Orthopedic Surgery Board Review MCQs: Spine, Trauma, & Foot & Ankle Part 215
Key Takeaway
This page presents Part 215 of a comprehensive OITE and AAOS Orthopedic Surgery Board Review quiz. Designed for orthopedic residents and surgeons, it features 100 high-yield, verified MCQs mirroring the official exam format. Ideal for rigorous board certification preparation, including detailed explanations for optimal learning.
About This Board Review Set
This is Part 215 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 215
This module focuses heavily on: Foot, Fracture, Ligament, Nerve, Spine.
Sample Questions from This Set
Sample Question 1: Following a fall from a height of 5 feet, a patient reports pain along the lateral border of the foot. The CT scan shown in Figure 54 indicates what pathology?...
Sample Question 2: Limited weight bearing usually is recommended following open reduction and internal fixation of intra-articular lower extremity fractures. A bone graft, or bone graft substitute is often placed in the metaphyseal void beneath the reduced ar...
Sample Question 3: A 58-year-old African-American female who sustained an injury to her upper arm six months ago presents with persistent arm pain. She was initially treated with splinting, with conversion to fracture bracing. She is neurovascularly intact. A...
Sample Question 4: In a retroperitoneal approach to the lumbar spine, what nerve is commonly found on the psoas muscle?...
Sample Question 5: When making a comparison to autograft incorporation, the inflammatory process in allograft tissue anterior cruciate ligament (ACL) reconstruction...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Following a fall from a height of 5 feet, a patient reports pain along the lateral border of the foot. The CT scan shown in Figure 54 indicates what pathology?
Explanation
REFERENCE: Robbins MI, Wilson MG, Sella EJ: MR imaging of anterosuperior calcaneal process fractures. Am J Roentgenol 1999;172:475-479.
Question 2
Limited weight bearing usually is recommended following open reduction and internal fixation of intra-articular lower extremity fractures. A bone graft, or bone graft substitute is often placed in the metaphyseal void beneath the reduced articular fragments. Which of the following bone grafts or bone graft substitutes will most likely permit earlier weight bearing without subsidence of the articular reduction?
Explanation
Question 3
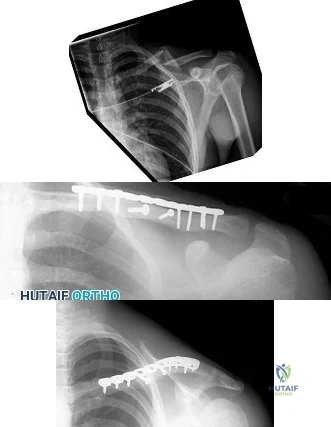
A 58-year-old African-American female who sustained an injury to her upper arm six months ago presents with persistent arm pain. She was initially treated with splinting, with conversion to fracture bracing. She is neurovascularly intact. An injury radiograph and a current radiograph are shown in Figures A and B respectively. What nutritional or metabolic disturbance is the most likely associated with this patient's diagnosis? Review Topic

Explanation
The incidence of nonunion with non-operative management of humeral shaft injuries ranges from 2-10%. Risk factors include vitamin D deficiency (most common), open fractures, segmental injuries, smoking and obesity. The optimal treatment is compression plating with bone grafting, which has been shown to be superior to intramedullary nailing with bone grafting or compression plating alone.
Ring et al. reviewed factors that contributed to humeral diaphyseal nonunion after fracture bracing. Fractures in the proximal to middle one-third of the shaft or fractures with a spiral/oblique pattern were more likely to go on to nonunion.
Brinker et al. reviewed 37 low-energy fractures that went onto nonunion. These patients were evaluated by clinical endocrinologists for evaluation of metabolic abnormalities. Thirty-one of the 37 patients (84%) had a metabolic issue, with 68% (25 of 37 patients) having Vitamin D deficiency.
Figure A demonstrates a humeral shaft fracture. Figure B demonstrates an atrophic nonunion of the humeral shaft fracture.
Incorrect Answers:
Question 4
In a retroperitoneal approach to the lumbar spine, what nerve is commonly found on the psoas muscle?
Explanation
REFERENCES: Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107.
Johnson R, Murphy M, Southwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Gray’s Anatomy. New York, NY, Bounty Books, 1977, pp 1226-1227.
Question 5
When making a comparison to autograft incorporation, the inflammatory process in allograft tissue anterior cruciate ligament (ACL) reconstruction
Explanation
Question 6
Figure 3a is the initial radiograph of a 19-year-old man who sustained a closed clavicle fracture. Figures 3b and 3c show postoperative radiographs. If the patient had been treated nonsurgically, which of the following would most likely occur?
Explanation
Question 7
Radiographs shown in Figures 1 through 3 show two different prosthetic design variations of the same knee implant. When compared with the design of right knee prosthesis, the left can be expected to have a
Explanation
Question 8
An 18-year-old football halfback reports that he had immediate right knee pain after being tackled 1 week ago. Examination now reveals moderate tenderness over the proximal medial tibia and lateral joint and normal cruciate stability. In evaluating the integrity of the posterolateral knee structures, what is the most reliable examination finding?
Explanation
REFERENCES: Veltri DM, Warren RF: Isolated and combined posterior cruciate injuries. J Am Acad Orthop Surg 1993;1:67-75.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont IL, American Academy of Orthopaedic Surgeons, 2002, pp 489-511.
Question 9
A previously healthy 14-year-old boy now reports fatigue, and has a bilateral Trendelenburg gait, right hip pain, and bilateral knee and foot pain. Biopsy of a right sacral mass reveals intermediate grade osteosarcoma. There are no metastases. Laboratory studies reveal a serum calcium level of 7.7 mg/dL (normal 8.5 to 10.5), a phosphate level of 2.0 mg/dL (normal 2.7 to 4.5), a 1,25-dihydroxyvitamin D level of less than 10 pg/mL (normal 18 to 62), a parathyroid hormone level of 19 pg/mL (normal 10 to 60), and an alkaline phosphatase level of 428 U/L (normal 15 to 351). What is the most likely cause of the patient’s symptoms?
Explanation
REFERENCES: Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 29-2001. A 14-year-old with abnormal bones and a sacral mass. N Engl J Med 2001;345:903-908.
Jonsson KB, Zahradnik R, Larsson T, White KE, Sugimoto T, Imanishi Y, et al: Fibroblast growth factor 23 in oncogenic osteomalacia and X-linked hypophosphatemia. N Engl J Med 2003;348:1656-1663.
Question 10
Figures 51a and 51b show the AP and lateral radiographs of the elbow of a 26-year-old man who fell. Closed reduction was performed in the emergency department, and management consisted of immobilization for 3 weeks prior to the initiation of motion. At 12 weeks after injury, he reports continued feelings of instability and catching in his elbow when using his arms to rise from a chair. Which of the following procedures needs to be performed, at a minimum, to reestablish stability of the elbow? Review Topic

Explanation
Question 11
Varus malalignment after a talar neck fracture with medial comminution causes a decrease in what motion?

