Orthopedic Board Review MCQs: Knee, Shoulder & Foot/Ankle Arthroplasty | Part 256

Key Takeaway
This page offers an interactive MCQ set for orthopedic residents and surgeons preparing for OITE/AAOS board certification. It features 100 high-yield, verified questions mirroring exam format, with detailed clinical explanations and references in study and exam modes. Ideal for comprehensive prep.
About This Board Review Set
This is Part 256 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 256
This module focuses heavily on: Ankle, Arthroplasty, Foot, Infection, Knee, Ligament, Revision, Shoulder.
Sample Questions from This Set
Sample Question 1: A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant...
Sample Question 2: A patient underwent anterior stabilization of the shoulder 6 months ago, and examination now reveals lack of external rotation beyond 0°. The patient has a normal apprehension sign and normal strength, and the radiographs are normal. Based ...
Sample Question 3: A 63-year-old man with type I diabetes mellitus who underwent open forefoot amputation now has a high fever, and an elevated WBC count and blood glucose levels. Repeat laboratory studies the day after surgery show a WBC count of 9,500/mm 3 ...
Sample Question 4: Which of the following surgical devices employed for stabilization of the sternoclavicular joint is associated with the highest incidence of life-threatening complications?...
Sample Question 5: A 73-year-old man has stiffness after undergoing primary posterior cruciate ligament-retaining total knee arthroplasty 18 months ago. Extensive physiotherapy, dynamic splinting, and manipulations under anesthesia have failed to result in im...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal.
Explanation
Question 2
A patient underwent anterior stabilization of the shoulder 6 months ago, and examination now reveals lack of external rotation beyond 0°. The patient has a normal apprehension sign and normal strength, and the radiographs are normal. Based on these findings, the patient is at greater risk for the development of
Explanation
REFERENCES: Hawkins RJ, Angelo RL: Glenohumeral osteoarthritis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993, pp 98-116.
Question 3
A 63-year-old man with type I diabetes mellitus who underwent open forefoot amputation now has a high fever, and an elevated WBC count and blood glucose levels. Repeat laboratory studies the day after surgery show a WBC count of 9,500/mm 3 , a serum albumin level of 1.9 g/dL, and a total lymphocyte count of 1,900/mm 3 . Examination reveals that he is afebrile, and his blood glucose level is now normal. An ultrasound Doppler of the dorsalis pedis artery shows an ankle-brachial index of 0.6. A transcutaneous partial pressure measurement of oxygen at the ankle joint shows a level of 38 mm Hg. What is the best course of action?
Explanation
REFERENCE: Pinzur MS, Stuck RM, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Question 4
Which of the following surgical devices employed for stabilization of the sternoclavicular joint is associated with the highest incidence of life-threatening complications?
Explanation
REFERENCES: Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.
Lyons FA, Rockwood CA Jr: Migration of pins used in operations of the shoulder. J Bone Joint Surg Am 1990;72:1262-1267.
Question 5
A 73-year-old man has stiffness after undergoing primary posterior cruciate ligament-retaining total knee arthroplasty 18 months ago. Extensive physiotherapy, dynamic splinting, and manipulations under anesthesia have failed to result in improvement. Examination reveals range of motion from 30 degrees to 60 degrees of flexion. The components are well fixed, and the evaluation for infection is negative. In discussing the possibility of revision arthroplasty, the patient should be advised that
Explanation
REFERENCES: Babis GC, Trousdale RT, Pagnano MW, et al: Poor outcomes of isolated tibial insert exchange and arthrolysis for the management of stiffness following total knee arthroplasty. J Bone Joint Surg Am 2001;83:1534-1536.
Nicholls DW, Dorr LD: Revision surgery for stiff total knee arthroplasty. J Arthroplasty 1990;5:S73-S77.
Haidukewych GJ, Jacofsky DJ, Pagnano MW, et al: Functional results after revision of well-fixed components for stiffness after primary total knee arthroplasty. J Arthroplasty 2005;20:133-138.
Question 6
What is the structure indicated by the letter “A” in Figure A? Review Topic
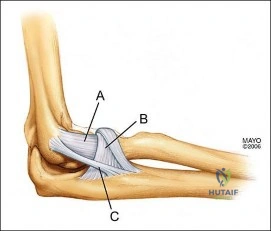
Explanation
Question 7
A 27-year-old woman with Down syndrome has a severe bunion with pain and deformity in the left forefoot. Nonsurgical management has failed to provide relief. She does not use any assistive ambulatory devices. A radiograph is shown in Figure 21. Treatment should now consist of
Explanation
REFERENCES: Coughlin MJ, Abdo RV: Arthodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
Mann RA: Disorders of the first metatarsophalangeal joint. J Am Acad Orthop Surg 1995;3:34-43.
Question 8
An otherwise healthy 45-year-old man has a 3-cm subcutaneous mass on his anterior thigh that is presumed to be a lipoma. Removal of the mass is performed in the office of his primary care physician. Pathologic evaluation shows a high-grade malignant fibrous histiocytoma. Staging reveals no evidence of metastatic disease. Management at this time should consist of
Explanation
REFERENCES: Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173.
Giuliano AE, Eilber FR: The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J Clin Oncol 1985;3:1344-1348.
Lewis JJ, Leung D, Espat J, Woodruff JM, Brennan MF: Effect of resection in extremity soft tissue sarcoma. Ann Surg 2000;231:655-663.
Noria S, Davis A, Kardel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 9
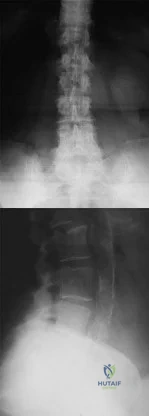
Figure 31 is the abdominal radiograph of a 70-year-old woman who experiences nausea and abdominal tightness 48 hours following left total knee arthroplasty performed under general anesthesia. She received 24 hours of cefazolin antibiotic prophylaxis and a patient-controlled analgesia narcotic pump for pain management. She has been receiving warfarin for thromboembolic prophylaxis. Her severe abdominal distension and markedly decreased bowel sounds are most likely secondary to
Explanation
The radiograph reveals severe intestinal dilatation, which has occurred as the result of acute colonic pseudo-obstruction and is associated with excessive narcotic administration following total joint arthroplasty. Anesthetic type, antibiotic administration, and warfarin have not been associated with this obstruction. Electrolyte imbalances such as hypokalemia have been associated with postsurgical acute colonic pseudo-obstruction.

CLINICAL SITUATION FOR QUESTIONS 32 THROUGH 35
Figures 32a through 32c are the radiographs of a 30-year old man who is experiencing right hip pain. He has no current medical problems, but, with a body mass index of 41, he is morbidly obese. He was previously treated for leukemia with chemotherapy that included
high-dose steroids. He undergoes total hip arthroplasty (THA) with a ceramic-on-ceramic bearing.
Question 10
A 13-year-old girl has had pain in her ankle and difficulty with sporting activities for the past 6 months. Nonsteroidal anti-inflammatory drugs and use of a short leg cast have provided minimal relief. A radiograph and MRI scan are shown in Figures 43a and 43b. What is the next most appropriate step in treatment?
Explanation
REFERENCES: McCormack TJ, Olney B, Asher M: Talocalcaneal coalition resection: A 10-year follow-up. J Pediatr Orthop 1997;17:13-15.
Thometz J: Tarsal coalition. Foot Ankle Clin 2000;5:103-118.
Question 11
The specificity of intraoperative frozen sections obtained for the evaluation of infected total hip arthroplasty may be improved by
Explanation
On the basis of cultures of specimens obtained at the time of the revision surgery, 19 of the 175 patients were considered to have an infection. Of the 152 patients who had negative frozen sections, three were considered to have an infection on the basis of the results of the final cultures. Of the 23 patients who had positive frozen sections, 16 were considered to have an infection on the basis of the results of the final cultures; all 16 had frozen sections that showed at least 10 polymorphonuclear leukocytes per high-powered field.
The sensitivity and specificity of the frozen sections were similar regardless of whether an index of 5 or 10 polymorphonuclear leukocytes per high-powered field was used. Analysis of the frozen sections had a sensitivity of 84% for both indices, whereas the specificity was 96% when the index was 5 polymorphonuclear leukocytes and 99% when it was 10 polymorphonuclear leukocytes. However, the positive predictive value of the frozen sections increased significantly (P < 0.05), from 70% to 89%, when the index increased from 5 to 10 polymorphonuclear leukocytes per high-powered field. The negative predictive value of the frozen sections was 98% for both indices. At least 10 polymorphonuclear leukocytes per high-powered field was predictive of infection, while 5 to 9 polymorphonuclear leukocytes per high-powered field was not necessarily consistent with infection. Less than 5 polymorphonuclear leukocytes per high-powered field reliably indicated the absence of infection.
REFERENCES: Feldman DS, Lonner JH, Desai P, Zuckerman JD: The role of intraoperative frozen sections in revision total joint arthroplasty. J Bone Joint Surg Am 1995;77:1807-1813.
Lonner JH, Desai P, Dicesare PE, Steiner G, Zuckerman JD: The reliability of analysis of intraoperative frozen sections for identifying active infection during revision hip or knee arthroplasty. J Bone Joint Surg Am 1996;78:1553-1558.
Spangehl MJ, Younger AS, Masri BA, Duncan CP: Diagnosis of infection following total hip arthroplasty, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 285-295.
Della Valle CJ, Bogner E, Desai P: Analysis of frozen sections of intraoperative specimens obtained at the time of reoperation after hip or knee resection arthroplasty for the treatment of infection. J Bone Joint Surg Am 1999;81:684-689.
Question 12
Figures 1 and 2 show the radiograph and CT obtained from a 78-year-old woman who underwent right total hip replacement in 1995. She initially did well with no pain. She was last seen 7 years ago and was having mild hip pain at that time. She was found to have a supra-acetabular cyst on radiographs. She has had severe right hip pain for the past 9 months while using a walker for ambulation. The initial blood work reveals an estimated erythrocyte sedimentation rate of 32 mm/hr, a C-reactive protein level of 0.5 mg/L, a serum cobalt level of 0.4 µg/L, and a serum chromium level of 0.6 µg/L. Right hip aspiration is performed, revealing a white blood cell count of 139, 52% neutrophils, and a negative leukocyte esterase test. What is the best next step?
Explanation
The hip replacement was performed in 1995, during the period when the previous generation of polyethylene was utilized. This polyethylene was subjected to irradiation in air, with subsequent oxidation and consequent osteolysis after implantation. The mechanism of osteolysis begins with the uptake of polyethylene particles by macrophages, which then initiate an inflammatory cascade and the release of osteolytic factors. This cycle continues, with eventual implant loosening and failure. The imaging shows significant osteolysis and raises concern for pelvic discontinuity and acetabular implant failure. The surgical treatment consists of acetabular reconstruction. In this patient, concern exists for discontinuity based on the substantial amount of bone loss and nonsupportive anterior and posterior columns. This scenario requires complex acetabular revision using a custom triflange device, distraction with a jumbo acetabular component, or placement of a porous metal cup/cage construct with augmentation. The laboratory values are not consistent with infection or failure due to metal debris.
Question 13
Mirror therapy is indicated for which of the following clinical conditions?
Explanation
Under mirror therapy, a patient is allowed to feel the imaginary movement of the removed body part behaving as normal body movement through a mirror. The mirror
image of the normal body part helps reorganize and integrate the mismatch between proprioception and visual feedback of the amputated segment.
Tilak et al. performed a randomized controlled trial of 26 patients with phantom limb pain, and found that mirror therapy as well as transcutaneous electrical nerve stimulation both significantly improved pain scores, but no difference was seen between the two groups. They recommend use of both modalities in treatment of phantom limb pain, as they are noninvasive and inexpensive.
Chan et al. reviewed 22 patients utilizing mirror therapy for amputation related phantom limb pain, and found that patients reported a significant decrease in pain when utilizing this treatment modality as compared to covered mirror therapy or mental imagery therapy.
Illustration A shows a patient with an upper extremity amputation using a mirror to perform movements during a mirror therapy session.
Incorrect Answers:
Question 14
-Figure is the radiograph of a 55-year-old veteran who developed avascular necrosis after a traumatic hip dislocation. He was treated with hemiarthroplasty 10 years ago and also has posttraumatic stress disorder and chronic pain. He has had multiple spinal surgeries and takes 30 mg of methadone daily. He now has severe groin pain and is unable to ambulate. Laboratory studies showed a C-reactive protein level of 0.2 mg/L (reference range, 0-3 mg/L), erythrocyte sedimentation rate of 50 mm/h (reference range, 0-20 mm/h), hip aspiration of 500/mm3 white blood cell count, 50% polynucleated cells, 30%monocytes, and 20% lymphocytes What is the most likely cause of his hip pain?
Explanation
Question 15
A 10-year-old boy reports a gradual onset of weakness; however, he is fully ambulatory. History reveals that he has a 17-year-old brother who has just stopped walking because of a similar condition. Laboratory studies show a creatine kinase level of 5,480 IU/L (normal 25 to 232 IU/L), and examination shows a slightly positive Gower sign. What is the most likely diagnosis?
Explanation
REFERENCES: Matsuo M: From molecular diagnosis to gene therapy. Brain Dev 1996;18:167-172.
Darras BT: Molecular genetics of Duchenne and Becker muscular dystrophy. J Pediatr 1990;117:1-15.
Gutmann DH, Fischbeck KH: Molecular biology of Duchenne and Becker’s muscular dystrophy: Clinical applications. Ann Neurol 1989;26:189-194.
Question 16
A football player sustains a traumatic anterior inferior dislocation of the shoulder in the last game of the season. It is reduced 20 minutes later in the locker room. The patient is neurologically intact and has regained motion. If the patient undergoes arthroscopic evaluation, what finding is seen most consistently?
Explanation
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Bottoni CR, Wilckens JH, DeBerardino TM, et al: A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic,
first-time shoulder dislocations. Am J Sports Med 2002;30:576-580.
Question 17
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Explanation
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 18
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
REFERENCES: Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 2002;23:896-901.
Question 19
Figures 1 and 2 are the radiographs of a 35-year-old right-hand-dominant man who has had progressive right wrist pain for 1 year. There is no history of trauma, and he has had no treatment to date. He reports some pain at rest with limited motion and substantial pain with use. He is currently out of work on short-term disability because of this wrist problem. An examination reveals mild dorsal wrist swelling, decrease wrist range of motion, and decreased grip strength. Contralateral wrist examination findings are normal. What is the most appropriate course of treatment?

