OITE & ABOS Orthopedic Exam Prep: Trauma, Shoulder & Tendon MCQs | Part 164
Key Takeaway
This interactive quiz offers Part 164 of the OITE/AAOS Orthopedic Surgery Board Review. Featuring 100 verified, high-yield MCQs for orthopedic surgeons, it aids board certification exam preparation. Topics include Fracture, Shoulder, Tendon, and Trauma, ensuring focused, comprehensive study.
About This Board Review Set
This is Part 164 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 164
This module focuses heavily on: Fracture, Shoulder, Tendon, Trauma.
Sample Questions from This Set
Sample Question 1: A 21-year-old woman has a nontraumatic rupture of the Achilles tendon. Which of the following commonly prescribed medications has been associated with this condition?...
Sample Question 2: Figures 45a and 45b show the radiographs of a 40-year-old woman with rheumatoid arthritis who is unable to straighten her ring and little fingers. Examination reveals that the fingers can be passively corrected, but she is unable to activel...
Sample Question 3: A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?...
Sample Question 4: An investigation studying whether physical therapy or subacromial injection can be successfully used to treat shoulder pain is conducted. Two groups are identified. One group is prescribed physical therapy, while the other receives a subacr...
Sample Question 5: Which of the following is an FDA approved adjunctive treatment for an acute open tibia fracture being treated with an intramedullary nail?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 21-year-old woman has a nontraumatic rupture of the Achilles tendon. Which of the following commonly prescribed medications has been associated with this condition?
Explanation
REFERENCES: van der Linden PD, van de Lei J, Nab HW, et al: Achilles tendinitis associated with fluoroquinolones. Br J Clin Pharmacol 1999;48:433-437.
Bernard-Beaubois K, Hecquet C, Hayem G, et al: In vitro study of cytotoxicity of quinolones on rabbit tenocytes. Cell Biol Toxicol 1998;14:283-292.
Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Question 2
Figures 45a and 45b show the radiographs of a 40-year-old woman with rheumatoid arthritis who is unable to straighten her ring and little fingers. Examination reveals that the fingers can be passively corrected, but she is unable to actively maintain the fingers in extension. Management should consist of
Explanation
REFERENCES: Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases: Tendon ruptures, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999,
pp 1669-1684.
Moore JR, Weiland AJ, Valdata L: Tendon ruptures in the rheumatoid hand: Analysis of treatment and functional results in 60 patients. J Hand Surg Am 1987;12:9-14.
Leslie BM: Rheumatoid extensor tendon ruptures. Hand Clin 1989;5:191-202.
Question 3
A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?
Explanation
REFERENCES: Ring D, Allende C, Jafarnia K, et al: Ununited diaphyseal forearm fractures with segmental defects: Plate fixation and autogenous cancellous bone-grafting. J Bone Joint Surg Am 2004;86:2440-2445.
Question 4
An investigation studying whether physical therapy or subacromial injection can be successfully used to treat shoulder pain is conducted. Two groups are identified. One group is prescribed physical therapy, while the other receives a subacromial injection. The groups have similar baseline demographics and shoulder pathologies. Ten patients are randomized in each group and findings show that there is no significant difference in any patient-reported outcome measure. An increase in sample size would reduce the risk of what parameter?
Explanation
Question 5
Which of the following is an FDA approved adjunctive treatment for an acute open tibia fracture being treated with an intramedullary nail?
Explanation
Open tibial shaft fractures can present many treatment challenges. Although its use remains somewhat controversial, rhBMP-2 has been shown to have many positive effects when used to treat acute open tibia fractures. These benefits include accelerated early fracture healing, decreased rates of hardware failure, decreased need for subsequent bone grafting procedures, and decreased infection rates. rhBMP-2 does have FDA approval specifically for use in open tibia fractures being treated with an intramedullary nail.
Alt et al. present a comparison of patients with Grade III open tibia fractures treated
with un-reamed nails with or without rhBMP-2. They found significant decreases in need for secondary interventions such as bone grafting or nail exchange. Mean time to fracture healing was less in the rhBMP-2 group, but this difference was not statistically significant.
Govender et al. present a prospective randomized study of 450 patients with open tibia fractures treated with an intramedullary nail with or without rhBMP-2. They found statistically significant decreases in need for secondary intervention, hardware failure, and infection as well as faster wound healing and faster time to fracture union.
Wei et al. provide a meta analysis regarding use of rhBMP-2 in open tibia fractures. Due to decreased rates of secondary interventions they estimated a net savings of
$6,000 per case when rh-BMP2 was used. They found no significant difference in rates of infection, postoperative pain, hardware failure, or fracture healing at 20 weeks.
Incorrect answers:
Question 6
An 18-year-old lacrosse player is diagnosed with infectious mononucleosis. What is the recommendation for return to play? Review Topic
Explanation
Question 7
A 24-year-old former high school wrestler had anterior cruciate ligament (ACL) reconstruction with hamstring autograft 6 years ago. He now experiences daily instability of his knee with routine activities including walking. Examination reveals a grade 3+ Lachman test with a soft endpoint, varus laxity at 30°, and a positive dial test at 30° that dissipates at 90° of knee flexion. He has mild medial joint line tenderness. When walking, there is a slight varus thrust. What treatment is most likely to lead to a successful outcome?
Explanation
Question 8
What is the most common arthroscopic finding of internal impingement in an overhead athlete?
Explanation
REFERENCES: Jobe CM: Posterior superior impingement of the rotator cuff on the glenoid rim as a cause of shoulder pain in the overhead athlete. Arthroscopy 1993;9:697-699.
McFarland EG, Hsu C, Neir C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
Question 9
A 77-year-old man with a history of mild renal insufficiency and atrial fibrillation on warfarin therapy is scheduled to undergo a left total hip arthroplasty. He previously underwent a right total hip arthroplasty with development of significant heterotopic bone that resulted in limitation of motion. What is the most appropriate form of prophylactic treatment to minimize the formation of heterotopic bone on his left hip?
Explanation
REFERENCES: Kolbl O, Knelles D, Barthel T, et al: Preoperative irradiation versus the use of nonsteroidal anti-inflammatory drugs for prevention of heterotopic ossification following total hip replacement: The results of a randomized trial. Int J Radiat Oncol Biol Phys 1998;42:397-401.
Pakos EE, Ioannidis JP: Radiotherapy vs nonsteroidal anti-inflammatory drugs for the prevention of heterotopic ossification after major hip surgery: A meta-analysis of randomized trials. Int J Radiat Oncol Biol Phys 2004;60:888-895.
Seegenschmiedt MH, Makoski HB, Micke O, et al: Radiation prophylaxis for heterotopic ossification about the hip joint: A multicenter study. Int J Radiat Oncol Biol Phys 2001 ;51:756-765.
Figure 23 a Figure 23b
Question 10
A 21-year-old collegiate wrestler sustains a blow to his right eye during a match. Examination reveals anisocoria with a dilated right pupil. The globe is properly formed, and extra-occular movements and the visual field are grossly intact. What is the most likely diagnosis?
Explanation
REFERENCES: Brucker AJ, Kozart DM, Nichols CW, Irving MR: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby Year Book, 1991, pp 650-670.
Orlando RG, Doty JH: Ocular sports trauma: A private practice study. J Am Optom Assoc 1996;67:77-80.
Question 11
- Examination of a 32-year old woman who has pain in her shoulder as a result of a head-on motor vehicle accident reveals tenderness directly over the scapula and painful motion of the shoulder. Radiographs show a displaced extra-articular fracture of the scapula. Which of the following studies would best detect commonly associated injuries?
Explanation
Question 12
The gluteus maximus is innervated by which of the following nerves?
Explanation
REFERENCE: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 146-147.
Question 13
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?
Explanation
REFERENCES: Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Lester B, Jeong GK, Weiland AJ, Wickiewicz TL: Quadrilateral space syndrome: Diagnosis, pathology, and treatment. Am J Orthop 1999;28:718-722.
Question 14
- A 55 year-old man has multiple lytic lesions in the humeri, clavicles, and scapulae. Which of the following diagnostic studies best confirms a diagnosis of multiple myeloma?
