Orthopedic Surgery Board Exam MCQs: Arthroplasty, Spine & Trauma | Part 193
Key Takeaway
This page offers Part 193 of a comprehensive Orthopedic Surgery Board Review series, featuring 100 verified, high-yield MCQs for AAOS & ABOS board certification. Designed for orthopedic residents and surgeons, it provides clinical scenarios and interactive study/exam modes to optimize preparation for success in your board exams.
About This Board Review Set
This is Part 193 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 193
This module focuses heavily on: Arthroplasty, Deformity, Foot, Fracture, Hip, Knee, Ligament, Spine.
Sample Questions from This Set
Sample Question 1: Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show...
Sample Question 2: A 7-month-old girl has had a severe flatfoot deformity since birth. The talar head is prominent in the medial plantar arch of the foot. No other deformities of the spine or extremities are present. Motor and sensory examinations of the extr...
Sample Question 3: What is a known risk factor for lateral distal femoral locking plate failure when used for the fixation of comminuted extra-articular fractures?...
Sample Question 4: A 68-year-old woman who underwent a right total hip arthroplasty 1 year ago has dislocated her hip five times since surgery. Radiographs show a retroverted acetabular component. What is the best treatment for this patient?...
Sample Question 5: A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvio...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 43 shows the lateral radiograph of a patient who underwent anterior cruciate ligament reconstruction. Based on the tunnel placement shown in the radiograph, evaluation of postoperative knee range of motion will most likely show
Explanation
REFERENCES: Brown CH Jr, Carson EW: Revision anterior cruciate ligament surgery. Clin
Bernhardt DT, Landry GL: Sports injuries in young athletes. Adv Pediatr 1995;42:465- Sports Med 1999;18:109-171.
Brown HR, Indelicato PA: Complications of anterior cruciate ligament reconstruction. Op Tech Orthop 1992;2:125-135.
Question 2
A 7-month-old girl has had a severe flatfoot deformity since birth. The talar head is prominent in the medial plantar arch of the foot. No other deformities of the spine or extremities are present. Motor and sensory examinations of the extremities are normal. Figures 37a through 37c show simulated weight-bearing AP and lateral radiographs and a planter flexion lateral view. What is the most likely diagnosis?
Explanation
REFERENCES: Kodros SA, Dias LS: Single-stage surgical correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Stricker SJ, Rosen E: Early one-stage reconstruction of congenital vertical talus. Foot Ankle Int 1997;18:535-543.
Question 3
What is a known risk factor for lateral distal femoral locking plate failure when used for the fixation of comminuted extra-articular fractures?
Explanation
Implant failure is common in distal femur fractures stabilized with plate fixation. Contributors to failure include a short working length of the construct, plate-screw density more than 0.5 and short plate lengths. This will lead to failure as it causes increased strain on the plate over a short segment, and
does not allow enough motion at the fracture site to form bone for healing by secondary intention.
Ricci et al. reviewed 355 cases of distal femur plate fixation. 64 patients (19%) required reoperation to promote union, including 30 that had a planned staged bone grafting. Risk factors for proximal implant failure included open fracture, smoking, increased body mass index, and shorter plate length.
Kregor et al. reviewed 119 patients with distal femoral plate fixation. They found that 93% fractures healed without acute bone grafting. Complications included 5 losses of proximal fixation, 2 nonunions, and 3 acute infections.
Illustration A is an AP of the distal femur demonstrating a comminuted distal femur fracture which has failed fixation with a laterally based distal femur locking plate. It has undergone varus collapse which is a common mechanism of failure for these injuries. Illustration B is a series of AP radiographs of the distal femur of the same patient that was revised to an intramedullary retrograde nail. Illustration C and D show the concepts of plate length, plate-to-screw density and the working length of the plate.
Incorrect Answers:

OrthoCash 2020
Question 4
A 68-year-old woman who underwent a right total hip arthroplasty 1 year ago has dislocated her hip five times since surgery. Radiographs show a retroverted acetabular component. What is the best treatment for this patient?
Explanation
REFERENCES: Daly PJ, Morrey BF: Operative correction of an unstable total hip arthroplasty. J Bone Joint Surg Am 1992;74:1334-1343.
Jolles BM, Zangger P, Leyvraz PF: Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. J Arthroplasty 2002;17-282-288.
Hamilton W, McAuley JP: Evaluation of the unstable total hip arthroplasty. Inst Course Lect 2004;53:87-92.
Question 5
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Findlay JM: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;39:210.
Dickman CA, Mamourian A, Sonntag VK, et al: Magnetic resonance imaging of the transverse atlantal ligament for the evaluation of atlantoaxial instability. J Neurosurgery 1991;75:221-227.
Question 6
A 48-year-old ski instructor dislocates his nondominant shoulder in a fall. Management consisting of application of a sling for 1 week results in improvement in his pain. Follow-up examination 6 weeks after the injury reveals that the patient continues to have difficulty with shoulder elevation. Management should now include
Explanation
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 7
A 19-year-old man has had back pain with activity, especially running in soccer and baseball, for the past 4 months. He denies any history of trauma. Examination reveals no motor weakness or sensory changes in the lower extremities. Range of motion shows increased pain with extension and mild limitation with flexion. A sitting straight leg raising test is limited at approximately 60 degrees bilaterally by back and buttocks pain. Plain radiographs are normal. MRI scans are shown in Figures 13a through 13e. What is the most likely diagnosis?
Explanation
REFERENCES: Wiltse LL, Rothman SL: Spondylolisthesis: Classification, diagnosis and natural history. Sem Spine Surg 1993;5:264-280.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 8
Figure 37 reveals a periprosthetic fracture around a cemented femoral stem in an 81-year-old patient with Paget’s disease and mild coagulopathy. What is the most appropriate reconstructive management on the femoral side?
Explanation
REFERENCES: Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.
Klein GR, Parvizi J, Rapuri V, et al: Proximal femoral replacement for treatment of periprosthetic fractures. J Bone Joint Surg Am 2005;87:1777-1781.
Question 9
What inflammatory mediator has been most closely associated with the magnitude of the systemic inflammatory response to trauma and with the development of multiple organ dysfunction syndrome (MODS)?
Explanation
REFERENCES: Patrick DA, Moore FA, Moore EE, et al: Jack A. Barney Resident Research Award winner: The inflammatory profile of interleukin-6, interleukin-8, and soluble intercellular adhesion molecule-1 in postinjury multiple organ failure. Am J Surg 1996;172:425-429.
Pape HC, van Griesven M, Rice J, et al: Major secondary surgery in blunt trauma patients and perioperative cytokine liberation: Determination of the clinical relevance of biochemical markers. J Trauma 2001;50:989-1000.
Giannoudis PV: When is the safest time to undertake secondary definitive fracture stabilization procedures in multiply injured patients who were initially managed using a strategy of primary temporary skeletal fixation. J Trauma 2002;52:811-812.
Question 10
A study is proposed in which 50 patients with osteonecrosis of the knee are compared with 23 patients without osteonecrosis in terms of their alcohol consumption levels. This is an example of what type of study?
Explanation
Question 11
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
Explanation
A. Lateral head of triceps (radial nerve) and brachialis (musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii (musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis (musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis (musculocutaneous nerve)
Question 12
Figure 23 shows the postoperative radiograph of a patient who underwent an anterior cruciate ligament (ACL) reconstruction (with bone-patella tendon-bone autograft) that failed. He initially had loss of flexion postoperatively. What is the most likely cause of this failure? Review Topic

