Orthopedic Board Review MCQs: Foot & Ankle, Knee, & Deformity | Part 197
Key Takeaway
This page offers high-yield multiple-choice questions for orthopedic surgeons and residents. Modeled on OITE/AAOS board exams, it provides a crucial tool for certification preparation. Engage with interactive study and exam modes, complete with clinical explanations, across topics like Ankle, Deformity, Foot, and Knee.
About This Board Review Set
This is Part 197 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 197
This module focuses heavily on: Ankle, Deformity, Foot, Knee.
Sample Questions from This Set
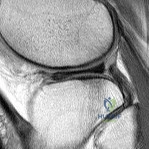
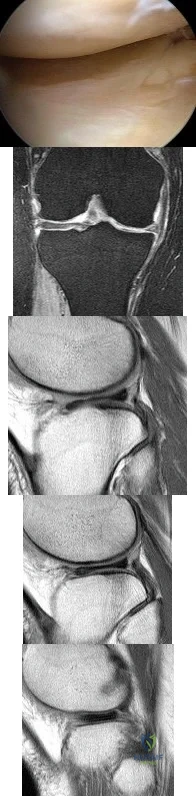
Sample Question 1: A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a...
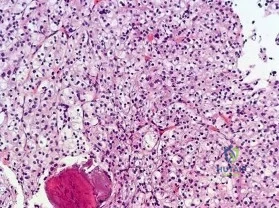
Sample Question 2: Figure 18a shows the clinical photograph of a 31-year-old man who has a slowly growing nodule on his right middle finger. It is minimally tender, and there is no erythema on examination. A biopsy specimen is shown in Figure 18b. What is the...
Sample Question 3: Figures 155a and 155b are the plain radiographs of a 17-year-old boy who recently noted painless swelling in his distal thigh. Examination reveals a firm, fixed, deep distal thigh mass. There is no associated tenderness. What is the best ne...
Sample Question 4: During percutaneous iliosacral screw placement for an unstable pelvic ring injury, use of the lateral sacral fluoroscopic image is critical to help avoid iatrogenic injury to what structure?...
Sample Question 5: A 17-year-old high school football player injures his right ankle during a game. Examination reveals swelling and a closed ankle deformity, with normal foot circulation and sensation. Radiographs are shown in Figures 10a and 10b. In additio...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a
Explanation
REFERENCES: Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Mink JH, Deutsch AL: The knee, in MRI of the Musculoskeletal System, ed 1. New York, NY, Raven Press, 1990, pp 251-387.
Question 2
Figure 18a shows the clinical photograph of a 31-year-old man who has a slowly growing nodule on his right middle finger. It is minimally tender, and there is no erythema on examination. A biopsy specimen is shown in Figure 18b. What is the most likely diagnosis?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 1074.
Halling AC, Wollan PC, Pritchard DJ, et al: Epithelioid sarcoma: A clinicopathologic review of 55 cases. Mayo Clin Proc 1996;71:636-642.
Question 3
Figures 155a and 155b are the plain radiographs of a 17-year-old boy who recently noted painless swelling in his distal thigh. Examination reveals a firm, fixed, deep distal thigh mass. There is no associated tenderness. What is the best next treatment step?

Explanation
Question 4
During percutaneous iliosacral screw placement for an unstable pelvic ring injury, use of the lateral sacral fluoroscopic image is critical to help avoid iatrogenic injury to what structure?

Explanation
In the 2000 reference by Routt et al, they state "a thorough knowledge of pelvic osseous anatomy, injury patterns, deformities, and their fluoroscopic correlations are mandatory for percutaneous pelvic fixation to be effective."
Illustration A shows a representative lateral sacral radiograph, with the major anatomic landmarks labeled. Safe SI screw insertion in the S1 body should be underneath the sacral ala line to minimize risk of a "in-out-in" screw that would come out in the area of the ala and injure the L5 nerve root that sits directly on top of this structure. Dysmorphic pelvic rings will often have a more vertical sacral line, or one that starts more inferiorly.
Question 5
A 17-year-old high school football player injures his right ankle during a game. Examination reveals swelling and a closed ankle deformity, with normal foot circulation and sensation. Radiographs are shown in Figures 10a and 10b. In addition to closed reduction, management should include
Explanation
REFERENCES: Browner BD, Jupiter JB, Levine AM, Trafton PG: Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 1887-1957.
Stiehl JB: Ankle fractures with diastasis. Instr Course Lect 1990;39:95-103.
Question 6
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?
Explanation
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 115-140.
Beaule PE, Dorey FJ, Matta JM: Letournel classification of acetabular fractures: Assessment of interobserver and intraobserver reliability. J Bone Joint Surg Am 2003;85:1704-1709.
Question 7
- Which of the following provides the most stable fixation for comminuted fractures of the posterior acetabular wall?
Explanation
According to Rockwood & Green and Browner & Jupiter the key to fixing these fractures is to re-establish a congruent articular surface. The other four distracters (i.e. cable, methylmethacrylate, multiple lag screws, and multiple K-wires) may achieve initial stability, but reduction will not be maintained. In addition, further studies show a higher incidence of mortality and complications with the use of lag screws and K-wires alone (Browner & Jupiter, Skeletal trauma, 1998)
Question 8
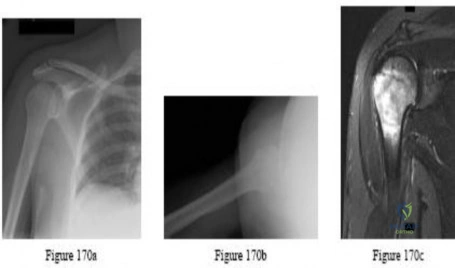
A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation 4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis?
Explanation
REFERENCES: Hattrup SJ, Cofield RH, Cha SS: Rotator cuff repair after shoulder replacement. J Shoulder Elbow Surg 2006;15:78-83.
Sperling JW, Potter HG, Craig EV, et al: Magnetic resonance imaging of painful shoulder arthroplasty. J Shoulder Elbow Surg 2002;11:315-321.
Question 9
Thoracic disk herniations most typically occur at what level of the thoracic spine? Review Topic
Explanation
Question 10
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Explanation
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Question 11
A 70-year-old man seen in the emergency department has had left shoulder pain and a fever of 101.5 degrees F (38.6 degrees C) for the past 3 days. He denies any history of trauma. Examination reveals tenderness anterosuperiorly and at the posterior glenohumeral joint line. He has very limited range of motion (passive and active). Laboratory studies show a WBC count of 12,000/mm 3 and an erythrocyte sedimentation rate of 48 mm/h. Initial management should consist of
Explanation
REFERENCES: Sawyer JR, Esterhai JL Jr: Shoulder infections, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997.
Leslie BM, Harris JM, Driscoll D: Septic arthritis of the shoulder in adults. J Bone Joint Surg Am 1989;71:1516-1522.
Question 12
Bleeding is encountered while developing the internervous plane between the tensor fascia lata and the sartorius during the anterior approach to the hip. The most likely cause is injury to what artery?
Explanation
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 312.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 304.
Question 13
You are counseling a 55-year-old woman for a right carpal tunnel release. What can you tell her about the treatment benefit (grip strength and paresthesia relief) 1 year after surgery compared with continued splinting, NSAID use, physical therapy, and a single steroid injection?
Explanation
Gerritsen and associates, Hui and associates, and Jarvik and associates compared the effectiveness of surgical versus nonsurgical treatment for the relief of carpal tunnel symptoms. All three studies showed that surgery was superior for the relief of paresthesias and the improvement of grip strength. According to the American Academy of Orthopaedic Surgeons Clinical Guidelines on the Treatment of Carpal Tunnel Syndrome, strong evidence supports the assertion that surgical treatment of carpal tunnel syndrome should have a greater treatment benefit at 6 and 12 months than splinting, NSAIDs, physical therapy, and a single steroid injection. The other choices, including no change in grip strength and
paresthesias, decrease in grip strength and increase in paresthesias, and increase in grip strength and paresthesias, are not supported by the evidence.
Question 14
A 39-year-old man has had a foot mass for the past several months. MRI scans are shown in Figures 78a through 78c. A core biopsy specimen reveals synovial sarcoma, and a staging chest CT scan is normal. Which of the following treatments offers the best local tumor control and expedites the patient’s return to normal function?
Explanation
REFERENCES: Ferguson PC: Surgical considerations for management of distal extremity soft tissue sarcomas. Curr Opin Oncol 2005;17:366-369.
Scully SP, Temple HT, Harrelson JM: Synovial sarcoma of the foot and ankle. Clin Orthop Relat Res 1999;364:220-226.
Question 15
Immobilization with a sling
Explanation
Radiographically Active Cyst (age 4 to 8 years old with pathologic fracture)
Align and immobilize
Observe for spontaneous healing
Reassess after 2 to 4 months and if recurrent, follow procedure for pathological fracture of radiographically active cysts described in the article above.
Question 16
A 21-year-old man who underwent repair of a distal biceps tendon rupture using a two-incision approach 4 months ago now reports difficulty gaining rotation of his forearm. Figures 49a and 49b show the AP and lateral radiographs. What is the most likely cause of his problem?
Explanation
REFERENCES: Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed. 2. Philadelphia, PA, WB Saunders, 1993, pp 492-503.
Failla JM, Amadio PC, Morrey BF, Beckenbaugh RD: Proximal radioulnar synostosis after repair of distal biceps brachii rupture by the two-incision technique: Report of four cases. Clin Orthop 1990;253:133-136.
Question 17
The iliopectineal fascia runs between which of the following structures?
Explanation
REFERENCES: Masquelet AC, McCullough CJ, Tubiana R: An Atlas of Surgical Exposures of the Lower Extremity. Philadelphia, PA, JB Lippincott, 1993.
Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1109-1149.
Question 18
A 38-year-old woman has a lesion on her left foot that has increased in size over the past 6 months. The clinical photograph is shown in Figure 17a, and a photomicrograph of the biopsy specimen is shown in Figure 17b. What is the most likely diagnosis?
Explanation
REFERENCES: Hughes LE, Horgan K, Taylor BA, Laidler P: Malignant melanoma of the hand and foot: Diagnosis and management. Br J Surg 1985;72:811-815.
Fortin PT, Freiberg AA: Malignant melanoma of the foot and ankle. J Bone Joint Surg Am 1995;77:1396-1403.
Question 19
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?
Explanation
REFERENCE: Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 2069.
Question 20
A 55-year-old male sustained the injury in Figure A. His injury was complicated by an acute compartment syndrome. He underwent external fixation of his extremity and four compartment fasciotomy. When should the treatment shown in Figure B be performed to minimize the risk of infection?