Explanation
Question 15
A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness? Review Topic
Explanation
Question 16
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?
Explanation
REFERENCES: Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
Martinez A, Sarmiento A, Latta LL: Closed fractures of the proximal tibia treated with a functional brace. Clin Orthop 2003;417:293-302.
Question 17
An 18-year-old man has had an enlarging mass in his hand for the past 3 months. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 54a through 54d. What is the most likely diagnosis?
Explanation
REFERENCES: Abramovici L, Steiner GC: Bizarre parosteal osteochondromatous proliferation (Nora’s lesion): A retrospective study of 12 cases, 2 arising in long bones. Hum Pathol 2002;33:1205-1210.
Nora FE, Dahlin DC, Beabout JW: Bizarre parosteal osteochondromatous proliferations of the hands and feet. Am J Surg Pathol 1983;7:245-250.
Question 18
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints? Review Topic
Explanation
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
Question 19
A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
Explanation
REFERENCES: Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am
2006;88:113-120.
Iannotti JP, Hennigan S, Herzog R, et al: Latissimus dorsi tendon transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am 2006;88:342-348.
Question 20
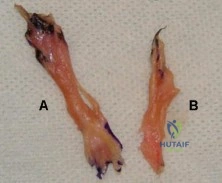
Figure A shows the 2 bundles of the ACL dissected from a cadaveric knee off their bony attachments. They are labeled Bundle A and Bundle B, respectively. Which of the following is true? Review Topic
Explanation
The ACL is comprised of 2 bundles. The AM bundle is longer than the PL bundle.
Their names reflect their relative anatomic positions on the tibial insertion site. On the femur, the AM bundle begins at the proximal-anterior aspect of the femoral insertion site, while the PL bundle begins at the posterior-inferior part. In flexion, the AM bundle is tight and the PL bundle is loose. In extension, the AM bundle is loose and the PL bundle is tight.
Bicer et al. reviewed the anatomy of the ACL. They found that the AM bundle was longer (32mm) compared with the PL bundle (18mm). PL bundle carries greater force near full extension, and the AM bundle carries greater force after 15-45° of flexion. Under combined rotatory loads (valgus and internal tibial torque at knee flexion
>30°), the AM bundle bore more force than the PL bundle.
Figure A shows the 2 bundles of the ACL. The AM bundle is longer than the PL bundle. The oft referred to length of ACL refers mainly to the length of the AM bundle. Illustrations A and B show the spatial relationships of the AM and PL bundles in a cadaveric knee. Illustration C shows the relative positions of the attachments of each bundle.
Incorrect
Question 21
A 48-year-old woman has an open subtrochanteric femur fracture. No other injuries are reported. After thorough evaluation, it is determined that she will need emergent surgical fixation. The patient and family indicate that they are practicing Jehovah's witnesses and desire adherence to the religious standards with respect to blood product usage. The patient signs a valid advanced directive confirming these wishes. Which of the following would be considered acceptable treatment?
Explanation
Question 22
Which of the following is considered the most effective means of identifying an evolving motor tract injury during cervical spine surgery? Review Topic
Explanation
which major changes were detected by both modalities. TceMEP monitoring was 100% sensitive and 100% specific. SSEP monitoring was only 25% sensitive and 100% specific.
Question 23
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had
Explanation
Question 24
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of
Explanation
REFERENCES: Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Burkhead WZ, Arcand MA, Zeman C, et al: The biceps tendon, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1996.
Question 25
A 54-year-old woman reports worsening pain in her buttock, especially when sitting for long periods of time. She has occasional pain and paresthesias radiating down her posterior leg. She has no significant medical history. MRI scans are shown in Figures 15a and 15b and a biopsy specimen is shown in Figure 15c. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1135-1136
Menendez LR: Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 251.
Question 26
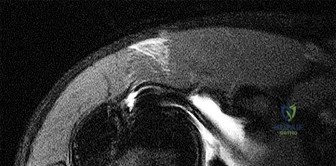
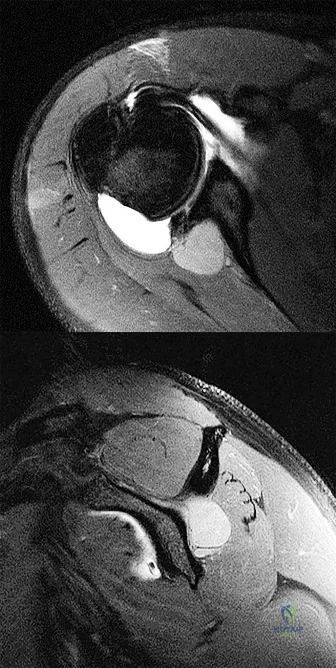
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of
Explanation
REFERENCES: Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10.
Deutsch A, Altcheck DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Walch G, Nove-Josserand L, Boileau P, et al: Subluxations and dislocations of the tendon of the long head of the biceps. J Shoulder Elbow Surg 1998;7:100-108.
Question 27
The bone avulsion shown in Figure 32 has a high correlation with tearing of the
Explanation
REFERENCES: Bach BR, Warren RF: Radiographic indicators of anterior cruciate ligament injury, in Feagin JA (ed): The Crucial Ligaments. New York, NY, Churchill Livingston, 1988, pp 301-327.
Segond P: Recherches cliniques et experimentales sur les epanchements sanguins du genou par entorse. Prog Med (Paris) 1987;7:297.
Johnson LL: Lateral capsular ligament complex: Anatomical and surgical considerations. Am J Sports Med 1979;7:156-160.
Question 28
A 10-year-old boy with severe hemophilia A (factor VIII) sustained an injury to his right forearm 2 hours ago when a classmate fell on his arm during a scuffle. Examination reveals moderate swelling in the forearm, decreased sensation in the distribution of the median and ulnar nerves, and pain on passive extension of the fingers. What is the most appropriate sequence of treatment?
Explanation
REFERENCES: Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 345-391.
Greene WB, McMillan CW: Nonsurgical management of hemophilic arthropathy, in Barr JS (ed): Instructional Course Lectures 38. Park Ridge, Ill, American Academy of Orthopaedic Surgeons, 1989, pp 367-381.
Naranja RJ Jr, Chan PS, High K, Esterhai JL Jr, Heppenstall RB: Treatment considerations in patients with compartment syndrome and an inherited bleeding disorder. Orthopedics 1997;20:706-711.
Question 29
What is the most common benign bone tumor in childhood?
Explanation
REFERENCES: Aboulafia AJ, Kennon RE, Jelinek JS: Benign bone tumors of childhood. J Am Acad Orthop Surg 1999;7:377-388.
Biermann JS: Common benign lesions of bone in children and adolescents. J Pediatr Orthop 2002;22:268-273.
Question 30
A characteristic genetic translocation has been noted in which of the following tumors?
Explanation
REFERENCES: Brockstein BE, Peabody TD, Simon MA: Soft tissue sarcomas, in Vokes EE Golomb HM (eds): Oncologic Therapies. New York, NY, Springer-Verlag, 1999, pp 925-952.
Simon MA, Springfield DS, et al: Management of Surgical Specimens: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 67-75.
Question 31
Which of the following nerves is most commonly injured during ankle arthroscopy?
Explanation
REFERENCES: Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Barber CL, Click J, Britt BT: Complications of ankle arthroscopy. Foot Ankle 1990;10:263-266.
Question 32
What is the most important sign of impending modulation with rapid progression of a spinal deformity in neurofibromatosis?
Explanation
REFERENCES: Crawford AH, Schorry EK: Neurofibromatosis in children: The role of the orthopaedist. J Am Acad Orthop Surg 1999;7:217-230.
Durrani AA, Crawford AH, Chouhdry SN, et al: Modulation of spinal deformities in patients with neurofibromatosis type 1. Spine 2000;25:69-75.
