OITE & ABOS Orthopedic MCQ Exam: Upper Extremity, Trauma & Nerve Part 34

Key Takeaway
This page provides Part 34 of a comprehensive OITE and AAOS Orthopedic Surgery Board Review. It features 100 verified, high-yield MCQs for orthopedic surgeons and residents preparing for board certification exams. Covering Elbow, Fracture, Nerve, Shoulder, Wrist, it offers interactive study and exam modes to ensure thorough preparation.
About This Board Review Set
This is Part 34 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 34
This module focuses heavily on: Elbow, Fracture, Nerve, Shoulder, Wrist.
Sample Questions from This Set
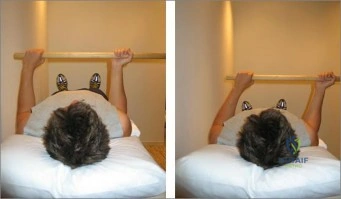
Sample Question 1: The right shoulder exercise seen in Figure A will put the LEAST amount of stretch on which structure? Review Topic...
Sample Question 2: What is the most common presenting problem in patients with cauda equina syndrome? Review Topic...
Sample Question 3: Figures 1 through 4 are the radiographs, sagittal-cut CT scan, and coronal T1 MR image of a 16-year-old boy who has wrist stiffness and pain after sustaining an injury 2 years ago. There is no bleeding from the proximal pole during surgery....
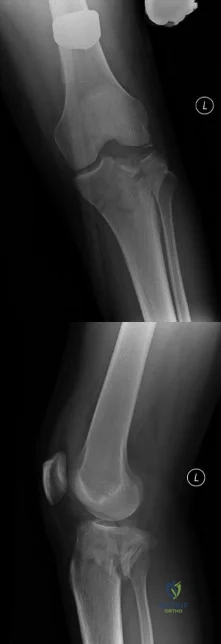
Sample Question 4: A medial plate is best used to treat tibial plateau fractures when there is...
Sample Question 5: A fracture of the radial head is surgically exposed using a posterolateral approach to the elbow. Once the radial head is exposed, how should the arm be positioned to best protect the posterior interosseous nerve from injury?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The right shoulder exercise seen in Figure A will put the LEAST amount of stretch on which structure? Review Topic
Explanation
External rotation shoulder wand exercises are commonly used for the treatment of adhesive capsulitis. Adhesive capsulitis is most commonly caused by contracture of the rotator interval. The rotator interval includes the anterior-superior capsule, superior glenohumeral ligament, coracohumeral ligament and long head biceps tendon. The structure most commonly contracted is the anterior-superior capsule, which limits external rotation when the arm is adducted.
Kuhn et al. showed that in the neutral position, each ligament except the posterior capsule significantly affected the torque required for external rotation. The greatest effect on resisting external rotation at 0 degrees of abduction was the entire inferior glenohumeral ligament > coracohumeral ligament > anterior band of the inferior glenohumeral ligament > superior and middle glenohumeral ligament.
Harryman et al. looked at the role of the rotator interval capsule in passive motion and stability of the shoulder. They found operative alteration of this capsular interval was found to affect flexion, extension, external rotation, and adduction of the humerus with respect to the scapula. Limitation of external motion was increased by operative imbrication of the rotator interval and decreased by sectioning of the rotator interval capsule.
Kim et al. reviewed shoulder MRIs to determine if abnormalities of the rotator interval were correlated with chronic shoulder instability. They found a significantly larger rotator interval height, rotator interval area, and rotator interval index in patients with chronic anterior shoulder instability compared to patients without instability.
Figure A shows a patient performing an exercise to increase right shoulder external rotation with a wand/stick. The right arm is fully adducted by her side, and her elbow flexed at 90 degrees.
Incorrect Answers:
Question 2
What is the most common presenting problem in patients with cauda equina syndrome? Review Topic
Explanation
Question 3
Figures 1 through 4 are the radiographs, sagittal-cut CT scan, and coronal T1 MR image of a 16-year-old boy who has wrist stiffness and pain after sustaining an injury 2 years ago. There is no bleeding from the proximal pole during surgery. Which procedure will most likely result in restoration of alignment and healing?

Explanation
The imaging studies show an established scaphoid waist nonunion with a humpback deformity (significant flexion through the nonunion site) and carpal collapse. In addition, the proximal pole appears sclerotic on the plain radiographs and appears poorly perfused on the MR image. Correction of alignment of this scaphoid nonunion would require a volar approach with a structural bone graft. Additionally, the graft would need to provide a vascular supply to the bone. Both the 1,2 ICSRA (the Zaidenberg graft) and the 4+5 ECA grafts are vascularized grafts from the dorsal distal radius. Neither of these grafts would correct the humpback deformity, and the 4+5 ECA graft pedicle is not long enough to reach the scaphoid. An iliac crest bone graft could be used to correct the deformity, but would not provide an adequate blood supply. A free-vascularized medial femoral condyle graft provides both adequate bone graft to correct the deformity and revascularization of the scaphoid.
Question 4
A medial plate is best used to treat tibial plateau fractures when there is
Explanation
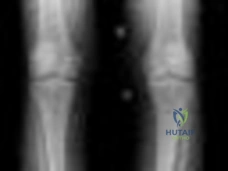
The patient's plain radiographs demonstrate a bicondylar tibial plateau fracture with complete separation of the diaphysis from the epiphysis, making this a Schatzker VI injury. Clinically, the patient is neurovascularly intact with symmetric palpable pulses, and ankle brachial indices are not necessary.
There is significant lateral tibial plateau displacement with the lateral femoral condyle down into the plateau defect. Considering the swelling, abrasions, and severity of the injury, a bridging external fixator is warranted followed by CT imaging.
The ligamentotaxis will provide better definition of the injury and joint fragments and allow for soft-tissue rest and subsidence of the swelling for eventual surgical intervention. Oblique views will not add as much information as CT imaging, which will show the bicondylar nature of the injury and the proximal tibia essentially split centrally with the tubercle as a separate fragment. A midline incision with medial and lateral plating has fallen out of
favor secondary to wound-healing complications. Comminution of the metaphysis or the lateral side is not an absolute indication for a medial plate. Open lateral fractures can still be managed with a laterally based plate depending on the soft-tissue injury.
RECOMMENDED READINGS
Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. doi: 10.1097/BOT.0b013e31818f8dc1. PubMed PMID: 19104303. View Abstract at PubMed Higgins TF, Klatt J, Bachus KN. Biomechanical analysis of bicondylar tibial plateau fixation: how does lateral locking plate fixation compare to dual plate fixation? J Orthop Trauma. 2007 May;21(5):301-6. PubMed PMID: 17485994. View Abstract at PubMed
Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164. View Abstract at PubMed
Barei DP, O'Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. doi:10.1097/BOT.0b013e318169ef08. PubMed PMID: 18317051.
View Abstract at PubMed
Barei DP, Nork SE, Mills WJ, Coles CP, Henley MB, Benirschke SK. Functional outcomes of severe bicondylar tibial plateau fractures treated with dual incisions and medial and lateral plates. J Bone Joint Surg Am. 2006 Aug;88(8):1713-21. PubMed PMID: 16882892. View Abstract at PubMed
Hall JA, Beuerlein MJ, McKee MD; Canadian Orthopaedic Trauma Society. Open reduction and internal fixation compared with circular fixator application for bicondylar tibial plateau fractures. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:74-88. doi: 10.2106/JBJS.G.01165. PubMed PMID: 19255201. View Abstract at PubMed
Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg Am. 2011 Aug 17;93(16):1548-59. PubMed PMID: 22204013. View Abstract at PubMed
Weil YA, Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Posteromedial supine approach for reduction and fixation of medial and bicondylar tibial plateau fractures. J Orthop Trauma. 2008 May-Jun;22(5):357-62. doi: 10.1097/BOT.0b013e318168c72e. PubMed PMID:
Question 5
A fracture of the radial head is surgically exposed using a posterolateral approach to the elbow. Once the radial head is exposed, how should the arm be positioned to best protect the posterior interosseous nerve from injury?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, p 100.
Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 106.
Question 6
An otherwise healthy 76-year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in Figures below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?

Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 7
Use of titanium elastic nailing for treatment of pediatric femur fractures is associated with a higher complication rate among
Explanation
Studies of titanium elastic nailing for femur fractures demonstrated a higher rate of complications, including angular deformity and construct failure, among patients weighing more than 50 kg (100 pounds). Other methods of fixation are recommended for these patients. Flexible nails are not commonly needed, but they also are not associated with a higher complication rate in children younger than age 6.5. Titanium elastic nailing works well in closed or minimally open transverse midshaft fractures, even in the setting of early or immediate weight bearing.

Video 8a
Video 8b
Question 8
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement? Review Topic

Explanation
Question 9
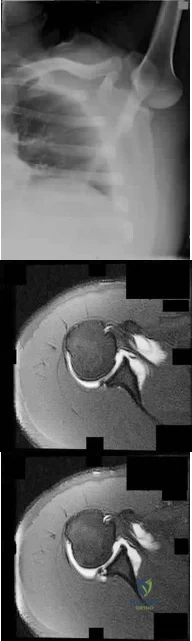
This image represents the end stage of an uncompensated rotator cuff tear.
Explanation
Axillary lateral and anteroposterior (AP) images of the right shoulder (Figures 59c and 59d) reveal osteoarthrosis of the glenohumeral joint, which typically is not associated with significant rotator cuff pathology. An examination often shows limitations in range of motion, crepitance, and pain with motion. An AP radiographic image of the right shoulder (Figure 59b) reveals proximal humeral migration, which normally correlates with rotator cuff tear size. Tears extending into the infraspinatus tendon are associated with more humeral migration than is seen with isolated supraspinatus tears. Presenting complaints are usually of pain and weakness. Examination findings include subacromial crepitance and weakness during rotator cuff testing. Rarely, this may be associated with pseudoparalysis in large uncompensated rotator cuff tears. The CT image of the right shoulder (Figure 59a) shows superior migration of the humerus with respect to the glenoid surface and end-stage
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. View Abstract at PubMed
Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
Question 10
A 48-year-old male is involved in a motorycycle accident and arrives in the trauma bay in hypovolemic shock. He receives 6 units of packed red blood cells during his resuscitation. Which of the following viral microbes is he most at risk of exposure from the transfusions?

Explanation
Question 11
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient experiences little improvement with activity modification and more physical therapy. An intra-articular corticosteroid injection provides excellent relief, but relief only lasts for 1 month. The player requests further treatment for his hip and is counseled regarding surgical intervention. Hip arthroscopy is performed. Intraoperatively, a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. Which treatment is most appropriate considering these findings?
Explanation
Question 12
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
REFERENCES: Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of twenty cases. J Pediatr Orthop 1990;10:442-444.
Hoffer MM, Wickenden R, Roper S: Brachial plexus birth palsies. J Bone Joint Surgery Am 1978;60:692-695.
Question 13
A 38-year-old man has an enlarging left paraspinal soft-tissue mass. Based on the MRI scans and biopsy specimens shown in Figures 32a through 32e, what is the most likely diagnosis?
Explanation
of surgical resection, radiation therapy, chemotherapeutic protocols, hormone modulation, and/or anti-inflammatory medications.
REFERENCES: Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 309-337.
Spear MA, Jennings LC, Mankin HJ, et al: Individualizing management of aggressive fibromatoses. Int J Radiat Oncol Biol Phys 1998;40:637-645.
Question 14
Arthritic change in cartilage is characterized by which of the following findings?
Explanation
Question 15
For patients undergoing a surgical procedure where the risk of requiring a transfusion is less than 10%, the International Committee of Effective Blood Usage suggests
Explanation
REFERENCES: Toy P, Beattie C, Gould S, et al: Transfusion alert: Use of autologous blood. National Heart, Lung, and Blood Institute Expert Panel on the use of autologous blood. Transfusion 1992;35:703-711.
Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 16
Which of the following structures is most commonly involved in lateral epicondylitis?
Explanation
REFERENCES: Nirschl RP: Elbow tendinosis/tennis elbow. Clin Sports Med 1992;11:851-870.
Regan W, Wold LE, Coonrad R, Morrey BF: Microscopic histopathology of chronic refractory lateral epicondylitis. Am J Sports Med 1992;20:746-749.
Question 17
Figures 1 through 5 show the radiographs obtained from a 37-year-old man who has a 10-year history of right, ulnar-sided wrist pain and a volar ulnar prominence with wrist supination. Approximately 20 years ago, he had a forearm injury that was definitively treated in a long arm cast. What surgical treatment option is most likely to improve his symptoms and maintain pronosupination?

