Orthopedic Board Review MCQs: Knee, Foot, Ankle & Arthroplasty | Part 21
Key Takeaway
This page offers Part 21 of a comprehensive Orthopedic Surgery Board Review MCQ set for orthopedic residents and surgeons. It features 100 high-yield, verified multiple-choice questions on Ankle, Arthroplasty, Foot, and Knee, designed to mirror OITE and AAOS exam formats. Utilize study or exam modes to excel in your board certification preparation.
About This Board Review Set
This is Part 21 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 21
This module focuses heavily on: Ankle, Arthroplasty, Foot, Knee.
Sample Questions from This Set
Sample Question 1: A 55-year-old woman is referred for evaluation of a painful knee replacement. She underwent total kneearthroplasty (TKA) more than 1 year ago without perioperative complications but has had consistent pain since the surgery. The patient’s ...
Sample Question 2: Which of the following antibiotics is contraindicated in children?...
Sample Question 3: A newborn has been referred for evaluation of a deformed foot. Prenatal and birth history are unremarkable. Examination reveals a rocker bottom appearance to the foot, and a longitudinal arch cannot be created. A palpable lump is appreciate...
Sample Question 4: Which of the following surgical techniques is associated with an increased incidence of patellar complications after total knee arthroplasty?...
Sample Question 5: A 40-year-old man has a painless mass around his left ankle. He notes minimal growth over the past year. An MRI scan is shown in Figure 73a, and biopsy specimens are shown in Figures 73b and 73c. What is the most likely diagnosis?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 55-year-old woman is referred for evaluation of a painful knee replacement. She underwent total knee arthroplasty (TKA) more than 1 year ago without perioperative complications but has had consistent pain since the surgery. The patient’s preoperative radiographs and postoperative radiographs are shown in Figures below. Examination reveals medial laxity during valgus stress testing and range of motion of 0° to 70°. Her erythrocyte sedimentation rate and C-reactive protein level are normal. What is the best next step?
Explanation
The radiographs show substantial valgus malalignment of the femoral component, with lateral mechanical axis deviation. Clinically, by examination she displays instability and stiffness as a result. Revision knee replacement is appropriate and should consist of total revision to stemmed femoral and tibial components with a varus-valgus constrained insert, given the likely attenuation of the medial collateral ligament. Open debridement with ligament balancing and polyethylene exchange do not address the underlying cause and are inappropriate. Distal femoral osteotomy is not useful in the setting of previous total knee replacement.
Nonsurgical treatment with an unloader brace would be ineffective in correcting the alignment.
Question 2
Which of the following antibiotics is contraindicated in children?
Explanation
REFERENCE: Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 3
A newborn has been referred for evaluation of a deformed foot. Prenatal and birth history are unremarkable. Examination reveals a rocker bottom appearance to the foot, and a longitudinal arch cannot be created. A palpable lump is appreciated on the plantar medial surface. What is the best course of action?
Explanation
REFERENCES: Napiontek M: Congenital vertical talus: A retrospective and critical review of 32 feet operated on by peritalar reduction. J Pediatr Orthop 1995;4:179-187.
Oppenheim W, Smith C, Christie W: Congenital vertical talus. Foot Ankle 1985;5:198-204.
Question 4
Which of the following surgical techniques is associated with an increased incidence of patellar complications after total knee arthroplasty?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337.
Barrack RL, et al: Resurfacing of the patella in total knee arthroplasty: A prospective, randomized, double-blind study. J Bone Joint Surg Am 1997;79:1121-1131.
Question 5
A 40-year-old man has a painless mass around his left ankle. He notes minimal growth over the past year. An MRI scan is shown in Figure 73a, and biopsy specimens are shown in Figures 73b and 73c. What is the most likely diagnosis?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 757.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 227.
Question 6
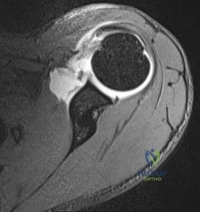
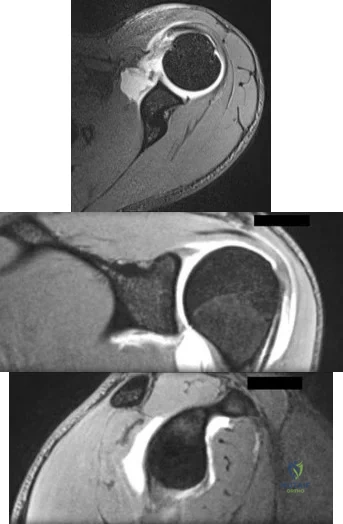
A 73-year-old man who underwent repair of the left rotator cuff 6 years ago reports good pain relief but notes residual weakness of the left shoulder, especially with overhead tasks. He denies having pain at night and has minimal discomfort with activities of daily living but is dissatisfied with his shoulder strength. Radiographs show an acromiohumeral interval of 2 mm. Appropriate management should consist of
Explanation
REFERENCES: Bigliani LU, Cordasco FA, McIlveen SJ, Musso ES: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
DeOrio JK, Cofield RH: Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am 1984;66:563-567.
Gerber C, Vinh TS, Hertel R, Hess CW: Latissimus dorsi transfer for the treatment of massive tears of the rotator cuff: A preliminary report. Clin Orthop 1988;232:51-61.
Question 7
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered? Review Topic

Explanation
Question 8
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior knee pain, a trace effusion, a 2+ posterior drawer, a grade 1A Lachman, no valgus laxity, and negative dial tests at 30° and 90°. What is the best treatment strategy at this time?
Explanation
A. Biceps tenotomy
B. Loose body removal
C. Latissimus dorsi transfer
D. Reverse total shoulder arthroplasty
Question 9
The modified Judet approach to the posterior scapula exploits the internervous interval between what two muscles?

Explanation
The reference by Obremskey et al argues the approach "combines several important goals including: 1) exposure of all bony elements of the scapula which have adequate bone stock for internal fixation; 2) minimal trauma to the rotator cuff musculature; and 3) protection of the major neurologic structures (suprascapular nerve superiorly and axillary nerve laterally)." They believe "the main advantage of the exposure is limiting muscular dissection, which can potentially improve rehabilitation and limit morbidity of the operation."
Question 10
A unilateral "piano key" sign, indicates
Explanation
The piano key sign is a demonstration of instability at the DRUJ, typically seen after healing from a distal radius fracture with an associated ulnar styloid fracture (as in this case) or other wrist injury. The hand is pushed down against a table top, and the distal radius translates dorsally (with the distal ulna apparently moving volarly). In fact, the distal radius is the mobile segment, while the distal ulna is fixed in space. Treatment involves repair or reconstruction of the foveal insertion of the triangular fibrocartilage complex (TFCC) and distal radioulnar ligaments. This type of instability is also common in malunions of the distal radius or distal one-third of the radial shaft (Galeazzi-type fractures). In malunions, DRUJ instability can be treated with a corrective osteotomy of the distal radius to restore the anatomic relationship between the distal ulna and the distal radius at the DRUJ. Radiocarpal and midcarpal instability do not involve the DRUJ. Disruption of the interosseous membrane (in isolation, with intact distal radioulnar ligaments and an intact TFCC) does not lead to translational instability of the DRUJ. Although hypermobility syndrome may lead to ligamentous laxity, it does not lead to unilateral DRUJ instability.
Question 11
Arthrodesis
Explanation
with OA or RA. Certainly in patients who have glenoid bone deficiency precluding placement of a glenoid component…" as is apparent in this radiograph.
Question 12
Which of the following vertebrae has the smallest pedicle isthmic width in a nondeformity patient?
