Orthopedic Surgery Board Review MCQs: Arthroplasty, Sports Medicine & Foot/Ankle | Part 217

Key Takeaway
This page offers Part 217 of an AAOS/OITE Orthopedic Surgery Board Review series. Featuring 100 high-yield, verified MCQs crafted by Dr. Mohammed Hutaif, it prepares orthopedic residents and surgeons for their board certification and OITE exams. Utilize interactive study and exam modes to master critical topics.
About This Board Review Set
This is Part 217 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 217
This module focuses heavily on: Ankle, Arthroplasty, Deformity, Dislocation, Hip, Knee, Ligament, Shoulder, Tendon.
Sample Questions from This Set
Sample Question 1: A patient has a painful metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis if this patient is having a reaction to metal debris?...
Sample Question 2: Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of...
Sample Question 3: A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?...
Sample Question 4: Figures 1 and 2 are the AP and lateral radiographs of a 32-year-old man 10 years after anterior cruciate ligament (ACL) reconstruction. The patient now has worsening medial knee pain and a failed ACL with instability. What is the best surgi...
Sample Question 5: A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A patient has a painful metal-on-metal (MOM) left total hip arthroplasty (THA). Which test(s) best correlate with prognosis if this patient is having a reaction to metal debris?
Explanation
Painful MOM THA and taper corrosion can cause substantial damage to a patient's hip if left untreated. In this case, the workup for a painful MOM THA starts the same as a workup for a painful metal-on-polyethylene bearing couple. Infection must be ruled out in every case with a set of inflammatory markers. If these markers are remotely elevated, this is an indication for joint aspiration. In patients with metal debris, the pathology report often indicates too many cells to count or cellular debris. Metal ion levels do not seem to correlate with prognosis. There are well-functioning patients with high ion levels and poor-functioning patients with low ion levels. Advanced imaging with MARS MRI to evaluate for peritrochanteric fluid collection, a soft-tissue mass, or synovial/capsular hypertrophy will reveal signs of a metal reaction that indicate the need for a revision discussion. A CT scan can show more advanced bony destruction as an indicator of poor prognosis. These films can be used to determine the need for a structural graft or augments for reconstruction of bone loss attributable to metal debris.
Question 2
Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Coughlin MJ, Mann RA: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby-Year Book, 2000, pp 150-269.
Skalley TC, Myerson MS: The operative treatment of acquired hallux varus. Clin Orthop 1994;306:183-191.
Question 3
A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?
Explanation
REFERENCES: Itoi E, Hatakeyama Y, Kido T, et al: A new method of immobilization after traumatic anterior dislocation of the shoulder: A preliminary study. J Shoulder Elbow Surg 2003;12:413-415.
Itoi E, Sashi R, Minagawa H, et al: Position of immobilization after dislocation of the glenohumeral joint: A study with use of magnetic resonance imaging. J Bone Joint Surg Am 2001;83:661-667.
Question 4
Figures 1 and 2 are the AP and lateral radiographs of a 32-year-old man 10 years after anterior cruciate ligament (ACL) reconstruction. The patient now has worsening medial knee pain and a failed ACL with instability. What is the best surgical option?

Explanation
Question 5
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
REFERENCES: Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Clare MP, Fitzgibbons TC, McMullen ST, et al: Experience with the vacuum assisted closure negative pressure technique in the treatment of non-healing diabetic and dysvascular wounds. Foot Ankle Int 2002;23:896-901.
Question 6
A 58-year-old woman with a history of severe asthma and long-term prednisone use reports a progression of chronic shoulder pain for the past 6 months. Radiographs and MRI scans are shown in Figures 30a through 30d. What is the most likely diagnosis?
Explanation
REFERENCES: Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 871-874.
Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
Question 7
When performing surgical excision of the lesion shown in the MRI scan in Figure 3, what nerve is most likely at risk?
Explanation
REFERENCE: Kozin SH: The anatomy of the recurrent branch of the median nerve. J Hand Surg Am 1998;23:852-858.
Question 8
Which of the following plain radiographic views of the shoulder best reveals a Hill-Sachs lesion of the humeral head?
Explanation

Question 9
When performing a saline load test to evaluate for a traumatic arthrotomy of the knee, a mininum of how much saline should be utilized?

Explanation
The study by Nord et al found that the volumes of saline that were needed in order to effectively diagnose 75%, 90%, 95%, and 99% of the knee arthrotomies were 110, 145, 155, and 175 mL, respectively.
The other referenced study by Keese et al found that 50 mL of saline successfully identified only 46% of known knee arthrotomies and that 194 mL was needed to reach a 95% identification rate.
Question 10
A 54-year-old woman sustains the injury seen in Figures 71a and 71b. The injury involves her nondominant extremity. What should the patient be told regarding her expected outcome?

Explanation
(SBQ12TR.101) An otherwise healthy young adult male sustains a transverse radial shaft and ulna fracture. He undergoes definitive surgical fixation with two nonlocking compression plates (LCPs) as shown in Figure A. What is the principle of this fixation technique on bone healing?

Absolute stability with direct healing by callus formation
Relative stability with indirect healing by callus formation
Absolute stability with direct healing by internal remodeling
Relative stability with indirect healing by internal remodeling
Absolute stability with endochondral bone formation
Definitive surgical fixation for a simple transverse both bone forearm fracture would include open reduction and internal fixation with absolute stability with direct healing by internal remodelling (i.e., primary bone healing). The radius is fixed with a 7-hole
Question 11
A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of
Explanation
REFERENCES: Froimson AI: Fracture of the coracoid process of the scapula. J Bone Joint Surg Am 1978;60:710-711.
Gil JF, Haydar A: Isolated injury of the coracoid process: Case report. J Trauma
1991;31:1696-1697.
Question 12
A 24-year-old professional basketball player reports the gradual onset of pain that is poorly localized to the left midfoot for the past 2 months. Examination reveals diffuse tenderness to palpation, full range of motion of the ankle and subtalar joint, and a normal neurovascular examination to the foot. An AP radiograph is shown in Figure 10. Definitive treatment should include
Explanation
REFERENCES: Torg JS, Pavlov H, Cooley JH, et al: Stress fractures of the tarsal navicular.
J Bone Joint Surg Am 1982;64:700-712.
Brodsky JW, Krause JO: Stress fractures of the foot and ankle, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2391-2409.
Question 13
Figures 7a and 7b show the radiographs of a 51-year-old woman who injured her left leg after falling off a stepladder. Surgical reconstruction is performed with a compression screw and side plate; the postoperative radiograph is shown in Figure 7c. Following gradual progression of weight bearing, she reports that she slipped again and placed full weight on the extremity. She now notes a new onset of increased pain in her left thigh and hip region. Follow-up radiographs are shown in Figures 7d and 7e. Reconstruction should consist of
Explanation
REFERENCES: Bridle SH, Patel AD, Bircher M, Calvert PT: Fixation of intertrochanteric fractures of the femur: A randomized prospective comparison of a gamma nail and dynamic hip screw. J Bone Joint Surg Br 1991;73:330-334.
DeLee JC: Fractures and dislocations of the hip, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1659-1825.
Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
Question 14
Which of the following is the strongest contraindication for expansive open door laminoplasty for cervical myelopathy? Review Topic
Explanation
Open door laminoplasty allows decompression direct posterior decompression of the neural elements, as well as an indirect anterior decompression by allowing the cord to drift posteriorly. Posterior drift of the cord relies upon the presence of natural cervical lordosis. In the setting of kyphosis, the cord is tensioned ventrally over the vertebral bodies and discs, and does not have the redundancy to drift backward. Patients without lordosis would therefore be expected to show less post-operative improvement than those with normal cervical curvature.
Chiba et al. performed a retrospective review of patients treated with expansive open door laminoplasty for cervical spondylotic myelopathy (CSM) and ossification of the posterior longitudinal ligament (OPLL). They found that for patients with OPLL, cervical kyphosis was associated with lower recovery rates than those patients with pre-operative lordosis. The authors recommended against posterior decompression for CSM in the setting of OPLL with concomitant cervical kyphosis.
Suda et al. performed a retrospective review of 114 patients who underwent expansive
open door laminoplasty for cervical myelopathy in order to evaluate clinical outcomes and effects on cervical alignment. They found patients with C2-C7 kyphosis >13° had much lower rates of improvement compared with those patients with less kyphosis. The authors suggest an anterior decompression be used for patients with kyphosis greater than 13°, unless kyphotic correction was planned in addition to a laminoplasty.
Illustrations:
Illustration A demonstrates a lateral cervical spine x-ray which shows focal kyphosis at C4-5 and C5-6. Illustration B demonstrates the C7-sagittal vertical axis. Illustration C demonstrates the compression ratio.
Incorrect
<0.4 implies a poor prognosis.
Question 15
A 15-year-old baseball pitcher who reports increasing pain in his right shoulder over the past 3 weeks states that the pain increases the more he pitches. Radiographs of both shoulders are shown in Figures 35a and 35b. What is the next most appropriate step in management?
Explanation
REFERENCES: Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in the adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Cahill BR, Tullos HS, Fain RH: Little league shoulder: Lesions of the proximal humeral epiphyseal plate. J Sports Med 1974;2:150-152.
Question 16
A 25-year-old patient who sustained multiple bilateral rib fractures, a pulmonary contusion, a left nondisplaced transtectal acetabular fracture, and a closed humerus fracture in a motor vehicle accident 2 weeks ago is transferred from another hospital. The humerus fracture has been surgically treated. There are no signs of infection, and the trauma surgeon wants to mobilize the patient as soon as possible. Radiographs are shown in Figures 15a and 15b. Management of the humerus fracture should consist of
Explanation
REFERENCE: Tingstad EM, Wolinsky PR, Shyr Y, Johnson KD: Effect of immediate weightbearing on plated fractures of the humeral shaft. J Trauma 2000;49:278-280.
Question 17
A 42-year-old woman has persistent thumb pain that she notes is worse with opening jars and turning her car key. Opponens splinting provides some relief, but she is poorly tolerant of the splint. Finkelstein’s test is negative, and a carpometacarpal grind test is positive. The radiographs shown in Figures 48a and 48b reveal minimal degenerative changes at the first carpometacarpal joint. What is the best course of action?
Explanation
REFERENCES: Tomaino MM: Treatment of Eaton stage I trapeziometacarpal disease with thumb metacarpal extension osteotomy. J Hand Surg Am 2000;25:1100-1106.
Pellegrini VD Jr, Parentis M, Judkins A, et al: Extension metacarpal osteotomy in the treatment of trapeziometacarpal osteoarthritis: A biomechanical study. J Hand Surg Am 1996;21:16-23.
Tomaino MM, Pellegrini VD, Burton RI: Arthroplasty of the basal joint of the thumb: Long-term follow-up after ligament reconstruction with tendon interposition. J Bone Joint Surg Am 1995;77:346-355.
Question 18
In overhead athletic activities, the kinetic chain generates what percentage of force from the leg and trunk segments of the chain?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, p 47.
McClure PW, Michener LA, Sennett BJ, et al: Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J Shoulder Elbow Surg 2001;10:269-277.
Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 2003;19:641-661.
Question 19
Figure 1 is the clinical photograph of a 42-year-old woman who has a lesion that has failed prior silver nitrate applications. She experiences frequent bleeding from this lesion. A tissue biopsy performed by a dermatologist revealed capillary hypertrophy with lobular arrangement. Which treatment is most appropriate to minimize recurrence?