Explanation
This patient has late-stage Kienböck disease. According to the Lichtman classification for Kienböck disease, this would represent stage IIIB, with lunate collapse/fragmentation, loss of carpal height secondary to proximal capitate migration, and a flexed scaphoid. The lateral radiograph reveals a radioscaphoid angle exceeding 60 degrees, so disease stage is IIIB. According to Condit and associates, when the presurgical radioscaphoid angle exceeds 60 degrees, results are poor when an attempt to maintain the lunate is made. As a result, the procedure with the most predictable outcome is a proximal row carpectomy. A radial-shortening osteotomy could be performed because the ulnar variance is negative. Considering the marked lunate fragmentation and collapse, a vascularized bone graft likely is contraindicated and associated with less predictable results than a proximal row carpectomy. There is no role for supervised hand therapy and splinting in the setting of advanced Kienböck disease. Similarly, there is no role for maintenance of the lunate in the setting of advanced collapse and fragmentation.
Question 20
A 30-year-old patient underwent open reduction internal fixation of a talar neck fracture 8 weeks ago. His current radiographs demonstrate a subchondral radiolucency of the dome of the talus. What is the next most appropriate course of action?

Explanation
Question 21
The condition seen in Figure 60 is attributable to

Explanation
Cephallomedullary implants for treatment of proximal femur fractures have gained in popularity over the last decade. Although these implants have improved outcomes for certain fracture types, multiple complications are associated with this implant. Failure may occur secondary to implant design (for example, mismatch of curvature of the nail to the femur, which can result in distal anterior cortical perforation).
RECOMMENDED READINGS
Bazylewicz DB, Egol KA, Koval KJ. Cortical encroachment after cephalomedullary nailing of the proximal femur: evaluation of a more anatomic radius of curvature. J Orthop Trauma. 2013 Jun;27(6):303-7. doi: 10.1097/BOT.0b013e318283f24f. PubMed PMID: 23287752.
View Abstract at PubMed
Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2008 Jul 16;(3):CD000093. doi: 10.1002/14651858.CD000093.pub4. Review. Update
in: Cochrane Database Syst Rev. 2010;(9):CD000093. PubMed PMID: 18646058. View Abstract at PubMed
Question 22
A 52-year-old man has shoulder pain and stiffness after undergoing a “mini-lateral” rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/ mm 3 (normal 3,500 to 10,500/ mm 3 ) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
Explanation
REFERENCES: Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121.
Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 23
What is the most common complication following total disk arthroplasty in the lumbar spine?
Explanation
REFERENCE: Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 24
Citrate dextrose - anticoagulant used with whole blood during the process of preparation of the PRP before centrifugation. 3,4,5) TGF-beta, IL-8, and PDGF are all proteins released by the platelets upon activation.
Explanation
Arrington et al reviewed 414 consecutive iliac crest harvest procedures and reported a 10% rate of minor complications and 5.8% of major complications (deep infection, nerve injuries, herniation, fractures, hematomas). They note that with proper surgical technique, the incidence of the complications can be minimized.
Ahlmann et al compared the morbidity related to the harvest of anterior iliac crest bone graft with that related to the harvest of posterior iliac crest bone graft and to determine differences in functional outcome. The rates of both minor complications (p = 0.006) and all complications (p = 0.004) were significantly higher after the anterior harvest procedures than they were after the posterior procedures. The postoperative pain at the donor site was significantly more severe (p = 0.0016) and of significantly greater duration (p
= 0.0017) after the anterior harvests.
Which of the following statements is inaccurate in describing the origin and purpose of the Institutional Review Boards (IRB)?
Began with the Nuremberg Code of Medical Ethics, which was developed by the Nuremberg Military Tribunal after the investigation of Nazi physicians
Fetuses, pregnant women, and children are considered vulnerable populations but prisoners are not
Emphasizes dignity and autonomy, and encompasses informed consent (quid vide)
The process for obtaining informed consent for patients included in clinical trials is mandated by the Institutional Review Board (IRB).
Requires fair selection of subjects and equal distribution of the benefits and burdens of research
Fetuses, pregnant women, prisoners, and children are all considered vulnerable populations by Institutional Review Boards (IRB). The process for obtaining informed consent for patients included in clinical trials is mandated by the IRB.
The article by Fisher is a commentary that reviews the clinical trials industry. She urges researchers to communicate the larger details of the research enterprise to patients and to compensate for asymmetrical power relations in society as a whole. Without these things, she believes, it will be impossible to protect against misunderstandings and therapeutic misconceptions.
Which of the following best describes a Bonferroni correction?
An analysis that starts with a particular probability of an event (the prior probability) and incorporates new information to generate a revised probability (a posterior probability)
Human behavior that is changed when participants are aware that their behavior is being observed.
Used to assess the relationship between two normally distributed continuous variables
A post-hoc statistical correction made to P values when several dependent
or independent statistical tests are being performed simultaneously on a single data set
The ability of a study to detect the difference between two interventions if one in fact exists
A Bonferroni correction is a post-hoc statistical correction made to P values when several dependent or independent statistical tests are being performed simultaneously on a single data set.
To perform a Bonferroni correction, divide the critical P value (alpha level) by the number of comparisons being made. For example, if 10 hypotheses are being tested, the new critical P value would be (alpha level)/10. The statistical power of the study is then calculated based on this modified P value.
Guyatt et al. discusses hypothesis testing and the role of alpha levels and P values. They report that the Bonferroni correction is derived from testing a dependent or independent hypotheses on a set of data and finding that the probability of a type I error is offset by testing each hypothesis at a statistical significance level divided by the number of times what it would be if only one hypothesis were tested.
Incorrect Answers:
A 10-year-old child falls from a standing height and sustains the injury shown in Figure A. Her medical history includes hearing defects and the facial appearance shown in Figure B. In addition to operative fixation of her fracture she is scheduled to receive cyclical intravenous
pamidronate administration as a treatment after the fracture is healed. Which of the following is associated with this form of treatment?
No change in bone pain
No change in future fracture incidence
An increase in osteoblast density
An increased risk of secondary osteosarcoma
An increase in bone density
The history and images are consistent with osteogenesis imperfecta (OI). Olecranon avulsion fractures are often seen in patients with OI and children presenting with these should be evaluated for OI. The clinical image of blue sclera can also be a characteristic finding in patients with OI. The Bisphosphonates have been shown to decrease fracture incidence and bone pain while improving bone density and overall function in OI patients.
Zeitlin et al performed a Level 5 review of OI. They state that Sillence Types I through IV are a mutation in the COL1A1 and COL1A2 genes that encode type I collagen. They report that cyclical intravenous pamidronate administration reduces bone pain and fracture incidence, and increases bone density and
level of ambulation.
Burnei et al also performed a Level 5 review of OI. They report that the use of bone marrow transplantation to increase osteoblast density in OI patients is currently being
researched as a potential treatment of OI.
A 35-year-old male presents with pain and limited range of motion 3 months after arthroscopic Bankart repair of his right shoulder. His postoperative course included a continuous intra- articular infusion pump for 3 days, use of a sling for 4 weeks, and initiation of passive range of motion below the level of the shoulder. At 4 weeks postoperatively he started active range of motion exercises, and started an isotonic strengthening program at the 9 week interval. Which of the following options is the MOST appropriate step in his management?
Reassurance and appropriate followup
Focused physical therapy on aggressive ROM exercises and modalities
Intra-articular injection of corticosteroids to decrease post-operative inflammation
Shoulder radiograph series to assess for chondrolysis
Arthroscopic vs open Bankart revision surgery for failed repair
The above patient was issued an intra-articular infusion of lidocaine for pain control after his surgery and may have developed shoulder chondrolysis. This complication after the use of intra-articular pumps has recently become more well known. The U.S. Federal drug and Administration (FDA) has issued a warning on the adminstration of continuous intra-articular infusion of local anesthestics for pain control.
The FDA has reviewed 35 cases of patients developing chondrolysis after intra- articular infusions, some being as early as 2 months after their surgery. The average time of diagnosis in these cases with chondrolysis were at an average of 8.5 months after the infusion. The majority of the reported cases occurred following shoulder surgeries. Joint pain, stiffness, and loss of motion were the most common physical complaints. As a result of their findings, the FDA issued
a warning for surgeons to be aware and monitor for signs and symptoms of chondrolysis.
Illustration A shows a radiograph consistent with chondrolysis in a patient status post arthroscopic Bankart repair. This image shows the loss of joint height in the glenohumeral joint due to chondrolysis. Also, 2 suture anchors are visible as well in the glenoid from the Bankart repair. Illustration B shows an arthroscopic image of chondrolysis and Illustrations C and D demonstrate chondrolyis viewed from an open approach.
Regarding bone densitometry, a T-score of -3.5 is defined as which of the following?
Normal bone
Osteopenia
Age appropriate bone loss
Osteoporosis
None. One cannot make this diagnosis without further information.
A T-score of -3.5 is defined as osteoporosis, regardless of the other clinical factors.
As described in the review by Kanis et al., the World Health Organization (WHO) has defined the following categories based on bone density in white women:
Normal bone: T-score greater than -1 Osteopenia: T-score between -1 and -2.5 Osteoporosis: T-score less than -2.5
The WHO committee did not have enough data to create definitions for men or other ethnic groups. T-score is a comparison of a patient's BMD to that of a healthy thirty-year- old of the same sex and ethnicity. Z-score is the number of standard deviations a patient's BMD differs from the average BMD of their age, sex, and ethnicity.
A 67-year-old female presented 2 months ago to her primary care physician with left sided thigh pain. A radiograph was taken at that time and is shown in Figure A. She was diagnosed at that time with a quadriceps strain and given a prescription for ibuprofen and physical therapy. She is now in the emergency room with severe left thigh pain and inability to bear weight on the left lower extremity after bending down to tie her shoes. She denies any constitutional symptoms. A current radiograph from the emergency room is shown in Figure B. Which of the following most likely explains this patient's fracture?
Long-term corticosteroid use
Secondary malignancy arising from Paget disease
Long-term alendronate use
Long-term ergocalciferol use
Short-term teraparatide use
Subtrochanteric stress reaction (Figure A) and low-energy transverse fracture (Figure B) is a complication of long-term bisphosphonate use documented in the literature. Of note, a healed right sided subtrochanteric femur fracture is also visualized in Figure A.
Neviaser et al conducted a Level 4 study of 70 patients with low energy femur fractures. They found that a simple, transverse pattern and hypertrophy of the diaphyseal cortex are associated with alendronate use with 98% specificity. They report that the average alendronate usage time was 6.9 years in patients exhibiting this pattern of fracture.
Capeci et al performed a Level 4 review of alendronate therapy and its association with unilateral low-energy subtrochanteric and diaphyseal femur fractures. They recommended consideration of discontinuing alendronate with the consultation of an endocrinologist if a fracture occurs. They also recommend routine contralateral leg surveillance after to rule out contralateral stress fracture. If contralateral stress fracture is found, it it is recommended that it is treated with prophylactic intramedullary fixation.
Imaging typically shows lateral cortical thickening in the subtrochanteric femur as demonstrating on the coronal and axial CT scans shown in Illustration A and B, respectively.
In the study by Moseley et al published in the New England Journal of Medicine, 180 patients with knee osteoarthritis were randomly assigned via sealed envelope to receive arthroscopic débridement, arthroscopic lavage, or placebo surgery. Outcomes were assessed by blinded evaluators at several points over a 2 year period
with the use of five self-reported pain and function scores. There was a greater than 90% follow-up in the study. This study is best described as having which level of evidence?
Therapeutic study, evidence level I
Therapeutic study, evidence level II
Diagnostic study, evidence level I
Diagnostic study, evidence level II
Prognostic study, evidence level I
Therapeutic studies investigate the results of treatment. Level 1 evidence includes randomized controlled trial with statistically significant difference or no statistically significant difference but narrow confidence interval.
A level II therapeutic study would include a lesser-quality randomized controlled trial (eg,
<80% follow-up, no blinding, or improper randomization). A non-randomized prospective cohort study that compares the results of treatment or systematic reviews of level II studies or level I studies with heterogenous results would also be considered a level II study.
Prognostic studies investigate the effect of a patient characteristic on the outcome of disease. Diagnostic studies investigate the efficacy of a diagnostic test. Illustration A is a table detailing the levels of evidence.
A clinical trial is underway for patients with wrist extensor tendinitis. One group of 100 patients are treated with short arm casting. Another group of 100 patients are treated with physical therapy. During analysis of the results, it becomes apparent that 30 patients in the physical therapy group did not complete the full course of physical therapy. Despite not completing a full course of physical therapy, these 30 patients were included in the physical therapy group for analysis. This analysis is an example of which of the following?
Per-protocol
Crossover analysis
Intent-to-treat
Bayesian analysis
Effect size
The following is an example of intent-to-treat analysis.
The intent-to-treat approach aims to keep similar groups similar by not
allowing for patient selection based on post-randomization outcomes (including failure to comply with the protocol). This type of analysis ensures the power of randomization so that important unknown variables that impact outcome are likely to be dispersed equally in each comparison group. Conversely, a per- protocol comparison in a clinical trial excludes patients who were not compliant with the protocol guidelines.
Berger et al., in a Level 5 review, discuss many of the principles beyond randomization that are critical for preserving the comparability of the different groups. They report that masking, allocation concealment, restrictions on the randomization, adjustment for prognostic variables, and the intent-to-treat approach to data analysis are important features of designing a good clinical trial.
Incorrect Answers:
guidelines
A 32-year-old male is being seen in your office for evaluation of a possible rotator cuff tear. He has been seen in your office by one of
your partners previously after surgical treatment of a femoral shaft fracture. How much time has to pass since last evaluation or treatment in your group for this patient to revert to a new patient under CPT guidelines?
6 months
1 year
18 months
2 years
3 years
By CPT definition, a new patient is “one who has not received any professional services from the physician, or another physician of the same specialty who belongs to the same group practice, within the past three years.” By contrast, an established patient has received professional services from the physician or another physician in the same group and the same specialty within the prior three years.
The referenced study by Shalowitz reviewed 500 Medicare claims and found an overall coding error rate of 32.4%, with high levels of consultation coding errors. He reports that changing ambulatory consultation codes to those for new patient visits would save Medicare $534.5 million per year.
As a result of this study, as well as others, Medicare does not recognize consultation codes.
A 55-year-old healthy female presents for a routine physical exam. When discussing bone health and osteoporosis prevention, what dose of calcium and vitamin D should be recommended for daily consumption?
1,500mg of calcium and 1,000 IUs of vitamin D
2,200mg of calcium and 1,000 IUs of vitamin D
750mg of calcium and 5,000 IUs of vitamin D
750mg of calcium and 10,000 IUs of vitamin D
2,200mg of calcium and 5,000 IUs of vitamin D
The National Osteoporosis Foundation recommends a daily intake of 1,200- 1500mg of calcium 800-1,000 IUs of vitamin D for adults over the age of 50.
The review article by Gehrig et al discusses the factors surrounding osteoporosis that can be modified to optimize fracture risk reduction. They report that non-prescription interventions such as calcium and vitamin D supplementation, fall prevention, hip protectors, and balance and exercise programs are treatment options.
What is the function of the core binding factor alpha-1 (Cbfa1/Runx2)?
Phosphorylation and intracellular activation of signal transducers and activators of transcription (STATs)
Chemotaxis of mesenchymal stem cells to sites of skeletal fractures
Tumor-induced osteolysis
Osteoclastic apoptosis
Osteoblastic differentiation
As described by Ducy et al., Cbfa1/Runx2 is a key transcription factor associated with osteoblast differentiation, skeletal morphogenesis, and acts as a scaffold for nucleic acids and regulatory factors involved in skeletal gene expression. A stop codon mutation in the Cbfa 1 gene causes cleidocranial dysplasia. Stem cell chemotaxis (moving to various sites in the body) is accomplished through a variety of cytokines, one of which is platelet derived growth factor. Tumor-induced osteolysis occurs secondary to tumor-produced cytokine activation of osteoclasts. Osteoclastic apoptosis occurs secondary to bisphosphonates.
Ballock and O'Keefe review the development, growth, and complex cytokine interaction required for normal growth plate function.
A 20-year-old male is involved in motor vehicle collision and sustains a depressed tibial plateau fracture. When performing surgery, if calcium sulfate is used as the primary bone substitute void filler, an increase in which of the following outcomes may be expected as compared to autograft?
Increased complications due to serous drainage
Improved clinical outcomes as shown by more rapid time to healing
Improved clinical outcomes as shown by SF-36 scores
Increased complications due to autoimmune reactions and graft rejection
Equivalent complication rates and clinical outcomes
Calcium sulfate bone graft substitute has demonstrated an increased rate of serous drainage at the surgical site. Evidence examining the use of calcium sulfate in the treatment of bone nonunions revealed a significant failure rate, suggesting that this material, used in isolation, is not optimal to promote union in that setting.
Beuerlein and Mckee reviewed the literature, showing that calcium sulfate is
an effective void filler in metaphyseal defects after impacted fracture reduction (calcaneus, tibial plateau) or simple bone cysts. However, they report that calcium sulfate is associated with serous wound drainage especially when used at subcutaneous sites and in amounts greater than 20ml.
Ziran et al present a series of 41 patients undergoing bone grafting for atrophic/avascular nonunions with adjunctive calcium sulfate-demineralized bone matrix (Allomatrix). Of the 41 patients, 13 (32%) had drainage that necessitated surgical procedures and 14 (34%) developed a deep infection.
A 46-year-old female begins to have personality changes, cognitive decline, and chorea. Her father began having similar but less severe symptoms at age 55 before passing away 6 years later. One of her 2 older siblings has also begun to show deterioration. Which of the following describes the hereditary pattern of this disease?
Autosomal dominant with variable penetrance
Autosomal recessive with variable penetrance
X-linked recessive
Autosomal dominant with anticipation
Autosomal dominant with imprinting
This clinical vignette describes a patient with Huntington's disease. Huntington's disease has an autosomal dominant hereditary pattern with anticipation.
Anticipation is a term used to describe trinucleotide repeat
disorders that if passed on, will present earlier and more severely in affected subjects than in their affected parent. In Huntington's disease, it is due to a "CAG" trinucleotide repeat on chromosome 4. Subjects with an affected parent have a 50% chance of inheriting the disease from them, and if present will have more severe disease.
Deighton et al provide a review on the genetics of musculoskeletal disease including the hereditary pattern of anticipation.
All of the following are indications for locked plating technology EXCEPT:
Periarticular fracture with metaphyseal comminution
Fracture in osteoporotic bone
Bridge plating for severely comminuted fractures
Compression plating of transverse fracture
Plating of fractures where anatomical constraints prevent plating on the tension side of the bone
Locked plates are indicated for indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, bridging severely comminuted fractures, and the plating of fractures where anatomical constraints prevent plating on the tension side of the bone.
Locked plates and conventional plates rely on completely different mechanical principles to provide fracture fixation and in so doing they provide different biological environments for healing. Approaches to internal fixation have become more biologic. Greater emphasis is placed on vascularity and soft tissue integrity. Locked plates, analogous to rigid internal fixators, can provide relative stability favorable to secondary fracture healing. If applied appropriately, they can
avoid soft tissue compromise. The key to this new generation of plates is the locking mechanism of the screw to the plate, which provides angular stability and avoids compression of the plate to the periosteum. Favorable biomechanical and clinical results continue to expand the number of appropriate indications for use of locked plating devices, although exact indications for their use have yet to be precisely defined.
The referenced articles by Haidukewych and Egol et al are reviews of the biomechanical characteristics of locked plating technology.
