo manipulation under anesthesia. In which of the following scenarios is this procedure best indicated?
Knee range of motion 0 to 60 degrees at 2 months postoperatively
Knee range of motion 0 to 60 degrees at 8 months postoperatively
Knee range of motion 30 to 120 degrees at 2 months postoperatively
Knee range of motion 30 to 120 degrees at 8 months postoperatively
Knee range of motion 30 to 120 degrees at 2 weeks postoperatively
Manipulation under anesthesia (MUA) can achieve the greatest gains in flexion when performed for patients with less than 90 degrees of flexion within the first three months.
There are many risk factors for postoperative stiffness, the most important being preoperative stiffness. MUA is indicated when flexion is less than 90 degrees. Flexion gains are generally greater when applied early (6-12 weeks postoperatively) rather than late (>12 weeks). In cases with late-presenting stiffness (>12wks), MUA may still be attempted. Failed MUA is addressed with arthroscopic or open adhesiolysis +/- MUA, quadricepsplasty, or component revision.
Namba et al. compared the results of early (<90 days) vs late (>90 days) MUA. They found that: (1) knee flexion improved a mean of 32 deg and 20 deg after early and late MUA respectively, (2) extension improved in the early MUA group, but not the late MUA group, and (3) pain improved after early but not late MUA. Despite early MUA being more desirable, the authors state that patients with limited flexion at 6-12 months may still benefit from late MUA.
Keating et al. assessed the outcomes of MUA in 113 knees at a mean of 10 weeks after surgery. They found that (1) 90% of patients achieved
improvement in knee flexion of 35 degrees at 5 year followup, (2) there was no difference in flexion gains between early (<12 weeks) and late (>12 weeks) MUA and (3) patients treated with MUA had better pain control than those without MUA. They concluded that manipulation can result in significant and lasting improvement in knee flexion.
Incorrect Answers
OrthoCash 2020
A 62-year-old man is scheduled for a total knee arthroplasty. In his pre-operative office visit, he asks questions about different tibial components. You tell him that compared with the tibial component shown in Figure A, the tibial component shown in Figure B:
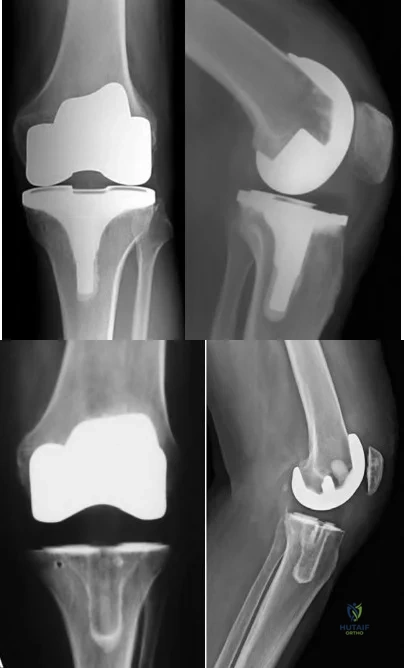
Is less expensive
Has greater durability
Has greater instability because of its monobloc nature
Provides improved short-term functional status, but no difference in long term functional status
Is associated with fewer adverse events because of easier implantation Corrent answer: 1
Figure B shows an all-polyethylene tibia (APT) component, which is $470 to
$1650 less expensive than metal-backed tibia (MBT) designs.
It was traditionally thought that modular MBT may have lower survivorship (compared to APT) because of locking mechanism dysfunction, breakage,
backside wear, and osteolysis. However, many studies now show the two to be comparable, with the only difference being that APT are less expensive.
Voight et al. performed a systematic review comparing APT and MBT. They found that the former was cheaper. There was no difference in adverse events, durability (need for revision or radiographic failure) at 2, 10, and 15 years, and functional status at 2, 8, and 10 years.
Toman et al. compared APT and MBT retrospectively. They found that APT implants perform as well as MBT implants in patients with BMI <37.5. There were 4 tibial implant failures in the MBT group in patients BMI >40.
Dalury et al. examined APT performance in obese patients (125 knees) after a minimum of 7 years. There were no implant failures. There were 5 nonprogressive tibial radiolucencies and 1 case of nonprogressive osteolysis.
Figure A shows a cemented metal-backed tibia component. Figure B shows a cemented all-polyethylene tibia component.
Incorrect Answers:
OrthoCash 2020
Figures A and B show pre- and post-operative radiographs of a sedentary 75-year-old female who underwent surgery on her left hip. Based on the radiographic findings, what was the most likely indication for revision surgery?
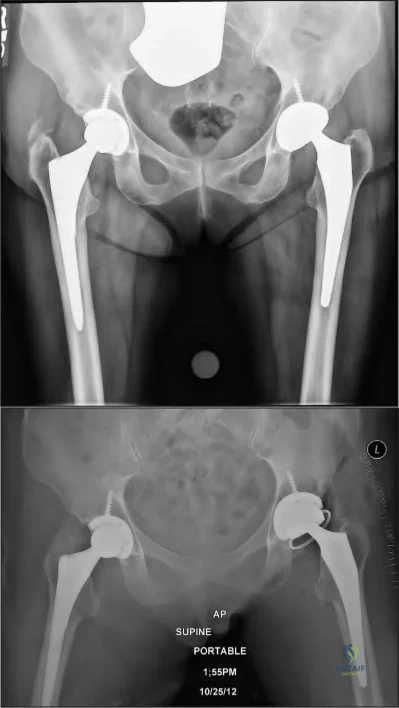
Left acetabular fracture
Left acetabular cup osteolysis
Left femoral stem osteolysis
Left hip instability
Left femoral stem valgus malalignment Corrent answer: 4
Figure A shows a left total hip arthroplasty with eccentric polyethylene wear. Figure B shows that her left hip was revised to a constrained acetabular liner, most likely a result of recurrent instability.
Revision strategies for hip instability are typically directed at correcting the underlying cause of instability. For example, instability most commonly occurs as a result of poor implant design, positioning or loosening, or the loss of soft-tissue function or tensioning. Operative strategies are designed to correct these etiologies by repositioning or exchanging components, integrating modular designs and improving soft tissue tensioning, etc. Constrained acetabular liners are often used in conjunction with these modalities to address the problem of recurrent instability relating to soft tissue deficiency and dysfunction in the affected hip.
Alberton et al. retrospectively reviewed 1548 revision arthroplasties for the incidence of dislocation. They found the overall dislocation rate to be 7.8%. Factors contributing to increased dislocations were found to be trochanteric non-unions, femoral heads <28mm in diameter and extensive soft-tissue dissection. Protective factors were modular acetabular components or liners, larger femoral heads >28mm and re-establishing abductor tensioning.
Paterno et al. retrospectively reviewed 438 primary and 181 revision total hip arthroplasties for patient factors contributing to dislocation. They found an overall dislocation rate of 6%. 23% of patients with a history of excessive intake of alcoholic beverages (more than six ounces a day) had at least one dislocation. There was no relationship between the variables of age, gender, obesity, or preoperative diagnosis and the incidence of dislocation.
Figure A shows bilateral primary cementless, nonconstrained total hip replacements. The left hip shows eccentric femoral head placement within the acetabulum indicative of eccentric polyethylene wear. Figure B shows the conversion to a constrained, dual-mobility, polyethylene liner. The overall metal component position appears satisfactory.
Incorrect Answers:
OrthoCash 2020
A 62-year-old woman is brought to the emergency room after falling down a flight of stairs. Prior to her fall, she had no knee pain and was a community ambulator without assistance. Intraoperatively,
it is determined that the implants are well-fixed. What is the best next treatment step to optimize her quality of life?

Closed reduction and long leg casting at 20 degrees of flexion for 6 weeks, followed by hinged-knee brace for 6 weeks.
Open reduction and internal fixation with a distal femoral locking plate
Open reduction and internal fixation with a condylar buttress plate
Distal femoral replacement arthroplasty
Closed reduction and fixation with an antegrade intramedullary nail Corrent answer: 2
This patient has a displaced far-distal supracondylar fracture around a stable TKA femoral component. Locked plating is the best option for management of this fracture.
Surgical fixation of periprosthetic fractures around a stable femoral component is challenging. Locked plating allows for multiple angle-stable fixation points around stems and lugs and does not depend on TKA design or quality of distal bone stock for fixation. Su Type I fractures may be treated with retrograde or antegrade intramedullary nailing. Type II fractures require retrograde intramedullary nailing or fixed-angle plating. Type III fractures require fixation with a fixed-angle device or revision arthroplasty when bone stock is poor.
Ricci et al. evaluated indirect reduction and locked lateral plating of Vancouver B1 THA fractures without allograft struts. They found that all fractures healed with satisfactory alignment and without implant loosening at an average of 12 weeks. They recommend this technique for stable Vancouver B1 fractures.
Streubel et al. examined the outcomes of locked plating in treatment of extreme distal periprosthetic supracondylar fractures located proximal to the flange (Su Types I and II) compared with fractures distal to the flange (Su Type III, see Illustration B). They found no difference in delayed union, nonunion, infection and failure rates between the 2 groups.
Figure A shows a Su Type III periprosthetic fracture around a TKA femoral component. Illustration A shows fixation of the same fracture with a distal femur locking plate. Illustration B shows the Su classification of fractures around the femoral component (Type I, proximal to the femoral component; Type II, starting at the anterior flange and extending proximally; Type III, fracture line distal to the anterior flange).
Incorrect Answers

OrthoCash 2020
Which of the following fractures would most likely require revision arthroplasty with a long-stemmed, uncemented prosthesis?

