Orthopedic Surgery Board Review MCQs: Spine, Trauma & Shoulder | Part 201

Key Takeaway
This page offers Part 201 of a comprehensive AAOS/OITE Orthopedic Surgery Board Review series. Authored by Dr. Mohammed Hutaif, it features 100 high-yield, verified MCQs directly modeled on the OITE and AAOS board exam formats. Designed for orthopedic residents and surgeons, this interactive quiz aids in critical board certification preparation.
About This Board Review Set
This is Part 201 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 201
This module focuses heavily on: Dislocation, Foot, Fracture, Hip, Nerve, Shoulder, Spine, Trauma.
Sample Questions from This Set
Sample Question 1: A 20-year-old college athlete is seen for follow-up after sustaining an injury at football practice 2 days ago. He reports that he tackled a player and felt neck pain and numbness in both arms. The numbness resolved within seconds, but his ...
Sample Question 2: The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the...
Sample Question 3: Which of the following medications may have a negative effect on bone healing following fracture?...
Sample Question 4: belowshowtheradiographsobtainedfromanyear-old-womanwhohashadchroniclefthippainforseveralyears.Shenowusesawalkerandawheelchairforambulation.Sheismedicallyhealthy. Whatisthemostappropriatesurgicalintervention?...
Sample Question 5: A 17-year-old high school football player sustains a traumatic anterior shoulder dislocation, resulting in a small bony Bankart lesion and small Hill-Sachs lesion. The patient undergoes an arthroscopic Bankart repair with incorporation of t...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 20-year-old college athlete is seen for follow-up after sustaining an injury at football practice 2 days ago. He reports that he tackled a player and felt neck pain and numbness in both arms. The numbness resolved within seconds, but his neck remains painful and stiff. He denies any history of neck pain or injury. Examination reveals limited neck motion. The neurologic examination and radiographs are normal. MRI scans of the cervical spine are shown in Figure 34. During counseling, the patient, his family, and his coach should be informed that he has an acute cervical disk herniation and cannot play
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, Burak C, Hosea T, Connolly PJ: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Vaccaro AR, Watkins B, Albert TJ, Pfaff WL, Klein GR, Silber JS: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-705.
Question 2
The anatomy of the sciatic nerve as it exits the pelvis is best described as exiting through the
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 347.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-34, 4-36.
Hollingshead WH: Anatomy for Surgeons: The Back and Limbs, ed 2. Hagerstown, MD, Harper & Row, 1969, pp 607-609.
Question 3
Which of the following medications may have a negative effect on bone healing following fracture?
Explanation
REFERENCES: Gerstenfeld LC, Thiede M, Seibert K, et al: Differential inhibition of fracture healing by non-selective and cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs. J Orthop Res 2003;21:670-675.
Harder AT, An YH: The mechanisms of the inhibitory effects of nonsteroidal anti-inflammatory drugs on bone healing: A concise review. J Clin Pharmacol 2003;43:807-815.
Question 4
below show the radiographs obtained from an year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 5
A 17-year-old high school football player sustains a traumatic anterior shoulder dislocation, resulting in a small bony Bankart lesion and small Hill-Sachs lesion. The patient undergoes an arthroscopic Bankart repair with incorporation of the bone fragment and returns to play football the following year. He has a recurrent dislocation at football practice but decides to finish the football season before considering additional treatment. He sustains nine additional dislocations, with the last dislocation occurring while sleeping. The patient has eroded one-third of the inferior glenoid surface area. What is the most appropriate surgical treatment?
Explanation
more likely to have pain after surgery. Age and activity level are lesser influences on satisfaction.
Question 6
A 51-year-old woman with shoulder pain responds transiently to a subacromial injection and physical therapy exercise program. When her symptoms recur, an arthroscopic subacromial decompression is recommended. During the surgery, a partial-thickness articular-sided supraspinatus tear is noted. The supraspinatus footprint is exposed for 3 mm from the articular margin. The remaining intra-articular structures are normal. Inspection from the bursal surface reveals the tendon to be intact. What is the most appropriate course of management? Review Topic
Explanation
Question 7
A 45-year-old IV drug abuser has sternoclavicular (SC) joint pain for the past 2 weeks. He is afebrile and physical exam findings include point tenderness and swelling. He most likely has septic arthritis of the sternoclavicular joint. If so, what is the most likely infecting organism?

Explanation
According to the reference by Ross et al, Staphylococcus aureus accounts for 49% of infections. SC joint arthritis accounts for 1% of septic arthritis in the general population but 17% in the IV drug abuse population. Symptoms include spontaneous swelling with the appearance of joint subluxation and localized pain. These patients are not uncommonly afebrile.
Question 8
Optimal management of the injury shown in Figure 31 should include which of the following?
Explanation
REFERENCES: Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Sanders RW, Clare MP: Fractures of the calcaneus, in Bucholz RW, Heckman JD, Court-Brown C (eds): Rockwood and Green’s Fractures in Adults, ed 6. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, vol 2, pp 2293-2336.
Question 9
below show the radiographs, and the CT obtained from a year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?
Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 10
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include
Explanation
REFERENCES: Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Fisher SE, Shelbourne KD: Arthroscopic treatment of symptomatic extension block complicating anterior cruciate ligament reconstruction. Am J Sports Med 1993;4:558-564.
Question 11
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear?
Explanation
REFERENCES: Farng E, Sherman O: Meniscal repair devices: A clinical and biomechanical literature review. Arthroscopy 2004;20:273-286.
Jones HP, Lemos MJ, Wilk RM, et al: Two-year follow-up of meniscal repair using a bioabsorbable arrow. Arthroscopy 2002;18:64-69.
Question 12
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?
Explanation
REFERENCES: Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Wu CD, Huang SC, Liu TK: Sleeve fracture of the patella in children: A report of five cases. Am J Sports Med 1991;19:525-528.
Question 13
Which of the following complications occurs more commonly after antegrade femoral nail insertion when compared with retrograde insertion?
Explanation
REFERENCES: Morgan E, Ostrum RF, DiCicco J, McElroy J, Poka A: Effects of retrograde femoral intramedullary nailing on the patellofemoral articulation. J Orthop Trauma 1999;13:13-16.
Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R: Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma 2001;15:161-169.
Ostrum RF, Agarwal A, Lakatos R, Poka A: Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma 2000;14:496-501.
Tornetta P III, Tiburzi D: Antegrade or retrograde reamed femoral nailing: A prospective, randomized trial. J Bone Joint Surg Br 2000;82:652-654.
Question 14
A 47-year-old woman underwent a bunionectomy and hallux valgus correction a few years ago. She now has the complication shown in Figures 38a and 38b. She has no pain with motion of the metatarsophalangeal or interphalangeal joints. What is the best reconstructive option in this setting?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 27-32.
Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 345-351.
Question 15
In the management of an open tibia fracture, what factor is considered most important in preventing deep infection?
Explanation
REFERENCES: Clifford P: Open fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 617-638.
Lee J: Efficacy of cultures in the management of open fractures. Clin Orthop 1997;339:71-75.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 16
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
REFERENCES: Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 2002;23:896-901.
Question 17
A 6-month-old child is seen in the emergency department with a spiral fracture of the tibia. The parents are vague about the etiology of the injury. There is no family history of a bone disease. In addition to casting of the fracture, initial management should include Review Topic
Explanation
(SBQ13PE.60) If a child develops dynamic supination after treatment of idiopathic clubfoot with Ponseti casting, at what age would it be appropriate to consider transfer of the tibialis anterior tendon to the lateral dorsum of the foot? Review Topic
In the first six months of life, immediately following failed cast treatment
12 months
4 years
12 years
15 years
Tibialis tendon transfer to the dorsum of the foot should be performed to address dynamic supination when the lateral cuneiform has ossified. This is typically after at least 2 years of age and usually not before age 3.
Question 18
Figure 31 shows the radiograph of an 8-year-old boy who has a swollen forearm after falling out of a tree. Examination reveals that all three nerves are functionally intact, and there is no evidence of circulatory embarrassment. Management should consist of
Explanation
REFERENCES: Gibson WK, Timperlake RW: Operative treatment of a type IV Monteggia fracture-dislocation in a child. J Bone Joint Surg Br 1992;74:780-781.
Stanley EA, DeLaGarza JF: Part IV: Monteggia fracture. Dislocations in children, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 576-577.
Question 19
What mechanism is associated with the spontaneous resorption of herniated nucleus pulposus?
Explanation
REFERENCES: Haro H, Kato T, Kamori H, et al: Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res 2002;20:409-415.
Doita M, Kanatani T, Ozaki T, et al: Influence of macrophage infiltration of herniated disc tissue on the production of matrix metalloproteinases leading to disc resorption. Spine
2001;26:1522-1527.
Question 20
Glenohumeral disarticulation often leads to which of the following changes?
Explanation
Question 21
An otherwise healthy adolescent girl was treated for left slipped capital femoral epiphysis. The contralateral hip had not slipped, but was stabilized prophylactically with a single cannulated screw. The implants were removed after 1 year. The pelvic radiographs (Figures 215a and 215b) and the MRI scans of the hip that had not originally slipped (Figures 215c through 215e) were obtained 10 months after screw removal (22 months after the original fixation). Which findings are shown in these studies?
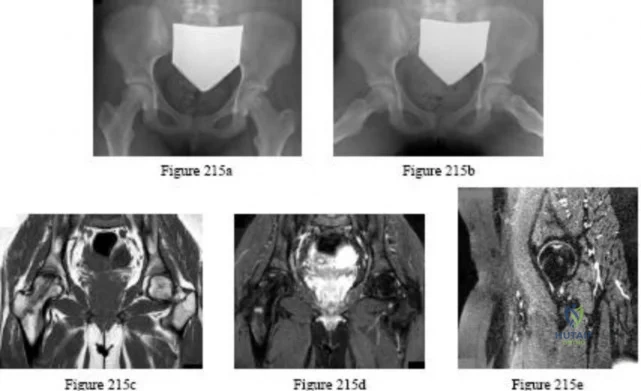
Explanation
Question 22
A 20-year-old elite college football player has ecchymosis, swelling, and pain on the lateral side of his foot after a game. Radiographs are shown in Figures 31a through 31c. Management should consist of
Explanation
REFERENCES: Glasgow MT, Naranja RJ Jr, Glasgow SG, et al: Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: The Jones fracture. Foot Ankle Int 1996;17:449-457.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-252.
Question 23
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement? Review Topic

