Orthopedic Board Review MCQs: Spine, Knee & Tendon | Part 176

Key Takeaway
This page presents Part 176 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review. It features 100 verified, high-yield MCQs, formatted like actual exams. Tailored for orthopedic residents and surgeons, it offers interactive study and exam modes to master critical topics for board certification success.
About This Board Review Set
This is Part 176 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 176
This module focuses heavily on: Deformity, Knee, Spine, Tendon.
Sample Questions from This Set
Sample Question 1: A 21-year-old collegiate wrestler sustains a blow to his right eye during a match. Examination reveals anisocoria with a dilated right pupil. The globe is properly formed, and extra-occular movements and the visual field are grossly intact....
Sample Question 2: Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?...
Sample Question 3: A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?...
Sample Question 4: During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?...
Sample Question 5: A 13-year-old girl is referred for a painful progressive valgus deformity of the right knee. Examination reveals an antalgic gait with an obvious valgus deformity. The right distal femur has a palpable, tender mass with erythema and warmth....
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 21-year-old collegiate wrestler sustains a blow to his right eye during a match. Examination reveals anisocoria with a dilated right pupil. The globe is properly formed, and extra-occular movements and the visual field are grossly intact. What is the most likely diagnosis?
Explanation
REFERENCES: Brucker AJ, Kozart DM, Nichols CW, Irving MR: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby Year Book, 1991, pp 650-670.
Orlando RG, Doty JH: Ocular sports trauma: A private practice study. J Am Optom Assoc 1996;67:77-80.
Question 2
Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?
Explanation
REFERENCES: Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 351-360.
Inaba K, Kirkpatrick AW, Finkelstein J, et al: Blunt abdominal aortic trauma in association with thoracolumbar spine fractures. Injury 2001;32:201-207.
Question 3
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?
Explanation
REFERENCES: Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539.
Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than
2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
Robinson CM, Court-Brown CM, McQueen MM, et al: Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am
2004;86:1359-1365.
Question 4
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Edwards TB, Walch G, Sirveaux F, et al: Repair of tears of the subscapularis. J Bone Joint Surg Am 2005;87:725-730.
Question 5
A 13-year-old girl is referred for a painful progressive valgus deformity of the right knee. Examination reveals an antalgic gait with an obvious valgus deformity. The right distal femur has a palpable, tender mass with erythema and warmth. Figures 4a and 4b show a clinical photograph and a radiograph. Management should consist of
Explanation
REFERENCES: Enneking W: Principles of musculoskeletal oncologic surgery, in Evarts C (ed): Surgery of the Musculoskeletal System. New York, NY, Churchill Livingston, 1990.
Herring JA: General principles of tumor management, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, from the Texas Scottish Rite Hospital for Children, ed 3. Philadelphia, PA, WB Saunders, 2002, pp 1897-1900.
Question 6
Figure 14 shows the clinical photographs and radiograph of an 8-year-old girl who has a progressive equinus deformity of the right ankle. There is no history of trauma or infection. What is the most likely diagnosis?
Explanation
REFERENCE: Bottoni CR, Reinker KA, Gardner RD, Person DA: Scleroderma in childhood: A 35-year history of cases and review of the literature. J Pediatr Orthop 2000;20:442-449.
Question 7
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
REFERENCES: O’Driscoll SW, Morrey BF: Elbow arthroscopy, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 21-34.
Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 8
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Explanation
REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Johnson RM, McGuire EJ: Urogenital complications of anterior approaches to the lumbar spine. Clin Orthop 1981;154:114-118.
Question 9
Figures 38a and 38b
Explanation
Inversion of the ankle can cause various injuries about the foot and ankle, all via the same mechanism. Fifth metatarsal base avulsion (Figure 35) fractures can be treated with use of a walking boot until pain subsides. Jones fractures (Figure 36) can be treated with surgical or nonsurgical treatment, although young, active patients are perhaps better treated with ORIF, which can decrease disability time. Treatment of an anterior process calcaneus fracture (Figure 37) is similar to that for a fifth metatarsal base avulsion fracture. Figures 38a and 38b show a calcaneal fracture-dislocation, which necessitates ORIF.
RECOMMENDED READINGS
Schepers T, Backes M, Schep NW, Carel Goslings J, Luitse JS. Functional outcome following a locked fracture-dislocation of the calcaneus. Int Orthop. 2013 Sep;37(9):1833-8. PubMed PMID: 23959223. View Abstract at PubMed
Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. View Abstract at PubMed
Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. View Abstract at PubMed
Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. View Abstract at PubMed
Question 10
Figure 48 shows an MRI scan of the knee. The arrow is pointing to what structure?
Explanation
REFERENCES: Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea and Febiger, 1918, 2000.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, pp 464-465.
Question 11
Which modality has the broadest application for the reduction of postsurgical transfusion?
Explanation
TXA is easy to administer, inexpensive, and safe for virtually all patients. Multiple studies have demonstrated transfusion rates lower than 3% for total knee arthroplasty and lower than 10% for total hip arthroplasty. Regional and hypotensive anesthesia effectively reduce transfusion; however, they cannot be used in as wide a range of patients as can TXA. A reduced transfusion trigger must be considered along with patient symptoms when determining the need for transfusion.
Question 12
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 13
A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of
Explanation
REFERENCE: Tasdemiroglu E, Tibbs PA: Long-term follow-up results of thoracolumbar fractures after posterior instrumentation. Spine 1995;20:1704-1708.
Question 14
An 11-year-old boy reports the acute onset of elbow pain and swelling after pushing his brother. The patient's mother and a younger sibling have experienced numerous fractures. You note that the patient and his mother have blue sclera and normal-appearing teeth. A radiograph of the elbow is shown in Figure 60. This patient's disorder is most likely the result of Review Topic

