Orthopedic Surgery Board Review MCQs: Trauma, Spine & Hip | Part 175

Key Takeaway
This page presents an interactive Orthopedic Surgery Board Review quiz, Part 175. It features 100 high-yield, verified MCQs, meticulously formatted like OITE and AAOS board exams. Tailored for orthopedic surgeons and residents, this resource aids rigorous board certification preparation via comprehensive study and exam modes.
About This Board Review Set
This is Part 175 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 175
This module focuses heavily on: Deformity, Foot, Fracture, Hip, Infection, Osteoporosis, Shoulder, Tendon, Trauma.
Sample Questions from This Set
Sample Question 1: A 35-year-old man who is left-hand dominant has pain and swelling around his left index metacarpal phalangeal (MCP) joint following a motor vehicle accident 2 months ago. Radiographs reveal no fractures. He has point tenderness over the rad...
Sample Question 2: A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and ...
Sample Question 3: Ayear-oldwomanwithahistoryofosteoporosisisinvolvedinahigh-speedmotorvehicleaccident,resultinginlefthippainanddeformity.TheinitialradiographfromthetraumabayisshowninPostreductionCTisshownin2throughWhatisthemostappropriatedefinitivesurgical t...
Sample Question 4: Which method of flexor tendon repair that necessitates excursion through the A2 pulley allows for the most thorough assessment of tendon gliding?...
Sample Question 5: A 19-year-old college football player reports persistent weakness, tingling, and numbness of both upper extremities at half time. He states that these symptoms initially occurred after tackling an opposing player with his head early in the ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 35-year-old man who is left-hand dominant has pain and swelling around his left index metacarpal phalangeal (MCP) joint following a motor vehicle accident 2 months ago. Radiographs reveal no fractures. He has point tenderness over the radial side of the MCP joint and increased laxity with ulnarly applied stress. He has failed conservative treatment including 5 weeks of immobilization. If the patient elects to live with this condition and not have surgery, what would be the most common outcome?
Explanation
The thumb MCP ulnar collateral ligament (UCL) and index MCP radial collateral ligament (RCL) are the primary stabilizers to pinch. Secondary stabilizers include the volar plate, dorsal capsule, and accessory collateral ligaments. With insufficiency of either the thumb MCP UCL or the index MCP RCL, pinch strength will be severely weakened. The other options listed are unlikely to occur with this particular injury.
Question 2
A 16-year-old girl was involved in a motorcycle accident that resulted in a significant right tibial fracture with soft-tissue loss over the distal 4 cm of the anterior medial tibia. The patient has had two irrigations and debridements and recently had an intramedullary nail placed for the skeletal injury. Vacuum-assisted closure (VAC) has been used to cover the defect since the injury. The risk of infection developing in the tibia is
Explanation
REFERENCES: Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
Dedmond BT, Kortesis B, Punger K, et al: The use of negative-pressure wound therapy (NPWT) in the temporary treatment of soft-tissue injuries associated with high-energy open tibia shaft fractures. J Orthop Trauma 2007;21:11-17.
Herscovici D Jr, Sanders RW, Scaduto JM, et al: Vacuum-assisted wound closure (VAC therapy) for the management of patients with high-energy soft tissue injuries. J Orthop Trauma 2003;17:683-688.
Question 3
A year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Postreduction CT is shown in 2 through What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 4
Which method of flexor tendon repair that necessitates excursion through the A2 pulley allows for the most thorough assessment of tendon gliding?
Explanation
Wide-awake repair under only local anesthesia, regardless of the technique, allows direct inspection of the tendon repair and active excursion. Regional anesthesia and Bier block anesthesia do not allow active motion (Bier block necessitates continued use of a tourniquet, which limits muscle function). The A2
pulley should be preserved, especially the distal 50%, to maintain tendon function. All of the listed techniques for suture repair are acceptable options.
Question 5
A 19-year-old college football player reports persistent weakness, tingling, and numbness of both upper extremities at half time. He states that these symptoms initially occurred after tackling an opposing player with his head early in the game. History reveals that he has had “burners” in the past that typically resolved within 15 to 30 minutes. Examination reveals pain-free cervical motion, weakness to shoulder abduction testing bilaterally, normal upper extremity reflexes, and decreased sensation over both shoulders and the upper arms. Appropriate initial management should consist of
Explanation
REFERENCES: Torg JS, Sennett B, Pavlov H, et al: Spear tackler’s spine: An entity precluding participation in tackle football and collision activities that expose the cervical spine to axial energy inputs. Am J Sports Med 1993;21:640-649.
Torg JS: Cervical spinal stenosis with cord neurapraxia and transient quadriplegia. Sports Med 1995;20:429-434.
Torg JS, Guille JT, Jaffe S: Injuries to the cervical spine in American football players. J Bone Joint Surg Am 2002;84:112-122.
Question 6
A 32-year-old male sustains a posterior wall acetabulum fracture as the result of a high-speed motor vehicle collision. Improved patient-reported outcomes after surgical treatment are associated with which of the following variables?

Explanation
The reference by Borrelli et al evaluated muscle strength and outcomes after acetabular surgery via an anterior approach. They report that hip extension strength was affected least(6%), whereas abduction, adduction, and flexion strength was affected to a greater degree. They note that hip muscle strength after operative treatment of a displaced acetabular fracture directly influences patient outcome.
The reference by Engsberg et al is a review of patients that underwent ORIF of acetabular fractures through anterior or posterior approaches. They report that maximizing hip muscle strength may improve gait, and improvement in hip muscle strength and gait is likely to improve functional outcome. Worsening functional outcomes were correlated with decreased gait kinematics and stride length.
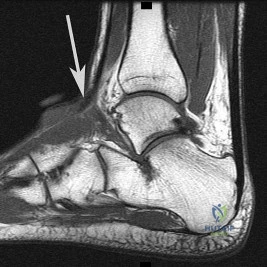
Question 7
The radiograph seen in Figure 67 reveals an ankle fracture in a 65-year-old woman who slipped on the ice. She has a history of diabetes mellitus for the past 7 years and reports that she maintains fair control of her diabetes; her last HgbA1c was 8%. The patient is a community ambulatory who lives independently. Examination reveals she has absent sensation with the 5.07 monofilament. When determining management, the physician must consider which of the following?

Explanation
Question 8
A patient sustained a puncture wound to the plantar aspect of his foot. He was wearing shoes and socks at the time of the injury. Systemic antibiotic administration with specific coverage for which bacterial species (in addition to Staphylococcus aureus) should be instituted?
Explanation
Puncture wounds sustained through a shoe and sock increase risk for Pseudomonas infection. Clostridium are associated with soil-contaminated wounds. Mycobacterium marinum is associated with injuries sustained within water.
RECOMMENDED READINGS
DeCoster TA, Miller RA. Management of Traumatic Foot Wounds. J Am Acad Orthop Surg. 1994 Jul;2(4):226-230. PubMed PMID: 10709013. View Abstract at PubMed
Raikin SM. Common infections of the foot. In: Richardson EG, ed. Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2004:199-205.
Question 9
Figures 28a through 28c show the MRI scans of a 30-year-old woman who weighs 290 lb and has low back and left leg pain. She also reports frequent urinary dribbling, which her gynecologist has advised her may be related to obesity. Examination will most likely reveal
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Appleton, WI, Century-Crofts, 1976.
Hollinshead WH (ed): Anatomy for Surgeons: The Back and the Limbs, ed 3. Philadelphia, PA, Harper & Rowe, 1982.
Question 10
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in Review Topic
Explanation
Question 11
When performing a Kocher approach to the radial head for open reduction internal fixation the forearm is held in pronation. What structure is this maneuver attempting to protect?