Explanation
Question 24
Compared with retention of the native patella in primary total knee arthroplasty, routine patellar resurfacing is associated with
Explanation
Despite concerns regarding fracture, osteonecrosis, and patellar clunk, the routine retention of the native patella during primary total knee replacement is associated with a 20% to 30% increased revision risk in
large joint registries. In addition, the retention of the native patella results in a 5.7% revision surgery rate in patients with anterior knee pain.
Question 25
Figures 2a and 2b are this patient’s proton density fat-saturated MR images. His tibial tubercle-trochlear groove (TT-TG) distance is 12 mm, and he has normal limb-alignment film findings. Treatment at this stage should include
Explanation
This patient’s examination and history indicate recurrent patellar dislocations. Radiographs show an osseous or osteochondral loose fragment. There is no evidence of an obvious nondisplaced fracture or physeal changes. In the setting of suspected patella dislocation or subluxation with loose fragment seen on radiograph, an MRI is indicated. Lateral release alone is seldom indicated in a knee that is normal before injury. The examination and MRI do not indicate a need for medial collateral ligament repair. Treatment should consist of arthroscopy or arthrotomy and attempted internal fixation of this fragment. If fixation is not possible, the loose body can be removed. Normal TT-TG values, an increased lateral patellar glide, and a history of recurrent patellar dislocations after trauma suggest MPFL incompetence and the need for reconstruction.
Question 26
Which of the following best describes heat stroke?
Explanation
[41 degrees C]), central nervous system dysfunction, and cessation of sweating with hot, dry skin. It is a medical emergency that results from failure of the thermoregulatory mechanisms of the body. It has a high death rate and requires rapid reduction in body core temperature. Heat syncope is characterized by a transient loss of consciousness with peripheral vasodilation and decreased cardiac output with normal body temperature. Heat cramps involve painful contractions of large muscle groups because of decreased hydration and a decrease of serum sodium and chloride. Heat exhaustion is distinguished by a core temperature of less than
Question 27
A 10-month-old boy has an untreated developmental hip dislocation.
Explanation
Early radiographic findings of avascular necrosis (AVN) of the hip include sclerosis and a subchondral lucency. A common presentation of Legg-Calve-Perthes disease (idiopathic pediatric hip AVN) is intermittent pain in the thigh, groin, or knee with an examination localizing to the hip; a Trendelenburg gait or sign; and painful, restricted passive hip range of motion. AVN also may be observed in association with a slipped capital femoral epiphysis (SCFE). AVN risk is highest in the setting of an unstable SCFE (10%-60%); risk is 0% to 1.4% when the SCFE is stable. A multicenter review of the modified Dunn procedure for treatment of unstable SCFE noted an AVN rate of 26%.
The most common deformity associated with SCFE is proximal femoral varus, flexion, and external rotation leading to an abnormal femoral head-neck junction offset. This causes a loss of passive hip flexion and internal rotation and the phenomenon of obligate external
rotation with flexion. The residual deformity frequently results in femoroacetabular impingement. Labral tears also are associated with cam impingement secondary to underlying osseous abnormalities including abnormal femoral head-neck junction offset.
Endocrinopathies potentially are associated with SCFE because of hormone-related physeal changes and subsequent mechanical insufficiency of the proximal femoral physis. With renal osteodystrophy, the physeal widening results from secondary hyperparathyroidism and progressive proximal femoral deformity may develop. Optimal medical management of hyperparathyroidism is essential. Surgical stabilization via in situ fixation of the proximal femur is indicated when SCFE is diagnosed.
The proximal femoral epiphysis secondary ossification center commonly appears between the ages of 4 and 7 months. In the setting of developmental hip dislocation, the appearance of the secondary ossification center is commonly delayed. After closed or open reduction of developmental dysplasia of the hip, failure of the femoral head ossific nucleus to appear within 12 months following the reduction is a sign of proximal femoral growth disturbance and AVN.