Explanation
Question 21
A 63-year-old woman is seen 10 weeks after sustaining a closed minimally displaced distal radius fracture. She has been in a short-arm cast and reports minimal pain but notes that she is having difficulty using her thumb. An extensor pollicis longus (EPL) tendon rupture is suspected. Which examination finding would confirm lack of EPL function?
Explanation
As many as to 5% of patients with a nondisplaced distal radius fracture experience EPL rupture. The extensor pollicis brevis (EPB) tendon often attaches to the extensor hood and sometimes continues more distally, providing weak metacarpophalangeal extension even in the setting of EPL disruption. However, because of the vector of its pull, the EPB cannot extend the thumb dorsal to the plane of the palm. A positive Froment sign is noted when flexion of the thumb interphalangeal joint with an attempted key pinch is caused by adductor pollicis weakness from ulnar nerve dysfunction. Compression of the median nerve in the carpal tunnel affects the recurrent motor branch of the abductor pollicis brevis, leading to thenar atrophy. The flexor pollicis longus tendon (FPL) is intact so the patient would not have difficulty flexing the thumb with the palm flat.
Question 22
-What gene is implicated in spinal muscular atrophy?
Explanation

Question 23
A 66-year-old man reports a 2-week history of worsening low back and leg pain. He reports that his pain is aggravated by lying down and relieved by standing and walking. He notes that he has been losing weight recently and that his pain has been awakening him during the night. His medical history is significant for hypertension, coronary artery disease, and prostate cancer. His physical examination is essentially unremarkable. Lumbar radiographs are within normal limits. What is the most appropriate management for this patient?
Explanation
REFERENCES: Agency for Health Care Policy and Research, Bigos SJ (ed): Acute Low Back Problems in Adults. Rockville, MD, US Department of Health and Human Services, AHCPR Publication 95-0642, Clinical Practice Guideline #14, 1994.
Gertzbein SD: Metastatic spine tumors, in Herkowitz HN, Dvorak J, Bell G, et al (eds): The Lumbar Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 792-802.
Question 24
Which of the following factors is most likely to be associated with prolonged survival of total knee arthroplasty?
Explanation
REFERENCES: Rand JA, Ilstrup DM: Survivorship analysis of total knee arthroplasty: Cumulative rates of survival of 9200 total knee arthroplasties. J Bone Joint Surg Am 1991;73:397-409.
Stern SH, Insall JN: Posterior stabilized prosthesis: Results after follow-up of nine to twelve years. J Bone Joint Surg Am 1992;74:980-986.
Knutson K, Lindstrand A, Lidgren L: Survival of knee arthroplasties: A nation-wide multicentre investigation of 8000 cases. J Bone Joint Surg Br 1986;68:795-803.
Question 25
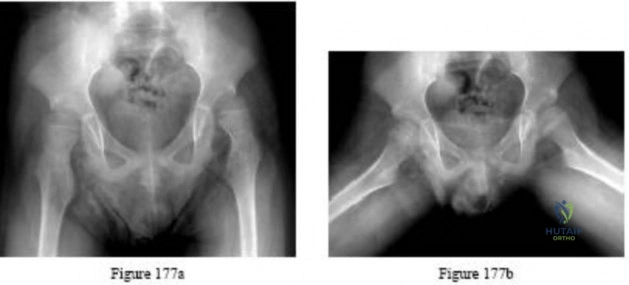
Figures 177a and 177b are the radiographs of a 7-year-old boy with spastic cerebral palsy. He has quadriparetic involvement and is unable to ambulate. He has very limited abduction, 30 degrees of flexion contractures, and pain on abduction. Bilateral varus osteotomies are scheduled with acetabular procedures to improve stability. Which type of acetabular osteotomy should be performed?
Explanation

Question 26
A 53-year-old woman reports a 4-month history of gradual onset diffuse shoulder pain and limited function. She has had no prior treatment, and her medical history is unremarkable. Examination reveals globally painful active range of motion to 120 degrees forward elevation, 25 degrees external rotation with the arm at the side, and internal rotation to the sacrum. Passive range of motion is also limited in comparison with the contralateral shoulder. Radiographs are shown in Figures 31a through 31c. What is the most appropriate management? Review Topic

Explanation
Question 27
Figure 1 is the T2 coronal MRI scan(Massive atraumatic rotator cuff tear) of a 52-year-old woman with a 6-month history of shoulder pain. She does not recall a history of trauma. Physical therapy is recommended. What is the most significant predictor of failure of nonoperative treatment?
Explanation
cuff tear and the severity of patient’s reported pain did not predict failure of nonoperative treatment. Patients who have low expectations regarding the effectiveness of physical therapy are more likely to fail nonoperative treatment.
Question 28
A 7-year-old boy is seen for follow-up for a scoliotic deformity. His parents are concerned because his deformity seems to have increased. He has no pain and is neurologically intact. A radiograph is shown in Figure 94, and measurement of his curve reveals that it has increased 10 degrees. What is the most appropriate recommendation for this patient at this time?
Explanation
REFERENCES: Nakamura H, Matsuda H, Konishi S, et al: Single-stage excision of hemivertebrae via the posterior approach alone for congenital spine deformity: Follow-up period longer than ten years.
Spine 2002;27:110-115.
Ruf M, Harms J: Posterior hemivertebra resection with transpedicular instrumentation: Early correction in children aged 1 to 6 years. Spine 2003;15:2132-2138.
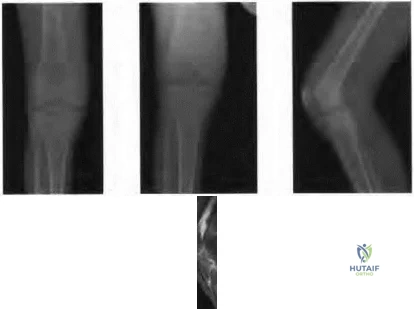
Figure 95a Figure 95b Figure 95c Figure 95d
Question 29
Triple arthrodesis in a reduced position
Explanation
Question 30
Initial repair of the large U-shaped rotator cuff tear shown in Figure 12 consists of closing the tear side-to-side to take advantage of margin convergence. The most significant biomechanical consequence of this repair step results in
Explanation
REFERENCES: Burkhart SS: A stepwise approach to arthroscopic rotator cuff repair based on biomechanical principles. Arthroscopy 2000;16:82-90.
Burkhart SS, Athanasiou KA, Wirth MA: Margin convergence: A method of reducing strain in massive rotator cuff tears. Arthroscopy 1996;12:335-338.
Question 31
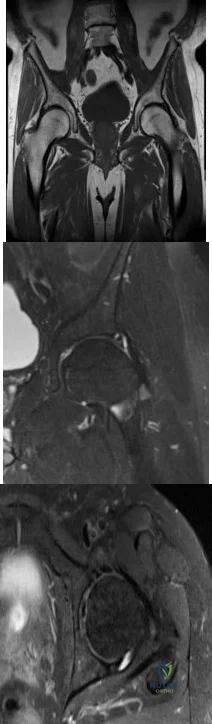
-Images from an MRI scan of this patient’s left hip are shown in Figure 30c through 30e. What is the most likely cause of his acute pain?
Explanation
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement.Surgical treatment for cam impingement can be effective for symptomatic patients. Even among highlevel athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable to those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment.Byrd and Jones described 5 patients who developed transient neurapraxias that resolved uneventfully.The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a periacetabular osteotomy can develop a more retroverted acetabulum as well.
Question 32
A 10-year-old boy with an L1 myelomeningocele has a low-grade fever and a swollen thigh that is warm to touch and erythematous. AP and lateral radiographs are shown in Figures 24a and 24b. Management should consist of
Explanation
REFERENCES: Lock TR, Aronson DD: Fractures in patients who have myelomeningocele. J Bone Joint Surg Am 1989;71:1153-1157.
Kumar SJ, Cowell HR, Townsend P: Physeal, metaphyseal, and diaphyseal injuries of the lower extremities in children with myelomeningocele. J Pediatr Orthop 1984;4:25-27.
Question 33
An 11-year-old boy reports the acute onset of elbow pain and swelling after pushing his brother. The patient's mother and a younger sibling have experienced numerous fractures. You note that the patient and his mother have blue sclera and normal-appearing teeth. A radiograph of the elbow is shown in Figure 60. This patient's disorder is most likely the result of Review Topic