Explanation
Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). These individuals have blue sclerae, and although the initial fracture usually occurs in the preschool years, it may occur at any age. Furthermore, olecranon apophyseal fractures that occur after relatively minor trauma have been associated with type I OI. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. In this patient, there are no indications that the child has been subjected to abuse. Radiographs of the elbow show no evidence of osteopetrosis (due to abnormal osteoclast function) or rickets (due to a deficiency of vitamin D). Morquio syndrome (characterized by a defect of the enzyme N-Ac-Gal-6 sulfate sulfatase) is not associated with blue sclera.
Question 15
-The center of rotation of the knee can be best described as
Explanation
Question 16
What is the most likely contributory factor to this patient's problem?
Explanation
Proximal humeral epiphysiolysis (little leaguer’s shoulder) is an overuse condition of the proximal humeral physis. Patients report diffuse pain that is worse with throwing. Little leaguer’s shoulder is caused by rotational stress placed on the proximal humeral epiphysis during overhead throwing. The growth plate is weakest to torsion stress and is most susceptible to injury during periods of rapid growth commonly seen during puberty. Most chronic shoulder injuries occur in throwing athletes between 13 and 16 years of age. Factors that contribute to the condition include excessive throwing, improper throwing mechanics, and muscle-tendon imbalance. Radiographic findings typically are normal but may indicate subtle widening of the proximal humeral physis, and, in more severe cases, metaphyseal demineralization or fragmentation. Surgical fixation is not required for healing. An initial 3-month period of rest and activity modification will typically result in resolution of symptoms. Nonsteroidal anti-inflammatory drugs may be used as needed. After the rest period, a gradual return to throwing is implemented until the patient’s condition returns to baseline. This protocol has a long-term success rate exceeding 90%. Pitching coaches should evaluate throwing mechanics and maintain pitch counts. The most common cause of this condition is overuse, as is seen in pitchers who throw all year. Internal rotation deficit and internal impingement is typically a finding in older athletes without open physes. This patient had no evidence of rotation deficit upon examination, making this diagnosis unlikely.
Question 17
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
REFERENCES: Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 18
Figure 1 is the radiograph of a 22-year-old man who underwent an open reduction and pinning of a perilunate dislocation 10 weeks ago. The hardware has been removed. What is the best next step?
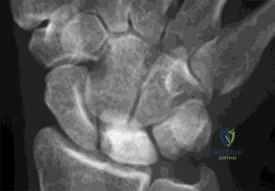
Explanation
Lunate or perilunate dislocations are usually treated with open reduction and internal fixation through a dorsal or combined dorsal and volar approach. A high index of suspicion is necessary when treating patients who sustain multiple trauma because as many as 25% of lunate or perilunate dislocations are missed initially. The radio dense appearance of the lunate seen in Figure 1 is an example of transient ischemia of the lunate that can occur following treatment of lunate and perilunate dislocations. It has been reported in up to 12.5% of cases. This usually is seen between 1 and 4 months post injury with a relative radio density of the lunate. This appearance of the lunate should not be over treated and usually is a benign self-limiting event. Surgery is not indicated at this time; the incorrect responses are treatment options for Kienbock disease. Treatment of the lunate or perilunate dislocation involves initial gentle closed reduction followed by open reduction, ligamentous and bone repair, and internal fixation. Median nerve dysfunction is common, and a simultaneous carpal tunnel release is often performed. Early treatment seems to produce better results, but good results have been reported when treatment is delayed for up to 6 months. The many questions regarding treatment of this problem involve the use of capsulodesis to supplement intercarpal ligament repair, repair/stabilization of the lunotriquetral interval vs no treatment of that articulation, and intercarpal fixation techniques. In delayed cases, proximal row carpectomy when the head of the capitate is intact and total wrist fusion if there are degenerative changes have been used. Chondral injuries are common, may not be recognized on radiographs, and may negatively affect longterm outcomes. Even when treatment is optimal, this injury is associated with a guarded prognosis and possible permanent partial loss of wrist motion and grip strength. At 10-year follow-up, radiographs will often demonstrate degenerative changes, but these changes do not always substantially negatively affect hand function.
Question 19
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?
Explanation
Question 20
A Trendelenburg gait is most likely to be seen in association with
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Andersson GB, Deyo RA: History and physical examination in patients with herniated lumbar discs. Spine 1996;21:10S-18S.
Question 21
A 23-year-old woman has had vague left knee pain for the past 6 months. A radiograph and CT scan are shown in Figures 50a and 50b. What is the most likely diagnosis?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 185-196.
Okada K, Frassica FJ, Sim FH, Beabout JW, Bond JR, Unni KK: Parosteal osteosarcoma. A clinicopathological study. J Bone Joint Surg Am 1994;76:366-378.
Question 22
A 5-year-old boy has had midfoot pain with activity for the past 3 months. He has no pain at rest. Radiographs are shown in Figures 29a and 29b. Management should consist of
Explanation
REFERENCE: Williams GA, Cowell HR: Koehler’s disease of the tarsal navicular. Clin Orthop 1981;158:53-58.
Question 23
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time? Review Topic
Explanation
Question 24
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Explanation
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 25
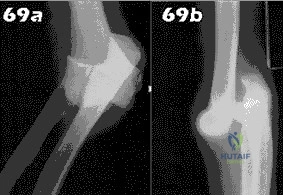
- Following closed reduction for the injury shown in Figures 69a and 69b, treatment should consist of
Explanation
Repair or reconstruction of the medial and lateral collateral ligaments-Acute dislocations can be reduced in supination and tested for valgus stability in pronation. Treatment is determined by the stability following reduction. When there are fractures, the principle is to fix the bones so that the only limitation is the ligaments and then to repair them if the elbow is not stable enough to permit early motion.
Immobilization for 14 days-The longer the immobilization had been, the larger the flexion contracture (p less than 0.001) and the more severe the symptoms of pain were. The results indicate that early active motion is the key factor in rehabilitation of the elbow after a dislocation. Simple dislocation of the elbow in the adult. Results after
closed treatment. Immobilization for 25 days- See above.
Question 26
BMP is FDA approved for well-defined medical conditions in limited patient populations. In which of the following clinical scenarios is use of rhBMP-2 FDA approved?
Explanation
rhBMP-2 is also FDA approved for use in open tibial shaft fractures stabilized with an IM nail and treated within 14 days of initial injury. rhBMP-7 has received FDA humanitarian device exemption approval as an alternative to autograft in recalcitrant long bone nonunions where use of autograft is unfeasible and alternative treatments have failed. It is also approved as an alternative to autograft in compromised patients (with osteoporosis, smoking or diabetes) requiring revision posterolateral/intertransverse lumbar fusion for whom autologous bone and bone marrow harvest are not feasible or are not expected to promote fusion.
Epstein reviewed the indications for rhBMP-2 use and its off-label use. She found that
anterior cervical surgery with BMP2 led to dysphagia and airway complications. With posterior lumbar spine surgery, complications included vertebral osteolysis (bone resorption) and ectopic bone formation/heterotopic ossifications, which made revision surgery difficult.
Burkus et al. prospectively compared 46 patients undergoing single-level ALIF with BMP-2 vs with autograft in an industry sponsored study. They found that patients receiving BMP-2 had higher rates of fusion and improvement in pain and neurologic status at 12 and 24 months compared with autograft, and there were no adverse events. They recommend rhBMP-2 in ALIF procedures to eliminate pain and scarring from iliac crest bone harvest.
Illustration A shows the FDA approved combination of INFUSE (rhBMP-2) and LT-CAGE device.
Incorrect Answers:
Question 27
A 12-year-old girl has scoliosis at T5-T10 that measures 62°. A clinical photograph of the axilla is shown in Figure 56. Management should consist of
Explanation
REFERENCES: Goldberg Y, Dibbern K, Klein J, Riccardi VM, Graham JM Jr: Neurofibromatosis type 1: An update and review for the primary pediatrician. Clin Pediatr 1996;35:545-561.
Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Question 28
Compared with percutaneous pinning with Kirschner wires (K-wires), the treatment of metacarpal neck fractures with cannulated intramedullary screws is associated with
Explanation
In a biomechanical study, headless compression screws showed superior load to failure, higher three-point bending strength, and greater strength in axial loading compared with percutaneous K-wire fixation for metacarpal neck fractures. Headless compression screws provide greater initial stability to allow earlier motion in the postoperative period. No data comparing infection rates between the two methods of fixation are available; however, it is assumed that K-wires placed outside of the skin would have increased rates of infection. Neither fixation method would increase the time to healing.
Question 29
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child’s back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of
Explanation
REFERENCES: McMaster MJ: Occult intraspinal anomalies and congenital scoliosis. J Bone Joint Surg Am 1984;66:588-601.
Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
McMaster MJ, David CV: Hemivertebrae as a cause of scoliosis: A study of 104 patients.
J Bone Joint Surg Br 1986;68:588-595.
Question 30
A research study is initiated on 500 patients undergoing total hip arthroplasty. The patients are followed and outcome is assessed according to body mass index (BMI). The effects of BMI on outcome should be reported as which of the following?
Explanation
Question 31
A 19-year-old woman has had a painful prominence on the lateral border of her fifth metatarsal head since she was a young girl. Nonsurgical management, including the use of a wide toe box shoe, has failed to provide relief. Examination reveals a callus over the lateral prominence and on the plantar portion as well. A clinical photograph and a radiograph are shown in Figures 34a and 34b. Treatment should consist of
Explanation
REFERENCES: Shereff MJ, Yang QM, Kummer FJ, Frey CC, Greenidge N: Vascular anatomy of the fifth metatarsal. Foot Ankle 1991;11:350-353.
Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Kitaoka HB, Holiday AD Jr: Metatarsal head resection for bunionette: Long-term follow-up. Foot Ankle 1991;11:345-349.
Question 32
A year-old patient fell 3 weeks after undergoing a total hip arthroplasty using cementless fixation of the femoral component. She sustained a comminuted Vancouver type B-2 fracture with displacement of the calcar fragment. What is the best treatment option?
Explanation
The patient has an acute postoperative fracture of the proximal femur with subsidence. It is also common that the stem retroverts relative to the femur. It is most often seen in proximally porous coated stems within 90 days of surgery, one paper found it to occur 0.7% of the time in modern implants. There is always a debate whether this is a missed intraoperative fracture, or a new fracture that has resulted from an event of increased hoop stresses. Removal of the primary stem, placement of a diaphyseal engaging
stem (most frequently a tapered-fluted stem), and cabling of the fracture is the most successful treatment.
Question 33
A 40-year-old woman underwent an arthroscopic acromioplasty and mini-open rotator cuff repair 4 weeks ago. At follow-up examination, the incision is painful, erythematous, and draining fluid. The patient is febrile and has an elevated WBC count. What infectious organism should be under high suspicion of causing this outcome?
Explanation
REFERENCES: Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 551-557.
Question 34
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include
Explanation
REFERENCES: Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141.
Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Hak DG, Lee SS, Goulet JA: Success of exchange reamed intramedullary nailing for femoral shaft nonunion or delayed union. J Orthop Trauma 2000;14:178-182.
Question 35
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
REFERENCE: O’Driscoll SW, Jaloszynski R, Morrey BF: Origin of the medial ulnar collateral ligament. J Hand Surg Am 1992;17:164-168.
Question 36
A professional baseball team has several pitchers with complaints of velocity loss with their pitches and shoulder pain of their dominant shoulders during spring training. Pitch counts are properly monitored. The average glenohumeral internal rotation deficit on the pitching staff is 45 degrees. The best intervention would be: Review Topic
Explanation
GIRD is a phenomenon that is frequently found in high-level overhead throwing athletes, predominantly baseball pitchers. It is defined as the measured difference in internal rotation between the non-dominant arm and dominant arm. Worsening range of motion deficits are seen with increased repetitions, both over a single season and a career. GIRD > 25º is associated with development of shoulder pathologies or pain requiring periods of inactivity. Cessation of overhead throwing activities and initiation of a stretching program to address posterior capsular contractures is largely effective (90% in some series).
Burkhart et al. reviewed the conditions associated with high-level overhead throwing athletes shoulders, culminating in a theory of pathologic progression to "dead arm syndrome" (loss of velocity and effective pitching). Their theory attributes adaptive hyperexternal rotation (occurs during late-cocking / early acceleration phases of pitching) to lead to posterior-inferior capsular contracture and GIRD. Subsequent injuries to anterior structures - including SLAP lesions - would then occur.
Illustration A is a cartoon depiction of how to perform the sleeper stretch. This is a common component of a pitcher's maintenance stretching program.
Incorrect Answers:
Question 37
Figures 12a through 12e show the radiograph, MRI scans, and biopsy specimens of a 17-year-old boy. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999,
pp 247-263.
Question 38
A 57-year-old man has had a 2-week history of neck pain. He has no history of radiating symptoms, and has no complaints of numbness or paresthesias. There was no trauma associated with the onset of the pain. Figure 26 shows the MRI scan initially obtained by his family physician. What should the patient be told regarding the prevalence of the MRI findings in his age group? Review Topic

