Orthopedic MCQ Mock Exam: Trauma, Oncology & Joint Surgery | Part 261

Key Takeaway
This page offers Orthopedic Surgery Board Review Part 261: 100 verified, high-yield MCQs. Designed for orthopedic residents and surgeons preparing for OITE/AAOS/ABOS exams, it covers Cartilage, Fracture, Hip, Shoulder, Tumor, Wrist. It’s an interactive tool for robust board certification success.
About This Board Review Set
This is Part 261 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 261
This module focuses heavily on: Cartilage, Fracture, Hip, Shoulder, Tumor, Wrist.
Sample Questions from This Set
Sample Question 1: Studies have shown that the parents and grandparents of people with developmental dysplasia of the hip (DDH)...
Sample Question 2: A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?...
Sample Question 3: When compared with reamed intramedullary nailing for an unstable diaphyseal tibia fracture, unreamed nailing is associated with which of the following?...
Sample Question 4: What is the most common primary malignant bone or cartilage tumor in children?...
Sample Question 5: A 38-year-old man sustained a complete thoracic spinal cord injury at age 14. An MRI scan of his shoulder, when compared with studies from uninjured controls, is more likely to show which of the following? Review Topic...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Studies have shown that the parents and grandparents of people with developmental dysplasia of the hip (DDH)
Explanation
The hip arthritis RR is significantly increased in patients with DDH (RR = 82.4; P < 2e-16), their parents (RR = 2.22; P = 0.0003), and their grandparents (RR = 1.33; P = 0.011). The THA RR also is significantly increased for patients with DDH (RR = 1168; P < 3e-08) and their grandparents (RR = 2.06; P = 0.01). First-degree and second-degree relatives were not at higher risk for knee arthritis or knee arthroplasty. The RR for DDH was significantly increased for first-degree relatives (RR = 12.1; P < 0.000001) and siblings (RR = 11.9; P < 0.000001).
Question 2
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?
Explanation
REFERENCE: Perlik PC, Guilford WB: Magnetic resonance imaging to assess vascularity of scaphoid nonunions. J Hand Surg Am 1991;16:479-484.
Question 3
When compared with reamed intramedullary nailing for an unstable diaphyseal tibia fracture, unreamed nailing is associated with which of the following?
Explanation
Question 4
What is the most common primary malignant bone or cartilage tumor in children?
Explanation
1 million children younger than age 15 years), and Ewing’s sarcoma is second (2.1 per
1 million children). Giant cell tumor and chondrosarcoma are rare in children. Osteochondroma is more common than any of the above tumors in children, but it is not malignant.
REFERENCES: Himelstein BP, Dormans JP: Malignant bone tumors of childhood. Pediatr Clin North Am 1996;43:967-984.
Pierz KA, Womer RB, Dormans JP: Pediatric bone tumors: Osteosarcoma, Ewing’s sarcoma, and chondrosarcoma associated with multiple hereditary osteochondromatosis. J Pediatr Orthop 2001;21:412-418.
Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence.
N Engl J Med 1999;341:342-352.
Question 5
A 38-year-old man sustained a complete thoracic spinal cord injury at age 14. An MRI scan of his shoulder, when compared with studies from uninjured controls, is more likely to show which of the following? Review Topic
Explanation
Question 6
To adequately expose the volar plate of the proximal interphalangeal joint of the finger, which of following pulleys is typically incised?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186.
Strickland J: Flexor tendon-acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2,
pp 1853-1855.
Lin GT, Amadio PC, An KN, et al: Functional anatomy of the human digital flexor pulley system. J Hand Surg Am 1989;14:949-956.
Question 7
A 40-year-old woman has local back pain and intense burning pain in her perianal region after being shot twice in the back. Motor and sensory examination of her lower extremities reveals no apparent deficit. She has present but decreased sensation in her perianal region, an intact anal wink, good rectal tone, and an intact bulbocavernosus reflex. Radiographs and CT scans are shown in Figures 3a through 3d. What is the next most appropriate step in management?
Explanation
REFERENCES: Bracken MB, Shepard MJ, Holford TR: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. JAMA 1997;277:1597-1604.
Waters RL, Adkins RH: The effects of removal of bullet fragments retained in the spinal canal: A collaborative study by the National Spinal Cord Injury Model Systems. Spine
1991;16:934-939.
Stauffer ES, Wood RW, Kelly EG: Gunshot wounds of the spine: The effects of laminectomy.
J Bone Joint Surg Am 1979;61:389-392.
Question 8
Radiographs of an 80-year-old woman with back pain reveal a compression fracture. Which of the following imaging studies best evaluates the acuity of the fracture?
Explanation
REFERENCES: Phillips FM: Minimally invasive treatments of osteoporotic vertebral compression fractures. Spine 2003;28:S45-S53.
Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 9
A 21-year-old basketball player reports increased left shoulder pain with all lifting and overhead activities. He denies any history of dislocations. Axial MRI arthrogram images are seen in Figures 34a and 34b. An expected finding on physical examination of the shoulder would be positive findings for which of the following tests? Review Topic
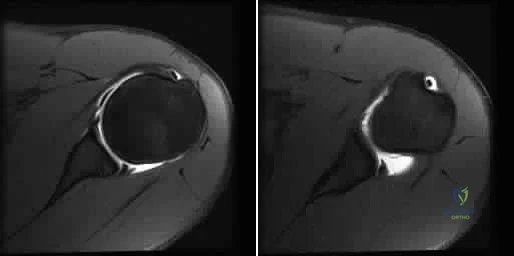
Explanation
then abducted, while maintaining the axial load, and the patient's subjective and objective response is observed. Comparison to the contralateral shoulder is important, especially if painless subluxation is noted, to determine potential evidence of generalized joint laxity.