Which of the following lists these materials in order of increasing modulus of elasticity?:
Cortical bone; Titanium; Cobalt-chrome; Stainless steel; Ceramic
Titanium; Cortical bone; Ceramic; Cobalt-chrome; Stainless steel
Cortical bone; Titanium; Stainless steel; Cobalt-chrome; Ceramic
Stainless steel; Titanium; Cortical bone; Ceramic; Cobalt Chrome
Cortical bone; Stainless steel; Titanium; Cobalt-chrome; Ceramic
Cortical bone has the lowest modulus of elasticity of the materials listed, followed by titanium, stainless steel, cobalt-chrome alloy, then ceramic.
Young's modulus of elasticity is the ratio of stress to strain, and represents the stiffness of a material and its ability to resist deformation when placed under tension. Of the materials listed, titanium has the stiffness closest to cortical bone. Ceramic has the highest modulus of elasticity, making it the most stiff of the materials listed.
Illustration A (from Miller's Review) shows the relative stiffnesses of various orthopaedically relevant materials. Young's modulus is the slope of the lines shown. Illustration B (Google images) charts their Young's Modulus.
Incorrect answers:
Which of the following substances increases the chondrogenic phenotype of intervertebral disk cells and matrix synthesis?
Osteoprotegrin
Osteonectin
Hyperosmotic saline
Corticosteroids
Bone morphogenic proteins
Bone morphogenic proteins have been shown to increase chondrogenic phenotype expression and increase matrix synthesis of the intervertebral disc in animal studies.
Bone morphogenetic protein-2, bone morphogenetic protein-7, and
transforming growth factor-beta are morphogens that have been shown to alter the phenotype of target cells without increasing cellular proliferation. Within the intervertebral disk, these factors have the potential to increase the chondrogenic phenotype among disk cells, and this results in the increased production of the disk matrix. Mitogenic molecules, such as insulin-like growth factor-1 and fibroblast growth factor, function to increase cellular proliferation.
Miyamoto et al. evaluated rabbits that underwent annulus fibrosus (AF) injury where they either injected a control or BMP into the nucleus pulposus. The BMP injection significantly restored disc height and improved the modulus as compared to control injections. They concluded the biochemical data suggested that the OP-1-induced restoration of the disc space was a consequence of the increased activity of anabolic pathways that resulted in biochemical changes in the IVD.
Kim et al. evaluated mRNA levels of BMP-2, BMP-7, and TGF-beta in a rabbit model of intervertebral discs. Compared to young rabbits, old rabbits generally had higher levels of mRNA expression of these three cytokines in both the annulus fibrosus and nucleus pulposus. The similar patterns of up-regulation in gene expression with age shown by these 3 anabolic cytokines suggest a common pathway in terms of regulation and transcription in the early stage of disc degeneration.
Incorrect Answers:
A colleague is struggling to obtain a perfect lateral radiograph for distal locking screw placement. Other than good technique, how might the surgeon best reduce the amount of radiation exposure to the patient and personnel when using fluoroscopy?
The use of continuous fluoroscopy while manipulating the leg
Standing directly behind the cathode ray tube
Advising the technician to position the fluoroscopy beam on command
Placement of the image intensifier receptor as close to the patient as possible
Placement of the cathode ray tube as close to the patient as possible
Placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
Numerous steps have been described to decrease radiation in the operating room. They include:
Decrease time of exposure
Decrease dose of exposure
Beam collimation
The use of mini C arm
Inverting the C arm (shortens distance between body part and collection surface)
Surgeon’s control of the C arm
Use of protective equipment (glasses, thyroid shields, aprons)
Increase the distance from the X ray source
Maniscalco et al. compared the amount radiation exposure during open lumbar microdiscectomy and minimally invasive microdiscectomy. MIS lumbar microdiscectomy cases expose the surgeon to significantly more radiation than open microdiscectomy.
Interestingly, standing in a substerile room during x- ray localization in open cases is not fully protective.
Illustration A shows an image of radiation scatter with fluoroscopy. Radiation hits the patient’s tissue, interacts and then changes direction. The greatest dose received is directly perpendicular to the fluoroscopy and next to the patient.
Incorrect Answers:
A 72-year-old active man presents with chronic right-sided pelvic pain for the last 2 years. His radiographs are depicted in Figure A. He has tried multiple courses of activity modification and anti- inflammatory medications to no avail. His orthopedic oncologist performs a biopsy (depicted in Figure B) and elects to initiate Zoledronate. Which of the following is a known complication
associated with this treatment if rendered long-term?
Malignant degeneration to osteosarcoma
Malignant degeneration to chondrosarcoma
Malignant degeneration to fibrosarcoma
Atypical distal femur transverse fractures
Osteonecrosis of mandible
This patient's pelvic radiograph reveals cortical thickening, coarse trabeculae, and sclerosis, which is characteristic of Paget's disease, depicted in the histological section in Figure B. Bisphosphonate treatment is an appropriate treatment for Paget's disease. However, long-term administration of intravenous (IV) bisphosphonates (i.e.
Zoledronate) may result in osteonecrosis of the jaw.
Osseous lesions from Paget's disease have increased osteoclastic bone resorption, marrow fibrosis, increased bone vascularity, and increased disorganized bone formation, resulting in a mosaic (woven and lamellar bone) appearance on histology. Asymptomatic patients may be treated with
observation and symptomatic management reserved as first-line management. When recalcitrant to symptomatic management, bisphosphonate therapy helps control osteoclast lytic activity and reduces pain. However, when administered long-term, side-effects may include atypical subtrochanteric femur fractures and jaw osteonecrosis (especially when given IV). Administration of Teriparatide (Forteo) is contraindicated in these patients due to the increased risk of Pagetoid malignant transformation. Malignant transformation to Paget's sarcoma occurs in 1% of patients.
Langston et al. performed a randomized trial of intensive bisphosphonate treatment versus symptomatic management in Paget's disease of bone. They reported that while serum alkaline phosphatase (ALP) levels were significantly lower in the intensive treatment group than in with the symptomatic treatment group, there was no difference in the quality of life, pain scores, hearing loss, or rates of surgical intervention in the two cohorts. They concluded that
striving to maintain normal ALP levels with intensive bisphosphonate therapy confers no clinical advantage over symptom-driven management in patients with Paget's disease of bone.
Figure A demonstrates Paget's disease of the right hemipelvis. Figure B demonstrates the
histology of Paget's disease of bone (woven bone and irregular broad trabeculae with disorganized cement lines in a mosaic pattern). Illustration A and B demonstrate osteonecrosis of the jaw and atypical subtrochanteric femur stress fracture, respectively, after long-term bisphosphonate use.
Incorrect Answers:
A long oblique diaphyseal fracture is internally fixed with 2 lag screws. There is 2 mm of residual fracture fragment gap following screw fixation. This construct has which of the following compared to a comminuted diaphyseal fracture
internally fixed with a long bridge plating technique?
Greater interfragmental strain
Greater ductility
Greater primary Haversian remodeling
Greater union rate
Greater callus volume formation
A long oblique diaphyseal fracture with 2 mm of residual displacement after being internally fixed with lag screws has greater interfragmental strain than comminuted fractures treated with bridge plating or fractures that are anatomically reduced and internally fixed.
Perrens’ theory of strain states that there is a relationship between decreasing strain and increasing the potential for osteogenesis across a fracture or fusion site. The strain theory states that for two given fracture segments, the healing interface will possess a force- generated motion potential that is contingent on the stability of the original fixation construct. Mathematically, the strain for
any given force is equal to the change in the interface length divided by the original interface length. Therefore, with an unstable construct, the healing gap may undergo excessive motion with resultant increasing strain. It has been shown that strain of less than 2% will yield absolute stability and subsequent primary bone healing. Comminuted fractures have multiple fracture lines therefore the force is dissipated over multiple fracture lines and interfragmentary strain is decreased.
A 75-year-old woman presents with acute severe back pain after sustaining a mechanical fall while walking out of her yard. She denies pain in her buttocks or legs. On physical exam she has point tenderness over the L1 spinous process. Figure A depicts her current radiograph. Which of the following statements is true regarding here underlying metabolic condition and associated pathology?
Kyphoplasty is indicated within the first week if the pain is severe enough to warrant narcotic medication.
Her underlying metabolic bone condition leads to decreased bone quantity with normal bone quality.
A DEXA T-score of -2.1 in this individual would confirm the diagnosis of osteoporosis according to the WHO.
A 25-hydroxy Vitamin D level of 16ng/mL in this individual would confirm the diagnosis of osteoporosis according to the WHO.
The fracture pattern in Figure A is the third most common fragility fracture in the United States
This clinical presentation is consistent with an L1 osteoporotic compression fracture due to underlying osteoporosis. Osteoporosis is characterized by decreased bone quantity with normal bone quality.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Vertebral compression fractures are the most common type of fragility fracture in patients with osteoporosis. Management should begin with a proper evaluation to identify the etiology of the fracture and appropriate intervention to rectify the underlying pathology.
Evaluation includes bone densitometry, lab testing of Vitamin D and calcium. The World Health Organization (WHO)
classifies bone density in postmenopausal women based on T-scores, with classification based on the lowest T-score of the spine, femoral neck, trochanter, or total hip. Osteoporosis is defined by T-scores 2.5 or greater standard deviations below the peak bone mass of a 25-year-old individual.
Gehrig et al. published an Instructional Course Lecture on the management and treatment strategies for orthopaedic surgeons. They reported that osteoporosis may be present in patients with and without fracture and that the ultimate goal in managing and treating osteoporosis is to optimize fracture risk reduction. They recommended non-pharmacologic interventions including calcium, vitamin D supplementation, fall prevention, hip protectors, and balance and exercise programs to minimize fracture risk.
The United States Preventive Services Task Force published clinical guidelines on osteoporosis screening. They recommended screening for osteoporosis in women aged 65 years or older and in younger women whose fracture risk is equal to or greater than that of a 65-year-old white woman who has no additional risk factors. They concluded that the current evidence is insufficient to assess the balance of risks and benefits of screening for osteoporosis in men.
Figure A depicts an L1 vertebral compression fracture. Incorrect Answers:
year-old woman with long standing rheumatoid arthritis presents with worsening bilateral foot pain. She sees a podiatrist for shaving of her plantar forefoot calluses. She has tried orthotics and custom shoes but notes worsening foot pain that is limiting her daily activities. Plain radiographs of her feet are pictured in Figure A. Which
of the following images depicts the surgical treatment that would result in the best functional outcome for this patient?
This patient has a classic rheumatoid arthritis (RA) forefoot deformity and would benefit most from first metatarsophalangeal (MTP) joint fusion, hammertoe correction and lesser metatarsal (MT) head resections, pictured in Figure E.
Nearly 90% of patients with chronic RA develop forefoot deformities, most commonly hallux valgus, fixed hammering of the lesser toes and subluxation/dislocation of the lesser MTP joints. Nonoperative management includes orthotic use and shoewear modification. The gold standard surgical treatment involves stabilization of the first ray with a first MTP joint fusion, hammertoe correction and resection of the lesser MT heads (Hoffman-Clayton procedure).
Coughlin et al highlighted that achievement of stable realignment of the first ray is the key factor in reconstruction of a RA forefoot. Stable fusion of the first MTP joint increases weight-bearing along the medial column, minimizes stress on the lesser MTP joints and protects the relocated plantar fat pad. Patients who underwent first MTP fusion, lesser MT head resections and open hammertoe correction had a high level of satisfaction postoperatively.
Mann et al performed a retrospective review of 20 patients with severe RA forefoot deformities who underwent first MTP joint fusion. These patients demonstrated an increase in weight-bearing of the hallux and resultant decrease in metatarsalgia and plantar callosities compared to patients who underwent a first MTP resection arthroplasty
(Keller arthroplasty). The patients in this study noted significant functional improvement postoperatively and no patients required custom shoes or orthotics.
Figure A is an AP radiograph of bilateral feet demonstrating the classic RA forefoot deformity with severe hallux valgus, dislocation of the lesser MTP joints and erosive changes of the MT heads. Figure B shows a hallux valgus realignment procedure with a distal osteotomy and hammertoe correction with a 2nd MT shortening osteotomy (Weil osteotomy), proximal interphalangeal (PIP) joint resection and K wire fixation. Figure C displays a first tarsometatarsal (TMT) joint fusion (Lapidus procedure) and Weil osteotomies
of the 2nd through 4th MTs. Figure D demonstrates a first MTP joint fusion and Weil osteotomies of the 2nd through 4th MTs. Figure E shows a first MTP joint fusion, resection of the 2nd through 5th MT heads and hammertoe correction with PIP joint resection and K wire fixation. Figure F displays a resection of the
first MTP joint proximal phalanx base (Keller arthroplasty) and hammertoe correction with PIP joint resection and K wire fixation.
Incorrect Responses:
What type of fracture healing occurs in a femoral shaft fracture treated with an intramedullary nail?
Primary fracture healing
Secondary fracture healing
Extramembranous ossification
Haversian remodelling
"Cutting cone" remodelling
Intramedullary nails function as internal splints that allow for secondary fracture healing.
Secondary bone healing involves responses in the periosteum and external soft tissues. Here both committed osteoprogenitor cells and uncommitted undifferentiated mesenchymal cells contribute to the process of fracture healing by recapitulation of embryonic intramembranous ossification and endochondral bone formation. The response from the periosteum is a fundamental reaction to bone injury and is enhanced by motion and inhibited by rigid fixation.
Bong et al. reviewed the biomechanics and biology of long bone fracture healing with Intrameduallary nailing. They showed that reaming and the insertion of intramedullary nails can have early deleterious effects on
endosteal and cortical blood flow initially. However, the canal reaming appears to have an overall positive effect at the fracture site as it increases extra
osseous circulation and applies bone graft to the fracture site.
Illustration A shows a series of radiographs of a fracture healed by secondary intention with an IM nail.
Incorrect Answers:
healing of bone.
A 67-year-old woman sustained the injury shown in Figure A approximately 14 months ago, which was managed with closed reduction and casting. She presents with new symptoms of hyperalgesia, allodynia, and hyperhidrosis of her wrist. She denies any recent fevers or chills. Her current radiographs reveal a well-healed fracture without any significant malunion. What is the
pathophysiology likely attributable to her current symptoms?
Pre-ganglion brachial plexopathy
Aberrant inflammatory and vasomotor response
Exaggerated vasoconstriction of the wrist and digital arteries
Incomplete glycosaminoglycan breakdown products causing dysfunction
Connective tissue disorder
The patient is presenting with complex regional pain syndrome (CRPS) after a healed distal radial fracture. The pathophysiology of CRPS is that of aberrant inflammatory and vasomotor response in a region of prior trauma resulting in pain out of proportion, skin discoloration, and vasomotor disturbances.
Patients who develop CRPS often have a history of trauma, but the condition may also occur after surgery. Common symptoms of CRPS include hyperalgesia, often described as burning, throbbing, shooting, or aching. Patients may also experience hyperalgesia, allodynia, and hyperpathia. More objective signs of CRPS may include motor dysfunction (tremors, dystonia, loss of strength), skin, hair, and other trophic changes about the affected extremity, as are symptoms of autonomic dysfunction. CRPS is often sub- classified into 2 types. Type 1 is more common and does not involve specific nerve damage, whereas type 2 involves damage to a specific nerve.
Hogan et al. reviewed the evaluation and treatment of complex regional pain syndrome. They report that although there are many divergent and often conflicting theories, the cause of the severe pain, alterations in regional blood flow, and edema noted in CRPS is unknown. They concluded that CRPS is a challenging diagnosis and as such should be managed by a multidisciplinary team, including chronic pain management specialists,
physical therapists, and orthopedic surgeons.
Shah et al. reviewed the diagnosis and treatment of CRPS. They reported that sweat quantification testing, skin thermography, and electromyography may
be useful in the diagnosis of CRPS, but these tests are often unreliable given is a lack of diagnostic sensitivity. They concluded that the treatment of CRPS remains controversial, and includes medications (antiepileptics, antidepressants, NSAIDS, bisphosphonates, free radical scavengers, vitamin C, and topical anesthetics), physical therapy, regional anesthesia, and neuro- modulation.
Figure A depicts an extra-articular distal radius fracture. Illustration A depicts an example of a wrist affected by CRPS, with notably increased swelling, which is a common finding in patients afflicted with the disease.
Incorrect Answers:
After application of a unilateral tibial external fixator, it is observed that the frame does not provide sufficient rigidity across the fracture site. Altering the external fixator in which of the following ways will have the greatest impact on frame stiffness?
Increasing the distance between pins in each fragment
Increasing the pin diameter
Reducing the distance between bone and connecting bar
Increasing the connecting bar diameter
Adding one stacked connecting bar
While all of the aforementioned factors will increase frame stiffness, pin diameter has the greatest influence on stability of unilateral frames.
Unilateral frames are distinguished from circular frames in that they are positioned on one side of the limb. The overall stability of the frame can be varied by altering the number of pins, the distance between pins, pin diameter, connecting rod diameter, number of connecting rods, distance between bone and connecting rods, and use of multiplanar fixation. The pin diameter has the biggest contribution, as the stiffness of the pin is correlated to the fourth power of its radius.
Fragomen et al. looked at the mechanics of external fixation. They state that the diameter of the half Schantz pin should be less than one-third of the bone diameter to minimize the risk of fracture at the pin site. Unicortical half pins also increase the risk of fracture.
Therefore, pins should be bicortical.
Tencer et al. examined the mechanical properties of external fixation. They showed that frame rigidity could be maximized by increasing the pin separation distance in each fracture fragment, increasing the number of pins and decreasing the sidebar offset distance from bone.
Illustration A shows a schematic of the factors contributing to frame stability. Incorrect Answers:
Locking plate technology is least indicated for which of the following Figures?
Of the fracture patterns listed, all have some indication for locking plate fixation except answer 2. Transverse midshaft both bone forearm fractures are typically treated with non- locked compression plating techniques.
The use of locking plate fixation is an evolving topic in orthopaedics, and exact uses may vary. Well accepted indications for locking plate fixation include indirect fracture reduction, diaphyseal/metaphyseal fractures in osteoporotic bone, bridging of severely comminuted fractures, and plating of fractures where anatomical constraints prevent plating on the tension side of the bone (e.g. short segment fixation).
Anglen et al. performed a level-IV meta-analysis of 33 papers reviewing the use and outcomes of locking plate fixation. They found no standard indications for use, and due to heterogeneity of the studies reviewed had no specific
recommendations for use.
Cantu et al. presented a level-V review of the use of locking plate fixation. They cite 5 indications for use: metaphyseal or intra-articular fractures, highly comminuted fractures particularly involving diaphyseal and metaphyseal bone, osteoporotic bone, proximal tibia and distal femur fractures, and periprosthetic fractures. They also cite 4 relative contraindications: fractures best served
with a construct other than a plate, severe soft tissue injury precluding placement of a plate, simple fracture patterns that can be adequately treated with non-locking constructs, and fractures that would require bending the plate.
Figure A is a comminuted Schatzker VI tibial plateau fracture. Figure B is a transverse both bone forearm fracture. Figure C is an intra-articular pilon fracture. Figure D is a comminuted distal humerus fracture. Figure E Vancouver B1 periprosthetic hip fracture.
Incorrect Answers:
All of the following are true regarding osteocalcin EXCEPT which of the
following?
It is the most prevalent non-collagenous protein in bone
It is expressed by mature osteoblasts
It is considered a marker for osteoblast differentiation
It is a glycoprotein that binds calcium
Higher levels are correlated with increases in bone mineral density during osteoporosis treatment
Pure fact question from basic science. “Osteocalcin is the most prevalent noncollagenous protein in bone” (from Miller's Review). It is expressed by mature osteoblasts and is a marker of osteoblast differentiation. Osteocalcin is the most specific marker of the osteoblast phenotype and is expressed only in mature osteoblasts. During osteoporosis treatment, serum levels correlate
with increases in bone mineral density. Osteonectin, not osteocalcin, is a glycoprotein that binds calcium.
An otherwise healthy young male sustains a significantly comminuted fracture of the 2nd metacarpal shaft and undergoes external fixation as definitive management. The type of bony healing obtained with this treatment is similar to the bony healing for the appropriate treatment of all the following injuries EXCEPT?
The patient has undergone external fixation for his 2nd metacarpal shaft fracture which is an example of enchondral healing (secondary bone healing) which occurs with non- rigid fixation, such as bracing, casting, external fixation, bridge plating, and intramedullary nailing. Of the images shown, Figure D is an example of a patient with an unstable Weber B ankle fracture
