Orthopedic Board Prep MCQs: Hip, Knee, Spine & Nerve | Part 92

Key Takeaway
This page offers Part 92 of a comprehensive orthopedic surgery board review. It features 100 high-yield, verified MCQs modeled after OITE and AAOS exams. Designed for orthopedic residents and surgeons, this interactive quiz aids in rigorous preparation for board certification through distinct study and exam modes.
About This Board Review Set
This is Part 92 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 92
This module focuses heavily on: Hip, Knee, Nerve.
Sample Questions from This Set
Sample Question 1: A 12-year-old girl has had pain in her right knee for 1 month that started as activity-related and progressed to night pain. Radiographs are shown in Figures 16a and 16b, and a biopsy specimen is shown in Figure 16c. What is the recommended...
Sample Question 2: A 7-year-old girl with spinal muscular atrophy (SMA) type II has popping of the left hip. Examination reveals painless subluxation of the joint in adduction with palpable reduction in abduction. Radiographs show coxa valga, subluxation of t...
Sample Question 3: During an anterior approach to the bicipital53tuberosity, you encounter a nerve overlying the brachioradialis fascia (Figure 58). It provides innervation to the...
Sample Question 4: The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?...
Sample Question 5: A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann’s sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervica...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 12-year-old girl has had pain in her right knee for 1 month that started as activity-related and progressed to night pain. Radiographs are shown in Figures 16a and 16b, and a biopsy specimen is shown in Figure 16c. What is the recommended treatment?
Explanation
REFERENCES: Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 205.
Question 2
A 7-year-old girl with spinal muscular atrophy (SMA) type II has popping of the left hip. Examination reveals painless subluxation of the joint in adduction with palpable reduction in abduction. Radiographs show coxa valga, subluxation of the left hip, and pelvic obliquity with elevation of the left hemipelvis. Treatment should consist of
Explanation
REFERENCES: Sporer SM, Smith BG: Hip dislocation in patients with spinal muscular atrophy. J Pediatr Orthop 2003;23:10-14.
Thompson CE, Larsen LJ: Recurrent hip dislocation in intermediate spinal atrophy.
J Pediatr Orthop 1990;10:638-641.
Question 3
During an anterior approach to the bicipital 53 tuberosity, you encounter a nerve overlying the brachioradialis fascia (Figure 58). It provides innervation to the

Explanation
The structure shown is the lateral antebrachial cutaneous nerve (LABC). It is the terminal sensory branch of the musculocutaneous nerve and runs superficial to the brachioradialis. It supplies sensation to the anterolateral surface of the forearm. The flexor pollicis longus is innervated by the anterior interosseous nerve. The extensor indicis proprius is innervated by the radial nerve. The LABC does not innervate the skin of the anteromedial forearm. Careful
identification and protection of this nerve is critical to prevent the most common nerve injury during distal biceps repair.
RECOMMENDED READINGS
Agur AM. Grant's Atlas of Human Anatomy. 10th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:460.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1994:118-125.
RESPONSES FOR QUESTIONS 59 THROUGH 61

Please select the image that represents the most appropriate response to the question or statement below.
Question 4
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?
Explanation
REFERENCES: Wiesel SW, Rothman RH: Occipito-atlantal hypermobility.
Spine 1979;4:187-191.
Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 50-51.
Question 5
A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann’s sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervical kyphosis in the neutral position, with restoration of lordosis on extension. Which of the following procedures is most likely to result in poor long-term results?
Explanation
REFERENCES: Albert TJ, Vaccaro A: Postlaminectomy kyphosis. Spine 1998;23:2738-2745.
Truumees E, Herkowitz HN: Cervical spondylotic myelopathy and radiculopthy. Instr Course Lect 2000;49:339-360.
Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 6
A 42-year-old woman with a long-standing history of rheumatoid arthritis undergoes total shoulder arthroplasty for persistent pain that has failed to respond to nonsurgical management. Intraoperative radiographs reveal an oblique, minimally displaced fracture of the greater tuberosity. Based on these findings, what is the best course of action?
Explanation
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 215-225.
Frankle MA, Ondrovic LE, Markee BA, et al: Stability of tuberosity reattachment in proximal humeral hemiarthroplasty. J Shoulder Elbow Surg 2002;11:413-420.
Question 7
What is the typical MRI signal intensity of bone marrow affected by acute osteomyelitis?
Explanation
REFERENCES: Unger E, Moldofsky P, Gatenby R, et al: Diagnosis of osteomyelitis by MR imaging. Am J Roentgenol 1988;150:605-610.
Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 150-163.
Question 8
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of
Explanation
50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann’s kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann’s kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees.
REFERENCES: Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248.
Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
Tribus CB: Scheuermann’s kyphosis in adolescents and adults: Diagnosis and management.
J Am Acad Orthop Surg 1998;6:36-43.
Question 9
A 24-year-old man who was involved in a high speed motor vehicle accident is transferred for definitive care after having been diagnosed with an acute spinal cord injury from a fracture-dislocation at C6-7. He has a complete C6 neurologic level and it is now approximately 10 hours from his injury. What is the most appropriate pharmacologic treatment at this time?
Explanation
48 hours. In this patient, who is outside the 8-hour treatment window, no studies have supported starting the methylprednisolone protocol at this time.
REFERENCES: Braken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Kwon BK, Tetzlaff W, Grauer JN, et al: Pathophysiology and pharmacologic treatment of acute spinal cord injury. Spine J 2004;4:451-464.
Question 10
A 42-year-old man who is right-hand dominant injured his right shoulder when he fell from a ladder onto his outstretched arm 1 hour ago. Radiographs reveal a two-part greater tuberosity anterior fracture-dislocation. Initial management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Flatow EL, Cuomo F, Maday MG, Miller SR, McIlveen SJ, Bigliani LU: Open reduction and internal fixation of two-part displaced fractures of the greater tuberosity of the proximal part of the humerus. J Bone Joint Surg Am 1991;73:1213-1218.
Question 11
An AP radiograph of the pelvis is shown in Figure 4. What muscle attaches to the avulsed fragment of bone identified by the arrow?
Explanation
REFERENCES: Woodburne RT (ed): Essentials of Human Anatomy. New York, NY, Oxford University Press, 1978, pp 542-545.
Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 12
The cortical injury to the posterolateral distal fibula shown in Figure 25 indicates involvement of which of the following structures?
Explanation
REFERENCES: Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Clanton TO: Athletic injuries to the soft tissues of the foot and ankle, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1090-1209.
Question 13
When performing the exposure for an anterior approach to the cervical spine, excessive retraction of the trachea and esophagus should be avoided to prevent injury of the
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, chapter 2.
Flynn TB: Neurologic complication of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 14
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain.What is the most likely cause of this patient's pain?
Explanation
Question 15
Tension band wire fixation is best indicated for which of the following types of olecranon fractures?
Explanation
Question 16
In articular cartilage, Interleukin 1 (IL-1) increases
Explanation
Question 17
03 A 28-year-old man underwent surgical fixation for an intra-articular distal humeral fracture 8 weeks ago now reports progressively restricted elbow motion. Radiographs at the time of union are shown in Figures 13a and 13b. Management should now consist of
Explanation
delayed until the heterotopic ossification was “mature”. This was signified by a cold bone scan and normal serum alk phos, as well as a mature appearance on xray. It was thought that by waiting until the HO was mature, recurrence would be avoided. However, in the cited reference, out of the widely read Journal of Hand Surgery, the authors obtained good results with increased range of motion, resolution of cubital tunnel syndrome and no recurrence of contractures or loss of motion with excision of ectopic bone and elbow release that was performed once bony union of fracture was obtained. They also used a 5 day course of indomethacin post-op.
back to this question next question
Question 18
Figures 51a and 51b show the AP and lateral radiographs of the elbow of a 26-year-old man who fell. Closed reduction was performed in the emergency department, and management consisted of immobilization for 3 weeks prior to the initiation of motion. At 12 weeks after injury, he reports continued feelings of instability and catching in his elbow when using his arms to rise from a chair. Which of the following procedures needs to be performed, at a minimum, to reestablish stability of the elbow? Review Topic

