OITE & ABOS Orthopedic Board Prep MCQs: Arthroscopy, Trauma, Hip | Part 50

Key Takeaway
This interactive quiz, Part 50 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review, offers 100 high-yield, verified MCQs. It's designed for orthopedic surgeons and residents preparing for ABOS board certification and OITE exams, offering crucial interactive study and exam modes.
About This Board Review Set
This is Part 50 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 50
This module focuses heavily on: Arthroscopy, Fracture, Hip.
Sample Questions from This Set
Sample Question 1: The load versus deformation curve of the functional spinal unit (FSU) is made up of the neutral zone, the elastic zone, and the plastic zone. What is the plastic zone of the curve believed to represent?...
Sample Question 2: A 21-year-old female college athlete sustained a stress fracture of the fifth metatarsal 1 year ago which was treated successfully with surgical stabilization and she returned to normal activities. She now has a tension-sided femoral neck f...
Sample Question 3: Which of the following injuries is most likely associated with the fracture seen in Figure A?...
Sample Question 4: A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The artic...
Sample Question 5: The anterior portal of a hip arthroscopy places what structure at greatest risk for injury?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The load versus deformation curve of the functional spinal unit (FSU) is made up of the neutral zone, the elastic zone, and the plastic zone. What is the plastic zone of the curve believed to represent?
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 15-23.
Panjabi MM, White AA: Physical properties and functional biomechanics of the spine, in White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 1-83.
Question 2
A 21-year-old female college athlete sustained a stress fracture of the fifth metatarsal 1 year ago which was treated successfully with surgical stabilization and she returned to normal activities. She now has a tension-sided femoral neck fracture. Along with surgical fixation of the fracture, what is the next step in management? Review Topic
Explanation
Question 3
Which of the following injuries is most likely associated with the fracture seen in Figure A?

Explanation
Soft tissue pathology is common in tibial plateau fractures. In general, fractures that are largely displaced and/or a result of high energy trauma are more likely to have associated soft tissue pathology. A majority of meniscal injuries that occur in the setting of tibial plateau fractures are meniscocapsular detachments. This has important implications for healing (more reliable healing in the vascular zone). Additionally, the meniscus usually remains in close contact with the femoral condyle, while the tibial plateau widens around it. It is generally agreed upon that meniscal tears should be repaired, if possible, at the time of internal fixation to decrease the likelihood of
postraumatic arthritis.
Gardner et al. review 62 patients with Schatzker II tibial plateau fractures that had an MRI preoperatively. For displaced fractures, the incidence of lateral meniscal tears was 83%, while the incidence of lateral collateral and posterior cruciate ligament injuries was 30%.
Ringus et al. attempted to determine if the degree of lateral tibial plateau fracture depression on computed tomography (CT) images predicted the presence of lateral meniscus tears. Fractures with > 9mm depression had an eight-fold increase in lateral meniscal tears, and those younger than 48 years-old had a four-fold increase in lateral meniscal tears.
Illustration A shows an MRI of a Schatzker II tibial plateau fracture with a lateral meniscal detachment and a medial meniscal tear. Illustration B shows the Schatzker Classification, I-VI.
Incorrect Answers:
Question 4
A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of
Explanation
REFERENCES: Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Krakauer JD, Stern PJ: Hinged device for fractures involving the proximal interphalangeal joint. Clin Orthop 1996;327:29-37.
Question 5
The anterior portal of a hip arthroscopy places what structure at greatest risk for injury?
Explanation
at risk.
REFERENCES: Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 83-91.
Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 281-289.
Question 6
A 60-year-old man is evaluated in the ICU after a rollover motor vehicle accident 3 days ago. He has multiple upper and lower extremity trauma and was found unresponsive at the accident scene. Surgery is planned for the extremity trauma once the patient is medically stable. He remains intubated and the cervical spine is immobilized in a semi-rigid collar. Examination reveals mild erythema in the posterior occipital cervical region. Initial AP and lateral radiographs of the cervical spine have not revealed any obvious fracture. What is the most appropriate treatment option at this time? Review Topic
Explanation
Question 7
03 advancement at age 6 years. What is the most likely diagnosis?
Explanation
back to this question next question
Question 8
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate Review Topic

Explanation
Question 9
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
Explanation
REFERENCES: Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.
Question 10
Sclerostin and dickkopf-1 (Dkk-1) are direct inhibitors of what pathway related to bone and/or cartilage regulation?
Explanation
Adhesive wear
Abrasive wear
Fatigue wear
Delamination
For each scenario below, please choose the most likely dominant mechanism of wear from the list
above.
Question 11
During placement of an external fixator for a distal radius fracture, the most commonly injured nerve is a branch of which of the following nerves? Review Topic
Explanation
(SBQ12TR.106) A 67-year-old female sustains the injury shown in Figure A after a trip and fall. When discussing the outcomes of surgery with the patient, which of the following statements is true?

