OITE & ABOS Orthopedic Board Prep: Spine, Knee, & Ankle MCQs | Part 10
Key Takeaway
This page offers Part 10 of a comprehensive OITE & AAOS Orthopedic Surgery Board Review. It features 100 high-yield, verified MCQs covering Ankle, Arthroplasty, Fracture, Knee, and Revision topics. Designed for orthopedic residents and surgeons, it's essential for board certification and in-training exam preparation.
About This Board Review Set
This is Part 10 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 10
This module focuses heavily on: Ankle, Arthroplasty, Fracture, Knee, Revision.
Sample Questions from This Set
Sample Question 1: A 44-year-old farmer involved in a rollover accident on his tractor sustained an L1 burst fracture with a 20% loss of anterior vertebral body height, 30% canal compromise, and 15 degrees of kyphosis. He remains neurologically intact. The pr...
Sample Question 2: During a revision total knee arthroplasty (TKA), there is difficulty gaining exposure and a tibial tubercle osteotomy (TTO) is performed. The final components are stable and include a stemmed tibial component that bypasses the osteotomy sit...
Sample Question 3: -Work-related injuries to the lower back are most often related to which of the following risk factors?...
Sample Question 4: A 34-year-old male has persistent anterolateral ankle pain after a snowboarding injury 1 week ago and is unable to bear weight. Radiographs taken in the emergency room were negative. What is the next step in management?...
Sample Question 5: Following an episode of transient quadriplegia in contact sports, an athlete’s return to play is absolutely contraindicated when...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 44-year-old farmer involved in a rollover accident on his tractor sustained an L1 burst fracture with a 20% loss of anterior vertebral body height, 30% canal compromise, and 15 degrees of kyphosis. He remains neurologically intact. The preferred initial course of action should consist of
Explanation
REFERENCES: Hartman MB, Chrin AM, Rechtine GR: Nonoperative treatment of thoracolumbar fractures. Paraplegia 1995;33:73-76.
Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Kraemer WJ, Schemitsch EH, Lever J, McBroom RJ, McKee MD, Waddel JP: Functional outcome of thoracolumbar burst fractures without neurological deficit. J Orthop Trauma 1996;10:541-544.
Question 2
During a revision total knee arthroplasty (TKA), there is difficulty gaining exposure and a tibial tubercle osteotomy (TTO) is performed. The final components are stable and include a stemmed tibial component that bypasses the osteotomy site. The tibial tubercle is reattached to the osteotomy site with multiple cerclage wires. Following closure of the arthrotomy, the knee is flexed to 90 degrees, and there is no observed displacement of the TTO. What is the best next step in postsurgical rehabilitation?
Explanation
TTO is a recognized technique for improving exposure when performing TKA in a stiff knee. TTO has been reported to enhance surgical exposure and not adversely affect outcomes after TKA, but there is a 5% complication rate. The postsurgical routine following TTO
includes full weight-bearing activity and range of motion as tolerated. Caution should be exercised when manipulation is performed to improve knee flexion following a TTO.
Question 3
- Work-related injuries to the lower back are most often related to which of the following risk factors?
Explanation
Question 4
A 34-year-old male has persistent anterolateral ankle pain after a snowboarding injury 1 week ago and is unable to bear weight. Radiographs taken in the emergency room were negative. What is the next step in management?

Explanation
The reference by Vlahovich et al is a case report of a talus fracture in a snowboarder and argues the importance of CT scans in evaluating these injuries as radiographs may fail to show the injury and amount of displacement and comminution of the fracture.
The reference by Tucker et al is a review of the literature which emphasized the importance of early diagnosis to avoid long term complications. They recommend short leg casting for nondisplaced fractures and surgery for displaced or comminuted fractures.

Question 5
Following an episode of transient quadriplegia in contact sports, an athlete’s return to play is absolutely contraindicated when
Explanation
REFERENCES: Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146.
Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Bailes JE, Hadley MN, Quigley MR, Sonntag VK, Cerullo LJ: Management of athletic injuries of the cervical spine and spinal cord. Neurosurgery 1991;29:491-497.
Question 6
A 52-year-old woman with diabetes mellitus has had a plantar foot ulcer under the second metatarsal head for the past week. The patient had a similar ulcer 2 months ago, and total contact casting resulted in healing. Examination reveals no signs of infection. What procedure will best prevent recurrence of the ulcer?
Explanation
REFERENCES: Armstrong DG, Stacpoole-Shea S, Nguyen H, et al: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Meuller MJ, Sinacore DR, Hastings MK, et al: Effect of Achilles tendon lengthening on neuropathic plantar ulcers: A randomized clinical trial. J Bone Joint Surg Am
2003;85:1436-1445.
Question 7
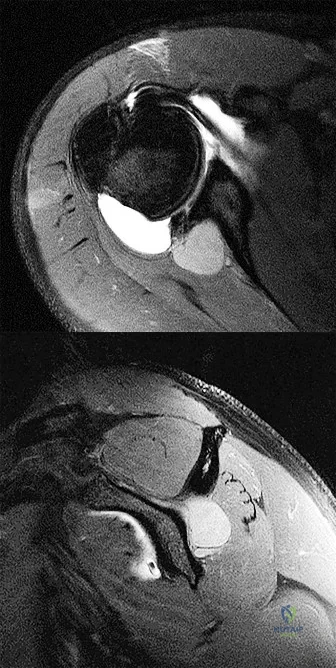
Based on the injury shown on the axial MRI scan of the shoulder in Figure 1, what other pathology should be closely examined for during surgery?
Explanation
specific to this pathology.
Question 8
What is the most important factor regarding the risk of recurrent instability in a patient with an acute anterior dislocation of the shoulder?
Explanation
REFERENCES: Hovelius L: The natural history of primary anterior dislocation of the shoulder in the young. J Orthop Sci 1999;4:307-317.
Simonet WT, Cofield RH: Prognosis in anterior shoulder dislocation. Am J Sports Med 1984;12:19-24.
Question 9
Figures 29a and 29b show the AP radiograph and CT scan of a 70-year-old man who has left thigh pain. Serum protein electrophoresis shows a monoclonal gammopathy. Additional radiographs of the femur show other lesions. Management should consist of
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 364.
Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 10
A 78-year-old patient undergoing revision total knee arthroplasty has bone loss throughout the knee at the time of revision. A distal femoral augment is used to restore the joint line. One month after surgery, the patient reports pain and is unable to ambulate. A lateral radiograph is shown in Figure 34. What is the most likely etiology of this problem?
Explanation
REFERENCES: Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
McAuley J, Engh GA, Ammeen DJ: Treatment of the unstable total knee arthroplasty. Inst Course Lect 2004;53:237-241.
Naudie DD, Rorabeck CH: Managing instability in total knee arthroplasty with constrained and linked implants. Instr Course Lect 2004;53:207-215.
Question 11
-If a physician elects to shorten a femur by 4 cm for traumatic bone loss treatment and places an intramedullary nail for fixation, which deformity will be created in the lower extremity?
Explanation

