Orthopedic Board Review MCQs: Spine, Knee & Trauma | Part 165
Key Takeaway
This page presents Part 165 of a comprehensive Orthopedic Surgery board review quiz. It features 100 high-yield MCQs on Cartilage, Knee, Trauma, and more. Designed for orthopedic surgeons and residents, it aids in preparing for AAOS/ABOS board certification and OITE exams, with flexible study modes.
About This Board Review Set
This is Part 165 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 165
This module focuses heavily on: Cartilage, Deformity, Knee, Ligament, Trauma.
Sample Questions from This Set
Sample Question 1: A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise...
Sample Question 2: A previously asymptomatic 12-year-old girl sustained a direct blow to the right lateral knee from a baseball bat. Examination reveals an area of ecchymosis and tenderness over the lateral thigh. The patient can walk without pain, but range ...
Sample Question 3: Which of the following rehabilitation techniques is appropriate for initial nonsurgical management of an isolated grade 2 posterior cruciate ligament injury? Review Topic...
Sample Question 4: Which factor is a contraindication to surgical treatment of a symptomatic CAM deformity?...
Sample Question 5: A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
REFERENCES: Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Hoppenfeld S: Orthopaedic Neurology: A Diagnostic Guide to Neurologic Levels. Philadelphia, PA, JB Lippincott, 1977, pp 7-43.
Question 2
A previously asymptomatic 12-year-old girl sustained a direct blow to the right lateral knee from a baseball bat. Examination reveals an area of ecchymosis and tenderness over the lateral thigh. The patient can walk without pain, but range of motion of the knee causes discomfort. Plain radiographs of the knee are shown in Figures 11a and 11b. To address the bone lesion, management should consist of
Explanation
REFERENCE: Davids JR, Glancy GL, Eilert RE: Fracture through the stalk of pedunculated osteochondromas: A report of three cases. Clin Orthop 1991;271:258-264.
Question 3
Which of the following rehabilitation techniques is appropriate for initial nonsurgical management of an isolated grade 2 posterior cruciate ligament injury? Review Topic
Explanation
Question 4
Which factor is a contraindication to surgical treatment of a symptomatic CAM deformity?
Explanation
Multiple studies have confirmed that CAM or pincer anatomy is commonly present in asymptomatic hips. According to a large systematic review, CAM deformities are present in approximately one-third of asymptomatic hips in young adults, and the proportion was higher than 50% in the subgroup of athletes.
Ganz and associates proposed that femoral acetabular impingement is the root cause of osteoarthritis in the majority of nontraumatic, nondysplastic hips, and functional improvement with surgical correction of the deformity has been demonstrated. Despite the link between CAM deformity and hip osteoarthritis, a corresponding link between correction of the deformity and prevention of osteoarthritis has never been proven.
Results of CAM deformity correction, typically including repair of the degenerative labral tear, are much poorer when there is significant joint space loss. A typical joint space cutoff of 2 mm or less is used to recommend against hip preservation surgery.
Question 5
A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?
Explanation
REFERENCES: Brittberg M, Peterson L, Sjogren-Jansson E, et al: Articular cartilage engineering with autologous chondrocyte transplantation. J Bone Joint Surg Am
2003;85:109-115.
Caplan AI, Elyaderani M, Mochizuki Y, et al: Principles of cartilage repair and regeneration. Clin Orthop 1997;342:254-269.
Question 6
A 47-year-old man has left-sided motor weakness in the extensor digitorum longus and extensor hallucis longus, sensory loss in the lateral calf and dorsal foot, and no discernible reflex loss.
Explanation
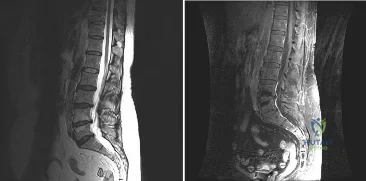
Figures 72a and 72b are the T1-weighted MR images of a disk bulge. Disk bulges are common in asymptomatic people and are not predictive of pathology. Figures 72c and 72d show T1 MR images of a far lateral disk herniation at the L4-L5 level. This would affect the exiting or L4 nerve root. Radicular symptoms would occur at the L4 level. Figures 72e and 72f show an annular tear at the L4-L5 level. This pathology is associated with discogenic low-back pain. Figures 72g and 72h show the T1 MR images of a central lateral disk herniation at the L4-L5 level. This would affect the traversing or L5 nerve root. Radicular symptoms would occur at the L5 level.
RECOMMENDED READINGS
Jarvik JG, Hollingworth W, Heagerty PJ, Haynor DR, Boyko EJ, Deyo RA. Three-year incidence of low back pain in an initially asymptomatic cohort: clinical and imaging risk factors. Spine (Phila Pa 1976). 2005 Jul 1;30(13):1541-8; discussion 1549. PubMed PMID: 15990670.View Abstract at PubMed
Hoppenfeld S. Physical Exam of the Spine and Extremities. Stamford, CT: Appleton and Lange; 1995.
Madigan L, Vaccaro AR, Spector LR, Milam RA. Management of symptomatic lumbar degenerative disk disease. J Am Acad Orthop Surg. 2009 Feb;17(2):102-11. Review. PubMed PMID: 19202123.View Abstract at PubMed
Question 7
The CT scan shows the involvement area is approximately 30% of the posterior facet. What is the most appropriate treatment?
Explanation
Radiographs reveal a talocalcaneal coalition. The incidence of tarsal coalition in the general population ranges between 2% and 13%. The incidence of tarsal coalition among patients with FGFR-related craniosynostosis syndromes is much higher than among the general population. Tarsal coalitions have been noted in FGFR-1-, FGFR-2-, and FGFR-3-related craniosynostosis syndromes of Apert, Pfeiffer, Crouzon, Jackson-Weiss, and Muenke, but not in Beare-Stevenson or Crouzonodermoskeletal syndromes. The FGFR genes are involved in cell proliferation, differentiation, migration, apoptosis, and pattern formation.
Additionally, nonsyndromic familial coalitions have been described with autosomal-dominant patterns of inheritance.
Cross-sectional imaging should always be obtained prior to resection of a radiographically evident coalition to define the extent of the coalition and determine the coexistence of an additional coalition. CT scan is the gold standard test; however, MRI can be helpful to define a suspected fibrous coalition if a CT scan is nondiagnostic. A bone scan may be useful if pain or history is atypical for a symptomatic coalition. Laboratory tests such as CBC, ESR, CRP, ANA, and RF may be indicated if the imaging evaluation does not confirm a tarsal coalition and if there is concern for malignancy, infection, or inflammatory arthritis.
Investigators have suggested that larger talocalcaneal coalitions with surface areas larger than 33% to 50% of the size of the posterior facet are unsuitable for resection and primary arthrodesis should be considered. However, a study by Koshbin and associates found that with long-term follow-up, favorable functional outcomes were seen even with resections of large talocalcaneal coalitions occupying more than 50% of surface area.
Question 8
A study is proposed in which 2 groups of patients are randomized to treatment with bisphosphonates or placebo. This is an example of what study type?
Explanation
Question 9
A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?