Explanation
Question 19
A 63-year-old male, with history of myocardial infarction, presents with buttock and leg pain. He states the pain is worse when climbing stairs, and is absent when walking down a hill. He reports when walking on a flat surface the pain begins after roughly 50 meters, but if he stops walking and remains standing upright, the pain resolves after a few minutes. He denies any leg pain when sitting and driving a car. These symptoms are most consistent with: Review Topic
Explanation
Vascular claudication refers to the pain, aching or fatigue of the muscles of the buttocks, thigh and/or calf that occurs with exertion, and is related to a failure to meet muscular oxygen requirements, usually caused by peripheral vascular disease impeding blood flow to the peripheral muscles.
Neurogenic claudication is the classic symptom caused by lumbar spinal stenosis. Neurogenic claudication classically presents with bilateral buttock pain with upright activities, but seems to improve by postural changes that flex the lumbar spine. These posture changes are thought to increase the cross sectional area of the central canal, which relieves pressure on the affected area.
Issack et al. reviewed degenerative lumbar spinal stenosis. They state that patients with vascular claudication will have similar symptoms of leg cramping, whether ambulating or riding a stationary bicycle. In comparison, patients with neurogenic
claudication have diminished symptoms of claudication while positioned seated.
Young et al. reviewed the use of lumbar epidural/transforaminal steroids for managing spinal disease. They report that two thirds of acute low back pain episodes resolve within 7 weeks, so the utility and practice patterns regarding the timing and number of epidural/transforaminal steroid injections is usually based on expert opinion, rather than high level research evidence.
Illustration A shows an angiogram of a patients with normal (left) vs abnormal (right) arterial vasculature. Illustration B shows the typical MRI of a patient with spinal stenosis.
Incorrect
Question 20
A 23-year-old male college quarterback presents with acute left shoulder pain after being tackled. A radiograph of the injury is shown in figure A. After successful closed reduction, what shoulder position should be avoided in order to minimize the risk of a repeat injury? Review Topic

Explanation
Shoulder stability is achieved through the both dynamic and static stabilizers. The static stabilizers include the bony morphology of the joint, glenoid labrum, capsule, and glenohumeral ligaments. The contributions of the glenohumeral ligaments to shoulder stability are dependent upon the position of the humerus relative to the glenoid. Posterior stability is afforded to the joint by the superior glenohumeral ligament (SGHL) and the posterior band of the inferior glenohumeral ligament (IGHL). The SGHL specifically is taught and provides posterior stability with the shoulder in flexion, adduction, and internal rotation.
Kim et. al. reviewed their experience treating 27 athletes diagnosed with traumatic posterior shoulder instability and treated with arthroscopic posterior labral repair and capsular shift. Most patients were found to have an incompletely stripped posterior capsulolabral complex. After arthroscopic repair and shift, all 26 of the 27 patients treated had improved shoulder function and objective scores, a stable shoulder, and were able to return to sport.
Millett et. al. reviewed posterior shoulder instability. They describe the static restraints of the posterior shoulder as the SGHL, posterior band of IGHL, and the coraohumeral ligament (CHL). The SGHL and CHL are both taught in the position of flexion, adduction, and internal rotation, whereas the posterior band of the IGHL is taught in abduction. They describe posterior instability occuring secondary to overhead sports due to repetitive microtrauma causing gradual capsular failure.
Figure A is an axillary radiograph of the left shoulder demonstrating a posterior dislocation and an engaging reverse Hill-Sachs lesion.
Incorrect Answers:
Question 21
A 15-year-old boy reports feeling a pop and notes sudden giving way of the left knee while playing basketball. He has immediate pain and swelling in the knee. An AP radiograph is shown in Figure 32. A small avulsion fragment from the lateral tibial margin is the only finding. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
Question 22
Where is the most common site for tuberculosis (TB) spondylitis in children? Review Topic
Explanation
Question 23
A 13-year-old girl with adolescent idiopathic scoliosis is otherwise healthy with a normal neurologic examination and she began her menstrual cycle 3 months ago. Standing radiographs show a high left thoracic curve from T1-T6 that measures 29 degrees, a right thoracic curve from T7-L1 that measures 65 degrees, and a left lumbar curve from L1-L5 that measures 31 degrees, correcting to 12, 37, and 10 degrees, respectively, on bending films. Her Risser sign is 1. What is the most appropriate management? Review Topic
Explanation
Question 24
The stiffness of a 16-mm femoral stem is mostly influenced by the
Explanation
REFERENCE: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, p 458.
Question 25
Figures 1 through 4 are the radiographs, sagittal-cut CT scan, and coronal T1 MR image of a 16-year-old boy who has wrist stiffness and pain after sustaining an injury 2 years ago. There is no bleeding from the proximal pole during surgery. Which procedure will most likely result in restoration of alignment and healing?

Explanation
The imaging studies show an established scaphoid waist nonunion with a humpback deformity (significant flexion through the nonunion site) and carpal collapse. In addition, the proximal pole appears sclerotic on the plain radiographs and appears poorly perfused on the MR image. Correction of alignment of this scaphoid nonunion would require a volar approach with a structural bone graft. Additionally, the graft would need to provide a vascular supply to the bone. Both the 1,2 ICSRA (the Zaidenberg graft) and the 4+5 ECA grafts are vascularized grafts from the dorsal distal radius. Neither of these grafts would correct the humpback deformity, and the 4+5 ECA graft pedicle is not long enough to reach the scaphoid. An iliac crest bone graft could be used to correct the deformity, but would not provide an adequate blood supply. A free-vascularized medial femoral condyle graft provides both adequate bone graft to correct the deformity and revascularization of the scaphoid.
Question 26
A 60-year-old man reports that he has had shoe pressure pain over his right great toe for several years but has minimal discomfort when barefoot or in sandals. A clinical photograph and radiographs are shown in Figures 1a through 1c. Management should consist of
Explanation
REFERENCES: Smith RW, Katchis SD, Ayson LC: Outcomes in hallux rigidus patients treated nonoperatively: A long-term follow-up study. Foot Ankle Int 2000;21:906-913.
Shereff MJ, Baumhauer JF: Hallux rigidus and osteoarthrosis of the first metatarsophalangeal joint. J Bone Joint Surg Am 1998;80:898-908.
Question 27
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management? Review Topic
Explanation
Question 28
Figures A and B are radiographic images of an 85-year-old woman with isolated left hip pain. She describes a non-syncopal fall from standing 4 hours ago. Physical examination reveals pain with log-rolling the left thigh and the inability to bear weight on the affected leg. The radiologist reports no fracture in the left hip. What would be the next best step? Review Topic

