Orthopedic Board Review MCQs: Spine, Trauma, Foot & Wrist | Part 185

Key Takeaway
This page offers Part 185 of a professional orthopedic surgery board review quiz. Designed for orthopedic residents and surgeons preparing for OITE/AAOS/ABOS exams, it features 100 high-yield, verified MCQs covering key topics like Deformity, Fracture, Hip, and Wrist to ensure comprehensive exam preparation.
About This Board Review Set
This is Part 185 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 185
This module focuses heavily on: Deformity, Dislocation, Foot, Fracture, Hip, Tendon, Wrist.
Sample Questions from This Set
Sample Question 1: A previously healthy 30-year-old woman has neck pain and bilateral hand and lower extremity tingling with weakness after falling down stairs. She is alert and oriented. Examination reveals incomplete quadriplegia at the C6 level that remain...
Sample Question 2: Which of the following are considered appropriate nonsurgical bracing/orthotic options for a supple adult-acquired flatfoot deformity with forefoot abduction, secondary to posterior tibial tendon insufficiency?...
Sample Question 3: A 14-year-old girl reports hip pain that is exacerbated by weight bearing. A radiograph and biopsy specimen are shown in Figures 16a and 16b. The best course of management should be...
Sample Question 4: A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of...
Sample Question 5: A 28-year-old man has had a 2-week history of right posterior leg pain, with numbness and tingling in the same distribution. He denies any problems with bowel or bladder function. Examination shows intact motor strength in his bilateral low...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A previously healthy 30-year-old woman has neck pain and bilateral hand and lower extremity tingling with weakness after falling down stairs. She is alert and oriented. Examination reveals incomplete quadriplegia at the C6 level that remains unchanged throughout her evaluation and initial treatment. Radiographs show a bilateral facet dislocation of C6 on C7 without fracture. Attempts at reduction with halo cervical traction up to her body weight are unsuccessful. What is the next most appropriate step?
Explanation
REFERENCES: Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217.
Fardon DF, Garfin SR, Abitbol J (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 247-262.
Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. J Bone Joint Surg Am 1991;73:1555-1560.
Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 2
Which of the following are considered appropriate nonsurgical bracing/orthotic options for a supple adult-acquired flatfoot deformity with forefoot abduction, secondary to posterior tibial tendon insufficiency?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Imhauser CW, Abidi NA, Frankel DZ, et al: Biomechanical evaluation of the efficacy of external stabilizers in conservative treatment of acquired flat foot deformity. Foot Ankle Int 2002;23:727-737.
Question 3
A 14-year-old girl reports hip pain that is exacerbated by weight bearing. A radiograph and biopsy specimen are shown in Figures 16a and 16b. The best course of management should be
Explanation
REFERENCES: Azouz EM, Karamitsos C, Reed MH, Baker L, Kozlowski K, Hoeffel JC: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420.
Hecht AC, Gebhardt MC: Diagnosis and treatment of unicameral and aneurysmal bone cysts in children. Curr Opin Pediatr 1998;10:87-94.
Question 4
A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of
Explanation
REFERENCES: Cooney WP, Linscheid RL, Dobyns JH, Wood MB: Scaphoid nonunion: Role of anterior interpositional bone grafts. J Hand Surg Am 1988;13:635-650.
Fernandez DL: A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-737.
Stark HH, Rickard TA, Zemel NP, Ashworth CR: Treatment of ununited fractures of the scaphoid by illiac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am
1988;70:982-991.
Feldman MD, Manske PR, Welch RL, Szerzinski JM: Evaluation of Herbert screw fixation for the treatment of displaced scaphoid nonunions. Orthopedics 1997;20:325-328.
Question 5
A 28-year-old man has had a 2-week history of right posterior leg pain, with numbness and tingling in the same distribution. He denies any problems with bowel or bladder function. Examination shows intact motor strength in his bilateral lower extremities, with numbness to light touch in the lateral border of his right foot. Over the past 2 weeks, his leg pain has improved significantly. MRI scans are shown in Figures 57a and 57b. What is the most appropriate course of management? Review Topic

Explanation
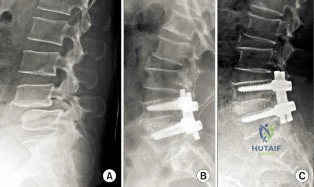
(SBQ12SP.9) A 62-year-old male underwent posterior spinal instrumented fusion for degenerative lumbar spondylolithesis one year ago. He presents to office complaining of persistent lower back pain. The pain initially improved but over the last 6 months he has had recurring pain at the site of the surgery primarily with activity. He denies back pain at rest or night pain. Physical examination reveals a well healed wound and no physical abnormalities. He has no tenderness to palpation to the thoracic or lumbar spine. He has no neurological deficits. His laboratory results show an erythrocyte sedimentation rate (ESR) = 8 mm/h and C-reactive protein (CRP) = 3 mg/L at the last visit which are both within normal limits. Figure A shows a series of radiographs from his pre-operative, 3 month post-operative and 1 year post-operative clinic visits, respectively. Which of the following investigations would best confirm the suspected underlying diagnosis? Review Topic
MRI of lumbar spine
Repeat ESR/CRP and whole body bone scan
CT of lumbar spine
Dynamic flexion/extension plain film radiographs
Dynamic lateral bending plain film radiographs
This patient has clinical and radiographic features of failed spinal arthrodesis. CT scan have been shown to be the most relable method for assessing spinal fusion postoperatively.
Reported rates of nonunion following posterior spinal fusion range from 0-70%. Rates are variable due to the various operative techniques, underlying diagnoses as well as asymptomatic patients. Non-union may lead to changes in alignment, spinal instability and potential neurological injury. Static radiographs have long been used as a practical method of fusion assessment, but these tend to significantly overestimate the presence of a solid fusion. Lack of movement at a fused segment, on dynamic views, does not confirm fusion. CT offers excellent bony resolution and are less affected by metal artifact compared to MRI.
Patel et al. showed that tobacco use, malnutrition, oral anti-inflammatory use, multilevel fusion, prior spine surgery, and sagittal imbalance are all risk factors for spinal nonunion.
Mok et al. looked at erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels after spinal surgery and compared their usefulness as predictors of infectious complications in the early postoperative period. They found that CRP is more applicable, predictable, and responsive in the early postoperative period compared with ESR. Using a second rise or failure to decrease as expected for CRP is sensitive for infection.
Shelby et al. reviewed the radiological assessment of spinal fusion. They comment that fine-cut imaging, multiplanar reconstruction, and metal artifact reduction have increased the ability to assess fusion on CT.
Figure A shows a series of lateral radiographs of the lumbar spine with posterior spinal instrumentation. Illustration A shows a lateral CT scan image of multi-level pseudoarthrosis after posterior spinal instrumented fusion. Illustration B shows an
intra-operative
view
of
spinal
pseudoarthrosis
(white
arrow).
Incorrect
(SBQ12SP.19) A 41-year-old male presents with acute onset of low back pain that started when he was trying to lift a heavy box while helping his brother move apartments two days ago. The pain has been severe enough to cause him to miss work yesterday. He has no neurologic deficits. What are the chances he will return to work within 6 weeks? Review Topic
1 80 to 90%
2 70 to 80%
3 60 to 70%
4 50 to 60%
5 40 to 50%
Most adults (up to 80%) will experience an episode of low back pain in their lifetime. In those whose pain is severe enough to cause them to miss work, 60 to 70% will return by 6 weeks, and 80 to 90% will return by 12 weeks.
Low back pain is common in adults. Most patients experience resolution of symptoms quickly and have no lasting loss of function. However, 5 to 10% develop chronic pain. Recurrence of pain is common, and is part of the natural history, occurring in 20 to 72% of patients. After 12 weeks, return to work rates are slow.
Shen et al. review the nonoperative management of acute and chronic low back pain. The authors note that none of the available interventions has been proven by high quality large randomized controlled trials. The authors believe that low dose oral
steroids are safe in the short term and that injection therapy should not be used without a reasonable presumptive diagnosis.
Madigan et al. review the management of lumbar degenerative disease. The authors emphasize that the majority of patients improve within 6 weeks with or without treatment. For patients that do not, the authors do not recommend epidural injection, as there are no good studies to support their use in the treatment of discogenic back pain. When surgical treatment is indicated they state that arthrodesis is the gold standard, although the long term results of total disk arthroplasty are being elucidated.
Illustration A shows a table of available non-operative treatment modalities for back pain. Illustration B shows a list of possible diagnoses associated with acute low back pain, with those associated with neurogenic pain italicized. Illustration C shows a list of 'red flag' symptoms indicating serious/emergent causes of low back pain.
Incorrect
2:
Longer
to than
90%
Question 6
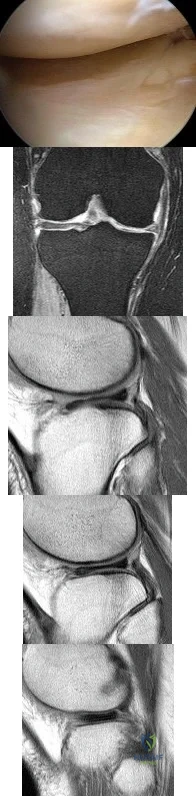
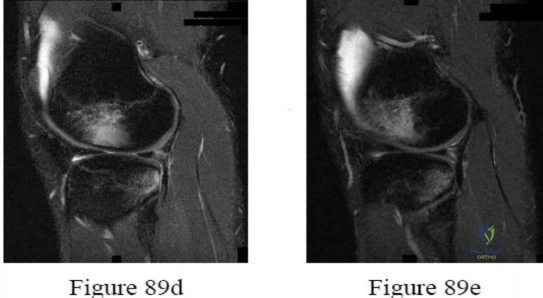
Figure 80a shows an arthroscopic view from an infralateral portal of a right knee. Figure 80b shows a coronal MRI scan, and Figures 80c through 80e show consecutive sagittal images of the knee. The images show what anatomic finding? Review Topic
Explanation
Question 7
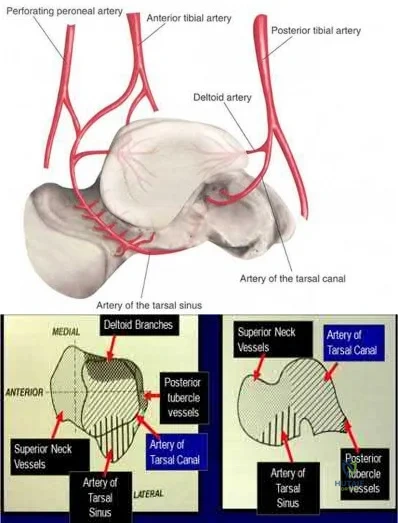
A 29-year-old male sustains the isolated lower extremity injury shown in Figure A. During open reduction, what structure must be kept intact in order to protect the remaining blood supply to the talar body?