with a simple oblique pattern that would preferentially be treated with primary bone healing with ORIF (anatomic stability).
Bone healing occurs via primary healing (intramembranous healing, absolute stability) or secondary healing (enchondral healing, relative stability) depending on the method of fixation. Fractures that require primary bone healing are ones in which anatomic reduction without callus formation is preferred (peri-articular fractures, both bone forearm fractures, non- comminuted ankle fractures with disruption of the ankle syndesmosis).
Primary healing leads to healing via cutting cones and occurs without the production of any callus (which may impede rotation in both bone forearm fractures and cause articular malalignment in peri-articular and peri- syndesmotic fractures). Fractures that may be treated with secondary bone healing and callus formation, do not require anatomic stability and may have fracture site micromotion during the healing process. Intramedullary nailing, external fixation and closed treatment with bracing/splinting/casting all allow motion at the fracture site and lead to secondary bone healing.
Perren reviews the biological and mechanical properties of bone remodeling and the complex interplay of patient, injury and surgical factors that influence healing. The use of relative stability fixation techniques allows the bone to overcome the initial excess strain at a fracture site and build a scaffold that brings the strain to more reasonable levels. The author stresses the importance of understanding bone biology to select optimal implant and methods of surgical fixation.
Bong et al. reviewed the biomechanics and biology of long bone fracture healing with Intramedullary nailing. They showed that reaming and the insertion of intramedullary nails can have early deleterious effects on
endosteal and cortical blood flow initially. However, the canal reaming appears to have an overall positive effect at the fracture site as it increases extraosseous circulation and applies bone graft to the fracture site.
Figure A shows the AP and lateral radiographs of a segmental oblique midshaft tibia fracture. Figure B is an AP radiograph of an unstable intertrochanteric femur fracture with disruption of the calcar. Figure C shows the AP and lateral radiographs of a midshaft transverse femur fracture. Figure D shows the AP and lateral radiographs of a simple oblique weber B ankle fracture with medial clear space widening. Figure E shows a displaced 5th metacarpal neck fracture with dorsal angulation.
Illustration A is the injury in Figure A treated with intramedullary nailing with resulted callus formation. Illustration B is the injury in Figure B treated with cephallomedullary nailing with resulting callus formation. Illustration C is the injury in Figure C treated with intramedullary nailing with resulting callus formation. Illustration D is the injury in Figure D treated with a lag screw and neutralization plating (anatomic stability). Illustration E is the injury in Figure
E treated with closed reduction and casting with subsequent healing with callus formation.
Incorrect Answers:
This is an example of secondary bone healing.
A 7-year-old recent immigrant presents with pain and tenderness over the legs. Physical exam shows the gums have a bluish-purple hue with areas of hemorrhages. A radiograph is shown in Figure A. In Figure B, what region of the growth plate is most affected in this condition?
A
B
C
D
E
The clinical presentation and radiographs are consistent with scurvy. The radiographs show a dense band (White line of Frankl) at the growing metaphyseal end which is characteristic of scurvy. Scurvy is a disease resulting from a deficiency of vitamin C (ascorbic acid), which is required for the synthesis of collagen in humans. Impaired collagen synthesis in scurvy leads to fragile capillaries, resulting in abnormal bleeding, and altered bone formation at the growth plate. More specifically, scurvy affects the spongiosa
the most (but not exclusively) in the metaphysis, which is depicted by region E in the illustration.
It is considered optimal to obtain written informed consent for an elective surgical procedure in which of the following clinical settings?
By the hospital risk manager upon admission
By the nurse in pre-op holding
By the surgeon in pre-op holding
By the surgeon's scheduler greater than 7 days prior
By the surgeon in the office within 7 days prior
The reference by Bhattacharyya et al notes that the location where the informed consent was obtained is important. When informed consent was obtained by the operating surgeon in the office, there was a decreased risk of indemnity payment (p < 0.004). This finding is likely due to the effect of communication on malpractice claims. Poor communication has been established as the critical factor linked to malpractice claims. It seems logical that the physician-patient communication that occurs in the office is more interactive and substantive than discussions that occur on the hospital floor or in the preoperative holding area. A closed claims analysis conducted in Florida, which included 127 mothers of infants who had experienced permanent perinatal injuries and who subsequently sued their physicians, showed that nearly all complained that their physicians would not talk, answer questions,
or listen. Clearly, the office is the best setting for quality discussions on informed consent to occur.
A 45 year-old woman who has not reached menopause yet falls from a standing height and sustains a distal radius fracture. A DEXA scan reveals a T- score of -2.2. Which of the following treatments is indicated in this patient?
1,700 mg of calcium
1,200 mg of calcium
1,700 mg of vitamin D
1,200 mg of iron
1,700 mg of PTH
The current recommendations for further prevention of any fragility fracture include 1200- 1500mg of elemental calcium intake per day and 400-800 IU of vitamin D per day. Of note, these doses are indicated only for prevention and not sufficient for active treatment of osteoporosis (T score less than -2.5).
Medications that are approved by the FDA for active treatment of osteoporosis: alendronate, risedronate, raloxifene, estrogen, calcitonin. These medications and preventative measures help to reduce fragility fractures by as much as 50%.
Freedman et al. performed a retrospective study that looked at a cohort of patients with fragility fractures and then looked at the type and frequency of osteoporosis related interventions. They found that only 60% of patients actually were either prescribed a
medication, given a referral, or ordered additional workup (DEXA scan).
Schulman et al. reviewed a series of 80 female patients regarding osteoporosis and bone health, and found that the outpatient sports medicine office setting was an excellent opportunity to educate patients on these topics. The patients' post-education test scores increased significantly after a brief counseling session, and increases in daily calcium intake and exercise levels were also seen.
Hypophosphatasia is associated with which of the following laboratory findings?
Hyperbilirubinemia
Decreased urinary phosphoethanolamine
Decreased urinary inorganic pyrophosphate
Decreased serum phosphate
Decreased serum alkaline phosphatase
Alkaline phosphatase is a marker of bone formation and is elevated when bone formation is increased. Hypophosphatasia is an autosomal recessive disorder caused by an inborn error in the production of alkaline phosphatase (tissue- nonspecific isoenzyme of alkaline phosphatase: TNSALP), leading to low alkaline phosphatase levels. Increased urinary phosphoethanolamine is also diagnostic.
Which of the following statements regarding COX-2 is FALSE?
It causes mesenchymal stem cells to differentiate into osteoblasts
COX-2 knockout mice heal fractures more quickly than control mice
COX-2 is an enzyme which converts arachidonic acid to prostaglandin endoperoxide H2
Most NSAIDS non-specifically inhibit both COX-1 and COX-2 enzymes
The expression of COX-2 is upregulated in several human cancers
Cycloxygenase-2 (COX-2,aka prostaglandin-endoperoxide synthase 2) is an enzyme which converts arachidonic acid to prostaglandin endoperoxide H2. COX-2 is not expressed under normal conditions, but elevated levels are found during general states of inflammation. Zhang et al and Simon et al have both studied the role of COX-2 with regard to fracture healing. Zhang et al created
a COX-2 knockout mouse (one which does not express the COX-2 gene). This COX-2 knockout mouse has been shown to heal fractures more slowly than COX-1 knockout
mice or normal controls, thus identifying the role of COX-2 in general inflammation and bone repair. Zhang et al hypothesize that COX-2 causes mesenchymal progenitor cells to differentiate into osteoblasts, thus promoting new bone formation. Simon et al showed the delayed effects of fracture healing when animals were treated with COX-2 inhibitors.
Gerstenfeld et al. studied the reversibility of COX-2 inhibition on the short term bone healing in an animal model. They found that COX-2 inhibitors block fracture healing more than NSAIDS and the magnitude of this effect is related to the duration of treatment.
While specific inhibitors of COX-2 exist, traditional
NSAIDs non-specifically inhibit both COX-1 and COX-2 enzymes. In addition to its role in inflammation, COX-2 has been shown to be upregulated in many human cancers such as gallbladder carcinoma.
A 60-year-old man has had intermittent pain in his right great toe for the past 2 years. What is the most likely cause for the lesions shown in Figure A?
Monosodium urate crystal deposition
Calcium pyrophosphate deposition
Renal osteodystrophy
Tuberculosis
Sarcoidosis
Gout is a disorder of nucleic acid metabolism that leads to monosodium urate crystal deposition in the joints. The most common area of the body to be affected by gout is the first toe. The radiograph in Figure A demonstrates joint space narrowing of the 1st
metarsalphalangeal joint and the arrows show medial soft tissue swelling at the 1st MTP with soft tissue radio-densities and some erosive changes consistent with gout.
Weinfeld et al report their experience over a 7 year period with hallux MTP arthritis in 439 patients they treated. Surgical indications included pain, shoewear problems, and failure of non-operative management.
Reber et al describe a rare case of tophaceous gout in the medial sesamoid of the hallux and review the diagnosis, pathophysiology, and suggested management.
Eggebeen reports "gout is caused by monosodium urate crystal deposition in tissues leading to arthritis, soft tissue masses (i.e., tophi), nephrolithiasis, and urate nephropathy. The biologic precursor to gout is elevated serum uric acid levels (i.e., hyperuricemia). The diagnosis is confirmed if monosodium urate crystals are present in synovial fluid."
Incorrect Answers:
Which of the following pharmacologic agents is associated with the highest risk of bleeding and thrombocytopenia?
Coumadin
Enoxaparin
Unfractionated heparin
Dalteparin
Protamine sulfate
Of the options listed unfractionated heparin is associated with the highest rate of bleeding and thrombocytopenia. This may occur as part of a syndrome called Heparin Induced Thrombocytopenia (HIT).
Unfractionated heparin works in the coagulation cascade by binding and enhancing the ability of antithrombin III to inhibit factors IIa, III, Xa. A known complication of unfractionated heparin use is Heparin Induced Thrombocytopenia (HIT). Heparin Induced Thrombocytopenia (HIT) is caused by the formation of abnormal antibodies that activate platelets leading to abnormal formation of blood clots inside a blood vessel, leading to
bleeding and thrombocytopenia.
Dorr et al. reviewed multimodal thromboprophylaxis for total hip and knee arthroplasty based on risk assessment in 1179 patients. They recommend careful use and monitoring of thromboprophylaxis after arthroplasty procedures to protect patients from thromboembolic events while also limiting adverse clinical outcomes secondary to thromboembolic, vascular, and bleeding complications.
Mont et al. performed a study on preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. They recommended all patients do early mobilization and receive pharmacologic prophylaxis and mechanical compressive devices for the prevention of thromboembolic disease. The group did not recommend any specific pharmacologic agents and/or mechanical devices.
Illustration A shows a figure of the coagulation cascade and the target molecule of both unfractionated heparin and low molecular weight heparin.
Incorrect Answers:
Which of the following series of lab values is most consistent with a diagnosis of high turnover renal osteodystrophy?
Decreased calcium, increased serum phosphate, increased alkaline phosphatase, increased parathyroid hormone
Decreased calcium, decreased serum phosphate, increased alkaline phosphatase, increased parathyroid hormone
Increased calcium, normal serum phosphate, increased alkaline
phosphatase, normal parathyroid hormone
Decreased calcium, increased serum phosphate, normal alkaline phosphatase, decreased parathyroid hormone
Increased calcium, normal serum phosphate, normal or high alkaline phosphatase, increased parathyroid hormone
Decreased calcium, increased serum phosphate, increased alkaline phosphatase, and increased parathyroid hormone are all characteristic of renal osteodystrophy.
Renal osteodystrophy represents a spectrum of disease seen in patients with chronic renal disease. It is characterized by bone mineralization deficiency due to electrolyte and endocrine abnormalities. High turnover renal osteodystrophy is classically associated with significantly increased phosphate and parathyroid hormone (PTH) levels. Chronic renal disease leads to a decrease in renal phosphorus excretion, which leads to phosphate retention and a significant increase in PTH levels. This ultimately can lead to tertiary hyperparathyroidism.
Tejwani et al present a review article on renal osteodystrophy. They state that in high- turnover renal osteodystrophy PTH secretion is increased and, in the absence of medical intervention, leads to parathyroid gland hyperplasia. This hyperplasia is associated with loss of feedback inhibition in normal regulation of PTH secretion; consequently, even after correction of the renal disease, the parathyroid gland continues to secrete excessive levels of PTH.
Illustration A shows a pathologic fracture secondary to renal osteodystrophy. Incorrect Answers:
This series of lab values is consistent with a diagnosis of nutritional rickets due to vitamin D deficiency.
This series of lab values is consistent with a diagnosis of low-turnover renal osteodystrophy. This is classically caused by excess deposition of aluminum into bone which impairs PTH release from the parathyroid gland and disrupts the mineralization process.
This series of lab values is consistent with a diagnosis of hypoparathroidism. 5-This series of lab values is consisten with a diagnosis of primary hyperparathryoidism.
A 28-year-old African-American male with a history of Sickle Cell Disease complains of progressive left hip pain for the past two years. He denies any causative injuries. His images are shown in Figures A and B. Which of the following mechanisms is most likely responsible for his symptoms?
Blood disorder due to abnormal hemoglobin S alleles
Progressive slippage of physis though the hypertrophic zone
Osteomyelitis most likely due to Salmonella species
Accumulation of glycosaminoglycan breakdown products
COL5A1 or COL5A2 mutation
The clinical presentation and images are most consistent with left hip osteonecrosis as a result of coagulation and vascular occlusion caused by sickle cell anemia.
Sickle cell disease is a genetic disorder of hemoglobin synthesis characterized by 2 abnormal hemoglobin S alleles. Under low oxygen conditions the affected blood cells become "sickle shaped" and unable to pass through vessels. This results in vascular occlusion that may have a variety of clinical consequences depending on the body part affected.
Hernigou et al. review the natural history of symptomatic osteonecrosis in adults with sickle cell disease. Once symptomatic , osteonecrosis of the hip in sickle cell disease has a high likelihood of progressing and leading to femoral head collapse. Deterioration can be rapid and in most patients operative intervention is necessary to prevent further collapse or alleviate intractable pain.
Mont et al. performed a literature review on the natural history of untreated asymptomatic osteonecrosis of the femoral head. Their findings supported that asymptomatic osteonecrosis had a high prevalence of progression to symptomatic femoral head collapse. Small, medially located lesions had a low rate of progression, while medium to large sized osteonecrotic lesions did progress in a substantial number of patients. They recommended
consideration of joint-preserving surgical treatment in asymptomatic patients with a medium-sized or large, laterally located lesion.
Figure A shows an AP pelvis with left hip osteonecrosis. Figure B shows a T2 coronal MRI with left hip osteonecrosis. Illustration A shows an example of a hemoglobin molecule which has become "sickle shaped," and as a result is unable to pass through vessels efficiently.
Incorrect Answers:
slipped capital femoral epiphysis.
What mechanism allows Staphylococcus epidermidis to adhere to surfaces and resist phagocytosis?
Creation of active efflux pumps
Methylation of 23s rRNA
Biofilm production
Alteration of cell wall permeability
Beta-lactamase production
Staphylococcus epidermidis is a gram-positive bacteria that utilizes a glycocalyx/biofilm to adhere to orthopedic implants and other surfaces and resist phagocytosis.
The biofilm creates a well-protected environment where bacteria can proliferate and thrive essentially undetected by the host immune system. This leads to chronic infections of orthopedic implants that can go undetected for years.
Arciola et al note that S. epidermidis can colonize surfaces in a self-generated viscous biofilm composed of polysaccharides and that the ica genes found in
56% of S. epidermidis isolates were associated with their ability to produce biofilm.
Olson et al discuss the importance of polysaccharide intercellular adhesin (PIA), a
substance produced by 50-60% of S. epidermidis strains, in the adherence of S. epidermidis to biomaterials through biofilm creation. PIA plays a critical role in initial adherence of S. epidermidis to biomaterials, biofilm
maturation and aggregation.
Illustration A shows microscopy of Staphylococcus epidermidis, which is a gram- positive, coagulase-negative cocci. Illustration B is an overview of the different classes of organisms in microbiology.
Incorrect Answers:
Compared to cold-forged cobalt chrome, titanium alloys have which property?
Increased fatigue strength
Increased yield strength
Increased endurance limit
Decreased ductility
Decreased tensile strength
Titanium implants have decreased tensile (ultimate) strength when compared to cobalt chrome.
Ultimate strength, or tensile strength, is the maximum stress a material can withstand before undergoing breakage or failure. The ranking of ultimate strength, from highest to lowest is: 1) cobalt chrome, 2)titanium, 3)stainless steel, and 4) cortical bone.
Young's modulus of elasticity is defined as the measure of stiffness of a material in the elastic zone. A higher Young's modulus indicates a stiffer material. While titanium is highly biocompatible with a low modulus of elasticity (Young's modulus), it has poor wear characteristics making it non- suitable for femoral heads in total hip arthroplasty.
Long et al. present a review on titanium implants with a focus on bio- mechanical properties. Their study supports previous data which showed high rates of ultra-high molecular weight polyethylene wear due to accelerated breakdown when in contact with a titanium surface.
Incorrect Answers:
Peak bone mass attainment in both men and women is most dependent on which sex-steroid?
Testosterone
Progesterone
Growth Hormone
Estrogen
Cortisol
Estrogen has been shown to be important for both men and women in attaining peak bone mass.
Risk factors for osteoporosis are: increasing age, female sex, early menopause, fair-skinned, family history of hip fracture, low body weight, smoking, glucocorticoid use, excessive alcohol, low protein intake, and anticonvulsant or antidepressant use.
Which of the following contributes most to the ability of hyaline cartilage to attract water?
Aggrecan
Biglycan
Decorin
Fibromodulin
Osteocalcin
Aggrecan molecules bind to hyaluronic acid molecules via link proteins to form a macromolecule complex, known as a proteoglycan aggregate, which attracts water.
Proteoglycans are composed of subunits known as glycosaminoglycans. Glycosaminoglycans include two subtypes: chondroitin sulfate and keratin sulfate. These glycosaminoglycans link to a protein core by sugar bonds to form an aggrecan molecule. Link proteins then stabilize many of these aggrecan molecules to hyaluronic acid to form the proteoglycan aggregate. Cartilage also contains ancillary proteoglycans that are much smaller than the aggregating proteoglycans. These small proteoglycans include decorin, biglycan, and fibromodulin. They bind to other molecules (eg, type II collagen) and assist in matrix stabilization.
Ulrich-Vinther et al. authored a Level 5 review on cartilage structure. The negative charge present within the hyaline cartilage extracellular matrix attracts cations and results in an increase in tissue osmolality. This then attracts water, which decreases the osmolality. Thus, articular cartilage has a high tissue pressure, but the presence of type II collagen matrix prevents it from swelling.
Nap et al. present a basic science review article on aggrecans. They discus that the main function of aggrecan in cartilage is to resist compressive forces.
They note that the negative charge of the aggrecan molecule disaccharides create the high osmotic swelling pressure of cartilage.
Illustration A depicts the molecular organization of an aggregated proteoglycan molecule. Incorrect Answers:
What effect do bisphosphonate medications have on spinal fusion surgery when taken in the postoperative period?
Any effect can be counteracted by taking calcium supplements
No effect
Increased risk of wound infection
Smaller fusion mass
Decreased fusion rate
Bisphosphonates (e.g. alendronate) are used to treat osteoporosis. The mechanism of action is inhibiting the formation of the ruffled border of osteoclasts, resulting in decreasing bone turnover.
Huang et al performed a rat study comparing alendronate to placebo and found that fusion rates were lower in those treated with alendronate. However,
the fusion masses were larger in the alendronate treated rats despite lower fusion rates (why #4 is incorrect).
Lehman et al in another placebo controlled rate study found that the fusion rates for placebo (76%) were greater than the alendronate group (45%). Alendronate works on osteoclasts and does not affect calcium directly. Taking calcium should have no effect on alendronate (why #1 is incorrect). At this time there are no formal recommendations of when to stop bisphosphonate medication prior to spinal fusion surgery.
A therapeutic study presents a systematic review of 15 high- quality randomized controlled trials with homogeneous results. What level of evidence is this considered?
I
II
III
IV
V
A systematic review of high-quality clinical trials is considered a Level I study.
A systematic review is a powerful tool used to identify, evaluate and appraise all high- quality research related to a specific question. Systematic reviews, in contrast to most narrative review articles, adhere to strict scientific design by following eight steps; 1) defining a question and developing inclusion criteria,
Question 25
Figure 17 shows the radiograph of an 82-year-old right-hand dominant woman who fell while weeding her garden. She has severe right shoulder pain. She is neurovascularly intact. What is the most appropriate treatment? Review Topic