Explanation
Question 39
A total shoulder arthroplasty (TSA) would be the most appropriate treatment in which of the following arthritic patients? Review Topic
Explanation
A TSA involves replacement of the humeral head with a metal head and resurfacing of the glenoid to a cemented all-polyethylene surface. In order to achieve optimal results, patients must be selected carefully. Patients with an irreparable rotator cuff tear, non-functioning deltoid, inadequate glenoid bone stock and brachial plexopathy
are poor candidates for TSA.
Edwards et al. conducted a multicenter randomized controlled trial to compare TSA versus hemiarthroplasty in patients with primary osteoarthritis of the shoulder. They found that TSA provided better scores for pain, mobility, and activity than hemiarthroplasty at 2 year follow-up.
Boileau et al. followed 45 consecutive patients who underwent reverse TSA (rTSA) for cuff tear arthropathy (CTA), post-traumatic arthritis, and failure of revision arthroplasty. After a mean follow-up of 40 months, they found that the reverse prosthesis improved function and was able to restore active elevation in patients with incongruent cuff-deficient shoulders. They also found that the results were less predictable and complication and revision rates were higher in patients undergoing revision surgery as compared to those patients undergoing rTSA for CTA.
Illustrations A and B show the preoperative and postoperative x-rays of a patient with characteristic OA of the glenohumeral joint that was treated with TSA.
Incorrect Answers:
Question 40
What structure is located at the tip of the arrow in Figure 18? Review Topic

Explanation
Question 41
- Which of the following shoulder girdle muscles is most active during forward flexion?
Explanation
Question 42
A 26-year-old man has recurrent right knee pain. Figures 9a and 9b show consecutive sagittal T2-weighted MRI scans, and Figure 9c shows a coronal T1-weighted MRI scan. What is the most likely diagnosis?
Explanation
The average width of a normal meniscus is less than 11 mm. A bow-tie appearance should not be seen on more than two consecutive sagittal images because the conventional thickness of the sagittal slices is 3 mm and the interval between two consecutive slices is 1.5 mm. Two sagittal slices will cover a 9-mm thickness. A discoid meniscus can be diagnosed on the sagittal views by noting a bow-tie appearance on more than two consecutive images.
REFERENCES: Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Mink JH, Deutsch AL: The knee, in MRI of the Musculoskeletal System, ed 1. New York, NY, Raven Press, 1990, pp 251-387.
Question 43
The Coleman block test is used to test for Review Topic
Explanation
Question 44
An 11-year-old child has a tibia-fibula fracture following a fall from a swing. The fracture is reduced and placed in a long leg splint in the emergency room. What is considered the most important symptom of a developing compartment syndrome of the leg?

Explanation
The Willis article also lists the most reliable signs of a developing compartment syndrome as severe pain with passive stretching of the involved compartment, pain with palpation of the involved compartment, sensory disturbances
Question 45
A 58-year-old woman sustained a ruptured Achilles tendon 1 year ago, and management consisted of an ankle-foot orthosis. She now reports increasing difficulty with ambulation and increasing pain. An MRI scan shows a 6-cm defect in the right Achilles tendon. Management should now consist of
Explanation
REFERENCE: Myerson MS: Achilles tendon ruptures. Instr Course Lect 1999;48:219-230.
Question 46
Figures 1 through 3 show the radiograph and MR arthrograms obtained from a 25-year-old woman who has had right groin pain since joining the military 4 years ago. She has undergone treatment with NSAIDs, physical therapy, and activity modification. Examination reveals positive flexion abduction and external rotation, a positive external log roll, and increased range of motion. What is the most appropriate treatment?

Explanation
This patient has symptomatic hip dysplasia that has been recalcitrant to nonsurgical management. Radiographs reveal an upsloping sourcil (acetabular index of 18) and a lateral center edge angle of 14, with posterior uncovering. The MR arthrogram shows no definitive evidence of a labral tear. Appropriate surgical management would include periacetabular osteotomy. Viscosupplementation in the hip is controversial in the treatment of osteoarthritis and plays no role in the treatment of dysplasia. Hip arthroscopy with labral repair is controversial in mild hip dysplasia, with studies demonstrating between 60% and 77% good and excellent results, inferior to the results for hip arthroscopy in a femoroacetabular impingement cohort. In moderate to severe dysplasia, hip arthroscopy is not recommended. Because the acetabular cartilage is well maintained, total hip arthroplasty would not be recommended in this young and active patient.
Question 47
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?
Explanation
REFERENCES: Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Johnson T, Steinbach L (eds): Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, p 44.
Question 48
A patient who sustained injuries in a motorcycle accident 30 minutes ago has significant motor and sensory deficits corresponding to a C6 level of injury. A lateral radiograph obtained during the initial on-scene evaluation reveals bilateral jumped facets at C5-C6; this appears to be an isolated injury. The patient is awake and alert. The next step in management of the dislocation should consist of
Explanation
REFERENCES: Delamarter RB, Sherman J, Carr JB: Pathophysiology of spinal cord injury: Recovery after immediate and delayed decompression. J Bone Joint Surg Am
1995;77:1042-1049.
Star AM, Jones AA, Cotler JM, Balderston RA, Sinha R: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets: Case report. J Bone Joint Surg Am
1991;73:1555-1560.
Question 49
A 58-year-old man has anterior knee pain after undergoing total knee arthroplasty for osteoarthritis 2 years ago. He denies any history of trauma. A Merchant view is shown in Figure 20. What is the most likely cause of his pain?
Explanation
REFERENCES: Reuben JD, McDonald CL, Woodard PL, Hennington LJ: Effect of patella thickness on patella strain following total knee arthroplasty. J Arthroplasty 1991;6:251-258.
Hsu HC, Luo ZP, Rand JA, An KN: Influence of patellar thickness on patellar tracking and patellofemoral contact characteristics after total knee arthroplasty. J Arthroplasty 1996;11:69-80.
Greenfield MA, Insall JN, Case GC, Kelly MA: Instrumentation of the patellar osteotomy in total knee arthroplasty: The relationship of patellar thickness and lateral retinacular release. Am J Knee Surg 1996;9:129-131.
Question 50
Long bone fracture repair following intramedullary stabilization occurs primarily through which of the following healing mechanisms?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 385-386.
Buckwalter JA, Einhorn TA, Bolander ME: Healing of the musculoskeletal tissues, in Rockwood CA Jr, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 261-276.
Question 51
9 degress Celsius, serum WBC is 14,000, and his C-reactive protein is elevated. He reports that he uses IV heroin. A coronal 3D CT scan of the left clavicle is shown in Figure B. Joint aspiration shows many grams stain positive organisms. Which of the following organisms is the most likely pathogen?
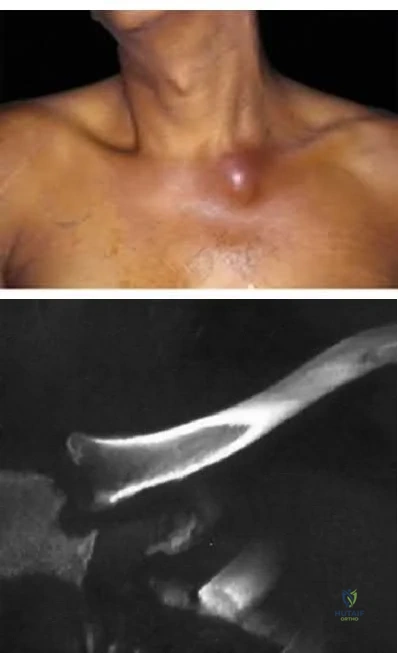
Explanation
Ross et al states "Staphylococcus aureus is now the major cause of
sternoclavicular septic arthritis in intravenous drug users. Pseudomonas aeruginosa infection in injection drug users declined dramatically with the end of an epidemic of pentazocine abuse in the 1980s."
The referenced article by Goldin et al is from the New England Journal of Medicine reports that all of their cases of SC joint septic arthritis were in intravenous drug abusers and that P. aeruginosa grew out of 3 patients and S. aureus grew out of 1 patient.
A more recent article by Abu Arab et al reported that Staph aureus was most common even in IV drug users. The review article by Higginbotham and Kuhn note that risk factors for SC joint septic arthritis include hemodialysis, immunocompromise, alcoholism, and HIV. Neisseria gonorrhoeae, fungal, and candida present in HIV patients.
Treatment is I&D and appropriate antibiotics, although aspiration and abx have shown some success too. CT and MRI are useful in diagnosis, and open biopsy or aspiration is recommended for definitive diagnosis.
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?
Degenerative lumbar spine changes
Ipsilateral ankle pain and stiffness
Ipsilateral hip joint degenerative changes
Contralateral hip joint degenerative changes
Ipsilateral medial knee degenerative changes Correct answer: 2
A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted
that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
A 33-year-old man sustains a femur fracture in a motorcycle accident. AP and lateral radiographs are provided in Figure A. Prior to surgery, a CT scan of the knee is ordered for preoperative planning. Which of the following additional findings is most likely to be discovered?

