Orthopedic Board Review MCQs: Adult Reconstruction, Trauma & Sports Medicine | Part 213

Key Takeaway
This page delivers Part 213 of a comprehensive Orthopedic Surgery Board Review. It features 100 high-yield, verified MCQs, replicating OITE and AAOS exam formats. Focusing on Arthroplasty, Fracture, Hip, and Knee, it aids orthopedic residents and surgeons in mastering board certification.
About This Board Review Set
This is Part 213 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 213
This module focuses heavily on: Arthroplasty, Fracture, Hip, Knee.
Sample Questions from This Set
Sample Question 1: 0 mg/L (reference range, 0.08-3.1 mg/L) and erythrocyte sedimentation rate (ESR) is 5 mm/h (reference range, 0-20 mm/h). What is the most appropriate next step in management of the patient?...
Sample Question 2: Which factor has the most negative influence on the success of knee osteochondral allograft transplantation?...
Sample Question 3: Passage of a sodium ion through a voltage-gated channel leads to which of the following?...
Sample Question 4: An 82-year-old osteoporotic woman undergoes total hip arthroplasty for osteoarthritis. During implant trialing, a crack is heard. Intraoperative fluoroscopy reveals a long, spiral fracture of the distal femur. The fracture is reduced and fi...
Sample Question 5: A radiograph of a 12-year-old boy who has had an insidious onset of pain in the right hip for the past 6 weeks shows diffuse narrowing of the joint space. Examination reveals that he is afrebile, and the range of motion of the hip is less t...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
0 mg/L (reference range, 0.08-3.1 mg/L) and erythrocyte sedimentation rate (ESR) is 5 mm/h (reference range, 0-20 mm/h). What is the most appropriate next step in management of the patient?
Explanation
Cryotherapy has been demonstrated to achieve what effect after total knee replacement?
Decreased transfusion requirement
Improved pain, swelling, and analgesia
Improved range of motion at the time of discharge
Better long-term knee range of motion Corrent answer: 3
In a meta-analysis of randomized controlled trials on the efficacy of cryotherapy after total knee arthroplasty, patients treated with cryotherapy had less blood loss but no difference in transfusion requirements. There was better range of motion at the time of discharge from the hospital. There was no improvement in pain, swelling, or analgesia requirements. Patients treated with cryotherapy did not have better long-term range of motion.
Compared to retention of the native patella in primary total knee arthroplasty, routine patella resurfacing is associated with
no patellar complications.
an increased occurrence of anterior knee pain.
a decreased patellar fracture rate.
a decreased risk for revision surgery.
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate in patients with anterior knee pain.
What clinical outcome is associated with total hip replacements that have metal-metal bearings (compared to total hip replacements with metal-polyethylene bearings)?
Soft-tissue sarcomas
Similar revision rates at 5 years
Increased nephrotoxicity
Pseudotumors
Patients with metal-metal total hip bearings have higher levels of cobalt and chromium in the bloodstream, but systemic migration of wear debris from total hip bearings is also common to total hip arthroplasties with polyethylene bearings. There is no direct evidence that patients with metal-metal total hip arthroplasties experience a higher incidence of cancer. Chromosome abnormalities have been detected in patients with metal-metal hip bearings, and the clinical consequences of this finding remain unknown. Also, pseudotumors can form around the periprosthetic joint space in response to localized metal ion debris and the host inflammatory response, although these tumors are not specific for failed metal-metal total hip arthroplasties. Metal-on-metal hip replacements have higher revision rates compared to conventional hip replacements in multiple registry studies. Although metal-on-metal articulations have not been shown to cause renal failure, they are not recommended in patients with chronic renal insufficiency.
A 55-year-old man with unilateral osteoarthritis of the hip underwent a total hip arthroplasty using cementless fixation. The acetabular cup was 52 mm and the femoral head was 28 mm and made of cobalt-chromium alloy. The bearing surface was made of annealed highly cross-linked polyethylene, with an estimated thickness of 6.5 mm. What should the orthopaedic surgeon tell the patient regarding wear of the bearing surface?
A highly cross-linked polyethylene bearing has superior wear characteristics compared to a conventional polyethylene bearing.
A highly cross-linked polyethylene bearing has similar wear characteristics compared to a conventional polyethylene bearing.
The incidence of osteolysis is expected to be higher with highly cross-linked polyethylene than with conventional polyethylene.
The volumetric wear rate would be lower if a 36-mm femoral head were used.
In a prospective, randomized clinical trial of 100 patients undergoing cementless total hip arthroplasties, the investigators compared highly crossed-linked polyethylene to conventional polyethylene. All of the femoral heads were 28 mm. The mean follow-up was 6.8 years. The mean head penetration was 0.003 mm/year for the highly cross-linked polyethylene group in comparison to 0.051 mm/year for the conventional polyethylene group (P =
.006). The improved wear is seen with larger-diameter heads as well. The volumetric wear rate of highly cross-linked polyethylene is equivalent to slightly higher with a larger head than a 28-mm head. Incidence of periarticular osteolysis is lower with highly cross-linked polyethylene.
A 49-year-old active man has groin pain 3 years after undergoing an uneventful total hip replacement using a cobalt-chrome femoral head articulating against a cobalt-chrome acetabular insert. The pain intensifies with activity and travels down his thigh. Examination and radiographic evaluation are not particularly helpful; there is no evidence of spinal or vascular disease. What is the next step in the evaluation of this patient?
A 3-phase bone scan
Measurement of synovial metal ions levels
Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and
possible hip aspiration
Bearing exchange to a metal-polyethylene combination Corrent answer: 3
ESR, CRP, and possible hip aspiration is the most logical next step even though at some point, bearing exchange may emerge as the ultimate treatment for a metal-metal adverse reaction in this patient. But the initial workup of a patient with a painful total hip that was otherwise functioning well must include the differential diagnosis of infection, which must be excluded with an appropriate laboratory workup, clinical history, and hip aspiration. The latter study may also help to diagnose a reaction to the metal bearing; cobalt and chromium levels in the aspirate can be investigated, and the color and quantity of the aspirate can be examined along with the cell count. Serum levels of metal ions at this stage could be both helpful and difficult to interpret.
Figures A and B are the radiographs of a 25-year-old woman whose right knee pain has progressed during the last several years to pain with any activity and pain at night. What is the most appropriate treatment?
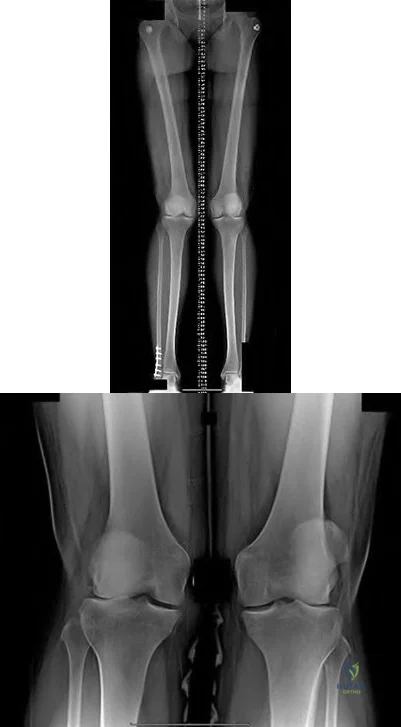
Proximal tibial osteotomy
Distal femoral osteotomy
Lateral unicompartmental arthroplasty
Total knee arthroplasty
Arthroscopic partial lateral meniscectomy Corrent answer: 2
This patient is a good candidate for a joint-preserving procedure. Her symptoms and radiographic findings reveal valgus malalignment of the knee with narrowing of the lateral joint space. The alignment can be corrected with a varus-producing distal osteotomy. Most patients do not proceed to knee arthroplasty for at least 10 years after this procedure. Osteotomy is preferred over partial or total knee arthroplasty because of the patient's young age.
Varus proximal tibial osteotomy would result in joint line obliquity.
An orthopaedic surgeon noticed a displaced calcar fracture during stem insertion when performing total hip arthroplasty using cementless fixation. What is the most appropriate course of action?
Intraoperative exploration to determine the extent of the fracture
Use of a longer stem without fixation of the calcar fracture
Complete insertion of the stem and measures to protect the patient against full weight bearing for 4 weeks
Removal of the stem, internal fixation of the fracture, and definitive reconstruction at a later stage after the fracture has healed
Calcar fractures can occur with both cemented and cementless stem fixation during surgery. The distal extent of the fracture must be identified either by direct visualization or intraoperative radiograph prior to fixation or implantation of the femoral component. The recommended treatment is to fix the calcar fracture with cerclage wires/cables to restore the mechanical stability of the femoral metaphysis. The same stem can be inserted successfully. The majority of these fractures unite without adverse stem fixation problems.
A 48-year-old woman had an 8-month history of spontaneous onset of left medial knee pain. She was otherwise healthy with an unremarkable past medical history. Prior to the onset of knee pain, she jogged, played tennis, and golfed regularly. She wished to remain active. Examination showed a fit woman with a BMI of 26, a stable left
knee with full range of motion, and some mild medial joint line tenderness. Radiograph results were normal. An MRI scan showed diffuse grade 3 and a focal area of grade 4 chondromalacia on the medial femoral condyle. The medial meniscus had a degenerative signal but no tear. The remainder of the knee showed no additional pathology. What is the most appropriate initial treatment?
Lateral heel wedge
Low-impact aerobic exercises
Glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day
Arthroscopic debridement and microfracture of the focal area of grade 4 chondromalacia to reduce risk for progression
This patient has early medial compartmental osteoarthritis of her knee. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Non-Arthroplasty), there is Level 1 evidence and an "A" recommendation for the use of low-impact aerobic exercises. The guideline also has "A" recommendations with Level 1 evidence indicating that glucosamine and chondroitin should not be prescribed and that arthroscopic debridement not be performed in the absence of symptoms of a meniscal tear or loose body. Lateral heal wedge is not appropriate; the AAOS guideline provides a "B" recommendation with Level 2 evidence indicating that a lateral heal wedge not be prescribed.
Figure 36 is the postoperative photograph of a patient who underwent a total knee arthroplasty 10 days after surgery. Knee aspiration suggests a Streptococcus infection.

Stop physical therapy and institute oral antibiotics.
Stop physical therapy and institute intravenous (IV) antibiotics.
Open irrigation and debridement, polyethylene spacer exchange, and IV antibiotics
Remove components and insert an antibiotic spacer.
An acute postoperative infection during the first 2 to 4 weeks should be treated with a return to the operating room for open irrigation and debridement of the wound. Polyethylene spacer exchange aides in washing out the entire knee joint. IV antibiotics are also indicated in this situation. To address persistent wound drainage, there is no role for oral or IV antibiotics alone. Removal of the arthroplasty components is recommended for infections after the initial 2- to 4-week postoperative period. However, several recent publications demonstrate a failure rate higher than 50% when the organism is a methicillin-resistant Staphylococcus aureus. Six weeks after surgery, this scenario is no longer considered an acute postoperative infection, and most authors recommend a 2-stage protocol with removal of components and placement of an antibiotic-impregnated cement spacer and 4 to 6 weeks of IV antibiotics.
What is the difference in outcome when comparing high tibial osteotomy (HTO) to total knee arthroplasty (TKA)?
TKA has a longer recovery period than HTO.
HTO provides more complete pain relief than TKA.
HTO is more reliable in older patients than TKA.
HTO outcomes among thin, active, young patients who undergo this procedure approach outcomes associated with TKA.
The ideal candidate for HTO is a thin, active person with a stable knee, unicompartmental knee symptoms, and age younger than 60. TKA offers a shorter recovery period and more complete pain relief than HTO. TKA is believed to be more reliable than HTO for patients older than age 60.
Figure 39 is a radiograph of a 72-year-old man who underwent an open reduction and internal fixation of a right femoral neck fracture. After 3 months he started to develop pain, and during the next 8 months he complained of progressive pain and shortening of the hip. What is the most appropriate treatment?