Explanation
The review article by Fortin et al discusses talar blood supply, injury mechanisms and classifications, and treatment options. They state that the main artery to the body of the talus is the artery of the tarsal canal, which is a branch of the posterior tibial artery. The peroneal and anterior tibial artery also contribute branches to the talus.
Illustration A and B show the arterial network of the talus.
OrthoCash 2020
Question 8
An 18-year-old patient sustains a comminuted left femoral fracture starting 6.5cm distal to the lesser trochanter. He undergoes antegrade femoral nailing in the supine position on a radiolucent table. Upon completion of proximal and distal interlocking, both patellae are positioned facing the ceiling and a lateral radiographs confirms that the posterior condyles of both limbs are aligned. On AP imaging of both femora, it is noted that the lesser trochanter of the left (injured) side is larger than the right (uninjured) side. Assuming symmetrical anteversion, the left femur has been nailed Review Topic
Explanation
Rotational malalignment is the most common complication of intramedullary nailing of a comminuted diaphyseal femoral fracture. The rotational profile of the lesser trochanter can be used to evaluate rotational alignment. The proximal femur is rotated until a neutral position is obtained as judged by the radiographic profile of the lesser trochanter. If the AP image shows a smaller lesser trochanter, there is IR of the LT. A larger LT indicates external rotation (ER) of the LT.
Jaarsma et al. describe CT imaging in determining rotational alignment. They note that the incidence of post-nailing malalignment > 10 ° is 40%, > 15 ° is 20-30%, and
> 20 ° is 16%. They also note that patients with ER deformities have more symptoms than those with IR deformities, and that small deformities <15 ° give rise to less complaints. This is because ER deformities lead to compensation with hip retroversion, which causes more symptoms than hip anteversion when compensating for IR deformities.
Incorrect Answers:
(SBQ12TR.37) A 44-year-old male presents with the isolated injury seen in Figure A after a motor vehicle accident and underwent the operative treatment seen in Figure B within 8 hours from the time of incident. Which of the following complications is this patient at highest risk of developing?

Pulmonary embolus
Periprosthetic fracture
Contralateral hip fracture
Osteonecrosis
Infection
This young male patient has sustained a displaced femoral neck fracture and underwent open reduction internal fixation with 3 cannulated screws. Based on the available options, the patient is most at risk of developing osteonecrosis of the femoral head.
Femoral neck fractures in young patients typically are the result of a high-energy trauma. Fracture displacement has been shown to disrupt vascular supply to the femoral head by interrupting retinacular vessels and ligament teres vascularization, as well as increasing intracapsular pressure, producing a tamponade effect. The incidence of osteonecrosis in patients younger than 60 years with displaced femoral neck fractures has been shown to be between 15-30%. Quality of reduction is one key factor that has been shown to influence outcomes postoperatively.
Loizou et al. prospectively studied 1,023 patients who sustained an intracapsular hip fracture that was treated with internal fixation using standard fixation modalities. They showed that osteonecrosis was less common for undisplaced (4.0%) than for displaced fractures (9.5%). The population at greatest risk were women younger than the age of 60 with displaced fractures.
Barnes et al. review subcapital hip fractures. They found that late segmental collapse was more common in displaced fractures in women younger than age 75 years than in those older than age 75 years treated with internal fixation.
Figure A shows a displaced, Garden 3/Pauwels I hip fracture. Figure B shows anatomical fixation with 3 cannulated screws.
Incorrect Answers:
Question 9
- The stability of the longitudinal arch of the foot during standing with equal weight on both feet is due primarily to
Explanation
Question 10
A 67-year-old retired steelworker was involved in a motor vehicle accident and sustained a midcervical spinal cord injury. Radiographs and MRI scans reveal severe cervical stenosis and spondylosis without fractures or dislocations. Neurologic examination reveals an ASIA C spinal cord impairment with greater motor involvement of the upper extremities than the lower extremities. What is the probability that the patient eventually will become ambulatory?
Explanation
(ASIA C and D) ultimately walked. The poorest prognosis, however, was in ASIA C patients older than age 50, in which only 40% walked.
REFERENCES: Penrod LE, Hegde SK, Ditunno JF Jr: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Northrup BE: Acute injuries to the spine and spinal cord: Evaluation and early treatment, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, p 735.
Question 11
What is the most consistent finding regarding glenohumeral kinematics in patients with symptomatic tears of the rotator cuff?
Explanation
REFERENCES: Yamaguchi K, Sher JS, Anderson WK, et al: Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000;9:6-11.
Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
Question 12
A 32-year-old man who sustained a tarsometatarsal (Lisfranc) injury 3 years ago now reports increasing pain in the left foot. Orthotics, nonsteroidal anti-inflammatory drugs, and injections have provided only temporary relief. Examination reveals swelling and tenderness over the tarsometatarsal joints. Radiographs show advanced arthrosis of the first and second tarsometatarsal joints. Management should now include
Explanation
REFERENCES: Sangeorzan BJ, Veith GR, Hansen ST Jr: Salvage of Lisfranc’s tarsometatarsal joints by arthrodesis. Foot Ankle 1990;10:193-200.
Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Question 13
Which method of flexor tendon repair that necessitates excursion through the A2 pulley allows for the most thorough assessment of tendon gliding?
Explanation
Wide-awake repair under only local anesthesia, regardless of the technique, allows direct inspection of the tendon repair and active excursion. Regional anesthesia and Bier block anesthesia do not allow active motion (Bier block necessitates continued use of a tourniquet, which limits muscle function). The A2
pulley should be preserved, especially the distal 50%, to maintain tendon function. All of the listed techniques for suture repair are acceptable options.
Question 14
-A 15-year-old boy with mild type I osteogenesis imperfecta (OI) has a midshaft radius/ulna fracture that is in bayonet apposition with loss of the radial bow and 40-degree apex volar and ulnar angulation. Closed reduction improves the angulation to 20 degrees; the bayonet apposition and loss of radial bow remains.His contralateral forearm has a normal appearance upon examination. What is the best treatment for this fracture?
Explanation

Question 15
Figure 65 is the lumbar spine MR image of a 63-year-old woman who has a 3-year history of increasingly bothersome back pain and bilateral buttock and leg pain. She has performed 6 weeks of physical therapy, received epidural injections, and experienced some good short-term results, but her leg pain continues to worsen. What is the most appropriate course of treatment?

