Orthopedic MCQ Exam: Arthroplasty, Trauma & Upper Extremity | Part 250

Key Takeaway
This page presents Part 250 of an interactive Multiple-Choice Question (MCQ) set designed for orthopedic surgeons preparing for their AAOS and ABOS board certification exams. It features 100 verified, high-yield questions, modeled on official formats. Users can choose between Study and Exam modes to master clinical scenarios and ensure comprehensive exam readiness.
About This Board Review Set
This is Part 250 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 250
This module focuses heavily on: Arthroplasty, Dislocation, Elbow, Hip, Knee, Nerve, Revision, Trauma, Wrist.
Sample Questions from This Set
Sample Question 1: At the time of revision total knee arthroplasty, the surgeon is trialing the knee and finds that it extends fully and is stable in flexion with a 23-mm trial spacer; however, the patella is impinging on the polyethylene spacer. No augments ...
Sample Question 2: Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?...
Sample Question 3: A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month follow-up appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph i...
Sample Question 4: Figures 48a and 48b show the elbow radiographs of a 5-year-old boy who fell from a tree after dinner. Examination reveals that he is unable to extend his wrist. Management should consist of immediate...
Sample Question 5: A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicatedleft primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A ra...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
At the time of revision total knee arthroplasty, the surgeon is trialing the knee and finds that it extends fully and is stable in flexion with a 23-mm trial spacer; however, the patella is impinging on the polyethylene spacer. No augments were used on the femur or the tibia because the components fit well without them. What is the most appropriate action at this time?
Explanation
REFERENCES: Laskin RS: Joint line position restoration during revision total knee replacement. Clin Orthop Relat Res 2002;404:169-171.
Yoshii I, Whiteside LA, White SE, et al: Influence of prosthetic joint line position on knee kinematics and patellar position. J Arthroplasty 1991;6:169-177.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction
Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 123-145. Question 100
A 68-year-old woman is undergoing a cementless medial/lateral tapered femoral placement during a total hip arthroplasty and the surgeon notices a small crack forming in the anteromedial femoral neck with final implant insertion. The most appropriate management should include which of the following?
Placement of a cerclage cable around the femoral neck above the lesser trochanter
Removal of the implant, placement of a cable around the femoral neck above the lesser trochanter, and reinsertion of the implant
Removal of the press-fit implant and cementing of the same femoral stem
Final seating of the cementless femoral component without additional measures
Removal of the cementless femoral component and placement of a revision modular taper- fluted femoral stem
DISCUSSION: The recognized treatment of the proximal periprosthetic fracture is first to identify its extent and then to optimize the correction. Removing the implant seems logical to accomplish the identification. Several studies indicate that proximal cerclage wiring is adequate to create a “barrel hoop” stability of the proxima l femur. The postoperative management may also include protected weight bearing and periodic radiographs.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Warren PJ, Thompson P, Fletcher MD: Transfemoral implantation of the Wagner SL stem: The abolition of
subsidence and enhancement of osteotomy union rate using Dall-Miles cables. Arch Orthop Trauma Surg 2002;122:557-560.
Your Source for Lifelong Orthopaedic Learning
Question 2
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
Question 3
A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month follow-up appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph is shown in Figure 21. What is the most likely diagnosis?
Explanation
REFERENCES: Schantz K, Reigels-Nielsen P: The anterior interosseous nerve syndrome.
J Hand Surg Br 1992;17:510-512.
Seror P: Anterior interosseous nerve lesions: Clinical and electrophysiological features. J Bone Joint Surg Br 1996;78:238-241.
Question 4
Figures 48a and 48b show the elbow radiographs of a 5-year-old boy who fell from a tree after dinner. Examination reveals that he is unable to extend his wrist. Management should consist of immediate
Explanation
REFERENCES: Iyengar SR, Hoffinger SA, Townsend DR: Early versus delayed reduction and pinning of type III displaced supracondylar fractures of the humerus in children: A comparative study. J Orthop Trauma 1999;13:51-55.
Leet AI, Frisancho J, Ebramzadeh E: Delayed treatment of type 3 supracondylar humerus fractures in children. J Pediatr Orthop 2002;22:203-207.
Question 5
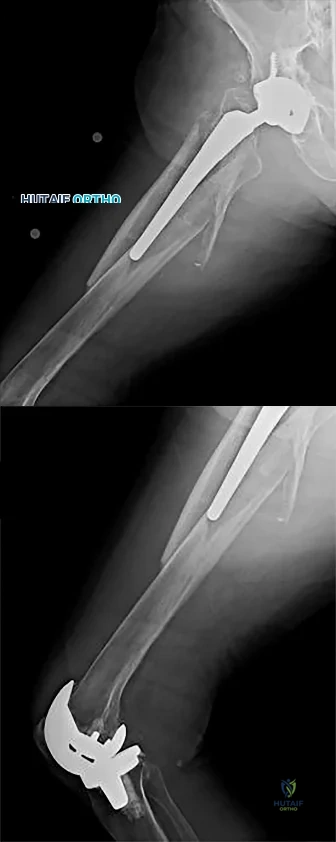
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?
Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 6
A year-old man who underwent left partial knee arthroplasty 6 months earlier was doing well until he experienced left knee pain and swelling for 4 weeks following a dental procedure. The left knee aspirate was bloody, with a white blood cell count of 8,000 and 70% neutrophils. Culture grew group B Streptococcus ( Granulicatella adiacens ), and serologies were elevated, with an erythrocyte sedimentation rate of 55 mm/h (reference range: 0 to 20 mm/h) and a C-reactive protein level of 24 mg/L (reference range: 08 to 1 mg/L). What is the best next step?
Explanation
This complication is best addressed with either a single-stage or two-stage total knee arthroplasty. A recent report suggests that a single-stage arthroplasty can be effective, although many surgeons would perform a two-stage procedure with an articulating or static spacer. Arthroscopic would be non-effective, especially given 4 weeks of symptoms. Resection arthroplasty without a spacer would leave an unstable and poorly functioning extremity. Knee fusion should be used as a salvage procedure.
ERGUIDE MCQ 401-450
ORTHOPEDICS HYPERGUIDE MCQ 351-400
ORTHOPEDICS HYPERGUIDE MCQ 301-350
ORTHOPEDICS HYPERGUIDE MCQ 251-300
ORTHOPEDICS HYPERGUIDE MCQ 201-250
ORTHOPEDICS HYPERGUIDE MCQ 151-200
ORTHOPEDICS HYPERGUIDE MCQ 101-150
FREE Orthopedics MCQS 2022 51-100
Orthopedics Hyperguide MCQ 1-50
Question 7
When the elbow is extended and an axial load is applied, what percent of stress distribution occurs across the ulnohumeral and radiohumeral articular surface, respectively?
Explanation
REFERENCES: Halls AA, Travill R: Transmission of pressure across the elbow joint. Anat Rec 1964;150:243.
Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000.
Question 8
An 18-year-old high school basketball player is being treated for Achilles tendinitis. What type of strengthening exercise has been shown to be helpful in the later phases of rehabilitation?
Explanation
All three types of these exercises have not been shown to benefit Achilles tendinitis as much as eccentric exercise.
REFERENCES: Jonsson P, Alfredson H, Sunding K, et al: New regimen for eccentric calf-muscle training in patients with chronic insertional Achilles tendinopathy: Results of a pilot study. Br J Sports Med
2008;42:746-749.
Maffulli N, Walley G, Say ana MK, et al: Eccentric calf muscle training in athletic patients with Achilles tendinopathy. Disabil Rehabil 2008;30:1677-1684.
Question 9
A patient with an unstable pelvic ring injury has just undergone an emergent laparotomy and currently has a packed abdomen. Stabilization of the pelvic ring is performed with an anterior external fixator. What is an advantage of using an external fixator with pins in the iliac crest rather than pins in the anterior inferior iliac spine?
Explanation
Question 10
What is the most common anatomic location for chondrosarcoma?
Explanation
REFERENCES: Marcove RC, Mike V, Hutter RV, et al: Chondrosarcoma of the pelvis and upper end of the femur: An analysis of factors influencing survival time in one hundred and thirteen cases. J Bone Joint Surg Am 1972;54:561-572.
Simon MA, Springfield DS, et al: Chondrosarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 276.
Question 11
Compared with wear rates of metal-on-standard polyethylene bearings (75 to 250 m m/y), the wear rate of metal-on-metal bearings for hip arthroplasty is approximately how many micrometers per year?
Explanation
REFERENCES: McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
Schmalzried TP, Callaghan JJ: Wear in total hip and knee replacements. J Bone Joint Surg Am 1999;81:115-136.
Question 12
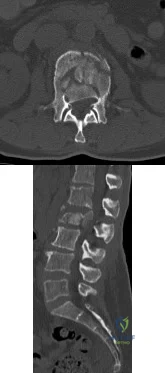
In a retroperitoneal approach to the lumbar spine, what structure runs along the medial aspect of the psoas and along the lateral border of the spine?
Explanation
REFERENCES: Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983, p 107.
Johnson R, Murphy M, Sourthwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Question 13
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis?
Explanation
REFERENCES: Gruen GS, Scioscia TN, Lowenstein JE: The surgical treatment of internal snapping hip. Am J Sports Med 2002;30:607-613.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
Question 14
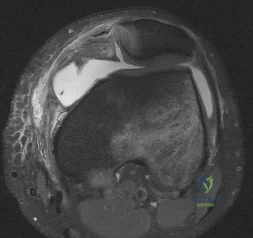
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
Explanation
REFERENCES: Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Fritschy D, Fasel J, Imbert JC, et al: The popliteal cyst. Knee Surg Sports Traumatol Arthrosc 2006;14:623-628.
Question 15
Figure 91 is the radiograph of a 20-year-old man who kicked a door while intoxicated. At the emergency department, his leg is placed into a long-leg cast. After 2 hours, he reports increasing pain, numbness, and tingling in his toes. What is the most appropriate initial treatment?

Explanation
(SBQ12TR.88) When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
A fracture of the radial head requiring ORIF
A highly comminuted radial head fracture requiring radial head arthroplasty or resection
An MCL injury requiring repair
A type I avulsion fracture of the coronoid
An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture. Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:
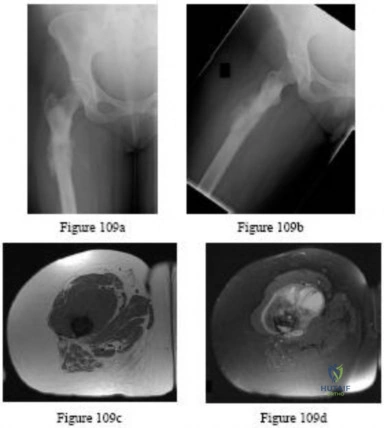
(SBQ12TR.78) A 67-year-old female patient presents with increasing right hip/thigh pain over the past three months, which is now recalcitrant to anti-inflammatories. There is no history of trauma or constitutional symptoms. Her past medical history consists of hypertension, coronary artery disease, osteoporosis and gastric reflux. Physical examination reveals mild pain at the extremes of range of motion of the hip and a painful right sided limp. A radiograph of the right hip is seen in Figure A. What would be the most appropriate treatment for this patient at this time? Review Topic