Question 33
- An otherwise healthy 65-year-old man has had chronic pain in his prosthetic knee for the past 9 months. Repeated aspirations reveal a coagulase-negative staphylococcus infection. To eradicate the infection while maintaining the best possible joint function, management should consist of
Explanation
Present recommendations are to avoid a one-stage reconstruction in a patient in whom a glycocalyx elaborating microorganism has been isolated. In one study 52% of the isolates of S. epidermidis and 28% of the isolates of S. aureus elaborated glycocalyx. The microbiology laboratory can be asked to determine if the microorganisms elaborate glycocalyx. In the present case it should be assumed that the staphylococci elaborate glycocalyx and are resistant to antibiotics. A two-stage procedure is indicated for these reasons alone.
Antibiotic therapy alone has been used for a select group of patients who could not medically tolerate either a one-stage or a two-stage arthroplasty. The patient in this case is listed as otherwise healthy.
The decision to perform a resection arthroplasty as a definitive procedure without reimplantation is based on the bacteria’s resistance to antibiotics, quality of the local soft tissues, the complexity of the reconstruction, the patient’s refusal to have another operation, the patient’s overall health, or a combination of these factors. None of which appear to be present in this case.
Question 34
What is the most common complication following surgical treatment of a displaced talar neck fracture?
Explanation
(SBQ12TR.14) Elevated interleukin 6 (IL-6) is most closely associated to which of the following clinical outcomes in orthopedic trauma patients?
Decreased mortality rates
Increased mortality rates
Decreased osteomyelitis infection rates
Increased rhabdomyolysis rates
Increased compartmental syndrome rates
Elevated levels of Interleukin 6 (IL-6) is most closely associated with higher injury severity scores and increased mortality rates in polytrauma orthopaedic patients.
Hyperstimulation of the inflammatory system by major trauma is considered to be the key element in the pathogenesis of severe inflammatory response syndrome and multi-organ dysfunction syndrome. IL-6 is a complex acute-reactant cytokinase that is expressed by cells in response to tissue injury. IL-6 levels are associated with injury severity, complications, and mortality. Patients with the most severe injuries have the highest IL-6 serum levels.
Sears et al. reviewed the markers of inflammation in major trauma. They suggest that interleukin-6 and human leukocyte antigen-DR class II molecules appear to have the greatest potential for use in predicting the clinical course and outcome in trauma patients. Early identification of traumatic patients, based on inflammatory markers and genomic predisposition, could help to guide intervention and treatment.
Pape et al measured the perioperative concentrations of interleukin-6 in sixty-eight blunt trauma patients with non-life threatening pelvic fractures. Release of proinflammatory cytokines were higher in patients undergoing surgical procedures that cause increased blood loss. The release of markers seems to be related to the type and magnitude of surgery, rather than to the duration of the procedure.
Illustration A shows a diagram of the acute inflammatory response after major trauma Incorrect Answers:
Question 35
While performing long fusion with osteotomies for a patient with adult scoliosis and sagittal plane deformity, the neurophysiologist reports a change in motor-evoked potentials in the lower extremities. What is the most appropriate next step?
Explanation
The use of intraoperative neuromonitoring is expanding, especially in the setting of deformity surgery. Changes in monitoring are concerning for the possibility of a neurologic injury; however, several other factors can alter signals. These include hypotension, changes in anesthesia depth and medications, the use of paralytic agents, and technical issues such as leads falling out or becoming disconnected. If a change in neuromonitoring signals is noted, these factors should be checked first to rule out false-positive findings. If this does not correct the problem, the wound should be explored to ensure there is no compression on the neural elements. Finally, if the deformity has been corrected, some of the correction can be released in an attempt to improve the signals. A wake-up test is difficult to perform and does not provide specific information regarding the location of the problem or how to correct it. Steroids may be used depending on surgeon preference, but should not be used until neurologic injury is ruled out. Any neuromonitoring changes always necessitate immediate investigation.
RECOMMENDED READINGS
Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. View Abstract at PubMed
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
Review. PubMed PMID: 21102290. View Abstract at PubMed
Question 36
What type of thoracolumbar spinal injury is associated with an increased risk of neurologic deterioration following admission to the hospital?
Explanation
REFERENCES: Gertzbein SD: Neurologic deterioration in patients with thoracic and lumbar fractures after admission to the hospital. Spine 1994;19:1723-1725.
Magerl F, Aebi M, Gertzbein SD, et al: A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 1994;3:184-201.
Question 37
What is the primary mechanism by which anabolic steroids increase muscle tissue? Review Topic
Explanation
Question 38
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of
Explanation
A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma.
REFERENCES: Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033.
Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
Dormans JP, Rang M: Fractures of the olecranon and radial neck in children. Orthop Clin North Am 1990;21:257-268.
Question 39
- When taken concomitantly with which of the following, erythromycin can cause an increase in the blood level of
Explanation
Question 40
Figure 63 shows the radiographs of a 23-year-old man who sustained a twisting injury at work. Swelling, tenderness, and ecchymosis are noted about the entire midfoot. What associated injury is most likely to be problematic?
Explanation
REFERENCE: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Question 41
If the patient had an isolated spine injury without neurologic deficit, the most appropriate next step would be
Explanation
The treatment of thoracolumbar burst fractures has evolved over the years. In the absence of a neurologic deficit or a posterior ligamentous complex injury, nonsurgical treatment is as effective as surgery. The degree of spinal canal compromise is not a risk factor for neurologic symptoms. Similarly, although kyphosis may be a marker of more significant injury, the degree of kyphosis does not correlate with chronic pain. In the setting of a burst fracture, MRI can be used to evaluate the integrity of the posterior ligamentous complex. Polytrauma may be considered a relative indication for surgical intervention in the setting of a stable burst fracture.
RECOMMENDED READINGS
Rechtine GR 2nd. Nonoperative management and treatment of spinal injuries. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S22-7; discussion S36. Review. PubMed PMID: 16685232. View Abstract at PubMed
Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999 Feb 15;24(4):412-5. PubMed PMID: 10065527. View Abstract at PubMed
Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. View Abstract at PubMed
Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. doi: 10.1016/j.spinee.2012.10.041. Review. PubMed PMID: 24332321.View Abstract at PubMed
Question 42
An 18-year-old collegiate basketball player has had a 3-month history of activity-related back pain. She describes isolated low back pain without radiation that increases with training and playing basketball. Her pain resolves with rest. Physical therapy for 6 weeks has failed to provide relief. An axial CT scan is shown in Figure 17a, and Figures 17b and 17c show sagittal CT reconstructions through the right and left lumbar facets, respectively. Further management should consist of which of the following?
Explanation
REFERENCES: Debnath UK, Freeman BJ, Grevitt MP, et al: Clinical outcome of symptomatic unilateral stress injuries of the lumbar pars interarticularis. Spine 2007;32:995-1000.
Bono CM: Low-back pain in athletes. J Bone Joint Surg Am 2004;86:382-396.
Question 43
A 22-year-old skier reports painful range of motion in the left thumb after falling forward on his outstretched hand while holding his ski pole. Examination of the left thumb reveals increased AP laxity and 45° of valgus laxity at the metacarpophalangeal (MCP) joint. Examination of the right thumb shows 25° of valgus laxity at the MCP joint. Radiographs are normal. Management should consist of
Explanation
REFERENCE: Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint. J Am Acad Orthop Surg 1997;5:224-229.
Question 44
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70° of the right knee. The active arc of motion is from 70° to 90°, and the opposite knee has a flexion contracture of 10°. Both hips are dislocated with flexion contractures of 10°, passive hip motion is from 10° to 90° of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
REFERENCES: Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469.
DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Sells JM, Jaffe KM, Hall JG: Amyoplasia, the most common type of arthrogryposis: The potential for good outcome. Pediatrics 1996;97:225-231.
Question 45
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?
Explanation
REFERENCES: Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
Question 46
A 25-year-old male presents to the emergency department with a mangled lower extremity that is not salvageable. He undergoes transfemoral amputation. Three months later the patient presents to the office with the limb sitting in an abducted position. What important step was forgotten during the amputation?