Explanation
This patient has symptoms consistent with neurogenic claudication secondary to lumbar spinal stenosis and degenerative spondylolisthesis. Her symptoms are chronic and she has undergone an appropriate course of nonsurgical care. Nevertheless, her symptoms are worsening and surgical intervention is a
reasonable consideration. Studies have shown that patients with lumbar spinal stenosis with associated degenerative spondylolisthesis benefit most from decompression of the neural elements that are stenotic and subsequent fusion across the degenerative slip. Anterior lumbar interbody fusion likely will not address stenosis at the level of the slip and may not result in adequate neurologic decompression. Partial laminotomy and diskectomy likely will not provide adequate neural decompression because these procedures would only address unilateral compression and this patient has bilateral issues. Lumbar laminectomy without fusion could be performed but has been associated with results inferior to lumbar laminectomy with fusion when addressing stenosis with spondylolisthesis.
RECOMMENDED READINGS
Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. PubMed PMID: 19487505. View Abstract at PubMed
Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991 Jul;73(6):802-8. PubMed PMID: 2071615. View Abstract at PubMed
Lombardi JS, Wiltse LL, Reynolds J, Widell EH, Spencer C 3rd. Treatment of degenerative spondylolisthesis. Spine (Phila Pa 1976). 1985 Nov;10(9):821-7. PubMed PMID: 4089657. View Abstract at PubMed
RESPONSES FOR QUESTIONS 66 THROUGH 69
Deep surgical-site infection
Adjacent segment degeneration
Pressure ulcers
Iatrogenic neurologic injury
Incidental durotomy
Hardware failure
Match the frequently encountered complication listed above with the appropriate clinical scenario below.
Question 16
Figure A is an AP radiograph of a 68-year-old man who presents to clinic with shoulder pain and dysfunction. On examination of his shoulder, he has pseudoparalysis with attempt at forward elevation and a positive hornblower's sign while demonstrating normal belly press test. Treatment should consist of: Review Topic

Explanation
RTSA can improve pain and function in shoulders with forward elevation pseudoparalysis secondary to rotator cuff tear arthropathy. Following arthroplasty, the deltoid alone can restore overhead elevation but it does not address active external rotation deficit. LDT is a well described procedure for treatment of irreparable posterosuperior rotator cuff tear. Combining RTSA and LDT can address both deficits and in select patients yields significant pain relief and restoration of function.
Walch et al found that hornblower's sign had 100% sensitivity and 93% specificity for irreparable degeneration of teres minor.
Puskas et al present clinical outcomes of RTSA combined with LDT for treatment of chronic combined pseudoparesis of elevation and external rotation of the shoulder in 40 patients. At a mean follow-up of 53 months, the author report excellent clinical outcomes.
Figure A demonstrates a proximal migration of the humerus resulting in femoralization of the humeral head and acetabularization of the acromion from a massive rotator cuff tear.
Incorrect answers:
Question 17
The mother of a 24-month-old girl reports that the child cannot rotate her right forearm. She also notes delayed development, with the child first walking at 18 months. The child has a five-word vocabulary and has not begun using simple phrases. Examination reveals that the right forearm is fixed in 80 degrees of pronation. The remainder of the examination of both upper extremities is otherwise normal. A radiograph is shown in Figure 41. Which of the following studies will best aid in diagnosis?
Explanation
not indicated.
REFERENCE: Rimoin DL, Connor JM, Pyeritz RE, Korf BR: Emery & Rimoin’s Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002,
pp 1196-1197.
Question 18
A 55-year-old man who works as a carpenter reports chronic right anterior shoulder pain and weakness. Examination reveals 90 degrees of external rotation (with the arm at the side) compared to 45 degrees on the left side. His lift-off examination is positive, along with a positive belly press finding. An MRI scan reveals a chronic, retracted atrophied subscapularis tendon. What is the most appropriate management of his shoulder pain and weakness? Review Topic
Explanation
Question 19
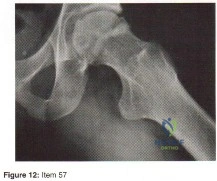
- Figure 12 shows the frog-lateral radiograph of a 45-year-old man who has a painful left hip. What is the most likely diagnosis?
Explanation
Question 20
Figures 34a and 34b show the clinical photographs of a 46-year-old woman who has a painful deformity of the second toe. Surgical treatment consisting of metatarsophalangeal capsulotomy and proximal interphalangeal joint resection arthroplasty resulted in satisfactory correction, but the toe remains unstable at the metatarsophalangeal joint. What is the next most appropriate step?
Explanation
REFERENCES: Coughlin MJ: Crossover second toe deformity. Foot Ankle 1987;8:29-39.
Thompson FM, Deland JT: Flexor tendon transfer for metatarsophalangeal instability of the second toe. Foot Ankle 1993;14:385-388.
Question 21
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Explanation
REFERENCES: Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
O’Hara LJ, Marshall RW: Far lateral lumbar disc herniation: The key to the intertransverse approach. J Bone Joint Surg Br 1997;79:943-947.
Question 22
Figure 199 is the clinical photograph of a 68-year-old man with a history of atrial fibrillation who was treated with warfarin. Nine days after undergoing elective total hip arthroplasty, he has a swollen left thigh. His wound remains dry and he is afebrile. His erythrocyte sedimentation rate (ESR) is 25 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein (CRP) level is 6.1 mg/L (rr, 0.08-3.1 mg/L). Aspiration reveals 3246 white blood cells (WBCs)/µL with 47% polymorphonucleocytes. Treatment at this time should consist of
Explanation
This patient has a large postsurgical hematoma. Although his ESR and CRP level are elevated, they are not considered elevated given his recent surgery. Additionally, the hip aspiration reveals a synovial cell count lower than 10000 WBC/µL along with a low percentage of polymorphonucleocytes. Treatment at this time should consist of observation. The hematoma is likely attributable to postsurgical anticoagulation, considering his history of atrial fibrillation.
Question 23
A 9-year-old girl has pain over the fifth toe that is aggravated by shoe wear. Clinical photographs are shown in Figures 28a and 28b. Treatment of this deformity should consist of
Explanation
REFERENCES: Black GB, Grogan DP, Bobechko WP: Butler arthroplasty for correction of adducted fifth toe: A retrospective study of 36 operations between 1968 and 1982. J Pediatr Orthop 1985;5:439-441.
Paton RW: V-Y plasty for correction of varus fifth toe. J Pediatr Orthop 1990;10:248-249.
Coughlin MJ, Mann RA: Lesser toe deformities, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 5. St Louis, MO, Mosby, 1986, pp 132-157.
Question 24
An otherwise healthy 25-year-old man underwent a right anterior cruciate ligament reconstruction with a bone-patellar tendon-bone allograft. Routine preimplantation cultures of the allograft taken by the surgeon were positive for coagulase-negative Staphylococcus 5 days postoperatively. The patient has exhibited no evidence of clinical infection and his postoperative course has been uncomplicated during this time. What is the ideal management of this patient?
Explanation
implanted with a "contaminated" graft develop a clinical infection. The results of the current literature suggest that the treatment of low-virulence organisms is unnecessary if no evidence of clinical infection exists. Preimplantation cultures do not appear to correlate with clinical infection. Therefore, the routine culture of allograft tissue is not recommended.
Question 25
The posterior horn of the medial meniscus receives its primary blood supply from what artery?
Explanation
REFERENCES: Insall J, Scott WN: Anatomy, in Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, pp 64-70.
Scapinelli R: Vascular anatomy of the human cruciate ligaments and surrounding structures. Clin Anat 1997;10:151-162.
Question 26
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
REFERENCE: Kelly MA: Nonprosthetic management of the arthritic knee, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 245-249.
Question 27
Hip pain of 1-month duration has developed in a 72-year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. What is this patient's prognosis for infection resolution?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin-resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was 21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 28
When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more than the extension space?
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point,
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 29
There is increasing concern about the ethical relationship of orthopaedists to the orthopaedic equipment industry. Which of the following describes the most appropriate relationship?
Explanation
REFERENCE: Opinions on ethics and professionalism, in Guide to The Ethical Practice of Orthopaedic Surgery, ed 6. American Academy of Orthopaedic Surgeons, Rosemont, IL, 2006, pp 38-42.
Question 30
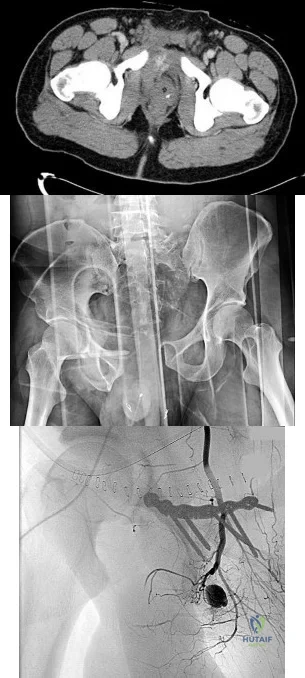
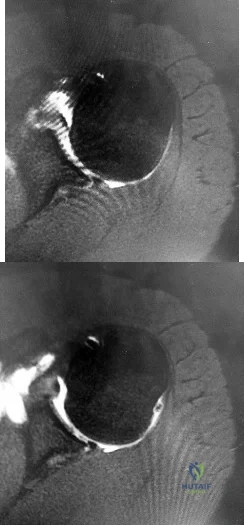
4A 4B 4C A 30-year-old man was involved in a high-speed motorcycle collision and sustained the injury shown in Figure 4a. Hypotension ensued shortly after arrival in the emergency department. Figure 4b is the initial contrast pelvic CT image with an unrecognized blush consistent with arterial bleeding. During surgical repair, the patient was noted to have active bleeding and an angiogram was obtained (Figure 4c). Which structure is the likely cause of his bleeding?
Explanation
Pelvic bleeding occurs predominantly from disruption of the posterior venous plexus and bleeding from the fractured bone. Occasionally arterial bleeding is seen, with injury to the superior gluteal artery most common. Anterior pelvic bleeding occurs from injury to the obturator artery (commonly from a pubic bone fracture laceration) and less frequently from the pudendal artery near the symphysis. The location of the bleeding on CT and angiography images does not correspond to the superior gluteal, external iliac, or femoral arteries.
RECOMMENDED READINGS
Suzuki T, Smith WR, Moore EE. Pelvic packing or angiography: competitive or complementary? Injury. 2009 Apr;40(4):343-53. Epub 2009 Mar 17. Review.PubMed PMID: 19278678. View Abstract at PubMed
Loffroy R, Yeguiayan JM, Guiu B, Cercueil JP, Krausé D. Stable fracture of the pubic rami: a rare cause of life-threatening bleeding from the inferior epigastric artery managed with transcatheter embolization. CJEM. 2008 Jul;10(4):392-5. PubMed PMID: 18652733. View Abstract at PubMed
White CE, Hsu JR, Holcomb JB. Haemodynamically unstable pelvic fractures.Injury. 2009 Oct;40(10):1023-30. Epub 2009 Apr 16. Review. PubMed PMID:19371871. View Abstract at PubMed
RESPONSES FOR QUESTIONS 5 THROUGH 8