Question 28
The posterior cord of the brachial plexus terminates into what two main branches?
Explanation
REFERENCE: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 228-236.
Question 29
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
REFERENCES: Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294.
Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Hawkins RJ, Mohtadi NG: Controversy in anterior shoulder instability. Clin Orthop 1991;272:152-161.
Question 30
Medial dislocation of the long head of the biceps tendon in the shoulder is most commonly caused by a Review Topic
Explanation
Question 31
A 52-year-old man who dislocated his dominant shoulder has it reduced in the emergency department and he is placed in a sling. At his 5-day followup evaluation, he reports that this is his first shoulder dislocation and that the pain is mostly gone but he notes difficulty using his arm overhead and away from his body. Examination reveals minimal pain with passive range of motion, a positive apprehension and relocation test, and 3/5 strength with the empty can test and external rotation at the side compared with 5/5 with those tests on the contralateral side. Cutaneous sensation over the lateral aspect of the shoulder is intact. Radiographs show the glenohumeral joint is reduced with no fractures or degenerative changes. What is the next step in management? Review Topic
Explanation
cuff tears following dislocation in young individuals warrants early surgical intervention. Delay of surgical repair for large, full-thickness tears may lead to irreversible changes, including atrophy and retraction of the tendon. As a result, clinical outcomes may be compromised. CT will demonstrate bony changes, but it is not as effective as MRI for soft-tissue pathology. While in the short term a sling for comfort might be helpful, 6 weeks of immobilization is unnecessary because recurrent instability is rarely an issue. Physical therapy can be beneficial but could potentially delay identification of an acute rotator cuff tear. In the event the MRI does not reveal a large, full-thickness rotator cuff tear, physical therapy would be an appropriate next step. There is no indication for urgent shoulder arthroscopy.
Question 32
A 5-month-old girl with arthrogryposis has a limb-length discrepancy. Examination and radiographs reveal unilateral hip dislocation. Management should consist of
Explanation
REFERENCES: Staheli LT, Chew DE, Elliot JS, Mosca VS: Management of hip dislocations in children with arthrogryposis. J Pediatr Orthop 1987;7:681-685.
Szoke G, Staheli LT, Jaffe K, Hall JG: Medial-approach open reduction of hip dislocation in amyoplasia-type arthrogryposis. J Pediatr Orthop 1996;16:127-130.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996.
Question 33
An 18-year-old man sustained a traumatic laceration of the common peroneal nerve when glass fell on the outer part of his leg 1 year ago. He has used a molded foot and ankle orthosis for the past 10 months, but would now like surgical intervention. Electromyography shows no function in the anterior or lateral compartments. He has 5/5 muscle strength of the superficial and deep posterior compartments. What is the most appropriate treatment?
Explanation
hallucis longus tendon transfer would not take the deforming force and make it a corrective force.
Question 34
Compared to similar patients who do not donate autologous blood, patients with normal baseline hemoglobin who donate autologous blood prior to undergoing primary total hip arthroplasty are likely to
Explanation
REFERENCES: Billote D, Glisson SN, Green D, Wixson RL: A prospective, randomized study of preoperative autologous donation for hip replacement surgery. J Bone Joint Surg Am 2002;84:1299-1304.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 47-53.
Question 35
Figures 31a and 31b are the radiographs of a 5-year-old boy with an elbow injury.
Explanation
Figure 26 shows lucent areas of both femoral condyles. This may represent a variation of ossification, in which case this boy’s knee pain is coincidental. Another possibility is atypical osteochondritis dissecans. An MRI will distinguish between the 2 entities and will guide treatment.
Figures 27a and 27b show healing rib and distal tibia fractures. These fractures likely are attributable to child abuse. A plain radiographic skeletal survey is sufficient for orthopaedic needs.
A triplane fracture of the distal tibia is revealed in Figure 28. A CT scan will quantify displacement and identify fracture fragments for planning of screw trajectories if open reduction and internal fixation is indicated (displacement > 2 mm).
In Figure 29, the linear lucency of the capitellum indicates an early osteochondritis dissecans. An MRI will allow staging of the lesion.
Figure 30 shows that the left radius and ulna do not align with the humerus; this is the likely result of a transphyseal fracture of the distal humerus. An arthrogram will outline the unossified distal humerus and allow for reduction. For an unstable neonate, this likely can be performed in the NICU.
Figures 31a and 31b reveal a widely displaced lateral condyle fracture for which open reduction and internal fixation is required. No advanced imaging is necessary.

Question 36
Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis?
Explanation
REFERENCES: Kondrashov DG, Hannibal M, Hsu KY, et al: Interspinous process decompression with the X-STOP device for lumbar spinal stenosis: A 4-year follow-up study.
J Spinal Disord Tech 2006;19:323-327.
Siddiqui M, Smith FW, Wardlaw D: One-year results of X Stop interspinous implant for the treatment of lumbar spinal stenosis. Spine 2007;32:1345-1348.
Question 37
A 19-year-old college cross-country runner is amenorrheic and has recurrent stress fractures. Long-term management should consist of
Explanation
REFERENCES: Nattiv A, Armsey TD Jr: Stress injury to bone in the female athlete. Clin Sports Med 1997;16:197-224.
Drinkwater BL: Exercise and bones: Lessons learned from female athletes. Am J Sports Med 1996;24:S33-S35.
Question 38
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain.What is the most likely cause of this patient's pain?
Explanation
Question 39
A 70-year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single-compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease of the knee.
Question 40
Figures below show the radiographs obtained from a 68-year old man with progressively worsening right side hip pain over the last 8 months. He is 6 feet tall, with a BMI of 51 kg/m2 and reports that his index total hip arthroplasty was performed 8 years ago. The preoperative work-up includes negative infectious laboratory results. What is the most appropriate surgical plan for revision of the femoral component in this patient?
Explanation
Submit Answer
The patient’s radiographs demonstrate varus femoral remodeling around a broken cylindrical, distally fixed femoral stem. Proximal femoral remodeling around loose or fractured stems occurs in 21% to 42% of femoral revisions, based on the definitions outlined by Foran and associates. In definition 1, varus femoral remodeling occurs when the template falls within 2 mm of the endosteal cortex of the metaphysis on templating with a diaphyseal engaging stem. In definition 2, varus femoral remodeling = when the template crosses the lateral femoral cortex proximally. Based on the templating or drawing a line from the isthmus proximally along the lateral cortex, implantation of a straight stem would perforate the cortex proximally, indicating varus femoral remodeling. An extended trochanteric osteotomy would aid in the removal of the well-fixed distal segment and enable the safe insertion of the new femoral component. The approach is not the concern in this case, because extended trochanteric osteotomies have been described from the posterior and direct lateral approaches with excellent outcomes and union rates. The key is that the extended osteotomy is necessary and not a trochanteric slide or standard (shorter or incomplete trochanteric) osteotomy. These types would not provide access to the well-fixed distal stem, nor would they afford a straight tube in which to insert a new femoral component.
Question 41
A 45-year-old man sustains an acute closed posterolateral elbow dislocation. The elbow is reduced, and examination reveals that the elbow dislocates posteriorly at 35 degrees with the forearm placed in supination. What is the best course of action?
Explanation
REFERENCE: O’Driscoll SW, Morrey BF, Korinek S, et al: Elbow subluxation and dislocation: A spectrum of instability. Clin Orthop 1992;280:186-197.
Question 42
Six months later, the patient’s fracture has healed and a CT scan to further evaluate the physis is performed (Video 85). Based on these findings, how should you advise the family?
Explanation
The hypertrophic zone is the weakest biomechanical zone of the physis and is most likely to fracture. The deep peroneal nerve supplies motor innervation to the ankle and toe
dorsiflexors (anterior compartment) and the first web space, which, in this history, have deficits. The superficial peroneal nerve supplies sensation to the dorsum of the foot and motor to the lateral compartment peroneal musculature (ankle evertors), which also has deficits. The injury must involve both peroneal branches (the common peroneal nerve). Because sensation to the sole of the foot and toe/ankle plantar flexion is intact, the tibial nerve is intact.
Because the nerve was visualized intact, a neuropraxia is the most likely type of nerve injury. This should recover in time and does not necessitate urgent exploration. In pediatric patients, an advancing Tinel sign and partial nerve recovery by 3 months is expected and can be followed clinically. If there is no sign of nerve recovery, an electromyogram should be ordered with consideration for nerve exploration if there is no sign of reinnervation. There is no sign of compartment syndrome because the patient has an unchanged neurologic deficit, is comfortable, and has no pain with passive range of motion.
These injuries are associated with a very high rate of growth arrest (up to 80% in some studies). The CT scan shows an asymmetric growth arrest, which suggests angulation through the distal femur.
Question 43
Figures 100a and 100b are the radiographs of a 90-year-old woman who is seen in the emergency department after a fall from a height. She has right hip and thigh pain and is unable to bear weight. Based on this patient’s history and imaging, what is the best next step?
Explanation
Periprosthetic fractures are the third-most-common (behind loosening and infection) reason for revision surgery after total hip arthroplasty (THA). Late periprosthetic fracture risk is 0.4% to 1.1% after primary THA and 2.1% to 4% after revision THA. Risk factors for periprosthetic fracture include patient age older than 70 years, decreasing bone mass, and loosening of implants and osteolysis. Risk for concomitant infection in the presence of a periprosthetic fracture is 11%, according to Chevillotte and associates. Obtaining presurgical aspiration or tissue for culture intrasurgically is recommended if concomitant infection is suspected.