Question 12
Figure 100 is the MRI scan of a 52-year-old runner who has right knee pain that has been occurring 10 minutes into her run for 2 months. On examination, she has tenderness over the lateral epicondyle. Her Ober test result is positive. What is the most appropriate initial treatment? Review Topic
Explanation
Question 13
A patient is seen in the emergency department after a motor vehicle accident. He reports right hip pain and chest pain. Initial hypotension has responded to a fluid bolus. Radiographs reveal a posterior hip dislocation with a small posterior acetabular wall fracture. You are called at home and informed of the findings. What is the next most appropriate step in management? Review Topic
Explanation
Question 14
What is the main biologic effect of aggrecan in cartilage? Review Topic
Explanation
Aggrecan is the predominant proteoglycan in cartilage. It contains a large number of negatively charged sequences that attract water called sulfated glycosaminoglycan (GAG) chains. Its the N-terminal globular domain of aggrecan that binds hyaluronan to form huge aggregates. Together with its chondroitin sulfate chains, they help to create a hydrophilic viscous gel that decreases the coefficient of friction as well as to help absorb compressive loads.
Ulrich-Vinthe et al. reviewed the biology of articular cartilage. They report that matrix metalloproteinases and aggrecanases play a major role in aggrecan degradation and their production is upregulated by mediators associated with joint inflammation and overloading.
Illustration A shows a depiction of the function of aggrecan in articular cartilage. In the relaxed state, the aggregates draw water into cartilage. With compressive loads, the water is displaced to cushion the load. Upon removal of the load, the water content is restored.
Incorrect Answers:
Question 15
The orthosis shown in Figure 47 is commonly used for
Explanation
REFERENCE: Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, p 1185.
Question 16
Which of the following changes occur in articular cartilage with age?
Explanation
Question 17
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be
Explanation
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Martin SD, Warren RF, Martin TL, Kennedy K, O’Brien SJ, Wickiewicz TL: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 18
What percent of patients initially diagnosed with classic, high-grade osteosarcoma of the extremity have visible evidence of pulmonary metastasis on CT of the chest?
Explanation
REFERENCES: Kaste SC, Pratt CB, Cain AM, et al: Metastases detected at the time of diagnosis of primary pediatric extremity osteosarcoma at diagnosis: Imaging features. Cancer 1999;86:1602-1608.
Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600-1606.
Question 19
Ulnohumeral distraction interposition arthroplasty is considered the most appropriate treatment for which of the following patients?
Explanation
REFERENCES: Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Mansat P: Surgical treatment of the rheumatoid elbow. Joint Bone Spine 2001;68:198-210.
Question 20
Which of the following aids in correction of patellar tracking after total knee arthroplasty (TKA)?
Explanation
REFERENCES: Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 1245-1258.
Merkow RL, Soudry M, Insall JN: Patellar dislocation following total knee replacement. J Bone Joint Surg Am 1985;67:1321-1327.
Question 21
A 22-year-old professional baseball catcher has posterior shoulder pain and severe external rotation weakness with the arm in adduction. Radiographs are normal. MRI scans are shown in Figures 15a through 15c. Management should consist of Review Topic

Explanation
Question 22
In patients without spondylolisthesis or scoliosis undergoing laminectomy for lumbar spinal stenosis, spinal fusion is generally recommended if Review Topic
Explanation
Question 23
Figure 19 is the clinical photograph of a 54-year-old man who underwent a total ankle replacement (TAR). Three weeks after surgery he has increasing pain and a deep wound as seen in the photograph. What is the best next step?

