Orthopedic Board Review MCQs: Trauma, Spine & Extremities | Part 51

Key Takeaway
This page offers Part 51 of a comprehensive Orthopedic Surgery Board Review. Featuring 100 verified, high-yield MCQs for AAOS and OITE exams, it's designed for orthopedic residents and surgeons. Utilize Study or Exam modes to master topics like Ankle, Elbow, and Trauma, ensuring robust board certification preparation.
About This Board Review Set
This is Part 51 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 51
This module focuses heavily on: Ankle, Elbow, Fracture, Ligament, Nerve, Trauma.
Sample Questions from This Set
Sample Question 1: The arthroscopic views shown in Figures 31a and 31b reveal extensive synovitis in the anterolateral corner of the ankle overlying a band of tissue sometimes implicated in soft-tissue impingement of the ankle following a chronic sprain injur...
Sample Question 2: An axillary nerve lesion may cause weakness in the deltoid and the...
Sample Question 3: A 12-year-old gymnast has had elbow pain for 4 weeks. She denies any specific trauma to the elbow. Examination reveals lateral pain and no instability on testing. Range of motion is as follows: 15 degrees, loss of elbow extension, normal fl...
Sample Question 4: Longitudinal radioulnar dissociation, including Essex Lopresti fractures, requires disruption of the interosseous membrane (IOM). The interosseous membrane (IOM) consists of all of the following ligaments EXCEPT?...
Sample Question 5: When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The arthroscopic views shown in Figures 31a and 31b reveal extensive synovitis in the anterolateral corner of the ankle overlying a band of tissue sometimes implicated in soft-tissue impingement of the ankle following a chronic sprain injury. This band is a portion of the
Explanation
REFERENCES: Bassett FH III, Gates HS III, Billys JB, et al: Talar impingement by the anteroinferior tibiofibular ligament: A cause of chronic pain in the ankle after inversion sprain.
J Bone Joint Surg Am 1990;72:55-59.
DiGiovanni BF, Fraga CJ, Cohen BE, et al: Associated injuries found in chronic lateral ankle instability. Foot Ankle Int 2000;21:809-815.
Question 2
An axillary nerve lesion may cause weakness in the deltoid and the
Explanation
REFERENCE: Hollinshead WH: Anatomy for Surgeons: The Back and Limbs. New York, NY, Harper & Row, 1969.
Question 3
A 12-year-old gymnast has had elbow pain for 4 weeks. She denies any specific trauma to the elbow. Examination reveals lateral pain and no instability on testing. Range of motion is as follows: 15 degrees, loss of elbow extension, normal flexion, and normal pronation and supination. Radiographs reveal a 3- x 7-mm radiolucency of the capitellum. A T1-weighted MRI scan reveals a single solitary lesion, and T2-weighted images show no signal around the lesion. There are no intra-articular loose bodies. Appropriate management should include which of the following? Review Topic
Explanation
Question 4
Longitudinal radioulnar dissociation, including Essex Lopresti fractures, requires disruption of the interosseous membrane (IOM). The interosseous membrane (IOM) consists of all of the following ligaments EXCEPT?

Explanation
The IOM bridges the radius and ulna and acts as a hinge for rotation of radius about ulna. The central portion is thickened, and forms the central band which is the most important ligament for IOM load distribution characteristics.
Noda et al, in a cadaver study, identified the precise anatomical insertions and attachment points of each of the 5 IOM components. They found the most distal and proximal ends of the radial origin of the central band were 53% and 64% of total radial length from the tip of the radial styloid, whereas those of the ulnar insertion were 29% and 44% of total ulnar length from the ulnar head.
Pfaeffle et al also performed a cadaveric biomechanical study applying compressive loads to specimens with IOMs that are intact, cut, or cut/reconstructed with flexor carpi radialis allografts. They found that reconstruction of the IOM can restore the normal load transfer chararcteristics and that the central band of the IOM is the most important portion of the IOM to be reconstructed.
Question 5
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in
Explanation
REFERENCES: Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Shen WJ, Liu TJ, Shen YS: Nonoperative treatment versus posterior fixation for thoracolumbar junction burst fractures without neurologic deficit. Spine 2001;26:1038-1045.
Question 6
A 7-year-old girl is hit by a motor vehicle and sustains the isolated ipsilateral injuries shown in Figures 16a and 16b. What is the optimal definitive method of treatment?
Explanation
REFERENCES: Poolman RW, Kocher MS, Bhandari M: Pediatric femoral fractures:
A systematic review of 2422 cases. J Orthop Trauma 2006;20:648-654.