Explanation
Question 26
A 42-year-old woman has cervical stenosis and radicular deficits at the C5-6 and C6-7 levels. History reveals that she has smoked one pack of cigarettes a day for 25 years. Because nonsurgical management has failed to provide relief, she is now seeking surgical treatment. After preoperative counseling, it becomes clear that she is not likely to stop smoking. Which of the following surgical procedures should be used?
Explanation
neck pain.
REFERENCES: Hilibrand AS, Fye MA, Emery SE, et al: Impact of smoking on the outcome of anterior cervical arthrodesis with interbody or strut-grafting. J Bone Joint Surg Am 2001;83:668-673.
Zdeblick TA, Ducker TB: The use of freeze-dried allograft bone for anterior cervical fusions. Spine 1991;16:726-729.
Question 27
Figures 9a and 9b show the radiographs of a 28-year-old woman who sustained a head injury and a closed injury, without soft-tissue compromise, to her right lower extremity in a motor vehicle accident. Appropriate management of the foot injury should include
Explanation
REFERENCE: Adelaar RS: Fractures of the talus. Instr Course Lect 1990;39:147-156.
Question 28
What structure (arrow) is shown in Figure 24?
Explanation
REFERENCES: Onibokun A, Khoo LT, Holly L: Anterior retroperitoneal approach to the lumbar spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 101-105.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 29
What is the preferred treatment of displaced distal clavicle fractures in children less than eight years old?

