Orthopedic Surgery Board Review MCQs: Shoulder, Elbow, Knee, & Ligament | Part 45
Key Takeaway
This page presents Part 45 of a comprehensive, interactive multiple-choice question set for orthopedic surgeons and residents preparing for their OITE and AAOS board certification exams. It features 100 high-yield MCQs with detailed clinical explanations and literature references, designed to simulate the actual exam experience for optimal preparation.
About This Board Review Set
This is Part 45 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 45
This module focuses heavily on: Elbow, Knee, Ligament, Shoulder.
Sample Questions from This Set
Sample Question 1: During the cocking and acceleration phases of the overhand throw (pitch), there are several static and dynamic restraints to provide medial elbow support and prevent valgus instability. The dynamic structures found to be most important duri...
Sample Question 2: What is the effect on knee kinematics following placement of an anterior cruciate ligament (ACL) graft at the 12 o’clock position?...
Sample Question 3: Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain r...
Sample Question 4: Second impact syndrome (SIS) after head injury is characterized by which of the following? Review Topic...
Sample Question 5: What muscle attaches to the site shown by the arrow in Figure 2?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
During the cocking and acceleration phases of the overhand throw (pitch), there are several static and dynamic restraints to provide medial elbow support and prevent valgus instability. The dynamic structures found to be most important during these phases of the overhand throw are the flexor digitorum Review Topic
Explanation
Question 2
What is the effect on knee kinematics following placement of an anterior cruciate ligament (ACL) graft at the 12 o’clock position?
Explanation
REFERENCES: Scopp JM, Jasper LE, Belkoff SM, et al: The effect of oblique femoral tunnel placement on rotational constraint of the knee reconstructed using patellar tendon autografts. Arthroscopy 2004;20:294-299.
Carson EW, Simonian PT, Wickiewicz TL, et al: Revision anterior cruciate ligament reconstruction. Instr Course Lect 1998;47:361-368.
Question 3
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient? Review Topic

Explanation
Question 4
Second impact syndrome (SIS) after head injury is characterized by which of the following? Review Topic
Explanation
Question 5
What muscle attaches to the site shown by the arrow in Figure 2?
Explanation
REFERENCES: Williams PL, Warwick R, Dyson M, Bannister LH: Neurology, in Gray’s Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 1131-1132.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 131-132.
Question 6
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?
Explanation
inlay reconstruction.
REFERENCES: Berg EE: Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy 1995;8:95-99.
Burks RT, Schaffer JJ: A simplified approach to the tibial attachment of the posterior cruciate ligament. Clin Orthop 1990;254:216-219.
Question 7
-If a physician elects to shorten a femur by 4 cm for traumatic bone loss treatment and places an intramedullary nail for fixation, which deformity will be created in the lower extremity?
Explanation

Question 8
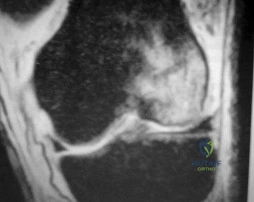
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 9
- What location is the primary source of vascular ingrowth for tendon-bone healing with rotator cuff repair?
Explanation
Question 10
A 220-lb 20-year-old man was involved in a motor vehicle accident. His work-up reveals that he has multiple long bone fractures as well as a splenic injury that is currently being managed nonsurgically. His initial blood pressure in the trauma bay was 70/30 mm Hg. After receiving 4 liters of fluid and 3 units of packed red blood cells, his blood pressure is currently 110/70, his heart rate is 100, his urine output is 90 mL/h (normal 0.5 to 1 mL/kg/h), and his core temperature is 97.9 degrees F (36.5 degrees C). At this point, the patient’s resuscitation can be described as which of the following?
Explanation
REFERENCES: Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: Endpoints of resuscitation. J Trauma 2004;57:898-912.
Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury,
a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Englehart MS, Schreiber MA: Measurement of acid-base resuscitation endpoints: Lactate, base deficit, bicarbonate or what? Curr Opin Crit Care 2006;12:569-574.
Question 11
A 32-year-old man has a closed oblique displaced fracture at the junction of the lower and middle third of the humeral shaft and a complete radial nerve palsy. Closed reduction is performed and is felt to be acceptable. Management of the radial nerve palsy should consist of
Explanation
REFERENCES: Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 237-247.
Question 12
A 78-year-old woman has a history of chronic low back pain. She denies any extremity problems. Her pain is worse in the morning, and gets better, although it does not go away, as the day goes on. An MRI scan of the lumbar spine is shown in Figure 88. She denies any acute worsening of her symptoms, although in general, her symptoms are slowly worsening. She takes nonsteroidal anti-inflammatory drugs as needed for her pain, but otherwise takes no other medications. What is the next most appropriate step in management? Review Topic