5A

5B
- Avascular necrosis, head collapse, and screw penetration
- Fixation failure and varus collapse
- Humeral stem loosening
- Glenoid component loosening
- Hardware failure (breakage of plate or screws)
- Shoulder dislocation
Please choose from the responses to identify the most likely complication in each scenario.
Question 31
What is the most common fracture associated with a lateral subtalar dislocation?

Explanation
Post-reduction x-rays need to be scrutinized carefully for fractures of the tarsal bones as this is the most common injury associated with subtalar dislocations. Occult fractures of the lateral process of the talus are also associated with these injuries.
The referenced study by Wagner et al noted radiographic subtalar DJD in 2/3 of their patients, but noted no correlation between radiographic and clinical outcomes. The referenced study by Bibbo et al noted an 88% incidence of other concurrent injuries and an 89% rate of radiographic DJD at 5 year follow-up. The referenced article by Saltzman et al is a review of hindfoot dislocations.
Question 32
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 33
Figure 1 is the T2 coronal MRI scan(Massive atraumatic rotator cuff tear) of a 52-year-old woman with a 6-month history of shoulder pain. She does not recall a history of trauma. Physical therapy is recommended. What is the most significant predictor of failure of nonoperative treatment?
Explanation
cuff tear and the severity of patient’s reported pain did not predict failure of nonoperative treatment. Patients who have low expectations regarding the effectiveness of physical therapy are more likely to fail nonoperative treatment.
Question 34
A 21-year-old male is brought to the emergency department after being involved in gang-related violence. A radiograph of his pelvis is shown in Figure A. The patient is hemodynamically stable. Which of the following imaging modalities is the next best step in evaluating this patient for the most common associated injury? Review Topic

Explanation
The incidence of GSW is increasing and it is the 2nd leading cause of death in young males in the US after motor vehicle accidents. The incidence of a GSW to the buttock is approximately 8% of all GSW to the extremities. Potential complications of pelvic and acetabular GSW include septic arthritis, enterocutaneous, enteroacetabular, and vesicoacetabular fistulas, infected nonunion, malunion, and injuries to the iliac vessels. The presence or absence of intra-abdominal injuries affects treatment and outcome.
Bartkiw et al. reviewed 2808 GSW and found 1235 associated fractures including 42 fractures of the hip and pelvis. Ten orthopaedic operative procedures were performed in 7 patients. Associated nonorthopaedic injuries included 15 small/large bowel perforations (36%), 7 vessel lacerations (17%), and 2 urogenital injuries (5%) that required surgery.
Najibi et al. reviewed 39 GSW to acetabulum. They found 32 simple and 7 associated fracture patterns. The most common simple and associated patterns were anterior column and both column, respectively. Bowel injuries were the most common associated injures (42%). Predictors of poor outcome include high-velocity missile, involvement of acetabular dome, abdominal injury, nerve injury, vascular injury, and male gender. Deep infection was associated with primary anastomosis of bowel injury and an associated fracture pattern.
Figure A shows a GSW to the right hip with acetabular fracture and visible bullet fragment.
Incorrect Answers:
Question 35
Which of the following factors is most likely to contribute to pseudarthrosis in a patient who has undergone a single-level anterior decompression and fusion procedure for the treatment of cervical radiculopathy? Review Topic
Explanation
diabetes mellitus, have been shown to significantly increase pseudarthrosis rates. The literature has been mixed with regard to fusion rates for allograft versus autograft, especially for one-level fusions; in that category, there is minimal, if any, difference. Similarly, several authors have shown higher rates of fusion with uninstrumented single-level rather than instrumented anterior cervical decompressions and fusions. The level (ie, cranial or caudal) of fusion and sagittal alignment have not been correlated with fusion rates.
Question 36
Halo treatment for preadolescent children typically requires the use of which of the following? Review Topic
Explanation
Question 37
A 45-year-old man sustains a low-velocity gunshot wound to the base of the right thumb. The open wound is allowed to heal by secondary intention, resulting in a contracture of the first web space. Clinical photographs are shown in Figures 49a through 49c. Treatment should now consist of
Explanation
REFERENCES: Buchler U, Frey HP: Retrograde posterior interosseous flap. J Hand Surg Am 1991;16:283-292.
Brunelli F, Valenti P, Dumontier C, et al: The posterior interosseous reverse flap: Experience with 113 flaps. Ann Plast Surg 2001;47:25-30.
Question 38
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for
Explanation
REFERENCES: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Song KM, Sloboda JF: Acute hematogenous osteomyelitis in children. J Am Acad Orthop Surg 2001;9:166-175.
Question 39
An intoxicated 68-year-old man fell at home. Examination reveals abrasions on his forehead, 2/5 weakness of his hand intrinsics and finger flexors, and 4/5 strength of the deltoid, biceps, and triceps bilaterally. Lower extremity motor function is 5/5. Sensory examination to pain and temperature is diminished in his hands but intact in his lower extremities. Deep tendon reflexes are depressed in all four extremities, but perianal sensation and rectal tone are intact. Foley catheterization yields 700 mL of urine. Radiographs of the cervical spine reveal multilevel spondylosis without fracture or subluxation. An MRI scan reveals high-intensity signal change within the cord substance at C5. What is the most likely diagnosis?
Explanation
REFERENCES: Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 541-549.
Schneider RC, Thompson JM, Rebin J: The syndrome of acute central cervical spinal cord injury. J Neurol Neurosurg Psychiatry 1958;21:216-227.
Question 40
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. Which of the four muscles of the rotator cuff provides the most resistance to this patient's direction of instability?
Explanation
indicated. If a patient has excessive glenoid retroversion (not seen in this scenario with 5 degrees of retroversion), a posterior opening-wedge osteotomy is appropriate.
Question 41
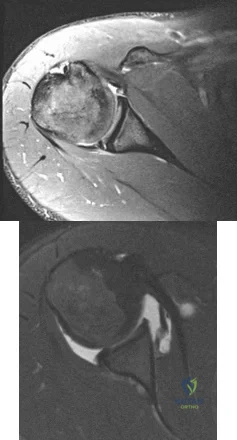
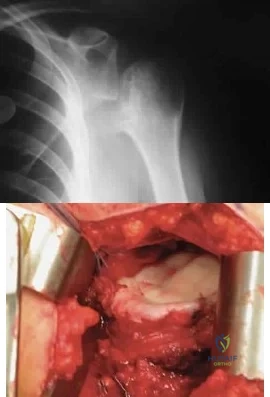
An 11-year-old boy has right shoulder pain and has been unwilling to use the arm after throwing a baseball in a Little League game 3 weeks ago. Examination reveals upper arm and shoulder tenderness with swelling. A radiograph and MRI scan are shown in Figures 27a and 27b. Management should consist of
Explanation
REFERENCES: Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 945-946.
Malawer MM: Tumors of the shoulder girdle: Techniques of resection and description of surgical classification. Orthop Clin North Am 1991;22:7-35.
Question 42
Which of the following physical examination findings is most likely present in the condition producing the MRI findings shown in Figure 92? Review Topic