Figure B shows a Vancouver B2 periprosthetic femur fracture with an unstable femoral stem that requires revision arthroplasty with a long-stemmed prosthesis.
The Vancouver classification for periprosthetic femur fractures can help guide treatment of these challenging problems. Vancouver A fractures involve the greater and lesser trochanter and can be initially managed with non-operative measures. Vancouver B fractures occur around the stem and are broken down into B1 (stable prosthesis), B2 (unstable prosthesis) and B3 (poor proximal bone quality) fractures. B1 fractures may be treated with internal fixation, B2 fractures require a revision arthroplasty, and B3 fractures often require more advanced reconstruction with a proximal femoral replacement versus revision with a distally fixed prosthesis. Vancouver C fractures occur distal to the stem and require internal fixation.
Springer et al. reviewed 118 patients who underwent revision arthroplasty for Vancouver B2 periprosthetic fractures. They had a 90% survival rate at 5-years and a 79.2% survival rate at 10-years. The most common reasons for revision were loosening, infection, and non-union.
Illustration A shows the Vancouver classification of periprosthetic fractures about the femur.
Incorrect Answers:
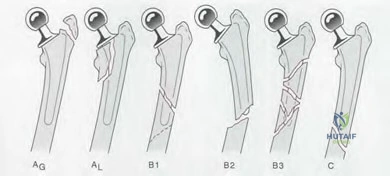
OrthoCash 2020
A 65-year-old female sustains a periprosthetic supracondylar femur fracture proximal to a well-fixed implant. She undergoes direct reduction and locked plating with a titanium distal femoral locking plate via an extensile lateral approach. At 9 months post-operatively, weightbearing is at 50% and is painful. Examination reveals mild swelling and warmth around the distal incision. Erythrocyte sedimentation rate and C-reactive protein are normal. Radiographs taken 9 months post-operatively are shown in Figure A. Which of the following may have increased the risk of this complication?
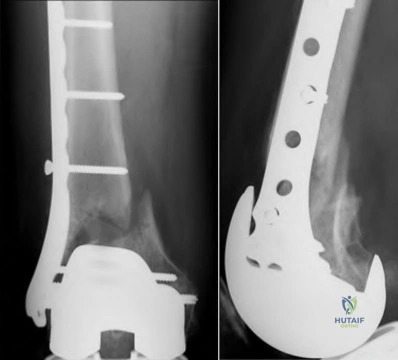
Neglecting to add topical rhBMP-2 on a carrier-scaffold
Neglecting to use lag screws and cerclage cables
Locked plating instead of locked antegrade nailing
Use of a titanium plate instead of a stainless steel plate
Use of an extensile lateral approach instead of a submuscular approach Corrent answer: 5
A submuscular approach has been shown to have less risk of nonunion than an extensile lateral approach. There is less disruption of soft tissue attachments and devitalization of fracture fragments with the submuscular approach.
The risks for periprosthetic fractures include notching, knee stiffness, osteoporosis, poor mobility and falls. The risk is higher in females and after revision surgery. The treatment of periprosthetic supracondylar fractures depends on the location of the fracture, fixation of the implant, and bone stock.
Hoffman et al. retrospectively reviewed 36 periprosthetic supracondylar femur fractures treated with locked plating. They found that submuscular plating had reduced nonunion risk compared to an extensive lateral approach. They recommend indirect reduction and submuscular plating to reduce the incidence of nonunion.
Hou et al. retrospectively reviewed 53 fractures fixed with retrograde nailing
(18) and locked plating (34). They found no difference in blood loss, time to union, operating time and hospital stay. They believe locked plating can
provide the same favorable results as retrograde nailing and recommend this technique for most patients and prosthetic designs.
Figure A shows nonunion and surrounding osteopenia after locked plating of a periprosthetic supracondylar fracture. Illustration A shows management of these fractures according to the Su classification.
Incorrect Answers
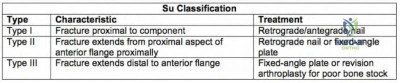
OrthoCash 2020
Immediately following a total hip arthroplasty (THA), a healthy 55-year-old patient is unable to dorsiflex her ankle or extend her great toe. After 4 weeks she continues to ambulate with a "slapping gait." Examination reveals passive ankle joint dorsiflexion to 10 degrees. What is the most appropriate next treatment option?
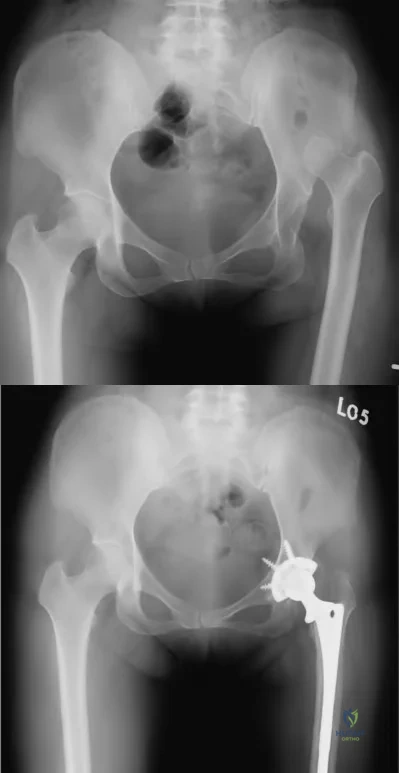
MRI of her spine and pelvis
Revision total hip arthroplasty
Ankle-foot orthosis
Posterior tibial tendon transfer to navicular bone
Neurology consult
This patient is presenting with foot drop after a THA for hip dysplasia (Crowe 4). The most appropriate treatment at this stage would be providing her with an ankle foot orthosis (AFO) for mobility.
Sciatic nerve injury after THA is an uncommon and difficult situation to manage. Patients with DDH that have undergone a large limb-lengthening procedure are at a greater risk due to the significant stretch of the sciatic nerve. Intra-operative procedures that have been shown to prevent this outcome include good pre-operative planning, limb lengthening <3 cm, subtrochanteric osteotomy, intra-operative wake-up test, and downsizing implant components if presenting with deficits peri-operatively. An ankle-foot orthosis may be used for foot drop when surgery is not warranted or during neurologic recovery.
Prahinski et al. reviewed the Bridle transfer for paresis of the anterior and lateral compartment musculature. Indications for the procedure include no neurological recovery for at least 18 months after injury or 18 months after the most recent attempt at exploration or repair of the nerve.
Electrodiagnostic changes must indicate permanent damage. In addition, there must be good passive range of motion, with at least 90° of dorsiflexion.
Edwards et al. reported on twenty-three peroneal and sciatic nerve palsies that occurred in patients following total hip arthroplasty. They showed that peroneal nerve palsy occurred with an average lengthening of 2.7 cm (1.9 cm-3.7 cm) in comparison with 4.4 cm (4.0 cm-5.1 cm) for sciatic nerve palsies.
Figure A and B show pre- and post-operative images of a patient with severe hip dysplasia treated with primary total hip arthroplasty.
Incorrect Answers:
OrthoCash 2020
A 60-year-old male with history of renal transplantation and previous intravenous drug abuse undergoes total knee arthroplasty. Two years later, he begins to have mild knee pain and low-grade swelling that persists for 10 months before he finally comes to the emergency room. Examination reveals no fever. Range of motion is 5 to 70 degrees. Erythrocyte sedimentation rate is 22mm/h, and C-reactive protein is 0.8mg/L. Knee aspiration reveals 12,000/mm3 nucleated cells with 76% neutrophils. Gram stain is negative and aerobic and anaerobic cultures are negative after 4 days in culture. His symptoms do not resolve after 5 days of empiric intravenous antibiotics and he is taken to the operating room for arthroscopic irrigation and debridement. Operative synovial tissue cultures are shown in Figure A. What is the best next step?
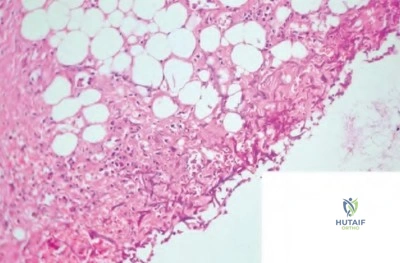
Cessation of immunosuppressant medication, lifelong antimycobacterial suppression
Open irrigation and debridement, implant retention and lifelong antifungal suppression
Open irrigation and debridement, resection arthroplasty, antimycobacterial drugs for 6 to 12 months
Open irrigation and debridement, single-stage exchange, antifungal drugs for 6 to 12 months
Open irrigation and debridement, two-stage exchange, antifungal drugs for 6 to 12 months
This patient has a fungal prosthetic joint infection (PJI) with Candida albicans. Optimal treatment involves resection arthroplasty, delayed reimplantation
arthroplasty, and antifungal drugs for 6-12 months.
Fungal PJI are uncommon. Risk factors include immune suppression and systemic illness e.g. diabetes and chronic renal failure. Candida species is usually the causative organism. The infection is usually indolent and systemic symptoms (e.g. fever) may be absent. ESR and CRP may be only minimally elevated. Two-stage exchange arthroplasty is standard of care.
Phelan et al. described delayed reimplantation in 10 patients with fungal PJI. They found that the median time from resection to reimplantation arthroplasty was 9 and 2 months for total hip and total knee arthroplasty respectively. Two patients had recurrence of infection. They recommend antifungal therapy and delayed reimplantation arthroplasty after confirmation of an infection-free period as the best chance for cure.
Azzam et al. retrospectively reviewed arthroplasty database data to identify 31 fungal PJIs in 6 centers. Delayed implantation was performed in 19 of 29 patients who underwent resection arthroplasty at an average of 7 months.
They recommend two-stage exchange arthroplasty as the treatment of choice, addition of antibacterial drugs to the cement spacer to prevent superinfection, antifungal drugs for 6-12 months, repeat joint aspirations prior to reimplantation, and optimization of host nutritional status prior to reimplantation.
Figure A is a high-powered micrograph showing synovial tissue covered by fibrinopurulent exudates containing fungal colonies of Candida albicans.
Incorrect Answers:
OrthoCash 2020
Which of the following non-operative treatments for osteoarthritis has the best evidence to support its use?
Combination of supervised and home exercise programs
Hyaluronic acid injections
Lateral heel wedge
Acetaminophen
Glucosamine
Of the options listed, a combination of home and supervised exercise has the best supporting evidence for the treatment of osteoarthritis.
The AAOS has recently developed guidelines for the treatment of osteoarthritis. Therapies that are recommended by the AAOS include weight loss, home and supervised exercise programs, and NSAIDs/tramadol.
Therapies that remain inconclusive (lack of supporting evidence) include electrotherapeutic modalities, manual therapy, bracing, acetaminophen/opiods, steroid injections and PRP. Glucosamine, lateral heel wedges and hyaluronic acid injections are not recommended, as current literature has shown them to be ineffective. Keep in mind that these guidelines are subject to change as new literature is published.
Zhang et al. present a systematic review of the literature on arthritis management in the three years following the original OA Research Society International (OARSI) guidelines published in 2006. While weight loss showed an increase in effectiveness with the addition of new studies, electromagnetic therapy, glucosamine, chondroitin sulfate, and hyaluronic acid injections showed a decrease in effectiveness.
Incorrect Answers:
OrthoCash 2020
Figure A shows the 2 bundles of the ACL dissected from a cadaveric knee off their bony attachments. They are labeled Bundle A and Bundle B, respectively. Which of the following is true?