Explanation
Question 13
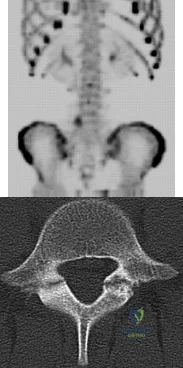
A 13-year-old girl presents with back pain for 6 months. Figures A and B are SPECT scan and CT images taken at the time of presentation. What is the most likely diagnosis? Review Topic
Explanation
patient
has
spondylolysis.
Spondylolysis is a common cause of back pain in children/adolescents. It is common in sports with repetitive hyperextension (gymnasts, weightlifters, football linemen). It is best seen on lateral and oblique radiographs, CT (best study to diagnose and delineate anatomy), and SPECT.
Saifuddin et al. reviewed the orientation of the pars fracture. They found that only 32% of defects were oriented within 15° of the 45° lateral oblique plane and would be
visible on oblique radiographs. They thus recommend CT scans for spondylolysis.
Cheung et al. reviewed spondylolysis and spondylolisthesis. They advocate pars repair for symptomatic spondylolysis and low-grade, mobile spondylolisthesis with pars defects cephalad to L5 and for those with multiple-level defects.
Figure A is a 99mTc-MDP SPECT scan showing increased uptake at the right L5 pars interarticularis. Figure B is an axial helical CT image showing bilateral spondylolysis at L5. Illustration A is a corresponding sagittal reconstruction image demonstrating right pars fracture into the right L5 superior facet. Illustration B shows the appearance of osteoblastic metastasis (green arrow). Illustration C shows the options for pars repair.
Incorrect
Question 14
Six weeks after open reduction internal fixation of a closed tibial pilon fracture, a patient has a draining wound with surrounding erythema and swelling. Radiographs show lucency around screws. What is the most appropriate treatment sequence?
Explanation
Question 15
Smoking has been associated with lower fusion rates in both cervical and lumbar fusion. Which of the following statements best describes an explanation for these findings?
Explanation
have been performed to offer an explanation of the mechanism mediating this effect. Whereas all of the above have been postulated as explanations, more recent studies have demonstrated that nicotine delivered via a transdermal patch significantly enhanced posterior spinal fusion in rabbits. Thus it appears that the effects of smoking on fracture healing are multifactorial and not yet fully understood.
Question 16
A patient has a large T11-T12 disk herniation that is causing substantial compression of the spinal cord. The patient reports walking imbalance over the past few weeks. Examination of the patient's reflexes is likely to show Review Topic
Explanation
Question 17
An 80-year-old African American woman who lives in a large city is scheduled for total hip arthroplasty to address primary osteoarthritis. Part of the presurgical protocol includes nasal swab screening to assess for methicillin-resistant Staphylococcus aureus (MRSA) colonization. Which demographic factor places this patient at highest risk for a positive result?
Explanation
Demographic factors are associated with increased risk for MRSA colonization, so it is important to identify vulnerable patients. Female gender and advanced age reduce the risk for colonization, whereas African American race increases this risk. Urban environments do not influence MRSA colonization.
Question 18
A 14-year-old patient has sustained a complete ACL tear of his right knee. Which of the following options has shown to be the most limiting factor for access to pediatric orthopaedic management in the United States?
Explanation
Access to pediatric orthopaedic management has been well investigated. Numerous Level 4 studies have shown that orthopaedic offices in urban and rural areas prefer treating patients with private insurance over patients with Medicaid.
Iobst et al. telephoned 100 urban and rural orthopaedic outpatient offices to schedule an appointment for a 10-year-old patient with a forearm fracture. They showed that 8/100 offices would schedule an appointment within 1 week to the child with Medicaid insurance, as compared to 36/100 that gave an appointment to a child with private insurance.
Pierce et al. contacted 42 orthopaedic practices to schedule an appointment for a 14-year-old patient with an ACL injury. They showed that 38/42 offices scheduled an appointment for the child within 2 weeks with private insurance. This compared to 6/42 that scheduled an appointment for a similar child with Medicaid.
Incorrect Answers:
Question 19
A polytrauma patient sustains a right bicondylar tibial plateau fracture and a right humeral shaft fracture both treated with open reduction and internal fixation. He also underwent statically locked intramedullary nailing of a left femoral shaft fracture. What is the appropriate weightbearing status?
Explanation
Tingstad et al found favorable results of immediate weightbearing on humeral shaft fractures treated with plating and full weightbearing did not have any effect on the union or malunion rates.
Brumback et al evaluated the feasibility, safety and efficacy of immediate
weightbearing after treatment of femoral shaft fractures with statically locked IM nail. All the patients went on to union and no loss of fixation occurred.
OrthoCash 2020
Question 20
Which of the following tumors have characteristic chromosomal translocations?
Explanation
REFERENCES: Sandberg AA: Cytogenetics and molecular genetics of bone and soft-tissue tumors. Am J Med Genet 2002;115:189-193.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 21
Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?
Explanation
REFERENCE: Flatow EL, Duralde XA, Nicholson GP, Pollock RG, Bigliani LU: Arthroscopic resection of the distal clavicle with a superior approach. J Shoulder Elbow Surg 1995;4:41-50.
Question 22
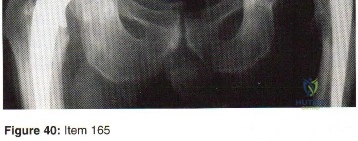
- A 75-year-old woman who has groin pain states that she had total hip arthroplasty 15 years ago. The radiograph shown in Figure 40 reveals that the left acetabular component is grossly loose. Revision of the acetabular component should include use of a
Explanation
Question 23
What is the minimum hours per day of wear that has been correlated with the effectiveness of bracing on curve progression in idiopathic scoliosis? Review Topic
Explanation
Question 24
A 61-year-old man reports right shoulder pain and loss of external rotation since having a seizure 5 months ago. MRI scans are shown in Figures 82a and 82b. What is the most appropriate treatment? Review Topic
Explanation
Question 25
5 mm of change in the atlanto-dens interval (ADI) between flexion and extension views
Explanation
With the introductions of disease-modifying antirheumatic agents (DMARDs), the incidence of RA patients undergoing cervical spine surgery has decreased significantly. Basilar invagination, atlantoaxial instability, and subaxial subluxation are the three most common manifestations of cervical disease. Multiple studies in RA patients with untreated or poorly controlled disease have led to the development of a set of measurements that identify patients who require surgical intervention and predict outcome after surgery. Additionally, progressive neurological compromise and
refractory
pain
are
indications
for
intervention.
Kim and Hilibrand reviewed management of the rheumatoid cervical spine and outline parameters for surgical intervention. These include a PADI < 14 mm, cervicomedullary angle <135 degrees, progressive neurological deficit, refractory pain, atlantoaxial impaction as determined by migration >5 mm rostral to McGregor's line, and subaxial canal diameter < 14 mm.
Boden et al. analyzed 73 patients followed for rheumatoid cervical spine disease with an average follow up of 7 years. They found that the PADI correlated with paralysis. Patients with PADI less than 10 mm had no recovery, and all patients with PADI greater than 14 mm had full recovery.
Illustration A demonstrates the measurement of the ADI and PADI. Illustration B demonstrates how to measure the cervicomedullary angle (as marked by A), which is typically determined on MRI
Incorrect
Question 26
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
REFERENCES: Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Hoppenfeld S: Orthopaedic Neurology: A Diagnostic Guide to Neurologic Levels. Philadelphia, PA, JB Lippincott, 1977, pp 7-43.
Question 27
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
REFERENCES: Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
Question 28
In the management of an open tibia fracture, what factor is considered most important in preventing deep infection?
Explanation
REFERENCES: Clifford P: Open fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 617-638.
Lee J: Efficacy of cultures in the management of open fractures. Clin Orthop 1997;339:71-75.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 29
An 18-year-old man sustained a knife injury to his midback, with the entry wound 2 cm to the left of the midline. He has been diagnosed with a hemicord transection. Neurologic examination will most likely reveal left-sided loss of
Explanation
REFERENCES: Northrup BE, Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 541-549.
Collins RD: Illustrated Manual of Neurologic Diagnosis. Philadelphia, PA, JB Lippincott, 1962, p 71.
Question 30
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and Review Topic
Explanation
Question 31
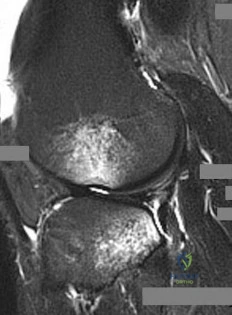
A 28-year-old man has left knee pain after a snow skiing accident. The MRI scan shown in Figure 47 reveals which of the following? Review Topic
Explanation
Question 32
Flow cytometry of tumors measures the
Explanation
Question 33
-What is the most likely mechanism of injury?
Explanation
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
Question 34
Which of the following is the primary mechanism of polyethylene wear in the hip?
Explanation
26-/28-mm heads (1-mm increase in size increased volumetric wear by 10%). The wear at the articulating surface was characterized by highly worn polished areas superiorly and less worn areas inferiorly separated by a ridge. Abrasion was very common, occurring after adhesion and plastic deformation of polyethylene fibrils, and abrasion secondary to third-body wear. Wear rates decreased with longer survival of components, indicating a “bedding in” phenomenon, arguing against oxidative and fatigue wear. Crevice corrosion occurs in fatigue cracks with low oxygen tension (under screw heads, etc). Oscillatory fretting consists of cyclical abrading of the outer surface from small movements. Fatigue and delamination is predominant in total knee arthroplasty where stresses are maximum just below the surface of the polyethylene component, causing fatigue over time with subsequent delamination. In contrast, hip wear occurs primarily at the surface of the polyethylene component.
REFERENCES: Jasty M, Goetz DD, Bragdon CR, et al: Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg Am 1997;79:349-358.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53.
Bell CJ, Walker PS, Abeysundera MR, et al: Effect of oxidation on delamination of
ultrahigh-molecular-weight polyethylene tibial components. J Arthroplasty 1998;13:280-290.
Sutula LC, Collier JP, Saum KA, et al: The Otto Aufranc Award: Impact of gamma sterilization on clinical performance of polyethylene in the hip. Clin Orthop 1995;319:28-40.
Question 35
Figure 25 shows the clinical photograph of a 48-year-old man who has had a forefoot ulcer for the past 4 months. History reveals that he has had type II diabetes mellitus for the past 10 years. Examination reveals sensory and motor neuropathy, with weak ankle dorsiflexion. The ankle cannot be passively dorsiflexed past a neutral position. Initial management should consist of
Explanation
REFERENCES: Lin SS, Lee TH, Wapner KL: Plantar forefoot ulceration with equinus deformity of the ankle in diabetic patients: The effect of tendo-Achilles lengthening and total contact casting. Orthopedics 1996;19:465-475.
Armstrong DG, Stacpoole-Shea S, Nguyen H, Harkless LB: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Question 36
A 6 year-old-boy falls from his bunk bed and suffers the injury seen in Figures A and B. Upon presentation to the emergency room he is noted to have a pink hand with brisk capillary refill, but no palpable pulses. After closed reduction in the operating room and the procedure seen in Figures C and D, he remains well perfused, pulses are still not palpable, but triphasic pulses can be heard on doppler examination. What is the most appropriate course of action? Review Topic