Girdlestone
Total hip replacement
Hardware removal
Hardware removal with revision open reductions and internal fixation Corrent answer: 2
Even though a relatively short amount of time has passed since the index surgery, this patient has developed significant osteonecrosis that has caused collapse of the bony structures and the hardware prominent. Total hip replacement gives the most efficient pain relief. Hardware removal with or without re-reduction does not provide reliable pain relief. A girdlestone does not allow the patient to function.
Figure 40 is the radiograph of a 68-year-old woman who has right knee pain that is limiting her activity and severe preoperative valgus deformity. During total knee arthroplasty, what pathologic features are typically encountered?

Lateral femoral hypoplasia
Internal rotation of the tibia relative to the femur
Medial patella tracking
Tight medial collateral ligament Corrent answer: 1
In patients with severe valgus deformity, problems frequently encountered include loose or attenuated medial collateral ligament, tight lateral retinaculum and lateral ligamentous structures (lateral collateral, posterolateral corner), atrophic lateral femoral condyle, lateral patella tracking, and external rotation of the tibia relative to the femur. The hypoplastic lateral condyle can cause internal rotation of the anteroposterior cutting block if the posterior condyler line is used for rotational alignment. The medial soft tissues are typically attenuated and stretched.
A 59-year-old active woman underwent elective total hip replacement using a posterior approach. She had minimal pain and was discharged to home 2 days after surgery. Four weeks later she dislocated her hip while shaving her legs. She underwent a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Observation and patient education regarding hip dislocation precautions
Revision to a larger-diameter femoral head
Revision to a constrained acetabular component
Application of a hip orthosis for 3 months Corrent answer: 1
First-time early dislocations are often successfully treated without revision surgery, especially when there is no component malalignment. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful, but is usually reserved for patients with recurrent dislocations.
Patellar pain, subluxation, or dislocation after total knee arthroplasty can result from which of the following component orientations?
Internal rotation of the tibial component
Lateralization of the tibial component
Lateralization of the femoral component
External rotation of the femoral component Corrent answer: 1
Internal rotation of the components of a total knee arthroplasty, both the tibial and femoral components, can lead to symptoms ranging from patellar pain to dislocation. Most researchers agree that proper external rotation of the femoral component is parallel or nearly so to the femoral epicondylar axis with the knee in the 90-degree flexed position. Proper rotational positioning of the tibial component places the midportion of the tibial component rotationally aligned within the medial one-third of the tibial tubercle. Internal rotation of the tibial component causes relative lateralization of the tibial tubercle and the extensor mechanism. Lateralization of the femoral component moves the trochlear groove laterally. Lateralization of the tibial component moves the tibial tubercle medially, which may be beneficial to patellar tracking.
How does the risk for periprosthetic infection after total knee arthroplasty compare to risk for infection after total hip arthroplasty?
Higher in primary arthroplasty
Lower in primary arthroplasty
Lower in revision arthroplasty
Equivalent in both primary and revision arthroplasty Corrent answer: 1
Risk for periprosthetic infection is higher in the knee (1%-2%) than it is in the hip (0.3%-1.3%). The risk for infection is higher after revision joint replacement surgery compared to primary joint replacement surgery.
Osteoarthritis is not associated with a higher risk for periprosthetic infection, but certain inflammatory conditions such as rheumatoid arthritis and psoriatic arthritis place patients at higher risk for postoperative infection.
What factor is associated with a higher risk for dislocation after total hip arthroplasty?
Male gender
Previous hip surgery
A direct lateral surgical approach
Metal-on-metal bearing surfaces Corrent answer: 2
Dislocation after total hip arthroplasty is a multifactorial problem. Numerous risk factors may act independently or cumulatively to increase risk for this complication. Previous hip surgery of any kind is associated with a twofold increased risk for dislocation. Other risk factors include female gender, impaired mental status, inflammatory arthritis, and older age. Numerous studies have shown a lower dislocation rate with a direct lateral approach, although surgical techniques such as capsular repair have significantly lowered the incidence of dislocation after using the posterior approach. Metal-on-metal bearings have been associated with other complications such as adverse tissue reactions but are often used with larger-diameter bearings, which pose lower risk for dislocation.
What surgical technique has been associated with increased risk for recurrent dislocation after revision total hip arthroplasty?
Posterior capsulorrhaphy
Use of a jumbo cup
Use of a lateralized liner
Use of a larger femoral head diameter Corrent answer: 2
When addressing recurrent dislocation after total hip arthroplasty, surgical considerations that must be addressed include approach, soft-tissue tension, component positioning, impingement, head size, and acetabular liner profile. These considerations most often involve tensioning or augmentation of soft tissues, as in capsulorrhaphy or trochanteric advancement; correction of malpositioned components; use of larger femoral head sizes that increase motion before impingement; improving the head-to-neck ratio; and increasing femoral offset. The use of a larger-diameter acetabular component may lead to soft-tissue overgrowth around the liner, causing impingement and increasing the risk for recurrent dislocation.
A 67-year-old active man returns for routine follow up 12 years after hip replacement. He has no hip pain. Radiographs revealed a
well-circumscribed osteolytic lesion around a single acetabular screw. All hip components were perfectly positioned. Six months later, comparison radiographs show an increase in the size of the osteolytic lesion. A CT scan shows a well-described lesion that is 3 cm at its largest diameter and is localized around 1 screw hole with an eccentric femoral head. What treatment is appropriate, assuming well-fixed cementless total hip components exist?
Revision of the polyethylene liner, removal of the screw, and debridement of the osteolytic lesion with or without bone grafting
Revision of the acetabular component to a newer design without screws
Removal of the screw, revision of the polyethylene liner, and stem cell injection into the lytic lesion
Removal of the offending screw from the metal socket and placement of a new polyethylene liner in the existing socket
With a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected with liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings during revision surgery. Here, complete cup revision is not warranted considering the appropriate implant position. Beaule and associates reviewed 83 consecutive patients (90 hips) in which a well-fixed acetabular component was retained in clinical scenarios such as the one described; no hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, or if the osteolytic lesion is not amenable to debridement through the screw hole, acetabular component revision may be indicated.
What has been identified as a risk factor for total knee arthroplasty failure after previous high tibial osteotomy?
Body mass index higher than 35
Female gender
Preoperative stiffness
Advanced age
Increased weight, male gender, young age at the time of total knee arthroplasty, laxity, and limb malalignment preoperatively have been identified
as risk factors for early failure for total knee arthroplasty following high tibial osteotomy.
You are caring for an 18-year-old boy with severe hip arthritis and pain from a missed slipped capital femoral epiphysis. You decide that a hip arthrodesis is the best treatment option. What is the optimum position for a hip arthrodesis to maximize function and prevent complications?
0° external rotation, 0° adduction, 0° hip flexion
5° external rotation, 5° adduction, 20° hip flexion
5° external rotation, 15° abduction, 5° hip flexion
15° external rotation, 0° adduction, 20° hip flexion
15° external rotation, 15° abduction, 5° hip flexion
Hip arthrodesis is a salvage procedure for patients with hip arthritis without ipsilateral knee, contralateral hip, or lumbar spine pathology. The optimal position for hip arthrodesis is 5 degrees of adduction, 5-10 degrees of external rotation, and 20-35 degrees of hip flexion.
In their review, Beaule et al. discuss the current indications and techniques regarding hip arthrodesis including appropriate leg position, surgical techniques, methods to optimize function, and later conversion to hip arthroplasty.
Callaghan et al. evaluated the long term efficacy (20-25 yrs) of hip arthrodesis. They found the onset of ipsilateral knee, contralateral hip, or lumbar spine pathology usually began 20 years after the arthrodesis. Of their patients, they found a 15% rate of conversion to hip arthroplasty by 20 years.
What limits indications for the use of constrained liners?
Association with periprosthetic fracture
Technical difficulty associated with insertion
High costs associated with their use
High failure rates associated with their use Corrent answer: 4
Because of reports of relatively high failure rates associated with constrained liners, indications are limited to continued instability after appropriate component position or deficient abductor mechanism and instability. Neither cost nor technical insertion issues are relevant with regard to indications for use. Periprosthetic fractures are not associated with constrained liner usage.
What serum inflammatory marker has the highest correlation with periprosthetic joint infection?
C-reactive protein
Serum white blood cell count
Erythrocyte sedimentation rate
Interleukin 6 (IL-6)
Although CRP and ESR can be elevated in the setting of infection, IL-6 has been shown to have the highest correlation with infection. Serum white blood cell count has been shown to be ineffective in correlating with periprosthetic joint infection.
A 68-year-old man reports hip pain 15 years after successful cementless total hip arthroplasty. Radiographs show 3 mm of linear wear of the modular acetabular liner and a retro-acetabular osteolytic lesion. Both the titanium femoral and acetabular components appear to be well fixed. The orthopaedic surgeon recommends revision of the acetabular liner and femoral head. This patient is at increased risk for
dislocation.
periprosthetic fracture.
infection.
progressive osteolysis.
Isolated acetabular liner revision is frequently performed in cases of liner wear and periprosthetic osteolysis in the absence of acetabular component loosening. Many reports have documented an increased incidence of dislocation following this type of revision surgery. This dislocation rate can be reduced by using a larger-diameter femoral head at the time of revision. If the
acetabular component is loose or malpositioned, it should be revised. If the locking mechanism is damaged, then a replacement liner may be cemented into the well-fixed shell. Numerous studies have shown that many osteolytic lesions will reduce in size or heal without bone grafting, and removal of the source of wear debris will arrest the progression of osteolysis. The risk for periprosthetic fracture and infection are lower than risk for dislocation in this setting.
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day.
weight loss through dietary management and low-impact aerobic exercises.
arthroscopic debridement and lavage.
a valgus-directing brace.
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Non-Arthroplasty), Level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day and arthroscopic debridement and lavage).
The range of knee mobility after total knee replacement is multifactorial and dependent upon implant design, surgical implantation accuracy, and patient-specific variables. What total knee implant design is associated with the most knee flexion after total knee replacement?
Highly conforming articular surface geometry
Higher-flexion femoral component design manufactured to allow the most knee flexion
Posterior cruciate-stabilized implant, with or without a higher flexion
manufacturing modification
Posterior cruciate-retaining design with a mobile bearing, custom implanted based on CT scan data
A posterior cruciate-stabilized implant has the best support in the literature in terms of the most favorable range of motion after knee arthroplasty, regardless of whether the femoral component is designed with a higher flexion variation. The higher flexion design is a manufacturing variation that is intended to increase motion by clearing the posterior condyles in flexion.
Although the knee may not gain more flexion, this design allows for more safety in deep flexion. The long-term outcomes of increased stresses on the polyethylene are not known, however. By itself, a higher-flexion design does not lead to increased knee mobility. The effects of mobile bearings, custom CT scan-based knee implantation, and highly conforming designs on ultimate knee range of motion are uncertain.
In total knee arthroplasty, in vitro testing has shown that crosslinking can diminish the rate of polyethylene wear by 30% to 80%.
What other change in material properties is possible when polyethylene is highly cross-linked?
Increased ductility
Increased wettability
Diminished fatigue strength
Decreased resistance to abrasive wear Corrent answer: 3
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been identified as causing implant failure in most recent clinical trials, but remain the most important mechanical issues associated with current material processing methods.
What factor is associated with a high risk for developing pseudotumors after metal-on-metal hip resurfacing?
Large-diameter components
Age 40 or older for men
Age 40 or younger for women
Diagnosis of primary osteoarthritis Corrent answer: 3
The recent experience of a large clinical cohort revealed the most likely risk factors as female gender, age younger than 40, small components, and the diagnosis of hip dysplasia causing osteoarthritis. Failure was least likely among men and procedures involving larger components. These data have prompted some authors to caution against use in women and to primarily target candidates who are men younger than age 50. Small components may be more prone to failure because of malpositioning and edge loading, which have been noted to be more common in dysplasia cases.
A 70-year-old man is scheduled to undergo bearing surface revision for wear and osteolysis 10 years after cementless total hip arthroplasty. The femoral head is 28 mm alumina-oxide ceramic material. The components are in good position, and there is no evidence of fixation loosening of either component by radiograph or preoperative bone scan. What outcome is associated with isolated polyethylene exchange?
Reduced risk for future wear and osteolysis with a larger femoral head
Reduced risk for future wear and osteolysis with a cobalt chrome femoral head
Similar risk for dislocation compared to primary total hip arthroplasty
Increased risk for dislocation compared to primary total hip arthroplasty Corrent answer: 4
The major complication associated with polyethylene exchange is postoperative dislocation. Maloney and associates noted a dislocation rate of 11% in a study of 35 hips after such revision. Boucher and associates reported a 25% rate of dislocation in a study of 25 patients. Larger femoral heads result in higher volumetric wear in contrast to smaller-diameter heads. Stem revision is not indicated because there is no fixation loosening. Moreover, stem biomaterial has no effect on polyethylene wear.
A healthy, active 68-year-old woman had a total hip arthroplasty 3 months ago. She has been to the emergency department with a posterior dislocation 3 times during the last 2 months. Plain radiographs and a CT scan confirm that the acetabular component is oriented in 5 degrees of retroversion and 55 degrees of abduction.
What is the most appropriate treatment?
Revision of the femoral and acetabular components
Maximizing head-neck ratio and increasing head length
Acetabular component revision
Closed reduction with an abduction brace and reinforcement of hip precautions
Acetabular malposition can lead to recurrent instability. When this cause is confirmed, reorientation of the component can lead to successful revision surgery. Revision of the femoral component may not be necessary if the acetabular component is repositioned. Increasing length and maximizing head-neck ratio cannot make up for component malposition. There is no role for nonsurgical treatment in the setting of recurrent instability with component malposition in an active, healthy patient.
A 55-year-old woman with history of HIV infection is scheduled for revision total knee arthroplasty to address instability. The index surgery was done 3 years ago. What is the white blood cell (WBC) count threshold in the synovial fluid for an infection diagnosis?
Question 2
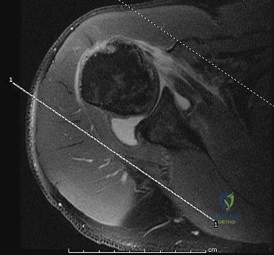
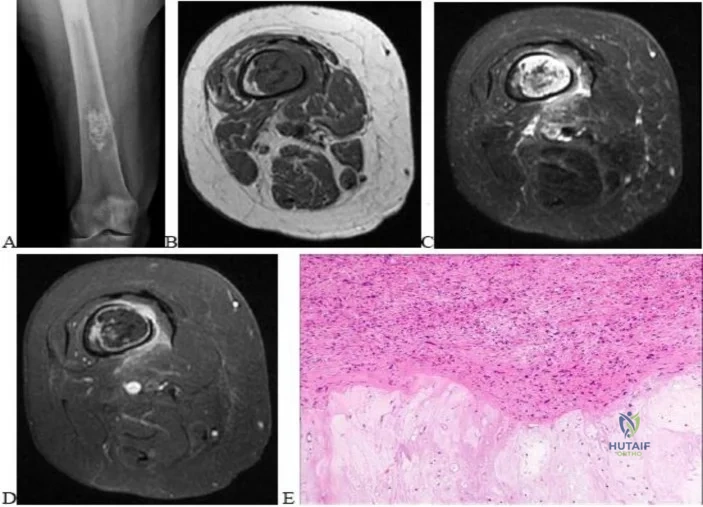
Which factor has the most negative influence on the success of knee osteochondral allograft transplantation?
Explanation
The images illustrate a large unstable osteochondral lesion of the medial femoral condyle. Radiographs and MR images clearly show deep subchondral bone involvement. The appropriate choice of surgery is OCA transplantation, which is indicated for primary treatment of large cartilage lesions, osteochondral lesions, and salvage procedure from failed prior cartilage surgery. Correction of mechanical axis malalignment, ligamentous insufficiency, and meniscal deficiency should also be addressed. ACI alone or an arthroscopic microfracture procedure would not address the bone defect, leaving an uneven articular surface. Although an osteotomy may be a viable choice, a distal femoral varus osteotomy would increase the contact pressure in the medial compartment and worsen the situation.
The histologic anatomy of articular cartilage is well described. The superficial layer or lamina splendens contains a small amount of proteoglycan with collagen fibrils arranged parallel to the articular surface. In contrast, the deep zone contains the largest-diameter
collagen fibrils, oriented perpendicular to the joint surface, and the highest concentration of proteoglycans.