The tibial attachment of Bundle A is anterior to Bundle B. In extension, Bundle B is loose and Bundle A is tight.
The tibial attachment of Bundle A is anterior to Bundle B. In flexion, Bundle B is loose and Bundle A is tight.
The tibial attachment of Bundle B is anterior to Bundle A. In flexion, Bundle B is loose and Bundle A is tight.
The tibial attachment of Bundle B is anterior to Bundle A. In flexion, Bundle A is loose and Bundle B is tight.
The tibial attachment of Bundle B is anterior to Bundle A. In extension, Bundle A is loose and Bundle B is tight.
Bundle A is the anteromedial (AM) bundle, which is longer, and is tight in flexion. Bundle B is the posterolateral (PL) bundle, which is shorter, and is loose in flexion. The AM bundle is attached anterior to the PL bundle on the tibia.
The ACL is comprised of 2 bundles. The AM bundle is longer than the PL bundle. Their names reflect their relative anatomic positions on the tibial insertion site. On the femur, the AM bundle begins at the proximal-anterior aspect of the femoral insertion site, while the PL bundle begins at the posterior-inferior part. In flexion, the AM bundle is tight and the PL bundle is loose. In extension, the AM bundle is loose and the PL bundle is tight.
Bicer et al. reviewed the anatomy of the ACL. They found that the AM bundle was longer (32mm) compared with the PL bundle (18mm). PL bundle carries greater force near full extension, and the AM bundle carries greater force after 15-45° of flexion. Under combined rotatory loads (valgus and internal tibial torque at knee flexion >30°), the AM bundle bore more force than the PL bundle.
Figure A shows the 2 bundles of the ACL. The AM bundle is longer than the PL bundle. The oft referred to length of ACL refers mainly to the length of the AM bundle. Illustrations A and B show the spatial relationships of the AM and PL bundles in a cadaveric knee. Illustration C shows the relative positions of the attachments of each bundle.
Incorrect Answers:
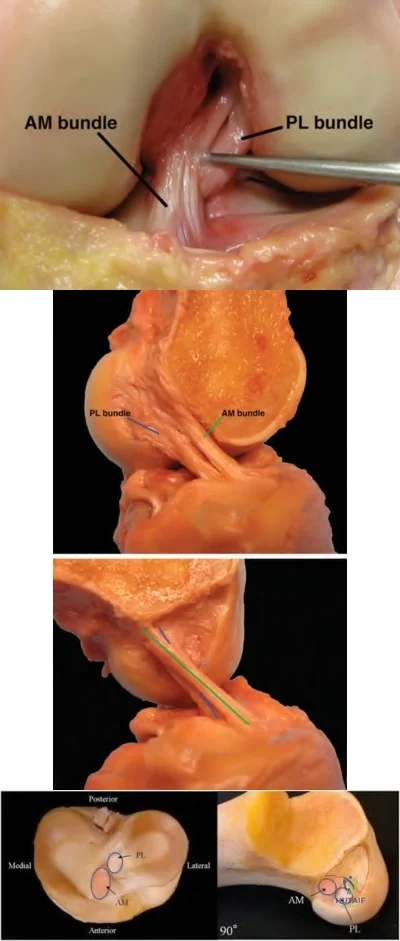
OrthoCash 2020
An 83-year-old man, who had a total hip arthroplasty performed 13 years ago, is referred to your office for evaluation. He reports worsening groin pain over the past year, which has been increasing in frequency. Prior to this past year, he had no other complaints. His current radiograph is shown in Figure A. If he continues to ambulate with this implant, he is at greatest risk for which of the following?

Infection
Acetabular component loosening
Femoral component loosening
Dislocation
Periprosthetic fracture
The patient has eccentric polyethylene wear secondary to component malpositioning. He is at highest risk for dislocation.
Late dislocation following total hip arthroplasty(THA) can occur and has a high recurrence rate, thereafter. Risk factors include eccentric polyethylene, THA at an early age, neurologic decline or associated neurologic conditions (i.e.
Parkinson's disease), or associated trauma.
Parvizi et al. noted in this instructional course lecture that eccentric, excessive polyethylene wear is one of the most common reasons for late, recurrent dislocation. Revision is recommended.
Pulido et al. in this review, reiterated that polyethylene wear can lead to increased inflammation, capsular distention, and instability, increasing risk for dislocation.
von Knoch et al. reviewing over 500 dislocated hips, also noted that eccentric wear was one of major causes linked to late dislocation.
Figure A. exhibits a left total hip arthroplasty with eccentric wear. Incorrect answers:
OrthoCash 2020
Figure A shows a radiograph of a 62-year-old female that underwent a left total hip arthroplasty 5 years ago. She presents to your office with insidious onset of left groin and buttock pain. She denies trauma, fever or chills. On physical examination, her left hip has mild pain with range of motion. She has a normal gait cycle, normal power across the hip and her vitals signs are stable. A left hip aspirate was performed and results are shown in Figure B. What is the most likely cause of her hip pain?
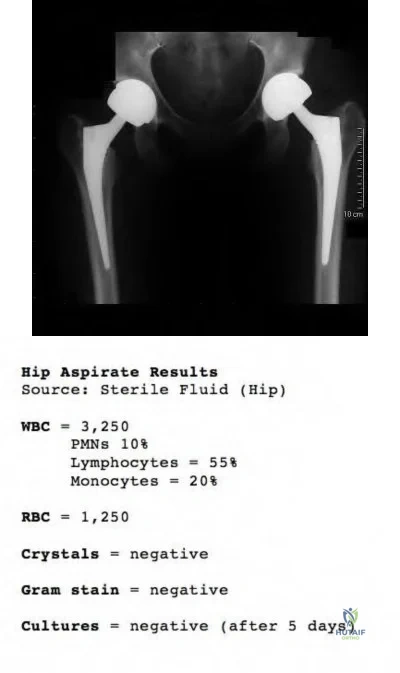
Periprosthetic bacterial hip infection
Periprosthetic hip fracture
Large-particle wear debris disease
Pseudotumor hypersensitivity response
Abductor tendon tear Corrent answer: 4
This patient is presenting with a metal induced system hypersensitivity response in the setting of a metal-on-metal total hip arthroplasty.
A hip aspiration of a painful THR is a very useful investigation for the work up of infection, having a sensitivity of 75-85% and specificity of 85-100% for
infection. Metal-on-metal THA may mimic infection as aspirate results will often show increased inflammatory infiltrate, with synovial WBC counts in the thousands. However, infected THA are more likely to produce higher percentages of PMNs (>70%) in comparison to hypersensitivity reactions/ adverse reaction to metal debris, which are more likely to produce a higher percentage of lymphocytes (>40%).
Campbell et al. looked at the histological features of pseudotumor-like tissues from metal-on-metal hips. They found that the patients with hip pain and suspected metal sensitivity had fewer metal particles but more aseptic lymphocytic vasculitis-associated lesions compared to patients with evidence of metallic wear. They concluded that pseudotumors occur more because of a hypersensitivity reaction than particle wear.
Kwon et al. examined a small cohort of patients with metal-on-metal hip arthroplasties to investigate the incidence and level of metal-induced systemic hypersensitivity. They found that lymphocyte reactivity to Co, Cr, and Ni did not significantly differ in patients with pseudotumors compared to those patients without pseudotumors. This suggests that systemic hypersensitivity type IV reactions may not be the dominant biological reaction involved in the occurrence of the soft tissue pseudotumors.
Figure A shows a patient with bilateral metal-on-metal total hip arthroplasties. There are no identifiable fractures. The position of the left acetabular cup is slightly vertical, which can increase edge loading and particle wear. Figure B shows the results from the hip aspirate.
Incorrect Answers:
OrthoCash 2020
A 72-year-old patient is scheduled to undergo revision total hip arthroplasty. A 3D-model of the patient's hemipelvis is constructed for pre-operative planning and is shown in Figure A. A custom-designed implant shown in Figure B is created. Which of the following is TRUE of the planned reconstruction?

The implant is a bilobed cup.
The most common complication is dislocation.
The acetabular defect can be classified as AAOS Type V.
Radiation-compromised bone stock is a contraindication.
The winged profile of the implant facilitates insertion through both anterior and anterolateral approaches.
The patient has pelvic discontinuity that will be reconstructed with a custom triflange acetabular component. Dislocation is the most common complication.
Custom triflange acetabular components are indicated for severe acetabular bone loss and pelvic discontinuity that are not amenable to treatment with off-the-shelf implants such as reconstruction plates, jumbo cups and antiprotrusio cages. Dislocation is common and possible etiologies include extensive dissection, less reliable soft tissue repair, deficient abductors/trochanteric nonunion, superior gluteal nerve stretch neuropraxia, and surgeon reluctance to use constrained liners in the face of poor bone stock.
Christie et al. reviewed reconstruction with the triflange cup in 78 hips with AAOS Type III (combined deficiency) or Type IV (pelvic discontinuity) defects. They found improvement in Harris hip scores, limp, need for walking aids.
Dislocation was the most common complication (15.6%, 12 patients), and half of these patients (6/12) needed re-operation for recurrent dislocation. They recommend the triflange cup for difficult reconstructions involving severe bone loss.
Taunton et al. reviewed 57 patients with pelvic discontinuity treated with a custom triflange component. They found that 21% developed instability (10 required revision, and 2 treated nonoperatively). Of note, 51% had preop trochanteric escape (nonunion of the greater trochanter to the femoral component or femur with >1cm of displacement. They recommend the custom triflange implant for discontinuity as it provides predictable midterm fixation and consistent healing.
Figure A is a 3D hemipelvis model generated by stereolithography from a patient’s CT scan. It shows massive bone loss and pelvic discontinuity. Figure B is a custom hydroxyapatite (HA)-coated porous triflange acetabular prosthesis with ilial and ischial screw holes. Illustration A shows a bilobed cup and its appearance on an AP radiograph.
Incorrect Answers:
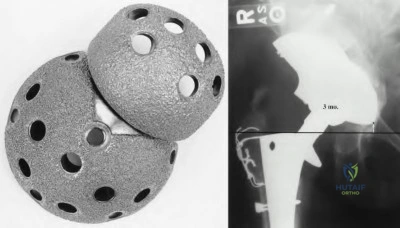
OrthoCash 2020
All of the following are risk factors for wear-related failure in total knee arthroplasty when using a polyethylene liner that underwent sterilization via gamma irradiation in air EXCEPT?
Increasing shelf age of polyethylene liner
Younger age of patient
Male gender
Posterior cruciate retaining knee design
Use of a rough tibial baseplate Corrent answer: 4
Increasing shelf age, younger age, male gender, and a rough tibial baseplate are all risk factors for wear-related failure in total knee arthroplasty when using a polyethylene liner. Posterior cruciate retaining knee design is not a documented risk factor.
Fehring et al reviewed 2091 TKA using the Press fit condylar system and noted that the 13-year survivorship for all patients was 82.6% with a 8.3% prevalence of wear-related failure. Cox hazards analysis revealed five variables that were correlated with wear-related failure: patient age, patient gender, polyethylene sheet vendor, polyethylene finishing method, and polyethylene shelf age. They were unable to identify one factor as the defining reason for these wear-related failures. They cautioned that these findings may only be specific to inserts that underwent sterilization via gamma irradiation in air.
Collier et al followed 365 TKA (PCL-retaining) for 5-10 yrs and noted that
factors related to polyethylene insert osteolysis included advanced shelf age, sterilization method, and the material from which it was machined. Osteolysis was identified in 34% with an insert that had been gamma-irradiated in air and affixed to a rough baseplate surface, but only 9% when the insert had been gamma-irradiated in an inert gas or not irradiated at all and joined to a polished surface.
OrthoCash 2020
A 65-year-old healthy patient fell 18 years after a total hip arthroplasty and sustained the fracture shown in Figure A. Which of the following would be the most appropriate treatment?