Explanation
Pediatric supracondylar humerus fractures presenting with vascular compromise can present a challenge for clinical decision making. If the hand lacks adequate perfusion on presentation it requires emergent treatment with closed reduction and pinning. If perfusion does not return, then surgical exploration of the antecubital fossa is required. Treatment of the "pink pulseless hand" remains controversial. If the hand is well perfused but lacks palpable pulses then it should be expeditiously reduced and pinned. If the hand remains well perfused with triphasic doppler signals, no additional intervention is required. Recommendations vary if the hand is perfused, and pulses cannot be detected on palpation or doppler.
If there is a normal neurovascular exam on presentation, but abnormal after reduction and pinning, then one must consider that the reduction may have entrapped the brachial artery. If hardware removal and fracture re-displacement does not improve pulses/perfusion of the hand, or if the fracture can not be reduced without diminishing perfusion, then open reduction is indicated to evaluate the brachial artery.
Shah et al. present their preferred algorithm for treatment of a pink pulseless hand. They note that even with good clinical perfusion there may be a vascular injury or entrapment of the brachial artery. Thus they recommend if the hand is pink with no palpable pulse, perform a doppler exam. Triphasic doppler signals allow for observation, while abnormal or non-detectable doppler signals require surgical exploration. If an AIN or median nerve injury is present, exploration is considered. A diagram of their algorithm can be seen in Illustration A.
Weller et al. present a retrospective review of 1297 supracondylar humerus fractures. They had 20 patients (1.5%) with a pink pulseless hand with good doppler signals following closed reduction and fixation. These patients were treated with close observation. One patient developed inadequate perfusion nine hours after reduction and required vascular repair. The remaining 19 patients regained palpable pulses prior to discharge or prior to the first follow-up visit. They recommend observation despite non-palpable pulses as long as other signs of perfusion (capillary refill and doppler signals) suggest the hand is well perfused.
Figures A and B are AP and lateral radiographs of a type III supracondylar humerus fracture. Figures B and C demonstrate this fracture following closed reduction and percutaneous pinning with three lateral pins. Illustration A is a flow chart of a proposed decision making algorithm for a pink pulseless hand as presented by Shah et al.
Incorrect Answers:
reduction and fixation. Answer 2- Changing the pattern of fixation would only be indicated if the current construct did not provide stable fixation of the fracture. Answer 3- Following reduction and fixation of a supracondylar humerus fracture the most appropriate dressing is rigid long arm immobilization in a splint or cast. If there is concern for edema or perfusion then a cast should be bivalved. Answer 5- Surgical exploration of the antecubital fossa would be indicated if the hand had inadequate perfusion, or if the fracture could not be reduced and fixed without causing a notable decrease in pulses or perfusion.
Question 37
Figure 41a shows the AP radiograph of a 15-year-old boy who reports lateral knee pain. Figures 41b and 41c show a radiograph of the distal femur that was obtained 5 years ago and a current CT scan. The indication for surgery in this patient would be
Explanation
REFERENCES: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1626-1659.
Simon MA, Springfield DS, et al: Common Benign Bone Tumors and Usual Treatment: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 181-205.
Question 38
An otherwise healthy 76-year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in Figures below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?

Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 39
A 62-year-old woman has loss of function of her left shoulder and dull pain. She denies any history of trauma, and there were no previous surgical procedures. MRI scans are shown in Figures 42a and 42b. The etiology of this pathology is most likely confirmed by Review Topic
Explanation
Question 40
A 70-year-old man who underwent an uncomplicated large rotator cuff repair 6 months ago is now seeking a second opinion regarding persistent pain and weakness in his shoulder. Examination reveals that his incision is well healed and unreactive. The surgical report suggests that the tendons were secured back to bone with sutures through the greater tuberosity. Figure 28 shows a radiograph that was obtained 1 week ago. What is the most likely diagnosis?
Explanation
REFERENCES: Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213.
Jost B, Pfirrmann CW, Gerber C, Switzerland Z: Clinical outcome after structural failure of rotator cuff repairs. J Bone Joint Surg Am 2000;82:304-314.
Question 41
A 40-year-old patient who has a type II odontoid fracture is placed in a halo vest for 12 weeks; however, current radiographs show no evidence of healing. The next most appropriate step in management should consist of
Explanation
REFERENCES: Montesano PX: Anterior and posterior screw and plate techniques used in the cervical spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1743-1761.
Bohler J: Anterior stabilization for acute fractures and non-unions of the dens. J Bone Joint Surg Am 1982;64:18-27.
Anderson PA, Steinmann JC: Internal fixation of the cervical spine, in Frymoyer JW (ed): The Adult Spine, Principles and Practice, ed 2. Philadelphia, PA, Lippincott Raven, 1997, pp 1119-1147.
Question 42
A 9-month-old nonambulatory girl is seen in the emergency department with a fracture of her right forearm. The mother says she fell from the changing table yesterday and continues to cry and not use her right arm. Radiographs are shown in Figure 31. Treatment should consist of which of the following? Review Topic