Video 54 this video is uploaded at
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a and 51b are the radiographs of an 18-year-old football linebacker who was involved in a tackle and fell onto an outstretched left arm. He had immediate pain and deformity of his left elbow.
Question 3
Passage of a sodium ion through a voltage-gated channel leads to which of the following?
Explanation
Voltage-gated channel are shut when the membrane potential is near the resting potential of the cell, but they rapidly begin to open if the membrane potential increases to a precisely defined threshold value. When the channels open (in response to depolarization in transmembrane voltage), they allow an inward flow of sodium ions, which changes the electrochemical gradient, which in turn produces a further rise in the membrane potential. This then causes more channels to open, producing a greater electric current across the cell membrane, and so on.
Lee et al. present a review article on nerve conduction and needle electromyography studies. They note that the three types of nerve conduction study are motor, sensory,
and mixed, of which motor is the least sensitive. In addition, they report that peripheral nerve entrapment initially results in focal demyelination; thus, nerve conduction velocity slows across the site. However, with radiculopathy and nerve root compression, the nerve conduction study may be normal.
Catterall presents a review article covering an overview of structural models of voltage-dependent activation, sodium selectivity and conductance, drug block and both fast and slow inactivation. He notes that voltage-gated sodium channels initiate action potentials in nerve, muscle and other excitable cells.
Illustration A is a diagram that shows the electrical recordings of an action potential, along with labels of each section of the process.
Question 4
An 82-year-old osteoporotic woman undergoes total hip arthroplasty for osteoarthritis. During implant trialing, a crack is heard. Intraoperative fluoroscopy reveals a long, spiral fracture of the distal femur. The fracture is reduced and fixed with an anatomic locking plate. The rest of the total hip arthroplasty proceeds uneventfully. Following surgery the surgeon has a meeting with the family and apologizes and provides full disclosure, accepts responsibility, provides a detailed explanation as to what happened, and gives reassurance that steps will be taken to prevent recurrences. This communication approach will most likely
Explanation
In the event of a medical error or adverse event, effective communication with the patient and family is necessary. Effective communication should comprise: an apology, full disclosure (an explanation of what happened), accepting responsibility, and corrective steps that will be taken to prevent recurrence.While accepting responsibility is integral to the explanation process, it is different from accepting blame.
Mazor et al. found patients would more likely change physicians and seek legal advice in situations with a life-threatening outcome where physicians chose nondisclosure. They recommend full disclosure, acceptance of responsibility, an apology, detailed explanations, and assurances that steps will be taken to prevent recurrences will result in positive outcomes in terms of patient satisfaction, trust, and emotional response.
MacDonald et al. addressed medical errors in an editorial. Besides full disclosure, they feel that an apology is necessary. This includes an acknowledgement of the event and one’s role in the event, and a genuine expression of regret. Apology laws exist to to reduce concerns about legal implications of disclosure and apology.
Incorrect Answers:
Question 5
A radiograph of a 12-year-old boy who has had an insidious onset of pain in the right hip for the past 6 weeks shows diffuse narrowing of the joint space. Examination reveals that he is afrebile, and the range of motion of the hip is less than 50% of normal in all planes. Laboratory studies show an erythrocyte sedimentation rate of 21 mm/hr and a WBC of 11,000/mm3. What is the most likely diagnosis?
Explanation
This patient has no history of hemophilia given. Hemophilic arthropathy begins with a hemarthrosis.
In osteoid osteoma the pain is typically unrelenting, sharp, boring, worse at night, and relieved with aspirin. It is not associated with joint space narrowing.
The most common age for Legg-Calve-Perthes disease is 4-8 years. It causes AVN of the femoral head and widening of the medial joint space is an early radiographic finding.
In Bleck’s report on Idiopathic Chondrolysis JBJS 1983 nine cases were seen at the reporting institution between 1973 and 1978. The average age was 11.5 years. All the patients were otherwise healthy and had no history of systemic illness of previous trauma. All the patients reported the insidious onset of pain in the anterior part of the hip. All had a decreased passive ROM. Radiographic examination showed regional osteoporosis, premature closure of the femoral capital physis, narrowing of the joint space, and lateral overgrowth of the femoral head on the neck. All laboratory examinations were negative for evidence of infection or rheumatoid arthritis. Treatment consists of administration of aspirin, active non-loading exercise of the hip, and protected weight-bearing with crutches.
Question 6
A 15-year-old boy who participates in track reports acute pain along the left iliac crest during a sprint. Examination reveals that the anterior superior iliac spine is nontender. The most likely diagnosis is an injury to the
Explanation
REFERENCES: Clancy WG Jr, Foltz AS: Iliac apophysitis and stress fractures in adolescent runners. Am J Sports Med 1976;4:214-218.
Waters PM, Millis MB: Hip and pelvic injuries in the young athlete, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 279-293.
Lombardo SJ, Retting AC, Kerlan RK: Radiographic abnormalities of the iliac apophysis in adolescent athletes. J Bone Joint Surg Am 1983;65:444-446.
Paletta GA Jr, Andrish JT: Injuries about the hip and pelvis in the young athlete. Clin Sports Med 1995;14:591-628.
Question 7
An 11-year-old boy reports the acute onset of elbow pain and swelling after pushing his brother. The patient's mother and a younger sibling have experienced numerous fractures. You note that the patient and his mother have blue sclera and normal-appearing teeth. A radiograph of the elbow is shown in Figure 60. This patient's disorder is most likely the result of Review Topic

Explanation
Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). These individuals have blue sclerae, and although the initial fracture usually occurs in the preschool years, it may occur at any age. Furthermore, olecranon apophyseal fractures that occur after relatively minor trauma have been associated with type I OI. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. In this patient, there are no indications that the child has been subjected to abuse. Radiographs of the elbow show no evidence of osteopetrosis (due to abnormal osteoclast function) or rickets (due to a deficiency of vitamin D). Morquio syndrome (characterized by a defect of the enzyme N-Ac-Gal-6 sulfate sulfatase) is not associated with blue sclera.
Question 8
A newborn has an anterolateral bow of the tibia and a duplication of the great toe. Which of the following conditions will develop as the infant grows?
Explanation
REFERENCE: Weaver KM, Henry GW, Reinker KA: Unilateral duplication of the great toe with anterolateral tibial bowing. J Pediatr Orthop 1996;16:73-77.
Question 9
Longitudinal radioulnar dissociation, including Essex Lopresti fractures, requires disruption of the interosseous membrane (IOM). The interosseous membrane (IOM) consists of all of the following ligaments EXCEPT?