Question 10
A 51-year-old woman who underwent a total knee arthroplasty 14 months ago for severe degenerative arthritis now reports progressive pain, swelling, and buckling of the knee. She must use crutches and is unable to negotiate stairs. Laboratory testing reveals a normal erythrocyte sedimentation rate and C-reactive protein. Radiographs of the patient are shown in Figures 17a through 17c. What is the most important test to further evaluate this problem?
Explanation
REFERENCES: Stiehl JB: Patellar instability in total knee arthroplasty. J Knee Surg 2003;16:229-235. Berger RA, Crossett LS, Jacobs JJ, et al: Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res 1998;356:144-153.
Question 11
Figures 59a and 59b are the radiographs of a 7-year-old boy who was seen 1 week after he underwent a closed reduction and casting in the emergency department after a fall on an outstretched arm. What is the most appropriate next step for this patient? Review Topic

Explanation
Question 12
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?
Explanation
REFERENCES: Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.
Hoppenfield S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp 156-176.
Question 13
A patient has a painful metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis if this patient is having a reaction to metal debris?
Explanation
Painful MOM THA and taper corrosion can cause substantial damage to a patient's hip if left untreated. In this case, the workup for a painful MOM THA starts the same as a workup for a painful metal-on-polyethylene bearing couple. Infection must be ruled out in every case with a set of inflammatory markers. If these markers are remotely elevated, this is an indication for joint aspiration. In patients with metal debris, the pathology report often indicates too many cells to count or cellular debris. Metal ion levels do not seem to correlate with prognosis. There are well-functioning patients with high ion levels and poor-functioning patients with low ion levels. Advanced imaging with MARS MRI to evaluate for peritrochanteric fluid collection, a soft-tissue mass, or synovial/capsular hypertrophy will reveal signs of a metal reaction that indicate the need for a revision discussion. A CT scan can show more advanced bony destruction as an indicator of poor prognosis. These films can be used to determine the need for a structural graft or augments for reconstruction of bone loss attributable to metal debris.
Question 14
After closed reduction of the dislocation shown in Figure 42, it is essential to avoid placing the upper extremity in what position for the first 4 to 6 weeks?
Explanation
REFERENCES: Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1986;68:724-731.
Pollock RG, Bigliani LU: Recurrent posterior shoulder instability: Diagnosis and treatment.
Clin Orthop 1993;291:85-96.
Question 15
A 12-year-old girl with foot pain who has been diagnosed with hereditary motor sensory neuropathy is seen for the foot deformity shown in Figure 59a. A “block test” is performed and shown in Figure 59b. What is the most appropriate management for this patient?
Explanation
REFERENCES: Paulos L, Coleman SS, Samuelson KM: Pes cavovarus: Review of a surgical approach
using selective soft-tissue procedures. J Bone Joint Surg Am 1980;62:942-953.
McCluskey WP, Lovell WW, Cummings RJ: The cavovarus foot deformity: Etiology and management. Clin Orthop Relat Res 1989;247:27-37.
Ward CM, Dolan LA, Bennett DL, et al: Long-term results of reconstruction for treatment of a flexible
cavovarus foot in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 2008;90:2631-2642.
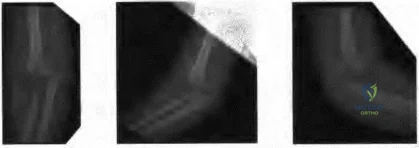
Figure 60a Figure 60b Figure 60c
Question 16
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
REFERENCES: Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
Question 17
A 35-year-old man falls off of a roof and sustains an extra-articular supracondylar elbow fracture. He had normal sensation in all fingers after the injury and before undergoing surgery to repair the fracture. The ulnar nerve was not transposed but was inspected prior to wound closure. Ten days after surgery, the patient has numbness in his small finger and is unable to cross his fingers. His elbow range of motion is 40° to 100°. What is the next appropriate step in management?
Explanation
Question 18
A 42-year-old patient undergoes resection of the medial clavicle for painful sternoclavicular degenerative joint disease. The postoperative course is complicated by an increase in symptoms, a medial bump, and subjective tingling in the digits. A clinical photograph and radiograph are shown in Figures 20a and 20b. What is the most appropriate procedure at this time?
Explanation
REFERENCES: Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA,
WB Saunders, 2004, vol 2, pp 608-609.
Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Question 19
An elite football player has sustained a left knee injury during play. A dynamic imaging analysis is performed on the affected knee, which shows anterior shift and internal rotation of the tibia at low flexion angles. There is also some mild medial translation of the tibia at greater flexion angles. What structure(s) have most likely been injury? Review Topic
Explanation
The ACL is the primary restraint to anterior translation of the tibia relative to the femur. It also acts as secondary restraint to tibial rotation and varus/valgus rotation. ACL-deficient knees have been shown to have abnormal knee kinematics, which has been thought to contribute to the osteoarthritis that develops after injury.
DeFrate et al. examined the knee joint kinematics of 8 patients with unilateral anterior cruciate ligament rupture using in vivo imaging. They found significant anterior shift and internal rotation of the tibia at low flexion angles in ACL-deficient knees. They also noted some medial translation of the tibia between 15° and 90° of flexion.
Illustration A shows the effect of medial tibial translation on tibiofemoral contact in ACL-deficient knees. The medial translation of the tibia causes increased contact between the tibial spine and inner surface of the medial femoral condyle. This might be a contributing factor to the joint degeneration observed in ACL-deficient patients.
