OITE & ABOS Orthopedic Board Prep: Fracture, Hip, Knee, Nerve MCQs Part 12

Key Takeaway
This page offers Part 12 of a comprehensive, interactive MCQ quiz bank for orthopedic surgeons and residents. Authored by Dr. Mohammed Hutaif, it features 100 high-yield, verified questions mirroring OITE/AAOS board exams, with study and exam modes to optimize your board certification preparation.
About This Board Review Set
This is Part 12 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 12
This module focuses heavily on: Fracture, Hip, Knee, Nerve.
Sample Questions from This Set
Sample Question 1: In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of...
Sample Question 2: Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with amonth history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?...
Sample Question 3: Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient’s knee joint. What is the most likely diagnosis?...
Sample Question 4: When performing surgical excision of the lesion shown in the MRI scan in Figure 3, what nerve is most likely at risk?...
Sample Question 5: An 18-year-old man sustained closed humeral shaft and forearm fractures of his dominant arm in a motor vehicle accident. Neurovascular examination is intact, and his condition is stable. The best course of action for management of the injur...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of
Explanation
REFERENCES: Zeitlin L, Fassier F, Glorieux FH: Modern approach to children with osteogenesis imperfecta. J Pediatr Orthop B 2003;12:77-87.
Falk MJ, Heeger S, Lynch KA, et al: Intravenous bisphosphonate therapy in children with osteogenesis imperfecta. Pediatrics 2003;111:573-578.
Glorieux FH, Bishop NJ, Plotkin H, et al: Cyclic administration of pamidronate in children with severe osteogenesis imperfecta. N Engl J Med 1998;339:947-952.
Question 2
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?
Explanation
Question 3
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient’s knee joint. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Kier R, McCarthy SM: Lipohemarthrosis of the knee: MR imaging. J Comput Assist Tomogr 1990;14:395-396.
Question 4
When performing surgical excision of the lesion shown in the MRI scan in Figure 3, what nerve is most likely at risk?
Explanation
REFERENCE: Kozin SH: The anatomy of the recurrent branch of the median nerve. J Hand Surg Am 1998;23:852-858.
Question 5
An 18-year-old man sustained closed humeral shaft and forearm fractures of his dominant arm in a motor vehicle accident. Neurovascular examination is intact, and his condition is stable. The best course of action for management of the injuries should be
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Bell MJ, Beachamp CG, Kellam JK, McMurtry RY: The results of plating humeral shaft fractures in patients with multiple injuries: The Sunnybrook experience. J Bone Joint Surg Br 1985;67:293-296.
Question 6
What role does quorum sensing play in the development of a bacterial biofilm?
Explanation
Question 7
A 68-year-old woman who underwent a right total hip arthroplasty 1 year ago has dislocated her hip five times since surgery. Radiographs show a retroverted acetabular component. What is the best treatment for this patient?
Explanation
REFERENCES: Daly PJ, Morrey BF: Operative correction of an unstable total hip arthroplasty. J Bone Joint Surg Am 1992;74:1334-1343.
Jolles BM, Zangger P, Leyvraz PF: Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. J Arthroplasty 2002;17-282-288.
Hamilton W, McAuley JP: Evaluation of the unstable total hip arthroplasty. Inst Course Lect 2004;53:87-92.
Question 8
- A 17-year old boy who sustained a closed clavicle fracture after he was ejected from an all-terrain vehicle was treated with a figure-of-8 brace 1 year ago. He now reports continuous pain at the site of the fracture and is unable to actively raise his arm above his head. A radiograph is shown in Figure 1. Management should now include
Explanation
Selection (1) would not provide adequate fixation to promote healing. (2) Electrical stimulation would not be sufficient for the above reasons. (3) Resection of the distal clavicle would not be indicate for this case because it promote further instability of the clavicle and increasing the affected forces to the clavicle.
(5) Kirschner wire fixation with bone graft, the author stated would provide fixation, but they achieved better results with plate fixation and bone graft Question 6 -
A 75-year-old woman sustains a fracture below the level of a total hip prosthesis. Radiographs demonstrate loosening of the prosthetic component. Treatment should consist of
a cast brace
a spica cast
plate fixation
allograft strut fixation
long stem revision
The key to this question lies in the radiographic evidence of loosening of the prosthetic component. The long stem revision is clearly indicated in this case because of various factors, one decreases impingement of the loose stem against the lateral femoral cortex. A non-surgical approach in the elderly patient will only increase the many risk factors such as atelectasis, pneumonia, and thromboembolic disease.[Instructional Course 44 pg. 293-303]
Question 9
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of Review Topic
Explanation
Question 10
- What is the primary immediate source of energy for muscle?
Explanation
Almost 90% of the total ATP formed by glucose metabolism is formed during oxidative phosphorylation. This is accomplished by a series of enzymatically catalyzed reactions in the mitochondria. When the body’s stores of carbohydrates decrease below normal, glucose can be formed from the breakdown of protein and fat via gluconeogenesis to yield more ATP.
Question 11
Flow cytometry of tumors measures the
Explanation
Question 12
Figure 16 shows the radiograph of a 56-year-old man who has neck pain after a rollover accident on his lawnmower. The injury appears to be isolated, and he is neurologically intact. Management of the fracture should consist of
Explanation
REFERENCES: Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries. J Am Acad Orthop Surg 2002;10:271-280.
Question 13
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management? Review Topic

Explanation
Question 14
A 10-year-old boy who is active in soccer has had activity-related heel pain for the past 3 months. Examination reveals tenderness over the posterior heel and a tight Achilles tendon. Radiographs demonstrate a 2-cm cyst in the anterior body of the calcaneus. His physes have not closed. Based on these findings, what is the most appropriate management?
Explanation
REFERENCES: Ogden JA, Ganey TM, Hill JD, et al: Sever’s injury: A stress fracture of the immature calcaneal metaphysis. J Ped Orthop 2004;24:488-492.
Pogoda P, Priemel M, Linhart W, et al: Clinical relevance of calcaneal bone cysts: A study of 50 cysts in 47 patients. Clin Orthop Relat Res 2004;424:202-210.
Question 15
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?
Explanation
MR arthrography provides improved sensitivity compared to conventional MRI, without contrast, for the detection of UCL pathology, particularly in the subacute or chronic setting. After the soft-tissue edema and joint fluid associated with the injury have resolved, the torn end of the ligament may lie in contact with its adjacent attachment and create a false-negative appearance. In this patient, a noncontrasted MR arthrogram showed no tear, yet the tear is apparent with intra-articular contrast and distention. MR arthrography of the elbow also may be useful in detecting intra-articular bodies or in evaluation for loose osteochondral fragments or flaps.
REFERENCES: Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 200-210.
Question 16
A 40-year-old right hand-dominant construction worker has had a 6-month history of aching left shoulder pain that is worse after working a long day. Examination reveals limited range of motion and good strength when compared to his asymptomatic right arm. He has not had any orthopaedic intervention to date. Radiographs are shown in Figures 43a and 43b. What is the most appropriate treatment?
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Skedros JG, O’Rourke PJ, Zimmerman JM, et al: Alternatives to replacement arthroplasty for glenohumeral arthritis, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 485-499.
Question 17
Figures 45a and 45b show the radiographs of a 46-year-old man who reports the acute onset of right knee pain and is unable to bear weight on the extremity. His medical history is unremarkable. The next most appropriate step in management should consist of
Explanation
REFERENCE: Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Question 18
A 29-year-old female has sustained the acute injury shown in Figure A. Which of the following is an indication for open reduction internal fixation in this patient?