Anglen JO, Choi L: Treatment options in pediatric femoral shaft fractures. J Orthop Trauma 2005;19:724-733.
Beaty JH: Operative treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 2005;434:114-122.
Question 7
Which of the following is considered a contraindication to cement injection techniques, such as kyphoplasty or vertebroplasty, in the treatment of osteoporotic compression fractures?
Explanation
REFERENCES: Phillips FM, Pfeifer BA, Leiberman IH, et al: Minimally invasive treatment of osteoporotic vertebral compression fractures: Vertebroplasty and kyphoplasty. Instr Course Lect 2003;52:559-567.
Truumees E, Hilibrand A, Vaccaro AR: Percutaneous vertebral augmentation. Spine J 2004;4:218-229.
Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 8
A 23-year-old man was a restrained backseat passenger in a head-on motor vehicle collision. Examination revealed extensive bruising diagonally across his chest and abdominal areas and extreme pain at the thoracolumbar junction posteriorly. The lateral chest radiograph showed splaying of the spinous processes and increased disk height at the level of the injury, but no fracture of the vertebral bodies. He underwent a posterior spine fusion with instrumentation to stabilize the spine after a full trauma workup revealed the spine to be his only injury. Where is the center of rotation for this injury? Review Topic
Explanation
Question 9
An 11-year-old basketball player reports that he felt a painful pop in the left knee when he stumbled while running. He is unable to bear weight on the extremity and cannot actively extend the knee against gravity. Examination reveals a large knee effusion. A lateral radiograph is shown in Figure 7. Management should consist of
Explanation
REFERENCES: Maguire JK, Canale ST: Fractures of the patella in children and adolescents.
J Pediatr Orthop 1993;13:567-571.
Grogan DP, Carey TP, Leffers D, et al: Avulsion fractures of the patella. J Pediatr Orthop 1990;10:721-730.
Question 10
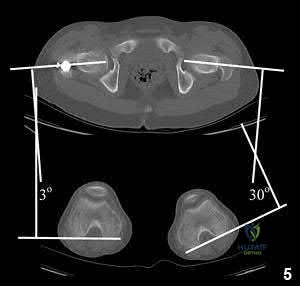
A 55-year-old male is involved in a motorcycle crash and sustains a closed, right-sided, midshaft femur fracture. This is an isolated injury. He is treated with retrograde femoral nailing, and postoperatively is noted to have 30 degrees of internal rotation of the operative extremity, when compared with his nonsurgical side. Which of the following is the most likely cause of this malrotation deformity?
Explanation
Postsurgical internal malrotation after treatment for a diaphyseal femur fracture typically occurs either via internal rotation of the distal segment relative to the proximal or external rotation of the proximal segment relative to the distal. These clinical findings are consistent with an iatrogenic increase in femoral anteversion.
Dimitriou et al. performed a study to quantify the side-to-side anatomic variation in the proximal femur and the implications for preoperative planning and leg length discrepancy following hip arthroplasty. CT-based 3D femoral models were reconstructed for 122 paired femurs in 61 young healthy subjects with no history of hip pathology. Significant side-to-side differences were found in femoral anteversion, horizontal offset, and femoral head center location.
They concluded that relying on the anatomic landmarks of the contralateral femur during hip arthroplasty may not necessarily result in restoration of native anatomy and leg-length.
Karaman et al. conducted a study which saught to clarify the influence of a femoral rotational malalignment of ≥10° after intramedullary nailing on daily activities. They evaluated twenty-four femoral shaft fracture patients treated with closed antegrade IMN, and determined the presence of malrotation with post-operative CT scans. Ten of the 24 patients had a CT-detected true rotational malalignment of ≥10° compared with the unaffected side, and were noted to have significantly worse functional outcome scores compared with normally rotated femoral shaft patients.
Espinoza et al. present a technique using intraoperative fluoroscopy and the anteversion inherent to the IM nail for obtaining appropriate femoral rotational alignment during surgery. The authors state that their technique reliably sets the femoral anteversion within a normal physiologic range with minimal additional intraoperative steps and without preoperative measurements.
Illustration A shows a CT evaluation of femoral malrotation. The angle on the uninjured side measures 30°, while the malrotated fractured side measures only 3°, indicating a 27° external rotation deformity.
Incorrect Answers:
OrthoCash 2020
Question 11
A 30-year-old woman sustains a transverse amputation of the distal phalanx of the index finger, leaving exposed bone. What is the most appropriate management of the soft-tissue defect?
Explanation
the thumb.
