Full Question & Answer Text (for Search Engines)
Question 1:
During C1-C2 transarticular screw fixation, screw misplacement is most likely to result in injury to the
Options:
- spinal cord if the screw is angled too medial.
- occiput-C1 joint if the screw is angled too cephalad.
- occiput-C1 joint if the screw is angled too lateral.
- vertebral artery if the screw is angled too cephalad.
- vertebral artery if the screw is angled too caudally.
Correct Answer: vertebral artery if the screw is angled too caudally.
Explanation:
DISCUSSION: With C1-C2 transarticular screw fixation, the following structures are potentially at risk: vertebral artery, spinal cord, occiput-C1 joint, and hypoglossal nerve. The vertebral artery is most vulnerable to injury with drill misdirection or anatomic variations in the vertebral foramen. The hypoglossal nerve may be injured if the drill, tap, or screw passes too far anterior to the lateral mass of C1. This complication is extremely rare. The occiput-C1 joint may be injured if the screw trajectory is too cephalad or cranially directed; however,this scenario is very unlikely because the exposure tends to direct the screw into a caudally inclined direction. This caudal orientation has the potential to cause vertebral artery injury, especially in patients who have a large vertebral foramen in the lateral mass of C2 because of erosions (rheumatoid arthritis) or anatomic variation. CT of the vertebral foramen is recommended when C1-C2 transarticular fixation is being considered. Spinal cord injury is extremely unlikely because of the very large size of the spinal canal in the upper cervical spine; the spinal cord lies far away from the lateral masses of C1 and C2.
REFERENCES: Mueller ME, Allgower M, et al: Manual of Internal Fixation, ed 3. New York, NY, Springer-Verlag, 1991, pp 634-636.
Gebhard JS, Schimmer RC, Jeanneret B: Safety and accuracy of transarticular screw fixation C1-C2 using an aiming device: An anatomic study. Spine 1998;23:2185-2189.
Question 2:
In a locking plate screw construct, axial forces are borne by which of the following?
Options:
- Plate
- Screw closest to the fracture
- Screw most distal to the fracture
- Bone-plate interface
- Opposite cortex
Correct Answer: Plate
Explanation:
In a traditional plate system, fracture security depends on the friction between the plate and the underlying bone. Bicortical fixation will decrease the toggle and improve stability. Locking plates absorb axial forces transmitted from the screws. Such plates do not require plate compression against the bone, thus preserving periosteal blood supply.
Question 3:
What is the most common complication following metatarsal osteotomy for a bunion deformity in an adolescent?
Options:
- Hallux varus
- Osteonecrosis
- Recurrence of the hallux valgus
- “Transfer” second metatarsalgia
- Physeal arrest of the first metatarsal
Correct Answer: Recurrence of the hallux valgus
Explanation:
Hallux varus-The question does not specify proximal or distal osteotomies, however it is the most common complication with overcorrection of proximal 1st metatarsal osteotomies. Mann. Pg. 329. “Transfer” 2nd metatarsaglia-most significant, not most common, complication of the Mitchell Osteotomy.Mann pg. 319.
Physeal arrest of the first metatarsal-“While an open epiphysis cannot be considered an absolute contraindication to an osteotomy in either the proximal phalanx, or proximal first metatarsal, it is
important at surgery to determine the exact location of the metaphyseal epiphysis to avoid injury.” Pg. 307 Mann, Surgery of Foot and Ankle.
In studies performed by Blais et. Al. A females full foot growth is usually achieved by 14 years and at 12 years an average less than 1 cm of total foot growth remains with less than 50% of this growth at the proximal epiphysis. Males’ terminal growth expected at 16 years of age with 3cm left at 12 years and approximately 1.5 cm of metatarsal growth.
Most studies show recurrence of Hallux Valgus deformity after surgical correction in the juvenile as inordinately high.
Question 4:
A 40-year-old man sustains a fall while mountain biking and presents with a posterior elbow fracture-dislocation. The elbow is reduced in the ER and noted to be grossly unstable with varus and valgus stress. Imaging demonstrates a two part radial head fracture involving 40% of the articular surface and a fracture involving less than 10% of the coronoid tip. He is taken to the OR for surgical reconstruction. After fixation of the radial head and repair of the LCL complex, the elbow is fluoroscopically examined and noted to be unstable with valgus stress. The elbow is ranged and dislocates at less than 45 degrees of flexion with the forearm in full supination. What is the next best step in management?
Options:
- Application of a hinged external fixator
- Conversion to radial head arthroplasty
- Open reduction internal fixation of the coronoid fragment
- Repair of the medial collateral ligament
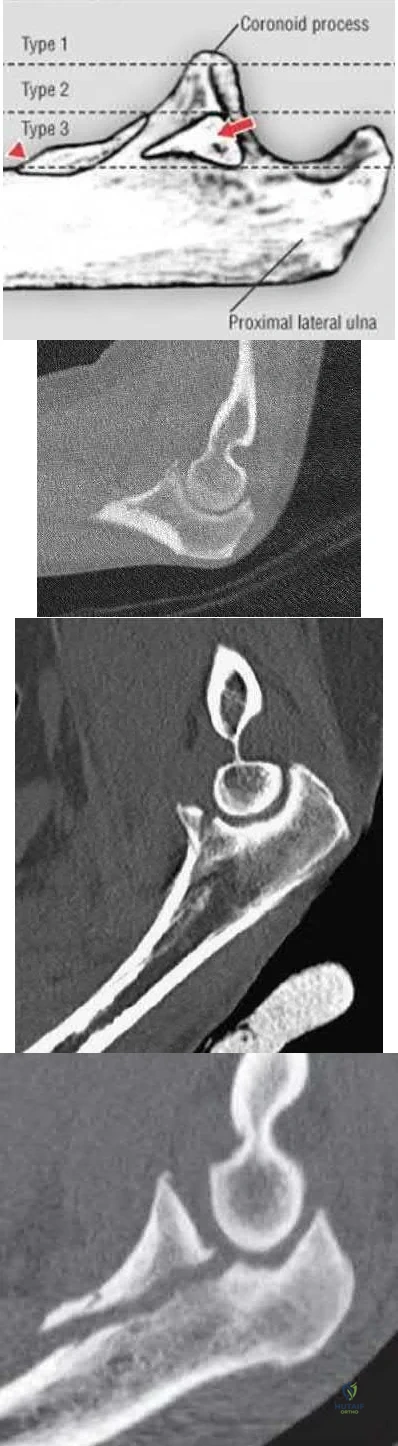
- Splint at 90 degree flexion and full pronation Corrent answer: 4 This patient has persistent elbow instability likely secondary to medial collateral ligament (MCL) rupture and therefore should undergo repair of the MCL, followed by repeat fluoroscopic examination. Small coronoid fractures involving less than or equal to 10% of the coronoid tip do not confer major elbow instability and do not necessitate repair. Terrible triad injuries of the elbow are characterized by: 1. Radial head fracture, 2. Coronoid fracture, and 3. Elbow dislocation. Whether to surgically address the coronoid fracture depends on the size of the fragment (Reagan-Morrey types I-III; Illustration A) as well as elbow stability. Reagan and Morrey suggested that small fractures of the coronoid tip (type I) involving less than 10% of the coronoid may represent anterior capsule avulsions; however, recent cadaveric studies demonstrate that the capsule inserts more distally on the tip and that small fractures often do not contain capsule insertion. Gross elbow instability in the presence of a type I fracture is most likely due to an independent MCL injury and NOT the coronoid avulsion. Surgical repair of type I fractures has not been shown to affect stability and may detrimentally affect elbow range of motion. Matthew et al reviewed the terrible triad injury of the elbow. While the coronoid process provides substantial resistance to posterior subluxation, small fractures involving 10% of the coronoid process have been shown to have little effect on elbow stability. In a cadaveric study of a simulated terrible triad injury, when residual instability was present after radial head repair or arthroplasty and lateral ulnar collateral ligament (LUCL) repair, repair of the MCL was more effective than fixation of small coronoid fractures in restoring elbow stability. However, the authors note that in clinical series of terrible triad injuries, most coronoid fragments were larger than 10%, suggesting that fixation of the coronoid process is usually part of the treatment of terrible triad injuries. Papatheodorou et al performed a retrospective analysis of 14 patients with acute terrible triad injuries and type I or type II coronoid fractures who underwent radial head fixation or arthroplasty and LUCL repair without coronoid fixation. Intraoperative stability was confirmed under fluoroscopy. At 2 year follow up, none of the patients demonstrated elbow instability. Mean elbow flexion-extension was 123 and forearm rotation 145. The authors concluded that terrible triad injuries with type I or II coronoid fractures can be treated without coronoid fixation when intraoperative stability is restored with radial head repair or arthroplasty and LUCL repair. Illustration A demonstrates the Regan-Morrey classification of coronoid fractures. Type I fractures involve < 10% of the coronoid tip and do not result in significant elbow instability. Type II fractures involve < 50% of the coronoid and may result in elbow instability secondary to loss of the anterior bony buttress that resists posterior displacement of the ulna, as well as loss of the anterior capsule insertion. These fractures are often repaired, particularly when associated with elbow instability. Type III fractures involve > 50% of the coronoid and often contain the insertion of the anterior band of the MCL (red arrow). The insertion of the brachialis (red triangle) may also be involved resulting in proximal displacement of the fracture fragment. Surgical repair of type III fractures is necessary to reconstitute the MCL and restore elbow stability. Illustration B is a CT scan of a type I coronoid fracture. Illustration C is a CT scan of a type II coronoid fracture. Illustration D is a CT scan of a type III coronoid fracture. Incorrect Answers:
Correct Answer: Splint at 90 degree flexion and full pronation Corrent answer: 4 This patient has persistent elbow instability likely secondary to medial collateral ligament (MCL) rupture and therefore should undergo repair of the MCL, followed by repeat fluoroscopic examination. Small coronoid fractures involving less than or equal to 10% of the coronoid tip do not confer major elbow instability and do not necessitate repair. Terrible triad injuries of the elbow are characterized by: 1. Radial head fracture, 2. Coronoid fracture, and 3. Elbow dislocation. Whether to surgically address the coronoid fracture depends on the size of the fragment (Reagan-Morrey types I-III; Illustration A) as well as elbow stability. Reagan and Morrey suggested that small fractures of the coronoid tip (type I) involving less than 10% of the coronoid may represent anterior capsule avulsions; however, recent cadaveric studies demonstrate that the capsule inserts more distally on the tip and that small fractures often do not contain capsule insertion. Gross elbow instability in the presence of a type I fracture is most likely due to an independent MCL injury and NOT the coronoid avulsion. Surgical repair of type I fractures has not been shown to affect stability and may detrimentally affect elbow range of motion. Matthew et al reviewed the terrible triad injury of the elbow. While the coronoid process provides substantial resistance to posterior subluxation, small fractures involving 10% of the coronoid process have been shown to have little effect on elbow stability. In a cadaveric study of a simulated terrible triad injury, when residual instability was present after radial head repair or arthroplasty and lateral ulnar collateral ligament (LUCL) repair, repair of the MCL was more effective than fixation of small coronoid fractures in restoring elbow stability. However, the authors note that in clinical series of terrible triad injuries, most coronoid fragments were larger than 10%, suggesting that fixation of the coronoid process is usually part of the treatment of terrible triad injuries. Papatheodorou et al performed a retrospective analysis of 14 patients with acute terrible triad injuries and type I or type II coronoid fractures who underwent radial head fixation or arthroplasty and LUCL repair without coronoid fixation. Intraoperative stability was confirmed under fluoroscopy. At 2 year follow up, none of the patients demonstrated elbow instability. Mean elbow flexion-extension was 123 and forearm rotation 145. The authors concluded that terrible triad injuries with type I or II coronoid fractures can be treated without coronoid fixation when intraoperative stability is restored with radial head repair or arthroplasty and LUCL repair. Illustration A demonstrates the Regan-Morrey classification of coronoid fractures. Type I fractures involve < 10% of the coronoid tip and do not result in significant elbow instability. Type II fractures involve < 50% of the coronoid and may result in elbow instability secondary to loss of the anterior bony buttress that resists posterior displacement of the ulna, as well as loss of the anterior capsule insertion. These fractures are often repaired, particularly when associated with elbow instability. Type III fractures involve > 50% of the coronoid and often contain the insertion of the anterior band of the MCL (red arrow). The insertion of the brachialis (red triangle) may also be involved resulting in proximal displacement of the fracture fragment. Surgical repair of type III fractures is necessary to reconstitute the MCL and restore elbow stability. Illustration B is a CT scan of a type I coronoid fracture. Illustration C is a CT scan of a type II coronoid fracture. Illustration D is a CT scan of a type III coronoid fracture. Incorrect Answers:
Explanation:
Question 5:
- What is the primary mechanism of wear of polyethylene acetabular components?
Options:
- Crevice corrosion
- Oscillatory fretting
- Oxidative degradation
- Adhesion and abrasion
- Fatigue and delamination
Correct Answer: Adhesion and abrasion
Explanation:
Although previous theories on acetabuIar wear implicated fatigue cracking and delamination which is a major mode of polywear in knees, the primary mechanism of wear of polyethylene acetabular components has been shown to be adhesion and abrasion. In an analysis of 128 componenets retrieved at autopsy or revision surgery, wear appeared to occur mostly at the surface of the components and to be due to large strain plastic deformation and orientation of the surface layers into fibrils that subsequently ruptured during multidirectional motion. It was also shown conclusively that 32 mm displayed significantly more wear (volumetric wear) than with either 22 or 26/28 mm heads ( 1 mm increase in size increased volumetric wear by 10%). The wear at the articulating surface was characterized by highly worn polished areas superiorly and less worn areas inferiorly separated by a ridge. Abrasion was very common, occurring after adhesion and plastic deformation of poly fibrils, and abrasion secondary to third body wear. As well, wear rates decreased with longer survival of components, indicating a "wearing in" phenomenon, arguing against oxidative and fatigue wear. Crevice corrossion = occurs in fatigue cracks with low 02 tension (under screw heads,etc.) Oscillatorry fretting = cyclical outer surface abrading from small movements. Fatigue and delamination = predominant in total knees, where stresses are maximum just below the surface of the poly, causing fatigue over time with susequent delamination. In contrast, hip wear occurs primarily at the surface of the poly.
Question 6:
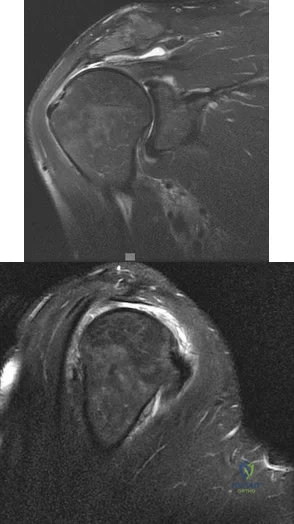
A 45-year-old man reports right shoulder pain with overhead activities only. Figures 47a through 47d show the radiographs, bone scan, and MRI scan of a lesion of the proximal shoulder. What is the most appropriate treatment?
Options:
- Needle biopsy
- Incisional biopsy
- Curettage and grafting
- Observation
- En bloc resection
Correct Answer: Observation
Explanation:
DISCUSSION: The figures show a lesion of the proximal humerus consistent with an enchondroma. The lesion is calcified on the radiographs. There is no cortical destruction, significant endosteal scalloping, or soft-tissue mass. The bone scan shows mild uptake in the area of the proximal humerus, and the T
2
-weighted MRI scan shows a lesion with high uptake, suggesting a lesion with high water content. A CT scan could also be obtained to rule out bone destruction or periosteal reaction. Pain with overhead activities is likely related to the rotator cuff. A biopsy is unlikely to add information because of inherent difficulties interpreting low-grade cartilaginous lesions. Curettage and grafting and en bloc resection are excessive treatments for a benign lesion that is apparently asymptomatic. Observation with a follow-up radiograph in 3 to 6 months is appropriate.
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Question 7:
What is the most frequent complication of both lateral closing wedge high tibial osteotomy and medial opening wedge osteotomy?