Explanation
efficient way to evaluate for other fractures. A MRI of the brain is not indicated unless fundoscopic examination reveals an abnormality.
Question 43
A 2-week-old infant has had diminished movement of the right upper extremity since birth. Examination reveals weakness of shoulder abduction and external rotation, elbow flexion, and forearm supination. Both pupils are equally round and responsive to light. The remainder of the examination is normal. Radiographs of the upper limb show a healing middle-third clavicle fracture. Management should consist of
Explanation
REFERENCES: Waters PM: Comparison of the natural history, the outcome of microsurgical repair, and the outcome of operative reconstruction in brachial plexus birth palsy. J Bone Joint Surg Am 1999;81:649-659.
Greenwald AG, Schute PC, Shiveley JL: Brachial plexus birth palsy: A 10-year report on the incidence and prognosis. J Pediatr Orthop 1984;4:689-692.
Question 44
A 15-year-old boy has a fracture of the proximal tibia extending from the apophysis of the tubercle up through the posterior part of the proximal tibial epiphysis and into the joint. What is the most likely mechanism of injury?
Explanation
Question 45
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?
Explanation
REFERENCES: Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Lester B, Jeong GK, Weiland AJ, Wickiewicz TL: Quadrilateral space syndrome: Diagnosis, pathology, and treatment. Am J Orthop 1999;28:718-722.
Question 46
A 20-year-old man has a symptomatic lesion of fibrous dysplasia in the femoral neck. Management should consist of
Explanation
REFERENCES: Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 197.
Enneking WF, Gearen PF: Fibrous dysplasia of the femoral neck: Treatment by cortical bone grafting. J Bone Joint Surg Am 1986;68:1415.
Question 47
Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?
Explanation
REFERENCES: Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207.
Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 48
A 48-year-old man has had pain and swelling of the hallux metatarsophalangeal joint for the past 9 months. A rocker bottom stiff-soled shoe has failed to provide relief; however, two cortisone injections have temporarily alleviated his symptoms. The radiographs shown in Figures 20a and 20b reveal diffuse arthritis of the entire hallux metatarsophalangeal joint. What is the most definitive surgical treatment?
Explanation
REFERENCES: Smith RW, Joanis TL, Maxwell PD: Great toe metatarsophalangeal joint arthrodesis: A user-friendly technique. Foot Ankle 1992;13:367-377.
Mann RA: Hallux rigidus. Instr Course Lect 1990;39:15-21.
Question 49
Figure 1 is the clinical photograph of a 64-year-old man who crashed while riding his motorcycle. An examination reveals his long-finger metacarpophalangeal (MP) joint is stuck in extension. He cannot passively or actively flex at the MP joint. A hand radiograph is seen in Figure 2. Which interposed structure is preventing reduction?

Explanation
This patient has a dorsally dislocated MP joint. In these cases, the volar plate can be displaced dorsal to the metacarpal head, preventing reduction. Although early publications described a “noose effect” of the lumbrical and flexor tendons, the primary block to reduction is the volar plate. Simple MP dislocations can be reduced closed by flexing the wrist and then gently sliding the base of the proximal phalanx over the end of the metacarpal. Longitudinal traction on the finger will only incarcerate the volar plate further and should be avoided. Patients with complex dislocations that fail closed reduction require open
reduction.
Question 50
- The familial occurrence of Legg-Calve-Perthes disease may, in some cases, be attributed to
Explanation
Question 51
A well-healed bulk proximal tibia osteoarticular allograft is removed 10 years after implantation due to arthropathy. Histologic examination of the host allograft junction site will most likely reveal
Explanation
Question 52
Figures 11a and 11b show the T 2 -weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a?
Explanation
REFERENCES: Banning CS, Thorell WE, Leibrock LG: Patient outcome after resection of lumbar juxtafacet cysts. Spine 2001;26:969-972.
Deinsberger R, Kinn E, Ungersbock K: Microsurgical treatment of juxta facet cysts of the lumbar spine. J Spinal Disord Tech 2006;19:155-160.
Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.
Question 53
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. What is the UKA survivorship for a 55- year-old patient, compared with the survivorship for total knee arthroplasty?
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress
faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 54
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What test should be performed to aid in this diagnosis?
Explanation
Question 55
A 46-year-old woman reports pain and a shortened appearance of her toe after undergoing a Keller resection arthroplasty 2 years ago for hallux rigidus. Examination reveals mild swelling and motion limited to 25 degrees at the metatarsophalangeal joint. Radiographs show large dorsal osteophytes on the first metatarsal head, 50% resection of the proximal phalanx, and complete loss of the metatarsophalangeal joint space. Which of the following is considered the most reliable procedure to improve her pain and the appearance of her toe?
Explanation
REFERENCES: Myerson MS, Schon LC, McGuigan FX, Oznur A:Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306.
Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 252-253.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 293-303.
Question 56
Figure 17 shows the radiograph of a 2-year-old girl who sustained a fracture of the femur in a fall while walking with her parents. History reveals that this is her third long bone fracture, having sustained a humerus fracture 1 year ago and a fracture of the opposite femur 9 months ago. There is no family history of any similar problem. Examination reveals distinctly blue sclerae, normal appearing teeth, and no skin lesions. What is the most likely cause of this patient’s disorder?
Explanation
REFERENCES: Kocher MS, Shapiro F: Osteogenesis imperfecta. J Am Acad Orthop Surg 1998;6:225-236.
Sillence DO, Senn A, Danks DM: Osteogenesis imperfecta: An expanding panorama of variants. Clin Orthop 1981;159:11-25.
Cole WG: Etiology and pathogenesis of heritable connective tissue diseases. J Pediatr Orthop 1993;13:392-403.
Question 57
When examining a patient with marked hyperreflexia, which of the following findings best suggests that the condition is not caused by a cerivcal spine pathology?
Explanation
REFERENCES: Montgomery DM, Brower RS: Cervical spondylotic myelopathy: Clinical syndrome and natural history. Orthop Clin North Am 1992;23:487-493.
Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K: Myelopathy hand: New clinical signs of cervical cord damage. J Bone Joint Surg Br 1987;69:215-219.
An HS, Simpson JM: Surgery of the Cervical Spine. Baltimore, MD, Williams and
Wilkins, 1994.
Question 58
Why is tendon considered an anisotropic material?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O’Keefe RJ,
Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 59
A 12-year-old boy who has had a 1-month history of right thigh pain and a limp reports worsening of the pain after a fall, and he can no longer walk or bear weight on the involved extremity. Radiographs of the pelvis reveal a slipped capital femoral epiphysis with moderate to severe displacement. While positioning the patient on the fracture table for screw fixation, partial reduction of the slip is achieved. No further reduction maneuvers are attempted, and the epiphysis is stabilized with a single cannulated screw. What complication is most likely to develop following this procedure?
Explanation
REFERENCES: Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 151-159.
Question 60
A 70-year-old female presents with right thigh ache for 6 months. Except for a history of osteoporosis, she is otherwise healthy. She has been on antiresorptive therapy for 8 years. Her radiograph is shown in Figure A. Four months later, she trips over a rug and falls, sustaining the injury shown in Figures B and C. Which of these statements is TRUE regarding surgical fixation of this fracture compared with conventional fractures?