Explanation
The patient sustained a radial shaft fracture with subsequent apex volar malunion. As a result, his distal ulna subluxates volarly with wrist supination. Radiographs of the wrist reveal minimal arthritic changes. The most appropriate treatment option is to surgically correct his radial shaft malunion, which would indirectly address his DRUJ instability. A DRUJ ligament reconstruction or triangular fibrocartilage complex repair could be used to augment DRUJ stability; however, they might be unnecessary after correction of the radial shaft malunion. A DRUJ ligament reconstruction alone would not achieve stability of the DRUJ joint and maintain full wrist pronosupination. An ulnar head implant arthroplasty would not be reliable in eliminating the instability or the pain. Similarly, a one-bone forearm procedure might
improve the patient's pain and instability but at the cost of abnormal wrist and forearm mechanics and kinematics.
Question 18
A 73-year-old man presents to your clinic many years after undergoing total shoulder arthroplasty with pain and the radiographic findings demonstrated in Figure 56. The most likely cause of this patient’s pain is

Explanation
The radiograph shows proximal humeral migration and loosening of the glenoid component. Proximal migration of the humeral head may represent rotator cuff dysfunction and can lead to progressive failure of the glenoid component. Stress shielding will not cause lysis or loosening of the glenoid component. Humeral osteolysis is an uncommon finding and is not shown. Progressive glenoid arthrosis is not possible with a resurfaced glenoid.
RECOMMENDED READINGS
Hill JM, Norris TR. Long-term results of total shoulder arthroplasty following bone-grafting of the glenoid. J Bone Joint Surg Am. 2001 Jun;83-A(6):877-83. PubMed PMID: 11407796.View Abstract at PubMed
Fox TJ, Cil A, Sperling JW, Sanchez-Sotelo J, Schleck CD, Cofield RH. Survival of the glenoid component in shoulder arthroplasty. J Shoulder Elbow Surg. 2009 Nov-Dec;18(6):859-63. doi: 10.1016/j.jse.2008.11.020. Epub 2009 Mar 17. PubMed
PMID: 19297199.View Abstract at PubMed
Question 19
A patient wakes up with a foot drop following open reduction internal fixation of a posterior wall/posterior column acetabular fracture. What position of the leg causes the highest intraneural pressure in the sciatic nerve?

Explanation
Question 20
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern? Review Topic
Explanation
Question 21
Titanium and its alloys are unsuitable candidates for which of the following implant applications?
Explanation
REFERENCES: McKellop HA, Sarmiento A, Schwinn CP, et al: In vivo wear of titanium-alloy hip prostheses. J Bone Joint Surg Am 1990;72:512-517.
Salvati EA, Betts F, Doty SB: Particulate metallic debris in cemented total hip arthroplasty. Clin Orthop 1993;293:160-173.
Evans BG, Salvati EA, Huo MH, et al: The rationale for cemented total hip arthroplasty. Orthop Clin North Am 1993;24:599-610.
Question 22
A 31-year-old woman has a history of a painful ankle that has failed to respond to conservative management. She has associated night pain that is relieved with nonsteroidal anti-inflammatory drugs. MRI and technetium Tc 99m scans are consistent with an osteoid osteoma. Management should now consist of
Explanation
REFERENCES: Donley BG, Philbin T, Rosenberg GA, Schils JP, Recht M: Percutaneous CT guided resection of osteoid osteoma of the tibial plafond. Foot Ankle Int 2000;21:596-598.
Kenzora JE, Abrams RC: Problems encountered in the diagnosis and treatment of osteoid osteoma of the talus. Foot Ankle 1981;2:172-178.
Shereff MJ, Cullivan WT, Johnson KA: Osteoid-osteoma of the foot. J Bone Joint Surg Am 1983;65:638-641.
Question 23
What is the most common donor site complication following a free vascularized fibular graft for osteonecrosis of the femoral head?
Explanation
REFERENCE: Urbaniak J, Harvey E: Revascularization of the femoral head in osteonecrosis. J Am Acad Orthop Surg 1998;6:44-54.
Question 24
What is the most anatomic location for placement of the femoral tunnel in anterior cruciate ligament reconstruction?
Explanation
REFERENCES: Johnson RJ, Beynnon BD, Nichols CE, Renstrom PA: The treatment of injuries of the anterior cruciate ligament. J Bone Joint Surg Am 1992;74:140-151.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Question 25
The attachments of the transverse carpal ligament include which of the following structures?
Explanation
REFERENCES: Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 471-472.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 168-170.
Question 26
Which of the following is the only nonreversible effect of anabolic steroids?
Explanation
Once anabolic steroids are stopped, muscle hypertrophy and training gains are quickly lost and the HDL/ LDL ratios return to their preexisting levels. Fortunately, the personality effects and the acute acne are reversible.
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Evans NA: Current concepts in anabolic-androgenic steroids. Am J Sports Med 2004;32:534-542.
Question 27
Which of the following best describes heat stroke? Review Topic
Explanation
Question 28
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the
Explanation
REFERENCES: Miller DB Jr: Arthroscopic meniscus repair. Am J Sports Med 1988;16:315-320.
Nawab A, Hester PW, Caborn DN: Arthroscopic meniscus repair, in Miller MD, Cole BJ (eds): Textbook of Arthroscopy. Philadelphia, PA, WB Saunders, 2004, pp 517-537.
Question 29
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What factor most strongly correlates with the development of compartment syndrome after this injury?
Explanation
REFERENCES: Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
Question 30
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?
Explanation
REFERENCES: Brodsky AE, Khalil MA: Talar compression syndrome. Am J Sports Med 1986;14:472-476.
Wredmark T, Carlstedt CA, Bauer H, Saartok T: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Question 31
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 32
Which muscles are responsible for the displacement of the proximal fragment of the fracture shown in Figure 75?