Explanation
This lesion is a pyogenic granuloma, which is a common benign vascular lesion that can occur on skin or mucosa. The etiology is unclear, although this lesion tends to occur in areas of physical trauma. Initial treatment with silver nitrate with an average of 1.6 applications has a success rate of 85%. This patient, however, has failed silver nitrate applications. Wide surgical excision (Figures below) is associated with the lowest recurrence rate and offers the benefit of a single procedure. Other options often necessitate repeated procedures to completely eradicate this lesion.

Question 20
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of
Explanation
REFERENCES: Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Warner JJ, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 21
A polytrauma patient underwent the following procedures: (1) statically locked intramedullary nailing for a right femoral shaft fracture; (2) open reduction with plate-and-screw fixation [ORIF] for a right simple distal fibula fracture; (3) ORIF right middle third radius and ulna fracture; and (4) ORIF left humeral shaft fracture. What is the appropriate weightbearing status for this patient? Review Topic
Explanation
Tingstad et al. examined the effect of immediate weightbearing on plated fractures of the humeral shaft. They reported that immediate weightbearing on humeral shaft fractures, treated with plating and full weightbearing, did not have any negative effect on the union or malunion rates.
Brumback et al. evaluated the feasibility, safety and efficacy of immediate weightbearing after treatment of femoral shaft fractures with statically locked IM nail. Using biomechanical and clinical data, they showed that all fractures united with no loss of fixation or hardware failure.
Starkweather et al. retrospectively assessed the complications and loss of reduction in patients who bore weight in a short leg cast within 15 days after surgical repair of acute unilateral closed ankle fractures. Of the 81 ankle fracture radiographs, 80 (98.8%) showed no displacement in fracture reduction on the final follow-up examination. These results suggest early protected weightbearing may be safe.
Incorrect Answers:
Question 22
Which of the following statements most accurately describes the layers of articular cartilage?
Explanation
REFERENCE: Schiller AL: Pathology of osteoarthritis, in Kuettner KE, Goldberg VM (eds): Osteoarthritic Disorders. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995,
pp 95-101.
Question 23
Spontaneous rupture of the extensor pollicis longus tendon is most frequently associated with which of the following scenarios?

Explanation
clinically satisfactory.
The referenced article by Gelb is a review of the etiology and treatment of this injury. He reviews the above discussion and findings.
Question 24
Anterior approach
Explanation
The nerve most commonly injured in the posterior approach to the hip is the sciatic nerve. Overall injury prevalence is 1% to 2%. This nerve is more commonly injured in cases of hip dysplasia with excessive leg lengthening. The superior gluteal nerve is at highest risk with the direct lateral approach to the hip. This nerve courses in the gluteus medius muscle and is
at risk when splitting the muscle 5 cm proximal to the greater trochanter. The lateral femoral 73
cutaneous nerve is commonly damaged with anterior total hip replacement surgery. Neuropraxia has been reported in 81% of patients. The inferior gluteal nerve travels from the greater sciatic notch and enters the gluteus maximus muscle. It is at risk when the posterior approach to the hip is used.
RECOMMENDED READINGS
Hoppenfeld S, deBoer P. Surgical Exposures in Orthopedics. 3rd ed. Philadelphia.
PA: Lippincott Williams & Wilkins; 2003:365-453.
DeHart MM, Riley LH Jr. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg. 1999 Mar-Apr;7(2):101-11. Review. PubMed PMID: 10217818. View Abstract at PubMed
Goulding K, Beaulé PE, Kim PR, Fazekas A. Incidence of lateral femoral cutaneous nerve neuropraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res. 2010 Sep;468(9):2397-404. doi: 10.1007/s11999-010-1406-5. PubMed PMID:
Question 25
Ulnar collateral ligament (UCL) reconstruction using a modified Jobe technique
Explanation
Certain complications are more strongly associated with the approach and surgical procedure for elbow pathology. With a 2-incision distal biceps repair, heterotopic ossification
with a radial-ulnar synostosis is a concern. This complication can be minimized through irrigation of bone debris and care to avoid dissection between the radius and ulna. With a single-incision distal biceps repair, the lateral antebrachial cutaneous nerve is retracted during the procedure. Numbness on the lateral side of the forearm is common, although often temporary. During arthroscopic debridement for lateral epicondylitis, injury to the radial UCL can occur, leading to posterolateral rotatory instability of the elbow. The modified Jobe technique for UCL reconstruction typically involves an ulnar nerve transposition during the procedure. Numbness and tingling in the fourth and fifth digits are concerns when this procedure is performed.
Question 26
To be an expert orthopaedic witness in a trial, an orthopaedic surgeon must
Explanation
Question 27
Varus deformity after talar fractures is often seen due to collapse of the medial cortex. What artery supplies this portion of the talus?
Explanation
REFERENCES: Halibruton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115.
Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
Question 28
-What gene is implicated in spinal muscular atrophy?
Explanation

Question 29
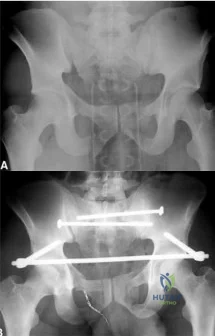
A 39-year-old female presents with the following motor vehicle crash with the injury seen in Figure A (immobilized in a pelvic binder). The iatrogenic neurologic injury most commonly caused by placement of the anterior construct for this injury, as shown in Figure B, would cause which of the following?
Explanation
Unstable pelvic fractures can be treated in a multitude of ways. The ASIF construct is typically created by placing long pelvic screws or polyaxial pedicle screws in the supraacetabular region, similar to the supraacetabular pins for an anterior external fixator. Then a curved bar is placed subcutaneously and connected to the supraacetabular screws. They are typically removed after 3-4 months when fracture healing is complete.
Vaidya et al. present a retrospective review of the use of ASIF as definitive treatment of unstable pelvic fractures. All patients in the study tolerated the construct well. LFCN irritation was seen in 30% of patients, and resolved in all but one patient.
Müller et al. present a retrospective review of the use of posterior stabilization and ASIF. They report an acceptably low complication rate, and good to excellent outcomes in 64.5% of patients.
Figure A is a radiograph demonstrating a right APC3 and left APC2 pelvic injury, imaged in a pelvic binder. Figure B is a postoperative radiograph following posterior stabilization and ASIF.
Incorrect answers:
Question 30
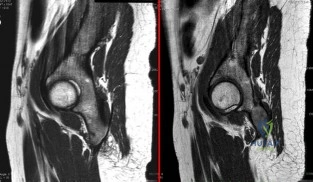
A 22-year-old ballet dancer undergoes hip arthroscopy for increasing hip pain and popping with activity. She experiences complete resolution of signs and symptoms post-operatively. Her pre- and post-operative magnetic resonance sagittal images shown in Figure A (left, pre-operative; right, post-operative). Which of the following pre-operative physical examination findings may have been positive? Review Topic
Explanation
Snapping hip exists in 3 forms: (1) external snapping hip, which is caused by the iliotibial band (ITB) sliding over the greater trochanter, (2) internal snapping hip, and
(3) intraarticular snapping hip, which is caused by loose bodies (traumatic, or from synovial chondromatoses) or labral tears. While painless snapping hip requires no treatment, painful snapping hip may be addressed with activity modification, physical therapy, steroid injections. Surgical release (ITB z-plasty or psoas tenotomy) is indicated if nonoperative management is unsuccessful.
Ilizaliturri et al. evaluated the results of endoscopic iliopsoas tendon release at the lesser trochanter (10 patients) vs endoscopic transcapsular psoas release from the peripheral compartment (9 patients). There were improvements in WOMAC scores in both groups, and no difference between groups. They conclude that both techniques are equally effective.
Marquez Arabia et al. evaluated if the psoas tendon regenerates after tenotomy in 27 patients. At 23 months, they found that tendon regeneration occurred in all patients, to
a mean circumference of 84% of the original. One patient had persistent pain, but all had 5/5 hip flexion strength. They hypothesize that the bulk of iliopsoas muscle fibers attaches directly to the proximal femoral shaft without a tendon, preventing retraction and allowing regeneration to occur easily.
Figure A shows pre- and post-operative arthroscopic psoas tenotomy magnetic resonance sagittal images. Illustration A shows the psoas tendon (white arrows) prior to transection. Illustration B shows the psoas tendon after transection (green arrows, proximal tendon segment; yellow arrows, distal segment). Illustration C and D are diagrams showing release at the level of the lesser trochanter and hip joint respectively.
Incorrect
90 degrees, but full external rotation. Answer 2: Decreased internal rotation and a positive impingement test (forced
flexion, adduction, femoroacetabular Answer 4: These
and internal
rotation) are classic findings
findings may
be found with intra-articular
for cam-type impingement loose bodies.
Question 31
A computed tomography (CT) scan has been shown to be indicated for evaluation of all of the following aspects of acetabular fractures, EXCEPT:

Explanation
with CT scanning and acetabular fractures, and noted a 25% change in surgical planning when CT was utilized versus plain radiographs; they also noted the ability to detect marginal impaction and fracture size/position was improved with CT.
Question 32
Which of the following best describes the course of the median nerve at the elbow?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
pp 46-47.
Question 33
below show the radiographs, and the CT obtained from a year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?
Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 34
What muscle attaches to the site shown by the arrow in Figure 2?
Explanation
REFERENCES: Williams PL, Warwick R, Dyson M, Bannister LH: Neurology, in Gray’s Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 1131-1132.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 131-132.
Question 35
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Explanation
REFERENCES: Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthroscopy 1990;6:301-305.
Question 36
A 22-year-old javelin thrower reports that he has had increasing discomfort in his right elbow and loss of distance from his throws for the past 3 months. Examination reveals tenderness over the medial elbow. Application of valgus torque to the elbow through a passive range of motion elicits pain from 70 degrees to 120 degrees of flexion, with no pain at the limits of extension. What structure is primarily responsible for the patient's symptoms? Review Topic
Explanation
is a secondary stabilizer at 30 degrees of flexion, and not susceptible to valgus load when the anterior bundle is intact. The annular ligament and triceps insertion are not involved with medial instability of the elbow. Olecranon osteophytes likely cause pain in terminal extension of the elbow.
Question 37
Compared to eumenorrheic athletes, amenorrheic athletes have more frequent occurrences of
Explanation
REFERENCES: Warren MP: Health issues for women athletes: Exercise-induced amenorrhea.
J Clin Endocrinol Metab 1999;84:1892-1896.
Rencken ML, Chesnut CH III, Drinkwater BL: Bone density at multiple skeletal sites in amenorrheic athletes. JAMA 1996;276:238-240.
Question 38
A 50-year-old patient underwent multiple debridements for an open radial shaft fracture with bone loss. The bed currently shows no evidence of infection but has a 14-cm diaphyseal bone defect. The most appropriate treatment includes open reduction and internal fixation along with
Explanation
A. clinical examination.
B. invasive pressure measurement.
C. arterial Doppler study.
D. MRI.
Compartment syndrome of the hand can result from a variety of factors, including a traumatic event such as crush injury, fracture, vascular insult, a high-pressure injection injury, or an insect or spider bite. The treatment involves decompressive fasciotomy of the involved compartments. The diagnosis of hand compartment syndrome is determined by history, examination, and objective testing. Patients experience pain out of proportion to the injury, along with swelling and tense skin. Pain may occur with passive motion of the metacarpophalangeal joints as the intrinsic muscles are stretched. Invasive intracompartmental pressures can be measured in the compartments of the hand but not in the fingers. Arterial Doppler studies assess arterial blood flow,
and an abnormality would be a late finding. 41
MRI would show edema of the hand and fingers, but the decision to perform surgical release is less likely made from the findings. The most appropriate method of determining the need for finger fasciotomy is the history and physical examination.
45- Figures 1 and 2 show the MRI studies of a 35-year-old manual laborer with persistent wrist pain despite immobilization. At the time of surgery, collapse of the capitate and arthritic changes of the midcarpal joint are noted. What is the most appropriate procedure for this condition?
A. Local vascularized bone graft
B. Proximal row carpectomy
C. Midcarpal fusion
D. Total wrist arthroplasty
The T1-weighted MRI reveals decreased signal that is consistent with avascular necrosis (AVN) of the capitate. Figure 2 demonstrates increased signal of the capitate consistent with edema. The etiology of AVN of the capitate may be related to trauma, abnormal interosseous vascular supply, and hypermobility. Surgical treatment is considered for patients who have had persistent symptoms despite immobilization. At the time of surgery, collapse of the capitate and arthritic changes would be treated most appropriately with a salvage procedure. A midcarpal fusion is a motion-preserving salvage procedure and is the most appropriate option given to address the pain associated with the midcarpal arthritic changes. The alternative options are not appropriate for this patient. Local vascularized bone grafts are considered for situations in which no evidence of capitate collapse or arthritis is observed.
Question 39
reduced the risk of nonvertebral fractures by 35 percent at the 20-µg dose and by 40 percent at the 40-µg dose and reduced the risk of nonvertebral fragility fractures by 53 and 54 percent, respectively
Explanation
Stoffel et al review the biomechanics of locking bridge plate constructs. The working distance is the most important determinant of axial stiffness and torsional rigidity.
Decreasing the distance from the plate to the bone, using a longer plate, and increasing the number of screws used also increased stiffness.
Egol et al reviews and compares the biomechanics of locked plates and conventional nonlocked plates. Locked plates are most indicated for diaphyseal- metaphyseal junction fractures in osteoporotic bone, severely comminuted fractures, indirect fracture reduction, and fractures where anatomical constraints prevent plating on the tension side of the bone. Conventional nonlocked plates are the fixation of choice for periarticular
fractures that require anatomic reduction, and nonunions that require compression to enhance healing.
A 47-year-old man complains of long standing pain involving the right index, middle, and ring fingers. A clinical image is shown in Figure A. A radiograph is provided in Figure B. Which of the following is the most likely diagnosis?
Gout
Osteoarthritis
Rheumatoid arthritis
Septic arthritis
Psoriatic arthritis
The clinical presentation and radiograph are consistent with psoriatic arthritis. Figure A shows a swollen "sausage digit" (dactylitis) and nail pitting (onychodystrophy)characteristic of this condition. Figure B demonstrates the classic "pencil-in-cup" radiographic deformity seen in DIP arthritis, a common orthopaedic manifestation of psoriatic arthritis. Psoriatic arthritis affects 5 to
10% of patients with psoriasis of the skin. However, the spectrum of
symptoms varies greatly from mild and self-limiting to destructive arthritis. It most commonly affects the hands and feet, but can also involve the spine and sacroiliac joints. Primary treatment is medicinal with NSAIDS, methotrexate, and TNF-alpha inhibitors.
High infection rates have been reported with surgical intervention. Illustration A is an closer image depicting psoriatic onychodystrophyis. Illustration B illustrates a "pencil-in- cup" deformity.
Which of the following study designs represent a level III evidence study?
Prospective, randomized controlled trial
Retrospective case-control study
Retrospective case series
Prospective cohort study
Expert opinion
The practice of evidence based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research. Therapeutic study hierarchy of evidence has been established to better analyze studies in a reproducible fashion. Level I studies include well- designed randomized controlled prospective studies (RCT). Level II include
lower quality designed prospective RCT as well as prospective cohort studies. Level III include retrospective cohort studies and case-control studies. Level IV include case series. Level V include case reports, expert opinion, and personal observation. This is summarized in illustration A. The referenced article by Brighton et al is a review of how the level of evidence has evolved and how the different levels can carry varied amounts of impact on clinical treatments and future research.
A prosthetic polycentric knee with hydraulic swing control is chosen for a very active 63-year-old transfemoral amputee. All of the following appropriately describe the features of this prosthesis EXCEPT:
Flexes in a controlled manner
Variable cadence
Ability to walk at a moderately fast pace
Knee center of rotation is fixed anterior to the line of weight bearing
Weighs more than a constant friction knee that has a manual extension locking mechanism
A polycentric knee has a variable, not fixed, center of rotation. When the center of rotation is posterior to the line of weight bearing it allows control in the stance phase, but makes flexion more difficult. However, when the center of rotation is anterior to the line of weight bearing, flexion is improved but control is sacrificed. An example of this prosthesis is shown in illustration A.
The piston mechanism in the hydraulic knee allows variable cadence by changing resistance to knee flexion. This prosthesis also flexes in a controlled manner by limiting excessive flexion and by extending earlier in the gait cycle.
The polycentric knee with hydraulic swing control is best for active patients who prefer greater utility and variability but it does weigh more than the constant-friction knee hinge that has a manual extension locking mechanism.
The review articles by Michael and Friel review the prescription options for lower extremity prostheses.
Level 1 evidence has shown vitamin C reduces the incidence of reflex sympathetic dystrophy (RSD) or complex regional pain syndrome type I (CRPS) in patients with which of the following?
Tarsal tunnel syndrome
Distal radius fractures
Carpal tunnel syndrome
Cervical radiculopathy from herniated nucleus pulposis
Ankle fractures Corrent answer: 2
Two different prospective, double-blind studies performed by the same institution have shown that vitamin C administration is associated with a lower risk of RSD (i.e CRPS) after wrist fractures. Vitamin C is thought to reduce
lipid peroxidation, scavenge free hydroxyl radicals, protect the capillary endothelium, and inhibit vascular permeability.
The first trial by Zollinger was published in Lancet and included 115 adults with 119 fractures treated with conservative management. They found that RSD/CRPS occurred in four (7%) wrists in the vitamin C group (500mg daily for 50 days) and 14 (22%) in the placebo group.
The second trial by Zollinger published in JBJS included 317 adult patients sustaining 328 distal radius fractures treated conservatively. They had allocated treatment groups to 200mg, 500mg, or 1500mg vitamin C dosages
for 50 days. RSD/CRPS occurrence was 4.2% in the 200mg group, 1.8% in the 500mg group, and 1.7% in the 1500mg group and thus the 500mg dosage for
50 days was recommended at the conclusion of the study. Patients making early cast- related complaints to their provider had a higher incidence of developing RSD/CRPS.
It should also be noted that a recent double blinded randomized controlled trial by Ekrol et al found no statistical significant benefit of Vitamin C on the outcome of distal radius fractures.
Which of the following best describes the mechanism by which osteoprotegerin (OPG) plays a role in RANKL-mediated osteoclast bone resorption?
inhibits RANKL-mediated osteoclast bone resorption by directly binding to RANKL
inhibits RANKL-mediated osteoclast bone resorption by directly binding to the RANK receptor on osteoclasts
stimulates RANKL-mediated osteoclast bone resorption by directly binding to RANKL
stimulates RANKL-mediated osteoclast bone resorption by directly binding to the
RANK receptor on osteoclasts
stimulates RANKL-mediated osteoclast bone resorption by directly binding to PTH
Osteoclastic bone resorption is the final common mechanism for osteolysis, whether due to a pathologic lytic lesion, macrophage activation in particle wear, or normal remodeling. The RANKL mechanism controls the coupling of osteoblast and osteoclast activation.
RANKL is expressed from osteoblasts and bone-marrow stromal cells. When RANKL binds to the RANKL receptor (receptor/activator of NF-[kappa]B) on the cell membrane of osteoclasts) it
stimulates differentiation from osteoclast progenitor cells to mature osteoclasts. Mature osteoclasts proceed with osteoclastic bone resporption. Osteoprotegerin (OPG) acts as a decoy receptor by binding to RANKL and blocking the interaction between RANKL and the RANK-receptor and consequently inhibiting osteoclast formation and activation.
The reference by Clohisy et al reviews recent developments in our understanding of the cellular and molecular events regulating osteoclast- mediated bone resorption and discusses the role of the RANKL pathway in several disease states, including osteolysis associated with inflammatory arthritis and cancer-induced bone loss.
The reference by Goater et al studied the potential of OPG gene therapy by evaluating the ability of transfected synoviocytes expressing OPG to prevent wear debris-induced osteoclastogenesis. They found a decrease in the amount of bone resorption in mice with the transfected OPG gene. The RANKL pathway is shown in Illustration A below and further described in the linked video.
Level 1 evidence has shown Low-intensity Pulsed Ultrasound Stimulation (LIPUS) decreased the time to fracture union in all of the the following injuries EXCEPT?
Radius shaft fracture
Distal radius fracture
Tibia shaft fracture treated with casting
Tibia shaft fracture treated with reamed intramedullary nailing
Scaphoid fracture
Tibia shaft fractures treated with reamed intramedullary nailing do not have Level 1 evidence supporting adjunctive LIPUS treatment. Low-intensity pulsed ultrasound (LIPUS) "bone stimulators" deliver 30mW/cm2 pulsed-waves via an external device over the fracture site.