Explanation
Question 47
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
Question 48
A 50-year-old woman with a 2-part surgical neck proximal humerus fracture and metaphyseal comminution
Explanation
Proximal humerus fractures account for approximately 5% of all fractures, with incidence increasing to reflect an aging population and related osteoporosis. Treatment is dependent upon the mechanism of injury, the patient’s physiologic age and activity level, the fracture pattern, and rotator cuff integrity. Most of these injuries are nondisplaced or minimally displaced and are associated with a good overall prognosis with nonsurgical treatment and temporary impairment. A patient with a nondisplaced surgical neck fracture should be treated without surgery. K-wire stabilization, although technically difficult to achieve, is an option for compliant patients with 2-part, 3-part, and valgus-impacted 4-part fractures who have adequate bone stock. Valgus-impacted 4-part fractures pose reduced risk for osteonecrosis because of the preserved blood supply through the medial hinge, which allows for this technique. For displaced 2-part fractures accompanied by
metaphyseal comminution, K-wire fixation cannot provide adequate stability to initiate a graduated home exercise or outpatient physical therapy program. Formal open reduction with intramedullary or plate fixation in addition to bone grafting (fibular strut allograft) is the best surgical option for the clinical scenario involving a displaced surgical neck fracture with comminution. Osteosynthesis of 3-part fractures may be feasible for physiologically young and active patients without humeral head involvement and osteoporosis.
Current indications for primary hemiarthroplasty include most 4-part fractures, 3-part fractures and dislocations in elderly patients with osteoporotic bone, head-splitting articular segment fractures, and chronic anterior or posterior humeral head dislocations with more than 40% of articular surface involvement. Because of the intra-articular nature of this patient’s 4-part injury in this scenario, hemiarthroplasty with anatomic reconstruction of the greater and lesser tuberosities is most appropriate. Relative indications for hemiarthroplasty also include fractures with more than 20 degrees of varus, associated moderate to severe osteopenia, and revision surgery for failed osteosynthesis. Currently accepted indications for rTSA include scenarios in which the fracture pattern, level of comminution, bone quality, and rotator cuff deficiency preclude plate fixation or hemiarthroplasty. Scenarios involving 4-part fractures and associated rotator cuff tears and tuberosity comminution are best served with a reverse shoulder prosthesis. One of the positive attributes of this implant is the ability to achieve functional forward flexion and abduction regardless of tuberosity healing, position, and degree of comminution. Caution is warranted with this surgical technique because complication rates are higher than for hemiarthroplasty reconstruction. Acute, irreducible 2-part fracture-dislocations of the proximal humerus necessitate open reduction and internal fixation of the affected tuberosities (posterior, lesser tuberosity; anterior, greater tuberosity) through screw, anchor, and/or suture fixation. These fracture-dislocations can be managed with this technique because of the integrity of the vascular supply, which is maintained by the soft-tissue attachments to the intact tuberosities. Repeated attempts at a closed reduction in the 37-year-old with the posterior fracture-dislocation could result in neurovascular injury and myositis ossificans and should be avoided. Arthroplasty reconstruction in this scenario should not be the index procedure in light of concerns regarding implant survivorship in patients of this age and their assumed elevated activity levels.
RECOMMENDED READINGS
Harrison AK, Gruson KI, Zmistowski B, Keener J, Galatz L, Williams G, Parsons BO, Flatow EL. Intermediate outcomes following percutaneous fixation of proximal humeral fractures. J Bone Joint Surg Am. 2012 Jul 3;94(13):1223-8. doi: 10.2106/JBJS.J.01371. View Abstract at PubMed
Iannotti JP, Ramsey ML, Williams GR Jr, Warner JJ. Nonprosthetic management of proximal humeral fractures. Instr Course Lect. 2004;53:403-16. Review. View Abstract at PubMed
Mata-Fink A, Meinke M, Jones C, Kim B, Bell JE. Reverse shoulder arthroplasty for treatment of proximal humeral fractures in older adults: a systematic review. J Shoulder Elbow Surg. 2013 Dec;22(12):1737-48. doi: 10.1016/j.jse.2013.08.021. Review. View Abstract at PubMed
Jobin CM, Galdi B, Anakwenze OA, Ahmad CS, Levine WN. Reverse shoulder arthroplasty for the management of proximal humerus fractures. J Am Acad Orthop Surg. 2015 Mar;23(3):190-201. doi: 10.5435/JAAOS-D-13-00190. Epub 2015 Jan 28. Review. View Abstract at PubMed
Bae JH, Oh JK, Chon CS, Oh CW, Hwang JH, Yoon YC. The biomechanical performance of locking plate fixation with intramedullary fibular strut graft augmentation in the treatment of unstable fractures of the proximal humerus. J Bone Joint Surg Br. 2011 Jul;93(7):937-41. View Abstract at PubMed
Kontakis G, Koutras C, Tosounidis T, Giannoudis P. Early management of proximal humeral fractures with hemiarthroplasty: a systematic review. J Bone Joint Surg Br. 2008 Nov;90(11):1407-13. doi: 10.1302/0301-620X.90B11.21070. Review. PubMed PMID: 18978256. View Abstract at PubMed
Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg. 2004 Jul-Aug;13(4):427-33. PubMed PMID: 15220884. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 67 THROUGH 70
Figure 67 is the radiograph of a right-hand-dominant 70-year-old woman who arrives at the emergency department with acute left shoulder pain following a fall down a flight of stairs. She expresses acute diffuse left shoulder pain and swelling. Prior to her injury, she had full active painless shoulder range of motion.

Question 49
After humeral head replacement for four-part fractures, what is the most commonly reported difficulty?
Explanation
REFERENCES: Goldman RT, Koval KJ, Cuomo F, Gallagher MA, Zuckerman JD: Functional outcome after humeral head replacement for acute three- and fourth-part proximal humeral fractures. J Shoulder Elbow Surg 1995;4:81-86.
Hawkins RJ, Switlyk P: Acute prosthetic replacement for severe fractures of the proximal humerus. Clin Orthop 1993;289:156-160.
Question 50
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk? Review Topic
Explanation
(SBQ13PE.27) A 15-year-old male patient presents requesting clearance to perform in the Special Olympics. He has had abnormal facies, has had mental developmental delay and cytogenetic analysis confirmed abnormalities on chromosome 21. Orthopaedically, he has been treated in the past for an elbow dislocation as well as bilateral patellar dislocation. He has already visited his cardiologist and endocrinologist and has been cleared. He has no complaints, denies any pain, difficulties with walking and reports that his training has been going well. What is the next best step? Review Topic
With a normal physical exam, patient can be cleared for participation
MRI bilateral knees and elbow to ensure no ligamentous injury
Referral to a neurologist for clearance
Lateral cervical spine flexion and extension radiographs
AP pelvis radiograph
Ruling-out C1-C2 instability with flexion/extension radiographs is necessary prior to any spine surgery or participation in sports in patients with Down's Syndrome.
Patients with Down's Syndrome typically present with generalized ligamentous laxity and decreased tone. Thus, dislocations (elbow or patella) along with asymptomatic instability in the cervical spine can commonly occur. Imaging analysis is necessary prior to sports participation.
McKay et al. performed a systematic review to summarize all congenital causes of cervical instability. They found in Down's patients, cervical instability due to ligamentous laxity is found mostly at C1-2. They recommend asymptomatic patients
with an ADI <4.5mm can resume unrestricted activities, while asymptomatic patients between 4.5-10mm should not participate in contact sports. With ADI >10mm OR symptoms/cord changes on MRI, surgery is recommended. Symptomatic patients with ADI between 4.5-10mm should be observed with activity restriction.
Dedlow et al. outlines the most recent 2011 update and guidelines for cervical instability in Down's syndrome patients. One of the major highlighted changes is the emphasis placed on radiographic re-examination, regardless of prior clearance. Re-examination should occur prior to participation in sports and/or the onset of new symptoms.
Illustrations A, B and C highlight the C1-2 instability on flexion-extension lateral radiographs. Careful attention can be placed on the relationship of the anterior arch of C1 and the dens (Illustration C). This allows for the measurements of ADI and the space available for the cord (SAC), which is highlighted in Illustration D.