Explanation
Question 30
What is the most significant benefit of percutaneous transforaminal lumbar interbody fusion (TLIF) vs open posterior lumbar interbody fusion (PLIF)?
Explanation
Humphreys and associates in a retrospective review of TLIF vs PLIF found fusion rates, surgical time, and length of hospital stay were similar with both procedures. The only benefits associated with TLIF were less blood loss and preservation of the paraspinal muscle sleeve. Manos and associates in a cadaver study found no difference in the volume of disk material evacuated or the area of endplate exposed in either procedure.
RECOMMENDED READINGS
Humphreys SC, Hodges SD, Patwardhan AG, Eck JC, Murphy RB, Covington LA. Comparison of posterior and transforaminal approaches to lumbar interbody fusion. Spine (Phila Pa 1976). 2001 Mar 1;26(5):567-71. PubMed PMID: 11242386. View Abstract at PubMed
Manos R, Sukovich W, Weistroffer J: Transforaminal lumbar interbody fusion: Minimally invasive versus open disc excision and endplate preparation. Presented at the 12th International Meeting of Advanced Spine Techniques, Banff, Alberta, Canada, July 7-9, 2005.
Question 31
A patient who underwent a high tibial osteotomy (HTO) is now scheduled to undergo total knee arthroplasty (TKA). When compared with a patient undergoing primary TKA without a prior HTO, the patient should be advised to expect a higher incidence of
Explanation
REFERENCE: Mont MA, Alexander N, Krackow KA, Hungerford DS: Total knee arthroplasty after failed high tibial osteotomy. Orthop Clin North Am 1994;25:515-525.
Question 32
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
REFERENCE: CA, January/February 2000, vol 50, no. 1 (Cancer Statistics).
Question 33
Suprapatellar intramedullary nailing for tibia fractures when compared to infrapatellar nailing is associated with
Explanation
Question 34
A patient who is an observant Jehovah’s Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?
Explanation
REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
www.watchtower.org. Official Web Site of Jehovah’s Witnesses. Link verified as active as of August 8, 2008.
Question 35
What is the most likely diagnosis based on the MRI findings shown in Figures 87a and 87b? Review Topic

Explanation
Question 36
A B Figures 19a and 19b are the CT scans of an 18-year-old man who was a restrained driver in a rollover motor vehicle collision. What was the primary mechanism of injury?
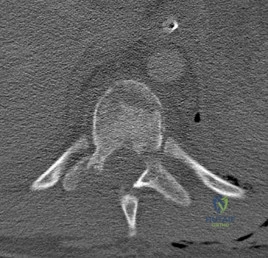
Explanation
This injury pattern represents a flexion distraction injury, or a Chance fracture. The imaging hallmark of this injury is the axial split of the pedicle seen on the sagittal CT scan. This injury necessitates surgical intervention to prevent progressive deformity and pain. A rotation mechanism results in a dislocation with a rotational deformity at the level of injury. An extension force causes failure of the anterior column in tension with compression of the posterior column. An axial load force would result in a burst fracture.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Vaccaro AR, Baron EM, Sanfilippo J, Jacoby S, Steuve J, Grossman E, DiPaola M, Ranier P, Austin L, Ropiak R, Ciminello M, Okafor C, Eichenbaum M, Rapuri V, Smith E, Orozco F, Ugolini P, Fletcher M, Minnich J, Goldberg G, Wilsey J, Lee JY, Lim MR, Burns A, Marino R, DiPaola C, Zeiller L, Zeiler SC, Harrop J, Anderson DG, Albert TJ, Hilibrand AS. Reliability of a novel classification system for thoracolumbar injuries: the Thoracolumbar Injury Severity Score. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S62-9; discussion S104. PubMed PMID:16685239.View Abstract at PubMed
Question 37
- The familial occurrence of Legg-Calve-Perthes disease may, in some cases, be attributed to
Explanation
Question 38
A 74-year-old man with ankylosing spondylitis falls off a step stool and now has a minimally displaced T10-T11 extension-type fracture. He is initially treated with percutaneous pedicle screw fixation from T8-L1 and has good pain relief. The next day, however, he experiences increased back pain and loss of strength in his lower extremities.
Explanation
Cauda equina syndrome, typically the result of severe central canal stenosis in the lower lumbar region, often is caused by a large central disk herniation. Symptoms include severe back or leg pain, perineal numbness, possible motor weakness, and initial urinary retention followed by an overflow incontinence. When bowel or bladder deficits are present, this is considered a surgical emergency because successful recovery is most likely if decompression occurs within the first 48 hours.
Ankylosing spondylitis can lead to progressive autofusion of the vertebrae and significant limitation in motion. Any sudden improvement in motion should be considered a fracture until proven otherwise. These fractures are commonly missed when using plain radiographs or even CT scan because minimal or no displacement often is noted. MR imaging can be useful to identify edema at
the fracture site. These fractures are typically very unstable and necessitate surgery to avoid displacement and potential neurologic injury.
Some fractures associated with ankylosing spondylitis can be effectively treated with percutaneous pedicle screw fixation. However, because of the highly vascular nature of some of these fractures, they pose risk for an epidural hematoma, potential neurologic deficit, and emergent decompression.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778. View Abstract at PubMed
Mathews M, Bolesta MJ. Treatment of spinal fractures in ankylosing spondylitis. Orthopedics. 2013 Sep;36(9):e1203-8. doi: 10.3928/01477447-20130821-25. PubMed PMID: 24025014.
View Abstract at PubMed
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
Question 39
When performing elbow arthroscopy, it is often necessary to evaluate the posterior compartment. When entering the posterior compartment of the elbow, what are the two safest and most commonly used portals? Review Topic
Explanation
Question 40
A patient with a cobalt-chromium alloy (Co-Cr) femoral stem has a periprosthetic fracture that is to be fixed with a cable-plate device. The surgeon should make sure that the plate, screws, and cable, respectively, are made of
Explanation
REFERENCES: Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 119-144.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 41
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?
Explanation
REFERENCE: Poynton AR, O’Rourke K: An analysis of skin perfusion over the Achilles tendon in varying degrees of plantar flexion. Foot Ankle Int 2001;22:572-574.
Question 42
The parents of a 10-year-old boy with Down syndrome are seeking sports clearance for participation in the high jump at the Special Olympics. He is asymptomatic, and the neurologic examination is normal. The hips and patellae are clinically stable. Radiographs of the cervical spine in flexion and extension show a maximum atlanto-dens interval (ADI) of 6 mm. Based on these findings, what recommendation should be made?
Explanation
REFERENCES: Atlantoaxial instability in Down syndrome: Subject review. American Academy of Pediatrics Committee on Sports Medicine and Fitness. Pediatrics 1995;96:151-154.
Tredwell SJ, Newman DE, Lockitch G: Instability of the upper cervical spine in Down syndrome. J Pediatr Orthop 1990;10:602-606.
Segal LS, Drummond DS, Zanotti RM, et al: Complications of posterior arthrodesis of the cervical spine in patients who have Down syndrome. J Bone Joint Surg Am 1991;73:1547-1554.
Question 43
Radial nerve palsy is most commonly associated with which of the following types of humeral fractures?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Question 44
Which patient would expect to have the longest implant survivorship after undergoing total elbow arthroplasty (TEA)? Review Topic
Explanation
The primary surgical management of the rheumatoid elbow is mainly synovectomy or total elbow arthroplasty (TEA). The indications for TEA include advanced disease of the elbow (grade III or IV), significant pain, and limitations in activities of daily living. Contraindications include active or historical elbow infection, upper extremity paralysis, and refusal to abide by postoperative instructions. Implant options are traditionally classified as linked (semiconstrained) or unlinked - with improved stability and survivorship of semiconstrained designs.
Aldridge et al. provide a 10- to 31-year survival analysis on total elbow arthroplasty with the Coonrad/Coonrad-Morrey prosthesis. They reviewed 40 patients (41 elbows) who had undergone a Coonrad/Coonrad-Morrey elbow arthroplasty. Of the 41 elbows, 21 were functional between 10 and 14 years after operation, ten between 15 and 19 years and ten between 20 and 31 years.
Skytta et al. reviewed 1,457 primary TEAs for rheumatoid elbow. 87% of the TEAs were performed in women. The most frequent reason for revision was aseptic loosening (47%). They found no differences in survival rates between different TEA designs.
Schneeberger et al. examined 41 post-traumatic osteoarthritic elbows treated with semiconstrained Coonrad-Morrey TEA. 11 patients (27 per cent) had major complications. These were attributed to lifting more weight across the implant than adviced by the surgeon; excessive preoperative deformity of the joint; and/or an unstable traumatic injury.
Cil et al. reviewed 91 patients who underwent total elbow arthroplasty for the treatment of a distal humeral nonunion. The rate of prosthetic survival without removal or revision for any reason was 96% at two years, 82% at five years, and 65% at both ten and fifteen years. They conclude that semiconstrained TEA is a salvage procedure in patients with a distal humeral nonunion that is not amenable to internal fixation.
Incorrect Answers:
Question 45
An 18-year-old man sustains an injury to his lateral ankle after being kicked while playing soccer. He reports persistent pain on the lateral ankle as well as a popping sensation with attempted ankle dorsiflexion and eversion. Which of the following structures anatomically restrains the retracted structure shown in Figure 12?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 81-89.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 46
The decision to perform fasciotomy of the fingers for a hand compartment syndrome is most appropriately made using
Explanation
Compartment syndrome of the hand can result from a variety of factors, including a traumatic event such as crush injury, fracture, vascular insult, a high-pressure injection injury, or an insect or spider bite. The treatment involves decompressive fasciotomy of the involved compartments. The diagnosis of hand compartment syndrome is determined by history, examination, and objective testing. Patients experience pain out of proportion to the injury, along with swelling and tense skin. Pain may occur with passive motion of the metacarpophalangeal joints as the intrinsic muscles are stretched. Invasive intracompartmental pressures can be measured in the compartments of the hand but not in the fingers. Arterial Doppler studies assess arterial blood flow, and an abnormality would be a late finding. MRI would show edema of the hand and fingers, but the decision to perform surgical release is less likely made from the findings. The most appropriate method of determining the need for finger fasciotomy is the history and physical examination.
Question 47
What structure is the primary restraint to inferior translation of the shoulder?
Explanation
REFERENCES: Harryman DTII, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53 -66.
Bigliani LU, Pollock RG, Soslowsky LJ, et al: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 48
Primary arthrodesis is associated with which outcome when compared to outcomes associated with open reduction and internal fixation (ORIF) without arthrodesis?
Explanation
There are longitudinal, oblique, and transverse ligaments at the TMT complex that are further defined by their location as dorsal, interosseous, or plantar. There are 3 ligaments between the medial cuneiform and the second MT base, the most important of which is the oblique interosseous ligament, which is also known as the Lisfranc ligament. Plantar and dorsal oblique ligaments contribute to stability to a lesser degree. The dorsal ligaments are weakest and may be the first to fail in a Lisfranc injury.
The second MT base should be aligned with the middle cuneiform at the medial borders, and the fourth MT base should be aligned with the cuboid at the medial borders on the oblique view. The dorsal and plantar aspects of the MTs
should align with the cuneiforms/cuboid on the lateral view. Any malalignment should raise the suspicion of a Lisfranc injury. Diastasis between the second MT and the first MT/medial cuneiform complex of more than 2 mm indicates injury, as does TMT joint subluxation of 2 mm more than seen on the uninjured contralateral side. Diastasis between the first and second MT up to 2.7 mm can be normal. Another radiographic sign of injury includes avulsion fracture of the second MT base or medial cuneiform. Additional imaging studies that may be helpful in identifying subtle injuries include weight-bearing radiographs and CT or MRI images.
Two prospective randomized studies compared primary fusion with ORIF Lisfranc injuries. The second study included fracture-dislocations, whereas the first looked at primarily ligamentous injuries. Results conflicted with an earlier study demonstrating improved results (less pain, better function) with primary fusion, while a more recent study showed no difference. Neither study showed worse results with primary fusion, and the rate of secondary surgery was more common in the ORIF group (salvage arthrodesis or hardware removal).
RECOMMENDED READINGS
Solan MC, Moorman CT 3rd, Miyamoto RG, Jasper LE, Belkoff SM. Ligamentous restraints of the second tarsometatarsal joint: a biomechanical evaluation. Foot Ankle Int. 2001 Aug;22(8):637-41. PubMed PMID: 11527024.View Abstract at PubMed
Watson TS, Shurnas PS, Denker J. Treatment of Lisfranc joint injury: current concepts. J Am Acad Orthop Surg. 2010 Dec;18(12):718-28. Review. PubMed PMID: 21119138.View Abstract at PubMed
Faciszewski T, Burks RT, Manaster BJ. Subtle injuries of the Lisfranc joint. J Bone Joint Surg Am. 1990 Dec;72(10):1519-22. PubMed PMID: 2254360.View Abstract at PubMed
Ly TV, Coetzee JC. Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation. A prospective, randomized study. J Bone Joint Surg Am. 2006 Mar;88(3):514-20. PubMed PMID: 16510816.View Abstract at PubMed
Henning JA, Jones CB, Sietsema DL, Bohay DR, Anderson JG. Open reduction internal fixation versus primary arthrodesis for lisfranc injuries: a prospective randomized study. Foot Ankle Int. 2009 Oct;30(10):913-22. doi: 10.3113/FAI.2009.0913. PubMed PMID: 19796583. View
Abstract at PubMed
Question 49
A 35-year-old woman who is a recreational runner reports posterior knee pain and tightness in the knee with flexion during running. She denies any history of trauma. Examination reveals normal patellar glide and tilt and no patellar apprehension. Range of motion is 5 degrees to 120 degrees, and quadriceps function and knee ligamentous examination are normal. Radiographs are normal. An MRI scan is shown Figure 18. What is the most likely diagnosis?
Explanation
REFERENCES: Deutsch A, Veltri DM, Altchek DW, et al: Symptomatic intraarticular ganglia of the cruciate ligaments of the knee. Arthroscopy 1994;10:219-223.
Brown MF, Dandy DJ: Intra-articular ganglia of the knee. Arthroscopy 1990;6:322-323.
Question 50
below demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. A further work-up reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MRI with MARS. Revision THA is recommended. The most common complication following revision of a failed metal-on- metal hip arthroplasty is
Explanation
Question 51
A 10-year-old girl with a history of an obstetrical brachial plexus palsy has been referred for evaluation. Examination reveals a severe adduction internal rotation contracture of the shoulder and a mild flexion contracture of the elbow. Hand function is normal. Radiographs show mild glenohumeral joint incongruity. To achieve the best functional outcome, management should consist of
Explanation
REFERENCES: Jahnke AH Jr, Bovill DF, McCarroll HR Jr, James P, Ashley RK: Persistent brachial plexus birth palsies. J Pediatr Orthop 1991;11:533-537.
Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of 20 cases. J Pediatr Orthop 1990;10:442-444.
Goddard NJ, Fixsen JA: Rotation osteotomy of the humerus for birth injuries of the brachial plexus. J Bone Joint Surg Br 1984;66:257-259.
Question 52
Use of long-term (at least 5 years) bisphosphonate medications for osteoporosis is associated with
Explanation
Fragility or osteoporotic fractures are common in postmenopausal women and older men and include fractures of the proximal humerus and distal radius and hip and vertebral compression fractures. The most reliable predictor of a fragility fracture is a past fragility fracture; consequently, it is important to elicit history. Assessment of vitamin D and calcium levels is important when treating these patients because many of them have low levels.
Use of bisphosphonates for treatment of osteoporosis results in atypical femur fractures and a decrease in risk for fragility fractures (including hip fractures). There also are reports of osteonecrosis of the mandible with prolonged use of these drugs. Current medical literature suggests stopping these drugs after 3 to 5 years to allow bone remodeling.
RECOMMENDED READINGS
Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster D, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Koval K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Sen HT, van der Meulen MC, Weinstein RS, Whyte M; American Society for Bone and Mineral Research. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010 Nov;25(11):2267-94. doi: 10.1002/jbmr.253. Erratum in: J Bone Miner Res. 2011 Aug;26(8):1987. PubMed PMID: 20842676. View Abstract at PubMed
Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F,McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone
Miner Res. 2014 Jan;29(1):1-23. doi:10.1002/jbmr.1998. Epub 2013 Oct 1. PubMed PMID: 23712442. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 92 THROUGH 95
A 23-year-old man is involved in a motorcycle collision and sustains a displaced transcervical femoral neck fracture with an associated open comminuted femoral shaft fracture.
Question 53
A 46-year-old man has acute tenderness along the ulnar aspect of the wrist after falling on his outstretched hand while playing basketball. Examination reveals tenderness and mild swelling along the volar ulnar aspect of the wrist. Radiogaphs are shown in Figures 14a through 14c. Management should consist of
Explanation
REFERENCES: Failla JM, Amadio PC: Recognition and treatment of uncommon carpal fractures. Hand Clin 1988;4:469-476.
Botte MJ, Gelberman RH: Fractures of the carpus, excluding the scaphoid. Hand Clin 1987;3:149-161.
Question 54
Figures 124a and 124b are the radiographs of a 30-year-old man who sustained an ankle injury and has swelling with lateral tenderness. The patient denies any previous ankle injuries. After 6 weeks of rest and use of a removable ankle brace, he continues to have swelling, lateral pain, and popping. An anterior drawer test reveals a solid end point. Recommended treatment should include which of the following?