CLINICAL SITUATION FOR QUESTIONS 101 THROUGH 104
Figures 101a and 101b are the right hip radiographs of a 26-year-old active man who has had pain in his right hip for 4 months. His pain is worse with prolonged periods in a seated position. He has no pain at rest and denies pain in other joints or systemic illness. Examination reveals passive range of motion of full extension, 80 degrees of flexion, internal rotation in flexion of 0 degrees, and external rotation in flexion of 30 degrees. Forced flexion, internal rotation, and adduction are very painful. A flexion, abduction, and external rotation test result is negative.
Question 44
Which of the following types of iliac osteotomy provides the greatest potential for increased coverage?
Explanation
REFERENCES: Millis MB, Poss R, Murphy SB: Osteotomies of the hip in the prevention and treatment of osteoarthritis, in Eilert RE (ed): Instructional Course Lectures XLI. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1992, pp 145-154.
Weinstein SL: Developmental hip dysplasia and dislocation, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 903-950.
Question 45
A 27-year-old man sustains a displaced femoral neck fracture and undergoes urgent open reduction internal fixation. What is the most prevalent complication after this injury?

Explanation
Haidukewych et al followed treatment of femoral neck fractures in young patients. They found almost 10% of displaced fractures were associated with the development of nonunion, where as 27% were associated with the development of osteonecrosis. Their results were influenced by fracture displacement and the quality of reduction. Varus malreduction most closely correlates with failure of fixation after reduction and cannulated screw fixation.
Swiontkowski reviews both the treatment and post operative complications in intracapsular hip fractures. In this Current Concept Review, the rate of AVN was discussed as being related to the pre-operative degree of displacement seen on radiographs.
Incorrect Responses:
Question 46
What radiographic measurement is best used to assess the adequacy of deformity correction for the patient shown in Figure 22?
Explanation
REFERENCES: Carroll K, Coleman S, Stevens PM: Coxa vara: Surgical outcomes of valgus osteotomies. J Pediatr Orthop 1997;17:220-224.
Cordes S, Dickens DR, Cole WG: Correction of coxa vara in childhood: The use of Pauwels’ Y-shaped osteotomy. J Bone Joint Surg Br 1991;73:3-6.
Question 47
When conducted at near physiologic strain rates, tensile studies of the inferior glenohumeral ligament (IGHL) have shown that the
Explanation
REFERENCES: Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Ticker JB, Bigliani LU, Soslowsky LJ, Pawluk RJ, Flatow EL, Mow VC: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Question 48
What form of fixation is associated with the highest incidence of osseous union when using segmental allograft reconstruction following tumor resection?
Explanation
REFERENCE: Vander Griend RA: The effect of internal fixation on the healing of large allografts. J Bone Joint Surg Am 1994;76:657-663.
Question 49
What is the most common cause for late revision (> 2 years post op) total knee arthroplasty?
Explanation
REFERENCE: Sharkey PF, Hozack WJ, Rothman RH, et al: Insall Award paper: Why are total knee arthroplasties failing today? Clin Orthop Relat Res 2002;404:7-13.
Question 50
Following surgery for an ankle fracture, which of the following is considered the most important factor in achieving a satisfactory outcome? Review Topic
Explanation
Question 51
A 47-year-old obese man with a body mass index of 42 comes in with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of his UKA secondary to poor patient selection. This young, heavy man likely loosened his component secondary to the ongoing varus alignment of the knee and his elevated weight. Despite this likely scenario, the next step is to determine if an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order an ESR and CRP to determine if aspiration is warranted. If laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.

CLINICAL SITUATION FOR QUESTIONS 69 THROUGH 72
Figures 69a through 69c are the radiograph and MR images of a 37-year-old woman who has had a 2-month history of left hip pain.
Question 52
Figures 37a and 37b show radiographs of a 24-year-old man who has a humeral bone lesion that was found during a screening chest radiograph. He denies any symptoms despite leading a very active lifestyle. What is the most likely diagnosis?
Explanation
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 53
The clinical factors shown to most significantly predict the long-term outcome of Perthes disease of the hip include which of the following? Review Topic
Explanation
(SBQ13PE.87) A 4-week-old child is suspected to have classic arthrogryposis, also known as amyoplasia. Clinical examination and hip ultrasound reveal a unilateral, non-reducible, hip dislocation. What do you recommend to reduce the hip? Review Topic
Pavlik harness application
Semi-rigid abduction brace application
Skeletal traction
Early closed reduction and spica casting
Delayed open reduction with or without pelvic and femoral osteotomy
Delayed open reduction with or without pelvic and femoral osteotomy is recommended in the management of unilateral hip deformities associated with amyoplassia. This procedure should be performed at 6-9 months of age. In order to proceed with reduction, there must be a reasonable arc of flexion/extension and active movement of the lower limbs.
Amyoplasia is the most common recognizable form of arthrogryposis. It most commonly occurs as a sporadic symmetric contracture syndrome that is characterized by symmetrical limb involvement, normal to above-average intelligence, and often a midline facial hemangioma. Approximately 80% of children with amyoplasia will have involvement of the hip ranging from soft tissue contractures to unilateral or bilateral hip dislocations.
Bevan et al. reviewed arthrogryposis. They state that open hip reduction is recommended for the management of unilateral dislocation. There is more controversy with regard to the treatment of bilateral hip dislocations. Open reduction can be performed by a medial or anterolateral approach, with or without pelvic and
femoral osteotomy. This procedure is generally delayed for 6-9 months to facilitate the procedure.
Bernstein et al. also reviewed arthrogryposis. They state that the term 'arthrogryposis' encompasses a broad spectrum of diseases, all with the common phenotype of multiple congenital contractures.
Illustration A shows the characteristic features of an infant with severe arthrogryposis. Note the internal rotation of the shoulders, elbow and knee hyperextension, flexed and ulnarly deviated wrists, flexed finger, external rotation of hips and bilateral clubfeet.
Incorrect answers:
Question 54
A 51-year-old male 2-pack per day smoker presents with a hyperkeratotic light brown plaque on the dorsum of his left ring finger that has been present for 7 years. It measures 14 mm by 13 mm. Initially, it responded to topical wart treatments, but has failed to do so recently so he sought evaluation by a dermatologist who biopsied the lesion. The results revealed squamous cell carcinoma (SCC) in situ, and he was referred for further surgical management. He has no other skin lesions, no history of SCC and no axillary lymphadenopathy. What is the next step in management?
Explanation
SCC in situ is a low-grade malignancy that typically presents as painless lesions on areas of high sun exposure such as the dorsum of the hand and fingers. The recommended treatment for lesions smaller than 100 mm is wide excision with 4 mm margins to a depth 1 layer below the tumor, along with any adjacent area of induration. Sentinel lymph node biopsy is typically not indicated in the setting of a low-grade tumor such as this one and in the absence of axillary lymphadenopathy.
Question 55
What is the primary benefit of using rhBMP-2 instead of autogenous bone graft inside an anterior spinal fusion cage?
Explanation
REFERENCE: Burkus JK, Gornet MF, Dickman CA, et al: Anterior lumbar interbody fusion using rhBMP-2 with tapered interbody cages. J Spinal Disord Tech 2002;15:337-349.
Question 56
A healthy, active collegiate soccer player returns to your office approximately 10 months after returning to full play and 18 months after undergoing ACL reconstruction with bone-patellar tendon-bone (BTB) autograft. The patient reports landing awkwardly after a jumping for a ball and felt his knee give way. He presents with pain, worse with weight bearing. On physical exam, there is a mild effusion and a grade 2B Lachman. Radiographs are shown in Figure A. What is the likely underlying cause of his current diagnosis? Review Topic