Options:
- Patella baja
- Fracture
- Peroneal nerve palsy
- Compartment syndrome
- Infection
Correct Answer: Patella baja
Explanation:
DISCUSSION: Scuderi and associates reported on patellar height after a high tibial osteotomy. Eighty-nine percent of the patellae, as measured by the Insall-Salvati index, and 76.3 percent, as measured by the Blackburne-Peel index, were observed to be lowered. More recently, Wright and associates reported a 64% incidence of patella baja in patients undergoing a medial opening wedge osteotomy. The incidence of intra-articular fracture during medial opening wedge osteotomy has been reported to be as high as 11% by Hernigou and associates, whereas the incidence of intra-articular fracture during lateral closing wedge high tibial osteotomy has been reported to be 10% to 20% by Matthews and associates. The incidence of peroneal nerve palsy with a lateral closing wedge high tibial osteotomy ranges from 0% to 20%, according to Marti and associates, whereas the incidence of peroneal palsy following a medial opening wedge osteotomy has been reported to be 15.7% by Flierl and associates. The exact incidence of compartment syndrome after a high tibial osteotomy is not known; however, it does not reach the level of patella baja. The incidence of deep infection after a lateral closing wedge high tibial osteotomy ranges from 0% to 4% according to Billings and associates.
REFERENCES: Scuderi GR, Windsor RE, Insall JN: Observations on patellar height after proximal tibial osteotomy. J Bone Joint Surg Am 1989;71:245-248.
Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005;13:279-289.
Hernigou P, Medevielle D, Debeyre J, et al: Proximal tibial osteotomy for osteoarthritis
with varus deformity: A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354.
Matthews LS, Goldstein SA, Malvitz TA, et al: Proximal tibial osteotomy: Factors that influence the duration of satisfactory function. Clin Orthop 1988;229:193-200.
Marti CB, Gautier E, Wachtl SW, et al: Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy 2004;20:366-372.
Marti RK, Verhigan RA, Kerkhoffs GM, et al: Proximal tibial varus osteotomy: Indications, technique, and five to twenty-one-year results. J Bone Joint Surg Am 2001;83:164-170.
Flierl S, Sabo D, Hornig K, et al: Open wedge high tibial osteotomy using fractioned drill osteotomy: A surgical modification that lowers the complication rate. Knee Surg Sports Traumatol Arthrosc 1996;4:149-153.
Billings A, Scott DF, Camargo MP, et al: High tibial osteotomy with a calibrated osteotomy guide, rigid internal fixation, and early motion: Long-term follow-up. J Bone Joint Surg Am 2000;82:70-79.
Question 8:
What is the most common indication for revision following unconstrained elbow arthroplasty?
Options:
- Polyethylene wear
- Loosening of the humeral component
- Loosening of the ulnar component
- Instability
- Component failure
Correct Answer: Instability
Explanation:
DISCUSSION: Instability following unconstrained elbow arthroplasty occurs in 10% of patients. Subluxation is twice as common as frank dislocation; however, only 20% of these patients undergo revision. Instability following unconstrained elbow arthroplasty can be caused by component malposition or ligament insufficiency.
REFERENCES: King GJ, Itoi E, Niebur GL, et al: Motion and laxity of the capitellocondylar total elbow prosthesis. J Bone Joint Surg Am 1994;76:1000-1008.
Ring D, Koris M, Jupiter JB: Instability after total elbow arthroplasty. Orthop Clin North Am 2001;32:671-677.
Question 9:
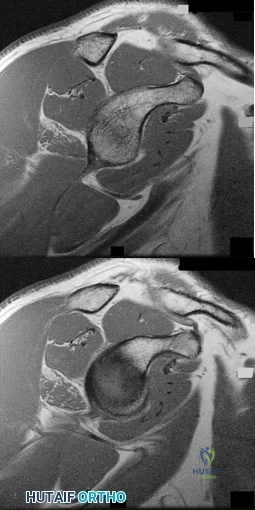
Figures 76a and 76b are the sagittal T1-weighted MRI scans of an active 27-year-old man who has had left dominant extremity shoulder pain and weakness for the past 5 months. He denies any history of a precipitating event but recalls that the pain began around the time he started lifting weights after a year off from lifting. Examination reveals full range of active and passive motion, negative Hawkins and Neer impingement signs, 5/5 abduction strength, 5/5 external rotation strength with arm adducted at his side, and a negative belly press, Gerber lift-off, and O'Brien's test. He does have weakness with resisted external rotation with the arm abducted to 90 degrees. Radiographs are unremarkable. An MRI arthrogram shows no rotator cuff tear or labral tears. What is the most likely diagnosis? Review Topic
Options:
- Scapular dyskenisia
- Quadrilateral space syndrome
- Subacromial impingement syndrome
- Suprascapular nerve compression by a spinoglenoid notch
- Suprascapular nerve compression at the suprascapular notch
Correct Answer: Quadrilateral space syndrome
Explanation:
Examination reveals weakness of the teres minor muscle, and the MRI scan shows moderate isolated atrophy of the teres minor muscle belly. This is consistent with quadrilateral space syndrome, which is compression of the axillary nerve and posterior circumflex humeral artery in the quadrilateral space (bounded by the teres minor, teres major, long head of triceps and the humerus). This syndrome has been related to compression of the neurovascular structures by muscle hypertrophy consistent with the patient's history of lifting weights near the onset of symptoms. The next step in confirming the diagnosis is a subclavian arteriogram with the arm in adduction as well as in abduction and external rotation. Suprascapular nerve compression would be manifested by atrophy and weakness of both the supraspinatus and infraspinatus (if occurring at the suprascapular notch) or just infraspinatus (if occurring at the spinoglenoid notch). The patient does not demonstrate signs or symptoms of either impingement syndrome or scapular dyskenisia.
Question 10:
Following application of topical lidocaine, copious arterial bleeding is noted from the region of 1 neurovascular bundle, and the digit remains cool and pale. What is the best next step?
Options:
- Intraoperative arteriogram
- Wound closure and observation
- Ligation of the digital artery
- Primary repair of the digital artery
Correct Answer: Primary repair of the digital artery
Explanation:
DISCUSSION
Used with permission from Benson LS, Williams CS, Kahle M. Dupuytren’s contracture. J Am Acad Surg. 1998
Jan-Feb;6(1):24-35. Review
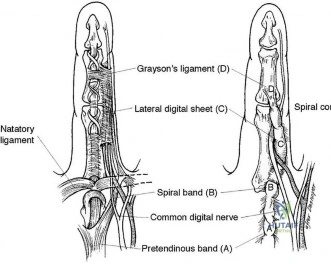
The spiral cord seen in Dupuytren disease arises from the confluence of abnormal fascial thickening of the spiral bands, lateral digital sheet, and Grayson’s ligament. The orientation of these contributing structures results in a continuous band of fibrous tissue spiraling around the neurovascular bundle. As the developing spiral cord contractures from distal to proximal, the cord itself becomes increasingly linear and shorter, causing displacement of the neurovascular bundle both centrally and superficially. This displacement of the neurovascular bundle brings it closer to the skin and midline, making it more vulnerable to surgical trauma.
Studies have demonstrated a high association between a PIP joint flexion contracture and a spiral cord (Figure 52). Spiral cords are also seen in association with a soft, fleshy mass between the proximal digital flexion crease and distal palmar crease in the interdigital space referred to as an interdigital soft-tissue mass. This represents displacement of normal subcutaneous tissues by contracture of the diseased fascia associated with the spiral cord. Dupuytren diathesis, MCP joint contracture, and the presence of knuckle pads are not indicative of a spiral cord.
A complication following surgical treatment of Dupuytren contracture is trauma to the neurovascular bundle. This can be a consequence of blunt or sharp trauma. In the case of traumatic stretch injury from retraction, vasospasm may develop. The treatment of vasospasm includes flexion, warming the digit, and application of topical medication to treat vasospasm. Allowing the newly extended digit to flex is an important first step, particularly in the case of chronic and severe PIP joint contractures. In these cases, the vessel may have shortened over time, and full extension may cause intimal trauma and secondary vasospasm. Cold is also a stimulus for reactive vasospasm, so warming the digit with warm saline irrigation can be helpful. Finally, topically applied lidocaine (without vasoconstrictive additives) can help diminish vasospasm and lead to digital reperfusion. Phentolamine is useful in cases of prolonged vasospasm secondary to administration of anesthetics containing epinephrine. Streptokinase is a thrombolytic agent that may be useful in treatment of embolic or thrombotic vascular disease. Systemic heparin is useful for digital vessel repair but should not be necessary to treat simple vasospasm.
Copious bleeding in the region of the neurovascular bundle following palmar fasciectomy is an indication of potential arterial trauma. In the setting of arterial laceration, direct repair is necessary, particularly when the digit is dysvascular. This means that both digital vessels are involved or that the intact vessel is insufficient to adequately perfuse the digit. During surgery, the vessels can be directly visualized, and arteriography is unlikely to add additional information of value. Streptokinase is not indicated in this situation because it is useful for thrombolysis rather than vascular repair. Ligation of a traumatized digital artery might be appropriate for a digit that is otherwise well perfused; however, this is not appropriate in the setting of a dysvascular digit. Direct suture of the arterial laceration or segmental grafting necessary to restore adequate digital perfusion in this scenario.
RECOMMENDED READINGS
Rayan GM. Dupuytren disease: Anatomy, pathology, presentation, and treatment. J Bone Joint Surg Am. 2007 Jan;89(1):189-98. Review. PubMed PMID: 17256226.
View Abstract at PubMed
Watson HK, Paul H Jr. Pathologic anatomy. Hand Clin. 1991 Nov;7(4):661-8. Review. PubMed PMID: 1769988.
View Abstract at PubMed
Jones NF, Huang JI. Emergency microsurgical revascularization for critical ischemia during surgery for Dupuytren's contracture: a case report. J Hand Surg Am. 2001 Nov;26(6):1125-8. PubMed PMID: 11721263.
View Abstract at PubMed
Question 11:
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of
Options:
- multiple flexible intramedullary nails.
- unreamed intramedullary nailing with static interlocking.
- unreamed intramedullary nailing with dynamic interlocking.
- reamed intramedullary nailing with static interlocking.
- reamed intramedullary nailing with dynamic interlocking.
Correct Answer: reamed intramedullary nailing with static interlocking.
Explanation:
DISCUSSION: The treatment of choice for closed diaphyseal femoral fractures in adults is reamed intramedullary nailing with static interlocking. Reaming allows placement of a larger, stronger implant and offers better healing rates than unreamed nailing. Static interlocking ensures that there is no loss of reduction because of underappreciated fracture lines or comminution.
REFERENCES: Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
Brumback RJ, Ellison TS, Poka A, et al: Intramedullary nailing of femoral shaft fractures: Part III. Long-term effects of static interlocking fixation. J Bone Joint Surg Am 1992;74:106-112.
Question 12:
What portion of the pitching phase creates forces approaching the tensile limit of the medial ulnar collateral ligament of the elbow? Review Topic
Options:
- Early cocking
- Late cocking / Early acceleration
- Ball release
- Follow-through
- Deceleration
Correct Answer: Late cocking / Early acceleration
Explanation:
The late cocking and early acceleration phases are often combined when discussing medial stress on the elbow of the overhand thrower. This is when the greatest valgus moment across the medial elbow occurs and the forces reach the tensile limits of the medial ulnar collateral ligament.
Fleisig et al. were among the first to elucidate the elbow and shoulder kinetics in healthy adult pitchers using high-speed motion capture analysis. Inability to generate sufficient elbow varus torque may result in medial tension, lateral compression, or posteromedial impingement injury.
According to Lynch et al. the late cocking phase of the overhand throw places a marked valgus moment across the medial elbow. This repetitive force reaches the tensile limits of the medial collateral ligament, subjecting it to microtraumatic injury and attenuation. The anterior bundle of the medial collateral ligament has been identified as the primary restraint to valgus load and is the focus of reconstruction.
Incorrect Responses:
1,4,5: The medial elbow forces are less during these phases. 4: Ball release is not one of the 5 phases of throwing and marks the end of the acceleration and beginning of deceleration phase.
Question 13:
Histologically, synovial chondromatosis is characterized by
Options:
- exuberant synovitis (Pannus).
- loose fragments of articular cartilage embedded in the synovium.
- ossified cartilage nodules embedded in the synovium.
- the presence of granulomas in the synovium.
- hemosiderin deposition in the synovium.
Correct Answer: ossified cartilage nodules embedded in the synovium.
Explanation:
DISCUSSION: Histologically, there is metaplastic cartilage arising from the synovium. These lobules of zonates hyaline cartilage are of variable size, are embedded within edematous synovium, and protrude into the joint. The lobules calcify and ossify, leading to the characteristic radiographic appearance. Inflammatory synovitis is not characteristic of synovial chondromatosis. The fluid is clear and serosanguin, not blood tinged.
REFERENCES: Milgram JM: Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;l59:792-801.
Murphy FP, Dahlin DC, Sullivan CR: Articular synovial chondromatosis. J Bone Joint Surg Am 1962;44:77.
Question 14:
What is the most common site of nerve compression in radial tunnel syndrome?
Options:
- Fibrous bands anterior to the radiocapitellar joint
- Recurrent radial vessels
- Medial edge of the extensor carpi radialis brevis (ECRB)
- Proximal aponeurotic edge of the supinator (arcade of Frohse) Radial tunnel syndrome occurs as the result of radial nerve compression at 5 potential sites. These are the fibrous bands anterior to the radiocapitellar joint, the radial recurrent vessels (known as the leash of Henry), the medial edge of the ECRB, the proximal aponeurotic edge of the supinator (arcade of Frohse), and the distal edge of the supinator. The arcade of Frohse is the most common site of compression. The chief discomfort is deep, aching pain in the dorsoradial proximal forearm. Motor and sensory symptoms usually are absent. This condition often is seen when pain persists after surgery for lateral epicondylitis. Lateral epicondylitis and radial tunnel syndrome coexist 5% of the time. Examination findings are tenderness 4 cm distal to the lateral epicondyle, pain with resisted supination, and pain with resisted long finger extension. Electromyogram/nerve conduction study and MRI results usually are normal. A steroid injection can be diagnostic and also may provide temporary relief of symptoms. Surgery involves decompression of all potential areas of compression and allows good to excellent results in only 50% to 90% of cases. Symptoms may take 9 to 18 months to resolve after surgery.
Correct Answer: Proximal aponeurotic edge of the supinator (arcade of Frohse) Radial tunnel syndrome occurs as the result of radial nerve compression at 5 potential sites. These are the fibrous bands anterior to the radiocapitellar joint, the radial recurrent vessels (known as the leash of Henry), the medial edge of the ECRB, the proximal aponeurotic edge of the supinator (arcade of Frohse), and the distal edge of the supinator. The arcade of Frohse is the most common site of compression. The chief discomfort is deep, aching pain in the dorsoradial proximal forearm. Motor and sensory symptoms usually are absent. This condition often is seen when pain persists after surgery for lateral epicondylitis. Lateral epicondylitis and radial tunnel syndrome coexist 5% of the time. Examination findings are tenderness 4 cm distal to the lateral epicondyle, pain with resisted supination, and pain with resisted long finger extension. Electromyogram/nerve conduction study and MRI results usually are normal. A steroid injection can be diagnostic and also may provide temporary relief of symptoms. Surgery involves decompression of all potential areas of compression and allows good to excellent results in only 50% to 90% of cases. Symptoms may take 9 to 18 months to resolve after surgery.
Explanation:
A 25-year-old man has an isolated flexor digitorum profundus laceration just proximal to the distal interphalangeal (DIP) flexion crease of his ring finger. The tendon ends are trimmed, removing 10 mm from each end (secondary to fraying) and the tendon repaired. Four months later, he reports limited finger motion of the long, ring, and small fingers. He cannot fully extend his wrist and all joints of the 3 fingers simultaneously. He has full passive flexion but cannot actively completely close his fingers into a fist. What is the most likely cause?