Explanation
Question 12
Using methylmethacrylate to fill a biopsy hole in the diaphysis of a femur theoretically achieves what purpose?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Biopsy: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 55-65.
Simon MA: Biopsy of musculoskeletal tumors. J Bone Joint Surg Am 1982;64:1253-1257.
Question 13
The mother of a 2-year-old boy reports that he had pain in the right hip all night and refuses to walk on the leg this morning. He is afebrile. Examination reveals pain on hip extension and adduction, but he is able to internally and externally rotate the hip approximately 20 degrees in each direction without pain. Laboratory studies reveal a WBC count of 7,400/mm 3 , with 62% polymorphonuclear neutrophil leukocytes. The AP radiograph shown in Figure 15 reveals a left teardrop distance of 8 mm, while the right side measures 10 mm. Which of the following diagnostic studies will best help confirm the diagnosis?
Explanation
REFERENCE: Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990, pp 1415-1435.
Question 14
Within the intervertebral disk, aggrecan is primarily responsible for: Review Topic
Explanation
Aggrecan, the most abundant proteoglycan within the intervertebral disk, is a hydrophillic molecule which helps attract and maintain water within the disc. This is important to maintain compressive strength. Early in life aggrecan has a high percentage of chondroitin sulfate chains. With aging this gradually changes to higher percentage of keratin sulfate. Other proteoglycans include decorin and versican. Decorin is believed to regulate cell cycles and influence fibrillogensis. Versican is a large extra-cellular matrix proteoglycan involved in cell adhesion and migration.
Roughley et al. provide a review of biologic changes within the intervertebral disc during development, maturation, and degeneration. They note that aggrecan works to maintain water content within the disc, thus improving its compressive strength. Aggrecan content decreases with age leading to a loss of compressive strength.
Illustration A shows the structure of aggrecan.
Incorrect answers:
Question 15
A 34-year-old man presents to clinic with 4 months of right elbow pain. He began going to the gym and playing squash about 3 months ago. On exam, he is tender over the lateral aspect of the elbow and has pain with resisted wrist extension. Which of the following choices lists the correct compartment of the muscle typically involved in this disease and then lists its antagonist muscle? Review Topic
Explanation
Lateral epicondylitis is an overuse injury, typically secondary to repetitive pronation and supination motion in extension, that leads to inflammation of the ECRB origin at the elbow. Histological analysis typically shows vascular hyperplasia and disorganized collagen. Clinically, patients will have pain over the lateral elbow exacerbated by resisted wrist extension. ECRB, the most commonly involved muscle origin, is innervated by the deep branch of the radial nerve and inserts on the base of the 3rd metacarpal. As it is radial wrist extensor, its antagonist is the ulnar sided wrist flexor.
Brummel et al. reviewed the clinical presentation and management options for lateral epicondylitis. They report acute symptoms in younger patients and chronic symptoms in older patients. NSAIDs, extensor stretching and activity modification are the mainstay of nonsurgical treatment.
Bunata et al. studies 85 cadavar elbows to determine anatomic factors contributing to tennis elbow. They found that the ECRB undersurface rubs against the lateral capitellium in elbow extension leading to tendinosis.
Illustration A is cross-sectional diagram of the forearm with muscle bellies labeled. Notice the location of ECRB in the mobile wad. Illustration B is a coronal T2 MRI showing fluid signal and undersurface tearing near the extensor origin as can be seen in lateral epicondylitis.
Incorrect Answers:
1-4: The ECRB is in the mobile wad and its antagonist is flexor carpi ulnaris. All other answers are incorrect.
Question 16
A 45-year-old man reports that he awoke 2 weeks ago with severe pain in his right arm. Examination reveals weakness in the biceps, brachialis, and wrist extensors. There is decreased sensation in the thumb and index finger and a diminished brachioradialis reflex. Assuming this patient has a posterolateral herniated nucleus pulposus, what level is involved?
Explanation
REFERENCES: Standaert CJ: The patient history and physical examination: Cervical, thoracic and lumbar, in Herkowitz HN, Garfin SR, Eismont FJ, et al (eds): Rothman-Simeone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, vol 1, pp 171-186.
Bates B: A Guide to Physical Examination and History Taking, ed 5. Philadelphia, PA,
JB Lippincott, 1991.
Question 17
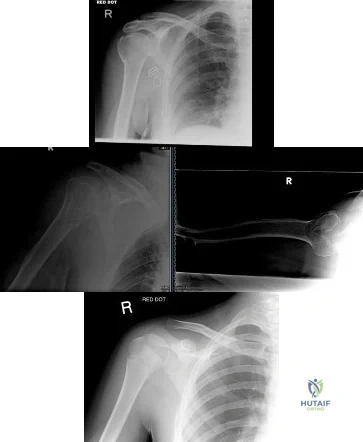
A 72-year-old woman who was doing well after undergoing total shoulder arthroplasty for arthritis 4 months ago is suddenly unable to elevate her arm. Examination reveals 70 degrees of external rotation compared with 45 degrees on the uninvolved side, and she is unable to lift her hand off her lower back. Radiographs are shown in Figures 43a through 43c. Treatment should consist of
Explanation
REFERENCES: Moeckel BH, Altchek DW, Warren RF, Wickiewicz TL, Dines DM: Instability of the shoulder after arthroplasty. J Bone Joint Surg Am 1993;75:492-497.
Gerber C, Hersche O, Farron A: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 18
A 56-year-old man who underwent a left total hip arthroplasty 8 years ago is seen following a fall from a standing height. A radiograph obtained at 2 years postoperatively is shown in Figure 55a and a current radiograph obtained in the emergency department is shown in Figure 55b. On further questioning, he reports pain in this thigh for the past 3 years that has been increasing in intensity. Appropriate management at this time includes which of the following?
Explanation
REFERENCES: Masri BA, Meek RM, Duncan CP: Periprosthetic fractures evaluation and treatment. Clin Orthop Relat Res 2004;420:80-95.
Springer BD, Berry DJ, Lewallen DB: Treatment of periprosthetic femoral fractures following total hip
arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162. Question 56
A 62-year-old woman who underwent a primary total knee arthroplasty under a combined spinal-epidural anesthetic presents 5 hours postoperatively with severe pain in the extremity that is unresponsive to narcotic pain medication. A tourniquet was used during the procedure. On examination, the patient is unable to dorsiflex or plantar flex the foot and the pulses appear to be asymmetric. What is the next most appropriate step in management?
Discontinuation of the epidural and serial neurologic exams
Loosening of the surgical bandages and elevation of the extremity
MRI of the spine to evaluate for an epidural hematoma
Return to the operating room for angiography and vascular bypass
Return to the operating room for angiography, vascular bypass, and four-compartment fasciotomy PREFERRED RESPONSE: 5
DISCUSSION: The patient has clinical evidence of vascular injury and compartment syndrome. An emergent
vascular consult and a return to the operating room for an angiogram and revascularization are needed. In these situations, thrombectomy alone is often not sufficient and a bypass is typically required. A four-compartment fasciotomy should be done following revascularization of the extremity.
REFERENCES: Calligaro KD, Dougherty MJ, Ryan S, et al: Acute arterial complications associated with total hip and knee arthroplasty. J Vase Surg 2003;38:1170-1177.
Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001;9:253-257.
Ninomiya JT, Dean JC, Goldberg VM: Injury to the popliteal artery and its anatomic location in total knee
arthroplasty. J Arthroplasty 1999;14:803-809.
Question 19
Figures 51a through 51c show the radiographs of a 7-year-old soccer player who reports a gradual onset of midfoot pain that began shortly after the start of soccer season. He states that the pain is worse with activity and is partially alleviated by rest. Examination reveals soft-tissue swelling, and tenderness and warmth in the region of the talonavicular and navicular cunieform joints. Management should consist of
Explanation
REFERENCE: Lutter LD: Sports-related injuries, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992.
Question 20
In children between the ages of 4 and 8 years, the major blood supply to the femoral head comes from the
Explanation
REFERENCES: Hughes LO, Beaty JH: Fractures of the head and neck of the femur in children. J Bone Joint Surg Am 1994;76:283-292.
Ogden JA: Changing patterns of proximal femoral vascularity. J Bone Joint Surg Am 1974;56:941-950.
Question 21
Presence of diabetes-induced peripheral neuropathy has been shown to be an independent risk factor for postoperative complications of which of the following injuries?

Explanation
Question 22
A 59-year-old construction worker who is right-hand dominant has had right shoulder pain for the past 9 months with no history of injury. Nonsurgical management consisting of two cortisone injections, physical therapy for 3 months, and nonsteroidal anti-inflammatory drugs has failed to provide lasting relief. Examination reveals tenderness over the acromioclavicular (AC) joint and over the subacromial bursa. He has positive Neer and Hawkins impingement signs and AC joint pain with adduction of the shoulder. Radiographs are shown in Figures 36a and 36b. An MRI scan reveals an intact rotator cuff. Management should now consist of
Explanation
REFERENCE: Peterson CA, Altchek DW, Warren RF: Shoulder arthroscopy, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 290-335.
Question 23
Which structure is the primary stabilizer of the lesser metatarsophalangeal (MTP) joint?
Explanation
Synovitis of the second MTP occurs in association with instability of the joint. This can be idiopathic or secondary to an external deforming force (such as a hallux valgus or shoe wear causing a claw toe). The primary stabilizer of the MTP joint for translation in the vertical plane is the plantar plate. The flexor digitorum brevis flexes the MTP joint, and the flexor digitorum longus flexes
all joints of the toe. The collateral ligaments are primary stabilizers in the transverse plane and secondary stabilizers in the sagittal plane.
RECOMMENDED READINGS
Deland JT, Sung IH. The medial crosssover toe: a cadaveric dissection. Foot Ankle Int. 2000 May;21(5):375-8. PubMed PMID: 10830654.View Abstract at PubMed
Suero EM, Meyers KN, Bohne WH. Stability of the metatarsophalangeal joint of the lesser toes: a cadaveric study. J Orthop Res. 2012 Dec;30(12):1995-8. doi: 10.1002/jor.22173. Epub 2012 Jun 13. PubMed PMID: 22696467. View Abstract at PubMed
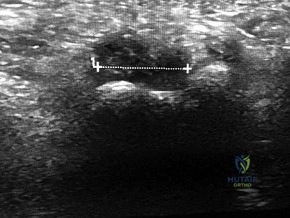
CLINICAL SITUATION FOR QUESTIONS 91 THROUGH 95
Figure 91a is the sagittal plane ultrasound of the second web space of a 48-year-old woman who has noted burning pain in the ball of her right foot for 2 years. The pain intermittently radiates into her second and the third toes. Figure 91b shows the surgical procedure and Figure 91c is the pathologic specimen.
A
B