Explanation
Subtrochanteric fractures are fractures extending from the lesser trochanter to 5cm distal to it. BP fractures are characterized by (1) focal lateral cortical thickening, (2) transverse fracture orientation, (3) medial spike and (4) lack of comminution. There is increased risk of iatrogenic fracture with IM nailing because BP fractures have thickened, brittle cortices and the mismatch between medullary diameter and increased proximal nail diameter results in iatrogenic fracture.
Weil et al. reviewed the outcome of surgically treated bisphosphonate fractures. IM nailing resulted in healing in 54% of bisphosphonate fractures with 98-99% of conventional fractures. In their study, 46% required revision procedures.
Prasarn et al. compared plate and nail treated bisphosphonate fractures with conventional fractures. They found that the bisphosphonate group had more major and minor complications (68%) than the conventional group (10%). The most common complications were intraoperative femoral shaft comminution (nail) and hardware failure (plate).
Figure A shows diffuse cortical thickening with an antero-lateral cortical ridge. Figure B shows a transverse subtrochanteric fracture extending through the middle of the cortical ridge seen previously. Note also healed fractures of the left superior and inferior rami. Figure C is a post-reduction radiograph showing the transverse fracture through the beak-shaped region of the previous insufficiency fracture. Illustration A shows a typical bisphosphonate-related fracture with transverse fracture orientation,
focal lateral cortical thickening (white arrows), medial beak (black arrow), and lack of comminution. Illustration B shows a conventional subtrochanteric fracture. Illustration C shows intraoperative iatrogenic fracture with anterolateral comminution during nailing. Illustration D shows fixation with a proximal femoral hook LCP Plate with late hardware failure at 3 months.
Incorrect Answers:
Question 61
Which of the following clinical disorders is the result of a mutation in fibroblast growth factor recepter 3 (FGFR3)?
Explanation
REFERENCES: Wagner T, Wirth J, Meyer J, et al: Autosomal sex reversal and camptomelic dysplasia are caused by mutations in and around the SRY-related gene SOX9. Cell 1994;79:1111-1120.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 111-131.
Dietz FR, Murray JC: Update on the genetic bases of disorders with orthopaedic manifestations, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 62
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Lucas DR, Nascimento AG, Sim FH: Clear cell sarcoma of soft tissues: Mayo Clinic experience with 35 cases. Am J Surg Pathol 1992;16:1197-1204.
Question 63
A 23-year-old male is involved in a motor vehicle accident and sustains a left open femur fracture, right open humeral shaft fracture, and an LC-II pelvic ring injury. Which of the following best describes the radiographic findings associated with this pelvic injury pattern using the Young-Burgess Classification system?

Explanation
Burgess et al discuss the effectiveness of a treatment protocol as determined by their pelvic injury classification and hemodynamic status. The injury classification system was based on lateral compression, anteroposterior compression, vertical shear, and combined mechanical injury types. They found that their classification-based treatment protocols reduce the morbidity and mortality related to pelvic ring disruption.
Tile discusses acute pelvic trauma and his classification system for pelvic injuries (ie. Types A, B, and C). He states that any classification system must be seen only as a general guide to treatment, and that the management of each patient requires careful, individualized decision making.
Incorrect
2:
This
describes
an
APC-II
injury
3:
This
describes
an
APC-III
injury
4:
This
describes
and
LC-I
injury
Question 64
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient’s left knee. Abnormal findings include
Explanation
REFERENCES: Ahn JH, Shim JS, Hwang CH, et al: Discoid lateral meniscus in children: Clinical manifestations and morphology. J Pediatr Orthop 2001;21:812-816.
Andrish JT: Meniscal injuries in children and adolescents: Diagnosis and management.
J Am Acad Orthop Surg 1996;4:231-237.
Question 65
An olecranon fracture-dislocation of the elbow in which the fracture line exits distal to the coronoid process is best managed by open reduction and
Explanation
REFERENCES: Jupiter JP, Kellam JF: Fractures of the forearm, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998,
pp 421-454.
Quintero J: Fracture of the forearm, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 323-337.
Jupiter JB, Leibovic SJ, Ribbans W, Wilk RM: The posterior Monteggia lesion. J Orthop Trauma 1991;5:395-402.
Question 66
The underlying cause of the neoplasm is
Explanation
The bone scan reveals multiple bone lesions, which does not rule out any of the responses. The radiographs reveal dysplastic bone with a “ground glass” appearance, suggesting fibrous dysplasia as the preferred response. Multiple myeloma typically demonstrates purely lytic, “punched out” lesions and would be highly unusual in a 23-year-old woman. Multiple hereditary exostosis would demonstrate more expansile lesions concentrated in the metaphysis. Metastatic carcinoma could have a lytic or blastic appearance but is less likely to occur in a 23-year-old woman.
McCune-Albright syndrome in polyostotic fibrous dysplasia is present in as many as 50% of patients and should be evaluated for during an endocrine consultation. Adrenal, pituitary, parathyroid, and thyroid endocrinopathies may be present. Untreated hyperthyroidism can be life threatening during a surgical procedure. There is no indication to repeat the nuclear bone scan. Although phosphate wasting and, rarely, oncogenic osteomalacia have been reported in polyostotic fibrous dysplasia, an endocrinology consultation always should be sought.
Café au lait macules are the most common extraskeletal manifestation of fibrous dysplasia, often referred to as “coast of Maine” in appearance because of their irregular borders (in comparison to the “Coast of California” with smooth borders as seen in neurofibromatosis). Multiple myeloma would not ordinarily appear with increased uptake on a bone scan unless a pathologic fracture of some duration were present. A long area of bone involvement would not appear in patients with metastatic lung adenocarcinoma.
An ALK rearrangement occurs in nonsmall-cell lung cancer. The translocation t(11;14)(q13;q32) should be recognized as a poor prognosticator in multiple myeloma. The germline alteration in EXT1 and EXT2 occurs in multiple hereditary exostosis.
All forms of fibrous dysplasia are caused by a nongerm-cell mutation that occurs during early embryogenesis. A missense mutation of the GNAS1 gene, which encodes the alpha subunit of the stimulatory G-protein-couple-receptor, Gs alpha, results in G-protein activation and the production of cyclic adenosine monophosphate affecting melanocytes, endocrine cells, and osteoprogenitor cells.
RECOMMENDED READINGS
DiCaprio MR, Enneking WF. Fibrous dysplasia. Pathophysiology, evaluation, and treatment. J Bone Joint Surg Am. 2005 Aug;87(8):1848-64. Review.View Abstract at PubMed
Parekh SG, Donthineni-Rao R, Ricchetti E, Lackman RD. Fibrous dysplasia. J Am Acad Orthop Surg. 2004 Sep-Oct;12(5):305-13. Review. PubMed PMID: 15469225. View Abstract at PubMed
Shin HJ, Kim K, Lee JJ, Song MK, Lee EY, Park SH, Kim SH, Jang MA, Kim SJ, Chung JS. The t(11;14)(q13;q32) translocation as a poor prognostic parameter for autologous stem cell transplantation in myeloma patients with extramedullary plasmacytoma. Clin Lymphoma Myeloma Leuk. 2015 Apr;15(4):227-35. doi: 10.1016/j.clml.2014.12.007. Epub 2014 Dec 12.View Abstract at PubMed
Esfahani K, Agulnik JS, Cohen V. A Systemic Review of Resistance Mechanisms and Ongoing Clinical Trials in ALK-Rearranged Non-Small Cell Lung Cancer. Front Oncol. 2014 Jul 21;4:174. doi: 10.3389/fonc.2014.00174. eCollection 2014. Review. PubMed PMID: 25101240. View Abstract at PubMed
Question 67
What do the T2-weighted, fat-saturated MRI scans shown in Figures 1 through 4 reveal?