A. Quadrigia
B. Intrinsic tightness
C. Lumbrical plus deformity
D. Disruption of the tendon repai
Question 15:
For patients undergoing a surgical procedure where the risk of requiring a transfusion is less than 10%, the International Committee of Effective Blood Usage suggests
Options:
- 1 unit of autologous blood.
- 2 units of autologous blood.
- 1 unit of direct donated blood.
- use of cell saver intraoperatively.
- no donation is necessary.
Correct Answer: no donation is necessary.
Explanation:
DISCUSSION: Recent studies have shown a high rate of waste of autologous blood. Therefore, the Committee does not recommend autologous blood donation for procedures that carry a transfusion risk of 10% or less.
REFERENCES: Toy P, Beattie C, Gould S, et al: Transfusion alert: Use of autologous blood. National Heart, Lung, and Blood Institute Expert Panel on the use of autologous blood. Transfusion 1992;35:703-711.
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 16:
Varus intertrochanteric osteotomy for coxa valga commonly produces which of the following results?
Options:
- Decreased abductor lever arm
- Increased hip joint reaction force
- Increased center edge angle
- Abductor lag and lurch
- Lengthening of the leg
Correct Answer: Abductor lag and lurch
Explanation:
DISCUSSION: The greater trochanter is raised as a by-product of varus osteotomy, and a temporary abductor lag and lurch is common for 6 months following surgery. In the absence of hip joint subluxation, varus intertrochanteric osteotomy has no effect on the center edge angle of Wiberg. Varus osteotomy typically increases femoral offset, thereby improving the abductor lever arm and reducing the hip joint reaction force. Even without taking a wedge, varus osteotomy always produces some degree of shortening.
REFERENCE: Millis MB, Murphy SB, Poss R : Osteotomies about the hip for the prevention and treatment of osteoarthrosis. Instr Course Lect 1996;45:209-226.
Question 17:
03 An 18 month old child has bilateral “corner fractures” of the distal femoral metaphyses of unknown origin. Following a skeletal survey, the first step in management should consist of
Options:
- notification of child protection services
- bilateral long leg casts and discharge
- bilateral percutaneous pinning, long leg casts, and discharge
- hospital admission and Bryant’s traction. 5- Hospital admission and modified Bryant’s traction Question 65.03
Correct Answer: notification of child protection services
Explanation:
The key to this question consists in realizing that corner fractures are highly diagnostic for battered children. Thus, the first step in management is to notify protective services. The cited references however remind us that any broken bone could be indicative of child abuse.
back to this question next question
Question 18:
Which of the following statements best describes the process of articular cartilage degeneration in osteoarthritis?
Options:
- In the second stage there is decreased catabolic activity with less matrix breakdown.
- In the second stage there is less chondrocyte proliferation and decreased matrix production.
- Matrix degradation includes increased proteoglycan production, more proteoglycan
- production, and longer glycosaminoglycan chains.
- Cartilage degeneration may be initiated by inflammation, overload, or decreased matrix production.
- Chondrocyte repair responses improve with aging.
Correct Answer: production, and longer glycosaminoglycan chains.
Explanation:
DISCUSSION: Inflammation, overload, or decreased matrix production may lead to cartilage degeneration. During the second stage of articular cartilage degeneration with osteoarthritis, there is increased chondrocyte activity with proliferation and increased production of extracellular matrix. At the same time, there is an increase in catabolic activity with removal of damaged matrix to facilitate matrix remodeling. Chondrocyte repair response decreases with aging. Matrix degradation includes decreased proteoglycan production, less aggregation, and shorter glycosaminoglycan chains.
REFERENCE: Buckwalter JA, Mankin HJ, Grodzinsky AJ: Articular cartilage and osteoarthritis. Instr Course Lect 2005;54:465-480.
Question 19:
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Options:
- Pasteurella
- Streptococcus
- Staphylococcus
- Bacteroides
- Moraxella
Correct Answer: Pasteurella
Explanation:
DISCUSSION: To define bacteria responsible for dog and cat bite infections, a prospective study yielded a median of five bacterial isolates per culture. Pasteurella is most common from both dog bites (50%) and cat bites (75%). Pasteurella canis was the most frequent pathogen of dog bites, and Pasteurella multocida was the most common isolate of cat bites. Other common aerobes included streptococci, staphylococci, moraxella, and neisseria.
REFERENCE: Talan DA, Citron DM, Abrahamian FM, et al: Bacteriologic analysis of infected dog and cat bites. Emergency Medicine Animal Bite Infection Study Group. N Engl J Med 1999;340:85-92.
Question 20:
When planning a research study, the power of the study may be increased by
Options:
- performing a retrospective study.
- performing a prospective study.
- using a case control design.
- decreasing the sample size.
- increasing the sample size.
Correct Answer: increasing the sample size.
Explanation:
The power of a study refers to the researchers' ability to detect a true association when one exists. Power is defined as 1-beta, with beta being the probability of concluding an association does not exist when one actually does (type II error). Increasing the sample size will increase the power of a study. A power analysis can be performed for both retrospective and prospective studies and is independent of the sample population used.
Question 21:
What strategy has proven most effective in preventing transmission of methicillin-resistant Staphylococcus aureus among teammates? Review Topic
Options:
- Separate players with infections in a separate locker room or changing area.
- Treat teammates of the infected player with prophylactic antibiotics.
- Cover any skin lesions with occlusive dressing during sporting activity.
- Ban players with infections from any team event.
Correct Answer: Cover any skin lesions with occlusive dressing during sporting activity.
Explanation:
Prevention is the key to controlling infections among athletes. Proper hygiene is critical and should mandate showering, hand washing, wearing breathable clothing, and shower sandals. The sharing of towels or athletic equipment should be forbidden. Daily skin surveillance by athletes, trainers, and physicians can allow early recognition and treatment initiation during the early stages of infection, limiting risk for further transmission. Additionally, disinfecting shared equipment, covering lesions with occlusive dressing during sporting activity, and restricting the contact activities of infected athletes can limit risk for an infectious outbreak among teammates.
Question 22:
Which of the following nerves travels with the deep palmar arch?
Options:
- Recurrent motor branch of the median nerve
- Medial branch of the median nerve
- Lateral branch of the median nerve
- Superficial branch of the ulnar nerve
- Deep motor branch of the ulnar nerve
Correct Answer: Deep motor branch of the ulnar nerve
Explanation:
DISCUSSION: The ulnar nerve divides alongside the pisiform, and the deep branch supplies the three hypothenar muscles and crosses the palm with the deep palmar arch to supply the two ulnar lumbricals, all interossei, and finally the adductor pollicis. The superficial branch supplies the ulnar digital branches to the small and ring fingers. The median nerve branches are more superficial in the palm near the superficial palmar arch.
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 166-169.
Question 23:
A collegiate football player who sustained a blow to the head during the first quarter of a game is confused for several minutes after the hit but does not lose consciousness. He had two similar episodes in games earlier in the season. When should he be allowed to return to play?
Options:
- Immediately
- In the second half
- In 1 week
- In 4 weeks
- Next season
Correct Answer: Next season
Explanation:
DISCUSSION: Using the traditional concussion grading scale, the patient sustained a grade I concussion because he did not lose consciousness and his abnormal cognitive level lasted less than 1 hour. If this was the player’s first concussion, theoretically he could return to play later in the game provided that he had no confusion, headache, or associated symptoms. However, because it was the third concussion for the year, participation in contact sports should be terminated for the season.
REFERENCES: Guskiewwicz KM, Barth JT: Head injuries, in Schenk RC Jr (ed): Athletic Training and Sports Medicine. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 143-167.
Kelly JP, Rosenberg JH: Diagnosis and management of concussion in sports. Neurology 1997;48:575-580.
Question 24:
A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of
Options:
- anterior diskectomy and fusion at C4-C5.
- immobilization in a Philadelphia collar and voluntary flexion and extension radiographs when awake.
- occipital-cervical fusion with instrumentation.
- halo immobilization for 12 weeks.
- left C6 superior facetectomy and posterior fusion at C6-C7 with instrumentation.
Correct Answer: occipital-cervical fusion with instrumentation.
Explanation:
DISCUSSION: The CT scans reveal an occipital-cervical dissociation with subluxation of the occipitocervical joints bilaterally. Definitive management should consist of an occipital-cervical fusion with instrumentation. Immobilization in a Philadelphia collar is inadequate for this highly unstable injury, and halo immobilization, while affording adequate temporary immobilization, is not appropriate definitive management for this ligamentous injury. The patient does not have an injury at C4-C5 or C6-C7.
REFERENCES: Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries.
J Am Acad Orthop Surg 2002;10:271-280.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 25:
A 12-year-old girl with juvenile rheumatoid arthritis (JRA) has had chronic pain and synovitis about the knee that is now well-controlled medically. Examination reveals 20° of valgus at the knee. Knee range of motion shows 10° to 90° of flexion. Treatment should consist of
Options:
- arthroscopic synovectomy.
- open synovectomy.
- staple hemiepiphyseodesis.
- knee arthrodesis.
- varus osteotomy.
Correct Answer: staple hemiepiphyseodesis.
Explanation:
DISCUSSION: Children with JRA frequently have valgus in association with hypervascularity because of chronic inflammation. This is normally caused by overgrowth of the medial femoral epiphysis. Staple hemiepiphyseodesis, if done early, can reverse the deformity. Osteotomy is usually unnecessary at this age, and there is a risk of stiffness of the knee following the procedure. Synovectomy may be helpful but will not prevent or correct a deformity.
REFERENCE: Rydholm U, Brattstrom H, Bylander B, Lidgren L: Stapling of the knee in juvenile chronic arthritis. J Pediatr Orthop 1987;7:63-68.
Question 26:
Following total knee arthroplasty, a patient is noted to have asymmetrical absent pulses and poor capillary refill. What is the next most appropriate step in management?
Options:
- Observation of the limb for 4 hours to see if the arterial spasm resolves
- Measurement of lower leg compartment pressures
- Magnetic resonance angiogram
- Emergent return to the operating room for wound exploration while the patient anesthesia
- Return to the operating room, obtain a vascular surgery consultation, and intraoperative arteriogram
Correct Answer: Return to the operating room, obtain a vascular surgery consultation, and intraoperative arteriogram
Explanation:
is still under
perform an
DISCUSSION: An assessment of the location of the vascular compromise is necessary prior to surgical exploration. Vascular repair will most likely require a separate surgical exposure. Vascular reperfusion may be accomplished at the time of an arteriogram with the use of a stent in certain situations. Return to the operating room with vascular surgical consultation and intraoperative arteriogram is appropriate.
An immediate postoperative compartment syndrome is unlikely. Magnetic resonance angiogram is not appropriate because of the potential for a delay in diagnosis.
REFERENCE: Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001 ;9;253-257.
Question 27:
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads? Review Topic
Options:
- Nucleus pulposus
- Cartilaginous end plate
- Anterior longitudinal ligament
- Annulus fibrosis
- Cellular matrix
Correct Answer: Annulus fibrosis
Explanation:
The annulus fibrosis has a multilayer lamellar architecture mode of type I collagen fibers. Each successive layer is oriented at 30 degrees to the horizontal in the opposite direction, leading to a “criss-cross” type pattern. This composition allows the annulus, which has the highest tensile modulus, to resist torsional, axial, and tensile loads.
Question 28:
Which medication or supplement is recommended to promote healing of atypical subtrochanteric fractures?
Options:
- - Bisphosphonates
- - Teriparatide
- - Vitamin D
- - Glucosamine chondroitin
Correct Answer: - Teriparatide
Explanation:
DISCUSSION
Use of teriparatide in association with fracture fixation promotes healing because these fractures are associated with delayed healing. The other responses are not associated with healing of these fractures.
RECOMMENDED READINGS
Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster D, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Koval K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Sen HT, van der Meulen MC, Weinstein RS, Whyte M; American Society for Bone and Mineral Research. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010 Nov;25(11):2267-94. doi: 10.1002/jbmr.253. Erratum in: J Bone Miner Res. 2011 Aug;26(8):1987. PubMed PMID: 20842676.
View Abstract at
PubMed
Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F,McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone Miner Res. 2014 Jan;29(1):1-23. doi:10.1002/jbmr.1998. Epub 2013 Oct 1. PubMed PMID: 23712442.
View Abstract at
PubMed
Question 29:
What is the most likely complication following treatment of the humeral shaft fracture shown in Figure 6?
Options:
- Nonunion
- Shoulder pain
- Infection
- Elbow injury
- Radial nerve injury
Correct Answer: Shoulder pain
Explanation:
DISCUSSION: The humerus was treated with an intramedullary nail. Findings from two prospective randomized studies of intramedullary nailing or compression plating of acute humeral fractures have shown approximately a 30% incidence of shoulder pain with antegrade humeral nailing. This is the most common complication in both of these series. Nonunions are present in approximately 5% to 10% of humeral fractures treated with an intramedullary nail. Infection has an incidence of approximately 1%. Elbow injury is unlikely unless the nail is excessively long. Rarely, injury to the radial nerve is possible if it is trapped in the intramedullary canal.
REFERENCES: Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
McCormack RG, Brien D, Buckley RE, et al: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective, randomised trial. J Bone Joint Surg Br 2000;82:336-339.
Question 30:
An 8-year-old boy with moderate factor VIII hemophilia played kickball earlier in the day and now reports progressively severe groin pain and is unable to walk. Examination reveals marked paresthesias over the medial aspect of the distal tibia. What is the most likely diagnosis?
Options:
- Hemorrhage into the iliacus muscle
- Hemorrhage into the quadriceps muscle
- Severe hip joint hemarthrosis
- Slipped capital femoral epiphysis
- Avulsion fracture of the anterior superior iliac spine
Correct Answer: Hemorrhage into the iliacus muscle
Explanation:
DISCUSSION: The iliacus muscle is a frequent site of hemorrhage in patients with severe or moderate hemophilia. In patients with moderate hemophilia, hemorrhage into the iliacus muscle often follows play or sporting events that include forceful contraction of the hip flexor muscles. An expanding iliacus hematoma compresses the adjacent femoral nerve, with one study reporting 60% complete femoral nerve palsy in hemophiliacs with an iliacus or iliopsoas hemorrhage. Femoral nerve compression typically includes paresthesias in the distribution of the terminal saphenous nerve branch. Hip joint hemarthrosis may occur, but this condition is not as frequent in hemophiliacs as muscle hemorrhage into the iliacus muscle. More importantly, a hip joint hemarthrosis is not associated with significant compression of the femoral nerve. Avulsion fractures of the anterior superior iliac spine typically occur during adolescence and are not associated with saphenous nerve paresthesias. Slipped capital femoral epiphysis does not have an increased association with hemophilia and usually occurs during the adolescent years.
REFERENCES: Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 379-426.
Gilbert MS, Radomisli TE: Therapeutic options in the management of hemophilic synovitis. Clin Orthop 1997;343:88-92.
Question 31:
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?
Options:
- Male gender
- Diaphyseal location
- Comminuted displaced fracture
- Young age
- Associated injuries
Correct Answer: Comminuted displaced fracture
Explanation:
DISCUSSION: The patient has a displaced comminuted clavicle middle one third fracture from a high-energy mechanism. Recent literature on high-energy clavicular fractures suggests a higher rate of nonunion than previously reported. A nonunion rate of 30% has been reported by Hill and associates when the fracture fragments are displaced more than 1.5 cm. In addition, several patients had neurologic symptoms related to the injury. Robinson and associates reported an increased risk of nonunion in women, elderly patients, comminuted fractures, and injuries with a lack of cortical contact.
REFERENCES: Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539.
Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than
2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
Robinson CM, Court-Brown CM, McQueen MM, et al: Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am
2004;86:1359-1365.
Question 32:
Figures 51a through 51c show the radiographs of a 7-year-old soccer player who reports a gradual onset of midfoot pain that began shortly after the start of soccer season. He states that the pain is worse with activity and is partially alleviated by rest. Examination reveals soft-tissue swelling, and tenderness and warmth in the region of the talonavicular and navicular cunieform joints. Management should consist of
Options:
- biopsy.
- curettage and bone grafting.
- open reduction and fixation.
- immobilization with a long leg cast and no weight bearing.