C

Question 24
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
REFERENCES: Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454.
Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Noyes FR, Butler DL, Grood ES, et al: Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am 1984;66:344-352.
Question 25
A large circumferential proximal femoral allograft is to be used in the reconstruction of a failed femoral component in a total hip arthroplasty. To enhance fixation of the graft to the implant, which of the following strategies should be used?
Explanation
REFERENCES: Allan DG, Lavoie GJ, Rudan JF, et al: The use of allograft bone in revision total hip arthroplasty, in Friedlaender GE, Goldberg VM (eds): Bone and Cartilage Allografts: Biology and Clinical Applications. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1991, pp 263-264.
Gross AE, Lavoie MV, McDermott P, Marks P: The use of allograft bone in revision of total hip arthroplasty. Clin Orthop 1985;197:115-122.
Head WC, Berklacich FM, Malinin TI, Emerson RH Jr: Proximal femoral allografts in revision total hip arthroplasty. Clin Orthop 1987;225:22-36.
Question 26
A diskectomy is performed in which the disk space is not aggressively debrided. When compared to techniques that involve aggressive debridement of the disk space, this results in
Explanation
This patient has disk herniation at the left L5-S1 level. This will generally affect the traversing S1 nerve. The S1 dermatome is on the lateral aspect and sole of the foot.
Surgical treatment generally involves a diskectomy with removal of the herniated fragment. This can be performed via a conventional open approach or minimally invasive endoscopic technique. Several recent meta-analyses have demonstrated equivalent outcomes with regard to leg pain and clinical outcomes. Although minimally invasive techniques have been associated with an increased rate of dural tear, the overall complication rate between the 2 techniques is not significantly different. Several studies have demonstrated a substantial learning curve associated with minimally invasive techniques, and the rate of complications decreases significantly with surgeon experience.
When performing a diskectomy, the herniated fragment alone can be removed (sequestrectomy) or some of the disk that remains in the disk space can be removed (complete diskectomy). Studies have shown no change in surgical time, blood loss, length of stay, or surgical complications when performing a sequestrectomy (compared to a more complete diskectomy). A sequestrectomy is associated with a higher rate of recurrent disk herniation at the surgical level.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis.
Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183. View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 27
A 2-year-old boy has complete absence of the sacrum and lower lumbar spine. What is the most likely long-term outcome if no spinal pelvic stabilization is performed?
Explanation
REFERENCES: Tachdjian MO: The spine: Congenital absence of the sacrum and lumbosacral vertebrae (lumbosacral agenesis), in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 3, p 2228.
Renshaw TS: Sacral agenesis: A classification and review of twenty-three cases. J Bone Joint Surg Am 1978;60:373-383.
Question 28
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?
Explanation
REFERENCES: Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby Year Book, 1995, p 688.
Question 29
A research study is initiated on 500 patients undergoing total hip arthroplasty. The patients are followed and outcome is assessed according to body mass index (BMI). The effects of BMI on outcome should be reported as which of the following?
Explanation
Question 30
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What factor most strongly correlates with the development of compartment syndrome after this injury?
Explanation
REFERENCES: Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
Question 31
Figure 31 is the sagittal MR image of a 30-year-old man with a clear-cell sarcoma of the foot. There is no evidence of disease elsewhere after standard staging of a soft-tissue sarcoma.
Explanation
For patients with rapidly enlarging painless masses, particularly those that are either large or deep, the diagnosis of a soft-tissue sarcoma should be entertained. Masses exceeding 5 cm in largest dimension that are subfascial and heterogenous on MRI are concerning. MRI with and without contrast is the preferred imaging modality for evaluation of soft-tissue sarcomas because it can delineate location of the lesion, involvement of neurovascular structures, intra-articular involvement, and underlying signal alteration in the osseous structures. Most patients can relate the onset of their symptoms to a traumatic event, and the interpretation of an MRI may include a hematoma. Ultrasound is more commonly used to confirm the clinical impression of a cyst and to distinguish cystic from solid masses.
A core needle biopsy can easily be performed in an outpatient setting or with image guidance to aid in the diagnosis. Core needle biopsies preserve the architectural relationship of cells, which is important in the diagnosis of mesenchymal lesions. A core needle biopsy is appropriate for soft-tissue lesions and osseous lesions and should be performed in a multidisciplinary setting with a surgeon performing the resection so unnecessary compartmental contamination is not introduced into the needle tract.
A fine-needle aspiration allows cytologic but not histologic analysis and generally is not favored for the diagnosis of a sarcoma. If an open biopsy is performed, the incision must be oriented in line with the long axis of the extremity to minimize contamination of surrounding structures. Meticulous hemostasis and closure of the tumor pseudocapsule must be achieved to minimize local tissue contamination. An open biopsy is commonly used if an initial needle biopsy is nondiagnostic. Transverse biopsy incisions should not be used.
Presurgical radiation for sarcomas is advantageous to decrease the field of radiation and overall radiation dose, but a significant postsurgical wound-healing complication rate (up to 35%) is associated with presurgical radiation therapy.
Staging of sarcomas is important to help predict prognosis. Not all sarcomas are reliably positive on a PET scan, so the preferred staging studies are CT scan of the chest and whole-body bone scan. Hematogenous spread of sarcomas is the most common route of metastatic disease, which speaks to the value of chest CT scans. Clear-cell sarcomas (in addition to synovial sarcoma, angiosarcoma, epithelioid sarcoma, and rhabdomyosarcoma) tend to involve lymphatic nodal metastatic disease, so sentinel node biopsy is considered when assessing these tumors. Evidence supports efficacy of sentinel node biopsy for clear-cell sarcomas in particular.
RECOMMENDED READINGS
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, eds. AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer; 2010.
Arbeit JM, Hilaris BS, Brennan MF. Wound complications in the multimodality treatment of extremity and superficial truncal sarcomas. J Clin Oncol. 1987 Mar;5(3):480-8.View Abstract at PubMed
Luce EA. The irradiated wound. Surg Clin North Am. 1984 Aug;64(4):821-9. PubMed PMID: 6591499. View Abstract at PubMed
Cheng EY, Dusenbery KE, Winters MR, Thompson RC. Soft tissue sarcomas: preoperative versus postoperative radiotherapy. J Surg Oncol. 1996 Feb;61(2):90-9.View Abstract at PubMed
Mankin HJ, Lange TA, Spanier SS. The hazards of biopsy in patients with malignant primary bone and soft-tissue tumors. J Bone Joint Surg Am. 1982 Oct;64(8):1121-7. View Abstract at PubMed
Singer S, Nielsen T, Antonescu CR. Molecular biology of soft tissue sarcoma. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:1522-1532.
Singer S, Maki RG, O'Sullivan B. Soft tissue sarcoma. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:1533-1577.
Malawer MM, Helman LJ, O'Sullivan B. Sarcomas of bone. In: DeVita VT Jr, Lawrence TS, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011:1578-1609.
O'Sullivan B, Davis AM, Turcotte R, Bell R, Catton C, Chabot P, Wunder J, Kandel R, Goddard K, Sadura A, Pater J, Zee B. Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: a randomised trial. Lancet. 2002 Jun 29;359(9325):2235-41. View Abstract at PubMed
Andreou D, Boldt H, Werner M, Hamann C, Pink D, Tunn PU. Sentinel node biopsy in soft tissue sarcoma subtypes with a high propensity for regional lymphatic spread--results of a large prospective trial. Ann Oncol. 2013 May;24(5):1400-5. doi: 10.1093/annonc/mds650. Epub 2013 Jan 31. PubMed PMID: 23372051. View Abstract at PubMed
Question 32
Figure 16 shows an axial MRI scan through the knee joint. What structure is identified by the arrow?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 675-699.
Fitzgerald SW, Remer EM, Friedman H, Rogers LF, Hendrix RW, Schafer MF: MR evaluation of the anterior cruciate ligament: Value of supplementing sagittal images with coronal and axial images. Am J Roentgenol 1993;160:1233-1237.
Question 33
A 10-month-old infant has a deformity of the right foot. Radiographs, including simulated weight-bearing AP and lateral views and a maximum plantar flexion lateral view, are shown in Figures 57a through 57c. Initial management of the foot should consist of Review Topic

Explanation
Question 34
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of
Explanation
REFERENCES: Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Weber TG, Manoli A II: Compartment syndromes of the foot. Foot Ankle Clin 1999;4:473-486.
Question 35
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow. The athlete undergoes repair of the injury, and postsurgical radiographs are shown in Figures 1 and 2. At his first postsurgical visit, he reports no pain but describes weakness in his hand and decreased sensation over his lateral forearm. Upon examination, he has decreased 2-point discrimination over the lateral forearm and an inability to actively extend his thumb and fingers at the metacarpophalangeal joints. He can extend at the finger interphalangeal joints. He can extend his wrist weakly, and it deviates radially as he extends. His distal sensation is intact. Considering his examination findings, which two nerves are injured?

Explanation
elbow) while still retaining elbow flexion (albeit weakened) because of the other elbow flexors (brachioradialis and brachialis). Consequently, treatment should be anatomic repair of the distal biceps insertion, which can be performed with a 2-incision or 1-incision technique. Although all of the listed complications have been reported with these techniques, LABC neuropraxia is by far the most common. Radiographs show that this athlete’s injury was repaired using a 1-incision technique with a cortical fixation device and a radial bone tunnel. This technique has gained favor because of its decreased incidence of heterotopic ossification and radioulnar synostosis compared with the 2-incision technique. The most troubling complication for most surgeons is the development of a posterior interosseous nerve (PIN) palsy, which this patient clearly demonstrates in addition to the more common LABCN upon postsurgical examination. Because the LABCN injury is typically a neuropraxia from retraction, a period of observation is indicated. PIN injury can result from excessive traction during surgical exposure or from entrapment by the fixation button. Considering the anatomy of the PIN, successful recovery of the nerve typically progresses based on the distance from the origin of the nerve to the muscle indicated. The extensor indicis proprius (EIP) muscle is the most distal muscle innervated and can be expected to recover last. First to return would be the EDC
followed by the ECU, EDQ, and, finally, the EIP.
Question 36
What is the most common site of nerve compression in radial tunnel syndrome?
Explanation
A. Quadrigia
B. Intrinsic tightness
C. Lumbrical plus deformity
D. Disruption of the tendon repai
Question 37
03 A 37 year-old woman with thoracic back pain has had hemoptysis and dyspnea for the past month. A thoracic spine radiograph shows a compression fracture of T-9 and a mass in the right lung. What is the best course of action?
Explanation

Here is an algorithm from OKU 6 Tumors of the Spine pp 723-736

This question gives you the history, skips right over physical exam and goes into plain films. With this patient’s history of hemoptysis and dyspnea and a lung mass, the next steps in this patients work-up would include the competion of initial work-up, metastatic work-up, then pre-operative planning. Goals of treatment are to 1) protect or restore neurologic function, 2) control pain,