Percutaneous locked plating
Open reduction internal fixation with a cable plate and allograft strut
Revision to a long femoral stem with allograft bone
Revision to a cemented revision femoral stem that bypasses the fracture site by 5 cm
Three months of non-weight bearing Corrent answer: 3
The Vancouver classification of periprosthetic femur fractures is based on the fracture site, implant stability, and remaining bone stock. The patient in the question has a type B3 fracture. The cemented stem is loose and there is very poor remaining bone stock. He should be treated with a long, cementless
revision stem with biplanar strut grafts. A tumor prosthesis or allograft-prosthesis composite would be alternate possibilities. Illustrations A and B are a diagram and table of the Vancouver classification of periprosthetic hip fractures.
Springer, et al. looked at the results and complications of revision total hip arthroplasty for the treatment of acute Vancouver type-B periprosthetic femoral fracture. In their series they treated these fractures in multiple ways, including cemented stems, uncemented stems, allograft-prosthetic composite, or tumor prosthesis. They concluded that the best results were with an uncemented, porous coated femoral stem, and the most common cause of revision was loosening.
Parvizi, et al. concluded that due to the poor bone quality and delayed healing of older patients & their periprosthetic fractures that it is imperative that a strong mechanical construct be achieved in the treatment of these fractures. They “advocate the use of numerous screws with purchase of at least ten cortices and reinforcement of fixation with biplanar strut allografts whenever possible. When a revision stem is used, we ensure that adequate diaphyseal fixation is obtained and the fracture is traversed by at least 5 to 8 cm.”
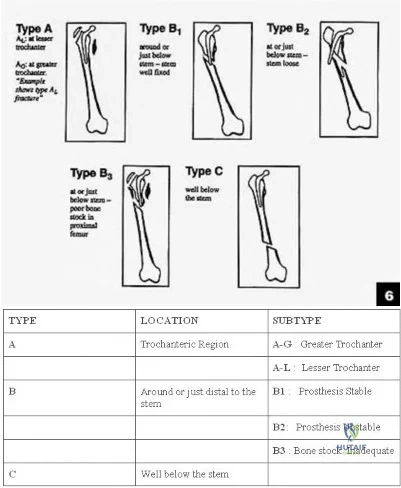
OrthoCash 2020
A 85-year-old man who underwent hemiarthroplasty 5 years ago now complains of thigh pain for the past four months. Laboratory studies show a normal white blood cell count (WBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). An aspiration of the hip is performed and is negative for infection. A radiograph is shown in Figure A. Which of the following is the best management option for the femoral implant?

Bone scan to look for loosening
Touch down weight bearing and physical therapy
Revision with a tumor prosthesis
Revision of femoral component with metaphyseal cement fixation of the stem
Revision to a cementless femoral component with diaphyseal press-fit fixation of the stem
The radiograph shows lucency around the femoral stem cement mantle consistent with loosening. There is bone loss in the proximal femur. Diaphyseal fixation is the best option from the choices available. Revision to a cementless femoral stem is the most appropriate management.
Paprosky et al. described their results of revision to cementless femoral components and report 95% survivorship with a minimum of 10 years follow
up.
Haydon et al showed that despite historical literature discouraging the use of cemented femurs for revision, in their experience cemented femoral revision had 91% survivorship when the cause was aseptic loosening. They found early generation cementing techniques, poor cement mantle, poor bone quality, age of less than 60, and male gender to be risk factors for failure in cemented revisions.
OrthoCash 2020
Figure A is a diagram showing the medial side of the knee. During a total knee arthroplasty, proximal tibia resection results in the transection of the ligament in Figure A along the red line. Intraoperative examination reveals coronal plane instability. What are the best next steps?

Use of the implant shown in Figure B, and use of a hinged knee brace postoperatively
Suture repair of the torn ligament, use of the implant shown in Figure C
Use of the implant shown in Figure D, and use of a knee immobilizer postoperatively
Suture repair of the torn ligament, use of the implant shown in Figure D, and use of a hinged knee brace postoperatively
Use of the implant shown in Figure C alone Corrent answer: 4
This patient has intraoperative midsubstance transection of the MCL. MCL repair, use of either a CR or PS implant, and postoperative knee bracing for 6 weeks is recommended. A possible alternative is the use of an unlinked constrained implant.
The MCL is likely to be compromised by medially placed retractors or during medial subperiosteal elevation (tibial avulsion) or injured by oscillating saw-blade during the tibial or posterior femoral condyle cut. There is no consensus for the treatment of intraoperative rupture. Acceptable salvage options include
(1) direct repair (heavy sutures for midsubstance rupture, and suture anchors for tibial sleeve avusions) and postop knee bracing for 6 weeks with either CR or PS implants, or (2) use of unlinked constrained implants with or without repair.
Lee and Lotke reviewed 37 patients with intraoperative MCL injury out of 1478 patients. They attempted repair in 14 patients, and increased constraint in 30
patients. They found higher failure rates (regardless of MCL repair technique) for cruciate retaining components. They recommend use of an unlinked constrained prosthesis (with or without ligament repair), especially for midsubstance injuries.
Leopold et al. reviewed 16 MCL injuries in 600 knees. They performed suture or suture anchor repair and used a hinged knee brace for 6 weeks postoperatively. All limbs were stable and did not require bracing beyond 6 weeks, demonstrated acceptable alignment, and did not require revision at 45 months. They recommend the use of primary MCL repair or reattachment and postoperative bracing instead of implants with increased constraint.
Figure A shows MCL transection in its midsubstance. Figure B shows a cruciate retaining implant. Figure C shows a hinged knee prosthesis (linked constrained implant). Figure D shows a posterior stabilized implant. Illustration A shows an unlinked constrained implant.
Incorrect Answers:

OrthoCash 2020
A 65-year-old woman complains of intermittent knee pain 12 years after a total knee arthroplasty. She has no history of fever or recent infections. Radiographs are shown in Figures A and B. Examination reveals minimal warmth and a moderate knee effusion. Range of motion is 5 to 100 degrees bilaterally. The C-reactive protein level is 15 mg/L (normal, 0.0-0.8mg/L), and erythrocyte sedimentation rate is 45mm/h (normal, 0-10mm/h). Arthrocentesis reveals 7500 white blood cells and 90% neutrophils. Gram stain is negative. Cultures are negative at 3 days. What is the next best step?

MRI with metal subtraction protocol
Arthroscopic debridement
Open debridement and polyethylene liner exchange
Single-stage revision total knee arthroplasty (TKA)
Explantation of components with two-stage revision TKA Corrent answer: 5
By the updated 2018 Musculoskeletal Infection Society (MSIS) criteria, this presentation is consistent with a diagnosis of periprosthetic joint infection (PJI). The patient has an elevated CRP (2), ESR (1), synovial WBC >3,000 (3), and >80% PMNs (2), for a total of 8 points. Given the chronicity of the infection, the patietn would be a candidate for two-stage revision.
This patient has clinical signs of PJI such as elevated laboratory values and radiographs suggestive of implant loosening. Even in the absence of positive cultures, the next most supported step in management if two-stage revision with explantation of the prosthesis and insertion of an antibiotic spacer.
Intraoperative cultures should be taken to guide post-operative antibiotic treatment.
Parvizi et al. recently released the updated 2018 MSI crtieria for diagnosis of PJI. The updated criteria (Illustration A) included new diagnostic tests and studies from the seven-year period since the previous criteria were established. Alpha defensin was a new addition. The two major criteria remained, each individually diagnostic of PJI. However the minor crtieria were broken down into pre-operative and intra-operative. The authors showed that a total of 6 points or more had a 97.7% SN and 99.5% SP for PJI.
Huang et al. retrospectively reported the infection control rates in 2-stage exchanges in 55 patients, and compared culture-negative cases with 295 culture-positive cases. They found that infection control in culture-negative cases was 73% at 1-year. Infection control rates were similar in culture-negative and culture-positive cases, and that infection-free survival is highest after 2-stage exchange with postoperative vancomycin. They recommend 2-stage exchange with postoperative vancomycin.
Buller et al. retrospectively assessed traits that would predict the success of debridement and liner exchange for 62 hips and 247 knees. They found that 149 (48.2%) cases failed to eradicate infection. Risks for recurrent infection include longer symptom, higher ESR, previous PJI or infection in the same joint, and an infection by a group 1 (MRSA, VRE, and methicillin-resistant S. epidermidis) or group 2 (MSSA or methicillin-sensitive coagulase-negative Staphylococcus) organism.
Della Valle et al. discuss the AAOS recommendations on diagnosis of periprosthetic hip and knee infections. They recommend repeat hip and knee aspirations when there is discrepancy between probability of PJI and initial aspiration culture result.
Aggarwal et al. prospectively compared the yield of intraoperative tissue and swab cultures in 74 hip, 43 knee, 30 septic and 87 aseptic cases. They found that tissue cultures had higher sensitivity, specificity, positive and negative predictive values for identifying PJI. Swab cultures had higher false positive and negative values. They recommend not using swab cultures, and only using tissue cultures.
Figures A and B are AP and lateral radiographs showing areas of bony erosion suggestive of loosening of the femoral and tibial components.
Illustration A is the 2018 MSIS criteria with point values.
Incorrect Answers:
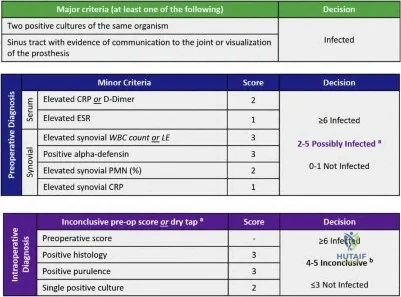
OrthoCash 2020
What are the affects on limb-length and offset according to the total hip arthroplasty template shown in Figure A?

Limb-length will stay the same, offset will be increased
Limb-length will be decreased, offset will be increased
Limb-length will stay the same, offset will be decreased
Limb-length will be increased, offset will be increased
No change in either limb-length or offset Corrent answer: 1
In Figure A, the center of rotation of the femoral component lies medial to the center of rotation of the acetabular component. If these components are implanted as shown, the offset will be increased and the leg-lengths will remain equal.
Offset and leg-length changes during templating and insertion of a total hip replacement are determined by the changes in the center of rotation (COR) of the femur relative to the acetabulum. If changes are made in the horizontal plane (x-axis), a change in offset will occur. If changes are made in the vertical plane (y-axis), changes in leg-lengths will occur. If the femoral COR is templated superior to the acetabular COR, the leg will be lengthened. In
contrast, if the femoral COR is templated inferior to the acetabular COR, the leg will be shortened. For offset, the same principles apply. If the femoral COR is templated medial to the acetabular COR, offset will be increased. In contrast, if the femoral COR is templated lateral to the acetabular COR, offset will be decreased. One should aim to restore native offset and leg-lengths in uncomplicated primary total hip arthroplasty.
Merle et al. retrospectively reviewed 152 patients to evaluate femoral offset on an AP pelvis and AP hip radiograph compared to a CT scan of the affected hip. They found that AP pelvis radiograph underestimated femoral offset by 13% when compared to a CT scan. In contrast, the AP hip radiograph showed no difference when compared to the CT scan. They recommend obtaining AP of the hip prior to templating for accurate assessment of femoral offset.
Della Valle et al. review preoperative planning for total hip arthroplasty. While they state that templating has a high predictive value in achieving the desired plan, the surgeon should always be prepared to make intraoperative adjustments based on tactile feedback.
Illustration A shows an example where leg-length will be shortened (femoral COR is inferior to acetabular COR) and offset will stay the same (femoral COR and acetabular COR are in the same horizontal plane). Illustration B is a table which summarizes the points we have discussed.
Incorrect Answers:

OrthoCash 2020
A 65-year-old patient is diagnosed with a periprosthetic joint infection 6 years after total knee arthroplasty. He recalls a history of knee realignment surgery many years prior. Examination reveals lateral patellar tracking and passive flexion to 65 degrees. A recent radiograph is shown in Figure A. During the exposure for explantation, a standard medial parapatellar approach is performed through the previous incision. It is found that adequate knee flexion to allow exposure of the prosthesis cannot be achieved even after release of the lateral gutters and excision of the scar. Which surgical exposure technique (depicted in Figures B through F) would provide the best
surgical exposure for the procedure and preserve the blood supply to the patella?