Explanation
Ideal tunnel placement on the femoral side should be at the approximately 2 o'clock (for a left knee) or 10 o'clock (for a right knee) position on the lateral wall, which facilitates a more horizontal, anatomic graft. On the tibial side, the tunnel trajectory in the coronal plane should be about 60-75 degrees from the horizontal and the tunnel entrance should be approximately 10-11mm from the anterior border of the PCL.
Noyes et al. emphasize the importance of anatomic reconstruction. They recommended against using a transtibial tunnel to make the femoral tunnel because it will result in a vertical orientation. The authors summarized and recommended the use of individual drilling of each tunnel, and using a anteromedial portal to obtain the ideal femoral tunnel.
Driscoll et al. compared the rotational properties of a BTB graft placed centrally in the tibial footprint in both groups, but on the femoral side, placed in the anteromedial aspect versus central portion of the ACL femoral origin. They noted a significantly stronger resistance to rotational failure when placed centrally. Thus, noting the importance of placing the graft anatomically, within the central areas of both the tibial footprint and femoral origin.
Figure A exhibits malpositioned tunnels, both of which are too vertical. Illustration A exhibits well-placed tunnels, with the horizontality exhibited on the femoral side and approximately 75 degrees from the horizontal on the tibial side.
Incorrect answers:
Question 57
A 69-year-old patient with diabetes has had acute-onset back pain and difficulty with ambulation for several hours. Evaluation reveals a temperature of 38.3°C, a white blood cell (WBC) count of 14000/µL (reference range [rr], 4500-11000/µL), C-reactive protein (CRP) level of 120 mg/L (rr, 0.08-3.1 mg/L), erythrocyte sedimentation rate of 130 mm/h (rr, 0-20 mm/h), normal rectal examination findings, and normal sensation to light touch. Motor function testing of the lower extremities reveals 3/5 ankle dorsiflexion and 4/5 plantar flexion strength bilaterally. An MR image reveals a large epidural abscess from L1-5. What is the most appropriate treatment at this time?
Explanation
Epidural abscess is a serious and potentially disastrous condition. Although medical management is effective in some situations, surgical decompression is considered urgent with the presence of a neurological deficit. Medical management can be considered in the case of a neurologically intact patient, particularly when the microorganism has been identified. If medical management is chosen, careful observation and serial examination for neurologic deterioration is required. Surgical decompression is indicated if a patient's neurologic status worsens or if medical management failure is noted. Additionally, diabetes, a CRP level higher than 115 mg/L, WBC higher than 12500/µL , and bacteremia have proven predictive of medical treatment failure. This patient would be a better candidate for urgent surgical decompression and subsequent IV antibiotics than for medical management.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778.View Abstract at PubMed
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 58
A 30-year-old man who sustained a tibial fracture with a peroneal nerve palsy 2 years ago now has a drop foot and weak eversion of the foot. He reports success with stretching exercises, but he catches his toes when his foot tires. Examination reveals that the foot is plantigrade and supple. What is the next most appropriate step in management?
Explanation
REFERENCES: Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Santi MD, Botte MJ: Nerve injury and repair in the foot and ankle. Foot Ankle Int
1996;17:425-439.
Question 59
A 12-year-old male sustains a ulnar fracture with an associated posterior-lateral radial head dislocation. After undergoing closed reduction, the radiocapitellar joint is noted to remain non-concentric. What is the most likely finding?

Explanation
Question 60
A 36-year-old woman reports vague right shoulder pain. She denies any previous shoulder problems or any recent trauma. MRI scans are shown in Figures 81a and 81b. Weakness of which of the following is the most likely finding in her physical examination? Review Topic
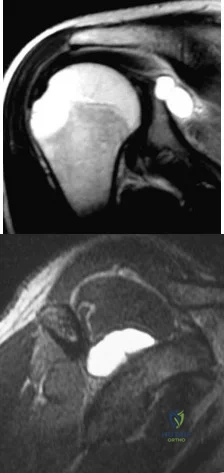
Explanation
Question 61
A 23-year-old soccer player sustains a grade III complete posterior cruciate ligament (PCL) tear after colliding with another player. In reconstructing the PCL, it is optimal to reconstruct the
Explanation
REFERENCES: Harner CD, Xerogeanes JW, Livesay GA, et al: The human posterior cruciate ligament complex: An interdisciplinary study. Ligament morphology and biomechanical evaluation. Am J Sports Med 1995;23:736-745.
Burns WC II, Draganich LF, Pyevich M, Reider B: The effect of femoral tunnel position and graft tensioning technique on posterior laxity of the posterior cruciate ligament-reconstructed knee. Am J Sports Med 1995;23:424-430.
Question 62
Figures 21a and 21b show a transverse MRI scan at L4/5 and a lateral radiograph of a 75-year-old man with a 2-year history of worsening low back and bilateral leg pain that occurs with ambulation beyond approximately a half a block. Management consisting of physical therapy, anti-inflammatory medications, and muscle relaxants has failed to successfully resolve his symptoms. He has minimal medical comorbidities. What is the best treatment approach for this patient? Review Topic

Explanation
Question 63
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.
Question 64
A 17-year-old presents with persistent left knee pain after a twisting injury during a soccer match 24 hours ago. On physical exam he has a mild effusion. He has tenderness to palpation on the medial joint line. Lachman test, anterior drawer test and posterior drawer test are attempted but limited secondary to pain. Dial test reveals a side-to-side external rotation difference of roughly 5 degrees. His MRI images are seen in Figures A-D. These findings would be most consistent with: Review Topic