Question 38
You perform an ACL reconstruction with bone-patella tendon-bone (BTB) autograft and are explaining the postoperative rehabilitation protocol to your patient. Which of the following is associated with increased quadriceps volume and improved quadriceps strength at 1 year without a higher risk of knee instability? Review Topic
Explanation
Proper rehabilitation following ACL reconstruction is vital to a successful outcome. The cornerstone of ACL rehabilitation is range of motion, strengthening and functional exercises without risk of destabilizing the knee. There are a variety of rehabilitation protocols and recently an effort has been made to standardize the approach to postoperative ACL care. An accelerated protocol starting at 3 weeks postoperatively has been deemed safe and may enhance the speed and safety with which an athlete returns to play.
Kruse et al completed a meta-analysis of 29 Level I and II studies focused on the ACL rehabilitation process. The authors concluded that immediate postoperative weightbearing and knee range of motion 0-90 is safe. Early eccentric strengthening appears to accelerate and improve strength gains at 1 year as compared to delayed eccentric strengthening. Home-based rehabilitation programs can be as effective as formal physical therapy. Postoperative bracing and CPM use is neither necessary nor beneficial.
Van Grinsven et al conducted a systematic review of ACL rehabilitation programs and physical therapy modalities to develop an evidence-based rehabilitation protocol. The authors demonstrated that an accelerated protocol without postoperative bracing focused on reduction of pain, swelling and inflammation and regaining range of motion, strength and neuromuscular control has significant advantages and does not lead to stability problems.
Gerber et al performed a randomized trial comparing two accelerated postoperative rehabilitation protocols – early eccentric (ECC) rehabilitation versus traditional (TRAD) rehabilitation starting at 3 weeks. There were no significant differences in knee pain, effusion or stability. However, quadriceps strength, hopping distance and activity level improved by a significantly greater amount in the ECC group versus the TRAD group at 26 weeks postoperatively. In a separate analysis of these patients, quadriceps and gluteus muscle cross-sectional area and volume in ECC patients were more than twice those in the TRAD group.
Illustration A depicts two eccentric ergometers that can be used in postoperative ACL rehabilitation.
Incorrect Responses:
another Answer
type of brace,
2:
There
duration is
of
bracing or no bracing at all.
no
advantage
to
CPM
use.
Question 39
Haversian canals are found in the center of an osteon in compact bone. They contain blood vessels and nerves.
Explanation
amputations have several options to optimize ambulation including solid, energy storing, and multi-axial prothesis.
Aaron et al. reviews the important considerations for patient specific prostheses and new developments on the horizon to maximize ambulation in prosthesis users.
Mesenchymal stem cells have the capacity to differentiate into all the following cell types EXCEPT?
Osteoclasts
Chondrocytes
Adipocytes
Osteoblasts
Fibroblasts
Mesenchymal stem cells are multipotent stem cells which retain the ability to self-renew and to form cells of the mesenchymal lineage. They can therefore form muscle, fat, tendon (made from fibroblasts), bone, cartilage, and the marrow stromal cells. Mesenchymal stem cells do not however form osteoclasts, which are formed from the monocyte lineage - from hematopoietic stem cells.
Caterson et al review the use of mesenchymal stem cells in tissue engineering and regeneration of musculoskeletal tissue.
A 60 year-old male was brought into the operating room for total hip replacement. Before making the incision, what precautionary procedure must be performed by the entire staff to minimize surgical error?
Mark the word "No" on the nonoperative extremities
Use intraoperative fluoroscopic imaging
Perform "timeout"
Have blood products ready in the operating room
Use the newest prosthesis
Surgical "timeout" is now part of the standard procedure which must be performed before starting surgery to minimize surgical error such as wrong site surgery.
Which of the following statements regarding articular cartilage is TRUE?
Cartilage is an isotropic material
Most of the water in articular cartilage exists in the deep layer next to the calcified cartilage
Cartilage only heals if the injury does not pass through the tidemark
Calcified cartilage is the only place that type IV collagen is found
Cartilage exhibits stress shielding of the solid matrix components
Cartilage exhibits significant stress shielding of the solid matrix components due to its high water content, the non-compressibility of water, and the structural organization of collagen and proteoglycans. Cartilage is composed of a permeable porous matrix and 65 to 80% of the total weight of articular cartilage is made up of water. A pressure gradient causes the water to flow through the porous-permeable solid matrix. Significant flow of fluid through the solid matrix requires high hydrodynamic pressures because of the low
permeability of the solid matrix.
The other answers are incorrect because cartilage is anisotropic, most of the water is located in the superficial layers, it only heals if the injury does pass through the tidemark, type X collagen is found in calcified cartilage and is thought to be involved in mineralization. Type IV collagen is found in the basal lamina.
A 38-year-old patient presents 6 months after intramedullary nailing of a distal third tibia fracture with symptoms consistent with complex regional pain syndrome. During the early stage of the disease he was treated with intermittent splinting, elevation and massage, contrast baths, and transcutaneous electrical nerve stimulation. Despite these modalities, he continues to have severe and debilitating symptoms. Which of the following treatment options is indicated as a second line of treatment?
Long leg cast immobilization for 3 months
Walking boot with non weight bearing for three months
Exchange nailing to stimulate healing response to the limb
Epidural spinal cord stimulator
Surgical sympathectomy of the affected limb
Complex regional pain syndrome is a chronic progressive disease of unknown etiology characterized by pain, swelling and skin changes. If nonoperative modalities fail, a surgical sympathectomy of the affected limb is indicated.
The first line of treatment is physical therapy including intermittent splinting, elevation and massage, contrast baths, and transcutaneous electrical nerve stimulation. Aggressive passive range-of-motion exercises should be avoided. If nonoperative modalites fail and symptoms remain severe, a surgical sympathectomy of the affected limb is indicated.
Keys to successful treatment include early clinical suspicion and treatment. Late CRPS is highly refractory to treatment and often results in permanent disability.
Two forms of Complex regional pain syndrome exist: 1) Reflex sympathetic dystrophy
- which does not demonstrate nerve lesions, and 2) Causalgia - which is associated with damage to peripheral nerves. Diagnostic criteria include:
Major criteria: intense and prolonged pain, swelling, stiffness, and discoloration (vasomotor disturbances).
Minor criteria: trophic changes, osseous demineralization, temperature changes, and palmar fibromatosis.
Tran et al present their systemic review of 41 RCTs of the research regarding treatment of CRPS. Their data suggest that only bisphosphonates offer clear medicinal benefits in the treatment of CRPS. Evidence regarding a beneficial effect of lumbar sympathetic blocks, gabapentin, and physical therapy is lacking. As such, these authors advocate for further study thru well-designed RCTs to better evaluate appropriate and effective treatment strategies.
You are planning an intramedullary nail to treat a geriatric patient with a peritrochanteric femur fracture. Which of the following preoperative considerations is correct regarding your implant?
The radius of curvature of an intramedullary nail is generally greater than the radius of curvature of the femur
Closed section nails have less stiffness than slotted nails
The medial/lateral nail starting point relative to the greater trochanter does not affect varus/valgus position in the fracture
The bending stiffness of your nail is proportional to the second power of the radius
Intramedullary nails allow for mostly direct intramembranous bone healing
The radius of curvature of an intramedullary nail is generally greater than the radius of curvature of the femur, which is why anterior distal femur
penetration is a known complication of intramedullary nailing procedures.
Egol et al. evaluated the radius of curvature of 948 femurs (474 matched pairs) and compared those data with current intramedullary nails. He found the average femoral anterior radius of curvature was 120 cm (± 36 cm)
whereas the radius of curvature of the intramedullary nails ranged from 186 to 300 cm.
The other answers are incorrect because closed section nails have more stiffness than slotted nails. The starting position on the greater trochanter greatly affects the post- operative varus/valgus of the fracture. Intramedullary nails allow for mostly indirect enchondral bone healing due to relative motion at the fracture site.
All of the following antibiotics function by interfering with protein synthesis by inhibiting ribosomes EXCEPT
gentamicin
tobramycin
vancomycin
erythromycin
linezolid
Gentamicin and tobramycin are aminoglycosides that function by inhibition of bacterial protein synthesis via irreversible binding to ribosomal subunits. Erythromycin functions by binding to the 50s subunit of the bacterial 70s rRNA complex and thereby inhibits protein synthesis. Linezolid binds to the 23s portion of the ribosomal subunit and inhibits protein synthesis. In contrast, Vancomycin acts by inhibiting proper cell wall synthesis and does not inhibit the ribosome.
The bending rigidity of the implant shown in Figure A is proportional to what power of the measured radius of the implant?
Question 40
A 69-year-old man has a painful slow-growing lesion of the distal phalanx of his thumb. History reveals that he has had chronic osteomyelitis of the thumb for the past 12 years. The radiograph and biopsy specimens are seen in Figures 9a through 9c. Treatment should consist of
Explanation
REFERENCES: Dell PC: Hand, in Simon MA, Springfield D (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 405-420.
McGrory JE, Pritchard DJ, Unni KK, Ilstrup D, Rowland CM: Malignant lesion arising in chronic osteomyelitis. Clin Orthop 1998;362:181-189.
Question 41
-Postsurgically, the patient recovers well and is fully rehabilitated. He demonstrates full motion with no instability or pain and is cleared to return to play 12 months after the surgery. He asks for your advice regarding use of a functional brace for playing basketball following his reconstruction. What is the most appropriate recommendation?
Explanation
The athlete most likely suffered an acute ACL rupture however the presence of a lipohemarthrosis is concerning for the possibility of an intraarticular fracture. Because of this, the patient should not be allowed full weight bearing until a fracture is ruled out with radiographs. Given the athlete’s inability to perform a straight leg raise, the extensor mechanism is not functioning and a telescoping knee brace locked in extension should be utilized. A neoprene knee sleeve does not have a role in the
treatment of this acute injury.The radiographs reveal a lateral avulsion fracture off of the proximal tibial epiphysis which is known as a Segond fracture. It is indicative of an ACL injury and the fracture fragment seen is the consequence of the lateral capsule injury sustained during the pivot-shift mechanism. There is no radiographic evidence of a medial tibial plateau fracture. A radiographic sign of a chronic MCL injury is known as a Pellegrini-Stieda lesion and this is seen as calcification of the femoral origin of the MCL. A radiographic sign of an acute LCL rupture would be an avulsion fracture of the tip of the fibula.The MRI shows kissing contusions of the posterolateral tibial plateau and the midpoint of the lateral femoral condyle. These “kissing lesions” are seen as a result of a pivot shift mechanism of injury and are diagnostic for an ACL rupture. The most common associated injury in an acute ACL rupture is a lateral meniscus tear. Medial meniscus tears are more common in chronic ACL injuries. PCL rupture and PLC injury are all associated injuries seen in acute ACL rupture; however, these are much less common than meniscal tears. The team physician has a role in encouraging, but
not demanding, the athlete to report the injury andtreatment to the scholarship school’s coaching staff. What the athlete decides to do is his decision; the physician would be violating the athlete’s HIPAA rights as well as their confidence by reporting it directly to the scholarship school. Clearly the physician should not discourage the athlete from reporting the injury. The athlete is 18 years old and, as such, the physician would need the athlete’s permission to discuss any medical issues with the family in keeping with HIPAA.
The athlete’s exam demonstrates incompetence of both bundles of the ACL as demonstrated by the loss of stability with anterior translation of the tibia (Lachman test) as well as with rotation (pivot shift). The external rotation stress with the knee in 30 degrees of flexion tests the competence of the posterolateral corner while rotation at 90 degrees of flexion tests the PCL. Since the athlete’s knee is stable to posterior drawer testing demonstrating an intact PCL and the external rotation at 30 degrees is equivalent to that at 90 degrees, the posterolateral corner in intact.
The ACL has two separate and distinct bundles, the AM and PL. Each bundle takes on tension at varying degrees of knee flexion and therefore each bundle is thought to have a varying contribution to the stability of the knee. The AM bundle takes on tension with the knee in flexion and the PL bundle is tight in extension. Neither bundle is isometric during knee range of motion. Both bundles have contributions to rotational stability of the knee throughout the range of motion.
The success of traditional trans-tibial single-bundle ACL reconstruction has recently been called into question given the demonstration of persistent rotational instability following reconstruction. The persistence of rotational instability in trans-tibial single bundle ACL reconstruction has been attributed to the location of the graft in a vertically malpositioned femoral tunnel. The goal of double-bundle ACL reconstruction is to more accurately reproduce the native ACL and provide grafts that contribute to anteroposterior stability as well as rotational stability by placing the grafts in more anatomic locations not central in the knee axis. There is an increased cost and surgical time associated with double-bundle reconstruction.
The use of functional braces following ACL reconstruction is a surgeon’s preference because there is no difference in retear rate with or without a brace. Some authors recommend brace use for one to two years following ACL reconstruction for all athletic activities, but this is not supported by the literature. No literature exists showing a higher rate of reinjury with a functional brace and off-the shelf and custom braces have been found to be equivalent leading those who advocate for braces to recommend off-theshelf braces given their significantly lower cost.
Question 42
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of
Explanation
REFERENCES: King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
Wang SY, Lomasney LM, Demos TC, Hopkinson WJ: Radiologic case study: Traumatic myositis ossificans. Orthopedics 1999;22:991-995, 1000.
Question 43
- A 40-year old man has limited, painful motion in dorsiflexion at the metatarsophalangeal (MTP) joint of the right great toe, despite nonsurgical treatment. Radiographs show dorsal and medial osteophytes and minimal narrowing of the articular space. Treatment should consist of
Explanation
Question 44
Figure 1 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. What is the main function of the structure delineated by the black asterisks?