Tibial eminence fracture
Sagittal plane fracture of the medial femoral condyle
Schatzker I tibia plateau fracture
Coronal plane fracture of the lateral femoral condyle
Axial plane fracture through the medial femoral condyle Correct answer: 4
The "Hoffa fracture" is a coronal plane fracture of the femoral condyle that is often missed on plain radiographs of supracondylar and intercondylar femur fractures. It involves the lateral condyle more frequently than the medial.
Identification is important as it may impact operative planning and likely require screw fixation in the anteroposterior plane.
Nork et al. reviewed 202 supracondylar-intercondylar distal femoral fractures and found a 38% prevalence of associated coronal plane fractures. The authors recommend CT scan imaging of all supracondylar and intercondylar fractures.
Ostermann et al reported on 24 unicondylar fractures of the distal femur treated with open reduction internal fixation with a screw construct. Twenty-
three patients acheived satisfactory results at 5 year follow-up. Illustrations A and B are another example of a supracondylar femur fracture with an associated Hoffa fracture identified on CT scan.

A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
closed reduction and early range of motion
radial head resection and lateral collateral ligament reconstruction
radial head resection and coronoid open reduction internal fixation
radial head arthroplasty and coronoid open reduction internal fixation
radial head arthroplasty, coronoid open reduction internal fixation, and lateral collateral ligament repair
A terrible triad of the elbow includes dislocation of the elbow with associated fractures of the radial head and the coronoid process. Ring et al. stressed that these injuries are prone to complications and advised against resection of the radial head due to instability, and instead recommended a radial head replacement if too comminuted for ORIF. Coronoid fractures compromise elbow stability as well and require open reduction and internal fixation as with the lateral collateral ligament. McKee et al. showed stable elbows in 34/36 with mean Mayo elbow score of 88 when the standard protocol of coronoid ORIF, radial head repair/replacement, and LCL repair were employed.
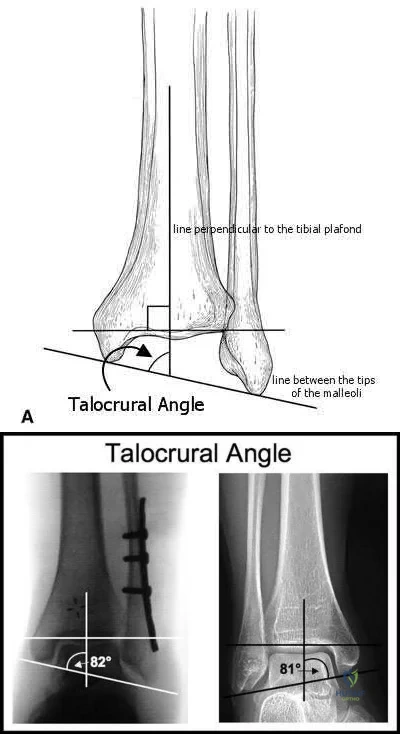
The talocrural angle of an ankle mortise x-ray is formed between a line perpendicular to the tibial plafond and a line drawn:
perpendicular to the medial clear space
parallel to the talar body
between the tips of the malleoli
perpendicular to the shaft of the fibular
parallel to the subtalar joint Correct answer: 3
The talocrural angle is formed by the intersection of a line perpendicular to the plafond with a line drawn between the malleoli (average = 83+/-4deg). When the lateral malleolus is shortened secondary to fracture, this can lead to increased talocrural angle. This malunion leads to lateral tilt of the talus.
Phillips et al looked at 138 patients with a closed grade-4 supination-external rotation or pronation-external rotation ankle fracture. Although the conclusions were limited due to poor follow up, they found the difference in the talocrural angle between the injured and normal sides was a statistically significant radiographic indicator of a good prognosis.
Pettrone et al looked at a series of 146 displaced ankle fractures, and the effect of open or closed treatment, and internal fixation of one or both malleoli. They found open reduction proved superior to closed reduction, and in bimalleolar fractures open reduction of both malleoli was better than fixing only the medial side.
Illustrations A and B are demonstrations of the talocrural angle.
A 33-year-old male sustains the injury shown in Figure A. He is initially treated with a spanning external fixator followed by definitive open reduction internal fixation of the tibia and fibula. His wounds healed without infection or other complications. Two years following surgery, which of the following parameters will most likely predict a poor clinical outcome and inability to return to work?

Joint line restoration
Degree of fracture displacement
Time before definitive ORIF
Open fracture
Lower level of education Correct answer: 5
Lower level of education is the parameter that correlated most closely with a poor clinical outcome and inability to return to work.
To determine what fracture- and patient-specific variables affect outcome, Williams et al evaluated 29 patients with 32 tibial plafond fractures at a minimum of 2 years from the time of injury. Outcome was assessed by four independent measures: a radiographic arthrosis score, a subjective ankle score, the Short Form-36 (SF-36), and the patient’s ability to return to work. The four outcome measures did not correlate with each other. Radiographic arthrosis was predicted best by severity of injury and accuracy of reduction. However, these variables did not show any significant relationship to the clinical ankle score, the SF-36, or return to work. These outcome measures were more influenced by patient-specific socioeconomic factors. Higher ankle
scores were seen in patients with college degrees and lower scores were seen in patients with a work-related injury. The ability to return to work was affected by the patient’s level of education.
Pollak et al performed a retrospective cohort analysis of pilon fractures. Patient, injury, and treatment characteristics were recorded. The primary outcomes that were measured included general health, walking ability, limitation of range of motion, pain, and stair-climbing ability. A secondary outcome measure was employment status. Multivariate analyses revealed that presence of two or more comorbidities, being married, having an annual personal income of less than $25,000, not having attained a high-school diploma, and having been treated with external fixation with or without limited internal fixation were significantly related to poorer results as reflected by at least two of the five primary outcome measures.
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?
Irrigation and local wound care in the emergency department
Emergent irrigation and debridement in the operating room with vacuum-assisted wound closure
Emergent irrigation and debridement in the operating room with 7 days of intravenous antibiotics
Wound closure in the emergency department with follow-up wound check in 1 week
Exploration and removal of all bullet fragments in the emergency department and 10 day course of oral antibiotics
The question refers to appropriate management of a gunshot wound to the forearm. The first question that must be answered when evaluating gunshot injuries is whether the gunshot is low velocity or high velocity. Low-velocity wounds are less severe, are more common in the civilian population, and are typically attributed to bullets with muzzle velocities below 1,000 to 2,000 feet per second. Tissue damage is usually more substantial with higher-velocity (greater than 2,000 to 3,000 fps) military and hunting weapons. In this question, a muzzle velocity of 1,000 ft/sec is provided. Low velocity injuries with stable, non-operative fractures can be treated with local wound care.
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds.
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?
pulselessness
pallor
paresthesia
paralysis
increasing analgesia requirement Correct answer: 5
Although pain, pallor, paresthesia, paralysis, and pulselessness are all possible signs and symptoms of compartment syndrome in children with fractures, studies have shown increasing analgesia requirement is more sensitive.
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of
compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
A 45-year-old man sustains the injury seen in Figures A and B following a motor vehicle accident. Postoperative radiographs are seen in Figures C and D. Which of the following is the most accurate when comparing outcomes between intramedullary nailing (IMN) and open reduction internal fixation (ORIF) for this injury?

Union rates at one year are higher with ORIF
Infection rates are higher with IMN
Functional shoulder outcomes at one year are equivalent with IMN and ORIF
Iatrogenic radial nerve injury rate is higher with ORIF
Shoulder stiffness rates at one year are equivalent with IMN and ORIF Correct answer: 3
Although shoulder pain and stiffness is increased following IMN compared to ORIF, functional outcome scores at one year have been shown to be equivalent
in both treatment groups.
Diaphyseal humeral shaft fractures outcomes following IMN and ORIF are under further investigation. Diaphyseal humeral shaft fractures have historically been treated with ORIF, however proponents for IMN cite benefits of less periosteal stripping and soft tissue dissection. Recent investigations have shown outcomes with regard to nonunion, infection, re-operation, and nerve palsy appear equivalent between both groups. Rates of shoulder stiffness and shoulder pain have been demonstrated to be higher in IMN compared to ORIF. American Shoulder and Elbow Scores (ASES) have shown no difference at one year post-operatively.
Bhandari et al. performed a meta-anaylsis of 3 prospective randomized trials. They found lower rates of re-operation and shoulder impingement with ORIF of humeral shaft fractures.
Wali et al. performed a prospective randomized study of IMN or ORIF on 50 patients with mid-diaphyseal humeral shaft fractures. They found IMN had shorter operative time, shorter hospital stay, and lower blood loss. They found no difference in union rates, complication, or shoulder functional outcomes scores. They conclude IMN to be an effective option for treating mid-diaphyseal humeral shaft fractures.
Heineman et al. have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF. The authors found no significant difference between the two treatment modalities for the secondary outcomes (nonunion, infection, nerve palsy, re-operation).
Figures A and B show a diaphyseal humeral shaft fracture. Figure C and D show postoperative radiographs following intramedullary nailing of a humeral shaft fracture.
Incorrect Answers:
A 25-year-old female presents complaining of progressive anteromedial pain in her left ankle. She underwent operative fixation 5 months prior at an outside hospital. The operative report indicated that, due to anterior fracture blisters, a direct medial incision was utilized, centered over the posterior colliculus of the medial malleolus, without violation of the deltoid ligament. A radiograph and computed tomographic scan of her initial injury are shown in Figures A and B, respectively. On exam, she has well-healed incisions, exhibits no tenderness to palpation over her hardware, but does endorse pain with deep palpation along the anteromedial joint line. Figure C shows an anteroposterior left ankle radiograph taken today. Labs are obtained and reveal a white blood cell count of 9.0 k/uL (reference range 4.5-11.0 k/uL) and a C-reactive protein value of 0.8 mg/dL (<0.9 mg/dL). What is the next best step in managing her problem?

