OITE & ABOS Orthopedic Board Review MCQs: Spine, Hip, & Shoulder | Part 20

Key Takeaway
This page is an interactive OITE/AAOS Orthopedic Surgery Board Review, Part 20. It provides 100 high-yield, verified MCQs covering Arthroplasty, Hip, and Spine. Designed for orthopedic residents and surgeons, its purpose is crucial preparation for board certification examinations.
About This Board Review Set
This is Part 20 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 20
This module focuses heavily on: Arthroplasty, Hip, Nerve, Shoulder, Spine, Wrist.
Sample Questions from This Set
Sample Question 1: 03 The sagittal oblique MRI scan shown in Figure 70 reveals a lesion in the shoulder that typically affects what neurologic structure?...
Sample Question 2: A 52-year-old man with a BMI of 40 and primary osteoarthritis undergoes total hip arthroplasty through a posterolateral approach. To retract the femur anteriorly when exposing the acetabulum, the surgeon places a sharp curved retractor over...
Sample Question 3: A 10-year-old girl was thrown over the handlebars of her bicycle and landed directly on her left shoulder. She was treated with a figure-of-8 strap and analgesics. Follow-up examination 2 weeks later reveals that the lateral end of the clav...
Sample Question 4: A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely o...
Sample Question 5: Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
03 The sagittal oblique MRI scan shown in Figure 70 reveals a lesion in the shoulder that typically affects what neurologic structure?
Explanation
The cysts form either because of a lesion of the capsulolabral complex at the superior/posterosuperior glenoid in the shoulder or because of myxoid degeneration of the capsule.
back to this question next question
Question 2
A 52-year-old man with a BMI of 40 and primary osteoarthritis undergoes total hip arthroplasty through a posterolateral approach. To retract the femur anteriorly when exposing the acetabulum, the surgeon places a sharp curved retractor over (anterior to) the anterior inferior iliac spine. Pulsatile bleeding is encountered. A branch of which artery has been injured?
Explanation
Video 182 for reference
The femoral artery crosses the hip joint anterior to the anterior hip capsule. The medial femoral circumflex artery enters the joint along the route of the obturator externus. The obturator artery enters the hip joint beneath the transverse acetabular ligament. The iliac circumflex vessel arises superior to the hip joint.

RESPONSES FOR QUESTIONS 183 THROUGH 188
For each clinical scenario described below, identify the corresponding anteroposterior pelvic radiographic image shown above.
Question 3
A 10-year-old girl was thrown over the handlebars of her bicycle and landed directly on her left shoulder. She was treated with a figure-of-8 strap and analgesics. Follow-up examination 2 weeks later reveals that the lateral end of the clavicle is superiorly dislocated relative to the acromion. A radiograph of the shoulder shows calcification lateral to the coracoid process at the level of the acromion, and the clavicle is superiorly displaced. Management should consist of
Explanation
REFERENCES: Falstie-Jensen S, Mikkelsen P: Pseudodislocation of the acromioclavicular joint. J Bone Joint Surg Br 1982;64:368-369.
Havranek P: Injuries of the distal clavicular physis in children. J Pediatr Orthop 1989;9:213-215.
Question 4
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
Question 5
Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?

Explanation
The fracture has occurred around the stem, representing a Vancouver type B fracture, and the stem is clearly loose, making it a type B2 fracture. The appropriate treatment is removal of the loose in situ stem; ORIF of the femur using cerclage wires, cables, or a plate; and insertion of a longer revision stem such as a tapered fluted modular titanium or fully porous coated cylindrical stem to bypass the fracture. All of the other options are incorrect, because they represent inappropriate treatment options for a Vancouver type B2 fracture.
Question 6
A study is designed that examines fractures in children with osteogenesis imperfecta after being treated with bisphosphonates compared with a placebo. A difference is found for which the P value is greater than what is considered to be statistically significant. What is the next appropriate statistical analysis?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 7.
Kocher MS, Zurakowski D: Clinical epidemiology and biostatistics: A primer for orthopaedic surgeons. J Bone Joint Surg Am 2004;86:607-620.
Question 7
Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
Explanation
A. Inability to flex the distal interphalangeal joint of the index finger
B. Positive Froment’s sign
C. Weakness with wrist extension
D. Decreased capillary refill
Question 8
A 44-year-old man reports persistent left leg pain following a L5-S1 hemilaminotomy and partial diskectomy. Examination shows a grade 4 weakness of the left extensor hallucis longus and a positive left straight leg raise. A radiograph is shown in Figure 1a, and sagittal and axial MRI scans are shown in Figures 1b and 1c. Nonsurgical management consisting of medication, physical therapy, and injections has failed to provide relief. Surgical management should consist of
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 311-317.
Moller H, Hedlund R: Instrumented and noninstrumented posterolateral fusion in adult spondylolisthesis: A prospective randomized study: Part 2. Spine 2000;25:1716-1721.
Question 9
A 16-year-old high school football player has diffuse pain with attempted digital flexion after injuring the ring finger of the dominant hand 1 week ago. Examination reveals that he is unable to flex the distal interphalangeal joint. Management should consist of
Explanation
REFERENCES: Strickland JW: Flexor tendons: Acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 1851-1897.
Leddy JP: Avulsions of the flexor digitorum profundus. Hand Clin 1985;1:77-83.
Question 10
The direct anterior (Smith-Peterson) approach to hip arthroplasty is most commonly associated with injury to what nerve?
Explanation
Some authors have reported the incidence of lateral femoral cutaneous nerve neuropraxia following hip arthroplasty with the direct anterior approach to be near 80%, but resolution of the sensory deficits has been observed in most patients over time. Femoral nerve palsy has been reported to occur in .64% to 2.3% direct lateral (Hardinge) and anterolateral (Watson-Jones) approaches, and the superior gluteal nerve may be injured with proximal extension of the abductor muscular dissection. The posterior approach has been reported to be associated with sciatic nerve injury, especially in cases of dysplasia. Pudendal nerve injury has not been reported with the anterior, anterolateral, direct lateral, or posterior approaches to hip
arthroplasty. It has been reported following hip arthroscopy and the use of a traction table, however.
Question 11
Performing reconstruction of the anterior cruciate ligament by drilling the femoral tunnel via an anteromedial portal, in contrast to transtibial drilling, affords what theoretical benefit? Review Topic
Explanation
Question 12
Decreased risk of shoulder and elbow injury in a throwing athlete has been demonstrated with which of the following? Review Topic
Explanation
Question 13
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals lumbar paraspinal spasm and a positive straight leg raising test. Deep tendon reflexes, motor strength, and sensation in the lower extremities are normal. Radiographic findings are normal. If symptoms persist for longer than a few weeks, what is the best course of action?
Explanation
REFERENCES: Epstein JA, Epstein NE, Marc J, et al: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Hashimoto K, Fujita K, et al: Lumbar disc herniation in children. J Pediatr Orthop
1990;10:394-396.
Question 14
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?
Explanation
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Ciccotti MG, Jobe FW: Medial collateral ligament instability and ulnar neuritis in the athlete’s elbow. Instr Course Lect 1999;48:383-391.
Question 15
The newborn foot deformity seen in Figures 64a and 64b should initially treated with
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American AcademAyL-oMfadOenrathCooppayedic Surgeons, 2006, pp 240-241.
Farsetti P, Weinstein SL, Ponseti IV: The Long-term functional and radiographic outcomes of untreated
and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265. Question 65
A 4-year-old girl has been limping for the past 2 months. There is no history of trauma, previous injury, fever, or other systemic complaints. Examination reveals a moderate right knee effusio n with a 10-degree knee flexion contracture. What is the next most appropriate step in evaluation?
Arthroscopy
Antinuclear antibody
MRI
Bone scan
HLA-B27
DISCUSSION: The patient presents with juvenile idiopathic arthritis manifestations. The American College of Rheumatology defines this as one or more joints involved with swelling of 6 weeks or longer. A positive antinuclear antibody test would be diagnostic. Consideration should be made to have the patient see an ophthalmologist for evaluation of possible uveitis. Although the patient could have Lyme disease, that choice is not an option. The presence of an elevated antinuclear antibody by itself should not necessarily be used for diagnosing arthritis; however, the test does have clinical utility as a screening test. The frequency of a positive antinuclear antibody test is greatest in younger girls with oligoarticular disease and carries an increased risk for anterior uveitis. Arthroscopy might be indicated if this patient was presenting with a discoid meniscus, but there is no history of clicking, which is often one of the classic signs of discoid meniscus. MRI would not be used to diagnose juvenile idiopathic arthritis, but
MRI would be useful to help diagnose discoid meniscus. A bone scan would show increased uptake in the patient’s knee but again, this would not help diagnose her condition. HLA-B27 has no role in diagnosing juvenile idiopathic arthritis, especially in females.
REFERENCES: Iesaka K, Kubiak EN, Bong LR, et al: Orthopaedic surgical management of hip and knee involvement in patients with juvenile rheumatoid arthritis. Am J Orthop 2006;35:67-73.
Wright DA: Juvenile idiopathic arthritis, in Morrissey RT, Weinstein SL (eds): Love l and Winter’s Pediatric Orthopaedics, ed 6. Philadelphia PA, Lippincott Williams and Wilkins, 2006, pp 405-438. Question 66
An 18-month-old girl is brought in by her parents because of concerns about intoeing, bowlegs, and tripping and fa ling. Prenatal and birth history are otherwise unremarkable. The child’s growth and
development appear to be normal and she has a normal neurologic exam, a straight spine with no defects, and the hips are stable. Examination reveals hip internal rotation of 40 degrees and hip external rotation of 60 degrees. The thigh-foot angle is internal 30 degrees. Feet are straight and supple. Gait is characterized by intoeing with occasional tripping and falling. Based on these findings, what is the most appropriate action?
No treatment because internal tibial torsion slowly resolves on its own
Immediate treatment with a Denis-Browne bar
Distal tibial osteotomies
Proximal femoral derotational osteotomies
Treatment with twister cables PREFERRED RESPONSE: 1
DISCUSSION: The child has classic internal tibial torsion that is very commonly seen in younger children who are just beginning to walk. The normal outcome is for slow resolution of this problem and it seldom requires any treatment. Treatment with a Denis-Browne bar or with twister cables has not been proven to be effective. Surgical treatment at this point is premature and clearly not indicated.
REFERENCES: Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Staheli LT, Corbett M, Wyss C, et al: Lower-extremity rotational problems in children: Normal values to guide management. J Bone Joint Surg Am 1985;67:39-47.