Explanation
disruption of the ACL. The medial meniscus images show a disruption of normal meniscus morphology consistent with a bucket handle medial meniscus tear. Note the appearance on the sagittal MRI scan of what appears to be a second soft-tissue density in line with the PCL. This "double PCL" sign is highly indicative of a displaced medial meniscus tear rather than a displaced lateral meniscus tear.
Question 68
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
REFERENCES: Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 2002;23:896-901.
Question 69
Wear particles of ultra-high molecular weight polyethylene that are generated by total hip implants are predominantly of what diameter?
Explanation
REFERENCES: Campbell P, Ma S, Yeom B, McKellop H, Schmalzried TP, Amstutz HC: Isolation of predominantly submicron-sized UHMWPE wear particles from periprosthetic tissues. J Biomed Mater Res 1995;29:127-131.
Shanbhag AS, Jacobs JJ, Glant TT, Gilbert JL, Black J, Galante JO: Composition and morphology of wear debris in failed uncemented total hip replacement. J Bone Joint Surg Br 1994;76:60-67.
Maloney WJ, Smith RL, Schmalzried TP, Chiba J, Huene D, Rubash H: Isolation and characterization of wear particles generated in patients who have had failure of a hip arthroplasty without cement. J Bone Joint Surg Am 1995;77:1301-1310.
Question 70
Figures 78a and 78b show the CT scans of a 22-year-old man with back pain after falling out of a tree. Examination reveals no palpable spinal step-offs, posterior spinal pain, and normal neurologic function in the lower extremities. Normal perineal sensation and normal rectal tone are present. What is the best management? Review Topic

Explanation
Question 71
The best definitive treatment for this patient’s left knee is
Explanation
This patient now has a major fixed flexion contracture and severe varus alignment and instability. Infection of the knee joint has to be ruled out. The radiograph shows all the hallmarks of Charcot arthropathy, including disintegration and fragmentation of the joint with major deformity. Infection of the knee joint and contiguous osteomyelitis still have to be ruled out. The clinical and radiographic findings are highly suggestive of a Charcot neurogenic arthropathy associated with uncontrolled diabetes. This patient is an unsuitable candidate for total knee arthroplasty (TKA) because he is noncompliant regarding his diabetes and has had a previously infected native joint that now is associated with Charcot arthropathy. He is nonambulatory. The failure rate of TKA or knee arthrodesis is extremely high in this setting. He will best be served with observation or amputation depending upon his symptom severity.
Question 72
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Explanation
REFERENCES: Braddom RL (ed): Physical Medicine and Rehabilitation, ed 2. Philadelphia, PA, Saunders, 2000, pp 975-976.
Childs DC, Irrang JJ: The language of exercise and rehabilitation, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 329.
Question 73
Which of the following benign bone lesions can develop lung metastases?
Explanation
REFERENCES: Roberts PF, Taylor JG: Multifocal benign chondroblastomas: Report of a case. Hum Pathol 1980;11:296-298.
Bloem JL, Mulder JD: Chondroblastoma: A clinical and radiological study of 104 cases. Skeletal Radiol 1985;14:1-9.
Question 74
Figure 62 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. What is the main function of the structure delineated by the black asterisks? Review Topic
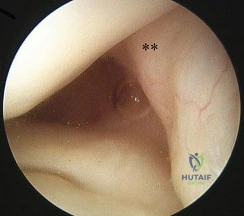
Explanation
Question 75
The mother of an otherwise healthy 1-month-old infant reports that he is not moving his left leg after falling from his high chair 2 days ago. He has a temperature of 99.5°F (37.5°C). Examination reveals that the left thigh is moderately tender to palpation. Because the infant is apprehensive, range of motion is difficult to quantify, but appears to be normal at the hips and ankles. Range of motion of the left knee is approximately 25° to 90°. A radiograph of the leg is shown in Figure 27. Management should consist of
Explanation
REFERENCES: Akbarnia BA: The role of the orthopaedic surgeon in child abuse, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1315-1334.
Black GB: Child abuse fractures, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 931-944.
Question 76
Which of the following alternatives to autogenous bone grafting functions through osteoinduction?
Explanation
Question 77
Which of the following is not a reported mode of failure for a constrained acetabular component?
Explanation
REFERENCES: Lachiewicz PF, Kelley SS: Constrained components in total hip arthroplasty. J Am Acad Orthop Surg 2002;10:233-238.
Anderson MJ, Murray WR, Skinner HB: Constrained acetabular components. J Arthroplasty 1994;9:17-23.
Fisher DA, Kiley K: Constrained acetabular cup disassembly. J Arthroplasty 1994;9:325-329.
Question 78
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of
Explanation
REFERENCES: Al-Duri ZA, Aichroth PM: Surgical aspects of patella tendonitis: Techniques and results. Am J Knee Surg 2001;14:43-50.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 218-219.
Question 79
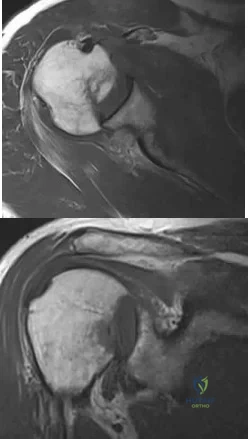
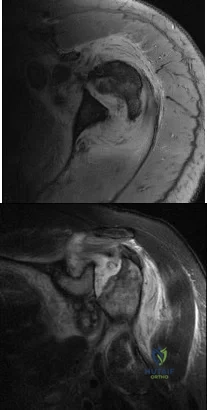
A 47-year-old landscaper presents with worsening left shoulder pain and weakness. Three years ago, he injured the left shoulder in a fall and elected for nonoperative management to minimize time off from work. Physical therapy was effective until 6 months ago when his shoulder function worsened to the point that he is now unable to work. Examination of his active range of motion reveals forward elevation 120° with pain, abduction 100°, IR at neutral to T8 and ER at neutral 5°. He has a positive ER lag sign and Hornblower's sign. Belly press and lift-off tests are normal. A recent radiograph is shown in Figures A. MRI images are shown in Figures B and C. Which of the following is the best treatment option? Review Topic
Explanation
Irreparable rotator cuff tears are marked by: (1) Superior displacement of the humeral head (AHI < 5-7mm), (2) Fatty infiltration of the rotator cuff muscles (Goutallier stage 3-4), (3) Increased duration of the tendon tear and (4) Profound external rotation weakness. These findings are predictive of poor-quality tissue and stiffness of the muscle-tendon unit, not amenable to primary repair. In this setting, a latissimus dorsi
transfer can be utilized to restore shoulder strength, function and improve pain. Relative contraindications include subscapularis deficiency, deltoid deficiency, pseudoparalysis of the shoulder and advanced glenohumeral arthritis.
Gerber et al. performed a case series analysis of 67 patients with irreparable rotator cuff tears managed with latissimus dorsi transfer. Patients with an intact subscapularis demonstrated improvement in pain, range of motion and strength postoperatively, while no improvement was noted in patients with subscapularis deficiency. The authors conclude that latissimus dorsi transfer should not be performed in the setting of poor subscapularis function.
Iannotti et al. found that better clinical results following latissimus dorsi transfer were associated with: preserved active shoulder range of motion and strength (specifically forward elevation > 90° and external rotation > 20°), synchronous firing of the transferred latissimus dorsi muscle and male gender.
Figure A is an AP radiograph of the left shoulder with superior migration of the humeral head (AHI < 5mm) and no evidence of glenohumeral arthritis. Figures B and C show a retracted posterosuperior rotator cuff tear and Goutallier stage 4 atrophy (more fat than muscle) of the supraspinatus, infraspinatus and teres minor, rendering this tear irreparable. Illustration A shows a latissimus dorsi transfer. The latissimus dorsi tendon is positioned over the top of the humeral head, covering most of the rotator cuff defect. The tendon is then secured to the subscapularis tendon edge and lesser tuberosity anteriorly, the remnant supraspinatus and infraspinatus tendons medially, and the greater tuberosity laterally.
Incorrect Answers:
Question 80
One advantage of using onlay strut allograft in femoral revision surgery is that it can
Explanation
REFERENCES: Emerson RH Jr, Malinin TI, Cuellar AD, Head WC, Peters PC: Cortical strut allografts in the reconstruction of the femur in revision total hip arthroplasty: A basic science and clinical study. Clin Orthop 1992;285:35-44.
Pak JH, Paprosky WG, Jablonsky WS, Lawrence JM: Femoral strut allografts in cementless revision total hip arthroplasty. Clin Orthop 1993;295:172-178.
Head WC, Emerson RH Jr, Malinin TI: Structural bone grafting for femoral reconstruction. Clin Orthop 1999;369:223-229.
Question 81
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
Explanation
REFERENCES: Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Fritschy D, Fasel J, Imbert JC, et al: The popliteal cyst. Knee Surg Sports Traumatol Arthrosc 2006;14:623-628.
Question 82
A 28-year-old man reports an episode of buckling and giving-way of his right knee. Figure 54a and 54b show a radiograph and sagittal MRI scan. What is the most likely diagnosis? Review Topic