Explanation
Question 13
..Figures 78a and 78b are the radiographs of a 47-year-old right-hand-dominant woman who has a 3-month history of gradually progressive right shoulder pain. She reports no previous trauma, but does report pain at night and with activity such as weight training. Examination demonstrates active and passive range of motion to be 110 degrees forward elevation, external rotation to 20 degrees, and internal rotation to the sacrum. The next treatment step should include

Explanation
Rotator cuff and scapular stabilizer strengthening exercises
Diagnostic and therapeutic corticosteroid injection
Arthroscopic debridement
Completion of rotator cuff tear, repair, and biceps tenotomy
Acromioplasty
Repair of rotator cuff and superior labrum anterior to posterior (SLAP) repair
Repair of subscapularis tendon and biceps tenodesis
Question 14
A characteristic genetic translocation has been noted in which of the following tumors?
Explanation
REFERENCES: Brockstein BE, Peabody TD, Simon MA: Soft tissue sarcomas, in Vokes EE Golomb HM (eds): Oncologic Therapies. New York, NY, Springer-Verlag, 1999, pp 925-952.
Simon MA, Springfield DS, et al: Management of Surgical Specimens: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 67-75.
Question 15
An 82-year-old woman fell on her right shoulder 2 days ago. She is alert, oriented, and in mild discomfort. Prior to falling, she lived alone and functioned independently. Examination reveals extensive ecchymosis extending to the midhumeral region. Her neurovascular examination is normal. Radiographs are shown in Figures 41a and 41b. What is the most appropriate management?
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-1089.
Bigliani LU, Flatow EL, Pollock RG: Fractures of the proximal humerus, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, pp 352-354.
Question 16
A 70-year-old man underwent primary total knee arthroplasty 3 months ago. Figures 7a and 7b show the radiograph and clinical photograph following incision and drainage of the wound 1 week ago. Aspiration of the joint reveals methicillin-sensitive Staphylococcus aureus. What is the next most appropriate step in management?
Explanation
REFERENCES: Harwin SF: The diagnosis and management of infected total knee replacement. Seminars Arthroplasty 2002;13:9-22.
Goldmann RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
Morrey BF, Westholm F, Schoifet S, Rand JA, Bryan RS: Long-term results of various treatment options for an infected total knee arthroplasty. Clin Orthop 1989;248:120-128.
Question 17
The first branch of the lateral plantar nerve innervates the
Explanation
REFERENCES: Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983,
pp 325-328.
Question 18
-The patient asks if something about her anatomy has resulted in this injury. ACL anatomy differs between men and women in what manner?
Explanation
This patient has the clinical findings of an ACL rupture that is confirmed on MRI scan. She is a professional athlete and would like to return to her sport. Immediate ACL reconstruction in the setting of a knee with limited motion carries an increased risk for postsurgical stiffness. Delayed surgery after the patient regains range of motion is the preferred response. It has been shown that a woman’s ACL is smaller in the cross-sectional area.

Question 19
Figure 23 is the radiograph of a 22-year-old woman who was involved in a motor vehicle collision. She reports isolated pain in her left shoulder. She is hemodynamically stable, respiring comfortably, and neurovascularly intact. Based on these findings, which of the following statements regarding treatment is most appropriate?

Explanation
Question 20
A 20-year-old man has a symptomatic lesion of fibrous dysplasia in the femoral neck. Management should consist of
Explanation
REFERENCES: Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 197.
Enneking WF, Gearen PF: Fibrous dysplasia of the femoral neck: Treatment by cortical bone grafting. J Bone Joint Surg Am 1986;68:1415.
Question 21
No fractures were identified and the patient was treated nonsurgically in a range-of-motion brace. Two months later, he continued to experience elbow pain and was unable to return to sports. He regained motion and strength with physical therapy, there was no gross instability with varus or valgus testing, and he had a negative moving-valgus stress test. The orthopaedic surgeon performed an examination under anesthesia in the operating room (Video 54). Which anatomic structure is injured?
Explanation
Ninety percent of elbow dislocations occur in a posterolateral direction. O’Driscoll and associates described the mechanism of injury in posterolateral elbow dislocations in 1992, reporting that they occur most typically after a fall onto an outstretched arm. As the arm hits the ground it causes axial compression, forearm supination, and valgus load across the elbow. The triceps fires, pulling the olecranon posterior; the forearm supinates while simultaneous shoulder internal rotators fire; and the elbow falls into valgus. These 3 mechanisms cause the elbow to subluxate and dislocate posterolaterally. The elbow is most stable following posterolateral dislocation in a flexed and pronated position. The elbow is least stable in extension and supination. Simple dislocation often can be treated nonsurgically, while fracture dislocation will usually necessitate surgical intervention. The video shows the elbow pivot-shift test, which evaluates for posterolateral rotatory instability. A positive test finding elicits apprehension and, in this case, radial head subluxation and confirms an insufficient lateral UCL.
Question 22
Which sterilization method is expected to produce the most degradation of an allograft used for anterior cruciate ligament reconstruction?
Explanation
A biomechanical study compared unprocessed, irradiated (2.0 Mrad-2.8 Mrad), and supercritical CO2-treated soft-tissue allografts and demonstrated a 27% to 36% decrease in stiffness of the supercritical CO2-treated grafts. No significant difference was found between the irradiated and untreated soft-tissue allografts. Low-dose (1.0 Mrad-1.2 Mrad) gamma irradiation of bone-patellar-tendon-allograft has been shown to produce a 20% decrease in graft stiffness. Deep freezing or cleansing with 4% chlorhexidine gluconate does not appear to adversely affect the biomechanical properties of the allograft tissue.