Post-surgical mortality rates are significantly lower after total hip arthroplasty compared to hemiarthroplasty
Internal fixation shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to arthroplasty
Bipolar hemiarthroplasty shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to unipolar hemiarthroplasty
A delay in surgery greater than 48 hours is recommended if the patient has multiple medical comorbiditiesm which are not fully optimized
Dislocation rates are equivalent between total hip arthroplasty and hemiarthroplasty
Moderate evidence supports that hip fracture surgery within 48 hours of admission is associated with better outcomes. However, patients with significant medical comorbidity should be fully optimized before surgery.
Although several studies have shown a benefit to surgery within 48 hours, no definitive time frame has been elucidated. The majority of literature has shown improved outcomes in regards to pain, complications, and length of stay with early surgery. Patients with significant medical comorbidities have been shown to have the highest mortality rates.
Moran et al. aimed to determine whether a delay in surgery for hip fractures had an affect on postoperative mortality among elderly patients. In an observational study of 2660 patients, they showed that mortality following hip fracture surgery was 9% at 30-days, 19% at 90-days, and 30% at 12-months. Patients with medical comorbidities had 2.5 times the risk of death within 30-days of surgery. In addition, individuals who had surgery delayed beyond 4 days had increased mortality at 90-days and 12-months.
Papakostidis et al. examined the timing of internal fixation of intracapsular fractures of the neck of femur on the development of late complications, particularly osteonecrosis of femoral head (ONFH) and non-union. They showed no benefit of
early surgery on incidence of AVN. However, delay of internal fixation of more than
24 hours showed increased rates of non-union.
Figure A shows a displaced right femoral neck fracture. Incorrect Answers:
Question 12
A normal functioning posterior tibialis tendon is best confirmed by which of the following physical findings?
Explanation
Question 13
A 65-year-old woman has significant neck pain after falling and striking her head. A radiograph and sagittal CT scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, pp 927-937.
Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2003, pp 455-458.
Question 14
Which modality has the broadest application for the reduction of postsurgical transfusion?
Explanation
TXA is easy to administer, inexpensive, and safe for virtually all patients. Multiple studies have demonstrated transfusion rates lower than 3% for total knee arthroplasty and lower than 10% for total hip arthroplasty. Regional and hypotensive anesthesia effectively reduce transfusion; however, they cannot be used in as wide a range of patients as can TXA. A reduced transfusion trigger must be considered along with patient symptoms when determining the need for transfusion.
Question 15
Reverse total shoulder arthroplasty with a latissimus dorsi transfer would be the most appropriate treatment for which of the following patients? Review Topic
Explanation
R-TSA has become the mainstay treatment for rotator cuff arthropathy. In the presence of severe loss of active elevation and external rotation, combined latisimus dorsi transfer and reverse total shoulder arthroplasty can restore elevation and external rotation, respectively. This may be used in the primary or revision setting.
Frankle et al. report the results of sixty patients with rotator cuff deficiency and glenohumeral arthritis who were followed for a minimum of two years. All were
treated with R-TSA. Their study showed that forward flexion increased from 55 to
105 degrees, and abduction increased from 41 to 102 degrees.
Boileau et al. followed 45 patients with severe cuff tear arthropathy and advanced atrophy/fatty infiltration of the infraspinatus or teres minor muscles. All patients were treated with R-TSA and a modified L'Episcopo procedure (latissimus dorsi and teres major transfer). Mean active elevation increased from 74 degrees preoperatively to
149 postoperatively, and external rotation increased from -21 to 13 degrees.
Illustrations A and B show the classic findings of rotator cuff arthropathy. There is significant acromial acetabularization and femoralization of humeral head. Other features include: asymmetric superior glenoid wear, osteopenia, "snowcap sign" due to subchondral sclerosis and anterosuperior escape. Illustration C shows a left shoulder after conversion from hemiarthroplasty to reverse total shoulder arthropathy.
Incorrect Answers:
Question 16
Figure 12 shows a lateral radiograph of the elbow. What is the most likely diagnosis?
Explanation
REFERENCE: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 132-133.
Keats TE, Anderson MW: Atlas of Normal Roentgen Variants That May Simulate Disease, ed 7. St Louis, MO, Mosby Inc, 2001, p 497.
Question 17
Figures 27a and 27b show the radiographs of a 32-year-old woman who was involved in a high-speed motor vehicle accident. She is neurologically intact. After stabilization and assessment, treatment should consist of
Explanation
REFERENCES: Lewandrowski KU, McLain RF: Thoracolumbar fractures: Evaluation, classification, and treatment, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 817-843.
Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Question 18
A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in
Explanation
REFERENCES: Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Farsetti P, Potenza V, Caterini R, Ippolito E: Long-term results of treatment of fractures of the medial humeral epicondyle in children. J Bone Joint Surg Am 2001;83:1299-1305.
Question 19
A 46-year-old patient with cervical myelopathy undergoes a multilevel posterior cervical laminectomy from C3 to C7. The risk of postlaminectomy kyphosis is greatest with removal of which of the following structures?
Explanation
REFERENCE: Zdeblick TA, Abitol JJ, Kunz DN, et al: Cervical stabilization after sequential capsule resection. Spine 1993;18:2005-2008.
Question 20
What is the most common organism found following a nail puncture wound through tennis shoes in a host without immunocompromise?
Explanation
REFERENCES: Green NE, Bruno J III: Pseudomonas infections of the foot after puncture wounds. South Med J 1980;73:146-149.
Riegler HF, Routson GW: Complications of deep puncture wounds of the foot. J Trauma 1979;19:18-22.
Question 21
- A 16-year-old girl who swims on her high school team reports pain in the shoulder after swimming. History reveals a glenohumeral dislocation at age 14 years while doing the backstroke. Examination shows a positive anterior apprehension sign. Treatment at this time should consist of
Explanation
p. 577: “A vigorous effort to stabilize the shoulder with exercises is particularly indicated in patients with multidirectional or posterior instability and in athletes requiring a completely normal or supranormal range of motion.”
p. 989: “If the [swimmer] has symptoms of subluxation, a conservative program that strengthens the external rotators is warranted. Surgery is seldom indicated.”
Question 22
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?
Explanation
REFERENCES: Albert MJ, Drvaric DM: Little League shoulder: Case report. Orthopedics 1990;13:779-781.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 23
A 24-year-old man is involved in a motor vehicle accident at 60 mph. He sustains multiple injuries including an intra-abdominal injury requiring a splenectomy and a closed right femoral shaft fracture. Which variable will best indicate the patient's resuscitation status when deciding whether to proceed with definitive care of the fracture at the conclusion of the laparotomy? Review Topic
Explanation
Question 24
What property of titanium alloys accounts for their high corrosion resistance in vivo?
Explanation
REFERENCES: Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott, 2003, vol 1, pp 269-278.
Lemons JE: Metallic alloys, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 19-27.
Question 25
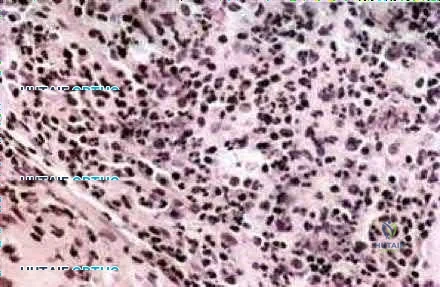
What is the most common location of osteosarcoma?
Explanation
REFERENCES: Malawer MM, Sugarbaker PH, Malawer M: Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Kluwer Academic Publishers, 2001.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 26
A 25-year-old man reports wrist pain following a motorcycle accident. Examination reveals minimal swelling, slightly limited active range of motion, and point tenderness in the snuff box region. AP and oblique radiographs are shown in Figures 40a and 40b. Management should consist of
Explanation
REFERENCES: Amadio PC, Taleisnik J: Fractures of the carpal bone, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 809-823.
Rettig ME, Kozin SH, Cooney WP: Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am 2001;26:271-276.
Cooney WP, Dobyns JH, Linscheid RL: Fractures of the scaphoid: A rational approach to management. Clin Orthop 1980;149:90-97.
Szabo RM, Manske D: Displaced fractures of the scaphoid. Clin Orthop 1988;230:30-38.
Question 27
A patient with rheumatoid arthritis with both ankle and subtalar involvement was treated as shown in Figures 11a and 11b. What complication is unique to this type of fixation?
Explanation
REFERENCES: Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 236-237.
Thordarson DB, Chang D: Stress fractures and tibial cortical hypertrophy after tibiotalocalcaneal arthrodesis with an intramedullary nail. Foot Ankle Int 1999;20:497-500.
Hammett R, Hepple S, Forster B, et al: Tibiotalocalcaneal (hindfoot) arthrodesis by retrograde intramedullary nailing using a curved locking nail: The results of 52 procedures. Foot Ankle Int 2005;26:810-815.
Question 28
Second impact syndrome (SIS) after head injury is characterized by which of the following? Review Topic
Explanation
Question 29
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management? Review Topic
Explanation
Question 30
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.
Question 31
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
Explanation
REFERENCES: Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337.
Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271.
Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Sneppen O, Fruensgaard S, Johannsen HV, Olsen BS, Sojbjerg JO, Anderson NH: Total shoulder replacement in rheumatoid arthritis: Proximal migration and loosening. J Shoulder Elbow Surg 1996;5:47-52.
Question 32
The Musculoskeletal Infection Society (MSIS) has adopted a definition of periprosthetic joint infection (PJI). This definition includes 2 major criteria and 5 minor criteria. Infection is present if 1 of 2 major criterions or 3 of 5 minor criterions are met. These criterions are
Explanation
In 2014, the MSIS published its revised PJI definition for clinical and research use. If 1 of 2 major criterions is met (phenotypically identical organisms obtained from 2 separate cultures or a draining sinus tract), then PJI is diagnosed. Alternatively, if 3 of 5 minor criterions are met, PJI is diagnosed.