Explanation
Question 45
Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?
Explanation
to 18 hours. This is greater than the 1 hour half-life of unfractionated heparin.
Low-molecular-weight heparin offers an advantage over unfractionated heparin by selectively targeting Factor Xa while having a lesser effect on circulating thrombin (Factor IIa). Circulating thrombin Factor IIa is needed for local hemostasis at the site of the surgical wound. Clinical studies have shown a reduction by one third in the incidence of thrombocytopenia with the use of low-molecular-weight heparin. Low-molecular-weight heparin has been shown to demonstrate similar clinical results compared to warfarin with respect to preventing thromboembolic disease after total hip arthroplasty and complications such as bleeding.
REFERENCES: Zimlich RH, Fulbright BM, Friedman RJ: Current status of anticoagulation therapy after total hip and total knee arthroplasty. J Am Acad Orthop Surg 1996;4:54-62.
Colwell CW Jr, Spiro TE, Trowbridge AA, et al: Use of enoxaparin, a low-molecular-weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Torholm C, Broeng L, Jorgensen PS, et al: Thromboprophylaxis by low-molecular-weight heparin in elective hip surgery: A placebo controlled study. J Bone Joint Surg Br 1991;73:434-438.
Question 46
A 23-year-old national team rower reports pain over the radial dorsum of the forearm that is made worse with flexion and extension of the wrist during competition. His primary physician initially diagnosed de Quervain’s tenosynovitis, and a subsequent corticosteroid injection into the first dorsal compartment at the wrist provided no relief. The patient continues to report pain and audible crepitus that is noted 5 cm proximal to the wrist joint, on the radial aspect. What structures are involved in the continued pathology?
Explanation
REFERENCES: Grundberg AB, Reagan DS: Pathologic anatomy of the forearm: Intersection syndrome. J Hand Surg Am 1985; 10:299-302.
Thorson E, Szabo RM: Common tendinitis problems in the hand and forearm. Orthop Clin North Am 1992;23:65-74.
Williams JG: Surgical management of traumatic non-infective tenosynovitis of the wrist extensors. J Bone Joint Surg Br 1977;59:408-410.
Wood MB, Dobyns JH: Sports-related extraarticular wrist syndromes. Clin Orthop Relat Res 1986;202:93-102.
Question 47
Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
Explanation
REFERENCES: Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Mazur JM, Schwartz E, Simon SR: Ankle arthrodesis: Long-term follow-up with gait analysis. J Bone Joint Surg Am 1979;61:964-975.
Question 48
Figure 48 shows the radiograph of a 17-year-old boy who sustained a gunshot wound to his forearm. There is a small entrance wound on the volar surface. The exit wound is dorsal and more than 15 cm in size, with loss of skin and an extensive amount of devitalized muscle hanging out of the wound. Vascular supply to the hand is excellent, the ulnar and median nerves are intact in the hand, but the radial sensory nerve function is absent. After repeated surgical debridements of the wound and bone, definitive treatment for the fracture would most likely be which of the following? Review Topic

Explanation
Question 49
A tall, thin 17-year-old basketball player and his parents request an evaluation of his flexible (hypermobile) pes planus/planovalgus foot deformities. As part of his evaluation, the orthopaedic surgeon notes pectus excavatum, disproportionately long arms, and scoliosis. In addition to providing treatment of his feet, what test or evaluation should the patient be referred for? Review Topic
Explanation
Question 50
A newborn girl is referred for evaluation of suspected hip instability. What information from her history would place her in the highest risk category?
Explanation
REFERENCES: Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 51
In Dupuytren’s disease, the retrovascular cord typically displaces the radial proper digital nerve of the ring finger in what direction?
Explanation
REFERENCE: Rayan GM: Palmar fascial complex anatomy and pathology in Dupuytren’s disease. Hand Clin 1999;15:73-86.
Question 52
A 32-year-old powerlifter who was performing a dead lift 3 days ago noted a sharp pain in the front of his dominant right arm just after beginning to lower the weight. He now reports pain in the anterior aspect of the arm that worsens when he opens a door. Examination reveals moderate ecchymosis and swelling of the forearm and tenderness in the antecubital fossa. The MRI scans are shown in Figures 15a and 15b. If the injury is left unrepaired, the greatest functional deficit will most likely be the loss of
Explanation
REFERENCES: D’Alessandro DF, Shields CL Jr, Tibone JE, Chandler RW: Repair of distal biceps tendon ruptures in athletes. Am J Sports Med 1993;21:114-119.
Agins HJ, Chess JL, Hoekstra DV, Teitge RA: Rupture of the distal insertion of the biceps brachii tendon. Clin Orthop 1988;234:34-38.
Question 53
A 28-year-old professional football player reports painless loss of ankle motion after sustaining a “severe” ankle sprain 12 months ago. A mortise radiograph is shown in Figure 1. Surgical treatment should be reserved for which of the following conditions?
Explanation
REFERENCES: Whiteside LA, Reynolds FC, Ellsasser JC: Tibiofibular synostosis and recurrent ankle sprains in high performance athletes. Am J Sports Med 1978;6:204-208.
Henry JH, Andersen AJ, Cothren CC: Tibiofibular synostosis in professional basketball players. Am J Sports Med 1993;21:619-622.
Andrish J: The leg, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2155-2181.
Question 54
An otherwise healthy 50-year-old man who is a smoker undergoes a posterior spine fusion with instrumentation for spondylolisthesis. What can the patient do to minimize his risk for pseudarthrosis?
Explanation
Question 55
The direct anterior (Smith-Peterson) approach to hip arthroplasty is most commonly associated with injury to what nerve?
Explanation
Some authors have reported the incidence of lateral femoral cutaneous nerve neuropraxia following hip arthroplasty with the direct anterior approach to be near 80%, but resolution of the sensory deficits has been observed in most patients over time. Femoral nerve palsy has been reported to occur in .64% to 2.3% direct lateral (Hardinge) and anterolateral (Watson-Jones) approaches, and the superior gluteal nerve may be injured with proximal extension of the abductor muscular dissection. The posterior approach has been reported to be associated with sciatic nerve injury, especially in cases of dysplasia. Pudendal nerve injury has not been reported with the anterior, anterolateral, direct lateral, or posterior approaches to hip
arthroplasty. It has been reported following hip arthroscopy and the use of a traction table, however.
Question 56
Figure 26 shows the radiograph of a 48-year-old woman who has right arm pain and hematuria. A bone scan reveals increased uptake in the left ribs and thoracic spine. A needle biopsy specimen shows that the lesion is highly keratin positive and composed primarily of clear cells. What is the best course of action?
Explanation
REFERENCES: Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1054.
Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Katzner M, Schvingt E: Operative treatment of bone metastases secondary to renal carcinoma: Basic research and treatment of renal cell carcinoma metastasis. Prog Clin Biol Res EORTC 1990;348:151-168.
Question 57
Compared to postoperative radiation therapy, preoperative radiation therapy has a higher rate of what complication?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Davis AM, O’Sullivan B, Turcotte R, et al: Late radiation morbidity following randomization to preoperative versus postoperative radiotherapy in extremity soft tissue sarcoma. Radiother Oncol 2005;75:48-53.
Question 58
Acetabular reconstruction followed by external beam irradiation The plain radiographs show a purely lytic destructive lesion that is poorly marginated. The technetium bone scan does not show any major uptake. The computerized tomography scan shows purely lytic bone destruction with breakthrough of the cortical bone. Complete destruction of the cortical bone is suggestive of a malignancy. The magnetic resonance image shows a lesion that is homogenously low on T1-weighted images and high on T2-weighted images. Surgeons cannot make a definitive diagnosis based upon the radiographic features. The most common malignancies in this age group are:
Explanation
A 50-year-old woman has had severe hip pain for 4 months. Her plain radiographs (Slide 1), technetium bone scan (Slide 2), computerized tomography scan (Slide 3), and coronal T1- and T2-weighted magnetic resonance images (Slide 4) are presented. The most likely diagnosis based upon the radiographs would be:
Question 59
Figures 1 and 2 are the radiographs of a 40-year-old woman who sustained a twisting injury to her lower extremity. What additional information or studies are important in determining treatment options?