Explanation
In patients who present with no medial widening on standard ankle radiographs and no clinical symptoms of deltoid ligament injury, the integrity of the deltoid ligament remains unknown. The gravity stress radiograph may be used to help identify a deltoid ligament injury in association with an isolated distal fibular fracture. Stage-IV supination-external rotation fractures, which involve the deltoid ligament, are more likely to be treated operatively as they are often considered unstable ankle fractures.
Egol et al. reviewed 101 patients with isolated fibular fracture and an intact mortise. They found that medial tenderness, swelling, and ecchymosis were not sensitive with regard to predicting widening of the medial clear space on stress radiographs. Interestingly, they report that good functional results can be obtained in patients with widening of the medial clear space on a stress radiograph in the absence of medial signs.
Gill et al. compared the effectiveness of gravity stress radiograph as compared to manual stress radiograph for the detection of deltoid ligament injury in isolated fibular fracture. A total of twenty-five patients with SER type-II fracture and SER Type IV-equivalent fractures were enrolled. They found the gravity stress radiograph was equivalent to the manual stress radiograph for determining deltoid ligament injury.
Figure A shows a mortise radiograph displaying a minimally displaced Weber B ankle fracture. Illustration A shows the positioning for a gravity stress radiograph. The patient is in the lateral decubitus position with the injured leg dependent and off the end of the table, a mortise view is taken in 10° of internal rotation of the tibia.
Incorrect Answers:
Question 19
A 45-year-old woman has a distal radius fracture, which is treated with open reduction and internal fixation. The surgery was uncomplicated, and the patient is discharged to home. At the first follow-up appointment, the patient demonstrates signs that are concerning for complex regional pain syndrome (CRPS). What factor is included in the International Association for the Study of Pain (IASP) criteria (Budapest criteria) for the diagnosis of CRPS?
Explanation
The diagnosis of CRPS is complex. The IASP has approved diagnostic criteria to standardize both the diagnosis and the study of CRPS. The criteria are:
Continuing pain disproportionate to any inciting event
At least one symptom in three of the following four categories
Sensory: reports of hyperesthesia and/or allodynia
Vasomotor: reports of temperature asymmetry and/or skin color changes and/or skin color asymmetry
Sudomotor/edema: reports of edema and/or sweating changes and/or sweating asymmetry
Motor/trophic: reports of decreased range of motion (ROM) and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, skin, nails)
At least one sign at the time of evaluation in two (for clinical diagnosis) or three (for inclusion in scientific studies) of the following categories
Sensory: evidence of hyperesthesia (to pinprick) and/or allodynia (to light touch and/or deep somatic pressure and/or joint movement)
Vasomotor: evidence of temperature asymmetry and/or skin color changes and/or skin color asymmetry
Sudomotor/edema: evidence of edema and/or sweating changes and/or sweating asymmetry
Motor/trophic: evidence of decreased ROM and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, skin, nails)
No other diagnosis better explains the signs and symptoms.
Decreased sensation and focal numbness are not consistent with CRPS. Laboratory and imaging studies can be helpful in evaluating for the exclusion of differential diagnoses for CRPS, including infection, rheumatic disease, fracture, nonunion, tenosynovitis, or osteomyelitis.
Question 20
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?
Explanation
REFERENCES: Tan AH, Lam KS, Lee EH: The treatment outcome of trigger thumb in children. J Pediatric Orthop B 2002;11:256-259.
Slakey JB, Hennrikus WL: Acquired thumb flexion contracture in children: Congenital trigger thumb. J Bone Joint Surg Br 1996;78:481-483.
Herring JA: Disorders of the upper extremity: Thumb dysplasia, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, p 445.
Question 21
A 22-year-old patient has had severe groin pain for many months and is unable to engage in any physical activity. The AP radiograph of the pelvis shows minimal arthritis. The lateral radiograph of the hip is shown in Figure 33a. An MR-arthrogram is shown in Figure 33b. What is the most appropriate treatment at this stage? Review Topic