Question 33
Figure 12 shows the radiograph of a patient who has anterior knee pain. History reveals a femoral fracture at age 5 years. What is the most likely cause of the deformity?
Explanation
REFERENCES: Hresko MT, Kasser JR: Physeal arrest about the knee associated with non-physeal injuries of the lower extremity. J Bone Joint Surg Am 1989;71:698-703.
Bowler JR, Mubarak SJ, Wenger DR: Tibial physeal closure and genu recurvatum after femoral fracture: Occurrence without a tibial traction pin. J Pediatric Orthop 1990;10:653-657.
Question 34
Which complication is most common after syndesmotic fixation?
Explanation
The injury radiographs reveal a supination external rotation IV ankle fracture with evidence of medial clear space widening exceeding 4 mm and an increase relative to the superior tibiotalar clear space. This indicates injury to the deltoid ligament and necessitates surgical reduction and fixation to restore and maintain ankle stability. Following stabilization of the fibula, an intraoperative stress examination of the syndesmosis such as an external rotation stress test under fluoroscopy or lateral pull on the fibula (the Cotton test) should be performed to determine the integrity of the syndesmosis. Radiographic evidence of tibiofibular clear space widening, medial clear space widening with external rotation, and lateral displacement of the distal fibula when pulled is consistent with syndesmotic injury. In contrast to the presurgical stress test, once the fibula has been reduced and stabilized lateral talar translation can occur only if the syndesmosis is injured in addition to the deltoid ligament. Failure of the syndesmotic screw without evidence of malalignment of the mortise and a pain-free ankle are not indications for further surgery because these patients have satisfactory outcomes when compared to those who have intact or removed screws. Hardware removal following fibula ORIF is indicated when patients have pain directly related to hardware prominence. Resolution of joint pain or stiffness is not a reliable outcome following hardware removal. Although fibular fracture can occur, this is a rare complication. Malreduction of the syndesmosis is the most common complication following ORIF of the syndesmosis and is improved with direct visualization; however, malreduction still may occur with direct visualization.
RECOMMENDED READINGS
Manjoo A, Sanders DW, Tieszer C, MacLeod MD. Functional and radiographic results of patients with syndesmotic screw fixation: implications for screw removal. J Orthop Trauma. 2010 Jan;24(1):2-6. doi: 10.1097/BOT.0b013e3181a9f7a5. PubMed PMID: 20035170. View
Abstract at PubMed
Jenkinson RJ, Sanders DW, Macleod MD, Domonkos A, Lydestadt J. Intraoperative diagnosis of syndesmosis injuries in external rotation ankle fractures. J Orthop Trauma. 2005 Oct;19(9):604-9. PubMed PMID: 16247304. View Abstract at PubMed
Stark E, Tornetta P 3rd, Creevy WR. Syndesmotic instability in Weber B ankle fractures: a clinical evaluation. J Orthop Trauma. 2007 Oct;21(9):643-6. PubMed PMID: 17921840. View Abstract at PubMed
Brown OL, Dirschl DR, Obremskey WT. Incidence of hardware-related pain and its effect on functional outcomes after open reduction and internal fixation of ankle fractures. J Orthop Trauma. 2001 May;15(4):271-4. PubMed PMID: 11371792. View Abstract at PubMed
Question 35
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of
Explanation
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Kelly IG, Foster RS, Fisher WD: Neer total shoulder replacement in rheumatoid arthritis. J Bone Joint Surg Br 1987;69:723-726.
Question 36
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. What is the next diagnostic step?
Explanation
Question 37
A mother brings in her 6-month-old infant with a knee deformity. The child had previously been treated with serial casting in flexion for 3 month at an outside facility. Examination reveals passive hyperextension to 25° and passive flexion to 15° as shown in Figures A and B respectively. A lateral radiograph of the knee is shown in Figure C. What is the most appropriate next step in treatment? Review Topic

Explanation
Congenital knee dislocation is rare. The etiology is thought to be quadriceps contracture. It is associated with developmental dysplasia of the hip (DDH) and clubfoot (CTEV). In newborn infant, casting or bracing with the knee in flexion
should be performed. If this fails, percutaneous or open VY quadricepsplasty, followed by above-knee casting, is indicated.
Abdelaziz et al. proposed a new grading system (Tarek CDK grading system-see Illustrations A and B) and treatment protocol as follows: (1) Serial casting for Grade 1 regardless of age and in neonates with grade 2 <1mth. If flexion to >90° is achieved within 4 weeks, then serial casting is continued; if range remains <90°, percutaneous quadriceps recession (PQR) is performed. (2) PQR is performed in Grade 2 CDK in infants >1 month of age upon presentation. (3) VY quadricepsplasty is indicated in patients with Grade 3 CDK or in recurrent cases.
Klingele et al. describe ACL shortening and reinforcement in 2 patients with congenital knee dislocation who developed ACL incompetence due to elongation. They conclude that stabilizing and reinforcing the ACL may prevent long-term anterior instability, hyperextension and recurrent deformity.
Figures A and B show the range of motion of the knee (25deg hyperextension to 15deg flexion). Figure C is a lateral radiograph showing congenital dislocation of the knee. Illustrations A and B show the Tarek grading system. Illustration C shows the different techniques of quadricepsplasty (upper row, structures divided and skin incisions used; lower row, how lengthening of the quadriceps mechanism is achieved). The most common PQR is the Roy-Crawford technique. The most common VYQ is the Curtis-Fisher technique.
Incorrect Answers:
Question 38
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
Explanation
REFERENCES: Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.
Question 39
A 4-year-old boy with arthrogryposis has little active motion of his knees or elbows. Both elbows are in full extension with good triceps strength, but he is unable to bring his hand to his face or feed himself. Management should consist of
Explanation
REFERENCES: Van Heest A, Waters PM, Simmons BP: Surgical treatment of arthrogrypsosis of the elbow. J Hand Surg Am 1998;23:1063-1070.
Caroll RE, Hill NA: Triceps transfer to restore elbow flexion: A study of fifteen patients with paralytic lesions and arthrogryposis. J Bone Joint Surg Am 1970;52:239-244.
Question 40
What tendon has an intra-articular (instrasynovial) location in the knee joint?
Explanation
REFERENCES: Kimura M, Shirakura K, Hasegawa A, Kobayashi Y, Udagawa E: Anatomy and pathophysiology of the popliteal tendon area in the lateral meniscus: 1. Arthroscopic and anatomical investigation. Arthroscopy 1992;8:419-423.
Arnoczky SP, Skyhar MJ, Wickiewicz TL: Basic science of the knee, in McGinty JB (ed): Operative Arthroscopy. New York, NY, Raven Press, 1991, pp 155-182.
Question 41
A 25-year-old lineman is referred to your office for a second opinion. 1 year ago, he underwent an arthroscopic procedure for shoulder instability. He complains of persistent sense of instability despite the surgery. Which of the following is a contraindication to revision arthroscopic labral repair for recurrent anterior glenohumeral instability? Review Topic
Explanation
Thermal capsulorrhaphy utilizes heat generated by radiofrequency or laser ablation to cause capsular shrinkage in an effort to treat shoulder instability. However, high recurrence rates have been found, especially around two to three weeks after the index procedure, when the capsular tissue is the weakest. In the setting of recurrence following thermal capsulorrhaphy, open revision is recommended.
Creighton et al. reported on a series of 18 patients undergoing revision arthroscopic stabilization. Of the 18, 3 failed with recurrent instability, all with previous thermal capsulorrhaphy.
Miniaci et al. reviewed the outcomes following thermal capsulorrhaphy noting high rates of recurrent instability, especially in the setting of initial treatment for multidirectional instability.
Park et al. reported on a series of 14 patients undergoing revision following thermal capsulorrhaphy. Ten out of 14 patients had signs of capsular thinning, insufficiency and attenuation.
Wong et al. surveyed 379 shoulder surgeons on the complications following thermal capsulorrhaphy. Capsular insufficiency and thinning were commonly associated with recurrent instability.
Hecht et al. performed thermal capsulorrhaphy and biomechanical analysis of the capsule in a sheep model. The authors found that the capsule was weakest at the 2-3 week post-operative timepoint, leading to the highest rate insufficiency, attenuation and mechanical failure at this time.
Incorrect answers:
Question 42
Figure 6a shows the radiograph of a 50-year-old man who sustained an anterior dislocation of the shoulder. He undergoes closed reduction, and the postreduction radiograph is shown in Figure 6b. Management should now consist of
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Flatow EL, Cuomo F, Maday MG, et al: Open reduction and internal fixation of two-part displaced fractures of the greater tuberosity of the proximal part of the humerus. J Bone Joint Surg Am 1991;73:1213-1218.
Question 43
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 19-year-old man with a closed right humeral shaft fracture as well as a right femoral shaft fracture and a left ankle fracture-dislocation after a motor vehicle collision. On initial examination, he is noted to have a complete radial nerve palsy of his right upper extremity. Postoperative radiographs are shown in Figures 3 and 4. How does the plate function?

