Orthopedic Board Review MCQs: Deformity, Foot, & Fracture | Part 252
Key Takeaway
This interactive MCQ bank, Part 252, is for orthopedic surgeons and residents prepping for OITE and AAOS/ABOS board certification. It offers 100 high-yield, verified questions in official exam formats, focusing on Deformity, Foot, and Fracture. Utilize this resource for comprehensive board review.
About This Board Review Set
This is Part 252 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 252
This module focuses heavily on: Deformity, Foot, Fracture.
Sample Questions from This Set
Sample Question 1: -What is the etiology of this patient’s problem?...
Sample Question 2: Kinematic testing of patellofemoral motion demonstrates that malalignment that produces increased Q angle causes a shift of the patella laterally in the trochlear groove and is most pronounced during what phase of the flexion arc? Review To...
Sample Question 3: A 63-year-old male, with history of myocardial infarction, presents with buttock and leg pain. He states the pain is worse when climbing stairs, and is absent when walking down a hill. He reports when walking on a flat surface the pain begi...
Sample Question 4: What is the most common foot deformity associated with myelomeningocele?...
Sample Question 5: Figures 32a and 32b show the radiographs of a 13-year-old boy who sustained a fracture while playing football 1 week ago. Management at the time of injury included application of a cast and the use of crutches. A follow-up office visit reve...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
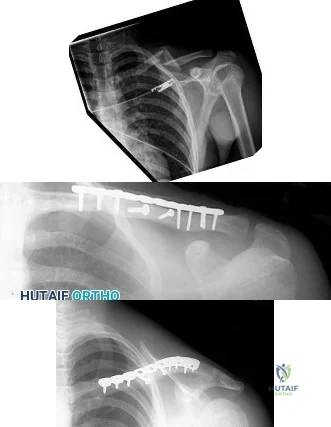
-What is the etiology of this patient’s problem?
Explanation
Little leaguer’s shoulder is an overuse condition of the proximal humeral physis. Patients report diffuse pain that is worse with throwing. Factors that contribute to the condition include excessive throwing,improper throwing mechanics, and muscle-tendon imbalance. Radiographs usually show widening of the proximal humeral physis, and, in more severe cases, metaphyseal demineralization or fragmentation. Surgical fixation is not required for healing. Treatment involves rest until symptoms resolve, followed by initiation of an interval throwing program. Pitching coaches should evaluate throwing mechanics and maintain pitch counts. The dominant shoulders of throwing athletes undergo adaptive changes, resulting in increased external rotation and decreased internal rotation. These changes occur secondary to softtissue and bony adaptations, including increased humeral retroversion. Ischemia has been implicated as a potential cause of osteochondritis dissecans lesions. Rotator cuff tendonitis presents with anterolateral shoulder pain that is worse with activity. Pain is reproduced with resisted supraspinatus testing, and radiograph findings are typically normal.
Adolescent shoulder injuries are often caused by subtle, atraumatic instability most often sustained in sports with overhead movements, including baseball. These symptoms are more likely to occur in athletes with evidence of increased soft-tissue laxity.
Question 2
Kinematic testing of patellofemoral motion demonstrates that malalignment that produces increased Q angle causes a shift of the patella laterally in the trochlear groove and is most pronounced during what phase of the flexion arc? Review Topic
Explanation
Question 3
A 63-year-old male, with history of myocardial infarction, presents with buttock and leg pain. He states the pain is worse when climbing stairs, and is absent when walking down a hill. He reports when walking on a flat surface the pain begins after roughly 50 meters, but if he stops walking and remains standing upright, the pain resolves after a few minutes. He denies any leg pain when sitting and driving a car. These symptoms are most consistent with: Review Topic
Explanation
Vascular claudication refers to the pain, aching or fatigue of the muscles of the buttocks, thigh and/or calf that occurs with exertion, and is related to a failure to meet muscular oxygen requirements, usually caused by peripheral vascular disease impeding blood flow to the peripheral muscles.
Neurogenic claudication is the classic symptom caused by lumbar spinal stenosis. Neurogenic claudication classically presents with bilateral buttock pain with upright activities, but seems to improve by postural changes that flex the lumbar spine. These posture changes are thought to increase the cross sectional area of the central canal, which relieves pressure on the affected area.
Issack et al. reviewed degenerative lumbar spinal stenosis. They state that patients with vascular claudication will have similar symptoms of leg cramping, whether ambulating or riding a stationary bicycle. In comparison, patients with neurogenic
claudication have diminished symptoms of claudication while positioned seated.
Young et al. reviewed the use of lumbar epidural/transforaminal steroids for managing spinal disease. They report that two thirds of acute low back pain episodes resolve within 7 weeks, so the utility and practice patterns regarding the timing and number of epidural/transforaminal steroid injections is usually based on expert opinion, rather than high level research evidence.
Illustration A shows an angiogram of a patients with normal (left) vs abnormal (right) arterial vasculature. Illustration B shows the typical MRI of a patient with spinal stenosis.
Incorrect
Question 4
What is the most common foot deformity associated with myelomeningocele?
Explanation
REFERENCES: Stans AA, Kehl DK: The pediatric foot, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, pp 702-703.
Lindseth RE: Myelomeningocele, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott, Williams & Wilkins, 2001,
pp 622-628.
Question 5
Figures 32a and 32b show the radiographs of a 13-year-old boy who sustained a fracture while playing football 1 week ago. Management at the time of injury included application of a cast and the use of crutches. A follow-up office visit reveals a normal neurologic examination, and the patient reports no discomfort with the cast and crutches. Management should now include
Explanation
REFERENCES: Heinrich SD: Fractures of the shaft of the tibia and fibula, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1340-1346.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 583-595.
Question 6
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, p 1550.
Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 212-214.
Kaplan FS, August CS, Fallon MD, et al: Successful treatment of infantile malignant osteopetrosis by bone-marrow transplantation: A case report. J Bone Joint Surg Am 1988;70:617-623.
Question 7
Failure of posterolateral corner repair or reconstruction of the knee may be associated with which of the following? Review Topic
Explanation
Question 8
An 18-year-old football player has intense pain and is unable to bear weight on the right knee after being tackled from the front. A posterior knee dislocation is reduced on the field. Because the game took place in a remote location, the patient is not examined in the emergency department until 5 hours after the injury. Examination now shows a grossly swollen knee with moderate ischemia in the lower leg. Posterior tibial and dorsalis pedis pulses are diminished. The best course of action should be to
Explanation
REFERENCES: Kremchek TE, Welling RE, Kremchek EJ: Traumatic dislocation of the knee. Orthop Rev 1989;18:1051-1057.
Reckling FW, Peltier LF: Acute knee dislocations and their complications. J Trauma 1969;9:181-191.
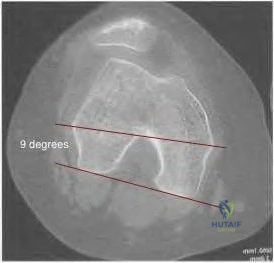
Question 9
98 degrees (range, 0 degrees to 9 degrees). In knees with varus joint lines
Explanation
Question 10
-Which gene mutation is associated with the condition shown in Figures a and b?

Explanation

Question 11
- A 32-year-old has diffuse pain, weakness, and limited overhead motion in the shoulder as a result of falling on his outstretched arm 2 months ago. Examination reveals medial scapular winging, and an electromyogram shows denervation of the long thoracic nerve. Management should consist of
Explanation
Question 12
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient participates in physical therapy for 8 weeks with his team's trainer but notes little improvement. What is the most appropriate next diagnostic step to determine the cause of his pain?