Explanation
The patient is 3 weeks out from TAR. The wound is erythematous, and the tendon is visible. At 3 weeks this is an acute wound breakdown. The preferred treatment is a return to the operating room, an exchange of the polyethylene because the wound appears deep enough to go down to the joint, and a flap for coverage. Removal of the total ankle and placement of an antibiotic spacer should be considered in the settings of subacute (6 weeks postop) or chronic infection following TAR. A below-the-knee amputation may be considered with a failed salvage or a chronically infected TAR. Conversion to a fusion may be considered in situations in which the wound bed is not infected. In this case, there is concern for ongoing active infection, and an intercalary allograft is not appropriate.
RECOMMENDED READINGS
Cho EH, Garcia R, Pien I, Thomas S, Levin LS, Hollenbeck ST. An algorithmic approach for managing orthopaedic surgical wounds of the foot and ankle. Clin Orthop Relat Res. 2014 Jun;472(6):1921-9. doi: 10.1007/s11999-014-3536-7. Epub 2014 Feb 28. PubMed PMID:
Question 24
What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?
Explanation
REFERENCES: Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
Steinmann SP, Linsheid RL: Pisotriquetral loose bodies. J Hand Surg 1997;22:918-921.
related link ortho mcqs bank
Question 25
Which of the following is considered the lowest level that a standard thoracolumbosacral orthosis (TLSO) can immobilize?
Explanation
REFERENCES: White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 475-509.
Norton PL, Brown T: The immobilizing efficiency of back braces. J Bone Joint Surg Am 1957;39:111-139.
Question 26
Figures 43a and 43b show the T 1 - and T 2 -weighted MRI scans of a 78-year-old woman who reports the sudden atraumatic onset of well-localized medial knee pain. Pain is worse at night and also occurs with weight-bearing activity. What is the most likely diagnosis?
Explanation
REFERENCES: Soucacos PN, Berris AE, Xenakis TH, et al: Knee osteonecrosis: Distinguishing features in differential diagnosis, in Urbanik JR, Jones JD (eds): Osteonecrosis. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-424.
Ecker ML, Lotke PA: Osteonecrosis of the medial part of the tibial plateau. J Bone Joint Surg Am 1995;77:596-601.
Question 27
Figure 62a and Figure 62b
Explanation
Figure 58 reveals a posttraumatic valgus deformity. Correction of valgus with lateral soft-tissue release places tension on the peroneal nerve, resulting in an increased risk for nerve palsy. Figures 59a (lateral view) and 59b (Merchant view) illustrate juvenile rheumatoid arthritis with tibiofibular fusion and lateral patellar dislocation. Chronic patellar dislocation is associated with contracture of the lateral retinacular soft tissues and increased risk for patellar subluxation or dislocation after TKA. Extensor mechanism realignment, possibly including tibial tubercle osteotomy and/or proximal soft-tissue realignment, may be required during TKA to centralize the extensor mechanism. Figures 60a (anteroposterior [AP] view) and 60b (lateral view) reveal a fused knee in full extension.
TKA after fusion is associated with multiple complications including skin necrosis, infection, and instability. The skin is contracted because of limited knee motion and has multiple scars (Figure 60c). Mobilization of the skin during and after knee arthroplasty can place excess tension on the soft tissues, resulting in skin necrosis and infection. Treatment consisting of prompt debridement and soft-tissue coverage, usually with medial gastrocnemius muscle transposition, is required. Figure 61 shows a knee with prior tibial tubercle fixation and marked patella infera. Shortening of the patellar ligament is associated with restricted knee motion. This may necessitate more extensile exposure using tibial tubercle osteotomy or rectus snip during TKA to obtain adequate surgical exposure. The inferior position of the patella can cause impingement between the patellar component and tibial insert, resulting in anterior knee pain. Restoring a more normal position of the patella may necessitate distal positioning of the femoral component as well as tibial tubercle osteotomy with proximal recession of the osteotomized tibial tubercle. Figures 62a (AP view of the distal femur) and 62b (AP view of the proximal femur) show a posttraumatic deformity with a large retained intramedullary rod. There is a varus distal femoral deformity that is not severe enough to necessitate extra-articular corrective osteotomy. However, intramedullary hardware precludes use of conventional intramedullary instrumentation, so computer navigation or patient-specific cutting guides will be necessary to orient the bone cuts and avoid implant malalignment.
Question 28
Figure 18 is the radiograph of a 52-year-old woman who has leg length inequality and chronic activity-related buttock discomfort. This has been a life-long problem, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step vs. oblique cut, or strut grafts.
Question 29
A clinical trial is underway for patients with wrist extensor tendinitis. One group of 100 patients are treated with short arm casting. Another group of 100 patients are treated with physical therapy. During analysis of the results, it becomes apparent that 30 patients in the physical therapy group did not complete the full course of physical therapy. Despite not completing a full course of physical therapy, these 30 patients were included in the physical therapy group for analysis. This analysis is an example of which of the following?
Explanation
The intent-to-treat approach aims to keep similar groups similar by not allowing for patient selection based on post-randomization outcomes (including failure to comply with the protocol). This type of analysis ensures the power of randomization so that important unknown variables that impact outcome are likely to be dispersed equally in each comparison group. Conversely, a per-protocol comparison in a clinical trial excludes patients who were not compliant with the protocol guidelines.
Berger et al., in a Level 5 review, discuss many of the principles beyond randomization that are critical for preserving the comparability of the different groups. They report that masking, allocation concealment, restrictions on the randomization, adjustment for prognostic variables, and the intent-to-treat approach to data analysis are important features of designing a good clinical trial.
Incorrect Answers:
Question 30
A 45-year-old man has persistent hindfoot pain that is aggravated by weight-bearing activities. History reveals that he sustained a calcaneus fracture 2 years ago, and he underwent a subtalar fusion 1 year ago. Examination reveals tenderness in the sinus tarsi and across the transverse tarsal joint. A plain radiograph and a CT scan are shown in Figures 24a and 24b. A technetium Tc 99m bone scan reveals uptake at the subtalar joint and at the transverse tarsal joints. Management should now consist of
Explanation
REFERENCES: Graves SC, Mann RA, Graves KO: Triple arthrodesis in older adults: Results after long-term follow-up. J Bone Joint Surg Am 1993;75:355-362.
Haddad SL, Myerson MS, Pell RF IV, Schon LC: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Sangeorzan BJ, Smith D, Veith R, Hansen ST Jr: Triple arthrodesis using internal fixation in treatment of adult foot disorders. Clin Orthop 1993;294:299-307.
Sangeorzan BJ: Salvage procedures for calcaneus fractures. Instr Course Lect 1997;46:339-346.
Wapner KL: Triple arthrodesis in adults. J Am Acad Orthop Surg 1998;6:188-196.
Question 31
A 36-year-old nurse has had redness, pain, and small vesicles on the pulp of her middle finger for the past 3 days. Management should consist of
Explanation
REFERENCES: Fowler JR: Viral Infections. Hand Clin 1989;5:613-627.
Jebsen PL: Infections of the fingertip: Paronychias and felons. Hand Clin 1998;14:547-555.
Question 32
A 58-year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 33
What gene is expressed the earliest during the differentiation of a chondrocyte during endochondral ossification?
Explanation
REFERENCES: Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Sandell LJ: Genes and gene expression. Clin Orthop 2000;379:S9-S16.
Question 34
A 35-year-old construction worker has developed isolated lateral compartment arthritis. He has lost 50 pounds, now has a body mass index of 30, and still has pain that limits his activities of daily living and work despite receiving a 4-month course of nonsteroidal anti-inflammatory medications and 2 intra-articular cortisone injections. His range of motion is 5 to 110 degrees, and his mechanical axis is 18 degrees of valgus. What is the most appropriate surgical treatment for this patient?
Explanation
Knee arthritis in a young laborer is challenging to address. A surgeon could perform an arthroplasty, but there is concern for early failure and the subsequent need for multiple revisions during this patient’s lifespan. Indications for distal femoral varus osteotomy include at least a 12- to 15-degree valgus mechanical axis and range of motion of at least 15 to 90 degrees. Contraindications for this procedure include inflammatory arthritis and restricted knee motion.
RESPONSES FOR QUESTIONS 138 THROUGH 141
Acute periprosthetic infection
Chronic periprosthetic infection
Joint dislocation
Periprosthetic fracture
Pseudotumor
Femoral nerve palsy
Sciatic nerve palsy
Aseptic prosthetic loosening
Select the total hip arthroplasty (THA) complication listed above that most commonly is associated with the clinical scenario described below.
Question 35
A 27-year-old man has neck pain after being involved in a motor vehicle accident. A lateral cervical radiograph is shown in Figure 21. What would be the most common neurologic finding?
Explanation
REFERENCES: Levine AM: Traumatic spondylolisthesis of the axis (Hangman’s fracture), in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 287-288.
Francis WR, Fielding JW, Hawkins RJ, Pepin J, Hensinger R: Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br 1981;63:313-318.
Question 36
A 3-year-old child sustains a T2/T3 fracture-dislocation with complete paraplegia secondary to a car accident in which the child was an unrestrained passenger. What is the likelihood that this child will develop subsequent spinal deformity in the future?
Explanation
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Dearolf WW III, Betz RR. Vogl LC, et al: Scoliosis in pediatric spinal cord-injured patients. J Pediatr Orthop 1990;10:214-218.
Mehta S, Betz RR. Mulcahey MJ, et al: Effect of bracing on paralytic scoliosis secondary to spinal cord injury. J Spinal Cord Med 2004;27:S88-S92.
Question 37
-Four months after injury, the tibia is showing evidence of slow healing on radiographs. What is the optimal treatment for this potential nonunion?
Explanation
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
Question 38
Accurate evaluation of the upper portion of the subscapularis muscle is best accomplished with active internal rotation
Explanation
REFERENCES: Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ: Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 1998;26:210-220.
Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 39
Figure 29 shows the radiograph of a 25-year-old woman who has had a 3-month history of ankle pain after sustaining an inversion injury to the ankle. She reports occasional catching, but no sense of instability. Examination reveals ligament stability. Management should consist of
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Pettine KA, Morrey BF: Osteochondral fractures of the talus: A long-term follow-up. J Bone Joint Surg Br 1987;69:89-92.
Question 40
Genetic mutations that may result in the cervical abnormalities noted in the figures generally affect the
Explanation
The figures are characteristic of a child with Klippel-Feil syndrome (congenital cervical spine abnormalities) in association with congenital scoliosis in the upper thoracic spine and a right-sided Sprengel deformity (congenital elevation of the scapula). Sprengel deformity occurs in as many as 30% of children with Klippel-Feil syndrome. Other congenital conditions that are commonly associated with Klippel-Feil, and that should be screened for, include deafness in 30%, genitourinary abnormalities in 25% to 35%, and cardiovascular abnormalities in 4% to 29% of children with Klippel-Feil syndrome.
In Sprengel deformity, there is usually a tether called the omovertebral connection between the abnormally elevated scapula and the spinous processes in the upper thoracic region. This tether is most commonly bony but also may be cartilaginous or fibrous. Although there also may be abnormalities in the ribs, clavicle, or humerus, they are morphologic abnormalities only, not tethers.
Patients with Klippel-Feil syndrome should be discouraged from participating in contact or collision sports if they have a massive fusion of the cervical spine, any involvement of C2, or limited cervical motion. Fusions at 1 or 2 interspaces below C3 and normal cervical motion do not preclude participation in activities. A Sprengel deformity may limit abduction of the shoulder and normal racquet or throwing mechanics, but, in the absence of pain, is not a contraindication to attempted participation.
Klippel-Feil syndrome affects a heterogenous cohort of patients and different inheritance patterns have been seen, including autosomal-dominant and autosomal-recessive types, with varying levels of penetrance. The first human Klippel-Feil syndrome locus was identified on chromosome 8 and is called SGM1. Other candidates for mutations in Klippel-Feil include PAX genes and Notch pathway genes. In general, the involved genes help regulate the formation and segmentation of the vertebrae.
Between days 20 and 30 following conception, the paraxial mesoderm subdivides into segments called somites. As they mature, somites develop into 3 layers called the sclerotome, myotome, and dermatome. The sclerotome undergoes a process of resegmentation during which the caudal section from 1 somite joins with the rostral section of the immediately caudal somite to form the vertebral bodies. It is during the processes of segmentation and resegmentation that the abnormalities leading to Klippel-Feil syndrome occur. Gastrulation refers to the phase early in embryonic development when the single-layered blastula is reorganized into a trilaminar structure with 3 germ layers: the ectoderm, mesoderm, and endoderm. Neurulation refers to the process by which the notochord induces formation of the neural tube from the neural plate, forming the brain and spinal cord.

