OITE & ABOS Orthopedic Board Prep MCQs: Spine, Foot, Shoulder & Knee | Part 168

Key Takeaway
This page offers Part 168 of a comprehensive OITE/AAOS Orthopedic Surgery Board Review. Featuring 100 verified, high-yield MCQs in exam and study modes, it aids orthopedic residents and surgeons. Authored by Dr. Mohammed Hutaif, it's crucial for board certification exam preparation, covering key clinical topics.
About This Board Review Set
This is Part 168 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 168
This module focuses heavily on: Dislocation, Foot, Knee, Scoliosis, Shoulder.
Sample Questions from This Set
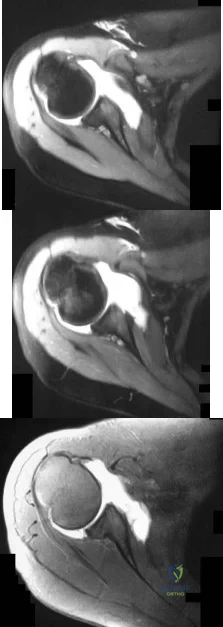
Sample Question 1: Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?...
Sample Question 2: A 25-year-old recreational soccer player has recurrent shoulder dislocations. He first dislocated his shoulder playing football in high school, was treated in a sling for 6 weeks, and returned to play for the remainder of the season. He did...
Sample Question 3: Figures 33a and 33b show the standing posteroanterior and lateral radiographs of a 59-year-old woman with adult idiopathic scoliosis. She underwent a prior decompressive laminectomy and fusion at L4-S1 to address lumbar stenosis. She now re...
Sample Question 4: A 24-year-old female soccer player has had lateral joint line pain and a recurrent effusion in the left knee after sustaining a twisting injury 6 weeks ago. She reports that symptoms worsen with athletic activities. MRI scans are shown in F...
Sample Question 5: A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 2
A 25-year-old recreational soccer player has recurrent shoulder dislocations. He first dislocated his shoulder playing football in high school, was treated in a sling for 6 weeks, and returned to play for the remainder of the season. He did well until 2 years later when he reinjured the shoulder. He says that his shoulder dislocates with little injury and always "feels loose." Examination reveals anterior instability and an MR arthrogram reveals an anterior-inferior labral tear and surgical treatment is recommended. He inquires about the benefits of arthroscopic vs open procedure. Which of the following statements reflects an advantage associated with arthroscopic procedures compared to open stabilization? Review Topic
Explanation
Question 3
Figures 33a and 33b show the standing posteroanterior and lateral radiographs of a 59-year-old woman with adult idiopathic scoliosis. She underwent a prior decompressive laminectomy and fusion at L4-S1 to address lumbar stenosis. She now reports progressive lower back pain and a feeling of being shifted to the right. If surgical intervention is considered, what is the most important goal in improving her health-related quality of life (HRQL) outcomes? Review Topic

Explanation
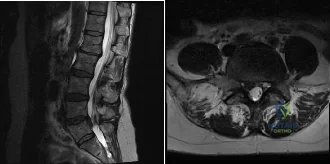
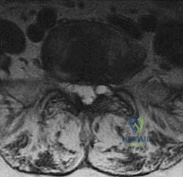
(SBQ12SP.24) A 39-year-old man presents to clinic with a 3-week history of low back pain that radiates to the right lower extremity. On examination, he has mildly decreased sensation over the dorsum of the foot and positive straight leg raise on the right side. MRI images are shown in Figure A and B. Which of the following is true regarding this patient's condition? Review Topic
Nonoperative management with NSAIDS and physical therapy is effective for 50% of patients
Surgical treatment is indicated in patients with diminished sensation
Surgical treatment is equivalent to nonoperative management in terms of pain and function
Good surgical outcome is associated with mainly back complaints
Size of disc herniations typically decrease over time without surgical intervention
The patient is presenting with a lumbar disc herniation at the L4-L5 level. The size of disc herniations decrease in most patients over time without surgical intervention.
Lumbar disc herniations are the result of recurrent torsional strain, which leads to small tears of the annulus fibrosus, ultimately allowing herniation of the nucleus pulposis. First line treatment consists of NSAIDS, muscle relaxants and physical therapy and is effective in 90% of patients. Second line treatment typically involves epidural and selective nerve root corticosteroid injections. Microdiscectomy is reserved for patients with more than 6 weeks of disabling pain that has failed nonoperative management, progressive weakness, or cauda equina syndrome.
In the Spine Patient Outcomes Research Trial (SPORT), Weinstein et al. investigated patient outcomes and satisfaction after operative and nonoperative management of lumbar disc herniations. While the randomized arm of the study did show statistically significant differences in the intent-to-treat analysis due to significant crossover of patients, the observational cohort revealed a significant improvement in pain, function, and disability for patients treated with surgery versus nonoperative measures.
Benson et al. looked at the natural history of massive herniated discs in 37 patients with 7-year follow up. They found a more than 60% reduction in disc size over this time period. Reduction in disc size did not correlate with clinical improvement.
Figure A and B are sagittal and axial T2 MRI images, respectively, showing a right sided lumbar disc herniation at the L4-L5 level.
Incorrect Answers:
Question 4
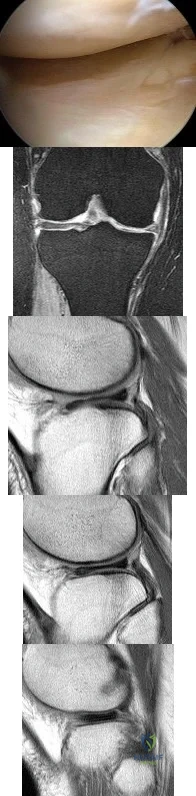
A 24-year-old female soccer player has had lateral joint line pain and a recurrent effusion in the left knee after sustaining a twisting injury 6 weeks ago. She reports that symptoms worsen with athletic activities. MRI scans are shown in Figures 2a through 2c. What is the most likely diagnosis?
Explanation
REFERENCES: Jordan MR: Lateral meniscal variants: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:191-200.
Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 625-630.
Question 5
A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of
Explanation
REFERENCES: Froimson AI: Fracture of the coracoid process of the scapula. J Bone Joint Surg Am 1978;60:710-711.
Gil JF, Haydar A: Isolated injury of the coracoid process: Case report. J Trauma
1991;31:1696-1697.
Question 6
Figure A is the radiograph of an 11-year-old boy who fell directly on his left shoulder while riding a bicycle. He complained of pain in his left shoulder. An MRI scan of the injury is likely to reveal what findings? Review Topic

Explanation
Question 7
Regarding the role of the orthopaedic surgeon in addressing domestic and family violence, all of the following statements are true EXCEPT:

Explanation
state. The AAOS Advisory statement gives information to assist in meeting the ethical and legal obligations on Domestic and Family Violence and Abuse.
Domestic and family violence affects over 10% of the US population (approximately 32 million Americans). Child abuse and neglect contributed to 1,400 fatalities in 2002 and there was 565,747 reports of suspected elder abuse.
Reporting of suspected child abuse is required in all states. The orthopaedic surgeon should hospitalize elderly victims who are in immediate danger and help develop a plan to insure their safety.
Question 8
What is the most common location of osteosarcoma?
Explanation
REFERENCES: Malawer MM, Sugarbaker PH, Malawer M: Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Kluwer Academic Publishers, 2001.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 9
What complication is most likely to occur following proximal humeral fixation with a locked plate-and-screw construct?
Explanation
reduction which can result in failure. However, penetration of the screws remains the most commonly reported complication.
Question 10
A cord-like middle glenohumeral ligament and absent anterosuperior labrum complex can be a normal anatomic capsulolabral variant. If this normal variation is repaired during arthroscopy, it will cause Review Topic
Explanation
Question 11
An 18-year-old male soccer player sustains a knee injury during a game. Examination is notable for a positive pivot shift test. What other physical examination finding is most likely to be present? Review Topic
Explanation
ACL tears usually occur as a result of a non-contact pivoting injury. Abnormal anterior translation results in bone contusions of mid-lateral femoral condyle and posterolateral tibia, which can be seen on MRI. Other concomitant intraarticular injuries include meniscal tears (lateral > medial), chondral damage and other ligamentous injury (MCL, LCL, PLC) usually found in cases of higher energy trauma such as a knee dislocation.
Piasecki et al prospectively analyzed intraarticular injuries associated with ACL tears in high school athletes by gender and sport. There was no significant difference in mechanism of injury between sexes. Female basketball and soccer players had fewer intraarticular injuries (medial femoral condyle lesions, medial and lateral meniscus tears) compared to male athletes. The authors hypothesized that women may therefore enjoy a better prognosis following reconstruction.
Spindler et al performed a prospective cohort study investigating concomitant intraarticular injuries in patients who underwent ACL reconstruction. Eighty percent of patients had a bone bruise on MRI, 68% involving the lateral condyle. At time of arthroscopic reconstruction, meniscal tears were identified in 56% of lateral menisci and 37% of medial menisci.
Incorrect Responses:
Question 12
The fracture seen in Figure 1 is most likely associated with injury to what ligamentous structure?
Explanation
A. Methicillin-resistant Staphylococcus aureus (MRSA)
B. Cutibacterium acnes
C. Enterococcus species
D. Staphylococcus epidermidis
C acnes is the most common organism recovered in prosthetic shoulder infections (33%), Coagulase-negative Staphylococcus is second (21%), Methicillin-sensitive S aureus (13%), and S epidermidis (10%). MRSA accounts for 5% and Enterococcus species, 1.5%.
Question 13
What is the most common reason an individual with a malignant soft-tissue tumor in the extremities seeks medical attention?
Explanation
REFERENCES: Brouns F, Stas M, De Wever I: Delay in diagnosis of soft tissue sarcomas. Eur J Surg Oncol 2003;29:440-445.
Rougraff B: The diagnosis and management of soft tissue sarcomas of the extremities in the adult. Curr Probl Cancer 1999;23:1-50.
Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 14
Figure 23 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain? Review Topic
Explanation
Question 15
A 23-year-old right-hand dominant professional baseball pitcher has right shoulder pain when releasing the ball. He has noticed his velocity has decreased over the past 2 months. Examination reveals supine abducted external rotation of 110 degrees compared to 100 degrees on the left side. His internal rotation is 30 degrees on the right compared to 70 degrees on the left side. Rotator cuff strength is normal. All other clinical tests are normal. MRI with contrast reveals no intra-articular lesions. What is the best course of treatment? Review Topic
Explanation
should then be followed by appropriate rotator cuff and scapular stabilization exercises. Only if this management fails to relieve the patient's symptoms should surgery be considered. This patient clearly does not need external rotation stretching given the fact that he has normal external rotation.
Question 16
A 13-year-old boy has a mild deformity of the left sternoclavicular joint after being involved in a rollover accident while riding an all-terrain vehicle. Examination in the emergency department reveals that he is hemodynamically stable, and his neurovascular examination is normal. The CT scan shown in Figure 22 was obtained because radiographs were inconclusive. Management should consist of
Explanation
REFERENCES: Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, p 581.
Wirth MA, Rockwood CA Jr: Acute and chronic traumatic injuries of the sternoclavicular joint. J Am Acad Orthop Surg 1996;4:268-278.
Question 17
Figures 1 and 2 are the radiographs of a 35-year-old right-hand-dominant man who has had progressive right wrist pain for 1 year. There is no history of trauma, and he has had no treatment to date. He reports some pain at rest with limited motion and substantial pain with use. He is currently out of work on short-term disability because of this wrist problem. An examination reveals mild dorsal wrist swelling, decrease wrist range of motion, and decreased grip strength. Contralateral wrist examination findings are normal. What is the most appropriate course of treatment?

Explanation
This patient has late-stage Kienböck disease. According to the Lichtman classification for Kienböck disease, this would represent stage IIIB, with lunate collapse/fragmentation, loss of carpal height secondary to proximal capitate migration, and a flexed scaphoid. The lateral radiograph reveals a radioscaphoid angle exceeding 60 degrees, so disease stage is IIIB. According to Condit and associates, when the presurgical radioscaphoid angle exceeds 60 degrees, results are poor when an attempt to maintain the lunate is made. As a result, the procedure with the most predictable outcome is a proximal row carpectomy. A radial-shortening osteotomy could be performed because the ulnar variance is negative. Considering the marked lunate fragmentation and collapse, a vascularized bone graft likely is contraindicated and associated with less predictable results than a proximal row carpectomy. There is no role for supervised hand therapy and splinting in the setting of advanced Kienböck disease. Similarly, there is no role for maintenance of the lunate in the setting of advanced collapse and fragmentation.
Question 18
A 6-year-old sustains the injury shown in Figures A and B. The nerve most commonly affected by this fracture pattern innervates which of the following motor groups?

Explanation
The most common neurapraxia after pediatric extension-type supracondylar fractures involve the AIN. It supplies the FPL (thumb IP flexion), the pronator quadratus, and the FDP of the index/long fingers. Subsequently, patients are often unable to make an “a-ok” sign. Most of these neuropraxias resolve without complication. The ulnar nerve is most commonly implicated with flexion-type supracondylar fractures.
Abzug et al. review management of supracondylar fractures. They note that the AIN
is most commonly injured nerve in extension type supracondylar fractures. They note that nerve injuries often resolve within 6-12 weeks.
Babal et al. completed a meta-analysis to determine the risk of neurapraxia associated with pediatric supracondylar fractures. The rate of traumatic neurapraxia was 11.4% amongst 5000 patients. The AIN was affected 34.1% of the time. AIN neurapraxia was most common in extension type injuries.
Figures A and B show an AP and lateral radiographs of a displaced pediatric supracondylar fracture
Incorrect Answers
Question 19
A transverse humeral shaft fracture that occurs between a stiff arthritic shoulder joint; a stiff, arthritic elbow joint is treated nonsurgically in a hanging-arm cast
Explanation
In 1977, Perren and Cordey penned a German manuscript that first described an interpretation of mechanical influences on tissue differentiation. This became known as the Strain Theory of Perren. In 1980, a second manuscript by the same authors was published in English. Within this manuscript, Perren wrote, "These thoughts about the mechanical influences on tissue differentiation are not intended as conclusive evidence since precise data are still not available, but we hope that they will stimulate thought and provide a basis for discussion." More than 30 years later, these thoughts continue to stimulate discussion and research on cell mechanotransduction. This theory is still being manipulated in surgical theatres all around the world in an attempt to more consistently achieve fracture healing. Strain is a magnitude of deformation. As typically defined, it is the change in dimension of a deformed object during loading divided by its original dimension. This is difficult to work with intraoperatively. The fraction below illustrates a simpler way to regard this concept:
Strain = Magnitude of displacement between fragments during loading / Total resting distance between fragments after stabilization
By remembering that low strain generally leads to bone formation and healing, it is possible to manipulate this fraction intraoperatively to achieve success. When a simple fracture pattern is anatomically reduced and compressed, then the total resting distance between fragments after stabilization approaches 0. This means the numerator must be near 0 to achieve a low-strain environment. This is what occurs in absolute stability (no motion between fracture fragments under physiologic load) and primary bone healing occurs. When a multifragmentary fracture pattern is treated with bridge plating, the total resting distance between fragments after stabilization is a larger number (consider the additive distance between the different fragments). In this case, the numerator can be larger to achieve a low-strain environment. This is what happens in relative stability (controlled motion between fracture fragments under physiologic load). Secondary bone healing occurs. Now consider the third scenario: a simple fracture pattern that is fixed with a small gap. The total resting distance is still a small number. Based on the theory, eliminating motion by creating a stiff construct should lead to healing, but it does not. Creating absolute stability with a gap means that primary bone healing cannot occur (because cutting cones cannot cross the gap) and secondary bone healing cannot occur (because there is not enough motion to induce callus formation). This is where the strain theory breaks down and how many nonunions occur. In the fourth scenario, a high-strain environment is present and commonly leads to a nonunion (as predicted by the theory). The simple fracture pattern is too mobile, and nonfunctional callus often occurs.
RECOMMENDED READINGS
Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002 Nov;84(8):1093-110. Review. PubMed PMID: 12463652. View Abstract at PubMed
Epari DR, Duda GN, Thompson MS. Mechanobiology of bone healing and regeneration: in vivo models. Proc Inst Mech Eng H. 2010 Dec;224(12):1543-53. Review. PubMed PMID: 21287837.View Abstract at PubMed
Question 20
Scapular notching following reverse shoulder arthroplasty may be minimized by what technical modification? Review Topic
Explanation
Question 21
A computed tomography (CT) scan has been shown to be indicated for evaluation of all of the following aspects of acetabular fractures, EXCEPT:

Explanation
with CT scanning and acetabular fractures, and noted a 25% change in surgical planning when CT was utilized versus plain radiographs; they also noted the ability to detect marginal impaction and fracture size/position was improved with CT.
Question 22
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416.
Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
Renaldo N, Egol K: Damage-control orthopaedics: Evolution and practical applications.
Am J Orthop 2006;35:285-291.
Question 23
Patient outcome after open reduction and internal fixation of tibial plateau fractures shows that patients older than 50 years of age when compared to younger patients have
Explanation
Question 24
A deficiency of which of the following is associated with an increased risk of venous thromboembolism?
Explanation
Question 25
A total knee arthroplasty is recommended to a mentally competent 68-year-old woman who has disabling knee pain caused by degenerative arthritis. Her son has researched the procedure on the internet and prefers the Acme Female Knee for his mother. You have designed the Axis Woman's Knee, for which you receive royalties, and use it exclusively. Which of the following ethical principles takes precedence in guiding her treatment?
Explanation
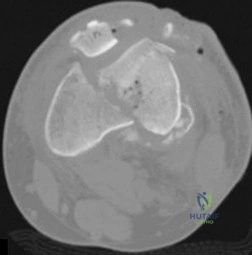
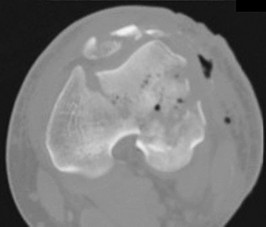
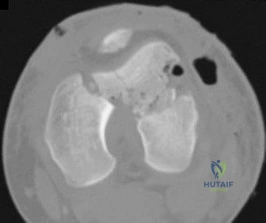
Question 26
Figure A shows intraoperative images of a right knee in an 8-year-old boy after he sustained an injury. Which of the following is the most common indication for performing this procedure? Review Topic
Explanation
Arthroscopic treatment of lateral discoid meniscus injuries has the advantages of reducing trauma, precise resection or repair of the meniscus and saucerization of the remaining discoid meniscus. Operative treatment is usually limited to patients with pain and mechanical symptoms that are undergoing partial meniscectomy or repair. Asymptomatic discoid meniscus without tears are not considered a surgical indication for routine saucerization.
Kramer et al. reviewed the diagnosis and treatment of traumatic discoid meniscal tears in children. They report that knee shape, size and skeletal maturity must be considered when determining the optimal method of repair. However, all symptomatic torn discoid menisci are best treated with saucerization and repair.
Good et al. looked at the arthroscopic techniques of discoid meniscus repair. Arthroscopic saucerization was successful in 28 of 30 knees and meniscal repair in 23 of 30 knees. At final follow-up, all patients exhibited full knee flexion beyond 135 degrees. In 3 of 30 patients there was residual knee pain, and four reported intermittent mechanical symptoms.
Figure A shows a series of arthroscopic images of the right knee lateral compartment. There is a sequential saucerization of the discoid meniscus.
Incorrect Answers:
(SBQ13PE.83) 8-year-old boy complains of intermittent painless clicking in his knee. His physical examination is normal. His family doctor orders an MRI, which reveals an incomplete lateral discoid meniscus without evidence of tear. What is the most appropriate treatment? Review Topic
Observation only
Diagnostic arthroscopy
Saucerization of meniscus
Saucerization of meniscus and microfracture
Saucerization and stabilization of the mensicus
The clinical presentation is consistent with a asymptomatic discoid meniscus. The most appropriate treatment at this time would be observation only.
MRI scans of the knee are very sensitive for identifying discoid menisci. Diagnosis is usually made when there are 3 or more 5mm sagittal MRI images showing meniscal continuity. Treatment is mostly focused on conservative modalities. Asymptomatic tears are usually treated with observation only. Saucerization is indicated for recurrent locking, swelling, persistent pain, or radiographic evidence of a meniscal tear.
Watanabe et al. described three types of discoid lateral menisci based on arthroscopic appearance. In this classification, discoid menisci with normal peripheral attachments are either type I (complete) or type II (incomplete). Type III discoid menisci, the so-called Wrisberg ligament type, are lacking posterior capsular attachments with the exception of the posterior meniscofemoral ligament.
Kramer et al. looked at the presentation of pediatric knee pain and discoid meniscus. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the meniscus.
Illustration A shows the cross-section of normal meniscus. Illustration B shows the Watanabe classification.
Incorrect Answers:
Question 27
Which of the following clinical scenarios represents the strongest indication for locked plating technique in a 70-year-old woman?
Explanation
Question 28
What effect does deep freezing have on allograft tissue?
Explanation
REFERENCES: Shelton WR, Treacy SH, Dukes AD, Bomboy AL: Use of allografts in
knee reconstruction: I. Basic science aspects and current status. J Am Acad Orthop Surg 1998;6:165-168.
Caspari RB, Botherfield S, Horwitz RL, et al: HIV transmission via allograft organs and tissues. Sports Med Arthroscopy Rev 1993;1:42-46.
Question 29
Figure 80a shows an arthroscopic view from an infralateral portal of a right knee. Figure 80b shows a coronal MRI scan, and Figures 80c through 80e show consecutive sagittal images of the knee. The images show what anatomic finding? Review Topic
Explanation
Question 30
When treating thoracic disk herniations, which of the following surgical approaches has the highest reported rate of neurologic complications?
Explanation
REFERENCES: Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
Benjamin V: Diagnosis and management of thoracic disc disease. Clin Neurosurg
1983;30:577-605.
Russell T: Thoracic intervertebral disc protrusion: Experience of 67 cases and review of the literature. Br J Neurosurg 1989;3:153-160.
Fessler RG, Sturgill M: Review: Complications of surgery for thoracic disc disease. Surg Neurol 1998;49:609-618.
Question 31
An 11-year-old boy with bipolar disorder fell from a tree and sustained an open fracture dislocation of the right ankle with extensive abrasions of the leg. Immediate irrigation, debridement, reduction, and provisional fixation with Kirschner wires was performed. Twenty-four hours later, the patient’s blood pressure is 190/100 mm Hg and pulse rate is 120. He has required only 1 dose of an oral analgesic for pain control. His foot and ankle are markedly swollen, but there is no pain on passive extension of the toes. The dorsalis pedis pulse cannot be palpated. What is the most appropriate next treatment step? Review Topic
Explanation
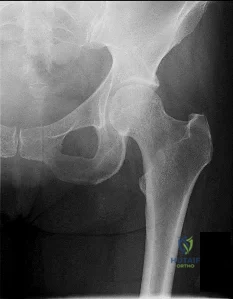
(SBQ13PE.91) An 12-year-old girl presents with right hip pain. Bilateral frog laterals are shown in Figure A. Laboratory work-up reveals TSH 11 mIU/L (Ref range: 0.4-4.0 mIU/L) and Free T4 is 0.5 ng/dL (Ref range: 0.7-1.9 ng/dL). What is the most appropriate treatment recommendation? Review Topic