Explanation
Herscovici et al review the appropriate management of complex ankle and hindfoot injuries in this instructional course lecture.
Daniels et al performed a cadaveric study where they osteotomized the talar neck and then studied ankle motion with and without removal of a medially based wedge of bone. They found that subtalar eversion was specifically decreased.
Sanders et al found that secondary reconstructive procedures following talar neck fractures were most commonly performed to treat subtalar arthritis or misalignment.
Question 12
Scapular notching following reverse shoulder arthroplasty may be minimized by what technical modification? Review Topic
Explanation
Question 13
A 71-year-old woman has a failed revision hip arthroplasty and is undergoing a re-revision hip arthroplasty. Her last hip surgery was 4 years ago with revision of the acetabular component. Radiographs show a well-fixed extensively porous-coated femoral component and a failed acetabular component with proximal and medial migration through the floor of the acetabulum. Preoperative laboratory studies reveal an erythrocyte sedimentation rate (ESR) of 70 mm/h (normal 0-29 mm/h), a C-reactive protein (CRP) of 23.3 (normal 0.2-8.0), and a negative hip aspiration. At the time of surgery, tissues look inflamed and a frozen section shows 20 WBC per high power field; however, a Gram stain is negative. What is the most appropriate action at this point?
Explanation
REFERENCES: Sanzen L, Sundberg M: Periprosthetic low-grade hip infections: Erythrocyte sedimentation rate and C-reactive protein in 23 cases. Acta Orthop Scand 1997;68:461-465.
Spangehl MJ, Hanssen AD, Osman DR: Diagnosis and treatment of the infected hip arthroplasty, in Morrey BF(edA)L:-MJoaidnetnaRCeopplyacement Arthroplasty, ed 3. Philadelphia, PA, Churchill Livingstone, 2003, pp 856-874. Question 71
A 79-year-old patient has a history of peripheral vascular disease and reports chronic knee pain. She has had coronary artery disease treated with angiography and stents on two occasions. Peripheral pulses are absent in both lower extremities, but the patient is disabled by advanced chronic degenerative arthritis in her right knee and would like to proceed with a total knee arthroplasty. The next most appropriate evaluation should include which of the following?
Ankle-brachial index of the affected lower extremity
Femoral popliteal angiography
Venous Dopplers of both lower extremities
MRI of the popliteal fossa
Radiographs to identify calcified plaques in the femoral artery
DISCUSSION: This question is designed to draw attention to the fact that peripheral vascular disease carries an increased risk of complications for the patient and should be carefully evaluated. The vascular surgeon will make the choice of revascularization or surgical clearance for knee reconstruction based on the initial results of the ankle-brachial index.
REFERENCE: Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001 ;9:253-257.
Question 14
An otherwise healthy 78-year-old woman has low back and buttock pain. Rectal examination reveals a large sacral mass. Figures 7a and 7b show a CT scan and a sagittal MRI scan of the lumbosacral spine. A biopsy specimen is shown in Figure 7c. What is the most likely diagnosis?
Explanation
REFERENCES: Mindell ER: Chordoma. J Bone Joint Surg Am 1981;63:501-505.
Samson IR, Springfield DS, Suit HD, Mankin HJ: Operative treatment of sacrococcygeal chordoma: A review of twenty-one cases. J Bone Joint Surg Am 1993;75:1476-1484.
Question 15
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Explanation
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Question 16
What normal tissue has a low signal intensity (appears black) on both T1- and T2-weighted images?
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-70.
Slucky AV, Potter HG: Use of magnetic resonance imaging in spinal trauma: Indications, techniques, and utility. J Am Acad Orthop Surg 1998;6:134-145.
Question 17
A 24-year-old man sustained a bilateral C5-6 facet dislocation in a car accident and was intubated at the scene. He remains sedated in the intensive care unit
Explanation
Question 18
In long-term follow-up studies of cemented total knee arthroplasty (TKA), the lowest rates of osteolysis have been associated with which design feature?
Explanation
The lowest reported rates of osteolysis involving cemented TKAs are associated with monolithic tibial components. Modular components and cemented metal-backed patella components are associated with a high prevalence of backside tibial insert wear and osteolysis.
Question 19
According to Musculoskeletal Infection Society (MSIS) guidelines, which set of patient laboratory study results fits the definition of chronic prosthetic joint infection?
Explanation
The MSIS definition of periprosthetic joint infection was updated in 2014 with two major and six minor criteria. The presence of one major criterion or three minor criteria is diagnostic for infection. The major criteria are two positive cultures with the same organism or a draining sinus tract. The current MSIS minor criteria are 1) an elevated ESR (more than 30 mm/hr) and CRP level (more than 10 mg/L), 2) an elevated synovial WBC count (more than 3,000 cells per/microliter), 3) an elevated synovial fluid polymorphonuclear count (more than 80%), 4) a positive histological analysis of periprosthetic tissue, and 5) a single positive culture.
Question 20
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
Explanation
REFERENCES: Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Fritschy D, Fasel J, Imbert JC, et al: The popliteal cyst. Knee Surg Sports Traumatol Arthrosc 2006;14:623-628.
Question 21
Which of the following pieces of equipment currently offers the greatest opportunity for lowering the number of equestrian injuries?
Explanation
REFERENCES: Ball CG, Ball JE, Kirkpatrick AW, et al: Equestrian injuries: Incidence, injury patterns, and risks factors for 10 years of major traumatic injuries. Am J Surg 2007;193:636-640.
Frankel HL, Haskell R, Digiacomo JC, et al: Recidivism in equestrian trauma. Am Surg 1998;64:151-154.
A 38-year-old man is three quarters of the way through the Hawaiian Ironman events run in a temperature of 60°F. He is sweating profusely and suddenly collapses. Prior to this he had been drinking large amounts of bottled water at every water stop. What is the most likely diagnosis?
Hypernatremia
Hypothermia
Hyponatremia
Subendocardial myocardial infarction
Ruptured berry aneurysm
DISCUSSION: Hyponatremia is often seen in endurance athletes such as triathloners, ultramarathoners, and marathoners after prolonged exertion. It is commonly attributed to excess free water intake that fails to replete massive sodium losses that result from sweating as reported by O’Connor. Exercise-induced hyponatremia is generally asymptomatic, particularly in patients in whom the sodium is only mildy reduced. Up to 10% of ultradistance athletes have a sodium level of 135 mEq/L or less, but those who are symptomatic usually have a sodium level of 125 mEq/L as reported by Noakes and O’Connor. The best way to prevent hyponatremia is to maintain the proper volume and types of fluid intake to ensure fluid balance during exercise. Beverages containing carbohydrates in concentrations of 4% to 8% (ie, “sports drinks”) are recommended for athletes participating in exercise lasting more than an hour (eg, marathon runners, etc.) To avert brainstem herniation and death, severe, acute hyponatremia requires rapid correction. Oral rehydration with salty solutions is safe and effective in patients with mild symptoms.
Too rapid correction has been reported to cause central pontine myelinolysis; therefore, correction ought to be performed slowly. Hypernatremia, hypothermia, subendocardial myocardial infarction, or ruptured berry aneurysm are unlikely in this scenario.
REFERENCES: O’Connor RE: Exercise-induced hyponatremia: Causes, risks, prevention, and management. Cleve Clin J Med 2006;73:S13-S18.
Noakes T: Hyponatremia in distance runners: Fluid and sodium balance during exercise. Curr Sports Med Rep
2002;1:197-207.
Laureno R, Karp BI: Myelinolysis after correction of hyponatremia. Ann Int Med 1997;126:57-62. Question 50
A 20-year-old male tennis player reports the acute onset of ulnar-sided wrist pain after hitting a forehand shot. Examination reveals dorsoulnar tenderness and minimal swelling. The pain is recreated with supination, wrist flexion, and ulnar deviation. Radiographs are normal. What structure is most likely involved?
Ulnar styloid
Flexor carpi radialis tendon
Extensor carpi ulnaris tendon
Scapholunate ligament
Transverse carpal ligament PREFERRED RESPONSE: 3
DISCUSSION: Extensor carpi ulnaris (ECU) lesions produce pain at the dorsoulnar aspect of the wrist, particularly during wrist supination, wrist flexion, and ulnar deviation. It has been frequently described in tennis players. Most ECU tenosynovitis can be successfully treated nonsurgically with immobilization techniques. Surgical treatment is generally indicated for ECU tenosynovitis or tendinopathy that does not respond to rest. Anatomically, the ECU retinaculum can rupture and the tendon can leave its sheath. With supination, the tendon can leave the sheath and then return to its position during pronation.
REFERENCES: Montalvan B, Parier J, Brasseur JL, et al: Extensor carpi ulnaris injuries in tennis players: A study of 28 cases. Br J Sports Med 2006;40:424-429.
Allende C, Le Viet D: Extensor carpi ulnaris problems at the wrist: Classification, surgical treatment and results. J Hand Surg Br 2005;30:265-272.
Question 22
An 80-year-old man has had increasing shoulder pain for the past 4 months. He reports that it began with soreness and stiffness after chopping some wood. A coronal MRI scan is shown in Figure 16. Initial management should consist of
Explanation
REFERENCES: Rockwood CA Jr, Williams GR Jr, Burkhead WZ Jr: Debridement of degenerative, irreparable lesions of the rotator cuff. J Bone Joint Surg Am 1995;77:857-866.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 299-312.
Question 23
A 17-year-old male soccer player sustains repeated lateral patellar dislocations refractory to physical therapy, bracing, and taping. After a workup including radiographs and MRI, the orthopaedic surgeon considers an isolated tibial tubercle osteotomy (TTO). He plans a 60-degree anteromedialization to address instability and to unload the patellofemoral joint. What is a relative contraindication to this procedure?
Explanation
TTO is a common treatment for patellofemoral instability. The angle of correction must be customized to each patient’s anatomy. For this patient, the orthopaedic surgeon plans an osteotomy that will both anteriorize and medialize the tubercle. This will consistently result in
a change of patellofemoral kinematics and contact pressures. Medialization decreases lateral and increases medial patellofemoral contact pressures, and anteriorization shifts contact pressures from distal to proximal. Significant anteriorization may not be desired in a patient with proximal patellar chondrosis unless a concomitant chondral procedure is performed as well. The patellar height (Caton-Deschamps ratio) is normal, precluding the need for distalization but not medialization. The TT-TG distance, at more than 20 mm, is a strong indication for osteotomy. The Q angle, although a less precise indicator of malalignment, is also elevated and would be considered an indication for osteotomy.

CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 41
A healthy, active 18-year-old man has acute-onset right knee pain and an inability to fully extend his knee following an attempt to stand from a seated position yesterday. He sustained a noncontact injury to his right knee while playing basketball 2 years ago and underwent primary anterior cruciate ligament (ACL) reconstruction with bone-patella-tendon-bone autograft and medial meniscus repair. He sustained another noncontact injury to the same knee 8 months later and underwent a revision ACL reconstruction using soft-tissue allograft and revision medial meniscus repair. He reports multiple episodes of “giving way” of his knee, but no pain prior to yesterday’s acute injury.
Question 24
A 35-year-old man who is involved in an improvised explosive device attack is hit by a piece 57 of shrapnel. He has a solitary penetrating wound in his left tibia. Radiographs show no fracture. He has significant pain and his calf is grossly swollen. He has good sensation and palpable dorsalis pedis and tibialis posterior pulses. He has elevated pressure in all 4 compartments. When performing a 4-compartment fasciotomy using the 2-incision technique, which structure is at risk when opening the deep posterior compartment?
Explanation
Compartment syndrome is commonly seen in lower-extremity trauma, especially in blast injuries or high-energy trauma to the lower extremity. It is important to recall the neurovascular structures present in each of the 4 compartments. The posterior tibial artery is in the deep posterior compartment along with the tibial nerve, the peroneal artery and vein, and the posterior tibial vein. The lateral compartment contains the superficial peroneal nerve.
The anterior compartment contains the deep peroneal nerve and the anterior tibial artery and vein. The superficial posterior compartment does not have any neurovascular structures. The saphenous nerve is superficial.
RECOMMENDED READINGS
Thompson JC, ed. Netter’s Concise Atlas of Orthopaedic Anatomy. Teterboro: NJ: Icon Learning Systems; 2002.
Mubarak SJ, Owen CA. Double-incision fasciotomy of the leg for decompression in compartment syndromes. J Bone Joint Surg Am. 1977 Mar;59(2):184-7. PubMed PMID: 15455478.View Abstract at PubMed
Question 25
Figures 8a and 8b show the clinical photograph and radiograph of a 4-month-old infant who has a left foot deformity. Examination reveals that the foot deformity is an isolated entity, and the infant has no known neuromuscular conditions or genetic syndromes. Which of the following studies will best confirm the diagnosis?
Explanation
REFERENCES: Kumar SJ, Cowell HR, Ramsey PL: Vertical and oblique talus. Instr Course Lect 1982;31:235-251.
Kodros SA, Dias LS: Single-stage correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Herring JA: Disorders of the foot, vertical talus, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, from the Texas Scottish Rite Hospital for Children, ed 3. Philadelphia, PA,
WB Saunders, 2002, pp 959-967.
Question 26
Which radiographic abnormality most accurately serves as a predictor of ankle syndesmosis disruption?
Explanation
Normal syndesmotic relationships include a tibiofibular clear space smaller than 6 mm on both AP and mortise views. In a 1989 cadaveric study by Harper and Keller, a tibiofibular clear space exceeding 6 mm on both the AP and mortise views was the most reliable predictor of early syndesmotic widening. Tibiofibular overlap is measured 1 cm proximal to the plafond. Normal values exceed 6 mm or 42% of the width of the fibula on the AP view, or 1 mm on the mortise view. Proximal fibula fracture can occur in isolation without syndesmotic injury, frequently after direct trauma. The medial clear space is the distance between the lateral border of the medial malleolus and the medial border of the talus and is measured at the level of the talar dome. In the mortise view with the ankle in neutral dorsiflexion, the medial clear space should be equal to or smaller than the superior clear space between the talar dome and the tibial plafond. ?A normal medial clear space may be present with syndesmotic injury and consequently lacks sensitivity and specificity.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Wuest TK. Injuries to the Distal Lower Extremity Syndesmosis. J Am Acad Orthop Surg. 1997 May;5(3):172-181. PubMed PMID: 10797219. View Abstract at PubMed
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle. 1989 Dec;10(3):156-60. PubMed PMID: 2613128. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 37 THROUGH 40
A 41-year-old man sustained a twisting injury while running up stairs 4 weeks ago. He was treated in an ankle brace and has been bearing weight since the injury occurred. He has no history of ankle problems, but he now has ankle pain, swelling, and instability. The pain is aggravated by stairs, and the instability is worse on unlevel ground. Radiographs do not show a fracture.
Question 27
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Explanation
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Early JS: Fractures and dislocations of the midfoot and forefoot, in Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 2181-2245.
Question 28
The presence of S100B tumor marker typically corresponds with which of the following as being the most likely source of the metastasis?
Explanation
(TTF-1) can help to determine the origin of an adenocarcinoma or aid in the recognition of other tumors. In patients who do not have an obvious primary site of disease or screening radiographs, these new markers can help focus the search for and guide the treatment of the underlying lesion. CA125 is positive in patients with ovarian cancer, CK7 is positive in patients with breast and lung carcinoma, and CK20 is indicative of colon carcinoma if the CK7 marker is negative. Gastrointestinal stromal tumor (GIST) is positive for CD117 (c-kit) and CD34, whereas 75% of bronchogenic carcinomas are positive for TTF-1. Histochemical staining of the S100 protein family has been used for many years in the diagnosis of malignant melanoma. Recent markers HMB-45, MART-1, and Melan-A have proved to be useful in diagnosis of melanoma. S100B protein has been implicated in downregulation of p53 (oncosuppressor gene).
REFERENCES: Harpio R, Einarsson R: S100 proteins as cancer biomarkers with focus on S100B in malignant melanoma. Clin Biochem 2004;37:512-518.
Roodman GD: Mechanisms of bone metastasis. N Engl J Med 2004;350:1655-1664.
Question 29
On physical examination, he has no open wounds and is neurologically intact in both lower extremities. Imaging of the right femur (Figures A and B) and the left femur (Figures C and D) is shown. What is the next best step in treatment?