Explanation
(SBQ12TR.39) A 36-year-old male falls from a 10-ft scaffold and suffers the injuries shown in Figures A and B. The patient is placed in a spanning external fixator and brought back to the operating room once his soft tissues are amenable. Planning to use a dual-incision approach, what is the correct interval to use when approaching the medial side?
Popliteus and pes anserine
Lateral head of the gastrocnemius and pes anserine
Politeus and lateral head of the gastrocnemius
Iliotibial band and medial head of the gastrocnemius
Pes anserine and medial head of the gastrocnemius
The posteromedial approach to the tibial plateau is between the the pes anserine tendons and the medial head of the gastrocnemius.
A dual-incision approach is often utilized to optimally place definitive fixation for bicondylar tibial plateau fractures. For fractures that require posterior or posteromedial fixation, the correct interval is between the pes anserine and the medial head of the gastrocnemius.
Higgins et al. in a large cohort morphological review, noted a high incidence of a posteromedial fragment in bicondylar fractures. Occurring at a high frequency, the
authors recommended direct visualization and reduction via a dual approach rather than using indirect reduction techniques.
Falker et al. describes a step-by-step approach to utilizing the posteromedial approach for the tibial plateau and placing an anti-glide plate.
Figure A and B exhibit a bicondylar tibial plateau fracture with a posteromedial fragment noted on the lateral x-ray. Illustration A exhibits the surrounding anatomy and interval in between the medial head of the gastrocnemius and the pes anserine.
Incorrect answers:
Question 33
Os naviculare is present in which percentage of normal feet?
Explanation
Accessory navicular is found in 10% to 14% of normal feet, is generally asymptomatic, and involves 3 radiographic types. Type I represents a small ossicle embedded within the posterior tibial tendon, type II is larger with a synchondrosis, and type III is fused to the navicular tuberosity. Approximately 50% of patients with symptoms have flexible flatfoot; however, os naviculare is not directly associated with pes planovalgus deformity.
Subtalar arthroereisis describes the use of a sinus tarsi plug or implant to restrict eversion of the subtalar joint. This surgical procedure has been used in combination with tendon reconstruction for treatment of flexible flatfoot deformity. Known complications of subtalar arthroereisis include persistent sinus tarsi pain, foreign body reaction, implant failure, and osteonecrosis of the talus.
The FDL tendon travels within the same compartment adjacent to the posterior tibial tendon and is the most commonly used tendon transfer for treatment of stage II PTTD (strength characteristics are similar). The plantaris has inferior tendon strength to the FDL, and the peroneus longus travels in a different compartment than the FDL.
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Alvarez RG, Price J, Marini A, Turner NS, Kitaoka HB. Adult acquired flatfoot deformity and posterior tibial tendon dysfunction. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:215-229.
Pinney SJ, Lin SS. Current concept review: acquired adult flatfoot deformity. Foot Ankle Int. 2006 Jan;27(1):66-75. Review. PubMed PMID: 16442033. View Abstract at PubMed
Viladot R, Pons M, Alvarez F, Omaña J. Subtalar arthroereisis for posterior tibial tendon dysfunction: a preliminary report. Foot Ankle Int. 2003 Aug;24(8):600-6. PubMed PMID: 12956565. View Abstract at PubMed
Question 34
An otherwise healthy 32-year-old man who underwent an uneventful L5-S1 lumbar microdiskectomy 6 weeks ago now reports increasing and severe back pain that awakens him from sleep. Examination reveals a benign-appearing wound, and the neurologic examination is normal. Laboratory studies show an erythrocyte sedimentation rate (ESR) of 90 mm/h and a WBC of 9,000/mm3. Plain radiographs are normal. What is the next most appropriate step in management?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 35
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms?
Explanation
L4 root which exits a level above this at the L4-5 foramen. A stocking distribution is nonanatomic and not indicative of a specific root.
REFERENCES: Magee D: Principles and concepts, in Orthopaedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Aeschbach A, Mekhail NA: Common nerve blocks in chronic pain management. Anesthesiol Clin North Am 2000;18:429-459.
Question 36
Which of the following factors will adversely affect bone ingrowth in a revision porous-coated stem?
Explanation
REFERENCES: Berry DJ, Harmsen WS, Ilstrup D, Lewallen DG, Cabanela ME: Survivorship of uncemented proximally porous-coated femoral components. Clin Orthop 1995;319:168-177.
Cook SD, Thomas KA, Haddad RJ Jr: Histologic analysis of retrieved human porous-coated total joint components. Clin Orthop 1988;234:90-101.
Spector M: Historical review of porous-coated implants. J Arthroplasty 1987;2:163-177.
Question 37
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
REFERENCES: Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Weinstein DM, McCann PD, McIlveen SJ, Flatow EL, Bigliani LU: Surgical treatment of complete acromioclavicular dislocation. Am J Sports Med 1995;23:324-331.
Question 38
Figure 14 is a sagittal-cut MR image from the hindfoot of a 54-year-old woman who has had plantar heel pain for 3 months. There is no history of trauma. Her pain is worse when she rises and at the end of the day. Upon examination she has localizable tenderness over the plantar medial tubercle of the calcaneus. The Achilles is intact and nontender, and subtalar joint motion is full and painless. A Tinel test result is negative. What is the most likely diagnosis?

Explanation
Plantar fasciitis is inflammation of the plantar fascia at its insertion onto the medial calcaneus. The T2-weighted sagittal MR image reveals thickening of the plantar fascia with no evidence of a calcaneal stress fracture, coalition, or inflammation of the insertion of the Achilles tendon.
RECOMMENDED READINGS
Lareau CR, Sawyer GA, Wang JH, DiGiovanni CW. Plantar and medial heel pain: diagnosis and management. J Am Acad Orthop Surg. 2014 Jun;22(6):372-80. doi: 10.5435/JAAOS-22-06-
Question 39
A 26-year-old man sustained an isolated injury to his left hip joint in a motor vehicle accident. Closed reduction was performed, and the postreduction radiograph is shown in Figure 29. Management should now consist of
Explanation
REFERENCES: Tile M, Olson SA: Decision making: Non operative and operative indications for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 496-532.
Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993, pp 337-339, p 507.
Question 40
A 40-year-old unrestrained passenger reports chest wall pain after a motor vehicle accident. Which of the following structures is most important in preventing the injury shown in Figure 33?
Explanation
REFERENCES: Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.
Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Question 41
A 13-year-old girl is diagnosed with a stage IIB osteosarcoma of the proximal tibia. Following neoadjuvant chemotherapy, local control should consist of
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue. Philadelphia, PA, Lippincott Raven, 1998, p 274.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 42
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms? Review Topic
Explanation
Question 43
A 10-year-old girl has a midshaft both bone forearm fracture. After attempted closed reduction, alignment consists of bayonet apposition, 10° of malrotation, and 8° of volar angulation. Management should now consist of
Explanation
REFERENCES: Do TT, Strub WM, Foad SL, et al: Reduction versus remodeling in pediatric distal forearm fractures: A preliminary cost analysis. J Pediatr Orthop B 2003;12:109-115.
Flynn JM: Pediatric forearm fractures: Decision making, surgical techniques, and complications. Instr Course Lect 2002;51:355-360.
Ring D, Waters PM, Hotchkiss RN, et al: Pediatric floating elbow. J Pediatr Orthop 2001;21:456-459.
Noonan KJ, Price CT: Forearm and distal radius fractures in children. J Am Acad Orthop Surg 1998;6:146-156.
Question 44
What is the best option for treatment of the fracture shown in Figure 55?

Explanation
Question 45
Figures 1 and 2 are the radiographs of a 40-year-old woman who sustained a twisting injury to her lower extremity. What additional information or studies are important in determining treatment options?