Explanation
Question 22
A 27-year-old right hand dominant construction worker falls off a scaffold onto his outstretched arm. Figure A exhibits the radiograph taken at a local emergency room. Following treatment, he is placed in a sling and follows up at your office two weeks later. He complains of a feeling that his arm is going to 'pop out'. Which specific physical examination finding is likely to be present? Review Topic
Explanation
Posterior dislocations occur less frequently than anterior dislocations, and are often missed. Following closed reduction, persistent instability can occur, usually associated with posterior capsular or labral pathology. Posteriorly directed provocative maneuvers, such as the Kim test can be positive.
Robinson et al. performed an epidemiologic analysis on 120 posterior dislocations. Recurrent instability occurred at a rate of 17.7%. Risk factors for recurrent instability included age less than 40-years-old, dislocation during seizure, and a large reverse Hill-sachs (>1.5 cm3).
Kim et al. describe the Kim lesion, a separation between the posteroinferior labrum and the articular cartilage without complete detachment of the labrum, which cause persistent posterior instability.
Figure A depicts a posterior dislocation on xray. Illustration A depicts the Kim test, which is performed by having the patient seated, arm at 90° abduction, followed by flexing the shoulder to 45° forward flexion while simultaneously applying axial load on the elbow and posterior-inferior force on the upper humerus. The test is positive when there is pain. Video 1 depicts the proper way to perform a Kim Test.
Incorrect answers:
Question 23
When treating a proximal tibia fracture, the surgeon decides to (1) use blocking screws in the proximal fragment, and (2) pick the intramedullary nail based on the location of the Herzog curve. Which of the following combinations will best prevent the classic deformity associated with this fracture?
Explanation
Up to 58% of proximal tibial fractures are malaligned. Malalignment arises because the nail fits loosely in the wide metaphyses and cannot control alignment. Without close fit of the nail at the fracture site, the nail will not align the fracture independent of a stable reduction and careful nail path. Blocking screws serve to reduce the size of the proximal metaphyseal canal and guide final nail passage.
Stinner et al. discuss strategies in proximal tibial fracture nailing. They describe an accurate starting point (using the twin peaks AP view or fibular bisector AP view, and flat plateau lateral view). They emphasize fracture reduction prior to reaming and implant placement.
Hiesterman reviewed nailing of extra-articular proximal tibial fractures. Techniques described include blocking screws, unicortical plating, using a universal distractor, nailing in flexion/locking in extension, semiextended nailing (including percutaneous suprapatellar quads-splitting approaches), multiple proximal interlocking screws (>=3).
Illustration A shows placement of a coronal blocking screw. Illustration B shows placement of a sagittal blocking screw. Illustration C shows the effect of the Herzog curve. A more distal Herzog curve leads to a "wedge" effect and fracture displacement whereas a proximal Herzog curve contains the fracture. The "wedge" effect occurs as the nail is seated and impinges on the posterior cortex of the distal segment accentuating an apex anterior deformity because of the effective widening of the nail above the bend and posterior force on the distal segment to match the nail shape.
Incorrect Answers:
Question 24
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Explanation
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 25
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
(range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon’s finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle.
REFERENCES: Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804.
Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
Johnson DH, Fanelli GC, Miller MD: PCL 2002: Indications, double-bundle versus inlay technique and revision surgery. Arthroscopy 2002;18:40-52.
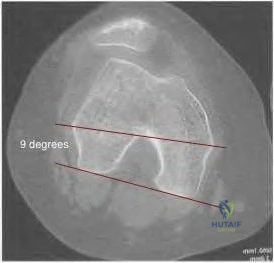
Question 26
98 degrees (range, 0 degrees to 9 degrees). In knees with varus joint lines
Explanation
Question 27
Figures 55a through 55c are the clinical photograph and radiographs of a 5-year-old boy who fell and injured his right elbow. His radial pulse is thready. Which neurologic deficit most commonly is associated with this injury?
Explanation
This injury is a type III supracondylar humerus fracture with posterolateral displacement. The area of ecchymosis is anteromedial, corresponding to the proximal spike of the humeral metaphysis. The brachial artery is likely tented over this spike, leading to diminished perfusion. The median nerve also resides in this area, and any neurological deficit is likely in its most vulnerable fibers, those of the anterior interosseous nerve (AIN). The AIN contains no sensory fibers, and its motor function involves flexion of both the thumb IP joint and the index distal IP joint.
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.

Question 28
A 12-year-old boy falls from a bicycle. A radiograph of his injured shoulder is shown in Figure 41. What is the optimal method of treatment?
Explanation
REFERENCES: Bishop JY, Flatow EL: Pediatric shoulder trauma. Clin Orthop Relat Res 2005;432:41-48.
Question 29
A 77-year-old man with a history of mild renal insufficiency and atrial fibrillation on warfarin therapy is scheduled to undergo a left total hip arthroplasty. He previously underwent a right total hip arthroplasty with development of significant heterotopic bone that resulted in limitation of motion. What is the most appropriate form of prophylactic treatment to minimize the formation of heterotopic bone on his left hip?
Explanation
REFERENCES: Kolbl O, Knelles D, Barthel T, et al: Preoperative irradiation versus the use of nonsteroidal anti-inflammatory drugs for prevention of heterotopic ossification following total hip replacement: The results of a randomized trial. Int J Radiat Oncol Biol Phys 1998;42:397-401.
Pakos EE, Ioannidis JP: Radiotherapy vs nonsteroidal anti-inflammatory drugs for the prevention of heterotopic ossification after major hip surgery: A meta-analysis of randomized trials. Int J Radiat Oncol Biol Phys 2004;60:888-895.
Seegenschmiedt MH, Makoski HB, Micke O, et al: Radiation prophylaxis for heterotopic ossification about the hip joint: A multicenter study. Int J Radiat Oncol Biol Phys 2001 ;51:756-765.
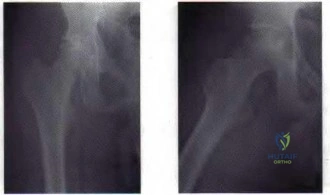
Figure 23 a Figure 23b
Question 30
An obese 4-year-old boy has infantile Blount’s disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of
Explanation
REFERENCES: Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Loder RT, Johnston CE: Infantile tibia vara. J Pediatr Orthop 1987;7:639-646.
Question 31
Reverse total shoulder arthroplasty improves kinematics in the rotator cuff deficient joint by what directional change to the center of rotation? Review Topic
Explanation
Question 32
- Which of the following conditions is associated é the highest mortality in patients é a pelvic fracture?
Explanation
Question 33
A 21-year-old female college athlete sustained a stress fracture of the fifth metatarsal 1 year ago which was treated successfully with surgical stabilization and she returned to normal activities. She now has a tension-sided femoral neck fracture. Along with surgical fixation of the fracture, what is the next step in management? Review Topic
Explanation
Question 34
Which of the following is the preferred treatment for symptomatic localized pigmented villonodular synovitis (PVNS) of the knee?
Explanation
REFERENCES: Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis.
J Am Acad Orthop Surg 2006;14:376-385.
Kim SJ, Shin SJ, Choi NH, et al: Arthroscopic treatment for localized pigmented villonodular synovitis of the knee. Clin Orthop Relat Res 2000;379:224-230.
Question 35
What is the main benefit of using metal-backed tibial components in total knee arthroplasty?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Question 36
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of
Explanation
REFERENCES: Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Gerber C, et al: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 37
Figure 55 shows the radiograph of a 30-year-old man who sustained a closed comminuted fracture of the right clavicle. Examination reveals decreased sensation in the radial nerve distribution. Weakness is noted with shoulder abduction, internal rotation, and wrist extension. A displaced bone fragment is most likely pressing on what portion of the brachial plexus? Review Topic