Explanation
used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has important functions for hip stability and maintenance of the suction seal of the joint.
Question 13
Which of the following infectious organisms may be associated with underlying malignancy?
Explanation
REFERENCES: Schaaf RE, Jacobs N, Kelvin FM, et al: Clostridium septicum infection associated with colonic carcinoma and hematologic abnormality. Radiology 1980;137:625-627.
Katlic MR, Derkac WM, Coleman WS: Clostridium septicum infection and malignancy. Ann Surg 1981;193:361-364.
Question 14
What is the effect on knee kinematics following placement of an anterior cruciate ligament (ACL) graft at the 12 o’clock position?
Explanation
REFERENCES: Scopp JM, Jasper LE, Belkoff SM, et al: The effect of oblique femoral tunnel placement on rotational constraint of the knee reconstructed using patellar tendon autografts. Arthroscopy 2004;20:294-299.
Carson EW, Simonian PT, Wickiewicz TL, et al: Revision anterior cruciate ligament reconstruction. Instr Course Lect 1998;47:361-368.
Question 15
A patient has a displaced midshaft transverse fracture of the humerus and is neurologically intact. Following closed reduction and application of a coaptation splint, the patient cannot dorsiflex the wrist or the fingers at the metacarpophalangeal joints of the hand. What is the next most appropriate step in management?
Explanation
REFERENCES: Bostman O, Bakalim G, Vainionpaa S, Wilppula E, Patiala H, Rokkanen P: Radial palsy in shaft fracture of the humerus. Acta Orthop Scand 1986;57:316-319.
Shaz JJ, Bhatti NA: Radial nerve paralysis associated with the fractures of the humerus: A review of 62 cases. Clin Orthop 1983;172:171-176.
Holstein A, Lewis GB: Fractures of the humerus with radial nerve paralysis. J Bone Joint Surg Am 1963;458:1382-1388.
Question 16
A 42-year-old woman has a history of nontraumatic ankle swelling with tenderness over the Achilles tendon and plantar fascia. She reports that while vacationing in Connecticut 2 months ago she noted the presence of a “red bull’s eye” rash. Management should consist of
Explanation
REFERENCES: Neu HC: A perspective on therapy of Lyme infection. Ann NY Acad Sci 1988;539:314-316.
Faller J, Thompson F, Hamilton W: Foot and ankle disorders resulting from Lyme disease. Foot Ankle 1991;11:236-238.
Question 17
A 13-year-old pitcher is hit in the left intercostal space by a line drive ball. He collapses, is apneic and unresponsive, and his radial pulse is absent. What is the next step in management? Review Topic
Explanation
Question 18
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral Review Topic
Explanation
Question 19
During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this athlete be managed? Review Topic
Explanation
Question 20
50%
Explanation
Enneking et al. conducted both radiographic and histologic studies of sixteen massive retrieved human allografts four to sixty-five months after implantation. Analysis of the articular cartilage revealed no evidence that any chondrocytes had survived, even when the graft had been cryoprotected before it was preserved by freezing.
A 64-year-old woman with a longstanding history of rheumatoid arthritis complains of finger dysfunction for the past 6 months. Figure A displays her hand during active extension of all fingers. Figure B displays her hand maintaining her fingers extended following passive extension. What is the next most appropriate treatment for the ring finger?
Spiral oblique retinacular ligament reconstruction
Sagittal band reconstruction
Lateral band reconstruction
Central slip reconstruction
Triangular ligament and transverse retinacular ligament reconstruction
Sagittal band disruption is often associated with rheumatoid arthritis. When this patient attempts to actively extend the affected digit, the extensor tendon
subluxates ulnarly as a result of the sagittal band rupture, and is left with an extensor lag. If one passively extends the finger fully, the patient is able to maintain this position, as the tendon is intact.
Sagittal band reconstruction can be performed with Watson's technique of creating a distally based tendon graft harvested from the central third of the extensor tendon, passed deep to the intermetacarpal ligament and sutured back to itself. Illustration A depicts an intraoperative view of the tendon before reconstruction and Illustration B displays tendon following sagittal band reconstruction. Illustration C displays all of the anatomic locations
of the options listed above.
A splenectomy is performed in a 7-year-old boy following a motor vehicle accident. All of the following are recommended for long-term management EXCEPT:
Pneumococcal vaccination
Haemophilus influenza type B vaccination
Meningococcal group C vaccination
Lifelong prophylactic antibiotics
Hepatitis A vaccination
All of the responses are correct except the need for Hepatitis A vaccine. Hepatitis A is a virus with tropism for hepatocytes which causes infection from fecal-oral contaminated food/water, and shows no increased rate of either infectivity or morbidity in patients with hyposplenism.
Basic recommendations for splenectomized patients include:
All splenectomized patients and those with functional hyposplenism should receive pneumococcal immunization.
Patients not previously immunized should receive haemophilus influenza type B vaccine.
Patients not previously immunized should receive meningococcal group C conjugate vaccine.
Influenza immunization should be given.
Lifelong prophylactic antibiotics are still recommended (oral phenoxymethylpenicillin or erythromycin). This is seemingly despite lack of good data demonstrating a role for lifelong chemoprophylaxis and the acknowledgement that long-term compliance may be problematic.
Davies et al review the current level of evidence supporting these guidelines
for infection prevention in patients with hyposplenism. New to these guidelines are issues regarding occupational exposure and the use of the meningococcal group C and the seven-valent pneumococcal vaccine in non-immunized hyposplenic patients.
Gandhi et al evaluated their nonoperative management of blunt splenic injury in pediatric trauma care. They found compared to historical controls, children with blunt splenic injuries who were hemodynamically stable could be safely monitored with a protocol which required 4 days of inpatient care, 3 weeks of quiet home activities, and 3 months of light activity. This protocol seems to allow for safe return to unrestricted activity.
Incorrect Answer:
Ligaments attach to bone by both direct insertion and indirect insertion. Which of the following most accurately describes the order of the four transition zones of direct insertion?
Ligament > fibrocartilage > mineralized fibrocartilage > bone
Ligament > mineralized fibrocartilage > fibrocartilage > bone
Ligament > mineralized fibrocartilage > periosteum > bone
Ligament > Sharpey's fiber > periosteum > bone
Ligament > periosteum > fibrocartilage > bone
There are two types of tendon/ligament insertion into bone: direct and indirect insertion. The more common, indirect insertion, occurs when the superficial ligament fibers insert into the periosteum. Direct insertion of tendon/ligaments
into bone occurs through a transition of 4 distinct phases: 1) ligament, 2) fibrocartilage, 3) mineralized fibrocartilage, and 4) bone.
While flexing the elbow to perform a biceps curl, what type of muscle contraction is occuring?
Isometric
Isokinetic
Plyometric
Eccentric
Concentric
Concentric muscle contractions occur when a muscle shortens during contraction, as in the upward motion when performing a biceps curl. An eccentric contraction occurs when a muscle lengthens with contraction, as in the "negative" or lowering motion of a biceps curl. An example of an isometric (muscle contracts while maintaining constant length) contraction would be pushing against an immovable object. An example of an isokinetic (muscle has constant speed of contraction) occurs with specialized equipment like Cybex machines. Plyometric contractions occur when a muscle rapidly lengthens just prior to contraction - like during repetitive box jumping.
Woo and Buckwalter describe the mechanisms, barriers, and molecular processes involved in ligament and tendon injury and repair.
A 34-year-old laborer has her left foot crushed in a piece of farming equipment as shown in Figure A. All of the following are reasons for a poor outcome following a crush injury to the foot EXCEPT:
Workers compensation injury
Development of reflex sympathetic dystrophy (complex regional pain syndrome)
Delayed soft-tissue coverage in mangled extremities
Immediate skeletal stabilization
Ongoing litigation
This patient has a mangled extremity. Rigid skeletal stabilization is recommended to enhance soft-tissue healing.
Level 4 evidence from Myerson et al found that delayed soft-tissue coverage in mangled extremities correlated with poor outcome. Poor results also occurred
if treatment was not immediately initiated (immediate debridement shown in Illustration A), if patients subsequently had neuritis or reflex sympathetic dystrophy, or if patients were involved in ongoing workers' compensation and litigation. Neuroischemia following substantial soft-tissue injury likely plays a role in the development of chronic pain after crush injuries to the foot, either through direct trauma to the peripheral nerves or by intraneural or extraneural fibrosis. This trauma to the nerve may cause chronic neuritis, which then triggers a sympathetically mediated reflex sympathetic dystrophy (complex regional pain syndrome).
A 65-year-old man undergoes total knee replacement and is found to have deep vein thrombosis two days later. What molecule is
thought to be involved in this process when it is released during surgical dissection?
Prothrombin
RANKL
IL-1b
Thromboplastin
Factor XI Corrent answer: 4
Thromboplastin is also known more commonly as Tissue Factor (TF), which is involved in the Extrinsic Pathology of the coagulation cascade.
During surgical dissection, insults occur to the endothelial walls of blood vessels. There are three ways in which the body reacts to form a clot so that the patient does not bleed excessively. One is via vessel contraction, another is by collagen release, and a third is by tissue thromboplastin release. Thromboplastin release is part of the extrinsic coagulation pathway (see
Illustration A). Thromboplastin release activates Factor VII which activates Factor X which converts prothrombin to thrombin. Thrombin is the catalyst for converting fibrinogen to fibrin which induces clot formation. While this is useful for decreasing bleeding, it is the same mechanism by which a deep venous thrombosis (DVT) develops.
Which of the following materials has a Young's modulus of elasticity that is most similar to cortical bone
Titanium
Zirconia
Stainless steel
Ceramic (Al2O3)
Alloy (Co-Cr-Mo)
Of the materials listed Titanium has an elastic moduli closest to cortical bone. Titanium is extra-ordinarily light, strong, highly ductile, and corrosion resistant. Titanium is however very notch sensitive and has poor wear resistance.
Young Modulus of Elasticity is defined as the stiffness (ability to maintain
shape under external loading) of a material. On the stress vs. strain curve it is defined as the slope of the line in the elastic zone (see Illustration A). Young’s modulus is constant and different for each material. The relevant moduli (unit GPa) are approximated below:
Question 21
A patient undergoes hip arthroscopy, and the pathology is seen in Figure 18. What is the most likely diagnosis?
Explanation
REFERENCE: Byrd JWT: Operative Hip Arthroscopy. New York, NY, Thieme Medical Publishers, 1998, pp 93-104.
Question 22
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has
Explanation
Question 23
A 19-year-old man has had pain and swelling in his left forearm for the past 8 months. Laboratory studies show a mildly elevated WBC count and erythrocyte sedimentation rate. Radiographs are shown in Figures 58a and 58b, a CT scan is shown in Figure 58c, and T 1 - and T 2 -weighted MRI scans are shown in Figures 58d and 58e, respectively. A biopsy specimen is shown in Figure 58f. Immunohistochemistry demonstrates that the lesion is negative for leukocyte common antigen (CD34). What is the most common cytogenetic translocation associated with this lesion?
Explanation
REFERENCES: Womer R: The cellular biology of bone tumors. Clin Orthop Relat Res 1991;262:12-21.
Yamaguchi U, Hasegawa T, Morimoto Y, et al: A practical approach to the clinical diagnosis of Ewing’s sarcoma/primitive neuroectodermal tumour and other small round cell tumours sharing EWS rearrangement using new fluorescence in situ hybridisation probes for EWSR1 on formalin fixed, paraffin wax embedded tissue. J Clin Pathol 2005;58:1051-1056.
Lazar A, Abruzzo LV, Pollock RE, et al: Molecular diagnosis of sarcomas: Chromosomal translocations in sarcomas. Arch Path Lab Med 2006;130:1199-1207.
Question 24
A year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single- compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease
of the knee.
Question 25
A 22-year-old college baseball pitcher reports the recent onset of anterior and posterosuperior shoulder pain in his throwing shoulder. Examination shows a 15-degree loss of internal rotation, tenderness over the coracoid, and a positive relocation test. Radiographs are normal, and an MRI scan without contrast shows no definitive lesions. A rehabilitation program is prescribed. Which of the following regimens should be initially employed? Review Topic
Explanation
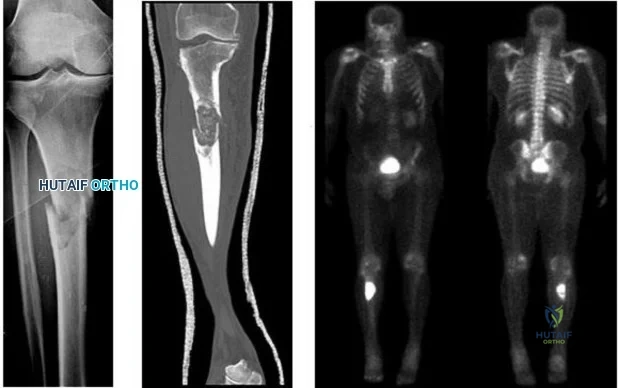
Question 26
A 58-year-old man with a 50-year history of osteomyelitis of the left tibia has a painful ulceration of the anterior lower limb. Figure 1 is the clinical photograph of the wound, which had purulent discharge and an unpleasant odor. Figures 2 and 3 are radiographs of the left tibia. A biopsy reveals malignant degeneration. What are the most likely findings?