Explanation
The IOM bridges the radius and ulna and acts as a hinge for rotation of radius about ulna. The central portion is thickened, and forms the central band which is the most important ligament for IOM load distribution characteristics.
Noda et al, in a cadaver study, identified the precise anatomical insertions and attachment points of each of the 5 IOM components. They found the most distal and proximal ends of the radial origin of the central band were 53% and 64% of total radial length from the tip of the radial styloid, whereas those of the ulnar insertion were 29% and 44% of total ulnar length from the ulnar head.
Pfaeffle et al also performed a cadaveric biomechanical study applying compressive loads to specimens with IOMs that are intact, cut, or cut/reconstructed with flexor carpi radialis allografts. They found that reconstruction of the IOM can restore the normal load transfer chararcteristics and that the central band of the IOM is the most important portion of the IOM to be reconstructed.
Question 10
A 12-year-old gymnast has had elbow pain for 4 weeks. She denies any specific trauma to the elbow. Examination reveals lateral pain and no instability on testing. Range of motion is as follows: 15 degrees, loss of elbow extension, normal flexion, and normal pronation and supination. Radiographs reveal a 3- x 7-mm radiolucency of the capitellum. A T1-weighted MRI scan reveals a single solitary lesion, and T2-weighted images show no signal around the lesion. There are no intra-articular loose bodies. Appropriate management should include which of the following? Review Topic
Explanation
Question 11
- Figures 59a and 59b show the plain radiographs, and Figures 59c and 59d show the CT scan of a 77-year-old woman who has had pain in her back and both buttocks for the past 6 months. She reports that the pain radiates down her right thigh and leg when she is standing. What is the most likely diagnosis?
Explanation
Question 12
Which of the following is considered the most useful screening method for the evaluation of protective foot sensation in a patient with diabetes mellitus?
Explanation
REFERENCES: Pinzur MS, Shields N, Trepman E, Dawson P, Evans A: Current practice patterns in the treatment of Charcot foot. Foot Ankle Int 2000;21:916-920.
Smith KD, Emerzian GJ, Petrov O: A comparison of calibrated and non-calibrated 5.07 nylon monofilaments. Foot Ankle Int 2000;21:852-855.
Question 13
Figure 36 shows an AP radiograph of a 65-year-old man who reports activity-related groin pain. History reveals that he underwent total hip arthroplasty 12 years ago. What is the most likely diagnosis?
Explanation
REFERENCES: Visuri T, Pulkkinen P, Paavolainen P: Malignant tumors at the site of total hip prosthesis: Analytic review of 46 cases. J Arthroplasty 2006;21:311-323.
Bezwada HP, Shah AR, Zambito K, et al: Distal femoral allograft reconstruction for massive osteolytic bone loss in revision total knee arthroplasty. J Arthroplasty 2006;21:242-248.
Kitamura N, Naudie DD, Leung SB, et al: Diagnostic features of pelvic osteolysis on computed tomography: The importance of communication pathways. J Bone Joint Surg Am 2005;87:1542-1550.
Question 14
Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management should consist of
Explanation
REFERENCES: Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Pemberton PA: Pericapsular osteotomy of the ilium for the treatment of congenital subluxation and dislocation of the hip. J Bone Joint Surg Am 1965;47:65-86.
Question 15
A 19-year-old college football player reports persistent weakness, tingling, and numbness of both upper extremities at half time. He states that these symptoms initially occurred after tackling an opposing player with his head early in the game. History reveals that he has had “burners” in the past that typically resolved within 15 to 30 minutes. Examination reveals pain-free cervical motion, weakness to shoulder abduction testing bilaterally, normal upper extremity reflexes, and decreased sensation over both shoulders and the upper arms. Appropriate initial management should consist of
Explanation
REFERENCES: Torg JS, Sennett B, Pavlov H, et al: Spear tackler’s spine: An entity precluding participation in tackle football and collision activities that expose the cervical spine to axial energy inputs. Am J Sports Med 1993;21:640-649.
Torg JS: Cervical spinal stenosis with cord neurapraxia and transient quadriplegia. Sports Med 1995;20:429-434.
Torg JS, Guille JT, Jaffe S: Injuries to the cervical spine in American football players. J Bone Joint Surg Am 2002;84:112-122.
Question 16
Figures 5a and 5b show the radiographs of an active 52-year-old man who has increasing knee pain and progressive varus deformity after undergoing total knee arthroplasty 7 years ago. Examination reveals a small effusion, but he has good motion and stability. What is the most likely diagnosis?
Explanation
REFERENCES: O’Rourke MR, Callaghan JJ, Goetz DG, et al: Osteolysis associated with a cemented modular posterior-cruciate-substituting total knee design. J Bone Joint Surg Am 2002;84:1362-1371.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 529-530.
Question 17
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?

Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 18
Eosinophilic granuloma frequently occurs as a solitary lesion in the tubular long bones. After biopsy, what is the best course of action?
Explanation
REFERENCE: Simon M, Springfield D, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 200.
Question 19
What is the primary goal of the initial (acute) rehabilitation phase of an overhead athlete’s shoulder?
Explanation
REFERENCES: Wilk KE, Meister K, Andrews JR: Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
Wilk KE, Arrigo C: Current concepts in the rehabilitation of the athletic shoulder. J Orthop Sports Phys Ther 1993;18:365-378.
Question 20
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
REFERENCES: Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JS (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 21
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a
Explanation
REFERENCES: Matsen FA, Thomas SC, Rockwood CA, et al: Glenohumeral instability, in Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998,
pp 611-754.
Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principals of techniques, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Question 22
A 57-year-old man who plays recreational sports reports pain in his dominant shoulder. An MR arthrogram is shown in Figure 57. During arthroscopy of the shoulder, what pathology is most likely to be found? Review Topic
Explanation
Question 23
Nutritional rickets is associated with which of the following changes in chemical blood level?
Explanation
and low to normal serologic levels of calcium. To boost serum calcium levels, there is a compensatory increase in PTH and bone resorption, leading to increased alkaline
phosphatase levels.
REFERENCES: Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
Pettifor J: Nutritional and drug-induced rickets and osteomalacia, in Farrus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 399-466.
Einhorn TA: Metabolic bone disease, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 24
A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of
Explanation
REFERENCES: Cooney WP, Linscheid RL, Dobyns JH, Wood MB: Scaphoid nonunion: Role of anterior interpositional bone grafts. J Hand Surg Am 1988;13:635-650.
Fernandez DL: A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-737.
Stark HH, Rickard TA, Zemel NP, Ashworth CR: Treatment of ununited fractures of the scaphoid by illiac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am
1988;70:982-991.
Feldman MD, Manske PR, Welch RL, Szerzinski JM: Evaluation of Herbert screw fixation for the treatment of displaced scaphoid nonunions. Orthopedics 1997;20:325-328.
Question 25
A 70-year-old female with a history of poorly controlled diabetes mellitus presents with purulent ulcers along the plantar aspect of her right forefoot and exposed metatarsal bone. She elects to undergo an amputation. She is insensate to the midfoot bilaterally. Her ankle-brachial index (ABI) for her right posterior tibial artery is 0.4. Further preoperative evaluation demonstrates a transcutaneous oxygen pressure of 45 and an albumin of 3.4. Which of the following would be a contraindication to performing a Syme amputation (ankle disarticulation) in this patient?

Explanation
Pinzur et al retrospectively reviewed their results when performing a single-stage Syme ankle disarticulation in patients with diabetes either for peripheral neuropathy or infection. Patients with ABIs less than 0.5 for the posterior tibial artery had significantly decreased healing rates and smokers had a three-fold increased risk of postoperative infection.
Incorrect Answers:
Question 26
A 53-year-old man has had a long history of multiple joint symptoms, and he notes that the worst pain is from his left shoulder. A radiograph and MRI scan are shown in Figures 13a and 13b. Prior to surgical treatment of the shoulder, what is the most appropriate work-up?
Explanation
5-year period were retrospectively reviewed. Nearly one half of the patients had radiographic evidence of cervical instability on the basis of traditional measurements. While radiographic evidence of cervical instability was not infrequent in this population of patients who underwent total joint arthroplasty for rheumatoid arthritis, radiographic predictors of paralysis were much less common. MRI prior to surgery may also be a consideration if the radiographic appearance of the rotator cuff alters the consideration of surgical treatment. In a series of patients undergoing prosthetic arthroplasty for a variety of shoulder disorders, the presence of a rotator cuff tear has been shown to be associated with a less favorable outcome. Most often, the presence of a rotator cuff tear was associated with a diagnosis of rheumatoid or other inflammatory arthritis and the tears were large and generally irreparable. Some case series demonstrated a higher prevalence of loosening of the glenoid component in patients with a large rotator cuff tear associated with superior migration of the humeral head. However, obtaining an MRI scan of the shoulder is not considered the best response since failure to determine cervical instability may result in anesthetic death. Whereas MRI may be helpful in planning reconstruction, it would be a less important priority.
REFERENCES: Grauer JN, Tingstad EM, Rand N, et al: Predictors of paralysis in the rheumatoid cervical spine in patients undergoing total joint arthroplasty. J Bone Joint Surg Am 2004;86:1420-1424.
Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Question 27
A 27-year-old man sustains a Gustilo and Anderson type II open tibia fracture during a motorcycle accident. He had his full 3 doses of tetanus vaccination as an infant. He also had a tetanus booster vaccination 18 months ago when he began a new job. In addition to intravenous antibiotics, what tetanus prophylaxis should be administered?