REFERENCES: Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Atasoy E, Ioakimidis E, Kasdan ML, et al: Reconstruction of the amputated fingertip with a triangular volar flap: A new surgical procedure. J Bone Joint Surg Am 1970;52:921-926.
Question 12
A right-handed 44-year-old construction worker reports pain and limited range of motion in his right elbow that has limited his ability to work for the past year. Examination reveals range of motion from 60 to 90 degrees, and he has pain at the extremes of flexion and extension. Pronation and supination are minimally restricted. Anti-inflammatory drugs have failed to provide relief. A radiograph is shown in Figure 8. Management should now consist of
Explanation
REFERENCES: Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: Long-term outcome and complications. J Bone Joint Surg Am 2002;84:2168-2173.
Phillips NJ, Ali A, Stanley D: Treatment of primary degenerative arthritis of the elbow by ulnohumeral arthroplasty: A long-term follow-up. J Bone Joint Surg Br 2003;85:347-350.
Question 13
Based on the radiograph shown in Figure 4, the innervation of what muscle is most at risk with total hip arthroplasty?
Explanation
REFERENCES: Eggli S, Hankemayer S, Muller ME: Nerve palsy after leg lengthening in total replacement arthroplasty for developmental dysplasia of the hip. J Bone Joint Surg Br 1999;81:843-845.
Schmalzried TP, Amstutz HC, Dorey FJ: Nerve palsy associated with total hip replacement:
Risk factors and prognosis. J Bone Joint Surg Am 1991;73:1074-1080.
Question 14
Figures A and B are radiographic images of an 85-year-old woman with isolated left hip pain. She describes a non-syncopal fall from standing 4 hours ago. Physical examination reveals pain with log-rolling the left thigh and the inability to bear weight on the affected leg. The radiologist reports no fracture in the left hip. What would be the next best step? Review Topic

Explanation
Moderate evidence supports MRI as the advanced imaging of choice for diagnosis of presumed hip fracture not apparent on initial radiographs. MRI has been shown to be able to detect occult fractures earlier than bone scan, with better spatial resolution. Usually the MRI should be obtained in less than 24 hours from the time of injury. For situations in which MRI is not immediately available, bone scan can be considered after 72 hours form the time of injury. However, this may compromise patient care and put the patient at risk of fracture displacement.
Cannon et al. reviewed the imaging of choice in occult hip fracture. They showed that physical examination yields a poor sensitivity identifying occult hip fractures, with log-rolling and straight-leg raise as 50% and 70%, respectively. The most sensitive modality for occult fracture identification was MRI.
Iwata et al. retrospectively reviewed a cohort of 35 patients with clinically suspected fractures of the hip that underwent MRI. All radiographs were negative. In 26 of these patients, a T1-weighted coronal MRI showed a hip fracture with 100% sensitivity.
Roberts et al. reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. They report moderate evidence that supports MRI as the advanced imaging of choice for diagnosis of presumed hip fractures not apparent on initial radiographs.
Figure A is a AP radiograph of the left hip and pelvis. Apart from a healed fracture of the ischiopubic rami and generalized osteopenia, there is no obvious hip fracture. Figure B is a coronal CT image that does not demonstrate evidence of an acute hip fracture. Illustration A is a T1 weighted MR image that shows a non displaced fracture (white arrow) through the intertrochanteric region of the left proximal femur.
Incorrect Answers:
(SBQ12TR.32) A 20-year-old male is taken to the emergency department following a motorcycle collision with the injury seen in Figures A and B. He undergoes serial debridements with placement of an antibiotic bead pouch, followed by intramedullary nailing and free tissue transfer. His preoperative examination is notable for absent plantar sensation. Which of the following is predictive of a worse long term outcome in this patient?

Absent plantar sensation at presentation
Depression at 3 months post-injury
Use of an intramedullary nail
Free tissue transfer instead of rotational flap
Need for multiple debridements
The presence of depression at the 3 months post-injury is a significant predictor of worse long term outcome as well as lower return to work rates in patients that present with limb threatening lower extremity trauma.
The findings of the Lower Extremity Assessment Project (LEAP study) has challenged many of the long-held beliefs of lower extremity trauma surgery, including the concept that patients with absent plantar sensation should undergo immediate amputation . The LEAP study has also brought to light the importance of socioeconomic and psychosocial factors in patient outcomes following these injuries.