Explanation
Question 43
An anatomic reduction is obtained at the femoral neck. The most likely reason for development of avascular necrosis (AVN) in this scenario would be
Explanation
A damage-control approach is indicated for this patient. Debridement of the open fracture wound and rapid stabilization without an extensive surgical
approach are indicated. Rapid percutaneous fixation of the femoral neck would compromise long-term outcomes for this displaced fracture because obtaining a quality reduction and fixation construct is critical for the long-term outcome. This patient likely would not tolerate cephalomedullary nailing or open approaches very well at this time.
A vertically oriented (Pauwels 3) femoral neck fracture is more common in younger patients who sustain high-energy injuries. Because of the mechanism of injury, many of these patients have associated injuries. This is a biomechanically challenging fracture because the fracture is subject to shear forces rather than compression, making it inherently unstable. This type of fracture often necessitates different fixation strategies to counter shearing forces, such as use of a transversely oriented (Pauwels) screw to compress the fracture or a fixed-angle device.
The femoral neck fracture should be prioritized in this scenario. This does not necessarily mean that the femoral neck should be repaired first, but the strategy should emphasize optimal fixation of the femoral neck. It has been demonstrated that this is less successful when using a single implant to repair both fractures. It is possible to place femoral neck fixation around an antegrade femoral nail; however, it is much more likely that optimal fixation will be achieved with shaft fixation that does not obstruct placement of fixation for the femoral neck.
AVN is more common among physiologically young patients after femoral neck fractures. The higher energy of injury is a likely contributor. Closed reduction has not been shown to increase the risk for AVN when an anatomic reduction is obtained. A surgical delay of 24 hours does not cause AVN. Patients with associated femoral shaft fractures are not at increased risk for AVN; in fact, some studies have shown a relatively lower rate of AVN when a femoral neck fracture is associated with a femoral shaft fracture.
RECOMMENDED READINGS
Liporace F, Gaines R, Collinge C, Haidukewych GJ. Results of internal fixation of Pauwels type-
3 vertical femoral neck fractures. J Bone Joint Surg Am. 2008 Aug;90(8):1654-9. doi: 10.2106/JBJS.G.01353. PubMed PMID: 18676894. View Abstract at PubMed
Bedi A, Karunakar MA, Caron T, Sanders RW, Haidukewych GJ. Accuracy of reduction of ipsilateral femoral neck and shaft fractures--an analysis of various internal fixation strategies. J Orthop Trauma. 2009 Apr;23(4):249-53. doi: 10.1097/BOT.0b013e3181a03675. PubMed PMID: 19318867. View Abstract at PubMed
Haidukewych GJ, Rothwell WS, Jacofsky DJ, Torchia ME, Berry DJ. Operative treatment of femoral neck fractures in patients between the ages of fifteen and fifty years. J Bone Joint Surg Am. 2004 Aug;86-A(8):1711-6. PubMed PMID: 15292419. View Abstract at PubMed Peljovich AE, Patterson BM. Ipsilateral femoral neck and shaft fractures. J Am Acad Orthop Surg. 1998 Mar-Apr;6(2):106-13. PubMed PMID: 9682073. View Abstract at PubMed
Upadhyay A, Jain P, Mishra P, Maini L, Gautum VK, Dhaon BK. Delayed internal fixation of fractures of the neck of the femur in young adults. A prospective, randomised study comparing closed and open reduction. J Bone Joint Surg Br. 2004 Sep;86(7):1035-40. PubMed PMID: 15446534. View Abstract at PubMed
RESPONSES FOR QUESTIONS 96 THROUGH 99
- Warfarin (Coumadin)
- Dabigatran (Pradaxa)
- Rivaroxaban (Xarelto)
- Apixaban (Eliquis)
Match the appropriate oral anticoagulant listed with the description.
This medication is a vitamin K antagonist and can be reversed.
- Warfarin (Coumadin)
- Dabigatran (Pradaxa)
- Rivaroxaban (Xarelto)
- Apixaban (Eliquis)
Question 44
Figure 35 shows the radiograph of a 35-year-old weightlifter who has had pain with overhead lifts for the past 7 months. Cortisone injections in the acromioclavicular joint provided only temporary relief. A bone scan reveals increased activity of the acromioclavicular joint. Treatment should now consist of
Explanation
REFERENCES: Flatow EL, Cordasco FA, McCluskey GM, Bigliani LU: Arthroscopic resection of the distal clavicle via a superior portal: A critical quantitative radiographic assessment of bone removal. Arthroscopy 1990;6:153-154.
Lyons FR, Rockwood CA: Osteolysis of the clavicle, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 541-546.
Question 45
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Explanation
REFERENCES: Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 46
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be
Explanation
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Martin SD, Warren RF, Martin TL, Kennedy K, O’Brien SJ, Wickiewicz TL: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 47
A 25-year-old man sustains a left brachial plexus injury from a fall while rock climbing. Examination reveals poor intrinsic function of the hand, ptosis, and miosis. He is able to abduct and forward flex his shoulder with full strength. This combination of physical findings is most suggestive of what pattern of nerve injury?
Explanation
A preganglionic lesion occurs proximal to the spinal foramen, whereas a postganglionic lesion occurs distal to the spinal foramen in the root, trunk, division, cord, or branches of the brachial plexus. The Horner sign, which is characterized by miosis, ptosis, anhydrosis, and enophthalmos, results from an injury to the sympathetic ganglion, which lies in close proximity to the T1 root level. The presence of a Horner sign is highly suggestive of a T1 preganglionic injury. Other physical examination indicators of a preganglionic injury include atrophy of the parascapular muscles (injury to the dorsal rami of the cervical spinal nerve roots), winged scapula (injury to the long thoracic nerve) and hemidiaphragmatic paralysis (phrenic nerve injury). The lack of intrinsic hand function in this patient is also suggestive of an injury at the level of C8-T1. Preservation of shoulder abduction and forward flexion would not typically be seen with an injury to the C5-C6 roots or the upper trunk.
Question 48
A 16-year-old boy has had a painful ingrown nail on his great toe for the past 3 months. When initial management consisting of soaking the foot in Epsom salts and trimming the nail failed to provide relief, his family physician recommended 2 weeks of oral antibiotics. His symptoms persist, and he is now seeking a second opinion. A clinical photograph is shown in Figure 18. Management should now consist of
Explanation
REFERENCES: Pettine KA, Cofield RH, Johnson KA, Bussey RM: Ingrown toenail: Results of surgical treatment. Foot Ankle 1988;9:130-134.
Coughlin MJ, Mann RA: Toenail abnormalities, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1033-1070.
Question 49
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. Risk for vascular injury during transtibial drilling for reconstruction of this injury is increased by