Explanation
the past 5 years so he does not need an update of the vaccination or immune globulin. Illustration A is a concise table that can be used as an algorithm to provide appropriate tetanus prophylaxis.
Question 28
A 28-year-old woman sustained an injury to her dominant right arm after falling off her porch. Examination reveals a deformity at the elbow. She is neurovascularly intact. Figures 46a and 46b show the radiographs obtained before closed reduction, and postreduction radiographs are shown in Figure 46c and 46d. What is the most likely early complication?
Explanation
REFERENCES: Ring D, Jupiter JB: Reconstruction of posttraumatic elbow instability. Clin Orthop 2000;370:44-56.
O’Driscoll SW: Classification and evaluation of recurrent instability of the elbow. Clin Orthop 2000;370:34-43.
O’Driscoll SW, Morrey BF, Korinek S, An KN: Elbow subluxation and dislocation. Clin Orthop 1992;280:186-197.
Question 29
A 13-year-old boy who has a history of a pituitary adenoma has an unstable unilateral slipped capital femoral epiphysis. What is the indication for prophylactic pinning of the contralateral, unslipped side? Review Topic
Explanation
Question 30
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?
Explanation
REFERENCES: Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.
Question 31
..Figures 87a through 87e are the radiograph, MRI scans, and biopsy specimen of an 83-year-old woman who is experiencing pain in her distal thigh with activity and at night. She has undergone total hip arthroplasty for hip osteoarthritis. The most appropriate treatment is
Explanation
Figures 88a and 88b are the radiographs of a 70-year-old woman with a remote history of localized renal cell carcinoma. She has insidious onset of right shoulder pain that worsens with any activity and at night. She appears otherwise healthy.


Question 32
Figure 2a shows the radiograph of a 48-year-old man who was involved in a motorcycle accident. A CT scan is shown in Figure 2b. The patient underwent pelvic angiography for persistent hypotension despite resuscitation. What vessel is most likely to be injured?
Explanation
REFERENCES: O’Neill PA, Riina J, Sclafani S, et al: Angiographic findings in pelvic fractures. Clin Orthop 1996;329:60-67.
Belley G, Gallix BP, Derossis AM, et al: Profound hypotension in blunt trauma associated with superior gluteal artery rupture without pelvic fracture. J Trauma 1997;43:703-705.
Question 33
Of the following factors, which is considered the most important prognostic indicator in soft-tissue sarcomas?
Explanation
REFERENCE: Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173.
Question 34
Which of the following statements best describes the outcome of the routine use of continuous passive motion (CPM) machines after total knee arthroplasty (TKA)?
Explanation
REFERENCES: Pellicci PM, Tria AJ, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 287-293.
McInnes J, Larson MG, Daltroy LH, et al: A controlled evaluation of continuous passive motion in patients undergoing total knee arthroplasty. JAMA 1992;268:1423-1428.
Kumar PJ, McPherson EJ, Dorr LD, et al: Rehabilitation after total knee arthroplasty: A comparison of 2 rehabilitation techniques. Clin Orthop 1996;331:93-101.
Question 35
A 42-year-old woman who observes traditional Muslim practices is seen in your office accompanied by her physician husband to discuss possible elective bunion correction. In considering the treatment of this patient, what is one of the most important considerations?
Explanation
REFERENCE: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 36
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain? Review Topic

Explanation
Question 37
Figures 43a and 43b show the T 1 - and T 2 -weighted MRI scans of a 78-year-old woman who reports the sudden atraumatic onset of well-localized medial knee pain. Pain is worse at night and also occurs with weight-bearing activity. What is the most likely diagnosis?
Explanation
REFERENCES: Soucacos PN, Berris AE, Xenakis TH, et al: Knee osteonecrosis: Distinguishing features in differential diagnosis, in Urbanik JR, Jones JD (eds): Osteonecrosis. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-424.
Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.
Question 38
-Figures 222a and 222b are the radiograph and MRI scan of a 41-year-old man who has had severe leg pain for 6 months despite physical therapy and medications. Examination reveals normal strength and sensation in both lower extremities. What is the most effective treatment option?
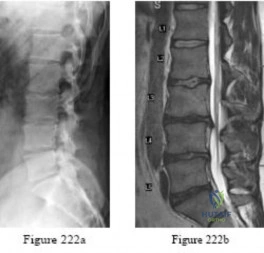
Explanation

Question 39
Figure 53 shows the arteriogram of a 45-year-old man who has severe vasculitis. What do the findings show?
Explanation
REFERENCE: Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadephia, PA, Mosby-Year Book, 1998, p 110.
Question 40
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child’s ability to walk in the future?
Explanation
REFERENCES: Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Tachdjian MO: The neuromuscular system: Cerebral palsy, in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 2, p 1621.
Question 41
A 12-year-old Little League pitcher reports lateral elbow pain and “catching.” Examination reveals painful pronation and supination and tenderness over the lateral elbow. Radiographs are shown in Figures 22a and 22b. Initial management should consist of Review Topic

Explanation
Question 42
Which of the following statements is true regarding the posterior oblique portion of the medial collateral ligament of the elbow? Review Topic
Explanation
The medial ulnar collateral ligament is one of the primary static stabilizers of the elbow and is composed of three parts: anterior, posterior and transverse. The MCL provides resistance to valgus and distractive stresses. The anterior oblique fibers (of the anterior bundle) are the most important against valgus stresses. The posterior bundle is involved elbow contractures and releasing it can yield significant flexion gains, without creating valgus instability.
Morrey et al. performed a pilot study on 4 specimens and found the valgus stability is equally divided among the medial collateral ligament complex, anterior capsule, and bony articulation in full extension; whereas, at 90 degrees of flexion the contribution of the anterior capsule is assumed by the medial collateral ligament which provides approximately 55% of the stabilizing contribution to valgus stress.
Regan et al. was a subsequent study by the same group that found the posterior medial collateral ligament (PMCL) was taut only when the elbow was in a flexed position. Among the collateral ligaments, the anterior (AMCL) was the strongest and stiffest. (Of note, using present terminology these would be referred to as posterior oblique and anterior oblique portions of the medial ulnar collateral complex).
Wada et al. reported a series of open medial releases for post-traumatic elbow contracture and found scarring on the posterior oblique bundle in all cases. Large increases in flexion were achieved by releasing this structure and the capsule without the need for a lateral incision in most cases.
Illustrations A and B show the posterior oblique portion of the medial collateral ligament. Illustration C shows the most recent terminology and identifies the area to be resected for stiffness.
Incorrect Answers:
Question 43
After closed reduction of the dislocation shown in Figure 42, it is essential to avoid placing the upper extremity in what position for the first 4 to 6 weeks?
Explanation
REFERENCES: Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1986;68:724-731.
Pollock RG, Bigliani LU: Recurrent posterior shoulder instability: Diagnosis and treatment.
Clin Orthop 1993;291:85-96.
Question 44
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
REFERENCES: Herring JA: Metabolic and endocrine bone diseases, in Tachdjian’s Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743.
Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Staheli LT: Practice of Pediatric Orthopedics. Philadelphia, PA, Lippincott Williams & Wilkins, 2001.
Question 45
Intramembranous ossification during fracture repair is characterized by absence of which of the following elements?
Explanation
REFERENCES: Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Buckwalter JA, Einhorn TA, Bolander ME: Healing of the musculoskeletal tissues, in Rockwood CA Jr, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 261-276.
Question 46
Figures 142a and 142b are the current radiographs of an 89-year-old woman who had open reduction and internal fixation (ORIF) of a distal periprosthetic femur fracture 4 months ago. An examination reveals well-healed incisions, a painful range of motion from 15 to 85 degrees, and normal neurovascular function. An infection workup, including an erythrocyte sedimentation rate and C-reactive protein level, is negative. The most appropriate treatment option is
Explanation
Current periprosthetic fracture treatments after TKA include ORIF via plating, retrograde nailing, or revision using standard revision TKA components or a distal femoral arthroplasty. Locked plating has demonstrated a trend toward increased nonunion rates when compared to retrograde nailing, as evidenced in this patient. The advanced age of the patient, the presence of failed fixation, and the significant amount of bone loss preclude a trial of further nonsurgical treatment or revision ORIF. A review of 3 methods for treatment of comminuted distal periprosthetic femur fractures in patients older than age 70 demonstrated that distal femur arthroplasty should be considered in patients with advanced age and poor bone quality who require early mobilization. As a result, treatment of this patient with a revision TKA using a distal femoral arthroplasty would be the preferred response because of the bone quality and fracture pattern. Above-knee amputation is a salvage procedure and is not indicated at this time.
Question 47
A 56-year-old man has had a 2-year history of slowly progressive neck pain and bilateral arm aching. Over the past year, he has noticed intermittent, diffuse numbness in both hands, with decreased grip strength and mild hand clumsiness. He denies any problems with balance. Examination shows a wide-based gait, intrinsic wasting, and a postive Hoffman's sign bilaterally. An MRI scan of the cervical spine is shown in Figure 16. What is the most appropriate treatment? Review Topic