Explanation
Myerson reported 3/43 patients in his series below had chronic foot compartment syndrome. There are 9 compartments in the foot: (1) medial, (2) superficial, (3) lateral, (4) adductor, (5-8) four interossei, and (9) calcaneal. The plantar fascia limits the space available for hematoma and swelling, causing damage to the intrinsic flexors of the foot (particularly the lumbricals and interossei), resulting in clawtoes.
Question 10
A female cross-country runner has an insidious onset of right groin pain. Radiographs of the right hip reveal a tension-side stress fracture. History reveals that she was treated for a “foot” fracture 1 year ago. In addition to performing internal fixation of the femoral neck, which of the following should be obtained?
Explanation
REFERENCES: Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Barrow GW, Saha H: Menstrual irregularity and stress fractures in collegiate female distance runners. Am J Sports Med 1988;16:209-216.
Question 11
Figure 17 shows the AP radiograph of a 5-year old child who has mild short stature and a painless bilateral gluteus medius lurch. Initial work-up should include
Explanation
REFERENCES: Sponseller PD: Skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 269-270.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 689-691.
Question 12
Metastatic disease of several cancers create lytic lesions because these cancers:
Explanation
Cancers that originate or metastasize to bone can be blastic, lytic, or mixed when viewed on radiographs. Lytic lesions appear radiolucent due to bone resorption that occurs around the cancer cells. This is secondary to direct production and release of RANKL by the cancer cells themselves. RANKL then stimulates osteoclastogenesis and an increase in local bone resorption. Denosumab is a monoclonal antibody against RANKL that has been shown to decrease rates of pathologic fractures.
Lynch et al. review the progression of metastatic disease. They note that cancer cells can stimulate both osteogenesis and osteolysis, and that this pathologic increase in bone matrix turnover is what allows the cancer to progressively expand or metastasize to distant sites. They discuss the role of matrix metalloproteinases as primary regulators of this process.
Illustration A is a diagram illustrating how the binding of RANKL to receptors on the surface of osteoclast precursors activates them and begins the process of bone resorption. Cancer cells can directly produce RANKL thus increasing the rate of local bone resorption.
Incorrect Answers:
Question 13
What property of titanium alloys accounts for their high corrosion resistance in vivo?
Explanation
REFERENCES: Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott, 2003, vol 1, pp 269-278.
Lemons JE: Metallic alloys, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 19-27.
Question 14
Figure 3 is the clinical photograph of a 20-year-old college soccer player who has a 7-day history of worsening left ankle pain and swelling after being slide-tackled in a game. Radiograph findings of his ankle and foot are normal. He complains of malaise. His history includes a severe ankle sprain 3 months ago. The sprain caused him to miss half the season, but he was able to play in the last 2 games. What is the most appropriate treatment? Review Topic

Explanation
Question 15
An 76-year-old woman falls from standing and sustains the injury shown in Figure A. Her most recent T score was -1.9, 3 months prior to presentation. If labwork were performed, which values would be consistent with her bone density score?

Explanation
In the setting of osteopenia/osteoporosis, there is a positive feedback to increase PTH in response to low serum calcium levels. In response, there is a corresponding increase in alkaline phosphatase and decrease in phosphorous and circulating vitamin D levels.
Fraser writes a concise, yet thorough synopsis on primary and secondary hyperparathyroidism. In the article, the summary regarding osteopenia/osteoporosis (typically a state of hypovitamin D) begins by stating an initial state of decreased ionised calcium, which increases PTH, results in 3 primary effects: an attempt to increase gut absorption of Ca, mobilize Ca from the bone via osteoclasts and activate vitamin D at the kidney (1,25-vitamin D).
Figure A exhibits a left femoral neck fracture, which is a fragility fracture associated with poor bone density. Illustration A is a figure from Fraser's article exhibiting the feedback loop from the hypothalamus, pituitary, adrenal/glandular axis.
Incorrect answers:
Question 16
Figure 33a shows a line drawing of a normal hemipelvis. The anterior acetabular rim is bold. Figure 33b illustrates a hemipelvis with a crossover sign, which is indicative of what acetabular pathology? Review Topic

Explanation
Question 17
03 A 23 year old sustains an isolated right knee dislocation in an MVA. A closed reduction is performed and confirmed with radiographs. What is the next appropriate study?
Explanation
OKU Truama 2 says “the use of ABI with the blood pressure cuff and Doppler evaluation of the distal circulation has been proposed as effective in determining any occult vascular injury. A ratio > 0.9indicates a normal study.”[1] The referenced article confirms this. “Confirmation of the safety and accuracy of physical exam in the evaluation of knee dislocation for injury of the popliteal artery.” J. Trauma2002; 52: 247-252
back to this question next question
[1] OKU Trauma 2 pg 151-153
Question 18
Which of the following is the most sensitive parameter to detect the increased inflammatory response seen with both postoperative infection and the use of instrumentation in spinal surgery?

Explanation
DISCUSSION: The most sensitive parameter to detect inflammation elicited by implants and infection is the C-reactive protein (CRP).
CRP is an acute phase reactant that increases sharply immediately after surgery within 6 hours after tissue damage. CRP then peaks 2-3 days later and returns to normal levels 5-21 days after the inciting event. In contrast, ESR reaches its peak on days 4-11, then remains elevated for a prolonged period of time.
Takahashi et al performed a Level 3 study of patients who had undergone spinal surgery with and without instrumentation, with a primary outcome of infection. They concluded that renewed elevation of C-reactive protein, white blood cell count, and body temperature after postoperative days 4 to 7 may be a key indicator of postoperative infection.
Question 19
A computed tomography (CT) scan has been shown to be indicated for evaluation of all of the following aspects of acetabular fractures, EXCEPT:

Explanation
with CT scanning and acetabular fractures, and noted a 25% change in surgical planning when CT was utilized versus plain radiographs; they also noted the ability to detect marginal impaction and fracture size/position was improved with CT.
Question 20
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time?
Explanation
REFERENCES: Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217.
Hart RA: Cervical facet dislocation: When is magnetic resonance imaging indicated? Spine 2002;27:116-117.
Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 21
A 65-year-old woman has significant neck pain after falling and striking her head. A radiograph and sagittal CT scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, pp 927-937.
Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2003, pp 455-458.
Question 22
Ten years after undergoing TKA, a 77-year-old woman experiences 2 weeks of pain, swelling, and erythema following a routine dental cleaning procedure (Figures 109a and 109b). Her erythrocyte sedimentation rate is 25 mm/h (reference range 0-20 mm/h), her C-reactive protein level is 1.7 mg/L (reference range, 0.08-3.1 mg/L), and alpha-defensin findings are negative.
Explanation
Managing complications following a failed TKA requires an understanding of the mode of failure and treatment principles. Generally, TKA can fail for the following reasons: infection, instability, aseptic loosening, stiffness, and extensor mechanism dysfunction.
Managing an infected TKA requires knowledge of the timing and circumstances surrounding the infected implant. Patients with acute infections (symptom duration of fewer than 3 weeks) are candidates for debridement and prosthesis retention. Chronic infections (symptoms lasting longer than 3 weeks and for more than 3 months from the time of index arthroplasty) should be treated with resection arthroplasty, parenteral antibiotics, and reimplantation surgery at a later date. Evaluation of possible acute infections should include aspiration, serology, and alpha-defensin.
Instability following TKA is a common cause of early failure and revision surgery. The etiology of instability can include overresection of the posterior condyles, collateral ligament insufficiency, and late rupture of the posterior cruciate ligament. Recognizing the cause of instability is critical to eventual successful revision. Typically, isolated polyethylene exchange is not effective or reliable to address instability. In many cases, component malrotation and ligament imbalance contribute to instability. Revision surgery focuses on restoration of the joint line, proper femoral and tibial component rotation, and restoration of the femur posterior condylar.
Component loosening and osteolysis are the common mechanisms of TKA failure. Prior to revision, concurrent infection must be ruled out as a source of failure. At the time of revision, proper fixation and rotation of the femoral and tibial components must be ensured. If the components are well fixed and rotated, successful isolated bearing exchange and bone grafting in the setting of osteolysis is possible. Isolated component exchanges also can be successfully performed, provided the remaining components are in an acceptable position. However, when in doubt, revision of both components generally yields more consistent results.
Stiffness following TKA can affect as many as 10% of patients following surgery. Depending on the timing and extent of arthrofibrosis, treatment options include manipulation under anesthesia or revision TKA. Manipulation typically is effective early during the postsurgical
course (for up to 4 months) and is most effective for loss of flexion. To address chronic stiffness and arthrofibrosis, revision TKA offers modest improvements in range of motion. Isolated polyethylene exchange has proven inconsistent in this setting, so revision of both components to ensure proper component rotation and joint line restoration offers the best chance to improve range of motion.
Extensor mechanism complications also can occur following TKA. Although the frequency is decreasing with improved component design and surgical techniques, periprosthetic patella fractures can occur. Treatment centers on the integrity of the extensor mechanism and fixation of the patellar component (if resurfaced). In general, if the extensor mechanism is intact, nonsurgical treatment is favored. Surgical treatment of periprosthetic patellar fractures following TKA has been associated with high complication rates and low healing rates.
Question 23
Figure 49 shows an acute axial MRI scan of a left knee. What is the most likely diagnosis?
Explanation
REFERENCES: Elias DA, White LM, Fithian DC: Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002;225:736-743.
Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 24
A 10-year-old girl is treated for a tibia/fibula fracture with a long leg cast. The on-call resident is called to evaluate the patient for increasing pain medicine requirements and tingling in her foot. Examination of the cast reveals that the ankle has been immobilized in 10 degrees of dorsiflexion. What ankle position results in the safest compartment pressures in a casted lower leg?