Explanation
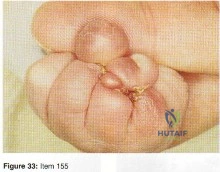
Question 27
Which of the following conditions is most commonly associated with the congenital hand problem shown in Figure 33?
Explanation
Question 28
The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the
Explanation
REFERENCES: Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F: Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577-583.
Moser RP Jr, Madewell JE: An approach to primary bone tumors. Radiol Clin North Am 1987;25:1049-1093.
Question 29
A 43-year-old woman has a 2-week history of right shoulder pain. She denies any injury to initiate her symptoms but states that she has shoulder pain with range of motion and lifting objects. Examination reveals mild pain with abduction, empty can testing, and with the Neer and Hawkins impingement tests. Her range of motion with the right shoulder reveals passive forward flexion to 90 degrees, abduction to 90 degrees, external rotation at the side to 15 degrees, and internal rotation to her buttock. The uninvolved left shoulder has forward flexion to 160 degrees, abduction to 150 degrees, external rotation at the side to 60 degrees, and internal rotation to T6. Radiographs of the shoulder are normal. What is the next most appropriate step in management? Review Topic
Explanation
Question 30
What is the most common complication after distal biceps tendon repair at the elbow?
Explanation
Cain and associates retrospectively reviewed 198 consecutive surgical repairs of the biceps and noted a 36% overall complication rate, including 26% paresthesia of the lateral antebrachial cutaneous nerve, 6% paresthesia of the sensory branch of the radial nerve, 2% superficial infection, 4% injury to the posterior interosseous nerve, 3% symptomatic heterotopic ossification, and 2% rerupture. Grewal and associates randomized 47 patients to have single-incision repair with two suture anchors and 44 patients to have two-incision transosseous suture repair. They reported that the single-incision technique had a higher rate of transient neurapraxia to the lateral antebrachial cutaneous nerve, affecting 19 of 47 in the suture anchor group and three of 43 in the transosseous group. Also, four reruptures occurred, which appeared to be independent of the repair technique. Recordon and associates found only three complications in their series of 46 patients, 19 having endobutton repair and 27 with transosseous suture repair. They reported two injuries to the lateral antebrachial cutaneous nerve and one case of heterotopic ossification. The review by Banerjee and associates showed one rupture of repair (disengagement of the cortical button), two persistent lesions of the superficial branch of the radial nerve, and one symptomatic heterotopic ossification. Co hen remarked that rerupture of the tendon after repair is uncommon in both one-incision and two-incision techniques. Van den Bogaerde and Shin presented a case of posterior interosseous nerve
incarceration with endobutton repair.
Question 31
What mechanism is associated with the spontaneous resorption of herniated nucleus pulposus?
Explanation
REFERENCES: Haro H, Kato T, Kamori H, et al: Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res 2002;20:409-415.
Doita M, Kanatani T, Ozaki T, et al: Influence of macrophage infiltration of herniated disc tissue on the production of matrix metalloproteinases leading to disc resorption. Spine
2001;26:1522-1527.
Question 32
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
REFERENCES: Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
MacDonald SJ, Hersche O, Ganz R: Periacetabular osteotomy in the treatment of neurogenic acetabular dysplasia. J Bone Joint Surg Br 1999;81:975-978.
Question 33
Which of the following is most important to acheive a good outcome following a Syme amputation?

Explanation
Question 34
A displaced pediatric supracondylar humerus fracture is treated with closed manipulation and placement of 2 Kirschner wires placed from the lateral side. What would be the effect of adding a third pin from the lateral side? Review Topic
Explanation
Question 35
A 17-year-old high school football player is seen for follow-up after sustaining an injury 3 days ago. He reports that he tackled a player, felt numbness throughout his body, and could not move for approximately 15 seconds. A spinal cord injury protocol was initiated on the field. Evaluation in the emergency department revealed a normal neurologic examination and full painless neck motion. He states that he has no history of a similar injury. An MRI scan of the cervical spine is normal. During counseling, the patient and his family should be informed that he has sustained
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Odor JM, Watkins RG, Dillin WH, et al: Incidence of cervical spinal stenosis in professional and rookie football players. Am J Sports Med 1990;18:507-509.
Torg JS, Naranja RJ Jr, Palov H, et al: The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football players. J Bone Joint Surg Am 1996;78:1308-1314.
Vaccaro AR, Watkins B, Albert TJ, et al: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-703.
Question 36
A 77-year-old man who underwent right total knee replacement surgery 2 and a half years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3° and 120°. Radiographs show well-fixed and well-aligned implants. What is the most appropriate initial treatment?
Explanation
This patient's history and physical findings are concerning for deep infection. Inflammatory markers, including ESR and CRP, should be obtained first. If the levels are elevated, knee aspiration should be performed for the synovial cell count and culture. A bone scan is not indicated in an initial investigation for deep infection; it is rarely helpful and is not cost effective. CT to assess implant rotation is an appropriate investigation for knee pain when the clinical scenario is not suspicious for a deep infection and when infection has been excluded.
Question 37
A 23-year-old man reports a 6-year history of recurrent instability in the right dominant shoulder. He has not undergone surgery and has essentially stopped all of his sporting activities. On examination, he has instability and apprehension in the midrange of motion (abduction of 45 to 60 degrees with external rotation) and a palpable clunk representing a transient dislocation over the anterior glenoid rim. A three-dimensional CT scan is shown in Figure 31. What is the most appropriate surgical intervention to provide him with reliable stability postoperatively?
Explanation
A bony augmentation procedure such as the Lataijet has been well-described to provide a well functioning and stable shoulder joint. A hemiarthroplasty is not indicated in the absence of arthritis. Subscapularis
advancement will not address the bone loss.
REFERENCES: Hovelius L, Sandstrom B, Sundgren K, et al: One hundred eighteen Bristow-Latarjet repairs for recurrent anterior dislocation of the shoulder prospectively followed for fifteen years: Study I— clinical results. J Shoulder Elbow Surg 2004;13:509-516.
Schroder DT, Provencher MT, Mologne TS, et al: The modified Bristow procedure for anterior shoulder instability: 26-year outcomes in Naval Academy midshipmen. Am J Sports Med 2006;34:778-786.
Itoi E, Lee SB, Berglund LJ, et al: The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: A cadaveric study. J Bone Joint Surg Am 2000;82:35-46.
Question 38
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mm P 3 P and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of
Explanation
REFERENCES: Ring D, Johnston CE II, Wenger DR: Pyogenic infectious spondylitis in children: The convergence of discitis and vertebral osteomyelitis. J Pediatr Orthop
1995;15:652-660.
Crawford AH, Kucharzyk DW, Ruda R, et al: Diskitis in children. Clin Orthop 1991;266:70-79.
Question 39
A 30-year-old man has had severe knee pain and swelling for 1 week. He reports he previously had acromioclavicular joint pain that disappeared. He denies any fever. Aspiration of a cloudy fluid from the knee reveals a WBC count of greater than 50,000 with 90% polymorphonucleocytes. While awaiting culture results, what is the most appropriate action?
Explanation
Question 40
A 74-year-old man underwent a hemiarthroplasty with acromioplasty for rotator cuff tear arthropathy 2 years ago. Despite continued therapy, he is still unable to elevate his arm beyond 40 degrees. Attempted elevation is painful and demonstrates bulging in the anterosuperior aspect of his shoulder. Radiographs show a well-positioned hemiarthroplasty without signs of loosening. What is the most appropriate treatment for this patient? Review Topic
Explanation
Question 41
Based on the findings shown in Figures 22a and 22b, corrective surgery to obtain maximal safe correction and optimal instrumentation fixation should be performed at which of the following locations?
Explanation
REFERENCES: Shufflebarger HL, Clark CE: Thoracolumbar osteotomy for postsurgical sagittal imbalance. Spine 1992;17:S287-S290.
Murrey DB, Brigham CD, Kiebzak GM, et al: Transpedicular decompression and pedicle subtraction osteotomy (eggshell procedure): A retrospective review of 59 patients. Spine 2002;27:2338-2345.
Question 42
A 35-year-old runner has pain beneath the second metatarsophalangeal joint. He reports that he has significantly decreased his running distance since the onset of the pain. He denies any history of trauma or injury to the foot. A radiograph is shown in Figure 14. Initial management should consist of
Explanation
REFERENCES: Trepman E, Yeo SJ: Nonoperative treatment of metatarsophalangeal joint synovitis. Foot Ankle Int 1995;16:771-777.
Mizel MS, Michelson JD: Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint. Foot Ankle Int 1997;18:424-426.
Question 43
- A form of renal osteodystrophy that is characterized by pure osteomalacia is caused by
Explanation
Question 44
A 32-year-old female sustained the injury seen in Figure A after a motor vehicle accident. On physical exam there was obvious deformity about the arm with a laceration that probed to bone over the lateral aspect of the arm. The patient was neurovascularly intact. She was treated with an intramedullary nail. Which of the following is true?