Explanation
Question 48
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
REFERENCES: Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 49
A 70-year-old golfer has pain in her dominant shoulder. She reports that initially the pain was at night but now she is unable to play. Examination reveals weakness in external rotation and shoulder abduction. Radiographs reveal the humeral head articulating with a thin acromion. Management should consist of
Explanation
REFERENCES: Bokor DJ, Hawkins RJ, Huckell GH, et al: Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
Wirth MA, Basamania C, Rockwood CA Jr: Nonoperative management of full-thickness tears of the rotator cuff. Orthop Clin North Am 1997;28:59-67.
Question 50
A 58-year-old reports pain and stiffness in his left shoulder following a seizure episode. Diagnosis at the time of the seizure is a frozen shoulder, and management consists of an aggressive physical therapy program of stretching exercises. Four months later he continues to have shoulder pain and has not gained any additional range of motion. A CT scan is shown in Figure 50. Management should now consist of
Explanation
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Checchia SL, Santos PD, Miyazaki AN: Surgical treatment of acute and chronic posterior fracture-dislocation of the shoulder. J Shoulder Elbow Surg 1998;7:53-65.
Question 51
Which of the following is considered an important factor in improved cemented femoral stem survivorship?
Explanation
REFERENCES: Noble PC, Collier MB, Maltry JA, Kamaric E, Tullos HS: Pressurization and centalization enhance the quality and reproducibility of cement mantles. Clin Orthop 1998;355:77-89.
Crowninshield RD, Brand RA, Johnston RC, Milroy JC: The effect of femoral stem cross-sectional geometry on cement stresses in total hip reconstruction. Clin Orthop 1980;146:71-77.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 52
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 53
The Lisfranc ligament connects the base of the
Explanation
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Solan MC, Moorman CT III, Miyamoto RG, et al: Ligamentous restraints of the second tarsometatarsal joint: A biomechanical evaluation. Foot Ankle Int 2001;22:637-641.
Question 54
.Figures 89a and 89b are the radiographs of an 18-year-old woman who has had elbow pain after falling on an outstretched hand. She is evaluated 5 days after the injury. Examination reveals the wrist is normal and her elbow has a limited arc of motion of 30 to 90 degrees of flexion/extension and 20 to 20 degrees of pronation and supination, with tenderness isolated to the lateral side of the elbow. What is the most appropriate treatment option?
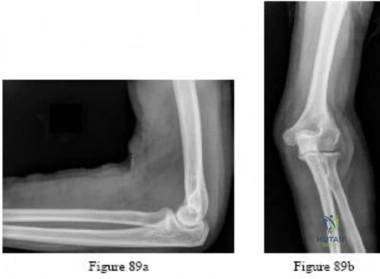
Explanation
Question 55
A 48-year-old man undergoes arthroscopy to repair a rotator cuff tear. During the arthroscopy, the tear is characterized and found to involve the entire supraspinatus and a majority of the infraspinatus tendons. After mobilization, the posterior rotator cuff can reach the greater tuberosity. However, the supraspinatus tendon cannot reach its insertion point at the greater tuberosity. What is the most appropriate treatment? Review Topic
Explanation
release, reverse acromioplasty, and tenotomy of the biceps tendon may improve shoulder pain. If these procedures fail, then a muscle transfer procedure can also be considered in select patients. If, however, a portion of the rotator cuff can be repaired, even partial repair can balance the coronal and axial forces about the shoulder to restore the kinematics of the joint. Reverse total shoulder arthroplasty is not appropriate for this relatively young patient.
Question 56
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
Question 57
When compared with a patient who has a subluxated hip, a patient with a dislocated hip who is undergoing acetabular reconstruction for developmental dysplasia of the hip will most likely have
Explanation
REFERENCES: Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360.
Schmalzried TP, Noordin S, Amstutz HC: Update on nerve palsy associated with total hip replacement. Clin Orthop 1997;344:188-206.
Question 58
A 24-year-old man is involved in a motor vehicle accident at 60 mph. He sustains multiple injuries including an intra-abdominal injury requiring a splenectomy and a closed right femoral shaft fracture. Which variable will best indicate the patient's resuscitation status when deciding whether to proceed with definitive care of the fracture at the conclusion of the laparotomy? Review Topic
Explanation
Question 59
The transverse diameter of the pedicle is most narrow at which of the following levels?
Explanation
REFERENCES: O’Brien MF, Lenke LG, Mardjetko S, et al: Pedicle morphology in thoracic adolescent idiopathic scoliosis: Is pedicle fixation an anatomically viable technique? Spine 2000;25:2285-2293.
Vaccaro AR, Rizzolo SJ, Allardyce TJ, et al: Placement of pedicle screws in the thoracic spine: Part I. Morphometric analysis of the thoracic vertebrae. J Bone Joint Surg Am
1995;77:1193-1199.
Question 60
In a patient who has had low back pain for less than 2 weeks, which of the following findings is an indication for continued observation and symptomatic treatment rather than more aggressive evaluation and/or treatment?
Explanation
REFERENCES: Frymoyer JW: Back pain and sciatica. N Engl J Med 1988;318:291-300.
McCullough JA, Transfeldt EE: Macnab’s Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 240-357.
Question 61
Which of the following muscles attaches to the coracoid process of the scapula?
Explanation
REFERENCES: Jobe CM: Anatomy and surgical approaches, in Jobe FW (ed): Operative Techniques in Upper Extremity Sports Injuries. St Louis, MO, Mosby, 1996, pp 140-142.
Jobe CM: Gross anatomy of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 49-66.
Question 62
Preservation or reconstruction of which of the following structures is essential to minimize the risk of hallux valgus developing after removal of part or all of the medial sesamoid?
Explanation
REFERENCES: Dedmond BT, Cory JW, McBryde A Jr: The hallucal sesamoid complex. J Am Acad Orthop Surg 2006;14:745-753.
Lee S, James WC, Cohen BE, et al: Evaluation of hallux alignment and functional outcome after isolated tibial sesamoidectomy. Foot Ankle Int 2005;26:803-809.
Question 63
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of
Explanation
REFERENCES: Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Warner JJ, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 64
A 23-year-old woman falls from a bicycle and sustains a right knee injury. Figures 12a through 12d show radiographs and MRI scans of the knee. What is the most likely diagnosis?
Explanation
REFERENCES: Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiss DA, Watson JT: Fractures of the tibial plateau, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott-Raven, 1996, pp 1920-1953.
Lubowitz JH, Elson WS, Guttmann D: Arthroscopic treatment of tibial plateau fractures: Intercondylar eminence avulsion fractures. Arthroscopy 2005;21:86-92.
Question 65
Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?

Explanation
The fracture has occurred around the stem, representing a Vancouver type B fracture, and the stem is clearly loose, making it a type B2 fracture. The appropriate treatment is removal of the loose in situ stem; ORIF of the femur using cerclage wires, cables, or a plate; and insertion of a longer revision stem such as a tapered fluted modular titanium or fully porous coated cylindrical stem to bypass the fracture. All of the other options are incorrect, because they represent inappropriate treatment options for a Vancouver type B2 fracture.
Question 66
What clinical finding is associated with the least favorable prognosis in an adolescent patient who has been diagnosed with a high-grade osteosarcoma of the distal femur?
Explanation
REFERENCE: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlation. Philadelphia, PA, Lea and Febiger, 1989, pp 344-350.
Question 67
Figures 1a and 1b show the clinical photograph and oblique radiograph of a 52-year-old man who has plantar first metatarsal pain. A felt pad in the shoe proximal to the area of pain has failed to provide relief. Management should now consist of
Explanation
REFERENCES: Mann RA, Wapner KL: Tibial sesamoid shaving for treatment of intractable plantar keratosis. Foot Ankle 1992;13:196-198.
Mann RA, Mann JA: Keratotic disorders of the plantar skin. Instr Course Lect 2004;53:287-302.
Question 68
The scoring system for impending pathologic fractures devised by Mirels involves assessment of which of the following factors?
Explanation
REFERENCES: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. 1989. Clin Orthop Relat Res 2003;415:S4-S13.
Damron TA, Morgan H, Prakash D, et al: Critical evaluation of Mirels’ rating system for impending pathologic fractures. Clin Orthop Relat Res 2003;415:S201-S207.
Question 69
What tendon is closest to an appropriately placed anterolateral portal for ankle arthroscopy?
Explanation
REFERENCE: Ogut T, Akgun I, Kesmezacar H, et al: Navigation for ankle arthroscopy: Anatomical study of the anterolateral portal with reference to the superficial peroneal nerve. Surg Radiol Anat 2004;26:268-274.
Question 70
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
Explanation
REFERENCES: Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Mader TJ: Avulsion of the rectus femoris tendon: An unusual type of pelvic fracture. Pediatr Emerg Care 1990;6:198-199.
Question 71
A 45-year-old male auto mechanic presents to your office with left lateral elbow pain for 6 weeks. On physical exam he has tenderness to palpation over the lateral epicondyle and pain with resisted wrist extension. An MRI is shown in figures A and B. After failing non-surgical treatment modalities, he undergoes arthroscopic surgical management. At 3 months post-operatively, the patient reports persistent left elbow pain and an audible clicking since surgery which occurs when he lifts heavy objects and when he pushes himself up out of a chair. What is the best surgical treatment option? Review Topic
Explanation
PLRI is the result of an incompetent lateral ulnar collateral ligament (LUCL), a component of the elbow lateral collateral ligament complex. The LUCL originates on the lateral epicondyle of the humerus and inserts upon the supinator crest of the ulna. When deficient from acute trauma or from repetitive microtrauma, the elbow becomes rotationally unstable with elbow extension, supination, and an applied valgus force. In this case, the patient has had iatrogenic damage to the LUCL from an arthroscopic release of the extensor carpi radialis brevis (ECRB) for treatment of lateral epicondylitis. This patient exhibits an important manifestation of this: a positive chair pushup test. This test is positive when pushing off of a chair with a supinated forearm causes pain and instability. Due to the chronicity of the injury (3 months) and his persistent symptoms of instability (pain and clicking) the patient would benefit from surgical reconstruction of the damaged LUCL using either palmaris longus or gracilis allograft.
Kelly et. al. reviewed the known major and minor complications of elbow arthroscopy among 473 consecutive cases at their institution from 1980-1998. The most common complications were transient nerve palsies in 10 patients. Among them, the major
nerves involved included the anterior interosseous nerve, posterior interosseous nerve, ulnar nerve, superficial radial nerve, and medial antebrachial cutaneous nerve. The risk of iatrogenic nerve injury was increased among patients with rheumatoid arthritis. The most frequent complication was prolonged drainage from the portal sites.
Calfee et. al. reviewed the management of lateral epicondylitis. The authors suggest open or arthroscopic surgical debridement of the common extensor origin after failure of rest, orthoses, nonsteroidal drugs, physical therapy, cortisone and platelet-rich plasma injections. They do acknowledge that excessive debridement may compromise lateral elbow stability and cause PLRI.
O'Brien et. al. described the surgical techniques for managing PLRI, including an open technique for chronic injuries or revision treatment. In this setting, the authors suggest use of palmaris or gracilis allograft for reconstruction.
Figures A and B are an axial and coronal T2 weighted MRI of an elbow demonstrating signal intensity in the origin of the ECRB, consistent with lateral epicondylitis.
Incorrect Answers:
Question 72
A 5-year-old boy reports intermittent left elbow pain. History reveals that he injured his elbow 4 months ago, but had no treatment. He is now using his arm normally but reports pain almost daily. Examination reveals tenderness over the lateral epicondyle and a prominence is evident. Range of motion is from -5 2010 Pediatric Orthopaedic Examination Answer Book • 55 degrees to 120 degrees. Radiographs are shown in Figure 67. Management should include
Explanation
REFERENCES: Wattenbarger JM, Gerardi J, Johnson CE: Late open reduction internal fixation of lateral condyle fractures. J Pediatr Orthop 2002;223:94-398.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 73
A 7-year-old boy has had chronic left leg pain that is worse at night but is not activity related. Use of nonsteroidal anti-inflammatory drugs for the past 6 months has failed to provide relief. A CBC count with differential, erythrocyte sedimentation rate, and C-reactive protein are within normal limits. Radiographs and a CT scan are shown in Figures 31a through 31c. Management should consist of
Explanation
REFERENCES: Donahue F, Ahmad A, Mnaymneh W, Pevsner NH: Osteoid osteoma: Computed tomography guided percutaneous excision. Clin Orthop 1999;366:191-196.
Rosenthal DI, Hornicek FJ, Wolfe MW, et al: Percutaneous radiofrequency coagulation of osteoid osteoma compared with operative treatment. J Bone Joint Surg Am 1998;80:815-821.
Question 74
A 24-year-old baseball pitcher reports pain over the posterior aspect of his shoulder that occurs only during throwing. He notes that the discomfort is greatest during the late cocking and early acceleration phases. Examination reveals localized tenderness with palpation over the external rotators and posterior glenoid. Radiographs are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCES: Meister K, Andrews JR, Batts J, Wilk K, Baumgarten T, Baumgartner T: Symptomatic thrower’s exostosis: Arthroscopic evaluation and treatment. Am J Sports Med 1999;27:133-136.
Ferrari JD, Ferrari DA, Coumas J, Pappas AM: Posterior ossification of the shoulder: The Bennett lesion. Etiology, diagnosis, and treatment. Am J Sports Med 1994;22:171-176.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posteriorsuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 75
Which of the following procedures is not part of the routine evaluation of a patient with suspected metastatic disease to bone?
Explanation
REFERENCES: Simon MA, Bartucci EJ: The search for the primary tumor in patients with skeletal metastases of unknown origin. Cancer 1986;58:1088-1095.
Frassica FJ, Gitelis S, Sim FH: Metastic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 76
Figure 12 shows an arthroscopic view from an inferolateral portal of a right knee. The asterisk indicates which structure?