In situ pinning of right hip
Protected weight bearing and MRI of right hip
Immediate endocrine referral and treatment
Open biopsy right hip
In situ pinning bilateral hips PREFERRED RESPONSE 5
In patients with slipped capital femoral epiphysis (SCFE) and concomitant endocrinopathy, bilateral pinning is the recommended treatment.
This patient's laboratory values reveal hypothyroidism, which increases the risk of bilateral involvement. Thus, the most appropriate treatment recommendation is surgical fixation of both hips.
Wells et al. analyzed 131 SCFEs over a 30-year period. The authors noted that 100% of patients with associated endocrinopathy went onto contralateral slip and recommended not only prophylactic pinning, but in those with open triradiate cartilage, recommended preventative screening with TSH/Free T4 laboratory studies.
Riad et al. followed 90 patients and analyzed impact of age, gender and race on contralateral slip development. Girls under the age of 10 and boys under the age of 12 had a significantly increased risk of contralateral involvement. Therefore, the authors recommended contralateral pinning for girls and boys that met those age criteria, respectively.
Figure A exhibits a right SCFE on bilateral frog lateral views. Incorrect Answers:
Question 32
Which of the following is not a characteristic of synovial sarcomas?
Explanation
REFERENCES: Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1109-1126.
Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Question 33
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?
Explanation
REFERENCE: Lansinger O, Bergman B, Korner L, et al: Tibial condylar fractures: A twenty-year follow-up. J Bone Joint Surg Am 1986;68:13-19.
Question 34
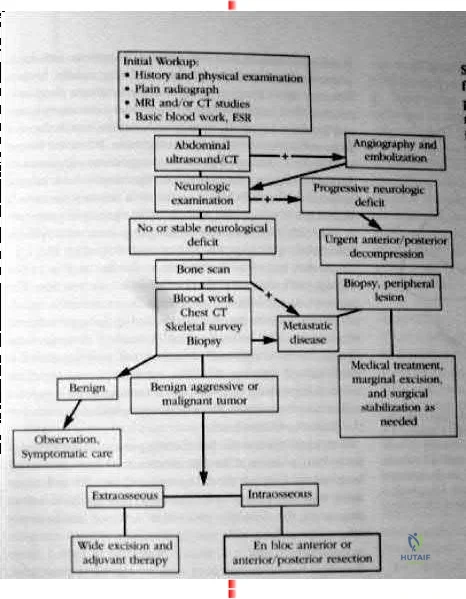
maximize physical capacity and 4) obtain local control of the disease. Other trivia from the references include: After the lung and liver the skeletal system is the third most common site of metastasis. The spine is the most common site of skeletal metastasis. 60% of all skeletal lesions and 36% are asymptomatic. Breast, prostate, lung and renal carcinoma comprise 80% of the carcinomatous skeletal metastasis. 70% metastasis occur in the thoracic and thoracolumbar regions. 21% had involvement of the lumbar and sacral regions. 8% involved the cervical and cervicothoracic regions together. As many as 90% of patients who die of cancer may have Spinal metastasis at autopsy, and only half of patients who die from cancer will have symptoms from spinal mets. Fewer than 10% with spinal mets are treated surgically. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont IL., American academy of orthopaedic surgeons, 2002, pp 723-736. back to this question next question 03 What is the most frequently encountered complication following juvenile hallux valgus correction?
Explanation

Coglin’s referenced paper is a study out of Idaho. 11 year retrospective study of 45 patients (60 feet). A multiprocedural approach was used to surgically correct the deformity. There were 6 recurrences of the deformities and eight
complications (6 cases of hallux varus, one case of wire breakage and one case of undercorrection.) So according to their reference this question has two correct answers.

Postoperative complications have been frequently reported following juvenile hallux valgus corrections. Recurrence following surgery is probably the most frequently reported complication and is likely due to the high rate of congruency associated with a juvenile hallux valgus deformity.

OKU Foot and Ankle 2 Rosemont IL., American academy of orthopaedic surgeons, pp135-150.
back to this question next question
Question 35
Figure 37 shows the clinical photograph of a 1-day-old infant who weighed 10.25 lb at birth. Examination reveals an absent right Moro reflex and limited active motion of the right shoulder, elbow, and wrist, but flexion of the fingers. Passive range of motion of the shoulder and elbow is normal. What is the most likely diagnosis?
Explanation
REFERENCES: Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:997-1001.
Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667.
Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:668-677.
Question 36
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?
Explanation
REFERENCES: Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, p 855.
Manske PR (ed): Hand Surgery Update. Rosemont, IL, American Society for Surgery of the Hand, 1994, pp 77-84.
Question 37
In patients with Crowe types III and IV developmental dysplasia of the hip with high hip centers, acetabular reconstruction often requires lowering the acetabular component into the native acetabulum. In doing so, considerable risk for limb lengthening beyond 4 cm exists, making the hip difficult to reduce and raising the risk for nerve injury. Which technique is used to overcome this problem?
Explanation
When substantial lengthening of a dysplastic hip will occur because a high dislocation is relocated into a considerably lower acetabulum, a femoral shortening may be necessary to reduce the hip and avoid a stretch injury to the sciatic nerve. No other choice specifically addresses the need for femoral shortening, and high offset stems and lateralized liners may exacerbate the problem if used alone and without femoral shortening.
Question 38
Which of the following findings is a prerequisite for a high tibial valgus osteotomy for medial compartment gonarthrosis?
Explanation
REFERENCES: Naudie D, Bourne RB, Rorabeck CH, Bourne TT: The Insall Award: Survivorship of the high tibial valgus osteotomy. A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 255-264.
Question 39
Which of the following tissues has the highest maximum load to failure?
Explanation
REFERENCES: Woo SL, Hollis JM, Adams DJ, et al: Tensile properties of the human femur-anterior cruciate ligament-tibia complex: The effects of specimen age and orientation. Am J Sports Med 1991;19:217-225.
Staubli HU, Schatzmann L, Brunner P, et al: Quadriceps tendon and patellar ligament cryosectional anatomy and structural properties in young adults. Knee Surg Sports Traumatol Arthrosc 1996;4:100-110.
Wilson TW, Zafuta MP, Zobitz M: A biomechanical analysis of matched bone-patellar tendon-bone and doubled looped semitendinosus and gracilis tendon grafts. Am J Sports Med 1999;27:202-207.
Question 40
Which of the following best describes athletic pubalgia?
Explanation
REFERENCES: Meyers WC, Foley DP, Garrett WE, Lohnes JH, Mandlebaum BR: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Albers SL, Spritzer CE, Garrett WE Jr, Meyers WC: MR findings in athletes with pubalgia. Skeletal Radiol 2001;30:270-277.
Question 41
A 30-year-old woman sustains a transverse amputation of the distal phalanx of the index finger, leaving exposed bone. What is the most appropriate management of the soft-tissue defect?
Explanation
the thumb.
REFERENCES: Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Atasoy E, Ioakimidis E, Kasdan ML, et al: Reconstruction of the amputated fingertip with a triangular volar flap: A new surgical procedure. J Bone Joint Surg Am 1970;52:921-926.
Question 42
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time? Review Topic
Explanation
point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis.
(SBQ12SP.20) Amphotericin B is most appropriate for the treatment of which type of spine infection? Review Topic
Fungal osteomyelitis
Bacterial osteomyelitis with a gram-positive organism
Bacterial osteomyelitis with a gram-negative organism
Tuberculous osteomyelitis
Viral meningomyelitis
Amphotericin B would be most appropriate for the treatment of fungal infections of the spine.
Amphotericin B is a broad-spectrum anti-fungal medication. It is commonly used as the first-line agent for treatment of fungal infections of the spine. The most common fungi involving the spine include cryptococcus, candida, and aspergillus. The indications for débridement and stabilization with spinal fusion, includes resistance to antibiotic therapy, spinal instability, and/or neurologic deficits.
Kim et al. reviewed fungal infections of the spine. They comment that fungus infections are most commonly spread by hematogenous or direct spread. Access to the vascular system may include intravenous lines, during implantation of prosthetic devices, or during surgery.
Frazier et al. retrospectively reviewed 11 patients with fungal osteomyelitis of the spine. Nine of the patients were immunocompromised secondary to diabetes mellitus, corticosteroid use, chemotherapy for a tumor, or malnutrition. All were treated with anti-fungal medication. 10 of 11 patients were also treated with surgical debridement. Paralysis secondary to the spine infection developed in eight patients. After an average of 6.3 years of follow-up, the infection had resolved in all nine surviving patients.
Illustration A shows the mechanism of action of Amphotericin. Illustration B shows T1- (Image A and B) and T2-weighted (Image C) images of the lower thoracic and lumbar spine. There are hypointense signals within the T12 and L1 vertebral bodies (Images A and B) indicative of fungal osteomyelitis.
IncorrectAnswers:
Question 43
Figures 1 and 2 are the most recent radiographs of an 18-year-old high school student who sustains an anterior shoulder dislocation playing recreational football. He has a low Beighton score on physical examination. He was closed reduced and underwent a course of physical therapy but had a second dislocation playing recreational basketball. What is the most appropriate course of treatment, with the lowest complication rate, to prevent further dislocation?