Explanation
OrthoCash 2020
Question 30
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of
Explanation
A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma.
REFERENCES: Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033.
Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
Dormans JP, Rang M: Fractures of the olecranon and radial neck in children. Orthop Clin North Am 1990;21:257-268.
Question 31
What type of physical therapy is most effective for chronic noninsertional Achilles tendinopathy?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 91-102.
Vora AM, Myerson MS, Oliva F, et al: Tendinopathy of the main body of the Achilles tendon.
Foot Ankle Clin 2005;10:293-308.
Question 32
A 34-year-old female is involved in a high-speed motor vehicle collision and sustains a traumatic proximal forearm amputation. She successfully undergoes debridement and closure, and six weeks later, is fitted with her temporary prosthesis. In order to optimize her outcomes upon returning to work as a secretary, which of the following is recommended?
Explanation
Richards et al surveyed 34 patients who had emergency upper extremity surgery and found high levels of psychological distress in patients, including 29% with high levels of both depression and post-traumatic stress disorder (PTSD). They also found that disability was strongly related to pain, depression, and PTSD symptoms.
Mallette et al assessed the attitudes of hand surgery patients and hand surgeons regarding psychologic influences on illness and compared their attitudes with those of the general population. They found that surgeons underestimated the openness of patients to discuss psychological issues and that patients believed in the strong effect of psychologic factors on healing and pain.
Illustration A shows a myoelectric prosthesis in a military veteran. Incorrect Answers:
Question 33
A healthy 16-year-old boy has had increasing pain in the right knee for the past 3 months. Examination reveals warmth and swelling around the distal femur. Radiographs and an MRI scan are shown in Figures 51a through 51c, and a biopsy specimen is shown in Figure 51d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 205.
Question 34
A 10-year-old boy reports heel pain with sporting activities. An examination demonstrates gastrocnemius contracture and tenderness at the calcaneal apophysis. Radiographs are unremarkable. What is the best next step?
Explanation
Sever disease, or calcaneal apophysitis, is best treated with activity modification that includes rest, restriction from sports and running, and Achilles tendon stretching exercises. The diagnosis is clinical (rendering MRI study unnecessary) and the course is usually self-limited, obviating the need for surgery. Occasionally, children with severe symptoms may benefit from a short period of cast or fracture brace immobilization.
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
Question 35
Figures 1 and 2 are the radiographs of a 36-year-old man who has had left wrist pain for the past 6 months following a fall onto his outstretched arm. Examination reveals a positive ballottement test, dorsal and ulnar carpal tenderness, and a painful snap with ulnar deviation, pronation, and axial compression. Injury to what ligament is the cause of this patient's pain?
Explanation
The radiographs reveal a volarly tilted lunate on the lateral view (Figure 1) and an incongruous lunotriquetral articulation on the AP gripped view (Figure 2). The patient has what appears to be radiographic findings of volar intercalated segmental instability (VISI), a type of carpal instability, dissociative. An injury to the volar lunotriquetral ligament is the most important contributor to this type of instability. An injury to the dorsal scapholunate ligament typically leads to a dorsal intercalated segmental instability. Isolated injuries to the dorsal radiocarpal ligament and the radioscaphocapitate
ligament do not lead to VISI, although combined injuries may lead to instability between the radius and the proximal row.
Question 36
Figures 41a and 41b show the radiographs of a 22-year-old woman who has a bunion on her left foot. She denies pain in the foot, but she reports increasing difficulty with shoe wear. Management should consist of
Explanation
REFERENCE: Mann RA, Coughlin MJ: Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 174.
Question 37
After full healing from this injury, which option most likely will help to optimize this patient's activities?
Explanation
Midfoot fracture dislocations typically occur after a fall from a height or a motor vehicle collision involving severe dorsiflexion loading of the foot from a brake pedal or the floorboards. The deformity that results may be subtle because the subluxation may be a valgus or varus rotation around the midfoot rather than pure dorsiflexion. Early recognition and reduction is indicated to minimize secondary complications such as nerve injury or vascular compromise. Closed reduction usually necessitates formal anesthesia in an operating room to permit adequate relaxation and reduction. In many cases, satisfactory reduction can be accomplished closed, but the surgeon must be prepared to perform an open reduction if needed. The most common reason for failed closed reduction is that the talar head is caught by the tibialis posterior tendon (under which the talar head has protruded). This acts as a Chinese finger trap, preventing relocation by the usual distraction followed by
a plantar flexion maneuver. In these cases, open reduction is performed through a dorsomedial incision through which the tibialis posterior is retracted medially, allowing reduction of the talonavicular joint. The joints usually require pinning to maintain stability during healing. The long-term prognosis for these injuries is guarded because many patients develop degenerative changes in the Chopart joint. If symptomatic arthritis develops, helpful external supports are designed to limit sagittal motion at the joint (for example, carbon fiber inserts or rocker-bottom soles).
RECOMMENDED READINGS
Swords MP, Schramski M, Switzer K, Nemec S. Chopart fractures and dislocations. Foot Ankle Clin. 2008 Dec;13(4):679-93, viii. Doi: 10.1016/j.fcl.2008.08.004. Review. PubMed PMID: 19013402.View Abstract at PubMed
Richter M, Thermann H, Huefner T, Schmidt U, Goesling T, Krettek C. Chopart joint fracture-dislocation: initial open reduction provides better outcome than closed reduction. Foot Ankle Int. 2004 May;25(5):340-8. PubMed PMID: 15134617. View Abstract at PubMed
Question 38
Figures 1 and 2 depict the postoperative radiographs obtained from a 22-year-old man who was involved in a motor vehicle accident. The most likely limitation in motion arising from this treatment is

Explanation
This patient sustained fractures of his radius and ulna; both were treated with plate and screw fixation. The plate used on the radius was straight, resulting in loss of the radial bow, which is critical for enabling the radius to curve around the ulna during pronation. This patient is unable to pronate beyond 20°. Schemitsch and Richards correlated a good functional outcome, defined as more than 80% of normal rotation of the forearm, with restoration of the normal amount and location of the radial bow. Additionally, they related the restoration of grip strength with appropriate restoration of the radial bow. Matthews and associates reported little significant loss of rotation with 10° of angulation; however, 20° of angulation resulted in a statistically and clinically significant loss of forearm rotation.
Question 39
Figures 1 and 2 are the right shoulder MRI scans of a 22-year-old right-handed professional male volleyball player with 4 months of right shoulder pain. The pain began insidiously and is exacerbated by overhead activities and hitting during games. He has maintained a daily program of shoulder stretching and strengthening exercises but has experienced a steady decline in function to the point of not being able to participate in volleyball. Examination reveals some mild atrophy at the posterior shoulder, full forward elevation, mild weakness of external rotation on the right shoulder, negative empty-can testing, positive O’Brien’s and negative apprehension. Surgical intervention would aim to resolve pathology related to which nerve?
Explanation
Question 40
Overgrowth of a limb in a patient with neurofibromatosis type 1 (NF1) is most likely associated with the presence of
Explanation
REFERENCES: Alman BA, Goldberg MJ: Syndromes of orthopaedic importance, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 287-338.
Greene WB: Neurofibromatosis type I, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1584-1588.
Question 41
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in
Explanation
REFERENCES: Shelton WR, Barrett GR, Dukes A: Early season anterior cruciate ligament tears: A treatment dilemma. Am J Sports Med 1997;25:656-658.
Snyder-Mackler L, Fitzgerald GK, Bartolozzi AR III, Ciccotti MG: The relationship between passive joint laxity and functional outcome after anterior cruciate ligament injury. Am J Sports Med 1997;25:191-195.
Question 42
- A patient has a noncomminuted displaced fracture of the radial head with a distal radioulnar dissociation. What is the most appropriate treatment for the radial head?
Explanation
Question 43
Figure 33 shows the CT scan of a 40-year-old man who injured his left shoulder while skiing. What structure is attached to the bony fragment?
Explanation
REFERENCES: O’Brien SJ, Neves MC, Arnoczky SP, et al: The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. Am J Sports Med 1990;18:449-456.
Warner JP: The gross anatomy of the joint surfaces, ligaments, labrum and capsule, in Matsen FA, Fu FF, Hawkins RJ (eds): The Shoulder: A Balance of Mobility and Stability. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1992, pp 7-28.
Question 44
Figure below depicts the radiograph obtained from a 52-year-old woman who has leg-length inequality and chronic, activity-related buttock discomfort. This problem has been lifelong, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe type IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step versus oblique cut, or strut grafts.
Question 45
A 33-year-old female with generalized ligamentous laxity is diagnosed with spontaneous atraumatic subluxation of the sternoclavicular joint. She notes mild, intermittent pain and a small amount of prominence to that area. What is the most appropriate treatment at this time?