Question 16
A 28-year-old construction worker sustains the closed injury shown in Figures A and B after a fall from a height. He is taken to the operating room. What is the next best step?

Explanation
In the distal tibial metaphysis, there is no snug endosteal fit for an IM nail. Center-center nail placement in both proximal and distal fragments is necessary to maintain alignment. There is also increased stress on distal locking bolts to maintain fracture alignment. Assuming static medial-lateral distal locking screws, accurate coronal plane and rotational alignment is achieved by fibular plating as a first step. This also
prevents late loss of alignment because of distal locking screw toggle. Reamed nailing allows a stiffer, larger nail to be placed, and allows redistribution of endosteal osteogenic material to the fracture site. Although there is endosteal vascular compromise, this does not affect fracture healing because of intact periosteal supply.
Bhandari et al. conducted a prospective, randomized, blinded comparison of 622 patients who had reamed nailing, and 604 who had unreamed nailing. For closed fractures, a significantly greater number in the unreamed group required bone grafting, implant exchange and dynamization. There was no difference in groups for open fracture nailing.
Egol et al. retrospectively reviewed distal metaphyseal tibia-fibula fractures treated with IM nailing with (25 cases) and without (47 cases) adjunctive plating. They found that plating was associated with maintenance of reduction (significant) as was the use of 2 medial-lateral distal locking bolts (not significant). They recommend fibular plating when IM nailing for distal tibia fractures.
Figures A and B show an extraarticular distal tibia fracture with distal fibula fracture. Incorrect Answers
Question 17
- The Magnetic resonance imaging signal characteristics of a high-grade soft-tissue sarcoma are best described as
Explanation
other characteristics, such as size, pattern of growth, integrity of natural boundaries, and homogeneity.
Intravenous contrast agents are not necessary to evaluate neurovascular structures. Both the T1 & T2 weighted images are essential to detect and characterize soft tissue lesions.
Most Tumors have long T1 and T2 relaxation times, therefore, in most instances signal intensity alone is of limited benefit. Exceptions are lipoma, hematoma, intra-lesional hemorrhage.
Hemorrhage may occur in some soft tissue lesions, especially sarcomas, leading to the low T1 and high T2 intensity sound on MR. Miller, indicates that Water, CSF, acute hemorrhage and soft tissue tumors appear dark on T1 and light on T2.
Question 18
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Pick TP, Howden R (edS): Gray’s Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 19
When performing a saline load test to evaluate for a traumatic arthrotomy of the knee, a mininum of how much saline should be utilized?

Explanation
The study by Nord et al found that the volumes of saline that were needed in order to effectively diagnose 75%, 90%, 95%, and 99% of the knee arthrotomies were 110, 145, 155, and 175 mL, respectively.
The other referenced study by Keese et al found that 50 mL of saline successfully identified only 46% of known knee arthrotomies and that 194 mL was needed to reach a 95% identification rate.
Question 20
The scoring system for impending pathologic fractures devised by Mirels involves assessment of which of the following factors?
Explanation
REFERENCES: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. 1989. Clin Orthop Relat Res 2003;415:S4-S13.
Damron TA, Morgan H, Prakash D, et al: Critical evaluation of Mirels’ rating system for impending pathologic fractures. Clin Orthop Relat Res 2003;415:S201-S207.
Question 21
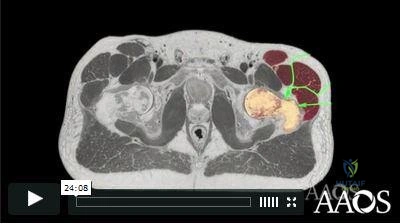
A 30-year-old woman has pain in her right hand. The radiograph, CT scan, and biopsy specimen are seen in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCES: Shimizu K, Kotoura Y, Nishijima N, Nakamura T: Enchondroma of the distal phalanx of the hand. J Bone Joint Surg Am 1997;79:898-900.
Takigawa K: Chondroma of the bones of the hand: A review of 110 cases. J Bone Joint Surg Am 1971;53:1591-1600.
Question 22
Figure 53a shows the AP radiograph of a 70-year-old patient who is scheduled to undergo unicompartmental knee arthroplasty. Figure 53b shows the immediate postoperative radiograph, and the radiograph shown in Figure 53c, obtained 6 months after surgery, shows a medial tibial plateau fracture. The etiology of the fracture is best related to
Explanation
REFERENCES: Brumby SA, Carrington R, Zayontz S, et al: Tibial plateau stress fracture: A complication of unicompartmental knee arthroplasty using 4 guide pinholes. J Arthroplasty 2003;18:809-812.
Yang KY, Yeo SJ, Lo NN: Stress fracture of the medial tibial plateau after minimally invasive unicompartmental knee arthroplasty: A report of 2 cases. J Arthroplasty 2003;18:801-803.
Vince KG, Cyran LT: Unicompartmental knee arthroplasty: New indications, more complications? J Arthroplasty 2004;19:9-16.
Question 23
A 10-year-old boy has 2 months of right knee pain that started at summer camp. The patient denies constitutional symptoms. There is no lymphadenopathy present. CT of the chest shows no signs of metastatic disease. Imaging studies and biopsy results are shown in Figures A-E. What is the most likely diagnosis?
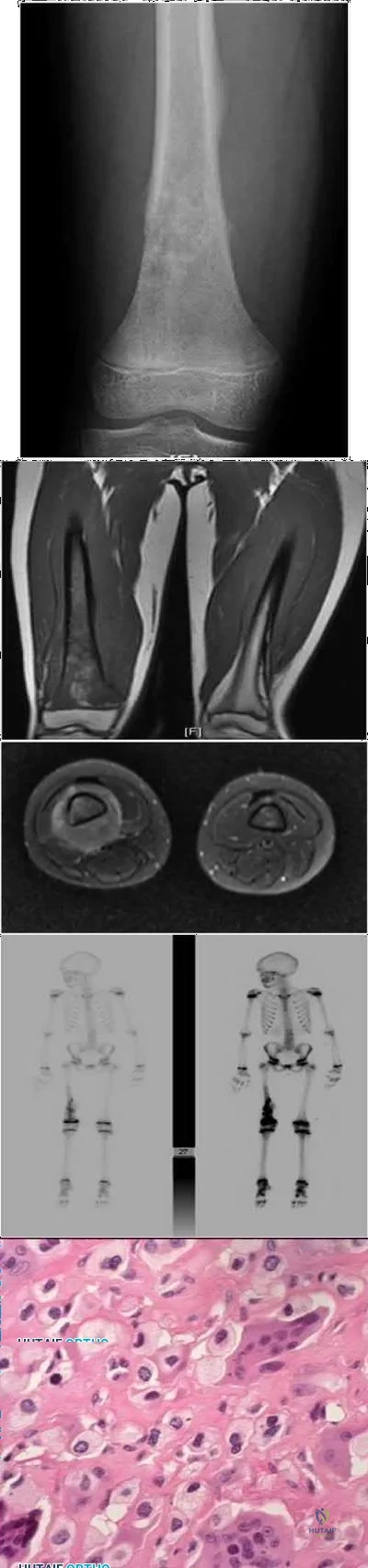
Explanation
Treatment for osteosarcoma includes neoadjuvant chemotherapy, wide resection, and adjuvant chemotherapy.
Question 24
A 45-year-old woman has had radiating pain in the medial ankle for the past 3 months. Examination reveals a small mass in the retromedial ankle region and a positive Tinel’s sign. An intraoperative photograph and a hematoxylin/eosin biopsy specimen are shown in Figures 24a and 24b. Treatment should consist of
Explanation
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Simon M, Springfield D: Surgery for the Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 530-531.
Question 25
.What is the most appropriate treatment if instability is present at the time of evaluation?
Explanation