The meta-analysis by Busse et al found 6 randomized, controlled trials evaluating LIPUS. They concluded that low-intensity pulsed ultrasound treatment may significantly reduce the time to fracture healing for fractures treated nonoperatively.
The metanalysis cites that Emami et al found no benefit to LIPUS treatment on intramedullary fixed tibial fractures. Injuries described in the metaanalysis as having positive benefits from LIPUS include radius shaft(Cook et al), distal radius(Kristiansen et al), scaphoid(Mayr et al), and tibia treated with casting (Heckman et al).
The Level 1 study by Heckman et al of 67 patients found a significant decrease in the time to clinical healing in tibia fractures treated with casting and no serious complications with its use.
A 58-year-old Jehovah's Witness male presents with severe right hip pain due to osteoarthritis. He has failed exhaustive physical therapy, steroid injections, and activity modifications, and now wishes to proceed with a right total hip arthroplasty. During the procedure, there is profound blood loss with associated hypotension. Which of the following is generally the most preferred method for treating the patient's acute intraoperative anemia?
Iron supplementation
Subcutaneous erythropoietin administration
ABO-matched allogeneic blood transfusion
Continuous tranexamic acid infusion
Use of cell salvage
The patient has experienced a greater than expected blood loss during the procedure and has developed hemodynamic instability as a result. Given that the patient is a Jehovah's Witness, the use of a cell salvage (Cell Saver) is most preferred method for treating the patient's acute blood loss anemia.
Signficant intraoperative blood loss is a risk associated with major orthopedic procedures such as joint arthroplasty, and spine, tumor, and trauma surgeries. The most effective method of mitigating this risk is by maintaining good hemostasis during the procedure.
Tranexamic acid (TXA), cell saver, and allogeneic blood transfusion are adjunctive modalities to limit and address excessive intraoperative blood loss. Patients who are Jehovah's Witnesses are generally not amenable to allogeneic blood transfusions but can often be transfused with their own blood. The use of intraoperative cell saver allows for the recycling of the patient's own blood that is obtained with suction, and this can then be used later to transfuse the patient. However, this should be discussed with the patient pre- operatively, as some Jehovah's witnesses may be amenable to allogenic blood transfusion or conversely be opposed to cell saver.
Moonen et al. reviewed perioperative blood management in elective orthopedic surgery procedures. The authors stated that the gold standard for preventing intraoperative blood loss was by maintaining adequate hemostasis and dissecting through anatomically correct tissue planes. They proposed the use
of pre-operative erythropoietin and iron supplementation, pre-operative autologous blood donation, platelet-rich plasmapheresis, hypotensive epidural anesthesia, and intra- operative cell saving as adjunctive blood loss management modalities. The authors concluded that allogenic blood transfusion should be based on physiologic variables, risks of disease transmission, and patient preference.
Imai et al. performed a retrospective study of intraoperative and postoperative blood loss in patients undergoing primary total hip arthroplasty that were treated with either a control or TXA at various time points in the perioperative period. They found that patients who received TXA either 10 minutes prior to surgery or 6 hours after the original dose had a significant decrease in periopreative blood loss. Postoperative blood loss was significantly decreased
in all patients that received TXA. The authors concluded that TXA is an effective adjunct for minimizing blood loss during arthroplasty procedures.
Incorrect Answers:
According to the 2008 National Osteoporosis Foundation Guidelines for Pharmacologic Treatment of Osteoporosis, when are bisphosphonates indicated for the treatment or prevention of osteoporosis?
DEXA T-score between -1.0 and -2.5
FRAX calculated 10-year hip fracture risk of >3%
FRAX calculated 10-year risk of major osteoporosis-related fracture of
>10%
The 2008 National Osteoporosis Foundation Guidelines for Pharmacologic Treatment of Osteoporosis suggests that pharmacologic treatment should be considered for a DEXA T-score between -1.0 and -2.5 at the femoral neck/spine AND 10-year risk of hip fracture ≥ 3%.
Osteoporosis affects more than 12 million Americans per year, with the burden falling heaviest on postmenopausal women. Because of decreased bone strength, patients with osteoporosis are susceptible to fragility fractures. With no additional risk factors, a 65- year-old Caucasian woman has an estimated
10% 10-year risk of a fragility fracture. FRAX (World Health Organization Fracture Risk Assessment Tool) calculates 10-year risk of fracture based on the following variables: age, sex, race, height, weight, BMI, history of fragility
fracture, parental history of hip fracture, use of oral glucocorticoids, secondary osteoporosis and alcohol use to calculate 10-year risk of fracture.
Unnanuntana et al. discussed the utility of the FRAX tool as an assessment modality for prediction of fracture risk. The authors advocated for treatment with osteopenia (T-score of
-1.0 to -2.5) combined with either a ten-year risk of hip fracture >= 3% or a ten-year risk of major osteoporosis-related fracture
of >= 20% as calculated by FRAX. They also discussed biochemical markers of bone formation and resorption, which are useful for monitoring the efficacy of antiresorptive therapy and may help identify patients at high risk for fracture.
Cosman et al. review the 2008 National Osteoporosis Foundation guidelines and support that pharmacologic treatment for osteoporosis should be considered if patients are postmenopausal women or men > 50 years of age AND meet one of the following criteria: have a prior hip or vertebral fracture, a T score -2.5 or less at the femoral neck or spine, OR a T score between -1.0 and -2.5 at the femoral neck or spine AND a 10-year risk of hip fracture
greater than 3% or 10-year risk of major osteoporosis-related fracture greater than 20%. They conclude that DEXA scans should be repeated every 1-2 years if patients are undergoing pharmacologic treatment.
Gass et al. review the epidemiology and tiered management strategy for osteoporosis. They discuss the first line prevention, treatment of secondary causes of osteoporosis, and finally pharmacologic interventions, all in an effort to mitigate fracture risk and the burden that osteoporotic fractures on the health care system.
Illustrations:
Illustration A outlines the variables taken into account in the FRAX score calculator.
Incorrect answers:
ADDITIONALLY has either a ten-year risk of hip fracture >= 3% or a ten-year risk of major osteoporosis-related fracture of >= 20% (or both) as calculated by the FRAX tool.
>20% as calculated by the FRAX tool in order to meet the criterion set forth in the 2008 National Osteoporosis Foundation guidelines. Combined with documented osteopenia (T- score of -1.0 to -2.5), bisphosphonate therapy would be indicated.
>20% as calculated by the FRAX tool in order to meet the criterion set forth in the 2008 National Osteoporosis Foundation guidelines.
Which of the following bone graft substitutes has the fastest resorption characteristics?
Calcium sulfate
Tricalcium phosphate
Hydroxyapatite
Fibular allograft
Cortical iliac crest autograft
Of the three bone graft substitutes listed (calcium sulfate, tricalcium phosphate, and hydroxyapatite), calcium sulfate has the fastest resorption characteristics. Fibular allograft and cortical iliac crest autograft are not considered bone graft substitutes.
Calcium sulfate, tricalcium phosphate, and hydroxyapatite are all "osteoconductive" bone graft substitutes, meaning that these implants provide a surface and structure that facilitates the attachment, migration, proliferation, differentiation and survival of osteogenic stem and progenitor cells. Each has different chemical, macro- and microstructural properties. Calcium sulfate (plaster of Paris) is a low-molecular weight soluble compound that must be implanted adjacent to viable periosteum to work. It is reabsorbed by a
process of dissolution over a period of 5-7 weeks.
Jamali, et al., found that calcium sulphate was completely reabsorbed by 6 weeks. Tricalcium phosphate has compressive strength similar to cancellous bone, but is brittle and weak under tension and shear. It undergoes reabsorbtion via dissolution and fragmentation over 6-18 months; unfortunately less bone volume is produced than tricalcium phosphate absorbed. For this reason, it is used clinically as an adjunct with other less
absorbable substitutes.
Moore et al discuss that hydroxyapatite forms the principle mineral content of bone. Synthetically, it is available in ceramic and non-ceramic forms as porous or solid, blocks or granules. HA has good compressive strength, but is weak in tension and shear and brittle making it fracture-prone in shock loading. Ceramic HA preparations are resistant to absorption in vivo, which occurs at 1-
2% per year. Non-ceramic HA is more readily absorbed.
Which of the following techniques increases strength and stability to an external fixation construct?
Unicortical pin fixation
Decreasing total pin separation distance
Increased working distance from the pin to fracture site
Decreasing the distance between the bone and the construct
Using smaller diameter pins
There are several methods that can be used to increase the strength of an external fixation construct. Decreasing the distance from the bar to the bone increases stability and strengthens the construct. Some other methods to increase stability include: good bone- to-bone fracture end apposition, using an increased number of pins, using larger pins, small distance from the near pins to the fracture site (smaller working distance), increased spacing between the near and far pins, and bicortical pin fixation.
Tencer et al looked at biomechanical aspects of external fixation systems. They demonstrated that system rigidity could be increased by maximizing pin separation distance in the fracture component and the number of pins used while minimizing pin separation distance across the fracture site and the sidebar offset distance from bone.
Incorrect Answers: Answer choices 1,2,3, and 5 all act to decrease external fixation construct strength.
A 62-year-old woman with Paget’s disease is started on a non- nitrogen containing bisphosphonate for treatment of her condition.
What is the mechanism of action of this drug?
Inhibition of farnesyl diphosphate synthase
Conversion of drug into a non-functioning ATP-analogue
Interference of isoprenylation of small GTPases
Inhibition of geranylgeranyl diphosphate synthase (GGPPS)
Downregulation of the undecaprenyl diphosphate synthase (UPPS) pathway
Bisphosphonates are a class of antiresorptive agents used to treat diseases characterized by osteoclast-mediated bone resorption. Non-nitrogen containing bisphosphonates (such as etidronate) are metabolized into non-functioning
ATP analogues which cause eventual osteoclast apoptosis. Nitrogen containing bisphsphonates (alendrolate/Fosamax and Zoledronic acid/Zometa) act by inhibiting farnesyl diphosphate synthase (FPPS), resulting in decreased prenylation of small GTPases.
Reszka et al reviewed nitrogen containing bisphosphonates. They outlined the mechanism of action on farnesyl diphosphate synthase in the cholesterol biosynthesis pathway.
Guo et al also reviewed the mechanism of nitrogen-containing bisphosphonates. In addition to showing the decrease in prenylation of GTPase, they were shown to inhibit geranylgeranyl diphosphate synthase (GGPPS), as well as undecaprenyl diphosphate synthase (UPPS).
Morris et al reviewed the bisphosphonates currently approved by the FDA. They outlined their use in the treatment of Paget disease, metastatic bone disease and widening applications in OI and fibrous dysplasia.
Incorrect answers:
1,3,4,5: Mechanism of nitrogen-containing bisphosphonates.
A 58-year-old female falls and sustains the injury shown in Figures A and B. Following surgical treatment of the fracture, which of the following is the most appropriate additional investigation?
MRI of the pelvis
Urine electrophoresis
CT scan of the pelvis
Bone scan
DEXA scan
Figures A and B depicts a femoral neck fracture. Medical management of postmenopausal women with fragility fractures (distal radius, femoral neck, vertebral compression fractures) includes dual-energy x-ray absorptiometry (DEXA) testing.
Following the diagnosis of osteoporosis, bisphosphonates, calcitonin or other medical treatments may be initiated.
Oyen et al examined 1794 patients with fractures of the distal radius. As one- third of the men and half of the women had bone mineral density (BMD) suggesting osteoporosis, they concluded that all patients aged 50 or above should have bone densitometry testing.
Freedman et al reviewed 1162 women with distal radius fractures. They determined that the rate of diagnostic workup and medical treatment decreases as patient age increases at the time of fracture.
A 52-year old woman who is not on any hormone replacement therapy (HRT) falls from standing height and sustains the injury seen in Figure A. Review of her medical history reveals that she carries a diagnosis of osteoporosis, and that her latest T-score was -3.0. How much calcium should she have been consuming on a daily basis prior to sustaining her injury?
Question 40
..The orthopaedic surgeon obtains tissue with the histology shown in Figure 40c. Treatment should consist of
Explanation