Explanation
Question 46
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient’s left knee. Abnormal findings include
Explanation
REFERENCES: Ahn JH, Shim JS, Hwang CH, et al: Discoid lateral meniscus in children: Clinical manifestations and morphology. J Pediatr Orthop 2001;21:812-816.
Andrish JT: Meniscal injuries in children and adolescents: Diagnosis and management.
J Am Acad Orthop Surg 1996;4:231-237.
Question 47
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?
Explanation
REFERENCES: Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
Wirth MA, Rockwood CA Jr: Complications of total shoulder replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Question 48
Prescribing touch (10 to 15 kg) weight-bearing would be most appropriate in the following scenario?
Explanation
The definition of touch weight bearing (also known as touch-down weight bearing) is ill-defined in the literature. Published data suggest touch weight bearing to be 10 to 15 kg of load applied to ground by the affected limb or less than 20% of body weight. In contrast, partial weight bearing is reported as 20 to 25 kg or 30% to 50% of body weight. Joint reaction forces across the hip have been shown to be lowest with touch weight-bearing. In this scenario, the foot should be flat against the ground so the flexor and extensor musculature that cross the hip are relaxed. With non-weight bearing restrictions, the musculature across the hip will be contracted, which increases contact pressures and joint reaction forces.
Rubin et al. looked at the validity of touch weight-bearing and partial weight bearing regimens. They found that most patients overload the limb up to 50% more than the target weight prescribed.
Lewis et al. showed that maintaining non-weight-bearing position of the involved leg produces increased compressive forces across the hip joint due to activation of the hip flexors compared to restricted weight-bearing.
Incorrect Answers:
Question 49
-A likely candidate for treatment with a thoracic lumbosacral orthosis scoliosis brace is seen in
Explanation

Question 50
A 7-year-old boy sustains an acute injury to the distal radial metaphysis, along with a completely displaced Salter-Harris type I fracture of the ulnar physis, as shown by the arrows in Figure 12. After satisfactory reduction of both injuries, what is the major concern?
Explanation
REFERENCES: Nelson OA, Buchanan JR, Harrison CS: Distal ulnar growth arrest. J Hand Surg Am 1984;9:164-170.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, pp 632-635.
Question 51
Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?
Explanation
REFERENCES: Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 351-360.
Inaba K, Kirkpatrick AW, Finkelstein J, et al: Blunt abdominal aortic trauma in association with thoracolumbar spine fractures. Injury 2001;32:201-207.
Question 52
Figure 29 shows the radiograph of a 25-year-old woman who has had a 3-month history of ankle pain after sustaining an inversion injury to the ankle. She reports occasional catching, but no sense of instability. Examination reveals ligament stability. Management should consist of
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Pettine KA, Morrey BF: Osteochondral fractures of the talus: A long-term follow-up. J Bone Joint Surg Br 1987;69:89-92.
Question 53
An osteoconductive bone graft material has which of the following properties?
Explanation
substitution, which allows for graft incorporation. An osteoinductive graft will stimulate the recruitment of progenitor cells that can differentiate into osteoblastic cells. Specific BMPs are osteoinductive. Osteogenic material contains viable cells with the ability to form bone. The ability to provide osteoprogenitor cells is only seen in fresh autograft. Other grafts rely on the recruitment of host progenitor cells to differentiate.
Question 54
The radiograph shown in Figure 27 shows measurement of what angle?
Explanation
REFERENCES: Coughlin MJ: Juvenile hallux valgus: Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Steel MW III, Johnson KA, DeWitz MA, et al: Radiographic measurements of the normal foot. Foot Ankle 1980;1:151-158.
Richardson EG, Graves SC, McClure JT, et al: First metatarsal head-shaft angle: A method of determination. Foot Ankle 1993;14:181-185.
Question 55
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
REFERENCES: O’Driscoll SW, Morrey BF: Elbow arthroscopy, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 21-34.
Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 56
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome?
Explanation
REFERENCES: Lalonde F, Letts M, Yang JP, et al: An analysis of burst fractures of the spine in adolescents. Am J Orthop 2001;30:115-120.
Clark P, Letts M: Trauma to the thoracic and lumbar spine in the adolescent. Can J Surg 2001;44:337-345.
Been HD, Bouma GJ: Comparison of two types of surgery for thoraco-lumbar burst fractures: Combined anterior and posterior stabilization vs posterior instrumentation only. Acta Neurochir (Wien) 1999;141:349-357.
Question 57
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Howard FM, Dell PC: The unreduced carpal dislocation: A method of treatment. Clin Orthop 1986;202:112-116.
Question 58
Osteoclastic bone resorption is stimulated primarily by what molecular interaction?
Explanation
osteoclasts to enhance bone resorption. The pannus of rheumatoid arthritis and monosodium urate crystals of gouty tophi have been shown to trigger release of inflammatory cytokines such as IL-6, IL-8 and tumor necrosis factor alpha. The key to osteoclastic bone resorption of inflammatory arthropathy is regulated by the interaction of RANKL, expressed in osteoblasts and activated T cells, and RANK, expressed in osteoclast progenitors and mature osteoclasts. In inflammatory arthropathy, RANKL expression is increased and OPG is reduced, resulting in increased cortical and subchondral bone.
Question 59
A 10-year-old girl with a history of an obstetrical brachial plexus palsy has been referred for evaluation. Examination reveals a severe adduction internal rotation contracture of the shoulder and a mild flexion contracture of the elbow. Hand function is normal. Radiographs show mild glenohumeral joint incongruity. To achieve the best functional outcome, management should consist of
Explanation
REFERENCES: Jahnke AH Jr, Bovill DF, McCarroll HR Jr, James P, Ashley RK: Persistent brachial plexus birth palsies. J Pediatr Orthop 1991;11:533-537.
Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of 20 cases. J Pediatr Orthop 1990;10:442-444.
Goddard NJ, Fixsen JA: Rotation osteotomy of the humerus for birth injuries of the brachial plexus. J Bone Joint Surg Br 1984;66:257-259.
Question 60
- Which of the following surgical approaches to the hip is associated with the highest incidence of heterotopic ossification?
Explanation
Prevention:
incision choice: ilioinguinal if possible
radiation
indocin (give pepcid with it)
Question 61
A 19-year-old soccer player feels a pop in his knee while making a cut and notes the development of an effusion over several hours. Examination reveals medial joint line tenderness, but the knee is stable to manual stress testing of all ligaments. Examination under anesthesia confirms a stable knee. What is the most critical factor in determining healing after repair of the lesion shown in Figure 14?
Explanation
REFERENCES: DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
Henning CE, Lynch MA, Clark JR: Vascularity for healing of meniscus repairs. Arthroscopy 1987;3:13-18.
Question 62
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 68-year-old woman who comes to the emergency department after stepping into a hole and twisting her ankle. She is complaining of isolated ankle pain and is unable to bear weight. After closed manipulative reduction and splint placement, she is scheduled for operative treatment. The stability of the syndesmosis should be evaluated after