Question 41
What factor is associated with the highest risk for in-hospital complications for patients undergoing a lumbar fusion for degenerative spondylolisthesis? Review Topic
Explanation
Question 42
Treatment of a cruciate-retaining total knee that is unstable in flexion is best accomplished by
Explanation
REFERENCE: Pagnano MW, Hanssen AD, Lewallen DG, Stuart MJ: Flexion instability after primary posterior cruciate-retaining total knee arthroplasty. Clin Orthop 1998;356:39-46.
Question 43
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 44
Pain associated with a proximal medial tibial osteochondroma in a 10-year-old patient is most commonly the result of
Explanation
REFERENCES: Borges AM, Huvos AG, Smith J: Bursa formation and synovial chondrometaplasia associated with osteochondromas. Am J Clin Pathol 1981;75:648-653.
Hudson TM, Springfield DS, Spanier SS, Enneking WF, Hamlin DJ: Benign exostoses and exostotic chondrosarcomas: Evaluation of cartilage thickness by CT. Radiology 1984;152:595-599.
Question 45
A 16-year-old boy has had knee pain for the past 6 months, and activity restrictions have not provided relief. An MRI scan reveals a stable 1.5 cm by 1 cm osteochondritis dissecans on the weight-bearing surface of the lateral femoral condyle. What is the best course of treatment? Review Topic
Explanation
Question 46
A 51-year-old woman with no preoperative neurologic deficit is undergoing elective anterior cervical diskectomy and fusion (ACDF) with plating and fusion for a C5-6 disk herniation with right-sided neck pain. Thirty minutes into the surgery the neurophysiologic monitoring shows a rapid drop and then loss of amplitude in the right cortical somatosensory-evoked potential waveform. All other waveforms remained normal and unchanged, including right-sided cervical (subcortical) and peripheral (Erb’s point), and those from the left-sided upper extremity and both lower extremities. What is the most likely cause of the change?
Explanation
REFERENCES: Drummond JC, Englander RN, Gallo CJ: Cerebral ischemia as an apparent complication of anterior cervical discectomy in a patient with an incomplete circle of Willis. Anesth Analg 2006;102:896-899.
Yeh YC, Sun WZ, Lin CP, et al: Prolonged retraction on the normal common carotid artery induced lethal stroke after cervical spine surgery. Spine 2004;29:E431-E434.
Question 47
A 48-year-old man reports localized plantar forefoot pain. Examination reveals a discrete callus (intractable plantar keratosis) with well-localized tenderness beneath the second metatarsal head. The callus most likely lies beneath what structure?
Explanation
REFERENCES: Coughlin MJ, Mann RA: Keratotic disorders of the plantar skin, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby-Year Book, 1993, pp 413-465.
Cracchiolo A: Surgical procedures of the lateral metatarsals, in Jahss MH (ed): Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1269-1283.
Question 48
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function? Review Topic
Explanation
Question 49
A 28-year-old man has had a 2-week history of right posterior leg pain, with numbness and tingling in the same distribution. He denies any problems with bowel or bladder function. Examination shows intact motor strength in his bilateral lower extremities, with numbness to light touch in the lateral border of his right foot. Over the past 2 weeks, his leg pain has improved significantly. MRI scans are shown in Figures 57a and 57b. What is the most appropriate course of management? Review Topic

Explanation
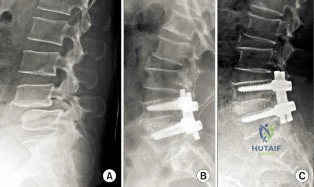
(SBQ12SP.9) A 62-year-old male underwent posterior spinal instrumented fusion for degenerative lumbar spondylolithesis one year ago. He presents to office complaining of persistent lower back pain. The pain initially improved but over the last 6 months he has had recurring pain at the site of the surgery primarily with activity. He denies back pain at rest or night pain. Physical examination reveals a well healed wound and no physical abnormalities. He has no tenderness to palpation to the thoracic or lumbar spine. He has no neurological deficits. His laboratory results show an erythrocyte sedimentation rate (ESR) = 8 mm/h and C-reactive protein (CRP) = 3 mg/L at the last visit which are both within normal limits. Figure A shows a series of radiographs from his pre-operative, 3 month post-operative and 1 year post-operative clinic visits, respectively. Which of the following investigations would best confirm the suspected underlying diagnosis? Review Topic
MRI of lumbar spine
Repeat ESR/CRP and whole body bone scan
CT of lumbar spine
Dynamic flexion/extension plain film radiographs
Dynamic lateral bending plain film radiographs
This patient has clinical and radiographic features of failed spinal arthrodesis. CT scan have been shown to be the most relable method for assessing spinal fusion postoperatively.
Reported rates of nonunion following posterior spinal fusion range from 0-70%. Rates are variable due to the various operative techniques, underlying diagnoses as well as asymptomatic patients. Non-union may lead to changes in alignment, spinal instability and potential neurological injury. Static radiographs have long been used as a practical method of fusion assessment, but these tend to significantly overestimate the presence of a solid fusion. Lack of movement at a fused segment, on dynamic views, does not confirm fusion. CT offers excellent bony resolution and are less affected by metal artifact compared to MRI.
Patel et al. showed that tobacco use, malnutrition, oral anti-inflammatory use, multilevel fusion, prior spine surgery, and sagittal imbalance are all risk factors for spinal nonunion.
Mok et al. looked at erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels after spinal surgery and compared their usefulness as predictors of infectious complications in the early postoperative period. They found that CRP is more applicable, predictable, and responsive in the early postoperative period compared with ESR. Using a second rise or failure to decrease as expected for CRP is sensitive for infection.
Shelby et al. reviewed the radiological assessment of spinal fusion. They comment that fine-cut imaging, multiplanar reconstruction, and metal artifact reduction have increased the ability to assess fusion on CT.
Figure A shows a series of lateral radiographs of the lumbar spine with posterior spinal instrumentation. Illustration A shows a lateral CT scan image of multi-level pseudoarthrosis after posterior spinal instrumented fusion. Illustration B shows an
intra-operative
view
of
spinal
pseudoarthrosis
(white
arrow).
Incorrect
(SBQ12SP.19) A 41-year-old male presents with acute onset of low back pain that started when he was trying to lift a heavy box while helping his brother move apartments two days ago. The pain has been severe enough to cause him to miss work yesterday. He has no neurologic deficits. What are the chances he will return to work within 6 weeks? Review Topic
1 80 to 90%
2 70 to 80%
3 60 to 70%
4 50 to 60%
5 40 to 50%
Most adults (up to 80%) will experience an episode of low back pain in their lifetime. In those whose pain is severe enough to cause them to miss work, 60 to 70% will return by 6 weeks, and 80 to 90% will return by 12 weeks.
Low back pain is common in adults. Most patients experience resolution of symptoms quickly and have no lasting loss of function. However, 5 to 10% develop chronic pain. Recurrence of pain is common, and is part of the natural history, occurring in 20 to 72% of patients. After 12 weeks, return to work rates are slow.
Shen et al. review the nonoperative management of acute and chronic low back pain. The authors note that none of the available interventions has been proven by high quality large randomized controlled trials. The authors believe that low dose oral
steroids are safe in the short term and that injection therapy should not be used without a reasonable presumptive diagnosis.
Madigan et al. review the management of lumbar degenerative disease. The authors emphasize that the majority of patients improve within 6 weeks with or without treatment. For patients that do not, the authors do not recommend epidural injection, as there are no good studies to support their use in the treatment of discogenic back pain. When surgical treatment is indicated they state that arthrodesis is the gold standard, although the long term results of total disk arthroplasty are being elucidated.
Illustration A shows a table of available non-operative treatment modalities for back pain. Illustration B shows a list of possible diagnoses associated with acute low back pain, with those associated with neurogenic pain italicized. Illustration C shows a list of 'red flag' symptoms indicating serious/emergent causes of low back pain.
Incorrect
2:
Longer
to than
90%
Question 50
Which of the following tumors have characteristic chromosomal translocations?
Explanation
REFERENCES: Sandberg AA: Cytogenetics and molecular genetics of bone and soft-tissue tumors. Am J Med Genet 2002;115:189-193.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 51
A 13-year-old baseball pitcher presents with worsening medial-sided elbow pain. He pitches 7 months out of the year, throws 85 pitches per game and plays in two games per week. His fastball speed is approximately 75mph. He regularly plays outfield once he has been relieved of pitching. Which of the following is most likely contributing to his elbow pain? Review Topic
Explanation
Little League elbow is a medial-sided overuse injury that occurs in the skeletally immature athlete. During execution of the baseball pitch, tremendous valgus and extension stresses occur at the elbow. Repetitive microtrauma can ultimately injure the medial epicondyle apophysis, ulnar collateral ligament or the flexor-pronator muscle mass. Limiting the number of pitches and innings played per game, as well as the number of months of competitive pitching per year, has been recommended to prevent these overuse injuries in the young athlete.
Olsen et al performed a case control study to determine risk factors associated with the development of shoulder and elbow injuries in adolescent baseball pitchers. Greater than 8 months of competitive pitching per year, more than 80 pitches per game and a fastball speed of greater than 85mph were all associated with increased risk of injury. Continued pitching despite arm fatigue and pain, being a starting pitcher, greater number of warm-up pitches, participating in showcases and regular use of NSAIDs were also associated with injury. The type of pitch (fastball, changeups and breaking balls) and continued play in a different position once being relieved was not associated with increased risk of injury.
Andrews et al authored a review article on ulnar collateral ligament injuries in throwing athletes. According to the USA Baseball Medical/Safety Advisory Committee, young baseball pitchers should avoid breaking pitches, such as curveballs and sliders, and avoid year-round baseball. A minimum of 3 months of complete rest from pitching per year is vital. Youth pitching coaches should be educated to ensure proper pitching mechanics are being reinforced.
Illustration A is a table depicting the recommended maximum number of pitches by age group.
Incorrect Answers:
Question 52
A corset-type brace may help reduce symptoms during an episode of acute low back pain as the result of
Explanation
REFERENCES: Nachemson A, Morris JM: In vivo measurements of intradiscal pressure: Discometry, a method for determination of pressure in the low lumbar disc. J Bone Joint Surg Am 1964;46:1077-1092.
Axelsson P, Johnsson R, Stromqvist B: Effect of lumbar orthosis on intervertebral mobility: A roentgen stereophotogrammetric analysis. Spine 1992;17:678-681.
Question 53
A 35-year-old woman undergoes an L4-5 anterior fusion via a left retroperitoneal approach. Postoperative examination reveals that her right foot is cool and pale. Her neurologic examination is normal, and her pedal pulses are asymmetric. What is the most likely reason for the right foot finding?
Explanation
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, p1550.
Benzel EC (ed): Spine Surgery Techniques, Complication Avoidance and Management. New York, NY, Churchill Livingstone, 1999, p 190.
Question 54
A 47-year-old man with Charcot-Marie-Tooth (CMT) disease was treated with a fifth metatarsal head resection for a symptomatic bunionette 2 years ago. What is the most likely complication seen at this time?
Explanation
REFERENCES: Kitaoka HB, Holiday AD Jr: Metatarsal head resection for bunionette: Long-term followup. Foot Ankle 1991;11:345-349.
Coughlin MJ, Mann RA, Saltzman CL: Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 1312-1315.
Question 55
What significant structure is most at risk during a posterior approach of the Achilles tendon near its musculotendinous junction?
Explanation
REFERENCES: Webb J, Moorjani N, Radford M: Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-477.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Question 56
The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced
Explanation
REFERENCES: Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U: Operative versus nonoperative treatment of Achilles tendon rupture: A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-799.
Nistor L: Surgical and non-surgical treatment of Achilles tendon rupture. J Bone Joint Surg Am 1981;63:394-399.
Question 57
The most appropriate next surgical procedure is
Explanation
This patient’s arthritis likely has progressed to the lateral compartment. The location and degree of local pain and tenderness are the most important physical findings. History and physical findings indicate arthritis progression to the lateral and anterior compartments. This scenario suggests the need for conversion of the unicompartmental arthroplasty to TKA.