Explanation
REFERENCE: Ofiram E, Polly DW, Gilbert TJ Jr, et al: Is it safe to place pedicle screws in the lower thoracic spine than in the upper lumbar spine? Spine 2007;32:49-54.
Question 13
-In zone II flexor tendon lacerations, repairing only 1 slip compared to repairing both slips of the flexor digitorum sublimis results in
Explanation

Question 14
What term in statistics defines rejecting the null hypothesis when it is in fact true?
Explanation
Type-I errors, to put it simply, detect an effect that is not present. In contrast, a type-II error fails to detect an effect that is present. In simple studies, the rate of a type-I error is denoted by a (alpha). For a 95% confidence level, the value of alpha is 0.05. This means that there is a 5% probability that we will reject a true null hypothesis.
Illustration A shows the difference between type-I and type-II errors. Incorrect Answers;
not technically considered "errors," but instead are variables that properly constructed studies attempt to avoid. Answer 4: Variance is an estimate of the variability of each individual data point from the mean.
Question 15
What is the most common contracture deformity of the spastic shoulder secondary to a cerebrovascular accident?
Explanation
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
Question 16
Figure 25 shows the CT scan of an adult patient who has neck pain following a motor vehicle accident. What is the most likely diagnosis?
Explanation
REFERENCES: Dickman CA, Greene KA, Sonntag VK: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;38:44-50.
Clark CR: The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 362-363.
Question 17
During right knee anterior cruciate ligament (ACL) reconstruction, after drilling an appropriately positioned and referenced tibial tunnel, the surgeon finds that the transtibial guide is placing the femoral tunnel at 11:30 within the intercondylar notch. Which of the following choices will best enable appropriate graft placement in this clinical scenario? Review Topic
Explanation
minimize errant tunnel placement, demonstrated in the literature as the most common cause of ACL failure and need for revision. In this not uncommon clinical scenario, simply converting to a two-incision ACL technique or drilling through the anteromedial portal with the knee hyperflexed will permit accurate femoral tunnel placement and increase the likelihood of an optimal clinical outcome. Femoral tunnel accuracy with these techniques is enhanced by a lower starting point in the intercondylar notch. Familiarity with these techniques is valuable for surgeons performing ACL reconstruction. Revising the tibial tunnel in this scenario would likely lead to bone compromise of the proximal tibia and may interfere with graft fixation and incorporation. Converting to a double-bundle ACL with a transtibial technique would not correct the vertical femoral tunnel. Hyperflexion of the knee may improve femoral tunnel placement to some extent, but is unlikely to allow anatomic placement of a femoral tunnel when the transtibial guide lies in a clearly excessive vertical position.
Question 18
When performing a Green transfer for cerebral palsy—flexor carpi ulnaris (FCU) to extensor carpi radialis brevis (ECRB)—in addition to improving wrist extension, what other motion may be improved if the FCU is routed around the ulna instead of through the interosseous membrane?
Explanation
The typical upper extremity deformity in spastic hemiplegic cerebral palsy consists of shoulder internal rotation, elbow flexion, forearm pronation and wrist flexion, and ulnar deviation. The pronation position of the forearm can make bimanual activities more challenging for the child. The wrist flexion and ulnar deviation deformity interferes with finger function and therefore with grasp and release patterns. By transferring the FCU tendon to the ECRB, the deforming force is released, and central wrist extension is augmented. This transfer can lead to a supination moment when it is routed around the ulna to the ECRB insertion on the dorsum of the wrist. Thumb and finger extension are not affected by an FCU-to-ECRB tendon transfer. Forearm supination, not pronation, is potentially improved with this tendon transfer.
Question 19
Figures 32a and 32b show the radiographs of a 13-year-old right hand-dominant boy who sustained a closed Salter-Harris type II fracture of the proximal humerus during a hockey game. The shoulder has significant swelling, but is neurovascularly intact. What treatment offers the best chance of reestablishing normal shoulder motion?
Explanation
REFERENCES: Dobbs MB, Luhmann SJ, Gordon JE, et al: Severely displaced proximal humerus epiphyseal fractures. J Pediatr Orthop 2003;23:208-215.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, p 701.
Sarwark JF, King EC, Luhmann SJ: Proximal humerus, scapula, and clavicle, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, pp 703-715.
Question 20
An active 55-year-old man who felt a sudden pop in the left heel while playing tennis 6 months ago was diagnosed with an ankle sprain around the time of injury. He now reports calf atrophy and severe weakness with running. Examination reveals a palpable defect in the Achilles tendon and only trace passive ankle flexion when the calf is squeezed. At the time of surgery, an Achilles tendon defect of 6 cm cannot be approximated. Surgical management of the Achilles tendon should include
Explanation
REFERENCES: Myerson M: Achilles tendon ruptures. Instr Course Lect 1999;48:219-230.
Mandelbaum BR, Myerson MS, Forster R: Achilles tendon ruptures: A new method of repair, early range of motion, and functional rehabilitation. Am J Sports Med 1995;23:392-395.
Question 21
An obtunded 80-year-old man was found alone in his apartment after an apparent fall. A CT scan performed in the emergency department shows that he has an extensile injury of an ankylosed cervical spine. The fracture extends across the ossified C5-C6 disk space and into the lamina of C5. There is 1.5 cm of widening between the C5 and C6 vertebrae anteriorly. The patient's family asks you about the long-term impact of the fracture on his functional capacity and survival. You advise them that patients with fractures of the cervical spine with ankylosing conditions have
Explanation
Several studies have found that rates of neurologic deficit and mortality are higher for patients with ankylosing spondylitis and a spinal fracture than for age-matched controls. The 2011 work of Schoenfeld and associates, which directly compared patients with cervical fractures in ankylosed spines to age-and sex-matched controls who also had cervical fractures but no ankylosing condition, demonstrated that those with ankylosing spondylitis were at elevated risk for mortality for up to 2 years after sustaining a fracture. In a study by Westerveld and associates, the rate of neurologic deficit among patients with ankylosing spondylitis and a spinal fracture was 57.1% compared to 12.6% among controls.
RECOMMENDED READINGS
Westerveld LA, van Bemmel JC, Dhert WJ, Oner FC, Verlaan JJ. Clinical outcome after traumatic spinal fractures in patients with ankylosing spinal disorders compared with control patients. Spine J. 2014 May 1;14(5):729-40. doi: 10.1016/j.spinee.2013.06.038. Epub 2013 Aug 27. PubMed PMID: 23992936. View Abstract at PubMed
Schoenfeld AJ, Harris MB, McGuire KJ, Warholic N, Wood KB, Bono CM. Mortality in elderly patients with hyperostotic disease of the cervical spine after fracture: an age- and sex-matched study. Spine J. 2011 Apr;11(4):257-64. doi: 10.1016/j.spinee.2011.01.018. Epub 2011 Mar 5. PubMed PMID: 21377938. View Abstract at PubMed
Question 22
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45° lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
REFERENCES: Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629.
Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Edwards CC II, Bridwell KH, Patel A, et al: Long adult deformity fusions to L5 and the sacrum: A matched cohort analysis. Spine 2004;29:1996-2005.
Question 23
A 38-year-old woman is polytraumatized in a motor vehicle crash. She has multiple injuries including a unilateral femur fracture. The patient is felt to be borderline and, although she is currently stable, she could potentially deteriorate quickly. Which of the following parameters has been suggested as an indicator of which patients would benefit from damage control?
Explanation
Question 24
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
Explanation
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
Question 25
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of
Explanation
REFERENCES: Carson WG Jr, Gasser SI: Little Leaguer’s shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in adolescent baseball pitchers. A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 26
The findings in Brown-Sequard syndrome include loss of which of the following? Review Topic
Explanation
Question 27
What is the primary goal of the initial (acute) rehabilitation phase of an overhead athlete's shoulder?