- immobilization with a short leg walking cast or fracture boot.
Correct Answer: immobilization with a short leg walking cast or fracture boot.
Explanation:
DISCUSSION: Osteochondrosis of the tarsal navicular (Kohler disease) is an infrequent cause of midfoot pain in children, and the etiology is unknown. The typical radiographic findings include flattening and irregular ossification of the tarsal navicular. The medial cunieform and talus maintain their normal articular contours. The acute process is best treated with rest and immobilization. A short leg walking cast results in relief of pain and a quicker return to activity compared with orthotics, although long-term success is similar with either method of treatment. Children may return to activities when the symptoms subside. The radiographic appearance of the talus begins to normalize by about 8 to 10 months following the onset of symptoms.
REFERENCE: Lutter LD: Sports-related injuries, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992.
Question 33:
Which of the following is the preferred treatment for symptomatic localized pigmented villonodular synovitis (PVNS) of the knee?
Options:
- Observation
- External beam radiation therapy
- Intra-articular radiation therapy
- Resection of nodule only
- Open complete synovectomy
Correct Answer: Resection of nodule only
Explanation:
DISCUSSION: Localized PVNS is a variant of the disease process where the synovial proliferation occurs in one area and usually presents as a discrete mass. It has been effectively treated with complete excision. This may be performed arthroscopically or with arthrotomy. Complete synovectomy and radiation therapy are unnecessary to eradicate the localized form of PVNS.
REFERENCES: Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis.
J Am Acad Orthop Surg 2006;14:376-385.
Kim SJ, Shin SJ, Choi NH, et al: Arthroscopic treatment for localized pigmented villonodular synovitis of the knee. Clin Orthop Relat Res 2000;379:224-230.
Question 34:
Regarding the role of the orthopaedic surgeon in addressing domestic and family violence, all of the following statements are true EXCEPT:
Options:
- Report all cases of child abuse, as this is required by all states
- Report all cases of adult spousal or intimate partner abuse, as this is required by all states
- Hospitalize elderly victims who are in immediate danger and help develop a plan to ensure their safety
- Advocate for appropriate legislation and public policy on violence and abuse related to health care
- Orthopedic surgeons are responsible for knowing the reporting laws and procedures for suspected abuse
Correct Answer: Report all cases of child abuse, as this is required by all states
Explanation:
DISCUSSION: Reporting requirements for adult spousal or intimate partner abuse is not standardized among states and it is the responsibility of the orthopaedic surgeon to understand the laws of his or her
state. The AAOS Advisory statement gives information to assist in meeting the ethical and legal obligations on Domestic and Family Violence and Abuse.
Domestic and family violence affects over 10% of the US population (approximately 32 million Americans). Child abuse and neglect contributed to 1,400 fatalities in 2002 and there was 565,747 reports of suspected elder abuse.
Reporting of suspected child abuse is required in all states. The orthopaedic surgeon should hospitalize elderly victims who are in immediate danger and help develop a plan to insure their safety.
Question 35:
An 18-month-old infant with myelomeningocele and rigid clubfeet has grade 5 quadriceps and hamstring strength, but no muscles are functioning below the knee. What is the best treatment option for the rigid clubfeet?
Options:
- Triple arthrodesis
- Soft-tissue releases as necessary
- Tendon transfers to balance the feet in a neutral plantigrade position
- Physical therapy for range of motion and stretching
- Botulinum injections followed by serial casting
Correct Answer: Soft-tissue releases as necessary
Explanation:
DISCUSSION: This child has the potential to walk and therefore should have all the contracted structures in the feet released as necessary to place the feet in a plantigrade position for fitting of ankle-foot orthoses. Physical therapy, manipulation, and casting may provide some benefit in a newborn with flexible feet but are not effective in an older infant with rigid clubfeet. Botulinum injections and tendon transfers are of no use because there are no muscles functioning below the knee. Tendon releases are more effective than tendon transfers in children with myelomeningocele.
REFERENCES: Mazur JM: Management of foot and ankle deformities in the ambulatory child with myelomeningocele, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 155-160.
Dias LS: Surgical management of acquired foot and ankle deformities, in Sarwark JR, Lubicky JP (eds): Caring for the Child with Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 161-170.
Question 36:
- Which of the following factors is most likely to predispose a patient to dislocation of the patellar component following total knee arthoplasty?
Options:
- Internal rotation of the femoral component
- External rotation of the tibial component
- Lateral placement of the femoral component
- Medial placement of the patellar component
- Excessive resection of the patella
Correct Answer: Internal rotation of the femoral component
Explanation:
The experimental data for this answer came from Anouchi et al The Effects of Axial Rotational Alignment of the Femoral Component on Knee Stability and Patellar Tracking in Total Knee Arthroplasty Demonstrated on Autopsy Specimens. This study looked at knee stability, patellar tracking, and patellofemoral contact points with the femoral component positioned in 5 degrees internal, 5 degrees external, and neutral alignment in relation to the posterior femoral condyles. Total knee arthroplasty was performed on four cadavaric specimens without lateral release.
Internally rotating the femoral component produced abnormal laxity seen at 30, 60, and 90 degrees of flexion. There was no gapping noted in the neutral or externally rotated specimens.
The normal pattern for patellar tracking was a gentle curve with maximal deflection at 15 and 60 degrees of flexion. The maximal medial displacement were lowest for the externally rotated specimens.
Although contact areas could not be quantitatively measured accurately, the contact areas were more evenly distributed between the medial and lateral sides of the patella in the externally rotated specimens than they were in either the internally rotated or neutral specimens.
You have to be careful interpreting this data at least in reference to knee stability. In this study a perpendicular tibial cut was made. The normal tibia has a 30 degree varus slope and thus more bone is resected from the lateral surface. External rotation of the femoral component compensates for this.
No tests were done with lateral placement of the femoral component or medial placement of the patellar component.
Question 37:
A 58-year-old woman who underwent a successful total hip replacement for degenerative arthritis 8 years ago reports groin pain for the past 6 months. A radiograph of the hip is shown in Figure 32. At revision, severe deficiency of the posterior column is noted. What reconstructive option would be most appropriate for the acetabulum?
Options:
- Cementless cup without graft
- Cemented cup without graft
- Cemented cup with structural bone graft
- Bone graft, reconstruction cage, and cemented cup
- Bilobed cementless acetabular component
Correct Answer: Bone graft, reconstruction cage, and cemented cup
Explanation:
DISCUSSION: The radiograph shows medial migration of the cementless acetabular component, strongly suggesting acetabular discontinuity with a combined segmental and cavitary medial deficiency. The treatment of choice is a morcellized or structural graft, supported with a reconstructive cage bridging the pelvic discontinuity, and a cemented cup.
REFERENCES: Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 38:
A 45-year-old man has had left thigh pain for the past 4 months. An AP radiograph, bone scan, MRI scans, and biopsy specimens are shown in Figures 6a through 6f. What is the most appropriate treatment?
Options:
- Physical therapy
- Medical management
- Radiation therapy
- Prophylactic internal fixation
- Wide resection
Correct Answer: Medical management
Explanation:
DISCUSSION: The radiograph demonstrates thickened trabeculae and thickened cortices in the left proximal femur compared to the right, and the bone scan shows increased uptake in this area. The MRI scans show thickened trabeculae with normal marrow signal. These findings are diagnostic of Paget’s disease. Medical treatment, including bisphosphonates and calcitonin, is indicated for painful bone lesions.
REFERENCES: Hadjipavlou AG, Gaitanis IN, Kontakis GM: Paget’s disease of the bone and its management. J Bone Joint Surg Br 2002;84:160-169.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 187-196.
Question 39:
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel’s sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?
Options:
- Biopsy of the soft-tissue mass
- Epidural corticosteroid injection into the lumbar spine
- Four-compartment fasciotomy of the leg
- Fascial release and neurolysis of the superficial peroneal nerve
- Closure of the fascial defect of the superficial peroneal nerve
Correct Answer: Fascial release and neurolysis of the superficial peroneal nerve
Explanation:
DISCUSSION: The patient has entrapment of the superficial peroneal nerve against its fascial opening in the distal leg. It is typically exacerbated by passive or active plantar flexion and inversion of the foot, which leads to traction of the nerve as it exits this opening. Treatment involves release of the fascial opening to reduce this traction phenomenon. Closure of the defect will only aggravate the condition and potentially result in an exertional compartment syndrome. A four-compartment fasciotomy is only indicated for an established compartment syndrome of the leg.
REFERENCES: Styf J: Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165-169.
Sridhara CR, Izzo KL: Terminal sensory branches of the superficial peroneal nerve: An entrapment syndrome. Arch Phys Med Rehabil 1985;66:789-791.
Styf J: Entrapment of the superficial peroneal nerve: Diagnosis and results of decompression.
J Bone Joint Surg Br 1989;71:131-135.
Question 40:
Using methylmethacrylate to fill a biopsy hole in the diaphysis of a femur theoretically achieves what purpose?
Options:
- Local tumor control by chemical cytotoxic effect
- Local tumor kill from heat generation
- Minimizes tumor contamination
- Decreases rate of wound infection
- Reinforces the bone to prevent fracture
Correct Answer: Minimizes tumor contamination
Explanation:
DISCUSSION: Placing cement over a bone biopsy site prevents tumor contamination by controlling hematoma. Even though the use of cement may impart some strength, the femur is still at significant risk for fracture. The use of bone cement in this manner has not been cleared by the FDA, but many physicians feel that it is appropriate when the patient’s health status has been given careful consideration, and the physician has the necessary knowledge and training. The other options are not important reasons to use methylmethacrylate in biopsies.
REFERENCES: Simon MA, Springfield DS, et al: Biopsy: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 55-65.
Simon MA: Biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1982;64:1253-1257.
Question 41:
An active 47-year-old woman with rheumatoid arthritis reports forefoot pain and deformity and has difficulty with shoe wear. Examination reveals hallux valgus and claw toes. A radiograph is shown in Figure 10. What is the most appropriate surgical treatment?
Options:
- Distal chevron osteotomy bunionectomy with lesser metatarsal head resections
- Proximal first metatarsal osteotomy with flexor-to-extensor tendon transfer for the lesser toes
- First metatarsophalangeal arthrodesis with lesser metatarsal head resections
- First tarsometatarsal realignment arthrodesis (Lapidus procedure) with flexor-to-extensor tendon transfer for the lesser toes
- Resection of the base of the hallux proximal phalanx (Keller procedure) with flexor-to-extensor tendon transfer for the lesser toes
Correct Answer: First metatarsophalangeal arthrodesis with lesser metatarsal head resections
Explanation:
DISCUSSION: Rheumatoid arthritis commonly affects the metatarsophalangeal joints, which become destabilized with time resulting in hallux valgus and dislocated lesser claw toes. The result is metatarsalgia as the dislocated claw toes “pull” the fat pad distally. Severe hallux valgus reduces first ray load, which compounds the metatarsalgia because the load is transferred to the lesser metatarsal heads. First metatarsophalangeal arthrodesis restores weight bearing medially and corrects the painful bunion. Metatarsal head resection slackens the toe tendons to allow correction of the claw toes by whatever means necessary and decreases plantar load over the forefoot. Rheumatoid arthritis in the first metatarsophalangeal joint will continue to progress if osteotomies or a Lapidus procedure are performed. Keller resection arthroplasty increases transfer metatarsalgia and reduces push-off power during gait. Flexor-to-extensor tendon transfer of the lesser toes does not address the metatarsalgia and does not correct the dislocation of the metatarsophalangeal joint.
REFERENCES: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 572.
Abdo RV, Iorio LJ: Rheumatoid arthritis of the foot and ankle. J Am Acad Orthop Surg 1994;2:326-332.
Question 42:
- A clinical trial is being conducted on a new orthopaedic device that is different from existing devices that are moderately successful, but have frequent complications when used to treat fractures in the elderly. To comply with international standards for clinical trials, the investigator must include in the study design
Options:
- reassurance that Medicare will pay for the treatment.
- consent forms that patients or their guardians are able to understand.
- a detailed description of the device, omitting the fact that it is part of a study.
- a provision that the patient’s care will be discontinued if he or she does not enroll in the study.
- a provision that the study will be carried out to completion, whether or not the device is as effective as those currently in existence.
Correct Answer: consent forms that patients or their guardians are able to understand.
Explanation:
In any research on human beings, each potential subject must be adequately informed of the aims. methods, anticipated benefits and potential hazards of the study and the discomfort it may entail. He or she should be informed that he or she is at liberty to abstain from participation in the study and that he or she is free to withdraw his or her consent to participation at any time. The physician should then obtain the subject’s freely-given informed consent. preferably in writing.
Question 43:
When a patient has recurrent anterior shoulder instability, a bony glenoid reconstructive procedure should be considered in which clinical setting?
Options:
- Associated humeral avulsion of the glenohumeral ligament (HAGL) lesion
- Non-engaging Hill-Sachs lesion
- Glenoid bone loss of at least 25%
- Anterior labral periosteal sleeve avulsion (ALPSA)
Correct Answer: Glenoid bone loss of at least 25%
Explanation:
HAGL lesions may initially be treated without surgery. Recurrent instability in the setting of a HAGL lesion may be treated with a soft-tissue repair. A non-engaging or non-tracking Hill-Sachs lesion may be treated with an anterior soft-tissue (Bankart) repair. A tracking or engaging lesion may be treated with a bony glenoid procedure or a soft-tissue procedure plus remplissage. An ALPSA lesion may be treated with a soft-tissue procedure unless it is associated with a glenoid bony defect >25%. A glenoid bony defect >25% is associated with substantially higher recurrence than defects <20%, and consideration for bony glenoid reconstruction is advised. Consideration of bone augmentation procedures with less severe glenoid bone loss may be considered
in collision athletes.
Question 44:
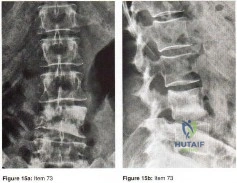
Figures 15a and 15b show the AP and lateral radiographs of the lumbar spine of a 51 year old woman who has had back pain that radiates into the right thigh for the past 3 months. Her medical history is unremarkable except for a mastectomy for breast cancer 12 years ago. What is the most likely diagnosis?
Options:
- Lymphoma
- Hemangioma
- Osteosarcoma
- TB of the spine
- Metastatic breast carcinoma
Correct Answer: Metastatic breast carcinoma
Explanation:
Metastatic disease of the spine occurs in as many as 70% of patients with disseminated cancer and may result in vertebral collapse, spinal instability, and progressive neurologic compromise. Three fourths of these originate from breast, prostate, kidney, or lung carcinoma or myeloma or lymphoma. The vertebral body is affected due to a rich blood supply and sinusoidal vascular distribution. Cord compression is the extrusion of tumor tissue and detritus of bone or disk in the spinal canal following the partial collapse of a vertebral body that has been infiltrated and weakened by a metastatic deposit.
Question 45:
A 68-year-old woman had advanced right knee arthritis and total knee replacement was planned. She learned she had primary biliary cirrhosis at age 41 and now has advancing liver failure. Preoperative coagulation tests show a baseline International Normalized Ratio (INR) of 1.36. Appropriate methods to prevent thromboembolic disease as recommended by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty , include
Options:
- use of mechanical prophylaxis (eg, pneumatic calf compressors) while in the hospital.
- oral warfarin with a goal INR between 2.0 and 3.0.
- low-dose warfarin for 3 weeks postsurgically beginning 48 hours after surgery.
- no prophylaxis because this patient already is partially anticoagulated secondary to her liver disease.
Correct Answer: use of mechanical prophylaxis (eg, pneumatic calf compressors) while in the hospital.
Explanation:
The 2011 AAOS Clinical Practice Guideline,
Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty
, recommends the use of mechanical prophylaxis for patients at increased risk for bleeding (including those with liver disease or hemophilia). This recommendation is the consensus of the workgroup that established these guidelines because there was insufficient evidence to justify a stronger recommendation in this clinical scenario. The other responses use no prophylaxis or pharmacological prophylaxis. Pharmacological prophylaxis is not recommended in patients who are at increased risk for bleeding.