Explanation
(SBQ12TR.24) In each of the following scenarios, atrophic fracture nonunion occurred after initial treatment with intramedullary nail fixation. Which scenario has shown to have the highest rate of osseous union if treated with exchange intramedullary nailing?
Oligotrophic nonunion of a comminuted humeral shaft fracture
Oligotrophic nonunion of a transverse humeral shaft fracture
Oligotrophic nonunion of an oblique distal femur fracture
Oligotrophic nonunion of a comminuted tibial shaft fracture
Oligotrophic nonunion of an oblique tibial shaft fracture
Reamed exchange nailing is recommended for the management of aseptic nonunions of noncomminuted tibial shaft fractures. Union rates have been reported between 76-96% in large studies.
Tibial exchange nailing promotes osseous bone healing of non-unions by providing biological and mechanical support. The biological support is provided by reaming the medullary canal. This increases periosteal blood flow and stimulates periosteal new-bone formation. The mechanical support is provided by a larger-diameter intramedullary nail, which increases the rigidity and strength of the nail.
Brinker et al. reviewed the concept of exchange nailing of nonunited long bone fractures. They showed that exchange nailing is the most successful in the treatment of nonunions following closed or open fractures without substantial bone loss. Aseptic, noncomminuted diaphyseal femoral and tibial shaft fractures showed the highest rates of union with exchange nailing, which were found to be 76-100% and 72-96%, respectively.
Illustration A shows a heterotrophic non-union of the tibia after intramedullary nailing. The patient was treated with exchange nailing with a larger nail. On the right shows a 4 month post-op radiograph after exchange nailing showing osseous union at the fracture site.
Incorrect Answers:
(SBQ12TR.79) A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2 weeks. Which of the following would be an indication for surgical management?
Age greater than 70 years.
Fracture pattern in Figure A
Significant medical comorbidities.
Fracture pattern in Figure B
Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is
displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:
Question 60
- What posterior pelvic ring injury is most commonly associated with neurologic compromise?
Explanation
associated with partial damage to the 5th lumbar root (5.9%). Zone 2-Sacral foramina region, outside of the sacral canal (i.e. distracters #3 and #4); associated with sciatica (28.4%) but rarely bladder dysfunction. Zone 3-Central sacral canal (AKA: Transverse Fx) (i.e. correct answer #2); associated with saddle anesthesia and loss of sphincter tone; neurologic damage (56.7%) and involvement of bowel, bladder, and sexual dysfunction (76.1%).
Question 61
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of Review Topic
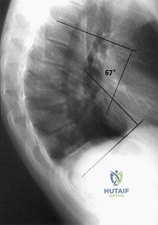
Explanation
Question 62
An 85-year-old right hand dominant male sustains a fall onto his elbow while trying to get out of the car. His past medical history is significant for diabetes, congestive heart failure, and COPD. He lives in a nursing home, and is able to ambulate at baseline without and assistive devices. What would be the ideal definitive surgical treatment options in this patient? Review Topic

Explanation
TEA is a preferred alternative for ORIF in elderly patients with complex distal humeral fractures that are not amenable to stable fixation. Elderly patients appear to accommodate to objective limitations in function with time, and suffer less complications with TEA than ORIF in select cases.
Sorensen et al evaluated short- to medium term outcome of total elbow arthroplasty (TEA) in complex fractures of the distal humerus by evaluating 24 consecutive cases. Twenty of the patients were followed for almost 2 years, and their MEPS were 15 excellent, 4 good and 1 fair result. They concluded that TEA in complex fractures of the distal humerus in elderly patients can result in acceptable short- to medium term outcome.
Mckee et al conducted a prospective, randomized, controlled trial to compare
functional outcomes, complications, and reoperation rates in elderly patients with displaced intra-articular, distal humeral fractures treated with open reduction-internal fixation (ORIF) or primary total elbow arthroplasty (TEA). They randomized 42 patients and found that TEA for the treatment of comminuted intra-articular distal humeral fractures resulted in more predictable and improved 2-year functional outcomes compared with ORIF, based on the MEPS.
Illustration A shows radiographs of a TEA. Incorrect Answers:
Question 63
In patients who have undergone nonsurgical management for idiopathic adhesive capsulitis, long-term follow-up studies have shown which of the following results?
Explanation
REFERENCES: Griggs SM, Ahn A, Green A: Idiopathic adhesive capsulitis: A prospective functional outcome study of nonoperative treatment. J Bone Joint Surg Am 2000;82:1398-1407.
Shaffer B, Tibone JE, Kerlan RK: Frozen shoulder: A long-term follow-up. J Bone Joint Surg Am 1992;74:738-746.
Question 64
A 17-year-old high school football player reports wrist pain 5 months after the conclusion of the football season. A radiograph and MRI scan are shown in Figures 29a and 29b. What is the recommended intervention?
Explanation
REFERENCES: Waters PM, Stewart SL: Surgical treatment of nonunion and avascular necrosis of the proximal part of the scaphoid in adolescents. J Bone Joint Surg Am 2002;84:915-920.
Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg Am 2002;27:391-401.
Question 65
A 10-year-old girl with a history of an obstetrical brachial plexus palsy has been referred for evaluation. Examination reveals a severe adduction internal rotation contracture of the shoulder and a mild flexion contracture of the elbow. Hand function is normal. Radiographs show mild glenohumeral joint incongruity. To achieve the best functional outcome, management should consist of
Explanation
REFERENCES: Jahnke AH Jr, Bovill DF, McCarroll HR Jr, James P, Ashley RK: Persistent brachial plexus birth palsies. J Pediatr Orthop 1991;11:533-537.
Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of 20 cases. J Pediatr Orthop 1990;10:442-444.
Goddard NJ, Fixsen JA: Rotation osteotomy of the humerus for birth injuries of the brachial plexus. J Bone Joint Surg Br 1984;66:257-259.
Question 66
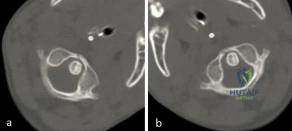
A 3-year-old girl developed torticollis eight months ago after a severe respiratory tract infection. A initial trial of halter traction was attempted without success. A trial of halo traction was then performed for 3 weeks and then a dynamic computed tomographic (CT) was obtained and shown in Figure A. Panel (a) shows an axial image with maximal rotation to the left. Panel (b) shows an axial image with maximal rotation to the right. What is the most appropriate next step in management? Review Topic
Explanation
Common causes of Atlantoaxial rotatory displacement (AARD) include infection, trauma, and recent neck surgery. Diagnosis is challenging and is best confirmed with dynamic CT (CT with the head turned maximally to either side and at neutral). If the symptoms are acute (less than 7 days) then initial treatment with a soft collar and anti-inflammatory medications is indicated. If the condition has been present for more than a week, more aggressive treatment with halter traction (present 1 week to 1 month) or halo traction (present for 1-3 months) is indicated. If nonoperative modalities fail, the condition has been present for > 3 months, or the patient has neurologic deficits, then posterior C1-C2 fusion is indicated.
Copley et al discuss the evaluation and treatment of various congenital and traumatic conditions of the pediatric cervical spine. They report that the underlying mechanism of Atlantoaxial rotatory displacement (AARD) is inflammation and spasm which can be caused by infection, prior surgery, trauma, and rheumatoid arthritis.
Subach et al reviewed at 20 children with atlantoaxial rotatory subluxation. They found that of the 20 patients treated overall, conservative management failed in 6 (30%), and they required posterior fusion because of recurrence of the atlantoaxial rotatory subluxation or unsuccessful reduction. The major factor predicting the failure of conservative management was the duration of subluxation before initial reduction. Patients with long-standing subluxation were more likely to experience recurrence and require surgery.
Figure A shows an asymmetric placed odontoid within the ring of C1. There is an increased distance from the odontoid to the right arch of C1 which is fixed and minimally changes with maximal rotation to the left. This radiographic finding is indicative of fixed subluxation. Illustration A further demonstrates this.
Incorrect
(SBQ12SP.1) A 65-year-old female with a history of breast cancer presents with bilateral buttock and leg pain that is worse with walking and improves with sitting. In addition, she reports that she feels unsteady on her feet and requires holding the railing when going up and down stairs. On physical exam she is unable to complete a tandem gait and has hip flexion weakness, ankle dorsiflexion weakness, and ankle plantar flexion weakness. Her reflex exam shows 3+ bilateral patellar reflexes. Radiographs and an MRI are shown in Figure A and B. What is the next most appropriate step in management. Review Topic