Fig B
Fig C
Fig D
Fig E
Fig F
A tibial tubercle osteotomy (TTO) would provide the best surgical exposure without compromising patellar blood supply. This patient has patella baja arising from previous high tibial osteotomy, with a scarred, contracted patellar tendon leading to knee stiffness.
A TTO is able to provide good exposure while protecting the extensor mechanism and preventing inadvertent avulsion of a contracted patellar tendon. Further, proximal transfer of the osteotomized tibial tubercle may be used to correct patella baja, bearing in mind that excessive superior translation alters the mechanics of the knee by making the quadriceps less efficient.
Mendes et al. used TTO for surgical exposure in 67 knees undergoing revision TKA. There were good-excellent knee scores at 30 months in 87%. There were no patellofemoral complications, no component malalignments, and no avulsions of the patellar tendon occurred. They advocate TTO for cases where the patellar cannot be retracted laterally with knee in 90deg of flexion.
Whiteside described a series of TTO in 136 TKA. At 2 years, mean range of motion was 94deg. There were 2 tibial tubercle avulsion fractures and 3 tibial fractures (2 in a patient with Charcot arthropathy, and 1 following manipulation after open adhesiolysis. He advises using stemmed tibial components in patients with insensate knees and in cases where manipulation is expected.
Figure A is a lateral radiograph showing severe patella baja. Figure D shows a TTO. See below for Figures B, C, E and F. Illustration A shows the surgical technique for TTO. The distal saw cut angles out of the anterior cortex at a gentle angle to reduce the stress riser effect and risk of postoperative tibial stress fracture.
Incorrect Answers:
sufficient in the presence of severe patellar baja and patellar tendon contracture.
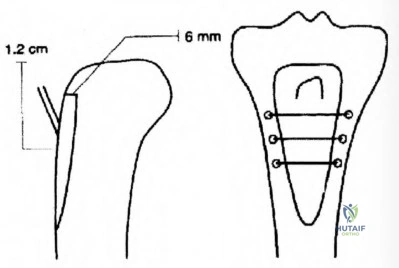
OrthoCash 2020
Figure A show pre- and post-operative radiographs, from left to right respectively, of a 79-year-old male that underwent revision total hip arthroplasty 2 years ago. He presents today for consultation after 4 episodes of right hip dislocation within the past 6 months. Physical examination reveals a trendelenburg gait with no clinical or radiographic limb length discrepancy. An Infection work-up is negative. Results from a CT scan are shown in Figure B. What would be the best treatment option?
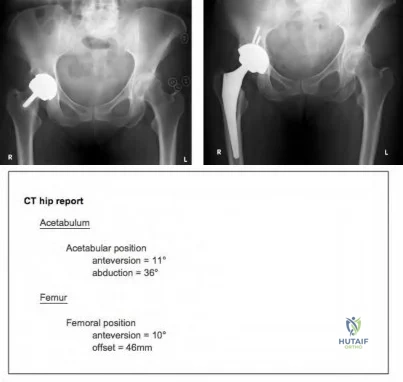
Physiotherapy and application of abductor brace
Revision arthroplasty to medialize the cementless cup and surgical repair of the abductor tendon
Revision arthroplasty to a constrained polyethylene liner
Revision arthroplasty to a femoral component with extended offset
Revision arthroplasty to a large ceramic femoral head and offset polyethylene cup
On the left, Figure A shows a metal-on-metal (MOM) bearing hip resurfacing. On the right, Figure A shows a large head, uncemented metal-on-polyethylene (MOP) total hip replacement. In this setting, the most appropriate treatment option would be revision arthroplasty with constrained polyethylene liner.
Constrained liners should be reserved for patients demonstrating recurrent instability despite treatment with a large femoral head. Other indications include elderly patients who do not require implant longevity or have a low functional demand, as well as patients with deficient or non-repairable abductor mechanisms.
Sikes et al. report on the results of a series of 41 patients (52 hips) with recurrent dislocations. They recommend that large femoral heads (LFH) be used as a first-line treatment in high-risk patients (patients of any age with dementia, neuromuscular disability, and inability to comply with precautions). Constrained liners should be reserved for patients demonstrating recurrent
instability despite treatment with an LFH.
Kilampali et al. reviewed late instability of bilateral metal on metal hip resurfacings. They suggest that late instability of hip resurfacing should raise concerns relating to possible local tissue reaction and muscle damage.
Concerning features include steeply-inclined acetabular components a large abduction angle of more than 55 degrees along with a combination of small size component.
Figure A shows an image of a revised socket which was performed to convert the MOM THA to a MOP THA. Figure B shows normal parameters of THA components. The recommendation for acetabular position is anteversion 20° ± 10° and abduction 45° ± 10°. For the femur, recommendations are 10°- 15° of anteversion and 41mm - 45mm of offset.
Incorrect Answers:
OrthoCash 2020
Which of the following has been shown to increase the rate of failure of cemented femoral components in total hip arthroplasty?
Stems that are precoated with polymethylmethacrylate
Calcar contact of the collar
Smoother implant corners
Cement mantle of 2 millimeters
Stem material with a Young's modulus higher than 115 GPa Corrent answer: 1
Precoating a stem with PMMA adds an additional inferface at risk of failure.
Stiffer stem materials (higher Young's modulus) improve performance. Titanium has a Young's modulus of 115 GPa with alloy and stainless steel
having a higher Young's modulus than titanium. Calcar collar contact adds minimal strength to the construct, but does not lead to premature failure. Smoother corners decrease the rate of failure since they decrease stress risers. The ideal cement mantle is ~2mm. Obtaining less than this would decrease the strength of the construct.
OrthoCash 2020
An 80-year-old male sustains a fall down the stairs and presents with knee swelling. He is a community ambulator who does not use walking aids. Injury radiographs are shown in Figures A and B. What is the next best step?

Intramedullary nailing
Locked plating
Long leg casting
External fixation
Revision total knee arthroplasty Corrent answer: 5
This patient sustained a periprosthetic femoral fracture around the femoral component which is now loose. Revision of the femoral component is necessary.
Various classifications exist for periprosthetic fractures around TKA. In general, for the femoral component, treatment depends on fracture displacement, fracture location, bone stock, and whether the component is loose. For loose femoral components, revision TKA using distal femoral replacement prosthesis is an option.
Kim et al. proposed a new classification for periprosthetic fractures. Type IA fractures (good bone stock, well fixed, nondisplaced or easily reducible) are managed conservatively. Type IB fractures (good bone stock, well fixed, irreducible closed) are managed with reduction and fixation. Type II fractures (good bone stock, reducible, loose or malpositioned components) are managed with revision. Type III fractures (poor bone stock, loose or malpositioned components) are treated with distal femoral replacement.
Johnston et al. reviewed the options for treating periprosthetic fractures about the knee. They advocate revision of the femoral component when the prosthesis is loose, where there is poor bone stock, or insufficient bone to gain purchase for locked plates or distal locking screws of intramedullary nails.
Nauth et al. review the current concepts in treatment of periprosthetic fractures. They prefer minimally invasive locked plating unless the fracture is significantly proximal to the anterior flange and amenable to retrograde intramedullary nailing. Then they choose nails with options for distal interlocking screws and locking condylar bolts. In extreme osteopenia, they use intramedullary fibular strut allografts (with locked plating). For loose prostheses or poor bone stock, they perform alloprosthetic composite in younger patients and a distal femoral replacement in elderly patients.
Figures A and B are AP and lateral radiographs showing periprosthetic femoral fracture around a loose femoral component. Illustrations A and B are postoperative radiographs showing revision to a hinged prosthesis with long-stemmed components. Illustration C shows Kim' proposed classification of
periprosthetic fractures around the femoral component of a TKA.
Incorrect Answers:

OrthoCash 2020
Utility of the implant seen in Figure A would be best considered in which of the following revision total hip arthroplasty scenarios?
Minimal acetabular deformity, intact rim
Superior acetabular bone lysis with intact superior rim
Localized acetabular destruction of medial wall
Absent superior acetabular rim, superolateral migration
Significant acetabular bone loss, pelvic discontinuity Corrent answer: 5
Paprosky Type 3B acetabular bone defects describes significant acetabular bone loss, with pelvic discontinuity. Type 3 defects often require reconstruction cages (as seen in Figure A) or acetabular distraction techniques
to treat severe bone loss with an associated pelvic discontinuity.
Deficient acetabular bone stock poses a technical challenge in hip arthroplasty surgery. Paprosky classification for acetabular bone loss to helps guide treatment for revision total hip arthroplasty. The classification is as follows:
Type 1: Minimal deformity, intact rim
Type 2A: Superior bone lysis with intact superior rim Type 2B: Absent superior rim, superolateral migration Type 2C: Localized destruction of medial wall
Type 3A: Significant bone loss, superolateral cup migration Type 3B: Significant bone loss, pelvic discontinuity
Sheth et al. reviewed acetabular bone loss in revision total hip arthroplasty. They state that Paprosky Type 1 and 2 defects can usually be managed with porous-coated hemisphere cup secured with screws. Type 3 defects require reconstruction cages to protect with cups and structural augments or custom triflange implants.
Taunton et al. investigated clinical outcomes and cost-effectiveness of using a custom triflange acetabular component to treat pelvic discontinuity in revision THA. They found satisfactory clinical outcomes (81% had a stable triflange component with healed pelvic discontinuity) and cost equivalence with Trabecular Metal cup-cage constructs.
Figure A shows a lateral image of the pelvis with a reconstruction cage and cup construct. Illustration A shows an illustration of the Paprosky classification. Illustration B shows a table of the Saleh/Gross classification. Illustration C shows a table of the AAOS classification.
Incorrect Answers:
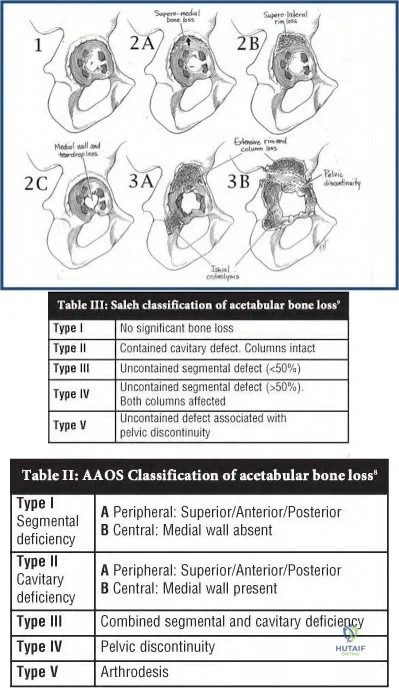
OrthoCash 2020
A 65-year-old male who had a total knee arthroplasty 8 years ago comes into the office with worsening knee pain. The orthopaedic surgeon is concerned about infection and aspirates the knee. Which of the following are the lowest laboratory values from a synovial aspirate suggestive of infection?
WBC of 500 cells/ml and PMN 25%
WBC of 1,000 cells/ml and PMN 25%
WBC of 1,500 cells/ml and PMN 70%
WBC of 5,000 cells/ml and PMN 70%
WBC of 25,000 cells/ml and PMN 70%
WBC of 1,500 cells/ml and PMN 70% indicates the lowest synovial aspirate suggestive of infection.
Mason et al in 2003 reviewed 440 revision TKA's of which 86 had preoperative aspirations. The aspirations yield 55 aseptic failures and 31 septic failures. The mean WBC of the aseptic group was 645 cells/mm(3) compared to 25,951 cells/mm(3) for the septic group (P=<.001). The mean percentage of polymorphonuclear cells (PMNs) was statistically higher in the septic group compared with the aseptic group (72.8% vs 27.3%; P=<.001). With these results, the authors concluded that aspirates with a WBC count greater than 2,500 and 60% PMNs are highly suggestive of infection.
However, in a more recent and larger study, Ghanem et al reviewed 161 infected TKA's vs 268 aseptic failures and concluded that aspiration with WBC of >1100 cells/mm3 and PMN > 64% are suggestive of infection. When both tests yielded results below their cutoff values, the negative predictive value was 98.2% (95% confidence interval, 95.5% to 99.5%), whereas when both tests yielded results greater, infection was confirmed in 98.6% (95% confidence interval, 94.9% to 99.8%) of the cases. Thus, according to the most recent literature, WBC >1100 and PMN > 64% should be considered suggestive of infection in a TKA.
OrthoCash 2020
A 50-year-old man with a past medical history significant for diabetes and end-stage renal disease presents with a chief complaint of instability 6-months following a total knee arthroplasty. Preoperative radiographs are shown in Figures A-C. Physical exam at that time was notable for a large effusion, maltracking patella, extensor lag of 15 degrees, medial instability, and gross laxity to anterior and posterior forces. The procedure was uncomplicated, and was completed using a posterior-stabilized prosthesis with tibial augements and uncemented intramedullary rods in both the femur and tibia. Which of the following surgical techniques should have been implemented to avoid this complication?

Cementing the intramedullary rods in the tibia and femur
Explant with placement of an antibiotic spacer
Taking 5mm of extra bone from the distal femur to elevate the joint line
Use of a hinged total knee arthroplasty
Taking 5mm of extra bone from the tibia to distalize the joint line Corrent answer: 4
The patient has a neuropathic joint with ligamentous instability and a maltracking patella. The appropriate procedure would have included use of a hinged total knee arthroplasty.
Choosing the appropriate constraint during a total knee arthroplasty ensures the best possible outcome. Hinged total knee arthroplasty prostheses are indicated in the setting of global instability, massive bone loss in a neuropathic joint, oncologic procedures, and hyperextension instability. In a hinged prosthesis, the tibial and femoral components are linked with an axle that restricts varus/valgus and translational stresses. While hinged prostheses are useful in the setting of major revision surgery, they are at increased risk for aseptic loosening due to the high degree of constraint inherent to the device.
Petrou et al. review the results of 100 primary cemented rotating-hinge total knee arthroplasty at 7- to 15-years. At 15 years, survival was 96.1%.
Complications included DVT (n=3), skin necrosis (n=2), subcutaneous hematoma (n=5), intra-operative fracture of either the femur or tibia (n=4), and early infection (n=2).
Figures A-C show a neuropathic joint with considerable lateral bone loss and a frankly dislocated patella. Illustration A shows an example of a hinged total knee arthroplasty. Note how the tibial and femoral components are linked using an axle.
Incorrect Answers:

OrthoCash 2020
A 63-year-old man returns for follow-up 4 years after metal-on-metal left total hip arthroplasty complaining of mild chronic hip pain with ambulation. He is afebrile and ESR and CRP are within normal limits. Radiograph of the left hip is shown in Figure A. What is the best next step?

Anti-inflammatory medication
Serum cobalt and chromium levels
MRI with metal subtraction
Physical therapy
Revision hip arthroplasty Corrent answer: 2
Metal-on-metal total hip arthroplasties (THA) have been associated with complications presumably due to metal debris and toxicity. Serum cobalt and chromium levels are recommended as part of follow-up evaluation for patients with metal-on-metal hips, even when asymptomatic.
Many patients with metal-on-metal hips have been found to have elevated serum cobalt and chromium levels, for which MR with metal subtraction is recommended to look for pseudotumors and other pathologies. These solid or cystic masses are thought to be related to metal debris and macrophage infiltration and may be associated with pain in some patients.
Lombardi et al summarize and present on behalf of The Hip Society an algorithmic approach to evaluating and treating patients with metal-on-metal THA in follow-up. They state the goals of care as determining the etiology of any pain, managing any intrinsic problems with the arthroplasty, and reassuring/observing when appropriate. They organize the types of patients seen in followup and components of the evaluation.
Chang et al evaluate the correlation between symptoms and MRI findings and report that symptomatic patients tend to have bone marrow edema and tendon tearing on MRI. They report a 69% prevalence of pseudotumors on MRI after metal-on-metal hip arthroplasty, but did not find a correlation between pseudotumor presence and pain.
Hayter et al focus on MRI findings in symptomatic (painful) patients with metal-on-metal THA in a review including 31 hip resurfacing and 29 THA. In the THA group, they report 86% rate of synovitis, 10% extracapsular disease, and 24% osteolysis, with no statistically significant difference in rates between resurfacing and THA.
Figure A is an AP view radiograph of a left hip after metal-on-metal total hip arthroplasty with components well positioned and no osteolysis.
Illustrations A and B from Lombardi et al depict a recommended algorithm for the workup and management of symptomatic and asymptomatic patients, respectively, with metal-on-metal THA.
Incorrect Answers:
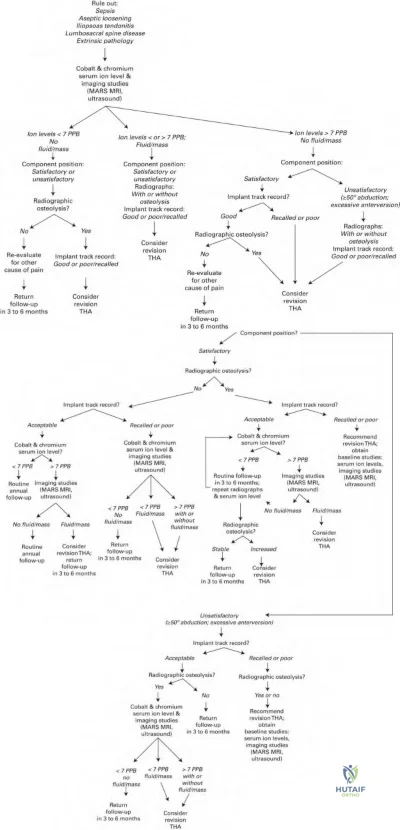
OrthoCash 2020
A 72-year-old woman sustains a fall onto her knee three years after an uncomplicated total knee replacement. The fracture pattern is seen in Figure A. The operative note reveals that a cemented patellar component was used. On exam, she has a large effusion and an
inability to straight leg raise. If the patellar component is well fixed, what is the best treatment option?