Explanation
injury and hardware problems, exceeds that of arthroscopic Bankart repair.
Question 44
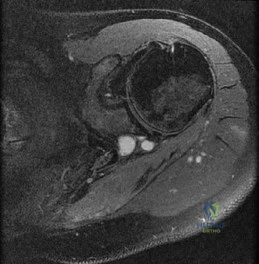
What is the most likely cause of the lesion shown in Figures 35a and 35b?
Explanation
REFERENCES: Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Jarvinen TA, Jarvinen TL, Kaariainen M, et al: Muscle injuries: Biology and treatment. Am J Sports Med 2005;33:745-764.
Question 45
Figure 12 shows an arthroscopic view from an inferolateral portal of a right knee. The asterisk indicates which structure?

Explanation
The asterisk indicates the anteromedial bundle of the anterior cruciate ligament. The anterior cruciate ligament consists of 2 functional bundles: anteromedial and posterolateral. During extension of the knee, the posterolateral bundle becomes taut. In flexion, the anteromedial bundle is tight and the posterolateral bundle relaxes. Recently, techniques for double-bundle reconstruction have been described to recreate the normal anatomic relationship of the 2 bundles.
RECOMMENDED READINGS
Chhabra A, Zelle BA, Feng MT, Fu FH. The arthroscopic appearance of a normal anterior cruciate ligament in a posterior cruciate ligament-deficient knee: the posterolateral bundle (PLB) sign. Arthroscopy. 2005 Oct;21(10):1267. PubMed PMID: 16226658. View Abstract at PubMed
Cha PS, Brucker PU, West RV, Zelle BA, Yagi M, Kurosaka M, Fu FH. Arthroscopic double-bundle anterior cruciate ligament reconstruction: an anatomic approach. Arthroscopy. 2005 Oct;21(10):1275. PubMed PMID: 16226666. View Abstract at
PubMed
Question 46
In the first dorsal compartment of the wrist, what tendon most frequently contains multiple slips?
Explanation
REFERENCES: Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM: Anatomical variations in the first extensor compartment of the wrist: A clinical and anatomical study. J Bone Joint Surg Am 1986;68:923-926.
Minamikawa Y, Peimer CA, Cox WL, Sherwin FS: DeQuervain’s syndrome: Surgical and anatomical studies of the fibro-osseous canal. Orthopedics 1991;14:545-549.
Question 47
Figure 12 shows the lumbar CT scan of a 24-year-old man who was injured in a snowmobile accident. What is the mechanism of injury?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Spivak JM, Vaccaro AR, Cotler JM: Thoracolumbar spine trauma: Principles of management. J Am Acad Orthop Surg 1995;3:353-360.
Question 48
Figure 33 shows the oblique radiograph of an 11-year-old boy who has a mild left flatfoot deformity. Examination reveals that subtalar motion is limited and painful. Despite casting for 6 weeks, the patient reports foot pain that limits participation in sport activities. A CT scan shows no subtalar joint abnormalities. Management should now include
Explanation
has been described for treatment of the peroneal spastic flatfoot without demonstrable
tarsal coalition.
REFERENCES: Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interposition of the extensor digitorum brevis muscle. J Bone Joint Surg Am 1990;72:71-77.
Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Luhmann SJ, Rich MM, Schoenecker PL: Painful idiopathic rigid flatfoot in children and adolescents. Foot Ankle Int 2000;21:59-66.
Question 49
A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of 25 degrees. The O’Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management? Review Topic
Explanation
Question 50
Which of the following pelvic injury types has the highest reported mortality rate?
Explanation

OrthoCash 2020
Question 51
Which of the following is considered a contraindication to cement injection techniques, such as kyphoplasty or vertebroplasty, in the treatment of osteoporotic compression fractures?
Explanation
REFERENCES: Phillips FM, Pfeifer BA, Leiberman IH, et al: Minimally invasive treatment of osteoporotic vertebral compression fractures: Vertebroplasty and kyphoplasty. Instr Course Lect 2003;52:559-567.
Truumees E, Hilibrand A, Vaccaro AR: Percutaneous vertebral augmentation. Spine J 2004;4:218-229.
Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 52
A middle-aged man sustains traumatic loss of the second, third, and fourth toes in a lawnmower accident. The wound is grossly contaminated with soil. Penicillin is added to his antibiotic regimen for coverage of what bacteria? Review Topic
Explanation
Question 53
Figures 1 and 2 are the radiographs of a 20-year-old college multisport athlete who has had longstanding pain in his left hip. He denies any specific event that initiated his pain, but he notes that he had hip problems when he was an infant. He denies pain with activities of daily living, but he believes his pain is increasingly limiting his ability to exercise. He localizes the pain to his groin. He denies low-back or buttock pain or pain that radiates down his leg. What is the most likely diagnosis for the source of this patient's pain?

Explanation
Question 54
Which of the following nerves is most commonly injured when obtaining a bone graft from the posterior ilium?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 295-297.
Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 379.
Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 23.
Ebraheim NA, Elgafy H, Xu R: Bone-graft harvesting from iliac and fibular donor sites: Techniques and complications. J Am Acad Orthop Surg 2001;9:210-218.
Question 55
A 20-year-old basketball player has tenderness and bruising after sustaining a blow to the knee. A radiograph is shown in Figure 15. What is the most likely diagnosis?
Explanation
REFERENCES: Schmidt DR, Henry JH: Stress injuries of the adolescent extensor mechanism. Clin Sports Med 1989;8:343-355.
Weaver JK: Bipartite patellae as a cause of disability in the athlete. Am J Sports Med 1977;5:137-143.
Question 56
An investigation studying whether physical therapy or subacromial injection can be successfully used to treat shoulder pain is conducted. Two groups are identified. One group is prescribed physical therapy, while the other receives a subacromial injection. The groups have similar baseline demographics and shoulder pathologies. Ten patients are randomized in each group and findings show that there is no significant difference in any patient-reported outcome measure. An increase in sample size would reduce the risk of what parameter?
Explanation
Question 57
- Radiographs of a 20-year-old college athlete who sustained an injury to the ankle reveal no fractures or widening of the ankle mortise. Examination shows swelling at the ankle region and pain with medial lateral compression of the distal tibiofibular joint. Which of the following studies would best help in confirming a diagnosis?
Explanation
2 and 3 are occasionally utilized when there is questionable involvement of surrounding bone or tendons. 4 rarely indicated for acute ankle sprain but can help in the diagnosis of RSD following ankle injury.
Question 58
During the ilioinguinal approach to the pelvis, the corona mortis artery must be identified and ligated if present. The corona mortis artery joins the external illiac artery with which other major artery?