Syndesmotic fixation
Intra-articular corticosteroid injection
Referral to physical therapy
Surgical correction of malunion
Removal of hardware Correct answer: 4
This patient sustained a supination-adduction (SAD) injury with a vertical shear fracture of her medial malleolus and a fibular avulsion fracture. She sustained a medial plafond articular impaction injury that was not addressed at the time of surgery.
In SAD injuries, supination of the foot is combined with inward rotation at the ankle, adduction of the hindfoot, and inversion of the forefoot. This results in the following sequence of events: 1. Talofibular sprain or distal fibular avulsion (equivalent to Weber A). 2. Vertical medial malleolus fracture as the talus strikes the tibia. Associated injuries may include osteochondral damage to the talus and marginal impaction of the medial plafond. It is important to evaluate the medial plafond for articular impaction. When present, an arthrotomy must be performed, typically utilizing an anteromedial incision, with direct visualization of the articular surface to restore the joint line appropriately.
Weber et al. provided a review article on corrective osteotomies for malleolar fracture malunions. They stress that malunions can lead to ankle instability, abnormal load transfer, and post-traumatic arthritis. They conclude that corrective osteotomies that restore anatomical alignment show good results in long-term follow-up.
Perera et al. provided additional commentary on the surgical reconstruction of malunited ankle fractures. The authors emphasize the link between malunion and poor outcomes. They state that successful salvage procedures involve a clear understanding of the deformity, careful preoperative planning, and a solid understanding of reconstructive techniques. They provide several instructive case examples in their review.
McConnell et al. provided a discussion on SAD ankle fractures at their institution and emphasized the importance of recognizing marginal impaction of the tibial plafond when treating these injuries. Of 800 ankle fractures identified over a 5-year period, 44 were SAD injuries, 19 of the 44 displayed a vertical shear fracture of the medial malleolus, and 8 of the 19 demonstrated marginal impaction of the tibial plafond. These 8 impaction injuries were treated with open reduction internal fixation with elevation of the articular impaction; all had good to excellent outcomes without arthritic changes at last
follow-up.
Figure A is an anteroposterior left ankle radiograph demonstrating a SAD injury with a vertical shear fracture of the medial malleolus, a fibular avulsion fracture, and articular impaction of the medial tibial plafond. Figure B is a coronal CT demonstrating articular impaction of the medial plafond. Illustration A is an intra-operative photograph with the medial malleolus retracted allowing inspection of the articular surface; mild anteromedial plafond impaction is present.
Incorrect Answers:

A 90-year-old female slips and falls at home. She is a community ambulator and has no medical problems. She reports right hip pain at this time. Injury radiographs are shown in Figures A & B. Delay of more than 48 hours may result in:

Increased intraoperative time
Increased 30-day mortality
No impact on the rate of postoperative pneumonia
Higher rates of blood transfusion
Increased risk of post-operative infection Correct answer: 2
Figures A & B demonstrate a right, unstable intertrochanteric femur fracture. Surgical stabilization within 48 hours improves short-term and 30-day mortality.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:

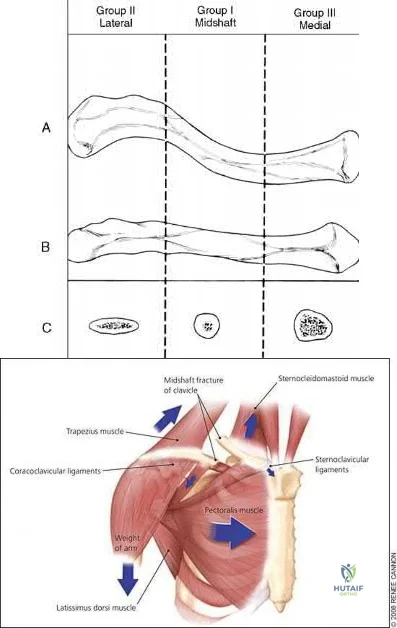
A 22-year-old healthy left hand dominant male presents to the ED with left shoulder pain after falling from an ATV. Figure A is the radiograph of his left clavicle. He is neurovascularly intact and there is no evidence of skin tenting or open fracture. Which of the following most predisposes this patient to nonunion?

Diaphyseal fracture
Fracture displacement
Age
Male Gender
Injury involving the dominant extremity Correct answer: 2
Displaced clavicle fractures are associated with higher rates of nonunion.
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
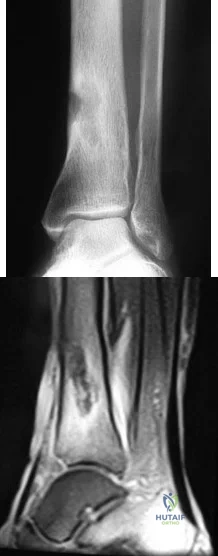
A 24-year-old male presents with ankle pain after being involved in a motor vehicle accident. His injury radiograph is shown in Figure A. Which of the following has been shown to contribute to the development of post-traumatic arthritis in this injury pattern?

Initial superficial zone cartilage cell death via apoptosis at the fracture margins
Initial superficial zone cartilage cell death via apoptosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis at the fracture margins
Delayed superficial zone cartilage cell death via necrosis at the fracture margins
Figure A demonstrates a tibial plafond fracture. Initial superficial zone cartilage cell death via necrosis at the fracture margins has been shown to contribute to post-traumatic arthritis.
Post-traumatic osteoarthritis typically occurs after an intra-articular fracture. Impacted chondrocytes die by either necrosis or apoptosis, which have both been implicated in post-traumatic osteoarthritis. Initial cell death in the superficial cartilage zones at the fracture margins occurs by necrosis. Apoptosis occurs in a delayed fashion and is mitigated by several bioactive agents.
Apoptosis also affects the superficial cartilage zones near the fracture margins. Deep cartilaginous zones and areas away from the fracture margins do not seem to be involved in these processes.
McKinley et al. performed a review of the basic science of intra-articular fractures and posttraumatic osteoarthritis. They report that initial damage to the cartilage in combination with the ensuing pathomechanical and pathobiologic response of the cartilage after a fracture contribute to posttraumatic arthritis. Chronic abnormal joint loading is also thought to contribute to this process as well. They conclude that the relative contribution of each is unknown.
Tochigi et al. performed a study to determine the distribution and progression of chondrocyte damage after intra-articular ankle fractures. They harvested 7 normal human ankles and subjected them to impaction. They found that immediate superficial zone chondrocyte death was greater in fracture-edge regions than on-fracture regions. Subsequent cell death over the next 48 hours was significantly higher in fracture-edge regions as well. They conclude that cartilage damage in intra-articular fractures was characterized by chondrocyte death at fracture margins.
Figure A is an ankle mortise radiograph demonstrating an intra-articular tibial plafond fracture.
Incorrect Answers:
A 35-year-old male presents with left knee pain after sustaining the injury seen in Figure A. He is neurovascularly intact and can perform a straight leg raise, but has pain with passive range of motion. Figures B and C show an anteroposterior and lateral radiograph of the left knee, respectively. 175 cc of saline is injected into the superolateral quadrant with no egress of fluid from the inferolateral
laceration. What percentage of traumatic arthrotomies would be detected with this test?