Question 46:
A 58-year-old woman has had a slowly progressing mass over the distal interphalangeal (DIP) joint of her dominant hand with a worsening deformity of her nail. She has no significant medical history but underwent bilateral knee arthroplasties 1 year ago. Radiographs reveal a small osteophyte at the DIP joint dorsally. A clinical photograph and a biopsy specimen are shown in Figures 76a and 76b. What is the most likely diagnosis?
Options:
- Metastatic lung carcinoma
- Mucous cyst
- Synovial sarcoma
- Inclusion cyst
- Felon abscess
Correct Answer: Mucous cyst
Explanation:
DISCUSSION: A mucous cyst is thought to be a ganglion arising from the DIP joint in patients with osteoarthritis. They are frequently associated with nail deformities. Treatment involves removal of the cyst with debridement of DIP joint osteophytes.
REFERENCES: Fritz GR, Stern PJ, Dickey M: Complications following mucous cyst excision. J Hand Surg Br 1997;22:222-225.
Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
Question 47:
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Options:
- Aspiration of joint fluid to obtain a cell count
- Revision of the UKA using primary total knee arthroplasty (TKA) components
- Revision of the UKA using a revision TKA with augments
- Procurement of the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level
Correct Answer: Procurement of the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level
Explanation:
DISCUSSION:
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.
Question 48:
What is the most likely cause of recurrent symptoms following excision of a third web space neuroma?
Options:
- Traumatic neuroma tethered by plantar neural branches
- Regeneration of the transverse intermetatarsal ligament
- Development of an intermetatarsal synovial cyst
- Complex regional pain syndrome
- Metatarsophalangeal joint synovitis
Correct Answer: Traumatic neuroma tethered by plantar neural branches
Explanation:
DISCUSSION: When a recurrent neuroma forms at the end of the resected nerve, it does not retract far enough because either the transection was not proximal enough or it is tethered by plantar neural branches. The transverse intermetatarsal ligament may reform, but it is not associated with pathology. Synovial cysts and synovitis are part of the differential diagnosis but are not associated with neuroma excision. Complex regional pain syndrome may result from neuroma excision, but this is rare and the symptoms are different.
REFERENCES: Beskin JL: Recurrent interdigital neuromas, in Nunley JA, Pfeffer GB, Sanders RW, Trepman E (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 481-484.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
Question 49:
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Options:
- directly posterior to the posterior cruciate ligament (PCL).
- posteromedial to the PCL.
- posterolateral to the PCL.
- in the posteromedial corner of the knee.
Correct Answer: posterolateral to the PCL.
Explanation:
DISCUSSION:
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 50:
Figures 174a and 174b are the radiograph and clinical photograph of a 64-year-old obese woman (body mass index [BMI] of 48) who has controlled diabetes and hypertension. She has failed nonsurgical treatment and a weight loss program. She is considering total knee arthroplasty (TKA). What is the most significant postsurgical risk for this patient?
Options:
- Dissatisfaction after TKA
- Periprosthetic infection and wound complications
- Implant loosening
- Thromboembolic disease
Correct Answer: Periprosthetic infection and wound complications
Explanation:
DISCUSSION
The literature has demonstrated increased risk for complications among obese patients undergoing TKA (10%-30%). An evaluation of TKA among obese patients revealed 3- to 9-fold higher incidence of wound complications and deep-seated infection. Belmont and associates demonstrated that patients with a BMI higher than 40 are at higher risk for overall complications than patients with a BMI lower than 25, with a particularly high risk for developing local wound complications and infection. An increased risk for thromboembolic complications was not shown among obese patients undergoing TKA. Patient-reported outcome scores among obese patients undergoing TKA are equivalent to those of nonobese
patients. There are conflicting data regarding the outcome and survivorship following TKA for obese patients. Although some studies show a difference in patient-reported outcomes at differing postsurgical intervals, most obese patients undergoing TKA are satisfied with the procedure.
Question 51:
A 12-year-old male patient is scheduled to undergo femoral lengthening. The 2 techniques at your disposal are (1) femoral lengthening along the mechanical axis of the limb with an external fixator, and (2) femoral lengthening along the anatomical axis of the femur with a telescoping nail. What happens to the mechanical axis of the limb when performing these techniques? Review Topic
Options:
- There is no mechanical axis deviation in (1), and medial mechanical axis deviation in (2).
- There is lateral mechanical axis deviation in (1) and medial mechanical axis deviation in (2).
- There is no fixed direction of mechanical axis deviation in either technique.
- There is medial mechanical axis deviation in (1) and lateral mechanical axis deviation in (2).
- There is no mechanical axis deviation in (1), and lateral mechanical axis deviation in (2).
Correct Answer: There is no mechanical axis deviation in (1), and medial mechanical axis deviation in (2).
Explanation:
With femoral lengthening of the limb along its mechanical axis, the goal is overall mechanical axis preservation and this is not altered. When lengthening the limb along the anatomical axis of the femur, there is lateral mechanical axis deviation (LAD).
There is a difference of approximately 7° between the mechanical axis of the limb and the anatomical axis of the femur. Lengthening along the anatomical axis of the femur leads to lateral MAD. Similarly, shortening along the anatomical axis of the femur leads to medial MAD.
Kasis et al. described limb shortening of 4cm using external fixator assistance to dial in compression before fixation with a blade plate. They claimed this allowed correction of any tendency to medialize the mechanical axis of the limb prior to plate fixation.
Burghardt et al. described femoral lengthening over a telescoping nail and found lateral shift of the mechanical axis in 26 of 27 limbs, although many were minor and inconsequential. As a rule of thumb, the mechanical axis will shift about 1 mm laterally for every 1 cm of lengthening.
Illustration A illustrates how when lengthening with an external fixator (left), the mechanical axis can be preserved. On the other hand, when lengthening over a nail
(right), the anatomical axis is preserved, but there is lateral MAD (ISKD, intramedullary skeletal kinetic distractor).
Incorrect Answers:
Question 52:
The relocation test is most reliable for diagnosing anterior subluxation of the glenohumeral joint when
Options:
- posterior pressure placed on the humeral head results in increased pain.
- external rotation with the arm in 90 degrees of abduction produces apprehension that is relieved by posterior pressure on the humeral head.
- external rotation with the arm in 90 degrees of abduction produces pain that is relieved by posterior pressure on the humeral head.
- external rotation with the arm in 90 degrees of abduction produces no symptoms, but posterior pressure on the humeral head produces pain and apprehension.
- external rotation with the arm in 90 degrees of abduction produces no symptoms, but posterior pressure on the humeral head produces apprehension.
Correct Answer: external rotation with the arm in 90 degrees of abduction produces apprehension that is relieved by posterior pressure on the humeral head.
Explanation:
DISCUSSION: The relocation test is most accurate when true apprehension is produced with the arm in combined abduction and external rotation and then relieved when posterior pressure is placed on the humeral head. Pain with this test is a less specific response and may occur with other shoulder disorders such as impingement.
REFERENCE: Speer KP, Hannafin JA, Altchek DW, Warren RF: An evaluation of the shoulder relocation test. Am J Sports Med 1994;22:177-183.
Question 53:
Figure 13 shows the MRI scan of a 29-year-old rock climber who reports increasing shoulder pain and weakness. Based on these findings, atrophy will most likely occur in which of the following muscles?
Options:
- Infraspinatus and supraspinatus
- Infraspinatus
- Supraspinatus
- Teres minor
- Deltoid
Correct Answer: Infraspinatus
Explanation:
DISCUSSION: The MRI scan shows a cyst at the spinoglenoid notch. These cysts are often associated with a labral injury, such as a superior labrum anterior and posterior (SLAP) lesion. The suprascapular nerve passes through the suprascapular notch and sends motor branches to the supraspinatus and sensory branches to the capsule. At the spinoglenoid notch, the infraspinatus branch of the suprascapular nerve is compressed by the cyst, leading to isolated infraspinatus atrophy. The teres minor and the deltoid are innervated by the axillary nerve.
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Ianotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Tirman PF, Feller JF, Janzen DL, Peterfy CG, Bergman AG: Association of glenoid labral cysts and labral tears in glenohumeral instability: Radiologic findings and clinical significance. Radiology 1994;190:653-658.
Question 54:
Figure 46 shows the AP radiograph of a patient with right shoulder pain. What is the most likely diagnosis?
Options:
- Periosteal sleeve injury
- Acute type 2 acromioclavicular joint separation
- Rickets
- Traumatic osteolysis
- Distal clavicle fracture
Correct Answer: Traumatic osteolysis
Explanation:
DISCUSSION: Posttraumatic osteolysis of the distal portion of the clavicle is a condition that can be a complication of acute or repetitive trauma. The distal end of the clavicle is frayed and resorbed. Resorption may occur after weeks or months. The end of the clavicle may reconstitute over a period of months, or the acromioclavicular joint may remain widened. The differential diagnosis for distal clavicular erosion also includes rheumatoid arthritis, hyperparathyroidism, neoplastic destruction, cleidocranial dysplasia, and pyknodysostosis. Acutely, a type 2 acromioclavicular joint injury does not result in erosion or resorption of the clavicle. Periosteal sleeve injuries radiographically mimic acromioclavicular joint dislocation. Rickets occurs only in childhood.
REFERENCE: Cahill BR: Osteolysis of the distal part of the clavicle in male athletes. J Bone Joint Surg Am 1982;64:1053-1058.
Question 55:
Which of the following factors is associated with improved outcomes following surgery for hip fractures?
Options:
- Immediate surgical intervention
- Early discharge to a skilled nursing facility
- Choosing spinal versus general anesthesia for surgery
- Choosing total hip arthroplasty instead of hemiarthroplasty for a displaced femoral neck fracture
- Correction of metabolic abnormalities prior to surgical intervention
Correct Answer: Correction of metabolic abnormalities prior to surgical intervention
Explanation:
Many studies have looked at patient outcomes following hip fracture surgery. While early surgery in these patients is recommended, medical optimization prior to surgical intervention is warranted in all cases. Anesthetic type and discharge status have not been proven to alter patient outcomes. Total hip arthroplasty has improved function at 1 year compared with hemiarthroplasty; no changes in mortality have been reported.
Question 56:
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management? L Intensive physiotherapy
Options:
- Alendronate
- Indomethacin
- Radiotherapy
- Excision
Correct Answer: Alendronate
Explanation:
DISCUSSION: The presence of Brooker grade 1 or 2 heterotopic ossification (HO) does not influence the outcome of total hip arthroplasty, whereas restricted range of motion and pain may occur in patients with more severe grade 3 or 4 HO. Treatment may be nonsurgical or surgical. Nonsurgical management includes intensive physiotherapy during the maturation phase of the disease in an attempt to limit the final stiffness. There appears to be no data regarding the effectiveness of this treatment. There is no role for NSAIDs or radiotherapy as a treatment for preexisting HO. Surgical treatment involves excision of the heterotopic bone and can be expected to improve the functional outcome. Bisphosphonates have been used in the past, but their use has been discontinued as they only postpone ossification until treatment is stopped.
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Question 57:
The Arg-Gly-Asp (RGD) sequence of extracellular bone proteins directly allows which of the following?
Options:
- Interaction with integrins
- Chemoattraction of osteoclasts
- Binding to vinculin protein
- Attachment site of Sharpey's fibers
- Decrease in bone stiffness
Correct Answer: Interaction with integrins
Explanation:
The Arg-Gly-Asp (RGD) sequence of extracellular bone proteins such as fibronectin and vibronectin allow binding of integrins on the surface of osteoclasts to enable bone resorption.
Bone homeostasis involves molecular regulation that involves osteoblasts, osteoclasts, and bone. Osteoblasts upregulate and down regulate osteoclasts that absorb bone at the ruffled borders. Integrins, on the surface of osteoclasts bind to extracellular proteins on bone, such as vibronectin, to facilitate bone resorption at the ruffled border. The Arg-Gly-Asp (RGD) sequence plays an important roll in the binding of integrins and extraceullar proteins such as vibronectin and fibronectin. After binding, the intracellular side of these proteins binds to intracellular proteins to allow for change in the intracellular structures and function.
Bosseti et al. review the extracellular matrix interactions involved with bone induction and conduction mechanisms. They note that extracellular binding leads to intracellular protein alteration, which causes different intracellular effects depending on the specific ligand that binds.
Illustration A shows the binding of integrin and vibronectin.
Incorrect Answers:
(SBQ12SP.45) Which of the following lists these materials in order of increasing modulus of elasticity?:
Cortical bone; Titanium; Cobalt-chrome; Stainless steel; Ceramic
Titanium; Cortical bone; Ceramic; Cobalt-chrome; Stainless steel
Cortical bone; Titanium; Stainless steel; Cobalt-chrome; Ceramic
Stainless steel; Titanium; Cortical bone; Ceramic; Cobalt Chrome
Cortical bone; Stainless steel; Titanium; Cobalt-chrome; Ceramic
Cortical bone has the lowest modulus of elasticity of the materials listed, followed by titanium, stainless steel, cobalt-chrome alloy, then ceramic.
Young's modulus of elasticity is the ratio of stress to strain, and represents the stiffness of a material and its ability to resist deformation when placed under tension. Of the materials listed, titanium has the stiffness closest to cortical bone. Ceramic has the highest modulus of elasticity, making it the most stiff of the materials listed.
Illustration A (from Miller's Review) shows the relative stiffnesses of various orthopaedically relevant materials. Young's modulus is the slope of the lines shown. Illustration B (Google images) charts their Young's Modulus.
Incorrect answers:
Question 58:
Figures 1 and 2 are the MRI scans of a 57-year-old man who dislocated his left shoulder after a fall while playing tennis. On examination, he had full passive shoulder range of motion, but he was unable to actively elevate his injured shoulder. Sensation was intact to light touch over the lateral shoulder. What is the most likely etiology of his shoulder weakness?
Options:
- Axillary nerve injury
- Cervical radiculopathy involving the C6 nerve root
- Massive rotator cuff tear with loss of the transverse force couple
- Long head of the biceps tendon rupture with loss of superior stabilizing effect
Correct Answer: Massive rotator cuff tear with loss of the transverse force couple
Explanation:
This patient has a massive rotator cuff tear resulting in disruption of the transverse force couple between the subscapularis anteriorly and the infraspinatus and teres minor posteriorly. These muscles provide dynamic shoulder stability throughout active elevation, and loss of the force couple produces a pathologic increase in translation of the humeral head and decreased active abduction. Active shoulder elevation <90 degrees in the presence of full passive motion is termed pseudoparalysis. The most common neurologic deficit after shoulder dislocation is isolated injury to the axillary nerve. This patient's sensory examination suggests that the axillary nerve is intact. Cervical radiculopathy is less common after shoulder dislocation but has been reported. Conflicting evidence exists regarding the contribution of the long head of the biceps tendon to glenohumeral stability. One study reported minimal electromyographic activity in the biceps during ten basic shoulder motions.
Question 59:
Which of the following is considered the treatment of choice for a 3-cm chondroblastoma of the distal femoral epiphysis with no intra-articular extension?
Options:
- Observation
- Curettage and bone grafting
- Wide local excision with radiation therapy
- Radiation therapy only
- Radiofrequency ablation
Correct Answer: Curettage and bone grafting
Explanation:
DISCUSSION: Curettage and bone grafting typically are the preferred treatment of chondroblastoma, yielding acceptable local recurrence rates of less than 10%. Some surgeons advocate adjuvant therapies such as phenol, liquid nitrogen, or argon beam coagulation. Untreated, these lesions can destroy bone and invade the joint to a significant degree. Large intra-articular lesions may require major joint reconstruction. Wide local excision is rarely required to control the tumor. Radiation therapy is indicated only in unresectable lesions.
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748.
Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 60:
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Options:
- volar open reduction and pinning.
- open reduction, ligament repair, and pinning.
- closed reduction and splinting.
- closed reduction and pinning.
- dorsal open reduction and pinning.
Correct Answer: closed reduction and splinting.