Lumbar epidural injection
Physical therapy with core strengthening and anti-inflammatory medications as needed
Lumbar decompression
Lumbar decompression and fusion
MRI of the cervical and thoracic spine
The clinical scenario is consistent with a patient with symptoms of degenerative spondylolisthesis AND symptoms of myelopathy. Myelopathy must be ruled out by performing an MRI of the cervical and thoracic spine.
Tandem stenosis occurs in approximately 5 to 25% of patients. Because of the stepwise progressive nature of myelopathy, treatment of myelopathy often takes precedence over lumbar spinal stenosis.
Rhee et al. found that the sensitivity and specificity of specific physical exam findings varies. Both the upward babinski reflex and the presence of clonus were found to be very non-sensitive (13%). The most sensitive provacative test was found to be the Hoffman sign (59%).
Salvi et al. reviewed the classic presentations for cervical myelopathy including demographics, history, and physical exam findings (the inability to preform a tandem gait, hyperreflexia, an abnormal babinksi and hoffman reflex, the inability to preform rapid movements and bilateral muscle weakness). Additionally they identify other potential causes for myelopathy, including multiple sclerosis, amyotrophic lateral sclerosis, multifocal motor neuropathy, and Guillain-Barre´syndrome.
Maezawa et al. showed that gait analysis can identify a pattern in patients with myelopathy. Patients with severe myelopathy have a characteristic gait with hyperextension of the knee in the stance phase without plantar flexion of the ankle in the swing phase. They also have decreased walking speed and stride length with a prolonged stance phase.
Figure A and B show a classic degenerative spondylolisthesis.
Incorrect Answers:
Question 67
..Figures 87a through 87e are the radiograph, MRI scans, and biopsy specimen of an 83-year-old woman who is experiencing pain in her distal thigh with activity and at night. She has undergone total hip arthroplasty for hip osteoarthritis. The most appropriate treatment is
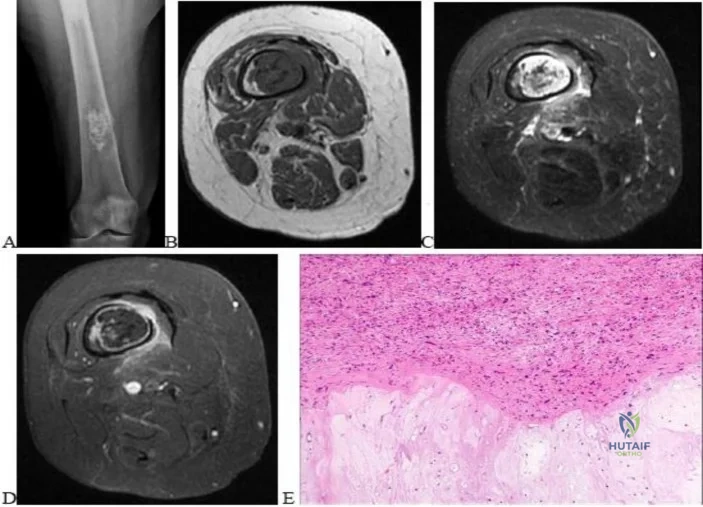
Explanation
Figures 88a and 88b are the radiographs of a 70-year-old woman with a remote history of localized renal cell carcinoma. She has insidious onset of right shoulder pain that worsens with any activity and at night. She appears otherwise healthy.


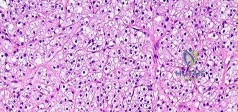
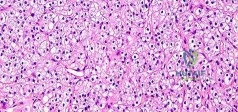
Question 68
0 mmol/L (normal < 2.5), 1 hour postinjury it was 3.5 mmol/L, and it is now 5 mmol/L. His core temperature is 93 degrees F (34 degrees C). What is the most appropriate management for the femoral shaft fracture at this point?
Explanation
Question 69
A 57-year-old man with type II diabetes mellitus was successfully treated for a first occurrence forefoot full-thickness (Wagner II) diabetic foot ulcer underlying the third metatarsal head with associated hammertoe with a series of weight-bearing total contact casts. There was no evidence of osteomyelitis. The ulcer is now fully healed. He is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. What is the next most appropriate step in management?
Explanation
REFERENCES: Pinzur MS, Slovenkai MP, Trepman E, et al: Guidelines for diabetic foot care: Recommendations endorsed by the Diabetes Committee of the American Orthopaedic Foot and Ankle Society. Foot Ankle Int 2005;26:113-119.
Pinzur MS, Dart HC: Pedorthic management of the diabetic foot. Foot Ankle Clin 2001;6:205-214.
Question 70
Figure 42 shows the radiograph of a patient with spinal muscular atrophy. Examination reveals good upper extremity function, and she can tie her shoes and propel a manual wheelchair. Posterior instrumentation and fusion may result in
Explanation
REFERENCES: Bentley G, Haddad F, Bull TM, Seingry D: The treatment of scoliosis in muscular dystrophy using modified Luque and Harrington-Luque instrumentation. J Bone Joint Surg Br 2001;83:22-28.
Furumasu J, Swank SM, Brown JC, Gilgoff I, Warath S, Zeller J: Functional activities in spinal muscular atrophy patients after spinal fusion. Spine 1989;14:771-775.
Granata C, Cervellati S, Ballestrazzi A, Corbascio M, Merlini L: Spine surgery in spinal muscular atrophy: Long-term results. Neuromuscul Disord 1993;3:207-215.
Question 71
Two years after undergoing a total shoulder arthroplasty, a patient reports increasing pain, stiffness, and swelling, and has an increased white blood cell count. Radiographs show lucencies around the glenoid and humeral components. You suspect infection. Which of the following is the most likely responsible organism? Review Topic
Explanation
Question 72
A 2-week-old infant has had diminished movement of the right upper extremity since birth. Examination reveals weakness of shoulder abduction and external rotation, elbow flexion, and forearm supination. Both pupils are equally round and responsive to light. The remainder of the examination is normal. Radiographs of the upper limb show a healing middle-third clavicle fracture. Management should consist of
Explanation
REFERENCES: Waters PM: Comparison of the natural history, the outcome of microsurgical repair, and the outcome of operative reconstruction in brachial plexus birth palsy. J Bone Joint Surg Am 1999;81:649-659.
Greenwald AG, Schute PC, Shiveley JL: Brachial plexus birth palsy: A 10-year report on the incidence and prognosis. J Pediatr Orthop 1984;4:689-692.
Question 73
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who has elbow pain after falling from a ladder onto an outstretched hand. Examination reveals elbow pain, swelling, limited motion, and normal neurologic function. A pathognomonic radiographic feature of this injury is a

Explanation
Ideal visualization of the fragment during surgery is provided through a laterally based elbow approach (Kaplan or Kocher) with the patient in the supine position. Extension of the approach can be accomplished by releasing the lateral collateral ligament origin, which must be repaired to prevent post-operative instability. Posterior comminution and lateral column impaction are occasionally seen. When present, a posterior approach with an olecranon osteotomy is considered an alternative, but still does not allow ideal visualization of the anterior articular cartilage or safe angles for anterior to posterior screw placement. Therefore, the posterior approach not the preferred approach.
Headless screws are useful because this is typically a partial articular injury and screw orientation is ideally from anterior to posterior. The anterior entry of the screw should be buried beneath the articular cartilage margin.
Question 74
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of
Explanation
REFERENCES: Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Warner JJ, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 75
The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?
Explanation
REFERENCE: Mazzoca AD: Principles of internal fixation, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 308-309.
Question 76
A 45-year-old man sustained the injury seen in Figure 130a 6 weeks ago. He denies any prior injury to his shoulder. After treatment of the injury in the emergency department, he was noted to have significant weakness with empty can testing and external rotation at the side. He has full passive range of motion with forward flexion, abduction, and internal and external rotation, but has difficulty initiating abduction with his arm at his side. He has negative apprehension and relocation signs. A detailed neurologic examination shows no deficits. A coronal image from a follow-up MRI scan is seen in Figure 130b. Follow-up radiographs reveal no fractures. What is the most appropriate next step in his treatment? Review Topic
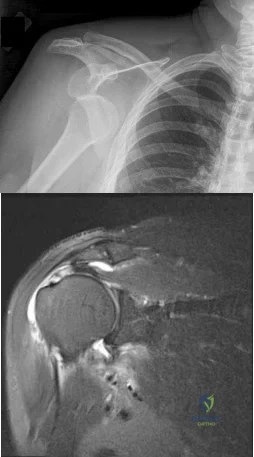
Explanation
Question 77
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?
Explanation
REFERENCES: Smith GR, Hotchkiss RN: Radial head and neck fractures: Anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg 1996;5:113-117.
Caputo AE, Mazzocca AD, Santoro VM: The nonarticulating portion of the radial head: Anatomic and clinical correlations for internal fixation. J Hand Surg Am 1998;23:1082-1090.
Question 78
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?
Explanation
REFERENCES: Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Callaghan JJ, Salvati EA, Pellicci PM, Wilson PD Jr, Ranawat CS: Results of revision for mechanical failure after cemented total hip replacement, 1979 to 1982: A two- to five-year follow-up. J Bone Joint Surg Am 1985;67:1074-1085.
Question 79
Hip pain of 1-month duration has developed in a 72-year-old man with a previous total hip arthroplasty. He underwent dental work 6 weeks ago. Aspiration shows a white blood cell count of more than 6,000 cells/μL (reference range 4,500 to 11,000 cells/μL) and the presence of gram-positive cocci in clusters on Gram stain. The orthopaedic surgeon recommends urgent debridement and irrigation. Fixation of the components is judged to be stable, and the surgeon elects to retain the implants. The patient has a final culture that reveals methicillin-resistant Staphylococcus aureus (MRSA). If the attending physician recommends the two-stage protocol, including the use of an antibiotic-cement spacer, what is the most likely prognosis for this patient?
Explanation
The patient has a late infection of at least 4 weeks symptomatic duration that most likely is hematogenous in etiology. This infection is not an acute hematogenous infection that can successfully be treated with irrigation and debridement. Retention of the implants with debridement and irrigation alone has been associated with a poor prognosis. In a recent study, the success rate was only 44% in a series of 104 patients at a mean 5.7-year follow-up. In one study of 50 infections attributable to MRSA or methicillin- resistant Staphylococcus epidermidis organisms treated with a two-stage protocol, the failure rate was
21%. Patients who experienced successful infection treatment had lower functional outcome measures using the Western Ontario and McMaster Universities Osteoarthritis Index, the University of California
Los Angeles Activity Score, and the 12-item Oxford Knee Score, however.
Question 80
Which of the following illustrations shown in Figures 21a through 21e correctly shows the projection of the sacroiliac joint on the outer table of the ilium?
Explanation
REFERENCES: Waldrop JT, Ebraheim NA, Yeasting RA, Jackson WT: The location of the sacroiliac joint on the outer table of the posterior ilium. J Orthop Trauma 1993;7:510-513.
Xu R, Ebraheim NA, Yeasting RA, Jackson WT: Anatomic considerations for posterior iliac bone harvesting. Spine 1996;21:1017-1020.
Question 81
The great medullary artery, also known as the Adamkiewicz artery, originates from which of the following arteries?
Explanation
REFERENCES: Lu J, Ebraheim NA, Biyani A, Brown JA, Yeasting RA: Vulnerability of great medullary artery. Spine 1996;21:1852-1855.
Rogers FB, Osler TM, Shackford SR, Wald SL: Isolated stab wound to the artery of Adamkiewicz: Case report and review of the literature. J Trauma 1997;43:549-551.
Question 82
A 35-year-old woman who is a recreational runner reports posterior knee pain and tightness in the knee with flexion during running. She denies any history of trauma. Examination reveals normal patellar glide and tilt and no patellar apprehension. Range of motion is 5 degrees to 120 degrees, and quadriceps function and knee ligamentous examination are normal. Radiographs are normal. An MRI scan is shown Figure 18. What is the most likely diagnosis?
Explanation
REFERENCES: Deutsch A, Veltri DM, Altchek DW, et al: Symptomatic intraarticular ganglia of the cruciate ligaments of the knee. Arthroscopy 1994;10:219-223.
Brown MF, Dandy DJ: Intra-articular ganglia of the knee. Arthroscopy 1990;6:322-323.
Question 83
Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the best treatment?
Explanation
REFERENCES: McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective.
Am J Orthop 1999;28:21-26.
Taylor MS: Cold weather injuries during peacetime military training. Milit Med 1992;157:602-604.
Question 84
What is the primary indication for performing an arthroscopic synovectomy on a patient with hemophilia that is the result of factor VIII deficiency? Review Topic
Explanation
Question 85
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?
Explanation
REFERENCES: Brodsky AE, Khalil MA: Talar compression syndrome. Am J Sports Med 1986;14:472-476.
Wredmark T, Carlstedt CA, Bauer H, Saartok T: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Question 86
A patient reports a sudden recurrence of sciatica on her left side after undergoing a successful left L4-L5 diskectomy 15 months ago. Which of the following imaging modalities is most accurate in differentiating recurrence of the disk herniation from postoperative epidural scar tissue?
Explanation
cause of the encroachment. Answer #2 makes no sense. Answers #3 and #4 are incorrect because the MRI is now the standard imaging modality.
Question 87
A 15-year-old girl sustained the injury shown in Figures 70a and 70b when she jumped from the back of a moving truck. She is seen in the emergency department 2 hours after her injury. She has no other injuries. Her foot is warm and she has a normal motor and sensory examination. Pulses are only evident on Doppler. What is the most appropriate management? Review Topic