Incorrect Answers:
Question 20
During a posterior cruciate ligament (PCL)-retaining total knee arthroplasty, a critical principle to remember is to
Explanation
Maintenance of the joint line and accurately tensioning the PCL are critical in the proper execution of a PCL-retaining total knee arthroplasty. Appropriate tension helps ensure femoral rollback and avoid stiffness or instability. Raising the joint line to help ensure full extension should be avoided in cruciate- retaining knees, because doing so creates an unfavorable kinematic environment. The three important principles of surgical technique needed to maintain appropriate tensioning of the PCL include 1) choosing the proper femur size to reproduce the native femoral anterior/posterior dimension, 2) reproducing the joint line by resecting as much tibia from the healthy side as will be replaced by the smallest thickness of the tibial component and, 3) ensuring that full extension is achieved by soft-tissue releases and not by taking additional distal femur, as may be done in a posterior stabilized approach. Another important principle is to re-create the natural degree of the patient’s posterior tibial slope to avoid tightness in
flexion.
Question 21
A 19-year-old female long-distance runner has an incomplete tension-side femoral neck stress fracture. Management should consist of
Explanation
REFERENCE: Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 22
A 30-year-old man has had severe knee pain and swelling for 1 week. He reports he previously had acromioclavicular joint pain that disappeared. He denies any fever. Aspiration of a cloudy fluid from the knee reveals a WBC count of greater than 50,000 with 90% polymorphonucleocytes. While awaiting culture results, what is the most appropriate action?
Explanation
Question 23
All of the following conditions are associated with the female athlete triad EXCEPT? Review Topic
Explanation
The female athlete triad is an interrelationship of menstrual dysfunction (i.e., amenorrhea or oligomenorrhea), low energy availability (insufficient caloric intake for demand, with or without an eating disorder) and decreased bone mineral density. It is relatively common among young women participating in sports. More recently, it has been suggested that endothelial dysfunction also results, due to an imbalance between vasodilating and vasoconstricting agents triggered from inappropirate levels of nitric oxide on the microscopic level, which predisposes these women to atherosclerotic changes and increases their risk of cardiovascular disease in the future.
Matheson et al. analyzed cases of 320 athletes with bone scan-positive stress fractures (M = 145, F = 175) seen over 3.5 years and assessed the results of conservative management. They found that conservative treatment of stress fractures in athletes is satisfactory in the majority of cases.
Constantini et al. evaluated the prevalence of vitamin D insufficiency and deficiency among young athletes and dancers. They found a higher rate of vitamin D insufficiency among participants who practice indoors, during the winter months, and in the presence of iron depletion.
Nazem et al. reviewed the major components and health consequences of the female athlete triad as well as strategies for diagnosis and treatment of the conditions. They concluded that treatment requires a multidisciplinary approach involving health care professionals as well as coaches and family members.
Yagi et al. followed 230 runners participating in high school running teams for a total of 3 years to report occurrence of medial tibial stress syndrome (MTSS) and stress fracture. Predictors of MTSS and stress fracture were investigated. The authors reported a significant relationship between BMI, internal hip rotation angle and MTSS infemales.
Incorrect Answers:
Question 24
Figures 191a and 191b are the radiographs of an 18-year-old man who had an ankle fracture requiring open reduction and internal fixation 2 years ago. He has a progressive symptomatic ankle deformity.Surgical intervention should consist of

Explanation

Question 25
A year old woman undergoes revision total knee arthroplasty for tibial component aseptic loosening. She is concerned about recurrent loosening, and tibial stem fixation options during revision are reviewed. Figure below displays a radiograph of the revision technique used for this patient. What is the incidence of intraoperative tibial shaft fracture that is associated with this type of revision surgery?
Explanation
Using press-fit tibial stems during a hybrid revision total knee arthroplasty is associated with a 3% to 5% incidence of intraoperative tibial shaft fracture. Diaphyseal fixation of press-fit stems has the advantage of setting component alignment, dispersing forces on the proximal tibia, and offers excellent clinical results. The disadvantages include proximal and distal tibia anatomic mismatch and tibial shaft fracture. Cipriano and associates reported a tibial shaft fracture incidence of 4.9% in a series of 420 consecutive
knee revisions. All fractures healed with nonsurgical management, and none led to implant loosening. In this patient, it is important to recognize on the radiograph that this technique is a hybrid method of revision total knee arthroplasty, with cementation along the tibial tray and metaphysis and with press-fit fixation of the diaphyseal engaging stem. Then, it is important to know the risk and management of intraoperative diaphyseal tibial fractures. Cemented tibial stems are associated with a low rate of intraoperative fracture, because the implant is typically undersized to allow for an appropriate cement mantle. Option C is incorrect, because this revision is not cemented. Option A underestimates the incidence of fracture,
whereas D overestimates the rate of fracture.
Question 26
Figures 34a through 34c show the radiographs of a 51-year-old woman who injured her elbow in a fall from standing height. Examination reveals that elbow range of motion is limited by pain only. Management should consist of
Explanation
function and minimize stiffness. A long arm cast for any length of time will result in severe elbow stiffness.
REFERENCES: Morrey BF: Radial head fracture, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 341-364.
Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Question 27
For this patient, which TKA design is most appropriate?
Explanation
TKA in the setting of valgus deformities poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when used as a rotational reference point, can lead to internal rotation of the femoral component if not recognized. This malrotation will in turn lead to patellofemoral maltracking or instability, which is a common complication associated with primary TKA. The deformity is too severe to consider a bicruciate-retaining TKA or unicompartmental arthroplasty and does not necessitate a hinged TKA.
Question 28
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?
Explanation
REFERENCES: Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 29
A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of 25 degrees. The O’Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management?
Explanation
REFERENCES: Wilk KE, Meister K, Andrews JR: Current concepts in rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
Myers JB, Laudner KG, Pasquale MR, et al: Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med 2006;34:385-391.
Question 30
Smoking has been associated with lower fusion rates in both cervical and lumbar fusion. Which of the following statements best describes an explanation for these findings?