Observation only
Referral to physiotherapy
MRI spine and hip
Total hip arthroplasty
Intramedullary femoral nail
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers
Question 16
Which of the following best describes the legal definition of standard of care?
Explanation
REFERENCES: Lewis MH, Gohagan JK, Merenstein DJ: The locality rule and the physician’s dilemma: Local medical practices vs the national standard of care. JAMA 2007;297:2633-2637.
AAOS Expert Witness Program, www3.aaos.org/member/expwit/expertwitaess.cfm
Question 17
A 22-year-old javelin thrower reports that he has had increasing discomfort in his right elbow and loss of distance from his throws for the past 3 months. Examination reveals tenderness over the medial elbow. Application of valgus torque to the elbow through a passive range of motion elicits pain from 70 degrees to 120 degrees of flexion, with no pain at the limits of extension. What structure is primarily responsible for the patient's symptoms? Review Topic
Explanation
is a secondary stabilizer at 30 degrees of flexion, and not susceptible to valgus load when the anterior bundle is intact. The annular ligament and triceps insertion are not involved with medial instability of the elbow. Olecranon osteophytes likely cause pain in terminal extension of the elbow.
Question 18
Figure 1 is the MRI scan of a patient with recurrent knee instability, which persists after a period of nonsurgical treatment. Anatomic reconstruction of the torn ligament is recommended. What radiographic finding is the most important independent predictor of recurrent instability following surgery?
Explanation
Question 19
Which of the following anatomic structures are in contact with internal impingement in the throwing athlete?
Explanation
85% of patients undergoing arthroscopy for various indications in one study. Internal impingement is defined as impingement of the posterior-superior rotator cuff between the humerus and posterior-superior glenoid rim. Symptomatic internal impingement is felt to be due to the frequency and magnitude of the impingement in throwers.
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 252.
Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40.
Question 20
Figure 24 shows the radiograph of a 47-year-old woman who has severe right hip pain and a limp. Management should consist of
Explanation
REFERENCE: Jaroszynski G, Woodgate IG, Saleh KJ, Gross AE: Total hip replacement for the dislocated hip. Instr Course Lect 2001;50:307-316.
Question 21
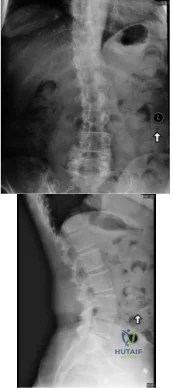
A 65 year-old female presents to your clinic with a chief complaint of difficulty walking. She states that she has had low back pain and balance difficulties for the last 2 years, but over the last few months new bilateral posterior thigh and buttock pain has prevented her from walking more than 100 feet. She states the only place she can walk comfortably is in the grocery store. On physical exam she is unable to preform a tandem gait, and she has 5/5 strength with hip flexion, knee flexion/extension, ankle dorsiflexion/plantar flexion and great toe extension. Her sensation is intact in L2-S2, and she has equal and symmetric 3+ achilles and patellar reflexes. She has 8 beats of clonus, and a down-going Babinski reflex bilaterally.
Explanation
While 79% of patients with cervical myelopathy will have at least one sign on physical exam, the absence of a one or more signs such as a Babinski reflex or a Hoffman's sign does not rule out the diagnosis of myelopathy. Tandem cervical and lumbar stenosis occurs in between 5 and 25% of patients with lumbar stenosis, and because of the stepwise progressive nature of myelopathy, it is critical not to miss this diagnosis.
Rhee et al. found that the sensitivity and specificity of specific physical exam findings varies in patients with myelopathy. Overall 79% of patients will have at least one physical exam sign of myelopathy, with biceps hyperreflexia (62%) and the Hoffman sign (59%) being the most sensitive. Classic upper motor neuron findings in the lower extremity such as an upward Babinski reflex (13%) and clonus (13%) are not sensitive.
Lee et al. performed a cadaveric study of 440 specimens to identify the overall prevalence of stenosis in the population. They found 5.4% of the specimens had cervical stenosis and 5.9% had lumbar stenosis. A total of 0.9% had both cervical and lumbar stenosis.
Bajwa et al. evaluated over 1,000 skeletal remains to determine if tandem stenosis (concomitant lumbar and cervical stenosis) is due to an increased risk of disc degeneration or a congenitally small vertebral canal, and they concluded that tandem stenosis is likely due to a congenitally small vertebral canal in both the cervical and lumbar spine.
Figure A and B demonstrate an AP and lateral radiograph of the lumbar spine respectively. A degenerative L4/5 spondylolisthesis is present.
Incorrect answers:
Question 22
A 78-year-old woman has a history of chronic low back pain. She denies any extremity problems. Her pain is worse in the morning, and gets better, although it does not go away, as the day goes on. An MRI scan of the lumbar spine is shown in Figure 88. She denies any acute worsening of her symptoms, although in general, her symptoms are slowly worsening. She takes nonsteroidal anti-inflammatory drugs as needed for her pain, but otherwise takes no other medications. What is the next most appropriate step in management? Review Topic

Explanation
Question 23
What neurologic structure is most at risk when performing intramedullary screw fixation of a fifth metatarsal base fracture?
Explanation
REFERENCES: Donley BG, McCollum MJ, Murphy GA, Richardson EG: Risk of sural nerve injury with intramedullary screw fixation of fifth metatarsal fractures: A cadaver study. Foot Ankle Int 1999;20:182-184.
Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 24
Figures 86a through 86c are the radiographs and biopsy specimen of a 14-year-old boy who has had left knee pain for 4 weeks. What is the most likely diagnosis?
Explanation
Question 25
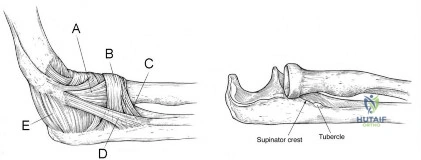
A 25-year-old athlete presents with symptoms attributed to injury to ligament D in Figure A. Which of the following symptoms and signs is characteristic of this injury? Review Topic
Explanation
PLRI can be diagnosed using the lateral pivot shift or posterolateral drawer. According to O’Driscoll, the elbow dislocates in 3 stages from lateral to medial (circle of Horii). Stage 1 involves disruption of the LUCL and partial/total disruption of the LCL complex (creating PLRI). Patients have pain with varus stress. Stage 2 includes disruption of the anterior capsule from incomplete elbow posterolateral dislocation. Stage 3 is divided into:
(a) Disruption of all soft tissues surrounding/ including the posterior MCL except for the anterior bundle. This bundle forms the pivot around which the elbow dislocates in a posterior direction by way of a posterolateral rotatory mechanism; and (b) complete disruption of the MCL.
O'Driscoll et al. describe PLRI diagnosed in 5 patients who had elbow dislocation using the posterolateral rotatory instability test, which they describe as being analogous to the test for lateral rotatory instability of the knee after ACL rupture. They believed the condition was laxity of the LUCL, which allowed transient rotatory subluxation of the ulnohumeral joint and secondary dislocation of the radiohumeral joint, without radio-ulnar joint dislocation. They recommended repair of the LUCL to eliminate PLRI.
Sanchez-Sotelo et al. retrospectively described 12 cases of direct repair and 33 ligamentous reconstructions for PLRI. 86% were satisfied with the procedure. Better results were obtained with patients with post-traumatic etiology, instability at presentation, and those with augmented reconstruction with tendon graft (compared with ligament repair alone).
Figure A shows structures on the lateral side of the elbow. The corresponding labels are seen in Illustration A. Illustration B shows the lateral pivot shift (also known as the posterolateral rotatory instability test).
Incorrect Answers:
Question 26
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
Explanation
A. Lateral head of triceps (radial nerve) and brachialis
(musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii
(musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis
(musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis
(musculocutaneous nerve)
Question 27
A 62-year-old woman undergoes a posterior laminectomy and fusion from L3 to S1. Postsurgical images show a pelvic incidence (PI) that is significantly larger than the lumbar lordosis (LL).
Explanation
Sagittal balance is becoming increasingly important. PI should be roughly equal to LL. A PI larger than the LL has been associated with a higher incidence of PJK. PJK also is associated with larger sagittal balance corrections. Additional risk factors include higher presurgical thoracic kyphosis, higher postsurgical lordosis, osteoporosis, fusion below L2, and older (greater than 65 years old) patient age. The loss of somatosensory-evoked potentials during surgery, especially during osteotomy correction, is concerning for neurological injury and should be investigated. If no other cause for a change in signals can be identified, the correction should be lessened to take pressure off of the nerves.
RECOMMENDED READINGS
Ghobrial GM, Thakkar V, Andrews E, Lang M, Chitale A, Oppenlander ME, Maulucci CM, Sharan AD, Heller J, Harrop JS, Jallo J, Prasad S. Intraoperative vancomycin use in spinal surgery: single institution experience and microbial trends. Spine (Phila Pa 1976). 2014 Apr 1;39(7):550-5. doi: 10.1097/BRS.0000000000000241. PubMed PMID: 24480966. View
Abstract at PubMed
Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. View Abstract at PubMed
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
Review. PubMed PMID: 21102290. View Abstract at PubMed
Kim HJ, Bridwell KH, Lenke LG, Park MS, Song KS, Piyaskulkaew C, Chuntarapas T. Patients with proximal junctional kyphosis requiring revision surgery have higher postoperative lumbar lordosis and larger sagittal balance corrections. Spine (Phila Pa 1976). 2014 Apr 20;39(9):E576-80. doi: 10.1097/BRS.0000000000000246. PubMed PMID: 24480958. View
Abstract at PubMed
Maruo K, Ha Y, Inoue S, Samuel S, Okada E, Hu SS, Deviren V, Burch S, William S, Ames CP, Mummaneni PV, Chou D, Berven SH. Predictive factors for proximal junctional kyphosis in long fusions to the sacrum in adult spinal deformity. Spine (Phila Pa 1976). 2013 Nov 1;38(23):E1469-76. doi: 10.1097/BRS.0b013e3182a51d43. PubMed PMID: 23921319. View
Abstract at PubMed
Radcliff KE, Kepler CK, Jakoi A, Sidhu GS, Rihn J, Vaccaro AR, Albert TJ, Hilibrand AS. Adjacent segment disease in the lumbar spine following different treatment interventions. Spine J. 2013 Oct;13(10):1339-49. doi: 10.1016/j.spinee.2013.03.020. Epub 2013 Jun 15. Review. PubMed PMID: 23773433. View Abstract at PubMed
Lee JH, Kim JU, Jang JS, Lee SH. Analysis of the incidence and risk factors for the progression of proximal junctional kyphosis following surgical treatment for lumbar degenerative kyphosis: minimum 2-year follow-up. Br J Neurosurg. 2014 Apr;28(2):252-8. doi: 10.3109/02688697.2013.835369. Epub 2013 Dec 9. PubMed PMID: 24313308.
View Abstract at PubMed
Question 28
With respect to the structure identified by the arrow in Figure 22b, the meniscofemoral 25 ligaments are
Explanation
The stress radiographs demonstrate posterior instability of the right knee in flexion. The MR images demonstrate injury to both the anterior and posterior cruciate ligament (PCL), with the stump identified with the arrow on the MR image (Figure 22b). The PCL has 2 functional bands. The anterolateral bundle originates from the roof of the intercondylar notch. It runs in a posterolateral direction onto the tibial crest between the posterior attachment of the medial and lateral menisci. During a double-bundled posterior ligament reconstruction, the
anterolateral bundle is tensioned with the knee in a position of mid flexion. The posteromedial bundle has a variable pattern of tension both in extension and in high flexion. Tensioning of the posteromedial bundle in extension may contribute to resistance against knee hyperextension.
The meniscofemoral ligaments are variably present. Although 93% of knees have been reported to have at least 1 meniscofemoral ligament present, both ligaments are simultaneously present in approximately 50% of knees. The ligament of Humphrey (anterior meniscofemoral ligament) and ligament of Wrisberg (posterior meniscofemoral ligament) are delineated by their anatomic relationship to the posterior cruciate.
RECOMMENDED READINGS
Amis AA, Bull AM, Gupte CM, Hijazi I, Race A, Robinson JR. Biomechanics of the PCL and related structures: posterolateral, posteromedial and meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2003 Sep;11(5):271-81. Epub 2003 Sep 5. Review. PubMed PMID: 12961064.View Abstract at PubMed
Amis AA, Gupte CM, Bull AM, Edwards A. Anatomy of the posterior cruciate ligament and the meniscofemoral ligaments. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):257-63. Epub 2005 Oct 14. Review. PubMed PMID: 16228178.
View Abstract at PubMed . 26
Question 29
Which of the following methods best aids in diagnosis of an interdigital neuroma?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 145-147.
Bennett GL, Graham CE, Mauldin DM: Morton’s interdigital neuroma: A comprehensive treatment protocol. Foot Ankle Int 1995;16:760-763.
Question 30
When planning a research study, the power of the study may be increased by
Explanation
Question 31
A 5-year-old girl sustained a comminuted Salter-Harris type IV fracture of the left distal tibia 2 years ago. The AP radiograph shown in Figure 54a reveals a growth arrest and a 1.4-cm limb-length discrepancy. The ankle is in approximately 20 degrees of varus. Figure 54b shows a coronal reconstruction image of the distal tibial physis, and Figure 54c shows a sagittal reconstruction image of the same area. On the sagittal reconstruction image, the bar extends from the 9-mm mark to the 24-mm mark in 3-mm increments. On the coronal image, the bar extends from the 9-mm mark to the 24-mm mark, also in 3-mm increments. A map of the physeal bar based on these measurements is shown in Figure 54d. Initial treatment should consist of
Explanation
REFERENCES: Carlson WO, Wenger DR: A mapping method to prepare for surgical excision of a partial physeal arrest. J Pediatr Orthop 1984;4:232-238.
Peterson HA: Partial growth plate arrest and its treatment. J Pediatr Orthop 1984;4:246-258.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 32
A teenager is undergoing a correction of deformity and lengthening of the femur. Distractions are proceeding as expected; however, during his 6-week follow-up examination, the patient reports that the distraction motors have become harder to turn over for the past 2 to 3 days. Figures 37a and 37b show current radiographs. What is the most likely complication being encountered?
Explanation
REFERENCES: Paley D: Problems, obstacles and complications of limb lengthening, in Maiocchi AB, Aronson J (eds): Operative Principles of Ilizarov. Baltimore, MD, Williams & Wilkins, 1991, p 360.
Herring JA: Limb length discrepancy, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics,
ed 3. Philadelphia, PA, WB Saunders, 2002, p 1088.
Question 33
A 30-year-old man has had leg pain for 6 months. A lesion is identified in the proximal femur and biopsy it taken. Histology is shown in Figure A and is consistent with a low-grade intramedullary osteogenic sarcoma. Additional imaging studies confirm that this is an isolated lesion with no metastasis. What is the standard treatment for this type of lesion?
Explanation
Choong et al. reviewed the long term follow-up of 20 patients diagnosed with low grade osteogenic sarcoma and found the 5 year survival rate was 90% and at 10 years was 85%. Local recurrence is a key feature in most cases and is typically the result of inadequate surgical margins frequently arising from initial misdiagnosis. Although amputation generally is successful for primary and recurrent tumors, limb salvage surgery is a definite option.
Kurt et al reviewed 80 well-differentiated osteosarcomas. They found local excision was almost always associated with recurrence. Wide excision was
almost never followed by recurrence. The recurrent tumor was a high-grade, conventional osteosarcoma in 15% of the patients, and this was associated with a poor prognosis. They recommend wide excision as the treatment of choice for this very rare variant of osteosarcoma.
A 32-year-old male sustains a the injury shown in Figure A after a high-speed motor vehicle collision. Which factor has been found to have the highest direct correlation with severe heterotopic ossification after traumatic knee dislocation?