Explanation
Moderate evidence supports MRI as the advanced imaging of choice for diagnosis of presumed hip fracture not apparent on initial radiographs. MRI has been shown to be able to detect occult fractures earlier than bone scan, with better spatial resolution. Usually the MRI should be obtained in less than 24 hours from the time of injury. For situations in which MRI is not immediately available, bone scan can be considered after 72 hours form the time of injury. However, this may compromise patient care and put the patient at risk of fracture displacement.
Cannon et al. reviewed the imaging of choice in occult hip fracture. They showed that physical examination yields a poor sensitivity identifying occult hip fractures, with log-rolling and straight-leg raise as 50% and 70%, respectively. The most sensitive modality for occult fracture identification was MRI.
Iwata et al. retrospectively reviewed a cohort of 35 patients with clinically suspected fractures of the hip that underwent MRI. All radiographs were negative. In 26 of these patients, a T1-weighted coronal MRI showed a hip fracture with 100% sensitivity.
Roberts et al. reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. They report moderate evidence that supports MRI as the advanced imaging of choice for diagnosis of presumed hip fractures not apparent on initial radiographs.
Figure A is a AP radiograph of the left hip and pelvis. Apart from a healed fracture of the ischiopubic rami and generalized osteopenia, there is no obvious hip fracture. Figure B is a coronal CT image that does not demonstrate evidence of an acute hip fracture. Illustration A is a T1 weighted MR image that shows a non displaced fracture (white arrow) through the intertrochanteric region of the left proximal femur.
Incorrect Answers:
(SBQ12TR.32) A 20-year-old male is taken to the emergency department following a motorcycle collision with the injury seen in Figures A and B. He undergoes serial debridements with placement of an antibiotic bead pouch, followed by intramedullary nailing and free tissue transfer. His preoperative examination is notable for absent plantar sensation. Which of the following is predictive of a worse long term outcome in this patient?

Absent plantar sensation at presentation
Depression at 3 months post-injury
Use of an intramedullary nail
Free tissue transfer instead of rotational flap
Need for multiple debridements
The presence of depression at the 3 months post-injury is a significant predictor of worse long term outcome as well as lower return to work rates in patients that present with limb threatening lower extremity trauma.
The findings of the Lower Extremity Assessment Project (LEAP study) has challenged many of the long-held beliefs of lower extremity trauma surgery, including the concept that patients with absent plantar sensation should undergo immediate amputation . The LEAP study has also brought to light the importance of socioeconomic and psychosocial factors in patient outcomes following these injuries.
Bosse et al analyzed a subgroup of 55 patients from the LEAP study with absent plantar sensation at presentation. Those patients that underwent limb salvage despite absent sensation (n=26) had no significant difference in functional outcome when compared with either insensate patients who underwent amputation or a matched control group of sensate patients with similar injuries. All but one patient in the salvage group had return of some sensation at 2-year follow up and the authors concluded that an insensate plantar foot at presentation should not be included in the algorithm for amputation.
Mackenzie and Bosse reviewed the results of the LEAP study with particular emphasis on the social and economic variables that influence outcomes in severe lower extremity. The authors note that 19% of patients screened positive for severe depression. The presence of anxiety, pain and depression at 3 months post-injury were significant predictors of poor outcome
Incorrect Answers:
tissue for type IIIB tibia fractures. Answer 5: The number of debridements has not been shown to influence outcome.
Question 29
Figure 7 shows the radiograph of an 18-year-old hockey player who sustained a shoulder injury during a fall into the side boards. Examination reveals a significant prominence at the acromioclavicular joint. Management should consist of
Explanation
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocations. Am J Sports Med 1995;23:324-331.
Question 30
Which of the following is considered a potential advantage of arthroscopic repair for anterior instability of the shoulder? Review Topic
Explanation
Question 31
A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?
Explanation
REFERENCES: Yi S, Yoon do H, Kim KN, et al: Postoperative spinal epidural hematoma: Risk factor and clinical outcome. Yonsei Med J 2006;47:326-332.
Uribe J, Moza K, Jimenez O, et al: Delayed postoperative spinal epidural hematomas. Spine J 2003;3:125-129.
Question 32
Figures 5a and 5b show the radiographs of a 21 -year-old wrestler who reports that his leg was rolled over while wrestling. The patient has decreased sensation and function in the distribution of the peroneal nerve, and he has absent pulses. What is the most appropriate initial management at this time?
Explanation
intervention of the artery, but documentation with studies would be appropriate. Delayed reconstruction of injured structures is appropriate.
REFERENCES: Fanelli GC, Orcutt DR, Edson CJ: The multiple- ligament injured knee: Evaluation, treatment, and results. Arthroscopy 2005;21:471 -486.
McDonough EB Jr, Wojtys EM: Multiligamentous injuries of the knee and associated vascular injuries.
Am J Sports Med 2009;37:156-159.
Wascher DC: High-velocity knee dislocation with vascular injury: Treatment principles. Clin Sports Med 2000;19:457-477.
Question 33
A 5-year-old boy has had midfoot pain with activity for the past 3 months. He has no pain at rest. Radiographs are shown in Figures 29a and 29b. Management should consist of
Explanation
REFERENCE: Williams GA, Cowell HR: Koehler’s disease of the tarsal navicular. Clin Orthop 1981;158:53-58.
Question 34
..First-line treatment recommendations include
Explanation
Ultrasound
MRI scan of the thigh
Chest CT scan and whole-body bone scan
Positron emission tomography (PET) scan
Presurgical radiation therapy
Marginal resection
Radical resection and postsurgical radiation
Transverse incision centered over the mass
Incision centered over the mass in line with long axis of limb
Sentinel node biopsy
Core needle biopsy
For each soft-tissue mass clinical scenario or question below, match the most appropriate next evaluation or treatment step listed above.
Question 35
A newborn has an anterolateral bow of the tibia and a duplication of the great toe. Which of the following conditions will develop as the infant grows?
Explanation
REFERENCE: Weaver KM, Henry GW, Reinker KA: Unilateral duplication of the great toe with anterolateral tibial bowing. J Pediatr Orthop 1996;16:73-77.
Question 36
Evaluation of the percent of necrosis in the resected specimen after preoperative chemotherapy is of prognostic value for what type of sarcoma?
Explanation
REFERENCES: Rosen G, Marcove RC, Caparros B, Nirenberg A, Kosloff C, Huvos AG: Primary osteogenic sarcoma: The rationale for pre-operative chemotherapy and delayed surgery. Cancer 1979,43:2163-2177.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423-431.
Wunder JS, Paulian G, Huvos AG, Heller G, Meyers PA, Healey JH: The histological response to chemotherapy as a predictor of the oncological outcome of operative treatment of Ewing sarcoma. J Bone Joint Surg Am 1998;80:1020-1033.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 37
Figures 42a and 42b shows the radiographs of a 20-year-old man who sustained a hyperextension injury to his little finger. Multiple attempts at closed reduction have been unsuccessful. Management should now consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 711-771.
Becton JL, Christian JD Jr, Goodwin HN, Jackson JG III: A simplified technique for treating the complex dislocation of the index metacarpophalangeal joint. J Bone Joint Surg Am 1975;57:698-700.
Green DP, Terry GC: Complex dislocation of the metacarpophalangeal joint: Correlative pathological anatomy. J Bone Joint Surg Am 1973;55:1480-1486.
Question 38
below show the radiographs obtained from an year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 39
Which of the following is the most sensitive parameter to detect the increased inflammatory response seen with both postoperative infection and the use of instrumentation in spinal surgery?