CLINICAL SITUATION FOR QUESTIONS 43 THROUGH 46
Figures 43a and 43b are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable.
Question 23
All of the following are factors associated with transfer of patients to Level 1 trauma centers EXCEPT:

Explanation
Question 24
A 9-year-old girl reports the immediate onset of severe groin pain and the inability to walk after tripping on a curb. Examination reveals marked hip pain with passive range of motion. A radiograph is shown in Figure 21. Regardless of treatment, what is the most common complication following this injury?
Explanation
REFERENCES: Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Rhoad RC, Davidson RS, Heyman S, et al: Pretreatment bone scan in SCFE: A predictor of ischemia and avascular necrosis. J Pediatr Orthop 1999;19:164-168.
Question 25
Complications following a reverse shoulder prosthesis occur most frequently when performed for what diagnosis? Review Topic
Explanation
Question 26
Figure 13a shows the radiograph of a 9-year-old girl who sustained complete transverse fractures of the radial and ulnar shafts while in-line skating. A manipulative closed reduction is performed, and the result is seen in Figure 13b. What is the next most appropriate step in management?
Explanation
REFERENCES: Price CT, Scott DS, Kurzner ME, Flynn JC: Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
Vittas D, Larsen E, Torp-Pedersen S: Angular remodeling of midshaft forearm fractures in children. Clin Orthop 1991;265:261-264.
Question 27
What is the most common mode of failure following unconstrained total elbow arthroplasty? Review Topic
Explanation
Question 28
An 18-year-old boxer sustained a blow to his right eye in a boxing match. Examination on the sideline reveals hyphema, reduced visual acuity and color vision, and a visual field cut. What is the next step in management? Review Topic
Explanation
Question 29
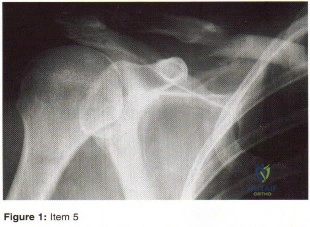
Figures below show the clinical photograph and radiograph obtained from a 62-year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?
Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 30
Figure 42 shows the radiograph of a 70-year-old woman who has had a painful near ankylosis of her dominant elbow for 1 year. Treatment should consist of
Explanation
REFERENCES: Ramsey ML, Morrey BF: Total elbow arthroplasty for nonunion and dysfunctional instability, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
Sim FH, Morrey BF: Nonunion and delayed union of distal humeral fractures, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 655-661.
Question 31
When standing, dorsiflexion of the great toe will accentuate
Explanation
REFERENCES: Mann RA: Biomechanics of the foot and ankle, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 1-44.
Hicks JH: The mechanics of the foot: II. The plantar aponeurosis and the arch. J Anat 1954;88:25.
Question 32
The newborn foot deformity seen in Figures 64a and 64b should initially treated with
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American AcademAyL-oMfadOenrathCooppayedic Surgeons, 2006, pp 240-241.
Farsetti P, Weinstein SL, Ponseti IV: The Long-term functional and radiographic outcomes of untreated
and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265. Question 65
A 4-year-old girl has been limping for the past 2 months. There is no history of trauma, previous injury, fever, or other systemic complaints. Examination reveals a moderate right knee effusio n with a 10-degree knee flexion contracture. What is the next most appropriate step in evaluation?
Arthroscopy
Antinuclear antibody
MRI
Bone scan
HLA-B27
DISCUSSION: The patient presents with juvenile idiopathic arthritis manifestations. The American College of Rheumatology defines this as one or more joints involved with swelling of 6 weeks or longer. A positive antinuclear antibody test would be diagnostic. Consideration should be made to have the patient see an ophthalmologist for evaluation of possible uveitis. Although the patient could have Lyme disease, that choice is not an option. The presence of an elevated antinuclear antibody by itself should not necessarily be used for diagnosing arthritis; however, the test does have clinical utility as a screening test. The frequency of a positive antinuclear antibody test is greatest in younger girls with oligoarticular disease and carries an increased risk for anterior uveitis. Arthroscopy might be indicated if this patient was presenting with a discoid meniscus, but there is no history of clicking, which is often one of the classic signs of discoid meniscus. MRI would not be used to diagnose juvenile idiopathic arthritis, but
MRI would be useful to help diagnose discoid meniscus. A bone scan would show increased uptake in the patient’s knee but again, this would not help diagnose her condition. HLA-B27 has no role in diagnosing juvenile idiopathic arthritis, especially in females.
REFERENCES: Iesaka K, Kubiak EN, Bong LR, et al: Orthopaedic surgical management of hip and knee involvement in patients with juvenile rheumatoid arthritis. Am J Orthop 2006;35:67-73.
Wright DA: Juvenile idiopathic arthritis, in Morrissey RT, Weinstein SL (eds): Love l and Winter’s Pediatric Orthopaedics, ed 6. Philadelphia PA, Lippincott Williams and Wilkins, 2006, pp 405-438. Question 66
An 18-month-old girl is brought in by her parents because of concerns about intoeing, bowlegs, and tripping and fa ling. Prenatal and birth history are otherwise unremarkable. The child’s growth and
development appear to be normal and she has a normal neurologic exam, a straight spine with no defects, and the hips are stable. Examination reveals hip internal rotation of 40 degrees and hip external rotation of 60 degrees. The thigh-foot angle is internal 30 degrees. Feet are straight and supple. Gait is characterized by intoeing with occasional tripping and falling. Based on these findings, what is the most appropriate action?
No treatment because internal tibial torsion slowly resolves on its own
Immediate treatment with a Denis-Browne bar
Distal tibial osteotomies
Proximal femoral derotational osteotomies
Treatment with twister cables PREFERRED RESPONSE: 1
DISCUSSION: The child has classic internal tibial torsion that is very commonly seen in younger children who are just beginning to walk. The normal outcome is for slow resolution of this problem and it seldom requires any treatment. Treatment with a Denis-Browne bar or with twister cables has not been proven to be effective. Surgical treatment at this point is premature and clearly not indicated.
REFERENCES: Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Staheli LT, Corbett M, Wyss C, et al: Lower-extremity rotational problems in children: Normal values to guide management. J Bone Joint Surg Am 1985;67:39-47.