Injury Severity Score (ISS )
Glascow Coma Scale (GCS )
Timing of knee reconstruction
Number of ligaments reconstructed
Open ligament reconstruction
Figure A shows a knee dislocation with cruciate ligament avulsion injuries. Development of significant heterotopic ossification (HO) formation has been shown to be most directly correlated to the ISS score.
Mills and Tejwani looked at multiple variables including injury severity score
( ISS), Glascow coma scale (GCS), closed head injury (CHI), timing of surgery (> or < 3 weeks) and type of surgery (open vs. arthroscopic, number of ligaments reconstructed) in its relation to the formation of HO following knee dislocation. In the final group the sensitivity and specificity of the ISS in relation to HO formation was 100%, while presence of CHI had a specificity of 97 %. Timing, type of surgery and approach did not influence HO formation.
A 52-year-old male presents with 6 months of swelling and pain in his leg. He states the lesion has not changed in size for several months and doesn't bother him. He is otherwise healthy and has no other complaints. Representative photograph and MRI are shown in Figures A through C. What is the best initial step in his management?
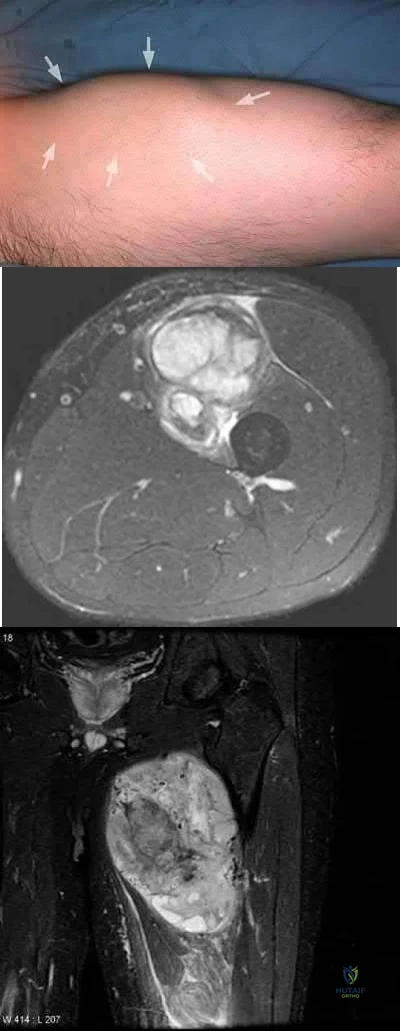
Follow-up in 6 months with repeat radiographs
Biopsy
Marginal excision
Radiation therapy
Neoadjuvant chemotherapy and wide excision
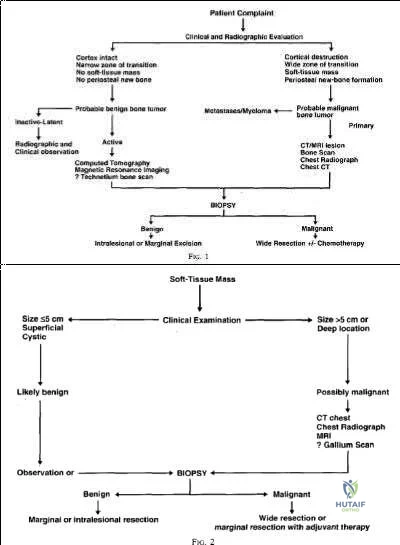
The initial step in management of a patient presenting with a large soft tissue mass deep to the fascia is to obtain a tissue diagnosis, via biopsy. Initiation of treatment prior to tissue diagnosis is inappropriate and can result in significant patient morbidity and potential mortality. While some soft tissue sarcomas may benefit from chemotherapy, this cannot be initiated prior to diagnosis.
Radiation therapy is used in the treatment of soft tissue sarcoma, but again, only after tissue diagnosis. Peabody et al review the appropriate evaluation and staging for musculoskeletal neoplasms and present flow-charts useful in the work-up of bone (Illustration A) and soft tissue (Illustration B) neoplasms. Skrzynski et al performed a comparison of outpatient core-needle biopsy with open surgical biopsy for musculoskeletal tumors. They found the diagnostic accuracy of core-needle biopsy was only 84% with many samples yielding no or different histological samples when compared to final resected specimens. They conclude that while core-needle biopsy is significantly less expensive
than surgical biopsy ($1106 vs. $7234), there is higher concern for sampling error or general diagnostic inaccuracy associated with a core-needle biopsy compared to open biopsy, the "gold standard".
What is the appropriate treatment for a 10-year-old boy with Ewing's sarcoma isolated to the proximal femur?
Neoadjuvant chemotherapy and surgical excision
Neoadjuvant chemotherapy, surgical excision, and radiation therapy
Neoadjuvant chemotherapy, surgical excision, and adjuvant chemotherapy
Neoadjuvant radiation therapy and surgical excision
Surgical excision and hormonal therapy
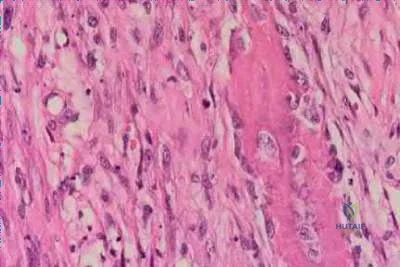
Ewing's sarcoma is a malignant small round blue cell neoplasm which has a predilection for long tubular bones, pelvis, and ribs. The radiographic appearance of "onion-skinning" seen in illustrations A and B is due to the body's periosteal reaction. Illustration C shows the large soft tissue extraosseous mass characteristic for Ewing's sarcoma. Finally, Illustration D shows the histology where the multiple small round blue neoplastic cells are seen.
Ewing's sarcoma is most commonly treated with neoadjuvant chemotherapy, surgical excision, and adjuvant chemotherapy - in particular for tumors located in bones which can be easily resected and reconstructed. For large tumors in areas which either cannot be completely excised or where excision is associated with significant morbidity, some centers consider chemotherapy and radiation therapy without surgical excision. There is a current trend towards surgical resection and away from irradiation for Ewing's sarcoma even though it is radiosensitive, because of the risk of secondary malignancy and growth disturbance due to radiation.
Pierz et al review many of the common bone tumors including Ewing's sarcoma and discuss the relevant diagnostic factors as well as specific treatment protocols for each tumor.

A 30-year-old female presents with a painful posterior knee mass. The mass gets larger and more painful with activity. Examination reveals a boggy soft tissue mass about her knee. Radiograph and MRI are shown in Figures A and B. What is the most likely diagnosis?

Synovial sarcoma
Hemangioma
Lipoma
Parosteal osteosarcoma
Pigmented villonodular synovitis (PVNS )
This patients history, physical exam, and imaging studies are suggestive of a hemangioma. Pain in hemangiomas is thought to occur due to vascular engorgement secondary to activity and increased blood flow to the lesion. The calcification on the plain radiograph and the fat of the T1 MRI are diagnostic for hemangioma. Current treatment for symptomatic hemangiomas includes some combination of sclerotherapy or vascular coiling, with surgical excision
reserved for few cases. The two attached reviews by Gilbert et al and Damron et al review the history, diagnosis, treatment, and controversial issues in soft tissue sarcomas and benign sarcoma like conditions such as hemangiomas.
Current treatment for soft tissue sarcomas includes radiotherapy and surgical excision. While many centers in the world use chemotherapy for soft tissue sarcomas, the data supporting its use is quite limited and likely too controversial to be tested. With regard to the other answer choices, synovial sarcoma and lipoma can show calcification on radiographs, but they are usually not painful and image differently on T1 MRI. Parosteal osteosarcoma typically occurs in this location (posterior distal femur) but occurs as a lesion stuck on the bone. PVNS can have a similar appearance on imaging, but doesn't cause this type of pain.
Question 34
A 21-year-old man with neurofibromatosis and multiple cutaneous neurofibromas has a rapidly enlarging painless mass on his buttock. Examination reveals a nontender, well-defined 6- x 6-cm soft-tissue mass that is deep to the fascia. The best course of action should be to order
Explanation
REFERENCES: Demas BE, Heelan RT, Lane J, Marcove R, Hajdu S, Brennan MF: Soft-tissue sarcomas of the extremities: Comparison of MR and CT in determining the extent of disease. Am J Roentgenol 1988;150:615-620.
Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft-tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547.
Question 35
A 24-year-old runner who underwent an allograft reconstruction of the anterior cruciate ligament (ACL) 3 years ago now reports anterior knee pain. Examination reveals no swelling or effusion, and the patient has full motion. A Lachman test and a pivot-shift test are negative. Palpation reveals tenderness on the patellar tendon and at the inferior pole of the patella. AP and lateral radiographs are shown in Figures 41a and 41b. Management should consist of
Explanation
REFERENCES: Fahey M, Indelicato PA: Bone tunnel enlargement after anterior cruciate ligament replacement. Am J Sports Med 1994;22:410-414.
Victoroff BN, Paulos L, Beck C, Goodfellow DB: Subcutaneous pretibial cyst formation associated with anterior cruciate ligament allografts: A report of four cases and literature review. Arthroscopy 1995;11:486-494.
Question 36
A 14-year-old girl has a painful hallux valgus deformity that has not responded to shoe modifications. Figure 21 shows a standing AP radiograph. What is the most appropriate surgical procedure?
Explanation
and a congruent metatarsophalangeal joint with an abnormal distal metatarsal articular
angle. Correction of both of these abnormalities requires a proximal and distal first
metatarsal osteotomy.
REFERENCES: Coughlin M: Juvenile bunions, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 297-339.
Peterson HA, Newman SR: Adolescent bunion treated with double osteotomy and longitudinal pin fixation of the first ray. J Pediatr Orthop 1993;13:80-84.
Question 37
After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office with continued pain 2 years after surgery. He describes instability, particularly when descending stairs. Upon examination, there is range of motion from 0 to 120 degrees with no extensor lag. The knee is stable to varus and valgus stress in extension, but there is flexion instability in both the anterior-posterior direction and in the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection workup is negative. What is the most appropriate surgical intervention at this time?
Explanation