Question 26
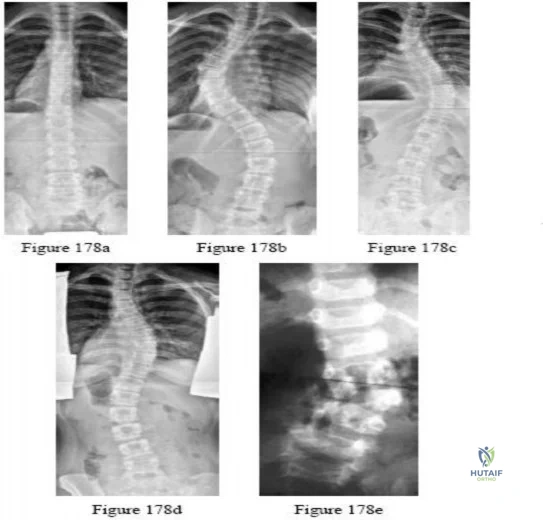
-Figures a and b are the posteroanterior and lateral radiographs of a 13-year-old girl with a progressive curve despite bracing with a thoracolumbosacral orthosis. Examination reveals no pain or neurologic findings. The lumbar curve measures 59 degrees and the thoracic curve measures 52 degrees.The most appropriate treatment is

Explanation
Question 27
An 11-year-old boy sustained an injury to his arm in gym class. He denies prior pain in the arm. Radiographs are shown in Figures 48a and 48b. What is the next most appropriate step in the management of this lesion?
Explanation
REFERENCES: Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Deyoe L, Woodbury DF: Unicameral bone cyst with fracture. Orthopedics 1985;8:529-531.
Question 28
1 and 2 show the radiograph and CT obtained from a year-old woman who underwent right total hip replacement in She initially did well with no pain. She was last seen 7 years ago and was having mild hip pain at that time. She was found to have a supra-acetabular cyst on radiographs. She has had severe right hip pain for the past 9 months while using a walker for ambulation. The initial blood work reveals an estimated erythrocyte sedimentation rate of 32 mm/hr, a C-reactive protein level of 5 mg/L, a serum cobalt level of 4 µg/L, and a serum chromium level of 6 µg/L. Right hip aspiration is performed, revealing a white blood cell count of 139, 52% neutrophils, and a negative leukocyte esterase test. What is the best next step?
Explanation
The hip replacement was performed in 1995, during the period when the previous generation of polyethylene was utilized. This polyethylene was subjected to irradiation in air, with subsequent oxidation and consequent osteolysis after implantation. The mechanism of osteolysis begins with the uptake of polyethylene particles by macrophages, which then initiate an inflammatory cascade and the release of osteolytic factors. This cycle continues, with eventual implant loosening and failure. The imaging shows significant osteolysis and raises concern for pelvic discontinuity and acetabular implant failure. The surgical treatment consists of acetabular reconstruction. In this patient, concern exists for discontinuity based on the substantial amount of bone loss and nonsupportive anterior and posterior columns. This scenario requires complex acetabular revision using a custom triflange device, distraction with a jumbo acetabular component, or placement of a porous metal cup/cage construct with augmentation. The laboratory values are not consistent with infection or failure due to metal debris.
Question 29
Which of the following parameters is considered most important when assessing an acetabular fracture for surgical indications?
Explanation
REFERENCES: Tile M: Assessment and management of acetabular fractures, in Tile M (ed): Pelvic and Acetabular Fractures, ed 2. Baltimore, MD, Williams and Wilkins, 1995, pp 305-354.
Letournel E: Acetabular fractures: Classification and management. Clin Orthop 1980;151:81-106.
Letournel E, Judet R: Fractures of the Acetabular, ed 2. Berlin, Springer-Verlag, 1993, pp 29-49.
Question 30
A 42-year-old woman who has had an 18-month history of severe low back pain is referred to your office for surgical evaluation. She reports that the pain initially began with right lower extremity pain and management consisted of oral analgesics, nonsteroidal anti-inflammatory drugs, and muscle relaxants. She has seen a chiropractor as well as a pain management specialist and she is status-post epidural steroid injections. She has also completed exhaustive physical therapy, as she is a certified athletic trainer and runs a health fitness program at a community hospital. Currently, she denies lower extremity pain and her pain is isolated to her low back and is subjectively graded as 8/10, with 10 being the worst pain she has ever experienced. The pain is interfering with her activities of daily living and she is seeking definitive treatment. Figures 32a through 32c show current MRI scans. Based on the current available medical literature, what is the most appropriate treatment?
Explanation
REFERENCES: Gibson JN, Waddell G: Surgery for degenerative lumbar spondylosis: Updated Cochrane Review. Spine 2005;30:2312-2320.
Fritzell P, Hagg O, Wessberg P, et al: 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine 2001;26:2521-2532.
Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Question 31
What is the most common complication following distal biceps tendon repair?
Explanation
The distal biceps tendon is commonly torn with an eccentric contraction of the biceps when the elbow is taken into extension. Patients treated nonsurgically will note loss of at least 50% supination strength and may develop discomfort with resistive activities. The video shows the squeeze test to evaluate the integrity of the biceps tendon. The test is similar to the Thompson test in the evaluation of an Achilles tendon rupture. The distal arm is squeezed with the elbow flexed 60 to 80 degrees and the forearm pronated. By shortening the musculotendinous unit, the intact biceps tendon will lead to forearm supination. If the biceps is torn, the forearm will not supinate as shown in the video. The maneuver is performed with the elbow in flexion to minimize tension on the brachialis muscle and isolate the biceps. Ruland and associates evaluated 25 patients with suspected distal biceps ruptures and correctly diagnosed all but 1 false-positive result that involved a partial tear. The lacertus fibrosus is not evaluated with this maneuver.
When considering a repair, a 1- or 2-incision technique may be performed. Chavan and associates performed a systematic review comparing the 2 techniques and reported similar complication rates. The 2-incision technique was associated with more instances of significant loss of forearm rotation and more unsatisfactory clinical results. The 1-incision technique is associated with a higher incidence of lateral antebrachial cutaneous neuropathy likely attributable to retraction. The biceps insertion is a thin semilunar area on the posterior/ulnar aspect of the radial tuberosity centered at approximately 30 degrees anterior to the lateral/coronal plane with the arm fully supinated. Forthman and associates used CT scan to asses 30 cadaveric specimens and noted that the biceps tuberosity orientation would prohibit an anatomic repair in 35% of arms for which the 1-incision technique was used.
Mazzocca and associates reported the highest load to failure of the Endobutton (440 newton (N)) compared to fixation with suture anchor (381 N), Wartenberg syndrome (310 N), and an interference screw (232 N). Greenberg and associates noted greater load to failure for the Endobutton (584 N) compared to suture anchor (254 N) and transosseous tunnel (178 N) constructs. Spang and associates reported comparable strength of the Endobutton repair when compared to suture anchors. Fifty N of force is required to hold the elbow flexed at 90 degrees against gravity, which is well below the strength of the repairs studied.
Neuropraxia of the lateral antebrachial cutaneous nerve branch is the most common complication associated with distal biceps repair, with a reported incidence as high as 40%. The nerve branch lies between the biceps and brachialis as it crosses the surgical field in the antecubital fossa. The neuropathy may be related to aggressive retraction, particularly when using the 1-incision technique, and often resolves with time. Cain and associates reported minor complications were common (but major complications uncommon) following distal biceps repair. Reported complications are lateral antebrachial cutaneous paresthesia (26%), radial sensory nerve paresthesia (6%), posterior interosseous nerve injury (4%), and rerupture (2%).
RECOMMENDED READINGS
Ruland RT, Dunbar RP, Bowen JD. The biceps squeeze test for diagnosis of distal biceps tendon ruptures. Clin Orthop Relat Res. 2005 Aug;(437):128-31. PubMed PMID: 16056039.
Forthman CL, Zimmerman RM, Sullivan MJ, Gabel GT. Cross-sectional anatomy of the bicipital tuberosity and biceps brachii tendon insertion: relevance to anatomic tendon repair. J Shoulder Elbow Surg. 2008 May-Jun;17(3):522-6. doi: 10.1016/j.jse.2007.11.002. Epub 2008 Mar 6. PubMed PMID: 18325797.
Chavan PR, Duquin TR, Bisson LJ. Repair of the ruptured distal biceps tendon: a systematic review. Am J Sports Med. 2008 Aug;36(8):1618-24. doi: 10.1177/0363546508321482. Review. PubMed PMID: 18658024.
Mazzocca AD, Burton KJ, Romeo AA, Santangelo S, Adams DA, Arciero RA. Biomechanical evaluation of 4 techniques of distal biceps brachii tendon repair. Am J Sports Med. 2007 Feb;35(2):252-
Question 32
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
REFERENCE: Ebraheim NA, Haman SP, Xu R, Stanescu S, Yeasting RA: The lumbosacral nerves in relation to dorsal SI screw placement and their locations on plain radiographs. Orthopedics 2000;23:245-247.
Question 33
What is the most common complication following metatarsal osteotomy for a bunion deformity in an adolescent?
Explanation
Physeal arrest of the first metatarsal-“While an open epiphysis cannot be considered an absolute contraindication to an osteotomy in either the proximal phalanx, or proximal first metatarsal, it is
important at surgery to determine the exact location of the metaphyseal epiphysis to avoid injury.” Pg. 307 Mann, Surgery of Foot and Ankle.
In studies performed by Blais et. Al. A females full foot growth is usually achieved by 14 years and at 12 years an average less than 1 cm of total foot growth remains with less than 50% of this growth at the proximal epiphysis. Males’ terminal growth expected at 16 years of age with 3cm left at 12 years and approximately 1.5 cm of metatarsal growth.
Most studies show recurrence of Hallux Valgus deformity after surgical correction in the juvenile as inordinately high.
Question 34
Figures 30a and 30b are the radiographs of a 61-year-old man with diabetes who fell from a ladder and sustained an isolated closed fracture. After realignment and splint application, what is the most appropriate next step in management?