Explanation
Question 28
Figure 35 shows the radiograph of a 35-year-old weightlifter who has had pain with overhead lifts for the past 7 months. Cortisone injections in the acromioclavicular joint provided only temporary relief. A bone scan reveals increased activity of the acromioclavicular joint. Treatment should now consist of
Explanation
REFERENCES: Flatow EL, Cordasco FA, McCluskey GM, Bigliani LU: Arthroscopic resection of the distal clavicle via a superior portal: A critical quantitative radiographic assessment of bone removal. Arthroscopy 1990;6:153-154.
Lyons FR, Rockwood CA: Osteolysis of the clavicle, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 541-546.
Question 29
What is the most important genetic element that distinguishes community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) from hospital-acquired MRSA? Review Topic
Explanation
encodes a penicillin-binding protein with a very low affinity for beta-lactam antibiotics, resulting in methicillin resistance. SCCmec mobile genetic units carry the mecA gene with additional genetic elements that together yield the multidrug-resistant strains found in healthcare environments. SCCmec type IV is specific to CA-MRSA and lacks these additional genetic elements, resulting in less multidrug resistance.
Question 30
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy? Review Topic
Explanation
Question 31
Which of the following statements is true regarding brake travel time after surgical treatment of complex lower extremity trauma?

Explanation
Egol et al used a computerized driving simulator to compare BTT in three groups of patients; 1)control group, 2)long bone lower extremity fracture group, 3)lower extremity articular fracture group. They concluded that BTT was significantly reduced until 6 weeks after initiation of weight bearing in both long bone and articular fractures of the right lower extremity, and that short musculoskeletal functional assessment scores improved with respect to function and other indexes, but did not correlate with improvement in BTT.
An earlier study by Egol et al looked at total brake time as it related to distance traveled by the automobile before braking at 6, 9, and 12 weeks after operative fixation of a right ankle fracture. When compared with controls, braking time was shown to return to normal by 9 weeks post-operatively, and no significant association was found between the functional scores and this normalization.
Giddins et al provide a review of the literature, the law and the views of the major motor insurers related to driving after injury or operations.
Question 32
Trabecular bone is remodeled through the formation of
Explanation
Question 33
Porous hydroxyapatite is placed into a bone defect. Incorporation of this bone graft substitute is expected to follow which of the following patterns?
Explanation
Question 34
- Demyelination diseases as multiple sclerosis and Guillain-Barre $ create neurologic symptoms by
Explanation
Question 35
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of Review Topic
Explanation
or tumor. Brace treatment is not required for this small curve unless future progression is demonstrated.
Question 36
Which of the following statements is correct regarding Vitamin D?
Explanation
Vitamin D is paramount to proper calcium homeostasis and has important clinical implications in the orthopaedic patient. Vitamin D3 is synthesized in the skin and is converted to 25-hydroxycholecalciferol in the liver. 25-hydroxycholecalciferol is then converted in the kidney into 1,25-dihydroxycholecalciferol, the active form of vitamin
D. The best test to determine Vitamin D deficiency is the measurement of 25-hydroxycholecalciferol, as it has a longer half-life and circulating levels are 1,000x more than 1,25-dihydrocholecalciferol.
Patton et al. review the importance of Vitamin D in the orthopaedic patient. They discuss the implications of Vitamin D deficiency, and urge orthopaedic surgeons to be proficient in both the diagnosis and treatment of the condition.
Bogunovic et al. measured the levels of 25-hydroxycholecalciferol in 723 patients who were to undergo orthopaedic surgery. 40% of these patients were noted to be deficient in Vitamin D, with the highest rates in patients scheduled to undergo trauma and sports surgery.
Illustration A reviews Vitamin D metabolism. 24,25-dihydroxycholecalciferol is referred to as pre-Vitamin D.
Incorrect Answers:
Question 37
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.
Question 38
A 32-year-old woman has left second toe dactylitis (sausage toe). Radiographs show a “pencil in cup” distal interphalangeal joint deformity. Examination reveals that subtalar motion is markedly reduced. What is the most likely diagnosis?
Explanation
REFERENCES: Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA,
WB Saunders, 1991, pp 1691-1693.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Question 39
A 70-year old woman undergoes revision total knee arthroplasty for tibial component aseptic loosening. She is concerned about recurrent loosening, and tibial stem fixation options during revision are reviewed. Figure below displays a radiograph of the revision technique used for this patient. What is the incidence of intraoperative tibial shaft fracture that is associated with this type of revision surgery?
Explanation
Using press-fit tibial stems during a hybrid revision total knee arthroplasty is associated with a 3% to 5% incidence of intraoperative tibial shaft fracture. Diaphyseal fixation of press-fit stems has the advantage of setting component alignment, dispersing forces on the proximal tibia, and offers excellent clinical results. The disadvantages include proximal and distal tibia anatomic mismatch and tibial shaft fracture. Cipriano and associates reported a tibial shaft fracture incidence of 4.9% in a series of 420 consecutive
knee revisions. All fractures healed with nonsurgical management, and none led to implant loosening. In this patient, it is important to recognize on the radiograph that this technique is a hybrid method of revision total knee arthroplasty, with cementation along the tibial tray and metaphysis and with press-fit fixation of the diaphyseal engaging stem. Then, it is important to know the risk and management of intraoperative diaphyseal tibial fractures. Cemented tibial stems are associated with a low rate of intraoperative fracture, because the implant is typically undersized to allow for an appropriate cement mantle. Option C is incorrect, because this revision is not cemented. Option A underestimates the incidence of fracture,
whereas D overestimates the rate of fracture.
Question 40
Intraoperative frozen section analysis reveals 10 neutrophils per high-power field and a positive gram stain result. What is the best next step?
Explanation
The radiograph reveals a rotator cuff dysfunction secondary to malpositioning of the humeral stem and a nonanatomic humeral head. Glenohumeral kinematics have been altered, resulting in damage to the rotator cuff, which in turn has led to impingement with the coracoacromial arch. This single radiograph reveals excessive humeral head height, “overstuffing” of the joint, and severe narrowing of the acromiohumeral interval. Osteolysis and implant loosening are not radiographically apparent. An orthogonal view (axillary lateral) would be necessary to evaluate for shoulder instability. A CT arthrogram is the most appropriate advanced imaging test in the setting of a retained shoulder arthroplasty to evaluate the integrity of the rotator cuff. An MRI evaluation would be obfuscated by artifact. Three-phase and indium-tagged white blood cell scans may be appropriate in the setting of an occult infection evaluation, but not as a test to evaluate rotator cuff injury.
In the absence of infection with rotator cuff compromise, the most appropriate procedure(s) during revision would involve humeral component explantation and conversion to rTSA Revision anatomic hemiarthroplasty may provide pain relief, but function may not appreciably change because of the unbalanced forced couples of the rotator cuff complex. Placement of a glenoid component in the setting of an irreparable rotator cuff tear is contraindicated because rapid glenoid loosening will occur due to eccentric loading during active shoulder motion. Resection arthroplasty should be reserved for recalcitrant cases of infection because this procedure does not provide functional improvement.
In the event that frozen section analysis and positive gram stain results indicate an infection, the treating surgeon should remove all components, perform a thorough debridement and irrigation of suspect tissue, implant an antibiotic spacer, and perform a second-stage reconstruction when deemed appropriate (in light of laboratory studies, repeat shoulder aspiration, frozen section analysis, and arthroscopic soft-tissue biopsy findings). Irrigation and debridement with primary exchange/conversion of components remains inferior to 2-stage reconstruction for infection eradication. Resection arthroplasty remains a salvage procedure for resistant cases that preclude reimplantation and generally is performed for symptom control and sepsis prevention.