Explanation
Weiner et al measured intramuscular compartment pressure in the anterior and deep posterior compartments of the leg in seven healthy adults who had long leg casts placed. They found that in a casted leg the intramuscular pressure in the anterior compartment was lowest with the ankle in neutral, and the deep posterior compartments was lowest when the ankle joint was in the resting position to approximately 37 degrees of plantar flexion. Based on this, they concluded that the safest ankle casting position regarding compartment pressure is between 0 and 37 degrees of plantar flexion. After the cast was bivalved, they noted a significant decrease in intramuscular pressure of 47 per cent in the anterior compartment and of 33 per cent in the deep posterior compartment. Constrictive casts and abberant ankle positioning can exacerbate pain/symptoms. Loosening of the cast by bivalving, spreading, and cutting underlying stockinette/softroll should always be the first step in management of possible compartment syndrome.
Question 25
A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T2-weighted MRI scan is shown in Figure 13a, and a contrast enhanced T1-weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient’s symptoms? Review Topic
Explanation
pseudomeningocele is not present. A revision diskectomy is useful for recurrent radiculopathy but would not be helpful for degenerative low back pain.
(SBQ12SP.29) A 17-year-old female is undergoing posterior instrumented fusion from T5-T12 for adolescent idiopathic scoliosis. At the time of the correction maneuver, the neurophysiologist notifies you of a 60% decrease in somatosensory evoked potential (SSEP) amplitude throughout bilateral lower extremities. Which of the following is an acceptable approach to manage this finding? Review Topic
Immediate wake-up test with examination for clonus
Drop the mean arterial pressure (MAP) to ~60mmHg
Discontinue instrumentation and optimize MAP to 85mmHg or greater
Immediate infusion of intravenous corticosteroids
Modification of the anesthesia plan to include inhalational agents only followed by repeated SSEP testing
The patient has a significant drop in SSEP amplitudes at the completion of the corrective maneuver. The most appropriate response is to raise the MAP to 85 mmHg or greater, discontinue the instrumentation, re-evaluate the SSEPs, and if there is no improvement, to consider reversing the reduction of the deformity.
Intra-operative neurophysiologic monitoring is an effective method to monitor insults to the spinal cord and its exiting roots during spinal instrumentation. The common measurements include SSEPs, which monitor sensory potentials transmitted through the dorsal column system, and motor-evoked potentials (MEPs), which monitor motor response to a trans-cranial stimulus. Decreases in amplitude and latency of the circuits are recorded, however diminished signal amplitudes are more sensitive for neurologic injury, and decreases of of >50-60% being highly concerning. The wake-up test involves reversal of anesthesia so that an intra-operative neurologic examination can be performed.
Devlin et al. reviewed the basic science and practice of neurophysiologic monitoring in spine surgery. They proposed an algorithmic approach to managing intraoperative alerts which include discontinuation of inhalational anesthetics, increasing the MAP to >90 mmHg, discontinuing instrumentation, and performing a wake-up test if neurologic signals fail to normalize.
Herdmann et al. reviewed the practice of neurophysiologic monitoring and the effects of anesthesia upon signal transduction. They report that anesthesia affecting a neuron's intrinsic excitability can alter the results of monitoring. Inhalational anesthetics and decreased MAPs can be responsible for decreased amplitudes.
Vitale et. al. developed a consensus-based intraoperative checklist for management of lost neuromonitoring signals. In this checklist, the first steps across the surgical and anesthetic teams should include: stop the case and announce signal losses to the room, optimize the mean arterial pressure, discuss the status of anesthetic agents, and discuss reversible surgical actions just prior to signal loss.
Incorrect
Question 26
Figures 177a and 177b are the radiographs of a 7-year-old boy with spastic cerebral palsy. He has quadriparetic involvement and is unable to ambulate. He has very limited abduction, 30 degrees of flexion contractures, and pain on abduction. Bilateral varus osteotomies are scheduled with acetabular procedures to improve stability. Which type of acetabular osteotomy should be performed?
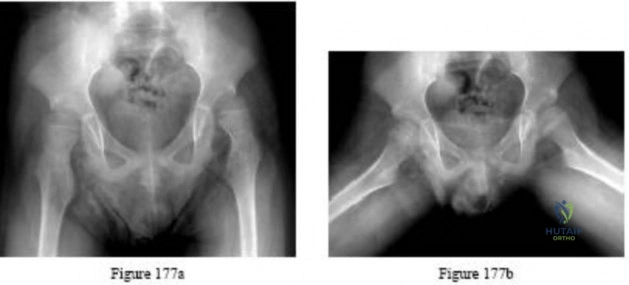
Explanation

Question 27
What structure provides the major blood supply to the humeral head?
Explanation
the major blood supply to the humeral head. The posterior circumflex humeral artery
supplies a much smaller portion of the proximal humerus. The nutrient humeral artery is the main blood supply for the humeral shaft. The thoracoacromial artery is primarily a muscular branch. The rotator cuff insertions contribute some blood supply to the tuberosities but not a major contribution.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Cushner MA, Friedman RJ: Osteonecrosis of the humeral head. J Am Acad Orthop Surg 1997;5:339-346.
Question 28
Anteromedial approach (Ludloff)
Explanation
The lateral femoral cutaneous nerve can be injured during a direct anterior approach to the hip. The superior gluteal nerve enters the gluteus medius from posterior to anterior approximately 5 cm above the greater trochanter. This nerve can be injured during the direct lateral and anterolateral approaches to the hip. Branches of the inferior gluteal nerve as well as the sciatic nerve can be injured during the posterior approach, and the obturator nerve can be damaged when performing a medial approach to the hip.

Question 29
Where is the watershed zone for tarsal navicular vascularity?
Explanation
REFERENCES: Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004,
pp 239-242.
Sarrafian SK: Anatomy of the Foot and Ankle. Philadelphia, PA, JB Lippincott, 1983,
pp 299-302.
Question 30
A right-handed 44-year-old construction worker reports pain and limited range of motion in his right elbow that has limited his ability to work for the past year. Examination reveals range of motion from 60 to 90 degrees, and he has pain at the extremes of flexion and extension. Pronation and supination are minimally restricted. Anti-inflammatory drugs have failed to provide relief. A radiograph is shown in Figure 8. Management should now consist of
Explanation
REFERENCES: Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: Long-term outcome and complications. J Bone Joint Surg Am 2002;84:2168-2173.
Phillips NJ, Ali A, Stanley D: Treatment of primary degenerative arthritis of the elbow by ulnohumeral arthroplasty: A long-term follow-up. J Bone Joint Surg Br 2003;85:347-350.
Question 31
The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports, and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation, patients who follow an early accelerated rehabilitation protocol experience
Explanation
The MR image shows bone bruises (“kissing contusions”) consistent with an ACL tear. During the ACL subluxation event, the posterolateral tibia plateau subluxes anteriorly, making contact with the mid portion of the lateral femoral condyle and resulting in this characteristic bone bruise pattern on MRI. Randomized clinical trials comparing early accelerated vs nonaccelerated rehabilitation programs have demonstrated no significant differences in longterm results with regard to function, reinjury, and successful return to play. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 32
Osteoporotic vertebral compression fractures are associated with Review Topic
Explanation
Question 33
A 72-year-old man sustains a displaced four-part fracture of the proximal humerus with head split component following a fall. A primary shoulder arthroplasty has been recommended for acute management. In counseling the patient on pros and cons of hemiarthroplasty versus reverse arthroplasty, what statement can be made based on the available literature?
Explanation
arthroplasty in the setting of fracture is that forward elevation is independent of tuberosity healing and relies mainly on the deltoid muscle. Active external rotation following a reverse total shoulder for fracture, however, does appear to depend on successful union of the greater tuberosity. In a randomized controlled trial, the incidence of tuberosity healing was higher and the incidence of tuberosity resorption was lower in reverse arthroplasty compared with hemiarthroplasty. Forward elevation following a hemiarthroplasty for fracture generally follows a bimodal distribution, whereas outcomes following a reverse total shoulder have been more
consistent.
Question 34
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
REFERENCES: Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 35
Which of the following deformities is most common after the amputation shown in Figure A?