Explanation:
DISCUSSION: The radiograph shows a volarly dislocated lunate. Initial emergent treatment of perilunate dislocations should consist of closed reduction and splinting, especially if the patient exhibits median nerve compression. Open reduction and pinning or ligament repair are necessary but are not emergent. A dorsal approach is sometimes required for ligament repair or bony visualization; however, this can be done in a more semi-elective manner.
REFERENCES: Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 61:
What mechanism is associated with the spontaneous resorption of herniated nucleus pulposus?
Options:
- Macrophage infiltration and phagocytosis
- Granuloma formation
- Antibody mediated destruction
- Complement cascade activation
- Major histocompatibility complex mediated pathways
Correct Answer: Macrophage infiltration and phagocytosis
Explanation:
DISCUSSION: Nonsurgical modalities remain the mainstay for treatment of herniated disks. Spontaneous resorption of herniated disks frequently is detected by MRI. Marked infiltration by macrophages and neovascularization are observed on histologic examination of herniated disks, and the resorption is believed to be related to this process. Many cytokines such as vascular endothelial growth factor, tumor necrosis factor-alpha, and metalloproteinases have been implicated in this process, but none has been found to be singularly responsible.
REFERENCES: Haro H, Kato T, Kamori H, et al: Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res 2002;20:409-415.
Doita M, Kanatani T, Ozaki T, et al: Influence of macrophage infiltration of herniated disc tissue on the production of matrix metalloproteinases leading to disc resorption. Spine
2001;26:1522-1527.
Question 62:
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Options:
- Biceps tear
- Bankart lesion
- Teres minor avulsion
- Suprascapular nerve injury
- Superior labrum anterior and posterior tear
Correct Answer: Suprascapular nerve injury
Explanation:
DISCUSSION: Repetitive overhead slams and serves may produce a traction injury to the distal branch of the suprascapular nerve. Bankart, biceps, and superior labrum anterior and posterior injuries can occur but usually do not produce visible atrophy. Muscle avulsion is uncommon.
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 63:
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of
Options:
- a short leg cast and elevation of the foot.
- fasciotomies of the foot.
- MRI.
- CT.
- stress radiographs.
Correct Answer: fasciotomies of the foot.
Explanation:
DISCUSSION: The patient has a classic history and examination for an acute compartment syndrome of the foot. CT, MRI, or stress radiographs are not necessary prior to emergent fasciotomies of the foot. These studies can be performed after the initial fasciotomies to determine the best long-term management of the fractures. There are nine compartments in the foot. These are decompressed through three incisions (two on the dorsal foot and one medially). A short leg cast does not address the compartment syndrome and could be limb threatening with excessive swelling in a circumferential cast. It is preferable to splint severe crush injuries rather than apply a cast.
REFERENCES: Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Weber TG, Manoli A II: Compartment syndromes of the foot. Foot Ankle Clin 1999;4:473-486.
Question 64:
The incidence of ipsilateral phrenic nerve blockade after an interscalene block approaches
Options:
- 15%.
- 25%.
- 50%.
- 75%.
- 100%.
Correct Answer: 100%.
Explanation:
DISCUSSION: The most common side effect of an interscalene block is ipsilateral phrenic nerve blockade. The phrenic nerve arises chiefly from the fourth cervical ramus (with contributions from the third and fifth) and is the sole motor supply to the diaphragm. Phrenic nerve palsy usually is well tolerated in healthy patients but should be avoided in patients with limited pulmonary function (severe restrictive or obstructive lung disease, myasthenia gravis, or contralateral hemidiaphragmatic dysfunction). The incidence of ipsilateral phrenic nerve blockade afer interscalene block approaches 100%.
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 65:
What is the most common turf toe mechanism of injury?
Options:
- Hyperdorsiflexion of the first metatarsophalangeal (MTP) joint and axial load with the foot fixed in equinus
- Hyperdorsiflexion of the first MTP joint with valgus thrust
- Hyperplantarflexion of the first MTP joint axial load with the foot fixed in equinus
- Hyperplantarflexion of the first MTP joint with valgus thrust
Correct Answer: Hyperdorsiflexion of the first metatarsophalangeal (MTP) joint and axial load with the foot fixed in equinus
Explanation:
DISCUSSION
Turf toe, or capsuloligamentous injury to the first MTP joint, most commonly is caused by an axial load being applied to a fixed, dorsiflexed great toe with the heel off the ground. The external force causes further dorsiflexion of the great toe, leading to injury to the capsuloligamentous complex. A less common mechanism of turf toe is hyperplantarflexion of the great toe with valgus stress, which is seen in beach volleyball players.
RECOMMENDED READINGS
Kadakia AR, Molloy A. Current concepts review: traumatic disorders of the first metatarsophalangeal joint and sesamoid complex. Foot Ankle Int. 2011 Aug;32(8):834-9. Review. PubMed PMID: 22049873.
View Abstract at PubMed
Clanton TO, McGarvey W. Athletic Injuries to the soft tissues of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:1526-1535
Question 66:
The patient returns 1 year later to report curling of her toes and numbness on the plantar surface of her foot. What is the most likely cause of this condition?
Options:
- CRPS
- Plantar fasciitis
- Plantar fibromatosis
- Subclinical compartment syndrome
Correct Answer: Subclinical compartment syndrome
Explanation:
DISCUSSION
Radiographs reveal a Lisfranc fracture dislocation with fractures of the first and second metatarsals. Tenting of skin that is over a bony prominence is an orthopaedic emergency. The fracture dislocation should be reduced without delay. There is no evidence of compartment syndrome of the foot, but this may develop and monitoring is necessary. Toe deformity may develop on a delayed basis because of the subclinical presentation. Nerve irritation is not uncommon with dorsal midfoot surgical incisions. A positive Tinel test result over the midfoot in the distribution of the superficial common peroneal nerve is consistent with a stretch injury to this nerve. CRPS is usually associated with multiple nerve distributions and autonomic nerve findings such as cold hypersensitivity and hyperhidrosis.
RECOMMENDED READINGS
Benirschke SK, Meinberg EG, Anderson SA, Jones CB, Cole PA. Fractures and dislocations of the midfoot: Lisfranc and Chopart injuries. Instr Course Lect. 2013;62:79-91. PubMed PMID: 23395016.
View Abstract at PubMed
Schepers T, Oprel PP, Van Lieshout EM. Influence of approach and implant on reduction accuracy and stability in lisfranc fracture-dislocation at the tarsometatarsal joint. Foot Ankle Int. 2013 May;34(5):705-10. doi: 10.1177/1071100712468581. Epub 2013 Jan 14. PubMed
PMID: 23637239.
View Abstract at PubMed
Question 67:
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal? Review Topic
Options:
- Lateral antebrachial cutaneous nerve
- Radial nerve
- Posterior interosseous nerve
- Median nerve
- Brachial artery
Correct Answer: Radial nerve
Explanation:
The radial nerve is 4 to 7 mm from the anterolateral portal, which is placed 1 cm anterior and 3 cm proximal to the lateral epicondyle. The posterior interosseous nerve can lie 1 to 14 mm from the portal site.
Question 68:
-An athletic 30-year-old sustained multiple injuries in a high-speed motor vehicle collision that resulted in a loss of approximately 30% of blood volume. On arrival to the emergency department, the heart rate is100 and blood pressure is 104/62. The best means with which to evaluate true hemodynamic status is
Options:
- hematocrit.
- serial heart rate.
- serial blood pressure with a manual cuff.
- serial blood pressure with an arterial line.
- lactate and base deficit levels.
Correct Answer: lactate and base deficit levels.
Question 69:
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20°. Management should consist of
Options:
- brace treatment.
- laminectomy, nerve root decompression, and in situ fusion of L4 to the sacrum.
- in situ fusion of L4 to the sacrum.
- excision of the L5 lamina.
- physical therapy.
Correct Answer: in situ fusion of L4 to the sacrum.
Explanation:
DISCUSSION: Indications for surgical treatment of spondylolisthesis include pain and/or progression of deformity. Specifically, surgery is necessary when there is persistent pain or a neurologic deficit that fails to respond to nonsurgical therapy, there is significant slip progression, or the slip is greater than 50%. For patients with mild spondylolisthesis, in situ posterolateral L5-S1 fusion is adequate. In patients with more severe slips (greater than 50%), extension of the fusion to L4 offers better mechanical advantage. Postoperative immobilization may be achieved with instrumentation, casting, or both. In patients with a slip angle of greater than 45°, reduction of the lumbosacral kyphosis with instrumentation or casting is desirable to prevent slip progression. Laminectomy alone is contraindicated in a child. Nerve root decompression is indicated if radiculopathy is present clinically.
REFERENCES: Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Newton PO, Johnston CE II: Analysis and treatment of poor outcomes following in situ arthrodesis in adolescent spondylolisthesis. J Pediatr Orthop 1997;17:754-761.
Question 70:
A 68-year-old man had a 3-year history of shoulder pain that failed to respond to nonsurgical management. Examination reveals forward elevation to 120 degrees and external rotation to 30 degrees. True AP and axillary radiographs and an axial CT scan are shown in Figures 1a through 1c. What management option would lead to the best long-term results?
Options:
- Hemiarthroplasty
- Total shoulder arthroplasty
- Reverse total shoulder arthroplasty
- Arthroscopic debridement
- Glenoid osteotomy and interposition arthroplasty
Correct Answer: Total shoulder arthroplasty
Explanation:
DISCUSSION: The radiographs and CT scan reveal osteoarthritis with posterior subluxation and posterior bone loss. Total shoulder arthroplasty with reaming of the high side to neutralize the glenoid surface has been shown to yield better results than hemiarthroplasty. The amount of bone loss in this patient does not require posterior glenoid augmentation. Reverse total shoulder arthroplasty is indicated for rotator cuff tear arthropathy; therefore, it is not applicable. Arthroscopic debridement has yielded poor results with advanced osteoarthritis and posterior subluxation. Results from glenoid osteotomy have been variable and glenoid osteotomy is not indicated with associated osteoarthritis.
REFERENCES: Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Rodosky MW, Bigliani LU: Indications for glenoid resurfacing in shoulder arthroplasty.
J Shoulder Elbow Surg 1996;5:231-248.
Question 71:
Which is the best initial study for the diagnostic evaluation of diskogenic low back pain? Review Topic
Options:
- MRI
- Diskography
- CT-diskography
- Radiography
- CT
Correct Answer: Radiography
Explanation:
Radiography is the best initial study for the evaluation of diskogenic low back pain. The normal degenerative process can be evaluated. Vacuum phenomenon may be found within the disk space. Other possible sources for back pain should also be evaluated. The other tests may be beneficial but represent later imaging options.
Question 72:
Which of the following conditions is not associated with an increased risk of developing Achilles tendinopathy?
Options:
- Fluoroquinolone antibiotics
- Diabetes mellitus
- Obesity
- Steroid exposure
- Estrogen deficiency
Correct Answer: Estrogen deficiency
Explanation:
DISCUSSION: Diabetes mellitus, obesity, and exposure to steroids have all been associated with the development of Achilles tendinopathy. In addition, Achilles tendinopathy has been associated with a history of hormone replacement therapy and the use of oral contraceptives. Quinolone antibiotics have also been linked to Achilles tendinopathy.
REFERENCES: Holmes GB, Lin J: Etiologic factors associated with symptomatic Achilles tendinopathy. Foot Ankle Int 2006;27:952-959.
Holmes GB, Mann RA, Well L: Epidemiological factors associated with rupture of the Achilles tendon. Contemp Orthop 1991;23:327-331.
Question 73:
Internal impingement of the shoulder and posterosuperior labral pathology in throwers has been most clearly associated with which of the following? Review Topic
Options:
- Posterior capsular contracture
- Anterior capsular laxity
- Coracoacromial arch stenosis
- Rotator cuff disease
- Bennet's lesion
Correct Answer: Posterior capsular contracture
Explanation:
Posterior capular contracture has been recognized to be the primary pathologic process resulting in internal impingement. Internal impingement of the shoulder describes contact between the posterosuperior glenoid labrum and the undersurface of the rotator cuff at the level of the posterior supraspinatus when the shoulder comes into abduction and external rotation. This contact may be physiologic or pathologic and is frequently seen in overhead throwing athletes, possibly resulting in articular-sided rotator cuff tears, glenoid labral tears, tendinitis of the long head of the biceps, anterior instability, glenohumeral internal rotation deficit, and dysfunction of scapular rhythm. Nonsurgical management is the initial treatment of choice with an emphasis on increasing range of motion and improving scapular mechanics. Anterior capsular laxity may be present with internal impingement but is variable and less directly associated with internal impingement than posterior capsular contracture.
Coracoacromial arch stenosis is associated with subacromial impingement and unrelated to internal impingement. Bennett's lesion refers to exostosis or calcification at the posterior capsule and while potentially associated with overhead throwing athletes who may have internal impingement, a causal link between the two has not been established and therefore posterior capsular contracture is the preferred response.
Question 74:
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of
Options:
- buddy taping to the adjacent digit.
- open reduction and surgical fixation of the bony fragment.
- excision of the bony fragment and advancement of the terminal extensor mechanism.
- splinting of the DIP joint with intermittent removal and range-of-motion exercises to prevent stiffness.
- full-time splinting of the DIP joint in slight hyperextension for 6 weeks.
Correct Answer: full-time splinting of the DIP joint in slight hyperextension for 6 weeks.
Explanation:
DISCUSSION: Mallet fingers without DIP joint subluxation can be treated with extension splinting. Surgical fixation may be necessary in bony mallet injuries when the joint is subluxated. Size of the bony fragment, while often correlating with stability, is not always an indication for fixation. Buddy taping allows motion; therefore, the fragment will not heal in the appropriate position. Intermittent splinting with range-of-motion exercises also will not allow the fragment to heal in the appropriate position.
REFERENCES: Crawford GP: The molded polyethylene splint for mallet finger deformities.
J Hand Surg Am 1984;9:231-237.
Wehbe MA, Schneider LH: Mallet fractures. J Bone Joint Surg Am 1984;66:658-669.
Question 75:
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Options:
- Subtrochanteric osteotomy with femoral shortening
- An offset femoral component
- A lateralized liner
- Extended trochanteric osteotomy
Correct Answer: Subtrochanteric osteotomy with femoral shortening
Explanation:
DISCUSSION:
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 76:
A 70-year-old woman has a 3-year history of gradually increasing diffuse and global right knee pain. Her main issues are difficulty with stairs, stiffness with prolonged sitting, and swelling. She has taken NSAIDs and has received intra-articular steroid injections, all with decreasing efficacy. Her right knee examination reveals a range of motion of 15° to 80° with a fixed deformity to varus and valgus stress. Her symptoms are no longer manageable nonsurgically. Radiographs reveal a 30-degree mechanical axis deformity. When using the measured resection technique during total knee arthroplasty (TKA), the best way to avoid femoral malrotation is to reference the
Options:
- anteroposterior axis.
- tibial intramedullary axis.
- posterior condylar axis.
- femoral intramedullary axis.
Correct Answer: anteroposterior axis.
Explanation:
DISCUSSION:
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point, can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 77:
What is the most common malignant bone tumor seen in patients with multiple hereditary exostosis?
Options:
- Dedifferentiated chondrosarcoma
- Mesenchymal chondrosarcoma
- Secondary chondrosarcoma
- Clear cell chondrosarcoma
- Periosteal osteosarcoma
Correct Answer: Secondary chondrosarcoma
Explanation:
DISCUSSION: Secondary chondrosarcomas are most common in patients with multiple hereditary exostosis. Dedifferentiated chondrosarcoma is less common and refers to bone lesions in which a high-grade spindle cell sarcoma component is located immediately adjacent to a low-grade cartilage neoplasm. Mesenchymal chondrosarcoma, clear cell chondrosarcoma, and periosteal osteosarcoma are no more common in patients with multiple hereditary exostosis than in the general population.
REFERENCES: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1660-1669.
Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Chondrosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 275-286.
Question 78:
- Which of the following radiographic findings would be characteristic of the knee joints of a patient with neuropathic osteoarthropathy of the knee?