Question 58
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has
been shown to be successful in the treatment of traumatic instability.
REFERENCES: Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002.
Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 59
In what decade does the peak incidence of conventional osteosarcoma occur?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266.
Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989.
Wold L, et al: Osteogenic sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, p 14.
Question 60
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of
Explanation
REFERENCES: Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Question 61
A 68-year-old woman stepped on a needle while walking barefoot 10 days ago. She is not certain but thinks it is imbedded in her foot, and she notes local tenderness at the puncture site and drainage. Her primary care physician has been treating her with oral antibiotics. A plain radiograph is shown in Figure 38. What is the best course of action?
Explanation
REFERENCES: Combs AH, Kernek CB, Heck DA: Orthopedic grand rounds: Retained wooden foreign body in the foot detected by computed tomography. Orthopedics 1986;9:1434-1435.
Markiewitz AD, Karns DJ, Brooks PJ: Late infections of the foot due to incomplete removal of foreign bodies: A report of two cases. Foot Ankle Int 1994;15:52-55.
Question 62
A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result?
Explanation
REFERENCES: Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.
Cannata G, De Maio F, Mancini F, et al: Physeal fractures of the distal radius and ulna: Long-term prognosis. J Orthop Trauma 2003;17:172-179.
Ray TD, Tessler RH, Dell PC: Traumatic ulnar physeal arrest after distal forearm fractures in children. J Pediatr Orthop 1996;16:195-200.
Aminian A, Schoenecker PL: Premature closure of the distal radial physis after fracture of the distal radial metaphysis. J Pediatr Orthop 1995;15:495-498.
Question 63
What three structures are considered the primary constraints necessary for elbow stability?
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 64
A 50-year-old man undergoes revision total knee arthroplasty (TKA). The tibial component shown in Figure 153 was retrieved at the time of revision. The wear damage demonstrated on the backside of the tibial component is most likely related to which wear mechanism(s)?
Explanation
Pitting and delamination seen in tibial component retrievals on the bearing surface of a TKA is related to fatigue wear. Backside wear is shown in the photograph; this is where the lot numbers usually are present, but now they are not distinguishable because of backside wear. This wear mechanism is attributable to adhesive and abrasive wear. The nanometer-size particles created by this wear mechanism account for the higher prevalence of osteolysis associated with modular tibial components.
CLINICAL SITUATION FOR QUESTIONS 154 AND 155
Five weeks ago, an 82-year-old man underwent revision total knee arthroplasty (TKA). Three weeks after surgery he had a dental cleaning. The patient now reports 2 days of worsening pain following a long physical therapy session. His C-reactive protein (CRP) level is 15.0 mg/L (reference range, 0.08-3.1 mg/L). Upon examination, there is no drainage and slight effusion, and he has a passive range of motion to 110 degrees. Radiographs are unremarkable.
Question 65
A 28-year-old woman sustained an injury to her dominant right arm after falling off her porch. Examination reveals a deformity at the elbow. She is neurovascularly intact. Figures 46a and 46b show the radiographs obtained before closed reduction, and postreduction radiographs are shown in Figure 46c and 46d. What is the most likely early complication?
Explanation
REFERENCES: Ring D, Jupiter JB: Reconstruction of posttraumatic elbow instability. Clin Orthop 2000;370:44-56.
O’Driscoll SW: Classification and evaluation of recurrent instability of the elbow. Clin Orthop 2000;370:34-43.
O’Driscoll SW, Morrey BF, Korinek S, An KN: Elbow subluxation and dislocation. Clin Orthop 1992;280:186-197.
Question 66
Delayed-onset muscle soreness (DOMS) is initially evident at the muscle tendon junction and can spread throughout the entire muscle. It is primarily associated with what type of exercise? Review Topic
Explanation
Question 67
What is the most prevalent adverse event associated with allogeneic blood transfusion?
Explanation
REFERENCES: Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.
Popovsky MA, Whitaker B, Arnold NL: Severe outcomes of allogeneic and autologous blood donation: Frequency and characterization. Transfusion 1995;35:734-737.
Question 68
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
REFERENCES: Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 69
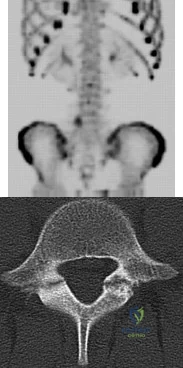
03 A 37 year-old woman with thoracic back pain has had hemoptysis and dyspnea for the past month. A thoracic spine radiograph shows a compression fracture of T-9 and a mass in the right lung. What is the best course of action?
Explanation