Explanation
Ng et al. review foot and ankle amputations, and review the issues inherent with each amputation level, including prosthesis fitting and use. They also mention that careful repair of all released or transected tendons is needed to maintain a plantigrade foot.
Early reviews the importance of soft tissue balancing with midfoot amputations. They note that the attachment of the resected tendons into the more proximal retained bones is critical for success in restoration of foot position and ambulation capabilities.
Figure A shows a midfoot amputation as the result of trauma. Illustration A shows the lateral view of the amputation, with an obvious equinus deformity.
Incorrect Answers:
Question 36
A 57-year-old woman had right total knee arthroplasty for varus gonarthrosis. Before surgery, her range of motion was 5 to 110 degrees. At skin closure, her range of motion was 0 to 120 degrees. Her range of motion at 10 weeks after surgery is 0 to 70 degrees. What is the best next treatment step?
Explanation
is more expensive.
is more susceptible to fracture.
is associated with an elevated risk for polyethylene wear.
has an equivalent rate of aseptic loosening.
has higher failure rates when used in patients younger than age 70.
Question. 17 . When the liquid monomer (monomethacrylate) is added to polymer powder (polymethylmethacrylate),the activator in the liquid monomer (N,N-Dimethyl-p-toluidine) comes in contact with the initiator in the polymer powder and polymerization is initiated. What is the initiator?
Hylamer
Polystyrene
Barium sulfate
Benzoyl peroxide
Zirconium dioxide
Question.18 . Figure 197 is the radiograph of a 62-year-old woman who is seen in the emergency department with a dislocated left total hip arthroplasty. This is her seventh dislocation during the last 3 months and she most recently had a liner revision. What is the best next treatment step?
Skeletal traction
Open reduction
Closed reduction
Component revision
Hip abduction orthosis

Question 37
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management? L Intensive physiotherapy
Explanation
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Question 38
All of the following conditions are associated with the female athlete triad EXCEPT? Review Topic
Explanation
The female athlete triad is an interrelationship of menstrual dysfunction (i.e., amenorrhea or oligomenorrhea), low energy availability (insufficient caloric intake for demand, with or without an eating disorder) and decreased bone mineral density. It is relatively common among young women participating in sports. More recently, it has been suggested that endothelial dysfunction also results, due to an imbalance between vasodilating and vasoconstricting agents triggered from inappropirate levels of nitric oxide on the microscopic level, which predisposes these women to atherosclerotic changes and increases their risk of cardiovascular disease in the future.
Matheson et al. analyzed cases of 320 athletes with bone scan-positive stress fractures (M = 145, F = 175) seen over 3.5 years and assessed the results of conservative management. They found that conservative treatment of stress fractures in athletes is satisfactory in the majority of cases.
Constantini et al. evaluated the prevalence of vitamin D insufficiency and deficiency among young athletes and dancers. They found a higher rate of vitamin D insufficiency among participants who practice indoors, during the winter months, and in the presence of iron depletion.
Nazem et al. reviewed the major components and health consequences of the female athlete triad as well as strategies for diagnosis and treatment of the conditions. They concluded that treatment requires a multidisciplinary approach involving health care professionals as well as coaches and family members.
Yagi et al. followed 230 runners participating in high school running teams for a total of 3 years to report occurrence of medial tibial stress syndrome (MTSS) and stress fracture. Predictors of MTSS and stress fracture were investigated. The authors reported a significant relationship between BMI, internal hip rotation angle and MTSS infemales.
Incorrect Answers:
Question 39
A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
Explanation
REFERENCES: Luhmann SJ, Gordon JE, Schoenecker PL: Intramedullary fixation of unstable both-bone forearm fractures in children. J Pediatr Orthop 1998;18:451-456.
Mehlman CT, Wall EJ: Injuries to the shafts of the radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 430-436.
Question 40
Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to
Explanation
REFERENCES: Kayanja MM, Ferrara LA, Lieberman IH: Distribution of anterior cortical shear strain after a thoracic wedge compression fracture. Spine J 2004;4:76-87.
Kayanja MM, Togawa D, Lieberman IH: Biomechanical changes after the augmentation of experimental osteoporotic vertebral compression fractures in the cadaveric thoracic spine. Spine J 2005;5:55-63.
Kayanja MM, Schlenk R, Togawa D, et al: The biomechanics of 1, 2, and 3 levels of vertebral augmentation with polymethylmethacrylate in multilevel spinal segments. Spine 2006;31:769-774.
Kayanja M, Evans K, Milks R, et al: The mechanics of polymethylmethacrylate augmentation. Clin Orthop Relat Res 2006;443:124-130.
Question 41
Which of the following statements best describes the typical early presentation of osteochondritis dissecans of the elbow? Review Topic
Explanation
Question 42
A 29-year-old quarterback falls onto his dominant shoulder and sustains the injury shown in Figures 14a and 14b. Management should consist of
Explanation
REFERENCES: Lemos MJ: The evaluation and treatment of the injured acromioclavicular joint in athletes. Am J Sports Med 1998;26:137-144.
Rockwood CA Jr, Green DP, Bucholz RW, et al: Fractures in Adults, ed 5. Philadelphia, PA, Lippincott-Raven, 2001, pp 1209-1240.
Question 43
On an axial CT image, which of the following dimensions is considered to be indicative of a critical amount of lumbar spinal stenosis? Review Topic
Explanation
Question 44
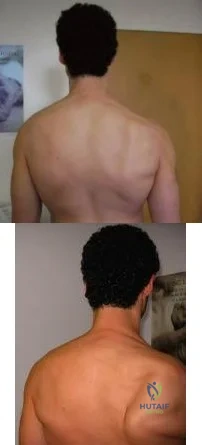
A 49-year-old male presents with right shoulder pain and weakness after undergoing open cervical lymph node biopsy approximately one year ago. A pertinent finding from the physical exam is seen in Figure A, with the patients arms by his side. Physical exam finding with the arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation are shown in Figure B. What nerve is most likely injured? Review Topic
Explanation
The spinal accessory nerve is fundamental to scapulothoracic function and essential for scapulohumeral rhythm. This nerve is vulnerable along its superficial course. The majority of injuries to the spinal accessory nerve are iatrogenic and occur secondary to head and neck surgery. There is often a marked delay in recognition and initiating treatment. Surgical treatment with the Eden-Lange transfer lateralizes the levator scapulae and rhomboids (transfer from medial border to lateral border)
Camp et al. reviewed the results of 111 patients who underwent operative management of a lesion to the spinal accessory nerve. They found that the majority (~80%) of injuries were sustained iatrogenically and that diagnosis was delayed for approximately 12 months.
Pikkarainen et al. reviewed the natural history of isolated serratus palsy. They found that symptoms mostly recover in 2 years, but at least one-fourth of the patients will have long-lasting symptoms, especially pain.
Figure A depicts a patient with lateral scapular winging. Figure B demonstrates physical exam of this patient with their arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation. Illustration A highlights the difference between medial and lateral scapular winging. Illustration B depicts another example of a patient with lateral scapular winging.
Incorrect Answers:
An injury to the long thoracic nerve would result in serratus anterior palsy which would lead to MEDIAL scapular winging.
An injury to the suprascapular nerve would result in weakness and wasting of the supraspinatus and/or infraspinatus.
An injury to the axillary nerve would result in deltoid muscle weakness.
An injury to the thoracodorsal nerve would result in latissimus dorsi weakness and would not cause scapular winging
Question 45
In a patient with a major head injury and a femoral shaft fracture, intraoperative hypotension during femoral fixation has been associated with which of the following?