Explanation
DISCUSSION: The most sensitive parameter to detect inflammation elicited by implants and infection is the C-reactive protein (CRP).
CRP is an acute phase reactant that increases sharply immediately after surgery within 6 hours after tissue damage. CRP then peaks 2-3 days later and returns to normal levels 5-21 days after the inciting event. In contrast, ESR reaches its peak on days 4-11, then remains elevated for a prolonged period of time.
Takahashi et al performed a Level 3 study of patients who had undergone spinal surgery with and without instrumentation, with a primary outcome of infection. They concluded that renewed elevation of C-reactive protein, white blood cell count, and body temperature after postoperative days 4 to 7 may be a key indicator of postoperative infection.
Question 40
Which of the following is considered a contraindication to the use of a reverse total shoulder arthroplasty? Review Topic
Explanation
Question 41
A 4-year-old girl has knee pain after a fall. Examination reveals tenderness about the proximal tibia with modest deformity. She has no neurovascular deficits. A radiograph is seen in Figure 24. What should her parents be told? 2010 Pediatric Orthopaedic Examination Answer Book • 25
Explanation
REFERENCES: Jordan SE, Alonso JE, Cook FF: The etiology of valgus angulation after metaphyseal fractures of the tibia in children. J Pediatr Orthop 1987;7:450-457.
Tuten HR, Keeler KA, Gabos PG, et al: Posttraumatic tibia valga in children: A long-term follow-up note. J Bone
Joint Surg Am 1999;81:799-810.
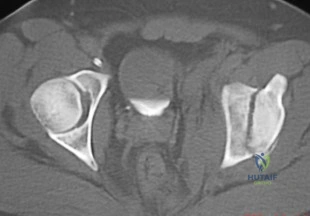
Question 42
A patient sustained a fracture of the left acetabulum. A single axial CT scan from a two-dimensional study is shown in Figure 61. This fracture pattern is best classified as
Explanation
Question 43
Figure 9 shows the AP radiograph of a 65-year-old man who has knee pain and swelling. What is the most likely diagnosis?
Explanation
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 188.
Berkow R (ed): The Merck Manual, ed 14. Rathway, NJ, Merck, 1984, pp 910, 1176, 1200.
Question 44
Figure 68 shows the MRI scan of a 13-year-old boy who has had knee pain and swelling following training lessons for ski racing for the past 6 months. The only abnormal finding on physical examination is an effusion. Management should consist of
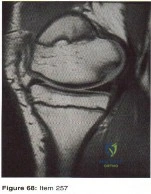
Explanation
Question 45
They found statistically significant decreases in need for secondary intervention, hardware failure, and infection as well as faster wound healing and faster time to fracture union.
Explanation
A 76-year old patient underwent partial foot amputation through the talonavicular and calcaneocuboid joints. Besides Achilles tendon lengthening, what additional procedure(s) may be required to prevent the most common post-operative deformity?
Posterior capsule release
Anterior tibialis transfer to the talar neck
Anterior tibialis transfer to cuboid
Flexor hallucis longus transfer to calcaneus
Peroneus brevis transfer to calcaneus Corrent answer: 2
Achilles tendon lengthening AND anterior tibialis transfer to the talar neck would be required to prevent equinovarus deformity.
Partial foot amputation through the talonavicular and calcaneocuboid joints is also known as the Chopart amputation. Chopart amputation alone is known to result in significant equinovarus deformity. This deformity results in excessive pressure on the anterior wound during gait, causing pain and wound complications. Transfer of the tibialis anterior tendon to talar neck will provide force, and muscle tone, that promotes ankle dorsiflexion. Lengthening of the Achilles tendon will also reduce the equinus moment force across the ankle joint.
Dillion et al. examined the gait patterns of partial foot amputees. They found that amputations proximal to the metatarsal heads compromised the normal propulsive function of the foot and ankle. The ideal level of amputation to maintain normal propulsive function was distal to the metatarsal heads (i.e., disarticulating the metatarsophalangeal (MTP) joint).
Illustration A is a lateral radiograph showing a Chopart amputation. Incorrect Answers:
prevent the equinovarus deformity.

OrthoCash 2020
A 32-year-old male is involved in a motor vehicle collision and sustains the injury seen in Figure A. What is the most common urological injury associated with this injury pattern?

Testicular torsion
Posterior urethral tear
Bladder denervation
Testicular rupture
Renal hematoma
The figure shows an anteroposterior pelvic ring injury. The most common urological injury with pelvic ring injuries remains the posterior urethral tear, followed by bladder rupture.
Watnik et al notes lower urinary tract (bladder to end of urethra) injuries in up to 25% of patients with this injury. He reports that when contaminated urine communicates with the anterior arch, the possibility of infection exists, and early repair of bladder disruptions with simultaneous anterior arch plating minimizes this risk.
Routt et al notes that even with simultaneous treatment of these injuries, complications are common (late stricture in 44%, impotence in 16%, delayed incontinence in 20% of females, anterior deep pelvic infection in 4%). Despite this, they report that early urological repairs are easily performed at the time of anterior pelvic open reduction and internal fixation.
OrthoCash 2020
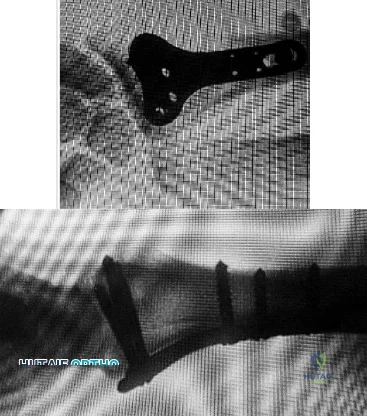
A 26-year-old women, 31-weeks pregnant, presents to the emergency department with the injury shown in Figure A. She states the injury occurred while lifting a heavy vacuum five days ago. She suffers from chronic headaches and sleep disturbances. On inspection, there are multiple dorsal and volar bruising over her wrist and upper arm. She is neurologically intact. After closed reduction and immobilizing the arm, what would be the next best step in management of this patient?