Explanation
have been performed to offer an explanation of the mechanism mediating this effect. Whereas all of the above have been postulated as explanations, more recent studies have demonstrated that nicotine delivered via a transdermal patch significantly enhanced posterior spinal fusion in rabbits. Thus it appears that the effects of smoking on fracture healing are multifactorial and not yet fully understood.
Question 31
Performing reconstruction of the anterior cruciate ligament by drilling the femoral tunnel via an anteromedial portal, in contrast to transtibial drilling, affords what theoretical benefit? Review Topic
Explanation
Question 32
What is the most appropriate initial diagnostic imaging study for a patient with presumed diskogenic low-back pain?
Explanation
Radiography is the best initial study. Vacuum phenomenon may be found within the disk space. Other possible sources for back pain such as osteoporotic collapse, osteolytic collapse, and deformity also can be evaluated. The other tests may be beneficial and are more appropriate as later imaging options.
RECOMMENDED READINGS
Yu WD, Williams SL. Spinal imaging: Radiographs, computed tomography, and magnetic resonance imaging. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine
Question 33
Figures 1a and 1b are the MR images of a 69-year-old woman with bilateral leg pain that is worse with ambulation. She feels better when she is sitting down or leaning on a grocery cart. Which condition or structure is indicated by the arrows?
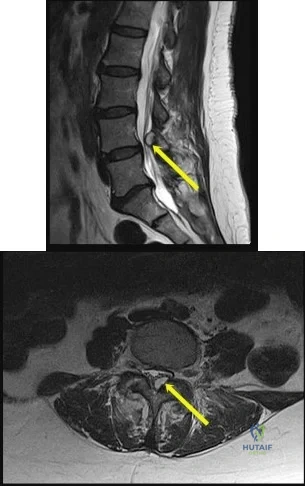
Explanation
This patient has neurogenic claudication as demonstrated by her “shopping cart” sign. Typically, spinal stenosis is attributable to bony spurs and/or a thick ligamentum flavum. However, for this patient, a large synovial cyst is the main contributing factor to stenosis. A cyst typically is filled with gelatinous material. If symptomatic, surgical excision is typically recommended because success with aspiration is unreliable. The need for fusion is debatable.
A disk herniation is not bright on T2. An arachnoid cyst is a sac filled with cerebrospinal fluid. Spinal arachnoid cysts are relatively uncommon, and typically are intradural, but they also can be extradural. Epidural lipomatosis is a condition caused by excessive accumulation of fat within the epidural space. It is not well circumscribed as seen with this lesion.
RECOMMENDED READINGS
Epstein NE, Baisden J. The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surg Neurol Int. 2012;3(Suppl 3):S157-66. doi: 10.4103/2152-7806.98576. Epub 2012 Jul 17. PubMed PMID: 22905322. View Abstract at PubMed
Xu R, McGirt MJ, Parker SL, Bydon M, Olivi A, Wolinsky JP, Witham TF, Gokaslan ZL, Bydon A. Factors associated with recurrent back pain and cyst recurrence after surgical resection of one hundred ninety-five spinal synovial cysts: analysis of one hundred sixty-seven consecutive cases. Spine (Phila Pa 1976). 2010 May 1;35(10):1044-53. PubMed PMID: 20173680. View Abstract at PubMed
Question 34
Total hip arthroplasty is most appropriate for the injury shown in Figure A for which of the following patients?

Explanation
Displaced femoral neck fractures can present a challenge to treat. In younger patients with good bone stock a closed vs. open reduction and internal fixation should be attempted. For active older patients a total hip arthroplasty is the best option, especially if there is pre-existing arthritis in the injured hip. THA provides the best function with the least pain and less need for repeat surgery (compared to hemiarthroplasty). For low-demand or debilitated patients, for patients older than age 80, or for those who can not reliably follow hip precautions a hemiarthroplasty provides the lowest risk of dislocation, and thus would be the treatment of choice.
Macaulay et al. present a prospective randomized trial of patients with femoral neck fractures treated with THA vs hemiarthroplasty. They found that functional outcomes and patient satisfaction were higher in the THA group without significant increased risk of complications. Inclusion criteria required patients to be over age 50, be a community ambulator, and were excluded for presence of dementia.
Abboud et al. retrospectively reviewed patients treated with THA for osteoarthritis and compared them to patients treated with THA for a femoral neck fracture. They found no significant difference between the two groups for outcomes or complications.
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture.
Incorrect Answers:
Question 35
A coronal MRI scan through the shoulder joint is shown in Figure 26. The cyst indicated by the arrow will most likely cause compression of what nerve?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 306-309.
Iannotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Question 36
A fracture in the following location is most commonly associated with procurvatum and valgus malalignment?
Explanation
Proximal third tibial shaft fractures are often difficult to reduce anatomically due to the tendency for both valgus and flexion deformity at the fracture site. Many different techniques have been devised to overcome the deforming forces. These include (1) Poller blocking screws posterior and lateral to the intramedullary nail (IMN), (2) utilizing a semiextended knee position during IMN of proximal tibia fractures (3) use of a suprapatellar approach for IMN, (4) usage of a slightly more lateral starting point during conventional IMN, and (5) application of unicortical plate.
Ricci et al. describe the technique and results of using blocking screws and intramedullary nails to treat patients with fractures of the proximal third of the tibia. Post-operatively, all patients in their series had less than 5 degrees of angular deformity in the planes in which blocking screws were used to control alignment. At 6 months follow-up, 10/11 patients maintained this alignment.
Illustration A shows intra-operative sagittal radiographs of the proximal tibia. Note the use of Poller blocking screws in the posterior and lateral aspects of the proximal tibia.