Explanation
Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). These individuals have blue sclerae, and although the initial fracture usually occurs in the preschool years, it may occur at any age. Furthermore, olecranon apophyseal fractures that occur after relatively minor trauma have been associated with type I OI. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. In this patient, there are no indications that the child has been subjected to abuse. Radiographs of the elbow show no evidence of osteopetrosis (due to abnormal osteoclast function) or rickets (due to a deficiency of vitamin D). Morquio syndrome (characterized by a defect of the enzyme N-Ac-Gal-6 sulfate sulfatase) is not associated with blue sclera.
Question 34
Figures 25a and 25b show the radiographs of a 66-year-old man who has had a long history of bilateral painful flatfoot deformities. Examination reveals that his foot is partially correctable passively, albeit with discomfort, and he has an Achilles tendon contracture. An ankle-foot orthosis has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004,
pp 115-120.
Walling AK: Symposium: Adult acquired flatfoot. Clin Orthop 1999;365:2-99.
Question 35
Figure 37 shows the radiograph of a 21-year-old collegiate basketball player who has had mild midfoot aching for the past 4 months. What is the best course of action?
Explanation
REFERENCES: Meyer SA, Saltaman CL, Albright JP: Stress fractures of the foot and ankle. Clin Sports Med 1993;12:395-413.
Kahn JM, Fuller PJ, Burkner PD, et al: Outcome of conservative and surgical management of navicular stress fractures in athletes: Eighty-six cases proven with computerized tomography. Am J Sports Med 1992;20:657-666.
Fitch KD, Blackwell JP, Gillmour WN: Application for non-union stress fractures of the tarsonavicular. J Bone Joint Surg Br 1989;71:105.
Question 36
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Pick TP, Howden R (edS): Gray’s Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 37
A 20-year-old elite college football player has ecchymosis, swelling, and pain on the lateral side of his foot after a game. Radiographs are shown in Figures 31a through 31c. Management should consist of
Explanation
REFERENCES: Glasgow MT, Naranja RJ Jr, Glasgow SG, et al: Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: The Jones fracture. Foot Ankle Int 1996;17:449-457.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-252.
Question 38
Which of the following patients has the highest risk of developing recurrent instability after an arthroscopic Bankart procedure for anterior shoulder instability? Review Topic
Explanation
The surgical management of anterior shoulder instability consists of both arthroscopic and open approaches. The guiding principles for treatment are the restoration of the normal glenoid labrum anatomy and retensioning of the inferior glenohumeral ligament which is achieved via soft-tissue reconstructions (repair of any labral detachment +/- capsular shift) or bony procedures (such as transfer of the coracoid process).
Ahmed et al. reviewed 302 patients who had undergone arthroscopic Bankart repair and capsular shift for the treatment of recurrent anterior glenohumeral instability. The prevalence of patient and injury-related risk factors for recurrence was assessed. The rate of recurrent glenohumeral instability after arthroscopic Bankart repair and capsular shift was 13.2%. The risk of recurrence was independently predicted by the patient’s age at surgery, the severity of glenoid bone loss, and the presence of an engaging Hill-Sachs lesion.
Balg et al. identified risk factors for recurrent instability after arthroscopic Bankart procedure in 131 consecutive patients. Age under 20 years at the time of surgery; involvement in competitive or contact sports or those involving forced overhead activity; shoulder hyperlaxity; a Hill-Sachs lesion present on an AP radiograph of the shoulder in external rotation and/or loss of the sclerotic inferior glenoid contour were all identified as risk factors. These factors were integrated into a 10-point preoperative instability severity index score (ISIS). Patients with a score over 6 points had an unacceptable recurrence risk of 70%.
Illustration A summarizes the components of the ISIS as developed by Balg and Boileau.
Incorrect Answers:
Question 39
What is the next most appropriate step in the orthopaedic management of this patient?

Explanation
OrthoCash 2020
Which of the following findings best describes the acetabular fracture shown in Figure 38?
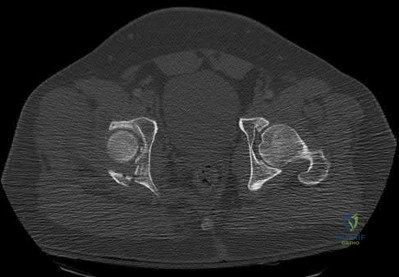
Posterior column with articular impaction and a free fragment
Anterior column with articular impaction
Posterior wall with an intra-articular fragment
Posterior wall with articular impaction and a free intra-articular fragment
Posterior wall with articular impaction Corrent answer: 4
The CT scan shows a posterior wall fracture with impaction of the articular surface and a free fragment within the joint. Proper treatment of this injury requires not only reduction and fixation of the posterior wall fragment but also removal of the free fragment and elevation of the depressed articular segment.
OrthoCash 2020
A 28-year-old female firefighter fell from the top of a three-story building in the line of duty. She sustained a displaced pelvic fracture with more than 5 mm displacement. Compared to normal healthy controls, these patients have a higher incidence of
normal sexual function and normal vaginal childbirth.
sexual dysfunction (dyspareunia) and normal vaginal childbirth.
normal sexual function and caesarean section childbirth.
sexual dysfunction (dyspareunia) and caesarean section childbirth.
normal sexual function and caesarean section childbirth until hardware removal.
Pelvic trauma in women has been shown to increase the risk of sexual dysfunction and dyspareunia. Additionally, caesarean section childbirth is
almost universal following pelvic trauma regardless of whether anterior pelvic hardware is present or not.
OrthoCash 2020
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?

Closed treatment and casting
Open reduction and internal fixation
Primary subtalar arthrodesis
Percutaneous fixation
External fixation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures.
OrthoCash 2020
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
Radial head resection, open reduction and internal fixation of the coronoid, and medial collateral ligament repair
Radial head resection and lateral collateral ligament repair
Radial head arthroplasty alone
Radial head arthroplasty and lateral collateral ligament repair
Radial head arthroplasty, open reduction and internal fixation of the coronoid, and lateral collateral ligament repair
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region.
OrthoCash 2020
A 30-year-old man is brought to the emergency department after a motor vehicle accident. He has a closed midshaft femoral fracture and an intra-abdominal injury. He is currently in the operating room and the exploration of his abdomen has been completed. His initial blood pressure was 70/30 mm Hg and is now 90/50 mm Hg after 4 liters of fluid and 2 units of blood. His initial serum lactate was 3.0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C).
What is the most appropriate management for the femoral shaft fracture at this point?
Reamed intramedullary nailing
Traction
External fixation
Open plating
Mast suit
The patient has several indications that he is not ready for definitive fixation of the femoral shaft fracture at this point. He is cold with a core temperature of 93 degrees F, and hypothermia of less than 95 degrees F (35 degrees C) has been shown to be associated with an increased mortality rate in trauma patients. The patient has also not been resuscitated based on his increasing lactate levels and although controversial, it has been shown that temporary external fixation leads to a lower incidence of multiple organ failure and acute respiratory distress syndrome.
OrthoCash 2020
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?