Explanation
(SBQ12TR.24) In each of the following scenarios, atrophic fracture nonunion occurred after initial treatment with intramedullary nail fixation. Which scenario has shown to have the highest rate of osseous union if treated with exchange intramedullary nailing?
Oligotrophic nonunion of a comminuted humeral shaft fracture
Oligotrophic nonunion of a transverse humeral shaft fracture
Oligotrophic nonunion of an oblique distal femur fracture
Oligotrophic nonunion of a comminuted tibial shaft fracture
Oligotrophic nonunion of an oblique tibial shaft fracture
Reamed exchange nailing is recommended for the management of aseptic nonunions of noncomminuted tibial shaft fractures. Union rates have been reported between 76-96% in large studies.
Tibial exchange nailing promotes osseous bone healing of non-unions by providing biological and mechanical support. The biological support is provided by reaming the medullary canal. This increases periosteal blood flow and stimulates periosteal new-bone formation. The mechanical support is provided by a larger-diameter intramedullary nail, which increases the rigidity and strength of the nail.
Brinker et al. reviewed the concept of exchange nailing of nonunited long bone fractures. They showed that exchange nailing is the most successful in the treatment of nonunions following closed or open fractures without substantial bone loss. Aseptic, noncomminuted diaphyseal femoral and tibial shaft fractures showed the highest rates of union with exchange nailing, which were found to be 76-100% and 72-96%, respectively.
Illustration A shows a heterotrophic non-union of the tibia after intramedullary nailing. The patient was treated with exchange nailing with a larger nail. On the right shows a 4 month post-op radiograph after exchange nailing showing osseous union at the fracture site.
Incorrect Answers:
(SBQ12TR.79) A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2 weeks. Which of the following would be an indication for surgical management?
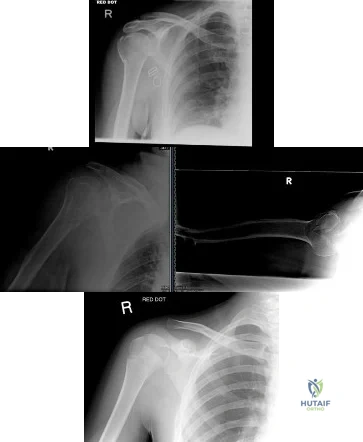
Age greater than 70 years.
Fracture pattern in Figure A
Significant medical comorbidities.
Fracture pattern in Figure B
Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is
displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:
Question 46
Figures 1 and 2 are the radiographs of an 18-year-old man who had surgery 6 months ago at an outside institution. He is being referred now because he has persistent pain. He is tender over the scaphoid at the snuffbox. What is the most appropriate next imaging step in his pain workup?

Explanation
Scaphoid nonunions are difficult to diagnose on plain radiographs, which offer poor reliability when attempting to determine if there is bridging trabeculae crossing the fractures site. CT scans are more useful for diagnosing scaphoid nonunion. When scanned using conventional axial cuts, the slices mayskip through the fracture nonunion site, thereby missing the defect, even with reformats. MR imaging is useful in diagnosing acute scaphoid fractures and has a high sensitivity and diagnostic value for excluding scaphoid fractures as well. Contrast does not enhance the utility of MR imaging in fracture diagnosis.
Question 47
A 3-year-old patient with L3 myelomeningocele has bilateral dislocated hips. Management should consist of
Explanation
REFERENCES: Fraser RK, Hoffman EB, Sparks LT, et al: The unstable hip and mid-lumbar myelomeningocele. J Bone Joint Surg Br 1992;74:143-146.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-76.
Question 48
A 59-year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Figure 1. Postreduction CT is shown in Figures 2 through 4. What is the most appropriate definitive surgical treatment?
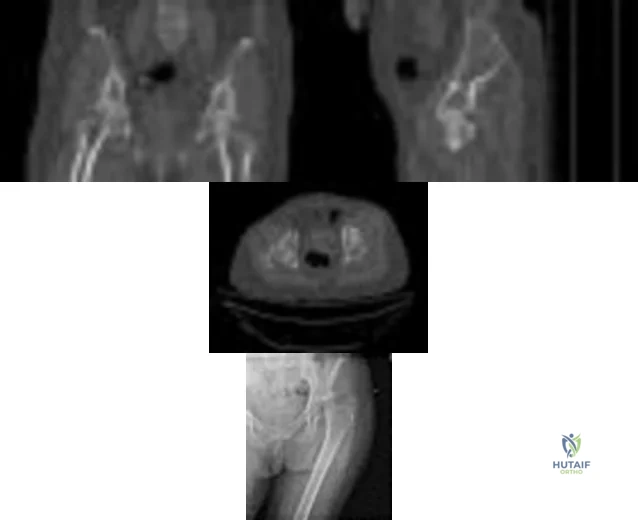
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 49
A 28-year-old man sustains the closed injury shown in Figures 3a through 3c after falling 8 feet while rock climbing. Management should consist of
Explanation
REFERENCES: Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp
1465-1518.
Grob D, Simpson LA, Weber BG, Bray T: Operative treatment of displaced talus fractures. Clin Orthop 1985;199:88-96.
Question 50
A patient has a C6 spinal cord injury. Following stabilization of the spine, the patient should be advised that their expected maximum level of function
Explanation
Question 51
An 84-year-old female community ambulator with a history of hypertension undergoes a right hip hemiarthroplasty for a femoral neck fracture. When performed in the post-operative period, the timed up and go (TUG) test may be used to predict which patient outcome?
Explanation
Hip fractures are a cause of significant functional decline for elderly patients. Many outcome tests have been developed to prediction function after hip fracture to manage patient expectations and to assist in rehabilitation planning. The TUG test objectively measures functional mobility and dynamic balance. The test is performed by timing the amount of seconds it requires for a patient to stand up from a chair, walk 10ft (3.05m), return to the chair, and sit.
Laflamme et al performed a prospective study evaluating the utility of the TUG test to predict functional outcomes in patients undergoing hip hemiarthroplasty for femoral neck fracture. The TUG scores were significantly higher at 4-days and 3-weeks postoperatively in patients requiring a walking aid compared with patients walking independently at two-years. Patients who performed the test in >58s at 4-days postoperatively had an eightfold greater risk of requiring an assistive device.
Springer et al prospectively analyzed the unipedal stance test (UPST) with eyes open and closed in healthy subjects to establish normative values for the test across age and gender groups. Performance on the test was found to be age-specific and not related to gender. The UPST is a method of quantifying static balance ability.
Kristensen et al studied the relative and absolute inter tester reliability of TUG in patients with hip fractures. The authors found that the TUG has a high interobserver reliability and an improvement by 6.2 seconds for a patient with a baseline of 20s indicates a change in functional mobility.
Video A shows the timed up and go test.
Incorrect Answers:
Question 52
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by
Explanation
REFERENCES: Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Miller SD: Ankle fractures, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1341-1366.
Question 53
Compact bone, titanium, stainless steel, cobalt-chrome Modulus of elasticities are as follows in Gpa (psi 3 10 6 ):
Explanation
Which of the following precautionary measures should be taken to prevent a periprosthetic fracture when removing components from a patient with a previous compression hip screw:
Question 54
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10°. Initial management should consist of
Explanation
REFERENCES: Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
Franco AH: Pes cavus and pes planus: Analyses and treatment. Phys Ther 1987;67:688-694.
Question 55
A 13-year-old boy has pain and a firm mass in his left knee. A radiograph and MRI scan are shown in Figures 2a and 2b, and a biopsy specimen is shown in Figure 2c. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 267.
Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990,
pp 14-15.
Question 56
What changes in muscle physiology would be expected in an athlete who begins a rigorous aerobic program for an upcoming marathon?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 89-125.
Thayer R, Collins J, Noble EG, et al: A decade of aerobic endurance training: Histological evidence for fibre type transformation. J Sports Med Phys Fitness 2000;40:284-289.
Question 57
Which of the following indicates resolution of a postoperative wound infection? Review Topic
Explanation
Question 58
An 18-month-old child was involved in a motor vehicle accident and sustained an isolated injury to the left upper extremity. A radiograph is shown in Figure 33. What is the most appropriate management for this injury?