Explanation
Question 46
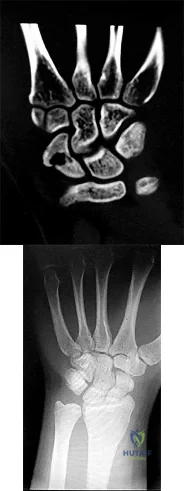
Figures 1 and 2 are the radiographs of a 17-year-old man who injured his wrist 6 months ago. He is experiencing pain and limited motion. What is the most effective treatment option?
Explanation
Figures 1 and 2 show a scaphoid nonunion with substantial bone resorption at the nonunion site. Cast immobilization and bracing with bone stimulator use would not be successful treatments at this point because the fracture is 6 months old and there is considerable bone resorption at the fracture site. Scaphoid excision with intercarpal fusion is an option to use only after bone-grafting procedures have failed or arthritis is present. Bone-grafting procedures using both vascularized and nonvascularized graft sources are associated with a high success rate that decreases with avascular necrosis of the proximal pole. If left untreated, scaphoid nonunions can progress to carpal collapse and degenerative arthritis.
Question 47
If the site of the pathologic lesion is revealed in Figure 54f and not in Figure 54e after traumatic anterior shoulder dislocation, the mechanism of shoulder injury is likely
Explanation
For patients with anterior shoulder instability, most commonly, a Bankart lesion, or detachment of the anteroinferior labrum with the attached inferior glenohumeral ligament from the glenoid rim is found. A medialized anteroinferior capsulolabral attachment (ALPSA lesion) is a common finding in shoulders with chronic anterior instability. The anterior band of the inferior glenohumeral ligament is tightest with the arm in 90 degrees of abduction with the shoulder externally rotated, creating a “hammock” that supports the humeral head. At 45 degrees of shoulder
abduction, the capsuloligamentous components of the shoulder are at their loosest, resulting in the most total superior-inferior translation.
During traumatic anterior glenohumeral dislocation, associated injuries commonly occur. In a prospective database of 3633 patients who sustained a traumatic anterior glenohumeral dislocation, 13.5% had a neurologic deficit following reduction, the majority of which were injuries to the axillary nerve. The injuries typically were sensory but not motor deficits and resolved spontaneously over time. These isolated axillary nerve injuries were more common in young, athletic patients. Associated rotator cuff tears and greater tuberosity fractures are commonly associated with shoulder dislocation as well and are more common in patients 60 years of age and older.
Large, engaging posterior humeral head Hill-Sachs lesions are associated with increased rates of recurrent shoulder instability. At the time of surgical arthroscopy, the Hill-Sachs lesion should be assessed for engagement with the glenoid. In the absence of significant glenoid bone loss, some patients with engaging Hill-Sachs defects may be suitable for combined Bankart repair and Hill-Sachs remplissage at the time of surgery. When these procedures are combined, patients have an approximate 10-degree decreased shoulder external rotation with the arm at the side and in abduction when compared to the contralateral, uninjured shoulder. Rates of recurrent dislocation and return to sport are comparable to those for patients undergoing Bankart repair alone.
Humeral avulsion of the glenohumeral ligaments (HAGL) has become a well-recognized cause of recurrent shoulder instability and is reported in 1% to 9% of patients. HAGL lesions can occur in isolation or, more commonly, may be associated with other abnormalities such as a tear of the rotator cuff, Bankart lesion, Hill-Sachs deformity, or labral tear. Recurrence of shoulder instability is more likely to occur if there is failure to identify a HAGL lesion. HAGL lesions can result from trauma in the setting of combined hyperabduction and external rotation. This is in contrast to a Bankart lesion, which is a result of trauma when the shoulder is hyperabducted without substantial associated rotation.
RECOMMENDED READINGS
Warner JJ, Deng XH, Warren RF, Torzilli PA. Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med. 1992 Nov-Dec;20(6):675-85. PubMed PMID: 1456361. View Abstract at PubMed
Robinson CM, Shur N, Sharpe T, Ray A, Murray IR. Injuries associated with traumatic anterior glenohumeral dislocations. J Bone Joint Surg Am. 2012 Jan 4;94(1):18-26. doi: 10.2106/JBJS.J.01795. PubMed PMID: 22218378. View Abstract at PubMed
Visser CP, Coene LN, Brand R, Tavy DL. The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery. A prospective clinical and EMG study. J Bone Joint Surg Br. 1999 Jul;81(4):679-85. PubMed PMID: 10463745. View Abstract at PubMed
Boileau P, O'Shea K, Vargas P, Pinedo M, Old J, Zumstein M. Anatomical and functional results after arthroscopic Hill-Sachs remplissage. J Bone Joint Surg Am. 2012 Apr 4;94(7):618-26. doi: 10.2106/JBJS.K.00101. PubMed PMID: 22488618. View Abstract at PubMed
Bui-Mansfield LT, Banks KP, Taylor DC. Humeral avulsion of the glenohumeral ligaments: the HAGL lesion. Am J Sports Med. 2007 Nov;35(11):1960-6. Epub 2007 Apr 9. Review. PubMed PMID: 17420506. View Abstract at PubMed
Question 48
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
Explanation
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
Question 49
Figure 30 shows the radiograph of a 38-year-old man who reports persistent pain laterally and plantarly about the fifth metatarsal head. Examination reveals calluses dorsolaterally and plantarly about the fifth metatarsal head. Nonsurgical management has failed to provide relief. Surgical treatment should include
Explanation
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Moran MM, Claridge RJ: Chevron osteotomy for bunionette. Foot Ankle Int 1994;15:684-688.
Question 50
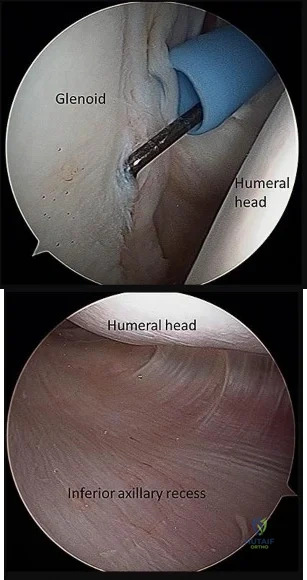
Figure 28 shows an arthroscopic view of a right shoulder in the lateral position through a posterior portal. What is the area between structure B (biceps) and SS (subscapularis tendon)? Review Topic
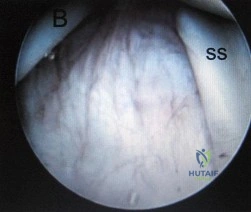
Explanation
Question 51
Tendons should have what ratio of matrix protein?
Explanation
Question 52
A 48-year-old woman reports bilateral thigh pain that is limiting her function as a librarian. A radiograph and a bone scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA,
WB Saunders, 1995, pp 956-957.
Wheeless’ Textbook of Orthopaedics: Acetabular Protrusio. www.wheelessonline.com/ortho/acetabular_protrusio
Question 53
A 3-year-old girl has had pain and swelling in her left thigh for the past 3 weeks. Her mother states she has had a temperature as high as 100.4 degrees F (38 degrees C) and a weight loss of 5 pounds. A CBC shows a WBC count of 11,000/mm3, an erythrocyte sedimentation rate of 13 mm/h, and a C-reactive protein of 0.3. A radiograph is shown in Figure 2. What is the next step in management?
Explanation
REFERENCES: Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Meyer JS, Nadel HR, Marina N, et al: Imaging guidelines for children with Ewing sarcoma and osteosarcoma: A report from the Children’s Oncology Group Bone Tumor Committee. Pediatr Blood Cancer 2008;51:163-170.
T
AL-Madena Copy
Question 54
Which of the following surgical options after resection of a sarcoma about the knee would require a patient to expend the greatest amount of energy while walking?
Explanation
Question 55
When conducted at near physiologic strain rates, tensile studies of the inferior glenohumeral ligament (IGHL) have shown that the
Explanation
REFERENCES: Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Ticker JB, Bigliani LU, Soslowsky LJ, Pawluk RJ, Flatow EL, Mow VC: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Question 56
A patient with an unstable pelvic ring injury has just undergone an emergent laparotomy and currently has a packed abdomen. Stabilization of the pelvic ring is performed with an anterior external fixator. What is an advantage of using an external fixator with pins in the iliac crest rather than pins in the anterior inferior iliac spine?
Explanation
Question 57
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?
Explanation
REFERENCES: Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 58
Which of the following methods best aids in diagnosis of an interdigital neuroma?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 145-147.
Bennett GL, Graham CE, Mauldin DM: Morton’s interdigital neuroma: A comprehensive treatment protocol. Foot Ankle Int 1995;16:760-763.
Question 59
An 11-year-old girl has had pain in the medial arch of her foot for the past 3 months. She reports that pain is present even with daily activities such as walking to class at school, and ibuprofen provides some relief. She denies any history of trauma. Examination reveals a flexible pes planus with focal tenderness over a prominent tarsal navicular tuberosity. Radiographs show a prominent accessory navicular. Management should consist of
Explanation
REFERENCE: Bordelon RL: Flatfoot in children and young adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 717-756.
Question 60
Which statement is true with respect to acetabular fracture surgery as the time between injury and surgery increases?