MRI scan
Physical examination
Workers’ compensation status
Surgeon availability
Patient age
The most important criteria in determining the need for surgery following a nondisplaced or minimally displaced tibial plateau fracture is knee stability to varus/valgus stress. Soft-tissue injury noted on MRI may be addressed at a later time following fracture healing. This fracture pattern is amenable to nonsurgical management. Decisions regarding surgical intervention may be made up to 2 weeks after injury.
OrthoCash 2020
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient’s family reports that he is a Jehovah’s Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient’s blood pressure becomes unstable. What is the most appropriate action?
Consult the ethics committee before giving blood.
Use cell saver blood.
Ask the patient’s family for consent to give blood.
Use plasma expanders.
Give the patient blood.
Certain medical procedures involving blood are specifically prohibited in the belief system of a Jehovah’s Witness whereas others are not doctrinally prohibited. For procedures where there is no specific doctrinal prohibition, a Jehovah’s Witness should obtain the details from medical personnel and make his or her own decision. Transfusions of allogeneic whole blood or its constituents or preoperative donated autologous blood are prohibited. Other procedures, while not doctrinally prohibited, are not promoted such as hemodilution, intraoperative cell salvage, use of a heart-lung machine, dialysis, epidural blood patch, plasmapheresis, white blood cell scans (labeling or tagging of removed blood returned to the patient), platelet gel, erythropoietin, or blood substitutes. The patient should not be given blood. Plasma expanders should be used first to restore hemodynamic stability. Cell saver blood from an open wound is not recommended nor would there likely be enough from an open pelvic fracture to salvage. The patient’s family may be expressing their own beliefs rather than the patient’s beliefs and it would be better to ask the patient when he or she is more alert to determine what procedures they would allow. A consult with the ethics committee will unnecessarily delay an intervention that should restore hemodynamic stability.
OrthoCash 2020
Figure 50 shows the radiograph of a 26-year-old man who sustained an isolated open injury to his foot. Examination reveals no gross contamination in the wound. There is a palpable dorsalis pedis pulse and sensation is present on the dorsal and plantar aspects of the foot. Initial treatment should consist of wound debridement, antibiotics, and

talectomy.
reimplantation of the talus.
reimplantation of the talus with acute triple arthrodesis.
Syme amputation.
transtibial amputation.
The radiograph shows a complete extrusion of the talus. Reimplantation of the talus after wound debridement has been reported to be safe and successful, and provides for flexibility with any future reconstructive procedures.
OrthoCash 2020
Which of the following long bone fracture patterns occurs after a pure bending force is exerted to the bone?
Spiral
Oblique
Transverse
Segmental
Comminuted
A pure bending force produces a transverse fracture pattern. Spiral fractures are mainly rotational, oblique are uneven bending, segmental are four-point bending, and comminuted are either a high-speed torsion or crush mechanism.
OrthoCash 2020
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?

Kocher-Langenbeck
Iliofemoral
Ilioinguinal
Extended iliofemoral
Triradiate approach
The fracture is an associated both column fracture. The best approach for this fracture is the ilioinguinal. The Kocher-Langenbeck is best for posterior injuries to the acetabulum and some transverse fractures. The iliofemoral alone is limited to high anterior column injuries. The extended iliofemoral and triradiate
approaches although useful for this fracture, have a higher rate of complications.
OrthoCash 2020
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes

plating of the radial shaft fracture then open repair of the triangular fibrocartilage complex.
open reduction and internal fixation of the radius and ulna.
plating of the radius then closed reduction and evaluation of the distal radioulnar joint (DRUJ).
closed reduction of the radius and DRUJ.
plating of the radius then pinning of the DRUJ in pronation.
This Galeazzi fracture is an injury that requires surgical treatment in an adult. The algorithm includes anatomic reduction of the radial shaft and closed reduction of the DRUJ with assessment of stability. If the DRUJ remains unstable, supination of the wrist may reduce the DRUJ. If not, either open or closed reduction with pinning is undertaken. The closer the radius fracture is to the DRUJ, the more likely it is to be unstable.
OrthoCash 2020
A 40-year-old laborer sustains the injury shown in the radiograph and CT scan in Figures 56a and 56b. What is the most common complication associated with surgical intervention?

Chronic osteomyelitis
Planovalgus hindfoot
Plantar nerve entrapment
Wound dehiscence
Painful hardware
The patient has a severe Sanders type 4 calcaneus fracture. By far the most common complication associated with surgical treatment of calcaneus fractures is wound dehiscence.
OrthoCash 2020
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
A primed immune system with an increased risk of a systemic inflammatory response
Nothing since they are no longer in uncompensated shock and their vital signs have normalized
Higher nonunion rates after fracture fixation
Higher infection rates after definitive fracture fixation
Higher complication rates after temporizing external fixation of long bone fractures
Patients who are in compensated shock have normal vital signs but still have hypoperfusion of organ beds such as the splanchnic circulation due to preferential perfusion of the heart and brain. The response to this continued hypoperfusion may be the development of a systemic inflammatory response that may lead to multiple organ failure. The patients are thought to be at risk for a “primed” immune system due to the ongoing stimulation of the immune system and may have an exaggerated response to a second stimulus such as surgery or infection. Other markers of resuscitation should be used besides vital signs to determine when resuscitation has been completed. The use of temporizing fixation has been shown to lower systemic complication rates, and the infection and union rate after staged fixation is not altered.
OrthoCash 2020
A 14-year-old boy sustains a right leg injury after being thrown from his motorcycle while racing. He reports diffuse right leg pain starting at his knee and proceeding distally to include his foot. After the injury the patient’s mother reports the tibia moving posteriorly then anteriorly while she was supporting the leg. In the emergency department 4 hours after injury, examination reveals a large knee effusion, firm compartments of the leg, a palpable posterior tibialis pulse with a warm, pink foot, and capillary refill of 2 seconds at the toes. His blood pressure is 100/50 mm Hg. Motor examination is
intact, but there is decreased sensation in the dorsal first interspace and plantar aspect of the foot. Compartment pressure measurement reveals all four compartments with pressures of 33, 36, 33, and 38 mm Hg respectively. Radiographs are shown in Figure 59a and 59b. The remainder of the skeletal examination is normal. What is the optimal management for this injury?

Emergent four compartment fasciotomies
Emergent four compartment fasciotomies and open reduction and internal fixation of the fracture
Elevation of the limb overnight and four compartment fasciotomies in the morning
Elevation of the limb overnight and a recheck of compartment pressures in the morning
Emergent MRI of the knee and leg Corrent answer: 2
The patient has a compartment syndrome based on the firm compartments of the leg and the elevated compartment pressures measured at the diastolic pressure reading. Muscle ischemia occurs quickly when compartment pressures are elevated, and within 6 hours irreversible damage can occur. Emergent fasciotomies permit decompression of all four compartments and reestablishment of vascular supply to the muscles. Stabilization of the fracture prevents further soft-tissue injury.
OrthoCash 2020
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
The mean arterial blood pressure is above 90 mm Hg.
The pulse pressure has normalized.
Urine output is greater than 0.5 to 1 mL/kg/h.
Oxygen delivery has been maximized.
Aerobic metabolism has been restored in all tissue beds.
Shock can be defined as inadequate tissue perfusion. Resuscitation or the resolution of shock is defined as when oxygen debt has been repaid, tissue acidosis is eliminated, and aerobic metabolism has been restored in all tissue beds. The end points for resuscitation are not clearly defined, but occult shock can still be present in the setting of normal vital signs and normal urine output due to selective perfusion of organ systems.
OrthoCash 2020
A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
Infection
Malunion
Loss of forearm rotation
Refracture
Delayed union/nonunion
Healing of forearm fractures in skeletally immature patients is the usual outcome. The use of intramedullary fixation has been reported to result in a lower frequency of refractures when compared to plate osteosynthesis due to the absence of diaphyseal holes after plate removal, which are considered stress risers. Regardless of implant technique, malunion and infection are infrequent. Loss of forearm pronation and supination is a common occurrence in surgically treated fractures due to the higher degree of soft-tissue injury, and periosteal stripping leads to fracture site instability and fracture comminution.
OrthoCash 2020
The teardrop shape marked with an asterisk in Figure 61 represents what anatomic structure?
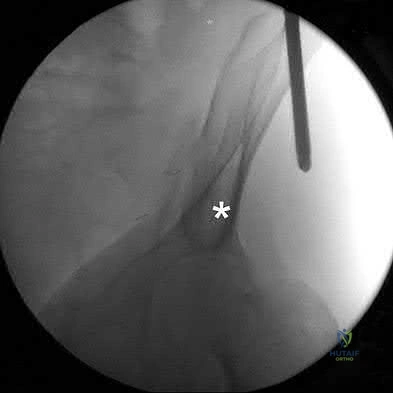
Anterior superior iliac spine
Sciatic buttress
A column of bone running from the anterior inferior iliac spine (AIIS) to the posterior superior iliac spine (PSIS)
The most superior portion of the roof of the acetabulum
Iliopectineal line
The teardrop can be visualized on the obturator outlet view of the pelvis and represents a thick column of bone that runs from the AIIS to the PSIS. Half pins for eternal fixation frames or screws can be inserted into this column for fixation of fractures.
OrthoCash 2020
A patient was treated with a revision reamed intramedullary nail for a nonunion 6 months ago. A current radiograph is shown in Figure
Question 40
During a posterior cruciate ligament (PCL)-retaining total knee arthroplasty, a critical principle to remember is to
Explanation
Maintenance of the joint line and accurately tensioning the PCL are critical in the proper execution of a PCL-retaining total knee arthroplasty. Appropriate tension helps ensure femoral rollback and avoid stiffness or instability. Raising the joint line to help ensure full extension should be avoided in cruciate- retaining knees, because doing so creates an unfavorable kinematic environment. The three important principles of surgical technique needed to maintain appropriate tensioning of the PCL include 1) choosing the proper femur size to reproduce the native femoral anterior/posterior dimension, 2) reproducing the joint line by resecting as much tibia from the healthy side as will be replaced by the smallest thickness of the tibial component and, 3) ensuring that full extension is achieved by soft-tissue releases and not by taking additional distal femur, as may be done in a posterior stabilized approach. Another important principle is to re-create the natural degree of the patient’s posterior tibial slope to avoid tightness in
flexion.
Question 41
Figure 59 shows properties of a material being tested for use as an implant. What is represented by the portion of the stress-strain curve from point A to point B?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 45-46.
El-Ghannam A, Ducheyne P: Biomaterials, in Mow VC, Huiskes R (eds): Basic Orthopaedic Biomechanics and Mechano-Biology, ed 3. Philadelphia, PA, Lippincott-Raven, 2005, pp 501-503.
Question 42
Your 25-year-old patient complains of anterior knee pain after retrograde femoral nailing for a diaphyseal fracture and asks you why you didn’t perform antegrade nailing as he has seen on the internet. You tell him that retrograde nailing is your preferred technique over antergrade nailing for diaphyseal femoral fractures because it has been shown to have?