Question 41
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.
Question 42
An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis? Review Topic

Explanation
Question 43
A 65-year-old woman undergoes a lumbar laminectomy for spinal stenosis at the L3-L4 level. The surgery and postsurgical course are uncomplicated. Eight weeks after surgery she has severe left anterior thigh, groin, and knee pain with ambulation and standing. Which condition is the most likely cause of her symptoms?
Explanation
Disorders of the hip can mimic and/or coexist with lumbar spine disorders. The prevalence of hip pain lasting longer than 1 month in patients ages 65 to 74 years is 19%. There is often overlap between their respective signs and symptoms. In a patient with failed back surgery syndrome, hip pathology may have been present before back surgery and not recognized. Osteoarthritis of
the hip typically causes groin and anterior thigh pain. Meralgia paraesthetica is more likely to manifest immediately after surgery. Trochanteric bursitis usually affects the proximal lateral thigh and often can radiate to the distal thigh. Facet joint pain causes low-back pain that can be referred to the gluteal region. Epidural hematoma 6 weeks after surgery is highly unlikely.
RECOMMENDED READINGS
Bolt PM, Wahl MM, Schofferman J: The roles of the hip, spine, sacroiliac joint, and other structures in patients with persistent pain after back surgery. Seminars in Spine surgery 2008;20:14-19.
Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res. 2004 Feb;(419):280-4. PubMed PMID: 15021166. View Abstract at PubMed
Question 44
A 27-year-old professional rugby player is sprinting down the field during a game and sustains a twisting injury to his right knee with immediate onset of swelling, pain, and difficulty with ambulation. Imaging of his right knee is demonstrated in Figures A, B, and C. Which of the following structures has most likely been injured? Review Topic

Explanation
The ACL is the most commonly injured knee ligament, with an incidence of between
100,000 and 200,000 ruptures per year in the United States. The majority of ACL tears occur from non-contact athletic injuries. Acute ACL tears are associated with lateral meniscal tears. Physical examination findings include positive Lachman and Pivot shift tests. Imaging includes radiographs which are usually normal; however, the presence of a Segond fracture (avulsion fracture of the proximal lateral tibia) is pathognomonic for an ACL rupture and represents bony avulsion by the anterolateral ligament (ALL). MRI demonstrates bone bruising of the middle third of the lateral femoral condyle (sulcus terminalis) and posterior third of the lateral tibial plateau in more than 50% of acute ACL tears.. Bone bruise patterns correlate with the direction of the abnormal anterior translation and abutment of the posterolateral tibia against the middle third of the lateral femur during the injury. Treatment options include nonoperative management with physical therapy and lifestyle modification or operative intervention if failure of conservative measures.
Bathala et al present a radiologic case study of a Segond fracture visualized on AP radiograph of the knee of a patient who sustained an ACL rupture. They discuss the critical nature of this finding and the need for further imaging, as it is associated with ACL tears, meniscal tears, and damage to structures in the posterolateral corner.
Viskontas et al discuss different patterns of bone bruising demonstrated on MRI in acute anterior cruciate ligament ruptures of 100 patients, 86 with non-contact and 14 with contact injuries. They found that the non-contact mechanism correlates with more severe bone bruising in both the medial and lateral compartments as demonstrated on MRI.
Figures:
Figure A - AP radiograph of the knee that demonstrates a Segond fracture Figures B and C - coronal T1 and T2 MRI slices that demonstrate bone bruising of the middle third of the lateral femoral condyle and posterior third of the lateral tibial plateau
INCORRECT ANSWERS:
Question 45
A 29-year-old ultramarathoner, who is halfway into a 50-mile race, is sweating profusely. He suddenly collapses, is unresponsive, and has violent muscle contractions. Prior to these symptoms, he had been drinking water at every water stop (every 1 mile). What is the most likely diagnosis?
Explanation
REFERENCES: Griffin LY: Emergency preparedness: Things to consider before the game starts. J Bone Joint Surg Am 2005;87:894-902.
Rehrer NJ: Fluid and electrolyte balance in ultra-endurance sport. Sports Med 2001;31:701-715.
Question 46
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. The surgical approach for definitive reduction and stabilization of this pattern is