Incorrect answers:
Question 51
A 15-year-old boy reports leg pain after being tackled during football practice. Radiographs and a CT scan are shown in Figures 46a through 46c. The patient has a pathologic fracture through what underlying lesion?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 52
Deep posterior compartment
Explanation
The structures at risk are the anterior tibial artery and deep peroneal nerve in the anterior compartment, superficial peroneal nerve in the lateral compartment, sural nerve in the superficial posterior compartment, and posterior tibial nerve and posterior tibial and peroneal arteries and veins in the deep posterior compartment.
Question 53
A 52-year-old woman with a 2-year history of a flexible (stage II) adult-acquired flatfoot deformity has failed to respond to nonsurgical management consisting of immobilization, custom orthotics, nonsteroidal anti-inflammatory drugs, and physical therapy. The patient is unable to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 30a through 30c. What is the most appropriate surgical correction?
Explanation
REFERENCES: Greisberg J, Assal M, Hansen ST Jr, et al: Isolated medial column stabilization improves alignment in adult-acquired flatfoot. Clin Orthop Relat Res 2005;435:197-202.
Greisberg J, Hansen ST Jr, Sangeorzan BJ: Deformity and degeneration in the hindfoot and midfoot joints of the adult acquired flatfoot. Foot Ankle Int 2003;24:530-534.
Question 54
In either a ceramic-on-highly-cross-linked polyethylene (HXPE) or metal-on-HXPE component, increasing the ball head size leads to
Explanation
Increasing the size of the ball head increases the primary arc of motion prior to impingement and the jump distance prior to dislocation, assuming an acetabular component abduction of less than 90 degrees. Although HXPE has demonstrated decreases in linear wear rates even with ball head sizes larger than 28 mm, volumetric wear remains a concern. A larger ball head size does not significantly change offset, and larger metal ball heads are not associated with decreased risk for corrosion.
Question 55
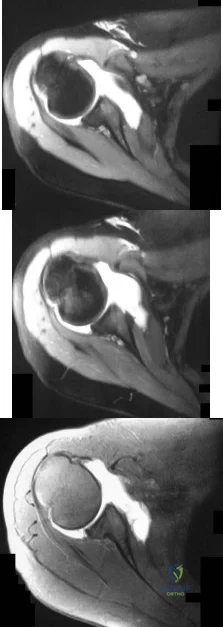
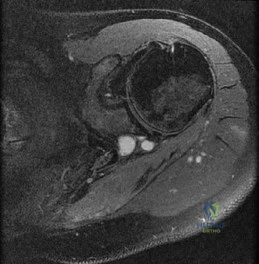
The CT scan shows the involvement area is approximately 30% of the posterior facet. What is the most appropriate treatment?
Explanation
Radiographs reveal a talocalcaneal coalition. The incidence of tarsal coalition in the general population ranges between 2% and 13%. The incidence of tarsal coalition among patients with FGFR-related craniosynostosis syndromes is much higher than among the general population. Tarsal coalitions have been noted in FGFR-1-, FGFR-2-, and FGFR-3-related craniosynostosis syndromes of Apert, Pfeiffer, Crouzon, Jackson-Weiss, and Muenke, but not in Beare-Stevenson or Crouzonodermoskeletal syndromes. The FGFR genes are involved in cell proliferation, differentiation, migration, apoptosis, and pattern formation.
Additionally, nonsyndromic familial coalitions have been described with autosomal-dominant patterns of inheritance.
Cross-sectional imaging should always be obtained prior to resection of a radiographically evident coalition to define the extent of the coalition and determine the coexistence of an additional coalition. CT scan is the gold standard test; however, MRI can be helpful to define a suspected fibrous coalition if a CT scan is nondiagnostic. A bone scan may be useful if pain or history is atypical for a symptomatic coalition. Laboratory tests such as CBC, ESR, CRP, ANA, and RF may be indicated if the imaging evaluation does not confirm a tarsal coalition and if there is concern for malignancy, infection, or inflammatory arthritis.
Investigators have suggested that larger talocalcaneal coalitions with surface areas larger than 33% to 50% of the size of the posterior facet are unsuitable for resection and primary arthrodesis should be considered. However, a study by Koshbin and associates found that with long-term follow-up, favorable functional outcomes were seen even with resections of large talocalcaneal coalitions occupying more than 50% of surface area.
Question 56
A 25-year-old man shot himself at the base of the right index finger while cleaning his handgun. Examination reveals that the finger is cool and cyanotic. A clinical photograph and radiograph are shown in Figures 44a and 44b. What is the recommended treatment?
Explanation
REFERENCES: Peimer CA, Wheeler DR, Barrett A, et al: Hand function following single ray amputation. J Hand Surg Am 1999;24:1245-1248.
Neumeister MW, Brown RE: Mutilating hand injuries: Principles and management. Hand Clin 2003;19:1-15.
Question 57
A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T 2 -weighted MRI scan is shown in Figure 13a, and a contrast enhanced T 1 -weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient’s symptoms?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 319-329.
Shen FH, Samartzis D, Andersson GBJ: Nonsurgical management of acute and chronic low back pain. J Am Acad Orthop Surg 2006;14:477-487.
Question 58
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?
Explanation
REFERENCES: Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
Wirth MA, Rockwood CA Jr: Complications of total shoulder replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Question 59
Of the following clinical situations, which is most likely to lead to osteonecrosis associated with a slipped capital femoral epiphysis (SCFE)?
Explanation
REFERENCES: Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 2, pp 711-745.
Question 60
A 49-year-old male presents with right shoulder pain and weakness after undergoing open cervical lymph node biopsy approximately one year ago. A pertinent finding from the physical exam is seen in Figure A, with the patients arms by his side. Physical exam finding with the arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation are shown in Figure B. What nerve is most likely injured? Review Topic
Explanation
The spinal accessory nerve is fundamental to scapulothoracic function and essential for scapulohumeral rhythm. This nerve is vulnerable along its superficial course. The majority of injuries to the spinal accessory nerve are iatrogenic and occur secondary to head and neck surgery. There is often a marked delay in recognition and initiating treatment. Surgical treatment with the Eden-Lange transfer lateralizes the levator scapulae and rhomboids (transfer from medial border to lateral border)
Camp et al. reviewed the results of 111 patients who underwent operative management of a lesion to the spinal accessory nerve. They found that the majority (~80%) of injuries were sustained iatrogenically and that diagnosis was delayed for approximately 12 months.
Pikkarainen et al. reviewed the natural history of isolated serratus palsy. They found that symptoms mostly recover in 2 years, but at least one-fourth of the patients will have long-lasting symptoms, especially pain.
Figure A depicts a patient with lateral scapular winging. Figure B demonstrates physical exam of this patient with their arms in a position of 90 degrees of forward elevation and 10 degrees of external rotation. Illustration A highlights the difference between medial and lateral scapular winging. Illustration B depicts another example of a patient with lateral scapular winging.
Incorrect Answers:
An injury to the long thoracic nerve would result in serratus anterior palsy which would lead to MEDIAL scapular winging.
An injury to the suprascapular nerve would result in weakness and wasting of the supraspinatus and/or infraspinatus.
An injury to the axillary nerve would result in deltoid muscle weakness.
An injury to the thoracodorsal nerve would result in latissimus dorsi weakness and would not cause scapular winging
Question 61
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in
Explanation
REFERENCES: Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Shen WJ, Liu TJ, Shen YS: Nonoperative treatment versus posterior fixation for thoracolumbar junction burst fractures without neurologic deficit. Spine 2001;26:1038-1045.
Question 62
Figure A is a glenoid CT 3D reconstruction of a 26-year-old accountant who has recurrent shoulder instability. His first dislocation occurred after a fall while skiing. He has now sustained his third dislocation, which was reduced in the emergency department prior to being sent to your office. What is the most appropriate definitive treatment? Review Topic
Explanation
patient would be arthroscopic bony Bankart repair.