Diagnostic wrist arthroscopy
Urgent MRI wrist
Skeletal survey radiographs
Request a consultation with social worker in the hospital
Urgent open reduction internal fixation Corrent answer: 4
This patient presents with classic features of domestic violence. The most appropriate next step would be consultation with a social worker at the hospital, assess for child and patient safety, and encouraging the patient to seek self-protection.
Factors suggestive of domestic violence in the patient include pregnancy, delayed presentation after injury, inconsistent history, multiple bruises and complaints of chronic headache/sleep disturbances. Victims frequently miss days of work and as a result are at risk for losing their jobs. Victims are also more likely to engage in high-risk behavior with sex, drugs, alcohol, smoking, and eating.
The AAOS published a document outlining the Orthopaedic Surgeon’s responsibilities in domestic and family violence. Musculoskeletal injuries that should raise a suspicion of a problem include (1) Multiple injuries/fractures; (2) Unusual patterns of injury/fracture; (3) Injuries/fractures of varying ages; (4)
Injuries/fractures inconsistent with or disproportional to the history; (5) Multiple injuries treated in different hospital emergency departments or by different providers.
Incorrect Answers:
OrthoCash 2020
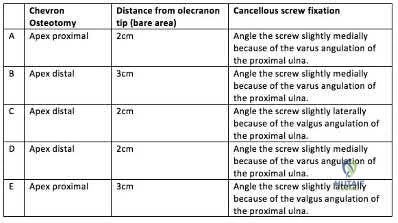
A 45-year-old man undergoes open reduction and internal fixation for a comminuted intra-articular humerus fracture . An olecranon osteotomy is performed and subsequently fixed with an intramedullary cancellous screw. Which of the following options in the table shown in Figure A best describes the characteristics of this osteotomy?
Question 46
One year after undergoing anterior cervical decompression and fusion, what percentage of patients still have dysphagia?
Explanation
Dysphagia after anterior cervical diskectomy and fusion is a common, usually transient finding after anterior cervical approaches to the spine. While it has been reported to occur in up to 70% of patients 2 weeks following surgery, in most cases the symptoms quickly resolve. There is, however, a small subset of patients for whom symptoms of dysphagia will persist. Lee and associates prospectively studied the rate of dysphagia after anterior cervical diskectomy and fusion, reporting a 15% rate of dysphagia at 12 months, and 12% at 24 months. Phillips and associates analyzed the 2-year data from the PCM FDE clinical trial and found a 12.1% incidence of dysphagia in the ACDF arm.
RECOMMENDED READINGS
Lee MJ, Bazaz R, Furey CG, Yoo J. Risk factors for dysphagia after anterior cervical spine surgery: a two-year prospective cohort study. Spine J. 2007 Mar-Apr;7(2):141-7. Epub 2007 Jan 22. PubMed PMID: 17321961. View Abstract at PubMed
Smith-Hammond CA, New KC, Pietrobon R, Curtis DJ, Scharver CH, Turner DA. Prospective analysis of incidence and risk factors of dysphagia in spine surgery patients: comparison of anterior cervical, posterior cervical, and lumbar procedures. Spine (Phila Pa 1976). 2004 Jul 1;29(13):1441-6. PubMed PMID: 15223936. View Abstract at PubMed
Edwards CC 2nd, Karpitskaya Y, Cha C, Heller JG, Lauryssen C, Yoon ST, Riew KD. Accurate identification of adverse outcomes after cervical spine surgery. J Bone Joint Surg Am. 2004 Feb;86-A(2):251-6. PubMed PMID: 14960668. View Abstract at PubMed
Phillips FM, Lee JY, Geisler FH, Cappuccino A, Chaput CD, DeVine JG, Reah C, Gilder KM, Howell KM, McAfee PC. A prospective, randomized, controlled clinical investigation comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion. 2-year results from the US FDA IDE clinical trial. Spine (Phila Pa 1976). 2013 Jul 1;38(15):E907-18. doi: 10.1097/BRS.0b013e318296232f.
Rihn JA, Kane J, Albert TJ, Vaccaro AR, Hilibrand AS. What is the incidence and severity of dysphagia after anterior cervical surgery? Clin Orthop Relat Res. 2011 Mar;469(3):658-65. PMID: 21140251.View Abstract at PubMed
Question 47
A 70-year-old woman has a 3-year history of gradually increasing diffuse and global right knee pain. Her main issues are difficulty with stairs, stiffness with prolonged sitting, and swelling. She has taken NSAIDs and has received intra-articular steroid injections, all with decreasing efficacy. Her right knee examination reveals a range of motion of 15° to 80° with a fixed deformity to varus and valgus stress. Her symptoms are no longer manageable nonsurgically. Radiographs reveal a 30-degree mechanical axis deformity. The deformity shown in Figure below is predominantly associated with

Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point, can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 48
A 25-year-old woman with a healed proximal tibiofibular fracture treated with an intramedullary nail 2 years ago is currently wearing an ankle-foot orthosis (AFO) and reports a persistent foot drop. She is unhappy with the AFO and has not seen any functional improvement despite months of physical therapy. Serial electromyograms (EMG) show no recent change over the past year. Examination and EMG findings are consistent with a tibialis anterior 1/5, extensor hallucis longus 2/5, extensor digitorum longus 2/5, posterior tibial tendon (PTT) 5/5, peroneals 3/5, flexor hallucis longus 5/5, and gastrocsoleus 5/5. No discrete nerve lesion was identified. The patient has a flexible equinovarus contracture. What is the most appropriate management?
Explanation
REFERENCES: Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 192.
Atesalp AS, Yildiz C, Komurcu M, et al: Posterior tibial tendon transfer and tendo-Achilles lengthening for equinovarus foot deformity due to severe crush injury. Foot Ankle Int 2002;23:1103-1106.
Scott AC, Scarborough N: The use of dynamic EMG in predicting the outcome of split posterior tibial tendon transfers in spastic hemiplegia. J Pediatr Orthop 2006;26:777-780.
Williams PF: Restoration of muscle balance of the foot by transfer of the tibialis posterior. J Bone Joint Surg Br 1976;58:217-219.
Question 49
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?
Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 50
Which of following is pathognomonic of intervertebral disk degeneration? Review Topic
Explanation
large proteoglycan molecules in
the nucleus pulposus is
pathognomonic
of intervertebral disk
(IVD) degeneration.
Degeneration of the intervertebral disk (IVD) is a major pathological process implicated in low back pain and is often considered a prerequisite for intervertebral disc herniation. While the pathophysiologic causes of IVD degeneration at the molecular level are not fully known, there are many physical and molecular changes that are known to contribute to the disease process. The most significant is loss of large proteoglycan molecules and decreased water content.
An et al. showed that large proteoglycans (PGs), such as aggrecan and versican, decrease in patients with intervertebral disk (IVD) degeneration.
Kepler et al. reviewed IVD degeneration. They report that degeneration leads to changes in the expression of matrix proteins, cytokines, and proteinases. They suggest treatment with gene therapy, such as Growth and Differentiation Factor-5 (GDF-5), may help to promote the healing of degenerated intervertebral disks.
Illustration A shows a cadaveric image of normal disk anatomy (left) and IVD degeneration (right)
Incorrect Answers:
Question 51
What is the incidence and significance of anterior cruciate ligament laxity following tibial eminence fractures in skeletally immature individuals?
Explanation
REFERENCES: Willis R, Blokker C, Stall TM, et al: Long-term follow-up of anterior
eminence fractures. J Pediatr Orthop 1993;13:361-364.
Smith JB: Knee instability after fracture of the intercondylar eminence of the tibia.
J Pediatr Orthop 1984;4:462-464.
Question 52
A 28-year-old man has a painful nodule on the plantar aspect of his foot in the midarch. Use of a soft orthosis has failed to provide relief. Examination reveals that the mass is approximately 2 1/2 cm in diameter, firm, and tender to palpation. An MRI scan confirms the presence of a plantar fibroma. Management should now consist of
Explanation
REFERENCES: Kirby EJ, Shereff MJ, Lewis MM: Soft-tissue tumors and tumor-like lesions of the foot: An analysis of 83 cases. J Bone Joint Surg Am 1989;71:621-626.
Cavolo DJ, Sherwood GF: Dupuytren’s disease of the plantar fascia. J Foot Surg 1982;21:12-15.
Question 53
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension?
Explanation
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through view, are useful for avoiding this complication.
Question 54
A 6-year-old boy is being treated for acute hematogeneous osteomyelitis of the distal femur with intravenous antibiotics. The best method to determine the success or failure of initial treatment is by serial evaluations of which of the following studies?
Explanation
REFERENCES: Unkila-Kallio L. Kallio MJ, Eskola J, et al: Serum C-reactive protein, erythrocyte sedimentation rate, and white blood cell count in acute hematogenous osteomyelitis of children. Pediatrics 1994;93:59-62.
Herring JA(ed): Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia. PA. WB Saunders, 2008, pp 2090-2100.
AL-Madena Copy
Question 55
Figures 42a and 42b show the radiographs of a 52-year-old man who sustained a fall from a motorcycle 6 months ago and now reports pain and stiffness in his left shoulder. What is the most reliable treatment to improve function and comfort of the shoulder?
Explanation
REFERENCES: Gerber C, Lambert SM: Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1996;78:376-382.
Spencer EE Jr, Brems JJ: A simple technique for management of locked posterior shoulder dislocations: Report of two cases. J Shoulder Elbow Surg 2005;14:650-652.
Sperling JW, Pring M, Antuna SA, et al: Shoulder arthroplasty for locked posterior dislocation of the shoulder. J Shoulder Elbow Surg 2004;13:522-527.
Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
McLaughlin HL: Posterior dislocation of the shoulder. J Bone Joint Surg Am 1952;34:584-590.
Question 56
A 44-year-old farmer involved in a rollover accident on his tractor sustained an L1 burst fracture with a 20% loss of anterior vertebral body height, 30% canal compromise, and 15 degrees of kyphosis. He remains neurologically intact. The preferred initial course of action should consist of
Explanation
REFERENCES: Hartman MB, Chrin AM, Rechtine GR: Nonoperative treatment of thoracolumbar fractures. Paraplegia 1995;33:73-76.
Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Kraemer WJ, Schemitsch EH, Lever J, McBroom RJ, McKee MD, Waddel JP: Functional outcome of thoracolumbar burst fractures without neurological deficit. J Orthop Trauma 1996;10:541-544.
Question 57
Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
Explanation
A. Inability to flex the distal interphalangeal joint of the index finger
B. Positive Froment’s sign
C. Weakness with wrist extension
D. Decreased capillary refill
Question 58
At the time of the revision surgery shown in Figure 14, the acetabular component was found to be stable. Polyethylene exchange with a standard ultra-high molecular weight polyethylene liner and grafting was performed. The patient is at significantly increased risk for
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 411-424.
Boucher HR, Lynch C, Young AM, et al: Dislocation after polyethylene liner exchange in total hip arthroplasty. J Arthroplasty 2003;18:654-657.
Maloney WJ, Herzwurm P, Paprosky W, et al: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
Question 59
Figures 6a through 6d show the radiographs and biopsy specimens of an 8-year-old girl with leg pain. Management of the lesion should consist of
Explanation
REFERENCES: Wilson AJ, Kyriakos M, Ackerman LV: Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-518.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 167-189.
Question 60
In the evaluation of somatosensory-evoked potential waveforms for intraoperative neuromonitoring for spinal surgery, the minimum criteria for determining potentially significant changes include Review Topic
Explanation
Question 61
Which of the following factors is considered most important when assessing an ankle fracture for surgical treatment?
Explanation
REFERENCES: Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 62
- Figure 12 shows the frog-lateral radiograph of a 45-year-old man who has a painful left hip. What is the most likely diagnosis?
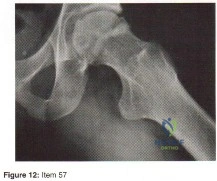
Explanation
Question 63
In an acute closed boutonniere injury, what is the most appropriate splinting technique for the proximal interphalangeal joint?
Explanation
REFERENCES: Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Lovet WL, McCalla MA: Management and rehabilitation of extensor tendon injuries. Orthop Clin North Am 1983;14:811-826.
Question 64
The force generated by a muscle is most highly dependent on its
Explanation
Question 65
What is the most common primary malignant tumor of bone in childhood?
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 226.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 66
A 14-year-old gymnast presents after a fall from the balance beam with a hyperextension injury to her left knee. She could ambulate with pain but was unable to continue exercise due to pain. On examination she has a swollen knee with painful