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Posterior partial articular tibial plateau fractures are rare. Failure to recognize this pattern can lead to poor patient outcomes secondary to poor surgical decision making. Pathognomonic findings on the lateral radiograph include maintenance of continuity between the anterior articular surface and tibial shaft along with subluxation of the knee joint with excessively anterior tibial station (the femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally
stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 47
A collegiate rower reports the sudden onset of right chest pain while rowing. The athlete states that the pain is worse with deep inspiration and coughing. Examination reveals localized tenderness over the posterolateral corner of the eighth rib. What is the most likely diagnosis?
Explanation
REFERENCES: Karlson KA: Rib stress fractures in elite rowers. Am J Sports Med 1998;26:516-520.
Holden DL, Jackson DW: Stress fractures of the ribs in female rowers. Am J Sports Med 1985;13:342-348.
Question 48
A 32-year-old football coach has had a 4-month history of increasing right wrist pain, particularly during blocking exercises, and he reports significant pain with range of motion and gripping activities. He denies any history of trauma. Examination reveals dorsal wrist tenderness and boggy fullness over the dorsum of the wrist. No erythema is noted. Grip strength is 60% compared with the opposite side. Radiographs are shown in Figures 5a and 5b. What is the most likely diagnosis?
Explanation
REFERENCES: Green DP, Hotchkiss RN, Pederson WC: Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, pp 837-848.
Gerwin M, Weiland AJ: Avascular necrosis of the carpals. Hand Clin 1993, p 761.
Question 49
Figure 40 shows the radiograph of a 30-year-old woman who has a painful elbow. Examination reveals a deformed skull, multiple cafe-au-lait spots, and bone deformities. What is the most likely diagnosis?
Explanation
REFERENCES: Albright F, Butler AM, Hampton AO, et al: Syndrome characterized by osteitis fibrosa disseminata, areas of pigmentation and endocrine dysfunction with precocious puberty in females. N Engl J Med 1937;216:727-746.
Danon M, Robboy SJ, Kim S, Scully R, Crawford JD: Cushing syndrome, sexual precocity, and polyostotic fibrous dysplasia (Albright syndrome) in infancy. J Pediatr 1975;87:917-921.
Grabias SL, Campbell CJ: Fibrous dysplasia. Orthop Clin North Am 1977;8:771-783.
Question 50
A 4-year-old child was born with bilateral congenital radial clubhands. Which of the following associated conditions is a contraindication to centralization of the hands on the ulna?
Explanation
REFERENCES: Green DP, Hotchkiss RN, Pederson WC: Green’s Operative Hand Surgery,
ed 4. New York, NY, Churchill Livingstone, 1999, pp 344-349.
Herring JA: Tachjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002,
vol 1, pp 382, 511.
Question 51
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered?
Explanation
REFERENCES: Ludwig S, Zarro CM: Complications encountered in the management of patients with ankylosing spondylitis, in Vaccaro AR, Regan JJ, Crawford AH, et al (eds): Complications of Pediatric and Adult Spine Surgery. New York, NY, Marcel Dekker, 2004,
pp 279-290.
Wu CT, Lee ST: Spinal epidural hematoma and ankylosing spondylitis: Case report and review of the literature. J Trauma 1998;44:558-561.
Question 52
What is the dominant component of articular cartilage extracellular matrix by weight?
Explanation
REFERENCES: Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Inst Course Lect 1998;47:487-504.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 3-18.
Question 53
A 22-year-old woman injures her neck in a motor vehicle accident. Examination reveals no sensory or motor function below T8. Radiographs and an MRI scan show a burst fracture at T7. Forty-eight hours later, the bulbocavernosus reflex is present but there is no evidence of motor or sensory recovery in the lower extremities. What is the most likely diagnosis?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.
Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1132-1133.
Question 54
A 72-year-old active man has shoulder pain after undergoing an explantation of an anatomic shoulder arthroplasty 6 months prior with an antibiotic cement spacer placed. The patient has 60° of forward flexion, 40° of external rotation, and a positive belly press with limited internal rotation. A recent work-up for continued infection is negative, and a follow-up MRI reveals grade 2 atrophy of the supraspinatus and grade 3 atrophy of the subscapularis with tendon retraction to the glenoid rim. What is the best next step in definitive management?
Explanation
is not indicated for this otherwise active patient.
Question 55
Which of the following is considered a risk factor for the development of low back pain?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 627-643.
Question 56
A 38-year-old man has an enlarging left paraspinal soft-tissue mass. Based on the MRI scans and biopsy specimens shown in Figures 32a through 32e, what is the most likely diagnosis?
Explanation
of surgical resection, radiation therapy, chemotherapeutic protocols, hormone modulation, and/or anti-inflammatory medications.
REFERENCES: Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 309-337.
Spear MA, Jennings LC, Mankin HJ, et al: Individualizing management of aggressive fibromatoses. Int J Radiat Oncol Biol Phys 1998;40:637-645.
Question 57
A 45-year-old man who has had recurrent pain and swelling of the left Achilles tendon insertion for the past 10 years reports that physical therapy and activity modification have provided relief in the past. He now has continued pain despite these efforts. He also reports occasional bouts of dysuria that he attributes to a history of prostatitis. He also notes recent eye irritation that he attributes to allergies. A lateral heel radiograph is shown in Figure 33. Which of the following laboratory studies would best aid in diagnosis?
Explanation
REFERENCE: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 560-650.
Question 58
Figures 52a and 52b show the plain radiographs of a 12-year-old girl who has right distal leg pain. She reports that symptoms are present with weight-bearing activities and improve with rest. Examination reveals diffuse tenderness over the distal tibial metaphysis and mild swelling. A photomicrograph of the biopsy specimen is shown in Figure 52c. What is the most likely diagnosis?
Explanation
REFERENCE: Picci P, Manfrini M, Zucchi Z, et al: Giant cell tumor of bone in skeletally immature patients. J Bone Joint Surg Am 1983;65:486-490.
Question 59
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
REFERENCES: Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Warner JJ, Deng XH, Warren RF, Torzilli PA: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Question 60
A 40-year-old man has a painful mass on his anterior ankle joint with limited range of motion. A radiograph, MRI scan, a gross specimen, and a hematoxylin/eosin biopsy specimen are shown in Figures 5a through 5d. What is the most likely diagnosis?
Explanation
REFERENCES: Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Hocking R, Negrine J: Primary synovial chondromatosis of the subtalar joint affecting two brothers. Foot Ankle Int 2003;24:865-867.
Question 61
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
REFERENCES: Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998,
p 583.
Question 62
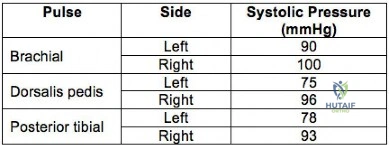
A 32-year-old professional skydiver lands awkwardly during a jump. He presents to the emergency room with bilateral knee injuries. Following successful closed reduction of both extremities, both feet are warm and pulses are present. Bedside doppler assessment is performed and the results are seen in Figure A. What would be the most appropriate next step in treatment?
Explanation
Injury to the popliteal artery is present in 10-40% of knee dislocations (KD). ABI
<0.9 has sensitivity of 87% and specificity of 97% for the diagnosis of arterial disruption. Delayed recognition of an occlusive injury (>8 hours) is likely to result in above knee amputation.
Stannard et al. examined the role of selective arteriography based on serial physical examination. They found arterial injury in 7% (9 out of 134 knees), and abnormal physical findings in 10 patients, with only 1 false positive. They recommend arteriography for patients with decreased pulses, color or temperature, expanding knee hematoma, or an abnormal physical examination prior to presentation in the emergency department.
Mills et al. reviewed the value of ABI for diagnosing arterial injury after knee dislocation. They found that of the 29% with ABI <0.9, all required surgery for arterial injury. Of the remaining patients with ABI >0.9, none had vascular injury. They concluded ABI >0.9 has negative predictive value of 100%.
Nicandri et al. reviewed an algorithm for selective angiography. They recommend the following: (1) Intact pulses and ABI >0.9, observation for 24 hours. (2) Asymmetric pulses or ABI <0.9, arteriogram. (3) Hard signs of vascular injury (absent distal pulses, distal ischemia, active hemorrhage, expanding pulsatile hematoma), surgical exploration.
Figure A is a table showing systolic pressure readings at different sites. To calculate the ABI, the highest measured arterial pressure in the ankle or foot is divided by the higher brachial arterial pressure from both upper extremities.
Incorrect Answers:
Question 63
A 62-year-old active man returns for routine follow-up 16 years after hip replacement. He has no hip pain. Radiographs reveal a well-circumscribed osteolytic lesion around a single acetabular screw. All hip components are perfectly positioned. Comparison radiographs obtained 6 months later show an increase in the size of the osteolytic lesion. CT depicts a well-described lesion that is 3 cm at its largest diameter and is localized around one screw hole with an eccentric femoral head. What treatment is appropriate, assuming that well-fixed cementless total hip components are in place?
Explanation
Given a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected from liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings arise during revision surgery. Here, complete cup revision is not warranted, considering the appropriate implant position. Beaulé and associates reviewed 83 consecutive patients (90 hips) in whom a well-fixed acetabular component was retained in a clinical scenario such as the one described. No hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, acetabular component revision may be indicated.
Question 64
A 4-month-old infant is unable to flex her elbow as a result of an obstetrical brachial plexus palsy. This most likely illustrates a predominate injury to what structure?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 28-29.
Wolock B, Millesi H: Brachial plexus-applied anatomy and operative exposure, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991,
pp 1255-1272.
Zancolli E: Reconstructive surgery in brachial plexus sequelae, in Gupta A, Kay S, Scheker L (eds): The Growing Hand. London, England, Mosby, 1999, p 807.
Question 65
What factor is associated with a higher risk of dislocation after total hip arthroplasty?
Explanation
Dislocation after total hip arthroplasty is a multifactorial problem. Numerous risk factors may act independently or cumulatively to increase the risk of this complication. Previous hip surgery of any kind is associated with a twofold increased risk for dislocation. Other risk factors include female gender, impaired mental status, inflammatory arthritis, and older age. Numerous studies have shown a lower dislocation rate with a direct lateral approach, although surgical techniques such as capsular repair have
significantly lowered the incidence of dislocation after using the posterior approach. Metal-on-metal bearings have been associated with other complications such as adverse tissue reactions but are often used with larger-diameter bearings, which pose a lower risk of dislocation.
Question 66
Figures 23a and 23b show the radiograph and clinical photograph of a patient who reports a reduced ability to flex the interphalangeal joint of her great toe after undergoing a Chevron-Akin bunionectomy. What is the most likely cause?
Explanation
REFERENCES: Tollison ME, Baxter DE: Combination chevron plus Akin osteotomy for hallux valgus: Should age be a limiting factor? Foot Ankle Int 1997;18:477-481.
Scaduto AA, Cracchiolo A III: Lacerations and ruptures of the flexor or extensor hallucis longus tendons. Foot Ankle Clin 2000;5:725-736.
Question 67
A 26-year-old woman sustained a nondisplaced femoral neck fracture and treatment consisted of use of percutaneous cannulated screws. At her 3-month follow-up visit, she reports hip pain and is unable to ambulate. A radiograph is shown in Figure 1. What is the next most appropriate treatment?
Explanation
REFERENCES: Hartford JM, Patel A, Powell J: Intertrochanteric osteotomy using a dynamic hip screw for femoral neck nonunion. J Orthop Trauma 2005;19:329-333.
Mathews V, Cabanela ME: Femoral neck nonunion treatment. Clin Orthop Relat Res 2004;419:57-64.
Question 68
A 34-year-old male arrives intubated with a closed head injury to the trauma bay after a motor vehicle accident. After initial hospital workup and resuscitation, he is transferred to the intensive care unit. In addition to multiple systemic injuries, he sustained the closed injury shown in Figure A. Intracompartmental pressure monitoring of the limb measure in a range from 28-30 mm Hg. Which of the following sustained blood pressure measurements would support the treatment of limb fasciotomy? Review Topic 1 110/60 mmHg 2 115/55 mmHg 3 92/64 mmHg