Patellectomy
Extensor mechanism allograft
Revision of the patellar component with cement and bone grafting of any residual defect
Open reduction and internal fixation of the patella fracture
Non-operative treatment in a knee brace locked in extension for 6 weeks Corrent answer: 4
Displaced, periprosthetic patella fractures with a deficient extensor mechanism and adequate bone stock are best treated with open reduction and suture or implant fixation.
Periprosthetic patella fractures are a rare, but potentially devastating complication associated with total knee arthroplasty. When evaluating patella fractures, it is important to consider 1) is the extensor mechanism intact, 2) is the patellar component well fixed or loose, and 3) is there sufficient bone stock remaining. Stable implants with an intact extensor mechanism should almost exclusively be treated non-operatively in a brace. In contrast, a deficient
extensor mechanism is an absolute indication for surgical management.
Adigweme et al. review the epidemiology, diagnosis, and treatment of periprosthetic patella fractures. When analyzing patella fractures, they suggest treatment should be based on fracture severity, remaining bone stock, patellar component stability, as well as extensor mechanism function.
Sarmah et al. review periprosthetic fracture around total knee arthroplasty. They provide an algorithm for treatment of periprosthetic patella fractures based on displacement, viability of remaining bone stock, and fracture type.
Figure A is a preoperative lateral radiograph showing a periprosthetic patellar fracture. The distal fragment is comminuted and separated from the proximal fragment by approximately 15 mm. The patellar component appears to be well fixed. Illustration A is intraoperative photograph showing the threads of the suture anchors in the proximal fragment passing through the tunnels in the distal fragment and exiting at the inferior pole of the patella. Illustration B demonstrates anatomical reduction after the knots were tied at the inferior pole of the patella. Illustration C is a lateral x-ray 1 year postoperatively showing fracture union.
Incorrect Answers:
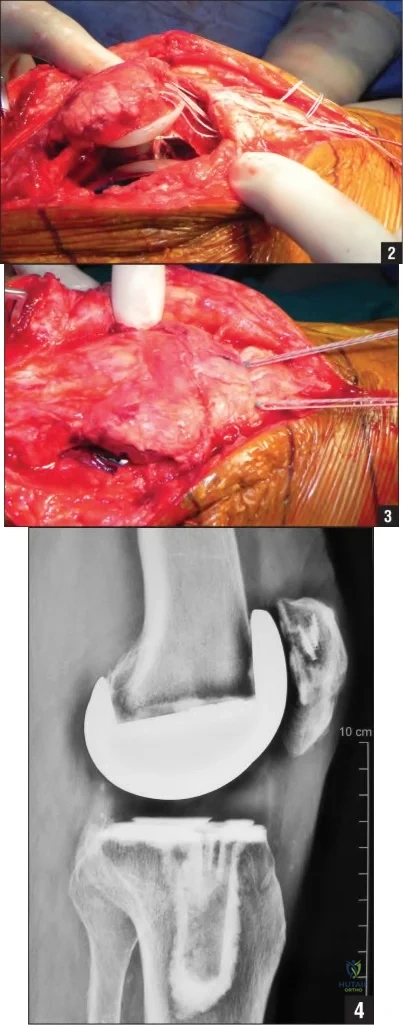
OrthoCash 2020
Knee pain and osteoarthritis are associated with "metabolic syndrome." All of the following are included in the collection of risk factors known as "metabolic syndrome" EXCEPT:
Peripheral vascular disease
Dyslipidemia
Hypertension
Impaired glucose tolerance
Central obesity
Peripheral vascular disease (PVD) may develop in patients with metabolic syndrome. However, no direct relationship between metabolic syndrome and PVD is known, and it is not a part of metabolic syndrome itself. Metabolic syndrome has been shown to be associated with knee pain and development of knee osteoarthritis (OA).
Metabolic syndrome is a collection of medical comorbidities that are known to
be risk factors for developing cardiovascular disease. Metabolic syndrome includes central (abdominal) obesity, dyslipidemia (high triglycerides and low-density lipoproteins), high blood pressure, and elevated fasting glucose levels. There is an increased prevalence of knee pain (and OA) among patients with metabolic syndrome. It is felt that the most important contributing factor to knee pain and OA in metabolic syndrome is obesity. Patients presenting with knee pain or OA and the risk factors included in metabolic syndrome should be counseled on the need to control those risk factors.
Inoue et al. present a study comparing metabolic syndrome and knee OA in a Japanese population. They found that knee OA and metabolic syndrome were highly correlated in females, but not in males.
Engström et al. present a study comparing metabolic syndrome with hip and knee OA. They found no relationship to hip OA, but did find a strong correlation between patients with metabolic syndrome and risk of developing knee arthritis. Patient BMI was the most predictive factor. They also compared prevalence of knee OA to CRP levels, but found no significant relationship.
Incorrect answers:
OrthoCash 2020
A 75-year-old male presents with recurrent dislocations of this left hip. He underwent bilateral total hip arthroplasties 12 and 8 years ago. There were no early post-operative complications with either hip. Despite a total of 5 dislocations in 6 months, he does not have pain or weakness across the left hip. On examination, there is a healthy appearing left lateral scar, equal limb lengths, normal gait and full abductor strength. Radiographs of the pelvis are shown in Figure A. His laboratory results show an erythrocyte sedimentation rate of 8 mm/h (reference range, 0-20 mm/h), and C-reactive protein of 3 mg/L (reference range, 0-5.0 mg/L). A hip aspirate culture is negative. What is the next best management option for this patient?

Magnetic resonance imaging of left hip to exclude an abductor muscle tear
Re-aspiration of left hip to exclude a subclinical infection
Continued observation for trochanteric bursitis
Supervised physiotherapy and gait training for abductor strengthening
Left revision total hip arthroplasty for polyethylene wear Corrent answer: 5
This patient presents with recurrent late hip instability with radiographic evidence of eccentric polyethylene wear. The best treatment option for this patient would be revision total hip arthroplasty (THA).
The etiology of late instability includes polyethylene wear, component malpositioning or loosening, trauma, infection or deterioration in neurological status of the patient. Identifying the cause of late instability will require a thorough work up. A good history, examination and scrutiny of radiographs can identify most causes. Advanced imaging may be requires when bone or soft-tissue pathology is suspected or radiographic evidence of osteolysis or malpositioning needs further assessment. Blood work to assess for an acute inflammatory response (ESR and CRP) should be ordered routinely as elevated markers may indicate an underlying infection.
Parvizi et al. evaluated the outcome of revision arthroplasty for polyethylene wear presenting as late dislocation. They found that revision surgery restored stability to eighteen of the twenty-two patients. Surgical treatment options may include liner-only exchange (contained or unconstrained) +/- soft-tissue repair, or revision of one or all components.
Berry et al. evaluated the long-term risk of dislocation in 6,623 consecutive primary total hip arthroplasties with a Charnley prosthesis. They found a 7% incidence of late dislocation at 25 years compared to 1% after 5 years.
Patients at highest risk were females, patients with osteonecrosis of the femoral head or an acute fracture, and nonunion of the proximal part of the femur.
Figure A shows an AP pelvis with bilateral, uncemented, total hip arthroplasties. There is eccentric wear of the left acetabular component. No fracture or loosening of the components can be identified. The components appear well-positioned.
Incorrect Answers:
This patient has no pain or weakness in the affected hip. Therefore, soft tissues can be evaluated intra-operatively during the revision THA procedure. Answer 2: A hip aspirate would not be warranted. There are no risk factors for infection in this patient (for example, no pain, no early wound complications or antibiotics, etc). Additionally, his inflammatory markers are normal.
OrthoCash 2020
A 58-year-old woman undergoes a total knee arthroplasty with a posterior stabilized design. Two years later, she returns with recurrent sterile joint effusions, a sensation of instability without giving way and difficulty with ascending and descending stairs. Examination reveals diffuse tenderness around the pes anserinus and peripatellar region, and increased anterior tibial translation most notable at 90° of flexion. Radiographs demonstrate well cemented implants with 5° of posterior tibial slope. Figure A represents a femoral cutting block with lines 1 through 5 corresponding to femoral bone cuts. The most likely cause of her symptoms is over-resection at:

Resection line 1
Resection line 2
Resection line 3
Resection line 4
Resection line 5
Over-resection of the posterior femoral condyles (resection line 2) in posterior-stabilized (PS) TKA leads to flexion instability without frank dislocation.
There are 7 bone cuts in a total knee replacement. The posterior condylar cut determines the flexion gap. Flexion instability in PS knees arises because of an enlarged flexion gap (excessive posterior condylar resection, or increased tibial slope), allowing anterior tibial translation, which is pathognomonic. There will not be posterior subluxation because of the cam-post design. Symptoms include sensation of instability without giving way, especially with stair climbing, recurrent knee effusions, and diffuse knee pain. Signs include anterior tibial translation at 90° flexion, tenderness at multiple sites (including pes anserinus, peripatellar, posterior hamstrings), and effusion. Revision surgery is indicated for symptomatic patients.
Clarke et al. reviewed flexion instability after primary TKA. They caution that most cases arise from failure to create symmetric balanced flexion and extension spaces. Treatment is usually revision TKA using the same principles. If this is not possible, increased constraint is required (constrained condylar prosthesis or hinged prosthesis).
Schwab et al. reviewed flexion instability without dislocation in PS knees in 10 patients. Revision surgery focused on flexion-extension gap balancing and filling the enlarged flexion gaps and successfully relieved pain, and improved stability to anterior tibial translation. Flexion space reconstruction includes using a larger femoral component or posterior augments. Isolated polyethylene exchange is not recommended.
Figure A shows a 5-in-1 cutting block with anterior femoral cut (line 1), posterior femoral cut (line 2), posterior chamfer cut (line 3), anterior chamfer cut (line 4), and distal femoral cut (line 5). Of note, most TKA systems have a 4-in-1 cutting block and the distal femoral cut is made separately. Illustration A shows restoration of the posterior condylar offset (line A) with the femoral component (line B).
Incorrect Answers
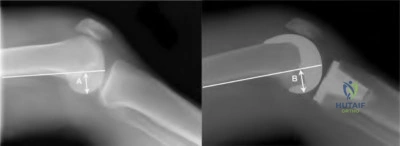
OrthoCash 2020
Which of the following is true regarding intra-operative fractures during total knee arthroplasty?
They occur more commonly in cruciate-retaining total knee replacements
Fractures of the medial femoral condyle are the most common fracture type
Fractures of the patella are the most common fracture type
Most can be treated without additional fixation at the time of surgery
Tibial fractures are more common than femoral fractures Corrent answer: 2
Fractures of the medial femoral condyle are the most common type of intraoperative fracture during a total knee arthroplasty.
Intra-operative fractures during total knee replacement are rare, but usually requiring alterations in surgical technique once they occur. The most common time for fractures to occur is during exposure and bone preparation, with fracture during trialing being the next most common. Fractures occur more commonly in posterior cruciate substituting designs, likely due the box cut.
Osteoporosis, female gender, chronic steroid use, advanced age, rheumatoid arthritis, and neurologic disorders are risk factors for post-operative fracture, but are also thought to be risk factors for intra-operative fractures.
Alden et al. reviewed 17,389 primary TKAs and found an intra-operative fracture rate of 0.39%. Of the 67 fractures, 49 were femur fractures, 18 were tibia fractures, and none were patella fractures. They recommend careful surgical technique in patients at high risk for fracture to avoid such a complication.
Sharkey et al. reviewed 10 intra-operative femoral fractures during primary, cementless total hip arthroplasty. They matched these with 20 patients who did not have this complication. At follow-up, there were no differences found between the two groups.
Incorrect Answers:
OrthoCash 2020
A 68-year-old male complains of increasing medial sided knee pain and buckling. The pain is exacerbated by sharp turns while
running. He undergoes knee arthroscopy. Recent radiographs and an arthroscopic photograph of the medial compartment are shown in Figure A. His pain has worsened since the arthroscopy. Which of the following images (Figures B through F) represents the best treatment recommendation for this patient?

This patient has isolated medial compartment osteoarthritis with Outerbridge IV medial compartment cartilage wear on arthroscopy. The best surgical option is a medial unicompartmental knee arthroplasty (UKA).
Indications for UKA include range of motion >100deg with <5deg flexion contracture, angular deformity <15deg valgus or <5deg varus that is passively correctable to neutral. Relative contra-indications include younger patients (age <60), obesity (BMI >30), and ACL deficiency in medial UKA. Asymptomatic patellofemoral chondromalacia is not a contraindication. In general, a UKA is preferred for older, less active patients with minimal varus, more severe arthritis, and no/little knee instability. A HTO is preferred for younger, active patients, with milder arthritis, more malalignment, and AP instability.
Steadman et al. retrospectively examined outcomes of TKA after arthroscopic treatment of OA in 73 patients. They found that mean survival time (conversion to TKA) after arthroscopy was 6.8 years (5.7 years in patients with Kellgren-Lawrence grade 4, and 7.5 years in those with grade 3). They conclude that in patients who want to avoid TKA, arthroscopy may help postpone TKA.
LaPrade et al. examined the results of proximal tibial opening wedge
osteotomies in 47 patients <55 years old with medial compartment osteoarthritis (OA) and genu varus. They found that there was improvement in knee scores and the mechanical axis at 3.6 years. They recommend this technique for patients with medial compartment OA and malalignment.
Figure A is a composite image showing isolated medial compartment osteoarthritis, and Outerbridge IV cartilage wear with large areas of visible subchondral bone. (See below for Figures B through F). Illustration A is a table comparing the indications of HTO vs UKA.
Incorrect Answers:
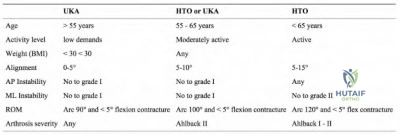
OrthoCash 2020
A 58-year-old female, with a BMI of 34 kg/m2, underwent a total knee arthroplasty for osteoarthritis 6 weeks ago. She has been participating in supervised rehabilitation since the procedure. Her preoperative, intra-operative and 6 week post-operative knee flexion are shown in Figure A. Current radiographs are shown in Figure B. What is the best step in management?