Bosse et al analyzed a subgroup of 55 patients from the LEAP study with absent plantar sensation at presentation. Those patients that underwent limb salvage despite absent sensation (n=26) had no significant difference in functional outcome when compared with either insensate patients who underwent amputation or a matched control group of sensate patients with similar injuries. All but one patient in the salvage group had return of some sensation at 2-year follow up and the authors concluded that an insensate plantar foot at presentation should not be included in the algorithm for amputation.
Mackenzie and Bosse reviewed the results of the LEAP study with particular emphasis on the social and economic variables that influence outcomes in severe lower extremity. The authors note that 19% of patients screened positive for severe depression. The presence of anxiety, pain and depression at 3 months post-injury were significant predictors of poor outcome
Incorrect Answers:
tissue for type IIIB tibia fractures. Answer 5: The number of debridements has not been shown to influence outcome.
Question 15
An 82-year-old woman reports right buttock pain after a car trip. Laboratory studies show an erythrocyte sedimentation rate of 30 mm/h and WBC of 4,600/mm 3 . Figure 34a shows a plain AP radiograph of the pelvis, and Figure 34b shows a delayed technetium Tc 99m bone scan. Management should consist of
Explanation
REFERENCES: Newhouse KE, el-Khoury GY, Buckwalter JA: Occult sacral fractures in osteopenic patients. J Bone Joint Surg Am 1992;74:1472-1477.
Marmor L: Stress fracture of the pubic ramus simulating a loose total hip replacement. Clin Orthop 1976;121:103-104.
Question 16
A healthy 2-year-old boy falls from a swing and sustains a displaced midshaft femoral fracture with 1 cm of shortening. What is the most appropriate treatment?
Explanation
DISCUSSION: For children between the ages of 1 and 6 years, closed reduction and early spica casting is recommended. In some instances, associated injuries or body habitus may preclude cast treatment. Pavlik harness treatment of femoral fractures is for infants younger than 1 year of age. Rarely is there an indication for traction. Internal fixation is reserved in general for children older than age 6 years or with confounding factors.
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 271-280.
Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-359.
Figure 29a Figure 29b
Question 17
What is the preferred treatment of a symptomatic curly toe deformity in a 6-year-old child?
Explanation
REFERENCES: Hamer A, Stanley D, Smith TW: Surgery for curly toe deformity: A
double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood.
J Bone Joint Surg Br 1984;66:770-771.
Question 18
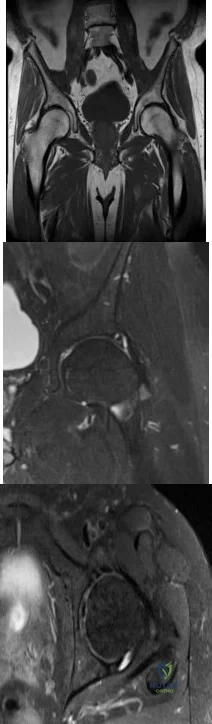
A 46-year-old woman has bilateral groin pain, with more severe pain on the left side than on the right side. Figures 44a and 44b show a radiograph and a T 1 -weighted MRI scan. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3160-3162.
Epstein RE, Dalinka MK: Ischemic necrosis, in Stark DD, Bradley WG (eds): Magnetic Resonance Imaging, ed 3. St Louis, MO, Mosby, 1999, vol 2, pp 1023-1027.
Question 19
Figure 24 shows the radiograph of a 4-year-old girl with spina bifida. Examination reveals an L3 motor level, excellent sitting and standing balance, and satisfactory range of motion at the hips. Management should consist of
Explanation
REFERENCE: Heeg M, Broughton NS, Menelaus MB: Bilateral dislocation of the hip in spina bifida: A long-term follow-up study. J Pediatr Orthop 1998;18:434-436.
Question 20
With increasing abduction in the scapular plane, maintaining neutral rotation, contact area, and contact pressure per unit area between the humeral head and glenoid follows what pattern if the total load across the joint is held constant?
Explanation
REFERENCES: Warner JJP, Bowen MK, Deng XH, et al: Articular contact patterns of the normal glenohumeral joint. J Shoulder Elbow Surg 1998;7:381-388.
Greis PE, Scuderi MG, Mohr A, et al: Glenohumeral articular contact areas and pressures following labral and osseous injury to the anteroinferior quadrant of the glenoid. J Shoulder Elbow Surg 2002;11:442-451.