RECOMMENDED READINGS
Bohsali KI, Wirth MA, Rockwood CA Jr. Complications of total shoulder arthroplasty. J Bone Joint Surg Am. 2006 Oct;88(10):2279-92. Review. PubMed PMID: 17015609. View Abstract at PubMed
Florschütz AV, Lane PD, Crosby LA. Infection after primary anatomic versus primary reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2015 Aug;24(8):1296-301. doi: 10.1016/j.jse.2014.12.036. Epub 2015 Feb 19. PubMed PMID: 25704211. View Abstract at PubMed
Padegimas EM, Maltenfort M, Ramsey ML, Williams GR, Parvizi J, Namdari S. Periprosthetic shoulder infection in the United States: incidence and economic burden. J Shoulder Elbow Surg. 2015 May;24(5):741-6. doi: 10.1016/j.jse.2014.11.044. Epub 2015 Jan 13. View Abstract at PubMed
Leung B, Horodyski M, Struk AM, Wright TW. Functional outcome of hemiarthroplasty compared with reverse total shoulder arthroplasty in the treatment of rotator cuff tear arthropathy. J Shoulder Elbow Surg. 2012 Mar;21(3):319-23. doi: 10.1016/j.jse.2011.05.023. Epub 2011 Aug 26. PubMed PMID: 21872496. View Abstract at PubMed
Iannotti JP, Spencer EE, Winter U, Deffenbaugh D, Williams G. Prosthetic positioning in total shoulder arthroplasty. J Shoulder Elbow Surg. 2005 Jan-Feb;14(1 Suppl S):111S-121S. PubMed PMID: 15726070. View Abstract at PubMed
Iannotti JP, Gabriel JP, Schneck SL, Evans BG, Misra S. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am. 1992 Apr;74(4):491-500. PubMed PMID: 1583043.View Abstract at PubMed
Grosso MJ, Frangiamore SJ, Ricchetti ET, Bauer TW, Iannotti JP. Sensitivity of frozen section histology for identifying Propionibacterium acnes infections in revision shoulder arthroplasty. J Bone Joint Surg Am. 2014 Mar 19;96(6):442-7. doi: 10.2106/JBJS.M.00258. View Abstract at PubMed
Question 41
During a percutaneous plating of a proximal tibia fracture requiring a 13-hole minimally invasive locking plate system, the placement of the distal most screws should be done through a small open incision to avoid injury to what structure?
Explanation
Question 42
A 20-year-old college athlete is seen for follow-up after sustaining an injury at football practice 2 days ago. He reports that he tackled a player and felt neck pain and numbness in both arms. The numbness resolved within seconds, but his neck remains painful and stiff. He denies any history of neck pain or injury. Examination reveals limited neck motion. The neurologic examination and radiographs are normal. MRI scans of the cervical spine are shown in Figure 34. During counseling, the patient, his family, and his coach should be informed that he has an acute cervical disk herniation and cannot play
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, Burak C, Hosea T, Connolly PJ: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Vaccaro AR, Watkins B, Albert TJ, Pfaff WL, Klein GR, Silber JS: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-705.
Question 43
Contraindications to cervical laminectomy as a treatment for cervical spondylotic myelopathy include which of the following findings?
Explanation
REFERENCES: Malone DG, Benzyl EC: Laminotomy and laminectomy for spinal stenosis causing radiculopathy or myelopathy, in Clark CR (ed.): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 817-825.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 673-680.
Question 44
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child’s back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of Review Topic

Explanation
Question 45
The above surgery was performed with recombinant human bone morphogenetic protein-2 (rhBMP-2). She reports immediate relief of her leg pain and is discharged home on postoperative day 2. The patient reports new-onset radicular pain and weakness in her leg 1 year later. Figures 22a and 22b are her postoperative CT myelogram images. What is the most likely cause of her pain? 22A B

Explanation
Transient thigh pain after lateral, transpsoas interbody fusion is common and generally lasts for less than 3 months. Transpsoas interbody fusion with slip reduction can result in indirect spinal decompression and often obviates the need for a laminectomy for most patients. Complications with this approach are comparable to those experienced with open surgery, but the hospital stay is generally shorter.
Use of BMP in interbody devices has also become common. The images above show heterotopic bone growth into the spinal canal causing nerve compression. This complication is more commonly encountered after posterior lumbar interbody fusions.
RECOMMENDED READINGS
Oliveira L, Marchi L, Coutinho E, Pimenta L. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements.
Spine (Phila Pa 1976). 2010 Dec 15;35(26 Suppl):S331-7. doi: 10.1097/BRS.0b013e3182022db0. PubMed PMID: 21160397. View Abstract at PubMed Cummock MD, Vanni S, Levi AD, Yu Y, Wang MY. An analysis of postoperative thigh symptoms after minimally invasive transpsoas lumbar interbody fusion. J Neurosurg Spine. 2011 Jul;15(1):11-8. doi: 10.3171/2011.2.SPINE10374. Epub 2011 Apr 8. PubMed PMID:
Question 46
A 56-year-old man has had a 2-year history of slowly progressive neck pain and bilateral arm aching. Over the past year, he has noticed intermittent, diffuse numbness in both hands, with decreased grip strength and mild hand clumsiness. He denies any problems with balance. Examination shows a wide-based gait, intrinsic wasting, and a postive Hoffman's sign bilaterally. An MRI scan of the cervical spine is shown in Figure 16. What is the most appropriate treatment? Review Topic

Explanation
Question 47
The CT scan reveals a nondisplaced greater trochanteric fracture. The patient is now experiencing severe pain. What is the most appropriate treatment at this time?
Explanation
This patient presents with significant polyethylene wear, which can lead to both osteolysis and synovitis. However, synovitis usually manifests as a mild to moderate chronic ache, which should explain the discomfort. Although infection should always be ruled out with new-onset pain, no clinical parameters suggest acute hematogenous infection. Similarly, without any mention of back pain or neuropathy, radicular pain from the spine is unlikely. If this patient has a nondisplaced greater trochanteric fracture noted on MR imaging, the optimal immediate mode of treatment is to not rush into surgery despite the mild osteolysis. The patient’s severe pain is likely attributable to the nondisplaced greater trochanteric fracture rather than wear-induced synovitis, which typically presents as a mild to moderate ache. It is recommended to
allow the fracture to heal to avoid fracture displacement. Once the fracture is healed, a revision surgery with liner exchange can be recommended. Based on this clinical scenario, the acetabular component is within what is largely considered the “safe-zone” in THA. Despite this patient’s dislocations, the preferred treatment modality is to revise to a constrained liner. This patient had a well-functioning hip for longer than 15 years. Therefore, conversion to a constrained liner is the best treatment.
Question 48
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700.
Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Fischer SP, Fox JM, Del Pizzo W, Friedman MJ, Snyder SJ, Ferkel RD: Accuracy of diagnoses from magnetic imaging of the knee: A multi-center analysis of one thousand and fourteen patients. J Bone Joint Surg Am 1991;73:2-10.
Question 49
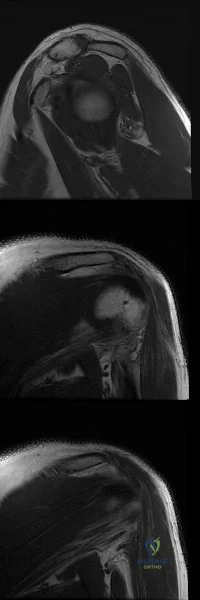
Figures A-C are images of a 37-year-old man who presents with isolated muscle atrophy due to a compressed nerve. Which of the following sequences correctly describes the pathway of this nerve through the brachial plexus, before it innervates the affected muscles?