Question 52
In a retroperitoneal approach to the lumbar spine, what nerve is commonly found on the psoas muscle?
Explanation
REFERENCES: Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107.
Johnson R, Murphy M, Southwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Gray’s Anatomy. New York, NY, Bounty Books, 1977, pp 1226-1227.
Question 53
Which of the following primary prognostic factors best predicts the outcome of the knee lesion shown in Figure 22?
Explanation
REFERENCES: Stanitski CL: Osteochondritis dissecans of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 387-405.
Cahill B: Treatment of juvenile osteochondritis dissecans and osteochondritis dissecans of the knee. Clin Sports Med 1985;4:367-384.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
Question 54
A 49-year-old woman noted pain in her right axilla 1 day after moving heavy furniture. Two weeks later, she now reports persistent numbness and paresthesias along the inner aspect of her upper arm radiating into the ulnar digits. Examination reveals full shoulder motion, tenderness over the first rib, and a decreased radial pulse with the shoulder placed overhead. What is the most likely diagnosis?
Explanation
REFERENCES: Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Todd TW: The descent of the shoulder after birth: Its significance in the production of pressure-symptoms on the lowest brachial trunk. Anat Anz 1912;41:385-397.
Question 55
An 85-year-old obese woman has left knee pain. She had surgery 5 years ago for a patellar nonunion after total knee arthroplasty that was complicated by infection, which was treated with implant removal and patellectomy. She has not been ambulatory since then. She states she is no longer on antibiotics. She has moderate pain, but her primary problem is instability of the knee. She has a 40° extensor lag. Darkening of the skin is present distal to the incision consistent with venous stasis changes. The erythrocyte sedimentation rate is 12 mm/h (reference range 0 to 20 mm/h) and her C-reactive protein level is 1.0 mg/L (reference range 0.08 to 3.1 mg/L). Left knee aspiration shows a white blood cell count of 800 and 20% neutrophils. What is the best next step?
Explanation
This patient is elderly, obese, and nonambulatory and has a chronic quadriceps tendon rupture after infected total knee arthroplasty. Her potential for ambulation after revision total knee arthroplasty is very low. Primary repair of the tendon is unlikely to be successful, even with augmentation, so revision total knee arthroplasty with primary quadriceps tendon repair and two-stage revision knee arthroplasty and quadricep repair with Achilles allograft are not the best management techniques. Extensor mechanism allograft could be done but would have a high failure rate in a patient of this size. No sign of infection is seen, based on laboratory studies, so a two-stage procedure is not necessary. The best management although not optimal, would be treatment in a drop-lock brace. Arthrodesis is also an option, but would have a high complication rate, and in a patient that is nonambulatory, a fused knee would be increasingly
difficult with activities of daily living and mobility.
Question 56
A 46-year-old woman reports pain and a shortened appearance of her toe after undergoing a Keller resection arthroplasty 2 years ago for hallux rigidus. Examination reveals mild swelling and motion limited to 25 degrees at the metatarsophalangeal joint. Radiographs show large dorsal osteophytes on the first metatarsal head, 50% resection of the proximal phalanx, and complete loss of the metatarsophalangeal joint space. Which of the following is considered the most reliable procedure to improve her pain and the appearance of her toe?
Explanation
REFERENCES: Myerson MS, Schon LC, McGuigan FX, Oznur A:Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306.
Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 252-253.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 293-303.
Question 57
A 13-year-old girl with Down syndrome has bilateral chronic patellar dislocations. She denies knee pain. She is able to straighten her knees and walks with a symmetric but awkward gait. She does not flex her knees in midstance. Examination reveals that the patellae cannot be brought into a reduced position. Management should consist of
Explanation
REFERENCES: Dugdale TW, Renshaw TS: Instability of the patellofemoral joint in Down syndrome. J Bone Joint Surg Am 1986;68:405-413.
Mendez AA, Keret D, MacEwen GD: Treatment of patellofemoral instability in Down’s syndrome. Clin Orthop 1988;234:148-158.
Question 58
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. This patient elects nonsurgical treatment and later experiences persistent instability. Examination reveals an asymmetric Dial test finding and a varus thrust during ambulation. Which osteotomy and correction appropriately addresses this chronic instability pattern?

Explanation
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 59
What is the most common non-anesthetic-related reversible cause of sustained changes in intraoperative neurophysiologic monitoring signals during spinal surgery? Review Topic
Explanation
Question 60
A 72-year-old woman underwent a primary total hip arthroplasty 14 months ago. She states that the hip has now dislocated four times when rising from a low chair, requiring closed reduction. A radiograph is shown in Figure 3a and a CT scan of her pelvis is shown in Figure 3b. What is the most reliable method for rectifying her instability?
Explanation
will most reliably rectify the instability in the face of severe component malposition.
REFERENCES: Parvizi J, Picinic E, Sharkey PF: Revision total hip arthroplasty for instability: Surgical techniques and principles. J Bone Joint Surg Am 2008;90:1134-1142.
DeWal H, Su E, DiCesare PE: Instability following total hip arthroplasty. Am J Orthop 2003;32:377-382. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3.
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475-503.
Question 61
Which of the following statements most accurately describes the layers of articular cartilage?
Explanation
REFERENCE: Schiller AL: Pathology of osteoarthritis, in Kuettner KE, Goldberg VM (eds): Osteoarthritic Disorders. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995,
pp 95-101.
Question 62
What clinical finding is associated with the least favorable prognosis in an adolescent patient who has been diagnosed with a high-grade osteosarcoma of the distal femur?
Explanation
REFERENCE: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlation. Philadelphia, PA, Lea and Febiger, 1989, pp 344-350.
Question 63
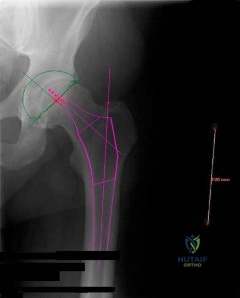
Figure below depicts the radiograph obtained from a 30-year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of Figure below reveals
Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 64
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Warner JJ, Johnson D, Miller M, Caborn DN: Technique for selecting capsular tightness in repair of anterior-inferior shoulder instability. J Shoulder Elbow Surg 1995;4:352-364.
Question 65
A 10-year-old boy with spastic diplegic cerebral palsy walks in a crouched position with the hips and knees flexed. Maximum knee flexion is 15 degrees during early swing phase. Instrumented gait analysis shows quadriceps activity from terminal stance throughout swing phase. Treatment should consist of
Explanation
REFERENCES: Aiona MD: Guidelines for managing lower extremity problems in cerebral palsy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1534-1541.
Chambers H, Laure A, Kaufman K, Cardelia M, Sutherland D: Prediction of outcome after rectus femoris surgery in cerebral palsy: The role of cocontraction of the rectus femoris and vastus lateralis. J Pediatr Orthop 1998;18:703-711.
Ounpuu S, Muik E, Davis RB, Gage JR, Deluca PA: Rectus femoris surgery in children with cerebral palsy. J Pediatr Orthop 1993;13:331-335.
Question 66
Figures 2a and 2b show the clinical photograph and radiograph of a 16-year-old cheerleader who fell on her left lower extremity while performing a pyramid. Following adequate sedation, closed reduction is performed, but an incomplete reduction is noted. What structure is most likely preventing a reduction?
Explanation
REFERENCES: Pehlivan O, Akmaz I, Solakoglu C, et al: Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-543.
Rivera F, Bertone C, De Martino M, et al: Pure dislocation of the ankle: Three case reports and literature review. Clin Orthop 2001;382:179-184.
Question 67
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
REFERENCES: Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Wholey MH, Browner AJ, Baker HL Jr: The lateral roentgenogram of the neck: With comments on the atlanto odontoid-basion relationship. Radiol 1958;71:350-356.
Question 68
A patient has a C6-7 herniated nucleus pulposus. What is the most likely distribution of symptoms? Review Topic
Explanation
(SBQ12SP.27) A 24-year-old male sustains the injury shown in Figure A. What was the most likely mechanism of injury? Review Topic

Hyperextension
Flexion-distraction
Flexion-compression
Rotational
Pure axial load
Figure A shows a quadrangular fracture pattern of C5. These injuries are observed with flexion-compression loads.
Quadrangular fractures of the cervical spine are considered flexion teardrop fractures. However, they present with a larger anterior lip fragment compared to the classic teardrop fracture pattern. The radiographic findings include a quadrangular-shaped fragment from the anterior one-third of the vertebral body with significant posterior vertebral subluxation, angular kyphosis, and an increased interspinous space with facet subluxation due to disruption of the posterior elements. These are unstable fractures, and almost always require anterior and posterior stabilization.
Moore et al. studied the reliability of Cervical Spine Injury Severity Score to measure stability after cervical spine trauma. The classification system is based on morphologic descriptions and, secondly, on stability based on a quantifiable value. They showed that the Cervical Spine Injury Severity Score had excellent reliability with intra-observer intraclass correlation coefficients (ICC) >0.97 and inter-observer ICC >0.88.
Vaccaro et al. published the subaxial cervical spine injury classification system (SLIC). This systems involves 3 main categories (injury morphology, disco-ligamentous complex, and neurologic status). The overall injury severity score is obtained by summing the scores from each category. They propose that SLIC < 4 can be treated non-operatively.
Allen et al. published a classification system of cervical spine injuries which breaks injuries of the subaxial spine into six phylogenic groups based on mechanism of injury. These include: 1) flexion-compression 2) vertical-compression 3) flexion-
distraction 4) extension-compression 5) extension-distraction 6) lateral flexion. Facet
dislocation
is
caused
by
flexion-distraction
force.
Figure A shows a lateral radiograph of the cervical spine demonstrating a typical flexion-compression fracture with anteriorly displaced quadrangular fragment. Illustration A shows a flexion-compression injury. Illustration B shows the mechanism of injury for a quadrangular fracture of the cervical spine. This unstable fracture pattern is characterized by anterior column failure in flexion/compression and posterior column failure in tension. Illustration C shows an illustration of the fracture morphology according to the Allen and Ferguson classification.
Incorrect Answer 1:
Hyperextension injuries
Flexion-distraction injuries usually result in facet dislocations.
Question 69
A 47-year-old woman has had a 1-month history of left hip and medial thigh pain that is exacerbated by sitting. Laboratory studies show a total protein level of 8.2 g/dL (normal 6.0 to 8.0) and an immunoglobulin G (IGG) level of 2,130 mg/dL (normal 562 to 1,835). A radiograph, CT scan, and biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 16.
Question 70
Figure 51 shows an arthroscopic view of the patellofemoral joint from an inferolateral portal. The arrow points to which of the following structures? Review Topic

Explanation
Question 71
What is the primary problem in rickets osteomalacia?
Explanation
Question 72
CLINICAL SITUATION Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities. What is the best next step in the patient’s evaluation?