Question 33
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient’s left knee. Abnormal findings include
Explanation
REFERENCES: Ahn JH, Shim JS, Hwang CH, et al: Discoid lateral meniscus in children: Clinical manifestations and morphology. J Pediatr Orthop 2001;21:812-816.
Andrish JT: Meniscal injuries in children and adolescents: Diagnosis and management.
J Am Acad Orthop Surg 1996;4:231-237.
Question 34
The injury shown in Figure 24 was most likely caused by what mechanism of injury?
Explanation
REFERENCE: Kellam JF, Mayo K: Pelvic ring disruptions, in Browner BD, Jupiter JB,
Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1,
pp 1052-1108.
Question 35
An 18-year-old high school football player sustains a thigh injury that results in the findings shown in Figure 1. Initial management should consist of
Explanation
REFERENCES: Anderson JE (ed): Grant’s Atlas of Anatomy. Baltimore, MD, Williams & Wilkins, 1978, pp 4.39-4.49.
Brumet ME, Hontas RB: The thigh, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Antao NA: Myositis of the hip in a professional soccer player: A case report. Am J Sports Med 1988;16:82-83.
Jackson DW, Feagin JA: Quadriceps contusions in young athletes: Relation of severity of injury to treatment and prognosis. J Bone Joint Surg Am 1973;55:95-105.
Question 36
During a posterior cruciate ligament-sacrificing total knee arthroplasty with anterior referencing, 8 mm of distal femur is resected. It is noted that the flexion gap is tight and the extension gap appears stable. What is the next most appropriate step in management?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 281-286, 339-365.
Question 37
When compared with a conventional ultra-high molecular weight polyethylene (UHMWPE) -bearing surface in total hip arthroplasty, a highly cross-linked polyethylene (XLPE) -bearing surface is associated with
Explanation
A. a functional result for at least 20 years.
B. a functional result that deteriorates within the first 10 years.
C. an eventual conversion to a constrained knee arthroplasty.
D. an eventual need for arthrodesis.
Distal femoral varus osteotomy (DFVO) is intended for patients younger than age 50, more active patients with isolated lateral compartment arthritis and valgus malalignment. Although the knee functional score improves at 1-year follow-up, the function scores significantly deteriorate at 10-year follow-up. At 15-year follow-up, the knee function further declines, resulting in an overall failure rate of 48.5%. DFVO provides longer lasting benefit in patients with better presurgical knee function.
Total knee arthroplasty following DFVO provides improved function and successful outcomes. Standard posterior stabilized components provide satisfactory stability after appropriate ligament balancing without the need for stemmed or highly constrained implants for most patients.
Question 38
Figure 16 shows the radiograph of an otherwise healthy 62-year-old woman who fell. Management should consist of
Explanation
REFERENCES: Springer BD, Berry DJ, Lewallen DG: Treatment of periprosthetic fractures following total hip arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162.
Duwelius PJ, Schmidt AH, Kyle RF, et al: A prospective, modernized treatment protocol for periprosthetic femur fractures. Orthop Clin North Am 2004;35:485-492.
Question 39
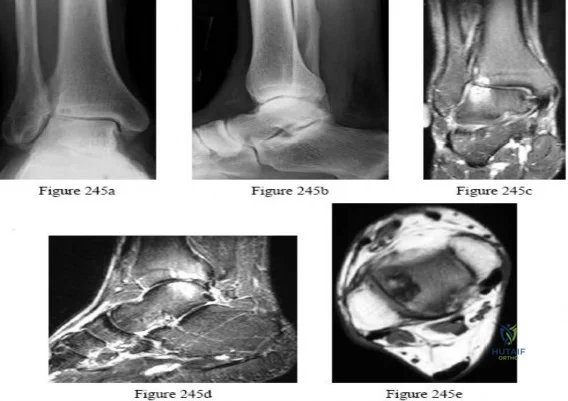
Figures 245a through 245e are the radiographs and MRI scans of a 50-year-old ice hockey referee with a 3-year history of progressive anterolateral ankle pain, a history of multiple ankle sprains, and a fibular fracture he sustained 30 years ago. Examination reveals mild bilateral pes planovalgus feet with passive ankle joint dorsiflexion range of motion of 10 degrees and plantar flexion of 45 degrees without pain. The physician should recommend
Explanation

Question 40
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?
Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the
osteoarthritis.
Question 41
A 52-year-old, right hand dominant man comes for evaluation of right shoulder pain that has been intermittently bothering him for three months. The pain is worse with overhead activities. He denies any history of trauma. His range of forward elevation in the plane of the scapula is painful and is limited to 145 degrees, compared to 170 degrees on his unaffected side. A radiograph is shown in Figure A. He saw another orthopedist a month ago, who ordered an MRI, which showed a small, partial thickness supraspinatus tendon tear. He received a subacromial injection of lidocaine at that time which temporarily relieved 90 percent of the pain he felt with passive forward elevation of his shoulder past 90 degrees. Today he is requesting a subacromial injection of platelet rich plasma (PRP). You tell him that with regard to pain, function and range of motion, subacromial injection of PRP: Review Topic

Explanation
PRP injection.
Platelet rich plasma has been used for the treatment of chronic tendinopathy in different areas with mixed results. No benefit to patients with symptoms of subacromial impingement has been demonstrated for subacromial injection of PRP, when added to a standard therapy program.
Kesikburun et al. conducted a randomized controlled trial in which patients with rotator cuff tendinopathy or partial rotator cuff tears were randomized to receive ultrasound-guided subacromial injection of either PRP or lidocaine, followed by a standard six-week therapy program. The authors found no difference in pain, range of motion or validated outcome scores at one year follow up.
Hall et al. reviewed sports medicine applications for PRP. At that time (2009), with regard to PRP, they concluded that there was "little clinical evidence for its use."
Ketola et al. sought to determine the effectiveness of subacromial decompression for the treatment of subacromial impingement syndrome. They randomized 140 patients to a supervised exercise program or arthroscopic subacromial decompression followed by a supervised exercise program. They found no clinically important differences between the two groups at 24 months follow up.
Figure A shows a right shoulder radiograph without osseous pathology. Incorrect answers:
Question 42
What structure is most at risk with anterior penetration of C1 lateral mass screws?
Explanation
REFERENCES: Currier BL, Todd LT, Maus TP, et al: Anatomic relationship of the internal carotid artery to the C1 vertebra: A case report of cervical reconstruction for chordoma and pilot study to assess the risk of screw fixation of the atlas. Spine 2003;28:E461-E467.
Grant JC: Grant’s Atlas of Anatomy, ed 6. Baltimore, MD, Williams & Wilkins, 1972.
Harms J, Melcher RP: Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine 2001;26:2467-2471.
Question 43
- A 50 year old man who has insulin-dependent diabetes mellitus with associated neuropathy has a stress fracture of the fourth metatarsal. Examination of the foot reveals acute swelling, warmth, and erythema; however, the patient reports very little pain. Treatment should include
Explanation
Question 44
A 40-year-old man is thrown off his motorcycle and sustains an open Type IIIA fracture shown in Figure A. He is taken to the operating room for debridement and reamed intramedullary nailing with a 10mm diameter nail. He returns at 10 months with persistent pain at the fracture site with ambulation. Examination reveals healed wounds with no erythema, warmth or tenderness. Erythrocyte sedimentation rate and C-reactive protein levels are within normal limits. Radiographs taken at that time are shown in Figure B. What is the next best treatment step?

Explanation
Tibial delayed union can be defined as lack of union from 20-26 weeks post-injury, while nonunion is defined as lack of healing at >9mths post-injury, or absence of progressive signs of healing on radiographs for 3 consecutive months. Persistent pain is a symptom of nonunion. ESR and CRP are performed to rule out infection.
Bhandari et al. performed a blinded, multicenter trial on 622 reamed tibial nails and 604 unreamed tibial nails. In closed fractures, patients in the unreamed nail group were at greater risk of primary events than the reamed nail group. There was no difference in groups for open fractures. Primary events were defined as bone-grafting, implant exchange/removal, dynamization, and debridement.
Hak reviewed aseptic tibial nonunion. They discuss exchanged reamed nailing for diaphyseal nonunion, adjunctive plate fixation for metaphyseal nonunion, and nail removal and plating for metadiaphyseal nonunion, external fixation for infected nonunion and distraction osteogenesis of defects.
Figure A shows a mid-diaphyseal tibial fracture Figure B shows nonunion following
IM nailing of the fracture. Illustration A shows union following exchange nailing with a larger 12mm diameter nail.
Incorrect Answers:
Question 45
A 12-year-old boy reports limping and chronic knee pain that is now inhibiting his ability to participate in sports. Clinical examination and radiographs of the knee are normal. Additional evaluation should include
Explanation
REFERENCES: Kocher MS, Bishop JA, Weed B, et al: Delay in diagnosis of slipped capital femoral epiphysis. Pediatrics 2004;113:322-325.
Matava MJ, Patton CM, Luhmann S, et al: Knee pain as the initial symptom of slipped capital femoral epiphysis: An analysis of initial presentation and treatment. J Pediatr Orthop 1999;19:455-460.
Question 46
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. View Abstract at PubMed
Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. Enzinger & Weiss’s Soft Tissue Tumors. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. View Abstract at PubMed
Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. View Abstract at PubMed
Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.View Abstract at PubMed
Question 47
A still active 86-year-old pastry chef falls in her kitchen and notes pain and deformity of her little finger. There are no open wounds. Radiographs are shown in Figures 49a and 49b. What is the most appropriate management?
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.
Question 48
A 6-year-old girl is brought in for orthopaedic examination because she “walks funny” and occasionally trips. Her feet are normal in appearance. Internal rotation of her hips is 60 degrees and external rotation is 40 degrees bilaterally. The thigh-foot angle on the right is -20 degrees, and +10 degrees on the left. What is the source of her gait abnormality?
Explanation
Question 49
Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?
Explanation
REFERENCE: Ofiram E, Polly DW, Gilbert TJ Jr, et al: Is it safe to place pedicle screws in the lower thoracic spine than in the upper lumbar spine? Spine 2007;32:49-54.
Question 50
Figures below show the radiographs, and the CT obtained from a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?

Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 51
A 16-year-old boy has a symptomatic flatfoot deformity that is causing pain, skin breakdown, and shoe wear problems. Shoe modification and an orthosis have failed to provide relief. Examination reveals hindfoot valgus, talonavicular sag, and forefoot abduction that are all passively correctable. Treatment should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631.
Evans D: Calcaneo-valgus deformity. J Bone Joint Surg Br 1975;57:270-278.
Mosca VS: Calcaneal lengthening for valgus deformity of the hindfoot: Results in children who had severe, symptomatic flatfoot and skewfoot. J Bone Joint Surg Am 1995;77:500-512.
Question 52
- A 25 year-old amateur baseball player sustained a dorsal fracture-dislocation of the proximal interphalangeal joint of his long finger. He underwent closed reduction 3 hours ago. Examination reveals mild laxity of the radial collateral fragment involving 30% of the volar articular surface of the middle phalanx. Management should now include
Explanation
“Intra-articular fractures that involve the base of the middle phalanx are usually one of three types 1. Dorsal chip fracture 2. Volar lip fracture, usually combined with a dorsal dislocation of subluxation of the middle phalanx 3. Lateral chip fracture, representing avulsion of bone by the collateral ligament.” Kuczynski has suggested that the volar plate is less mobile in the PIP joint than it is in the MP joint.
“What must always occur with dorsal dislocation, however, is rupture of the volar plate. According to Bowers, the plate is virtually always disrupted from its distal attachment into the base of the middle phalanx. This may with or without a small avulsion chip fracture.”
If the fracture involves more than a third of the joint or is unstable then the PIP joint must be stabilized in a reduced position with early range of motion while restricting PIP hyperextension.
The preferred method of treatment is dorsal extension block splinting for three weeks, then protected range of motion until united.
Question 53
Figure 65 is the lumbar spine MR image of a 63-year-old woman who has a 3-year history of increasingly bothersome back pain and bilateral buttock and leg pain. She has performed 6 weeks of physical therapy, received epidural injections, and experienced some good short-term results, but her leg pain continues to worsen. What is the most appropriate course of treatment?

Explanation
This patient has symptoms consistent with neurogenic claudication secondary to lumbar spinal stenosis and degenerative spondylolisthesis. Her symptoms are chronic and she has undergone an appropriate course of nonsurgical care. Nevertheless, her symptoms are worsening and surgical intervention is a
reasonable consideration. Studies have shown that patients with lumbar spinal stenosis with associated degenerative spondylolisthesis benefit most from decompression of the neural elements that are stenotic and subsequent fusion across the degenerative slip. Anterior lumbar interbody fusion likely will not address stenosis at the level of the slip and may not result in adequate neurologic decompression. Partial laminotomy and diskectomy likely will not provide adequate neural decompression because these procedures would only address unilateral compression and this patient has bilateral issues. Lumbar laminectomy without fusion could be performed but has been associated with results inferior to lumbar laminectomy with fusion when addressing stenosis with spondylolisthesis.
RECOMMENDED READINGS
Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. PubMed PMID: 19487505. View Abstract at PubMed
Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991 Jul;73(6):802-8. PubMed PMID: 2071615. View Abstract at PubMed
Lombardi JS, Wiltse LL, Reynolds J, Widell EH, Spencer C 3rd. Treatment of degenerative spondylolisthesis. Spine (Phila Pa 1976). 1985 Nov;10(9):821-7. PubMed PMID: 4089657. View Abstract at PubMed
RESPONSES FOR QUESTIONS 66 THROUGH 69
Deep surgical-site infection
Adjacent segment degeneration
Pressure ulcers
Iatrogenic neurologic injury
Incidental durotomy
Hardware failure
Match the frequently encountered complication listed above with the appropriate clinical scenario below.
Question 54
When polyethylene is exposed to radiation and subsequently heated, certain chemical changes occur in the material. Which of the following statements best describes these changes?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 32-33.
Question 55
The mangled extremity severity score (MESS) utilizes all of the following variables EXCEPT:

Explanation
The scoring system is as follows: 1. Skeletal / soft-tissue injury: Low energy = 1; Medium energy = 2; High energy = 3; very high energy = 4; 2. Limb ischemia: Pulse reduced or absent but perfusion normal = 1; Pulseless = 2; Cool, paralyzed, insensate = 3; 3. Shock: normotensive = 0; transient hypotension = 1; persistent hypotension = 2; 4. Age:
< 30 = 0; 30-50 = 1; >50 = 2. Limb category scores are doubled for ischemia > 6 hours. The system's original designers reported a cutoff of 7 as predicting amputation.
The referenced study by Ly et al found that the scoring system did not predict functional outcomes at 6 or 24 months. They also found that the Limb Salvage Index; the Predictive Salvage Index; the Nerve Injury, Ischemia, Soft-Tissue Injury, Skeletal Injury, Shock, and Age of Patient Score; and the Hannover Fracture Scale-98 all did not predict outcomes at 6 or 24 months.
Question 56
A 67-year-old retired steelworker was involved in a motor vehicle accident and sustained a midcervical spinal cord injury. Radiographs and MRI scans reveal severe cervical stenosis and spondylosis without fractures or dislocations. Neurologic examination reveals an ASIA C spinal cord impairment with greater motor involvement of the upper extremities than the lower extremities. What is the probability that the patient eventually will become ambulatory?
Explanation
(ASIA C and D) ultimately walked. The poorest prognosis, however, was in ASIA C patients older than age 50, in which only 40% walked.
REFERENCES: Penrod LE, Hegde SK, Ditunno JF Jr: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Northrup BE: Acute injuries to the spine and spinal cord: Evaluation and early treatment, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, p 735.
Question 57
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
Question 58
Which of the following is considered the most common complication of the impaction grafting technique for femoral revision surgery?
Explanation
REFERENCES: Gie GA, Linder L, Ling RS, Simon JP, Slooff TH, Timperley AJ: Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br 1993;75:14-21.
Meding JB, Ritter MA, Keating ME, Faris PM: Impaction bone-grafting before insertion of a femoral stem with cement in revision total hip arthroplasty: A minimum two-year follow-up study. J Bone Joint Surg Am 1998;79:1834-1841.
Question 59
A 55-year-old man presents with low back pain that has progressed over the last year. He reports the pain is worse with activity, especially when bending forward and lifting objects. He denies any pain in the buttocks or lower extremities. On physical he has age-appropriate motion in the lumbar spine. He is neurologically intact in the lower extremities. Figure A shows his axial and sagittal T2-weighted MRI scans. A histological sample of this lesion would most likely show Review Topic