Explanation
of lateral ankle ligament instability. Ankle rehabilitation and physical therapy may further damage the unstable tendons.
Question 55
- The Magnetic resonance imaging signal characteristics of a high-grade soft-tissue sarcoma are best described as
Explanation
other characteristics, such as size, pattern of growth, integrity of natural boundaries, and homogeneity.
Intravenous contrast agents are not necessary to evaluate neurovascular structures. Both the T1 & T2 weighted images are essential to detect and characterize soft tissue lesions.
Most Tumors have long T1 and T2 relaxation times, therefore, in most instances signal intensity alone is of limited benefit. Exceptions are lipoma, hematoma, intra-lesional hemorrhage.
Hemorrhage may occur in some soft tissue lesions, especially sarcomas, leading to the low T1 and high T2 intensity sound on MR. Miller, indicates that Water, CSF, acute hemorrhage and soft tissue tumors appear dark on T1 and light on T2.
Question 56
Figure 28 shows an AP radiograph of a 54-year-old woman who underwent lumbar laminectomy and fusion at the L4 and L5 levels with placement of a bone stimulator 8 years ago. She also underwent a left total hip arthroplasty 2 years ago; aspiration of that joint now reveals that it is infected with a gram-positive cocci organism. History is also significant for IV drug use and human immunodeficiency virus (HIV). The patient reports fever, chills, and left flank and abdominal pain. Examination reveals significant pain with resisted left hip flexion and passive hip extension. She also has lumbar hyperlordosis. Which of the following studies would best identify the underlying cause of her infection?
Explanation
REFERENCES: Santaella RO, Fishman EK, Lipsett PA: Primary vs secondary iliopsoas abscess: Presentation, microbiology, and treatment. Arch Surg 1995;130:1309-1313.
Malhotra R, Singh KD, Bhan S, Dave PK: Primary pyogenic abscess of the psoas muscle. J Bone Joint Surg Am 1992;74:278-284.
Question 57
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 376.
Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Waninger KN, Richards JG, Pan WT, et al: An evaluation of head movement in backboard-immobilized helmeted football, lacrosse, and ice hockey players. Clin J Sport Med
2001;11:82-86.
Donaldson WF III, Lauerman WC, Heil B, et al: Helmet and shoulder pad removal from a player with suspected cervical spine injury: A cadaveric model. Spine 1998;23:1729-1732.
Peris MD, Donaldson WF III, Towers J, et al: Helmet and shoulder pad removal in suspected cervical spine injury: Human control model. Spine 2002;27:995-998.
Question 58
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 59
..Oncologic outcome for this patient
Explanation
Question 60
.A patient is unable to actively externally rotate the shoulder when the arm is placed into 90 degrees of abduction and neutral rotation. This finding is most consistent with a tear of the
Explanation
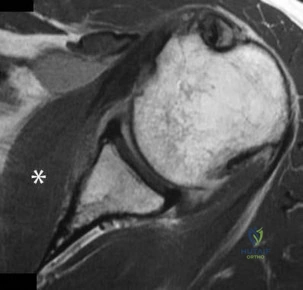
Question 61
What factor is associated with a higher risk of dislocation after total hip arthroplasty?
Explanation
Dislocation after total hip arthroplasty is a multifactorial problem. Numerous risk factors may act independently or cumulatively to increase the risk of this complication. Previous hip surgery of any kind is associated with a twofold increased risk for dislocation. Other risk factors include female gender, impaired mental status, inflammatory arthritis, and older age. Numerous studies have shown a lower dislocation rate with a direct lateral approach, although surgical techniques such as capsular repair have
significantly lowered the incidence of dislocation after using the posterior approach. Metal-on-metal bearings have been associated with other complications such as adverse tissue reactions but are often used with larger-diameter bearings, which pose a lower risk of dislocation.
Question 62
A 17-year-old javelin thrower reports medial-sided elbow pain and diminished grip strength while throwing. He has decreased sensation in the little and ring fingers of his throwing hand only while throwing. The sensory deficits resolve at rest. Examination of the elbow reveals no instability and full motion. He has a positive Tinel’s sign over the cubital tunnel and a positive elbow flexion test. Radiographs are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Posner MA: Compressive neuropathies of the ulnar nerve at the elbow and wrist. Instr Course Lect 2000;49:305-317.
Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 65-69.
Question 63
Deep anterior compartment
Explanation
Question 64
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?
Explanation
REFERENCES: Smith GR, Hotchkiss RN: Radial head and neck fractures: Anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg 1996;5:113-117.
Caputo AE, Mazzocca AD, Santoro VM: The nonarticulating portion of the radial head: Anatomic and clinical correlations for internal fixation. J Hand Surg Am 1998;23:1082-1090.
Question 65
Which of the following studies best increases the ability to diagnose femoral neck fractures in patients with femoral shaft fractures?
Explanation
REFERENCES: Tornetta P III, Kain MS, Creevy WR: Diagnosis of femoral neck fractures in patients with a femoral shaft fracture: Improvement with a standard protocol. J Bone Joint Surg Am 2007;89:39-43.
Yang KH, Han DY, Park HW, et al: Fracture of the ipsilateral neck of the femur in shaft nailing: The role of CT in diagnosis. J Bone Joint Surg Br 1998;80:673-678.
Question 66
Risks associated with vertebral compression fractures in the elderly population can be defined by which of the following? Review Topic
Explanation
fractures are more likely to fall and are five times more likely to sustain subsequent fractures than individuals without such a fracture. Analysis of data from Medicare patients with a vertebral fracture had an overall mortality rate that was approximately twice that of the matched controls. The survival rates following a fracture diagnosis, as estimated with the Kaplan-Meier method, were 53.9%, 30.9%, and 10.5% at 3, 5, and 7 years, respectively which were significantly lower than the rates for the controls. The mortality risk following a fracture was greater for men than for women. The mortality risk was greater when the fracture occurred at a younger age. The adjusted hazard ratio was 1.8 compared to the non-fracture group
Question 67
A 38-year-old man has an enlarging left paraspinal soft-tissue mass. Based on the MRI scans and biopsy specimens shown in Figures 32a through 32e, what is the most likely diagnosis?
Explanation
of surgical resection, radiation therapy, chemotherapeutic protocols, hormone modulation, and/or anti-inflammatory medications.
REFERENCES: Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 309-337.
Spear MA, Jennings LC, Mankin HJ, et al: Individualizing management of aggressive fibromatoses. Int J Radiat Oncol Biol Phys 1998;40:637-645.
Question 68
A 28-year-old woman undergoes a closing-wedge high tibial osteotomy (HTO) for medial compartment overload after medial meniscectomy. Postsurgically, she reports improvement in her medial pain and resumes normal activities. About 9 months after her surgery, however, she reports burning pain in the front of her knee with running. Her examination reveals no joint line tenderness, mild pain with patellar compression, and limited patellar glides. What is the most likely cause of her symptoms?
Explanation
Question 69
A patient who underwent a total knee arthroplasty for osteoarthritis 18 months ago now reports the sudden development of pain in the ipsilateral knee. Radiographs and examination of the knee are unremarkable. Aspiration of the synovial fluid 3 days later reveals a WBC count of 1,500/mm 3 . The cells consist of 30% neutrophils and 70% monocytes. Culture results will not be available for several days. The patient has not been on antibiotics prior to this point. Based on these findings, what is the most appropriate management?
Explanation
REFERENCES: Trampuz A, Hanssen AD, Osmon DR, et al: Synovial fluid leukocyte count and differential for the diagnosis of prosthetic knee infection. Am J Med 2004;117:556-562.
Mason JB, Fehring TK, Odum SM, et al: The value of white blood cell counts before revision total knee arthroplasty. J Arthroplasty 2003;18:1038-1043.
Kersey R, Benjamin J, Mason B: White blood cell counts and differential in synovial fluid of aseptically failed total knee arthroplasty. J Arthroplasty 2000;15:301-304.
Question 70
A 12-year-old boy has had progressive pain and flatfeet for the past year. Pain is increased with weight-bearing activities. Examination reveals that subtalar motion is absent. On standing, the patient has obvious hindfoot valgus and loss of the normal arch bilaterally. Plain radiographs are shown in Figures 43a through 43c, and a CT scan is shown in Figure 43d. What is the most likely diagnosis?
Explanation
REFERENCES: Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 583-595.
Question 71
Figures 36a and 36b show the MRI scans of a 15-year-old girl who has had pain and recurrent hemarthrosis in the knee for the past year. Plain radiographs are normal. What is the most likely diagnosis?
Explanation
REFERENCE: Price NJ, Cundy PJ: Synovial hemangioma of the knee. J Pediatr Orthop 1997;17:74-77.
Question 72
The parents of a 13-year-old boy with Down syndrome report that he has an increasing limp and decreased endurance with activities. Lateral flexion-extension radiographs of the cervical spine show no evidence of instability. Examination reveals a right Trendelenburg limp and an obvious limb-length discrepancy. Hip motion is symmetric except for some decreased abduction on the right side. A standing AP radiograph is shown in Figure 20. Management should consist of
Explanation
REFERENCES: Shaw ED, Beals RK: The hip joint in Down’s syndrome: A study of its structure and associated disease. Clin Orthop 1992;278:101-107.
Aprin H, Zinc WP, Hall JE: Management of dislocation of the hip in Down’s syndrome.
J Pediatr Orthop 1985;5:428-431.
Greene WB: Closed treatment of hip dislocation in Down syndrome. J Pediatr Orthop 1998;18:643-647.
Question 73
A 14-year-old boy is seen for back pain. Radiographic evaluation reveals a grade III isthmic spondylolisthesis. What measurement is most useful in predicting the likelihood of progression?
Explanation
REFERENCES: Huang RP, Bohlman HH, Thompson GH, et al: Predictive value of pelvic incidence in progression of spondylolisthesis. Spine 2003;28:2381-2385.
Mac-Thiong JM, Wang Z, de Guise JA, et al: Postural model of sagittal spino-pelvic alignment and its relevance for lumbosacral developmental spondylolisthesis. Spine 2008;33:2316-2325.