Explanation
but she has not had any issues since the flap. She has abundant callus formation but the fracture line is still visible and unchanged on 2 sets of radiographs. The patient has persistent pain. The best initial evaluation is to ensure that there is no underlying infection with laboratory studies, including a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Nuclear medicine studies have questionable utility, but may be helpful if the inflammatory markers from laboratory studies come back elevated. A CT scan is not warranted because the sequential radiographs show persistent fracture lines and no changes. The patient has a hypertrophic nonunion. Originally, she had appropriate treatment and has shown the ability to make callus, thus her biologic capacity appears to be intact and bone grafting is not needed. The hypertrophic nature of her fracture nonunion indicates that she needs more stability. The best treatment for a hypertrophic nonunion of the tibia is exchange nailing. Based on successive radiographs and the lack of healing, observation is probably just delaying the inevitable. Plating with retention of the nail can be useful in recalcitrant long bone non-union, especially in the femur.
Question 73
In revision total hip arthroplasty, an acetabular reconstruction cage is best indicated for which of the following patterns of bone loss?
Explanation
REFERENCES: Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 74
Figure 28 shows the postoperative radiograph of a 36-year-old patient. The cerclage cable was placed for a minimal medial calcar fracture seen during femoral preparation. In the immediate postoperative period, what is the highest level of activity that would be safely permitted?
Explanation
REFERENCES: Berend KR, Lombardi AV Jr, Mallory TH, et al: Cerclage wires or cables for the management of intraoperative fracture associated with a cementless, tapered femoral prosthesis: Results at 2 to 16 years. J Arthroplasty 2004;19:17-21.
Schmidt AH, Kyle RF: Periprosthetic fractures of the femur. Orthop Clin North Am 2002;33:143-152.
Greidanus NV, Mitchell PA, Masri BA, et al: Principles of management and results of treating the fractured femur during and after total hip arthroplasty. Instr Course Lect 2003;52:309-322.
Question 75
A 4-year-old girl sustains an isolated spiral femoral fracture after falling from her tricycle. Management should consist of
Explanation
REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.
Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365.
Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Levy J, Ward WT: Pediatric femur fractures: An overview of treatment. Orthopedics 1993;16:183-190.
Question 76
..Figure 93 is the radiograph of a 72-year-old woman. Treatment includes fixation of the ulna. What options are recommended for the radius?
Explanation

Figure 94 is the anteroposterior radiograph of a 75-year-old woman who has a 5-year history of progressive pain, crepitus, and loss of motion in her shoulder. She had a rotator cuff repair 10 years ago. Examination reveals 60 degrees of active forward elevation and 20 degrees of external rotation with her arm at her side. Passively she can be brought to 160 degrees of forward elevation and 90 degrees of external rotation with her arm at her side. A glenohumeral joint injection with local anesthetic eliminated pain, but there is no observed change in active motion.
Question 77
Figures 43a and 43b show the AP and lateral radiographs of the radius and ulna of a 9-year-old patient. The fracture is manipulated and placed in a long arm cast with the elbow flexed to 90 degrees and the forearm to neutral rotation. Figures 43c and 43d show the alignment of the fracture after the manipulation. What is the next most appropriate step in management?
Explanation
REFERENCES: Evans EM: Fractures of the radius and ulna. J Bone Joint Surg Br 1951;33:548-561.
Milch H: Roentgenographic differentiation between torsion and rotational fractures of the forearm. Bull Hosp Jt Dis 1949;10:216-225.
Question 78
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the aspiration and proceed to a revision TKA with possible augments on standby.
Question 79
The difference between vitamin D-dependent rickets type I (VDDR I) and vitamin D-dependent rickets type II (VDDR II) is
Explanation
VDDR I is a deficiency of 1a-hydroxylase [converts 25(OH)D to 1a,25(OH)2D3].
Lab tests show hypocalcemia, secondary hyperparathyroidism, elevated alkaline phosphatase (ALP) and low or undetectable calcitriol in the presence of adequate 25(OH)D levels. VDDR II or hereditary vitamin D resistant rickets (HVDRR) (autosomal recessive) is an inactivating mutation in the vitamin D receptor (VDR). Lab tests show low serum calcium and phosphate, elevated ALP and secondary hyperparathyroidism. Serum 25(OH)D values are normal and the 1,25(OH)2D levels are elevated (key difference from VDDR I).
Malloy et al. reviewed genetic disorders in vitamin D action. They state that VDDR I is an inborn error of vitamin D metabolism coded by the gene CYP27B1. Children with VDDR I present with joint pain/deformity, hypotonia, muscle weakness, growth failure, and hypocalcemic seizures or fractures in early infancy. Treatment is with calcitriol or 1a-hydroxyvitamin D (NOT cholecalciferol). Children with VDDR II present with bone pain, muscle weakness, hypotonia, hypocalcemic convulsions, growth retardation, severe dental caries or teeth hypoplasia. Affected children are resistant to therapy and supra-physiologic doses of all forms of vitamin D.
Illustration A shows the differences between VDDR I and VDDR II. Incorrect Answers
in the kidney). The liver enzyme vitamin D 25-hydroxylase (found in hepatocytes) is not responsible for VDDR. VDDR II is caused by an inactivating mutation (rather than an activating mutation).
Question 80
Augmentation of a Broström repair with the mobilized lateral portion of the extensor retinaculum (Gould modification) is expected to produce
Explanation
Question 81
In which scenario is application of NPWT contraindicated?
Explanation
The most common complication associated with NPWT is a rash on the skin resulting from contact with a suction sponge. In a 2001 study by Webb and Schmidt, 2.2% of patients treated with NPWT had a rash that resolved within 48 hours. To minimize risk for this rash, care should be taken to avoid overlap of the sponge onto intact skin. If skin overlap is unavoidable, a lower-pressure setting should be used.
Acute bacterial infection is possible in this scenario, but there would likely be additional findings such as purulence in the wound itself. Similarly, an acute allergic reaction could be found within the wound and not just at the skin edge. Skin irritation from excessive adhesive plastic tension can result in blistering or shearing avulsion but not skin-edge erythema. Skin necrosis from the original trauma would result in skin-edge duskiness instead of erythema.
A study by Timmers and associates showed a statistically significant increase in microvascular blood flow to the skin under a sponge at subatmospheric pressures. Angiogenesis occurs in the area of the wound vacuum from the negative pressure and increased blood flow, not from the sponge material itself. There has been no indication that antibiotic concentration is increased in the setting of negative pressure therapy because antibiotics would be evacuated along with the fluid. NPWT does not result in increased temperatures that would kill pathogens.
NPWT is contraindicated in the setting of neoplasm because its effect on tumors is unknown. There is potential for increased angiogenesis in residual tumor cells, which could lead to recurrence or even metastasis. NPWT has been used safely and effectively for coverage of open fractures between initial debridement and definitive coverage. Fasciotomy wounds are frequently covered with NPWT dressings on a temporary basis with excellent results.
NPWT has been used to temporize wounds with exposed bone before flap coverage. Wounds with excessive tension frequently can be closed after short-term coverage with NPWT dressings.
RECOMMENDED READINGS
Webb LX, Schmidt U. [Wound management with vacuum therapy]. Unfallchirurg. 2001 Oct;104(10):918-26. German. PubMed PMID: 11699301.View Abstract at PubMed
Webb LX. New techniques in wound management: vacuum-assisted wound closure. J Am Acad Orthop Surg. 2002 Sep-Oct;10(5):303-11. PubMed PMID: 12374481. View Abstract at PubMed
Timmers MS, Le Cessie S, Banwell P, Jukema GN. The effects of varying degrees of pressure delivered bynegative-pressure wound therapy on skin perfusion. Ann Plast Surg. 2005 Dec;55(6):665-71. PubMed PMID: 16327472. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 68 AND 69

Figure 68 is the radiograph of a 17-year-old girl who is treated with closed reduction and percutaneous screw fixation for her displaced femoral neck fracture. Capsulotomy of the hip is not performed. After surgery, the patient is instructed to maintain touch-down weight-bearing status for 3 months.
Question 82
A 25-year-old student sustains the injury shown in Figures 13a through 13c after falling off a curb. Initial management should consist of
Explanation
REFERENCES: Rosenberg GA, Sterra JJ: Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8:332-338.
Lawrence SJ, Botte MJ: Jones’ fracture and related fractures of the proximal fifth metatarsal. Foot Ankle 1993;14:358-365.
Question 83
When performing surgery on a patient with insertional Achilles tendinitis and a Haglund’s deformity, how much of the Achilles tendon insertion can be safely detached without having to consider reattachment with bone anchors?
Explanation
REFERENCES: Kolodziej P, Glisson RR, Nunley JA: Risk of avulsion of the Achilles tendon after partial excision for treatment of insertional tendinitis and Haglund’s deformity: A biomechanical study. Foot Ankle Int 1999;20:433-437.
Sammarco GJ, Taylor AL: Operative management of Haglund’s deformity in the nonathlete: A retrospective study. Foot Ankle Int 1998;19:724-729.
Question 84
Creatine is currently being used by athletes as a dietary supplement in an attempt to enhance performance. What is the physiologic basis for its use?
Explanation
REFERENCES: Greenhaff PL: Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5:S100-S110.
Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E: Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci 1993;84:565-571.
Trump ME, Heigenhauser GJ, Putman CT, Spriet LL: Importance of muscle phosphocreatine during intermittent maximal cycling. J Appl Physiol 1996;80:1574-1580.
Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL: Muscle creatine loading in men. J Appl Physiol 1996;81:232-237.
Question 85
-The patient experienced little improvement with activity modification and physical therapy. An intraarticular corticosteroid injection provides excellent but short-lived pain control. She requests surgical treatment for her hip and she is counseled regarding arthroscopy and consent is obtained. Intraoperatively,a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. What treatment is most appropriate considering these findings?
Explanation
The clinical scenario, examination, and MRI scans are consistent with a pincer-type FAI. The decreased range of motion is secondary to the pain produced by the continued abutment of the femoral head against the anterosuperior acetabulum. Flexing the hip while internally rotating and adducting the leg recreates this contact and is typically painful. No clinical signs suggest sacroiliac joint arthritis, an intra-articular loose body, or trochanteric bursitis, although these are all diagnoses that should be considered in a patient with a painful hip. The most sensitive and specific study to detect an acetabular labral tear is an MRI arthrogram of the hip. This study should be obtained in this patient to evaluate the labrum as well as the status of the articular cartilage. An MRI scan without intra-articular contrast is not as sensitive as an arthrogram. An ultrasound can provide a dynamic assessment of the hip and help in the setting of a snapping hip; however, this study is not reliable to determine the presence of a labral tear. In the setting of pincer FAI, the forced leverage of the anterosuperior femoral head upon the anterior acetabulum results in abnormal forces against the posteroinferior acetabulum. This continued force can lead to a chondral lesion in this location know as a “counter-coup” injury. Chondral lesions of the femoral head are rare in the setting of pincer FAI. The posterosuperior quadrant does not experience increased force and rarely sustains chondral injuries. The patient is a young, active individual with no pre-existing degenerative changes, so repair of the tear with bony resection of the pincer lesion is the most appropriate treatment.A capsulolabral detachment should be repaired because these tears can heal and the labrum functions as a seal, preventing egress of synovial fluid from the joint space. If the pincer lesion is not resected, the patient will continue to experience abnormal contact and the repair will likely fail. There is no evidence that the patient has a cam impingement, and recontouring of the femoral head/neck junction is not appropriate. Simple debridement should be reserved for intrasubstance tears of the labrum, which would not be expected to heal with repair.
CLINICAL SITUATION FOR QUESTIONS 30 THROUGH 32
Figures 30a and 30b are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he
believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg.