Explanation
Quadrilateral space syndrome is a condition defined by axillary nerve, +/- posterior humeral circumflex artery compression in the quadrilateral space. It most commonly affects the dominant shoulder in overhead movement athletes (e.g. basketball players) or other throwing athletes. Physical examination may reveal weakness with the arm positioned in abduction and external rotation. In situations of long-standing compression, there may also be atrophy of the teres minor and deltoid muscle.
Chafik et al. dissected thirty-one cadaveric human shoulders to describe the neuromuscular anatomy of teres minor. They showed that the primary nerve branch to teres minor travelled in a fascial sling 44 mm medial to the muscular insertion. This
area may be the potential site of greatest compression and tethering of this nerve in patients with isolated teres minor atrophy.
Friend et al. performed a cadaveric dissection of nine shoulder specimens to look at the anatomical variability in course, length and branching pattern of both the teres minor nerve and the axillary nerve. These were compared to a case-based study of these two male patients with isolated atrophy of teres minor. They concluded that there is no good anatomical predictor of nerve compression outside the quadrilateral space as there is considerable anatomical variation in its origin and course, as well as potential site of compression.
Figure A-C are MRI images that show atrophy of the teres minor muscle and possibly deltoid muscle. The rotator cuff muscles are labeled in Illustration A. The teres minor muscle is labeled in Illustration B. Illustration C shows a diagram of the brachial plexus.
Incorrect
1:
This
describes
the
musculocutaneous
nerve.
3:
This
describes
the
suprascapular
nerve.
4:
This
describes
the
long thoracic
nerve.
Question 50
Figures 10a and 10b show the radiographs of an athletic 9-year-old boy who has activity-related anterior knee pain with intact active knee extension. Examination reveals tenderness to palpation over the inferior pole of the patella. There is no effusion or ligamentous instability. Initial management should consist of
Explanation
REFERENCES: Stanitski CL: Anterior knee pain syndromes in the adolescent. J Bone Joint Surg Am 1993;75:1407-1416.
Stanitski CL: Anterior knee pain syndromes in the adolescent, in Schafer M (ed): Instructional Course Lectures 43. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1994, pp 211-220.
Question 51
03 A 35 year old man sustains a dislocation of his dominant shoulder in a fall. The shoulder is reduced and placed in a sling, but returns 6 hours later with shoulder dislocated again, despite use of a sling. A CT scan is shown in figure 36. Management should now consist of
Explanation
back to this question go to explanation
Question 52
What nerve is at greatest risk when developing the superficial plane between the tensor fascia lata and sartorious during the anterior (Smith-Peterson) approach to the hip?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 302-316.
Crenshaw AH (ed): Campbell’s Operative Orthopedics, ed 7. St Louis, MO, CV Mosby, 1987, pp 59-60.
Question 53
The newborn foot deformity seen in Figures 64a and 64b should initially treated with
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American AcademAyL-oMfadOenrathCooppayedic Surgeons, 2006, pp 240-241.
Farsetti P, Weinstein SL, Ponseti IV: The Long-term functional and radiographic outcomes of untreated
and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265. Question 65
A 4-year-old girl has been limping for the past 2 months. There is no history of trauma, previous injury, fever, or other systemic complaints. Examination reveals a moderate right knee effusio n with a 10-degree knee flexion contracture. What is the next most appropriate step in evaluation?
Arthroscopy
Antinuclear antibody
MRI
Bone scan
HLA-B27
DISCUSSION: The patient presents with juvenile idiopathic arthritis manifestations. The American College of Rheumatology defines this as one or more joints involved with swelling of 6 weeks or longer. A positive antinuclear antibody test would be diagnostic. Consideration should be made to have the patient see an ophthalmologist for evaluation of possible uveitis. Although the patient could have Lyme disease, that choice is not an option. The presence of an elevated antinuclear antibody by itself should not necessarily be used for diagnosing arthritis; however, the test does have clinical utility as a screening test. The frequency of a positive antinuclear antibody test is greatest in younger girls with oligoarticular disease and carries an increased risk for anterior uveitis. Arthroscopy might be indicated if this patient was presenting with a discoid meniscus, but there is no history of clicking, which is often one of the classic signs of discoid meniscus. MRI would not be used to diagnose juvenile idiopathic arthritis, but
MRI would be useful to help diagnose discoid meniscus. A bone scan would show increased uptake in the patient’s knee but again, this would not help diagnose her condition. HLA-B27 has no role in diagnosing juvenile idiopathic arthritis, especially in females.
REFERENCES: Iesaka K, Kubiak EN, Bong LR, et al: Orthopaedic surgical management of hip and knee involvement in patients with juvenile rheumatoid arthritis. Am J Orthop 2006;35:67-73.
Wright DA: Juvenile idiopathic arthritis, in Morrissey RT, Weinstein SL (eds): Love l and Winter’s Pediatric Orthopaedics, ed 6. Philadelphia PA, Lippincott Williams and Wilkins, 2006, pp 405-438. Question 66
An 18-month-old girl is brought in by her parents because of concerns about intoeing, bowlegs, and tripping and fa ling. Prenatal and birth history are otherwise unremarkable. The child’s growth and
development appear to be normal and she has a normal neurologic exam, a straight spine with no defects, and the hips are stable. Examination reveals hip internal rotation of 40 degrees and hip external rotation of 60 degrees. The thigh-foot angle is internal 30 degrees. Feet are straight and supple. Gait is characterized by intoeing with occasional tripping and falling. Based on these findings, what is the most appropriate action?
No treatment because internal tibial torsion slowly resolves on its own
Immediate treatment with a Denis-Browne bar
Distal tibial osteotomies
Proximal femoral derotational osteotomies
Treatment with twister cables PREFERRED RESPONSE: 1
DISCUSSION: The child has classic internal tibial torsion that is very commonly seen in younger children who are just beginning to walk. The normal outcome is for slow resolution of this problem and it seldom requires any treatment. Treatment with a Denis-Browne bar or with twister cables has not been proven to be effective. Surgical treatment at this point is premature and clearly not indicated.
REFERENCES: Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Staheli LT, Corbett M, Wyss C, et al: Lower-extremity rotational problems in children: Normal values to guide management. J Bone Joint Surg Am 1985;67:39-47.

Question 54
Where is the most common site for tuberculosis (TB) spondylitis in children? Review Topic
Explanation
Question 55
A 38-year-old man sustains a terrible triad injury consisting of an elbow dislocation, comminuted and displaced radial head fracture, and a type I coronoid fracture. Intraoperative findings after radial head replacement and lateral collateral ligament complex repair reveal persistent instability consisting of medial opening on valgus stress and posteromedial subluxation of the ulnohumeral and radiocapitellar joints. What is the best next step?
Explanation
normally correct the medial instability. Articulated versus static external fixation can be considered if
restoration of the ligamentous constraint of the medial side of the elbow cannot be accomplished surgically.
Question 56
Figure 1 is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence?

Explanation
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision (Figures below) is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.

Question 57
Figure 1 points to the "tear drop" of the wrist. This radiographic landmark represents which anatomic portion of the wrist?

Explanation
Question 58
A right-handed 24-year-old professional baseball player injured his left shoulder 6 weeks ago when he dove forward and landed hard with the arm extended. He reports that the shoulder “slipped out” and “went back in.” The shoulder did not need to be reduced. He now reports deep pain in the front of the shoulder when batting on either side and is hesitant to raise his left arm up over his head to catch a ball. Examination reveals no obvious deformities of the shoulder and a somewhat guarded, limited range of motion in all planes. Provocative tests for the rotator cuff and labrum are equivocal. MRI scans are shown in Figures 16a and 16b. What is the best course of action?