Here is an algorithm from OKU 6 Tumors of the Spine pp 723-736

This question gives you the history, skips right over physical exam and goes into plain films. With this patient’s history of hemoptysis and dyspnea and a lung mass, the next steps in this patients work-up would include the competion of initial work-up, metastatic work-up, then pre-operative planning. Goals of treatment are to 1) protect or restore neurologic function, 2) control pain,

Question 70
In a patient with a soft-tissue sarcoma treated by wide excision and radiation therapy, the risk of subsequent fracture is probably most influenced by
Explanation
REFERENCES: Bell RS, O’Sullivan B, Nguyen C, et al: Fractures following limb-salvage surgery and adjuvant irradation for soft-tissue sarcoma. Clin Orthop 1991;271:265-271.
Lin PP, Boland PJ, Healey JH: Treatment of femoral fractures after irradiation. Clin Orthop 1998;352:168-178.
Question 71
Figure 19 shows the radiograph of a 6-month-old infant who has limited hip motion. History reveals no complications during pregnancy or delivery. Examination reveals that hip abduction is 45 degrees in flexion bilaterally. The neurologic examination is normal. What is the best course of action?
Explanation
REFERENCE: Castelein RM, Korte J: Limited hip abduction in the infant. J Pediatr Orthop 2001;21:668-670.
Question 72
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18° of valgus compared with 3° of valgus on the opposite side. Management should now include
Explanation
REFERENCES: Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 73
Figure 7 shows a sagittal T 1 -weighted MRI scan. What muscle/tendon is identified by the arrow?
Explanation
REFERENCES: Goutallier D, Postel JM, Gleyze P, et al: Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears.
J Shoulder Elbow Surg 2003;12:550-554.
Agur AM (ed): Grant’s Atlas of Anatomy, ed 9. Baltimore, MD, Lippincott Williams & Wilkins, 1991, p 394.
Question 74
Figure 100 is the MR image of a 19-year-old man who sustains recurrent anterior shoulder dislocations. The lesion shown occupies approximately 10% of the articular surface. What is the most appropriate treatment?
Explanation
The MR image shows a bony Bankart lesion involving less than 20% of the glenoid joint surface. One series reported high success rates after arthroscopic treatment when the defect was incorporated into the repair. Anterior bony deficiencies occupying more than 25% to 30% of the glenoid joint surface treated with soft-tissue repair only are associated with high
recurrence rates. In these patients, an open or arthroscopic coracoid transfer or distal tibial allograft reconstruction should be considered. ORIF has been reported for treatment of large acute glenoid rim fractures, but is not recommended for recurrent anterior shoulder instability in the setting of a 10% glenoid rim fracture.
Question 75
A child born with myelomeningocele is expected to be an ambulator with bracing. Examination by the consulting orthopaedic surgeon reveals rigid clubfeet in addition to the neurologic issues. Management should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 65-78.
Kasser JE (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 503-514.
Question 76
A 13-year-old girl presents with back pain for 6 months. Figures A and B are SPECT scan and CT images taken at the time of presentation. What is the most likely diagnosis? Review Topic
Explanation
patient
has
spondylolysis.
Spondylolysis is a common cause of back pain in children/adolescents. It is common in sports with repetitive hyperextension (gymnasts, weightlifters, football linemen). It is best seen on lateral and oblique radiographs, CT (best study to diagnose and delineate anatomy), and SPECT.
Saifuddin et al. reviewed the orientation of the pars fracture. They found that only 32% of defects were oriented within 15° of the 45° lateral oblique plane and would be
visible on oblique radiographs. They thus recommend CT scans for spondylolysis.
Cheung et al. reviewed spondylolysis and spondylolisthesis. They advocate pars repair for symptomatic spondylolysis and low-grade, mobile spondylolisthesis with pars defects cephalad to L5 and for those with multiple-level defects.
Figure A is a 99mTc-MDP SPECT scan showing increased uptake at the right L5 pars interarticularis. Figure B is an axial helical CT image showing bilateral spondylolysis at L5. Illustration A is a corresponding sagittal reconstruction image demonstrating right pars fracture into the right L5 superior facet. Illustration B shows the appearance of osteoblastic metastasis (green arrow). Illustration C shows the options for pars repair.
Incorrect
Question 77
What is the most likely cause of recurrent symptoms following excision of a third web space neuroma?
Explanation
REFERENCES: Beskin JL: Recurrent interdigital neuromas, in Nunley JA, Pfeffer GB, Sanders RW, Trepman E (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 481-484.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
Question 78
A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment? Review Topic

Explanation
appears to be helpful. A hindfoot arthrodesis (usually triple) would be reserved if coalition resection proves to be unsuccessful. Achilles tendon lengthening and orthotic support, as well as debridement of the sinus tarsi, are not expected to result in a satisfactory outcome. The patient does not have a flatfoot deformity.
(SBQ13PE.64) A 5-year-old boy presents to clinic for evaluation of bilateral foot deformities shown in Figure 1. He is fully active and has no pain. The feet appear normal when he is sitting on the examination table, and there is supple passive motion at the subtalar joint. Passive ankle dorsiflexion is to neutral with knee in extension and 15 degrees with knee in flexion. What is the most appropriate next step? Review Topic

Spine MRI
Standing radiographs of the bilateral feet
Gastrocnemius stretching and nightime use of ankle foot orthosis
Gastrocnemius stretching and use of UCBL orthotic when ambulating
Gastrocnemius stretching
The patient is presenting with bilateral flexible pes planovalgus (or flexbile flatfoot). The most appropriate treatment in patients with a tight heel cord and no pain is gastrocnemius stretching
A flexible flatfoot in a child typically resolves spontaneously. Radiographs are typically indicated when there is pain to rule out other conditions. Treatment for patients without pain includes observation and gastrocnemius stretching. If there is pain, soft arch support or a more rigid UCBL can be used, but orthotics do not change the natural history. In patients with continued tightness in the heel cord despite aggressive stretching, gastrocnemius lengthening may be necessary.
Mosca reviews the management of flexible flatfeet in children and adolescents. He reports that there is no compelling evidence that an arch can be created with use of
orthotics. He proposes the following algorithm: patients with asymptomatic flatfeet are observed; symptomatic flatfeet with tight heel cords undergoing stretching until they become asymptomatic; symptomatic flatfeet with tight heel cords that do not respond to stretching (rare cases) are considered for surgery.
Figure A shows a young a patient with bilateral flatfeet when standing. Incorrect Answers:
abnormalities can seen in patients with cavovarus deformity Answer 2: Radiographs are indicated when there is pain to rule out other conditions. Answer 3: Ankle foot orthoses are not used for pes planovalgus Answer 4: UCBL would be indicated if the patient was having pain.
(SBQ13PE.42) Submuscular bridge plating is appropriate treatment for which of the following? Review Topic
A 2-month-old female with displaced, spiral, mid-diaphyseal femur fracture
A 26-month-old boy with a displaced spiral mid-diaphyseal femur fracture with
<2cm shortening
A 7-year old boy with a transverse, non-comminuted mid-diaphyseal femur fracture
A 7-year-old boy with a highly comminuted mid-diaphyseal femur fracture
A 15-year-old girl with a displaced butterfly fragmented mid-diaphyseal femur fracture
Submuscular bridge plating is appropriate for length-unstable femur fractures in skeletally immature patients ages 6 years and older.
Traditional plating of diaphyseal femur fractures in children has been abandoned due to the large incision and significant periosteal stripping involved. Submuscular plating with limited incisions and percutaneously applied fixation is a more biologically friendly way to achieve rigid internal fixation in length-unstable fracture patterns. External fixation is another acceptable option for these fractures. Locked plating, on the other hand, provides an 'internal external fixator,' avoids pin site issues and allows rapid mobilization while providing a biologically favorable environment for healing.
Kocher et al. provide the AAOS Clinical Practice Guideline for the treatment of pediatric diaphyseal femur fractures. They concluded that there was insufficient evidence regarding submuscular bridge plating to include it in the guideline.
Flynn et al. review the management of pediatric femoral shaft fractures. The note that
the narrow indications for plating of pediatric femoral fractures are open fractures, multiple trauma, head injury or compartment syndrome in patients less than 12 years old. Plating allows rigid fixation with readily available equipment and allows for rapid mobilization.
Hedequist et al. present a Technical Tricks paper in which they detail their surgical technique for submuscular bridge plating. They recommend this fixation strategy for patients between age 6 and skeletal maturity with comminuted diaphyseal femur fractures that are not easily treated by other methods.
Illustration A shows a preoperative and postoperative radiograph of a comminuted pediatric femur fracture treated with submuscular plating.
Incorrect answers:
(SBQ13PE.88) A 12-month-old boy attends a government regulated childcare center. His parents are called after a fall. Non-accidental trauma has been ruled out. On physical examination the right elbow is swollen and tender. He is unwilling to allow you to move the arm. Radiographs of the elbow are shown in Figure A. What is the orthopaedic management of this injury? Review Topic