Figure 22a Figure 22b
Question 74
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis? Review Topic
Explanation
Question 75
You are asked to evaluate the patient whose current clinical photographs are shown in Figures 46a and 46b following aortic valve replacement 9 days ago. He is currently taking anticoagulation medication. He has no systemic signs of sepsis. What is the best management?
Explanation
REFERENCES: Bowker JH, Pfeiffer MA (eds): The Diabetic Foot. St Louis, MO, Mosby, 2001,
pp 219-260.
Coughlin MJ, Mann RA: Soft tissue disorders of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1373-1397.
Question 76
A 49-year-old woman noted pain in her right axilla 1 day after moving heavy furniture. Two weeks later, she now reports persistent numbness and paresthesias along the inner aspect of her upper arm radiating into the ulnar digits. Examination reveals full shoulder motion, tenderness over the first rib, and a decreased radial pulse with the shoulder placed overhead. What is the most likely diagnosis?
Explanation
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
Question 77
A child born with myelomeningocele is expected to be an ambulator with bracing. Examination by the consulting orthopaedic surgeon reveals rigid clubfeet in addition to the neurologic issues. Management should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 65-78.
Kasser JE (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 503-514.
Question 78
The parents of a 14-year-old female soccer player are concerned about any future injury. They have been advised that she has the potential to play for the US Olympic team. They are especially concerned about the anterior cruciate ligament (ACL). What should you advise them?
Explanation
REFERENCES: Shea KG: ACL Injury: Epidemiology and Prevention Presented at Sports Related Injuries in the Skeletally Mature Athlete. POSNA: One Day Course, 2008.
Millett PJ, Willis AA, Warren RF: Associated injuries in pediatric and adolescent anterior cruciate
ligament tears: Does a delay in treatment increase the risk of meniscal tears? Arthroscopy 2002; 18:955-959.
Question 79
Which of the following is associated with the use of large femoral heads in total hip arthroplasty?
Explanation
REFERENCES: Peters CL, McPherson E, Jackson JD, et al: Reduction in early dislocation rate with large-diameter femoral heads in primary total hip arthroplasty. J Arthroplasty 2007;22:140-144.
Inoue A, Asaumi K, Endo H, et al: Assessment of head wear more than ten years after total hip arthroplasty: 22- mm zirconia vs metal heads. Acta Med Okayama 2006;60:311-318.
Question 80
A 17-year-old male soccer player sustains repeated lateral patellar dislocations refractory to physical therapy, bracing, and taping. After a workup including radiographs and MRI, the orthopaedic surgeon considers an isolated tibial tubercle osteotomy (TTO). He plans a 60-degree anteromedialization to address instability and to unload the patellofemoral joint. What is a relative contraindication to this procedure?
Explanation
TTO is a common treatment for patellofemoral instability. The angle of correction must be customized to each patient’s anatomy. For this patient, the orthopaedic surgeon plans an osteotomy that will both anteriorize and medialize the tubercle. This will consistently result in
a change of patellofemoral kinematics and contact pressures. Medialization decreases lateral and increases medial patellofemoral contact pressures, and anteriorization shifts contact pressures from distal to proximal. Significant anteriorization may not be desired in a patient with proximal patellar chondrosis unless a concomitant chondral procedure is performed as well. The patellar height (Caton-Deschamps ratio) is normal, precluding the need for distalization but not medialization. The TT-TG distance, at more than 20 mm, is a strong indication for osteotomy. The Q angle, although a less precise indicator of malalignment, is also elevated and would be considered an indication for osteotomy.

CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 41
A healthy, active 18-year-old man has acute-onset right knee pain and an inability to fully extend his knee following an attempt to stand from a seated position yesterday. He sustained a noncontact injury to his right knee while playing basketball 2 years ago and underwent primary anterior cruciate ligament (ACL) reconstruction with bone-patella-tendon-bone autograft and medial meniscus repair. He sustained another noncontact injury to the same knee 8 months later and underwent a revision ACL reconstruction using soft-tissue allograft and revision medial meniscus repair. He reports multiple episodes of “giving way” of his knee, but no pain prior to yesterday’s acute injury.
Question 81
A 23-year-old woman has had a 3-year history of snapping and pain in her left hip. She notes that the snapping started while marathon training and is only problematic about 15 minutes into a run. Examination is consistent with a negative Stinchfield, negative logroll, negative flexion abduction/external rotation test (FABER) of the hip; however, she has a positive Ober test as she has difficulty adducting her hip across the midline in the lateral decubitus position. Management consisting of nonsteroidal anti-inflammatory drugs and stretching has failed to improve her snapping. What is the most reliable surgical treatment? Review Topic
Explanation
Question 82
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of
Explanation
REFERENCES: Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Question 83
A 20-year-old man with fascioscapulohumeral dystrophy has severe scapular winging of both shoulders. He can no longer abduct above 80 degrees, and it affects his activities of daily living. A clinical photograph is shown in Figure 26. Definitive management should consist of
Explanation
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
Question 84
Figure 1 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
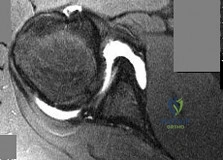
Explanation
Question 85
A 12-year-old girl has had right knee pain for the past 3 months. Radiographs and a coronal T 2 -weighted MRI scan are shown in Figures 10a through 10c. A biopsy specimen is shown in Figure 10d. What is the most appropriate treatment for this lesion?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 86
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?
Explanation
REFERENCES: Calvert E, Younger A, Penner M: Post talus neck fracture reconstruction.
Foot Ankle Clin 2007;12:137-151.
Migues A, Solari G, Carrasco NM, et al: Repair of talar neck nonunion with indirect corticocancellous graft technique: A case report and review of the literature. Foot Ankle Int 1996;17:690-694.
Question 87
A B Figures 18a and 18b are the lumbar spine radiographs of a 72-year-old man with no significant medical history who has had severe back pain for 3 weeks. He denies radiating symptoms, weakness, or numbness when he is seen in the emergency department. He is sent home with a soft corset. At his followup visit he continues to describe significant back pain with activity that is not relieved with oral narcotic mediations. A follow-up CT scan shows a nondisplaced fracture through all 3 columns of the spine. What is the most appropriate treatment?

Explanation
The patient has previously undiagnosed ankylosing spondylitis. Radiographs reveal nonmarginal syndesmophytes throughout the lumbar spine. The CT scan reveals a nondisplaced 3-column fracture. Many patients with missed spinal injuries present in followup with neurologic worsening or progressive deformity. Fractures can often involve all 3 columns, including the posterior elements. In patients with ankylosing spondylitis, this represents an unstable injury and a high likelihood of displacement with nonsurgical treatment. Surgical treatment in the form of a posterior spinal fusion is indicated. Because the fracture is nondisplaced and the patient is neurologically intact, decompression via an anterior approach is not indicated. Bracing either with a TLSO brace or a soft corset will not provide sufficient stability for this fracture pattern. Physical therapy and NSAIDS are not indicated in this scenario.
RECOMMENDED READINGS
Hu SS, Ananthakrishnan D. Ankylosing spondylitis. In: Herkowitz HN, Garfin SR, eds. The Spine. 5th ed. Philadelphia, PA: Elsevier; 2006:763-761.
Blam OG, Cotler JM: Fractures in the stiff and osteoporotic spine. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, eds. Skeletal Trauma: Basic Science, Management, and Reconstruction,. 3rd ed. Philadelphia, PA: Elsevier; 2003.

Question 88
Figures 45a and 45b show the CT scans of a 41-year-old man who was ejected from a vehicle after a high-speed collision. Examination reveals weak (2/5) toe flexion on the right side, but otherwise he has no voluntary motor function in his lower extremities and no sensation. He has some perianal sensation. He has no other associated injuries and his upper extremities are neurologically intact. Which of the following represents the best treatment option? Review Topic
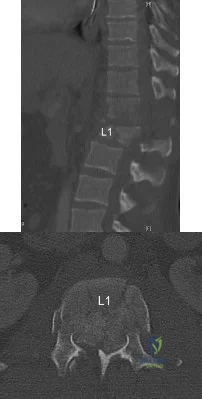
Explanation
(SBQ12SP.25) A 63-year-old female undergoes lumbar decompression and instrumented fusion for the condition shown in Figure A and B. Which of the following factors are associated with increased risk of early post-operative complications? Review Topic

Increasing Age
Intraoperative blood loss
Number of levels fused
All of the above
Age, intraoperative blood loss, and number of spinal levels fused are associated with increased rates of inpatient complication following lumbar decompression and fusion for degenerative spondylolisthesis. Older age correlates with the highest risk for complications.
Lumbar decompression and fusion is well supported in the literature to be effective in the treatment of degenerative spondylolithesis when nonoperative modalities fail. Common complications associated with lumbar decompression and fusion include asymptomatic or symptomatic pseudarthroses (estimated 5-30%), surgical site infection (0.10-2%),and adjacent level degeneration (2-3%). Age, intraoperative blood loss, longer operative times, number of levels fused are associated with increased risk of complication. Smoking is associated with worse outcome after surgery.
Kalanithi et al. reviewed the Nationwide Inpatient Sample adminstrative data on sixty six thousand patients undergoing lumbar laminectomy and fusion. They found the increased age and having 3 or more medical comorbidities was associated with increased risk of complication.
Carreon et al. reviewed cases of ninety eight patients who underwent laminectomy and fusion for lumbar degenerative disease. They found that rates of major and minor complication increased with older age, increased blood loss, longer operative time, number of levels fused.
Figure A is a AP lumbar spine radiograph. Figure B is a lateral lumbar spine radiograph showing degenerative spondylolisthesis at L4-L5. Illustration A shows the postoperative images of the patient treated with an L4-5 fusion with an interbody device.
Incorrect
Question 89
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
REFERENCE: Sarrafian SK: Anatomy of the Foot and Ankle, Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, p 364.
Question 90
A 30 year-old male is involved in a motor vehicle collision and sustains a scapular fracture. In patients with scapular fractures, what other fracture is MOST commonly observed?
Explanation
Scapular fractures are associated with high-energy trauma, with motor vehicle collisions being a common mechanism of injury. These fractures are also associated with increased Injury Severity Scores and therefore clinicians need to be cognizant of concomitant injuries. In addition to associated orthopaedic injuries, pulmonary injuries (contusions, hemothorax, and pneumothorax) and head injuries are associated with scapular fractures. A CT chest should be considered in patients with scapula
fractures, to best visualize associated rib fractures and pulmonary injuries.
Baldwin et al. conducted a retrospective case control analysis using the US National Trauma Database that included 9,453 scapular fractures. In their study, the most commonly associated fractures were rib fractures (52.9%), followed by fractures of the spine (29.2%), clavicle (25.2%), and pelvis (15.3%). Lung and head injuries occurred in 47.1% and 39.1% of the cases, respectively.
Incorrect Answers:
(SBQ12TR.107) An 87-year-old female sustains the injury shown in Figure A after a fall from standing. At baseline, she ambulates with a walker in her home and lives with a 24-hour home health aide. She has a past medical history of stroke and mild dementia. Following medical optimization, what is the most appropriate treatment modality?

Intramedullary nail
Hemiarthroplasty
Closed reduction percutaneous pinning
Total hip arthroplasty
Sliding hip screw
At baseline, with minimal ambulatory status and dependence on a 24-hour home health aide, the best treatment choice is hemiarthroplasty.
Arthroplasty is the gold standard for displaced femoral neck fractures in the elderly. In community ambulators with relative independent lives, total hip arthroplasty (THA) is recommended. For minimal ambulator, hemiarthroplasty is recommended.
van den Bekerom et al. randomized 252 patients over 70-years-old to either THA or hemiarthroplasty for displaced femoral neck fractures. With increased blood loss, operative time and dislocation risk, they did not recommend THA unless there was good preoperative ambulatory status, and/or pre-existing osteoarthritis or rheumatoid arthritis.
Figure A exhibits a displaced femoral neck fracture Incorrect answers:
Question 91
What is the main benefit of using metal-backed tibial components in total knee arthroplasty?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Question 92
Accurate evaluation of the upper portion of the subscapularis muscle is best accomplished with active internal rotation
Explanation
REFERENCES: Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ: Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 1998;26:210-220.
Greis PE, Kuhn JE, Schultheis J, Hintermeister R, Hawkins R: Validation of the lift-off test and analysis of subscapularis activity during maximal internal rotation. Am J Sports Med 1996;24:589-593.
Question 93
A 14-year-old boy is involved in a motor vehicle accident and sustains the injury shown in Figures 18a and 18b. What is the most likely diagnosis? Review Topic

Explanation
Question 94
A 27-year-old professional baseball pitcher who underwent arthroscopic olecranon debridement continues to have medial-sided elbow pain during late cocking. Physical examination reveals laxity and pain with valgus stress testing. What is the most likely cause of his pain?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 101-111.
Kamineni S, Hirahara H, Pomianowski S, et al: Partial posteromedial olecranon resection:
A kinematic study. J Bone Joint Surg Am 2003;85:1005-1011.
Question 95
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Explanation
REFERENCES: Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Apfelbaum RI, Kriskovich MD, Haller JR: On the incidence, cause, and prevention of recurrent laryngeal nerve palsies during anterior cervical spine surgery. Spine 2000;25:2906-2912.
Question 96
A 10-year-old child was referred for spinal curvature and a 2-year history of back pain. She has pain during the day and pain at night that wakes her from sleep and is temporarily relieved with nonsteroidal anti-inflammatory drugs. Examination shows very tight hamstrings and an irritative spinal curvature. Figures 71a through 7Id show radiographs, a bone scan, and a CT scan. What is the most appropriate treatment?
Explanation
REFERENCES: Frassica FJ, Waltrip RL, Sponseller PD, et al: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-
Question 97
An 8-year-old boy reports ankle pain after striking the ground with the medial aspect of his foot while attempting to kick a soccer ball. Radiographs reveal slight distal tibial physeal widening but no other abnormalities. In treating this injury, which of the following associated conditions is most likely present but may be missed without careful evaluation?
Explanation
REFERENCES: Phan VC, Wroten E, Yngve DA: Foot progression angle after distal tibial physeal fractures. J Pediatr Orthop 2002;22:31-35.
Brook GJ, Greer RB: Traumatic rotational displacements of the distal tibial growth plate. J Bone Joint Surg Am 1970;52:1666-1668.
Question 98
A 6-year-old girl sustains an ankle injury after falling on roller blades. An AP radiograph is shown in Figure 68. Treatment should consist of which of the following?
Explanation
REFERENCES: Cass JR, Peterson HA: Salter-Harris type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070. Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 99
A 54-year-old woman sustains the injury seen in Figures 71a and 71b. The injury involves her nondominant extremity. What should the patient be told regarding her expected outcome?

Explanation
(SBQ12TR.101) An otherwise healthy young adult male sustains a transverse radial shaft and ulna fracture. He undergoes definitive surgical fixation with two nonlocking compression plates (LCPs) as shown in Figure A. What is the principle of this fixation technique on bone healing?

Absolute stability with direct healing by callus formation
Relative stability with indirect healing by callus formation
Absolute stability with direct healing by internal remodeling
Relative stability with indirect healing by internal remodeling
Absolute stability with endochondral bone formation
Definitive surgical fixation for a simple transverse both bone forearm fracture would include open reduction and internal fixation with absolute stability with direct healing by internal remodelling (i.e., primary bone healing). The radius is fixed with a 7-hole
Question 100
Figure 6a shows the radiograph of a 50-year-old man who sustained an anterior dislocation of the shoulder. He undergoes closed reduction, and the postreduction radiograph is shown in Figure 6b. Management should now consist of
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Flatow EL, Cuomo F, Maday MG, et al: Open reduction and internal fixation of two-part displaced fractures of the greater tuberosity of the proximal part of the humerus. J Bone Joint Surg Am 1991;73:1213-1218.