Explanation
REFERENCES: Abrams JS, Savoie FH III, Tauro JC, et al: Recent advances in the evaluation and treatment of shoulder instability: Anterior, posterior and multidirectional. Arthroscopy 2002;18:1-13.
DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Question 59
Which of the following best describes heat stroke? Review Topic
Explanation
Question 60
Which of the following statements regarding the use of thermal shrinkage during arthroscopic shoulder surgery is most accurate? Review Topic
Explanation
Question 61
A 22-year-old woman injured her ankle when she fell off a ladder. Radiographs reveal a displaced large posterior malleolus fracture of about 45% of the joint. What is the best definitive treatment?
Explanation
optimal function can be achieved. Open reduction and internal fixation allows this achievement. In cases where comminution exists, absolute stability may have to be sacrificed so as to not strip small comminuted bone fragments. Therefore, a bridging technique is worthwhile. External fixation can be used as a temporary technique until the soft tissues are more amenable to definitive fixation. Cast treatment is not indicated in adult forearm fractures. Locking nails for forearm use are not reamed. With regards to articular fractures, anatomic reduction and rigid stabilization are required to achieve the best results and allow for fracture healing. This environment also allows for the best chance of the cartilage repair process to form "hyaline-like" cartilage. Open reduction and internal fixation with absolute stability is the mainstay of treatment for partial articular fractures such as split depression tibial plateau fractures and posterior malleolus fractures involving greater than about 25% to 30% of the joint. The gold standard for the treatment of a closed femur fracture is a reamed intramedullary locked nail. Results are uniformly excellent. This can be done without stripping of the soft tissues such as in open reduction and internal fixation. External fixation can be used as a temporary device in patients in extremis for damage control reasons.Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr. Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am. 1986 Sep;68(7):1008-17. http://www.ncbi.nlm.nih.gov/pubmed/3745238')">View Abstract at PubMedJones DB Jr, Kakar S. Adult diaphyseal forearm fractures: intramedullary nail versus plate fixation. J Hand Surg Am. 2011 Jul;36(7):1216-9. Epub 2011 May
Question 62
A 10-year-old child has leg discomfort with activity. A radiograph, bone scan, and biopsy specimen are shown in Figures 1a through 1c. What is the most likely diagnosis?
Explanation
REFERENCES: Harris WH, Dudley HR Jr, Barry RS: The natural history of fibrous dysplasia: An orthopaedic, pathological and roentgenographic study. J Bone Joint Surg Am 1962;44:207.
Campanacci M: Bone and Soft Tissue Tumors. Vienna, Austria, Springer-Verlag, 1990.
Question 63
Reverse total shoulder arthroplasty combined with latissimus dorsi transfer would be most appropriate for which of the following patients? Review Topic
Explanation
Combining a latissimus dorsi tendon transfers with reverse total shoulder arthroplasty (R-TSA) helps to restore control of active external rotation. Dysfunction with external rotation can be determined clinically with external rotation lag sign, a positive Hornblower's sign, and radiographically with fatty degeneration of the teres minor classified as stage 2 or greater according to the system of Goutallier et al. or Fuchs et al.
Gerber et al. found that R-TSA with combined lat dorsi transfer yielded minimal improvements in external rotation ROM (13 deg to 19 deg) compared to increases in shoulder ROM in flexion (94 deg to 137 deg) and abduction (87 deg to 145 deg), with this procedure.
Boileau et al. examined 17 consecutive patients treated with reverse shoulder arthroplasty and latissimus dorsi and teres major transfer (L'Episcopo). They found
that external rotation increased from -21 degrees to 13 degrees (+34 degrees ). They recommend transferring both the LD and TM, rather than the LD alone as it results in better active external rotation.
Illustration A is a radiograph showing a right reverse total shoulder replacement. Illustration B shows a cadaveric image of the positioning of the latissimus dorsi tendon transfer prior to implantation of the reverse total shoulder components.
Incorrect Answers
Question 64
A 21-year-old man has had right groin pain for the past year. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 50a through 50e. What is the most likely diagnosis?
Explanation
REFERENCES: Terek RM: Recent advances in the basic science of chondrosarcoma. Orthop Clin North Am 2006;37:9-14.
Donati D, El Ghoneimy A, Bertoni F, et al: Surgical treatment and outcome of conventional pelvic chondrosarcoma. J Bone Joint Surg Br 2005;87:1527-1530.
Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 65
A 62-year-old woman with a bone mass density (BMD) T-score of -2.0 sustained a subcapital fracture of her hip. She is an avid tennis player, and history reveals no previous fractures. What is the most appropriate follow-up care?
Explanation
REFERENCE: Gardner MJ, Brophy RH, Demetrakopoulos D, et al: Interventions to improve osteoporosis treatment following hip fracture: A prospective, randomized trial. J Bone Joint Surg Am 2005;87:3-7.
Question 66
A well-developed college football player reports swelling and a heaviness in the arm after lifting weights. Examination reveals that distal pulses are normal and equal in both arms. A venogram is shown in Figure 13. What is the most likely cause of this condition?
Explanation
REFERENCES: Angle N, Gelabert HA, Farooq MM, et al: Safety and efficacy of early surgical decompression of the thoracic outlet for Paget-Schroetter syndrome. Ann Vasc Surg 2001;15:37-42.
Azakie A, McElhinney DB, Thompson RW, et al: Surgical management of subclavian-vein effort thrombosis as a result of thoracic outlet compression. J Vasc Surg 1998;28:777-786.
Question 67
A 6-year-old girl is referred for the elbow injury seen in Figure 2. What is the most appropriate treatment?
Explanation
REFERENCES: Beaty JH, Kasser JR: The elbow: Physeal fractures, apophyseal injuries
of the distal humerus, avascular necrosis of the trochlea, and T-condylar fractures, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 625-703.
Rutherford A: Fractures of the lateral humeral condyle in children. J Bone Joint Surg Am 1985;67:851-856.
Hasler CC, von Laer L: Prevention of growth disturbances after fractures of the lateral humeral condyle in children. J Pediatr Orthop B 2001;10:123-130.
Question 68
Portions of which of the following normal structures help compose the spiral cord seen in Dupuytren’s contracture?
Explanation
REFERENCES: McGrouther D: Dupuytren’s contracture, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone,
1999, vol 1, pp 565-569.
McFarlane R: Patterns of diseased fascia in the fingers in Dupuytren’s contracture.
Plast Reconstr Surg 1974;54:31-44.
Question 69
A 45-year-old woman has had radiating pain in the medial ankle for the past 3 months. Examination reveals a small mass in the retromedial ankle region and a positive Tinel’s sign. An intraoperative photograph and a hematoxylin/eosin biopsy specimen are shown in Figures 24a and 24b. Treatment should consist of
Explanation
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Simon M, Springfield D: Surgery for the Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 530-531.
Question 70
The patient returns 1 year later to report curling of her toes and numbness on the plantar surface of her foot. What is the most likely cause of this condition?
Explanation
Radiographs reveal a Lisfranc fracture dislocation with fractures of the first and second metatarsals. Tenting of skin that is over a bony prominence is an orthopaedic emergency. The fracture dislocation should be reduced without delay. There is no evidence of compartment syndrome of the foot, but this may develop and monitoring is necessary. Toe deformity may develop on a delayed basis because of the subclinical presentation. Nerve irritation is not uncommon with dorsal midfoot surgical incisions. A positive Tinel test result over the midfoot in the distribution of the superficial common peroneal nerve is consistent with a stretch injury to this nerve. CRPS is usually associated with multiple nerve distributions and autonomic nerve findings such as cold hypersensitivity and hyperhidrosis.