Explanation
Question 61
Figures 1 and 2 are the radiographs of a 24-year-old male wrestler who underwent surgery for recurrent shoulder dislocations using coracoid autograft. At his first postoperative visit, the patient complains of decreased sensation on the lateral aspect of his forearm. The patient’s symptoms are most likely due to injury of the
Explanation
Question 62
Which of the following methods of treating a vertically oriented (eg, Pauwels III) femoral neck fracture is mechanically optimal?
Explanation
(SBQ12TR.68) Figure A is a radiograph of a 75-year-old woman that fell onto her non-dominant shoulder from a standing height. She was treated non-operatively for 9 months but continues to complain of pain when she elevates her arm. In patients with this type of fracture pattern, what factor has the greatest impact on fracture healing?

Hand dominance
Angulation of fracture
Smoking
Early physical therapy
Diet
This patient has an impacted varus proximal humerus fracture. Smoking has been shown to increase the nonunion risk up to 5.5 times with these fractures.
Impacted varus proximal humerus fractures can be managed effectively with nonoperative care. The major factors that influence non-union are age and smoking. Solid bony union can be seen in 93-98% of patients at 1 year, with more than 97% of people returning to pre-injury level of function. The angulation of fracture, hand dominance and physical therapy does not seem to influence bone union or functional outcomes with this fracture pattern.
Court-Brown et al. looked at the outcomes of impacted varus fractures. They determined that the age of the patient was the major factor in overall outcome. They showed that the best results occurred in younger patients, but results deteriorate with advancing age. Physical therapy was not found to impact outcome.
Hanson et al. showed that impacted varus fractures can be successfully managed with non-operative care. They found that overall fracture displacement had a minor impact of fracture healing and functional outcome. The predicted risk of delayed union and nonunion was 7% with patients that smoke. This was 5.5 times greater than nonsmokers.
Figure A shows an AP radiograph of a varus angulated proximal humerus fracture. This radiograph shows delayed atrophic union.
Incorrect Answers:
Question 63
The specificity of intraoperative frozen sections obtained for the evaluation of infected total hip arthroplasty may be improved by
Explanation
On the basis of cultures of specimens obtained at the time of the revision surgery, 19 of the 175 patients were considered to have an infection. Of the 152 patients who had negative frozen sections, three were considered to have an infection on the basis of the results of the final cultures. Of the 23 patients who had positive frozen sections, 16 were considered to have an infection on the basis of the results of the final cultures; all 16 had frozen sections that showed at least 10 polymorphonuclear leukocytes per high-powered field.
The sensitivity and specificity of the frozen sections were similar regardless of whether an index of 5 or 10 polymorphonuclear leukocytes per high-powered field was used. Analysis of the frozen sections had a sensitivity of 84% for both indices, whereas the specificity was 96% when the index was 5 polymorphonuclear leukocytes and 99% when it was 10 polymorphonuclear leukocytes. However, the positive predictive value of the frozen sections increased significantly (P < 0.05), from 70% to 89%, when the index increased from 5 to 10 polymorphonuclear leukocytes per high-powered field. The negative predictive value of the frozen sections was 98% for both indices. At least 10 polymorphonuclear leukocytes per high-powered field was predictive of infection, while 5 to 9 polymorphonuclear leukocytes per high-powered field was not necessarily consistent with infection. Less than 5 polymorphonuclear leukocytes per high-powered field reliably indicated the absence of infection.
REFERENCES: Feldman DS, Lonner JH, Desai P, Zuckerman JD: The role of intraoperative frozen sections in revision total joint arthroplasty. J Bone Joint Surg Am 1995;77:1807-1813.
Lonner JH, Desai P, Dicesare PE, Steiner G, Zuckerman JD: The reliability of analysis of intraoperative frozen sections for identifying active infection during revision hip or knee arthroplasty. J Bone Joint Surg Am 1996;78:1553-1558.
Spangehl MJ, Younger AS, Masri BA, Duncan CP: Diagnosis of infection following total hip arthroplasty, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 285-295.
Della Valle CJ, Bogner E, Desai P: Analysis of frozen sections of intraoperative specimens obtained at the time of reoperation after hip or knee resection arthroplasty for the treatment of infection. J Bone Joint Surg Am 1999;81:684-689.
Question 64
- A 40-year-old woman has had pain in the metatarsophal joint of the second toe for the past 6 months despite nonsurgical treatment. A dorsalplantar stress test reproduces the pain, and there is 10 mm of dorsal subluxation of the toe. Radiographs show a normal second metatarsophalangeal joint. Surgical treatment should consist of synovectomy and
Explanation
Question 65
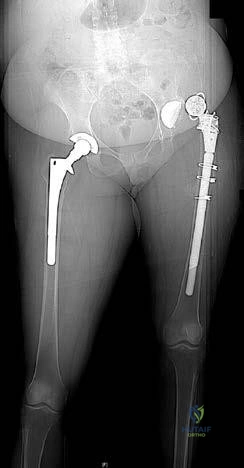
A 53-year-old man with a history of severe left hip pain has a significant limp that is the result of a 5-cm limb-length discrepancy. An AP radiograph is shown in Figure 48. The underlying etiology is most likely related to a history of
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 3-23.
Question 66
An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis? Review Topic

Explanation
Question 67
Physiologic bowing of the lower extremities should spontaneously correct by what age?
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 7.
Salenius P, Vankka E: The development of the tibiofemoral angle in children. J Bone Joint Surg Am
J V :
Question 68
The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?
Explanation
REFERENCES: McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Lister GD, McGregor IA Jackson IT: The groin flap in hand injuries. Injury 1973;4:229.
Question 69
A 47-year-old man with Charcot-Marie-Tooth (CMT) disease was treated with a fifth metatarsal head resection for a symptomatic bunionette 2 years ago. What is the most likely complication seen at this time?
Explanation
REFERENCES: Kitaoka HB, Holiday AD Jr: Metatarsal head resection for bunionette: Long-term followup. Foot Ankle 1991;11:345-349.
Coughlin MJ, Mann RA, Saltzman CL: Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 1312-1315.
Question 70
A Spanish speaking child sustained the injury seen in Figure A after a fall at school. He was casted in the emergency department without the assistance of an interpreter and advised to return to see an orthopaedic surgeon in 1 week. However, the family returns to the emergency department with the child 3 months later, still in the cast. What is the most likely reason the child did not attend the recommended orthopaedic follow-up visit.?

Explanation
Communication skills and cultural competence is a key element in good orthopaedic care. Poor communication can often lead to devastating outcomes. In this example, poor communication resulted in this patient being lost to follow-up. Language barriers must be accommodated and alternative methods of communication must be utilized.
Levinson et al. examined how patients present their medical issues in clinical encounters and how physicians respond to these clues in routine primary care and surgical settings. They showed that good communication relies mostly on the physicians ability to identify patient clues within the clinical encounter. Poor communication between the physician tended to delay clinical visits, poor follow-up and unsatisfactory outcomes.
Figure A is an AP radiograph of the elbow in a skeletally immature patient. Figure B is a lateral radiograph of the elbow with a posterior fat pad sign, suggestive of an occult fracture.
Incorrect Answers:
Question 71
A 15-year-old girl reports a 6-month history of activity-related knee pain and swelling. A radiograph, MRI scan, and biopsy specimen are shown in Figures 21a through 21c. What is the most likely diagnosis?
Explanation
REFERENCES: Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 295-313.
Lin PP, Thenappan A, Deavers MT, et al: Treatment and prognosis of chondroblastoma. Clin Orthop Relat Res 2005;438:103-109.
Question 72
Figure A shows immediate post-operative radiographs of a 75-year-old patient with primary osteoarthritis. She presents 3 years later with increasing pain and weakness in the shoulder despite home physical therapy. Examination reveals limited active range of motion, with forward elevation of 80 degrees and external rotation of 50 degrees. Her deltoid function is intact. Repeat radiographs are seen in Figure B.