Explanation
internal fixation in the acute phase (6 to 8 hours) or sub-acute phase (2 to 3 days) is difficult.
Question 35
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on-metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of childbearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 36
Figure 20 shows the plain radiograph of a 70-year-old woman who has shoulder pain and is unable to reach above chest level as a result of a fall 3 months ago. An MRI scan of the shoulder shows a large rotator cuff tear. Examination reveals atrophy of the infraspinatus muscle, active forward elevation of 40 degrees, active external rotation of 30 degrees, passive forward elevation of 150 degrees, and passive external rotation of 60 degrees. The patient has no external rotation strength against resistance. Treatment should include
Explanation
Question 37
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should consist of
Explanation
REFERENCES: Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Schepsis AA, Grafe MW, Jones HP, Lemos MJ: Rupture of the pectoralis major muscle: Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
Question 38
A 54-year-old woman undergoes an interposition arthroplasty that fails and requires conversion to a total elbow arthroplasty. She has progressive elbow pain and radiographic loosening. Erythrocyte sedimentation rate and C-reactive protein are normal. Joint aspiration is positive for Staphylococcus epidermidis. What surgical treatment would best optimize function and decrease risk of recurrence?
Explanation
is best reserved for low-demand or infirm patients.
Question 39
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Question 40
A patient has a C6 spinal cord injury. Following stabilization of the spine, the patient should be advised that their expected maximum level of function
Explanation
Question 41
The major benefit of irrigation with a castile soap solution over irrigation with bacitracin solution for the treatment of the open fracture shown in Figure 42 can be seen in which of the following outcomes?
Explanation
REFERENCE: Anglen JO: Comparison of soap and antibiotic solutions for irrigation of lower-limb open fracture wounds: A prospective, randomized study. J Bone Joint Surg Am 2005;87:1415-1422.
Question 42
Following total knee arthroplasty, a patient is noted to have asymmetrical absent pulses and poor capillary refill. What is the next most appropriate step in management?
Explanation
perform an
DISCUSSION: An assessment of the location of the vascular compromise is necessary prior to surgical exploration. Vascular repair will most likely require a separate surgical exposure. Vascular reperfusion may be accomplished at the time of an arteriogram with the use of a stent in certain situations. Return to the operating room with vascular surgical consultation and intraoperative arteriogram is appropriate.
An immediate postoperative compartment syndrome is unlikely. Magnetic resonance angiogram is not appropriate because of the potential for a delay in diagnosis.
REFERENCE: Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001 ;9;253-257.
Question 43
The use of nonsteroidal anti-inflammatory drugs following femoral nailing has been associated with which of the following?