Explanation
The posterior triceps-reflecting approach described can be extended proximally to the level of the axillary nerve. The radial nerve must be found and protected, but the dissection can be carried well proximal to it and the medial triceps origin. The anatomic neck of the humerus cannot be visualized through this approach.
The plate functions as a neutralization plate, as multiple lag screws are seen placed outside of the plate, suggesting anatomic reduction and fixation of the fracture prior to applying the plate.
The working length of the plate is the distance between the proximal and distal screws closest to the fracture. The length of screw purchase in bone represents the working length of the screw, not the plate. The other answer choices describe dimensions of the plate and the fixation construct, not its working length.
Question 44
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
REFERENCES: Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 161-167.
Question 45
Figures 26a and 26b show the radiograph and MRI scan of an 18-year-old man who fell from a trampoline. Examination reveals exquisite local tenderness at the thoracolumbar junction, but he is neurologically intact. Management should consist of
Explanation
REFERENCES: Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Lewandrowski KU, McLain RF: Thoracolumbar fractures: Evaluation, classification, and treatment, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 817-843.
Question 46
A number of potential complications are associated with the direct lateral approach to the lumbar spine; which complication is most common?
Explanation
Sofianos and associates examined the cases of 45 patients who underwent the lateral transpsoas approach and found that 18 of 45 patients (40%) experienced at least 1 complication. The most common complication was postsurgical weakness of the iliopsoas, which was an issue for 10 of 45 patients (22.2%). The second-most-common complication in this series was anterior thigh hypoesthesia. This occurred in 8 of 45 patients (17.8%). A series of 600 patients by Rodgers and associates noted that thigh pain and psoas weakness following a direct lateral approach to the lumbar spine were both "nearly universal" but almost "always transient."
RECOMMENDED READINGS
Sofianos DA, Briseño MR, Abrams J, Patel AA. Complications of the lateral transpsoas approach for lumbar interbody arthrodesis: a case series and literature review. Clin Orthop Relat Res. 2012 Jun;470(6):1621-32. doi: 10.1007/s11999-011-2088-3. Review. PubMed
PMID: 21948287.View Abstract at PubMed
Lee YP, Regev GJ, Chan J, Zhang B, Taylor W, Kim CW, Garfin SR. Evaluation of hip flexion strength following lateral lumbar interbody fusion. Spine J. 2013 Oct;13(10):1259-62. doi: 10.1016/j.spinee.2013.05.031. Epub 2013 Jul 12. PubMed PMID: 23856656. View Abstract at PubMed
Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011 Jan 1;36(1):26-32. doi: 10.1097/BRS.0b013e3181e1040a. PubMed PMID: 21192221. View
Abstract at PubMed
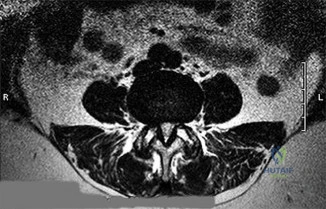
CLINICAL SITUATION FOR QUESTIONS 21 AND 22
Figures 21a through 21c are the preoperative lateral standing radiograph, axial T2-weighted MR image at L4-5, and supine sagittal MR image of a 45-year-old woman who has had back and leg pain for 2 years. Treatment had included nonsteroidal anti-inflammatory drugs, physical therapy, and epidural corticosteroid injections. Her pain limited her activities of daily living; she could walk only 1 to 2 blocks before her pain became intolerable.
21A