Explanation
Question 43
A 75-year-old patient returns for follow-up after undergoing bilateral total hip arthroplasty (THA). The right hip is a hybrid THA performed 12 years ago, whereas the left hip is a cementless THA performed 10 years ago. Both acetabular components are the same type, same size, and from the same manufacturer. Both femoral heads are 28-mm cobalt-chromium components. What is the most likely explanation for the advanced polyethylene wear in one hip?
Explanation
5 years of shelf life, polyethylene oxidized rather slowly. However, polyethylene components with a shelf life of more than 5 years would be expected to have minimal mechanical toughness and would likely fail rapidly if implanted. Bohl and associates evaluated 135 patients who had undergone total knee arthroplasty. Survivorship at 5 years was 100% for components with a shelf life of less than 4 years, 89% for components with a shelf life of 4 to 8 years, and 79% for components with a shelf life of more than 8 years. Sychterz and associates reported no correlation between shelf life and true wear rates for components with a shelf life of less
than 3 years. In summary, both in vivo and in vitro data suggest that shelf life in excess of
3 to 5 years has a direct effect on wear of polyethylene.
REFERENCES: Currier BH, Currier JH, Collier JP, et al: Shelf life and in vivo duration: Impacts on performance of tibial bearings. Clin Orthop 1997;342:111-122.
Bohl JR, Bohl WR, Postak PD, et al: The Coventry Award: The effects of shelf life on clinical outcome for gamma sterilized polyethylene tibial components. Clin Orthop 1999;367:28-38.
Sychterz CJ, Young AM, Orishimo K, et al: The relationship between shelf life and in vivo wear for polyethylene acetabular liners. J Arthroplasty 2005;20:168-173.
Question 44
A 20-year-old athlete sustains a 2- x 3-cm grade IV chondral injury to the right knee. After failure of nonsurgical management, which of the following procedures would ensure the highest percentage of hyaline-like cartilage?
Explanation
REFERENCES: Brittberg M, Lindahl A, Nilsson A, et al: Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med 1994;331:889-895.
Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 787-804.
Question 45
An elite gymnast injured her ankle in an awkward dismount 36 hours ago. Examination reveals weakness on single leg step-up. A clinical photograph of the medial ankle is shown in Figure 15. Plain radiographs are normal. To help confirm the diagnosis, the next step in evaluation should consist of
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 307-317.
Rosenberg ZS, Cheung Y, Jahss MH, Noto AM, Norman A, Leeds NE: Rupture of the posterior tibial tendon: CT and MR imaging with surgical correlation. Radiology 1988;169:229-235.
Question 46
Which of the following methods most reliably detects mechanical loosening of the hip?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Miniaci A, Bailey WH, Bourne RB, McLaren AC, Rorabeck CH: Analysis of radionuclide arthrograms, radiographic arthrograms, and sequential plain radiographs in the assessment of painful hip arthroplasty. J Arthroplasty 1990;5:143-149.
Question 47
A patient is treated with volar plating for a distal radius fracture. The CT scan shown in Figure 15 is obtained after union of the fracture because the patient reports ongoing symptoms. The prominent hardware is most likely injuring what tendon?
Explanation
REFERENCES: Benson EC, Decarvalho A, Mikola EA, et al: Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res 2006;451:218-222.
Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadelphia, PA, Mosby-Year Book, 1998.
Question 48
-A 75-year-old woman fell at home and sustained the injury seen in Figures 249a through 249c. What is the most appropriate treatment option?
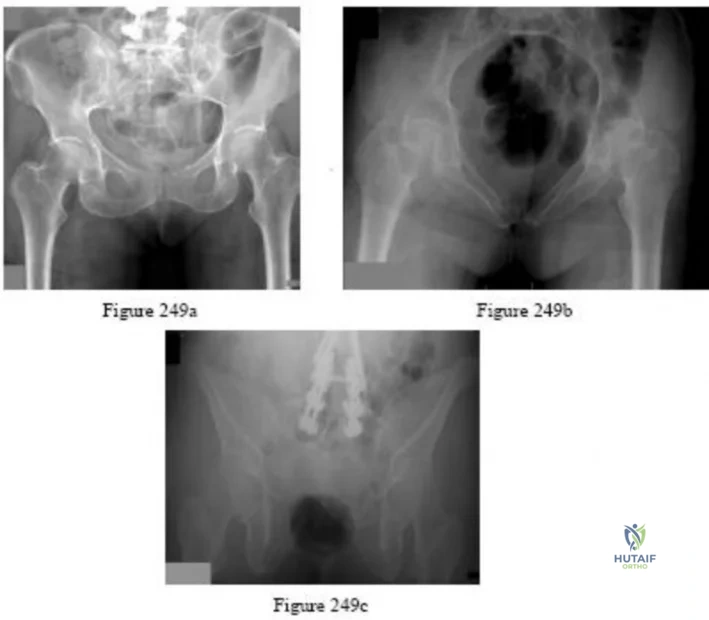
Explanation

Question 49
Figure 80a shows an arthroscopic view from an infralateral portal of a right knee. Figure 80b shows a coronal MRI scan, and Figures 80c through 80e show consecutive sagittal images of the knee. The images show what anatomic finding? Review Topic
Explanation
Question 50
A purulent flexor tenosynovitis of the thumb may communicate with the small finger flexor through which of the following structures?
Explanation
REFERENCES: Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1044-1045.
Burkhalter WE: Deep space infections. Hand Clin 1989;5:553-559.
Question 51
A 64-year-old female sustains a nondisplaced distal radius fracture and undergoes closed treatment using a cast. Three months after the fracture she reports an acute loss of her ability to extend her thumb. What is the most likely etiology of her new loss of function?

Explanation
Question 52
Osteonecrosis of the humeral head is a rare complication seen after dislocation of the glenohumeral joint in skeletally immature patients. When this complication is encountered, treatment should consist of
Explanation
REFERENCES: Pateder DB, Park HB, Chronopoulos E, et al: Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent: A case report. J Bone Joint Surg Am 2004;86:2290-2293.
Wang P Jr, Koval KJ, Lehman W, et al: Salter-Harris type III fracture-dislocation of the proximal humerus. J Pediatr Orthop B 1997;6:219-222.
Question 53
A 22-year-old professional baseball catcher has posterior shoulder pain and severe external rotation weakness with the arm in adduction. Radiographs are normal. MRI scans are shown in Figures 15a through 15c. Management should consist of
Explanation
REFERENCES: Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment.
J Bone Joint Surg Am 2000;82:415-424.
Martin SD, Warren RF, Martin TL, et al: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 54
- The lateral fragment of bone (Segond fracture) associated with an injury of the anterior cruciate ligament is the result of an avulsion of the
Explanation
Question 55
A 72-year-old woman falls onto her left hip after tripping over a curb during her daily 3-mile walk. An injury radiograph is shown in Figure A. What is the best long term solution?