Explanation
Tibial eminence fractures are rare but occur more often in pediatric populations, often in the setting of sports-related injuries. Debate continues over operative vs nonoperative treatment, as well as fixation type (screw vs suture) for openly treated fractures. Past evidence suggested closed treatment was adequate but there has been an increase in operative management. Closed treatment is suggested for minimally displaced fractures (Type I and reducible Type II) and open treatment for completely displaced fractures (non-reducible Type II and Type III).
Wilfinger et al provide the results of a closed reduction protocol at their institution including 38 patients with long term followup. All patients underwent aspiration and closed reduction in the OR under fluoroscopic guidance followed by long leg casting in hyperextension and graduated weight bearing over weeks. No patients complained of persistent pain, swelling, giving way, or disability at follow up.
However, Edmonds et al in a retrospective review compare open reduction internal fixation (ORIF), arthroscopic-assisted internal fixation (AAIF), and closed reduction with casting (CRC) for pediatric patients with displaced tibial spine fractures. They report improved reduction but also increased arthrofibrosis in ORIF and AAIF groups
compared to CRC, but of the 24% of patients with long term followup results, there was no difference in functional outcomes across all 3 groups. There was a 17% rate of later operation for the CRC group patients. They suggest closed treatment for fractures with <5mm displacement, otherwise ORIF or AAIF.
Gans et al conducted a systematic review focused on the questions of open vs closed reduction, and screw vs suture fixation. The 26-article review found insufficient evidence to have any clear recommendations. They did find reduced laxity and improved range of motion for minimally displaced fractures that had an open reduction, and that completely displaced fractures treated nonoperative had higher rates of nonunion.
Figures A and B are AP and lateral knee radiographs demonstrating a moderately displaced (Meyers and McKeever Type II) tibial spine fracture in a skeletally immature patient.
Incorrect Responses
Question 67
Figure 12 shows an arthroscopic view from an inferolateral portal of a right knee. The asterisk indicates which structure?