RECOMMENDED READINGS
Benirschke SK, Meinberg EG, Anderson SA, Jones CB, Cole PA. Fractures and dislocations of the midfoot: Lisfranc and Chopart injuries. Instr Course Lect. 2013;62:79-91. PubMed PMID: 23395016. View Abstract at PubMed
Schepers T, Oprel PP, Van Lieshout EM. Influence of approach and implant on reduction accuracy and stability in lisfranc fracture-dislocation at the tarsometatarsal joint. Foot Ankle Int. 2013 May;34(5):705-10. doi: 10.1177/1071100712468581. Epub 2013 Jan 14. PubMed
PMID: 23637239. View Abstract at PubMed
Question 71
A 54-year-old woman with idiopathic carpal tunnel syndrome undergoes open carpal tunnel release with a flexor tenosynovectomy. The pathology from the tenosynovium is likely to show
Explanation
REFERENCES: Shum C, Parisien M, Strauch RJ, et al: The role of flexor tenosynovectomy in the operative treatment of carpal tunnel syndrome. J Bone Joint Surg Am 2002;84:221-225.
Fuchs PC, Nathan PA, Myers LD: Synovial histology in carpal tunnel syndrome. J Hand Surg Am 1991;16:753-758.
Kerr CD, Sybert DR, Albarracin NS: An analysis of the flexor synovium in idiopathic carpal tunnel syndrome: Report of 625 cases. J Hand Surg Am 1992;17:1028-1030.
Question 72
For halo traction, what is the preferred site for anterior pin placement?
Explanation
REFERENCE: Ebraheim NA, Lu J, Biyani A, Brown JA: Anatomic considerations of halo pin placement. Am J Orthop 1996;25:754-756.
Question 73
Nerve conduction velocity is slowed by
Explanation
A number of factors affect nerve conduction velocity; for example, increased body temperature increases nerve conduction velocity. Nerve conduction velocity is slowed by advancing age, compression, decreased blood flow, and fibrosis (from large imprecise sutures used for nerve repair). There is no association between hand dominance and nerve conduction velocity.
Question 74
Which of the following is considered a risk factor for the development of low back pain?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 627-643.
Question 75
Because of the ongoing pain and instability and the demonstration of radiographic instability when the ankle is stressed, what surgical procedure should be performed to restore stability to the ankle joint based on the CT findings?
Explanation
The fracture at the insertion of the AITFL into the fibula represents a syndesmosis injury. In some cases, a direct repair of the fracture will stabilize the syndesmosis, but in most cases this injury should most likely be reinforced by placing a screw or suture tensioning device across the syndesmosis for additional support.A Brostrom or allograft reconstruction is indicated for an ankle sprain involving the ATFL or CFL.Simply excising the fragment will leave the patient with an incompetent syndesmosis. Repairing the SPR with or without a groove deepening procedure is indicated if there is evidence of subluxated or dislocated peroneal tendons, which is not demonstrated on the CT scans. The bone has been avulsed off the fibula by the portion of the AITFL that attaches to the fibula, therefore indicating that there is a syndesmosis injury. Allograft lateral ligament reconstruction and excision of loose body/fracture fragment are incorrect procedures based on location. The deltoid is a medial structure and this fracture is lateral. The ATFL and CFL attach at the inferior margin of the fibula near the lateral process of the talus and calcaneus. A SPR avulsion would present as an avulsion off the lateral wall of the fibula, not superior and not into the syndesmotic space as shown on the CT scans.
Question 76
A 71-year-old woman with coronary artery disease underwent an uncomplicated right total hip arthroplasty for osteoarthritis 12 years ago. Her hip has functioned well until approximately 18 months ago when she noted the spontaneous onset of groin, buttock, and proximal thigh pain that is present at rest and made worse with activity. A radiograph is shown in Figure 15. What is the recommended management at this point?
Explanation
Reassurance and follow-up if symptoms worsen places the patient at risk for further bone loss and periprosthetic fracture. Emergent surgery is not required because the symptoms have been present for more than a year; however, urgent revision hip arthroplasty is recommended when the patient is medically cleared. While there is data to suggest that bisphosphonates may slow the progression of osteolysis in animal modes, there is no clear evidence that bisphosphonate treatment prevents the progression of osteolysis in humans. Additionally, this patient has a loose symptomatic femoral component.
REFERENCES: Chiang PP, Burke DW, Freiberg AA, et al: Osteolysis of the pelvis: Evaluation and treatment. Clin Orthop Relat Res 2003;417:164-174.
Dunbar MJ, Blackley HR, Bourne RB: Osteolysis of the femur: Principles of management. Instr Course Lect 2001;50:197-209.
Rubash HE, Dorr LD, Jacobs JJ, et al: Does alendronate inhibit the progression of periprosthetic osteolysis? Trans
Orthop Res Soc 2004;29:1888.
)
Figure 16a Figure 16b
Question 77
A type 2A hangman’s fracture, which has the potential to overdistract with traction, has which of the following hallmark findings?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Levine AM, Edwards CC: The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am 1985;67:217-226.
Question 78
In the treatment of intra-articular calcaneal fractures, surgical reduction and fixation has been shown to have improved outcomes over nonoperative treatment in all of the following patient groups EXCEPT:

Explanation
Question 79
An 82-year-old woman fell on her right shoulder 2 days ago. She is alert, oriented, and in mild discomfort. Prior to falling, she lived alone and functioned independently. Examination reveals extensive ecchymosis extending to the midhumeral region. Her neurovascular examination is normal. Radiographs are shown in Figures 41a and 41b. What is the most appropriate management?
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-1089.
Bigliani LU, Flatow EL, Pollock RG: Fractures of the proximal humerus, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, pp 352-354.
Question 80
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of
Explanation
REFERENCES: Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Wredmark T, Carlstedt CA, Bauer H, et al: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Question 81
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include “onion bulb” formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?
Explanation
REFERENCES: Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422.
Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Miller GM, Hsu JD, Hoffer MM, Rentfro R: Posterior tibial tendon transfer: A review of the literature and analysis of 74 procedures. J Pediatr Orthop 1982;2:363-370.
Question 82
Figures 39a and 39b show the current radiographs of an 8-year-old girl who has had pain in the left thigh for the past 3 months. She was recently diagnosed with hypothyroidism and started treatment 1 week ago. Examination reveals a mild abductor deficiency limp on the left side. She lacks 30 degrees internal rotation on the left hip compared with the right hip. Management should consist of
Explanation
“pre-slip.” Muscle strengthening, hip spica casting, and closed reduction have no place in the primary treatment of a stable slipped capital femoral epiphysis.
REFERENCES: Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Loder R, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Aronson DD, Carlson WE: Slipped capital femoral epiphysis: A prospective study of fixation with a single screw. J Bone Joint Surg Am 1992;74:810-819.
Question 83
What mechanism is associated with the spontaneous resorption of herniated nucleus pulposus?
Explanation
REFERENCES: Haro H, Kato T, Kamori H, et al: Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res 2002;20:409-415.
Doita M, Kanatani T, Ozaki T, et al: Influence of macrophage infiltration of herniated disc tissue on the production of matrix metalloproteinases leading to disc resorption. Spine
2001;26:1522-1527.
Question 84
- A 39-year-old woman jammed her long finger playing softball 24 hours ago. She is unable to actively extend the proximal interphalangeal joint; however, when the joint is brought passively into full extension, she is able to maintain that position. Management should consist of
Explanation
Question 85
Which of the following procedures is considered most appropriate in patients with rheumatoid arthritis?