Explanation
Restores incisura competence thereby reducing the incidence of syndesmotic malreduction by creating containment
Assists in stabilizing the syndesmosis via the posterior inferior tibiofibular ligament, potentially limiting the need for additional syndesmotic stabilization
Maximizes the surface area for ankle joint loading
Enhances posterior translational stability of the talus
The traditional indication for stabilization of the posterior malleolus is based on fragment size. However, fracture orientation varies and makes evaluation of the fragment size challenging with a lateral radiograph alone. The three primary types include the posterolateral oblique, medial extension, and shell. Because of the additive syndesmotic stability which is gained through the deep deltoid ligament and medial malleolar fixation, the anterior talofibular ligament and lateral malleolar fixation, and the posterior inferior tibiofibular ligament and posterior malleolar fixation, syndesmotic stability should only be assessed after all other points of instability that are planned for fixation are fixed.
Syndesmotic instability should be assessed with direct manipulation on both the anteroposterior and lateral views with special attention to the lateral view. Syndesmotic reduction should be assessed either through open visualization or by comparing closed reduction parameters (clear space, overlap, and fibular position on the lateral view) with the patient’s contralateral side (assuming no injury). This is more effective than using population norms secondary to the two types of syndesmotic morphologies which create different absolute values for these parameters.
Question 63
What is the main function of collagen found within articular cartilage?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Mow VC, Ratcliffe A: Structure and function of articular cartilage and meniscus, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 113-177.
Question 64
Surgical restoration of sagittal balance of an adult spinal deformity will have which effect on outcome?
Explanation
The influence of sagittal balance on outcomes following fusion-based procedures for degenerative conditions of the lumbar spine has only recently been appreciated. Restoration of sagittal spinal balance improves low-back-pain outcomes and quality of life. Sagittal spinal balance has not been shown to relieve neurogenic claudication attributable to spinal stenosis.
RECOMMENDED READINGS
Li Y, Hresko MT. Radiographic analysis of spondylolisthesis and sagittal spinopelvic deformity. J Am Acad Orthop Surg. 2012 Apr;20(4):194-205. doi: 10.5435/JAAOS-20-04-194. Review. PubMed PMID: 22474089. View Abstract at PubMed
Korovessis P, Repantis T, Papazisis Z, Iliopoulos P. Effect of sagittal spinal balance, levels of posterior instrumentation, and length of follow-up on low back pain in patients undergoing posterior decompression and instrumented fusion for degenerative lumbar spine disease: a multifactorial analysis. Spine (Phila Pa 1976). 2010 Apr 15;35(8):898-905. doi: 10.1097/BRS.0b013e3181d51e84. PubMed PMID: 20354466. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 99 AND 100
Figures 99a and 99b are MR images of a 59-year-old man with a history of intravenous (IV) drug abuse who arrives at the emergency department with malaise and fever. Upon admission, the patient's temperature is 38.9°C, his white blood cell count is 17000/µL (reference range [rr], 4500-11000/µL), his erythrocyte sedimentation rate is 98 mm/h (rr, 0-20 mm/h), and his C-reactive protein level is 45 mg/L (rr, 0.08-3.1 mg/L). He is admitted to the medical service to evaluate the source of his fevers. On hospital day 1, the patient reports weakness in his left arm and leg. Blood cultures are positive for methicillin-resistant Staphylococcus aureus.
A B
Question 65
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
REFERENCES: Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Gerber C, Schneeberger AG: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 66
Compared with retention of the native patella in primary total knee arthroplasty, routine patellar resurfacing is associated with
Explanation
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in
large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate
in patients with anterior knee pain.
Question 67
A 14-year-old boy is seen for back pain. Radiographic evaluation reveals a grade III isthmic spondylolisthesis. What measurement is most useful in predicting the likelihood of progression? Review Topic
Explanation
Question 68
A subtrochanteric femur fracture in which the lesser trochanter is intact is associated with what deformity?
Explanation
Question 69
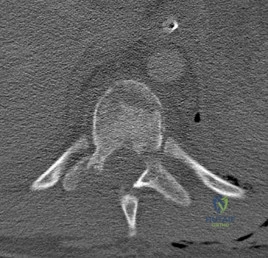
A B Figures 19a and 19b are the CT scans of an 18-year-old man who was a restrained driver in a rollover motor vehicle collision. What was the primary mechanism of injury?
Explanation
This injury pattern represents a flexion distraction injury, or a Chance fracture. The imaging hallmark of this injury is the axial split of the pedicle seen on the sagittal CT scan. This injury necessitates surgical intervention to prevent progressive deformity and pain. A rotation mechanism results in a dislocation with a rotational deformity at the level of injury. An extension force causes failure of the anterior column in tension with compression of the posterior column. An axial load force would result in a burst fracture.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Vaccaro AR, Baron EM, Sanfilippo J, Jacoby S, Steuve J, Grossman E, DiPaola M, Ranier P, Austin L, Ropiak R, Ciminello M, Okafor C, Eichenbaum M, Rapuri V, Smith E, Orozco F, Ugolini P, Fletcher M, Minnich J, Goldberg G, Wilsey J, Lee JY, Lim MR, Burns A, Marino R, DiPaola C, Zeiller L, Zeiler SC, Harrop J, Anderson DG, Albert TJ, Hilibrand AS. Reliability of a novel classification system for thoracolumbar injuries: the Thoracolumbar Injury Severity Score. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S62-9; discussion S104. PubMed PMID:16685239.View Abstract at PubMed
Question 70
Based on the radiographic findings shown in Figure 41, which of the following wrist ligaments is most likely disrupted?
Explanation
REFERENCES: Linscheid RL, Dobyns JH, Beabout JW, et al: Traumatic instability of the wrist: Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632.
Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Berger RA: Ligament anatomy, in Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist, Diagnosis and Operative Management. St Louis, MO, Mosby, 1998, pp 73-105.
Question 71
A 28-year-old painter has had increasing pain in his hand and forearm after sustaining a paint injection wound to the tip of his left index finger 24 hours ago. Management should consist of
Explanation
REFERENCES: Pinto MR, Turkula-Pinto LE, Cooney WP, Wood MB, Dobyns JH: High-pressure injection injuries of the hand: Review of 25 patients managed by open wound technique. J Hand Surg Am 1993;18:125-130.
Urbaniak JR, Evans JP, Bright DS: Microvascular management of ring avulsion injuries. J Hand Surg Am 1981;6:25-30.
Tsai TM, Manstein C, DuBou R, Wolff T, Kutz JE, Kleinert HE: Primary microsurgical repair of ring avulsion amputation injuries. J Hand Surg Am 1984;9:68-72.
Kay S, Werntz J, Wolff T: Ring avulsion injuries: Classification and prognosis. J Hand Surg Am 1989;14:204-213.
Schnall SB, Mirzayan R: High-pressure injection injuries to the hand, in Kozin SH (ed): Hand Clinics: Upper Extremity Trauma. Philadelphia, PA, 1999, pp 245-248.
Question 72
A 25-year-old male professional lacrosse player collides with another player, with injury resulting from a knee impacting the athlete’s thigh. He has immediate pain in the mid-thigh area and is unable to return to the game because of difficulty with running. Examination reveals developing swelling in the anterior mid-thigh area. The thigh compartments are soft, and he is able to extend his knee against gravity. Knee flexion at 90° gives him discomfort in the thigh but no knee pain. The knee and hip examinations are otherwise unremarkable. Plain films of the femur are negative. What is the best next step?
Explanation
A. only type 1 collagen.
B. only type 2 collagen.
C. type 1 and type 2 collagen.
D. neither type 1 or type 2 collagen.
The MRI scan shows a full-thickness cartilage defect. When treated with a marrow stimulation technique, such as a microfracture, the reparative tissue is fibrocartilage. Unlike hyaline cartilage, which is composed of only type 2 collagen, fibrocartilage is composed of both type 1 and type 2 collagen.
15- Figures 1 and 2 are the radiographs of a 58-year-old retired laborer who has had many years of right shoulder pain. He initially experienced relief with anti-inflammatory medication over the past year, but this no longer provides him pain relief. He has pain with overhead activities and is dissatisfied with his shoulder function. Examination indicates active and passive forward elevation to 130°, full strength with external rotation, and a negative belly press test. MRI demonstrates an intact rotator cuff. What is the best next step in treatment?
A. Anatomic total shoulder arthroplasty (TSA)
B. Hemiarthroplasty
C. Reverse shoulder arthroplasty
D. Arthroscopy with debridement and biceps tenodesis
The patient has glenohumeral osteoarthritis based on the radiograph. His examination demonstrates limited motion and no significant rotator cuff pathology – full strength with external rotation, negative belly press, and no pseudoparalysis. Of all the answer choices, an anatomic TSA would be the most appropriate treatment option. Hemiarthroplasty does not address glenoid pathology and provides inferior pain relief and function, compared with TSA. A reverse shoulder arthroplasty is utilized for patients with degenerative shoulder changes in conjunction with irreparable rotator cuff pathology. Shoulder arthroscopy with debridement and biceps tenodesis is not appropriate for those with severe degenerative changes of the shoulder.
16- According to the MRI scan shown in Figure 1, which pathologic finding is expected to be encountered during arthroscopy?
A. Figure 2
B. Figure 3
C. Figure 4
D. Figure 5
The sagittal MRI scan is a clear example of a double posterior cruciate ligament (PCL) sign. This sign has a high specificity for a displaced bucket handle tear of the medial meniscus as seen in Figure 4. The other arthroscopic
images show a flap tear of the medial meniscus (Figure 2), anterior cruciate ligament tear (Figure 3), and a full thickness articular cartilage defect (Figure 5). Other less likely causes of a double PCL sign include intermeniscal ligament, meniscofemoral ligaments, loose bodies, osteophytes, and fracture fragments. Correct answer : C 13
17- Figures 1 and 2 are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test, trace effusion, and range of motion from 0 to 85° of knee flexion. Which factor is most contributory to his examination findings?
A. Incorrect graft choice
B. Improper tunnel position
C. Tibial graft-tunnel mismatch
D. Femoral fixation at 80° flexion
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario.
Question 73
A 16-year-old male fell from a roof onto his right shoulder and presents with decreased pulses in his right upper extremity. Imaging reveals a posterior sternoclavicular dislocation. What is the best treatment at this time?