Explanation
Question 88
A 36-year-old softball player sustains a shoulder dislocation making a diving catch. The shoulder is successfully reduced in the emergency department. A postreduction MRI is shown in Figure 35. What anatomic lesion is a result of the dislocation? Review Topic

Explanation
Question 89
Figure 1 is the radiograph of an 18-year-old, right hand-dominant man who has right side thumb pain after a tackle during a rugby game. Examination shows ecchymosis and swelling of the right thumb along with tenderness to palpation about the thumb CMC joint and metacarpal base. What ligament is holding the small fracture fragment in anatomical location to the trapezium?

Explanation
Bennett fractures are defined as intra-articular thumb metacarpal base fractures. The fracture is often caused by axial loading, and concomitant injuries to the thumb MCP joint and trapezium are common. The palmar ulnar aspect of the base of the metacarpal stays in place through its attachment to the trapezium by way of the anterior oblique ligament. The metacarpal shaft is displaced dorsally, proximally, and radially by the pull of the abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and adductor pollicis brevis. These fractures are often considered unstable and are treated surgically.
Question 90
A 14-year-old boy is involved in a motor vehicle accident and sustains the injury shown in Figures 18a and 18b. What is the most likely diagnosis? Review Topic

Explanation
Question 91
A 58-year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 92
-Figure 235 is the radiograph of a 75-year-old woman who is seen in the emergency department following a low-energy fall. What is the most appropriate treatment based on her radiographic findings?
Explanation

Question 93
Figures 70a and 70b show the sagittal MRI scan and axial CT of a patient who has decreased range of motion in the cervical spine. In which of the following directions would the cervical motion be most significantly limited?
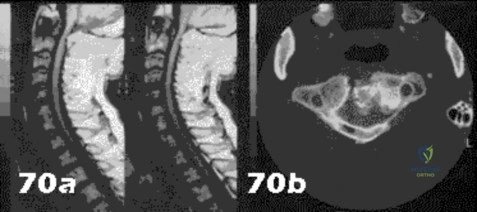
Explanation
Question 94
A researcher experimenting with limb patterning removes some tissue from 1 part of the limb bud (which we shall call Site A) and transplants it along the anteroposterior (AP) axis to create a mirror-hand duplication. Which of the following is true?
Explanation
The ZPA controls AP (radioulnar) growth. The signaling molecule is Shh, which is dose dependent. Higher Shh doses lead to posterior (ulnar) digits ulnar sided polydactyly. The extent of duplication is dose dependent (higher dose = more replication). Reduced Shh leads to loss of digits. Posterior elements (little finger/ulna) are formed EARLY prior to anterior elements which are formed LATE (radius/thumb). Disruption of AP patterning will result in loss of later forming elements (radius/thumb).
Al-Qattan et al. reviewed embryology of the upper limb. They summarized that embryology of the upper limb can be viewed in 2 distinct ways: the steps of limb development and the way that the limb is patterned along its 3 spatial axes. Cell signaling plays a major role in regulating growth and patterning of the vertebrate limbs. Signaling cell dysfunction results in congenital differences according to the affected signaling axis.
Illustration A shows an experiment to create ulnar dimelia by adding ZPA tissue to the anterior limb bud. The video shows development of the limb.
Incorrect Answers:
Question 95
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient? Review Topic
Explanation
Question 96
Figure 21 is the intraoperative fluoroscopic image of a 40-year-old man who felt a pop during a twisting injury to his right ankle. He underwent open reduction and internal fixation (ORIF) of a bimalleolar ankle fracture. During the surgery the medial and lateral malleoli fractures were reduced and rigidly was internally fixed. Following fracture fixation, which additional test is recommended to ensure mortise stability?

Explanation
Following ORIF of a known osseous injury, stress testing of the syndesmosis is recommended, especially for pronation-external rotation injuries. The Cotton test applies a laterally directed force to the fibula to assess for widening of the distal tibiofibular joint space. A positive Cotton test result indicates that syndesmotic stabilization is indicated. The Thompson test is used to determine Achilles tendon integrity. The squeeze test is a clinical, not intraoperative, assessment of syndesmotic injury. The anterior drawer test assesses the integrity of the anterior talofibular ligament.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Pakarinen H, Flinkkilä T, Ohtonen P, Hyvönen P, Lakovaara M, Leppilahti J, Ristiniemi J. Intraoperative assessment of the stability of the distal tibiofibular joint in supination-external rotation injuries of the ankle: sensitivity, specificity, and reliability of two clinical tests. J Bone Joint Surg Am. 2011 Nov 16;93(22):2057-61. doi: 10.2106/JBJS.J.01287. PubMed PMID:
Question 97
A 7-year-old girl sustains the fracture shown in Figure 29a. Casting results in uneventful healing. Ten months later, the patient has a progressive valgus deformity of the right lower extremity. A radiograph is shown in Figure 29b. Management should now consist of
Explanation
REFERENCES: Tuten HR, Keeler KA, Gabos PG, et al: Posttraumatic tibia valga in children: A long-term follow-up note. J Bone Joint Surg Am 1999;81:799-810.
McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 98
A 70-year-old woman reports anterior knee pain after undergoing an uncomplicated total knee arthroplasty 6 months ago. Examination reveals prepatellar tenderness, with no extensor lag. The radiographs shown in Figures 25a through 25c reveal a well-fixed patellar component. Management should consist of
Explanation
REFERENCES: Rorabeck CH, Angliss RD, Lewis PL: Fractures of the femur, tibia, and patella after total knee arthroplasty: Decision making and principles of management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 449-458.
Hozack WJ, Goll SR, Lotke PA, Rothman RH, Booth RE Jr: The treatment of patellar fractures after total knee arthroplasty. Clin Orthop 1988;236:123-127.
Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Question 99
Deep venous thromboses are primarily composed of red blood cells and fibrin. What is fibrin?
Explanation
Question 100
When compared with the normal anterior cruciate ligament (ACL), placement of an anterior cruciate ligament graft in the over-the-top position on the femoral side has what effect on its function?
Explanation
REFERENCES: Azar FM: Revision anterior cruciate ligament reconstruction. Instr Course Lect 2002;51:335-342.
Draganich LF, Hsieh YF, Sherwin SH, et al: Intra-articular anterior cruciate ligament graft placement on the average most isometric line on the femur: Does it reproducibly restore knee kinematics? Am J Sports Med 1999;27:329-334.
Bylski-Austrow DI, Grood ES, Hetzy MS, et al: Anterior cruciate ligament replacements: A mechanical study of femoral attachment location, flexion angle at tensioning, and initial tensioning. J Orthop Res 1990;8:522-531.