Explanation
RTSA is considered a viable treatment option for patients with failed shoulder arthroplasty. It allows for improved arm elevation and abduction in the setting of nonfunctional rotator cuff muscles, as seen in this example. Despite the expanding indications for rTSA, there are high complication rates in the revision setting. Complication rates for rTSA after failed shoulder arthroplasty have been reported to be between 11-36%. This procedure should, therefore, be performed by surgeons with extensive training in reconstructive shoulder arthroplasty.
Patel et al. retrospectively reviewed 31 patients (mean age, 68.7 years) who underwent rTSA for treatment of a failed shoulder arthroplasty. They found the greatest improvement with active forward elevation from 44° preoperatively to 108° postoperatively (P < .001). Complications occurred in 3 patients with periprosthetic fracture.
Hattrup et al. reviewed a series of 19 patients that underwent open rotator cuff repair after shoulder arthroplasty. Out of the 19 patients only 4 shoulders were successfully repaired. They concluded that successful rotator cuff repair after shoulder arthroplasty is possible but failure is more common.
Figure A shows a left total shoulder arthroplasty that is well reduced in the glenoid. Figure B shows antero-superior escape of the prosthesis, indicative of a massive rotator cuff tear.
Incorrect Answers:
Question 73
Figures 27a and 27b show the radiographs of a 32-year-old woman who was involved in a high-speed motor vehicle accident. She is neurologically intact. After stabilization and assessment, treatment should consist of
Explanation
REFERENCES: Lewandrowski KU, McLain RF: Thoracolumbar fractures: Evaluation, classification, and treatment, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 817-843.
Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Question 74
During establishment of an anterior portal for hip arthroscopy, what structure is at greatest risk for injury? Review Topic
Explanation
Question 75
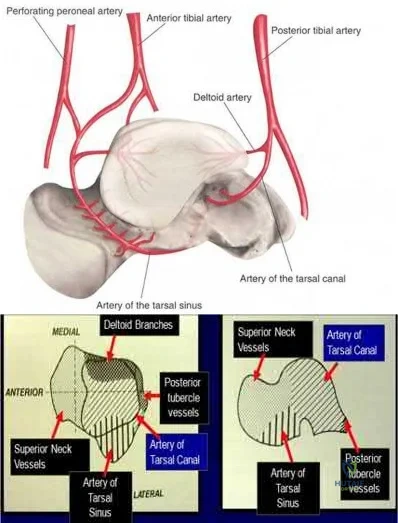
A 29-year-old male sustains the isolated lower extremity injury shown in Figure A. During open reduction, what structure must be kept intact in order to protect the remaining blood supply to the talar body?

Explanation
The review article by Fortin et al discusses talar blood supply, injury mechanisms and classifications, and treatment options. They state that the main artery to the body of the talus is the artery of the tarsal canal, which is a branch of the posterior tibial artery. The peroneal and anterior tibial artery also contribute branches to the talus.
Illustration A and B show the arterial network of the talus.
OrthoCash 2020
Question 76
An otherwise healthy 32-year-old man who underwent an uneventful L5-S1 lumbar microdiskectomy 6 weeks ago now reports increasing and severe back pain that awakens him from sleep. Examination reveals a benign-appearing wound, and the neurologic examination is normal. Laboratory studies show an erythrocyte sedimentation rate (ESR) of 90 mm/h and a WBC of 9,000/mm3. Plain radiographs are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 77
All of the following have been shown to negatively affect clinical outcomes in treating displaced acetabular fractures, EXCEPT:

Explanation
The referenced study by Matta evaluated outcomes of displaced acetabular fractures. The overall clinical result was excellent for 104 hips (40 per cent), good for ninety-five (36 per cent), fair for twenty-one (8 per cent), and poor for forty-two (16 per cent). The clinical result was related closely to the radiographic result. These findings indicate that in many patients who have a complex acetabular fracture the hip joint can be preserved and post-traumatic osteoarthrosis can be avoided if an anatomical reduction is achieved.
Question 78
There is a risk of impaired forearm rotation after tension band fixation of an olecranon fracture with which of the following?

Explanation
The referenced study by Candal-Couto et al is a cadaveric study that found that K-wire insertion in less than 30 degrees in an ulnar direction led to impingement of the K-wire on the radial head/neck, biceps or supinator. They recommend placing these wires away from this danger zone in order to minimize rotation blocks.
The referenced study by Matthews et al is a case series of two patients who had limited forearm rotation after K-wire fixation. The etiology of limited rotation was found to be from direct overpenetration of the K-wire, which led to a mechanical block.
Question 79
03 A 28-year-old man who sustained the injury shown in Figure 31 is hemodynamically unstable. In addition to fluid resuscitation, the next most appropriate step in management should include
Explanation
Cook RE, Keating JF, Gillespie I: The role of angiography in the management of haemorrhage from major fractures of the pelvis. J Bone Joint Surg Br 2002;84:178-182.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp395-405.
back to this question next question
Question 80
An otherwise healthy 31-year-old man has had right knee pain for the past 9 months. His former physician administered a cortisone injection and ordered 6 months of physical therapy. The patient later had an arthroscopy with debridement of the right knee by another physician and completed another course of physical therapy. The patient received minimal relief from these treatments and still is not able to walk longer distances or go on hikes. On examination, he is a healthy appearing male with a body mass index of 24 kg/m 2 . He has a small effusion, minimal quadriceps atrophy, no tenderness about the knee, full range of motion, stable to varus and valgus stress at 30° of flexion, a grade 1 Lachman test, and a normal posterior drawer. Figures 1 through 4 are his arthroscopic views, radiograph and MRI scan from his prior surgical procedure. What is the next most appropriate step in treatment?