Explanation
Options for operative management of humeral shaft fractures mainly consist of intramedullary nail or plate and screw constructs. The main advantage to intramedullary nailing is when the soft tissue envelope makes a large incision undesireable or the fracture pattern dictates a relative stability construct - such as segmental or massively comminuted injuries. The disadvantages include trauma to the rotator cuff, post operative shoulder pain, indirect reduction leading to increased risk of malrotation, and increased reoperation for implant removal.
Li et al. performed a randomized controlled trial with 45 patients that investigated the difference in post operative malrotation and functional outcomes when comparing intramedullary nails versus open reduction and internal fixation. They concluded that
when comparing the two operative options, patients who underwent intramedullary nailing had a greater degree of malrotation, which was associated with decreased range of motion. Additionally, they found lower functional scores with patients who underwent intramedullary nailing.
Kurup et al. performed a systematic review comparing outcomes between compression plating and intrameduallary nailing for operative treatment of humeral shaft fractures. With a total of 260 patients, they found no difference with blood loss, fracture union, iatrogenic radial nerve palsy, iatrogenic fracture comminution, elbow impingement, return to pre-injury occupation, and functional shoulder scores. They did show a statistically significant increase in shoulder impingement and reduction of range of motion when using an intramedullary nail.
Figure A is a AP radiograph of a comminuted humeral shaft fracture. Illustration A is a radiograph of a humerus fixed with an intramedullary nail. Illustration B is a radiograph of a humerus fixed with a compression plate.
Incorrect Answers:
Question 45
An 18-year-old boxer sustained a blow to his right eye in a boxing match. Examination on the sideline reveals hyphema, reduced visual acuity and color vision, and a visual field cut. What is the next step in management? Review Topic
Explanation
Question 46
A 28-year-old woman undergoes a closing-wedge high tibial osteotomy (HTO) for medial compartment overload after medial meniscectomy. Postsurgically, she reports improvement in her medial pain and resumes normal activities. About 9 months after her surgery, however, she reports burning pain in the front of her knee with running. Her examination reveals no joint line tenderness, mild pain with patellar compression, and limited patellar glides. What is the most likely cause of her symptoms?
Explanation
Question 47
Figures 1 and 2 are the AP and lateral radiographs of a 32-year-old man 10 years after anterior cruciate ligament (ACL) reconstruction. The patient now has worsening medial knee pain and a failed ACL with instability. What is the best surgical option?

Explanation
Question 48
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of
Explanation
REFERENCE: Callahan BC, Georgopoulos G, Eilert RE: Hemivertebral excision for congenital scoliosis. J Pediatr Orthop 1997;17:96-99.
Question 49
Which of the following patients is considered the most appropriate candidate for selective dorsal rhizotomy?
Explanation
REFERENCES: Peacock WJ, Arens LJ, Berman B: Cerebral palsy spasticity: Selective posterior rhizotomy. Pediatr Neurosci 1987;13:61-66.
Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
Mooney JF III, Millis MB: Spinal deformity after selective dorsal rhizotomy in patients with cerebral palsy. Clin Orthop 1999;364:48-52.
Question 50
In the initial evaluation of acute low back pain (duration of less than 4 weeks), plain radiographs are recommended in which of the following situations?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Helfgott SM: Sensible approach to low back pain. Bull Rheum Dis 2001;3:50.
Question 51
A 2-year-old girl was born with the toe deformity shown in Figure 2. She has difficulty wearing shoes despite having adequate room in the toe box. Management at this time should consist of
Explanation
REFERENCES: Hamer AJ, Stanley D, Smith TW: Surgery for curly toe deformity: A double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood. J Bone Joint Surg Br 1984;66:770-771.
Sullivan JA: The child’s foot, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1077-1135.
Question 52
Figures 20a and 20b are the radiographs of a 19-year-old woman who was involved in a motor vehicle accident. What mechanism of injury is most consistent with the injury?

Explanation
Question 53
What is the most common complaint in patients with a developmental radial head dislocation?
Explanation
REFERENCES: Lloyd-Roberts GC, Bucknill TM: Anterior dislocation of the radial head in children-etiology: Natural history and management. J Bone Joint Surg Am 1977;58:402.
Hamilton W, Parks JC II: Isolated dislocation of the radial head without fracture of the ulna. Clin Orthop Relat Res 1973;97:94-96.
Question 54
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?
Explanation
REFERENCES: Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head.
J Shoulder Elbow Surg 2002;11:281-298.
Mansat P, Huser L, Mansat M, et al: Shoulder arthroplasty for atraumatic avascular necrosis of the humeral head: Nineteen shoulders followed up for a mean of seven years. J Shoulder Elbow Surg 2005;14:114-120.
Question 55
Which of the following methods accurately describes the measurement of tip-apex-distance as it relates to placement of a lag screw in the femoral head?

Explanation
TAD is a useful intraoperative indicator of deep and central placement of the lag screw in the femoral head, regardless of whether a nail or a plate is chosen to fix a fracture. A TAD of <25mm has been shown to minimize the risk of fixation cut-out in stable and unstable intertrochanteric hip fractures.
Baumgaertner et al examined factors leading to the failure of sliding hip screws (SHS) in the treatment of 198 intertrochanteric fractures. They determined that the tip-apex distance (TAD) is a reproducible, standard measurement to predict SHS failure. The average TAD for successful fractures was 24mm while the average TAD for failures was 38mm. No screw with a TAD <25mm failed. Calculation of the TAD is shown in Illustration B.
Kyle et al reviewed 622 intertrochanteric fractures. For unstable patterns, a SHS was superior to a fixed angle nail. Early ambulation and weight bearing contributed to improved results
Question 56
Figure 77 shows the clinical photograph of a 21-year-old male ice hockey player who sustained a blow to the jaw from another player’s hockey stick. Examination reveals an unstable jaw, mild bleeding with exposed bone, and malocclusion. What is the most serious acute complication of this injury?
Explanation
The mandible suspends the tongue anteriorly. When the mandible is fractured and the patient is supine, the tongue falls posteriorly and obstructs the airway. Soft-tissue swelling around the injured oronasal structures can also result in a loss of airway patency. Endotracheal or nasotracheal intubation is often impossible and a surgical airway may often have to be created to prevent death by asphyxiation. Other injuries that may require immediate attention include head or cervical spine injury and hemorrhage. A cerebrovascular accident is also less common but is associated with injury to the common carotid artery or its branches. Periodontal disease is generally a long-term complication from dental injuries. Hearing loss is not a common complication of dental and facial trauma.
REFERENCES: Seyfer AE, Hansen JE: Facial trauma, in Moore EF, Feliciano DV, Maddox KL (eds): Trauma, ed 5. New York, NY, McGraw-Hill, 2004, pp 423-444.
Rohrich RJ, Shewmake KB: Evolving concepts of craniomaxillofacial fracture management. Clin Plast
Surg 1992;19:1-10.
Question 57
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
REFERENCES: Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 233-245.
Question 58
A 5-year-old boy has had midfoot pain with activity for the past 3 months. He has no pain at rest. Radiographs are shown in Figures 29a and 29b. Management should consist of
Explanation
REFERENCE: Williams GA, Cowell HR: Koehler’s disease of the tarsal navicular. Clin Orthop 1981;158:53-58.
Question 59
A 66-year-old woman was a restrained passenger in an automobile accident. She sustained a direct blow to her nondominant left hand as the airbag in her automobile deployed and she now reports pain, swelling, and difficulty moving her fingers. Radiographs are shown in Figures 58a and 58b. Appropriate definitive treatment should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 286.
Faraj AA, Davis TR: Percutaneous intramedullary fixation of metacarpal shaft fractures. J Hand Surg Br 1999;24:76-79.
Question 60
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?
Explanation
in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament.
REFERENCES: Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Lemos MJ, Tolo ET: Complications of the treatment of acromioclavicular and sternoclavicular joint injuries, including instability. Clin Sports Med 2003;22:371-385.
Question 61
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
REFERENCES: Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Conn RA, Colfield RH, Byer DE, Lindstromberg JW: Interscalene block anesthesia for shoulder surgery. Clin Orthop 1987;216:94-98.
Question 62
A 19-year-old man has had intermittent progressive knee pain with ambulation and pain at night following a rodeo accident 4 weeks ago. Figures 4a through 4e show the radiographs, a bone scan, CT scan, and T2-weighted MRI scan. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3800-3833.
Question 63
A 72-year-old man was scheduled for left total knee replacement. He has a history of hypertension and deep venous thrombosis (DVT) in his right lower extremity after an ankle fracture 2 years ago that was treated nonsurgically. The patient asked about the recommended types of DVT prophylaxis or investigations. Based on the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty , what is an acceptable option?
Explanation
Question 64
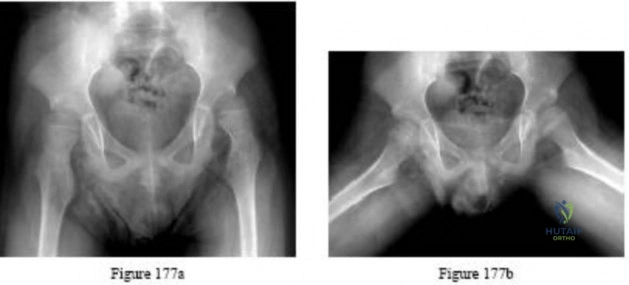
Figures 177a and 177b are the radiographs of a 7-year-old boy with spastic cerebral palsy. He has quadriparetic involvement and is unable to ambulate. He has very limited abduction, 30 degrees of flexion contractures, and pain on abduction. Bilateral varus osteotomies are scheduled with acetabular procedures to improve stability. Which type of acetabular osteotomy should be performed?
Explanation

Question 65
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. The surgical approach for definitive reduction and stabilization of this pattern is

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair,
but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 66
Which of the following associated type acetabular fracture patterns is defined based on the fact that all articular segments are detached from the intact portion of the ilium, which remains attached to the sacrum through the sacroiliac joint?