Older (>20 years old), recreational athletes with minor glenoid bone loss (<20% of the glenoid surface area) may be treated with soft tissue stabilization procedures using suture anchors. Goals of this procedure include tightening and repairing the torn ligament and labrum to the glenoid. Younger, contact sports athletes with large glenoid defect (>20%) may require bony augmentation type of procedures.
Lynch et al. review the clinical presentation, assessment and treatment algorithm for surgical management of bone loss associated with anterior shoulder instability. While defects larger than 25% of glenoid width should be managed with bony augmentation, they recommend soft-tissue stabilization in smaller defects.
Balg et al. analyzed 131 patients following Bankart procedure and identified following risk factors for failure: age <=20, competitive participation in contact sports, shoulder hyperlaxity, Hill-Sachs on AP radiograph, glenoid bone loss of contour on AP radiograph.
Using human cadaveric shoulders with various anterior glenoid defects sizes, The MOON Shoulder Group compared radiography, MRI and CT to determine the most reliable imaging modality for predicting bone loss. Three-dimensional CT, followed by regular CT were the most reliable and reproducible imaging modalities for predicting glenoid bone loss.
Figure A shows an en face sagittal 3D reconstruction of a glenoid with 10% surface area loss.
Incorrect Answers:
Question 63
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension?
Explanation
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through view, are useful for avoiding this complication.
Question 64
Which of the following radiographic parameters is most predictive of a poor result following multilevel fusion surgery for adult degenerative scoliosis? Review Topic
Explanation
Question 65
-Figures a through c are the MRI scans of a 21-year-old woman with recurrent shoulder instability and pain after an open anterior stabilization procedure. Positive belly-press test findings were positive.At surgery she was found to have an irreparable tear of the tendon injury identified preoperatively. The procedure to address the dynamic stabilizer deficit places which nerve at most risk?
Explanation
Question 66
The load versus deformation curve of the functional spinal unit (FSU) is made up of the neutral zone, the elastic zone, and the plastic zone. What is the plastic zone of the curve believed to represent?
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 15-23.
Panjabi MM, White AA: Physical properties and functional biomechanics of the spine, in White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 1-83.
Question 67
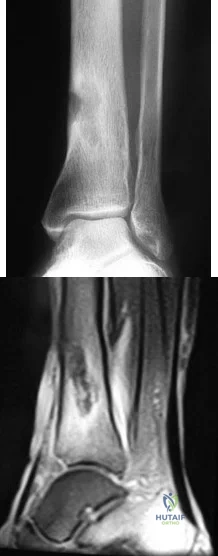
Six months later, the patient’s fracture has healed and a CT scan to further evaluate the physis is performed (Video 85). Based on these findings, how should you advise the family?
Explanation
The hypertrophic zone is the weakest biomechanical zone of the physis and is most likely to fracture. The deep peroneal nerve supplies motor innervation to the ankle and toe
dorsiflexors (anterior compartment) and the first web space, which, in this history, have deficits. The superficial peroneal nerve supplies sensation to the dorsum of the foot and motor to the lateral compartment peroneal musculature (ankle evertors), which also has deficits. The injury must involve both peroneal branches (the common peroneal nerve). Because sensation to the sole of the foot and toe/ankle plantar flexion is intact, the tibial nerve is intact.
Because the nerve was visualized intact, a neuropraxia is the most likely type of nerve injury. This should recover in time and does not necessitate urgent exploration. In pediatric patients, an advancing Tinel sign and partial nerve recovery by 3 months is expected and can be followed clinically. If there is no sign of nerve recovery, an electromyogram should be ordered with consideration for nerve exploration if there is no sign of reinnervation. There is no sign of compartment syndrome because the patient has an unchanged neurologic deficit, is comfortable, and has no pain with passive range of motion.
These injuries are associated with a very high rate of growth arrest (up to 80% in some studies). The CT scan shows an asymmetric growth arrest, which suggests angulation through the distal femur.
Question 68
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?
Explanation
REFERENCES: Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129.
Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Thompson JE: Anatomical methods of approach in operations on the long bones of the extremities. Ann Surg 1918;68:309-316.
Question 69
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle?
Explanation
REFERENCES: Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop Relat Res 1999;368:17 -27.
Warner JJ, Navarro RA: Serratus anterior dysfunction: Recognition and treatment. Clin Orthop Relat Res 1998;349:139-148.
Question 70
Two major pharmacologic classes of bisphosphonates exist: nitrogen-containing and non-nitrogen-containing compounds. The nitrogen-containing compounds work by which of the following actions?
Explanation
Question 71
Haversian canals are found in the center of an osteon in compact bone. They contain blood vessels and nerves.
Explanation
amputations have several options to optimize ambulation including solid, energy storing, and multi-axial prothesis.
Aaron et al. reviews the important considerations for patient specific prostheses and new developments on the horizon to maximize ambulation in prosthesis users.
Mesenchymal stem cells have the capacity to differentiate into all the following cell types EXCEPT?
Osteoclasts
Chondrocytes
Adipocytes
Osteoblasts
Fibroblasts
Mesenchymal stem cells are multipotent stem cells which retain the ability to self-renew and to form cells of the mesenchymal lineage. They can therefore form muscle, fat, tendon (made from fibroblasts), bone, cartilage, and the marrow stromal cells. Mesenchymal stem cells do not however form osteoclasts, which are formed from the monocyte lineage - from hematopoietic stem cells.
Caterson et al review the use of mesenchymal stem cells in tissue engineering and regeneration of musculoskeletal tissue.
A 60 year-old male was brought into the operating room for total hip replacement. Before making the incision, what precautionary procedure must be performed by the entire staff to minimize surgical error?
Mark the word "No" on the nonoperative extremities
Use intraoperative fluoroscopic imaging
Perform "timeout"
Have blood products ready in the operating room
Use the newest prosthesis
Surgical "timeout" is now part of the standard procedure which must be performed before starting surgery to minimize surgical error such as wrong site surgery.
Which of the following statements regarding articular cartilage is TRUE?
Cartilage is an isotropic material
Most of the water in articular cartilage exists in the deep layer next to the calcified cartilage
Cartilage only heals if the injury does not pass through the tidemark
Calcified cartilage is the only place that type IV collagen is found
Cartilage exhibits stress shielding of the solid matrix components
Cartilage exhibits significant stress shielding of the solid matrix components due to its high water content, the non-compressibility of water, and the structural organization of collagen and proteoglycans. Cartilage is composed of a permeable porous matrix and 65 to 80% of the total weight of articular cartilage is made up of water. A pressure gradient causes the water to flow through the porous-permeable solid matrix. Significant flow of fluid through the solid matrix requires high hydrodynamic pressures because of the low
permeability of the solid matrix.
The other answers are incorrect because cartilage is anisotropic, most of the water is located in the superficial layers, it only heals if the injury does pass through the tidemark, type X collagen is found in calcified cartilage and is thought to be involved in mineralization. Type IV collagen is found in the basal lamina.
A 38-year-old patient presents 6 months after intramedullary nailing of a distal third tibia fracture with symptoms consistent with complex regional pain syndrome. During the early stage of the disease he was treated with intermittent splinting, elevation and massage, contrast baths, and transcutaneous electrical nerve stimulation. Despite these modalities, he continues to have severe and debilitating symptoms. Which of the following treatment options is indicated as a second line of treatment?
Long leg cast immobilization for 3 months
Walking boot with non weight bearing for three months
Exchange nailing to stimulate healing response to the limb
Epidural spinal cord stimulator
Surgical sympathectomy of the affected limb
Complex regional pain syndrome is a chronic progressive disease of unknown etiology characterized by pain, swelling and skin changes. If nonoperative modalities fail, a surgical sympathectomy of the affected limb is indicated.
The first line of treatment is physical therapy including intermittent splinting, elevation and massage, contrast baths, and transcutaneous electrical nerve stimulation. Aggressive passive range-of-motion exercises should be avoided. If nonoperative modalites fail and symptoms remain severe, a surgical sympathectomy of the affected limb is indicated.
Keys to successful treatment include early clinical suspicion and treatment. Late CRPS is highly refractory to treatment and often results in permanent disability.