Explanation
Giannoudis et al assessed factors which could affect union in 32 patients with nonunion of a fracture of the diaphysis of the femur and 67 matched patients whose fracture had united. They found that there was no relationship between the rate of union and the type of implant, mode of locking, reaming, distraction or smoking. They also concluded that there was a marked association between nonunion and the use of NSAIDs after injury and delayed healing was noted in patients who took NSAIDs and whose fractures had united.
Burd et al performed a study to determine if patients with an acetabular fracture, who received indomethacin for prophylaxis against HO, were at risk of delayed healing or nonunion of any associated fractures of long bones. The study group consisted of 112 patients who had sustained at least one concomitant fracture of a long bone; of which 36 needed no prophylaxis, 38 received focal radiation and 38 received indomethacin. When comparing patients who received indomethacin with those who did not, a significant difference was noted in the rate of long bone nonunion (26% vs 7%).
Question 44
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the
Explanation
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Wright TA: Accessory spinal nerve injury. Clin Orthop 1975;109:15-18.
Question 45
A tendon repair is thought to be weakest during which phase of tendon healing?
Explanation
Question 46
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
Question 47
A 13-year-old boy has knee pain after sustaining a mild twisting injury while playing basketball 4 weeks ago. Radiographs and MRI scans are shown in Figures 24a through 24d, and biopsy specimens are shown in Figures 24e and 24f. Treatment should consist of
Explanation
REFERENCES: Simon MA, Springfield DS: Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274.
Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 48
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of
Explanation
REFERENCES: Morgan CD, Burkhart SS, Palmeri M, et al: Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998;14:553-565.
Mileski RA, Snyder RJ: Superior labral lesions in the shoulder: Pathoanatomy and surgical management. J Am Acad Orthop Surg 1998;6:121-131.
Levitz CL, Dugas J, Andrews JR: The use of arthroscopic thermal capsulorrhaphy to treat internal impingement in baseball players. Arthroscopy 2001;17:573-577.
Question 49
A 51-year-old woman with no preoperative neurologic deficit is undergoing elective anterior cervical diskectomy and fusion (ACDF) with plating and fusion for a C5-6 disk herniation with right-sided neck pain. Thirty minutes into the surgery the neurophysiologic monitoring shows a rapid drop and then loss of amplitude in the right cortical somatosensory-evoked potential waveform. All other waveforms remained normal and unchanged, including right-sided cervical (subcortical) and peripheral (Erb’s point), and those from the left-sided upper extremity and both lower extremities. What is the most likely cause of the change? Review Topic
Explanation
Question 50
A 52-year-old man has had right shoulder pain in the deltoid region that increases at night for the past 2 months. He denies any history of trauma. Examination reveals mild tenderness over the greater tuberosity, and the Neer and Hawkins impingement signs are positive. AP and outlet lateral radiographs are shown in Figures 24a and 24b. Initial management should consist of
Explanation
REFERENCES: Morrison DS, Frogameni AD, Woodworth P: Non-operative treatment of subacromial impingement syndrome. J Bone Joint Surg Am 1997;79:732-737.
Neer CS: Impingement lesions. Clin Orthop 1983;173:70-77.
Blair B, Rokito AS, Cuomo F, et al: Efficacy of injections of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am 1996;78:1685-1689.
Question 51
A 65-year-old man undergoes total shoulder arthroplasty. Examination in the recovery room reveals the absence of voluntary deltoid and biceps contraction, weakness of wrist extension, and absence of sensation over the lateral arm and radial forearm. Management should now consist of
Explanation
Question 52
It is important to avoid which of the following exercises in the immediate postoperative period after humeral head replacement for an acute four-part fracture?
Explanation
REFERENCES: Hartstock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humerus fractures. Orthop Clin North Am 1998;29:467-475.
Hughes M, Neer CS: Glenohumeral joint replacment and postoperative rehabilitation. Phys Ther 1975;55:850-858.
Question 53
In patients with suspected hepatitis C, which of the following tests is commonly used to confirm the diagnosis after a positive ELISA screening test?
Explanation
REFERENCES: de Medina M, Schiff ER: Hepatitis C: Diagnostic assays. Semin Liver Dis 1995;15:33-40.
McGrory BJ, Kilby AE: Hepatitis C virus infection: Review and implications for the orthopedic surgeon. Am J Orthop 2000;29:261-266.
Question 54
The anterior portal of a hip arthroscopy places what structure at greatest risk for injury?
Explanation
at risk.
REFERENCES: Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 83-91.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 281-289.
Question 55
A 37-year-old man with a history of congenital flatfoot reports worsening pain on the medial aspect of his ankle for the past year. The pain is worse with weight bearing and is better with rest and the use of an ankle brace. What findings are shown on the MRI scans shown in Figures 18a through 18c?
Explanation
REFERENCES: Slovenkai MP: Clinical and radiographic evaluation (Adult flatfoot: Posterior tibial tendon dysfunction). Foot Ankle Clin 1997;2:241-260.
Conti S, Michelson J, Jahss M: Clinical significance of magnetic resonance imaging in preoperative planning for reconstruction of posterior tibial tendon ruptures. Foot Ankle 1992;13:208-214.
Question 56
A 22-year-old man sustained a stable pelvic fracture, bilateral femur fractures, and a left closed humeral shaft fracture in a motor vehicle accident. Examination 24 hours after injury reveals that the patient is confused and has shortness of breath. A clinical photograph of his conjunctiva is shown in Figure 44. He has a temperature of 101 degrees F (38.3 degrees C) and a pulse rate of 120/min. Laboratory studies show a hemoglobin level of 8 g/dL, a platelet count of 50,000/mm3, and a PaO2 of 57 mm Hg on 2L of oxygen. What is the most likely diagnosis?
Explanation
REFERENCE: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 308-316.
Question 57
What significant structure is most at risk during a posterior approach of the Achilles tendon near its musculotendinous junction?
Explanation
REFERENCES: Webb J, Moorjani N, Radford M: Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-477.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Question 58
A 78-year-old man with ankylosing spondylitis sustains a minor fall. Shortly afterward he experiences sudden worsening of his chronic back pain and is brought to the emergency department by his caregiver. Radiographs and a CT scan of the spine do not show a clear fracture. What is the most appropriate next step?
Explanation
Patients with ankylosing spondylitis are at high risk for occult fractures after low-energy injuries. Although radiographs and a CT scan do not demonstrate a spinal fracture in this patient, high risk for an unstable occult fracture necessitates further imaging with MRI to ensure that no fractures are missed. Although a CT scan is typically the primary imaging modality for workup of spine injuries in similar patients, CT and MRI complement each other and each detects fractures that are missed using the other modality. A CT myelogram might detect cord or root compression but would not aid in the diagnosis of an occult fracture. Nonsteroidal anti-inflammatory drugs are first-line treatment for idiopathic low-back pain. In a patient with ankylosing spondylitis at high risk for fracture, further workup is needed to rule out an occult fracture. Flexion and extension radiographs of the spine are inferior to MRI for evaluating occult fractures and ligamentous injuries. The primary concern for this patient remains an unstable spinal fracture, which necessitates an MRI of the spine before initiating a workup for other possible causes of his back pain.
RECOMMENDED READINGS
Duane TM, Cross J, Scarcella N, Wolfe LG, Mayglothling J, Aboutanos MB, Whelan JF, Malhotra AK, Ivatury RR. Flexion-extension cervical spine plain films compared with MRI in the diagnosis of ligamentous injury. Am Surg. 2010 Jun;76(6):595-8. PubMed PMID: 20583514. View Abstract at PubMed
Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002 Sep;97(2 Suppl):218-22. PubMed PMID: 12296682. View Abstract at PubMed
Koivikko MP, Koskinen SK. MRI of cervical spine injuries complicating ankylosing spondylitis. Skeletal Radiol. 2008 Sep;37(9):813-9. doi: 10.1007/s00256-008-0484-x. Epub 2008 Apr
Question 59
Figure 12 shows the radiograph of a patient who has anterior knee pain. History reveals a femoral fracture at age 5 years. What is the most likely cause of the deformity?
Explanation
REFERENCES: Hresko MT, Kasser JR: Physeal arrest about the knee associated with non-physeal injuries of the lower extremity. J Bone Joint Surg Am 1989;71:698-703.
Bowler JR, Mubarak SJ, Wenger DR: Tibial physeal closure and genu recurvatum after femoral fracture: Occurrence without a tibial traction pin. J Pediatric Orthop 1990;10:653-657.
Question 60
Acetabular reconstruction followed by external beam irradiation The plain radiographs show a purely lytic destructive lesion that is poorly marginated. The technetium bone scan does not show any major uptake. The computerized tomography scan shows purely lytic bone destruction with breakthrough of the cortical bone. Complete destruction of the cortical bone is suggestive of a malignancy. The magnetic resonance image shows a lesion that is homogenously low on T1-weighted images and high on T2-weighted images. Surgeons cannot make a definitive diagnosis based upon the radiographic features. The most common malignancies in this age group are:
Explanation
A 50-year-old woman has had severe hip pain for 4 months. Her plain radiographs (Slide 1), technetium bone scan (Slide 2), computerized tomography scan (Slide 3), and coronal T1- and T2-weighted magnetic resonance images (Slide 4) are presented. The most likely diagnosis based upon the radiographs would be:
Question 61
Where does the median nerve pass in the proximal forearm?
Explanation
REFERENCES: Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams and Wilkins, 1978, pp 6-55.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 120.
Question 62
Figures 70a and 70b show the sagittal MRI scan and axial CT of a patient who has decreased range of motion in the cervical spine. In which of the following directions would the cervical motion be most significantly limited?
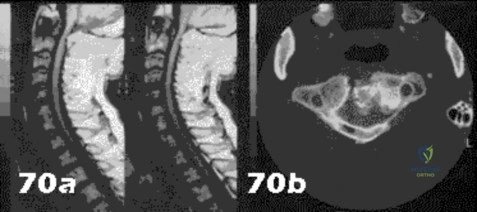
Explanation
Question 63
A further workup reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MARS MR imaging. Revision THA is recommended. The most common complication following revision of a failed metal-on-metal hip arthroplasty is
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on-metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.
The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts.
The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 64
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and
Explanation
REFERENCES: Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Morrey BF, King GJ: Revision of failed total elbow arthroplasty, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 685-700.
Question 65
-Which type of cells has been implicated in the process shown inFigure?
Explanation