Explanation
Juxtafacet cysts may include synovial cysts or ganglion cysts. Synovial cysts are lined with epithelium (cuboid synovial cells) and contain clear or xanthochromic fluid. Ganglion cysts which have no synovial lining, and contain gelatinous material from myxoid degeneration of the fibrous adventitial tissue.
Xu et al. reviewed the treatment of 195 synovial cysts. They found that patients treated with laminectomy had the highest risk of cyst recurrence (3%). In contrast, decompression with instrumented fusion had the lowest incidences of cyst recurrence (0%) or back pain (although they had the longest hospital stay, and greatest blood loss).
Figure A is a T2-weighted MRI (left, axial; right, sagittal) showing a facet synovial cyst arising from an arthritic left L3-4 facet joint. It occupies much of the space in the spinal canal and indents and displaces the thecal sac. Illustration A shows a hemorrhagic synovial cyst showing synovial cell lining, fibroconnective tissue with widespread hemorrhage, neoangiogenesis, and hemosiderin microdeposits.
Incorrect Answer Answer Answer
1:
2:
3:
Described histology is characteristic of Described histology is characteristic of
Described
histology
is
characteristic
Question 60
Figures 44a through 44c show the radiographs of an 18-year-old female soccer player who fell on her outstretched hand 1 day ago. She denies any history of wrist pain. Examination reveals tenderness at the anatomic snuffbox. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg 1999;24:1206-1210.
Raskin KB, Parisi D, Baker J, et al: Dorsal open repair of proximal pole scaphoid fractures. Hand Clin 2001;17:601-610.
Question 61
When performing a gastrocnemius recession, what structure should be protected?
Explanation
REFERENCES: Pinney SJ, Sangeorzan BJ, Hanen ST Jr: Surgical anatomy of the gastrocnemius resection (Strayer procedure). Foot Ankle Int 2004;25:247-250.
Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 415-417.
Question 62
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
Explanation
REFERENCES: Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
O’Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
Question 63
A 71-year-old man has worsening left hip pain and is indicated for a left total hip arthroplasty (THA). Figure 1 shows a preoperative plan for the patient. The patient is scheduled for a left THA using a direct anterior approach with the pictured implants. If this plan is followed as pictured, what is the likely outcome for this patient? Figure could not be loaded
Explanation
A. spinal fusion.
B. BMI and implant size.
C. mismatch between the metaphysis and diaphysis.
D. modular neck prosthesis.
Question 64
A 6-month-old child has the deformity seen in Figure 10. There are no other known associated problems. What is the etiology of this condition? Review Topic

Explanation
Question 65
A 45-year-old tennis player undergoes surgery for chronic lateral epicondylitis. After returning to play, he notes increasing lateral elbow pain with mechanical catching and locking. Examination shows positive supine posterolateral rotatory instability. What ligament has been injured? Review Topic
Explanation
Question 66
Which of the following best describes the mechanical response of the inferior glenohumeral ligament to repetitive subfailure strains?
Explanation
REFERENCES: Pollock RG, Wang VM, Bucchieri JS, et al: Effects of repetitive subfailure strains on the mechanical behavior of the inferior glenohumeral ligament. J Shoulder Elbow Surg 2000;9:427-435.
Malicky DM, Kuhn JE, Frisancho JC, et al: Nonrecoverable strain fields of the anteroinferior glenohumeral capsule under subluxation. J Shoulder Elbow Surg 2002;11:529-540.
Question 67
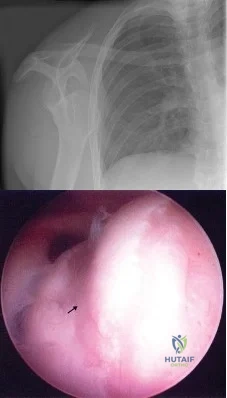
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a Review Topic
Explanation
Question 68
- A 17-year old boy who sustained a closed clavicle fracture after he was ejected from an all-terrain vehicle was treated with a figure-of-8 brace 1 year ago. He now reports continuous pain at the site of the fracture and is unable to actively raise his arm above his head. A radiograph is shown in Figure 1. Management should now include
Explanation
Selection (1) would not provide adequate fixation to promote healing. (2) Electrical stimulation would not be sufficient for the above reasons. (3) Resection of the distal clavicle would not be indicate for this case because it promote further instability of the clavicle and increasing the affected forces to the clavicle.
(5) Kirschner wire fixation with bone graft, the author stated would provide fixation, but they achieved better results with plate fixation and bone graft Question 6 -
A 75-year-old woman sustains a fracture below the level of a total hip prosthesis. Radiographs demonstrate loosening of the prosthetic component. Treatment should consist of
a cast brace
a spica cast
plate fixation
allograft strut fixation
long stem revision
The key to this question lies in the radiographic evidence of loosening of the prosthetic component. The long stem revision is clearly indicated in this case because of various factors, one decreases impingement of the loose stem against the lateral femoral cortex. A non-surgical approach in the elderly patient will only increase the many risk factors such as atelectasis, pneumonia, and thromboembolic disease.[Instructional Course 44 pg. 293-303]
Question 69
A B Figures 90a and 90b are MR images of a 34-year-old man who is referred to your office by his primary care physician after failing 4 months of nonsurgical treatment that included epidural steroids for severe right arm pain occurring in a C6 distribution. He also has associated paresthesias in this region. The patient is weak in elbow flexion and wrist extension. What are his likely outcomes if he is treated with a posterior foraminotomy instead of anterior cervical diskectomy and fusion (ACDF)?