Explanation
The aims of surgery for FNF in elderly patients are immediate pain relief, rapid mobilization, and low complications and revision. THA has best pain relief, fewer reoperations, best survivorship and is most cost-effective but has longer operative/anesthetic time, blood loss, higher infection rate, and potential instability compared with HA.
Healy and Iorio examined the optimal treatment for elderly FNF. They compared internal fixation (120 patients) with arthroplasty (HA, 43 patients; THA, 23 patients). There was no different in reoperation or mortality rates between the 2 groups, but arthroplasty was more cost effective, had independent living, and longer interval to reoperation/death. THA had less pain, better function, and lower rates of reoperation than HA, and was most cost-effective. They concluded that THA was the best treatment.
Yu et al. performed a meta-analysis of randomized controlled trials to determine whether THA or hemiarthroplasty (HA) was superior. They found that THA had lower risk of reoperation (RR = 0.53), higher risk of dislocation (RR = 1.99), and
higher functional scores at 1 and 4 years. There was no difference in mortality, infection and complication rates.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Question 56
Duchenne’s muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?
Explanation
REFERENCES: Fitzgerald RH, Kaufer H, Malkani AL: Orthopaedics. St Louis, MO, Mosby Year Book, 2002, pp 1573-1583.
Smith SA, Swaiman HF: Muscular dystrophies, in Swaiman KF, Ashwall S (eds): Pediatric Neurology Principles and Practice, ed 3. St Louis, MO, Mosby, 1999, pp 1235-1237.
Question 57
…A 56-year-old podiatrist with a negative past medical history had anterior knee pain after an injury. His radiographs, CT scan, and T1-weighted sagittal and fat-saturated axial MR images are shown in Figures 15a through 15e, respectively. After arthroscopic partial medial menisectomy, the patient was turned to the prone position and an open posterior arthrotomy and excision was performed. Low-power and high-power hematoxylin and eosin stained histologic specimens are shown in Figures 15f and 15g, respectively. Based on the history, radiographs, CT scan, MRI scans, and histologic findings, what is the most likely diagnosis?
Explanation
Figures 16a and 16b are the right femur radiographs of a 59-year-old man who has severe pain in his right distal thigh and knee with no significant trauma and an inability to bear weight. Blood tests demonstrate anemia, serum protein electrophoresis/urine protein electrophoresis findings are negative, and electrolyte levels are within defined limits.


Question 58
The insurance carrier of a patient who underwent total knee arthroplasty 4 days ago is now demanding that the patient be discharged from the hospital. However, examination reveals that the patient has a range of motion of only 10° to 55°, and the patient is concerned whether she will ever move her knee normally. The insurance company representative should be advised that
Explanation
REFERENCE: Mauerhan DR, Mokris JG, Ly A, Kiebzak GM: Relationship between length of stay and manipulation rate after total knee arthroplasty. J Arthroplasty 1998;13:896-900.
Question 59
What is the most common complication of halo vest immobilization in adults?
Explanation
REFERENCES: Baum JA, Hanley EN Jr, Pullekines J: Comparison of halo complications in adults and children. Spine 1989;14:251-252.
Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
Nemeth JA, Mattingly LG: Six-pin halo fixation and the resulting prevalence of pin-site complications. J Bone Joint Surg Am 2001;83:377-382.
Question 60
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?
Explanation
REFERENCES: Hartsock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29:467-475.
Hughes M, Neer CS: Glenohumeral joint replacement and postoperative rehabilitation.
Phys Ther 1975;55:850-858.
Compito CA, Self EB, Bigliani LU: Arthroplasty and acute shoulder trauma. Clin Orthop 1994;307:27-36.
Question 61
-A 15-year-old boy with mild type I osteogenesis imperfecta (OI) has a midshaft radius/ulna fracture that is in bayonet apposition with loss of the radial bow and 40-degree apex volar and ulnar angulation. Closed reduction improves the angulation to 20 degrees; the bayonet apposition and loss of radial bow remains.His contralateral forearm has a normal appearance upon examination. What is the best treatment for this fracture?
Explanation

Question 62
An 18-month-old child sustains a crush amputation of the tip of the index finger. Bone is exposed, but the nail is intact. Management should consist of
Explanation
REFERENCES: Das SK, Brown HG: Management of lost finger tips in children.
Hand 1978;10:16-27.
Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg
1996;4:84-92.
Question 63
A 34-year-old male presents with elbow pain after sustaining a ground level fall 2 weeks ago. An injury radiograph is shown in Figure
Explanation

OrthoCash 2020
Question 64
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?
Explanation
REFERENCES: Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Tewes DP, Fischer DA, Fritts HM, et al: MRI findings of acute turf toe: A case report and review of anatomy. Clin Orthop 1994;304:200-203.
Question 65
Examination of a hand with compartment syndrome is most likely to reveal which of the following?
Explanation
REFERENCES: Oullette EA, Kelly R: Compartment syndromes of the hand. J Bone Joint Surg Am 1996;78:1515-1522.
Dellaero DT, Levin LS: Compartment syndrome of the hand: Etiology, diagnosis, and treatment. Am J Orthop 1996;25:404-408.
Question 66
An 8-year-old girl sustained a displaced fracture at the base of the femoral neck in a motor vehicle accident. Management should consist of
Explanation
REFERENCES: Cheng JC, Tang N: Decompression and stable internal fixation of femoral neck fractures in children can affect the outcome. J Pediatr Orthop 1999;19:338-343.
Azouz EM, Karamitsos C, Reed MH, et al: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420.
Song KS, Kim YS, Sohn SW, et al: Arthrotomy and open reduction of the displaced fracture of the femoral neck in children. J Pediatr Orthop B 2001;10:205-210.
Morsy HA: Complications of fracture of the neck of the femur in children: A long-term follow-up study. Injury 2001;32:45-51.
Question 67
What structure has been described as having a risk of injury with retractor placement on the sacrum during combined acetabular-pelvic ring surgery using the Stoppa approach with a lateral window?

Explanation
Question 68
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
REFERENCES: Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Warner JJ, Deng XH, Warren RF, Torzilli PA: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Question 69
A 28-year-old male sustains a fall on icy ground and fractures his ankle. An intraoperative fluoroscopy image is shown in Figure A. This fixation suggests that the mechanism of injury was one of

Explanation
A vertical fracture of the medial malleolus is characteristic of a Lauge-Hansen SA fracture. Bimalleolar SA fractures will also demonstrate a distal fibular avulsion. Another characteristic is impaction of anteromedial distal tibia by the talar dome. An anteromedial surgical approach allows visualization of this region, elevation of impaction, and bone grafting of the defect if necessary.
Dumigan et al. analyzed 4 different methods of treating vertical shear fractures with polyurethane models. They found that fixation with a 4 hole 1/3 tubular plate with 2 screws in the distal fragment was stiffer than fixation with the same plate with 1 screw in the distal fragment (3 in the proximal), fixation with two 3.5mm cortical screws with washers, and fixation with two 4mm cortical screws with washers. They recommend plating over screw-alone constructs.
McConnell et al. reported 8 cases of anteromedial marginal impaction in SA fractures. They note that 44 fractures were SA type. Following reduction and fixation, all 8 patients had excellent outcome and no arthritis. They recommend an anteromedial approach to the medial malleolus for visualization.
Figure A is a lateral radiograph showing fixation of both malleoli with reconstruction plates. Illustration A is an postoperative AP fluoroscopy image. Illustration B is an injury film demonstrating the same SA ankle fracture. Illustration C shows articular impaction at the medial shoulder of the ankle joint typical of SA injuries. Illustration D shows marginal impaction in SA fractures.
Incorrect Answers
(SBQ12TR.76) A 24-year-old male sustains the fracture dislocation shown in Figure
A. How is this fracture pattern best classified?