Question 66
Exostoses in which of the following anatomic locations is the most likely to undergo malignant transformation in a patient with multiple hereditary exostosis (MHE)?
Explanation
REFERENCES: Peterson HA: Multiple hereditary osteochondromata. Clin Orthop 1989;239:222.
McCornack EB: The surgical management of hereditary multiple exostosis. Orthop Rev 1981;10:57.
Question 67
Refers to the effectiveness of various antibiotics against a particular microorganism.
Explanation
Knowledge of the basic nomenclature of antibiotic use is important to effectively treat patients and communicate with colleagues. The effectiveness of an antimicrobial against an infecting organism is measured by the MIC, which refers to the concentration needed to prevent growth of a microorganism on culture medium, and MBC, which is the smallest concentration of the antibiotic necessary to kill the microorganism in culture. Typically, an antibiotic is considered bactericidal if the MBC is no more than 4 times the MIC. The spectrum of antimicrobial coverage refers to an agent’s effectiveness against a range of bacteria. An antibiogram refers to the tabulation of prevalence of different bacteria in a specific setting or specific patient population. Antibiotic susceptibility and resistance refers to the bacteria’s ability to be affected or unaffected by a given antibiotic.

Question 68
A 45-year-old woman has severe anterior knee pain. Her radiographs indicate end-stage patellofemoral compartment osteoarthritis. The tibiofemoral compartments are preserved. Extensive nonsurgical treatment has failed to provide relief, and she is offered patellofemoral arthroplasty (PFA). What is the most common long-term mode of failure for PFA using an implant with an onlay prosthesis design?
Explanation
Contemporary onlay-design trochlear prostheses in PFA replace the entire anterior trochlear surface. Previous inlay designs were inset within the native trochlea and carried a higher risk of catching and patellar instability, particularly in patients with trochlear dysplasia; they also generally have higher failure rates. The current most common mode of failure is progression of arthritis throughout the knee, in some series as high as 25% at 15 years. Aseptic loosening, particularly of cemented implants, is less common. Infection is an uncommon long-term complication. Patients considering PFA should be advised of the risk of arthritis progression. Many authors routinely obtain a preoperative MRI to assess the status of the tibiofemoral compartments.
Question 69
- An MRI scan of the brain of a patient with spastic diplegia will most likely show
Explanation
Agnesis of the corpus callosum is a rare anomaly that is asymptomatic neurologically unless tests designed specifically to test the transfer of information from one cerebral hemisphere to another is employed. Additionally, the corpus callosum is intimately related to the development of the limbic system which governs major CNS roles as behavior, memory, and emotions. Therefore, this would not involve the neurologically challenged spastic diplegic individuals.
Question 70
Figure 99 shows a dorsal approach for a midfoot arthrodesis following a Lisfranc injury in a 43-year-old woman. The base of the second metatarsal is labeled with the letter B. The interval used to create this exposure is
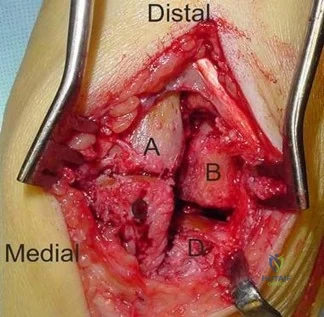
Explanation
The interval shown is between the extensor hallucis longus (left) and the extensor hallucis brevis (right), which is not an internervous plane because both are innervated by the deep peroneal nerve. The neurovascular bundle is under the extensor hallucis brevis muscle. Both
muscles are innervated by branches of the deep peroneal nerve. The superficial peroneal
Question 71
The subcutaneous nerve most at risk for transection during an anterior surgical exposure of the ankle is the
Explanation
The dorsal medial cutaneous nerve arising from the superficial peroneal nerve crosses the inferior extent of a routine extensile surgical exposure to the ankle joint. The extensile anterior incision develops the interval between the tibialis anterior and extensor hallucis tendons, and, although the deep peroneal nerve is lateral and posterior to the extensor hallucis longus, the nerve most at risk during this exposure is the cutaneous branch supplying the dorsal medial foot to the great toe. Ankle replacement surgery is becoming more common; consequently, surgeons must be familiar with this anatomic landmark and risks related to its transection during surgery.
The medial plantar nerve is at risk when medial hindfoot incisions are made through the
abductor hallucis muscle during tarsal tunnel release and harvest of the flexor hallucis tendon for transfer. The dorsal cutaneous branch of the sural nerve supplies the lateral dorsal
Question 72
A 16-year-old boy has had left knee pain and swelling after sustaining a minor twisting injury while playing basketball 2 weeks ago. Figures 5a through 5e show the radiograph, MRI scans, and biopsy specimens. What is the most likely diagnosis?
Explanation
REFERENCES: Sissons HA, Murray RO, Kemp HBS: Orthopaedic Diagnosis. Berlin, Springer-Verlag, 1984, pp 254-256.
Wafa H, Grimer RJ: Surgical options and outcomes in bone sarcoma. Expert Rev Anticancer Ther 2006;6:239-248.
Question 73
A 45-year-old man underwent a fingertip amputation through the distal phalanx after his ring finger was caught in a garage door. He was treated in the emergency department with a revision amputation by advancement of the flexor digitorum profundus (FDP) tendon to the extensor mechanism. Three months following the injury, he is able to fully flex his injured ring finger to touch his palm, but he reports that it is difficult for him to make a tight fist due to decreased flexion of his other fingers. What is this complication called?
Explanation
The quadrigia effect can occur due to over-advancement of the FDP tendon during repair (usually greater than 1 cm), development of FDP tendon adhesions, and (as in this case) "over the top" repair of the FDP tendon to the extensor tendon after amputation at the distal phalanx level. All of these conditions result in a functionally shortened FDP tendon of the injured digit. Because the FDP tendons of the long, ring, and small digits share a common muscle belly, excursion of the combined tendons is equal to the shortest tendon. Therefore, the uninjured digits will not have full excursion of their respective FDP tendons and will not be able to close into a full fisting position. Treatment of this condition is most commonly release
of the injured FDP tendon. A lumbrical plus deformity can occur in amputations distal to the flexor digitorum superficialis insertion through the middle phalanx. The FDP tendon retracts and increases tension on the lumbrical muscle, which leads to paradoxical interphalangeal (IP) joint extension with attempted flexion. Intrinsic tightness and interphalangeal joint contractures can be caused by hand trauma but would not lead to the clinical condition this patient has.
Question 74
Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
Explanation
REFERENCES: Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Mazur JM, Schwartz E, Simon SR: Ankle arthrodesis: Long-term follow-up with gait analysis. J Bone Joint Surg Am 1979;61:964-975.
Question 75
A 13-year-old gymnast presents with ongoing knee pain for the past few months. She tried conservative measures including kinesiotaping, physical therapy and rest. On physical exam, she has normal valgus alignment, negative patellar tilt and discomfort with resisted open chain knee extension. A representative radiographs are shown in Figure A-C. What is the most likely clinical diagnosis? Review Topic