Options:
- Fragmentation and subluxation of the normal joint articulation
- Varus deformity with medial subchondral sclerosis
- Preferential narrowing of the medial tibiofemoral compartment
- Narrowing of the medial, lateral, and patellofemoral compartments
- Bone proliferation at the patellar tendon and ligament insertion sites
Correct Answer: Fragmentation and subluxation of the normal joint articulation
Explanation:
Neuropathic osteoarthropathy (a.k.a. Charcot joint) develops most often in weight-bearing joints. The most likely cause is diabetes mellitus, but it is also associated with syphilis, leprosy, yaws, congenital insensitivity to pain, spina bifida, myelomeningocele, syringomyelia, aerodystrophic neuropathy, amyloid neuropathy, peripheral neuropathy of alcoholism, spinal cord injury, peripheral nerve injury, post-transplant neuropathy, and intraarticular steroid injections.
The loss of sensation to the joint is followed by severe degenerative changes, osteophyte formation, articular and subchondral fractures, and often calcification of surrounding soft tissues. In the knee, this is a tricompartmental disease and will not selectively affect one compartment over another.
Question 79:
Surgical arthroscopy performed 1 week after injury presents increased risk for
Options:
- deep venous thrombosis.
- popliteal artery dissection.
- complex regional pain syndrome.
- compartment syndrome.
Correct Answer: compartment syndrome.
Explanation:
DISCUSSION
The MR images show injuries to the ACL, PCL, and PLC consistent with a knee dislocation. The optimal timing of surgery after multiligament knee injury remains unclear. Two systematic reviews demonstrated superior clinical outcome scores after early treatment, including higher mean Lysholm scores and a higher percentage of good/excellent International
Knee Documentation Committee scores. Early treatment was associated with increased residual anterior knee instability but no difference in posterior instability, varus laxity, or valgus laxity. Although numbers were limited, the average range of motion and rate of extension loss of at least 5 degrees was similar between groups. More patients in the early-treatment group demonstrated a higher rate of flexion loss of 10 or more degrees and an increased need to undergo a second procedure to address arthrofibrosis, including manipulation under anesthesia and arthrolysis. Return to work did not significantly differ between groups, but return to sports was lower in the early-treatment group. Evidence demonstrates a higher rate of low-energy mechanisms resulting in multiligament knee injury and an increased odds ratio for complications among obese (= 30 degrees kg/m2 patients, including wound complications and neurovascular injury. The complication rate increased 9.2% for every 1-point increase in body mass index. There is no association between complication rate and age, injury mechanism, or timing of surgery. Orthopaedic surgeons performing arthroscopy during the early postinjury period must be mindful of the extensive soft-tissue damage present in these patients, including potential capsular defects. Use of high-pressure irrigation can lead to substantial fluid extravasation into the thigh or lower leg compartments, placing patients at increased risk for compartment syndrome. In addition to avoiding high-pressure irrigation, some orthopaedic surgeons have advocated the creation of generous capsular incisions during portal establishment to allow for ready egress of irrigation fluid from the portal sites rather than into soft tissues.
RESPONSES FOR QUESTIONS 85 THROUGH 88
Excessive medial placement of coracoid autograft
Excessive lateral placement of coracoid autograft
Excessive inferior dissection during the procedure
Excessive retraction and dissection of the medial portion of the conjoint tendon
A 20-year-old right-hand-dominant football player sustained a traumatic shoulder dislocation during a tackle. He has had multiple recurrent dislocations, and radiographs reveal anterior glenoid bone loss. He underwent a Latarjet procedure. Match the most likely complication described below with the surgical error listed above.
Question 80:
What is the most important preoperative factor predicting conversion to total hip arthroplasty after arthroscopic surgery of the hip?
Options:
- Age over 60 years
- Morbid obesity
- Diagnosis of osteoarthritis
- Tobacco use
Correct Answer: Morbid obesity
Explanation:
DISCUSSION:
The authors cited in the references examined large databases to determine the risk factors for conversion to total hip arthroplasty after arthroscopic surgery of the hip. In the study by Kester and associates, obesity had an odds ratio (OR) of 5.6 for conversion to hip arthroplasty, whereas age over 60 years had an OR of
Question 81:
- Which of the following surgical approaches to the hip is associated with the highest incidence of heterotopic ossification?
Options:
- Ilioinguinal
- Extended iliofemoral
- Combined ilioinguinal and Kocher-Langenbeck (posterior)
- Kocher-Langenbeck (posterior)
- Kocher-Langenbeck (posterior) with trochanteric osteotomy
Correct Answer: Extended iliofemoral
Explanation:
Significant extopic bone formation results from a combination of initial trauma to the gluteal muscle mass and surgical exposure of the lateral surface of the pelvis. Extensile (extended iliofemoral or triradiate) approaches are associated with the highest incidence of ectopic bone formation, whereas the ilioinguinal approach is rarely associated with this complication. Many of the fractures described in this chapter require a posterolateral or extensile approach in order to achieve acceptable fracture reduction. When these approaches must be used, local measures may be helpful in reducing the incidence of heterotopic ossification. Debridement of devitalized muscle, particularly the gluteus minimus, has been shown to limit the extent of ectopic bone formation.
Prevention:
incision choice: ilioinguinal if possible
radiation
indocin (give pepcid with it)
Question 82:
Which of the following factors has been shown to increase the risk of peroneal tendon pathology in patients who have undergone posterior plating of lateral malleolar fractures?
Options:
- Use of cut or trimmed plates
- Use of straight (uncontoured) plates
- Use of locked plating
- Low plate placement with a prominent screw head in the distal hole
- Low antiglide plate placement
Correct Answer: Low plate placement with a prominent screw head in the distal hole
Explanation:
Low plate positioning with a prominent screw head in the most distal hole of the plate was shown to be correlated with peroneal tendon lesions. Distal plate placement in the absence of prominent screws was not associated with tendon lesions. Trimmed plates, locked plates, and uncontoured plates have not been shown to increase the risk of peroneal tendon pathology.
Question 83:
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of
Options:
- methylprednisolone and observation.
- posterior laminectomy and spinal fusion.
- anterior spinal fusion.
- halo vest immobilization.
- posterior laminectomy followed by halo vest immobilization.
Correct Answer: posterior laminectomy and spinal fusion.
Explanation:
DISCUSSION: It is not uncommon for patients with ankylosing spondylitis to sustain extension-type fractures, most typically of the cervicothoracic junction. These fractures can appear nondisplaced or minimally displaced initially, making them difficult to diagnose. Because there is no mobility between vertebrae, fractures tend to occur more like those of a transverse fracture of a long bone. In addition, the vertebral bodies are vascular and their canals are relatively enclosed, making them vulnerable to epidural bleeding. The MRI scan reveals an epidural hematoma located posteriorly on the cord; therefore, the treatment of choice is surgical evacuation and a posterior laminectomy. Because of the intrinsic instability of such fractures at the time of the laminectomy, internal fixation and stabilization with a posterior fusion is warranted. A simple laminectomy will only increase instability, and control is unlikely with halo vest immobilization. An anterior procedure will not effectively treat the problem given the location of the hematoma. Consideration can be given to methylprednisolone and observation; however, this will not eradicate the problem.
REFERENCES: Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 84:
Which of the following agents increases the risk for a nonunion following a posterior spinal fusion?
Options:
- Ibuprofen
- Intranasal calcitonin
- Simvastatin
- Gentamycin
- Tamoxifen
Correct Answer: Ibuprofen
Explanation:
DISCUSSION: Nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to increase the risk of pseudarthrosis. In a controlled rabbit study, nonunions were reported with the use of toradol and indomethacin. NSAIDs are commonly used medications with the potential to diminish osteogenesis. Studies clearly have demonstrated inhibition of spinal fusion following the postoperative administration of several NSAIDs, including ibuprofen. Cigarette smoking is another potent inhibitor of spinal fusion.
REFERENCES: Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Martin GJ Jr, Boden SD, Titus L: Recombinant human bone morphogenetic protein-2 overcomes the inhibitory effect of ketorolac, a nonsteroidal anti-inflammatory drug (NSAID), on posterolateral lumbar intertransverse process spine fusion. Spine 1999;24:2188-2193.
Question 85:
Figure 27 shows the AP radiograph of a patient who has late instability. The problem most likely occurred as a result of
Options:
- greater trochanter detachment.
- femoral stem loosening.
- wear.
- osteolysis.
- infection.
Correct Answer: wear.
Explanation:
DISCUSSION: Although dislocation can occur anytime after hip arthroplasty, the highest incidence is observed within the first few months. Dislocation occurring many years after arthroplasty has also been described. In contrast to early dislocation, it appears that late dislocation frequently requires surgical intervention. Recent studies suggest that the incidence of late dislocation may be greater than initially appreciated and that the cumulative rate of dislocation rises with increasing follow-up. The presumed etiologic factors for late instability include long-standing problems with the prosthesis (such as malpositioning of the components) with late manifestation, trauma, deterioration in the neurologic status of the patient, and polyethylene wear. The eccentric position of the femoral head in this patient confirms polyethylene wear. The femoral stem is well-fixed, and the greater trochanter osteotomy has united well. The minor osteolysis observed around the proximal femur is also the consequence of wear and is not the cause of instability. Infection, without component loosening and massive soft-tissue destruction, is not otherwise known to result in late instability.
REFERENCES: Berry DJ, von Knoch M, Schleck CD, et al: The cumulative long-term risk of dislocation after primary Charnley total hip arthroplasty. J Bone Joint Surg Am 2004;86:9-14.
Parvizi J, Wade FA, Rapuri VR, et al: Revision hip arthroplasty for late instability secondary to polyethylene wear. Clin Orthop 2006, in press.
Question 86:
A 17-year-old football player is tackled with an opposing player's helmet hitting him hard in the abdomen. He is knocked backwards and suffers a diaphyseal femur fracture. He denies any loss of consciousness. Vital signs reveal a heart rate of 118, mean arterial pressure (MAP) of 68, and a respiration rate of 32 per minute. A FAST ultrasound study shows trace free fluid in the perisplenic space. A CBC taken prior to bolus IV fluids reveals a hematocrit of 48%, and a blood gas shows a lactate level of 1.8 and a base excess of -2.0. Which of the follow statements regarding the patient's hemodynamic status is correct?
Options:
- A well-placed and well-calibrated arterial line would be the most helpful clinical tool for determining when this patient is out of shock
- The hematocrit well within normal limits means the patient is not in hemodynamic shock
- A combination of heart rate greater than 120 and MAP less than 65 equates to poor tissue perfusion levels
- Normal lactate levels and base excess are markers of adequate tissue perfusion
- His orthopaedic injury alone cannot explain his vital sign derangements and an exploratory laparotomy is indicated
Correct Answer: A well-placed and well-calibrated arterial line would be the most helpful clinical tool for determining when this patient is out of shock
Explanation:
Normal lactate levels or base excess indicate adequate tissue perfusion.
Hypovolemic shock leads to poor tissue perfusion due to inadequate flow or oxygenation. If a patient is in compensated shock (i.e. normal vital signs), there may be ongoing inadequate perfusion of some end-organs. Elevated lactate or a base deficit are markers of poor end-organ perfusion, thus when normalized indicate appropriate end-organ perfusion even if vital sign derangements persist.
Rossaint et al. wrote a comprehensive review article in 2006 in which they discuss principles of fluid management, coagulopathy, hypothermia and tissue oxygenation in hypovolemic shock. In addition to prolonged elevated lactate levels correlating to mortality, lactate levels (or base deficits) can be used to evaluate for compensated shock in the setting of normal hemodynamic status.
Illustration A shows the classification of hypovolemic shock. Note the percent of blood loss required for vital sign abnormalities.
Incorrect Answers:
setting of massive blood loss. The hematocrit only changes once the patient has physiologic or iatrogenic fluid shifts in response to the blood loss. Answer 3: Vital sign derangements indicate uncompensated shock, but do not directly measure tissue perfusion or end-organ damage Answer 5: Though uncommon, bleeding from isolated femur fractures can lead to Class II shock (blood loss 15-30%)
Question 87:
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?
Options:
- Shelf procedure
- Salter osteotomy
- Chiari osteotomy
- Varus derotation osteotomy
- Physical therapy and range-of-motion exercises
Correct Answer: Physical therapy and range-of-motion exercises
Explanation:
DISCUSSION: The prognosis of Legg-Perthes disease in children younger than age 6 years is good. There is no indication that surgical treatment will improve the outcome. Range-of-motion exercises to prevent contracture may be helpful.
REFERENCES: Herring JA, Kim HT, Browne R: Legg-Calve-Perthes disease: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-2134.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 691-704.
Question 88:
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Options:
- a University of California Biomechanics Laboratory (UCBL) orthosis.
- subtalar arthrodesis.
- physeal bar resection.
- tibial epiphysiodesis.
- closing wedge distal tibial osteotomy.
Correct Answer: closing wedge distal tibial osteotomy.
Explanation:
DISCUSSION: Angular deformities of the ankle can occur following physeal injury. While an orthosis may be beneficial, the deformity is at the level of the ankle rather than the hindfoot. An epiphysiodesis or physeal bar resection would not be indicated as the growth plates are closed. Correction of the angular deformity should level the ankle joint and normalize the weight-bearing stresses on the ankle. This is most easily achieved with a closing wedge distal tibial osteotomy with or without concomitant osteotomy of the fibula.
REFERENCES: Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442.
Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 89:
A 72-year-old man injured his right shoulder after tripping over a chair leg. Radiographs obtained in the emergency department reveal an isolated anterior dislocation. After successful closed reduction, the patient has recurrent anterior instability and is unable to elevate the arm. What is the most likely cause of the recurrent instability?
Options:
- Infection of the anterior glenoid labral detachment
- Anterior glenoid fracture
- Axilllary nerve palsy
- Occult surgical neck fracture
- Rotator cuff tear
Correct Answer: Rotator cuff tear
Explanation:
DISCUSSION: A rotator cuff tear is the most common cause of recurrent instability following a first-time dislocation in patients older than age 40 years. Dislocations occur through a posterior mechanism rather than by an isolated labral avulsion or a Bankart lesion as seen in younger patients.
REFERENCES: Nevaiser RJ, Nevaiser TJ: Recurrent instability of the shoulder after age 40.
J Shoulder Elbow Surg 1995;4:416-418.
Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294.
Question 90:
Figures 157a and 157b are the radiographs of a 22-year-old laborer who has progressively increasing lateral knee pain that is unresponsive to nonsurgical treatment. What is the most appropriate treatment at this time?
Options:
- Distal femoral osteotomy
- Proximal tibial osteotomy
- Lateral unicompartmental knee arthroplasty
- Total knee arthroplasty (TKA)
Correct Answer: Distal femoral osteotomy
Explanation:
DISCUSSION
Distal femoral osteotomy is the preferred surgical treatment for this young patient. A varus-producing proximal tibial osteotomy is not indicated with valgus deformity and lateral femoral hypoplasia. Osteotomy on the tibial side would result in obliquity of the joint line and improper loading. Lateral unicompartmental arthroplasty or TKA are both less appropriate for this patient, who will be placing high demands on his knee; these demands will pose high risk for premature failure of an artificial knee implant and could necessitate revision surgery.
Question 91:
A 65-year-old woman has significant neck pain after falling and striking her head. A radiograph and sagittal CT scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Options:
- Degenerative spondylolisthesis
- Superior facet fracture
- Inferior facet fracture
- Perched unilateral facet dislocation
- Bilateral facet dislocation
Correct Answer: Perched unilateral facet dislocation
Explanation:
DISCUSSION: The radiograph shows a displacement of C5 on C6 of approximately 25%. The CT scan shows a perched facet at C5-6. There is no evidence of a facet fracture. A bilateral facet dislocation would show a displacement of more than 50%.
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, pp 927-937.
Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2003, pp 455-458.
Question 92:
A 10-year-old boy reports a gradual onset of weakness; however, he is fully ambulatory. History reveals that he has a 17-year-old brother who has just stopped walking because of a similar condition. Laboratory studies show a creatine kinase level of 5,480 IU/L (normal 25 to 232 IU/L), and examination shows a slightly positive Gower sign. What is the most likely diagnosis?