Explanation
Question 59
Posterior spinal fusion for scoliosis should be performed on a patient with Duchenne muscular dystrophy when
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 635-651.
Mubarak SJ, Morin WD, Leach J: Spinal fusion in Duchenne muscular dystrophy: Fixation and fusion to the sacropelvis? J Pediatr Orthop 1993;13:752-757.
Question 60
below show the radiographs obtained from an year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 61
Figure 27 shows the radiograph of a 68-year-old woman with a history of rheumatoid arthritis who was injured in a fall. History reveals that she has been asymptomatic since undergoing a left total knee arthroplasty 9 years ago. Management should consist of
Explanation
REFERENCE: Ayers DC: Supracondylar fracture of the distal femur proximal to a total knee replacement, in Springfield DS (ed): Instructional Course Lectures 46. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-203.
Question 62
Figures 25a and 25b show the radiograph and MRI scan of a 7 1/2-year-old boy who has been limping for 1 year. His pain has worsened over the past 2 weeks, and his parents note swelling over the dorsum of the foot for the past 4 days. Examination reveals no fever, and laboratory studies show a WBC of 6,700/mm 3 , an erythrocyte sedimentation rate of 26 mm/h, and a normal C-reactive protein level. What is the most likely diagnosis?
Explanation
REFERENCES: Wang MN, Chen WM, Lee KS, Chin LS, Lo WH: Tuberculous osteomyelitis in young children. J Pediatr Orthop 1999;19:151-155.
Watts HG, Lifeso RM: Tuberculosis of the bones and joints. J Bone Joint Surg Am 1996;78:288-298.
Question 63
-What is the most likely cause of an acute femur fracture in a 5-month-old child?
Explanation

Question 64
Figures 1 and 2 show the postreduction radiographs obtained from a 32-year-old man who fell from a ladder onto his outstretched right arm. He reports right wrist pain and dense numbness in his radial digits. What is the most appropriate treatment option?

Explanation
This patient sustained a lesser-arc perilunate dislocation. As a result of the injury, he also developed acute carpal tunnel syndrome. The closed reduction attempt was unsuccessful; therefore, this injury is best managed with emergent surgery, an open carpal tunnel release, an open reduction of the perilunate dislocation, scapholunate ligament repair, and intercarpal pinning. Outpatient surgery in a delayed fashion is not advised because of the acuity and severity of the carpal tunnel syndrome. Closed reduction and casting is not advised, because it commonly leads to continued carpal instability with subsequent dorsal
intercalated segment instability deformity and scaphoid lunate advanced collapse wrist arthritis.
Question 65
The wear resistance of ultra-high molecular weight polyethylene can be improved by exposing the polymer to high-energy radiation (eg, gamma or electron beam), followed by a thermal treatment. What is one detrimental side effect of this process?
Explanation
REFERENCES: Collier JP, Currier BH, Kennedy FE, et al: Comparison of cross-linked polyethylene materials for orthopaedic applications. Clin Orthop 2003;414:289-304.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 203-208.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 66
A 22-year-old professional ballet dancer reports a 3-month history of posterior ankle pain that occurs when she changes from a flat foot to pointe (hyperplantar flexed position). Examination does not elicit the pain with forced passive plantar flexion. A radiograph is shown in Figure 8. What is the most likely cause of the pain?
Explanation
REFERENCES: Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
Khan K, Brown J, Way S, et al: Overuse injuries in classical ballet. Sports Med
1995;19:341-357.
Question 67
An obtunded 80-year-old man was found alone in his apartment after an apparent fall. A CT scan performed in the emergency department shows that he has an extensile injury of an ankylosed cervical spine. The fracture extends across the ossified C5-C6 disk space and into the lamina of C5. There is 1.5 cm of widening between the C5 and C6 vertebrae anteriorly. The patient's family asks you about the long-term impact of the fracture on his functional capacity and survival. You advise them that patients with fractures of the cervical spine with ankylosing conditions have
Explanation
Several studies have found that rates of neurologic deficit and mortality are higher for patients with ankylosing spondylitis and a spinal fracture than for age-matched controls. The 2011 work of Schoenfeld and associates, which directly compared patients with cervical fractures in ankylosed spines to age-and sex-matched controls who also had cervical fractures but no ankylosing condition, demonstrated that those with ankylosing spondylitis were at elevated risk for mortality for up to 2 years after sustaining a fracture. In a study by Westerveld and associates, the rate of neurologic deficit among patients with ankylosing spondylitis and a spinal fracture was 57.1% compared to 12.6% among controls.
RECOMMENDED READINGS
Westerveld LA, van Bemmel JC, Dhert WJ, Oner FC, Verlaan JJ. Clinical outcome after traumatic spinal fractures in patients with ankylosing spinal disorders compared with control patients. Spine J. 2014 May 1;14(5):729-40. doi: 10.1016/j.spinee.2013.06.038. Epub 2013 Aug 27. PubMed PMID: 23992936. View Abstract at PubMed
Schoenfeld AJ, Harris MB, McGuire KJ, Warholic N, Wood KB, Bono CM. Mortality in elderly patients with hyperostotic disease of the cervical spine after fracture: an age- and sex-matched study. Spine J. 2011 Apr;11(4):257-64. doi: 10.1016/j.spinee.2011.01.018. Epub 2011 Mar 5. PubMed PMID: 21377938. View Abstract at PubMed
Question 68
A 36-year-old man has a 2-day history of acute lower back pain with severe radicular symptoms in the left lower extremity. The patient has a positive straight leg test at 40 degrees on the left side and mild decreased sensation on the dorsum of the left foot. What is the most appropriate management at this time? Review Topic
Explanation
Question 69
A 10-year-old child has leg discomfort with activity. A radiograph, bone scan, and biopsy specimen are shown in Figures 1a through 1c. What is the most likely diagnosis?
Explanation
REFERENCES: Harris WH, Dudley HR Jr, Barry RS: The natural history of fibrous dysplasia: An orthopaedic, pathological and roentgenographic study. J Bone Joint Surg Am 1962;44:207.
Campanacci M: Bone and Soft Tissue Tumors. Vienna, Austria, Springer-Verlag, 1990.
Question 70
A 7-year-old male is struck by a motor vehicle while crossing the street and suffers an open tibia fracture with a crush injury of the ipsilateral foot. After multiple attempts at limb salvage, the family and treating surgeon elect to proceed with a knee disarticulation. What complication of pediatric amputations is avoided with a knee disarticulation as opposed to a transtibial amputation?

Explanation
Krajbich reviews the management of pediatric patients with lower-limb deficiences and amputations. He advocates disarticulation as opposed to transosseous amputation when possible as bone overgrowth has not been observed in bone ends covered by articular cartilage.
O'neal et al retrospectively reviewed their rates of surgical revision for bone overgrowth in pediatric and adolescent amputees. The highest rates of revision were seen with metaphyseal-level amputations (50%) and with traumatic amputations (43%).
Benevenia et al reviewed their rates of overgrowth in skeletally immature transosseous amputees using an autogenous epiphyseal transplant from the amputated limb to cap the medullary canal. They found that only 1 of 10 patients undergoing amputation with this technique had complications due to bone overgrowth, compared with 6 of 7 patients undergoing traditional transosseous amputation.
Illustration A is a clinical photo of bone overgrowth eroding through the soft tissue in a transhumeral amputee. Illustration B demonstrates the radiographic appearance of bone overgrowth in a transtibial amputation.
Incorrect Answers:
Question 71
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?
Explanation
ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Paletta GA Jr, Laskins RS: Total knee arthroplasty after a previous patellectomy. J Bone Joint Surg Am 1995;77:1708-1712.
Question 72
What is a known risk factor for lateral distal femoral locking plate failure when used for the fixation of comminuted extra-articular fractures?
Explanation
Implant failure is common in distal femur fractures stabilized with plate fixation. Contributors to failure include a short working length of the construct, plate-screw density more than 0.5 and short plate lengths. This will lead to failure as it causes increased strain on the plate over a short segment, and
does not allow enough motion at the fracture site to form bone for healing by secondary intention.
Ricci et al. reviewed 355 cases of distal femur plate fixation. 64 patients (19%) required reoperation to promote union, including 30 that had a planned staged bone grafting. Risk factors for proximal implant failure included open fracture, smoking, increased body mass index, and shorter plate length.
Kregor et al. reviewed 119 patients with distal femoral plate fixation. They found that 93% fractures healed without acute bone grafting. Complications included 5 losses of proximal fixation, 2 nonunions, and 3 acute infections.
Illustration A is an AP of the distal femur demonstrating a comminuted distal femur fracture which has failed fixation with a laterally based distal femur locking plate. It has undergone varus collapse which is a common mechanism of failure for these injuries. Illustration B is a series of AP radiographs of the distal femur of the same patient that was revised to an intramedullary retrograde nail. Illustration C and D show the concepts of plate length, plate-to-screw density and the working length of the plate.
Incorrect Answers:

OrthoCash 2020
Question 73
Figure 51 shows an arthroscopic view of the patellofemoral joint from an inferolateral portal. The arrow points to which of the following structures?
Explanation
REFERENCES: Clarke HD, Scott WN, Insall JN: Anatomic aberrations, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 67-85.
Patel D: Plica as a cause of anterior knee pain. Orthop Clin North Am 1986;17:273-277.
Question 74
A corset-type brace may help reduce symptoms during an episode of acute low back pain as the result of
Explanation
REFERENCES: Nachemson A, Morris JM: In vivo measurements of intradiscal pressure: Discometry, a method for determination of pressure in the low lumbar disc. J Bone Joint Surg Am 1964;46:1077-1092.
Axelsson P, Johnsson R, Stromqvist B: Effect of lumbar orthosis on intervertebral mobility: A roentgen stereophotogrammetric analysis. Spine 1992;17:678-681.
Question 75
A 58-year-old African-American female who sustained an injury to her upper arm six months ago presents with persistent arm pain. She was initially treated with splinting, with conversion to fracture bracing. She is neurovascularly intact. An injury radiograph and a current radiograph are shown in Figures A and B respectively. What nutritional or metabolic disturbance is the most likely associated with this patient's diagnosis? Review Topic

Explanation
The incidence of nonunion with non-operative management of humeral shaft injuries ranges from 2-10%. Risk factors include vitamin D deficiency (most common), open fractures, segmental injuries, smoking and obesity. The optimal treatment is compression plating with bone grafting, which has been shown to be superior to intramedullary nailing with bone grafting or compression plating alone.
Ring et al. reviewed factors that contributed to humeral diaphyseal nonunion after fracture bracing. Fractures in the proximal to middle one-third of the shaft or fractures with a spiral/oblique pattern were more likely to go on to nonunion.
Brinker et al. reviewed 37 low-energy fractures that went onto nonunion. These patients were evaluated by clinical endocrinologists for evaluation of metabolic abnormalities. Thirty-one of the 37 patients (84%) had a metabolic issue, with 68% (25 of 37 patients) having Vitamin D deficiency.
Figure A demonstrates a humeral shaft fracture. Figure B demonstrates an atrophic nonunion of the humeral shaft fracture.
Incorrect Answers:
Question 76
A right-handed 24-year-old woman underwent an arthroscopic Bankart repair for recurrent anterior dislocations 9 months ago. Despite extensive physical therapy for 8 months, the patient has very limited range of motion (elevation to 130 degrees and external rotation to 10 degrees with the arm at the side). Shoulder radiographs are normal. The next step in management should consist of
Explanation
REFERENCES: Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Harryman DT II, Matsen FA III, Sidles JA: Arthroscopic management of refractory shoulder stiffness. Arthroscopy 1997;13:133-147.
Question 77
A 77-year-old woman underwent semiconstrained right total elbow arthroplasty 4 weeks ago through a Bryan-Morrey approach. Her recovery was uneventful until 2 days ago when she began her physical therapy session at an outpatient clinic. During resisted extension exercises, she felt a "pop" in her elbow, accompanied with pain and inability to extend her elbow against resistance. What is the most likely cause of her symptoms? Review Topic
Explanation
Question 78
Figure 19 shows the radiograph of a 12-year-old boy who sustained an injury to his hand when another child fell on him. Management should consist of
Explanation
REFERENCES: Carey TP: Fracture and dislocations of the phalanges, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 435-436.
Ogden JA: Skeletal Injury in the Child. New York, NY, Springer-Verlag, 2000, p 668.
Question 79
A 34-year-old male arrives intubated with a closed head injury to the trauma bay after a motor vehicle accident. After initial hospital workup and resuscitation, he is transferred to the intensive care unit. In addition to multiple systemic injuries, he sustained the closed injury shown in Figure A. Intracompartmental pressure monitoring of the limb measure in a range from 28-30 mm Hg. Which of the following sustained blood pressure measurements would support the treatment of limb fasciotomy? Review Topic 1 110/60 mmHg 2 115/55 mmHg 3 92/64 mmHg

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam - especially with intubated patients. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy.
McQueen et al. prospectively reviewed 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Olson et al. provide a review of compartment syndrome for the lower extremity. They discuss a variety of injuries and medical conditions that may initiate acute compartment syndrome, including fractures, bleeding disorders, and other trauma. Although the diagnosis is primarily a clinical one, they also recommend supplementation with compartment pressure measurements in equivocal cases.
Figure A shows a closed comminuted tibial shaft fracture. Incorrect Answers:
Question 80
The artery of Adamkiewicz (arteria radicularis, arteria magna) is most commonly found on the
Explanation
REFERENCES: Stambaugh J, Simeone F: Vascular complication in spine surgery, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1715.
Lazorthes G: Arterial vascularization of the spinal cord. J Neurosurg 1971;35:253-262.
Question 81
-Figure 19 is the lateral weight-bearing radiograph of a 28-year-old man with a 3-week history of unrelenting heel pain after increasing his marathon training intensity. The pain never improves throughout the day. Each step he takes is painful. Examination reveals pain with medial-to-lateral compression of the
Explanation
Question 82
A 13-year-old boy has a painless “knot” over his left hip. History reveals that he injured his left hip playing soccer 4 months ago. A radiograph and MRI scan obtained at the time of injury are shown in Figures 7a and 7b. He is very active and is currently asymptomatic. A current radiograph is shown in Figure 7c. What is the next most appropriate step in management?
Explanation
REFERENCES: Miller AE, Davis BA, Beckley OA: Bilateral and recurrent myositis ossificans in an athlete: A case report and review of treatment options. Arch Phys Med Rehabil 2006;87:286-290.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 15-27.
Question 83
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and Weinstein monofilament is normal. Tibialis anterior and peroneus brevis are weak but present. What is the most appropriate management?
Explanation
REFERENCES: Younger AS, Hansen ST Jr: Adult cavovarus foot. J Am Acad Orthop Surg 2005;13:302-315.
Sammarco GJ, Taylor R: Cavovarus foot treated with combined calcaneus and metatarsal ostetotomies. Foot Ankle Int 2001;22:19-30.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL,
American Academy of Orthopaedic Surgeons, 2003, pp 135-143.
Question 84
The anterior approach to total hip arthroplasty requires dissection between which of the following muscle planes?
Explanation
DISCUSSION: The anterior approach to the hip joint involves identifying the plane between the tensor fascia lata and the sartorius muscles.
REFERENCES: Berger RA, Duwelius PJ: The two-incision minimally invasive total hip arthroplasty: Technique and results. Orthop Clin North Am 2004;35:163-172.
Matta JM, Shahrdar C, Ferguson T: Single-incision anterior approach for total hip arthroplasty on an orthopaedic table. Clin Orthop Relat Res 2005;441:115-124.
28 • American Academy of Orthopaedic Surgeons
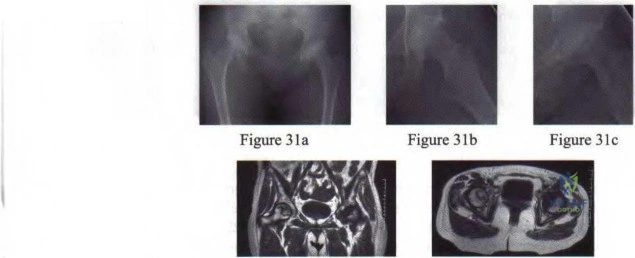
Figure 3Id Figure 31e
Question 85
At the first postoperative visit after mini-open carpal tunnel release, a patient reports hand weakness. Poor index finger interphalangeal joint extension and metacarpophalangeal joint flexion are present. This finding is most consistent with
Explanation
Complications after carpal tunnel release are relatively uncommon. The clinical picture described above is most consistent with lumbrical muscle weakness secondary to neuropraxia of the proper palmar digital nerve to the index finger supplying motor innervation to that muscle. The recurrent motor branch of the median nerve innervates the thenar musculature and would not present as index finger weakness. A new onset of trigger finger may result from a loss of the pulley effect of the transverse carpal ligament, postoperative tendon inflammation, or previously unrecognized flexor tendon triggering. Flexor digitorum profundus to the index finger lies deep within the carpal tunnel, making its injury unlikely. If it were injured, the result would not be weakness of interphalangeal joint extension.
Question 86
A 36-year-old man was injured in a motorcycle collision and sustained the injury shown in Figure 70. He has a blood pressure (BP) of 70/40 mm Hg, pulse of 148 beats per minute (bpm), and Glasgow Coma Scale score of 6 (scores lower than 8 indicate severe brain injury), and there is negligible urine output. His airway is secure and intravenous (IV) access is obtained. Two liters of warm crystalloid solution are given; repeated vital signs reveal the same BP and a pulse of 142 bpm. What is the best next step?