Explanation
Evaluation of a patient with patellofemoral pain requires a physical examination and plain radiographs. Appropriate examination of all structures around the knee is critical to rule out other diagnoses. An MRI is useful for evaluating intra-articular or intra-osseous lesions, if clinical suspicion is suggestive of this. Treatment is predominantly conservative, with focus on low impact exercises that maximize aerobic conditioning.
Earl et al. review the epidemiology, etiology and management of patellofemoral syndrome. They note that there is no clear cause of this issue, although issues related to the quadriceps and dynamic malalignment may be contributory.
Outerbridge et al. describe overuse injuries in the young athletic patient. They provide an overview of diagnosis and management specific to this patient population.
Figures A, B and C show AP, lateral and merchant radiographs of a normal knee in a skeletally immature individual. No osseous abnormalities are identified.
Incorrect
Question 76
An 18-year-old lacrosse player sustained a hamstring pull during a game. Examination the next day reveals ecchymosis through the posterior thigh and a palpable defect in the hamstring musculature in the middle third of the thigh. What is the most likely site of anatomic injury?
Explanation
REFERENCES: Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 17-33.
Clanton TO, Coupe KJ: Hamstring strains in athletes: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:237-248.
Question 77
A 52-year-old woman underwent open reduction and internal fixation for radial and ulnar shaft fractures 2 months ago. In a second fall she refractured her forearm and required revision surgery with bone grafting. One month after the second operation she notes erythema, swelling, and drainage from the volar radial incision. In addition to antibiotic treatment, management should consist of
Explanation
REFERENCES: Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 53-63.
Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr: Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68:1008-1017.
Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphysis of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169.
Question 78
A patient sustained the injuries shown in the radiographs and clinical photograph seen in Figures 10a through 10c. The neurovascular examination is normal. The first step in emergent management of the extremity injuries should consist of
Explanation
REFERENCES: Sahin V, Karakas ES, Aksu S, et al: Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-529.
Moed BR, WillsonCarr SE, Watson JT: Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am 2002;84:752-758.
Question 79
A 14-year-old boy reports a 4-month history of increasing backache with difficulty walking long distances. His parents state that he walks with his knees slightly flexed and is unable to bend forward and get his hands to his knees. He denies numbness, tingling, and weakness in his legs and denies loss of bladder and bowel control. A lateral radiograph of the lumbosacral spine is shown in Figure 18. What is the best surgical management for this condition?
Explanation
L5 to S1 usually is not successful for a slip that is greater than 50%. Isolated anterior spinal fusion has not been successful, and direct repair of the pars defect is only useful for spondylolysis without spondylolisthesis.
REFERENCES: Lenke LG, Bridwell KH: Evaluation and surgical treatment of high-grade isthmic dysplastic spondylolisthesis. Instr Course Lect 2003;52:525-532.
Ginsburg GM, Bassett GS: Back pain in children and adolescents: Evaluation and differential diagnosis. J Am Acad Orthop Surg 1997:5:67-78.
Question 80
What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty?
Explanation
REFERENCES: Chin PY, Sperling JW, Cofield RH, et al: Complications of total shoulder arthroplasty: Are they fewer or different? J Shoulder Elbow Surg 2006;15:19-22.
Hasan SS, Leith JM, Campbell B, et al: Characteristics of unsatisfactory shoulder arthroplasties. J Shoulder Elbow Surg 2002;11:431-441.
Question 81
-What gene is implicated in spinal muscular atrophy?
Explanation

Question 82
The swelling pressure in cartilage is predominantly due to the association of exchangeable water with which of the following substances? Review Topic
Explanation
Question 83
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of
Explanation
REFERENCES: Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Gerber C, et al: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 84
Vertebral fractures are common in the thoracolumbar spine. What is the most important factor that determines the strength of the cancellous bone in the vertebral body?
Explanation
REFERENCES: Carter DR, Hayes WC: The compressive behavior of bone as a two-phase porous structure. J Bone Joint Surg Am 1977;59:954-962.
Keaveny TM: Strength of trabecular bone, in Cowin SC (ed): Bone Mechanics Handbook. Boca Raton, FL, CRC Press, 2001, pp 16-1-16-8.
Question 85
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Explanation
REFERENCES: Chan BW, Chan KS, Koide T, et al: Maternal diabetes increases the risk of caudal regression caused by retinoic acid. Diabetes 2002;51:2811-2816.
Zaw W, Stone DG: Caudal regression syndrome in twin pregnancy with type II diabetes.
J Perinatol 2002;22:171-174.
Question 86
A 72-year-old man undergoes an uncomplicated cementless total hip arthroplasty for advanced osteoarthritis. At his 6-week postoperative follow-up, he has minimal pain and is progressing well with his mobility. Radiographs show early formation of Brooker grade III heterotopic bone around his hip. What is the best treatment of the heterotopic bone at this time?
Explanation
REFERENCES: Balboni TA, Gobezie R, Mamon HJ: Heterotopic ossification: Pathophysiology, clinical features, and the role of radiotherapy for prophylaxis. Int J Radiat Oncol Biol Phys 2006;65:1289-1299. Fransen M, Neal B: Non-steroidal anti-inflammatory drugs for preventing heterotopic bone formation after hip arthroplasty. Cochrane Database Syst Rev 2004;3:CD001160.
Neal BC, Rodgers A, Clark T, et al: A systematic survey of 13 randomized trials of non-steroidal antiinflammatory

drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand 2000;71:122-128.
Question 87
During an open reduction internal fixation of a humerus fracture using the posterior approach, a surgeon can identify the posterior antebrachial cutaneous nerve and trace it proximally to which of the following nerves?

Explanation
Question 88
Figure 42 shows the sagittal T2-weighted MRI scan of a patient’s right knee. These findings are most commonly seen with a complete tear of the
Explanation
fluid in the soft tissues laterally. Additionally, there is a large bone bruise on the medial
femoral condyle. This combination indicates injury to the posterolateral complex. These injuries often have coexisting anterior and/or posterior cruciate ligament injuries. Failure to recognize the posterolateral corner injury can lead to failure of anterior or posterior cruciate ligament reconstructions.
REFERENCES: LaPrade RF, Gilbert TJ, Bollom TS, et al: The magnetic resonance imaging appearance of individual structures of the posterolateral knee: A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 2000;28:191-199.
Ross G, Chapman AW, Newberg AR, et al: Magnetic resonance imaging for the evaluation of acute posterolateral complex injuries of the knee. Am J Sports Med 1997;25:444-448.
Question 89
A 24-year-old man has bilateral hip pain. An examination and imaging studies (plain radiographs and MR imaging) confirm evidence of femoroacetabular impingement (FAI) with a CAM deformity in both hips. The patient mentions that he has a 19-year-old brother who has occasional hip pain. With respect to his brother’s pain, how should you counsel the patient?
Explanation
Evidence suggests that FAI is more common in siblings of patients with FAI, particularly those with a CAM deformity. It is unlikely this patient has well-established osteoarthritis, even in the presence of FAI.

CLINICAL SITUATION FOR QUESTIONS 145 THROUGH 147
Figures 145a and 145b are the radiographs of a 56-year-old man who has had persistent pain in his right groin since undergoing primary total hip surgery 11 months ago. His erythrocyte sedimentation rate (ESR) is 38 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein (CRP) level is 28 mg/L (rr, 0.08-3.1 mg/L). A hip aspiration performed while the patient was taking antibiotics demonstrated 3200 white blood cells/µL with no growth. Treatment should consist of
Question 90
The nerve to the abductor digiti quinti, implicated in some patients who have chronic heel pain, is most commonly a branch of what larger nerve?
Explanation
REFERENCES: Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop 1992;279:229-236.
Schon LC, Glennon TP, Baxter DE: Heel pain syndrome: Electrodiagnostic support for nerve entrapment. Foot Ankle 1993;14:129-135.
Question 91
- A 30-year-old man underwent replantation of his dominant thumb at the metacarpophalangeal joint level 2 days ago. Since replantation, the temperature of the thumb has been between 87.8 F (31 C) and 93.2 F (34 C). The temperature is now 82.4 F (28 C), and there is brisk capillary refill and venous engorgement. Management at this time should include
Explanation
Question 92
Reconstruction of the injured structure is performed. After surgery, the patient initially notes limitation in motion, and later develops recurrent instability of the knee. Which factor most likely contributed to the development of instability?
Explanation
The anteromedial bundle originates on the anterior and proximal aspect of the lateral femoral condyle and inserts on the anteromedial aspect of the anterior cruciate ligament (ACL) footprint on the proximal tibia. The posterolateral bundle originates posterior and distal to 63 the anteromedial bundle and inserts on the posterolateral aspect of the tibial footprint. The fibers are parallel when the knee is in an extended position. As the knee moves into flexion,
the fibers of the anteromedial bundle rotate externally with respect to the posterolateral bundle. The anteromedial bundle is tensioned in both flexion and extension. The posteromedial bundle is tensioned in extension, but relaxes as the knee moves into flexion.
The lateral meniscus is more commonly injured with an acute injury to the ACL. The medial meniscus is injured more commonly when the ACL is chronically unstable.
The ACL is an intra-articular and intrasynovial structure. It is innervated by posterior articular branches from the tibial nerve. Innervation of the ACL involves several types of mechanoreceptors (Ruffini, Pacini, Golgi tendon, and free-nerve endings) that may contribute to proprioceptive function of the knee and modulation of quadriceps function.
Injury to the ACL is predominantly associated with instability to anterior translation of the tibia in extension. The ACL plays a secondary role to limit internal rotation of the tibia, and a loss of ACL stability is confirmed by the reduction of the tibia from a position of anterior translation and internal rotation (pivot shift). The radiographs demonstrate anterior placement of the femoral tunnel. The convex shape of the lateral femoral condyle can make it more difficult to visualize the anatomic femoral origin of the ACL. Failure to identify the
anatomic footprint can result in anterior placement of the femoral tunnel. Anterior ACL graft placement can result in its impingement against the posterior cruciate ligament and early limitation of knee flexion. Over time, impingement on the graft may result in stretching of the graft and recurrent knee instability symptoms.
RECOMMENDED READINGS
Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. Epub 2005 Oct 19. Review. PubMed PMID: 16235056. View Abstract at PubMed
Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Oct;14(10):982-92. Epub 2006 Aug 5. Review. PubMed PMID: 16897068. View Abstract at PubMed
Question 93
When treating a stable 2-part intertrochanteric hip fracture with a sliding hip screw construct, what is the minimum amount of screw holes that are needed in the side plate for successful fixation?