Explanation
Question 83
Because of the ongoing pain and instability and the demonstration of radiographic instability when the ankle is stressed, what surgical procedure should be performed to restore stability to the ankle joint based on the CT findings?
Explanation
The fracture at the insertion of the AITFL into the fibula represents a syndesmosis injury. In some cases, a direct repair of the fracture will stabilize the syndesmosis, but in most cases this injury should most likely be reinforced by placing a screw or suture tensioning device across the syndesmosis for additional support.A Brostrom or allograft reconstruction is indicated for an ankle sprain involving the ATFL or CFL.Simply excising the fragment will leave the patient with an incompetent syndesmosis. Repairing the SPR with or without a groove deepening procedure is indicated if there is evidence of subluxated or dislocated peroneal tendons, which is not demonstrated on the CT scans. The bone has been avulsed off the fibula by the portion of the AITFL that attaches to the fibula, therefore indicating that there is a syndesmosis injury. Allograft lateral ligament reconstruction and excision of loose body/fracture fragment are incorrect procedures based on location. The deltoid is a medial structure and this fracture is lateral. The ATFL and CFL attach at the inferior margin of the fibula near the lateral process of the talus and calcaneus. A SPR avulsion would present as an avulsion off the lateral wall of the fibula, not superior and not into the syndesmotic space as shown on the CT scans.
Question 84
It is important to avoid which of the following exercises in the immediate postoperative period after humeral head replacement for an acute four-part fracture?
Explanation
REFERENCES: Hartstock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humerus fractures. Orthop Clin North Am 1998;29:467-475.
Hughes M, Neer CS: Glenohumeral joint replacment and postoperative rehabilitation. Phys Ther 1975;55:850-858.
Question 85
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management? Review Topic