Explanation
Question 67
Examination of a 10-year-old girl with a hypoplastic breast and atrophic pectoralis major may also reveal which of the following findings?
Explanation
REFERENCES: Wilson MR, Louis DS, Stevenson TR: Poland’s syndrome: Variable expression and associated anomalies. J Hand Surg 1988;13:880-882.
Poland A: Deficiency of the pectoralis muscle. Guys Hosp Rep 1841;6:191.
Question 68
Which nerve root contributes to both the sciatic and femoral nerves?
Explanation
The lumbosacral plexus is formed from the lumbar and sacral roots that are redistributed into the obturator, femoral, and sciatic nerves. The obturator nerve is composed of the L1, L2, and L3 roots. The femoral nerve has contributions from the L3 and L4 roots. The sciatic nerve contains the L4, L5, S1, and lower sacral roots. Therefore, only the L4 root contributes to the femoral and sciatic (via the lumbosacral trunk) nerves, which allows it to innervate the quadriceps and the anterior tibialis muscles.
RECOMMENDED READINGS
Question 69
Figure 16 shows the lateral radiograph of a patient who is scheduled to undergo an anterior cruciate ligament (ACL) reconstruction. If the graft is tensioned at 20° of flexion and the femoral tunnel is created by passing a reamer over the guide wire marked “A,” the resulting ligament reconstruction will excessively
Explanation
REFERENCES: Daniel DM, Fritschy D: Anterior cruciate ligament injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine: Principles and Practice. Philadelphia, PA, WB Saunders, 1994, pp 1313-1360.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
Question 70
Rupture of the structure shown in the axial cross and the sagittal sections in Figures 100a and 100b causes weakness in

Explanation
The structure identified is the distal biceps tendon. Rupture of this tendon causes weakness in both flexion and supination. The biceps tendon does not affect extension or pronation.
RECOMMENDED READINGS
Baker BE, Bierwagen D. Rupture of the distal tendon of the biceps brachii. Operative versus non-operative treatment. J Bone Joint Surg Am. 1985 Mar;67(3):414-7. PubMed PMID: 3972865. View Abstract at PubMed
Mazzocca AD, Spang JT, Arciero RA. Distal biceps rupture. Orthop Clin North Am. 2008 Apr;39(2):237-49, vii. doi: 10.1016/j.ocl.2008.01.001. Review. PubMed PMID: 18374814. View Abstract at PubMed
Question 71
A 5-year-old boy has had pain in the right foot for the past month. Examination reveals tenderness and mild swelling in the region of the tarsal navicular. Radiographs are shown in Figure 30. Management should consist of
Explanation
REFERENCES: Karp M: Kohler’s disease of the tarsal scaphoid. J Bone Joint Surg
1937;19:84-96.
Borges JL, Guille JT, Bowen JR: Kohler’s bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-598.
Question 72
Figure 3a is the initial radiograph of a 19-year-old man who sustained a closed clavicle fracture. Figures 3b and 3c show postoperative radiographs. If the patient had been treated nonsurgically, which of the following would most likely occur?
Explanation
Question 73
A player on a professional football team sustains a knee injury and is diagnosed with an anterior cruciate ligament rupture. When employed as the team physician, your ethical obligation is to inform
Explanation
Question 74
Figure 24 shows the radiograph of an otherwise healthy 56-year-old patient who reports hip pain after undergoing a primary cementless hip replacement 4 months ago. The next most appropriate step should consist of
Explanation
REFERENCE: Fitzgerald RH Jr: Infected total hip arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:249-262.
Question 75
A 47-year-old woman has had a 1-month history of left hip and medial thigh pain that is exacerbated by sitting. Laboratory studies show a total protein level of 8.2 g/dL (normal 6.0 to 8.0) and an immunoglobulin G (IGG) level of 2,130 mg/dL (normal 562 to 1,835). A radiograph, CT scan, and biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 16.
Question 76
Induction coupling stimulates bone growth through all of the following direct effects EXCEPT:
Explanation
In basic science studies, electrical stimulation (i.e. induction coupling), has been shown to promote bone healing via release of growth factors that induce osteoblast differentiation/proliferation. Electrical current can be placed around bone in various ways, creating a current to stimulate growth factor release and subsequent osteoblast proliferation.
Aaron et al. summarized, in a systematic review, the effects of various types of electrical stimulation on bone and bone healing. Regardless of type (i.e. inductive coupling, capacitive coupling, direct current), they report electricity and/or electromagnetic fields promote gene expression of growth factors that promote an osteogenic environment.
Illustration A depicts a cathode placed directly to allograft with a subcutaneously placed electrical stimulator. Illustration B depicts cathodes placed anteriorly and posteriorly around the hip, connected to an outside power source to create the necessary current. Illustration C depicts an inductive coil placed laterally on the skin in order to create an electrical current.
Incorrect answers:
Question 77
Standard guidelines necessitate the use of intraoperative neurophysiological monitoring for patients undergoing surgery for which condition?
Explanation
There are currently no official guidelines on the appropriate use of neuromonitoring in spine surgery. In general, use of neuromonitoring is at surgeon discretion and often is based on the surgeon's perceived risk for neurologic injury during surgery and medicolegal concerns. In most reports,
neuromonitoring is considered useful in cases of deformity correction, spinal cord decompression, instrumentation placement, and revision surgery. However, even for some of these cases, studies have shown limited benefits of neuromonitoring and substantial associated costs.
RECOMMENDED READINGS
Lall RR, Lall RR, Hauptman JS, Munoz C, Cybulski GR, Koski T, Ganju A, Fessler RG, Smith ZA. Intraoperative neurophysiological monitoring in spine surgery: indications, efficacy, and role of the preoperative checklist. Neurosurg Focus. 2012 Nov;33(5):E10. doi: 10.3171/2012.9.FOCUS12235. Review. PubMed PMID: 23116090. View Abstract at PubMed Peeling L, Hentschel S, Fox R, Hall H, Fourney DR. Intraoperative spinal cord and nerve root monitoring: a survey of Canadian spine surgeons. Can J Surg. 2010 Oct;53(5):324-8. PubMed PMID: 20858377. View Abstract at PubMed
Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperative neurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improve patient outcome? Ochsner J. 2014 Spring;14(1):57-61. PubMed PMID: 24688334. View Abstract at PubMed
Question 78
A 6-year-old boy is being treated for acute hematogeneous osteomyelitis of the distal femur with intravenous antibiotics. The best method to determine the success or failure of initial treatment is by serial evaluations of which of the following studies? Review Topic
Explanation
Question 79
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension?
Explanation
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through view, are useful for avoiding this complication.
Question 80
A high school football player asks you about an oral supplement that increases body mass and improves sprint times. He would like to use it to improve performance. What is the most likely agent? Review Topic
Explanation
Question 81
A 25-year-old man has had an insidious onset of left hip pain over the past 11 months. A radiograph, coronal MRI scan, and histopathologic specimens are seen in Figures 2a through 2d. What is the most likely diagnosis?
Explanation
REFERENCE: Sucato DJ, Rougraff B, McGrath BE, et al: Ewing’s sarcoma of the pelvis: Long-term survival and functional outcome. Clin Orthop 2000;373:193-201.
Question 82
..Figures 107a through 107c are the radiograph, CT, and bone scan of a 68-year-old man. While walking, he collapsed and was unable to ambulate because of pain and deformity in his right leg. What is the most appropriate next step?
Explanation
Glomus tumor
Diffuse pigmented villonodular synovitis (PVNS)
Extra-abdominal fibromatosis
Schwannoma
Hemangioma
Please match the characteristics below to the condition listed above.
Question 83
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of
Explanation
REFERENCES: Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Asnis SE, Wanek-Sgaglione L: Intracapsular fractures of the femoral neck: Results of cannulated screw fixation. J Bone Joint Surg 1994;76A:1793-1803.
Question 84
0 mg/L (reference range, 0.08-3.1 mg/L) and erythrocyte sedimentation rate (ESR) is 5 mm/h (reference range, 0-20 mm/h). What is the most appropriate next step in management of the patient?
Explanation
Cryotherapy has been demonstrated to achieve what effect after total knee replacement?
Decreased transfusion requirement
Improved pain, swelling, and analgesia
Improved range of motion at the time of discharge
Better long-term knee range of motion Corrent answer: 3
In a meta-analysis of randomized controlled trials on the efficacy of cryotherapy after total knee arthroplasty, patients treated with cryotherapy had less blood loss but no difference in transfusion requirements. There was better range of motion at the time of discharge from the hospital. There was no improvement in pain, swelling, or analgesia requirements. Patients treated with cryotherapy did not have better long-term range of motion.
Compared to retention of the native patella in primary total knee arthroplasty, routine patella resurfacing is associated with
no patellar complications.
an increased occurrence of anterior knee pain.
a decreased patellar fracture rate.
a decreased risk for revision surgery.
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate in patients with anterior knee pain.
What clinical outcome is associated with total hip replacements that have metal-metal bearings (compared to total hip replacements with metal-polyethylene bearings)?
Soft-tissue sarcomas
Similar revision rates at 5 years
Increased nephrotoxicity
Pseudotumors
Patients with metal-metal total hip bearings have higher levels of cobalt and chromium in the bloodstream, but systemic migration of wear debris from total hip bearings is also common to total hip arthroplasties with polyethylene bearings. There is no direct evidence that patients with metal-metal total hip arthroplasties experience a higher incidence of cancer. Chromosome abnormalities have been detected in patients with metal-metal hip bearings, and the clinical consequences of this finding remain unknown. Also, pseudotumors can form around the periprosthetic joint space in response to localized metal ion debris and the host inflammatory response, although these tumors are not specific for failed metal-metal total hip arthroplasties. Metal-on-metal hip replacements have higher revision rates compared to conventional hip replacements in multiple registry studies. Although metal-on-metal articulations have not been shown to cause renal failure, they are not recommended in patients with chronic renal insufficiency.
A 55-year-old man with unilateral osteoarthritis of the hip underwent a total hip arthroplasty using cementless fixation. The acetabular cup was 52 mm and the femoral head was 28 mm and made of cobalt-chromium alloy. The bearing surface was made of annealed highly cross-linked polyethylene, with an estimated thickness of 6.5 mm. What should the orthopaedic surgeon tell the patient regarding wear of the bearing surface?
A highly cross-linked polyethylene bearing has superior wear characteristics compared to a conventional polyethylene bearing.
A highly cross-linked polyethylene bearing has similar wear characteristics compared to a conventional polyethylene bearing.
The incidence of osteolysis is expected to be higher with highly cross-linked polyethylene than with conventional polyethylene.
The volumetric wear rate would be lower if a 36-mm femoral head were used.
In a prospective, randomized clinical trial of 100 patients undergoing cementless total hip arthroplasties, the investigators compared highly crossed-linked polyethylene to conventional polyethylene. All of the femoral heads were 28 mm. The mean follow-up was 6.8 years. The mean head penetration was 0.003 mm/year for the highly cross-linked polyethylene group in comparison to 0.051 mm/year for the conventional polyethylene group (P =
.006). The improved wear is seen with larger-diameter heads as well. The volumetric wear rate of highly cross-linked polyethylene is equivalent to slightly higher with a larger head than a 28-mm head. Incidence of periarticular osteolysis is lower with highly cross-linked polyethylene.
A 49-year-old active man has groin pain 3 years after undergoing an uneventful total hip replacement using a cobalt-chrome femoral head articulating against a cobalt-chrome acetabular insert. The pain intensifies with activity and travels down his thigh. Examination and radiographic evaluation are not particularly helpful; there is no evidence of spinal or vascular disease. What is the next step in the evaluation of this patient?
A 3-phase bone scan
Measurement of synovial metal ions levels
Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and
possible hip aspiration
Bearing exchange to a metal-polyethylene combination Corrent answer: 3
ESR, CRP, and possible hip aspiration is the most logical next step even though at some point, bearing exchange may emerge as the ultimate treatment for a metal-metal adverse reaction in this patient. But the initial workup of a patient with a painful total hip that was otherwise functioning well must include the differential diagnosis of infection, which must be excluded with an appropriate laboratory workup, clinical history, and hip aspiration. The latter study may also help to diagnose a reaction to the metal bearing; cobalt and chromium levels in the aspirate can be investigated, and the color and quantity of the aspirate can be examined along with the cell count. Serum levels of metal ions at this stage could be both helpful and difficult to interpret.
Figures A and B are the radiographs of a 25-year-old woman whose right knee pain has progressed during the last several years to pain with any activity and pain at night. What is the most appropriate treatment?
Proximal tibial osteotomy
Distal femoral osteotomy
Lateral unicompartmental arthroplasty
Total knee arthroplasty
Arthroscopic partial lateral meniscectomy Corrent answer: 2
This patient is a good candidate for a joint-preserving procedure. Her symptoms and radiographic findings reveal valgus malalignment of the knee with narrowing of the lateral joint space. The alignment can be corrected with a varus-producing distal osteotomy. Most patients do not proceed to knee arthroplasty for at least 10 years after this procedure. Osteotomy is preferred over partial or total knee arthroplasty because of the patient's young age.
Varus proximal tibial osteotomy would result in joint line obliquity.
An orthopaedic surgeon noticed a displaced calcar fracture during stem insertion when performing total hip arthroplasty using cementless fixation. What is the most appropriate course of action?
Intraoperative exploration to determine the extent of the fracture
Use of a longer stem without fixation of the calcar fracture
Complete insertion of the stem and measures to protect the patient against full weight bearing for 4 weeks
Removal of the stem, internal fixation of the fracture, and definitive reconstruction at a later stage after the fracture has healed
Calcar fractures can occur with both cemented and cementless stem fixation during surgery. The distal extent of the fracture must be identified either by direct visualization or intraoperative radiograph prior to fixation or implantation of the femoral component. The recommended treatment is to fix the calcar fracture with cerclage wires/cables to restore the mechanical stability of the femoral metaphysis. The same stem can be inserted successfully. The majority of these fractures unite without adverse stem fixation problems.
A 48-year-old woman had an 8-month history of spontaneous onset of left medial knee pain. She was otherwise healthy with an unremarkable past medical history. Prior to the onset of knee pain, she jogged, played tennis, and golfed regularly. She wished to remain active. Examination showed a fit woman with a BMI of 26, a stable left
knee with full range of motion, and some mild medial joint line tenderness. Radiograph results were normal. An MRI scan showed diffuse grade 3 and a focal area of grade 4 chondromalacia on the medial femoral condyle. The medial meniscus had a degenerative signal but no tear. The remainder of the knee showed no additional pathology. What is the most appropriate initial treatment?
Lateral heel wedge
Low-impact aerobic exercises
Glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day
Arthroscopic debridement and microfracture of the focal area of grade 4 chondromalacia to reduce risk for progression
This patient has early medial compartmental osteoarthritis of her knee. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Non-Arthroplasty), there is Level 1 evidence and an "A" recommendation for the use of low-impact aerobic exercises. The guideline also has "A" recommendations with Level 1 evidence indicating that glucosamine and chondroitin should not be prescribed and that arthroscopic debridement not be performed in the absence of symptoms of a meniscal tear or loose body. Lateral heal wedge is not appropriate; the AAOS guideline provides a "B" recommendation with Level 2 evidence indicating that a lateral heal wedge not be prescribed.
Figure 36 is the postoperative photograph of a patient who underwent a total knee arthroplasty 10 days after surgery. Knee aspiration suggests a Streptococcus infection.