Explanation
The referenced article by Bolhofner et al reviews a series of 69 patients with a sliding hip screw and two hole side plate and notes that they did not have any failure of the side plate construct.
The referenced article by McLoughlin et al is a biomechanical evaluation of 2 versus 4 hole plates and found that peak load in the failure test was not found to be statistically different between the two-hole and four-hole designs. In cyclic testing, the two-hole configuration exhibited statistically smaller fragment migration in both shear and distraction than the four-hole design.
Question 94
Figures 1 through 3 are the weight-bearing radiograph and MRI scans of a 27-year-old man who twisted his knee coming down awkwardly from a lay-up during a basketball game. He felt a sharp stabbing pain in the posterior aspect of his knee at the time of the injury. Physical examination reveals a trace effusion, full range of motion but pain with hyperflexion >90° degrees and tenderness over the affected joint line. What is the most appropriate treatment at this time?

Explanation
root tears lead to progressive degenerative changes as a result of the altered tibiofemoral contact pressures and areas. Nonsurgical treatment including injections, physical therapy, and unloader braces are more appropriate in the older patient with pre-existing advanced degenerative changes.
Question 95
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action should be
Explanation
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosement, IL, American Academy of Orthopaedic Surgeons, 1997, pp 181-189.
Rockwood CA Jr, Thomas SC, Matsen FA III: Subluxations and dislocations about the glenohumeral joint, in Rockwood CA Jr, Green DP, Bucholz RW (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, vol 1, pp 1058-1065.
Question 96
Which repair technique for an osteochondral lesion of the medial talus shoulder produces hyaline cartilage that is similar to native cartilage and will not degrade over time?
Explanation
Autologous osteochondral transplantation (typically involving tubular grafts harvested from the knee) has been shown to replace a talar defect with viable hyaline cartilage. The results over the medium term show good clinical outcomes, and MRI studies reveal cartilage repair similar to native cartilage. Chondroplasty and arthroscopic bone-marrow stimulation are both associated with good clinical results for smaller lesions, but these techniques develop fibrocartilaginous repair tissue composed of type I collagen instead of hyaline cartilage. Osteochondral transplantation of fresh allografts performed less than 14 days after harvest contains high chondrocyte viability. Few clinical studies report long-term results, but radiographic studies demonstrate high rates of collapse and resorption. Joint space narrowing has been noted in 60% of ankles treated with bulk grafts after an average of 44 months. Autologous chondrocyte implantation (both periosteum-covered and matrix-associated techniques) has been shown to create hyaline cartilage in some studies, but fibrocartilage creation has been reported in others.
RECOMMENDED READINGS
Schachter AK, Chen AL, Reddy PD, Tejwani NC. Osteochondral lesions of the talus. J Am Acad Orthop Surg. 2005 May-Jun;13(3):152-8. Review. PubMed PMID: 15938604. View Abstract at PubMed
Mitchell ME, Giza E, Sullivan MR. Cartilage transplantation techniques for talar cartilage lesions. J Am Acad Orthop Surg. 2009 Jul;17(7):407-14. Review. PubMed PMID: 19571296. View Abstract at PubMed
Murawski CD, Kennedy JG. Operative treatment of osteochondral lesions of the talus. J Bone Joint Surg Am. 2013 Jun 5;95(11):1045-54. doi: 10.2106/JBJS.L.00773. Review. PubMed PMID: 23780543. View Abstract at PubMed
Question 97
A 45-year-old woman with stage II posterior tibial tendinitis has failed to respond to nonsurgical management. Recommended treatment now includes posterior tibial tendon debridement and medial calcaneal displacement osteotomy along with transfer of what tendon?
Explanation
REFERENCES: Sitler DF, Bell SJ: Soft tissue procedures. Foot Ankle Clin 2003;8:503-520.
Guyton GP, Jeng C, Krieger LE, et al: Flexor digitorum longus transfer and medial displacement calcaneal osteotomy for posterior tibial tendon dysfunction: A middle-term clinical follow-up. Foot Ankle Int 2001;22:627-632.
Question 98
The histology of the lesion is shown in Figure 101d. What is the most likely complication after treatment of this lesion?
Explanation
The MRI scans show a well-circumscribed inhomogenous mass at the anterior ankle joint consistent with a diagnosis of pigmented villonodular synovitis (PVNS), not an anatomic variant. An inflammatory mass,such as the pannus of rheumatoid arthritis, would reveal moderate signal intensity with relatively uniform signal throughout. The mass is well encapsulated, respecting tissue boundaries and not showing invasive characteristics as malignancies would. The arthroscopic image is also consistent with the reddish-brown frond-like tissue of PVNS. PVNS of the ankle can be treated arthroscopically. If this mode of treatment is chosen, a tissue sample should be sent to pathology for microscopic analysis; débridement should be performed on the remaining tissue. Removal of the instrumentation without débridement will not provide treatment and will result in disease progression. Tourniquet placement does not provide therapeutic benefit.
Brachytherapy has not been described for the treatment of PVNS of the ankle. The histologic image shows multiple multinucleated giant cells, hemosiderin, and very few mitotic figures – consistent with a diagnosis of PVNS. A common complication of PVNS treatment is local recurrence. Arthrofibrosis and chondrolysis are not seen with proper surgical care of these patients. Because this is not an infectious lesion, disseminated infection after treatment is highly unlikely. PVNS rarely metastasizes.
RESPONSES FOR QUESTIONS 104 THROUGH 106
Toe is fused too straight (plantar flexed)
Toe is fused in too much valgus
Toe is fused in too much dorsiflexion
There is a nonunion of the fusion
Excessive shortening of the first metatarsal during preparation for fusion What is the most likely diagnosis for each patient?
Question 99
A 20-year-old football player sustains a dorsiflexion external rotation injury to his right ankle. During sideline evaluation, which of the following findings best indicates a syndesmosis ankle sprain without diastasis?
Explanation
REFERENCES: Nussbaum ED, Hosea TM, et al: Prospective evaluation of syndesmosis ankle sprains without diastasis. Am J Sports Med 2001;29:31-35.
Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1985;23:746-750.
Amendola A: Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle 1992;13:44-50.
Question 100
A 61-year-old man reports right shoulder pain and loss of external rotation since having a seizure 5 months ago. MRI scans are shown in Figures 82a and 82b. What is the most appropriate treatment? Review Topic
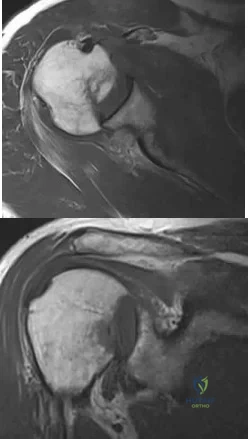
Explanation