Explanation
the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 50
Figures 1 and 2 are the MR arthrogram images of a 20-year-old right-hand dominant collegiate basketball player who sustained an initial shoulder dislocation 1 year ago. In the month prior to presentation, he dislocated his shoulder two more times. Each time it occurred when going up for a rebound and an opponent grabbed the ball from behind him, hyperextending his shoulder. Physical examination demonstrates full range of motion, absence of atrophy, a positive apprehension sign and relocation test, and a positive Kim test. What is the best next step?
Explanation
physical examination and advanced imaging in these patients are crucial in directing appropriate treatment.
Question 51
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show
Explanation
REFERENCES: Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Question 52
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function? Review Topic
Explanation
Question 53
A 26-year-old professional rodeo bull rider sustained a grade III midshaft femoral fracture after being thrown from his bull. He underwent closed interlocking intermedullary nailing with a titanium rod, and his recovery was uneventful. Prior to returning to competition, the patient must
Explanation
least 1 year.
REFERENCES: Brumback RJ, Ellison TS: Intermedullary nailing of femoral stress fractures. J Bone Joint Surg Am 1992;74:106-112.
Bucholz RW, Jones A: Fractures of the shaft of the femur. J Bone Joint Surg Am
1991;73:1561-1566.
Butler MS, Brumback RJ: Interlocking nailing for ipsilateral fractures of the femur, femoral shaft, and distal part of the femur. J Bone Joint Surg Am 1991;73:1492-1502.
Question 54
The wear resistance of ultra-high molecular weight polyethylene can be improved by exposing the polymer to high-energy radiation (eg, gamma or electron beam), followed by a thermal treatment. What is one detrimental side effect of this process?
Explanation
REFERENCES: Collier JP, Currier BH, Kennedy FE, et al: Comparison of cross-linked polyethylene materials for orthopaedic applications. Clin Orthop 2003;414:289-304.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 203-208.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 55
Figures below depict the radiographs obtained from a 60-year-old man with instability and pain 1 year after primary right total knee arthroplasty. He states that he had surgery on two occasions for a tendon rupture that was repaired with sutures but that his knee popped again, and now the leg is unable to hold his weight. On examination, he is in no acute distress. His height is 6'3", and he weighs 240 pounds. He is ambulatory with crutches. Range of motion of the right knee is 50° to 120° actively and 0° to 120° passively. More than 10° of varus/valgus laxity and more than 5 mm of anteroposterior drawer are present. A palpable defect is observed in the tissue just proximal to the patella. The incision is well healed. The erythrocyte sedimentation rate is 46 mm/h (reference range 0 to 20 mm/h) and the C-reactive protein level is 2.04 mg/L (reference range 0.08 to 3.1 mg/L). Aspiration of the right knee reveals hazy yellow fluid with a white blood cell count of 120 and 1% neutrophils. No growth of organisms is seen on routine culture. What is the best next step?

Explanation
This patient has a chronic quadriceps tendon rupture after total knee arthroplasty. Two previous primary repair attempts have failed, which is not surprising based on the poor results of primary repair reported in the literature. The patient also has an unstable knee and will require revision of some or all of the prosthesis to achieve a stable knee. Revision total knee arthroplasty with extensor mechanism allograft allows an allograft reconstruction of the ruptured quadriceps tendon. The other option is to utilize a synthetic mesh extensor mechanism reconstruction. These are likely to have the best result in this situation. Revision total knee arthroplasty with liner change and primary quadriceps repair is not the best form of management, because it involves a third attempt at primary tendon repair, which will likely fail again. Resection knee arthroplasty and arthrodesis with antegrade nail is a possible option but is not the best, because it would likely make driving and other daily activities difficult. Two-stage revision total
knee arthroplasty with extensor mechanism allograft is not the best option because the laboratory results show no signs of infection, so a single-stage procedure is preferred.
Question 56
.The least gliding resistance for a flexor tendon laceration at the thumb palmar-digital crease as shown inFigure 75 can be achieved with
Explanation

Patient age
Displacement of the radius fracture
Displacement of the ulnar styloid fracture
Position of the ulnar styloid after open reduction and internal fixation of the radius
Stability of the distal radioulnar joint after open reduction and internal fixation of the radius

Question 57
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis. J Bone Joint Surg Am 2005;87:725-730.
Question 58
A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management? Review Topic
Explanation
in management should be MRI. If the findings are negative, suspicion of nerve injury should lead to electromyography.
Question 59
Eosinophilic granuloma frequently occurs as a solitary lesion in the tubular long bones. After biopsy, what is the best course of action?
Explanation
REFERENCE: Simon M, Springfield D, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 200.
Question 60
A 58-year-old woman has a fracture through a metacarpal lesion after a motor vehicle accident. She denies any preinjury symptoms and the fracture heals uneventfully. Based on the radiograph and MRI scans shown in Figures 22a through 22c obtained following fracture healing, follow-up management should consist of
Explanation
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 213-228.
Marco RA, Gitelis S, Brebach GT, et al: Cartilage tumors: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:292-304.
Question 61
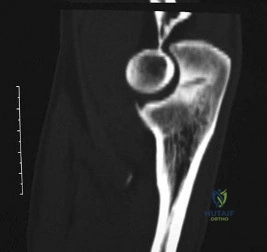
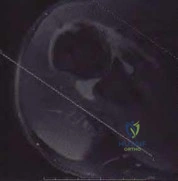
-Radiographs are shown in Figures 89a through 89c. What is the most likely diagnosis?
Explanation
Question 62
Figures 25a and 25b show the radiograph and MRI scan of a 7 1/2-year-old boy who has been limping for 1 year. His pain has worsened over the past 2 weeks, and his parents note swelling over the dorsum of the foot for the past 4 days. Examination reveals no fever, and laboratory studies show a WBC of 6,700/mm 3 , an erythrocyte sedimentation rate of 26 mm/h, and a normal C-reactive protein level. What is the most likely diagnosis?
Explanation
REFERENCES: Wang MN, Chen WM, Lee KS, Chin LS, Lo WH: Tuberculous osteomyelitis in young children. J Pediatr Orthop 1999;19:151-155.
Watts HG, Lifeso RM: Tuberculosis of the bones and joints. J Bone Joint Surg Am 1996;78:288-298.
Question 63
What mechanism is associated with the spontaneous resorption of herniated nucleus pulposus?
Explanation
REFERENCES: Haro H, Kato T, Kamori H, et al: Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res 2002;20:409-415.
Doita M, Kanatani T, Ozaki T, et al: Influence of macrophage infiltration of herniated disc tissue on the production of matrix metalloproteinases leading to disc resorption. Spine
2001;26:1522-1527.
Question 64
Serum phosphate levels are high. Tumoral calcinosis is a heritable condition that is characterized by periarticular metastatic calcification. Most patients are black, and the inheritance is usually autosomal recessive. Metastatic calcifications occur around joints and in the skin, marrow, teeth, and blood vessels. The periarticular masses may grow quite large and are attached to the fascia, but they are extra-articular. The masses may occur at the shoulder, hip, and elbow. Radiographically: The masses are composed of heavy, amorphous calcification in nodules. Laboratory:
Explanation
Question 65
Figure 7 shows the CT scan of a 22-year-old professional baseball pitcher who has had elbow pain for the past 6 months despite rest from throwing. Management should consist of Review Topic
Explanation
Question 66
A patient undergoes a simple excision of a 3-cm superficial mass in the thigh at another institution. The final pathology reveals a leiomyosarcoma, without reference to the margins. What is the recommendation for definitive treatment?
Explanation
a reexcision of the tumor bed is recommended.
REFERENCE: Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 67
A 20-year-old man sustained an isolated displaced type II odontoid fracture in a motor vehicle accident. He is neurologically intact. Treatment consists of placement in halo traction, and the fracture is reduced. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 193.
Kiovikko MP, Kiuru MJ, Koskinen SK, et al: Factors associated with nonunion in conservatively-treated type-II fractures of the odontoid process. J Bone Joint Surg Br 2004;86:1146-1151.
Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, p 1091.
Fiore AJ, Haid RW, Rodts GE, et al: Atlantal lateral mass screws for posterior spinal reconstruction: Technical note and case series. Neurosurg Focus 2002;12:E5.
Question 68
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?
Explanation
REFERENCE: Waters RL, Keenan ME: Surgical treatment of the upper extremity after stroke, in Chapman MW (ed): Operative Orthopedics. Philadelphia, PA, JB Lippincott, 1988, vol 2,
pp 1449-1450.
Question 69
The posterior horn of the medial meniscus receives its primary blood supply from what artery? Review Topic
Explanation
Question 70
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared to a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.

RESPONSES FOR QUESTIONS 58 THROUGH 62
Nerve palsy
Skin necrosis
Flexion instability
Patellar instability
Anterior knee pain
Malalignment
Total knee arthroplasty (TKA) is performed to address each condition shown in Figures 58 through 62b. Which complication is most commonly associated with each image?
Question 71
- A 19-year-old man sustains a complete spinal cord injury at the C7 level as a result of diving into a lake. He has a blood pressure of 90/50 mm Hg, a pulse of 60/min, and respirations of 20/min. These values most likely signify
Explanation
Question 72
What is the preferred treatment of displaced distal clavicle fractures in children less than eight years old?