Stop physical therapy and institute oral antibiotics.
Stop physical therapy and institute intravenous (IV) antibiotics.
Open irrigation and debridement, polyethylene spacer exchange, and IV antibiotics
Remove components and insert an antibiotic spacer.
An acute postoperative infection during the first 2 to 4 weeks should be treated with a return to the operating room for open irrigation and debridement of the wound. Polyethylene spacer exchange aides in washing out the entire knee joint. IV antibiotics are also indicated in this situation. To address persistent wound drainage, there is no role for oral or IV antibiotics alone. Removal of the arthroplasty components is recommended for infections after the initial 2- to 4-week postoperative period. However, several recent publications demonstrate a failure rate higher than 50% when the organism is a methicillin-resistant Staphylococcus aureus. Six weeks after surgery, this scenario is no longer considered an acute postoperative infection, and most authors recommend a 2-stage protocol with removal of components and placement of an antibiotic-impregnated cement spacer and 4 to 6 weeks of IV antibiotics.
What is the difference in outcome when comparing high tibial osteotomy (HTO) to total knee arthroplasty (TKA)?
TKA has a longer recovery period than HTO.
HTO provides more complete pain relief than TKA.
HTO is more reliable in older patients than TKA.
HTO outcomes among thin, active, young patients who undergo this procedure approach outcomes associated with TKA.
The ideal candidate for HTO is a thin, active person with a stable knee, unicompartmental knee symptoms, and age younger than 60. TKA offers a shorter recovery period and more complete pain relief than HTO. TKA is believed to be more reliable than HTO for patients older than age 60.
Figure 39 is a radiograph of a 72-year-old man who underwent an open reduction and internal fixation of a right femoral neck fracture. After 3 months he started to develop pain, and during the next 8 months he complained of progressive pain and shortening of the hip. What is the most appropriate treatment?

Girdlestone
Total hip replacement
Hardware removal
Hardware removal with revision open reductions and internal fixation Corrent answer: 2
Even though a relatively short amount of time has passed since the index surgery, this patient has developed significant osteonecrosis that has caused collapse of the bony structures and the hardware prominent. Total hip replacement gives the most efficient pain relief. Hardware removal with or without re-reduction does not provide reliable pain relief. A girdlestone does not allow the patient to function.
Figure 40 is the radiograph of a 68-year-old woman who has right knee pain that is limiting her activity and severe preoperative valgus deformity. During total knee arthroplasty, what pathologic features are typically encountered?