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam - especially with intubated patients. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy.
McQueen et al. prospectively reviewed 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Olson et al. provide a review of compartment syndrome for the lower extremity. They discuss a variety of injuries and medical conditions that may initiate acute compartment syndrome, including fractures, bleeding disorders, and other trauma. Although the diagnosis is primarily a clinical one, they also recommend supplementation with compartment pressure measurements in equivocal cases.
Figure A shows a closed comminuted tibial shaft fracture. Incorrect Answers:
Question 69
Which of the following treatment regimens for thromboembolic prophylaxis meets the American College of Chest Physicians Guidelines for 10-day treatment after total hip arthroplasty and total knee arthroplasty?
Explanation
Low-molecular-weight heparin and fondaparinox are also acceptable treatment options. Aspirin, adjusted dose unfractionated heparin, and elastic compressive stockings are not recommended as stand-alone options.
REFERENCES: Colwell C: Evidence based guidelines for prevention of venous thromboembolism: Symposia. Proceedings of the 2005 AAOS Annual Meeting. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 15-18.
Freedman KB, Brookenthal KR, Fitzgerald RH, et al: A meta-analysis of thromboembolic prophylaxis following elective total hip arthroplasty. J Bone Joint Surg Am 2000;82:929-938.
Question 70
Figures 174a and 174b are the radiograph and clinical photograph of a 64-year-old obese woman (body mass index [BMI] of 48) who has controlled diabetes and hypertension. She has failed nonsurgical treatment and a weight loss program. She is considering total knee arthroplasty (TKA). What is the most significant postsurgical risk for this patient?
Explanation
The literature has demonstrated increased risk for complications among obese patients undergoing TKA (10%-30%). An evaluation of TKA among obese patients revealed 3- to 9-fold higher incidence of wound complications and deep-seated infection. Belmont and associates demonstrated that patients with a BMI higher than 40 are at higher risk for overall complications than patients with a BMI lower than 25, with a particularly high risk for developing local wound complications and infection. An increased risk for thromboembolic complications was not shown among obese patients undergoing TKA. Patient-reported outcome scores among obese patients undergoing TKA are equivalent to those of nonobese
patients. There are conflicting data regarding the outcome and survivorship following TKA for obese patients. Although some studies show a difference in patient-reported outcomes at differing postsurgical intervals, most obese patients undergoing TKA are satisfied with the procedure.
Question 71
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of Review Topic
Explanation
or tumor. Brace treatment is not required for this small curve unless future progression is demonstrated.
Question 72
Which structure is the primary stabilizer of the lesser metatarsophalangeal (MTP) joint?
Explanation
Synovitis of the second MTP occurs in association with instability of the joint. This can be idiopathic or secondary to an external deforming force (such as a hallux valgus or shoe wear causing a claw toe). The primary stabilizer of the MTP joint for translation in the vertical plane is the plantar plate. The flexor digitorum brevis flexes the MTP joint, and the flexor digitorum longus flexes
all joints of the toe. The collateral ligaments are primary stabilizers in the transverse plane and secondary stabilizers in the sagittal plane.
RECOMMENDED READINGS
Deland JT, Sung IH. The medial crosssover toe: a cadaveric dissection. Foot Ankle Int. 2000 May;21(5):375-8. PubMed PMID: 10830654.View Abstract at PubMed
Suero EM, Meyers KN, Bohne WH. Stability of the metatarsophalangeal joint of the lesser toes: a cadaveric study. J Orthop Res. 2012 Dec;30(12):1995-8. doi: 10.1002/jor.22173. Epub 2012 Jun 13. PubMed PMID: 22696467. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 91 THROUGH 95
Figure 91a is the sagittal plane ultrasound of the second web space of a 48-year-old woman who has noted burning pain in the ball of her right foot for 2 years. The pain intermittently radiates into her second and the third toes. Figure 91b shows the surgical procedure and Figure 91c is the pathologic specimen.
A
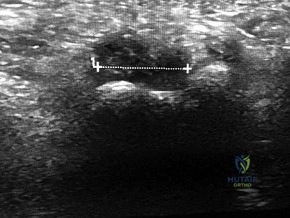
B