B

C
Question 47
During a posterior cruciate ligament (PCL)-retaining total knee arthroplasty, a critical principle to remember is to
Explanation
Maintenance of the joint line and accurately tensioning the PCL are critical in the proper execution of a PCL-retaining total knee arthroplasty. Appropriate tension helps ensure femoral rollback and avoid stiffness or instability. Raising the joint line to help ensure full extension should be avoided in cruciate- retaining knees, because doing so creates an unfavorable kinematic environment. The three important principles of surgical technique needed to maintain appropriate tensioning of the PCL include 1) choosing the proper femur size to reproduce the native femoral anterior/posterior dimension, 2) reproducing the joint line by resecting as much tibia from the healthy side as will be replaced by the smallest thickness of the tibial component and, 3) ensuring that full extension is achieved by soft-tissue releases and not by taking additional distal femur, as may be done in a posterior stabilized approach. Another important principle is to re-create the natural degree of the patient’s posterior tibial slope to avoid tightness in
flexion.
Question 48
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of
Explanation
REFERENCES: Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Burkhead WZ, Arcand MA, Zeman C, et al: The biceps tendon, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1996.
Question 49
A patient with an acromioclavicular dislocation has a very prominent distal clavicle. Examination reveals that the deformity increases rather than reduces with an isometric shoulder shrug. Which of the following structures is most likely intact?
Explanation
REFERENCE: Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 1995;23:324-331.
Question 50
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management? Review Topic
Explanation
Question 51
A 42-year-old man has increasing pain and, to a lesser extent, some occasional left knee instability. Several years earlier he sustained a noncontact twisting injury to his knee. He had some initial soreness and pain but was able to resume his normal activities while avoiding sports. On examination, the patient has medial joint line pain, a grade 2+ Lachman, and a slight varus thrust. His radiographs reveal mild-to-moderate medial compartment osteoarthritis with varus alignment. What surgical treatment strategy likely will alleviate his pain? Review Topic
Explanation
Question 52
A 30-year-old accountant and recreational softball player, who is seen at the end of his baseball season, reports a several month history of pain along the medial side of his dominant elbow. He cannot identify a specific injury and notes it only hurts when he throws the ball in from the outfield. Besides the pain, he remarks that his speed and distance while throwing have diminished considerably. Examination reveals tenderness along the medial elbow but no weakness or gross instability is found. Radiographs are normal. Based on the history, what is the most likely diagnosis? Review Topic
Explanation
the forearm during resisted forearm pronation and is not associated with the throwing motion in particular. Valgus extension overload may mimic medial collateral ligament injury, not varus extension injuries. Medial epicondylitis may be confused with ligament insufficiency but the examination and a history of pain only while throwing make this an unlikely diagnosis.
Question 53
An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis? Review Topic
Explanation
(SBQ07SM.48) Carbohydrate loading is a common practice among endurance athletes that works by what mechanism? Review Topic
Increasing serum fructose levels
Maximizing stored muscle glycogen for endurance after 90 minutes of exercise
Diuresis
Decreasing serum glucose levels
Maximizing stored liver glycogen for endurance after 60 minutes of exercise
Carbohydrate loading is a strategy that involves changes to training and nutrition which can maximize muscle glycogen stores prior to endurance exercise lasting longer than 90 minutes.
There continues to be varying scientific opinions as to whether athletes should eat low vs. high glycemic index foods, and how this will affect the amount that the serum glucose levels rise. Fructose is able to be converted to glycogen in the liver but not muscle, therefore high-fructose containing foods are suboptimal. This practice is recommended for athletes participating in events that are longer than 90 minutes (after the bodies normal supply of glycogen is depleted).
Coyle et al. analyzed 10 trained cyclists who performed two bicycle ergometer exercise tests 1 wk apart. They found that blood glucose concentration was 20-40% higher during the exercise after carbohydrate ingestion than during the exercise without carbohydrate feeding. The exercise-induced decrease in plasma insulin was prevented by carbohydrate feeding. Ultimately, fatigue was postponed by carbohydrate feeding during exercise in seven out of the ten subjects.
Costill et al. examined the effect of carbohydrates on muscle glycogen resynthesis in trained runners and found that muscle glycogen levels could be normalized with the proper use of carbohydrates after strenuous activity.
Sherman et al. used muscle biopsies to determine the effects of moderate- or high-carbohydrate diets on muscle glycogen and performance in runners and cyclists over 7 consecutive days of training. They found that a high carbohydrate diet restored muscle glycogen to more normal levels than a moderate carbohydrate diet but did not find any difference in the effect on performance.
Illustration A is a graph depicting the typical carbohydrate depletion/loading regimen that endurance athletes utilize to maximize muscle glycogen stores prior to endurance exercise. This typically involves a hard workout followed by three days of a low-carb diet, another hard workout, and another three days of a high-carb diet.
Incorrect
Question 54
Why is tendon considered an anisotropic material?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O’Keefe RJ,
Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 55
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45° lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
REFERENCES: Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629.
Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Edwards CC II, Bridwell KH, Patel A, et al: Long adult deformity fusions to L5 and the sacrum: A matched cohort analysis. Spine 2004;29:1996-2005.
Question 56
Following total elbow arthroplasty, patients should be instructed to Review Topic
Explanation
Question 57
What is the most common presenting sign or symptom in an adult with lumbar pyogenic infection?
Explanation
REFERENCES: Carragee EJ: Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am 1997;79:874-880.
Frazier DD, Campbell DR, Garvey TA, et al: Fungal infections of the spine: Report of eleven patients with long-term follow-up. J Bone Joint Surg Am 2001;83:560-565.
Hadjipavlou AG, Mader JT, Necessary JT, et al: Hematogenous pyogenic spinal infections and their surgical management. Spine 2000;25:1668-1679.
Question 58
Sterilization of ultra-high molecular weight polyethylene by gamma irradiation in air will degrade its wear performance because of
Explanation
REFERENCES: Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86.
McKellop H, Shen FW, Lu B, et al: Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene: A hip-simulator study. J Bone Joint Surg Am 2000;82:1708-1725.
Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 59
A 17-year-old male soccer player sustains repeated lateral patellar dislocations refractory to physical therapy, bracing, and taping. After a workup including radiographs and MRI, the orthopaedic surgeon considers an isolated tibial tubercle osteotomy (TTO). He plans a 60-degree anteromedialization to address instability and to unload the patellofemoral joint. What is a relative contraindication to this procedure?
Explanation
TTO is a common treatment for patellofemoral instability. The angle of correction must be customized to each patient’s anatomy. For this patient, the orthopaedic surgeon plans an osteotomy that will both anteriorize and medialize the tubercle. This will consistently result in
a change of patellofemoral kinematics and contact pressures. Medialization decreases lateral and increases medial patellofemoral contact pressures, and anteriorization shifts contact pressures from distal to proximal. Significant anteriorization may not be desired in a patient with proximal patellar chondrosis unless a concomitant chondral procedure is performed as well. The patellar height (Caton-Deschamps ratio) is normal, precluding the need for distalization but not medialization. The TT-TG distance, at more than 20 mm, is a strong indication for osteotomy. The Q angle, although a less precise indicator of malalignment, is also elevated and would be considered an indication for osteotomy.

CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 41
A healthy, active 18-year-old man has acute-onset right knee pain and an inability to fully extend his knee following an attempt to stand from a seated position yesterday. He sustained a noncontact injury to his right knee while playing basketball 2 years ago and underwent primary anterior cruciate ligament (ACL) reconstruction with bone-patella-tendon-bone autograft and medial meniscus repair. He sustained another noncontact injury to the same knee 8 months later and underwent a revision ACL reconstruction using soft-tissue allograft and revision medial meniscus repair. He reports multiple episodes of “giving way” of his knee, but no pain prior to yesterday’s acute injury.
Question 60
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should
Explanation
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
Question 61
A 31-year-old man sustained a closed injury to his arm in a motor vehicle accident 16 months ago. Treatment of the fracture consisted of intramedullary nailing of the humerus. He now reports pain with minimal activities. Clinical examination and laboratory studies suggest no signs of infection. Radiographs are seen in Figures 12a through 12c. Treatment should now consist of
Explanation
REFERENCES: Zuckerman J, Giordanno C, Rosen H: Treatment of humeral shaft non-unions, in Bigliani L (ed): Complications of shoulder surgery. Baltimore, MD, William & Wilkins, 1993, pp 173-190.
Jupiter JB: Complex non-union of the humeral diaphysis: Treatment with a medial approach,
an anterior plate, and a vascularized fibular graft. J Bone Joint Surg Am 1990;72:701-707.
Question 62
The palmar cutaneous branch of the median nerve (PCBMN) originates from the
Explanation
REFERENCES: Hobbs RA, Magnussen PA, Tonkin MA: Palmar cutaneous branch of the median nerve. J Hand Surg Am 1990;15:38-43.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
p 52.
Question 63
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads?
Explanation
REFERENCE: Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.
Question 64
A 51-year-old woman with shoulder pain responds transiently to a subacromial injection and physical therapy exercise program. When her symptoms recur, an arthroscopic subacromial decompression is recommended. During the surgery, a partial-thickness articular-sided supraspinatus tear is noted. The supraspinatus footprint is exposed for 3 mm from the articular margin. The remaining intra-articular structures are normal. Inspection from the bursal surface reveals the tendon to be intact. What is the most appropriate course of management? Review Topic
Explanation
Question 65
What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?
Explanation
REFERENCES: Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
Steinmann SP, Linsheid RL: Pisotriquetral loose bodies. J Hand Surg 1997;22:918-921.
related link ortho mcqs bank
Question 66
What would be the most appropriate surgical indication for transferring fascicles of the ulnar nerve to the motor nerve of the biceps and fascicles of the median nerve to the motor nerve of the brachialis?
Explanation
Plantar distal phalanges to medial navicular
Medial navicular to dorsal lateral cuneiform
Plantar 1st metatarsal to dorsal lateral cuneiform
5th metatarsal base to dorsal medial cuneiform
Plantar distal phalanx of the hallux to dorsal distal phalanx of hallux
Dynamic tendon transfer to restore active dorsiflexion of the foot involves transferring the posterior tibial tendon (PTT) insertion on the medial navicular to the dorsal lateral cuneiform.
Common peroneal nerve (CPN) injuries following traumatic knee dislocation are common, with an incidence of 25-40%. CPN palsy is characterized by foot drop due to loss of ankle dorsiflexors with a steppage gait and eventual development of a supinated equinovarus foot secondary to the unopposed pull of the PTT. Nonsurgical management involves use of an ankle-foot orthosis and physical therapy. Surgical
options include acute primary repair, nerve grafting with either autologous sural nerve or nerve conduits and dynamic tendon transfer. The PTT is harvested from its insertion at the navicular, passed through the interosseous membrane (IOM) and anchored to the lateral cuneiform (see Illustration A). The classic bridle procedure involves concomitant anastamosis of the PTT to the tibialis anterior (TA) and peroneus longus (PL) tendons.
Garozzo et al reported a case series of 62 patients with post-traumatic CPN palsy who underwent a one-stage procedure consisting of nerve repair and PTT transfer. Nerve repair combined with PTT transfer improved postoperative outcomes compared to nerve repair alone. At 2-year follow up, neural regeneration was demonstrated in 90% of patients. The authors hypothesized that poor outcomes following nerve repair alone are due to force imbalance between the functioning flexors and paralyzed extensors, which is somewhat equalized by performing a PTT transfer at time of repair.
Niall et al reviewed 55 patients with traumatic knee dislocation and reported a 41% incidence of CPN injury, exclusively associated with dislocations involving disruption of the posterior cruciate ligament (PCL) and posterolateral corner (PLC). Complete neurologic recovery was found in only 21% of patients. The best prognosis was found with lesions in continuity, less than 7cm of nerve involvement, and short conduction block and muscle activity on nerve conduction and EMG studies.
Vigasio et al described a dynamic tendon transfer technique for traumatic complete CPN injury, involving transfer of the PTT to the TA rerouted to a new origin at the lateral cuneiform to restore ankle dorsiflexion and flexor digitorum longus (FDL) to the extensor digitorum longus (EDL) and extensor hallucis longus (EHL) to restore digit dorsiflexion. Rerouting the TA towards the transferred PTT ensures the PTT harvest length is sufficient. This avoids excessive tensioning of the PTT, which may limit tendon excursion and result in a static tenodesis rather than dynamic function, as well as the need for PTT lengthening which may decrease strength of the transfer
Illustration A is a series of intraoperative photographs demonstrating PTT transfer from Garg et al. An incision is made distal to the medial malleolus and the PTT is harvested subperiosteally (A). The PTT is delivered through a second incision ~15cm proximal to the medial malleolus (B-C). The PTT is then passed through the interosseous membrane and out a third incision over the anterior fibula (D). Lastly, the PTT is passed through a fourth incision over the dorsal midfoot and anchored to the lateral cuneiform (E).
Incorrect Responses:
nerve and therefore would not be functional. Answer 5: Transferring the flexor hallucis longus (FHL; insertion = plantar distal phalanx of the hallux) to the insertion of the EHL (dorsal distal phalanx of hallux) is recommended for correction of claw toe deformity and would not help restore foot dorsiflexion in this patient.
Question 67
What is the most common behavioral effect of anabolic steroid use in athletes?
Explanation
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Blue JG, Lombardo JA: Steroids and steroid-like compounds. Clin Sports Med
1999;19:667-689.
Question 68
When posterior fusion with instrumentation to the sacrum is used to treat adult scoliosis, what instrumentation technique best increases the chance of a successful lumbosacral fusion?
Explanation
REFERENCES: Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173.
O’Brien N, et al: Sacral pelvic fixation and spinal deformity, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 601-614.
McCord DH, Cunningham BW, Shono Y, et al: Biomechanical analysis of lumbosacral fixation. Spine 1992;17:S235-S243.
Question 69
A hip compression screw is placed in a test jig and a bending load is applied to the tip of the screw. After the load is released, the screw returns completely to its original shape. What is this type of deformation called?
Explanation
Question 70
A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Raskin KB, Parisi D, Baker J, et al: Dorsal open repair of proximal pole scaphoid fractures. Hand Clin 2001;17:601-610.
Question 71
A 48-year-old woman has an open subtrochanteric femur fracture. No other injuries are reported. After thorough evaluation, it is determined that she will need emergent surgical fixation. The patient and family indicate that they are practicing Jehovah's witnesses and desire adherence to the religious standards with respect to blood product usage. The patient signs a valid advanced directive confirming these wishes. Which of the following would be considered acceptable treatment?
Explanation
Question 72
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Warner JJ, Johnson D, Miller M, Caborn DN: Technique for selecting capsular tightness in repair of anterior-inferior shoulder instability. J Shoulder Elbow Surg 1995;4:352-364.
Question 73
Figure 30 shows the AP radiograph of a 9-month-old girl who has been referred for evaluation of unequal leg lengths. Examination reveals symmetrical abduction of the hips. When the hips are flexed 90°, the right knee height is greater than the left knee. The girth of the right thigh and calf is larger than the contralateral side. There are no cutaneous lesions, and examination of the spine is normal. The infant is moving all extremities equally and spontaneously. Management should consist of
Explanation
REFERENCES: Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont Ill, American Academy of Orthopaedic Surgeons, 1996, pp 185-193.
Sponseller PD: Localized disorders of bone and soft tissue, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 305-344.
Beals RK: Hemihypertrophy and hemihypotrophy. Clin Orthop 1982;166:199-203.
Question 74
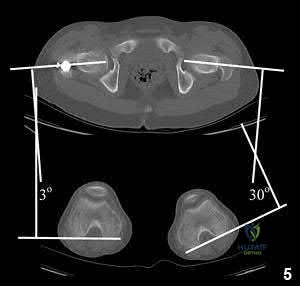
A 55-year-old male is involved in a motorcycle crash and sustains a closed, right-sided, midshaft femur fracture. This is an isolated injury. He is treated with retrograde femoral nailing, and postoperatively is noted to have 30 degrees of internal rotation of the operative extremity, when compared with his nonsurgical side. Which of the following is the most likely cause of this malrotation deformity?
Explanation
Postsurgical internal malrotation after treatment for a diaphyseal femur fracture typically occurs either via internal rotation of the distal segment relative to the proximal or external rotation of the proximal segment relative to the distal. These clinical findings are consistent with an iatrogenic increase in femoral anteversion.
Dimitriou et al. performed a study to quantify the side-to-side anatomic variation in the proximal femur and the implications for preoperative planning and leg length discrepancy following hip arthroplasty. CT-based 3D femoral models were reconstructed for 122 paired femurs in 61 young healthy subjects with no history of hip pathology. Significant side-to-side differences were found in femoral anteversion, horizontal offset, and femoral head center location.
They concluded that relying on the anatomic landmarks of the contralateral femur during hip arthroplasty may not necessarily result in restoration of native anatomy and leg-length.
Karaman et al. conducted a study which saught to clarify the influence of a femoral rotational malalignment of ≥10° after intramedullary nailing on daily activities. They evaluated twenty-four femoral shaft fracture patients treated with closed antegrade IMN, and determined the presence of malrotation with post-operative CT scans. Ten of the 24 patients had a CT-detected true rotational malalignment of ≥10° compared with the unaffected side, and were noted to have significantly worse functional outcome scores compared with normally rotated femoral shaft patients.
Espinoza et al. present a technique using intraoperative fluoroscopy and the anteversion inherent to the IM nail for obtaining appropriate femoral rotational alignment during surgery. The authors state that their technique reliably sets the femoral anteversion within a normal physiologic range with minimal additional intraoperative steps and without preoperative measurements.
Illustration A shows a CT evaluation of femoral malrotation. The angle on the uninjured side measures 30°, while the malrotated fractured side measures only 3°, indicating a 27° external rotation deformity.
Incorrect Answers:
OrthoCash 2020
Question 75
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of Review Topic

Explanation
Question 76
A 25 year-old-male presents with the injury seen in Figure A. Which of the following would be a contraindication to closed management with a functional brace?