Incorrect Answers:
Question 37
Which of the following factors is most likely to contribute to pseudarthrosis in a patient who has undergone a single-level anterior decompression and fusion procedure for the treatment of cervical radiculopathy? Review Topic
Explanation
diabetes mellitus, have been shown to significantly increase pseudarthrosis rates. The literature has been mixed with regard to fusion rates for allograft versus autograft, especially for one-level fusions; in that category, there is minimal, if any, difference. Similarly, several authors have shown higher rates of fusion with uninstrumented single-level rather than instrumented anterior cervical decompressions and fusions. The level (ie, cranial or caudal) of fusion and sagittal alignment have not been correlated with fusion rates.
Question 38
The patient develops an inability to dorsiflex her foot 2 days after surgical intervention while she is sitting in a chair after physical therapy. Initial treatment should consist of
Explanation
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis.
This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis, observation for 1 year would not be appropriate.
The psoas is the anatomic structure that runs anterior to the acetabulum. The femoral neurovascular structures are at risk if the retractor is placed anterior and inferior to the psoas tendon.
The patient develops a foot drop 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MR imaging or a CT scan may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be decreased by flexing the surgical knee and positioning the bed flat.
Question 39
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has
Explanation
Question 40
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
REFERENCES: Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Conn RA, Colfield RH, Byer DE, Lindstromberg JW: Interscalene block anesthesia for shoulder surgery. Clin Orthop 1987;216:94-98.
Question 41
Initial management should consist of Review Topic

Explanation
Question 42
Which of the following is a recognized predictor of mortality after hip fracture?

Explanation
The study by Richmond et al looked at 836 patients treated for a hip fracture and found that this injury is not associated with significant excess mortality amongst patients older than age 85. However, in younger patients, those with ASA classifications of 3 or 4 have significant excess mortality following hip fracture that persists up to 2 years after injury.
Question 43
A patient wakes up with a foot drop following open reduction internal fixation of a posterior wall/posterior column acetabular fracture. What position of the leg causes the highest intraneural pressure in the sciatic nerve?

Explanation
Question 44
A 21-year-old throwing athlete has persistent shoulder pain. Figures 73a and 73b are arthroscopic photographs taken from a posterior viewing portal and an anterior viewing portal. During which phase of the throwing motion did the injury most likely occur? Review Topic
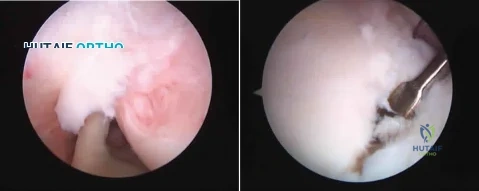
Explanation
Rotator cuff tears in throwing athletes may be the result of either tensile or compressive forces. Tensile failure is believed to be the result of repetitive eccentric contractions. Compressive failure is thought to result from direct contact of the articular side of the rotator cuff between the greater tuberosity and posterior glenoid. Compressive failure results in tearing of the posterior supraspinatus and anterior infraspinatus, in contrast to the more common partial tearing of the anterior supraspinatus seen in the general population. In addition to tearing of the articular side of the rotator cuff, compressive forces also contribute to the peel-back mechanism and resultant avulsion of the posterosuperior labrum and biceps anchor. Articular-sided posterior supraspinatus and infraspinatus tears in combination with posterosuperior labral and biceps anchor detachment has been termed internal impingement. It is believed to be the primary result of either posterior capsular contracture (GIRD) or anterior capsular laxity.
Question 45
A 55-year-old woman has slowly increasing pain at the distal end of her little finger that is exacerbated by cold temperatures. She denies any history of trauma to her hands and is employed as a school teacher. The histology of the resected specimen is shown in Figure 71. What is the most likely diagnosis?
Explanation
REFERENCES: Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
McDermott EM, Weiss AP: Glomus tumors. J Hand Surg Am 2006;31:1397-1400.
Question 46
- Figure 12 shows the frog-lateral radiograph of a 45-year-old man who has a painful left hip. What is the most likely diagnosis?
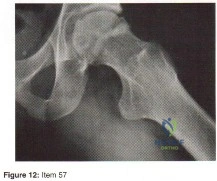
Explanation
Question 47
A 50-year-old woman who underwent a joint replacement of the hallux metatarsophalangeal joint 6 months ago now has pain and swelling about the great toe. Radiographs are shown in Figures 39a and 39b. What is the next most appropriate step in management?
Explanation
REFERENCE: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 265-266.
Question 48
Figures 6a through 6d show the radiographs and biopsy specimens of an 8-year-old girl with leg pain. Management of the lesion should consist of
Explanation
REFERENCES: Wilson AJ, Kyriakos M, Ackerman LV: Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-518.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 167-189.
Question 49
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20°. Management should consist of
Explanation
REFERENCES: Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Newton PO, Johnston CE II: Analysis and treatment of poor outcomes following in situ arthrodesis in adolescent spondylolisthesis. J Pediatr Orthop 1997;17:754-761.
Question 50
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?
Explanation
sudden death in young athletes. HCM phenotype becomes evident by age 13 to 14 years. Those at higher risk include individuals with cardiac symptoms, a family history of inherited cardiac disease, and those with a family history of premature sudden death. Echocardiography is useful for detecting structural heart disease, including the cardiomyopathies and valvular abnormalities. Trained adolescent athletes demonstrated greater absolute left ventricular wall thickness (LVWT) compared to controls. HCM should be considered in any trained adolescent male athlete with a LVWT of more than 12 mm (female of more than 11 mm) and a nondilated ventricle. Adolescent and adult athletes differ with respect to the range of LVWT measurements, as a manifestation of left ventricular hypertrophy (LVH). Differentiating LVH (“athlete’s heart”) from HCM involves looking at additional echocardiographic features. Sharma and associates reported that adolescents with HCM had a small or normal-sized left ventricle (less than 48 mm) chamber size, while those with LVH had a chamber size at the upper limits of normal (52 mm to 60 mm).