Explanation
This patient has a right-sided C5-C6 disk herniation causing C6 radicular symptoms in the right upper extremity. Studies have shown that both ACDF and posterior foraminotomy confer similar results in terms of pain relief and functional outcome. Patients treated with posterior foraminotomy are at higher risk for neck pain and recurrence of radiculopathy at the same level. Those who receive ACDF are at higher risk for occurrence of radiculopathy at an adjacent level.
RECOMMENDED READINGS
Rao RD, Currier BL, Albert TJ, Bono CM, Marawar SV, Poelstra KA, Eck JC. Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. J Bone Joint Surg Am. 2007 Jun;89(6):1360-78. Review. PubMed PMID: 17575617. View Abstract at PubMed Bolesta MJ, Gill K. Acute neck pain and cervical disk herniation. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:227-234.
Question 70
What is the known manner in which the growth hormone-insulin-like growth factor-I (GH-IGF-I) system functions to stimulate bone growth?
Explanation
REFERENCES: Binder G, Grauer ML, Wehner AV, et al: Outcome in tall stature: Final height and psychological aspects in 220 patients with and without treatment. Eur J Pediatr 1997;156:905-910.
Wang J, Zhou J, Cheng CM, et al: Evidence supporting dual, IGF-I-independent and IGF-I-dependent, roles for GH in promoting longitudinal bone growth. Endocrinol 2004;180:247-255.
Gertner JM: Childhood and adolescence, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 45-47.
Question 71
- Successful healing of a meniscal repair is most likely associated é which of the following tear patterns?
Explanation
Arnoczky et al described the vascular supply to the meniscus and showed that tears within the outer one third of the meniscus have the best healing potential. Rim width is the most important prognostic factor for meniscal repairs; the vascular one third of the meniscus is most conductive to healing. Scott et al found better results when the tear was within 2mm of the meniscosynovial junction. Stone et al found improved healing with rim widths of 6mm or less. Tenuta et al found best results within a rim width of 3mm or less.
Question 72
What is the most common nonanesthetic-related reversible cause of changes in intraoperative neurophysiologic monitoring data? Review Topic
Explanation
Question 73
Figure 1 shows a patient with an open tibia fracture who presents to the emergency department after a propeller injury in brackish water (river water and sea water). What is the most appropriate antibiotic coverage for this patient?

Explanation
soil-borne pathogens (clostridial species). Vancomycin is not indicated for coverage in marine environments, rather it is more commonly used for populations with a high prevalence of nosocomial infections. Sulfamethoxazole-trimethoprim is not used for open fracture coverage.
Question 74
A 9-year-old boy has a painless enlarged mass on the dorsum of his hand. Figures 14a through 14d show the clinical photograph, radiographs, and biopsy specimen. What is the most likely diagnosis?
Explanation
REFERENCES: Porter DE, Emerton ME, Villanueva-Lopez F, Simpson AH: Clinical and radiographic analysis of osteochondromas and growth disturbance in hereditary multiple exostoses. J Pediatr Orthop 2000;20:246-250.
Pierz KA, Stieber JR, Kusumi K, Dormans JP: Hereditary multiple exostoses: One center’s experience and review of etiology. Clin Orthop 2002;402:49-59.
Question 75
A 66-year-old man who underwent shoulder arthroplasty 7 years ago reports progressively worsening shoulder pain for the past 4 weeks after hospital discharge for community-acquired pneumonia. He is afebrile and reports no chills or night sweats. Laboratory studies show a white blood cell count of 11,200/mm3 and an erythrocyte sedimentation rate of 25/h. Shoulder radiographs are negative for fracture, dislocation, or signs of implant loosening. What is the most appropriate management? Review Topic
Explanation
Question 76
Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Coughlin MJ, Mann RA: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby-Year Book, 2000, pp 150-269.
Skalley TC, Myerson MS: The operative treatment of acquired hallux varus. Clin Orthop 1994;306:183-191.
Question 77
Figure 28 shows the postoperative radiograph of a 36-year-old patient. The cerclage cable was placed for a minimal medial calcar fracture seen during femoral preparation. In the immediate postoperative period, what is the highest level of activity that would be safely permitted?
Explanation
REFERENCES: Berend KR, Lombardi AV Jr, Mallory TH, et al: Cerclage wires or cables for the management of intraoperative fracture associated with a cementless, tapered femoral prosthesis: Results at 2 to 16 years. J Arthroplasty 2004;19:17-21.
Schmidt AH, Kyle RF: Periprosthetic fractures of the femur. Orthop Clin North Am 2002;33:143-152.
Greidanus NV, Mitchell PA, Masri BA, et al: Principles of management and results of treating the fractured femur during and after total hip arthroplasty. Instr Course Lect 2003;52:309-322.
Question 78
Figure 2 shows the AP radiograph of an 18-year-old woman with progressive and severe right hip pain. Nonsteroidal anti-inflammatory drugs no longer control her pain. What is the next most appropriate step in management?
Explanation
REFERENCE: Millis MB, Murphy SB, Poss R: Osteotomies about the hip for the prevention and treatment of osteoarthritis. Instr Course Lect 1996;45:209-226.
Question 79
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty? Review Topic
Explanation
Question 80
Compared with surgically treated patients, patients with extra-articular distal third humeral shaft fractures that are treated nonsurgically with functional bracing can be expected to show which of the following findings?
Explanation
Question 81
A 24-year-old baseball pitcher reports pain over the posterior aspect of his shoulder that occurs only during throwing. He notes that the discomfort is greatest during the late cocking and early acceleration phases. Examination reveals localized tenderness with palpation over the external rotators and posterior glenoid. Radiographs are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCES: Meister K, Andrews JR, Batts J, Wilk K, Baumgarten T, Baumgartner T: Symptomatic thrower’s exostosis: Arthroscopic evaluation and treatment. Am J Sports Med 1999;27:133-136.
Ferrari JD, Ferrari DA, Coumas J, Pappas AM: Posterior ossification of the shoulder: The Bennett lesion. Etiology, diagnosis, and treatment. Am J Sports Med 1994;22:171-176.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posteriorsuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 82
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92? Review Topic

Explanation
Question 83
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Explanation
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 84
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?
Explanation
REFERENCES: Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856.
Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Flint L, Babikian G, Anders M, Rodriguez J, Steinberg S: Definitive control of mortality from severe pelvic fracture. Ann Surg 1990;211:703-707.
Question 85
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
Explanation
REFERENCES: Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815.
Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Moro JK, Werier J, MacDermid JC, et al: Arthroplasty with a metal radial head for unreconstructable fractures of the radial head. J Bone Joint Surg Am 2001;83:1201-1211.
Question 86
A 15-year-old boy has had pain in the right knee for the past 3 months. He denies any history of trauma. Examination reveals a firm mass in the distal thigh; the remainder of the examination is unremarkable. A radiograph is shown in Figure 24. What further work-up should be completed prior to biopsy?
Explanation
REFERENCES: Simon MA, Finn HA: Diagnostic strategy for bone and soft tissue tumors. J Bone Joint Surg Am 1993;75:622-631.
Simon M, Springfield D, et al: Biopsy: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 6.
Question 87
A 13-year-old boy has had a painless mass in the arm for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 46a through 46c. What is the most likely diagnosis?
Explanation
REFERENCE: Bernstein KE, Lattes R: Nodular (pseudosarcomatous) fasciitis, a nonrecurrent lesion: Clinicopathologic study of 134 cases. Cancer 1982;49:1668-1678.
Question 88
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?
Explanation
REFERENCES: Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167.
Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 89
Figures 39a through 39c show a clinical photograph and the radiographs of a 32-year-old woman who has been unable to actively extend her dominant ring and small finger for the past two weeks. She has no history of trauma and has minimal pain. Examination reveals full passive range of motion (ROM) of the fingers. Active ROM of the wrist is extension of 40 degrees and flexion of 35 degrees. Active forearm pronation is 45 degrees, and supination is 50 degrees. Treatment should consist of
Explanation
“like a buzzsaw” on the overlying tendons. This is called a Vaughan-Jackson lesion when extensor tendons are ruptured at the distal radial-ulnar joint. Of the dorsal/extensor compartments, typically the digiti minimi is involved first and further ruptures progress radially as the hand ulnarly deviates and the other tendons sublux and are brought within range of the “buzzsaw.” The cited articles state that after a dorsal exposure the hypertrophic tenosynovium is removed from each tendon sytematically, and the wrist joint then evaluated. Any bony spicules which may further damage tendons are removed, and the distal ulna is excised. Tendon transfers, grafts, or repairs are then performed. Surgical results tend to be better with single or double tendon ruptures than with multiple tendon ruptures.
Question 90
Figure 1 is the radiograph of a 50-year old woman with lateral-sided left knee pain. She noticed the pain over the last few months and has had no new injury. She had a microfracture performed of her lateral femoral condyle 5 years ago. What is the likely cause of the finding noted on her radiograph?