Explanation
The asterisk indicates the anteromedial bundle of the anterior cruciate ligament. The anterior cruciate ligament consists of 2 functional bundles: anteromedial and posterolateral. During extension of the knee, the posterolateral bundle becomes taut. In flexion, the anteromedial bundle is tight and the posterolateral bundle relaxes. Recently, techniques for double-bundle reconstruction have been described to recreate the normal anatomic relationship of the 2 bundles.
RECOMMENDED READINGS
Chhabra A, Zelle BA, Feng MT, Fu FH. The arthroscopic appearance of a normal anterior cruciate ligament in a posterior cruciate ligament-deficient knee: the posterolateral bundle (PLB) sign. Arthroscopy. 2005 Oct;21(10):1267. PubMed PMID: 16226658. View Abstract at PubMed
Cha PS, Brucker PU, West RV, Zelle BA, Yagi M, Kurosaka M, Fu FH. Arthroscopic double-bundle anterior cruciate ligament reconstruction: an anatomic approach. Arthroscopy. 2005 Oct;21(10):1275. PubMed PMID: 16226666. View Abstract at
PubMed
Question 77
A 45-year-old woman with grade II adult-acquired flatfoot deformity has pain on the lateral side of her foot just distal to the tip of the fibula. Which component of a comprehensive flatfoot reconstruction most likely will address the deformity responsible for this pain?
Explanation
Patients develop lateral ankle pain with progression of adult-acquired flatfoot deformity. This is associated with increased hindfoot valgus deformity. Calcaneal fibular impingement has been considered the primary cause of this pain. Studies demonstrate that arthrosis of the posterior facet of the subtalar joint strongly correlates with lateral pain in adult-acquired flatfoot deformity. Both conditions are related to hindfoot valgus deformity. Although lateral column lengthening is a powerful tool for correction of flatfoot deformity, its effect on hindfoot deformity is less defined. Lateral column lengthening provides better correction of the longitudinal arch of the midfoot and realignment of the medial column than other osteotomies. A medializing calcaneal osteotomy has a significant linear effect on hindfoot valgus alignment. Spring ligament reconstruction and medial cuneiform opening-wedge osteotomies have less effect on hindfoot alignment than the medial calcaneal slide.
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
Question 78
Sciatic nerve
Explanation
The principal thrombogenic stimulus leading to the production of venous thromboembolic disease during total hip arthroplasty occurs at which time:
Question 79
In the anterior cruciate ligament-deficient knee, what structure provides an important secondary restraint to anterior tibial translation? Review Topic
Explanation
Question 80
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time?
Explanation
REFERENCES: Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Carragee EJ: Clinical practice: Persistent low back pain. N Engl J Med 2005;352:1891-1898.
Question 81
A 75-year-old man sustains an anterior dislocation of his reverse total shoulder arthroplasty. What activity places the arm in the position most commonly associated with reverse total shoulder dislocation?
Explanation
such as pushing out of a chair. The other positions described do not involve extension of the shoulder.
Question 82
The subcutaneous nerve most at risk for transection during an anterior surgical exposure of the ankle is the
Explanation
The dorsal medial cutaneous nerve arising from the superficial peroneal nerve crosses the inferior extent of a routine extensile surgical exposure to the ankle joint. The extensile anterior incision develops the interval between the tibialis anterior and extensor hallucis tendons, and, although the deep peroneal nerve is lateral and posterior to the extensor hallucis longus, the nerve most at risk during this exposure is the cutaneous branch supplying the dorsal medial foot to the great toe. Ankle replacement surgery is becoming more common; consequently, surgeons must be familiar with this anatomic landmark and risks related to its transection during surgery.
The medial plantar nerve is at risk when medial hindfoot incisions are made through the
abductor hallucis muscle during tarsal tunnel release and harvest of the flexor hallucis tendon for transfer. The dorsal cutaneous branch of the sural nerve supplies the lateral dorsal
Question 83
What is the most common complication of halo vest immobilization in adults?
Explanation
REFERENCES: Baum JA, Hanley EN Jr, Pullekines J: Comparison of halo complications in adults and children. Spine 1989;14:251-252.
Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
Nemeth JA, Mattingly LG: Six-pin halo fixation and the resulting prevalence of pin-site complications. J Bone Joint Surg Am 2001;83:377-382.
Question 84
A 22-year-old skier reports painful range of motion in the left thumb after falling forward on his outstretched hand while holding his ski pole. Examination of the left thumb reveals increased AP laxity and 45° of valgus laxity at the metacarpophalangeal (MCP) joint. Examination of the right thumb shows 25° of valgus laxity at the MCP joint. Radiographs are normal. Management should consist of
Explanation
REFERENCE: Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint. J Am Acad Orthop Surg 1997;5:224-229.
Question 85
- A healed fracture of the tibia that demonstrates 25 degrees apex posterior angulation and 28 degrees varus angulation on AP and lateral radiographs is most accurately described as a
Explanation
Question 86
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?
Explanation
REFERENCES: Ginsburg GM, Bassett GS: Back pain in children and adolescents: Evaluation and differential diagnosis. J Am Acad Orthop Surg 1997;5:67-78.
Schwend RM, Hennrikus W, Hall JE, et al: Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am 1995;77:46-53.
Question 87
A 12-year-old male patient is scheduled to undergo femoral lengthening. The 2 techniques at your disposal are (1) femoral lengthening along the mechanical axis of the limb with an external fixator, and (2) femoral lengthening along the anatomical axis of the femur with a telescoping nail. What happens to the mechanical axis of the limb when performing these techniques? Review Topic
Explanation
There is a difference of approximately 7° between the mechanical axis of the limb and the anatomical axis of the femur. Lengthening along the anatomical axis of the femur leads to lateral MAD. Similarly, shortening along the anatomical axis of the femur leads to medial MAD.
Kasis et al. described limb shortening of 4cm using external fixator assistance to dial in compression before fixation with a blade plate. They claimed this allowed correction of any tendency to medialize the mechanical axis of the limb prior to plate fixation.
Burghardt et al. described femoral lengthening over a telescoping nail and found lateral shift of the mechanical axis in 26 of 27 limbs, although many were minor and inconsequential. As a rule of thumb, the mechanical axis will shift about 1 mm laterally for every 1 cm of lengthening.
Illustration A illustrates how when lengthening with an external fixator (left), the mechanical axis can be preserved. On the other hand, when lengthening over a nail
(right), the anatomical axis is preserved, but there is lateral MAD (ISKD, intramedullary skeletal kinetic distractor).
Incorrect Answers:
Question 88
The dominant arterial blood supply to the patella enters at which anatomical location?
Explanation
The arterial blood supply to the patella is made up of branches of six main arteries: the descending genicular, the superior medial and lateral genicular, the inferior medial and lateral genicular, and the anterior genicular. Several of these branches contribute to the anastomotic network that surround the patella. From the ring, there are two main interosseous blood supply systems to enter the patella, known as the midpatellar and polar vessel systems. The distal pole of the patella is considered to be the largest arterial contribution to the peripatellar ring and the polar vessel system.
Lazaro et al. used twenty matched pairs of fresh-frozen cadaveric knees to isolate the dominant blood supply to the patella. After cannulating the superficial femoral artery, anterior tibialis artery, and posterior tibialis artery and performing magnetic resonance imaging, they found that the largest arterial contribution to the patella entered at the inferior pole in 100% of the specimens. In sixteen specimens (80%), the dominant artery entered the medial aspect of the distal pole. In three specimens (15%), it entered the lateral aspect of the distal pole.
Illustation A shows the arterial supply system to the patella. The dominant arterial supply enters at the distal (inferior) pole of the patella, with the dominant geniculate arteries entering inferomedially (labelled with a green star). Illustration B shows an anatomical illustration of the patellar blood supply. Note the dominant distal pole blood supply (arrow).
Incorrect Answers:
Question 89
A 42-year-old man has a symptomatic flatfoot deformity and walks with a slight limp after falling off a scaffold 9 months ago. He also reports that he has had difficulty returning to work. Orthotics have failed to provide relief. Current radiographs are shown in Figures 19a and 19b. To relieve his pain and return the patient to work, treatment should consist of
Explanation
REFERENCES: Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Sangeorzan BJ, Veith RG, Hansen ST Jr: Salvage of Lisfranc’s tarsometatarsal joint by arthrodesis. Foot Ankle 1990;10:193-200.
Question 90
An injury to the axillary nerve would result in deltoid muscle weakness. 5 . An injury to the thoracodorsal nerve would result in latissimus dorsi weakness and would not cause scapular winging.

Explanation
The medial ulnar collateral ligament, or medial collateral ligament of the elbow, is composed of three bundles: an anterior bundle, a posterior bundle, and a variable
transverse oblique bundle. During late cocking and early acceleration phases of the overhead throw, the medial UCL is subjected to the greatest amount of valgus stress to the elbow. During this phase, the forearm lags behind the upper arm and generates valgus stress while the elbow is primarily dependent on the anterior band of the UCL for stability. This puts the ligament at greatest risk of injury during this phase.
Fleisig et al. examined the kinetics of baseball pitching and the implications on injury mechanisms. They showed that the UCL contributes to 54% of the varus torque that is generated during the early acceleration of throwing. The position of greatest load occurred when the arm was flexed to 95 +/14 degrees with an applied valgus load.
Illustration A shows a diagram of the medial ulnar collateral ligament ligament bundles. Incorrect Answers:
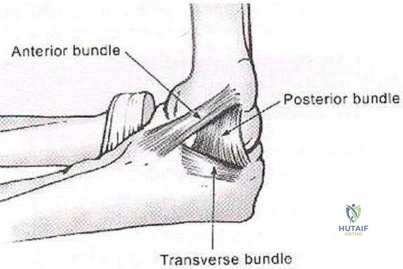
A 14-year-old elite basketball player develops acute medial elbow pain after a fall. Physical examination reveals medial elbow tenderness over the submlime tubercle, but full range of motion. The provocative tests seen in Figure A exacerbate his elbow pain. Radiographs of the elbow are normal. What would be the next best step in treatment?
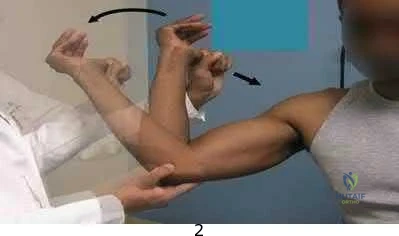
Supervised elbow stretching program Therapeutic elbow arthroscopy

Static elbow external fixation for 3 to 6 weeks, then MR arthrography if pain continues Activity avoidance for 6 weeks