Lateral femoral hypoplasia
Internal rotation of the tibia relative to the femur
Medial patella tracking
Tight medial collateral ligament Corrent answer: 1
In patients with severe valgus deformity, problems frequently encountered include loose or attenuated medial collateral ligament, tight lateral retinaculum and lateral ligamentous structures (lateral collateral, posterolateral corner), atrophic lateral femoral condyle, lateral patella tracking, and external rotation of the tibia relative to the femur. The hypoplastic lateral condyle can cause internal rotation of the anteroposterior cutting block if the posterior condyler line is used for rotational alignment. The medial soft tissues are typically attenuated and stretched.
A 59-year-old active woman underwent elective total hip replacement using a posterior approach. She had minimal pain and was discharged to home 2 days after surgery. Four weeks later she dislocated her hip while shaving her legs. She underwent a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Observation and patient education regarding hip dislocation precautions
Revision to a larger-diameter femoral head
Revision to a constrained acetabular component
Application of a hip orthosis for 3 months Corrent answer: 1
First-time early dislocations are often successfully treated without revision surgery, especially when there is no component malalignment. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful, but is usually reserved for patients with recurrent dislocations.
Patellar pain, subluxation, or dislocation after total knee arthroplasty can result from which of the following component orientations?
Internal rotation of the tibial component
Lateralization of the tibial component
Lateralization of the femoral component
External rotation of the femoral component Corrent answer: 1
Internal rotation of the components of a total knee arthroplasty, both the tibial and femoral components, can lead to symptoms ranging from patellar pain to dislocation. Most researchers agree that proper external rotation of the femoral component is parallel or nearly so to the femoral epicondylar axis with the knee in the 90-degree flexed position. Proper rotational positioning of the tibial component places the midportion of the tibial component rotationally aligned within the medial one-third of the tibial tubercle. Internal rotation of the tibial component causes relative lateralization of the tibial tubercle and the extensor mechanism. Lateralization of the femoral component moves the trochlear groove laterally. Lateralization of the tibial component moves the tibial tubercle medially, which may be beneficial to patellar tracking.
How does the risk for periprosthetic infection after total knee arthroplasty compare to risk for infection after total hip arthroplasty?
Higher in primary arthroplasty
Lower in primary arthroplasty
Lower in revision arthroplasty
Equivalent in both primary and revision arthroplasty Corrent answer: 1
Risk for periprosthetic infection is higher in the knee (1%-2%) than it is in the hip (0.3%-1.3%). The risk for infection is higher after revision joint replacement surgery compared to primary joint replacement surgery.
Osteoarthritis is not associated with a higher risk for periprosthetic infection, but certain inflammatory conditions such as rheumatoid arthritis and psoriatic arthritis place patients at higher risk for postoperative infection.
What factor is associated with a higher risk for dislocation after total hip arthroplasty?
Male gender
Previous hip surgery
A direct lateral surgical approach
Metal-on-metal bearing surfaces Corrent answer: 2
Dislocation after total hip arthroplasty is a multifactorial problem. Numerous risk factors may act independently or cumulatively to increase risk for this complication. Previous hip surgery of any kind is associated with a twofold increased risk for dislocation. Other risk factors include female gender, impaired mental status, inflammatory arthritis, and older age. Numerous studies have shown a lower dislocation rate with a direct lateral approach, although surgical techniques such as capsular repair have significantly lowered the incidence of dislocation after using the posterior approach. Metal-on-metal bearings have been associated with other complications such as adverse tissue reactions but are often used with larger-diameter bearings, which pose lower risk for dislocation.
What surgical technique has been associated with increased risk for recurrent dislocation after revision total hip arthroplasty?
Posterior capsulorrhaphy
Use of a jumbo cup
Use of a lateralized liner
Use of a larger femoral head diameter Corrent answer: 2
When addressing recurrent dislocation after total hip arthroplasty, surgical considerations that must be addressed include approach, soft-tissue tension, component positioning, impingement, head size, and acetabular liner profile. These considerations most often involve tensioning or augmentation of soft tissues, as in capsulorrhaphy or trochanteric advancement; correction of malpositioned components; use of larger femoral head sizes that increase motion before impingement; improving the head-to-neck ratio; and increasing femoral offset. The use of a larger-diameter acetabular component may lead to soft-tissue overgrowth around the liner, causing impingement and increasing the risk for recurrent dislocation.
A 67-year-old active man returns for routine follow up 12 years after hip replacement. He has no hip pain. Radiographs revealed a
well-circumscribed osteolytic lesion around a single acetabular screw. All hip components were perfectly positioned. Six months later, comparison radiographs show an increase in the size of the osteolytic lesion. A CT scan shows a well-described lesion that is 3 cm at its largest diameter and is localized around 1 screw hole with an eccentric femoral head. What treatment is appropriate, assuming well-fixed cementless total hip components exist?
Revision of the polyethylene liner, removal of the screw, and debridement of the osteolytic lesion with or without bone grafting
Revision of the acetabular component to a newer design without screws
Removal of the screw, revision of the polyethylene liner, and stem cell injection into the lytic lesion
Removal of the offending screw from the metal socket and placement of a new polyethylene liner in the existing socket
With a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected with liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings during revision surgery. Here, complete cup revision is not warranted considering the appropriate implant position. Beaule and associates reviewed 83 consecutive patients (90 hips) in which a well-fixed acetabular component was retained in clinical scenarios such as the one described; no hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, or if the osteolytic lesion is not amenable to debridement through the screw hole, acetabular component revision may be indicated.
What has been identified as a risk factor for total knee arthroplasty failure after previous high tibial osteotomy?
Body mass index higher than 35
Female gender
Preoperative stiffness
Advanced age
Increased weight, male gender, young age at the time of total knee arthroplasty, laxity, and limb malalignment preoperatively have been identified
as risk factors for early failure for total knee arthroplasty following high tibial osteotomy.
You are caring for an 18-year-old boy with severe hip arthritis and pain from a missed slipped capital femoral epiphysis. You decide that a hip arthrodesis is the best treatment option. What is the optimum position for a hip arthrodesis to maximize function and prevent complications?
0° external rotation, 0° adduction, 0° hip flexion
5° external rotation, 5° adduction, 20° hip flexion
5° external rotation, 15° abduction, 5° hip flexion
15° external rotation, 0° adduction, 20° hip flexion
15° external rotation, 15° abduction, 5° hip flexion
Hip arthrodesis is a salvage procedure for patients with hip arthritis without ipsilateral knee, contralateral hip, or lumbar spine pathology. The optimal position for hip arthrodesis is 5 degrees of adduction, 5-10 degrees of external rotation, and 20-35 degrees of hip flexion.
In their review, Beaule et al. discuss the current indications and techniques regarding hip arthrodesis including appropriate leg position, surgical techniques, methods to optimize function, and later conversion to hip arthroplasty.
Callaghan et al. evaluated the long term efficacy (20-25 yrs) of hip arthrodesis. They found the onset of ipsilateral knee, contralateral hip, or lumbar spine pathology usually began 20 years after the arthrodesis. Of their patients, they found a 15% rate of conversion to hip arthroplasty by 20 years.
What limits indications for the use of constrained liners?
Association with periprosthetic fracture
Technical difficulty associated with insertion
High costs associated with their use
High failure rates associated with their use Corrent answer: 4
Because of reports of relatively high failure rates associated with constrained liners, indications are limited to continued instability after appropriate component position or deficient abductor mechanism and instability. Neither cost nor technical insertion issues are relevant with regard to indications for use. Periprosthetic fractures are not associated with constrained liner usage.
What serum inflammatory marker has the highest correlation with periprosthetic joint infection?
C-reactive protein
Serum white blood cell count
Erythrocyte sedimentation rate
Interleukin 6 (IL-6)
Although CRP and ESR can be elevated in the setting of infection, IL-6 has been shown to have the highest correlation with infection. Serum white blood cell count has been shown to be ineffective in correlating with periprosthetic joint infection.
A 68-year-old man reports hip pain 15 years after successful cementless total hip arthroplasty. Radiographs show 3 mm of linear wear of the modular acetabular liner and a retro-acetabular osteolytic lesion. Both the titanium femoral and acetabular components appear to be well fixed. The orthopaedic surgeon recommends revision of the acetabular liner and femoral head. This patient is at increased risk for
dislocation.
periprosthetic fracture.
infection.
progressive osteolysis.
Isolated acetabular liner revision is frequently performed in cases of liner wear and periprosthetic osteolysis in the absence of acetabular component loosening. Many reports have documented an increased incidence of dislocation following this type of revision surgery. This dislocation rate can be reduced by using a larger-diameter femoral head at the time of revision. If the
acetabular component is loose or malpositioned, it should be revised. If the locking mechanism is damaged, then a replacement liner may be cemented into the well-fixed shell. Numerous studies have shown that many osteolytic lesions will reduce in size or heal without bone grafting, and removal of the source of wear debris will arrest the progression of osteolysis. The risk for periprosthetic fracture and infection are lower than risk for dislocation in this setting.
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day.
weight loss through dietary management and low-impact aerobic exercises.
arthroscopic debridement and lavage.
a valgus-directing brace.
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Non-Arthroplasty), Level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1500 mg/day and chondroitin sulfate 800 mg/day and arthroscopic debridement and lavage).
The range of knee mobility after total knee replacement is multifactorial and dependent upon implant design, surgical implantation accuracy, and patient-specific variables. What total knee implant design is associated with the most knee flexion after total knee replacement?
Highly conforming articular surface geometry
Higher-flexion femoral component design manufactured to allow the most knee flexion
Posterior cruciate-stabilized implant, with or without a higher flexion
manufacturing modification
Posterior cruciate-retaining design with a mobile bearing, custom implanted based on CT scan data
A posterior cruciate-stabilized implant has the best support in the literature in terms of the most favorable range of motion after knee arthroplasty, regardless of whether the femoral component is designed with a higher flexion variation. The higher flexion design is a manufacturing variation that is intended to increase motion by clearing the posterior condyles in flexion.
Although the knee may not gain more flexion, this design allows for more safety in deep flexion. The long-term outcomes of increased stresses on the polyethylene are not known, however. By itself, a higher-flexion design does not lead to increased knee mobility. The effects of mobile bearings, custom CT scan-based knee implantation, and highly conforming designs on ultimate knee range of motion are uncertain.
In total knee arthroplasty, in vitro testing has shown that crosslinking can diminish the rate of polyethylene wear by 30% to 80%.
What other change in material properties is possible when polyethylene is highly cross-linked?
Increased ductility
Increased wettability
Diminished fatigue strength
Decreased resistance to abrasive wear Corrent answer: 3
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been identified as causing implant failure in most recent clinical trials, but remain the most important mechanical issues associated with current material processing methods.
What factor is associated with a high risk for developing pseudotumors after metal-on-metal hip resurfacing?
Large-diameter components
Age 40 or older for men
Age 40 or younger for women
Diagnosis of primary osteoarthritis Corrent answer: 3
The recent experience of a large clinical cohort revealed the most likely risk factors as female gender, age younger than 40, small components, and the diagnosis of hip dysplasia causing osteoarthritis. Failure was least likely among men and procedures involving larger components. These data have prompted some authors to caution against use in women and to primarily target candidates who are men younger than age 50. Small components may be more prone to failure because of malpositioning and edge loading, which have been noted to be more common in dysplasia cases.
A 70-year-old man is scheduled to undergo bearing surface revision for wear and osteolysis 10 years after cementless total hip arthroplasty. The femoral head is 28 mm alumina-oxide ceramic material. The components are in good position, and there is no evidence of fixation loosening of either component by radiograph or preoperative bone scan. What outcome is associated with isolated polyethylene exchange?
Reduced risk for future wear and osteolysis with a larger femoral head
Reduced risk for future wear and osteolysis with a cobalt chrome femoral head
Similar risk for dislocation compared to primary total hip arthroplasty
Increased risk for dislocation compared to primary total hip arthroplasty Corrent answer: 4
The major complication associated with polyethylene exchange is postoperative dislocation. Maloney and associates noted a dislocation rate of 11% in a study of 35 hips after such revision. Boucher and associates reported a 25% rate of dislocation in a study of 25 patients. Larger femoral heads result in higher volumetric wear in contrast to smaller-diameter heads. Stem revision is not indicated because there is no fixation loosening. Moreover, stem biomaterial has no effect on polyethylene wear.
A healthy, active 68-year-old woman had a total hip arthroplasty 3 months ago. She has been to the emergency department with a posterior dislocation 3 times during the last 2 months. Plain radiographs and a CT scan confirm that the acetabular component is oriented in 5 degrees of retroversion and 55 degrees of abduction.
What is the most appropriate treatment?
Revision of the femoral and acetabular components
Maximizing head-neck ratio and increasing head length
Acetabular component revision
Closed reduction with an abduction brace and reinforcement of hip precautions
Acetabular malposition can lead to recurrent instability. When this cause is confirmed, reorientation of the component can lead to successful revision surgery. Revision of the femoral component may not be necessary if the acetabular component is repositioned. Increasing length and maximizing head-neck ratio cannot make up for component malposition. There is no role for nonsurgical treatment in the setting of recurrent instability with component malposition in an active, healthy patient.
A 55-year-old woman with history of HIV infection is scheduled for revision total knee arthroplasty to address instability. The index surgery was done 3 years ago. What is the white blood cell (WBC) count threshold in the synovial fluid for an infection diagnosis?
Question 85
Figures 11a and 11b show the T2-weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a? Review Topic
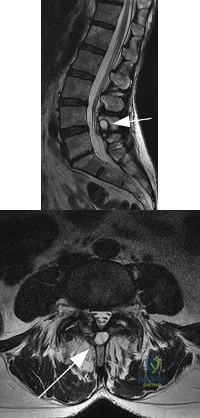
Explanation
Question 86
Figure 33 shows the MRI scan of a 55-year-old woman who has had a 6-week history of back and leg pain. Which of the following clinical scenarios is most consistent with the MRI scan findings at L4-L5? Review Topic
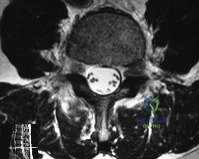
Explanation
Question 87
A 62-year-old active man returns for routine follow-up 16 years after hip replacement. He has no hip pain. Radiographs reveal a well-circumscribed osteolytic lesion around a single acetabular screw. All hip components are perfectly positioned. Comparison radiographs obtained 6 months later show an increase in the size of the osteolytic lesion. CT depicts a well-described lesion that is 3 cm at its largest diameter and is localized around one screw hole with an eccentric femoral head. What treatment is appropriate, assuming that well-fixed cementless total hip components are in place?
Explanation
Given a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected from liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings arise during revision surgery. Here, complete cup revision is not warranted, considering the appropriate implant position. Beaulé and associates reviewed 83 consecutive patients (90 hips) in whom a well-fixed acetabular component was retained in a clinical scenario such as the one described. No hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, acetabular component revision may be indicated.
Question 88
A 72-year-old woman falls onto her left hip after tripping over a curb during her daily 3-mile walk. An injury radiograph is shown in Figure A. What is the best long term solution?