Explanation
REFERENCES: Granberry WM, Brewer EJ Jr: Early surgery in juvenile rheumatoid arthritis, in Calundruccio RA (ed): Instructional Course Lectures XXIII. St Louis, MO, CV Mosby, 1974, pp 32-37.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JD (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 86
Figures 174a through 174c are the MRI scans of a 16-year-old football player who dislocated his dominant left shoulder 3 weeks ago while landing on his outstretched arm. The dislocation was reduced in the emergency department. He has since had two episodes where he felt like his shoulder slipped partially out of place. Which of the following statements to the athlete and his parents is most accurate regarding treatment options? Review Topic
Explanation
Question 87
The essential lesion responsible for posterolateral rotatory instability of the elbow is disruption of the
Explanation
REFERENCES: O’Driscoll SW, Jupiter JB, King GJW, Hotchkiss RN, Morrey BF: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
Olsen BS, Sojbjerg JO, Dalstra M, Sneppen O: Kinematics of the lateral constraints of the elbow. J Shoulder Elbow Surg 1996;5:333-341.
O’Driscoll SW, Morrey BF, Korinek S, An KN: Elbow subluxations and dislocation: A spectrum of instability. Clin Orthop 1992;280:186-197.
Question 88
A 21-year-old man has had posterior neck discomfort for the past 6 months. Radiographs, an MRI scan, and a photomicrograph of the biopsy specimen are shown in Figures 17a through 17d. What is the most likely diagnosis?
Explanation
REFERENCES: Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991,
vol 2, pp 1143-1174.
Enneking WF: Musculoskeletal Tumor Surgery. New York, NY, Churchill Livingstone, 1983, pp 1043-1053.
Question 89
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. She has symmetric knee flexion, extension, and frontal alignment to her contralateral knee. She has a 1-cm limb-length discrepancy of the femur. She has always been in the 50th percentile for height and her skeletal age matches her chronologic age. She has a complete physeal closure of the right distal femur. What is the expected limb-length discrepancy at maturity? Review Topic
Explanation
Question 90
Kyphosis from a vertebral osteoporotic compression fracture often results in progressive kyphosis due to Review Topic
Explanation
Question 91
A 57-year-old woman with diabetes mellitus has purulent drainage from a lateral incision after undergoing open reduction and internal fixation of a displaced ankle fracture 10 days ago. Examination reveals moderate erythema and a foul odor coming from the wound. Cultures are obtained. What is the next most appropriate step in management?
Explanation
REFERENCES: Carragee EJ, Csongradi JJ, Bleck EE: Early complications in the operative treatment of ankle fractures: Influence of delay before operation. J Bone Joint Surg Br 1991;73:79-82.
Blotter RH, Connolly E, Wasan A, Chapman MW: Acute complications in the operative treatment of isolated ankle fractures in patients with diabetes mellitus. Foot Ankle Int 1999;20:687-694.
Question 92
A well-healed bulk proximal tibia osteoarticular allograft is removed 10 years after implantation due to arthropathy. Histologic examination of the host allograft junction site will most likely reveal
Explanation
Question 93
03 A patient with carpometacarpal joint arthritis of the thumb undergoes trapezium excision and interposition arthroplasty. One year after treatment, radiographs reveal that there has been 25% subsidence of the thumb metacarpal compared with its preoperative height. This degree of subsidence will have what effect on the surgical outcome?
Explanation
pinch stress causes a large amount of axial compressive force through the CMC joint. They also compared preoperative and postoperative functional measurements, including key pinch strength, tipto-tip pinch strength, grip strength, and thumb ROM. Their findings were that postoperatively the first metacarpal subsided 21% at rest (p=0.001). and it subsided another 10.5% during maximal lateral key pinch. Even with this degree of subsidence, the patients experienced increases in pinch strength and grip strength. Also, all patients except for one who had bony impingement reported that they were subjectively much better and more functional.
Lin et. al. also studied trapezium excision and interposition arthroplasty and found no significant differences between results in patients with varying degrees of subsidence. Thus, subsidence does not affect the results of interposition arthroplasty for basal thumb arthritis.
back to this question next question
Question 94
What type of cementless femoral fixation results in the highest rate of distal femoral osteolysis?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Emerson RH Jr, Sanders SB, Head WC, Higgins L: Effect of circumferential plasma-spray porous coating on the rate of femoral osteolysis after total hip arthroplasty. J Bone Joint Surg Am 1999;81:1291-1298.
Question 95
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Explanation
REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Johnson RM, McGuire EJ: Urogenital complications of anterior approaches to the lumbar spine. Clin Orthop 1981;154:114-118.
Question 96
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as
Explanation
REFERENCE: O’Rourke M, Callaghan J, Goetz D, Sullivan P, Johnson R: Osteolysis associated with a cemented modular posterior cruciate substituting total knee design. J Bone Joint Surgery Am 2002;84:1362-1371.
Question 97
Figures 1 and 2 are the radiographs of a 17-year-old man who injured his wrist 6 months ago. He is experiencing pain and limited motion. What is the most effective treatment option?

Explanation
Figures 1 and 2 show a scaphoid nonunion with substantial bone resorption at the nonunion site. Cast immobilization and bracing with bone stimulator use would not be successful treatments at this point because the fracture is 6 months old and there is considerable bone resorption at the fracture site. Scaphoid excision with intercarpal fusion is an option to use only after bone-grafting procedures have failed or arthritis is present. Bone-grafting procedures using both vascularized and nonvascularized graft sources are associated with a high success rate that decreases with avascular necrosis of the proximal pole. If left untreated, scaphoid nonunions can progress to carpal collapse and degenerative arthritis.
Question 98
A 70-year-old woman with a body mass index (BMI) of 34 and a history of hypercholesterolemia has elected to undergo total hip arthroplasty. Her son recently learned he has factor V Leiden following an episode of pulmonary embolism. What are this patient's risk factors for thromboembolic disease?
Explanation
Risk stratification is one of the most critical clinical evaluations to undertake before performing total joint arthroplasty. Many factors have been identified that increase the risk for venous thromboembolism (VTE) The major factors include previous VTE, obesity, type of surgery (such as total joint arthroplasty), hypercoagulable states, myocardial infarction, congestive heart failure, family history of VTE, and
hormone replacement therapy. Hypercholesterolemia is not a risk factor for thromboembolic disease.
Question 99
A positive Froment sign indicates weakness of which of the following muscles?
Explanation
REFERENCE: Burton RI: The Hand: Examination and Diagnosis. Chicago, IL, American Society for Surgery of the Hand, 1978, pp 26-27.
Question 100
Figures 31a and 31b are the radiographs of a 5-year-old boy with an elbow injury.
Explanation
Figure 26 shows lucent areas of both femoral condyles. This may represent a variation of ossification, in which case this boy’s knee pain is coincidental. Another possibility is atypical osteochondritis dissecans. An MRI will distinguish between the 2 entities and will guide treatment.
Figures 27a and 27b show healing rib and distal tibia fractures. These fractures likely are attributable to child abuse. A plain radiographic skeletal survey is sufficient for orthopaedic needs.
A triplane fracture of the distal tibia is revealed in Figure 28. A CT scan will quantify displacement and identify fracture fragments for planning of screw trajectories if open reduction and internal fixation is indicated (displacement > 2 mm).
In Figure 29, the linear lucency of the capitellum indicates an early osteochondritis dissecans. An MRI will allow staging of the lesion.
Figure 30 shows that the left radius and ulna do not align with the humerus; this is the likely result of a transphyseal fracture of the distal humerus. An arthrogram will outline the unossified distal humerus and allow for reduction. For an unstable neonate, this likely can be performed in the NICU.
Figures 31a and 31b reveal a widely displaced lateral condyle fracture for which open reduction and internal fixation is required. No advanced imaging is necessary.