REFERENCES: Sharma S, Maron BJ, Whyte G, et al: Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete’s heart and hypertrophic cardiomyopathy. J Am College Cardiol 2002;40:1431-1436.
Maron BJ, Spirito P, Wesley Y, et al: Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med 1986;315:610-614.
Pelliccia A, Culasso F, Di Paolo FM, et al: Physiologic left ventricular cavity dilatation in elite athletes. Ann Intern Med 1999;130:23-31.
Question 51
Figure 44 shows the AP radiograph of the hip of a patient who underwent screw fixation of the acetabulum. Which of the following structures is at least risk for injury during screw placement in the acetabular component?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 207-215.
Question 52
A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of
Explanation
REFERENCE: Tasdemiroglu E, Tibbs PA: Long-term follow-up results of thoracolumbar fractures after posterior instrumentation. Spine 1995;20:1704-1708.
Question 53
Which 2 tendons are identified in the dissection shown in Video 92?
Explanation
RECOMMENDED READINGS
Babb JR, Detterline AJ, Noyes FR. AAOS Orthopaedic Video Theater. The Key to the Knee: A Layer-by-Layer Video Demonstration of Medial and Anterior Anatomy. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2009.
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:493-568.
Question 54
A 60-year-old man reports increasing pain in his right foot with limited ankle dorsiflexion and anterior ankle pain after sustaining a fracture of the calcaneus in a fall several years ago. Bracing, nonsteroidal anti-inflammatory drugs, and cortisone injections have failed to provide significant relief. Radiographs are shown in Figures 19a and 19b. What is the next most appropriate step in management?
Explanation
REFERENCE: Robinson TF, Murphy GA: Arthrodesis as salvage for calcaneal avulsions. Foot Ankle Clin 2002;7:107-120.
Question 55
Kinematic analysis of the medial and lateral menisci has demonstrated that the lateral meniscus has which of the following characteristics compared with the medial meniscus?
Explanation
REFERENCES: Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. New York, NY, Churchill Livingstone, 2001, vol 1, p 474.
Thompson WO, Thaete FL, Fu FH, et al: Tibial meniscal dynamics using 3D reconstructions
of MR images, in Proceedings of the Orthopaedic Research Society 1990;389.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy
of Orthopaedic Surgeons, 2005, pp 15-28.
Question 56
What muscle attaches to the site shown by the arrow in Figure 2?
Explanation
REFERENCES: Williams PL, Warwick R, Dyson M, Bannister LH: Neurology, in Gray’s Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 1131-1132.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 131-132.
Question 57
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Explanation
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 58
An 11-year-old basketball player reports that he felt a painful pop in the left knee when he stumbled while running. He is unable to bear weight on the extremity and cannot actively extend the knee against gravity. Examination reveals a large knee effusion. A lateral radiograph is shown in Figure 7. Management should consist of
Explanation
REFERENCES: Maguire JK, Canale ST: Fractures of the patella in children and adolescents.
J Pediatr Orthop 1993;13:567-571.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990;10:721-730.
Question 59
Patients with rheumatoid arthritis may exhibit an increase in viral load for which of the following viruses?
Explanation
REFERENCES: Callan MF: Epstein-Barr virus, arthritis, and the development of lymphoma in arthritis patients. Curr Opin Rheumatol 2004;16:399-405.
Baecklund E, Sundstrom C, Ekbom A, et al: Lymphoma subtypes in patients with rheumatoid arthritis: Increased proportion of diffuse large B cell lymphoma. Arthritis Rheum
2003;48:1543-1550.
Question 60
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in Review Topic
Explanation
Question 61
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management? Review Topic

Explanation
Question 62
An 18-year-old man sustained closed humeral shaft and forearm fractures of his dominant arm in a motor vehicle accident. Neurovascular examination is intact, and his condition is stable. The best course of action for management of the injuries should be
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Bell MJ, Beachamp CG, Kellam JK, McMurtry RY: The results of plating humeral shaft fractures in patients with multiple injuries: The Sunnybrook experience. J Bone Joint Surg Br 1985;67:293-296.
Question 63
Which of the following is most associated with local recurrence of the lesion seen in the radiograph and MRI scan shown in Figures 27a and 27b?
Explanation
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Vergel De Dios AM, Bond JR, Shives TC, et al: Aneurysmal bone cyst: A clinicopathologic study of 238 cases. Cancer 1992;69:2921-2931.
Question 64
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. Unicompartmental knee arthroplasty (UKA) is discussed with the patient. The most appropriate next radiographic evaluation should be
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 65
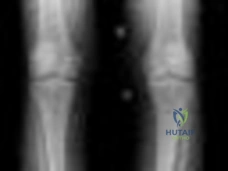
Figure 11 shows the radiograph of a 2-year-old child with marked genu varum and tibial bowing. Based on these findings, what is the best initial course of action?

Explanation
Question 66
A 32-year-old man has posttraumatic arthritis after undergoing open reduction and internal fixation of a left acetabular fracture. A total hip arthroplasty is performed, and the radiograph is shown in Figure 18. What is the most common mode of failure leading to revision in this group of patients?
Explanation
REFERENCES: Jimenez ML, Tile M, Schenk RS: Total hip replacement after acetabular fracture. Orthop Clin 1997;28:435-446.
Romness DW, Lewallen DG: Total hip arthroplasty after fracture of the acetabulum: Long-term results. J Bone Joint Surg Br 1990;72:761-764.