Explanation
Question 73
A 22-year-old volleyball player reports the insidious onset of superior and posterior shoulder pain. Radiographs are normal. An MRI scan is shown in Figure 25. What is the most specific physical examination finding?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR Jr: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Question 74
Figure 56 shows an arthroscopic view of the long head of the biceps; it has an incompetent biceps sling and is unstable, and an axial glenohumeral MRI scan reveals that it is dislocated medially out of the intertubercular groove. What structure is also most likely injured?
Explanation
REFERENCES: Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Tung GA, Yoo DC, Levine SM, et al: Subscapularis tendon tear: Primary and associated signs on MRI. J Comput Assist Tomogr 2001;25:417-424.
46 • American Academy of Orthopaedic Surgeons
Question 75
A 60-year-old man is evaluated in the ICU after a rollover motor vehicle accident 3 days ago. He has multiple upper and lower extremity trauma and was found unresponsive at the accident scene. Surgery is planned for the extremity trauma once the patient is medically stable. He remains intubated and the cervical spine is immobilized in a semi-rigid collar. Examination reveals mild erythema in the posterior occipital cervical region. Initial AP and lateral radiographs of the cervical spine have not revealed any obvious fracture. What is the most appropriate treatment option at this time? Review Topic
Explanation
Question 76
An elderly patient falls and sustains an extension injury to the neck that results in upper extremity weakness, spared perianal sensation, and lower extremity spasticity. These findings best describe what syndrome?
Explanation
motor function.
REFERENCES: Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Leventhal MR: Fractures, dislocations and fracture-dislocations of spine, in Crenshaw AH (ed): Campbell’s Operative Orthopaedics, ed 8. St. Louis, MO, Mosby, 1992.
Question 77
-What is the most likely mechanism of injury?
Explanation
The MRI scan shows a bone bruise of the lateral femoral condyle and lateral tibial plateau. This injury pattern is commonly associated with anterior cruciate ligament (ACL) rupture and an abnormal pivot shift test result. Treatment of an ACL tear in a high-demand athlete should consist of ligament reconstruction.In this patient, surgery should be delayed until she regains full range of motion to minimize risk for arthrofibrosis after surgery. Recent analysis has shown that the noncontact mechanism is more consistent with anterior translation, affecting both the medial and lateral compartments. The bone bruise in the lateral femoral condyle occurs more anterior than that of the medial femoral condyle, suggesting that internal rotation has occurred. The external rotation recurvatum test assesses for posterolateral corner injury, and a positive quadriceps active test is consistent with posterior cruciate ligament rupture. An abnormal patellar apprehension test result is suggestive of patellar instability. Nonsurgical treatment is unlikely to result in sufficient stability if this patient returns to sports at her preinjury level of activity.Primary ACL repair is associated with high failure rates. Although the precise mechanism of injury varies,injuries can be broadly classified into contact and noncontact injuries. Noncontact injuries occur with the knee in slight flexion, valgus, and internal rotation, and contact injuries typically involve a lateralside impact producing a valgus force to the knee. The valgus component of noncontact injuries has been thought to cause mainly lateral compartment bone bruising. Posterior translation is the most common mechanism of posterior cruciate ligament rupture, and hyperextension and varus is associated with posterolateral corner injury.
Question 78
Which of the following studies has the highest sensitivity and specificity in diagnosis of osteonecrosis of the femoral head?
Explanation
REFERENCES: Steinberg ME: Early diagnosis, evaluation, and staging of osteonecrosis, in Jackson DW (ed): Instructional Course Lectures 43. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 513-518.
Glickstein MF, Burk DL Jr, Schiebler ML, et al: Avascular necrosis versus other diseases of the hip: Sensitivity of MR imaging. Radiology 1988;169:213-215.
Question 79
The AP radiograph of a 5-year-old boy shows a 20-degree left thoracic scoliosis. He was noted by his pediatrician to have asymmetry on a forward bend test. On examination he is neurologically intact except for decreased sensation on the lateral aspect of both flanks and to pinprick in both hands. He has no pain. What is the best initial step in treatment at this time? Review Topic
Explanation
Question 80
A 61-year-old man with a body mass index of 31 had a 6-month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
Explanation
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Nonarthroplasty), level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1,500 mg/day and chondroitin sulfate 800 mg/day as well as arthroscopic debridement and lavage).
Question 81
A 10-year-old girl has been unable to walk for the past 5 days because of bilateral hip pain. Administration of IV morphine has provided some pain relief. She is afebrile. History reveals that she had an upper respiratory tract infection 3 weeks ago that resolved uneventfully. Examination reveals moderate pain with internal rotation and abduction, while log rolling maneuvers do not cause significant pain. An MRI scan shows a small effusion of one hip; however, a bone scan and plain radiographs are normal. Initial laboratory studies showed a markedly elevated WBC count, which subsequently declined to normal levels with IV antibiotics. Current studies show an erythrocyte sedimentation rate (ESR) of 100 mm/h. Aspiration of the hip obtains 3 mL of fluid; Gram stain is negative for bacteria, but a cell count shows a WBC count of 16,500/mm 3 . Streptozyme titer of the peripheral blood is 200 units (normal is less than 100 units). Management should now consist of
Explanation
REFERENCES: De Cunto CL, Giannini EH, Fink CW, et al: Prognosis of children with poststreptococcal reactive arthritis. J Pediatr Infect Dis 1988;7:683-686.
Haueisen DC, Weiner DS, Weiner SD: The characterization of “transient synovitis of the hip” in children. J Pediatr Orthop 1986;6:11-17.
Question 82
Figures 23a and 23b show the MRI scans of a 50-year-old woman who has increasing gait disturbance. She reports three falls in the past week. Examination reveals hyperreflexia, motor weakness in the biceps and triceps, and a positive Hoffman’s sign. What is the most appropriate treatment plan?
Explanation
REFERENCES: Emery SE, Bohlman HH, Bolesta MJ, et al: Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy: Two to seventeen-year follow-up. J Bone Joint Surg Am 1998;80:941-951.
Ferguson RJ, Caplan LR: Cervical spondylotic myelopathy. Neurol Clin 1985;3:373-382.
Herkowitz HN: A comparison of anterior cervical fusion, cervical laminectomy, and cervical laminoplasty for the surgical management of multiple level spondylotic radiculopathy. Spine 1988;13:774-780.
Question 83
A 30-year-old patient underwent open reduction internal fixation of a talar neck fracture 8 weeks ago. His current radiographs demonstrate a subchondral radiolucency of the dome of the talus. What is the next most appropriate course of action?

Explanation
Question 84
Following a partial muscle laceration, keeping the affected extremity immobilized for 2 weeks before starting an exercise program will likely lead to: Review Topic
Explanation
Healing a muscle injury involves two competing processes: regeneration of muscle fibers and formation of granulation tissue. Starting motion too soon after injury may increase the area of fibrous scar, and limit the ability of new muscle fibers to penetrate this area. Prolonged immobilization limits scar production but penetrating muscle fibers will lack appropriate orientation, and the muscle as whole begins to atrophy. Three to 5 days of immobilization has been shown to limit scar tissue production
while the early motion helps generate appropriately organized muscle fibers and maintain strength and range of motion.
Järvinen et al. present a review of muscle injury and healing. They found that immediate mobilization led to a large area of dense scar tissue that regenerating muscle fibers could not adequately penetrate. Prolonged immobilization allowed muscle fibers to regenerate but they lacked appropriate morphology. Following 3-5 days of immobilization they found less scar tissue, better penetration of regenerated muscle fibers, and the regenerated fibers were more well aligned with the uninjured fibers surrounding them.
Menetrey et al. present a mouse model of muscle laceration comparing a short period of immobilization (5 days) to suture repair of the muscle. They found quicker healing and greater strength in the suture repair group. Tetanus strength at one month after injury was (compared to an uninjured control) 81% for sutured muscle, 35% for the early mobilization only group, and 18% for the prolonged immobilization group.
Illustration A is a histology section of lacerated muscle after 7 days of immobilization. The area is infiltrated with granulation tissue and few regenerating myofibers. Illustration B is a histology section of lacerated muscle after 14 days of immobilization. Further infiltration with granulation tissue and mononuclear cells can be seen with regenerating myofibers only at the periphery.
Incorrect answers:
Question 85
During the early swing phase of the normal gait cycle, what lower extremity muscle is primarily contracting?
Explanation
REFERENCES: Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Wootten ME, Kadaba MP, Cochran GV: Dynamic electromyography II: Normal patterns during gait. J Orthop Res 1990;8:259-265.
Question 86
Lateral malleolus fractures can be treated with a variety of techniques, including posterior antiglide plating or lateral neutralization plating. What is an advantage of using lateral neutralization plating instead of posterior antiglide plating?