Video 99 for reference
This patient has valgus knee alignment, and, after undergoing appropriate bone resections and soft-tissue balancing, has demonstrated a tight PCL on trial reduction as evidenced by lift-off of the trial insert as described by Scott and Chmell. The appropriate maneuver is PCL recession with partial release of tight (usually anterolateral) PCL fibers. However, for this patient, instability resulted in increased anterior translation. At this stage, the options are to convert to either a deeper-dish insert with increased sagittal conformity or a posterior stabilized insert. The only appropriate choice among the responses is use of an insert with increased sagittal conformity to prevent excessive anterior translation. Increasing the polyethylene could improve stability in flexion, but, considering there is good stability in extension, this likely would lead to an inability to achieve full extension. The patient’s valgus deformity, flexion contracture, correction with release of the iliotibial band, and posterolateral capsule predispose him to increased risk for peroneal nerve palsy. His symptoms at follow-up suggest knee flexion
instability with pain, swelling, and difficulty descending stairs. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant depending on the condition of the ligaments likely is needed to address his symptoms. The difference in extension vs flexion stability makes polyethylene exchange a poor option. There is no reason to believe a constrained rotating hinge design is necessary. Repeat use of a PCL-retaining insert is not recommended.
Question 38
Radiographs of an 80-year-old woman with back pain reveal a compression fracture. Which of the following imaging studies best evaluates the acuity of the fracture?
Explanation
REFERENCES: Phillips FM: Minimally invasive treatments of osteoporotic vertebral compression fractures. Spine 2003;28:S45-S53.
Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 39
The afferent pain innervation of the L3-L4 facet joint arises from the medial branch nerve of
Explanation
REFERENCES: Nade SL, Bell E, Wyke BD: The innervation of the lumbar spinal joint and its significance. J Bone Joint Surg Br 1980;62:255-261
Kornick C, Kramarich SS, Lamer TJ, et al: Complications of lumbar facet radiofrequency denervation. Spine 2004;29:1352-1354.
Question 40
As a diaphyseal fracture heals, peripheral callus forms about the shaft axis, creating a structure with a substantially larger diameter than the original diaphyseal shaft. What biomechanical properties does this callus impart to the healing fracture site?
Explanation
The biomechanical role of the peripheral callus is to provide initial stability to the fracture and to act as a scaffold for gradual mineralization. Because the bending stiffness of a structure is proportional to the 4th power of the diameter, a peripherally located callus provides substantial stability to the fracture, despite the relatively low stiffness and strength of callus. For example, doubling the diameter of the callus increases the resistance to bending by a factor of 16. As mineralization progresses, the bending stiffness and strength of the healed fracture eventually may be substantially greater than that of the original, intact bone.
Augat et al. review the mechanical and biological aspects of fracture healing. They report that increased diameter of periosteal callus formation benefits healing by enlarging the cross-sectional area of area of the bridging tissue and reducing interfragmentary motion. Patients with osteoporosis are known to have decreased callus mineralization and biomechanical properties.
Incorrect Answers:
Question 41
The natural history of cervical spondylolytic myelopathy is best described as
Explanation
REFERENCES: Emery SF: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Lees F, Turner JA: The natural history and prognosis of cervical spondylosis. Brit Med J 1963;2:1607-1610.
Clarke E, Robinson PK: Cervical myelopathy: A complication of cervical spondylosis. Brain 1956;79:486-510.
Question 42
A 13-year-old girl who competes in gymnastics reports the insidious onset of lateral left elbow pain over the past 6 months. She also notes occasional catching episodes in the elbow; however, she denies any history of trauma. Examination reveals tenderness over the lateral epicondyle and extensor muscle origin. The elbow is stable and has full flexion, but lacks 10° of full extension. An AP plain radiograph and an MRI scan are shown in Figures 17a and 17b. Management of the elbow should consist of
Explanation
REFERENCES: Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med
1998;26:520-530.
Jackson DW, Silvino N, Reiman P: Osteochondritis in the female gymnast’s elbow. Arthroscopy 1989;5:129-136.
Ruch DS, Cory JW, Poehling GG: The arthroscopic management of osteochondritis dissecans of the adolescent elbow. Arthroscopy 1998;14:797-803.
Question 43
A 68-year-old man presents with severe right shoulder pain. He had a prolonged course of physical therapy and received several cortisone injections for his pain without improvement. Examination reveals pseudoparalysis of the right shoulder with a 20-degree external rotation lag with the shoulder adducted. With the shoulder placed in 90 degrees of abduction, he can actively externally rotate his shoulder. The patient was treated with a medialized reverse prosthesis shown in Figure A. Which of the following statement is true regarding this treatment option? Review Topic

Explanation
RTSA is most commonly indicated for rotator cuff arthropathy. However, indications for use now include shoulder pseudoparalysis, anterosuperior escape of the humeral head, acute 3 or 4-part proximal humerus fractures, and greater tuberosity fracture nonunions. Contraindications to RTSA included deltoid dysfunction, insufficient glenoid bone stock, and bony deficiency of the acromion.
Edwards et al. prospectively evaluated the risk of shoulder dislocation after reverse TSA. They found a significantly increased risk of dislocation (p=0.012) in patients with an irreparable subscapularis at time of surgery. There were no dislocations in the reparable group. Dislocations were more likely in patients with proximal humeral nonunions and failed prior arthroplasty.
Mulieri et al. looked at the use of reverse TSA in patients with irreparable massive rotator cuff tears without evidence of glenohumeral arthritis. All outcomes were improved postoperatively, and they advocate for reverse TSA in this subset of patients. Survivorship was over 90% at more than 4 years average follow up.
Boileau et al. evaluated the clinical outcomes of isolated biceps tenotomy/tenodesis in patients with massive rotator cuff tears and a biceps lesion. They found that the procedure can effectively treat pain and improve function in these patients. There was no difference in patients undergoing tenotomy versus tenodesis.
Figure A is a right shoulder radiograph status post RTSA with components in adequate position.
Incorrect Answers:
Question 44
A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb “feels” different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?
Explanation
REFERENCES: Levy BA, Zlowodzki MP, Graves M, et al: Screening for extremity arterial injury with the arterial pressure index. Am J Emerg Med 2005;23:689-695.
Abou-Sayed H, Berger DL: Blunt lower-extremity trauma and politeal artery injuries: Revisiting the case for selective arteriography. Arch Surg 2002;137:585-589.
Mills WJ, Barei DP, McNair P: The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: A prospective study. J Trauma 2004;56:1261-1265.
Question 45
Retrograde ejaculation is most commonly associated with what surgical approach?
Explanation
REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983,
p 107.
An HS, Riley LH III: An Atlas of Surgery of the Spine. New York, NY, Lippincott Raven, 1998, p 263.
Question 46
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury? Review Topic
Explanation
Question 47
A 48-year-old ski instructor dislocates his nondominant shoulder in a fall. Management consisting of application of a sling for 1 week results in improvement in his pain. Follow-up examination 6 weeks after the injury reveals that the patient continues to have difficulty with shoulder elevation. Management should now include
Explanation
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 48
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the
Explanation
REFERENCES: Miller DB Jr: Arthroscopic meniscus repair. Am J Sports Med 1988;16:315-320.
Nawab A, Hester PW, Caborn DN: Arthroscopic meniscus repair, in Miller MD, Cole BJ (eds): Textbook of Arthroscopy. Philadelphia, PA, WB Saunders, 2004, pp 517-537.
Question 49
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior-stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful total knee arthroplasty.
Question 50
Which of the following diseases has documented transmission by allograft tissue transplantation in the last 20 years?
Explanation
REFERENCES: McAllister DR, Joyce MJ, Mann BJ, et al: Allograft update: The current status of tissue regulation, procurement, processing, and sterilization. Am J Sports Med 2007;35:2148-2158.
Safety of tissue transplants. American Association of Tissue Banks, 2006. Question 74
Which of the following types of intra-articular pathology is associated with lateral meniscal cysts?
Discoid meniscus
Posterolateral comer injury
Vertical meniscal tears
Middle third lateral meniscal tears
Popliteus tendon tears
DISCUSSION: Lateral meniscal cysts often arise from myxoid degeneration that progresses from the meniscal center and then outside the meniscus. Horizontal cleavage tears are commonly associated with the condition.
Cysts of the lateral meniscus are most commonly the consequence of a tear located in the medial third. If the
tear communicates with the joint, arthroscopic partial meniscectomy and cyst decompression are indicated. If the tear does not open into the joint, arthroscopy should be followed by an open cystectomy.
REFERENCES: Hulet C, Souquet D, Alexandre P, et al: Arthroscopic treatment of 105 lateral meniscal cysts with 5-year average follow-up. Arthroscopy 2004;20:831-836.
Ferrer-Roca O, Vilalta C: Lesions of the meniscus: Part I. Macroscopic and histologic findings. Clin Orthop
Relat Res 1980;146:289-300.
Ferrer-Roca O, Vilalta C: Lesions of the meniscus: Part II. Horizontal cleavages and lateral cysts. Clin Orthop Relat Res 1980:146:301-307.
Question 51
A 13-year-old baseball pitcher presents with worsening medial-sided elbow pain. He pitches 7 months out of the year, throws 85 pitches per game and plays in two games per week. His fastball speed is approximately 75mph. He regularly plays outfield once he has been relieved of pitching. Which of the following is most likely contributing to his elbow pain? Review Topic
Explanation
Little League elbow is a medial-sided overuse injury that occurs in the skeletally immature athlete. During execution of the baseball pitch, tremendous valgus and extension stresses occur at the elbow. Repetitive microtrauma can ultimately injure the medial epicondyle apophysis, ulnar collateral ligament or the flexor-pronator muscle mass. Limiting the number of pitches and innings played per game, as well as the number of months of competitive pitching per year, has been recommended to prevent these overuse injuries in the young athlete.
Olsen et al performed a case control study to determine risk factors associated with the development of shoulder and elbow injuries in adolescent baseball pitchers. Greater than 8 months of competitive pitching per year, more than 80 pitches per game and a fastball speed of greater than 85mph were all associated with increased risk of injury. Continued pitching despite arm fatigue and pain, being a starting pitcher, greater number of warm-up pitches, participating in showcases and regular use of NSAIDs were also associated with injury. The type of pitch (fastball, changeups and breaking balls) and continued play in a different position once being relieved was not associated with increased risk of injury.
Andrews et al authored a review article on ulnar collateral ligament injuries in throwing athletes. According to the USA Baseball Medical/Safety Advisory Committee, young baseball pitchers should avoid breaking pitches, such as curveballs and sliders, and avoid year-round baseball. A minimum of 3 months of complete rest from pitching per year is vital. Youth pitching coaches should be educated to ensure proper pitching mechanics are being reinforced.
Illustration A is a table depicting the recommended maximum number of pitches by age group.
Incorrect Answers:
Question 52
A 72-year-old man has had persistent pain after undergoing a hemiarthroplasty 18 months ago. Radiographs are shown in Figures 50a and 50b. What is the most likely cause of his problem?
Explanation
REFERENCES: Haidukewych GJ, Israel TA, Berry DJ: Long-term survivorship of cemented bipolar hemiarthroplasty for fracture of the femoral neck. Clin Orthop Relat Res 2002;403:118-126.
Lestrange NR: Bipolar hemiarthroplasty for 496 hip fractures. Clin Orthop Relat Res 1990;251:7-19.
Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, p 158.
Question 53
The initiating cellular event in development of posttraumatic osteoarthritis is attributed to which of the following?
Explanation
Question 54
A 4-year-old girl sustains an isolated spiral femoral fracture after falling from her tricycle. Management should consist of
Explanation
REFERENCES: Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659.
Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365.
Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Levy J, Ward WT: Pediatric femur fractures: An overview of treatment. Orthopedics 1993;16:183-190.
Question 55
A 3-year old child from an isolated mountain area is evaluated for multiple medical problems, including vomiting, loss of appetite, polyuria, and failure to thrive. History reveals the child was normal at birth. The parents, who appear healthy, are second cousins and have two other children who are normal. The parents state that they know of another family member who died at age 6 years after a similar medical history. Radiographs of the lower extremities show bowing of the long bones with cupping and widening of the physes. What is the most likely diagnosis?
Explanation
hemolytic anemia, rhabdomyolysis, and hepatocellular injury that began during refeeding and resolved with treatment. The signs and symptoms, pathophysiology, and treatment of refeeding hypophosphatemia are reviewed.
Renal Osteodystrophy-Musculoskeletal complications in patients with chronic renal failure are common and may be related to the disease itself or to treatment. The altered metabolism in patients with chronic renal failure leads to renal osteodystrophy, which consists of osteomalacia and secondary hyperparathyroidism [1]. Erosive changes attributable to secondary hyperparathyroidism may be easily confused with rheumatoid arthritis, seronegative spondyloarthropathies, infection, or even malignancy.
Primary Hyperparathyroidism-Preferential involvement of cortical bone with apparent preservation of cancellous bone in primary hyperparathyroidism was confirmed by percutaneous bone biopsy. Over 80% of patients had a mean cortical width below the expected mean, whereas cancellous bone volume in over 80% of patients was above the expected mean.
Skeletal disease in primary hyperparathyroidism J Bone Miner Res 1989 Jun; 4(3):283-91
Nutritional vitamin D deficiency-Rickets, osteomalacia, and renal osteodystrophy are disorders of the mineralization of bone that result from a lack of available calcium, phosphorus, or both. The diseases that result from numerous mechanisms present with a symptom-sign-radiographic complex with such a high degree of stereotypy that laboratory investigation is often required to distinguish one form from another. The disorders in children, known as rickets, produce bowing and other deformities of the long bones and dwarfism. These disorders are principally related to the profound effect of the deficiency states on the epiphyseal plate; whereas the same disorders in adults produce an often severe osteopenia and pathologic fractures. Because of newer developments in our understanding of the factors affecting calcium-phosphorus
hemostasis and vitamin D metabolism, many of the children and Rickets, osteomalacia, and renal osteodystrophy.
Question 56
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?
Explanation
REFERENCES: Kelly MA: Extensor mechanism complications in total knee arthroplasty.
Instr Course Lect 2004;53:193-199.
Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Norman AJ, Scott S, David GN (eds): Master Techniques in Knee Arthroplasty, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2003.
Question 57
Figures 174a through 174c are the MRI scans of a 16-year-old football player who dislocated his dominant left shoulder 3 weeks ago while landing on his outstretched arm. The dislocation was reduced in the emergency department. He has since had two episodes where he felt like his shoulder slipped partially out of place. Which of the following statements to the athlete and his parents is most accurate regarding treatment options? Review Topic
Explanation
Question 58
A 42-year-old woman underwent an instrumented posterior spinal fusion at L3-S1 with transforaminal lumbar interbody fusion. She had an excellent
Explanation
Question 59
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include
Explanation
REFERENCES: Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459.
Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Skrzynski MC, Biermann JS, Montag A, Simon MA: Diagnostic accuracy and charge-savings of outpatient core needle biopsy compared with open biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1996;78:644-649.
Question 60
A 16-year-old competitive female swimmer has a 1-year history of left shoulder pain. She denies any specific injury to her shoulder. She reports that the pain is worse with swimming but also has pain with daily activities. She also notes similar occasional symptoms in her right shoulder. Examination reveals symmetric range of motion and rotator cuff strength. Examination of the left shoulder reveals 2+ anterior and posterior translation with pain in both directions and a 2-cm sulcus sign. The right shoulder also has 2+ anterior and posterior translation and a 2-cm sulcus sign with no pain. She also has hyperextension of the elbows and the ability to touch the radial border of her thumb to her forearm. What is the next step in management? Review Topic
Explanation
Question 61
- A 32-year-old has diffuse pain, weakness, and limited overhead motion in the shoulder as a result of falling on his outstretched arm 2 months ago. Examination reveals medial scapular winging, and an electromyogram shows denervation of the long thoracic nerve. Management should consist of
Explanation
Question 62
Treatment of an atrophic nonunion of the radial diaphysis should include which of the following?