Explanation
Many provocative tests have been described to aid in the diagnosis of meniscus tears.
The Apley test is performed with the patient prone, by axially loading the tibiofemoral joint at 90° of knee flexion. Pain with compression and external rotation (medial meniscus) or internal rotation (lateral meniscus) is considered positive.
The Ege's test is performed by having the patient squat with their knees maximally externally rotated or internally rotated. The test is positive when pain and/or a click is felt by the patient.
The McMurray test is performed by passively moving the knee from flexion to extension while externally or internally rotating the leg. A palpable click at the joint line with external rotation (medial meniscus) or internal rotation (lateral meniscus) is considered positive.
The Thessaly test is performed by supporting the patient as they internally or externally rotate their knee and body while keeping the foot planted, with the knee in 5° of flexion and then 20° of flexion. The test is positive when joint line pain and/or sense of locking/catching is experienced by the patient.
Ryzewicz et al. performed a systematic review of prospective cohort studies comparing magnetic resonance imaging (MRI) and clinical examination to arthroscopy in the diagnosis of meniscus tears. The Apley test, Ege's test, McMurray test and Thessaly test at 5° were shown have high specificity but low sensitivity. Joint line tenderness has a higher sensitivity, but lower specificity. The Thessaly test at 20° demonstrated the highest sensitivity and specificity, although there was only one available study evaluating this test.
Abdon et al. performed a prospective study looking at 68 clinical parameters to
determine which combinations of symptoms and signs indicated the presence of a meniscus tear. They found that joint-line tenderness and mechanical locking were predictive of a meniscus tear, while the McMurray sign did not prove valuable. Pain at rest, sick leave and medial patellar tenderness all negated the presence of a meniscus tear. The clinical accuracy in diagnosing meniscal tears was 61% in this study.
Figures A and B are T1 sagittal MR images demonstrating an intact anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), respectively. Figures C and D are T2 coronal and sagittal MR images showing a complex tear of the posterior horn of the medial meniscus. Illustration A demonstrates the Ege's test. Illustration B shows the Thessaly test at 5° of flexion.
Incorrect
Question 65
04 Which of the following laboratory studies is predictive of wound healing prior to performing a lower extremity amputation?
Explanation
(eliminates false positive predictions with using area under the Doppler waveform). Pressures less than 20 mm Hg are predictive of poor healing. Miller 505-6
back to this question next question
Question 66
A 7-year-old girl has pain and a mass in the left scapula. A MRI scan and biopsy specimen are shown in Figures 30a and 30b. After staging studies, initial management should consist of
Explanation
REFERENCES: Grier HE: The Ewing family of tumors: Ewing’s sarcoma and primitive neuroectodermal tumors. Pediatr Clin North Am 1997;44:991-1004.
Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 67
A 16-year-old high school football player has diffuse pain with attempted digital flexion after injuring the ring finger of the dominant hand 1 week ago. Examination reveals that he is unable to flex the distal interphalangeal joint. Management should consist of
Explanation
REFERENCES: Strickland JW: Flexor tendons: Acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, 1999,
pp 1851-1897.
Leddy JP: Avulsions of the flexor digitorum profundus. Hand Clin 1985;1:77-83.
Question 68
Figures 18a and 18b show the radiographs of a 13-year-old baseball player who sustained a patellar dislocation with an associated lateral femoral condyle fracture. What ligament is attached to this fragment?
Explanation
REFERENCES: Jobe CM, Wright M: Anatomy of the knee, in Fu FH, Harner CD, Vince KG (eds): Knee Surgery. Baltimore, MD, Williams & Wilkins, 1994, pp 1-54.
Moore KL, Dalley AF: Lower limb, in Moore KL, Dalley AF (eds): Clinically Oriented Anatomy, ed 4. Philadelphia, PA, Lippincott, Williams & Wilkins, 1999, pp 503-664.
Question 69
A 7-year-old boy has a swollen and deformed right arm after falling off his bicycle. Radiographs reveal a completely displaced posterolateral supracondylar humeral fracture. Examination reveals a warm, pink hand and forearm but absent pulses. What is the next most appropriate step in management?
Explanation
REFERENCES: Shaw BA: The role of angiography in assessing vascular injuries associated with supracondylar humerus fractures remains controversial. J Pediatr Orthop 1998;18:273.
Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Schoenecker PL, Delgado E, Rotman M, et al: Pulseless arm in association with totally displaced supracondylar fracture. J Orthop Trauma 1996;10:410-415.
Question 70
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
Explanation
ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Paletta GA Jr, Laskins RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
Question 71
A 13-year-old girl has had pain in her ankle and difficulty with sporting activities for the past 6 months. Nonsteroidal anti-inflammatory drugs and use of a short leg cast have provided minimal relief. A radiograph and MRI scan are shown in Figures 43a and 43b. What is the next most appropriate step in treatment?
Explanation
REFERENCES: McCormack TJ, Olney B, Asher M: Talocalcaneal coalition resection: A 10-year follow-up. J Pediatr Orthop 1997;17:13-15.
Thometz J: Tarsal coalition. Foot Ankle Clin 2000;5:103-118.
Question 72
Figure 1 is the anteroposterior radiograph of a 20-year-old dancer who fell during his routine and injured his right foot. What is the most appropriate treatment?
Explanation
Question 73
A 30-year-old woman who runs approximately 30 miles a week has had right hip and groin pain for the past 3 weeks. Examination reveals an antalgic gait, limited motion of the right hip, and pain, especially with internal and external rotation. Plain radiographs are normal, and an MRI scan is shown in Figure 21. Management should consist of
Explanation
REFERENCES: Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 239-253.
Fullerton LR Jr, Snowdy HA: Femoral neck stress fractures. Am J Sports Med
1988;16:365-377.
Question 74
A 17-year-old girl with Charcot-Marie-Tooth disease reports the development of progressive instability when walking on uneven surfaces. Her involved heel is positioned in varus when viewed from behind. Examination reveals that she walks on the outer border of the involved foot. She has full passive motion of the ankle and hindfoot joints. She is able to dorsiflex the ankle against resistance. The heel varus fully corrects with the Coleman block test. Standing radiographs reveal a cavus deformity with valgus of the forefoot. She would like to avoid using an ankle-foot orthosis. What is the best surgical option?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Upate: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 135-144.
Dehne R: Congenital and acquired neurologic disorders, in Coughlan MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 525-557.
Question 75
Which study is most useful for diagnosis of exertional compartment syndrome?
Explanation
The most sensitive study in the diagnosis of exertional compartment syndrome is intracompartmental pressures taken at rest (compared to pressures taken immediately after exercise). MRI often can reveal nonspecific muscle edema in exertional compartment syndrome, but this is usually not diagnostic. Arterial Doppler studies are usually unremarkable unless they are taken after exercise, in which case these findings may be abnormal.

CLINICAL SITUATION FOR QUESTIONS 48 THROUGH 50
Figures 48a through 48f reveal the radiographs and MR images of a 30-year-old man who has a 1-year history of atraumatic medial-sided left knee pain refractory to nonsurgical measures.
Question 76
What factor is associated with a high risk of developing pseudotumors after metal-on-metal hip resurfacing?
Explanation
Question 77
A 19-year-old man has had back pain with activity, especially running in soccer and baseball, for the past 4 months. He denies any history of trauma. Examination reveals no motor weakness or sensory changes in the lower extremities. Range of motion shows increased pain with extension and mild limitation with flexion. A sitting straight leg raising test is limited at approximately 60 degrees bilaterally by back and buttocks pain. Plain radiographs are normal. MRI scans are shown in Figures 13a through 13e. What is the most likely diagnosis?
Explanation
REFERENCES: Wiltse LL, Rothman SL: Spondylolisthesis: Classification, diagnosis and natural history. Sem Spine Surg 1993;5:264-280.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 78
A patient reports pain in the hip with functional positioning. With the patient supine, pain in which of the following positions would be typical for femoral acetabular impingement? Review Topic
Explanation
(SBQ13PE.10) Which statement is true regarding discoid menisci? Review Topic
Most commonly involves the medial meniscus
Bilateral in >75% of cases
Asymptomatic discoid meniscus should undergo saucerization
Radiographs will commonly show a hyperplastic lateral intercondylar spine
Radiographs will commonly show squaring of affected condyle with cupping of tibial plateau
Radiographs of knees with discoid menisci will commonly show squaring of affected condyle (lateral>medial) with cupping of tibial plateau.
Discoid meniscus refers to the abnormal development of a hypertrophic and discoid shaped meniscus. It occurs in 3-5% of the population and it is considered the most common cause of a symptomatic clicking or clunking in a childs knee. The lateral meniscus is most commonly affected and it will occur bilaterally in 25% of affected
people. The Watanabe Classification describes the 3 types of discoid menisci. Type 1
= Incomplete, Type 2 = Complete, Type 3 = Wrisberg (lack of posterior meniscotibial attachment to tibia)
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Lee et al. retrospectively reviewed 36 patients aged less than 15 years who underwent arthroscopic procedures for torn discoid menisci. The mean patient age at the time of surgery was 9.5 years. They showed that partial meniscectomy yielded better radiologic results than subtotal/total meniscectomy for torn discoid menisci in this population.
Illustration A shows the 3 classifications of discoid menisus as originally described by Watanabe. Type 4 is a ring type discoid that was not originally described by Watanabe in his 1978 paper. Illustration B shows an AP and lateral radiograph of a discoid meniscus knee. Note squaring of affected lateral condyle in the presence of a lateral discoid meniscus. Illustration C shows 4 consecutive sagittal MRI images with meniscus continuity. It is important to note that the diagnosis of discoid menisci can be made when 3 or more 5mm sagittal images show meniscal continuity.
Incorrect Answers:
Question 79
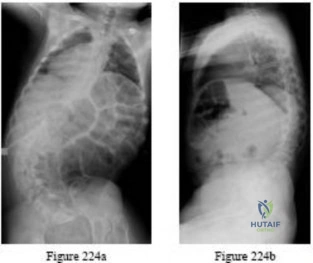
Figures 92a through 92c are the radiographs of a 34-year-old man with low-back pain and an inability to walk upright. What is the appropriate surgical treatment? A B C