Explanation
The review article by Wirth and Rockwood notes the following complications with posterior dislocation: respiratory distress, venous congestion or arterial insufficiency, brachial plexus compression, and myocardial conduction abnormalities. They recommend reconstruction of the costoclavicular ligaments with resection of the medial clavicular head as needed for unstable injuries.
The referenced article by Waters et al noted 100% excellent short-term outcomes in adolescents with open reduction and reconstruction of the costoclavicular ligament in pure dislocations or with suture fixation of the medial physis in physeal injuries.
Question 74
Figures 42a and 42b show the radiographs of a 52-year-old man who sustained a fall from a motorcycle 6 months ago and now reports pain and stiffness in his left shoulder. What is the most reliable treatment to improve function and comfort of the shoulder?
Explanation
REFERENCES: Gerber C, Lambert SM: Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1996;78:376-382.
Spencer EE Jr, Brems JJ: A simple technique for management of locked posterior shoulder dislocations: Report of two cases. J Shoulder Elbow Surg 2005;14:650-652.
Sperling JW, Pring M, Antuna SA, et al: Shoulder arthroplasty for locked posterior dislocation of the shoulder. J Shoulder Elbow Surg 2004;13:522-527.
Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;34:584-590.
Question 75
A 45-year-old woman with grade II adult-acquired flatfoot deformity has pain on the lateral side of her foot just distal to the tip of the fibula. Which component of a comprehensive flatfoot reconstruction most likely will address the deformity responsible for this pain?
Explanation
Patients develop lateral ankle pain with progression of adult-acquired flatfoot deformity. This is associated with increased hindfoot valgus deformity. Calcaneal fibular impingement has been considered the primary cause of this pain. Studies demonstrate that arthrosis of the posterior facet of the subtalar joint strongly correlates with lateral pain in adult-acquired flatfoot deformity. Both conditions are related to hindfoot valgus deformity. Although lateral column lengthening is a powerful tool for correction of flatfoot deformity, its effect on hindfoot deformity is less defined. Lateral column lengthening provides better correction of the longitudinal arch of the midfoot and realignment of the medial column than other osteotomies. A medializing calcaneal osteotomy has a significant linear effect on hindfoot valgus alignment. Spring ligament reconstruction and medial cuneiform opening-wedge osteotomies have less effect on hindfoot alignment than the medial calcaneal slide.
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
Question 76
A 2-year-old boy has complete absence of the sacrum and lower lumbar spine. What is the most likely long-term outcome if no spinal pelvic stabilization is performed?
Explanation
REFERENCES: Tachdjian MO: The spine: Congenital absence of the sacrum and lumbosacral vertebrae (lumbosacral agenesis), in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 3, p 2228.
Renshaw TS: Sacral agenesis: A classification and review of twenty-three cases. J Bone Joint Surg Am 1978;60:373-383.
Question 77
Figure 39 shows the radiograph of a 4-month old infant who has been undergoing weekly casting since birth for a congenital equinovarus deformity. Management should now consist of
Explanation
REFERENCES: Lehman WB, Atar D: Complications in the management of talipes equinovarus, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992,
pp 135-136.
Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002,
pp 927-935.
Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990,
pp 2461-2564.
Question 78
A 45-year-old man feels a pop in the anterior aspect of his elbow while lifting furniture. He denies any antecedent pain or injury. Which examination method is best for diagnosing a distal biceps rupture?
Explanation
Question 79
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to
Explanation
REFERENCES: Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442.
Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Question 80
-Figure 235 is the radiograph of a 75-year-old woman who is seen in the emergency department following a low-energy fall. What is the most appropriate treatment based on her radiographic findings?
Explanation

Question 81
A Trendelenburg gait is most likely to be seen in association with
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Andersson GB, Deyo RA: History and physical examination in patients with herniated lumbar discs. Spine 1996;21:10S-18S.
Question 82
Which of the following tissues used for anterior cruciate ligament (ACL) reconstruction has the highest maximum load to failure?
Explanation
REFERENCES: Hamner DL, Brown CH Jr, Steiner ME, Hecker AT, Hayes WC: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Cooper DE, Deng XH, Burstein AL, Warren RF: The strength of the central third patellar tendon graft: A biomechanical study. Am J Sports Med 1993;21:8l8-823.
Brown CH Jr, Steiner ME, Carson EW: The use of hamstring tendons for anterior cruciate ligament reconstruction: Technique and results. Clin Sports Med 1993;12:723-756.
Engebretsen L, Lewis JL: Graft selection and biomechanical considerations in ACL reconstruction. Sports Med Arthroscopy Rev 1996;4:336-341.
Question 83
Figure 26 shows the MRI scan of a 60-year-old man who has had groin pain for the past 2 months. The patient reports pain with ambulation, and examination reveals an antalgic gait. He denies any history of steroid or alcohol abuse. Plain radiographs are normal. Management should include
Explanation
REFERENCE: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Question 84
Figures 169a through 169c show the radiograph and MRI scans of a 74-year-old woman who has had back and bilateral leg pain for the past 6 months. Nonsurgical management has failed to provide relief. What is the best option for surgical treatment? Review Topic