Explanation
Question 63
Figure 29 shows the radiograph of a 55-year-old patient who has recurrent total hip dislocation. Dislocation is most likely to occur in this patient when the hip is in which of the following positions?
Explanation
REFERENCE: Paterno SA, Lachiewicz PF, Kelley SS: The influence of patient-related factors and the position of the acetabular component on the rate of dislocation after total hip replacement. J Bone Joint Surg Am 1997;79:1202-1210.
Question 64
Figures 28a and 28b show the radiographs of a 79-year-old man who has constant knee pain. Prior to performing elective knee replacement surgery, management should include
Explanation
REFERENCES: Kaplan FS, Singer FS: Paget’s disease of bone: Pathophysiology, diagnosis, and management. J Am Acad Orthop Surg 1995;3:336-344.
Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 129-184.
Siris ES: Paget’s disease of bone, in Favus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. New York, NY, Raven Press, 1993, pp 375-384.
Question 65
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?
Explanation
REFERENCES: Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
McFarland EG, Hsu CY, Neira C, O’Neil O: Internal impingement of the shoulder: A clinical and arthroscopic analysis. J Shoulder Elbow Surg 1999;8:458-460.
Question 66
Figure A is a pelvic radiograph of a healthy 20-month old girl with a limb leg discrepancy. A hip arthrogram under general anesthesia reveals concentric reduction of the left hip ONLY when the hip is positioned in 70 to 80 degrees of abduction. The next best step in treatment would be: Review Topic

Explanation
capsulorrhaphy, +/- femoral osteotomy +/- pelvic osteotomy
In children older than 18 months, open reduction is the preferred treatment for hip dysplasia. Open reduction is also considered when concentric closed reduction cannot be achieved or when excessive abduction (>60 degrees) is required to maintain reduction (due to increasing risk of avascular necrosis). The goal of open reduction is to remove the blocks to reduction and to increase stability by preforming soft-tissue or bone procedures.
Wenger et al. reviewed the surgical treatment of DDH. They say that the impediment to congruent reduction are the iliopsoas muscle, joint capsule, ligamentum teres, pulvinar, labrum, and transverse acetabular ligament. The most commonly used approaches are anterior and medial/anteromedial to the hip.
Gholve et al. reviewed DDH and the factors that contribute to secondary procedures. In their study, neither age nor unilateral vs bilateral dislocation had a direct influence on the outcome or the need for secondary procedures. The variable that significantly influenced the need for a secondary procedure was the concomitant use of a femoral osteotomy during initial surgical treatment. Of the 27 patients who did not have concurrent femoral osteotomy at index surgery, 19/27 (73%) required a secondary procedure (P<0.001).
Figure A shows an AP pelvic radiograph of an infant. Focusing on the left hip, there is lateral and superior subluxation of the femoral head, with the femoral head lateral to Perkin's line. The medial joint space is increased. The acetabular index is increased
>30 degrees. Shenton's line is disrupted. These are all features of DDH.
Incorrect Answers:
Question 67
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 261-270.
Snyder SJ, Banas MP, Karzel RP: An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg 1995;4:243-248.
Question 68
Osteoclasts originate from which of the following cell types?
Explanation
REFERENCES: Zaidi M, Blair HC, Moonga BS, et al: Osteoclastogenesis, bone resorption, and osteoclast-based therapeutics. J Bone Miner Res 2003;18:599-609.
Brinker MR: Bone (Section 1), in Miller M (ed): Review of Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1996, pp 1-35.
Zuscik MJ, Drissi MH, Reynolds PR, et al: Molecular and cell biology in orthopaedics, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 69
When compared to smokers who do not quit, an improvement in the rate of lumbar fusion is seen in patients who cease smoking for at least how many months postoperatively? Review Topic
Explanation
Question 70
A 70-year-old male with longstanding diabetic neuropathy sustains a fall down a flight of stairs and sustains the injury shown in Figures A and B. In the operating room, direct reduction of the fracture is performed. The syndesmosis is assessed and found to be intact. The fibula is fixed with a small fragment locking plate and the medial malleolus is fixed with screws. What is the next best step? Review Topic

Explanation
Diabetics with ankle fractures are prone to complications. Nonoperatively treated cases have up to a 50% incidence of skin breakdown in a cast. Surgically treated patients have up to 40% complication rate. Supplemental fixation can include include multiple syndesmotic screws, spanning external fixation, tibio-talar Steinmann pins, more rigid fibular plates, supplemental intramedulary fibular pinning. Weightbearing after surgery should be delayed (8-12weeks).
McCormack and Leith reviewed the complications in 26 diabetic ankle fractures. 19 patients had surgery. The incidence of complications was 42%. Two required amputation and died. None of the non-diabetic control group had complications. They concluded that in the older, diabetic patient with lower demands, especially if insulin-dependent, it may be preferable to accept a loss of reduction and malunion rather than risk the potentially devastating complications associated with operative intervention. If surgery is necessary, the results of this study provides a more accurate prognosis and allows for better discussion of surgical risks with the patient.
Roseunbaum et al polled AOFAS members on the treatment of diabetic ankle fractures. (1) For nondisplaced bimalleolar fracture with diabetic neuropathy, respondents preferred casting and nonweightbearing (NWB) for 8-12 weeks. (2) For Weber B fracture dislocation without neuropathy, without syndesmotic injury,
respondents preferred either 1/3 tubular or small fragment locking plates with syndesmotic screws and NWB for 8-12 weeks. (3) For bimalleolar fracture dislocation with neuropathy, without syndesmotic injury, respondents preferred small fragment locking plates with syndesmotic screws and NWB for 8-12 weeks.
Wukich and Kline reviewed the management of ankle fractures in diabetics. They found that neuropathy is more prevalent in patients with ankle fractures than without. They stress that 1% reduction in HbA1C results in 30% reduction in complication rate. Fracture healing is slower, callus is smaller, with less stiffness, tensile strength and collagen content. Amputation rate is up to 5% for patients treated operatively or nonoperatively. Complications are higher in patients with vasculopathy, neuropathy, or Charcot arthropathy.
Incorrect Answers:
Question 71
Which of the following nerves is most commonly injured during revision surgery following a Bristow procedure?
Explanation
REFERENCES: Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993,
pp 98-116.
Flatow EL, Bigliani LU, April EW: An anatomic study of the musculocutaneous nerve and its relationship to the coracoid process. Clin Orthop 1989;244:166-171.
Question 72
below shows the standing AP radiograph obtained from a year-old man who has a year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. Unicompartmental knee arthroplasty (UKA) is discussed with the patient. The most appropriate next radiographic evaluation should be
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress
faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 73
2 months with 5/66 cases going on to non-union, which were all successfully treated with bone grafting, and 1/66 resulting in a malunion. They conclude that blocking screws help maintain fixation and alignment of proximal third tibia fractures treated with intramedullary nails.
Explanation
Figures 1 and 2 are the radiographs of a 41-year-old diabetic male presenting with right lower extremity pain after cutting his leg it on a piece of rusty metal yesterday. Serial physical exam demonstrates rapid progression of the overlying erythema and worsening pain. In the emergency department, labs are significant for a C-reactive protein (CRP) of 180 mg/L, white blood cell (WBC) count of 19,000/mm3, glucose of 11 mmol/L, creatinine of 150 umol/L, and sodium of 120 mmol/L. He has a temperature of 102°F and a heart rate of 110 bpm. What additional laboratory value is needed to calculate this patient’s LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score?