Explanation
Question 81
Which of the following is most frequently associated with heterotopic ossification about the shoulder?
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 291.
Neer CS: Displaced proximal humerus fractures: Part II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
Question 82
Figure 30 shows the MRI scan of a 68-year-old woman who has left hip pain. What is the most appropriate treatment?
Explanation
REFERENCES: Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 213-223.
Watson RM, Roach NA, Dalinka MK: Avascular necrosis and bone marrow edema syndrome. Radiol Clin North Am 2004;42:207-219.
Question 83
The superior glenohumeral ligament primarily restrains
Explanation
REFERENCES: Warner JJ, Deng XH, Warren RF, et al: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy Orthopaedic Surgeons, 1994, pp 165-177.
Question 84
Spindled cells that are surrounded in mature osteoid that connect to other similar cells via canaliculi are best described as which of the following? Review Topic
Explanation
Question 85
An 8-year-old girl injures her elbow playing soccer. After attempted reduction in the emergency department, radiographs of the elbow are shown in Figures 35a through 35c. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Hashemi-Nejad A, Goddard NJ: Radial head fractures. Br J Hosp Med 1994;51:223-226.
Rodriguez Merchan EC: Displaced fractures of the head and neck of the radius in children: Open reduction and temporary transarticular internal fixation. Orthopedics 1991;14:697-700.
Question 86
In overhead athletic activities, the kinetic chain generates what percentage of force from the leg and trunk segments of the chain?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 47.
McClure PW, Michener LA, Sennett BJ, et al: Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg 2001;10:269-277.
Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 2003;19:641-661.
Question 87
-What is the most likely area of injury?
Explanation
This patient likely has a physeal injury to the distal femoral physis. Stress radiographs or an MRI scan will most reliably reveal this diagnosis. The growth plate, when injured, is most commonly fractured through the hypertrophic zone of cartilage, its weakest point. This patient is optimally treated in a cylindrical or long-leg cast. Younger patients can be treated with a hip spica with a leg extension.
Question 88
A 10-year-old boy with severe hemophilia A (factor VIII) sustained an injury to his right forearm 2 hours ago when a classmate fell on his arm during a scuffle. Examination reveals moderate swelling in the forearm, decreased sensation in the distribution of the median and ulnar nerves, and pain on passive extension of the fingers. What is the most appropriate sequence of treatment?
Explanation
REFERENCES: Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 345-391.
Greene WB, McMillan CW: Nonsurgical management of hemophilic arthropathy, in Barr JS (ed): Instructional Course Lectures 38. Park Ridge, Ill, American Academy of Orthopaedic Surgeons, 1989, pp 367-381.
Naranja RJ Jr, Chan PS, High K, Esterhai JL Jr, Heppenstall RB: Treatment considerations in patients with compartment syndrome and an inherited bleeding disorder. Orthopedics 1997;20:706-711.
Question 89
A 58-year-old man has anterior knee pain after undergoing total knee arthroplasty for osteoarthritis 2 years ago. He denies any history of trauma. A Merchant view is shown in Figure 20. What is the most likely cause of his pain?
Explanation
REFERENCES: Reuben JD, McDonald CL, Woodard PL, Hennington LJ: Effect of patella thickness on patella strain following total knee arthroplasty. J Arthroplasty 1991;6:251-258.
Hsu HC, Luo ZP, Rand JA, An KN: Influence of patellar thickness on patellar tracking and patellofemoral contact characteristics after total knee arthroplasty. J Arthroplasty 1996;11:69-80.
Greenfield MA, Insall JN, Case GC, Kelly MA: Instrumentation of the patellar osteotomy in total knee arthroplasty: The relationship of patellar thickness and lateral retinacular release. Am J Knee Surg 1996;9:129-131.
Question 90
A 46-year-old male construction worker has right hip pain that has failed to respond to nonsurgical management. His body mass index (BMI) is 32, he is 6’2” tall, and he has no other medical comorbidities. AP and lateral radiographs of the right hip are shown in Figures 23a and 23b. The patient inquires about his suitability for metal-on-metal hip resurfacing. The patient should be educated that he is at higher risk for failure secondary to which of the following?
Explanation
The results of hip resurfacing arthroplasty have been reported to be best in young, male patients who are younger than 55 years of age with a diagnosis of osteoarthritis. Although some authors advocate metal- on-metal hip resurfacing as an option for patients with osteonecrosis of the femoral head, in this particular patient, given the size of the necrotic segment, he would be at higher risk for failure and a conventional total hip arthroplasty would be a more conservative option. As the acetabulum is resurfaced in metal- on-metal hip resurfacing, the secondary changes of the acetabulum are not an issue and his BMI is in an acceptable range for the procedure.
REFERENCES: Mont MA, Ragland PS, Etienne G, et al: Hip resurfacing arthroplasty. J Am Acad Orthop Surg 2006;14:454-463.
Revell MP, McBryde CW, Bhatnagar S, et al: Metal-on-metal hip resurfacing in osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88:98-103.
Buergi ML, Walter WL: Hip resurfacing arthroplasty: The Australian experience. J Arthroplasty 2007;22:61-65. Question 24
A 31-year-old woman had disabling right knee pain. An arthroscopic assessment reveals chondromalacia of both the lateral femoral condyle and tibial plateau. The standing femorotibial axis measures 10 degrees of valgus. The
optimum treatment of this condition should include
distal femoral varus osteotomy.
osteoarticular transplant to the lateral femoral condyle.
unicondylar arthroplasty.
high tibial osteotomy.
Fulkerson tibial tubercle transfer. PREFERRED RESPONSE: 1
DISCUSSION: The long-term outcome of a distal femoral varus osteotomy has been quite favorable and should remain the primary choice for this young active woman. Sharma and associates have shown that a 5-degree valgus malalignment has a five-fold chance of progressing at least one grade within 18 months, making a corrective osteotomy the most important surgical maneuver.
REFERENCES: Sharma L, Song J, Felson DT, et al: The role of knee alignment in disease progression and function decline in knee osteoarthritis. JAMA 2001 ;286:188-195.
Murray PB, Rand JA: Symptomatic valgus knee: The surgical options. J Am Acad Orthop Surg 1993; 1:19.
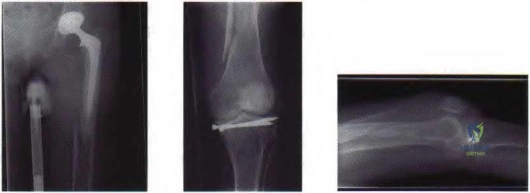
Figure 25a Figure 25b Figure 25c
Question 91
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
REFERENCES: Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Warner JJ, Deng XH, Warren RF, Torzilli PA: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Question 92
A 45-year-old female returns to your clinic with 10-weeks of severe pain that starts in her back and extends down her right leg to the top of her foot. On physical exam she has decreased sensation on the dorsal aspect of her foot and 4/5 strength in her EHL. She has a positive straight leg raise on the right. The remaining physical exam is unremarkable, including normal achilles and patellar reflexes bilaterally, no clonus, and a down-going Babinski sign. Her pain has not been relieved by NSAIDs, epidural steroids or physical therapy. Figure A is a sagittal MRI and figure B is a axial MRI through the L4/5 disc space. What is the best treatment option at this time? Review Topic

Explanation
Patients with paracentral herniated lumbar discs present with radicular pain affecting the traversing (caudal) nerve root. Unless the patient develops progressive neurologic decline, patients with herniated lumbar discs should undergo no less than 6 weeks of conservative treatment consisting of anti-inflammatory medications, rest and therapy. Most patients improve with nonoperative modalities. If appropriate conservative care fails, the correct surgical option is a unilateral microdiscectomy.
In the Spine Patient Outcomes Research Trial (SPORT) Weinstein et al. reported on the results of 501 patients with herniated lumbar discs who had failed at least six weeks of non-operative care. The patients were randomized to operative or nonoperative care, however there was a high amount of crossover between the two groups. Because of this, there was no difference reported between the two groups at final follow-up using an intent-to-treat analysis.
Weinstein et al., because of the flaws with the intent-to-treat analysis, also published an observational study on 528 patients who received surgery and 191 who received nonoperative care for a herniated lumbar disc. They reported that while both groups had an improvement from baseline, at two years, patients who elected to undergo surgery had significantly better outcomes than those who chose conservative care.
Lurie et al. reported the eight-year results from the observational group of the SPORT data, and found that the patients who underwent surgery continued to have statistically superior outcomes compared to those who underwent conservative care at long-term follow-up.
Figure A is a T2 sagittal MRI of the lumbar spine demonstrating a right sided L4/5 disc herniation, and Figure B is an axial image again demonstrating a paracentral L4/5 disc herniation.
Incorrect answers:
Question 93
Figure 9 shows the radiograph of a 75-year-old woman who reports the sudden onset of disabling medial knee pain. What is the most likely diagnosis?
Explanation
REFERENCES: Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-418.
Insall JN, Windsor RE, Scott WN, Kelly MA, Aglietti P (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 609-634.
Question 94
The radiograph shown in Figure 27 shows measurement of what angle?
Explanation
REFERENCES: Coughlin MJ: Juvenile hallux valgus: Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Steel MW III, Johnson KA, DeWitz MA, et al: Radiographic measurements of the normal foot. Foot Ankle 1980;1:151-158.
Richardson EG, Graves SC, McClure JT, et al: First metatarsal head-shaft angle: A method of determination. Foot Ankle 1993;14:181-185.
Question 95
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?
Explanation
REFERENCES: Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.
Question 96
When comparing surgical and nonsurgical extremities in patients who underwent anterior cruciate ligament (ACL) reconstruction using patellar tendon or hamstrings autografts, isokinetic strength measurements obtained 6 months after the surgery would most likely reveal
Explanation
REFERENCES: Carter TR, Edinger S: Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 1999;15:169-172
Howell SM, Taylor MA: Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am 1996;78:814-825.
Shelbourne KD, Nitz P: Accelerated rehabilitation after anterior cruciate ligament reconstruction. Am J Sports Med 1990;18:292-299.
Question 97
When performing a Kocher approach to the radial head for open reduction internal fixation the forearm is held in pronation. What structure is this maneuver attempting to protect?

Explanation
Question 98
A 26-year-old man with chronic lateral ankle instability underwent a modified Broström procedure 8 months ago. He reports persistent pain and swelling of the lateral ankle. Examination reveals lateral ankle tenderness and swelling and a negative anterior drawer test. Laboratory studies show a WBC count of 6,500/mm 3 and an erythrocyte sedimentation rate of 15 mm/h. Radiographs of the ankle are normal. What is the most likely cause of this problem?
Explanation
REFERENCES: Bonnin M, Tavernier T, Bouysset M: Split lesions of the peroneus brevis tendon in chronic ankle laxity. Am J Sports Med 1997;25:699-703.
Sobel M, Geppert MJ, Warren RF: Chronic ankle instability as a cause of peroneal tendon injury. Clin Orthop Relat Res 1993;296:187-191.
Question 99
- Posterior cruciate insufficiency diagnosed using the quadriceps active test is confirmed with tibial translation
Explanation
Question 100
A 36-year-old skier sustains a grade III posterior cruciate ligament (PCL) tear. Where will increased contact pressures develop over time?
Explanation
REFERENCE: Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 767.