Explanation
Question 59
What is the most common non-anesthetic-related reversible cause of sustained changes in intraoperative neurophysiologic monitoring signals during spinal surgery? Review Topic
Explanation
Question 60
What malignant disease most commonly develops in conjunction with chronic osteomyelitis?
Explanation
REFERENCES: Dell PC: Hand, in Simon MA, Springfield D (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 405-420.
McGrory JE, Pritchard DJ, Unni KK, Ilstrup D, Rowland CM: Malignant lesion arising in chronic osteomyelitis. Clin Orthop 1998;362:181-189.
Question 61
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?
Explanation
REFERENCES: Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 62
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis?
Explanation
REFERENCES: Neviaser TJ: The anterior labroligamentous periosteal sleeve avulsion lesion:
A cause of anterior instability of the shoulder. Arthroscopy 1993;9:17-21.
Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the shoulder. Am J Sports Med 2005;33:1088-1105.
Question 63
Oxidation of polyethylene after sterilization occurs most rapidly when the implant undergoes
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Wright TM: Ultra-high molecular weight polyethylene, in Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 37-46.
Collier JP, Sutula LC, Currier BH, et al: Overview of polyethylene as a bearing material: Comparison of sterilization methods. Clin Orthop 1996;333:76-86.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 64
Figures 41a and 41b show the radiographs of a 22-year-old woman who has a bunion on her left foot. She denies pain in the foot, but she reports increasing difficulty with shoe wear. Management should consist of
Explanation
REFERENCE: Mann RA, Coughlin MJ: Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 174.
Question 65
ofhat parameter is most commonly used to estimate the maximum tension a muscle can generating?
Explanation
The concept of physiologic cross section of a muscle from Weber and Fick, identifies the critical importance of the cross sectional area of all the fibers of a muscle as proportional to maximum tension. (Relationship between muscle size and muscle strength).
Question 66
What is the mechanism of action of bisphosphonates?
Explanation
REFERENCES: Gass M, Dawson-Hughes B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 226-227.
Question 67
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient? Review Topic
Explanation
Question 68
A 35-year-old man sustains a closed Monteggia fracture. Examination reveals that sensation, vascular status, and finger flexion are normal. When he extends his wrist, it deviates radially, and he is unable to extend his fingers or thumb. After reduction of the fracture, what is the next step in treatment for the extensor deficits of the thumb and fingers?
Explanation
REFERENCES: Jessing P: Monteggia lesions and their complicating nerve damage. Acta Orthop Scand 1975;46:601-609.
Stein F, Grabias SL, Deffer PA: Nerve injuries complicating Monteggia lesions. J Bone Joint Surg Am 1971;53:1432-1436.
Question 69
A subtrochanteric femur fracture in which the lesser trochanter is intact is associated with what deformity?
Explanation
Question 70
When the great toe deviates into a valgus position, the action of the abductor hallucis muscle becomes one of
Explanation
REFERENCES: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 71
A 10-year-old boy has activity-related knee pain that is poorly localized. He denies locking, swelling, or giving way. Examination shows mild tenderness at the medial femoral condyle and painless full range of motion without ligamentous instability. Radiographs are shown in Figures 2a through 2c. What is the best course of action?
Explanation
REFERENCES: Linden B: Osteochondritis dissecans of the femoral condyles: A long term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
Cahill BR: Osteochondritis dissecans of the knee: Treatment of juvenile and adult forms. J Am Acad Orthop Surg 1995;3:237-247.
Cahill BR, Navarro R: The results of conservative management of juvenile osteochondritis dissecans using joint scintigraphy: A prospective study. Am J Sports Med 1989;17:601-606.
Question 72
Figure 14 shows an intra-articular gadolinium-enhanced MRI scan of a 52-year-old woman who has stopped playing tennis because of pain in her left shoulder while serving. What is the most likely diagnosis?
Explanation
REFERENCES: Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Iannotti JP, Zlatkin MB, Esterhai JL, et al: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29.
Question 73
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?