Explanation
Question 38
A 13-year-old girl is referred for a painful progressive valgus deformity of the right knee. Examination reveals an antalgic gait with an obvious valgus deformity. The right distal femur has a palpable, tender mass with erythema and warmth. Figures 4a and 4b show a clinical photograph and a radiograph. Management should consist of
Explanation
REFERENCES: Enneking W: Principles of musculoskeletal oncologic surgery, in Evarts C (ed): Surgery of the Musculoskeletal System. New York, NY, Churchill Livingston, 1990.
Herring JA: General principles of tumor management, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, from the Texas Scottish Rite Hospital for Children, ed 3. Philadelphia, PA, WB Saunders, 2002, pp 1897-1900.
Question 39
Figure 10 shows patellar radiographs of a 68-year-old woman who underwent bilateral total knee arthroplasty 2 months ago. Following a recent fall onto the left side, she now reports anterior pain in the left knee. A CT scan shows that the femoral and tibial components are appropriately externally rotated and radiographs show acceptable axial alignment and no evidence of loosening. What is the most appropriate treatment option?
Explanation
If the components are determined to be in satisfactory position, soft-tissue procedures can be pursued. Lateral retinacular release is usually the first soft-tissue procedure used to improve patellofemoral mechanics. In this patient, the patellar fracture fragment is so small that it can be excised. Distal realignment is not usually used as the first line of treatment for patellar maltracking following TKA.
REFERENCES: Fehring TK, Christie MJ, Lavemia C, et al: Revision total knee arthroplasty: Planning, management, and controversies. Instr Course Lect 2008;57:341-363.
Patel J, Ries MD, Bozic KJ: Extensor mechanism complications after total knee arthroplasty. Instr Course Lect 2008;57:283-294.
Question 40
An 11-year-old child has Ewing’s sarcoma of the femoral diaphysis with a small soft-tissue mass. Staging studies show no evidence of metastases. Treatment should consist of
Explanation
REFERENCES: Toni A, Neff JR, Sudanese A, et al: The role of surgical therapy in patients with non-metastatic Ewing’s sarcoma of the limbs. Clin Orthop 1991;286:225.
Picci P, Rougraff BT, Bacci G, et al: Prognostic significance of histopathologic response to chemotherapy in non-metastatic Ewing’s sarcoma of the extremities. J Clin Oncol 1993;11:1763.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant Bone Tumors. Instr Course Lect 2002;51:413-428.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 41
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure A. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion? Review Topic

Explanation
Question 42
What would be the advantage of surgery for the patient described in this scenario?
Explanation
The MR image of the lumbar spine postgadolinium contrast shows a ring-enhancing fluid collection. Ring-enhancing lesions within the spinal canal on postgadolinium MR images are indicative of epidural abscess. It is important to obtain a culture-specific diagnosis to inform the choice of antibiotics and educate patients regarding the likelihood of failure for standalone antibiotic therapy. Infection with MSSA, age younger than 65 years, the absence of neurologic deficit, and lumbar abscess location are all factors that point toward a patient being a reasonable candidate for a trial of culture-specific IV antibiotics. In this case, nafcillin is a suitable treatment for MSSA. The antibiotic should be initiated and closely observed with serial labs (WBC, ESR, CRP, repeat blood cultures) to ensure that the patient responds appropriately to therapy and that neurologic deficits do not develop. In the setting of epidural abscess, surgery is performed to evacuate the abscess and reverse or prevent neurologic deterioration. In the current scenario in which sepsis is not an issue, scant high-quality evidence shows that surgical intervention influences risk for mortality or chronic pain following epidural abscess.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.View Abstract at PubMed
Adogwa O, Karikari IO, Carr KR, Krucoff M, Ajay D, Fatemi P, Perez EL, Cheng JS, Bagley CA, Isaacs RE. Spontaneous spinal epidural abscess in patients 50 years of age and older: a 15-year institutional perspective and review of the literature: clinical article. J Neurosurg Spine. 2014 Mar;20(3):344-9. doi: 10.3171/2013.11.SPINE13527. Epub 2013 Dec 20. Review.
PubMed PMID: 24359002.View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014
Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 43
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
Explanation
REFERENCES: Waldrop JT, Ebraheim NA, Yeasting RA, Jackson WT: The location of the sacroiliac joint on the outer table of the posterior ilium. J Orthop Trauma 1993;7:510-513.
Xu R, Ebraheim NA, Yeasting RA, Jackson WT: Anatomic considerations for posterior iliac bone harvesting. Spine 1996;21:1017-1020.
Question 44
A 15-year-old female field hockey player sustains a blow to the mouth from a hockey stick. Three front teeth are knocked out and shown in Figure 4. In addition to calling a dentist immediately, what is the next best step in management?
Explanation
REFERENCES: Krasner P: Management of sports-related tooth displacements and avulsions. Dent Clin North Am 2000;44:111-135.
Sullivan JA, Anderson SJ (eds): Care of the Young Athlete. Rosemont IL, American Academy of Orthopaedic Surgeons, Elk Grove Village, IL, American Academy of Pediatrics, 2000, p 190.
Galante A: Facial trauma, in Baker CL (ed): The Hughston Clinic Sports Medicine Book. Baltimore, MD, Williams & Wilkins, 1995, p 121.
Question 45
What nerve is at the highest risk for injury with a percutaneous repair of an Achilles tendon injury?
Explanation
REFERENCE: Hockenbury RT, Johns JC: A biomechanical in vitro comparison of open versus percutaneous repair of tendon Achilles. Foot Ankle 1990;11:67-72.
Question 46
Figures 9a and 9b show the radiographs of a 75-year-old man who underwent a revision total knee arthroplasty with a long-stemmed tibial component. In rehabilitation, he reports fullness and tenderness in the proximal medial leg (at the knee). The strategy that would best limit this postoperative problem is use of
Explanation
REFERENCE: Gustke K: Cemented tibial stems are not requisite in revision. Orthopedics 2004;27:991-992.
Question 47
Figure 11 shows the lateral radiograph of a 16-year-old boy who has been unable to participate in sports activities because of pain in the anterior aspect of the knee. He states that the pain is aching in nature and is located in the region of the tibial tuberosity. He denies having joint effusion or symptoms of instability. Management should consist of
Explanation
REFERENCES: Flowers MJ, Bhadreshwar DR: Tibial tuberosity excision for symptomatic Osgood-Schlatter disease. J Pediatr Orthop 1995;15:292-297.
Greene WB: Osteochondrosis and tibia vara, in Canale ST, Beaty JH (eds): Operative Pediatric Orthopaedics, ed 2. Philadelphia, Pa, Mosby, 1995, pp 804-854.
Question 48
An otherwise healthy 33-year-old man who works in construction reports a 3-month history of knee pain. Radiographs are shown in Figures 9a and 9b. An axial T 1 -weighted MRI scan with contrast, an angiogram, and histologies are shown in Figures 9c through 9f. What is the most likely diagnosis?
Explanation
REFERENCES: Sheth DS, Yasko AW, Raymond AK, et al: Conventional and dedifferentiated parosteal osteosarcoma: Diagnosis, treatment, and outcome. Cancer 1996;78:2136-2145.
Lewis VO, Gebhardt MC, Springfield DS: Parosteal osteosarcoma of the posterior aspect of the distal part of the femur: Oncological and functional results following a new resection technique. J Bone Joint Surg Am 2000;82:1083-1088.
Question 49
Which of the following is considered a potential advantage of arthroscopic repair for anterior instability of the shoulder? Review Topic
Explanation
Question 50
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?
Explanation
REFERENCES: Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 51
A patient has multidirectional instability of the shoulder that has not responded to nonsurgical management. Successful surgical treatment will most likely include which of the following? Review Topic
Explanation
instability treated surgically following failure to respond to nonsurgical management has been shown to be associated with classic Bankart lesions, Hill-Sachs defects, glenoid chondral lesions, and even SLAP lesions (Werner). However, these lesions were seen in a lower percentage than that found for unidirectional anterior dislocations. Likewise, these lesions do not appear to be significant in influencing treatment in the majority of patients.
Question 52
78A B Figures 78a and 78b are the emergency department radiographs of an 83-year-old woman who tripped and braced herself against a wall; this was followed by shoulder pain. Which intervention would provide optimal treatment for this patient?