Explanation
Schaffer et al showed from a biomechanical standpoint that posterior antiglide plating was superior to lateral neutralization plating for distal fibula fracture fixation.
Weber et al reported a (30/70) 43% rate of plate removal secondary to peroneal discomfort. In addition, peroneal tendon lesions were found in 9 of the 30 patients.
Question 87
A 65-year man has right hip pain after a fall. Radiographs reveal a reverse oblique intertrochanteric femoral fracture. Treatment consists of reduction and internal fixation. Which of the following implants is most commonly associated with nonunion and hardware failure?
Explanation
REFERENCES: Haidukewych GJ, Israel TA, Berry DB: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
Baumgaertner MR, Chrostowski JH, Levy RN: Intertrochanteric hip fracture, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1833-1881.
Question 88
A 79-year-old healthy male has 1 year of progressively worse left hip pain. He denies any significant weight loss but does complain of night pain. Radiograph and MRI are shown in Figures A & B. Bone scan and histology is shown in Figures C-E. What is the definitive treatment of this?
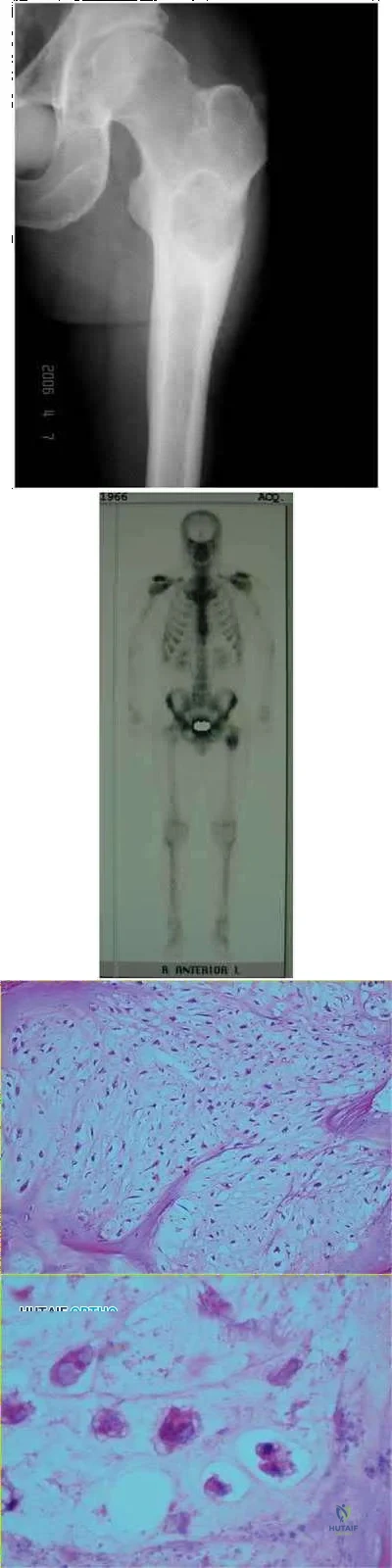
Explanation
Chondrosarcoma tends to occur in an older individuals and the most common sites of origin are the femur, tibia, humerus, ribs, scapula then pelvis.
Chondrosarcomas grow slowly and patients present with dull aching pain.
X-rays typically have a subtle, radiolucent, permeative lesion or may have hazy or speckled calcifications with either a diffuse "salt & pepper" pattern or a more discrete "popcorn" pattern. The MRI defines the amount of marrow and soft-tissue involvment, and typically has high T2 signal intensity. Bone scintigraphy will be positive.
In pathological sections, low-power imaging demonstrates lobulated clusters of chondrocytes, and high-power imaging demonstrates a bland cellular appearance, extensive basophilic cytoplasm, and no mitotic figures (low grade chondrosarcoma).
Question 89
A 25-year-old motorcyclist has a knee dislocation that is reduced by the trauma surgeon in the emergency department. Radiographs show no fracture and a reduced knee joint. What is the most appropriate initial step for evaluation of a potential arterial injury?
Explanation
Question 90
Figure 63 shows the radiographs of a 23-year-old man who sustained a twisting injury at work. Swelling, tenderness, and ecchymosis are noted about the entire midfoot. What associated injury is most likely to be problematic?
Explanation
REFERENCE: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Question 91
A 32-year-old powerlifter who was performing a dead lift 3 days ago noted a sharp pain in the front of his dominant right arm just after beginning to lower the weight. He now reports pain in the anterior aspect of the arm that worsens when he opens a door. Examination reveals moderate ecchymosis and swelling of the forearm and tenderness in the antecubital fossa. The MRI scans are shown in Figures 15a and 15b. If the injury is left unrepaired, the greatest functional deficit will most likely be the loss of
Explanation
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Agins HJ, Chess JL, Hoekstra DV, Teitge RA: Rupture of the distal insertion of the biceps brachii tendon. Clin Orthop 1988;234:34-38.
Question 92
Medial dislocation of the long head of the biceps tendon in the shoulder is most commonly caused by a Review Topic
Explanation
Question 93
During total hip arthroplasty, profuse bleeding is noted following predrilling for placement of an acetabular component screw. The drill most likely penetrated too deep in the
Explanation
REFERENCES: Wasielewski RC, Cooperstein LA, Kruger MP, et al: Acetabular anatomy and the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg Am 1990;72:501-508.
Keating EM, Ritter MA, Faris PM: Structures at risk from medially placed acetabular screws.
J Bone Joint Surg Am 1990;72:509-511.
Question 94
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling’s test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis? Review Topic
Explanation
Question 95
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for
Explanation
REFERENCES: Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249.
Linscheid RL, O’Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452.
O’Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Ross G, McDevitt ER, Chronister R, Ove PN: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
Question 96
03 A 28-year-old man who sustained the injury shown in Figure 31 is hemodynamically unstable. In addition to fluid resuscitation, the next most appropriate step in management should include
Explanation
Cook RE, Keating JF, Gillespie I: The role of angiography in the management of haemorrhage from major fractures of the pelvis. J Bone Joint Surg Br 2002;84:178-182.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp395-405.
back to this question next question
Question 97
Figure 42 shows the sagittal T2-weighted MRI scan of a patient’s right knee. These findings are most commonly seen with a complete tear of the
Explanation
fluid in the soft tissues laterally. Additionally, there is a large bone bruise on the medial
femoral condyle. This combination indicates injury to the posterolateral complex. These injuries often have coexisting anterior and/or posterior cruciate ligament injuries. Failure to recognize the posterolateral corner injury can lead to failure of anterior or posterior cruciate ligament reconstructions.
REFERENCES: LaPrade RF, Gilbert TJ, Bollom TS, et al: The magnetic resonance imaging appearance of individual structures of the posterolateral knee: A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 2000;28:191-199.
Ross G, Chapman AW, Newberg AR, et al: Magnetic resonance imaging for the evaluation of acute posterolateral complex injuries of the knee. Am J Sports Med 1997;25:444-448.
Question 98
A 23-year-old man reports a 6-year history of recurrent instability in the right dominant shoulder. He has not undergone surgery and has essentially stopped all of his sporting activities. On examination, he has instability and apprehension in the midrange of motion (abduction of 45 to 60 degrees with external rotation) and a palpable clunk representing a transient dislocation over the anterior glenoid rim. A three-dimensional CT scan is shown in Figure 31. What is the most appropriate surgical intervention to provide him with reliable stability postoperatively?
Explanation
A bony augmentation procedure such as the Lataijet has been well-described to provide a well functioning and stable shoulder joint. A hemiarthroplasty is not indicated in the absence of arthritis. Subscapularis
advancement will not address the bone loss.
REFERENCES: Hovelius L, Sandstrom B, Sundgren K, et al: One hundred eighteen Bristow-Latarjet repairs for recurrent anterior dislocation of the shoulder prospectively followed for fifteen years: Study I— clinical results. J Shoulder Elbow Surg 2004;13:509-516.
Schroder DT, Provencher MT, Mologne TS, et al: The modified Bristow procedure for anterior shoulder instability: 26-year outcomes in Naval Academy midshipmen. Am J Sports Med 2006;34:778-786.
Itoi E, Lee SB, Berglund LJ, et al: The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: A cadaveric study. J Bone Joint Surg Am 2000;82:35-46.
Question 99
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?
Explanation
REFERENCES: Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.
Question 100
A 30-year-old man is brought to the emergency department after a motor vehicle accident. He has a closed midshaft femoral fracture and an intra-abdominal injury. He is currently in the operating room and the exploration of his abdomen has been completed. His initial blood pressure was 70/30 mm Hg and is now 90/50 mm Hg after 4 liters of fluid and 2 units of blood. His initial serum lactate was 3.0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C). What is the most appropriate management for the femoral shaft fracture at this point?
Explanation
REFERENCES: Shafi S, Elliot AC, Gentilello L: Is hypothermia simply a marker of shock and injury severity or an independent risk factor for mortality in trauma patients? Analysis of a large national trauma registry. J Trauma 2005;59:1081-1085.
Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-454.