Explanation
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (<24 hours) or multiorgan failure (>24 hours).
Incorrect Answers: Choices 1-4 are not as predictive of mortality as choice 5.
Question 74
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. Unicompartmental knee arthroplasty (UKA) is discussed with the patient. The most appropriate next radiographic evaluation should be
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 75
A previously healthy 30-year-old woman has neck pain and bilateral hand and lower extremity tingling with weakness after falling down stairs. She is alert and oriented. Examination reveals incomplete quadriplegia at the C6 level that remains unchanged throughout her evaluation and initial treatment. Radiographs show a bilateral facet dislocation of C6 on C7 without fracture. Attempts at reduction with halo cervical traction up to her body weight are unsuccessful. What is the next most appropriate step?
Explanation
REFERENCES: Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217.
Fardon DF, Garfin SR, Abitbol J (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 247-262.
Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. J Bone Joint Surg Am 1991;73:1555-1560.
Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 76
Communication breakdown is the leading cause of which of the following?
Explanation
Poor communication sets up environments in which medical errors can take place. Per the Joint Commission, medical errors may be the among the top 10 causes of death in the United States. Establishing open lines of communication is critical to reduce the risk of error and enhance patient safety.
Gandhi et al. designed a framework to study missed or delayed diagnoses and their causes. The most significant factors contributing to errors were poor handoffs, failures in judgment, failures in memory and failures in knowledge.
O’Daniel et al. review the importance of professional communication and collaborative team efforts. They note that patient safety is at risk when poor communication is in place. The leading cause for medication errors, treatment delays and wrong-site surgeries is communication failure.
Illustration A shows the leading causes of death in the United States. This includes “preventable errors” as a cause.
Incorrect Answers:
Question 77
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
REFERENCES: Colwell CW Jr, Collis DK, Paulson R, et al: Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty:. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999;81:932-940.
Salvati EA, Pelligrini VD Jr, Sharrock NE, et al: Recent advances in venous thromboembolic prophylaxis during and after total hip replacement. J Bone Joint Surg Am 2000;82:252-270.
Question 78
A 12-year-old boy has had progressive pain and flatfeet for the past year. Pain is increased with weight-bearing activities. Examination reveals that subtalar motion is absent. On standing, the patient has obvious hindfoot valgus and loss of the normal arch bilaterally. Plain radiographs are shown in Figures 43a through 43c, and a CT scan is shown in Figure 43d. What is the most likely diagnosis?
Explanation
REFERENCES: Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 583-595.
Question 79
A 57-year-old woman with diabetes mellitus has purulent drainage from a lateral incision after undergoing open reduction and internal fixation of a displaced ankle fracture 10 days ago. Examination reveals moderate erythema and a foul odor coming from the wound. Cultures are obtained. What is the next most appropriate step in management?
Explanation
REFERENCES: Carragee EJ, Csongradi JJ, Bleck EE: Early complications in the operative treatment of ankle fractures: Influence of delay before operation. J Bone Joint Surg Br 1991;73:79-82.
Blotter RH, Connolly E, Wasan A, Chapman MW: Acute complications in the operative treatment of isolated ankle fractures in patients with diabetes mellitus. Foot Ankle Int 1999;20:687-694.
Question 80
Figure 43 shows an arthroscopic view of a right shoulder through a lateral portal in the beach chair position. The arrow is pointing to what structure?
Explanation
REFERENCES: Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principles of techniques, in McGinty JB (ed): Operative Arthroscopy,
ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Burkhart, SS: Arthroscopic management of rotator cuff tears, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 508-546.
Question 81
The newborn foot deformity seen in Figures 64a and 64b should initially treated with Review Topic

Explanation
Question 82
What portion of the pitching phase creates forces approaching the tensile limit of the medial collateral ligament?
Explanation
REFERENCES: Fleisig GS, Andrews JR, Dillman CJ, et al: Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med 1995;23:233-239.
Lynch JR, Waitayawinyu T, Hanel DP, et al: Medial collateral ligament injury in the overhand-throwing athlete. J Hand Surg 2008;33:430-437.