Explanation
Low-energy fractures in elderly patients typically are treated with nonsurgical care that involves early immobilization followed by early rehabilitation/therapy, especially when proximal humerus and distal humerus fractures are involved. Physical therapy should be initiated within the first 2 weeks. If surgery is needed ORIF is preferred for most fractures, but replacement may improve outcomes for unreconstructable fractures. The use of hemiarthroplasty vs reverse shoulder replacement is currently being debated.
For treatment of distal radius fractures in elderly patients, cast immobilization for about 6 weeks will allow for optimal fracture healing. This should be followed by aggressive therapy to improve range of motion and function. Moderately displaced fractures in elderly patients will result in satisfactory outcomes even though reduction may not be "anatomic."
RECOMMENDED READINGS
Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M. A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and older. J Bone Joint Surg Am. 2011 Dec 7;93(23):2146-53. doi: 10.2106/JBJS.J.01597. PubMed PMID: 22159849. View Abstract
at PubMed
Tejwani NC, Liporace F, Walsh M, France MA, Zuckerman JD, Egol KA. Functional outcome following one-part proximal humeral fractures: a prospective study. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):216-9. doi: 10.1016/j.jse.2007.07.016. Epub 2008 Jan 22. PubMed
PMID: 18207430. View Abstract at PubMed
Solberg BD, Moon CN, Franco DP, Paiement GD. Locked plating of 3- and 4-part proximal humerus fractures in older patients: the effect of initial fracture pattern on outcome. J Orthop Trauma. 2009 Feb;23(2):113-9. doi: 10.1097/BOT.0b013e31819344bf. PubMed PMID:
Question 53
Figure 18 is the radiograph of a 52-year-old woman who has leg length inequality and chronic activity-related buttock discomfort. This has been a life-long problem, but it is getting worse and increasingly causing back pain. What is the best current technique for total hip arthroplasty?
Explanation
A high hip center is not recommended for Crowe IV hips because of the lack of acetabular bone and altered hip biomechanics. An anatomic center is a better option but necessitates a technique to address the tight soft-tissue envelope. A trochanteric osteotomy with progressive femoral shortening has been described but can be prone to trochanter nonunion. Iliofemoral lengthening prior to surgery has been described but may not be tolerated by all patients. A shortening subtrochanteric osteotomy avoids trochanter nonunion and allows adjustment of femoral anteversion. Fixation of the osteotomy can include a stem with distal rotational control, plate fixation, a step vs. oblique cut, or strut grafts.
Question 54
On an axial CT image, which of the following dimensions is considered to be indicative of a critical amount of lumbar spinal stenosis? Review Topic
Explanation
Question 55
An otherwise healthy 76-year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in Figures below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?

Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 56
A 43-year-old woman has a 2-week history of right shoulder pain. She denies any injury to initiate her symptoms but states that she has shoulder pain with range of motion and lifting objects. Examination reveals mild pain with abduction, empty can testing, and with the Neer and Hawkins impingement tests. Her range of motion with the right shoulder reveals passive forward flexion to 90 degrees, abduction to 90 degrees, external rotation at the side to 15 degrees, and internal rotation to her buttock. The uninvolved left shoulder has forward flexion to 160 degrees, abduction to 150 degrees, external rotation at the side to 60 degrees, and internal rotation to T6. Radiographs of the shoulder are normal. What is the next most appropriate step in management? Review Topic
Explanation
Question 57
What is the most specific physical examination finding? Review Topic

Explanation
Question 58
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals no other injuries. Radiographs are shown in Figures 35a and 35b. Initial management of this fracture should consist of
Explanation
REFERENCES: Meyers MH, McKeever FM: Fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60
Janarv PM, Westblad P, Johansson C, Hirsch G: Long-term follow-up of anterior tibial spine fractures in children. J Pediatr Orthop 1995;15:63-68.
Kuhn JE, Sailer MJ, Sterett WI, Hawkins RJ: Arthroscopic technique for the treatment of tibial spine fractures in the skeletally immature patient. J Ortho Tech 1995;3:7-12.
Question 59
Examination of a 28-year-old woman reveals a moderate hallux valgus deformity and a prominence of the medial eminence. She reports that she can participate in all activities, wear 3-inch heels with minimal discomfort, and walk in a 1-inch heel with no pain. However, she is concerned that the deformity will get worse and requests recommendations regarding surgical correction. What is the best course of action?
Explanation
REFERENCES: Donley BG, Tisdel CL, Sferra JJ, Hall JO: Diagnosing and treating hallux valgus: A conservative approach for a common problem. Cleve Clin J Med 1997;64:469-474.
Teitz CC, Hu SS, Arendt EA: The female athlete: Evaluation and treatment of sports-related problems. J Am Acad Orthop Surg 1997;5:87-96.
Question 60
Figure 22 shows the radiograph of a 7-year-old boy who underwent retrograde elastic nailing of a femoral shaft fracture. What is the most common problem following this procedure?
Explanation
REFERENCES: Flynn JM, Luedtke LM, Ganley TJ, et al: Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am 2004;86:770-777.
Flynn JM, Hresko T, Reynolds RA, et al: Titanium elastic nails for pediatric femur fractures: A multicenter study of early results with analysis of complications. J Pediatr Orthop 2001;21:4-8.
Ligier JN, Metaizeau JP, Prevot J, et al: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Question 61
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. The patient undergoes surgery to repair/reconstruct the damaged structure and has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they want to “get the therapy over with as fast as possible" to expedite his return to sports, and the surgeon and rehabilitation team consider their request. Compared with nonaccelerated rehabilitation, patients who follow an early accelerated rehabilitation protocol experience