Observation only
Elbow sling for 3 to 4 weeks
Rigid elbow immobilisation for 4 to 5 weeks
Admit for 24-48 hours for continuous intracompartmental pressure measurements
Operative fixation with percutaneous pinning PREFERRED RESPONSE 5
This patient presents with a distal humeral physeal separation. The most appropriate treatment would be closed reduction with internal fixation with percutaneous pins.
Displaced distal humerus physeal separation is typically seen in children under the age of 3 and has a high association with child abuse. The diagnosis can be a difficult as radiographs of a distal humeral physeal separation may be subtle. Often, radiographs show no obvious fracture, but can appear like an elbow dislocation since the secondary ossification centers have not yet developed. MRI or arthrogram can be used to aid in diagnosis.
Shrader et al. reviewed pediatric supracondylar fractures and pediatric physeal elbow fractures. They state the key to diagnosis of distal humerus physeal separation is the assessment is the radial head–capitellum relationship. These injuries should be fixed with closed reduction and smooth wire pinning. An elbow arthrogram may be considered intraoperatively for these patients because of the difficulty visualizing the distal humeral anatomy in children so young.
Skaggs et al. reviewed the diagnosis and management of pediatric elbow fractures. He states that child abuse should be suspected in all cases of elbow fracture when the child is less than 3 years of age and/or the injury pattern occur from a shearing mechanism. The displacement of physeal elbow fractures is almost always posteromedial.
Figure A shows AP and lateral radiographs with posteromedial displacement of the radial and ulnar shafts relative to the distal humerus. This is consistent with distal humeral physeal separation.
Incorrect Answers:
Question 79
A 25-year-old man has an isolated flexor digitorum profundus laceration just proximal to the distal interphalangeal (DIP) flexion crease of his ring finger. The tendon ends are trimmed, removing 10 mm from each end (secondary to fraying) and the tendon repaired. Four months later, he reports limited finger motion of the long, ring, and small fingers. He cannot fully extend his wrist and all joints of the 3 fingers simultaneously. He has full passive flexion but cannot actively completely close his fingers into a fist. What is the most likely cause?
Explanation
If a single flexor digitorum profundus (FDP) tendon is debrided more than 1 cm prior to repair, the tendon is advanced too far distally, essentially shortening the musculotendon unit. The finger will likely develop a flexion posture. Because of the common muscle belly and interconnections of the profundi, the long and small fingers adjacent to the injured finger will be affected because of loss of some of their normal proximal excursion. The result is an inability of the adjacent fingers to completely flex. This condition, known as quadrigia, is named after the Roman chariot driver who held control of the reins of 4 horses, forcing them to move as 1. Quadrigia occurs when the FDP tendon is advanced too far distally, when a tendon graft is too short, or when the profundus is sutured over the end of an amputated digit. Intrinsic muscles of the hand flex the metacarpophalangeal (MP) joints and extend the PIP joint. Intrinsic tightness causes decreased PIP flexion when the MP joint is in extension. The lumbrical muscle modulates tension on the flexor profundus tendon. When a tendon graft to repair the profundus tendon is too long, a lumbrical plus deformity occurs. This is a paradoxical PIP extension as the finger is flexed. Disruption of the tendon
repair causes limited flexion of the injured finger.
Question 80
A 29-year-old patient sustains a closed, displaced joint depression intra-articular calcaneus fracture. In discussing potential complications of surgical intervention through an extensile lateral approach, which of the following is considered the most common complication following surgery?
Explanation
REFERENCES: Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD,
Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.
Question 81
A patient undergoes a proximal tibial resection that is reconstructed with a fresh frozen osteoarticular allograft. Eleven months later, the graft is retrieved. Histologically, the articular cartilage and subchondral bone retrieved would be expected to show evidence of
Explanation
REFERENCES: Enneking WF, Campanacci DA: Retrieved human allografts:
A clinicopathological study. J Bone Joint Surg Am 2001;83:971-986.
Enneking WF, Mindell ER: Observations on massive retrieved human allografts.
J Bone Joint Surg Am 1991;73:1123-1142.
Question 82
Deep posterior compartment
Explanation
The structures at risk are the anterior tibial artery and deep peroneal nerve in the anterior compartment, superficial peroneal nerve in the lateral compartment, sural nerve in the superficial posterior compartment, and posterior tibial nerve and posterior tibial and peroneal arteries and veins in the deep posterior compartment.
Question 83
Which of the following is considered a limitation of the Short Form 36 (SF-36) general health status instrument when applied to musculoskeletal conditions?
Explanation
Multilingual validated translations have been produced in addition to international population data sets. The survey can be patient self-administered via office visit, mail, or telephone. A bias of lower over upper extremity function with regard to outcome measures employing the SF-36 has been demonstrated. Limits on the detection of certain changes in quality of life status may impose ceiling and floor effects on analysis and interpretation.
Question 84
A 3-year-old patient with L3 myelomeningocele has bilateral dislocated hips. Management should consist of
Explanation
REFERENCES: Fraser RK, Hoffman EB, Sparks LT, et al: The unstable hip and mid-lumbar myelomeningocele. J Bone Joint Surg Br 1992;74:143-146.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-76.
Question 85
A 26-year-old man has recurrent right knee pain. Figures 9a and 9b show consecutive sagittal T2-weighted MRI scans, and Figure 9c shows a coronal T1-weighted MRI scan. What is the most likely diagnosis?
Explanation
The average width of a normal meniscus is less than 11 mm. A bow-tie appearance should not be seen on more than two consecutive sagittal images because the conventional thickness of the sagittal slices is 3 mm and the interval between two consecutive slices is 1.5 mm. Two sagittal slices will cover a 9-mm thickness. A discoid meniscus can be diagnosed on the sagittal views by noting a bow-tie appearance on more than two consecutive images.
REFERENCES: Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Mink JH, Deutsch AL: The knee, in MRI of the Musculoskeletal System, ed 1. New York, NY, Raven Press, 1990, pp 251-387.
Question 86
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?
Explanation
REFERENCE: Baxter DE, Pfeffer GB, Thigpen M: Chronic heel pain: Treatment rationale. Orthop Clin North Am 1989;20:563-569.
Question 87
- A 16-year-old girl who swims on her high school team reports pain in the shoulder after swimming. History reveals a glenohumeral dislocation at age 14 years while doing the backstroke. Examination shows a positive anterior apprehension sign. Treatment at this time should consist of
Explanation