Explanation
Question 86
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
REFERENCES: Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Eaton RG, Crowe JF, Parkes JC III: Anterior transposition of the ulnar nerve using a non-compressing fasciodermal sling. J Bone Joint Surg Am 1980;62:820-825.
Question 87
The peroneus tertius is a commonly used landmark for arthroscopic portal placement. What is the function of this tendon?
Explanation
REFERENCES: Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle.
Clin Anat 2006;19:611-614.
Williams PL, Bannister LH, Berry MM, et al (eds): Gray’s Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.
Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 21.
Question 88
A 42-year-old woman has a history of nontraumatic ankle swelling with tenderness over the Achilles tendon and plantar fascia. She reports that while vacationing in Connecticut 2 months ago she noted the presence of a “red bull’s eye” rash. Management should consist of
Explanation
REFERENCES: Neu HC: A perspective on therapy of Lyme infection. Ann NY Acad Sci 1988;539:314-316.
Faller J, Thompson F, Hamilton W: Foot and ankle disorders resulting from Lyme disease. Foot Ankle 1991;11:236-238.
Question 89
A 74-year-old man with ankylosing spondylitis falls off a step stool and now has a minimally displaced T10-T11 extension-type fracture. He is initially treated with percutaneous pedicle screw fixation from T8-L1 and has good pain relief. The next day, however, he experiences increased back pain and loss of strength in his lower extremities.
Explanation
Cauda equina syndrome, typically the result of severe central canal stenosis in the lower lumbar region, often is caused by a large central disk herniation. Symptoms include severe back or leg pain, perineal numbness, possible motor weakness, and initial urinary retention followed by an overflow incontinence. When bowel or bladder deficits are present, this is considered a surgical emergency because successful recovery is most likely if decompression occurs within the first 48 hours.
Ankylosing spondylitis can lead to progressive autofusion of the vertebrae and significant limitation in motion. Any sudden improvement in motion should be considered a fracture until proven otherwise. These fractures are commonly missed when using plain radiographs or even CT scan because minimal or no displacement often is noted. MR imaging can be useful to identify edema at
the fracture site. These fractures are typically very unstable and necessitate surgery to avoid displacement and potential neurologic injury.
Some fractures associated with ankylosing spondylitis can be effectively treated with percutaneous pedicle screw fixation. However, because of the highly vascular nature of some of these fractures, they pose risk for an epidural hematoma, potential neurologic deficit, and emergent decompression.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778. View Abstract at PubMed
Mathews M, Bolesta MJ. Treatment of spinal fractures in ankylosing spondylitis. Orthopedics. 2013 Sep;36(9):e1203-8. doi: 10.3928/01477447-20130821-25. PubMed PMID: 24025014.
View Abstract at PubMed
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
Question 90
A 68-year-old woman who sustained a closed distal tibia fracture 2 years ago was initially treated with an external fixator across the ankle for 12 weeks, followed by intramedullary nailing of the fibula and lag screw fixation of the tibia. She continued to report persistent pain so she was treated with a brace and a bone stimulator. She now reports pain in her ankle. Examination reveals ankle range of motion of 8 degrees of dorsiflexion to 25 degrees of plantar flexion. She is neurovascularly intact. Current radiographs are shown in Figures 9a through 9c. What is the next most appropriate step in management?
Explanation
REFERENCES: Carpenter CA, Jupiter JB: Blade plate reconstruction of metaphyseal nonunion of the tibia. Clin Orthop 1996;332:23-28.
Lonner JH, Siliski JM, Jupiter JB, Lhowe DW: Posttraumatic nonunion of the proximal tibial metaphysis. Am J Orthop 1999;28:523-528.
Stevenson S: Enhancement of fracture healing with autogenous and allogeneic bone grafts. Clin Orthop 1998;355:S239-S246.
Wiss DA, Johnson DL, Miao M: Compression plating for non-union after failed external fixation of open tibial fractures. J Bone Joint Surg Am 1992;74:1279-1285.
Question 91
Figures 1 through 3 are the weight-bearing radiograph and MRI scans of a 27-year-old man who twisted his knee coming down awkwardly from a lay-up during a basketball game. He felt a sharp stabbing pain in the posterior aspect of his knee at the time of the injury. Physical examination reveals a trace effusion, full range of motion but pain with hyperflexion >90° degrees and tenderness over the affected joint line. What is the most appropriate treatment at this time?

Explanation
root tears lead to progressive degenerative changes as a result of the altered tibiofemoral contact pressures and areas. Nonsurgical treatment including injections, physical therapy, and unloader braces are more appropriate in the older patient with pre-existing advanced degenerative changes.
Question 92
What is the preferred treatment of a symptomatic curly toe deformity in a 6-year-old child?
Explanation
REFERENCES: Hamer A, Stanley D, Smith TW: Surgery for curly toe deformity: A
double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood.
J Bone Joint Surg Br 1984;66:770-771.
Question 93
A 68-year-old man embarks on a 24-week strength training program. He trains at 80% of his single repetition maximum for both the upper and lower extremities. Which of the following changes can be anticipated?
Explanation
REFERENCES: Kirkendall DT, Garrett WE Jr: The effects of aging and training on skeletal muscle. Am J Sports Med 1998;26:598-602.
Frontera WR, Meredith CN, O’Reilly KP, Knuttgen HG, Evans WJ: Strength conditioning in older men: Skeletal muscle hypertrophy and improved function. J Appl Physiol 1988;64:1038-1044.
Question 94
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of
Explanation
REFERENCES: Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int
2002;23:922-926.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 95
Item Deleted by AAOS Question 40 - Figure 8 shows the AP radiograph of a 38-yea-old woman who has constant pain in her shoulder as the results of a motor vehicle accident. Examination reveals marked restriction in external rotation. Which of the following studies should be ordered to aid in making a diagnosis?
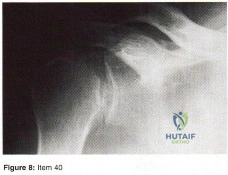
Explanation
Question 96
- A 47-year-old woman who reports mild, aching pain in her knee has no history of trauma. Examination of the knee is normal. Figure 23a shows the AP radiograph. A bone scan shows increased uptake at this site only. Figure 23b shows the CT scan, and Figure 23c shows the histology from the CT scan-guided needle biopsy. Treatment should include
Explanation
The modern technique for the removal of a giant cell tumor involves wide decortication of all the bone overlying the area of the tumor. The cavity is filled with methylmethacrylate bone cement and covered with demineralized bone matrix to stimulate the restoration of strong cortical
boundaries. The other procedures are much more invasive and not necessary to treat a low-grade neo-plastic lesion such as a giant cell tumor. Fewer complications and better functional results have been found after intralesional excision and insertion of methylmethacrylate than other techniques.
Question 97
What percent of patients initially diagnosed with classic, high-grade osteosarcoma of the extremity have visible evidence of pulmonary metastasis on CT of the chest?
Explanation
REFERENCES: Kaste SC, Pratt CB, Cain AM, et al: Metastases detected at the time of diagnosis of primary pediatric extremity osteosarcoma at diagnosis: Imaging features. Cancer 1999;86:1602-1608.
Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600-1606.
Question 98
A 69-year-old man has nonpainful weakness in the upper and lower extremities. He also notes progressive instability in his gait and increasing difficulty ambulating, as well as manipulating small objects with his hands. MRI scans of his cervical spine are shown in Figures 85a and 85b. When would be the most appropriate time to proceed with surgical treatment? Review Topic

Explanation
Question 99
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
REFERENCES: Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 100
- A 17-year old boy who sustained a closed clavicle fracture after he was ejected from an all-terrain vehicle was treated with a figure-of-8 brace 1 year ago. He now reports continuous pain at the site of the fracture and is unable to actively raise his arm above his head. A radiograph is shown in Figure 1. Management should now include
Explanation
Selection (1) would not provide adequate fixation to promote healing. (2) Electrical stimulation would not be sufficient for the above reasons. (3) Resection of the distal clavicle would not be indicate for this case because it promote further instability of the clavicle and increasing the affected forces to the clavicle.
(5) Kirschner wire fixation with bone graft, the author stated would provide fixation, but they achieved better results with plate fixation and bone graft Question 6 -
A 75-year-old woman sustains a fracture below the level of a total hip prosthesis. Radiographs demonstrate loosening of the prosthetic component. Treatment should consist of
a cast brace
a spica cast
plate fixation
allograft strut fixation
long stem revision
The key to this question lies in the radiographic evidence of loosening of the prosthetic component. The long stem revision is clearly indicated in this case because of various factors, one decreases impingement of the loose stem against the lateral femoral cortex. A non-surgical approach in the elderly patient will only increase the many risk factors such as atelectasis, pneumonia, and thromboembolic disease.[Instructional Course 44 pg. 293-303]