Question 86
Which of the following preoperative findings is a predictor of poor outcome following arthroscopic debridement for glenohumeral arthritis? Review Topic
Explanation
Question 87
Figures 1 through 3 demonstrate the radiographs obtained from a 25-year-old man who injured his right, by punching a wall 3 weeks earlier. He notes pain and deformity about the ulnar aspect of his hand. The best treatment option is

Explanation
The initial radiographs reveal a fourth and fifth carpometacarpal (CMC) joint fracture dislocation. The injury is associated with a shear fracture of the dorsal rim of the hamate. Further assessment with CT might be helpful in fully evaluating the extent of injury. Extensor carpi ulnaris is a deforming force at the base of the fifth metacarpal. This unstable fracture dislocation could be treated with closed reduction and pinning if the patient presented within a few days of injury. However, because he presented in a delayed fashion (3 weeks after injury), open reduction with internal fixation was required (Figures 4 and 5). In the series by Zhang and associates, patients with fourth and fifth CMC fracture dislocations presenting in a delayed fashion and treated nonsurgically had suboptimal results. Therefore, closed reduction and casting are not appropriate. An arthrodesis and resection arthroplasty are salvage procedures considered for a painful arthritic joint and would less likely should not be considered for this acute injury.



Question 88
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should consist of
Explanation
REFERENCES: Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Schepsis AA, Grafe MW, Jones HP, Lemos MJ: Rupture of the pectoralis major muscle: Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15.
Question 89
A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
Explanation
REFERENCES: Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am
2006;88:113-120.
Iannotti JP, Hennigan S, Herzog R, et al: Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am 2006;88:342-348.
Question 90
A 16-year-old girl sustained the injury shown in Figure 7a. CT scans are shown in Figures 7b through 7d. The results of treatment of this injury have been shown to most correlate with which of the following factors?
Explanation
REFERENCES: Letournel E, Judet R (eds): Fractures of the Acetabulum, ed 2.
Berlin, Germany, Springer-Verlag, 1991.
Matta JM: Fractures of the acetabulum: Accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am
1996;78:1632-1645.
Question 91
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of Review Topic
Explanation
Question 92
A 25-year-old man sustained an L1 compression fracture in a fall from his roof. He is neurologically intact and has no other injuries. Radiographs reveal a 25% loss of height anteriorly and 5 degrees of kyphosis at the fracture site. A CT scan reveals no compromise of the posterior column. Management should consist of
Explanation
REFERENCES: Cantor JB, Lebwohl NH, Garvey T, Eismont FJ: Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993;18:971-976.
Rechtine GR II, Cahill D, Chrin AM: Treatment of thoracolumbar trauma: Comparison of complications of operative versus nonoperative treatment. J Spinal Disord 1999;12:406-409.
Question 93
The patient undergoes further testing and it is discovered that the lesion encompasses 70% of the joint. What is the best next treatment option?
Explanation
A tarsal coalition is an abnormal connection of 2 or more bones in the foot. Although tarsal coalitions are present at birth, children and adults typically do not show signs of the disorder until early adolescence or later. The exact incidence of the disorder is hard to determine; however, it is caused by a gene mutation that affects cells that produce the tarsal bones. The 2 most common locations for tarsal coalitions are between the calcaneus and the navicular or between the talus and the calcaneus. It is estimated that 1 out of every 100 people may have a tarsal coalition. In 50% of cases, both feet are affected. Tarsal coalitions are rarely discovered until symptoms arise. Symptoms may include stiff and painful feet, a rigid flatfoot, or increased pain or a limp with high-level activities. Upon examination, symptoms may include tenderness in the area of the coalition, loss of motion, rigid flat feet, and arthritic changes of the joint. Imaging studies begin with radiographs. A CT scan can provide bony detail for imaging tarsal coalitions and determining the extent of the coalition and any accompanying degenerative change. MRI can provide details of the soft tissues. Treatment includes nonsurgical care including rest, orthotics, a temporary boot or cast, and injections. Surgical options include resection with interposition of muscle or fatty tissue from another area of the body or fusions when large (exceeding 50% of the joint), more severe coalitions are encountered.
RECOMMENDED READINGS
Lemley F, Berlet G, Hill K, Philbin T, Isaac B, Lee T. Current concepts review: Tarsal coalition. Foot Ankle Int. 2006 Dec;27(12):1163-9. Review. PubMed PMID: 17207452. View Abstract at PubMed
Badgley CE. Coalition of the calcaneus and the navicular. Arch Surg. 1927;15:75-88. Conway JJ, Cowell HR. Tarsal coalition: clinical significance and roentgenographic demonstration. Radiology. 1969 Mar;92(4):799-811. PubMed PMID: 5767760. View Abstract at PubMed
Herzenberg JE, Goldner JL, Martinez S, Silverman PM. Computerized tomography of talocalcaneal tarsal coalition: a clinical and anatomic study. Foot Ankle. 1986 Jun;6(6):273-
Question 94
A 70-year-old golfer has pain in her dominant shoulder. She reports that initially the pain was at night but now she is unable to play. Examination reveals weakness in external rotation and shoulder abduction. Radiographs reveal the humeral head articulating with a thin acromion. Management should consist of
Explanation
REFERENCES: Bokor DJ, Hawkins RJ, Huckell GH, et al: Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
Wirth MA, Basamania C, Rockwood CA Jr: Nonoperative management of full-thickness tears of the rotator cuff. Orthop Clin North Am 1997;28:59-67.
Question 95
Fluoroquinolones work by inhibiting what enzyme?
Explanation
antibiotics called quinolones that interfere with DNA metabolism. Fluoroquinolones are synthetic derivatives of nalidixic acid. Its mechanism of action involves interfering with the function of DNA gyrase. DNA gyrase ia a type-II topoisomerase, and "unwinds" DNA to allow replication.
Question 96
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of
Explanation
REFERENCES: Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 97
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in Review Topic
Explanation
Question 98
When compared with a conventional ultra-high molecular weight polyethylene (UHMWPE) -bearing surface in total hip arthroplasty, a highly cross-linked polyethylene (XLPE) -bearing surface is associated with
Explanation
A. a functional result for at least 20 years.
B. a functional result that deteriorates within the first 10 years.
C. an eventual conversion to a constrained knee arthroplasty.
D. an eventual need for arthrodesis.
Distal femoral varus osteotomy (DFVO) is intended for patients younger than age 50, more active patients with isolated lateral compartment arthritis and valgus malalignment. Although the knee functional score improves at 1-year follow-up, the function scores significantly deteriorate at 10-year follow-up. At 15-year follow-up, the knee function further declines, resulting in an overall failure rate of 48.5%. DFVO provides longer lasting benefit in patients with better presurgical knee function.
Total knee arthroplasty following DFVO provides improved function and successful outcomes. Standard posterior stabilized components provide satisfactory stability after appropriate ligament balancing without the need for stemmed or highly constrained implants for most patients.
Question 99
Figures 45a and 45b show the radiographs of a 40-year-old woman with rheumatoid arthritis who is unable to straighten her ring and little fingers. Examination reveals that the fingers can be passively corrected, but she is unable to actively maintain the fingers in extension. Management should consist of
Explanation
REFERENCES: Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases: Tendon ruptures, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999,
pp 1669-1684.
Moore JR, Weiland AJ, Valdata L: Tendon ruptures in the rheumatoid hand: Analysis of treatment and functional results in 60 patients. J Hand Surg Am 1987;12:9-14.
Leslie BM: Rheumatoid extensor tendon ruptures. Hand Clin 1989;5:191-202.
Question 100
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