C

Question 73
A 73-year-old man who underwent repair of the left rotator cuff 6 years ago reports good pain relief but notes residual weakness of the left shoulder, especially with overhead tasks. He denies having pain at night and has minimal discomfort with activities of daily living but is dissatisfied with his shoulder strength. Radiographs show an acromiohumeral interval of 2 mm. Appropriate management should consist of
Explanation
REFERENCES: Bigliani LU, Cordasco FA, McIlveen SJ, Musso ES: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
DeOrio JK, Cofield RH: Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am 1984;66:563-567.
Gerber C, Vinh TS, Hertel R, Hess CW: Latissimus dorsi transfer for the treatment of massive tears of the rotator cuff: A preliminary report. Clin Orthop 1988;232:51-61.
Question 74
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?
Explanation
REFERENCES: Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Lester B, Jeong GK, Weiland AJ, Wickiewicz TL: Quadrilateral space syndrome: Diagnosis, pathology, and treatment. Am J Orthop 1999;28:718-722.
Question 75
Among patients with adolescent idiopathic scoliosis, a thoracolumbosacral orthosis is most effective for which type of curve?
Explanation
A thoracolumbosacral orthosis is most effective for bracing of curves when the apex is at T7 or below. Bracing is used for patients who are skeletally immature (Risser stage 0, 1, or 2), and it is recommended that the brace be worn 16 to 23 hours per day and continued until skeletal maturity or until the curve progresses to beyond 45 degrees, at which point bracing is no longer considered effective.
RECOMMENDED READINGS
Luhmann SJ, Skaggs DL: Pediatric spine conditions, in Lieberman JR (ed): AAOS Comprehensive Orthopaedic Review. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2009, pp 245-265.
Shaughnessy WJ. Advances in scoliosis brace treatment for adolescent idiopathic scoliosis. Orthop Clin North Am. 2007 Oct;38(4):469-75, v. Review. PubMed PMID: 17945126. View Abstract at PubMed
Question 76
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of Review Topic
Explanation
Question 77
Hybrid locked plating for distal femoral fractures refers to the use of nonlocked and locked screws in the same construct. The advantages of using the combination of nonlocked and locked screws in both the proximal and distal fragments are that nonlocked screws
Explanation
Question 78
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
Explanation
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
Question 79
Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?
Explanation
REFERENCES: Markel DC, Femino JE, Farkas P, et al: Analysis of lower extremity embolic material after total knee arthroplasty in a canine model. J Arthroplasty 1999;14:227-232.
Pell AC, Christie J, Keating JF, et al: The detection of fat embolism by transoesophageal echocardiography during reamed intramedullary nailing: A study of 24 patients with femoral and tibial fractures. J Bone Joint Surg Br 1993;75:921-925.
McGrath BJ, Hsia J, Boyd A, et al: Venous embolization after deflation of lower extremity tourniquets. Anesth Analg 1994;78:349-353.
Question 80
After sustaining a muscle contusion injury, prolonged immobilization leads to Review Topic
Explanation
Question 81
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings? Review Topic
Explanation
Question 82
What structure is the primary restraint to inferior translation of the shoulder?
Explanation
REFERENCES: Harryman DTII, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53 -66.
Bigliani LU, Pollock RG, Soslowsky LJ, et al: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 83
Figure 8 shows the CT scan of an 11-year-old boy who has had a 1-year history of worsening painful flatfeet. He reports pain associated with physical education at school, especially with running and jumping. Management consisting of activity restriction, anti-inflammatory drugs, and casting has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
Kitaoka HB, Wikenheiser MA, Schaughnessy WJ, et al: Gait abnormalities following resection of talocalcaneal coalition. J Bone Joint Surg Am 1997;79:369-374.
Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 84
A young man sustains a lumbar strain in an on-the-job motor vehicle accident. Both he and his treating physician feel that he is capable of limited duty with appropriate restrictions shortly after the injury. What term best describes his work status?
Explanation
REFERENCE: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 131-137.
Question 85
Triple arthrodesis in a reduced position
Explanation
Question 86
A young gymnast fell awkwardly onto an outstretched hand during a competition. At the time of impact, his forearm was positioned in supination. Axial and posterolateral forces were loaded along the forearm into the elbow and the elbow underwent a significant valgus thrust. What injury pattern is most likely to result from the combination of these forces at the elbow?
Explanation
The key features of a terrible triad injury include a radial head fracture, coronoid fracture, and dislocation of the elbow. Disruption of the lateral collateral ligament complex often concomitantly occurs. While restoration of the bony anatomy is important for static stability, the key primary stabilizer that needs to be addressed is the lateral collateral ligament complex. In acute injuries LCL repair may be possible. In chronic injury, LCL reconstruction would need to be considered.
O'Driscoll et al. 1991, examined 5 patients with recurrent posterolateral rotatory instability of the elbow. They showed that by applying supination of the forearm with a valgus moment and an axial compression force to the elbow while it is flexed from full extension, this can demonstrate posterolateral rotatory instability of the elbow. The elbow is reduced in full extension and must be subluxated as it is flexed in order to obtain a positive test result (a sudden reduction of the subluxation).
O'Driscoll et al. 1992 looked at a cadaveric study of the elbow. They showed that external rotation and valgus moments with axial forces resulted in posterior dislocations in 12 of the 13 specimens when the anterior medial collateral ligament (AMCL) remained intact. Clinically, it valgus stability in pronation is demonstrated, the AMCL can be assumed to be intact.
Illustration A and B shows radiographs of a terrible triad injury. There is posterolateral dislocation of the elbow with associated radial head fracture, coronoid fracture.
Incorrect Answers:
Question 87
Which of the following post-reduction forearm fractures patterns may be treated non-operatively in an otherwise healthy 22-year old male?
Explanation
Even in the setting of minimal displacement, fractures involving the radial diaphysis, or both bones of the forearm, are at high risk of displacing further and progressing to malunion or nonunion. Given the potential for a resulting loss of forearm rotation, open reduction internal fixation is indicated for almost all adult diaphyseal radius and both bone fractures.
Schulte et al. review the management of both bone forearm fractures in adults. They review biomechanics, fixation techniques, outcomes and complications. They note that the goals of fixation in simple patterns are 'cortical opposition, compression, and restoration of forearm geometry.'
Anderson et al. treated 330 acute diaphyseal forearm fractures with compression plating from 1960 to 1970. At 4 months to 9 years follow up, they achieved a 97.9%
union rate for the radius and 96.3% union rate for the ulna.
Illustration A shows measurement of radial bow. A dotted line perpendicular to the line drawn from the radial tuberosity to the ulnar aspect of the distal radius can be used to measure radial bow when drawn at the point of maximum distance to the ulnar edge of the radius.
Incorrect answers:
Question 88
Which of the following patients is more likely to have an overall poorer outcome following a lower extremity amputation?
Explanation
Question 89
A 47-year-old obese man with a body mass index of 42 comes into the office with left knee pain 1 year after undergoing an uncomplicated left medial unicompartmental knee arthroplasty (UKA). Radiographs show a loose tibial component in varus. What is the most appropriate next step to treat this failed construct?
Explanation
This patient likely is experiencing failure of the UKA secondary to poor patient selection. In this young, heavy man, the component likely loosened due to the ongoing varus alignment of the knee and his elevated
weight. Despite this likely scenario, the next step is determining whether an infection is the cause of his pain. Prior to obtaining an aspiration, the surgeon can order ESR and CRP studies to determine whether aspiration is warranted. If the laboratory studies are unremarkable, the surgeon likely can forgo the
aspiration and proceed to a revision TKA with possible augments on standby.
Question 90
A 52-year-old man has a stage IIB malignant fibrous histiocytoma of the distal femur. Local treatment should consist of
Explanation
REFERENCE: Bacci G, Picci P, Mercuri M, Bertoni F, Ferrari S: Neoadjuvant chemotherapy for high grade malignant fibrous histiocytoma of bone. Clin Orthop 1998;346:178-189.
Question 91
A 55-year-old man presents with low back pain that has progressed over the last year. He reports the pain is worse with activity, especially when bending forward and lifting objects. He denies any pain in the buttocks or lower extremities. On physical he has age-appropriate motion in the lumbar spine. He is neurologically intact in the lower extremities. Figure A shows his axial and sagittal T2-weighted MRI scans. A histological sample of this lesion would most likely show Review Topic

Explanation
Juxtafacet cysts may include synovial cysts or ganglion cysts. Synovial cysts are lined with epithelium (cuboid synovial cells) and contain clear or xanthochromic fluid. Ganglion cysts which have no synovial lining, and contain gelatinous material from myxoid degeneration of the fibrous adventitial tissue.
Xu et al. reviewed the treatment of 195 synovial cysts. They found that patients treated with laminectomy had the highest risk of cyst recurrence (3%). In contrast, decompression with instrumented fusion had the lowest incidences of cyst recurrence (0%) or back pain (although they had the longest hospital stay, and greatest blood loss).
Figure A is a T2-weighted MRI (left, axial; right, sagittal) showing a facet synovial cyst arising from an arthritic left L3-4 facet joint. It occupies much of the space in the spinal canal and indents and displaces the thecal sac. Illustration A shows a hemorrhagic synovial cyst showing synovial cell lining, fibroconnective tissue with widespread hemorrhage, neoangiogenesis, and hemosiderin microdeposits.
Incorrect Answer Answer Answer
1:
2:
3:
Described histology is characteristic of Described histology is characteristic of
Described
histology
is
characteristic
Question 92
-If a physician elects to shorten a femur by 4 cm for traumatic bone loss treatment and places an intramedullary nail for fixation, which deformity will be created in the lower extremity?
Explanation

Question 93
Pharmacoprophylaxis should be avoided in favor of a pneumatic compression device for a patient with
Explanation
For patients with known bleeding disorders, a pneumatic compression device alone is recommended over pharmacoprophylaxis to minimize risk for excessive bleeding and wound complications. Factor VIII deficiency (hemophilia) and active liver disease are the 2 conditions for which support is strongest to withhold anticoagulation. Protein C deficiency and protein S deficiency are associated with increased risk for thrombosis, as is the factor V Leiden mutation.
RESPONSES FOR QUESTIONS 159 THROUGH 162
Lateral femoral cutaneous
Superior gluteal
Inferior gluteal
Obturator
Sciatic
Which nerve listed above is at increased risk for injury when performing hip surgery through the following approaches?
Question 94
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?
Explanation
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Koti M, Maffulli N: Bunionette. J Bone Joint Surg Am 2001;83:1076-1082.
Question 95
A 36-year-old woman has pain and swelling of the anterior arm after undergoing arthroscopic shoulder surgery 8 months ago. At the time of the procedure, extensive debridement and synovectomy of the anterior aspect of the joint was performed to remove scar tissue that had formed after an open rotator cuff repair. Examination reveals a golf ball-sized swelling just lateral to the coracoid. The area is not warm and shows no other signs of infection. An MRI scan is shown in Figure 1. Management should now consist of
Explanation
REFERENCES: Cole BJ, Rodeo SA, O’Brien SJ, et al: The anatomy and histology of the rotator interval capsule of the shoulder. Clin Orthop 2001;390:129-137.
Jost B, Koch PP, Gerber C: Anatomy and functional aspects of the rotator interval. J Shoulder Elbow Surg 2000;9:336-341.
Question 96
What is the primary problem in rickets osteomalacia?
Explanation
Question 97
- A 32-year-old has diffuse pain, weakness, and limited overhead motion in the shoulder as a result of falling on his outstretched arm 2 months ago. Examination reveals medial scapular winging, and an electromyogram shows denervation of the long thoracic nerve. Management should consist of
Explanation
Question 98
A 40-year-old man has had hip pain with increased activity over the past year. Examination reveals restriction of motion and tenderness with combined hip flexion, adduction, and internal rotation. An AP radiograph is shown in Figure 34. What is the most likely diagnosis? Review Topic

Explanation
Question 99
When compared with reamed intramedullary nailing for an unstable diaphyseal tibia fracture, unreamed nailing is associated with which of the following?
Explanation
Question 100
A 29-year-old man undergoes surgery for a grade I isthmic spondylolisthesis at L5. Following surgery, what type of brace will best immobilize the L5-S1 motion segment?
Explanation
REFERENCES: Connolly PJ, Grob D: Bracing of patients after fusion for degenerative problems of the lumbar spine: Yes or no? Spine 1998;23:1426-1428.
Fidler MW, Plasmans CM: The effect of four types of support on the segmental mobility of the lumbosacral spine. J Bone Joint Surg Am 1983;65:943-947.