Explanation
Question 85
Figures 21a and 21b show the radiographs of a 12-year-old patient with an L4-level myelomeningocele who has scoliosis that has been slowly progressing for the past several years. There has been no loss of motor function. An MRI scan shows no syringomyelia or increased hydrocephalus. Management should consist of
Explanation
REFERENCES: Ward WT, Wenger DR, Roach JW: Surgical correction of myelomeningocele scoliosis: A critical appraisal of various spinal instrumentation systems. J Pediatr Orthop 1989;9:262-268.
Muller EB, Nordwall A: Brace treatment of scoliosis in children with myelomeningocele. Spine 1994;19:151-155.
Question 86
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?
Explanation
REFERENCES: Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Wu YW, Day SM, Strauss DJ, et al: Prognosis for ambulation in cerebral palsy: A population-based study. Pediatrics 2004;114:1264-1271.
Question 87
Figure 33 shows the AP and lateral radiographs of an obese 58-year-old man who underwent a cementless total hip arthroplasty 6 years ago. He reports no pain, and examination reveals a normal gait and painless hip range of motion. What is the most likely diagnosis?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Engh CA, Massin P, Suthers KF: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop 1990;257:107-128.
Question 88
The radiograph seen in Figure 67 reveals an ankle fracture in a 65-year-old woman who slipped on the ice. She has a history of diabetes mellitus for the past 7 years and reports that she maintains fair control of her diabetes; her last HgbA1c was 8%. The patient is a community ambulatory who lives independently. Examination reveals she has absent sensation with the 5.07 monofilament. When determining management, the physician must consider which of the following?

Explanation
Question 89
Figure 40 shows the radiograph of a 30-year-old woman who has a painful elbow. Examination reveals a deformed skull, multiple cafe-au-lait spots, and bone deformities. What is the most likely diagnosis?
Explanation
REFERENCES: Albright F, Butler AM, Hampton AO, et al: Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction with precocious puberty in females. N Engl J Med 1937;216:727-746.
Danon M, Robboy SJ, Kim S, Scully R, Crawford JD: Cushing syndrome, sexual precocity, and polyostotic fibrous dysplasia (Albright syndrome) in infancy. J Pediatr 1975;87:917-921.
Grabias SL, Campbell CJ: Fibrous dysplasia. Orthop Clin North Am 1977;8:771-783.
Question 90
What is the most common malignant bone tumor seen in patients with multiple hereditary exostosis?
Explanation
REFERENCES: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1660-1669.
Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Chondrosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 275-286.
Question 91
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management? Review Topic
Explanation
Question 92
An 18-year-old man sustained closed humeral shaft and forearm fractures of his dominant arm in a motor vehicle accident. Neurovascular examination is intact, and his condition is stable. The best course of action for management of the injuries should be
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Bell MJ, Beachamp CG, Kellam JK, McMurtry RY: The results of plating humeral shaft fractures in patients with multiple injuries: The Sunnybrook experience. J Bone Joint Surg Br 1985;67:293-296.
Question 93
A 14-year-old boy has an asymptomatic mass on the right arm. MRI scans and biopsy specimens are shown in Figures 51a through 51d. Immunostaining is positive for desmin. Additional staging studies should include
Explanation
REFERENCES: Lawrence W, Jr., Hays DM, Heyn R, Tefft M, Crist W, Beltangady M, et al: Lymphatic metastases with childhood rhabdomyosarcoma: A report from the Intergroup Rhabdomyosarcoma Study. Cancer 1987;60:910-915.
Schleiermacher G, Peter M, Oberlin O, et al: Increased risk of systemic relapses associated with bone marrow micrometastasis and circulating tumor cells in localized ewing tumor. J Clin Oncol 2003;21:85-91.
Question 94
A 70-year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single-compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease of the knee.
Question 95
Which of the following factors has been shown to increase mortality in poly-trauma patients with severe head injuries?

Explanation
Chesnut et al demonstrated that hypotension (SBP <90mmHg) was profoundly detrimental, occurring in 35% of these patients and associated with 150% increase in mortality.
Pietropaoli et al reviewed 53 patients with severe head injuries and required early surgical intervention (surgery within 72 hours of injury). All patients were initially normotensive on arrival. There were 17 patients (32%) who developed intra-operative hypotension and 36 (68%) who remained normotensive throughout surgery. The mortality rate was 82% in the IH group and 25% in the normotensive group.
Question 96
A 74-year-old patient is seen for follow-up 6 weeks after undergoing a total shoulder arthroplasty for glenohumeral osteoarthritis. The patient missed the 2-week follow-up appointment and is currently wearing a sling. The incision is well healed with no signs of breakdown. Examination reveals that passive range of motion is forward elevation of 90 degrees, external rotation at the side 0 degrees, and internal rotation up the back is to the level of the greater trochanter. A radiograph shows no signs of fracture or dislocation. What is the next most appropriate management for this patient? Review Topic
Explanation
Question 97
- A 50-year-old alcoholic man has erythema and swelling in his entire dominant upper extremity. He has a WBC of 15,000/mm3, a temp of 101 oF (38.3 oC), and a blood pressure of 90/60 mm Hg. After hemodynamic stabilization, the cellulitic forearm is longitudinally incised dorsally and volarly. The forearm muscles are normal in appearance; however, the subcutaneous fat is necrotic. A culture will most likely reveal
Explanation
Question 98
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time? Review Topic
Explanation
Question 99
03 Which of the following findings is the best indication for the use of temporary external fixation of a femoral shaft fracture?

Explanation

These days, femoral shaft fractures at Tulane / Charity are commonly encountered by orthopaedic residents on the night-float team.
Despite the presence of a well-rested 4th year surgeon, definitive orthopaedic fixation is not always the correct answer for each trauma patient.

Tulane defines “Orthopaedic Tunnel Vision” as a condition commonly associated with a young MD at the Bulldog without a proper wing-man, trying to make advances on the wrong patron due to his relatively easy 80-hour work week schedule and a few too many refined hops.

Skeletal Trauma (p. 1967) describes “Orthopaedic Tunnel Vision” as looking at the orthopaedic injury without considering the patient’s injury in general. Femoral shaft fractures are typically high energy injuries which often do not occur in isolation. In these fractures, it is particularly important to not have tunnel vision.

Indications for temporary bridging external fixation includes hemodynamic instability
(ans. 2), acidosis, hypothermjia, hypoxemia, coagulopathy, sepsis or severely contaminated soft tissues that cannot be adequately debrided. Definitive fixation is performed after the general surgical and medical issues have resolved.

The other answer choices, including the type IIIA open fracture are not contraindications to definitive fixation in themselves (typically IM nailing—antegrade or retrograde).
Question 100
- A 15-year-old dancer who has had brief episodes of back pain over the past 2 years now reports a 3 month history of low back pain and a decreased tolerance for dance. Figure 22a-c show flexion and extension x-rays and CT scan. She reports no leg pain, nor any bowel or bladder difficulties. Management should now consist of
Explanation