Explanation
This patient has a marked fixed sagittal imbalance and a mild coronal imbalance. His fused sacroiliac joints indicate ankylosing spondylitis. Sufficient correction likely can be achieved with a pedicle subtraction osteotomy in the midlumbar spine. Smith-Petersen osteotomies necessitate flexibility of the anterior column, which is not associated with this diagnosis. Also, osteoclasis can result in vascular injuries. Vertebral column resection should not be needed in this case.
RECOMMENDED READINGS
Patel NM, Jenis LG. Inflammatory arthritis of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:339-349.
Kim KT, Suk KS, Cho YJ, Hong GP, Park BJ. Clinical outcome results of pedicle subtraction osteotomy in ankylosing spondylitis with kyphotic deformity. Spine (Phila Pa 1976). 2002 Mar 15;27(6):612-8. PubMed PMID: 11884909. View Abstract at PubMed
Question 80
Which of the following orthotic features best reduces pain in patients with hallux rigidus?
Explanation
REFERENCES: Beskin JL: Hallux rigidus. Foot Ankle Clin 1999;4:335-353.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 17-25.
Question 81
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. Which of the following represents an acceptable arrangement?
Explanation
Question 82
A well-healed bulk proximal tibia osteoarticular allograft is removed 10 years after implantation due to arthropathy. Histologic examination of the host allograft junction site will most likely reveal
Explanation
Question 83
A 40-year-old woman is admitted to the hospital with a history of new-onset right lower extremity weakness resulting in frequent falls. She reports that a few weeks prior to the onset of the lower extremity symptoms, she experienced an episode of acute back pain, which has since resolved. Examination reveals 1-2/5 strength in the right hip flexors, abductors, and quadriceps. There is 0-1/5 strength

Explanation
(SBQ12SP.39) Which of the following is associated with increased risk of surgical site infection following lumbar spinal decompression? Review Topic
Use of intra-wound vancomycin powder
Hair removal by clipping at the time of surgery
Use of morphine nerve paste applied to the dura after spinal decompression
Skin preparation with an alcohol-based prep solution rather than povidone iodine
Failure to use chlorhexidine gluconate wash the night prior to surgery
The use of morphine nerve paste applied to the dura after decompressive spine surgery has been used in an effort to mitigate postoperative pain but has been associated with epidemic levels of surgical site infection.
Surgical site infection risk is modulated by a myriad of factors, both host factors and perioperative factors. Perioperative strategies to reduce infection that have been shown to be effective include: 1) hair removal by clipping (not shaving) at the time of surgery, 2) use of an alcohol based skin preparation agent, 3) use of perioperative prophylactic antibiotics, 4) limiting operating room traffic from OR personnel.
Kramer et al. did a retrospective analysis of 148 patients who underwent laminectomy in order to identify risk factors for infection in the context of a sudden increase in infections. Regression analysis showed that use of morphine paste resulted in an 18-fold increase in the risk of surgical site infection. 17 of 148 had developed infection during the epidemic period, compared to 15/995. Cultures were positive in 10 of 16 cases; 7 of these involved skin flora. Histological exam showed foreign body reaction.
Devin et al. did a multi-center analysis of patients undergoing spine surgery at seven spine centers to determine whether there was a difference in infection risk based on whether or not intra-wound vancomycin was used. They analyzed 2056 patients, of whom 47% had vancomycin used in their wounds. The risk of surgical site infection was higher in those patients that did not have vancomycin (relative risk 2.5).
Incorrect answers:
Question 84
Reconstruction of the injured structure is performed. After surgery, the patient initially notes limitation in motion, and later develops recurrent instability of the knee. Which factor most likely contributed to the development of instability?
Explanation
The anteromedial bundle originates on the anterior and proximal aspect of the lateral femoral condyle and inserts on the anteromedial aspect of the anterior cruciate ligament (ACL) footprint on the proximal tibia. The posterolateral bundle originates posterior and distal to 63 the anteromedial bundle and inserts on the posterolateral aspect of the tibial footprint. The fibers are parallel when the knee is in an extended position. As the knee moves into flexion,
the fibers of the anteromedial bundle rotate externally with respect to the posterolateral bundle. The anteromedial bundle is tensioned in both flexion and extension. The posteromedial bundle is tensioned in extension, but relaxes as the knee moves into flexion.
The lateral meniscus is more commonly injured with an acute injury to the ACL. The medial meniscus is injured more commonly when the ACL is chronically unstable.
The ACL is an intra-articular and intrasynovial structure. It is innervated by posterior articular branches from the tibial nerve. Innervation of the ACL involves several types of mechanoreceptors (Ruffini, Pacini, Golgi tendon, and free-nerve endings) that may contribute to proprioceptive function of the knee and modulation of quadriceps function.
Injury to the ACL is predominantly associated with instability to anterior translation of the tibia in extension. The ACL plays a secondary role to limit internal rotation of the tibia, and a loss of ACL stability is confirmed by the reduction of the tibia from a position of anterior translation and internal rotation (pivot shift). The radiographs demonstrate anterior placement of the femoral tunnel. The convex shape of the lateral femoral condyle can make it more difficult to visualize the anatomic femoral origin of the ACL. Failure to identify the
anatomic footprint can result in anterior placement of the femoral tunnel. Anterior ACL graft placement can result in its impingement against the posterior cruciate ligament and early limitation of knee flexion. Over time, impingement on the graft may result in stretching of the graft and recurrent knee instability symptoms.
RECOMMENDED READINGS
Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. Epub 2005 Oct 19. Review. PubMed PMID: 16235056. View Abstract at PubMed
Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Oct;14(10):982-92. Epub 2006 Aug 5. Review. PubMed PMID: 16897068. View Abstract at PubMed
Question 85
Figure 1 shows the radiograph of a 68-year-old man who underwent revision hip arthroplasty with impaction grafting of the femur and cementing of a tapered component into the graft 2 years ago. The patient remains symptom-free. Which of the following best describes the most likely histologic appearance of the proximal femur if a biopsy was performed?
Explanation
REFERENCES: Nelissen RG, Bauer TW, Weidenhielm LR, LeGolvan DP, Mikhail WE: Revision hip arthroplasty with the use of cement and impaction grafting: Histological analysis of four cases. J Bone Joint Surg Am 1995;77:412-422.
Gie GA, Linder L, Ling RS, Simon JP, Slooff TJ, Timperley AJ: Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br 1993;75:14-21.
Question 86
Which of the following statements about hoarseness due to vocal cord paralysis after anterior cervical diskectomy and fusion is most accurate?
Explanation
REFERENCES: Beutler WJ, Sweeney CA, Connolly PJ: Recurrent laryngeal nerve injury with anterior cervical spine surgery risk with laterality of surgical approach. Spine 2001;26:1337-1342.
Kilburg C, Sullivan HG, Mathiason MA: Effect of approach side during anterior cervical discectomy and fusion on the incidence of recurrent laryngeal nerve injury. J Neurosurg Spine 2006;4:273-277.
Question 87
What is the most common fracture associated with a lateral subtalar dislocation?