Options:
- Spinal muscular atrophy, type II
- Myotonic dystrophy
- Duchenne muscular dystrophy
- Becker muscular dystrophy
- Hereditary motor sensory neuropathy, type II (HMSN)
Correct Answer: Becker muscular dystrophy
Explanation:
DISCUSSION: The patient has Becker muscular dystrophy. Patients with this condition have a slower rate of progression of disease compared with patients who have Duchenne muscular dystrophy, and walking may continue into the late teens. The creatine kinase level is not as high as in Duchenne muscular dystrophy, which can range from 20,000 to 30,000 IU/L. Becker muscular dystrophy is allelic to Duchenne muscular dystrophy, resulting in a mutation in the dystrophin gene. Myotonic dystrophy is characterized by a progressive inability to relax the muscles after contracture. The Gower sign is not helpful in this disease. Patients with Charcot-Marie-Tooth disease, one type of which is also known as HMSN type II, do not have elevated creatine kinase levels and usually present with a foot deformity. Spinal muscular atrophy, type II, usually presents with severe weakness in the second year of life.
REFERENCES: Matsuo M: From molecular diagnosis to gene therapy. Brain Dev 1996;18:167-172.
Darras BT: Molecular genetics of Duchenne and Becker muscular dystrophy. J Pediatr 1990;117:1-15.
Gutmann DH, Fischbeck KH: Molecular biology of Duchenne and Becker’s muscular dystrophy: Clinical applications. Ann Neurol 1989;26:189-194.
Question 93:
A 32-year-old male presents with left leg pain and weakness. An axial image from his MRI is shown in Figure A. Which of the following physical exam findings would be most consistent with this MRI finding. Review Topic
Options:
- Numbness over dorsal aspect of the foot, weakness to gluteus medius
- Numbness over plantar foot, weakness to his gastrocsoleus complex
- Numbness over medial malleolus, and weakness to quadriceps
- Numbness over medial calf, weakness in his EHL
- Numbness over lateral malleolus, weakness to hip adduction
Correct Answer: Numbness over medial calf, weakness in his EHL
Explanation:
The MRI demonstrates a left paracentral L4/5 disc protrusion which leads to compression of the traversing (descending) left L5 nerve root. Numbness over the dorsal aspect of the foot and weakness to gluteus medius is consistent with a L5
radiculopathy.
While nerve root innervation shows some variability by patient, L5 is "characteristically" responsible for the sensation to the dorsal aspect of the foot, ankle dorsiflexion (tibialis anterior - along with L4), great toe extension (EHL), and hip abduction (gluteus medius).
Suri et al. reported on specific physical exam findings that significantly increased the likelihood of nerve root impingement at specific lumbar levels. They found: L2 was associated with decreased anterior thigh sensation. L3 was associated with a positive femoral stretch test. L4 was associated with a blunted patellar reflex, decreased medial ankle sensation or a positive crossed femoral stretch test. L5 was associated with was associated with decreased hip abductor strength.
Luri et al. reported 8-year follow up on the patients in the spine patient outcomes research trial who underwent surgical vs. conservative care for treatment of lumbar herniated disc. They found that patients who underwent surgical treatment had superior results that were maintained at 8 years compared to patients who underwent conservative management.
Figure A is an axial MRI at the L4/5 disc space that shows a left paracentral disc herniation compressing the descending L5 nerve root. Illustration A identifies the structures in the MRI image. Illustration B demonstrates the dermatome, reflex and motor function associated with the L4, L5 and S1 nerve root.
Incorrect Answers:
(SBQ13PE.102) An 26-year-old male presents to your office complaining of bilateral hip and low back pain. On physical examination, he has 10 degree bilateral hip flexion contractures. An AP pelvis radiograph is demonstrated in figure A. Which of the following findings is consistent with this patient's presentation?
Review Topic
A positive flexion, adduction, internal rotation (FADDIR) test
A history of untreated slipped capital femoral epiphysis (SCFE)
A thrombophilia
Normal serum ESR and CRP
Positive Human Leukocyte Antigen B27 (HLA-B27)
The patient has large joint arthralgia and sacroiliac joint sclerosis on AP pelvis radiograph, which is consistent with ankylosing spondylitis. Patients with ankylosing spondylitis have positive Human Leukocyte Antigen B27 (HLA-B27).
Ankylosing spondylitis (AS) is a seronegative spondyloarthropathy that affects the axial skeleton as well as large joints including the hips and knees. The most common initial site of pain is the sacroiliac (SI) joint, and is demonstrated as sacroiliitis on pelvic radiograph. Hip involvement is common, and typically manifests as hip pain and flexion contracture. Serologic studies will be typically be negative for rheumatoid factor, but positive for HLA-B27 in 90% of patients.
Kubiak et. al. review orthopaedic management of AS. Common orthopaedic manifestations include SI joint pain, hip flexion contractures, and stiffness of the cervical and lumbar spine. They report that laboratory analysis of patients with active disease will typically demonstrate mild elevation of ESR, CRP, and WBC. Patients with chronic AS may demonstrate a normocytic anemia. If HLA-B27 is negative, a high clinical suspicion should still be maintained.
Gensler et al. review the different clinical conditions that compose of juvenile-onset spondyloarthritis. They report on the different spondyloarthritides includes ankylosing spondylitis, reactive arthritis, arthropathy associated with inflammatory bowel disease, and that associated with psoriasis. They emphasize that the appearance of sacroiliac joint and spinal disease in the form of ankylosing spondylitis usually takes 5–10 years after initial symptom presentation, and therefore, a definite diagnosis can take several years leading to a delay in diagnosis.
Figure A is an AP pelvis radiograph of a skeletally mature individual demonstrating sclerosis of the SI joint indicative of sacroiliitis. Illustration A shows a axial CT image of the patient in the stem. Sclerosis and bone erosion can be seen in the sacroiliac joint.
Incorrect Answers:
osteonecrosis Answer 3: A infarctions,
of
the
femoral
epiphysis.
thrombophilia may have
osseous manifestations such as bone
which
are
not
evident
on
this
image.
Question 94:
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman with a soft endpoint, varus laxity at 30 degrees, and a positive dial test at 30 degrees that dissipates at 90 degrees of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome? Review Topic
Options:
- Hamstring autograft
- Revision ACL reconstruction and posterior cruciate ligament (PCL) reconstruction
- Revision ACL reconstruction and posteromedial corner reconstruction
- Revision ACL reconstruction and posterolateral corner reconstruction
Correct Answer: Hamstring autograft
Explanation:
This patient underwent an ACL reconstruction that has now failed. Based on his examination, he also has a posterolateral corner injury. Because this concomitant injury was not treated, the patient had undue strain on his graft, resulting in ultimate failure. Hamstring grafts are as effective as other graft types for ACL reconstruction. The medial meniscus provides secondary stabilization to the knee; however, this patient has a missed lateral ligamentous injury, and meniscus tears do not result in the development of a varus thrust. An unrecognized PCL tear likely results in mild-to-moderate medial and patellofemoral osteoarthritis without significant lateral laxity and thrust.
(SBQ12SP.35) A 16-year-old male football player is tackled into the ground during a game. He comes to the sideline with unilateral upper extremity pain, burning dysesthesias, and muscle weakness. Several minutes later, his symptoms resolve. In this scenario, what muscles are most likely to be affected?
Review Topic
Deltoid and biceps
Triceps
Wrist flexors
Finger flexors
Interossei
This patient presents with a 'burner' or 'stinger,' a transient unilateral neurapraxia that most commonly involves the biceps, deltoid and rotator cuff muscles.
Hypotheses for the mechanism of neurapraxia in stingers include nerve root compression in the neural foramen as a result of extension and compression, traction on the brachial plexus or a direct blow to the plexus. C5-C6 is the most commonly involved level, indicating root injury or upper trunk brachial plexus injury. Unilateral and transient symptoms are required for diagnosis. Bilateral 'stinger' symptoms of numbness, tingling, and weakness are consistent with cervical spinal cord neurapraxia. Return to play in contact sports is contraindicated with bilateral symptoms prior to MRI evaluation of the cervical spine.
Shannon et al. review burner syndrome in athletes. They emphasize that criteria for return to play are based on a complete and thorough neurologic and physical exam. Normal strength and sensation in both upper extremities as well as a normal cervical spine exam (including range of motion, compression, Spurling's, Adson's, and resistive head pressures) are required for return to play. Any positive findings mandate withdrawal of the player from competition.
Illustration A shows hypothesized areas of involvement by mechanism according to
Shannon et al. A, Extension-ipsilateral compression. B, Flexion-contralateral flexion (traction) or direct trauma.
Incorrect Answer Answer Answer
2:
3:
4:
Wrist Finger
Triceps
flexors flexors
C7 C7 C8
Question 95:
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include
Options:
- ultrasonic stimulation for 3 months.
- removal of the nail and plate fixation.
- continued observation.
- removal of the distal locking screws to dynamize the nail.
- exchange reamed nailing with bone graft.
Correct Answer: exchange reamed nailing with bone graft.
Explanation:
DISCUSSION: The patient has an oligotrophic nonunion of the distal femoral fracture. Although the proximal fracture appears incompletely united, it was stable at exchange nailing. The treatment of choice is exchange reamed nailing to at least 2 mm above the nail in place. Bone grafting is debatable. Recent studies have shown a 70% to 75% success rate with exchange nailing only, so in nonhypertrophic nonunions, bone grafting can be considered. Nonsurgical management consisting of observation or external stimulation runs the risk of implant failure. Plate fixation is acceptable but is considered a second choice because of the need to consider stabilization of the proximal fracture until union is achieved. Also, plate fixation definitely requires bone grafting.
REFERENCES: Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141.
Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Hak DG, Lee SS, Goulet JA: Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma 2000;14:178-182.
Question 96:
- Examination of a 32-year old woman who has pain in her shoulder as a result of a head-on motor vehicle accident reveals tenderness directly over the scapula and painful motion of the shoulder. Radiographs show a displaced extra-articular fracture of the scapula. Which of the following studies would best detect commonly associated injuries?
Options:
- Echocardiogram
- Electrocardiogram
- Radiograph of the chest
- CT scan of the shoulder
- Ultrasound of the shoulder
Correct Answer: Radiograph of the chest
Explanation:
Ninety-six percent of patients with scapular fractures has associated injuries, with rib fractures in the upper thorax being the most common. Pulmonary injuries were second in frequency (37%) with hemopneumothorax (29%) and pulmonary contusion (8%). Head injury was third (34%) and there were nine skull fractures. Clavicle fractures on the ipsilateral side occurred in 25%. The most frequent level of spinal cord injury was cervical (12%). Four patients suffered a permanent cord injury: two quadriplegics, one paraplegic, and one Brown-Sequard Syndrome. There were four brachial plexus injuries. Three recovered and the one with a persistent deficit also had a reflex sympathetic dystrophy. His injury was caused by a self-inflicted shotgun blast. Radiograph of the chest would provide the best overall survey for evaluation. The remaining studies would only evaluate isolated areas.
Question 97:
Figure 57 is the radiograph of a 58-year-old woman who is right-hand dominant and has fallen on her flexed right elbow and is seen in the emergency department reporting isolated episodes of right elbow pain. Examination reveals that the skin is contused but intact, and her distal neurovascular examination is normal. What is the most appropriate treatment? Review Topic
Options:
- Percutaneous pinning
- Closed reduction and extension casting
- Fragment excision and triceps advancement
- Open reduction and internal fixation with plate fixation
- Open reduction and internal fixation with tension band wire construct
Correct Answer: Open reduction and internal fixation with plate fixation
Explanation:
The patient has sustained an isolated, closed fracture of the olecranon without associated instability. The bone is radiographically osteopenic and the fracture is displaced, comminuted, and includes articular marginal impaction. Plate fixation is preferred in the presence of comminution or associated transolecranon or radiocapitellar instability. Displaced fractures are generally treated surgically in an effort to restore articular congruity, restore extensor function, and to allow for early mobilization in an effort to maximize functional outcomes. A tension band wire
construct is a commonly used technique but is reserved for simple fracture patterns without comminution. Excision and triceps advancement can be considered in elderly, low-demand patients that have small unreconstructable fracture patterns without associated elbow instability.
Question 98:
During excision of a Baker cyst, the base or stalk is usually found between the
Options:
- popliteus muscle and posterior cruciate ligament.
- posterior cruciate ligament and lateral gastrocnemius muscle.
- medial gastrocnemius muscle and posterior cruciate ligament.
- semimembranosus and medial head of the gastrocnemius muscles.
- semitendinosus and medial head of the gastrocnemius muscles.
Correct Answer: semimembranosus and medial head of the gastrocnemius muscles.
Explanation:
DISCUSSION: Although there are several bursae in the posterior portion of the knee, the most prevalent one with a connection to the knee joint is the one in the interval between the semimembranosus and the medial head of the gastrocnemius muscle. The popliteus muscle and posterior cruciate ligament, the posterior cruciate ligament and lateral gastrocnemius muscle, and the medial gastrocnemius muscle and posterior cruciate ligament are all too lateral and uncommon. The semitendinosus and medial head of the gastrocnemius muscles do not come in contact in the posterior aspect of the knee.
REFERENCES: Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA,
WB Saunders, 1995, p 379.
Justis EJ Jr: Nontraumatic disorders, in Crenshaw AH (ed): Campbell’s Operative Orthopaedics, ed 7. Philadelphia, PA, Lippincott, 1987, vol 3, p 2257.
Question 99:
Wear particles of ultra-high molecular weight polyethylene that are generated by total hip implants are predominantly of what diameter?
Options:
- Less than 1 micron
- 10 to 50 microns
- 100 to 200 microns
- 500 to 750 microns
- Greater than 1,000 microns
Correct Answer: Less than 1 micron
Explanation:
DISCUSSION: Multiple studies have shown that the size of an ultra-high molecular weight polyethylene particle generated by total hip implants is typically less than 1 micron. This finding is significant in that particles of that size are readily phagocytized by macrophages.
REFERENCES: Campbell P, Ma S, Yeom B, McKellop H, Schmalzried TP, Amstutz HC: Isolation of predominantly submicron-sized UHMWPE wear particles from periprosthetic tissues. J Biomed Mater Res 1995;29:127-131.
Shanbhag AS, Jacobs JJ, Glant TT, Gilbert JL, Black J, Galante JO: Composition and morphology of wear debris in failed uncemented total hip replacement. J Bone Joint Surg Br 1994;76:60-67.
Maloney WJ, Smith RL, Schmalzried TP, Chiba J, Huene D, Rubash H: Isolation and characterization of wear particles generated in patients who have had failure of a hip arthroplasty without cement. J Bone Joint Surg Am 1995;77:1301-1310.
Question 100:
During a revision total knee arthroplasty (TKA), there is difficulty gaining exposure and a tibial tubercle osteotomy (TTO) is performed. The final components are stable and include a stemmed tibial component that bypasses the osteotomy site. The tibial tubercle is reattached to the osteotomy site with multiple cerclage wires. Following closure of the arthrotomy, the knee is flexed to 90 degrees, and there is no observed displacement of the TTO. What is the best next step in postsurgical rehabilitation?
Options:
- Limit flexion to 90 degrees with nonweight-bearing activity with crutches for the first 6 weeks
- Limit flexion to 30 degrees for the first week, progress 10 degrees per week, and allow partial weight-bearing activity with crutches
- The knee should be immobilized in extension; partial weight-bearing activity with crutches may be allowed for the first 6 weeks
- An initial range-of-motion restriction to 90 degrees or weight-bearing restriction is not needed
Correct Answer: An initial range-of-motion restriction to 90 degrees or weight-bearing restriction is not needed
Explanation:
DISCUSSION
TTO is a recognized technique for improving exposure when performing TKA in a stiff knee. TTO has been reported to enhance surgical exposure and not adversely affect outcomes after TKA, but there is a 5% complication rate. The postsurgical routine following TTO
includes full weight-bearing activity and range of motion as tolerated. Caution should be exercised when manipulation is performed to improve knee flexion following a TTO.