Question 67
A 48-year-old man has had pain and swelling of the hallux metatarsophalangeal joint for the past 9 months. A rocker bottom stiff-soled shoe has failed to provide relief; however, two cortisone injections have temporarily alleviated his symptoms. The radiographs shown in Figures 20a and 20b reveal diffuse arthritis of the entire hallux metatarsophalangeal joint. What is the most definitive surgical treatment?
Explanation
REFERENCES: Smith RW, Joanis TL, Maxwell PD: Great toe metatarsophalangeal joint arthrodesis: A user-friendly technique. Foot Ankle 1992;13:367-377.
Mann RA: Hallux rigidus. Instr Course Lect 1990;39:15-21.
Question 68
A 13-year-old girl has had right groin pain for the past 3 weeks. She denies any history of trauma. Examination of the hip reveals no palpable soft-tissue mass or lymphadenopathy, and there is full range of motion. A plain radiograph and MRI scan are shown in Figures 15a and 15b. Biopsy specimens are shown in Figures 15c and 15d. What is the most likely diagnosis?
Explanation
REFERENCES: Enneking WF, Gearen PF: Fibrous dysplasia of the femoral neck: Treatment by cortical bone grafting. J Bone Joint Surg Am 1986;68:1415-1422.
Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
Question 69
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?
Explanation
REFERENCE: Poynton AR, O’Rourke K: An analysis of skin perfusion over the Achilles tendon in varying degrees of plantar flexion. Foot Ankle Int 2001;22:572-574.
Question 70
Figure 31 shows the radiograph of a 64-year-old woman who is seen in the emergency department following a motor vehicle accident. She has no

Explanation
Question 71
Which of the following rehabilitation techniques is appropriate for initial nonsurgical management of an isolated grade 2 posterior cruciate ligament injury? Review Topic
Explanation
Question 72
An 80-year-old man with a history of chronic obstructive pulmonary disease (COPD) and dementia is involved in a fall from standing height, striking his forehead. He is seen in the emergency department with predominantly mechanical neck pain but no obvious neurologic deficits. Radiographs reveal a nondisplaced type II odontoid fracture. What is the most appropriate treatment? Review Topic
Explanation
Question 73
The swelling pressure in cartilage is predominantly due to the association of exchangeable water with which of the following substances? Review Topic
Explanation
Question 74
A sedentary 60-year-old woman has had good elbow function and pain relief after undergoing an ulnohumeral interposition arthroplasty 10 years ago. However, she currently reports pain and stiffness for the past 6 months, and nonsurgical management has failed to provide relief. Examination reveals range of motion of 40 to 110 degrees of flexion with pain during the entire range. Radiographs are shown in Figures 43a and 43b. What is the next most appropriate step in management? Review Topic

Explanation
Question 75
A healthy 2-year-old boy falls from a swing and sustains a displaced midshaft femoral fracture with 1 cm of shortening. What is the most appropriate treatment?
Explanation
DISCUSSION: For children between the ages of 1 and 6 years, closed reduction and early spica casting is recommended. In some instances, associated injuries or body habitus may preclude cast treatment. Pavlik harness treatment of femoral fractures is for infants younger than 1 year of age. Rarely is there an indication for traction. Internal fixation is reserved in general for children older than age 6 years or with confounding factors.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 271-280.
Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-359.
Figure 29a Figure 29b
Question 76
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include
Explanation
REFERENCES: Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Wenger DR, Ditkoff TJ, Herring JA, Mauldin DM: Protrusio acetabuli in Marfan’s syndrome. Clin Orthop 1980;147:134-138.
Question 77
Which of the following terms describe a rehabilitative exercise in which the foot is mobile and the motion of the knee is independent of hip and ankle motion?
Explanation
Question 78
What is the most common short-term complication following femoral impaction grafting for revision total hip arthroplasty?
Explanation
REFERENCES: Mikhail MWE, Weidenhielm L, Jazrawi LM, et al: Collarless, polished, tapered stem failure. J Bone Joint Surg Am 2000;82:1513-1514.
Leopold SS, Rosenberg AG: Current status of impaction allografting for revision of a femoral component. Instr Course Lect 2000;49:111-118.
Question 79
Figures 11a and 11b show the T 2 -weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a?
Explanation
REFERENCES: Banning CS, Thorell WE, Leibrock LG: Patient outcome after resection of lumbar juxtafacet cysts. Spine 2001;26:969-972.
Deinsberger R, Kinn E, Ungersbock K: Microsurgical treatment of juxta facet cysts of the lumbar spine. J Spinal Disord Tech 2006;19:155-160.
Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.
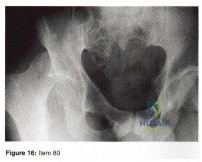
Question 80
- Figure 16 shoes the AP radiograph of a 32-year-old man with a fracture cephalad to the fovea of the femoral head. A CT scan shows a single head fragment. After closed reduction of the hip, there is 5 mm of residual articular incongruity. Management should now include
Explanation
Question 81
A 20-year-old athlete sustains a 2- x 3-cm grade IV chondral injury to the right knee. After failure of nonsurgical management, which of the following procedures would ensure the highest percentage of hyaline-like cartilage?
Explanation
REFERENCES: Brittberg M, Lindahl A, Nilsson A, et al: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 787-804.
Question 82
Arthritic change in cartilage is characterized by which of the following findings?
Explanation
Question 83
A patient has pain 2 years after undergoing a metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with a prognosis if this patient is having a reaction to metal debris?
Explanation
Question 84
What is the most common site of nerve compression in radial tunnel syndrome?
Explanation
A. Quadrigia
B. Intrinsic tightness
C. Lumbrical plus deformity
D. Disruption of the tendon repai
Question 85
Figures 2a and 2b show the radiograph and MRI scan of a 56-year-old woman who has low back pain and right leg pain. She has grade 3/5 toe and ankle dorsiflexion strength on the right side. Nonsurgical management has failed to provide relief; therefore, surgery should include Review Topic
Explanation
Question 86
A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis.