Explanation
This patient has an anteroposterior compression pelvic fracture associated with shock. In patients with closed pelvic fractures and hypotension, mortality rises to approximately 1 in 4 (10%-42%) and hemorrhage is the major reversible contributing factor. Initial management of a major pelvic disruption associated with hemorrhage requires hemorrhage control and rapid fluid resuscitation. A pelvic binder should be placed to reduce pelvic volume. The patient has signs and symptoms of class IV hemorrhage, which include marked tachycardia exceeding 140, a significant decrease in BP, and a very narrow pulse pressure. Urinary output is negligible, and mental status is markedly depressed. The skin is cold and pale. The degree of exsanguination with class IV hemorrhage is immediately life threatening, and rapid transfusion and immediate surgical intervention are necessary. Nonresponse to fluid administration indicates persistent blood loss. Blood preparation should be emergency blood release. Type and cross-match of blood can be used for additional resuscitation in transient responders.
RECOMMENDED READINGS
Olson SA, Reilly MC, eds. Acetabular and Pelvic Fractures. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:15-42.
Advanced Trauma Life Support for Doctors, ed 8. Chicago, IL, American College of Surgeons, 2008.
RESPONSES FOR QUESTIONS 71 THROUGH 74
- Retrograde intramedullary (IM) nailing
- Open reduction and internal fixation (ORIF) with screws alone
- Locking condylar plate
- Circular external fixation
- Lateral and medial plates
Which treatment option listed is best for each patient described?
71A

B
C
D
A 54-year-old healthy man with the condition seen in Figures 71a through 71d
- Retrograde intramedullary (IM) nailing
- Open reduction and internal fixation (ORIF) with screws alone
- Locking condylar plate
- Circular external fixation
- Lateral and medial plates
Question 87
In a pilon fracture, the Chaput fragment typically maintains soft tissue attachment via which of the following structures?

Explanation
Question 88
-Figures a through c are the MRI scans of a 21-year-old woman with recurrent shoulder instability and pain after an open anterior stabilization procedure. Positive belly-press test findings were positive.At surgery she was found to have an irreparable tear of the tendon injury identified preoperatively. The procedure to address the dynamic stabilizer deficit places which nerve at most risk?
Explanation
Question 89
Hybrid locked plating for distal femoral fractures refers to the use of nonlocked and locked screws in the same construct. The advantages of using the combination of nonlocked and locked screws in both the proximal and distal fragments are that nonlocked screws
Explanation
Question 90
A 10-year-old girl reports activity-related bilateral arm pain. Examination reveals no soft-tissue masses in either arm, and she has full painless range of motion in both shoulders and elbows. The radiograph and bone scan are shown in Figures 20a and 20b, and biopsy specimens are shown in Figures 20c and 20d. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 118-119.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 197.
Question 91
A 30-year-old man has had severe knee pain and swelling for 1 week. He reports he previously had acromioclavicular joint pain that disappeared. He denies any fever. Aspiration of a cloudy fluid from the knee reveals a WBC count of greater than 50,000 with 90% polymorphonucleocytes. While awaiting culture results, what is the most appropriate action?
Explanation
Question 92
-A collegiate offensive football lineman has decreased bench-press strength and shoulder pain as off-season workouts begin. Examination revealed no atrophy, and deltoid and rotator cuff strength testing findings were normal. Translational testing was difficult to achieve because of his large size.Apprehension and relocation test findings were negative. An O’Brien’s active compression test result was negative. Jerk testing was positive on the affected side. Which diagnosis is most likely revealed on an MRI arthrogram?
Explanation
Question 93
- A 45-year-old man sustains the shoulder injury shown in the radiographs in Figure 55a and 55b and the CT scan in Figures 55c and 55d. Management should consist of
Explanation
Question 94
You are interested in learning a new technique for minimally invasive total knee arthroplasty. The Keyhole Genuflex system seems appealing to you because the instrumentation comes with wireless controls. What is an acceptable arrangement to learn more about this system?
Explanation
Question 95
Which of the following studies best increases the ability to diagnose femoral neck fractures in patients with femoral shaft fractures?
Explanation
REFERENCES: Tornetta P III, Kain MS, Creevy WR: Diagnosis of femoral neck fractures in patients with a femoral shaft fracture: Improvement with a standard protocol. J Bone Joint Surg Am 2007;89:39-43.
Yang KH, Han DY, Park HW, et al: Fracture of the ipsilateral neck of the femur in shaft nailing: The role of CT in diagnosis. J Bone Joint Surg Br 1998;80:673-678.
Question 96
Local administration of recombinant bone morphogenetic protein-2 (rhBMP-2) to patients with type III-A and III-B open tibial shaft fractures at the time of initial surgery has shown all of the following when compared to standard treatment EXCEPT:

Explanation
Question 97
A patient has multidirectional instability of the shoulder that has not responded to nonsurgical management. Successful surgical treatment will most likely include which of the following? Review Topic
Explanation
instability treated surgically following failure to respond to nonsurgical management has been shown to be associated with classic Bankart lesions, Hill-Sachs defects, glenoid chondral lesions, and even SLAP lesions (Werner). However, these lesions were seen in a lower percentage than that found for unidirectional anterior dislocations. Likewise, these lesions do not appear to be significant in influencing treatment in the majority of patients.
Question 98
A 63-year-old woman with a history of poliomyelitis has a fixed 30-degree equinus contracture of the ankle, rigid hindfoot valgus, and normal knee strength and stability. She reports persistent pain and has had several medial forefoot ulcerations despite a program of stretching, bracing, and custom footwear. What is the next most appropriate step in management?
Explanation
REFERENCES: Perry J, Fontaine JD, Mulroy S: Findings in post-poliomyelitis syndrome: Weakness of muscles of the calf as a source of late pain and fatigue of muscles of the thigh after poliomyelitis. J Bone Joint Surg Am 1995;77:1148-1153.
Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 99
The posterior circumflex artery provides blood supply to what portion of the proximal humerus?
Explanation
REFERENCES: Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 267-274.
Gerber C, Schneeberger AG, Vinh TS: The arterial vascularization of the humeral head:
An anatomical study. J Bone Joint Surg Am 1990;72:1486-1494.
Question 100
A 55-year-old man sustained an elbow dislocation in a fall. Postreduction radiographs are shown in Figures 40a and 40b. What is the best course of management?
Explanation
REFERENCES: Hildebrand KA, Patterson SD, King GJ: Acute elbow dislocations: Simple and complex. Orthop Clin North Am 1999;30:63-79.
O’Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. Instr Course Lect
2001;50:89-102.