Moore I
Moore II
Schatzker III
Schatzker V
OTA type 41B3
Figure A shows a Moore Type II fracture. Moore type II fractures consist of fractures involving the entire tibial condyle, where the fracture line begins in the opposite compartment and extends across the tibial eminence.
A number of classification systems are used to describe tibial plateau fractures. The main classification systems that are widely used include Schatzker, AO/OTA, Hohl and Moore. The Moore classification describes high energy fracture-subluxation injuries of the knee. This is thought to have clinical implications as the type of fracture pattern can indicate an associated soft-tissue injury.
Moore retrospectively reviewed over a 1000 proximal tibia fractures to devise a classification systems based on the characteristic of five types of tibia plateau fracture patterns. He believed this system helped to better understand knee instability and concomitant soft-tissue injury. For example, Moore Type III fractures (rim avulsion) are associated with a high rate of neurovascular injury.
Figure A shows a fracture involving the entire tibial condyle. Illustration A shows a schematic diagram of the Moore classification (I - V). Illustration B shows a table that
describes the Moore classification (I - V).
Incorrect Answers:
Question 70
Radial nerve palsy is most commonly associated with which of the following types of humeral fractures?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Pollock FH, Drake D, Bovill EG, Day L, Trafton PG: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Question 71
A healthy 27 year-old-male is brought into the emergency department after a fall from height. He has a suspected left C8-T1 nerve injury. Which of the following findings would most suggest a root avulsion injury rather than a brachial plexus injury at this level?
Explanation
Brachial plexus injuries are often classified as preganglionic vs. postganglionic injuries. Preganglionic injuries are typically avulsion injuries proximal to the dorsal root ganglion. Clinical features suggestive of lower root avulsion injury include a person falling from height clutching on object to save himself, Horner’s syndrome (drooping of the eyelid (ptosis), pupillary constriction (miosis) and anhidrosis), absence of a Tinel sign or tenderness to percussion in the neck, and a normal histamine test (C8-T1 sympathetic ganglion - intact triple response (redness, wheal, flare)).
Caporrino et al. reviewed 102 patients to assess the best modality (e.g. physical examination, MRI and nerve conduction studies [NCSs]) for diagnosing and localizing brachial plexus injuries. They found the best diagnostic performance with physical examination (sensitivity = 97.8%; specificity = 30.8%) and NCSs (sensitivity
= 98.9%; specificity = 23.1%). MRI had inferior performance for all measurements. They conclude that NCSs exhibited superior performance to MRI, and should be considered a more reliable supporting tool after detailed physical examination.
Incorrect Answers:
Question 72
A 62-year-old man who underwent total knee arthroplasty 6 months ago now reports pain after falling on the anterior portion of the knee. Examination reveals weakness of knee extension but no extensor lag. Flexion that had once measured 115 degrees is now limited to 70 degrees because of pain. A radiograph is shown in Figure 25. Management should now consist of
Explanation
REFERENCES: Brown TE, Diduch DR: Fractures of the patella, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1290-1312.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 323-337.
Question 73
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured? Review Topic
Explanation
Question 74
On an axial CT image, which of the following dimensions is considered to be indicative of a critical amount of lumbar spinal stenosis? Review Topic
Explanation
Question 75
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-247.
Question 76
An otherwise healthy 25-year-old man sustained a wound with a 1-cm by 1.5-cm soft-tissue loss over the volar aspect of the middle phalanx of his middle finger. After appropriate debridement and irrigation, the flexor digitorum profundus tendon and neurovascular bundles are visible. The wound should be treated with a
Explanation
flap is ideal for small wounds on the volar aspect of digits. A thenar flap is suitable for tip injuries. A lateral arm flap will not reach the fingers. A Moberg flap is limited to distal injuries of the thumb.
REFERENCES: Kappel DA, Burech JG: The cross-finger flap: An established reconstructive procedure. Hand Clin 1985;1:677-683.
Lister GD: Skin flaps, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1741.
Question 77
Figure 131 is the abdominal radiograph of a 70-year-old man who experiences nausea and abdominal tightness 48 hours after undergoing left total knee arthroplasty. An examination reveals severe abdominal distension and markedly decreased bowel sounds. Insertion of a nasogastric tube does not relieve abdominal tightness. What is the best next step?
Explanation
The abdominal radiograph reveals an acute colonic pseudo-obstruction. It is associated with parenteral narcotic use and hypokalemia. Initial treatment is insertion of a nasograstric tube, discontinuation of parenteral narcotics, and correction of electrolyte imbalances. If a pseudo-obstruction is not relieved, colonoscopy should be performed.
Question 78
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals lumbar paraspinal spasm and a positive straight leg raising test. Deep tendon reflexes, motor strength, and sensation in the lower extremities are normal. Radiographic findings are normal. If symptoms persist for longer than a few weeks, what is the best course of action?
Explanation
REFERENCES: Epstein JA, Epstein NE, Marc J, et al: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Hashimoto K, Fujita K, et al: Lumbar disc herniation in children. J Pediatr Orthop
1990;10:394-396.
Question 79
Figures 5a and 5b show the radiograph and MRI scan of a patient who has severe mechanical neck pain but no neurologic problems. Biopsy and work-up show the lesion to be a solitary plasmacytoma. Treatment should consist of
Explanation
REFERENCES: Corwin J, Lindberg RD: Solitary plasmacytoma of bone vs. extramedullary plasmacytoma and their relationship to multiple myeloma. Cancer 1979;43:1007-1013.
Durr HR, Wegener B, Krodel A, et al: Multiple myeloma: Surgery of the spine. Retrospective analysis of 27 patients. Spine 2002;27:320-324.
Question 80
Figure 25 shows the radiograph of an 84-year-old woman who has pain and is unable to extend her knee. History reveals that she underwent total knee arthroplasty 8 years ago. Aspiration and studies for infection are negative. During revision surgery, management of the tibial bone loss should consist of
Explanation
REFERENCES: Mow CS, Wiedel JD: Structural allografting in revision total knee arthroplasty. J Arthroplasty 1996;11:235-241.
Engh GA, Herzwurm PJ, Parks NL: Treatment of major defects of bone with bulk allografts and stemmed components during total knee arthroplasty. J Bone Joint Surg Am 1997;79:1030-1039.
Clatworthy MG, Ballance J, Brick GW, et al: The use of structural allograft for uncontained defects in revision total knee arthroplasty: A minimum five-year review. J Bone Joint Surg Am 2001;83:404-411.
Question 81
A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result?
Explanation
REFERENCES: Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.
Cannata G, De Maio F, Mancini F, et al: Physeal fractures of the distal radius and ulna: Long-term prognosis. J Orthop Trauma 2003;17:172-179.
Ray TD, Tessler RH, Dell PC: Traumatic ulnar physeal arrest after distal forearm fractures in children. J Pediatr Orthop 1996;16:195-200.
Aminian A, Schoenecker PL: Premature closure of the distal radial physis after fracture of the distal radial metaphysis. J Pediatr Orthop 1995;15:495-498.
Question 82
What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?
Explanation
REFERENCES: Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis.
J Am Acad Orthop Surg 2006;14:376-385.
Kim SJ, Shin SJ, Choi NH, et al: Arthroscopic treatment for localized pigmented villonodular synovitis of the knee. Clin Orthop Relat Res 2000;379:224-230.
Question 83
A 17-year-old high school gymnast who has peripatellar knee pain has been unable to practice on a consistent basis for the past 3 years. She denies any specific injury events. Physical therapy for modalities, quadriceps strengthening, and hamstring stretching provide temporary relief. A trial of patellar taping significantly reduces her pain. Examination reveals an 15-degree Q angle, moderate lateral facet tenderness, negative patellar apprehension, and the inability to evert the patella. Radiographs show a moderate lateral patellar tilt. Treatment should now consist of
Explanation
REFERENCES: Gambardella RA: Techical pitfalls of patellofemoral surgery. Clin Sports Med 1999;18:897-903.
Post WR: Clinical evaluation of patients with patellofemoral disorders. Arthroscopy 1999;15:841-851.
Question 84
If a percutaneous iliosacral screw is placed too anteriorly, and the screw exits anterior to the sacral ala before re-entering the sacral body, what will be the most likely finding postoperatively?

Explanation
Question 85
A 52-year-old man has pain in the sternal area after landing on his right shoulder in a fall from his bicycle. In addition, he reports that he had difficulty swallowing and breathing immediately after the fall, but the symptoms resolved. A CT scan reveals a posterior sternoclavicular dislocation. Initial management should include
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont IL, American Academy of Orthopaedic Surgeons, 1999, pp 287-297.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 1010-1017.
Question 86
When performing a revision total knee arthroplasty, trial components are inserted and the knee is stable in extension and loose in flexion. Which step should be taken to create a stable construct?
Explanation
The surgeon is facing a common scenario that occurs in revision knee surgery: a loose flexion gap with an appropriate extension gap. A flexion gap can be tightened by translating the femoral component more posteriorly and using an oversized femoral component. Insertion of a thicker tibial component changes both the flexion and extension gap. Augmentation of the distal femur tightens only the extension gap. A constrained insert would only be indicated if oversizing of the femoral component did not adequately tension the flexion gap.
Question 87
When posterior fusion with instrumentation to the sacrum is used to treat adult scoliosis, what instrumentation technique best increases the chance of a successful lumbosacral fusion?
Explanation
REFERENCES: Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173.
O’Brien N, et al: Sacral pelvic fixation and spinal deformity, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 601-614.
McCord DH, Cunningham BW, Shono Y, et al: Biomechanical analysis of lumbosacral fixation. Spine 1992;17:S235-S243.
Question 88
Figure 1 is the MRI scan of a 35-year-old female soccer player who injured her knee during a game. Given the findings of the scan, physical examination is most likely to reveal
Explanation
Question 89
03 A patient with carpometacarpal joint arthritis of the thumb undergoes trapezium excision and interposition arthroplasty. One year after treatment, radiographs reveal that there has been 25% subsidence of the thumb metacarpal compared with its preoperative height. This degree of subsidence will have what effect on the surgical outcome?
Explanation
pinch stress causes a large amount of axial compressive force through the CMC joint. They also compared preoperative and postoperative functional measurements, including key pinch strength, tipto-tip pinch strength, grip strength, and thumb ROM. Their findings were that postoperatively the first metacarpal subsided 21% at rest (p=0.001). and it subsided another 10.5% during maximal lateral key pinch. Even with this degree of subsidence, the patients experienced increases in pinch strength and grip strength. Also, all patients except for one who had bony impingement reported that they were subjectively much better and more functional.
Lin et. al. also studied trapezium excision and interposition arthroplasty and found no significant differences between results in patients with varying degrees of subsidence. Thus, subsidence does not affect the results of interposition arthroplasty for basal thumb arthritis.
back to this question next question
Question 90
What do the T2-weighted, fat-saturated MRI scans shown in Figures 1 through 4 reveal?