Explanation
Post-reduction x-rays need to be scrutinized carefully for fractures of the tarsal bones as this is the most common injury associated with subtalar dislocations. Occult fractures of the lateral process of the talus are also associated with these injuries.
The referenced study by Wagner et al noted radiographic subtalar DJD in 2/3 of their patients, but noted no correlation between radiographic and clinical outcomes. The referenced study by Bibbo et al noted an 88% incidence of other concurrent injuries and an 89% rate of radiographic DJD at 5 year follow-up. The referenced article by Saltzman et al is a review of hindfoot dislocations.
Question 88
Pacinian corpuscles are lamellated nerve endings that are responsible for providing the perception of
Explanation
REFERENCE: Sunderland SS: Nerves and Nerve Injuries, ed 2. New York, NY, Churchill Livingstone, 1978, pp 343-347.
Question 89
Which of the following definitions best describes Batson’s vertebral vein system?
Explanation
REFERENCES: Batson OV: Function of vertebral veins and their role in spread of metastases. Ann Surg 1940;112:138-149.
Coman DR, de Long RP: Role of vertebral venous system in metastasis of cancer to spinal column: Experiments with tumor-cell suspensions in rats and rabbits. Cancer 1951;4:610-618.
Question 90
Free flap coverage for severe trauma to the upper extremity has the fewest complications when performed within what time period after injury?
Explanation
REFERENCES: Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
Manske PR (ed): Hand Surgery Update. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 31-37.
Question 91
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?
Explanation
REFERENCES: Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214.
McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Ouzounian TJ: Metatarsophalangeal arthrodesis for salvage of failed hallux valgus surgery. Foot Ankle Clin 1997;2:741-752.
Question 92
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?

Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the inability to gain purchase for extraction.
Question 93
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain? Review Topic

Explanation
Question 94
A 24-year-old collegiate pitcher has had increasing pain over his medial elbow for 3 months. He has point tenderness over his medial epicondyle and reproduction of his symptoms with a valgus stress test. What phase of the throwing cycle most likely will reproduce his symptoms? Review Topic
Explanation
Question 95
Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
Explanation
A. Inability to flex the distal interphalangeal joint of the index finger
B. Positive Froment’s sign
C. Weakness with wrist extension
D. Decreased capillary refill
Question 96
A 75-year-old woman who sustained a fall now reports neck pain and upper extremity weakness. Examination reveals 4 of 5 strength in the upper extremities and 5 of 5 strength in the lower extremities. Radiographs show multilevel degenerative disk disease. An MRI scan is shown in Figure 96. Her clinical presentation is most compatible with which of the following? Review Topic

Explanation
Question 97
Figures 9a through 9c are the preoperative radiographs and a T2-weighted MR image of a patient treated with surgery for spondylolisthesis and neuroforaminal stenosis. Figure 9d is the postsurgical radiograph. Interbody fusion offers which advantage over posterolateral fusion (PLF)? A B C D
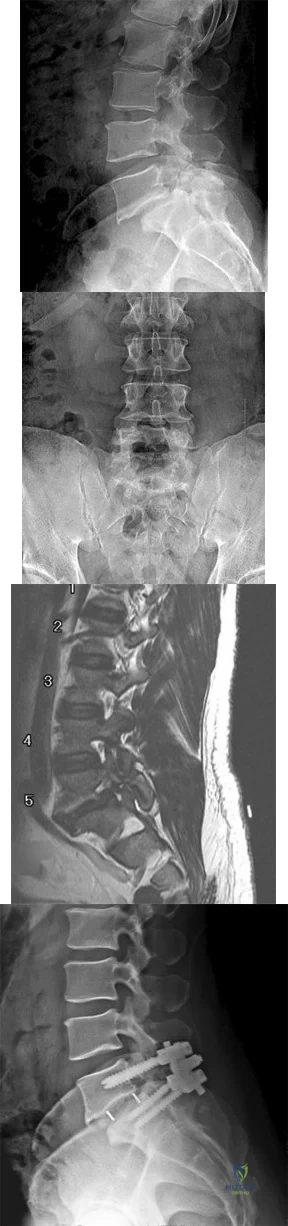
Explanation
Interbody fusion, when compared to PLF, is a predictor of more substantial blood loss. Multilevel posterior lumbar interbody fusion (PLIF) is an independent predictor of blood loss for posterior spine fusion. Some retrospective studies suggest that fusion rates are higher for transforaminal lumbar interbody fusion (TLIF) than PLF, but this finding has not been borne out in prospective studies. The main advantage of TLIF in the context of this question is restoration of neuroforaminal height, and many surgeons will consider TLIF or PLIF for that reason. The parasagittal MR image seen in Figure 9c shows neuroforaminal narrowing. The pre- and postsurgical radiographs show a difference in neuroforaminal height.
RECOMMENDED READINGS
DiPaola CP, Molinari RW. Posterior lumbar interbody fusion. J Am Acad Orthop Surg. 2008 Mar;16(3):130-9. Review. PubMed PMID: 18316711. View Abstract at PubMed
Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. View Abstract at PubMed
McAfee PC, DeVine JG, Chaput CD, Prybis BG, Fedder IL, Cunningham BW, Farrell DJ, Hess SJ, Vigna FE. The indications for interbody fusion cages in the treatment of spondylolisthesis: analysis of 120 cases. Spine (Phila Pa 1976). 2005 Mar 15;30(6 Suppl):S60-5. PubMed PMID: 15767888. View Abstract at PubMed
RESPONSES FOR QUESTIONS 10 THROUGH 14
Postoperative deep surgical site infection
Proximal junctional kyphosis
Pedicle screw cut-out
Pseudarthrosis
Sagittal imbalance
Please match the scenario described below with the most likely complication listed above.
Question 98
An otherwise healthy 13-year-old boy sustains the fracture shown in Figure 40 while throwing a fastball. Management should consist of
Explanation
REFERENCES: Ogawa K, Yoshida A: Throwing fracture of the humeral shaft: An analysis of 90 patients. Am J Sports Med 1998;26:242-246.
Kaplan H, Kiral A, Kuskucu M, et al: Report of eight cases of humeral fracture following the throwing of hand grenades. Arch Orthop Trauma Surg 1998;117:50-52.
Question 99
Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?
Explanation
REFERENCES: Gramstad GD, Galatz LM: Management of elbow osteoarthritis. J Bone Joint Surg Am 2006;88:421-430.
Steinmann SP, King GJ, Savoie FH III, et al: Arthroscopic treatment of the arthritic elbow.
J Bone Joint Surg Am 2005;87:2114-2121.
Question 100
A 68-year-old woman had advanced right knee arthritis and total knee replacement was planned. She learned she had primary biliary cirrhosis at age 41 and now has advancing liver failure. Preoperative coagulation tests show a baseline International Normalized Ratio (INR) of 1.36. Appropriate methods to prevent thromboembolic disease as recommended by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty , include
Explanation