Convert to a resurfaced patella
Downsize the polyethylene liner
Arthroscopic lysis of adhesions and release of posterior capsule
Continuous passive motion at home for two weeks
Manipulation under anesthesia Corrent answer: 5
This patient has early post-operative stiffness after total knee arthroplasty (TKA). The next best step would be manipulation under anesthesia.
Management of stiffness following TKA can be challenging. The standard initial treatment option for post-operative knee stiffness is physical therapy. When this fails to achieve knee range of motion (ROM) greater than or equal to 90°, alternative treatment modalities should be considered, such as knee manipulation under anesthesia (MUA). MUA is a non-invasive treatment shown to achieve dramatic improvement in knee flexion during the early postoperative period (usually considered less than three months). Periprosthetic fracture during manipulation is rare, with an overall incidence less than 1%.
Issa et al. examined a cohort of patients that underwent MUA after TKA. At a mean follow-up of 51 months (range, 24 to 85 months), the mean gain in flexion in the MUA cohort was 33° (range, 5° to 65°). There was one periprosthetic fracture in 134 patients. The authors noted a significant improvement in ROM from pre-manipulation values.
Manrique et al. reviewed stiffness after total knee arthroplasty. MUA may be considered within the first three months after the index TKA if physical therapy fails to improve the ROM. Beyond this point, consideration should be given to surgical intervention such as lysis of adhesions, either arthroscopic or open.
Maniar et al. looked at the effectiveness of continuous passive motion immediately after TKA. A total of 84 patients were allocated to no CPM; 1 day CPM; or 3 day CPM. They found that continuous passive motion immediately after TKA did not improve short or mid-term knee ROM.
Figure B shows a cruciate sacrificing total knee arthroplasty with implants in a good position.
Incorrect Answers:
OrthoCash 2020
Which of the following fracture patterns (Figures A-E) would require revision of the femoral component to a long-stemmed, cementless prosthesis?

Figure C depicts a Vancouver B2 periprosthetic fracture, which is optimally treated with a long-stem, fully porous-coated, revision femoral prosthesis.
The Vancouver classification for total hip periprosthetic femoral fractures takes into account the three most important factors in management of these injuries: the site of the fracture, the stability of the femoral component, and the quality of the surrounding femoral bone stock. Type A fractures include those involving the lesser trochanter or the greater trochanter. Type B fractures occur around the stem or just below it. More specifically, B1 fractures have a well fixed stem, B2 fractures have a loose stem but good proximal bone stock and B3 fractures have a loose stem with proximal bone that is of poor quality or severely comminuted. Type C fractures are well below the tip of the femoral stem.
O'Shea et al. assessed the outcome of patients with Vancouver type B2 and B3 periprosthetic fractures treated with femoral revision using an uncemented extensively porous-coated implant. Union of the fracture was successfully achieved in 20 of the 22 patients. Overall, they found good early survival rates and a low incidence of nonunion using this implant.
Figure A depicts a radiograph of a Vancouver type C periprosthetic femur fracture, occurring distal to the stem of the total hip arthroplasty. Figure B demonstrates a Vancouver type A periprosthetic fracture of the greater trochanter. Figure C is an x-ray of a Vancouver type B2 periprosthetic fracture adjacent to the stem with an unstable implant, but adequate bone stock.
Figure D depicts a radiograph of a Vancouver type C periprosthetic femur fracture, occurring distal to the stem of the total hip arthroplasty. Figure E is a Vancouver type B1 periprosthetic fracture at the level of the stem that is well fixed. Illustration A shows a table summarizing the Vancouver classification of periprosthetic femur fractures and the corresponding management options.
Incorrect Answers:
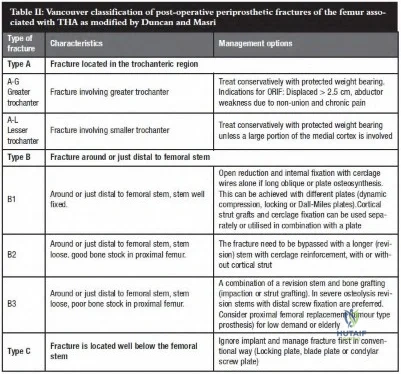
OrthoCash 2020
Which of the following maneuvers places the obturator artery at greatest risk during a total hip arthroplasty?
Placement of a posterior retractor along the posterior wall
Placement of an acetabular screw in the posterior-superior quadrant
Placement of an inferior retractor under the transverse acetabular ligament
Placement of an acetabular screw in the anterior-superior quadrant
Placement of an anterior retractor along the anterior wall Corrent answer: 3
Damage to the obturator artery most commonly occurs from placement of an inferior retractor inferior to the transverse acetabular ligament (into the obtrator foramen), and/or placement of an acetabular screw in the anterior-inferior quadrant.
Vascular injury during total hip arthroplasty is a rare but devastating complication with a reported incidence of 0.1%-0.2%. The obturator artery travels along the quadrilateral surface of the acetabulum and exits the pelvis at the superolateral corner of the obturator foramen. If the vessel is severely
damaged and bleeding cannot be controlled, ligation of the internal iliac artery has been reported.
Nachbur et al. report on 15 cases of severe arterial injury during hip reconstructive surgery over a period of 8 years. The most common injury was injury to the external iliac artery, the common femoral artery, or main branches of the lateral and medial circumflex femoral artery. These were thought to be caused by the tip of a narrow-pointed Hohmann retractor used for exposure of the hip joint.
Rue et al. review neurovascular injuries during total hip arthroplasty. Among other things, they recommend against placement of screws in the anterior-superior quadrant, prudent retractor placement, and avoiding excessive tension on the sciatic nerve.
Della Valle and Di Cesare review complications resulting from total hip replacement. They state that injury to the obturator artery can occur with acetabular screw fixation in the antero-inferior quadrant or from retractors placed underneath the transverse acetabular ligament.
Illustration A shows the obturator artery as it exits the pelvis at the superolateral corner of the obturator foramen. Illustration B reviews acetabular screw placement and the structures at risk in each quadrant.
Incorrect Answers:
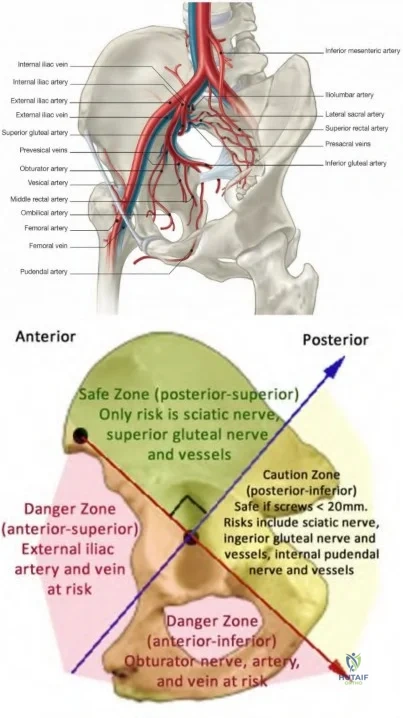
OrthoCash 2020
A 65-year-old male sustains a fall onto his left hip 3 years after a total hip arthroplasty. A radiograph taken at the emergency room is shown in Figure A. What is the next best step?

Open reduction and internal fixation with locked plates and cables through an extensile approach
Revision with a proximally porous-coated stem
Revision with an extensively porous-coated stem
Nonoperative management
Minimally invasive plate osteosynthesis Corrent answer: 3
The patient has a Vancouver B2 periprosthetic fracture. There is a loose stem that should be treated with revision to an extensively coated stem that bypasses the fracture site.
Revision of the femoral component is recommended for Vancouver B2 and B3 periprosthetic fractures. Type B1 fractures are treated with ORIF and stem retention, and proximally deficient B3 fractures may be treated with alloprosthetic composites or tumor prostheses.
Springer et al. retrospectively reviewed 118 hips with Vancouver B fractures. Seventy-seven percent of 30 extensively coated stems, 60% of 42 cemented stems, 36% of 28 proximally coated stems, and 61% of 18 tumor prosthesis/allo-prosthetic composite stems were well fixed and demonstrated
fracture union. Nonunion and loosening were the most common complications. They recommend extensively porous-coated stems for better results.
Haidukewych et al. review revision of periprosthetic fractures. They found that most acetabular components are well fixed. When the distal fragment has parallel endosteal cortices with >=5 cm of tubular diaphysis (usually with a diameter of <18 mm), they recommend an extensively coated, uncemented, monoblock long-stemmed prosthesis. If the distal diaphysis is divergent, has
<5 cm of parallel endosteal cortex, or large endosteal diameters, a fluted, grit-blasted, titanium, tapered modular stem can be used.
Figure A shows Vancouver B2 fracture. The stem has subsided relative to the proximal fracture fragment, indicating that it is loose. Illustration A shows revision of the same fracture with an extensively porous-coated stem.
Illustration B shows the endoskeleton technique using an osteotomy to split the proximal fragment coronally for stem removal, followed by insertion of a modular, fluted, tapered stem and cerclage fixation of the proximal fragments.
Incorrect Answers:
Question 96
A 9-year-old girl has had bilateral knee and leg pain for the past 2 years. The family has noted increasing deformity in both lower extremities. She is less than the fifth percentile for height. Examination reveals bilateral femoral bowing, mild medial-lateral laxity of the knees, and the deformities shown in the radiograph seen in Figure 3. What is the most likely diagnosis? Review Topic

Explanation
Question 97
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?

Explanation
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
Question 98
What is an example of cognitive rest after concussion? Review Topic
Explanation
Question 99
In 1980, a 32-year-old woman was found to have right breast mass, and a biopsy revealed adenocarcinoma. She underwent a mastectomy at that time, with no other treatment. Five years later, she noticed a lump in the left breast and underwent a left mastectomy. Seven lymph nodes were positive. In 2006, she now reports hip and thigh pain for the past 3 months. Figures 69a and 69b show AP and lateral radiographs of the femur. A bone scan shows a solitary lesion. Following radiographic staging, what is the next most appropriate step in management?
Explanation
REFERENCES: Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Simon MA, Karluk MB: Skeletal metastases of unknown origin: Diagnostic strategy for orthopedic surgeons. Clin Orthop Relat Res 1982;166:96-103.
Question 100
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. View Abstract at PubMed
Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. Enzinger & Weiss’s Soft Tissue Tumors. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. View Abstract at PubMed
Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. View Abstract at PubMed
Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.View Abstract at PubMed