Explanation
Question 62
During the cocking and acceleration phases of the overhand throw (pitch), there are several static and dynamic restraints to provide medial elbow support and prevent valgus instability. The dynamic structures found to be most important during these phases of the overhand throw are the flexor digitorum Review Topic
Explanation
Question 63
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
REFERENCES: Cantu RC: Second-impact syndrome. Clin Sports Med 1998;17:37-44.
Saunders RL, Harbaugh RE: Second impact in catastrophic contact-sports head trauma. JAMA 1984;252:538-539.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 64
- An orthopaedic surgeon who is the developer of a knee arthroplasty system is discussing treatment options with a patient who has tricompartmental osteoarthritis. As a part of this discussion, the orthopaedic surgeon has an obligation to disclose
Explanation
III. Conflicts of Interest
B. Where there are financial interests involved in the ownership of a pharmacy, rehabilitation center, imaging equipment, surgery center, or health care facility where the orthopaedic surgeon’s financial interest is not immediately obvious, the orthopaedic surgeon must disclose that financial interest to the patient and to colleagues.
C. When an orthopaedic surgeon receives anything of value, including royalties, from a manufacturer, the orthopaedic surgeon must disclose this fact to the patient and to colleagues. It is unethical for an orthopaedic surgeon to receive compensation (excluding royalties) from a manufacturer for using a particular device or medication. Reimbursement for administrative costs in conducting or participating in a scientifically sound research trial is acceptable.
Question 65
A 14-year-old girl has had progressive heel pain for the past several months. Based on the radiograph, MRI scan, and biopsy specimens shown in Figures 37a through 37d, treatment should include
Explanation
blood-filled spaces with bland fibrous connective tissue septa. The stroma has histiocytes, fibroblasts, scattered giant cells, hemosiderin, and occasional inflammatory cells. Treatment of these lesions consists of extended curettage, plus or minus the use of adjuvants (liquid nitrogen, phenol, argon beam coagulation), and finally filling the bone void (allograft or other bone substitute).
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Ramirez AR, Stanton RP: Aneurysmal bone cyst in 29 children. J Pediatr Orthop 2002;22:533-539.
Question 66
The iliopectineal fascia runs between which of the following structures?
Explanation
REFERENCES: Masquelet AC, McCullough CJ, Tubiana R: An Atlas of Surgical Exposures of the Lower Extremity. Philadelphia, PA, JB Lippincott, 1993.
Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1109-1149.
Question 67
A 28-year-old woman has a moderate hallux valgus deformity and a prominence of the medial eminence. She can participate in all activities and reports that she could wear 3-inch heels in the past, but she now notes medial eminence pain even while wearing a soft leather flat shoe with a cushioned sole. She requests recommendations regarding surgical correction. Examination reveals a 1-2 intermetatarsal angle of 10 degrees. A clinical photograph and radiograph are shown in Figures 13a and 13b. What is the best course of action?
Explanation
REFERENCES: Chou LB, Mann RA, Casillas MM: Biplanar chevron osteotomy. Foot Ankle Int 1998;19:579-584.
Coughlin MJ: Roger A. Mann Award: Juvenile hallux valgus. Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Pochatko DJ, Schlehr FJ, Murphey MD, Hamilton JJ: Distal chevron osteotomy with lateral release for treatment of hallux valgus deformity. Foot Ankle Int 1994;15:457-461.
Question 68
Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?
Explanation
to 18 hours. This is greater than the 1 hour half-life of unfractionated heparin.
Low-molecular-weight heparin offers an advantage over unfractionated heparin by selectively targeting Factor Xa while having a lesser effect on circulating thrombin (Factor IIa). Circulating thrombin Factor IIa is needed for local hemostasis at the site of the surgical wound. Clinical studies have shown a reduction by one third in the incidence of thrombocytopenia with the use of low-molecular-weight heparin. Low-molecular-weight heparin has been shown to demonstrate similar clinical results compared to warfarin with respect to preventing thromboembolic disease after total hip arthroplasty and complications such as bleeding.
REFERENCES: Zimlich RH, Fulbright BM, Friedman RJ: Current status of anticoagulation therapy after total hip and total knee arthroplasty. J Am Acad Orthop Surg 1996;4:54-62.
Colwell CW Jr, Spiro TE, Trowbridge AA, et al: Use of enoxaparin, a low-molecular-weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Torholm C, Broeng L, Jorgensen PS, et al: Thromboprophylaxis by low-molecular-weight heparin in elective hip surgery: A placebo controlled study. J Bone Joint Surg Br 1991;73:434-438.
Question 69
A 30-year-old man sustains a head injury as well as a femur and pelvis fractures as the result of a rollover motor vehicle accident. He is initially comatosed, but recovers cognitive function after 10 days in the hospital. Soon after awakening he complains of wrist pain and an x-ray demonstrates a distal radius fracture. What is the most likely explanation for this delayed diagnosis?