ESR
Hemoglobin
Potassium
Bicarbonate
Calcium
The LRINEC score is based on the patient's serum CRP, WBC count, hemoglobin, sodium, creatinine, and glucose.
The LRINEC score is a clinical tool designed to help distinguish between necrotizing fasciitis and other soft tissue infections using these 6 key laboratory values. The most important of these is CRP, as a value >150 mg/L
contributes 4 of a possible 13 points. Illustration A demonstrates the scoring system for each laboratory value used in the calculation of the LRINEC score. A score >6 has been shown to have a PPV of 92% for having necrotizing fasciitis. The patient in this vignette already has a score of 10 without knowledge of the hemoglobin level, which is very concerning for necrotizing fasciitis. As a result, emergent surgical debridement is indicated.
Stoneback et al. reviews the presentation and management of necrotizing fasciitis. The authors note that the incidence of necrotizing fasciitis is between 500 and 1500 cases per year in the United States, and that the mortality rate averages 21.9%. They emphasize that necrotizing fasciitis may be difficult to distinguish from more common skin infections such as cellulitis or soft tissue abscess in its early stages but will often rapidly deteriorate, as illustrated in this vignette.
Wong et al. developed the LRINEC scoring system. In a retrospective review of 145 patients with necrotizing fasciitis and 309 patients with severe cellulitis or abscesses, they used their scoring system to demonstrate that a LRINEC score of 6 points or greater had a PPV of 92.0% and an NPV of 96.0%.
Tsai et al. challenged the utility of the LRINEC score in aiding in the diagnosis of Vibrio Necrotizing Fasciitis. In their retrospective review of 70 patients with Vibrio Necrotizing Fasciitis, they showed that only 11% of patients had a LRINEC score >6. The authors concluded that the LRINEC scoring system is of more limited utility for this subset of the disease and propose that severe hypoalbuminemia, thrombocytopenia, and increased banded forms of leukocytes may have greater utility.
Figures A and B are AP and lateral radiographs of the lower leg demonstrating diffuse subcutaneous gas. This is concerning for necrotizing fasciitis.
Illustration A is a table showing the LRINEC scoring breakdown. A maximum total score of 13 could be achieved.
Incorrect Answers:
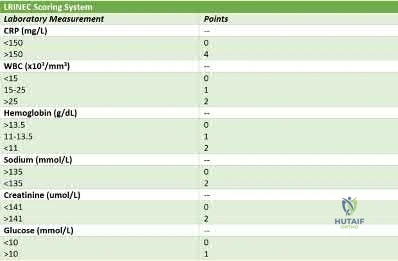
OrthoCash 2020
A 35-year-old male presents to the emergency department following a motorcycle accident. On initial examination in the emergency department, he is found to have a left flail arm and multiple other injuries. There is a concern for a brachial plexus injury. What examination findings would support a diagnosis of a pre-ganglionic injury?
Abnormal histamine response
Flail arm
Intact sensory nerve action potentials (SNAPs)
Lateral scapular winging
Normal cervical paraspinal signal on EMG/NCV Corrent answer: 3
Brachial plexus injuries are classified as either pre-ganglionic or post-ganglionic. A pre-ganglionic injury would be supported by intact sensory nerve action potentials (SNAPs).
Diagnosing brachial plexus injuries as either pre- or post-ganglionic is multi-faceted and begins with a thorough physical examination. Findings suggestive of a pre-ganglionic injury would include Horner Syndrome (due to disruption of the sympathetic chain), MEDIAL scapular winging resulting from rhomboid and serratus anterior paralysis, cervical paraspinal muscle weakness, absent sensation, and hemidiaphragmatic paralysis. CT myelography may demonstrate pseudomeningocele, and NCS/EMG would show intact sensory nerve action potentials (SNAPs) with denervation of the cervical paraspinal musculature. Finally, a histamine test would show a triple response, with redness, wheal, AND flare. Conversely, a post-ganglionic injury would be
supported by BOTH motor and sensory deficits of the flail arm, maintained innervation to cervical paraspinal muscles, and an abnormal histamine response test (redness and wheal with NO flare).
Limthongthang et al. reviews the common clinical findings associated with pre-and post-ganglionic injuries. The authors discuss the diagnostic algorithm, including a thorough history, physical examination, electrodiagnostic studies, and CT myelogram or MRI. They emphasize that an angiogram should additionally be considered given that 20% of brachial plexus injuries have associated major vascular injuries. The authors conclude with appropriate surgical timing and suggest potential treatments depending on injury location.
Giuffree et al. reviews management of brachial plexus injuries. The authors discuss appropriate timing of treatment based on the injury mechanism. They emphasize the priorities of functional restoration, beginning with elbow flexion, followed by a stable shoulder, and lastly intrinsic hand function. The authors present various surgical options to attain these goals and discuss their outcomes.
O'Shea et al. discusses the utilization of advanced imaging and electrodiagnostic testing for evaluation of brachial plexus injuries. The authors note the utility of CT myelogram toward identifying root avulsions. They also suggest that electrodiagnostic studies be obtained no sooner than 4 weeks following injury and subsequently at 6-week intervals to monitor progression. They note that SNAPs are the most important criteria in distinguishing between pre- and post-ganglionic injuries, and conclude that electromyographic studies are crucial in determining not only the level of injury but also donor nerves for transfers.
Incorrect Answer:
indicative of a pre-ganglionic injury due to involvement of the dorsal scapular nerve (branching from the C5 root) and the long thoracic nerve (branching from the C5-7 roots).
OrthoCash 2020
A 47-year-old male diabetic has developed a calcaneal ulcer, as shown in figure A, that has been managed with wound care and a total contact cast. He presents to the emergency department with worsening erythema progressing up his leg with new draining wounds. On admission, despite antibiotics and intravenous fluids, he develops worsening pain and new bullae shown in Figure B. His laboratory studies indicate CRP >200, WBC 25k, Sodium 127, glucose 233, and hemoglobin 12. What is the best next step in the management of his condition?

Emergent vascular exploration
Upgrade level of care ICU with antibiotic escalation
MRI foot for osteomyelitis evaluation
Emergent surgical debridement including possible amputation
CT with contrast of lower extremity Corrent answer: 4
This patient meets the clinical criteria for the diagnosis of necrotizing fascitis, therefore the next step in management is surgical debridement with possible amputation.
Necrotizing fasciitis is an aggressive infection with rapid spread along fascial planes. Initial presentation may be consistent with cellulitis; however, rapid progression along fascial planes may result in skin necrosis, muscular invasion, and subsequent myonecrosis. The rapidity of diagnosis and emergent surgical debridement is essential. Risk factors including intravenous drug abuse, alcohol abuse, and diabetes should be assessed, and if necrotizing fascitis is on the differential, the LRINEC score may be employed for diagnosis in equivocal cases. This scoring system can be found on our associated Orthobullets page.
Wong et. al. developed the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score to assist in early diagnosis of necrotizing soft tissue infections. The authors used logistic regression to identify significant predictors of necrotizing fasciitis. The score utilizes a total white cell count, hemoglobin, sodium, glucose, serum creatinine, and CRP. A LRINEC score of 6 points or higher has a positive predictive value of 92%, and below 6 points a negative predictive value of 96%. Importantly, ESR is not a component in the scoring system as it correlated poorly with risk. The patient presented already has two positive serum findings with an LRINEC score of 6.
Stoneback et al. review the diagnosis and management of necrotizing fasciitis. They note that Group A streptococcus is one of the most prevalent organisms, but infections are typically polymicrobial. Because of the need for prompt initiation of treatment, adjunctive diagnostic tests should not impede the timing of surgical exploration and debridement. Necrotizing fasciitis is a clinical diagnosis where only emergent surgical debridement and appropriate antibiotic treatment can prevent progression and death.
Tsai et al. retrospectively reviewed 70 patients with 71 episodes of Vibrio necrotizing fasciitis and sepsis. Of the 70 patients, 68 had a history of contact with seawater or raw seafood; 66 had underlying chronic diseases. They noted that severe hypoalbuminemia, severe thrombocytopenia, and increased banded forms of leukocytes are laboratory risk indicators of necrotizing fasciitis
that aid in pointing toward the initiation of early surgery and predict a higher risk of death.
Figure A is a clinical photograph of a calcaneal ulcer. Figure B shows ascending erythema and bullae consistent with a necrotizing skin infection. Illustration A demonstrates the LRINEC scoring system. The scoring system is not largely utilized as a screening tool due to its poor sensitivity in studies that attempted to validate it.
Incorrect answers:

OrthoCash 2020
A 36-year-old man with HIV, chronic kidney failure, and chronic IV drug use presents with worsening fevers, chills, and purulent drainage from his leg. His infection progresses rapidly and he becomes acutely septic. He is therefore taken urgently to the OR for radical debridement of the fascia and surrounding tissues, with a plan for delayed closure. His CRP is 90 mg/dL and he is hyponatremic. Intraoperative cultures are obtained. To cover the most common organism(s) associated with this condition, what antibiotic would you initially recommend?

Intravenous vancomycin
Intravenous vancomycin and gentamicin
Intravenous gentamicin
Intravenous linezolid and meropenem
Intravenous micafungin
This patient with lower extremity necrotizing fasciitis underwent a radical debridement of fascia and surrounding tissues. The most common culture isolate from necrotizing fasciitis is polymicrobial, which should be the target of initial antibiotic treatment. Of the above options, intravenous Linezolid and Meropenem would be an acceptable empiric therapy as Linezolid would cover MRSA and invasive group A Streptococcus while Meropenem would cover gram-positive/negative anaerobic coverage and enteric organisms.
Necrotizing fasciitis is an aggressive infection with rapid spread along fascial planes. While the initial presentation may suggest cellulitis, rapid progression along fascial planes may result in skin necrosis and subsequent myofascial necrosis. The time from admission to debridement has been shown to be a significant predictor of outcomes. Immediate empiric antibiotics covering
polymicrobial species including aerobic, anaerobic, gram-positive and gram-negative bacteria are of equal importance.
Stoneback et al. reviewed the diagnosis and management of necrotizing fasciitis. They reported that while most necrotizing fasciitis infections are polymicrobial, group A Streptococcus remains one of the more prevalent organisms in isolation. They recommended surgical debridement as the utmost importance in necrotizing fasciitis management and emphasized appropriate antibiotic selection in treating sepsis and halting the further bacterial spread.
Wong et al. developed the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score, a novel diagnostic scoring system for distinguishing necrotizing fasciitis from other soft tissue infections based on laboratory tests routinely performed for the evaluation of severe soft tissue infections. This score allocated 1 point each to the following labs: total white cell count, hemoglobin, sodium, glucose, serum creatinine, and C-reactive protein. They reported that a cutoff value of 6 points had a positive predictive value of 92.0% and a negative predictive value of 96.0%, and concluded that the LRINEC score is a powerful score that can detect even clinically early cases of necrotizing fasciitis.
Tsai et al. investigated whether clinical indicators predict laboratory findings during the initial stages of necrotizing fasciitis and the relationship between the LRINEC score and the diagnosis of vibrio infection. They reported that a systolic blood pressure of 90mmHg or less at the time of admission predicted mortality and that patients with a LRINEC score of >6 had an 11% chance of surviving vibro-specific necrotizing fasciitis.
Figure A is a clinical image depicting necrotizing fasciitis of the lower extremity, with characteristic ischemic patches, cutaneous gangrene, dermal induration, bullae formation. Illustration A is a table from Wong's study that demonstrates the components, clinical values, and scoring system for the LRINEC score.
Scores of 6 or greater are highly concerning. They concluded that severe hypoalbuminemia, severe thrombocytopenia, and increased leukocytosis were reliable markers.
Incorrect Answers:
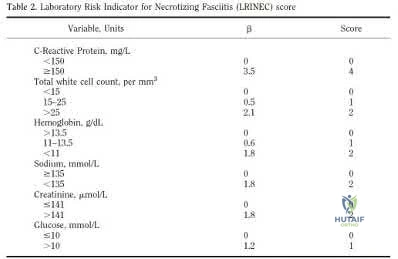
OrthoCash 2020
A 27-year-old male is involved in a motor vehicle collision and presents to the ER with the right lower extremity injury shown in Figures A and B. He undergoes immediate closed reduction and the post-reduction CT is shown in Figures C and D. The patient undergoes percutaneous surgical screw fixation of the injury. At 2 years followup, he presents with a supination deformity with decreased eversion of the foot at rest. Radiographs reveal no evidence of talus subchondral sclerosis or collapse. Which of the following is the most likely cause of the finding in this patient?