Explanation
Complications are numerous in adult spinal deformity surgery. Many complications are related to the patient's sagittal balance following surgery and recognition of the potential to develop sagittal imbalance or flat-back syndrome following spinal fusion. The quality of bone density is important in spinal instrumented fusions, especially among older patients. Patients with osteopenia or osteoporosis have a higher incidence of proximal-level screw cut-out through the vertebral body into the cephalad disk space.
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
Question 87
The patient decides to pursue surgical intervention. Which compartments should be released?
Explanation
>30 mm Hg at 1 minute post exercise, or >20 mm Hg at 5 minutes post-exercise. The anterior and lateral compartments are the only ones that meet strict diagnostic criteria for chronic exertional compartment syndrome. The superficial posterior compartment, although close to meeting criteria, is not responsible for the patient's symptoms and falls below current thresholds for diagnosis.
Question 88
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 89
Passive glycation of articular cartilage results in
Explanation
REFERENCES: DeGroot J, Verzijl N, Wenting-van Wijk MJ, et al: Accumulation of advanced glycation end products as a molecular mechanism for aging as a risk factor in osteoarthritis. Arthritis Rheum 2004;50:1207-1215.
Chen AC, Temple MM, Ng DM, et al: Induction of advanced glycation end products and alterations of the tensile properties of articular cartilage. Arthritis Rheum 2002;46:3212-3217.
Question 90
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior knee pain, a trace effusion, a 2+ posterior drawer, a grade 1+ stable Lachman, no valgus laxity, and negative dial tests at 30 degrees and 90 degrees. What is the best treatment strategy at this time? Review Topic
Explanation
Question 91
A 35-year-old male sustains a closed tibial shaft fracture after falling from 12 feet. Which of the following measurements would be concerning for an evolving compartment syndrome?

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. Determining if a patient needs fasciotomies in the operating room while a patient is under anesthesia is complicated by the fact that obtaining a clinical exam is impossible, and that the diastolic blood pressure may be falsely decreased compared to normal pre- or postoperative measurements. Currently, it is recommended that intraoperative compartment pressures be compared to preoperative diastolic blood pressures, with delta p < 30 indicating the need for fasciotomies.
Kakar et al. review the preoperative, intraoperative, and postoperative diastolic blood pressure (DBP) in 242 patients with a tibia fracture treated operatively. They found the mean DBP was 18 points lower in the operating room compared to the preoperative measurement. In addition, they found the difference between preoperative and postoperative diastolic blood pressures to be within 2 points, indicating the decrease seen intraoperatively is likely a spurious value induced by anesthetic.
McQueen and Court-Brown prospectively review 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Incorrect Answers:
Question 92
An 11-year-old boy has right shoulder pain and has been unwilling to use the arm after throwing a baseball in a Little League game 3 weeks ago. Examination reveals upper arm and shoulder tenderness with swelling. A radiograph and MRI scan are shown in Figures 27a and 27b. Management should consist of
Explanation
REFERENCES: Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 945-946.
Malawer MM: Tumors of the shoulder girdle: Techniques of resection and description of surgical classification. Orthop Clin North Am 1991;22:7-35.
Question 93
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child’s ability to walk in the future? Review Topic
Explanation
Question 94
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of
Explanation
50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann’s kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann’s kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees.
REFERENCES: Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248.
Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
Tribus CB: Scheuermann’s kyphosis in adolescents and adults: Diagnosis and management.
J Am Acad Orthop Surg 1998;6:36-43.
Question 95
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?
Explanation
REFERENCES: Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
DiCaprio MR, Enneking WF: Fibrous dysplasia: Pathophysiology, evaluation, and treatment.
J Bone Joint Surg Am 2005;87:1848-1864.
Question 96
A workers' compensation carrier for a local manufacturing company requests a second opinion on a 59-year-old man who sustained a crush injury to his foot and leg at work 6 months ago. His leg and foot were pinned between a forklift and a wall when an employee he was supervising lost control of the forklift. The employer suspects that the injured worker is malingering because the treating physician released him to work, but he has not returned to work. Which of the following elements of your history will best help you determine that the injured worker does not want to return to work out of fear of a confrontation with the employee he was supervising?
Explanation
Question 97
Figure 24 shows the radiograph of an otherwise healthy 56-year-old patient who reports hip pain after undergoing a primary cementless hip replacement 4 months ago. The next most appropriate step should consist of
Explanation
REFERENCE: Fitzgerald RH Jr: Infected total hip arthroplasty: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:249-262.
Question 98
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
Explanation
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Nonarthroplasty), level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1,500 mg/day and chondroitin sulfate 800 mg/day as well as arthroscopic debridement and lavage).
Question 99
A 10-year-old boy with an L1 myelomeningocele has a low-grade fever and a swollen thigh that is warm to touch and erythematous. AP and lateral radiographs are shown in Figures 24a and 24b. Management should consist of
Explanation
REFERENCES: Lock TR, Aronson DD: Fractures in patients who have myelomeningocele. J Bone Joint Surg Am 1989;71:1153-1157.
Kumar SJ, Cowell HR, Townsend P: Physeal, metaphyseal, and diaphyseal injuries of the lower extremities in children with myelomeningocele. J Pediatr Orthop 1984;4:25-27.
Question 100
Which of the following is considered the best method to measure limb-length discrepancy in a patient with a knee flexion contracture?
Explanation
REFERENCES: Aaron A, Weinstein D, Thickman D, et al: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Tachdjian MO: Clinical Pediatric Orthopaedics: The Art of Diagnosis and Principles of Management. Stamford, CT, Appleton and Lange, 1997, pp 237-240.