Explanation
Indications for operative management of humeral shaft fractures are limited given the high rates of union and ability of adjacent joints to compensate for deformity. Intact muscular tone is necessary to effect bony apposition in closed treatment with a functional brace. The absence of neurologic and muscle function in patients with a flail extremity leads to increased rates of nonunion and malunion.
Rutgers and Ring conducted a retrospective review of patients managed with functional bracing of humeral shaft fractures at a single institution. The authors found a 90% overall union rate, with maintenance of shoulder and elbow motion. They caution though, that 29% of their proximal third fractures went on to nonunion.
Figure A demonstrates an AP radiograph of a comminuted humeral shaft fracture with varus alignment.
Incorrect Answers:
Question 77
Contraindications to cervical laminectomy as a treatment for cervical spondylotic myelopathy include which of the following findings?
Explanation
REFERENCES: Malone DG, Benzyl EC: Laminotomy and laminectomy for spinal stenosis causing radiculopathy or myelopathy, in Clark CR (ed.): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 817-825.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 673-680.
Question 78
When the iliac apophysis starts ossifying in the normal adolescent, growth of the sitting height or trunk height is characterized by
Explanation
REFERENCES: Anderson M, Hwang SC, Green WT: Growth of the normal trunk in boys and girls during the second decade of life: Related to age, maturity, and ossification of the iliac epiphyses. J Bone Joint Surg Am 1965;47:1554-1564.
Zaoussis AL, James JIP: The iliac apophysis and the evolution of curves in scoliosis. J Bone Joint Surg Br 1958;40:442-453.
Question 79
Placing a plate too anteriorly against the lateral aspect of the bicipital groove while performing open reduction and internal fixation (ORIF) of a proximal humerus fracture has an increased risk of what complication?
Explanation
the other complications noted.
Question 80
-Postsurgically, the patient recovers well and is fully rehabilitated. He demonstrates full motion with no instability or pain and is cleared to return to play 12 months after the surgery. He asks for your advice regarding use of a functional brace for playing basketball following his reconstruction. What is the most appropriate recommendation?
Explanation
The athlete most likely suffered an acute ACL rupture however the presence of a lipohemarthrosis is concerning for the possibility of an intraarticular fracture. Because of this, the patient should not be allowed full weight bearing until a fracture is ruled out with radiographs. Given the athlete’s inability to perform a straight leg raise, the extensor mechanism is not functioning and a telescoping knee brace locked in extension should be utilized. A neoprene knee sleeve does not have a role in the
treatment of this acute injury.The radiographs reveal a lateral avulsion fracture off of the proximal tibial epiphysis which is known as a Segond fracture. It is indicative of an ACL injury and the fracture fragment seen is the consequence of the lateral capsule injury sustained during the pivot-shift mechanism. There is no radiographic evidence of a medial tibial plateau fracture. A radiographic sign of a chronic MCL injury is known as a Pellegrini-Stieda lesion and this is seen as calcification of the femoral origin of the MCL. A radiographic sign of an acute LCL rupture would be an avulsion fracture of the tip of the fibula.The MRI shows kissing contusions of the posterolateral tibial plateau and the midpoint of the lateral femoral condyle. These “kissing lesions” are seen as a result of a pivot shift mechanism of injury and are diagnostic for an ACL rupture. The most common associated injury in an acute ACL rupture is a lateral meniscus tear. Medial meniscus tears are more common in chronic ACL injuries. PCL rupture and PLC injury are all associated injuries seen in acute ACL rupture; however, these are much less common than meniscal tears. The team physician has a role in encouraging, but
not demanding, the athlete to report the injury andtreatment to the scholarship school’s coaching staff. What the athlete decides to do is his decision; the physician would be violating the athlete’s HIPAA rights as well as their confidence by reporting it directly to the scholarship school. Clearly the physician should not discourage the athlete from reporting the injury. The athlete is 18 years old and, as such, the physician would need the athlete’s permission to discuss any medical issues with the family in keeping with HIPAA.
The athlete’s exam demonstrates incompetence of both bundles of the ACL as demonstrated by the loss of stability with anterior translation of the tibia (Lachman test) as well as with rotation (pivot shift). The external rotation stress with the knee in 30 degrees of flexion tests the competence of the posterolateral corner while rotation at 90 degrees of flexion tests the PCL. Since the athlete’s knee is stable to posterior drawer testing demonstrating an intact PCL and the external rotation at 30 degrees is equivalent to that at 90 degrees, the posterolateral corner in intact.
The ACL has two separate and distinct bundles, the AM and PL. Each bundle takes on tension at varying degrees of knee flexion and therefore each bundle is thought to have a varying contribution to the stability of the knee. The AM bundle takes on tension with the knee in flexion and the PL bundle is tight in extension. Neither bundle is isometric during knee range of motion. Both bundles have contributions to rotational stability of the knee throughout the range of motion.
The success of traditional trans-tibial single-bundle ACL reconstruction has recently been called into question given the demonstration of persistent rotational instability following reconstruction. The persistence of rotational instability in trans-tibial single bundle ACL reconstruction has been attributed to the location of the graft in a vertically malpositioned femoral tunnel. The goal of double-bundle ACL reconstruction is to more accurately reproduce the native ACL and provide grafts that contribute to anteroposterior stability as well as rotational stability by placing the grafts in more anatomic locations not central in the knee axis. There is an increased cost and surgical time associated with double-bundle reconstruction.
The use of functional braces following ACL reconstruction is a surgeon’s preference because there is no difference in retear rate with or without a brace. Some authors recommend brace use for one to two years following ACL reconstruction for all athletic activities, but this is not supported by the literature. No literature exists showing a higher rate of reinjury with a functional brace and off-the shelf and custom braces have been found to be equivalent leading those who advocate for braces to recommend off-theshelf braces given their significantly lower cost.
Question 81
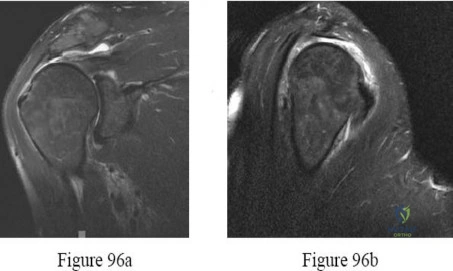
A 32-year-old powerlifter who was performing a dead lift 3 days ago noted a sharp pain in the front of his dominant right arm just after beginning to lower the weight. He now reports pain in the anterior aspect of the arm that worsens when he opens a door. Examination reveals moderate ecchymosis and swelling of the forearm and tenderness in the antecubital fossa. The MRI scans are shown in Figures 15a and 15b. If the injury is left unrepaired, the greatest functional deficit will most likely be the loss of
Explanation
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Agins HJ, Chess JL, Hoekstra DV, Teitge RA: Rupture of the distal insertion of the biceps brachii tendon. Clin Orthop 1988;234:34-38.
Question 82
A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient? Review Topic

Explanation
Question 83
Excision of heterotopic bone about the forearm or elbow can be done with limited recurrence rates as early as which of the following after initial injury?

Explanation
The referenced study by McAuliffe et al is a retrospective review of heterotopic ossification (HO) about the elbow followed by 100 cGY (5 fractions over 1 week) of XRT as early as 3 months post-injury. They were able to achieve an average arc of motion > 100 degrees.
The other referenced study by Beingessner et al is a review of HO excision of the forearm. They found that excision and XRT, followed by 6 weeks of indomethacin, led to an increase of forearm motion from an average of 17 degrees to 136 degrees when the excision was done at 4 months post-injury.
Question 84
What muscles are responsible for the most common deformity after antegrade intramedullary nailing for a subtrochanteric femur fracture?