Two forms of Complex regional pain syndrome exist: 1) Reflex sympathetic dystrophy
- which does not demonstrate nerve lesions, and 2) Causalgia - which is associated with damage to peripheral nerves. Diagnostic criteria include:
Major criteria: intense and prolonged pain, swelling, stiffness, and discoloration (vasomotor disturbances).
Minor criteria: trophic changes, osseous demineralization, temperature changes, and palmar fibromatosis.
Tran et al present their systemic review of 41 RCTs of the research regarding treatment of CRPS. Their data suggest that only bisphosphonates offer clear medicinal benefits in the treatment of CRPS. Evidence regarding a beneficial effect of lumbar sympathetic blocks, gabapentin, and physical therapy is lacking. As such, these authors advocate for further study thru well-designed RCTs to better evaluate appropriate and effective treatment strategies.
You are planning an intramedullary nail to treat a geriatric patient with a peritrochanteric femur fracture. Which of the following preoperative considerations is correct regarding your implant?
The radius of curvature of an intramedullary nail is generally greater than the radius of curvature of the femur
Closed section nails have less stiffness than slotted nails
The medial/lateral nail starting point relative to the greater trochanter does not affect varus/valgus position in the fracture
The bending stiffness of your nail is proportional to the second power of the radius
Intramedullary nails allow for mostly direct intramembranous bone healing
The radius of curvature of an intramedullary nail is generally greater than the radius of curvature of the femur, which is why anterior distal femur
penetration is a known complication of intramedullary nailing procedures.
Egol et al. evaluated the radius of curvature of 948 femurs (474 matched pairs) and compared those data with current intramedullary nails. He found the average femoral anterior radius of curvature was 120 cm (± 36 cm)
whereas the radius of curvature of the intramedullary nails ranged from 186 to 300 cm.
The other answers are incorrect because closed section nails have more stiffness than slotted nails. The starting position on the greater trochanter greatly affects the post- operative varus/valgus of the fracture. Intramedullary nails allow for mostly indirect enchondral bone healing due to relative motion at the fracture site.
All of the following antibiotics function by interfering with protein synthesis by inhibiting ribosomes EXCEPT
gentamicin
tobramycin
vancomycin
erythromycin
linezolid
Gentamicin and tobramycin are aminoglycosides that function by inhibition of bacterial protein synthesis via irreversible binding to ribosomal subunits. Erythromycin functions by binding to the 50s subunit of the bacterial 70s rRNA complex and thereby inhibits protein synthesis. Linezolid binds to the 23s portion of the ribosomal subunit and inhibits protein synthesis. In contrast, Vancomycin acts by inhibiting proper cell wall synthesis and does not inhibit the ribosome.
The bending rigidity of the implant shown in Figure A is proportional to what power of the measured radius of the implant?
Question 72
open biopsy and plating
Explanation
The differential diagnosis would include Adamantinoma (rarely seen under age 10, but commonly seen in the tibia), Fibrous dysplasia (usually older child and commonly seen in the tibia), Fibrous dysplasia (usually older child and commonly polyostotic), and Osteofibrous dysplasia (almost always prepubescent in age, isolated tibia/fibula, and eccentric osteolytic lesions).
“The radiographic features are so characteristic that the diagnosis can often be made, with confidence, from the radiographs alone, before or without histological confirmation.”
Therefore, any open biopsy or procedure answers would be wrong for test (OITE) purposes. However, it is not uncommon for thse to be biopsied and the pathology is also characteristic with two fundamental patterns: fibrous tissue surrounding bone trabeculae bordered by active osteoblasts and zonal architecture. Also, the absence of epithelia tissue would exclude adamantimona. Of note regarding Osteofibrous dysplasia, when biopsy/resection is performed, the benign tumor commonly locally returns if the patient is under age 10 to 15 years, but doesn’t if older.
“Marginal subperiosteal excision should not be attempted in patients who are less than fifteen years old, because most likely the lesion will recur. In many cases a biopsy appears to be unnecessary, because clinically and radiographically the lesion is so typical that the physician can be reasonably confident about the diagnosis. The occasional pathological fracture can be treated by plaster-cast immobilization.” Question 197 -
A 25-year-old woman who sustains a direct blow to the anteromedial aspect of her leg while playing basketball has immediate pain and cannot walk. Examination of the knee reveals an increase in posterior translation and external rotation at 90 degrees of flexion. At 30 degrees of flexion, posterior translation and external rotation decrease. Radiographs are normal. Which of the following structures has been injured?
Posterolateral complex
Posterior cruciate ligament
Lateral collateral ligament
Posterior cruciate ligament and posterolateral complex
Posterior cruciate ligament and medical collateral ligament
External rotation of the knee at 30 degrees of flexion averages 29 degrees with a range of 10-45. External rotation of the knee at 90 degrees of external rotation averages 37 degrees with a range of 15-
Question 73
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Explanation
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Question 74
A 14-year-old boy has a midshaft fibular lesion. Biopsy results are consistent with Ewing’s sarcoma. Following induction chemotherapy, local control typically consists of
Explanation
REFERENCES: Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodal therapy for the management of primary, nonmetastatic Ewing’s sarcoma of bone: A long-term follow-up of the First Intergroup study. J Clin Oncol 1990;8:1664-1674.
Simon MA, Springfield DS, et al: Ewing’s Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 287-297.
Question 75
The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?
Explanation
REFERENCES: McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Lister GD, McGregor IA Jackson IT: The groin flap in hand injuries. Injury 1973;4:229.
Question 76
A researcher experimenting with limb patterning removes some tissue from 1 part of the limb bud (which we shall call Site A) and transplants it along the anteroposterior (AP) axis to create a mirror-hand duplication. Which of the following is true?
Explanation
The ZPA controls AP (radioulnar) growth. The signaling molecule is Shh, which is dose dependent. Higher Shh doses lead to posterior (ulnar) digits ulnar sided polydactyly. The extent of duplication is dose dependent (higher dose = more replication). Reduced Shh leads to loss of digits. Posterior elements (little finger/ulna) are formed EARLY prior to anterior elements which are formed LATE (radius/thumb). Disruption of AP patterning will result in loss of later forming elements (radius/thumb).
Al-Qattan et al. reviewed embryology of the upper limb. They summarized that embryology of the upper limb can be viewed in 2 distinct ways: the steps of limb development and the way that the limb is patterned along its 3 spatial axes. Cell signaling plays a major role in regulating growth and patterning of the vertebrate limbs. Signaling cell dysfunction results in congenital differences according to the affected signaling axis.
Illustration A shows an experiment to create ulnar dimelia by adding ZPA tissue to the anterior limb bud. The video shows development of the limb.
Incorrect Answers:
Question 77
A 44-year-old patient who has had a proximal first metatarsal osteotomy has recurrent pain and difficulty wearing many types of shoes. Radiographs show a large 1-2 intermetatarsal angle (IMA).
Explanation

Question 78
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time? Review Topic
Explanation
Question 79
A 25-year-old semiprofessional football player sustains a hyperextension injury to the left foot. He is unable to bear weight. Examination reveals tenderness along the midfoot with swelling and plantar ecchymosis. Radiographs are negative. What is the next step in evaluation of this patient?
Explanation
REFERENCES: Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green’s Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Hunt SA, Ropiak C, Tejwani NC: Lisfranc joint injuries: Diagnosis and treatment. Am J Orthop 2006;35:376-385.
Question 80
- A 16-year-old girl who swims on her high school team reports pain in the shoulder after swimming. History reveals a glenohumeral dislocation at age 14 years while doing the backstroke. Examination shows a positive anterior apprehension sign. Treatment at this time should consist of
Explanation
p. 577: “A vigorous effort to stabilize the shoulder with exercises is particularly indicated in patients with multidirectional or posterior instability and in athletes requiring a completely normal or supranormal range of motion.”
p. 989: “If the [swimmer] has symptoms of subluxation, a conservative program that strengthens the external rotators is warranted. Surgery is seldom indicated.”
Question 81
When the data are normally distributed, what statistical test is best used to compare means of three or more independent groups?