Explanation
Question 70
A researcher experimenting with limb patterning removes some tissue from 1 part of the limb bud (which we shall call Site A) and transplants it along the anteroposterior (AP) axis to create a mirror-hand duplication. Which of the following is true?
Explanation
The ZPA controls AP (radioulnar) growth. The signaling molecule is Shh, which is dose dependent. Higher Shh doses lead to posterior (ulnar) digits ulnar sided polydactyly. The extent of duplication is dose dependent (higher dose = more replication). Reduced Shh leads to loss of digits. Posterior elements (little finger/ulna) are formed EARLY prior to anterior elements which are formed LATE (radius/thumb). Disruption of AP patterning will result in loss of later forming elements (radius/thumb).
Al-Qattan et al. reviewed embryology of the upper limb. They summarized that embryology of the upper limb can be viewed in 2 distinct ways: the steps of limb development and the way that the limb is patterned along its 3 spatial axes. Cell signaling plays a major role in regulating growth and patterning of the vertebrate limbs. Signaling cell dysfunction results in congenital differences according to the affected signaling axis.
Illustration A shows an experiment to create ulnar dimelia by adding ZPA tissue to the anterior limb bud. The video shows development of the limb.
Incorrect Answers:
Question 71
A cortisone injection in the subacromial space will most likely result in
Explanation
REFERENCES: Matsen FA III, Arntz CT: Subacromial impingement, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 623-646.
Koehler BE, Urowitz MB, Killinger DW: The systemic effects of intra-articular corticosteroid. J Rheumatol 1974;1:117-125.
Question 72
A 30-year-old man caught his dominant little finger on the straps of his windsurfing board 10 days ago. He reports swelling about the distal phalanx and has difficulty completely extending the distal interphalangeal joint. A radiograph is shown in Figure 47. What is the most appropriate treatment for this injury?
Explanation
REFERENCES: Baratz ME, Schmidt CC, Hughes TB: Extensor tendon injuries, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 192.
Bendre AA, Hartigan BJ, Kalainov DM: Mallet finger. J Am Acad Orthop Surg 2005;13:336-344.
Question 73
You are studying a single continuous variable after administration of a defined treatment intervention. Your statistician informs you the data are not normally distributed. What is the best test to analyze the data?
Explanation
Question 74
- Which of the following rehabilitation methods should be used for the first 24 hours following a blunt injury to the quadriceps musculature to avoid short-term stiffness?
Explanation
In the past immobilization in full extension was recommended, but it was noticed that the lack of flexion prolonged disability. Flexion of the knee during the first 24 hours also aids in limiting the extent of intramuscular hematoma.
Myositis ossificans is higher in any patient presenting after a quad contusion and has active knee ROM of less than 120 degrees and delay in treatment greater than 3 days.
Question 75
The main arterial supply to the humeral head is provided by which of the following arteries?
Explanation
REFERENCES: Brooks CH, Revell WJ, Heatley FW: Vascularity of the humeral head after proximal humeral fractures: An anatomical cadaver study. J Bone Joint Surg Br 1993;75:132-136.
Gerber C, Schneeberger AG, Vinh TS: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 76
A 52-year-old man has pain in the sternal area after landing on his right shoulder in a fall from his bicycle. In addition, he reports that he had difficulty swallowing and breathing immediately after the fall, but the symptoms resolved. A CT scan reveals a posterior sternoclavicular dislocation. Initial management should include
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont IL, American Academy of Orthopaedic Surgeons, 1999, pp 287-297.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 1010-1017.
Question 77
After humeral head replacement for four-part fractures, what is the most commonly reported difficulty?
Explanation
REFERENCES: Goldman RT, Koval KJ, Cuomo F, Gallagher MA, Zuckerman JD: Functional outcome after humeral head replacement for acute three- and fourth-part proximal humeral fractures. J Shoulder Elbow Surg 1995;4:81-86.
Hawkins RJ, Switlyk P: Acute prosthetic replacement for severe fractures of the proximal humerus. Clin Orthop 1993;289:156-160.
Question 78
What is a common clinical finding in patients with severe hypercalcemia secondary to bony metastasis?
Explanation
REFERENCE: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 79
A tendon repair is thought to be weakest during which phase of tendon healing?
Explanation
Question 80
Figures below show the clinical photograph and radiograph obtained from a 62-year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?

Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 81
A patient has had a locked posterior dislocation of the shoulder for the past 6 months. After undergoing total shoulder arthroplasty that includes adequate anterior releases and posterior capsulorrhaphy, the patient still exhibits posterior instability intraoperatively. The postoperative rehabilitation regimen should include
Explanation
REFERENCES: Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Loebenberg MI, Cuomo F: The treatment of chronic anterior and posterior dislocations of the glenohumeral joint and associated articular surface defects. Orthop Clin North Am 2000;31:23-24.
Question 82
Examination of a 30-year-old professional singer who has persistent neck and shoulder pain reveals a positive Hoffman’s sign and clonus because of anterior C2-3 cord compression. The MRI scan shown in Figure 11a and the cervical CT scan shown in Figure 11b reveal focal anterior cord compression at the C2-3 level. Which of the following surgical approaches would least affect her professional career?
Explanation
REFERENCES: McAfee PC, Bohlman HH, Reilly LH Jr, Robinson RA, Southwick WO, Nachlas NE: The anterior retropharyngeal approach to the upper part of the cervical spine. J Bone Joint Surgery Am 1987;69:1371-1383.
Lu J, Ebraheim NA, Nadim Y, Huntoon M: Anterior approach to the cervical spine: Surgical anatomy. Orthopedics 2000;23:841-845.
Question 83
What is the best surgical approach for the scapular fracture shown in Figure 46?
Explanation
REFERENCES: Kavanagh BF, Bradway JK, Cofield RH: Open reduction and internal fixation of displaced intra-articular fractures of the glenoid fossa. J Bone Joint Surg Am 1993;75:479-484.
Leung KS, Lam TP: Open reduction and internal fixation of ipsilateral fractures of the scapular neck and clavicle. J Bone Joint Surg Am 1993;75:1015-1018.
Ideberg R: Unusual glenoid fractures: A report on 92 cases. Acta Orthop Scand 1995;66:395-397.
Question 84
Figures 14a and 14b show the plain radiographs of an 85-year-old woman who has had severe pain in the right knee for the past 4 months. Management should consist of
Explanation
REFERENCES: Bergman NR, Rand JA: Total knee arthroplasty in osteonecrosis. Clin Orthop 1991;273:77-82.
Lotke PA, Abend JA, Ecker ML: The treatment of osteonecrosis of the medial femoral condyle. Clin Orthop 1982;171:109-116.
Question 85
Which of the following best characterizes the injury shown in Figure 53? Review Topic

Explanation
Question 86
An 11-year-old boy has had a fever and pain and swelling over the lateral aspect of his right ankle for the past 3 days. Examination reveals warmth, swelling, and tenderness over the lateral malleolus, and he has a temperature of 103.2 degrees F (39.5 degrees C). Laboratory studies show a WBC count of 13,200/mm 3 with 61% neutrophils, an erythocyte sedimentation rate of 112 mm/h, and a C-reactive protein of 15.7. Radiographs and a T 2 -weighted MRI scan are shown in Figures 13a through 13c. Aspiration yields 1 mL of purulent fluid. Management should now consist of
Explanation
definitive treatment.
REFERENCES: Scott RJ, Christofersen MR, Robertson WW Jr, et al: Acute osteomyelitis in children: A review of 116 cases. J Pediatr Orthop 1990;10:649-652.
Vaughan PA, Newman NM, Rosman MA: Acute hematogenous osteomyelitis. J Pediatr Orthop 1987;7:652-655.
Question 87
An 18-year-old football player reports acute pain and swelling after a direct injury to his plantar flexed foot. Examination reveals midfoot swelling and tenderness. Nonstanding radiographs are normal. What is the next most appropriate step in management?
Explanation
to activity.
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries with the transmetatarsal joint. Orthop Clin North Am 2001;32:11-20.
Question 88
To prevent injury to the posterior interosseous nerve during the approach for reduction and fixation of a fracture of the radial head, anterior retraction should be performed with the forearm
Explanation
Deep surgical dissection-Fully pronate the forearm to move the posterior interosseous nerve away from the operative field. Incise the capsule of the elbow joint longitudinally to reveal the underlying capitulum, the radial head, and the annular ligament. Do not incise the capsule too far anteriorly; the radial nerve runs over the front of the anterolateral portion of the elbow capsule. Do not continue their dissection below the annular ligament or retract vigorously, distally, or anteriorly, because the posterior interosseous nerve lies within the substance of the supinator muscle and is vunerable to injury.
Dangers: Nerves-The posterior interosseous nerve is in no danger as long as the dissection remains proximal to the annular ligament. Pronation of the forearm keeps the nerve as far from the operative field as it possible can be. To ensure the safety of the nerve, take great care to place the retractors directly on the bone and be careful in their placement. Because the posterior interosseous nerve actually may touch the bone of the radial neck, directly opposite the bicipital tuberosity, placing retractors behind it poses a risk.
Question 89
Which group experiences the highest rate of anterior cruciate ligament (ACL) tears?
Explanation
ACL tears are several times more common among women than men. Women who land from jumps in increased valgus and external rotation are at particularly increased risk for ACL tears. Women have smaller notch widths and a smaller ACL cross-sectional area than men, but these factors have not been proven to increase risk for ACL tears.

CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 67
Figure 64 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain.
Question 90
An otherwise healthy year-old woman has pain 2 years after total hip arthroplasty. The clinical photograph in below demonstrates her skin envelope, and associated radiograph. Her C-reactive protein level is normal, and her erythrocyte sedimentation rate is mildly elevated. The white blood cell count is normal. Hip aspiration attempted under fluoroscopy generates no fluid. What is the best definitive treatment?
Explanation
This patient clearly has a chronically infected total hip arthroplasty, indicated by the open, draining sinus, as well as trochanteric bone resorption on radiographs, and two years of pain. Recently, specific guidelines have been published to better help the clinician define infection. Repeating the hip aspiration is unnecessary, because infection is already evident. Initiating a wound care consult would not address the underlying infection. The determination whether to retain the components or perform a two-stage exchange is based more on the acuity of infection. In this particular case, the patient is chronically infected. Irrigation and debridement with a liner exchange and retention of the components are reserved for the acute setting.
Question 91
No fractures were identified and the patient was treated nonsurgically in a range-of-motion brace. Two months later, he continued to experience elbow pain and was unable to return to sports. He regained motion and strength with physical therapy, there was no gross instability with varus or valgus testing, and he had a negative moving-valgus stress test. The orthopaedic surgeon performed an examination under anesthesia in the operating room (Video 54). Which anatomic structure is injured?
Explanation
Ninety percent of elbow dislocations occur in a posterolateral direction. O’Driscoll and associates described the mechanism of injury in posterolateral elbow dislocations in 1992, reporting that they occur most typically after a fall onto an outstretched arm. As the arm hits the ground it causes axial compression, forearm supination, and valgus load across the elbow. The triceps fires, pulling the olecranon posterior; the forearm supinates while simultaneous shoulder internal rotators fire; and the elbow falls into valgus. These 3 mechanisms cause the elbow to subluxate and dislocate posterolaterally. The elbow is most stable following posterolateral dislocation in a flexed and pronated position. The elbow is least stable in extension and supination. Simple dislocation often can be treated nonsurgically, while fracture dislocation will usually necessitate surgical intervention. The video shows the elbow pivot-shift test, which evaluates for posterolateral rotatory instability. A positive test finding elicits apprehension and, in this case, radial head subluxation and confirms an insufficient lateral UCL.
Question 92
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Explanation
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 93
A 27-year-old man has recurrent anterior shoulder instability following an arthroscopic Bankart repair 4 years ago. Current CT scans are shown in Figures 19a and 19b. Deficiency of what mechanism is most likely to contribute to the current joint instability? Review Topic

Explanation
Question 94
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 95
A patient who underwent intramedullary nailing of a femoral shaft fracture 2 weeks ago now reports groin pain. What is the next most appropriate step in management?
Explanation
obtaining a dedicated AP radiograph of the hip with the leg internally rotated 15 to 20 degrees. Because the femoral neck is anteverted, 15 to 20 degrees of internal rotation of the hip offers the best view of the femoral neck. Whereas associated lumbar spine pathology may cause groin pain, the presence of a missed femoral neck fracture must first be ruled out prior to investigating other sources of pain.
Question 96
A 54-year-old woman underwent prophylactic intramedullary fixation for an impending fracture of her right femur secondary to metastatic breast cancer. A bone scan revealed a second lesion in her inferior pubic ramus. Her oncologist has recommended that she receive the intravenous bisphosphonate, zoledronic acid, because the medication would
Explanation
REFERENCES: Mundy GR, Yoneda T: Bisphosphonates as anticancer drugs. N Engl J Med 1998;339:398-400.
Rosen LS, Gordon D, Kaminski M, et al: Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patients with breast cancer or osteolytic lesions of multiple myeloma: A phase III, double-blind, comparative trial. Cancer J 2001;7:377-387.
Question 97
Which of the following tumors have characteristic chromosomal translocations?
Explanation
REFERENCES: Sandberg AA: Cytogenetics and molecular genetics of bone and soft-tissue tumors. Am J Med Genet 2002;115:189-193.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 98
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
REFERENCES: Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 99
Figure 1 is the radiograph of an 18-year-old right-hand-dominant man who has pain and stiffness 3 months after sustaining an injury to his dominant ring finger while playing basketball. An examination reveals significant proximal interphalangeal (PIP) joint swelling with active and passive PIP joint motion of 15/40 degrees of flexion. What is the best next step?

Explanation
This patient has a subacute PIP joint dorsal fracture dislocation with involvement of 50% to 60% of the palmar articular surface of the base of P2. A "V sign" (Figure 2) is evident, indicating dorsal subluxation of the joint. In some cases, an ORIF is possible, but substantial comminution often precludes proper restoration of the critical volar buttress. Therapy is not the answer because the joint is dorsally subluxated and must be corrected. Dynamic external fixation on its own would not result in a reduced joint. The hemi-hamate autograft has proven useful in this type of scenario and serves to restore the volar buttress of P2 using an osteochondral autograft harvested from the distal articular aspect of the hamate at its articulation with the fourth/fifth metacarpal bases. Intraoperative clinical photographs and a postsurgical radiograph are shown in Figures 3 through 5.






Question 100
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include
Explanation
REFERENCES: Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459.
Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Skrzynski MC, Biermann JS, Montag A, Simon MA: Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1996;78:644-649.