Figure 5a Figure 5b
Question 83
Which of the following statements is true regarding articular cartilage?
Explanation
Proteoglycans, the most common of which is aggrecan, are produced by chondrocytes and give articular cartilage its hydrophilic properties. Multiple glycosaminoglycans (GAGs), such as chondroitin and keratin can attach to core proteins to form aggrecans. Link proteins then help aggrecans interact with hyaluronic acid. The negative charge of this complex helps create a strong osmotic gradient, which attracts water and increases tissue pressures. Normal aging involves a decrease in the water content of the extracellular matrix while osteoarthritis is associated with increased water content, which leads to loss of strength and elasticity.
Chen et al. evaluated the strain and depth related properties of articular cartilage in bovine models. They found that the zero-strain permeability, zero-strain equilibrium confined compression modulus, and deformation dependence constant differed among the layers of cartilage. They suggest that the complex strain-dependent properties of articular cartilage of different thickness and location have clinical implications for tissue engineering.
Illustration A is a diagram depicting the extracellular matrix of articular cartilage. Incorrect Answers:
Question 84
Figure 83a shows an axillary radiograph and Figures 83b and 83c show axial MR arthrograms of a 20-year-old collegiate offensive lineman who has shoulder pain while pass-blocking. He sustained a shoulder injury 3 months earlier when he "jammed it." Prior to this injury, he denies any pain or instability in either shoulder. Despite undergoing rehabilitation with a physical therapist and trainer and abstaining from playing for 6 weeks, he is currently unable to play because of his symptoms. Examination reveals full active range of motion, a positive jerk test which reproduces his symptoms, and a grade 2 posterior translation of the humeral head with load and shift testing which also reproduces his symptoms. What is the best management option to allow him to return to his pre-injury function next season? Review Topic
Explanation
Question 85
What is the peak period of onset in children with pauciarticular juvenile rheumatoid arthritis?
Explanation
2 years and 9 months, with half the cases lasting less than 2 years.
REFERENCES: Arthritis, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 3.
St Louis, MO, WB Saunders, 2002, pp 1811-1839.
Griffin PP, Tachdjian MO, Green WT: Pauciarticular arthritis in children. JAMA
1963;184:23-28.
Question 86
The mother of a 5-year-old child reports that he has had a fever of 103°F (39.4°C), leg swelling, and has been unwilling to bear weight on his right lower leg for the past 7 days. Examination reveals point tenderness at the distal femur. Aspiration at the metaphysis yields 10 mL of purulent fluid, and a Gram stain reveals gram-positive cocci. In addition to hospital admission, management should include
Explanation
REFERENCE: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 87
A concern when choosing irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene rather than lower dose–irradiated (4 Mrad) polyethylene is related to its inferior resistance to
Explanation
The higher the dose of radiation to the polyethylene, the higher the amount of cross-linking. Adhesive and abrasive wear resistance increases with an increase in cross-linking. However, fatigue properties of the material are decreased when polyethylene is melted (to remove free radicals) during the cross-linking process. Creep (deformation without wear) is also slightly increased with cross-linking of polyethylene.
Question 88
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?
Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the
inability to gain purchase for extraction.
Question 89
Which of the following bones is most frequently involved in stress fractures in athletes? Review Topic
Explanation
Question 90
A tall, thin 17-year-old basketball player and his parents request an evaluation of his flexible (hypermobile) pes planus/planovalgus foot deformities. As part of his evaluation, the orthopaedic surgeon notes pectus excavatum, disproportionately long arms, and scoliosis. In addition to providing treatment of his feet, what test or evaluation should the patient be referred for? Review Topic
Explanation
Question 91
A clinical trial is underway for patients with wrist extensor tendinitis. One group of 100 patients are treated with short arm casting. Another group of 100 patients are treated with physical therapy. During analysis of the results, it becomes apparent that 30 patients in the physical therapy group did not complete the full course of physical therapy. Despite not completing a full course of physical therapy, these 30 patients were included in the physical therapy group for analysis. This analysis is an example of which of the following?
Explanation
The intent-to-treat approach aims to keep similar groups similar by not allowing for patient selection based on post-randomization outcomes (including failure to comply with the protocol). This type of analysis ensures the power of randomization so that important unknown variables that impact outcome are likely to be dispersed equally in each comparison group. Conversely, a per-protocol comparison in a clinical trial excludes patients who were not compliant with the protocol guidelines.
Berger et al., in a Level 5 review, discuss many of the principles beyond randomization that are critical for preserving the comparability of the different groups. They report that masking, allocation concealment, restrictions on the randomization, adjustment for prognostic variables, and the intent-to-treat approach to data analysis are important features of designing a good clinical trial.
Incorrect Answers:
Question 92
A 66-year-old patient with type 1 diabetes mellitus has a deep, nonhealing ulcer under the first metatarsal head and a necrotic tip of the great toe. He has been under the direction of a wound care clinic for 4 months, and has had orthotics and shoe wear changes. What objective findings are indicative of the patient’s ability to heal the wound postoperatively?
Explanation
A transcutaneous oxygen level should be greater than 40 mm Hg for healing.
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-122.
Pinzur MS, Stuck R, Sage R: Benchmark analysis on diabetics at high risk for lower extremity amputation. Foot Ankle Int 1996;17:695-700.
Question 93
(3875) Q4-7658:
Explanation
False
Missile wounds can cause a blast stretch injury to peripheral nerves and may recover with observation. Correct Answer: True
Question 94
What is the most common secondary malignancy arising in pagetic bone?
Explanation
REFERENCES: Grimer RJ, Carter SR, Tillman RM, et al: Osteosarcoma of the pelvis. J Bone Joint Surg Br 1999;81:796-802.
Harrington KD: Surgical management of neoplastic complications of Paget’s disease. J Bone Miner Res 1999;14:45-48.
Question 95
You perform an ACL reconstruction with bone-patella tendon-bone (BTB) autograft and are explaining the postoperative rehabilitation protocol to your patient. Which of the following is associated with increased quadriceps volume and improved quadriceps strength at 1 year without a higher risk of knee instability? Review Topic
Explanation
Proper rehabilitation following ACL reconstruction is vital to a successful outcome. The cornerstone of ACL rehabilitation is range of motion, strengthening and functional exercises without risk of destabilizing the knee. There are a variety of rehabilitation protocols and recently an effort has been made to standardize the approach to postoperative ACL care. An accelerated protocol starting at 3 weeks postoperatively has been deemed safe and may enhance the speed and safety with which an athlete returns to play.
Kruse et al completed a meta-analysis of 29 Level I and II studies focused on the ACL rehabilitation process. The authors concluded that immediate postoperative weightbearing and knee range of motion 0-90 is safe. Early eccentric strengthening appears to accelerate and improve strength gains at 1 year as compared to delayed eccentric strengthening. Home-based rehabilitation programs can be as effective as formal physical therapy. Postoperative bracing and CPM use is neither necessary nor beneficial.
Van Grinsven et al conducted a systematic review of ACL rehabilitation programs and physical therapy modalities to develop an evidence-based rehabilitation protocol. The authors demonstrated that an accelerated protocol without postoperative bracing focused on reduction of pain, swelling and inflammation and regaining range of motion, strength and neuromuscular control has significant advantages and does not lead to stability problems.
Gerber et al performed a randomized trial comparing two accelerated postoperative rehabilitation protocols – early eccentric (ECC) rehabilitation versus traditional (TRAD) rehabilitation starting at 3 weeks. There were no significant differences in knee pain, effusion or stability. However, quadriceps strength, hopping distance and activity level improved by a significantly greater amount in the ECC group versus the TRAD group at 26 weeks postoperatively. In a separate analysis of these patients, quadriceps and gluteus muscle cross-sectional area and volume in ECC patients were more than twice those in the TRAD group.
Illustration A depicts two eccentric ergometers that can be used in postoperative ACL rehabilitation.
Incorrect Responses:
another Answer
type of brace,
2:
There
duration is
of
bracing or no bracing at all.
no
advantage
to
CPM
use.
Question 96
A 24-year-old baseball pitcher reports pain over the posterior aspect of his shoulder that occurs only during throwing. He notes that the discomfort is greatest during the late cocking and early acceleration phases. Examination reveals localized tenderness with palpation over the external rotators and posterior glenoid. Radiographs are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCES: Meister K, Andrews JR, Batts J, Wilk K, Baumgarten T, Baumgartner T: Symptomatic thrower’s exostosis: Arthroscopic evaluation and treatment. Am J Sports Med 1999;27:133-136.
Ferrari JD, Ferrari DA, Coumas J, Pappas AM: Posterior ossification of the shoulder: The Bennett lesion. Etiology, diagnosis, and treatment. Am J Sports Med 1994;22:171-176.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posteriorsuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 97
A 62-year-old man slips on ice and sustains an elbow dislocation. Post-reduction imaging reveals a highly comminuted radial head fracture and coronoid fracture through its base. What is the most appropriate treatment?

Explanation
Pugh et al reported their experiences with this difficult population. Their protocol consisted of ORIF or replacement of the radial head, ORIF of the coronoid fracture, repair of the LCL and capsule, and repair of the MCL and/or hinged external fixation. Of the 36 cases, the outcome was graded as 28 excellent to good, 7 fair, and 1 poor. 8 cases required re-operation. The authors concluded that their surgical protocol restored sufficient elbow stability to allow early motion post-op, thereby enhancing the functional outcome. In fracture dislocation of the elbow with radial head
and coronoid fracture, the radial head must be fixed or replaced to restore stability. The ORIF of coronoid fracture and radial head restores some valgus stability therefore MCL repair may not be needed. However, the varus stability must be restored by LCL repair.
Question 98
A 52-year-old woman has bicompartmental osteoarthritis following patellectomy. Treatment should consist of
Explanation
REFERENCES: Martin SD, Haas SB, Insall JN: Primary total knee arthroplasty after patellectomy. J Bone Joint Surg Am 1995;77:1323-1330.
Pagnano MW, Cushner FD, Scott WN: Role of the posterior cruciate ligament in total knee arthroplasty. J Am Acad Orthop Surg 1998;6:176-187.
Question 99
Figures 28a and 28b show the posteroanterior and lateral radiographs of a 38-year-old woman with adult idiopathic scoliosis. She reports symptoms of long-standing lower back pain, progressive loss of height, and the inability to stand upright at the end of the day. What radiographic finding has been found to most closely correlate with symptoms of lower back pain? Review Topic

Explanation
Question 100
A year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