p. 577: “A vigorous effort to stabilize the shoulder with exercises is particularly indicated in patients with multidirectional or posterior instability and in athletes requiring a completely normal or supranormal range of motion.”
p. 989: “If the [swimmer] has symptoms of subluxation, a conservative program that strengthens the external rotators is warranted. Surgery is seldom indicated.”
Question 88
A 66-year-old woman with known poorly controlled rheumatoid arthritis reports that for the past 4 weeks she has been unable to extend the metacarpophalangeal (MCP) joints of her right hand index, middle, ring and little fingers. She cannot hyperextend the thumb interphalangeal joint. Active wrist extension is possible, but shows radial deviation. Examination reveals mild synovitis at the wrist and MCP joints of the affected hand. There is no ulnar deviation at the MCP joints with normal alignment. When the MCP joints are passively extended, the patient is unable to maintain them in this position. There is no piano key sign at the distal ulna. Passive wrist motion shows a normal tenodesis effect. Which of the following would most likely confirm your diagnosis? Review Topic
Explanation
Question 89
An osteoconductive bone graft material has which of the following properties?
Explanation
substitution, which allows for graft incorporation. An osteoinductive graft will stimulate the recruitment of progenitor cells that can differentiate into osteoblastic cells. Specific BMPs are osteoinductive. Osteogenic material contains viable cells with the ability to form bone. The ability to provide osteoprogenitor cells is only seen in fresh autograft. Other grafts rely on the recruitment of host progenitor cells to differentiate.
Question 90
A 21-year-old man has had posterior neck discomfort for the past 6 months. A whole-body bone scan and a cervical single-photon emission CT reveal increased activity at the C7 spinous process. MRI reveals multifocal involvement of the spinous process lamina and facet of C7. A CT-directed needle biopsy reveals osteoblastoma. What is the best course of action?
Explanation
REFERENCES: Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1143-1174.
Ozaki T, Liljenquist U, Hillmann A, et al: Osteoid osteoma and osteoblastoma of the spine: Experience with 22 patients. Clin Orthop 2002;397:394-402.
Question 91
When counseling a patient with hypophosphatemic rickets, which of the following scenarios will always result in a child with the same disorder?
Explanation
REFERENCES: Evans GA, Arulanantham K, Gage JR: Primary hypophosphatemic rickets: Effect of oral phosphate and vitamin D on growth and surgical treatment. J Bone Joint Surg Am 1980;62:1130-1138.
Greene WB, Kahler SG: Hypophosphatemic rickets: Still misdiagnosed and inadequately treated. South Med J 1985;78:1179-1184.
Question 92
Figure 12 shows the radiograph of an 80-year-old woman who has had an 8-month history of back pain after a fall. What is the most likely diagnosis based on the radiographic findings at the fractured vertebrae?
Explanation
REFERENCES: Murakami H, Kawahara N, Gabata T, et al: Vertebral body osteonecrosis without vertebral collapse. Spine 2003;28:E323-E328.
Jang JS, Kim DY, Lee SH: Efficacy of percutaneous vertebroplasty in the treatment of intravertebral pseudarthrosis associated with noninfected avascular necrosis of the vertebral body. Spine 2003;28:1588-1592.
Question 93
Which of the following methods of meniscal repair has the highest load to failure strength?
Explanation
REFERENCES: DeHaven KE: Meniscus repair. Am J Sports Med 1999;27:242-250.
Dervin GF, Downing KJ, Keene GC, McBride DG: Failure strengths of suture versus biodegradable arrow for meniscal repair: An in vitro study. Arthroscopy 1997;13:296-300.
Barber FA: Endoscopic meniscal repair: The T-fix technique. Sports Med Arthroscopy Rev 1999;7:28-33.
Question 94
A 58-year-old man has had a 3-year history of recurrent ulcerations of the left ankle and instability despite multiple attempts at custom bracing, contact casting, and surgical debridement. He has an ankle-brachial index of 0.76. A clinical photograph and radiographs are shown in Figures 16a through 16c. Treatment should now consist of
Explanation
REFERENCES: Pinzur MS, Kelikian A: Charcot ankle fusion with a retrograde locked intramedullary nail. Foot Ankle Int 1997;18:699-704.
Herbst SA: External fixation of Charcot arthropathy. Foot Ankle Clin 2004;9:595-609.
Question 95
What is the most likely complication after surgical treatment in this scenario?
Explanation
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, and internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through as seen in this patient.
The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The 4 muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the 4 rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation.
This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Brighton sign findings would be negative), a posterior capsular shift with rotator interval closure is indicated. If a patient has excessive glenoid retroversion, a posterior opening-wedge osteotomy is appropriate.
The most common complication seen after arthroscopic posterior labral repair is stiffness, followed by recurrent instability and degenerative joint disease.
Question 96
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals lumbar paraspinal spasm and a positive straight leg raising test. Deep tendon reflexes, motor strength, and sensation in the lower extremities are normal. Radiographic findings are normal. If symptoms persist for longer than a few weeks, what is the best course of action?
Explanation
REFERENCES: Epstein JA, Epstein NE, Marc J, et al: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Hashimoto K, Fujita K, et al: Lumbar disc herniation in children. J Pediatr Orthop
1990;10:394-396.
Question 97
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?
Explanation
REFERENCES: Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Callaghan JJ, Salvati EA, Pellicci PM, Wilson PD Jr, Ranawat CS: Results of revision for mechanical failure after cemented total hip replacement, 1979 to 1982: A two- to five-year follow-up. J Bone Joint Surg Am 1985;67:1074-1085.
Question 98
Oxidation of polyethylene after sterilization occurs most rapidly when the implant undergoes
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Wright TM: Ultra-high molecular weight polyethylene, in Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 37-46.
Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 99
..Figures 112a and 112b are the anteroposterior and lateral radiographs of a 65-year-old man who has a significant history of tobacco abuse and a 6-week history of right thigh pain. Axial and sagittal MRI scans are seen in Figures 112c and 112d. His MR angiogram is shown in Figure 112e. A biopsy of a lesion is shown in Figure 112f. What is the most likely diagnosis?
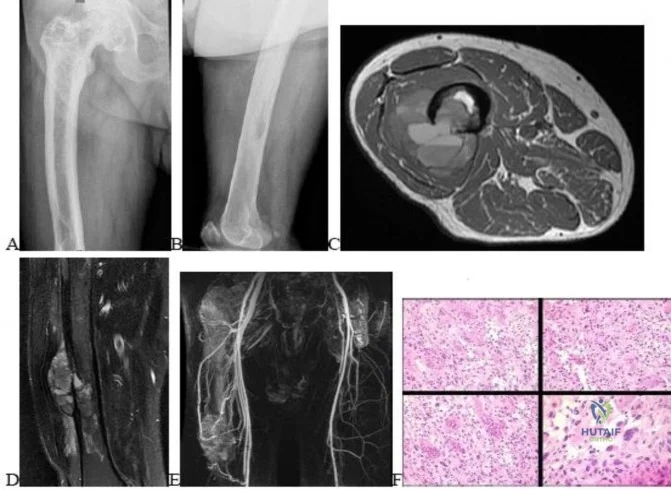
Explanation
Figures 113a and 113b are the radiographs of a 68-year-old-man who has increasing pain in his left groin with weight-bearing activities and a Trendelenburg gait. Radiographs reveal a lytic lesion of the greater trochanter. An initial diagnosis of adenocarcinoma of the lung was made 1 year before this presentation. His lung cancer treatment consisted of partial lobectomy and postsurgical radiation therapy.


Question 100
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?
Explanation
REFERENCE: Perlik PC, Guilford WB: Magnetic resonance imaging to assess vascularity of scaphoid nonunions. J Hand Surg Am 1991;16:479-484.