Explanation
The asterisk indicates the anteromedial bundle of the anterior cruciate ligament. The anterior cruciate ligament consists of 2 functional bundles: anteromedial and posterolateral. During extension of the knee, the posterolateral bundle becomes taut. In flexion, the anteromedial bundle is tight and the posterolateral bundle relaxes. Recently, techniques for double-bundle reconstruction have been described to recreate the normal anatomic relationship of the 2 bundles.
RECOMMENDED READINGS
Chhabra A, Zelle BA, Feng MT, Fu FH. The arthroscopic appearance of a normal anterior cruciate ligament in a posterior cruciate ligament-deficient knee: the posterolateral bundle (PLB) sign. Arthroscopy. 2005 Oct;21(10):1267. PubMed PMID: 16226658. View Abstract at PubMed
Cha PS, Brucker PU, West RV, Zelle BA, Yagi M, Kurosaka M, Fu FH. Arthroscopic double-bundle anterior cruciate ligament reconstruction: an anatomic approach. Arthroscopy. 2005 Oct;21(10):1275. PubMed PMID: 16226666. View Abstract at
PubMed
Question 68
What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?
Explanation
REFERENCES: Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 69
The underlying cause of the neoplasm is
Explanation
The bone scan reveals multiple bone lesions, which does not rule out any of the responses. The radiographs reveal dysplastic bone with a “ground glass” appearance, suggesting fibrous dysplasia as the preferred response. Multiple myeloma typically demonstrates purely lytic, “punched out” lesions and would be highly unusual in a 23-year-old woman. Multiple hereditary exostosis would demonstrate more expansile lesions concentrated in the metaphysis. Metastatic carcinoma could have a lytic or blastic appearance but is less likely to occur in a 23-year-old woman.
McCune-Albright syndrome in polyostotic fibrous dysplasia is present in as many as 50% of patients and should be evaluated for during an endocrine consultation. Adrenal, pituitary, parathyroid, and thyroid endocrinopathies may be present. Untreated hyperthyroidism can be life threatening during a surgical procedure. There is no indication to repeat the nuclear bone scan. Although phosphate wasting and, rarely, oncogenic osteomalacia have been reported in polyostotic fibrous dysplasia, an endocrinology consultation always should be sought.
Café au lait macules are the most common extraskeletal manifestation of fibrous dysplasia, often referred to as “coast of Maine” in appearance because of their irregular borders (in comparison to the “Coast of California” with smooth borders as seen in neurofibromatosis). Multiple myeloma would not ordinarily appear with increased uptake on a bone scan unless a pathologic fracture of some duration were present. A long area of bone involvement would not appear in patients with metastatic lung adenocarcinoma.
An ALK rearrangement occurs in nonsmall-cell lung cancer. The translocation t(11;14)(q13;q32) should be recognized as a poor prognosticator in multiple myeloma. The germline alteration in EXT1 and EXT2 occurs in multiple hereditary exostosis.
All forms of fibrous dysplasia are caused by a nongerm-cell mutation that occurs during early embryogenesis. A missense mutation of the GNAS1 gene, which encodes the alpha subunit of the stimulatory G-protein-couple-receptor, Gs alpha, results in G-protein activation and the production of cyclic adenosine monophosphate affecting melanocytes, endocrine cells, and osteoprogenitor cells.
RECOMMENDED READINGS
DiCaprio MR, Enneking WF. Fibrous dysplasia. Pathophysiology, evaluation, and treatment. J Bone Joint Surg Am. 2005 Aug;87(8):1848-64. Review.View Abstract at PubMed
Parekh SG, Donthineni-Rao R, Ricchetti E, Lackman RD. Fibrous dysplasia. J Am Acad Orthop Surg. 2004 Sep-Oct;12(5):305-13. Review. PubMed PMID: 15469225. View Abstract at PubMed
Shin HJ, Kim K, Lee JJ, Song MK, Lee EY, Park SH, Kim SH, Jang MA, Kim SJ, Chung JS. The t(11;14)(q13;q32) translocation as a poor prognostic parameter for autologous stem cell transplantation in myeloma patients with extramedullary plasmacytoma. Clin Lymphoma Myeloma Leuk. 2015 Apr;15(4):227-35. doi: 10.1016/j.clml.2014.12.007. Epub 2014 Dec 12.View Abstract at PubMed
Esfahani K, Agulnik JS, Cohen V. A Systemic Review of Resistance Mechanisms and Ongoing Clinical Trials in ALK-Rearranged Non-Small Cell Lung Cancer. Front Oncol. 2014 Jul 21;4:174. doi: 10.3389/fonc.2014.00174. eCollection 2014. Review. PubMed PMID: 25101240. View Abstract at PubMed
Question 70
Tendons should have what ratio of matrix protein?
Explanation
Question 71
Optimal management of the injury shown in Figure 31 should include which of the following?
Explanation
REFERENCES: Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.
Question 72
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan?
Explanation
at 3 weeks risks tearing the subscapularis tendon repair. Active strengthening should not begin for 6 weeks postoperatively to allow the subscapularis tendon repair time to heal.
REFERENCES: Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
Matsen FA III, Lippitt SB, Sidles JA, et al: Practical Evaluation and Management of the Shoulder. Philadelphia, PA, WB Saunders, 1994, pp 215-218.
Question 73
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Explanation
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. These arteries arise from the popliteal artery. If this artery is not adequately mobilized, a gastrocnemius soleus flap can be devascularized.
Question 74
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in
Explanation
REFERENCES: Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417.
D’Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Pearl ML, Bessos K, Wong K: Strength deficits related to distal biceps tendon rupture and repair: A case report. Am J Sports Med 1998;26:295-296.
Question 75
-A 23-year-old man had a laparotomy and splenectomy with packing of the abdomen after a motorcycle collision. Laboratory studies show a hemoglobin level of 7.1 g/dL (reference range [rr], 14.0-17.5 g/dL) and a lactate level of 8.0 mmol/L (rr, 0.6-1.7 mmol/L). He also has a left humeral fracture,an anteroposterior compression I pelvic fracture, bilateral distal third femur fractures, and an open GustilotypeIIIA tibial diaphysis fracture with moderate contamination. What is the most appropriate treatment to administer before leaving the operating room?
Explanation

Question 76
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Question 77
Overgrowth of a limb in a patient with neurofibromatosis type 1 (NF1) is most likely associated with the presence of
Explanation
REFERENCES: Alman BA, Goldberg MJ: Syndromes of orthopaedic importance, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 287-338.
Greene WB: Neurofibromatosis type I, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1584-1588.
Question 78
-A 24-year-old collegiate pitcher has had increasing pain over his medial elbow for 3 months. He has point tenderness over his medial epicondyle and reproduction of his symptoms with a valgus stress test. What phase of the throwing cycle most likely will reproduce his symptoms?
Explanation
Question 79
What is the most likely consequence of a vertebral compression fracture associated with osteoporosis?
Explanation
REFERENCES: Heaney RP: The natural history of vertebral osteoporosis: Is low bone mass an epiphenomenon? Bone 1992;13:S23-S26.
Tohmeh AG, Mathias JM, Fenton DC, et al: Biomechanical efficacy of unipedicular versus bipedicular vertebroplasty for the management of osteoporotic compression fractures. Spine 1999;24:1772-1776.
Question 80
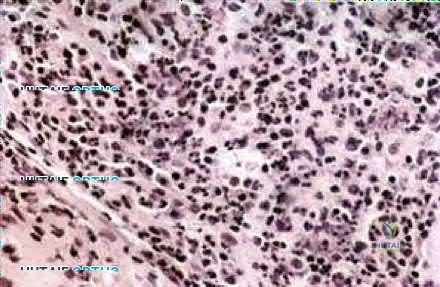
A 16-year-old girl has had hip pain for 1 year. Approximately 2 months ago she noted the development of a hard mass in the right buttock that has steadily increased in size. She now reports severe pain in the right buttock, with radiation down the leg and numbness involving the right foot and toes. A radiograph is shown in Figure 70a and an axial postcontrast T 1 -weighted MRI scan is shown in Figure 70b. A biopsy specimen is shown in Figure 70c. The chest CT shows multiple lung metastases. Treatment of this lesion should consist of
Explanation
REFERENCES: Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Thacker MM, Temple HT, Scully SP: Current treatment for Ewing’s sarcoma. Expert Rev Anticancer Ther 2005;5:319-331.
Weber KL: Current concepts in the treatment of Ewing’s sarcoma. Expert Rev Anticancer Ther 2002;2:687-694.
Question 81
The use of a screw between the clavicle and the coracoid process to maintain the clavicle and acromioclavicular (AC) joint in a reduced position is a treatment option for AC joint separations. Screw removal is generally recommended after soft-tissue healing. What effect does this rigid coracoclavicular fixation have on shoulder kinematics?
Explanation
REFERENCES: Flatow EL: The biomechanics of the acromioclavicular, sternoclavicular, and scapulothoracic joints. Instr Course Lect 1993;42:237-245.
Kenedy JC, Cameron H: Complete dislocation of the acromioclavicular joint. J Bone Joint Surg Br 1954;36:202-208.
Rockwood CA Jr, Williams GR, Young CD: Disorders of the acromioclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 483-553.
Inman VT, Saunders JB, Abbott LC: Observations of the function of the shoulder joint. Clin Orthop 1996;330:3-12.
Question 82
Because the patient shown in Figure 27 can no longer fit in shoes, treatment of the deformity should consist of
Explanation
REFERENCES: Turra S, Santini S, Cagnoni G, Jacopetti T: Gigantism of the foot: Our experience in seven cases. J Pediatr Orthop 1998;18:337-345.
Guidera KJ, Brinker MR, Kousseff BG, et al: Overgrowth management in Klippel-Trenaunay-Weber and Proteus syndromes. J Pediatr Orthop 1993;13:459-466.
Question 83
The patient in Figure 55 is actively attempting to make a fist. This clinical scenario suggests which of the following anatomic lesions?
Explanation
REFERENCE: Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, p 189.
Question 84
The most appropriate next surgical procedure is
Explanation
This patient’s arthritis likely has progressed to the lateral compartment. The location and degree of local pain and tenderness are the most important physical findings. History and physical findings indicate arthritis progression to the lateral and anterior compartments. This scenario suggests the need for conversion of the unicompartmental arthroplasty to TKA.

Question 85
03 advancement at age 6 years. What is the most likely diagnosis?
Explanation
back to this question next question
Question 86
A tendon repair is thought to be weakest during which phase of tendon healing?
Explanation
Question 87
Which of the following is true regarding anterior sternoclavicular joint dislocations?