Explanation
disruption of the ACL. The medial meniscus images show a disruption of normal meniscus morphology consistent with a bucket handle medial meniscus tear. Note the appearance on the sagittal MRI scan of what appears to be a second soft-tissue density in line with the PCL. This "double PCL" sign is highly indicative of a displaced medial meniscus tear rather than a displaced lateral meniscus tear.
Question 91
- Examination of a 45 year old construction worker who was crushed by falling dirt and buried to midchest level reveals hemodynamic instability; however, radiographs of the chest are normal, and results of a diagnostic peritoneal lavage are negative. Despite the administration of a fluid bolus and packed red blood cells, hemodynamic instability persists. A radiograph of the pelvis is shown in Figure 4. The next step in the management should be
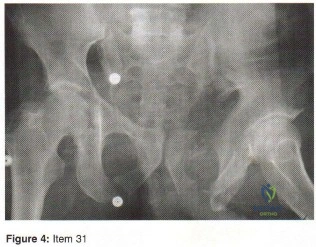
Explanation
Question 92
below show the radiographs, MRI, and MR arthrogram obtained from a year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. What is the primary cause of a cam deformity?
Explanation
Question 93
During head-on motor vehicle collisions occurring at highway speeds, airbag-protected individuals have a decreased rate (as compared to non-airbag protected individuals) of all of the following EXCEPT:

Explanation
Question 94
- A 25-year-old patient who was wearing a seat belt in the back chair of a car involved in a head-on collision undergoes a laparotomy. During surgery, an injury to the sigmoid colon is identified and treated. Two days later the patient has back pain when sitting in a chair. What is the most likely diagnosis?
Explanation
Question 95
Two years ago, a 63-year-old man underwent right total hip arthroplasty (THA) with a modular femoral head-neck and neck-stem prosthesis (a photograph of the removed implant is shown in Figure 181). He now has increasing hip pain. Radiographs reveal a stable hip arthroplasty and elevated serum cobalt and chromium levels. MR imaging is obtained, and, based on these findings, the patient’s hip is revised. Which corrosion type likely is responsible for this THA failure?
Explanation
Micromotion at the femoral head-neck or stem-neck junction can lead to fretting corrosion. Fretting corrosion is among the most common causes of failure in modular components. Modularity gives surgeons additional intraoperative flexibility but has resulted in corrosion-related failure and an implant recall. Although titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer, resulting in fretting corrosion. This may eventually lead to excessive metal ion formation and painful synovitis that necessitates a revision procedure. Galvanic corrosion is attributable to a mismatch in electrochemical gradients between dissimilar metals. Crevice or pitting corrosion occurs in fatigue cracks because of differences in oxygen tension.
Question 96
A 14-year-old boy is involved in a motor vehicle accident and sustains the injury shown in Figures 18a and 18b. What is the most likely diagnosis? Review Topic

Explanation
Question 97
Video 1 shows a 20-year-old right-hand dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted. What is the most appropriate course of treatment?
Explanation
A. Abductor pollicis longus reconstruction with palmaris autograft
B. Extensor pollicis brevis repair
C. Extensor pollicis longus (EPL) repair
D. Extensor indicis proprius (EIP) to extensor pollicis longus tendon transfer
The EPL is the only tendon that will lift a thumb off of a table as described. It is the most frequently ruptured tendon associated with distal radius fractures. Rupture is more common with nondisplaced fractures. Rupture after a nondisplaced or minimally displaced fracture suggests an ischemic etiology. The patient will not be able to lift her thumb off of a table with her hand lying flat, palm-down. Direct repair is often difficult because of retraction of tendon ends, atrophy, and fraying. The EIP has a similar amplitude and direction of pull. Prerequisites for the use of the EIP to EPL tendon transfer include independent extension of the index finger.
15- Figure 1 is the clinical photograph of a very functional 17-year-old boy with cerebral palsy and quadriplegia. He has no active supination but has full passive supination. His ability to determine position and sensibility without visual input are good. Radiographs show no osseous malalignment. Which treatment can best improve this patient's function?
A. Physical therapy for supination strengthening
1- Figures 1 through 3 are the radiographs of a 40-year-old woman who sustained a minor injury to her left ring finger. Prior to this injury she was asymptomatic, but she now notes pain and swelling. What is the best course of treatment?
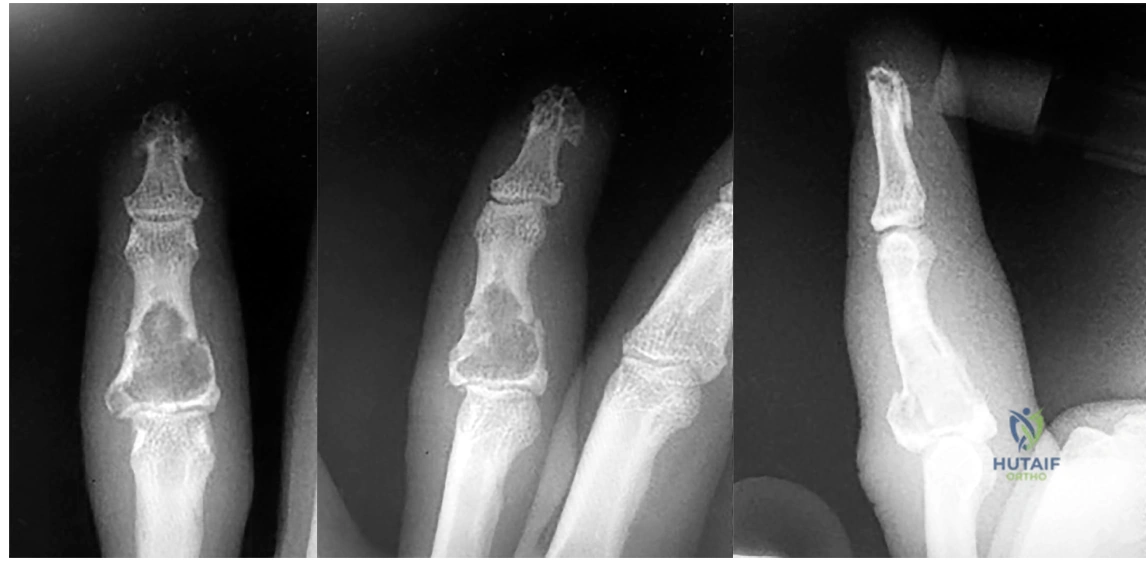
A. Observation only
B. Fluoroscopic-guided intralesional steroid injection followed by serial radiographs
C. Immediate curettage without bone grafting
D. Splint immobilization with curettage and possible grafting after the fracture has healed
This patient has a fracture of the middle phalanx attributable to the presence of an enchondroma. Enchondromas are the most common benign bone tumor affecting the hand. This particular enchondroma has thinned the cortices extensively so that even minor trauma can cause a pathologic fracture. Observation is not the best treatment because a fracture is present, and, at a minimum, the digit should be immobilized.
Question 98
A 65-year-old woman fell onto her outstretched right arm and immediately had pain. She has a history of osteoporosis. Examination of the right arm reveals lateral arm swelling, ecchymosis, and she is unable to move the elbow due to pain. Her neurovascular status is intact. Radiographs are shown in Figures 14a and 14b. Appropriate treatment should include
Explanation
REFERENCES: Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Beredjiklian PK, Nalbantoglu U, Potter HG, et al: Prosthetic radial head components and proximal radial morphology: A mismatch. J Shoulder Elbow Surg 1999;8:471-475.
Question 99
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman test with a soft endpoint, varus laxity at 30°, and a positive dial test at 30° that dissipates at 90° of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
Explanation
Question 100
Figure 49 shows an acute axial MRI scan of a right knee. What is the most likely diagnosis? Review Topic
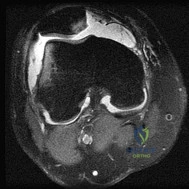
Explanation