Explanation
Question 91
An obese 62-year-old man reports a 10-year history of progressive flatfoot deformity and a 3-month history of a painful callus along the plantar medial midfoot that has not improved with custom shoe wear, pedorthics, and callus care. There is no hindfoot motion, but functional ankle motion remains. He does not have diabetes mellitus. Radiographs are shown in Figures 27a and 27b. What is the best surgical option at this point?
Explanation
REFERENCES: Johnson JE, Yu JR: Arthrodesis techniques in the management of Stage II and III acquired adult flatfoot deformity. Instr Course Lect 2006;55:531-542.
Pinney SJ, Lin SS: Current concept review: Acquired adult flatfoot deformity. Foot Ankle Int 2006;27:66-75.
Question 92
Figure A is a glenoid CT 3D reconstruction of a 26-year-old accountant who has recurrent shoulder instability. His first dislocation occurred after a fall while skiing. He has now sustained his third dislocation, which was reduced in the emergency department prior to being sent to your office. What is the most appropriate definitive treatment? Review Topic
Explanation
patient would be arthroscopic bony Bankart repair.
Older (>20 years old), recreational athletes with minor glenoid bone loss (<20% of the glenoid surface area) may be treated with soft tissue stabilization procedures using suture anchors. Goals of this procedure include tightening and repairing the torn ligament and labrum to the glenoid. Younger, contact sports athletes with large glenoid defect (>20%) may require bony augmentation type of procedures.
Lynch et al. review the clinical presentation, assessment and treatment algorithm for surgical management of bone loss associated with anterior shoulder instability. While defects larger than 25% of glenoid width should be managed with bony augmentation, they recommend soft-tissue stabilization in smaller defects.
Balg et al. analyzed 131 patients following Bankart procedure and identified following risk factors for failure: age <=20, competitive participation in contact sports, shoulder hyperlaxity, Hill-Sachs on AP radiograph, glenoid bone loss of contour on AP radiograph.
Using human cadaveric shoulders with various anterior glenoid defects sizes, The MOON Shoulder Group compared radiography, MRI and CT to determine the most reliable imaging modality for predicting bone loss. Three-dimensional CT, followed by regular CT were the most reliable and reproducible imaging modalities for predicting glenoid bone loss.
Figure A shows an en face sagittal 3D reconstruction of a glenoid with 10% surface area loss.
Incorrect Answers:
Question 93
A deficiency of which of the following is associated with an increased risk of venous thromboembolism?
Explanation
Question 94
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Henry A: Extensile Exposure, ed 3. Edinburgh, UK, Churchill Livingstone, 1995, pp 100-107.
Question 95
Which of the following methods most reliably detects mechanical loosening of the hip?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Miniaci A, Bailey WH, Bourne RB, McLaren AC, Rorabeck CH: Analysis of radionuclide arthrograms, radiographic arthrograms, and sequential plain radiographs in the assessment of painful hip arthroplasty. J Arthroplasty 1990;5:143-149.
Question 96
A 13-year-old girl presents with back pain for 6 months. Figures A and B are SPECT scan and CT images taken at the time of presentation. What is the most likely diagnosis? Review Topic
Explanation
patient
has
spondylolysis.
Spondylolysis is a common cause of back pain in children/adolescents. It is common in sports with repetitive hyperextension (gymnasts, weightlifters, football linemen). It is best seen on lateral and oblique radiographs, CT (best study to diagnose and delineate anatomy), and SPECT.
Saifuddin et al. reviewed the orientation of the pars fracture. They found that only 32% of defects were oriented within 15° of the 45° lateral oblique plane and would be
visible on oblique radiographs. They thus recommend CT scans for spondylolysis.
Cheung et al. reviewed spondylolysis and spondylolisthesis. They advocate pars repair for symptomatic spondylolysis and low-grade, mobile spondylolisthesis with pars defects cephalad to L5 and for those with multiple-level defects.
Figure A is a 99mTc-MDP SPECT scan showing increased uptake at the right L5 pars interarticularis. Figure B is an axial helical CT image showing bilateral spondylolysis at L5. Illustration A is a corresponding sagittal reconstruction image demonstrating right pars fracture into the right L5 superior facet. Illustration B shows the appearance of osteoblastic metastasis (green arrow). Illustration C shows the options for pars repair.
Incorrect
Question 97
Figures 87a and 87b are the radiographs of an 18-year-old pedestrian who was struck by a car. During intramedullary nailing, it is difficult to maintain proper alignment. Poller blocking screws placed in the proximal fragment at which position(s) relative to the nail can help prevent the typical deformity?

Explanation
Question 98
Early postoperative infections following primary total hip arthroplasty are most likely caused by which organism?
Explanation
S aureus is the most common organism cultured in early (fewer than 4 weeks postoperative) periprosthetic infections. Methicillin-resistant S aureus is becoming a more common pathogen in certain patient populations. B hemolytic Streptococcus and some gram-negative infections can also be found in early postoperative infections. S epidermidis, S viridans, and P acnes are more commonly found in late (more
than 4 weeks postoperative) infections.
Question 99
Figure 59 shows properties of a material being tested for use as an implant. What is represented by the portion of the stress-strain curve from point A to point B?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 45-46.
El-Ghannam A, Ducheyne P: Biomaterials, in Mow VC, Huiskes R (eds): Basic Orthopaedic Biomechanics and Mechano-Biology, ed 3. Philadelphia, PA, Lippincott-Raven, 2005, pp 501-503.
Question 100
During total hip arthroplasty, what characteristic of irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene should provide a more wear-resistant construct than traditional gamma- irradiated (2.5-4 Mrad)-in-air polyethylene mated with the same head?
Explanation
Highly cross-linked polyethylene makes material resistant to adhesive wear. Abrasive wear from third bodies does not decrease wear. The fatigue strength of such material is inferior to that of traditional polyethylene, and its resistance to creep is the same, if not lower, than that of traditional polyethylene.