Explanation
Question 88
What is the most common cause of mechanical failure of an orthopaedic biomaterial during clinical use?
Explanation
REFERENCES: Lewis G: Fatigue testing and performance of acrylic bone-cement materials: State-of-the-art review. J Biomed Mater Res Br 2003;66:457-486.
Stolk J, Verdonschot N, Huiskes R: Stair climbing is more detrimental to the cement in hip replacement than walking. Clin Orthop 2002;405:294-305.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 89
A 13-year-old girl who competes in gymnastics reports the insidious onset of lateral left elbow pain over the past 6 months. She also notes occasional catching episodes in the elbow; however, she denies any history of trauma. Examination reveals tenderness over the lateral epicondyle and extensor muscle origin. The elbow is stable and has full flexion, but lacks 10° of full extension. An AP plain radiograph and an MRI scan are shown in Figures 17a and 17b. Management of the elbow should consist of
Explanation
REFERENCES: Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med
1998;26:520-530.
Jackson DW, Silvino N, Reiman P: Osteochondritis in the female gymnast’s elbow. Arthroscopy 1989;5:129-136.
Ruch DS, Cory JW, Poehling GG: The arthroscopic management of osteochondritis dissecans of the adolescent elbow. Arthroscopy 1998;14:797-803.
Question 90
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 91
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include
Explanation
REFERENCES: Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Hawkins RJ, Murnaghan JP: The shoulder, in Gruess RL, Ronnie WRJ (eds): Adult Orthopaedics. New York, NY, Churchill Livingstone, 1984, pp 945-1054.
Question 92
Figures 1 and 2 are the radiographs of an 18-year-old man who had surgery 6 months ago at an outside institution. He is being referred now because he has persistent pain. He is tender over the scaphoid at the snuffbox. What is the most appropriate next imaging step in his pain workup?

Explanation
Scaphoid nonunions are difficult to diagnose on plain radiographs, which offer poor reliability when attempting to determine if there is bridging trabeculae crossing the fractures site. CT scans are more useful for diagnosing scaphoid nonunion. When scanned using conventional axial cuts, the slices mayskip through the fracture nonunion site, thereby missing the defect, even with reformats. MR imaging is useful in diagnosing acute scaphoid fractures and has a high sensitivity and diagnostic value for excluding scaphoid fractures as well. Contrast does not enhance the utility of MR imaging in fracture diagnosis.
Question 93
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?
Explanation
REFERENCE: Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 2069.
Question 94
All of the following indicators of resuscitation may be within normal limits for a trauma patient that is in "compensated" shock EXCEPT:

Explanation
Question 95
The postoperative neurologic prognosis of a patient who has a tumor that is compressing the spinal cord and causing a neurologic deficit depends primarily on the
Explanation
REFERENCES: Weinstein JN: Differential diagnosis and surgical treatment of primary benign and malignant neoplasms, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 1, pp 829-860.
Siegal T, Siegal T: Current considerations in the management of neoplastic spinal cord compression. Spine 1989;14:223-228.
Question 96
- Which of the following provides the most stable fixation for comminuted fractures of the posterior acetabular wall?
Explanation
According to Rockwood & Green and Browner & Jupiter the key to fixing these fractures is to re-establish a congruent articular surface. The other four distracters (i.e. cable, methylmethacrylate, multiple lag screws, and multiple K-wires) may achieve initial stability, but reduction will not be maintained. In addition, further studies show a higher incidence of mortality and complications with the use of lag screws and K-wires alone (Browner & Jupiter, Skeletal trauma, 1998)
Question 97
-What is the recommended treatment for this injury?
Explanation
The hypertrophic zone of the growth plate has been implicated as the weak link in the physis in acute injuries. Epiphysiolysis of the proximal humerus in throwing athletes occurs as the result of tension and shear on the physis. More than 90% of affected patients who are treated with rest for an average of 3 months become asymptomatic. Prevention is the best option. Set limitations of the number of pitches and types of pitches depending on the age of the player. Also recommend use of proper pitching mechanics.
Question 98
The patient returns 4 days after surgery and says he has noticed a red, swollen knee since yesterday. He reports a fever of 38.0°C since last evening and denies traumatic injury. He has an erythematous knee with a large, tense effusion; his range of motion is limited; and the surgical incisions are not draining. Radiographs taken in the office show no change from the immediate postsurgical images. Aspiration in the office returns 50 cc of cloudy, blood-tinged synovial fluid, and analysis of the fluid reveals a white blood cell count of 92000 (reference range 4500-11000 /µL). Which bacteria is most commonly responsible for this clinical scenario?
Explanation
This patient has a history of failed primary and revision ACL reconstructions, both times with medial meniscus repairs. The clinical scenario suggests a recurrent ACL injury with a recurrent medial meniscus tear that is now locked. The most critical risk factor for ACL reconstruction is age younger than 20 years. The meniscal repair success rate using an all-inside device is between 80% and 90%. Traditionally, it was believed that healing rates were
higher in ACL reconstruction, but current literature demonstrates a similar rate of healing associated with ACL reconstruction and no reconstruction of stable knees.
The images show a vertical femoral tunnel resulting from this patient’s prior reconstruction and revision. The MR images reveal a locked bucket-handle tear of the medial meniscus, and the examination shows a positive Lachman test finding attributable to ACL graft failure. In the setting of a young individual who has failed 2 meniscal repairs, a third repair is not indicated. In addition to a revision ACL reconstruction to stabilize the knee, a partial medial meniscectomy is indicated. An attempt at revision medial meniscus repair would be indicated if the technique were poor in the first attempt, but a failed repair otherwise should indicate the need for partial meniscectomy. The postsurgical images reveal a much more anatomic position of the femoral tunnel that should provide better rotational control of the knee, thereby improving the pivot shift (compared to the vertical femoral tunnel).
This patient has an obvious postsurgical infection based on the timing, examination, and results of the aspiration. In multiple studies of septic arthritis following ACL reconstruction, the most common pathogen was coagulase-negative staph (Staphylococcus epidermidis), followed by S. aureus. If S. aureus is the causative pathogen, the rate of necessary graft removal is higher because of the aggressive nature of this specific bacteria.
Question 99
Six months later, the patient’s fracture has healed and a CT scan to further evaluate the physis is performed (Video 85). Based on these findings, how should you advise the family?
Explanation
The hypertrophic zone is the weakest biomechanical zone of the physis and is most likely to fracture. The deep peroneal nerve supplies motor innervation to the ankle and toe
dorsiflexors (anterior compartment) and the first web space, which, in this history, have deficits. The superficial peroneal nerve supplies sensation to the dorsum of the foot and motor to the lateral compartment peroneal musculature (ankle evertors), which also has deficits. The injury must involve both peroneal branches (the common peroneal nerve). Because sensation to the sole of the foot and toe/ankle plantar flexion is intact, the tibial nerve is intact.
Because the nerve was visualized intact, a neuropraxia is the most likely type of nerve injury. This should recover in time and does not necessitate urgent exploration. In pediatric patients, an advancing Tinel sign and partial nerve recovery by 3 months is expected and can be followed clinically. If there is no sign of nerve recovery, an electromyogram should be ordered with consideration for nerve exploration if there is no sign of reinnervation. There is no sign of compartment syndrome because the patient has an unchanged neurologic deficit, is comfortable, and has no pain with passive range of motion.
These injuries are associated with a very high rate of growth arrest (up to 80% in some studies). The CT scan shows an asymmetric growth arrest, which suggests angulation through the distal femur.
Question 100
1 and 2 demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