Serial inflammatory markers and rheumatology referral
Figure A shows a moving valgus stress, which is a provocative test for ulnar collateral ligament (UCL) injury and elbow valgus instability. The initial treatment would be a short period of immobilization, rest and flexor pronator strengthening in this patient population.
Adolescent UCL injuries can be effectively treated with a short period of rest and NSAIDs to control pain. As the acute inflammation resolves, the patient can be started on a supervised therapy program. This should target flexor pronator muscles, as they are important secondary dynamic stabilizers of valgus stress. Once symptoms have improved and the athlete has regained full range of motion and strength, a mediated throwing program may be initiated. Throwing athletes should be educated to avoid provocative activities during this period.
Chen et al. wrote a JAAOS article on shoulder and elbow injuries in the skeletally immature athlete. They state that surgery is reserved for older athletes with persistent valgus instability despite > 6 months of non-surgical management.
Murthi et al. reviewed recurrent elbow instability. They state the anterior bundle of the medial ulnar collateral ligament complex is the primary valgus stabilizer of the elbow. The anterior band is taut for the first 60° of elbow flexion, and the posterior band is taut from 60° to 120° of flexion. The secondary valgus stabilizers of the elbow joint include the radial head, the anterior and posterior aspects of the capsule, and the muscular forces around the joint.
Figure A is showing a moving valgus stress. Illustration A shows provocative tests for valgus instability of the elbow. The image on the left shows a valgus stress test. This assesses the anterior bundle of the medial ulnar collateral ligament complex by flexing the elbow to 25-30 degrees and applying a valgus load across the elbow. The image on the right shows milking maneuver. This assesses the posterior bundle of the medial ulnar collateral ligament complex by pulling on the

beyond 90°. Incorrect Answers:
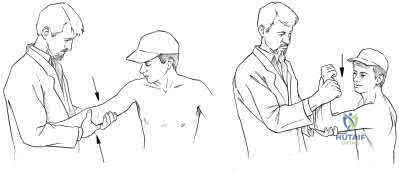
A young, healthy male undergoes a distal biceps repair and sustains an iatrogenic nerve injury during the procedure. Which of the following clinical findings are most likely to be seen in this circumstance? Inability to extend the thumb

Lateral volar forearm numbness Inability to flex the middle finger Medial volar forearm numbness Dorsal thumb numbness
The most commonly injured nerve during a distal biceps repair is the lateral antebrachial cutaneous nerve (LABCN). Injury to this nerve would result in lateral volar forearm numbness.
Distal biceps avulsions can be partial or complete. Indications for surgical management include young, healthy patients who do not wish to sacrifice function, as well as partial biceps avulsions that do not respond to conservative management. Repair of a distal biceps avulsion can be approached through either an anterior one-incision technique or a two-incision technique (BoydAnderson). The one-incision technique uses the interval between the brachioradialis (radial nerve) and pronator teres (median nerve), while the two-incision technique uses this same interval in addition to a second posterolateral elbow incision. The lateral antebrachial cutaneous nerve is the most common nerve injured during either approach.
Kelly et al. retrospectively reviewed 74 distal biceps tendon repairs, and found five sensory nerve paresthesias. The lateral antebrachial cutaneous nerve was most commonly injured, followed by the superficial radial nerve.
Cain et al. retrospectively reviewed 198 distal biceps tendon repairs, and found a 36% complication rate. Lateral antebrachial cutaneous nerve paresthesias were found in 26%, while radial sensory nerve paresthesias were found in 6%, and posterior interosseous nerve (PIN) injury in 4%.
Illustration A shows the close relationship between the lateral antebrachial cutaneous nerve (LABCN) and the distal biceps. Illustration B shows the sensory nerves of the upper extremity and their respective areas of innervation.
Incorrect Answers:
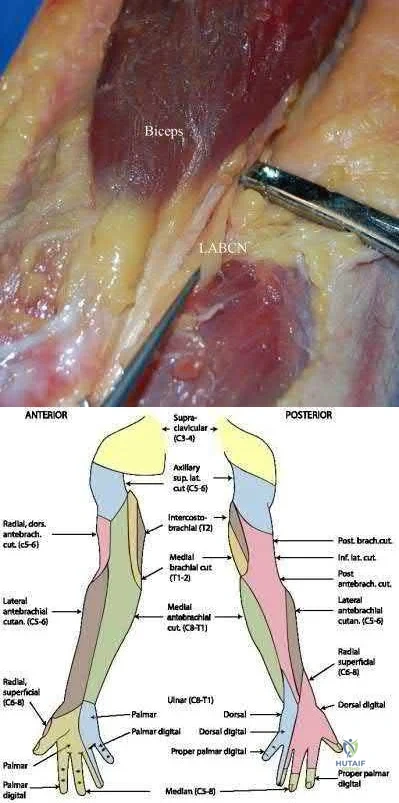
A 33-year-old female presents with left shoulder weakness. Two weeks prior to presentation, the patient experienced sudden-onset, left shoulder pain, which occurred a few days after receiving the influenza vaccine. The pain subsided over the next day, followed by gradual weakness of her shoulder and eventual general disuse of her left upper extremity. An initial visit to her primary care provider resulted in the recommendation of observation. On physical exam, there is weakness and gross atrophy of the shoulder girdle. Figures A & exhibit T2-weighted MRI images of her left shoulder. To further confirm her suspected diagnosis, she is sent for electromyography.
What is the expected result?
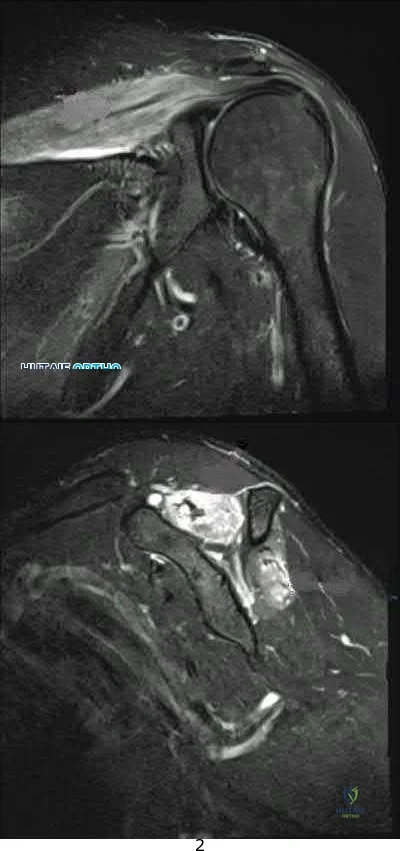
Normal results
Fibrillation potentials consistent with compression at the spinoglenoid notch 3 . Sharp waves and fibrillations potentials associated with the deltoid and biceps

Acute denervation of both peripheral nerve and nerve root distribution with sharp waves and fibrillation potentials

Early reinnervation with polyphasic motor unit potentials
This patient has Parsonage-Turner Syndrome, which, when tested on EMG during the first 3 weeks, exhibits acute denervation of both peripheral nerve and nerve root distributions with positive sharp waves and fibrillation potentials.
Parsonage-Turner Syndrome is an idiopathic disorder with an etiology that is still unknown. Typical antecedent events can involve a viral illness, recent immunization, or elective surgery. Clinical presentation is usually initiated by acute onset shoulder pain, which quickly subsides and is followed by gradual weakness. Early MRI exhibits edema in the effected muscles, and fatty infiltration in later stages. Treatment is typically non-operative, and resolution can be seen as early as 6 weeks from onset.
Tjoumakaris et al. provide a thorough review of the diagnosis and management of ParsonageTurner Syndrome. The authors report the usefulness of MRI, which exhibits early edema and later fatty infiltration in the affected muscles, and urge the use of EMG as a confirmatory diagnostic measure as well as a monitoring tool to track resolution. Early identification and diagnosis may be treated with a short course of steroids, which may help shorten symptoms.
Stutz et al. concisely summarize Parsonage-Turner Syndrome and provide typical presentation, diagnosis and management principles. The authors note the common association with viral illness and/or recent immunization along with the importance of obtaining a baseline chest radiograph to rule out a compressive Pancoast tumor. Management is typically supportive with eventual resolution.
Figures A, B, and C are T2-weighted coronal, sagittal, and axial cuts of the shoulder girdle with associated edema in the supraspinatus and infraspinatus typically seen in Parsonage-Turner Syndrome.
Incorrect answers:
A total shoulder arthroplasty (TSA) would be the most appropriate treatment in which of the following arthritic patients?
Question 91
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of
Explanation
REFERENCES: Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int
2002;23:922-926.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 92
An osteoprogenitor cell is expected to commit to a bone lineage in the presence of what transcription factor?
Explanation
C/EBPa are transcription factors leading to adipocytes, MyoD promotes myoblasts, and Sox 9 corresponds to chondroblasts.
Question 93
Outcome measures should have established psychometric properties of reliability, validity, and responsiveness. Reliability refers to which of the following?
Explanation
REFERENCE: Kocher MS, Horan MP, Briggs KK, et al: Reliability, validity, and responsiveness of the American Shoulder and Elbow Surgeons subjective shoulder scale in patients with shoulder instability, rotator cuff disease, and glenohumeral arthritis. J Bone Joint Surg Am 2005;87:2006-2011.
Question 94
A 28-year-old painter has had increasing pain in his hand and forearm after sustaining a paint injection wound to the tip of his left index finger 24 hours ago. Management should consist of
Explanation
REFERENCES: Pinto MR, Turkula-Pinto LE, Cooney WP, Wood MB, Dobyns JH: High-pressure injection injuries of the hand: Review of 25 patients managed by open wound technique. J Hand Surg Am 1993;18:125-130.
Urbaniak JR, Evans JP, Bright DS: Microvascular management of ring avulsion injuries. J Hand Surg Am 1981;6:25-30.
Tsai TM, Manstein C, DuBou R, Wolff T, Kutz JE, Kleinert HE: Primary microsurgical repair of ring avulsion amputation injuries. J Hand Surg Am 1984;9:68-72.
Kay S, Werntz J, Wolff T: Ring avulsion injuries: Classification and prognosis. J Hand Surg Am 1989;14:204-213.
Schnall SB, Mirzayan R: High-pressure injection injuries to the hand, in Kozin SH (ed): Hand Clinics: Upper Extremity Trauma. Philadelphia, PA, 1999, pp 245-248.
Question 95
A 42-year-old man sustained the periprosthetic fracture shown in Figures 19a and 19b. The femoral component is well fixed. What is the next most appropriate step in management?
Explanation
REFERENCES: Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Bono JV, McCarthy JC, Thornhill TS, Bierbaum BE, Turner RH (eds): Revision Total Hip Arthroplasty. New York, NY, Springer Verlag, 1999, pp 530-592.
Question 96
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management? L Intensive physiotherapy
Explanation
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Question 97
A 77-year-old man has had increasing right knee pain for the past 3 months. A radiograph and coronal T 1 -weighted MRI scan are shown in Figures 19a and 19b. A biopsy specimen is shown in Figure 19c. What is the most likely diagnosis?
Explanation
REFERENCES: Mitchell AD, Ayoub K, Mangham DC, et al: Experience in the treatment of dedifferentiated chondrosarcoma. J Bone Joint Surg Br 2000;82:55-61.
Frassica FJ, Unni KK, Beabout JW, Sim FH: Dedifferentiated chondrosarcoma: A report of the clinicopathological features and treatment of seventy-eight cases. J Bone Joint Surg Am 1986;68:1197-1205.
Question 98
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include
Explanation
REFERENCES: Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459.
Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Skrzynski MC, Biermann JS, Montag A, Simon MA: Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1996;78:644-649.
Question 99
..One week after closed reduction of a primary anterior shoulder dislocation, a 25-year-old athlete should be counseled that
Explanation
A 65-year-old man experienced 6 years of worsening shoulder pain. Examination demonstrates stiffness and crepitus with range of motion, but full rotator cuff strength in all planes. Radiographs show advanced shoulder osteoarthritis, and an MRI scan ordered by the patient's primary care physician shows an intact rotator cuff.
Question 100
Oxidation of polyethylene after sterilization occurs most rapidly when the implant undergoes
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Wright TM: Ultra-high molecular weight polyethylene, in Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 37-46.
Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