Avascular necrosis
Subtalar arthritis
Tibiotalar arthritis
Varus malunion
Planovalgus
The patient has sustained a displaced talar neck fracture with medial comminution which requires open reduction and internal fixation to restore anatomic alignment. The patient has likely sustained varus malunion which is a common deformity noted with non-anatomical reduction leading to hindfoot supination and decreased eversion.
Talar neck fractures, while uncommon, can lead to significant morbidity in the ambulatory patient. Treatment of these injuries requires prompt reduction due to the tenuous blood supply to the talus. The most common complications noted after a talar neck fracture are avascular necrosis, subtalar arthritis, tibiotalar arthritis, and varus malunion. A talus varus malunion generally occurs due to medial talar neck comminution and/or non-anatomic reduction of the injury. This deformity can lead to decreased eversion and a supination deformity causing patients to ambulate on the lateral aspect of the foot. These malunions are generally treated with a medial opening wedge osteotomy.
Fortin and Balazsy review the pathology and treatment of traumatic talus fractures. They cite that injuries to the head, neck, or body of the talus can result in permanent pain, loss of motion, and deformity. They note that failure to recognize fracture displacement (even when minimal) can lead to undertreatment and poor outcomes. They conclude that unrecognized medial talar neck comminution can lead to varus malunion and a supination deformity with a decreased range of motion of the subtalar joint.
Lindvall et al. performed a retrospective review to evaluate the long-term results (average of 74-month followup) of surgical treatment of isolated, displaced talar neck and/or body fractures with stable internal fixation in 25 patients. They noted an overall union rate of 88% regardless of surgical timing. The authors noted posttraumatic subtalar arthritis in all patients (100%) and talus osteonecrosis in 13/26 (50%) of patients. The authors concluded that a delay in surgical fixation does not appear to affect the outcome, union, or prevalence of osteonecrosis and that posttraumatic arthritis is a more common complication than osteonecrosis following operative treatment.
Figures A and B are the Lateral and AP radiographs of a displaced talar neck fracture with tibiotalar dislocation. Figures C and D are the post-reduction sagittal foot CT cuts that reveal a displaced talar neck fracture with medial
comminution.
Incorrect Answers:
OrthoCash 2020
Figures A-C are a 32-year-old female who presents to the trauma bay after falling off a roof. Paramedics state that she was initially complaining of back pain, but she now appears irritable and lethargic. She has received 2 liters of crystalloid since arriving in the trauma bay. Her blood pressure is now 76/42. A Foley catheter is placed, and her urine output is 12 ml/hour. What additional finding would suggest hemorrhagic shock over neurogenic shock?
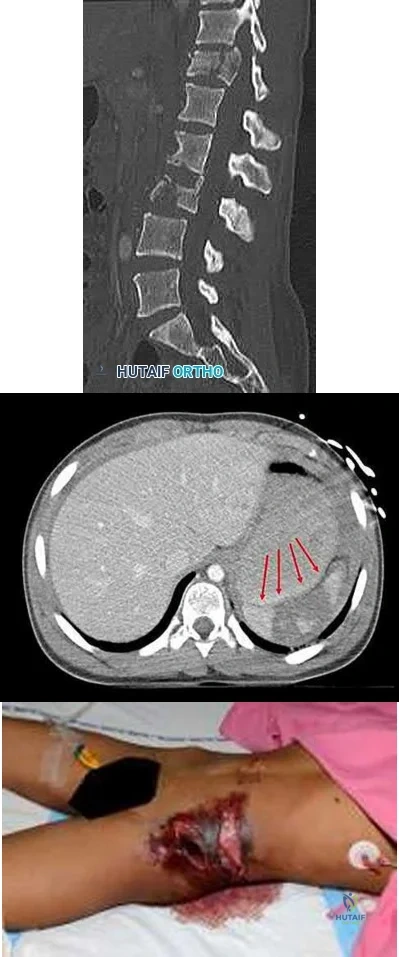
Tachycardia
Bradycardia
Decreased cardiac output
Vasodilation
Warm dry skin Corrent answer: 1
This patient sustained a multi-traumatic injury and is suffering from hemorrhagic shock. The presence of tachycardia would favor the diagnosis of hemorrhagic shock over neurogenic shock.
In initial hypovolemic shock (stage I, <15% blood loss), heart rate, blood pressure, urine output, pH, and mental status are largely unaffected, as the body can typically compensate for this amount of volume loss. With increasing blood loss, tachycardia, hypotension, low urine output, decreased pH, hemoconcentration, cool clammy skin, and altered mental status can be observed. This patient sustained a splenic injury and T12 and L3 vertebral injuries. Both hemorrhagic and neurogenic shock may result in a decrease in cardiac output and hypotension; however, neurogenic shock may also present with warm dry skin, vasodilation, loss of sympathetic tone, and paradoxical bradycardia.
Schouten et al. review the initial management of the spinal column and spinal cord injury (SCI) in the emergency room. The authors discuss that acutely, deep tendon reflexes are absent and paralysis is flaccid, but that this transitions to hyper-reflexia and spasticity with time. They conclude that spinal shock is a temporary physiologic state of the acutely traumatized spinal cord, evident by the transient absence of reflexive function caudal to the spinal cord injury followed by gradual return of reflex activity. Additionally, the diagnosis of a "complete" spinal cord injury cannot be made until the neural "shock" resolves.
Spector et al. review cauda equina syndrome. They report on the characteristic findings such as varying patterns of low back pain, sciatica, lower extremity sensorimotor loss, and bowel and bladder dysfunction. Classical findings include urinary retention, saddle anesthesia of the perineum, bilateral lower extremity pain, numbness, and weakness. The authors conclude that there should be a high index of suspicion in the postoperative spine patient with back and/or leg pain refractory to analgesia, especially in the setting of urinary retention.
Hadley et al. review the presentation of acute SCI. The authors report that hypotension has been associated with an increased risk of mortality following
spinal cord injuries. They conclude that hypotension (systolic blood pressure
<90 mm Hg) should be avoided after acute SCI, with the maintenance of mean arterial blood pressure at 85 to 90 mm Hg for the first 7 days after acute spinal cord injury in order to improve spinal cord perfusion.
Sekhon et al. review the epidemiology, demographics, and pathophysiology of SCI. They discuss primary and secondary injury, with the mediators of secondary injury including vascular mechanisms, excitatory amino acids, calcium, sodium, free radicals, inflammation, and apoptosis.
Figures A is a sagittal CT image demonstrating T12 and L3 vertebral fractures. Figure B is an axial CT image demonstrating a splenic injury with hematoma. Figure C is a clinical photograph demonstrating left abdominal flank injury.
Illustration A shows the classification of hemorrhagic shock.
Incorrect Answers:
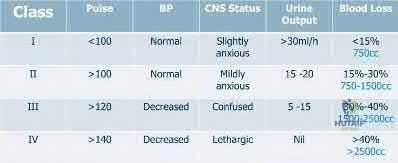
OrthoCash 2020
A 32-year-old inebriated male falls from a mechanical bull at a bar and sustains a closed displaced intra-articular distal radius fracture. He presents to your clinic and given his age and the fracture characteristics, he is taken for open reduction with volar locking plate
fixation. After completing instrumentation, radiocarpal screw penetration is best assessed on which fluoroscopic view?
Extended wrist tangential view
Flexed wrist tangential view
PA anatomic tilt view
Radial inclination view
Standard lateral view Corrent answer: 4
While no single radiographic view can completely rule out intra-articular screw penetration, radial inclination views (most commonly a 22-degree anatomic tilt lateral view) best demonstrates screw penetration of the radiocarpal joint.
Intra-articular screw penetration is a potential complication of distal radius fracture fixation. Due to the complex native geometry, standard PA and lateral fluoroscopic views are not effective in evaluation of the joint reduction, screw length or screw position. For this reason, various supplemental views have been described to facilitate identification of articular incongruity as well as dorsal or intra-articular penetration of screws, either into the radiocarpal or distal radioulnar joint.
Tweet et al. reviewed the most commonly used imaging techniques and views for the evaluation of intra-articular screw penetration during volar plate fixation of distal radius fractures. Of nearly 700 ASSH members surveyed, 87% relied exclusively on fluoroscopy, three-quarters (74%) of which implemented tilt views or rotational fluoroscopy. Cadaveric analysis supported use of a 22-degree lateral projection and rotational fluoroscopy as adjuncts for the detection of intra-articular screw penetration. They concluded that no combination of imaging effectively allowed the detection of all intra-articular screws.
Patel et al. evaluated the utility of supplemental radiography in assessing screw placement in distal radius fracture fixation using volar locking plates. The authors found that supplementation of the standard AP and lateral views with lateral tilt views significantly increased accuracy and confidence.
Specifically, more acute angles (15 and 23-degree views) provided better visualization of ulnar screws while larger angles (30 degrees) allowed assessment of more radial-sided distal plate screws.
Illustration A is an example of an extended wrist tangential view showing clear visualization of the sigmoid notch and distal radioulnar joint (DRUJ), with intraarticular penetration of the DRUJ shown on the left and extra-articular screws
free of the DRUJ.
Illustration B is an example of a flexed wrist tangential view, or “skyline” view, demonstrating no dorsal penetration of the screws, which can be obscured on a true lateral due to Lister’s tubercle.
Illustration C shows an example of a standard PA view (left) and 11-degree anatomic tilt PA view, allowing better visualization of the articular surface. Illustration D shows a standard true lateral view (left) and 22-degree radial inclination lateral view (right), allowing better visualization of screw relationship to the radiocarpal joint.
Incorrect Answers:

OrthoCash 2020
A 40-year-old slips on the ice on a wintery Michigan day and sustains a comminuted intra-articular distal radius fracture. Which of the regions on the patient's injury AP radiograph in Figure A, if not addressed properly during surgery, represents a risk for radiocarpal instability?

Question 74
Patients with tarsal tunnel syndrome are most likely to obtain a favorable outcome from decompression of the posterior tibial nerve if which of the following conditions is present?
Explanation
REFERENCES: Frey C, Kerr R: Magnetic resonance imaging and the evaluation of tarsal tunnel syndrome. Foot Ankle 1993;14:159-164.
Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
Pfeiffer WH, Cracchiolo A III: Clinical results after tarsal tunnel decompression. J Bone Joint Surg Am 1994;76:1222-1230.
Question 75
Figures below depict the radiographs obtained from a 76-year-old woman who comes to the emergency department after experiencing a fall. She is an unassisted community ambulator with a history of right hip pain. What is the most appropriate surgical treatment for this fracture?