Explanation
The reference by French et al is a review on 45 patients with subtrochanteric fractures treated with cephalomedullary interlocked nailing. Based on femoral neck-shaft angle, 61% of the fractures were reduced in at least 5º varus. The authors attributed this malalignment to failure to counteract muscle forces acting on the proximal fragment, combined with the adducted position of the distal femur during portal creation.
The reference by Ricci et al is a report of 403 femoral shaft fractures treated with intramedullary nailing. Patients with proximal femoral shaft fractures were found to have the highest incidence of malalignment. The most common deformity in this group was varus, followed by procurvatum (or flexion).
Question 85
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints?
Explanation
After activity, pain persists longer with tibial stress fractures.
DISCUSSION: Anterior tibial pain can often be difficult to diagnose. A bone scan showing the tibial cortex in a diffuse, longitudinal orientation is consistent with shin splints compared to a more discreet, localized uptake more commonly seen with a stress fracture. Bone stress injuries are due to cyclical overuse of the bone. They are relatively common in athletes and military recruits but are also seem in otherwise healthy people who have recently started new or intensive physical activity. Diagnosis of bone stress injuries is based on the patient’s history of increased physical activity and on imaging findings.
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
REFERENCES: Mubarak SJ, Gould RN, Lee YF, et al: The medial tibial stress syndrome: A cause of shin splints. Am J Sports Med 1982;10:201-205.
Knobloch K, Yoon U, Vogt PM: Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int 2008:29:671-676.
Kiuru MJ, Pihlajamaki HK, Ahovuo JA: Bone stress injuries. Acta Radiol 2004;45:317-326.
Question 86
A 14-year-old boy is lifting weights and feels a sudden pain in his back, associated with sciatica bilaterally. The sciatica persists for several weeks. The radiograph shown in Figure 7a is negative, and the CT scan shown in Figure 7b is available for evaluation. An MRI scan is read as a disk bulge. Management should consist of
Explanation
REFERENCE: Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 694.
2010 Pediatric Orthopaedic Examination Answer Book • 13
Question 87
Which of the following therapies has a direct anabolic effect on bone?
Explanation
Question 88
Figures 45a and 45b show the AP and lateral radiographs of a 15-year old patient who is undergoing surgery to add 3 cm of length to the femur. Based on the radiographic findings, what is the next most appropriate step in management?
Explanation
REFERENCES: Raney EM: Limb-length discrepancy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1519-1526.
Ilizarov GA: Pseudarthroses and defects of long tubular bones, in Transosseous Osteosynthesis: Theoretical and Clinical Aspects of the Regeneration and Growth of Tissue. Berlin, Springer-Verlag, 1992, p 453.
Question 89
Which of the following is considered a contraindication to the use of a reverse total shoulder arthroplasty? Review Topic
Explanation
Question 90
A 75-year-old woman with rheumatoid arthritis and a long history of oral corticosteroid use sustains a comminuted intra-articular distal humerus fracture. What is the best surgical option?
Explanation
superior to ORIF at a minimum of 2 years of follow-up. TEA was especially useful in patients with comorbidities that compromise bone stock, including osteoporosis and oral corticosteroid use. Closed
reduction and percutaneous pinning studies have not been published on the adult population.
Question 91
When compared to patients with osteoarthritis, patients with ankylosing spondylitis undergoing total hip arthroplasty can expect a
Explanation
REFERENCE: Joshi A, Markovic L, Hardinge K, Murphy J: Total hip arthroplasty in ankylosing spondylitis: An analysis of 181 hips. J Arthroplasty 2002;17:427-433.
Question 92
When compared with reamed intramedullary nailing for an unstable diaphyseal tibia fracture, unreamed nailing is associated with which of the following?
Explanation
Question 93
- What is the most common sequela of turf toe (hyperextension of the first metatarsophalangeal joint)?
Explanation
What they found was a decreased ROM of the first MTPJ in patients with turf toe and stated that it demonstrates the POSSIBILITY of long-term sequelae to the turf toe injury and that hallux rigidus must be considered in the athlete with progressively limited ROM. Other possible
sequelae cited were hallux valgus, production of a dorsal osteophyte, calcification in periarticular soft tissue, and chondromalacia of the head of the first metatarsal. NO MENTION WAS MADE OF THE MOST COMMON SEQUELAE OF TURF TOE!
Clanton & Schon Chapter 27 Mann Foot & Ankle state that it remains unclear whether these sprains (turf toe) will ultimately result in arthritic changes in the affected joint. No mention is made of hallux rigidus. Again in Mann Chapter 14 on hallux rigidus states that the etiology is degenerative arthritis of the first MTPJ and what predisposes the patient to degenerative arthritis is not known. No mention is made of turf toe.
Question 94
The so-called high ankle sprain from an external rotation mechanism of injury typically involves injury to which of the following structures?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 182.
Kaye RA: Stabilization of ankle syndesmosis injuries with a syndesmosis screw. Foot Ankle 1989;9:290-293.
Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
Pfeffer GB (ed): Chronic Ankle Pain in the Athlete. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 11.
Question 95
Which of the following changes is seen with age and degeneration in the intervertebral disk? Review Topic
Explanation
Question 96
A 47-year-old woman has had medial ankle pain and swelling for the past 3 months. She recalls no specific injury, and casting and nonsteroidal anti-inflammatory drugs have failed to provide relief. Examination reveals a pes planus with heel valgus that is passively correctable. Radiographs show no evidence of arthritis. An MRI scan is shown in Figure 16. What is the most appropriate surgical procedure to alleviate her pain?
Explanation
REFERENCES: Myerson MS, Corrigan J: Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon transfer and calcaneal osteotomy. Orthopedics 1996;19:383-388.
Mosier-LaClair S, Pomeroy G, Manoli A II: Operative treatment of the difficult stage 2 adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:95-119.
Question 97
A 54-year-old laborer has a 6-month history of lateral elbow pain. An elbow examination reveals full range of motion, tenderness over the lateral epicondyle, and pain with resisted wrist extension with the elbow in extension. Elbow radiograph findings are normal. You perform a steroid injection and the patient's symptoms are decreased 6 weeks later. One year after receiving the injection, this patient—when compared to a patient who did not have a steroid injection—is likely to
Explanation
This patient has signs and symptoms of lateral epicondylitis. Treatments include various forms of physical therapy, iontophoresis, corticosteroid injection, nitroglycerin patch treatment, blood injections, prolotherapy, and surgical intervention. No single treatment is superior to other treatments for this common problem. Several studies have demonstrated a short-term decrease in symptoms following steroid injection (6 weeks) but an increased likelihood of persistent symptoms 1 year after treatment. Steroid injection at this site has not been associated with increased risk for tendon rupture or need for surgical intervention.
Question 98
03 A 13 y/o girl sustains the injury shown in Figures 69a and 69b in a fall. Examination reveals this to be an isolated injury, and the patient’s neurologic and vascular examinations are normal. Based on these findings, management should consist of
Explanation
pinning may be performed. If the articular surface shows that the fx line has extended into the joint and the articular surface is separated, open reduction and pinning are necessary. Once the fx is stabilized, the elbow is immobilized for 4 wks. The pins are then removed & motion is begun.
back to this question next question
Question 99
Which of the following is considered the best cementless acetabular reconstruction method when planning for total hip arthroplasty in a patient with developmental dysplasia of the hip (DDH)?
Explanation
REFERENCES: Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360.
Dorr LD, Tawakkol S, Moorthy M, Long W, Wan Z: Medial protrusio technique for placement of a porous-coated, hemispherical acetabular component without cement in a total hip arthroplasty in patients who have acetabular dysplasia. J Bone Joint Surg Am 1999;81:83-92.
Jasty M, Anderson MJ, Harris WH: Total hip replacement for developmental dysplasia of the hip. Clin Orthop 1995;311:40-45.
Question 100
- Figures 42a and 42b show the sagittal and axial MRI scans of a 24-year-old patient who has sciatia. Which of the following combinations of physical findings is most consistent wit the MRI studies?
Explanation