Explanation
The aims of surgery for FNF in elderly patients are immediate pain relief, rapid mobilization, and low complications and revision. THA has best pain relief, fewer reoperations, best survivorship and is most cost-effective but has longer operative/anesthetic time, blood loss, higher infection rate, and potential instability compared with HA.
Healy and Iorio examined the optimal treatment for elderly FNF. They compared internal fixation (120 patients) with arthroplasty (HA, 43 patients; THA, 23 patients). There was no different in reoperation or mortality rates between the 2 groups, but arthroplasty was more cost effective, had independent living, and longer interval to reoperation/death. THA had less pain, better function, and lower rates of reoperation than HA, and was most cost-effective. They concluded that THA was the best treatment.
Yu et al. performed a meta-analysis of randomized controlled trials to determine whether THA or hemiarthroplasty (HA) was superior. They found that THA had lower risk of reoperation (RR = 0.53), higher risk of dislocation (RR = 1.99), and
higher functional scores at 1 and 4 years. There was no difference in mortality, infection and complication rates.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Question 89
A 65-year-old woman has significant neck pain after falling and striking her head. A radiograph and sagittal CT scan are shown in Figures 23a and 23b. What is the most likely diagnosis?
Explanation
REFERENCES: Rothman RH, Simeone FA (eds): The Spine, ed 4. Philadelphia PA, WB Saunders, 1999, pp 927-937.
Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2003, pp 455-458.
Question 90
A healthy 70-year-old man has a swollen knee after undergoing a knee replacement 10 years ago. Aspiration of the knee reveals cloudy, viscous synovial fluid. Laboratory studies show an erythrocyte sedimentation rate of 10 mm/h and a C-reactive protein level of less than 0.5. What is the most likely diagnosis?
Explanation
REFERENCE: Barrack RL, Jennings RW, Wolfe MW, Bertot AJ: The value of preoperative aspiration before total knee revision. Clin Orthop 1997;345:8-16.
Question 91
Figure 19 shows the radiograph of a 45-year-old woman who has a painful nonunion. Treatment should consist of
Explanation
REFERENCES: Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Koval KJ, Zuckerman JD: Intertrochanteric fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1635-1681.
Question 92
A 28-year-old woman fell on her right wrist while rollerblading 2 days ago. She was seen in the emergency department at the time of injury and was told she had a sprain. Examination now reveals dorsal tenderness in the proximal wrist but no snuffbox or ulnar tenderness. Standard wrist radiographs are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Walsh JJ, Berger RA, Cooney WP: Current status of scapholunate interosseous ligament injuries. J Am Acad Orthop Surg 2002;10:32-42.
Browner BD, Levine AM, Jupiter JB, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1366-1367.
Question 93
A 47-year-old woman underwent a bunionectomy and hallux valgus correction a few years ago. She now has the complication shown in Figures 38a and 38b. She has no pain with motion of the metatarsophalangeal or interphalangeal joints. What is the best reconstructive option in this setting?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 27-32.
Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 345-351.
Question 94
- The radiograph shown in Figure 50a and the CT scan shown in Figure 50b reveal a lesion in the left femoral neck of a 12-year-old boy who has pain in the left hip. The most likely cause of the osteopenia of the left proximal femur is
Explanation
Question 95
A patient who underwent total knee arthroplasty 6 years ago now reports knee pain for the past 3 days following dental surgery. Cultures of the aspirate are positive for Staphylococcus epidermidis. Management should consist of
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337.
Goldman RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
Question 96
What tendon has an intra-articular (instrasynovial) location in the knee joint?
Explanation
REFERENCES: Kimura M, Shirakura K, Hasegawa A, Kobayashi Y, Udagawa E: Anatomy and pathophysiology of the popliteal tendon area in the lateral meniscus: 1. Arthroscopic and anatomical investigation. Arthroscopy 1992;8:419-423.
Arnoczky SP, Skyhar MJ, Wickiewicz TL: Basic science of the knee, in McGinty JB (ed): Operative Arthroscopy. New York, NY, Raven Press, 1991, pp 155-182.
Question 97
A 56-year-old woman has a painful mass on the bottom of her left foot, and orthotic management has failed to provide relief. Examination reveals that the mass is contiguous with the plantar fascia. An MRI scan shows a homogenous nodule within the plantar fascia. Resection of the tumor is shown in the clinical photograph in Figure 39. What type of cell is most likely responsible for the formation of this tumor?
Explanation
REFERENCE: Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 98
When placing a percutaneous retrograde pubic rami screw for fixation of an acetabular fracture, which of the following radiographic views can best ensure that the screw does not exit the posterior aspect of the superior pubic ramus?

Explanation
Question 99
A 7-year-old boy presents to the ED with visible right elbow deformity after a fall on the playground. His injury films are shown in figures A and B. The injury is closed, and there is a palpable radial pulse with a well-perfused hand. He undergoes multiple attempts at closed reduction and percutaneous pinning with 3 lateral pins in the operating room. Final radiographs show some gapping at the fracture site. At the end of the case, the radial pulse is no longer palpable and the hand appears pale. What is the next best step in management? Review Topic

Explanation
The management of supracondylar humerus fractures is dictated significantly by the neurovascular examination. Loss of pulse and a pale, cool hand warrants emergent closed reduction and percutaneous pinning. If the vascular status does not change, open exploration is warranted. When a hand becomes pulseless and cool after reduction, it is typically due to the brachial artery being interposed in the fracture site. Undoing the reduction can often help. If there is still evidence of vascular compromise, open exploration is warranted. A pale (poorly perfused) hand or any change in neurovascular status requires urgent intervention. A pink, pulseless but well perfused hand can be observed.
Carter et al. surveyed over 300 pediatric orthopaedic surgeons on the management of type III supracondylar humerus fractures. They found an increasing trend toward lateral pin configuration and non-emergent delayed treatment.
Abzug et al. reviewed current concepts regarding management of supracondylar humerus fractures. They report an increased trend in surgical management of type II supracondylar humerus fractures. For the pink pulseless hand, they recommend admission for observation and splinting in 45 degrees of flexion.
Babal et al. reviewed nerve injuries in pediatric supracondylar humerus fractures. Anterior interosseous nerve palsy ranks highest, with ulnar nerve palsy highest with flexion type injuries. Medial pinning leads to risk of iatrogenic ulnar nerve injury.
Figures A and B are AP and lateral elbow radiographs showing a Gartland type III supracondylar humerus fracture.
Incorrect Answers:
Question 100
A B Figures 19a and 19b are the CT scans of an 18-year-old man who was a restrained driver in a rollover motor vehicle collision. What was the primary mechanism of injury?
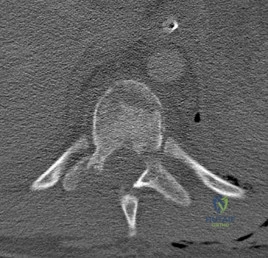
Explanation
This injury pattern represents a flexion distraction injury, or a Chance fracture. The imaging hallmark of this injury is the axial split of the pedicle seen on the sagittal CT scan. This injury necessitates surgical intervention to prevent progressive deformity and pain. A rotation mechanism results in a dislocation with a rotational deformity at the level of injury. An extension force causes failure of the anterior column in tension with compression of the posterior column. An axial load force would result in a burst fracture.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Vaccaro AR, Baron EM, Sanfilippo J, Jacoby S, Steuve J, Grossman E, DiPaola M, Ranier P, Austin L, Ropiak R, Ciminello M, Okafor C, Eichenbaum M, Rapuri V, Smith E, Orozco F, Ugolini P, Fletcher M, Minnich J, Goldberg G, Wilsey J, Lee JY, Lim MR, Burns A, Marino R, DiPaola C, Zeiller L, Zeiler SC, Harrop J, Anderson DG, Albert TJ, Hilibrand AS. Reliability of a novel classification system for thoracolumbar injuries: the Thoracolumbar Injury Severity Score. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S62-9; discussion S104. PubMed PMID:16685239.View Abstract at PubMed