Explanation
Question 82
Figure 14 shows the AP radiograph of a patient who underwent prosthetic arthroplasty 8 years ago and has now become symptomatic again over the past 18 months. A WBC count and erythrocyte sedimentation rate are within normal limits, and aspiration of the glenohumeral joint yields a negative Gram stain and cultures. Which of the following procedures will most likely provide the best pain relief and function?
Explanation
REFERENCES: Antuna SA, Sperling JW, Cofield RH, et al: Glenoid revision surgery after total shoulder arthroplasty. J Shoulder Elbow Surg 2001;10:217-224.
Rodosky MW, Bigliani LU: Surgical treatment of non-constrained glenoid component failure. Oper Tech Orth 1994;4:226-236.
Question 83
When a patient has recurrent anterior shoulder instability, a bony glenoid reconstructive procedure should be considered in which clinical setting?
Explanation
in collision athletes.
Question 84
Figures 23a and 23b show the radiograph and clinical photograph of a patient who reports a reduced ability to flex the interphalangeal joint of her great toe after undergoing a Chevron-Akin bunionectomy. What is the most likely cause?
Explanation
REFERENCES: Tollison ME, Baxter DE: Combination chevron plus Akin osteotomy for hallux valgus: Should age be a limiting factor? Foot Ankle Int 1997;18:477-481.
Scaduto AA, Cracchiolo A III: Lacerations and ruptures of the flexor or extensor hallucis longus tendons. Foot Ankle Clin 2000;5:725-736.
Question 85
A 47-year-old woman falls and sustains a direct blow to her middle finger. She notes pain and swelling and is unable to move the proximal interphalangeal (PIP) or distal interphalangeal (DIP) joints. Radiographs are shown in Figures 8a through 8c. Proper management should consist of
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.
Question 86
Which of the following structures is at risk during proximal dissection of a single lateral perifibular approach for compartment syndrome of the leg?

Explanation
Question 87
A 28-year-old man has left knee pain after a snow skiing accident. The MRI scan shown in Figure 47 reveals which of the following? Review Topic
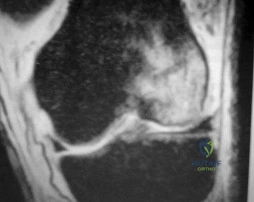
Explanation
Question 88
When comparing arthroscopic lavage and knee debridement with placebo in patients with chronic symptomatic osteoarthritis, what outcome has been demonstrated?
Explanation
Excluding a diagnosis of meniscal tear, loose body, or mechanical derangement, treating knee osteoarthritis of indeterminate cause with arthroscopic lavage and debridement has been found to provide no discernable benefit to offset the risk of surgery. The effects of arthroscopy have not been clinically significant in the vast majority of patient-oriented outcomes measures for pain and function at multiple
times between 1 week and 2 years after surgery.
Question 89
A direct lateral (Hardinge) approach is used during total hip arthroplasty. The structure labeled A in Figure 7 is the
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 333-335.
Ramesh M, O’Byrne JM, McCarthy N, et al: Damage to the superior gluteal nerve after the Hardinge approach to the hip. J Bone Joint Surg Br 1996;78:903-906.
Question 90
A 45-year-old man reports severe discomfort following a twisting injury to his right ankle and foot. Plain radiographs are negative; however, the CT scans shown in Figures 39a and 39b reveal a fracture. Management should consist of
Explanation
REFERENCES: Heckman JD: Fractures and dislocations in the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2267-2405.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 91
-Where is the physis with the highest growth rate (in mm per year) located?
Explanation

Question 92
What molecules have been shown to promote fibrosis during muscle injury?
Explanation
Question 93
Which of the following therapies has a direct anabolic effect on bone?
Explanation
Question 94
Recurrence of this deformity after initial treatment should be treated with
Explanation
Single nuclear polymorphism (SNP) on chromosome 12q24.31, an intergenic SNP, is the PITX1-TBX4 transcriptional pathway that codes for hindfoot formation and is associated with clubfoot. The COLIA-1 gene is related to osteoporosis. Mutations in EXT genes that control formation of tumors cause multiple hereditary exostosis. Mutations in the COL5A or COL3A genes are associated with Ehlers-Danlos syndrome. All idiopathic clubfeet involve abnormalities of or around the talus.
The classic Ponseti technique is associated with a low recurrence rate when followed precisely. The most common reason for recurrence is noncompliance with postsurgical bracing. The initial treatment for recurrence after Ponseti casting is recasting.
NCOA2 fusion transcripts has been noted in mesenchymal chondrosarcoma. Ring chromosomes with CDK4 and MDM2 amplification may be identified with low-grade central osteosarcoma or parosteal osteosarcoma. Fusion transcripts of CDH11-USP6 have been observed in aneurysmal bone cysts.

Video 85
CLINICAL SITUATION FOR QUESTIONS 82 THROUGH 85
Figures 82a and 82b are the radiographs of a 10-year-old girl who was an unrestrained back seat passenger in a motor vehicle collision. Her sole injury is to her left leg. She has a deformed valgus knee with lateral swelling and bruising, and no wound is visible. Upon examination, she has symmetric pulses to her right leg but diminished sensation on the dorsum of the foot and in the first web space. She cannot dorsiflex her left foot or toes but can plantar flex and invert them. Weak ankle eversion is present. Sensation to the plantar foot, medial ankle, and lateral ankle is intact. She likely will reach skeletal maturity at age 14.
Question 95
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?
Explanation
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
Question 96
A patient who sustained a cerebrovascular accident (CVA) 18 months ago has a long-standing spastic adduction contracture of the shoulder with a rigid block to passive external rotation. Significant hygiene problems exist with maceration and continued skin breakdown. Management should consist of
Explanation
REFERENCES: Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
McCollough NC III: Orthopaedic evaluation and treatment of the stroke patient. Instr Course Lect 1975;24:45-55.
Question 97
Figures 29a and 29b show the AP and lateral radiographs of a 30-year-old man who has increasingly worse back pain and stiffness. Examination shows painful, limited spinal range of motion. There is no neurologic deficit. What laboratory study would be most helpful in confirming the diagnosis?
Explanation
REFERENCES: Calin A: Ankylosing spondylitis. Clin Rheum Dis 1985;11:41-60.
Booth R, Simpson J, Herkowitz H: Arthritis of the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 431.
van der Linden S, Valkenburg H, Cats A: The risk of developing ankylosing spondylitis in HLA-B27 positive individuals: A family and population study. Br J Rheumatol 1983;22:18-19.
Question 98
Figures below show the radiographs, MRI, and MR arthrogram obtained from a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has competed or practiced 5 to 6 times per week since the age of 10. He denies any specific hip injury that necessitated treatment, but his trainer contends that he had a groin pull. He reports groin pain with passive flexion and internal rotation of the left hip, and his hip has less internal rotation than his asymptomatic right hip. He is otherwise healthy. What is the primary cause of a cam deformity?
Explanation
Question 99
- Which of the following methods of treatment of a displaced Lisfranc fracture-dislocation will most reliably lead to good functional results?
Explanation
Question 100
Figure 56 is the MR image of a 20-year-old Division I baseball pitcher who has a 1-month history of medial elbow pain in his throwing arm. He also notes a decrease in both control and pitching velocity. An examination reveals tenderness at the medial epicondyle that is exacerbated with valgus elbow stress. The strongest indication for ulnar collateral ligament (UCL) reconstruction is
Explanation
All responses represent findings that may be associated with chronic UCL insufficiency. Responses 1 and 3 reflect injury to the UCL itself. In most patients, particularly young patients, UCL reconstruction should not be considered until an appropriate trial of nonsurgical measures has failed. This trial should include, at a minimum, 6 weeks of throwing abstinence followed by rehabilitation to address pitching mechanics and shoulder motion deficits and core strengthening. Although the decision to enter the MLB draft may influence surgical decision making, a pitcher with a 1-month history of elbow symptoms should attempt nonsurgical therapy before making a surgical decision that is not based on clinical data.