Explanation
This patient has pre-existing right hip osteoarthritis. The most correct option for the treatment of this active patient is a right total hip arthroplasty. Hemiarthroplasty would not address the patient's pain from osteoarthritis, and open reduction and internal fixation would not fix the femoral head issue or the osteoarthritis.
Question 76
Figures 35a and 35b show the radiographs of a 7-year-old patient who has progressive deformity of the right thigh accompanied by a dull persistent pain radiating to the knee. Examination reveals an obvious bulge in the right thigh, with flexion of the hip beyond 50° only if the hip is allowed to externally rotate. Management should consist of
Explanation
REFERENCES: Zionts LE, Ebramzadeh E, Stott NS: Complications in the use of the Bailey-Dubow extensible nail. Clin Orthop 1998;348:186-195.
Luhmann SJ, Sheridan JJ, Capelli AM, Schoenecker PL: Management of lower-extremity deformities in osteogenesis imperfecta with extensible intramedullary rod technique: A 20-year experience. J Pediatr Orthop 1998;18:88-94.
Glorieux FH, Bishop NJ, Plotkin H, Chabot G, Lanoue G, Travers R: Cyclic administration of pamidronate in children with severe osteogenesis imperfecta. N Engl J Med 1988;339:947-952.
Question 77
- Figures 42a and 42b show the sagittal and axial MRI scans of a 24-year-old patient who has sciatia. Which of the following combinations of physical findings is most consistent wit the MRI studies?
Explanation
Question 78
Figure 18 shows the radiograph of a patient with a total hip arthroplasty dislocation. During revision, increasing the diameter of the femoral head while maintaining the ratio of head-to-neck diameter constant has the effect of
Explanation
Scifert and associates used a three-dimensional finite element model to study various combinations of femoral head size and neck ratios. They found that increasing the diameter of the femoral head while maintaining a constant head-to-neck diameter had the effect of significantly increasing the resisting moment necessary to induce a dislocation. The higher the head-to-neck ratio, the greater the range of motion until impingement and the greater the range of motion to dislocation.
REFERENCE: Scifert CF, Brown TD, Pedersen DR, Callaghan JJ: A finite element analysis of factors influencing total hip dislocation. Clin Orthop 1998;355:152-162.
Question 79
A 25-year-old female presents to the emergency room for the fourth time in the last week. She has vague complaints of extremity pain. Physical examination by a male ER resident has been limited each visit because she is terrified of the pain that the clinician may cause. On physical examination, she is withdrawn and frightened. Regions of ecchymosis are noted throughout chest and abdomen. She has requested multiple radiographs, MRI and CT scans. Today's imaging (radiographs, MRI, CT scan) has been unrevealing. What is the most likely diagnosis? Review Topic
Explanation
Domestic violence or intimate partner violence can be in the form of mental or physical abuse, neglect or abandonment. Close to 25% of women will experience domestic violence. Risk factors include young age (19-29 years of age), females, pregnancy and lower socioeconomic status. Affected patients will have repeated visits to the emergency room, find reasons to stay in a treatment facility for an extended period of time and constantly seek approval of their partner.
Shields et al. reviewed factors influence outcome in treatment of patients affected by domestic violence. They found that positive outcomes were associated with interdisciplinary approaches to management. This included better history assessment, providing written documentation regarding intervention and better access to information on community resources.
Illustration A is a chart documenting the frequency of female domestic violence throughout the world as of 2012.
Incorrect Answers
Question 80
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Explanation
REFERENCES: Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder’s foot and ankle. Am J Sports Med 1998;26:271-277.
Ebraheim NA, Skie MC, Podeszwa DA, Jackson WT: Evaluation of process fractures of the talus using computed tomography. J Orthop Trauma 1994;8:332-337.
Question 81
A 70-year-old woman with known osteoporosis sustains a distal radius fracture of her dominant arm with some metaphyseal comminution. Adequate maintenance of reduction by non-operative treatment is unsuccesful. Which plating option provides the most appropriate treatment of this fracture?

Explanation
Question 82
Surgical treatment of an adult cavovarus foot with fixed forefoot valgus that does not correct on Coleman block testing should consist of Review Topic
Explanation
Question 83
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of
Explanation
REFERENCES: Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Jupiter JB, Ring D: Operative treatment of post-traumatic proximal radioulnar synostosis.
J Bone Joint Surg Am 1998;80:248-257.
Question 84
When making a comparison to autograft incorporation, the inflammatory process in allograft tissue anterior cruciate ligament (ACL) reconstruction
Explanation
Question 85
The use of a screw between the clavicle and the coracoid process to maintain the clavicle and acromioclavicular (AC) joint in a reduced position is a treatment option for AC joint separations. Screw removal is generally recommended after soft-tissue healing. What effect does this rigid coracoclavicular fixation have on shoulder kinematics?
Explanation
REFERENCES: Flatow EL: The biomechanics of the acromioclavicular, sternoclavicular, and scapulothoracic joints. Instr Course Lect 1993;42:237-245.
Kenedy JC, Cameron H: Complete dislocation of the acromioclavicular joint. J Bone Joint Surg Br 1954;36:202-208.
Rockwood CA Jr, Williams GR, Young CD: Disorders of the acromioclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 483-553.
Inman VT, Saunders JB, Abbott LC: Observations of the function of the shoulder joint. Clin Orthop 1996;330:3-12.
Question 86
A 43-year-old former professional hockey player reports severe pain in his chest after being checked from the side in a pick-up hockey game. An MRI scan and plain radiographs are shown in Figures 25a through 25c. What is the most likely diagnosis?
Explanation
REFERENCES: Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 566-572.
Omer GE Jr: Osteotomy of the clavicle in surgical reduction of anterior sternoclavicular dislocation. J Trauma 1967;7:584-590.
Question 87
In providing culturally competent care to a Muslim woman with a cervical spine injury, which of the following most accurately describes the steps a male orthopaedist should take to respect her religious beliefs during his examination?
Explanation
REFERENCE: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 88
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time?
Explanation
REFERENCES: Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Carragee EJ: Clinical practice: Persistent low back pain. N Engl J Med 2005;352:1891-1898.
Question 89
Figures 34a and 34b show the clinical photographs of a 46-year-old woman who has a painful deformity of the second toe. Surgical treatment consisting of metatarsophalangeal capsulotomy and proximal interphalangeal joint resection arthroplasty resulted in satisfactory correction, but the toe remains unstable at the metatarsophalangeal joint. What is the next most appropriate step?
Explanation
REFERENCES: Coughlin MJ: Crossover second toe deformity. Foot Ankle 1987;8:29-39.
Thompson FM, Deland JT: Flexor tendon transfer for metatarsophalangeal instability of the second toe. Foot Ankle 1993;14:385-388.
Question 90
Denosumab, a monoclonal antibody used to treat osteoporosis, works through inhibition of
Explanation
Question 91
Five weeks after the patient completes a 6-week course of antibiotics, his ESR is 24 mm/h and CRP level is 10 mg/L, which is similar to the levels at 6 weeks. What is the most appropriate treatment at this time?
Explanation
This patient has both serologic and synovial fluid findings that are concerning for indolent infection. He was taking antibiotics at the time of aspiration. The AAOS clinical practice guideline, The Diagnosis of Periprosthetic Joint Infections of the Hip and Knee, suggests that patients discontinue antibiotics for a minimum of 2 weeks and that a repeat aspiration should be performed in cases of contradictory findings. In this situation, the cell count is elevated
along with an elevated ESR and CRP level. As a result, the appropriate treatment at this time is to reaspirate his hip.
This patient has a periprosthetic joint infection with a draining sinus tract. He has had symptoms for several months and, as a result, irrigation and debridement are not indicated. A single-stage surgery may be performed in some centers for healthy patients with susceptible organisms. However, single-stage reconstructions are generally performed with cemented implants in patients without a draining sinus tract. A 2-stage procedure with an antibiotic spacer is the surgical treatment modality most likely to eradicate this infection.
Serologic findings have significantly improved since the time of the prior surgical procedure. Surgical intervention does not need to be delayed until these values have completely normalized.
Question 92
A 21-year-old man has had posterior neck discomfort for the past 6 months. Radiographs, an MRI scan, and a photomicrograph of the biopsy specimen are shown in Figures 17a through 17d. What is the most likely diagnosis?
Explanation
REFERENCES: Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991,
vol 2, pp 1143-1174.
Enneking WF: Musculoskeletal Tumor Surgery. New York, NY, Churchill Livingstone, 1983, pp 1043-1053.
Question 93
Figure 35 shows the radiograph of a 12-year-old boy who fell off a snowmobile and landed on his left shoulder. He has a closed injury. Management should consist of
Explanation
REFERENCES: Kohler R, Trillaud JM: Fracture and fracture separation of the proximal humerus in children: Report of 136 cases. J Pediatr Orthop 1983;3:326-332.
Beaty JH: Fractures of the proximal humerus and shaft in children. Instr Course Lect 1992;41:369-372.
Dobbs MB, Luhmann SL, Gordon JE, et al: Severely displaced proximal humeral epiphyseal fractures. J Pediatr Orthop 2003;23:208-215.
Beringer DC, Weiner DS, Noble JS, et al: Severely displaced proximal humeral epiphyseal fractures: A follow-up study. J Pediatr Orthop 1998;18:31-37.
Wang P Jr, Koval KJ, Lehman W, et al: Salter-Harris type III fracture-dislocation of the proximal humerus. J Pediatr Orthop B 1997;6:219-222.
Question 94
The knee arthroplasty type associated with the highest 5-year revision rate is
Explanation
Revision rates for UKA at 10 years are lower than 5% at specialty centers. However, the 10-year revision rate associated with UKA in registries such as the National Joint Registry for England and Wales is 2 to 3 times that of TKA. Among partial knee replacements, patellofemoral arthroplasty is associated with the highest revision rate at every time interval.

CLINICAL SITUATION QUESTIONS 167 THROUGH 169
Figures 167a and 167b are the radiographs of a middle-age man. He is a noncompliant patient who has severe insulin-dependent diabetes and a below-knee amputation on the right side. He is usually in a wheelchair, does not use a prosthesis, transfers using a walker, and resides in an institution. He had an infection in the left leg years ago, which was treated successfully with intravenous antibiotics (the details are unknown). His left knee is mildly painful, swollen but not warm, has limited range of motion (40-140 degrees), and is grossly unstable.
Question 95
The MRI scan shown in Figure 24 reveals a right-sided herniated nucleus pulposus at L4-5 in a patient with pain in the right leg. Administration of a caudal epidural steroid injection provides immediate relief. Over the next week he notes generalized weakness of the lower extremities and has one episode of urinary incontinence. What is the next most appropriate step in management?
Explanation
REFERENCES: Knight JW, Cordingley JJ, Palazzo MG: Epidural abscess following epidural steroid and local anaesthetic injection. Anaesthesia 1997;52:576-578.
Abram SE, O’Connor TC: Complications associated with epidural steroid injections. Reg Anesth 1996;21:149-162.
Question 96
What is a risk factor for interdigital neuroma?
Explanation
The only proven risk factor for development of an interdigital neuroma is female gender, which likely is related to the use of fashionable shoes that force plantar flexion of the metatarsal heads and secondary hyperdorsiflexion of the metatarsophalangeal joints. The other factors listed have not been proven to cause interdigital neuroma, as well as mediolateral compression of the forefoot.
RECOMMENDED READINGS
Hill KJ. Peripheral nerve disorder. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:307-327.
Schon LC, Mann RA. Diseases of the nerves. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby-Elsevier; 2007:613-686.
Question 97
A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?
Explanation
REFERENCES: Ring D, Allende C, Jafarnia K, et al: Ununited diaphyseal forearm fractures with segmental defects: Plate fixation and autogenous cancellous bone-grafting. J Bone Joint Surg Am 2004;86:2440-2445.
Question 98
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?
Explanation
REFERENCES: Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540.
Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 99
A 28-year-old construction worker sustains the closed injury shown in Figures A and B after a fall from a height. He is taken to the operating room. What is the next best step?

Explanation
In the distal tibial metaphysis, there is no snug endosteal fit for an IM nail. Center-center nail placement in both proximal and distal fragments is necessary to maintain alignment. There is also increased stress on distal locking bolts to maintain fracture alignment. Assuming static medial-lateral distal locking screws, accurate coronal plane and rotational alignment is achieved by fibular plating as a first step. This also
prevents late loss of alignment because of distal locking screw toggle. Reamed nailing allows a stiffer, larger nail to be placed, and allows redistribution of endosteal osteogenic material to the fracture site. Although there is endosteal vascular compromise, this does not affect fracture healing because of intact periosteal supply.
Bhandari et al. conducted a prospective, randomized, blinded comparison of 622 patients who had reamed nailing, and 604 who had unreamed nailing. For closed fractures, a significantly greater number in the unreamed group required bone grafting, implant exchange and dynamization. There was no difference in groups for open fracture nailing.
Egol et al. retrospectively reviewed distal metaphyseal tibia-fibula fractures treated with IM nailing with (25 cases) and without (47 cases) adjunctive plating. They found that plating was associated with maintenance of reduction (significant) as was the use of 2 medial-lateral distal locking bolts (not significant). They recommend fibular plating when IM nailing for distal tibia fractures.
Figures A and B show an extraarticular distal tibia fracture with distal fibula fracture. Incorrect Answers
Question 100
A 12-year-old boy reports knee discomfort after prolonged strenuous activities. He denies knee swelling or catching and has no pain with activities of daily living. A radiograph is shown in Figure 4. Prognosis for the pathology shown is most influenced by
Explanation
REFERENCES: Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
Linden B: Osteochondritis dissecans of the femoral condyles: A long-term follow-up study. J Bone Joint Surg Am 1977;59:769-776.