Question 21
An 80-year-old man who was involved in a fall from ground height is evaluated in the emergency department for head lacerations and mild neck pain. Examination reveals only mild tenderness of the posterior neck region with some limitation of motion. Neurologic examination is normal. Radiographs of the cervical spine are shown in Figures 58a and 58b. What is the next most appropriate step in management for this patient? Review Topic

Explanation
Question 22
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Explanation
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 23
-An athletic 30-year-old sustained multiple injuries in a high-speed motor vehicle collision that resulted in a loss of approximately 30% of blood volume. On arrival to the emergency department, the heart rate is100 and blood pressure is 104/62. The best means with which to evaluate true hemodynamic status is
Explanation
Question 24
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
REFERENCES: Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186.
Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
Question 25
Figures 28a and 28b show AP and lateral radiographs of the knee. Based on these findings, which of the following structures has most likely been injured?
Explanation
REFERENCES: Schenck RC Jr, Hunter RE, Ostrum RF, et al: Knee dislocations. Instr Course Lect 1999;48:515-522.
Wascher DC, Dvirnak PC, DeCoster TA: Knee dislocation: Initial assessment and implications for treatment. J Orthop Trauma 1997;11:525-529.
Question 26
A 35-year-old man presents one week after an acute right shoulder posterior dislocation after being electrocuted. He is evaluated in the emergency department and undergoes closed reduction. The patient reports global right shoulder pain and limited active and passive range of motion. He has mild anterior and lateral bruising. He is distally neurovascularly intact. Current radiographs and an MRI scan are shown in Figures 1 through 3. What is the best next step?
Explanation
Question 27
A 36-year-old woman with familial neurofibromatosis has an enlarging mass in the posterior thigh. The lesion has slowly increased in size and is now constantly painful. Pressure on the mass causes dysesthesias in the foot. Figures 44a through 44c show T 1 -weighted, STIR, and T 1 -weighted fat-saturated gadolinium scans, respectively. Figure 44d shows a PET scan. What does this lesion most likely represent?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 225-230.
Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4218-4235.
Question 28
CLINICAL SITUATION Figure 1 is the radiograph taken 6 weeks ago of a 41-year-old woman with persistent pain in her right leg after sustaining a tibia fracture 12 months ago in a motor vehicle collision. On examination, she has well-healed scars and a well-healed flap on the medial aspect at the level of the fracture. She reports having an infection after the initial surgery, which resulted in debridement of the soft tissue and need for the local rotational flap. There are no changes at the fracture site as shown in the most recent radiograph (Figure 2). She is healthy and has no comorbidities. What is the best next step in the patient’s evaluation?

Explanation
but she has not had any issues since the flap. She has abundant callus formation but the fracture line is still visible and unchanged on 2 sets of radiographs. The patient has persistent pain. The best initial evaluation is to ensure that there is no underlying infection with laboratory studies, including a complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Nuclear medicine studies have questionable utility, but may be helpful if the inflammatory markers from laboratory studies come back elevated. A CT scan is not warranted because the sequential radiographs show persistent fracture lines and no changes. The patient has a hypertrophic nonunion. Originally, she had appropriate treatment and has shown the ability to make callus, thus her biologic capacity appears to be intact and bone grafting is not needed. The hypertrophic nature of her fracture nonunion indicates that she needs more stability. The best treatment for a hypertrophic nonunion of the tibia is exchange nailing. Based on successive radiographs and the lack of healing, observation is probably just delaying the inevitable. Plating with retention of the nail can be useful in recalcitrant long bone non-union, especially in the femur.
Question 29
A 14-year-old boy sustained a femoral neck fracture in a fall from a tree and underwent open reduction and internal fixation 6 months ago. Follow-up examination now reveals an antalgic Trendelenburg gait and painful range of motion. A radiograph is shown in Figure 23, and a CT scan shows a nonunion. Treatment should consist of
Explanation
REFERENCES: Lam SF: Fractures of the neck of the femur in children. J Bone Joint Surg Am 1971;53:1165-1179.
Canale ST, Beaty JH: Pelvic and hip fractures, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1109-1193.
Question 30
A 26-year-old man is involved in a high-speed motorcycle accident. He sustains a grade IIIB open tibia fracture. Examination reveals a large soft-tissue defect and an insensate foot. What is the expected outcome in this scenario? Review Topic
Explanation
Question 31
The arrow in the axial T 1 -weighted MRI scan shown in Figure 18 is pointing to which of the following structures?
Explanation
REFERENCES: Goss MS, Gelberman RH: The anatomy of the distal ulnar tunnel. Clin Orthop 1985;196:238-247.
Denman EE: The anatomy of the space of Guyon. Hand 1978;10:69-76.
Question 32
What is the recommended optimal timing of presurgical antibiotic administration to prevent infection in patients undergoing total joint replacement surgery?
Explanation
Question 33
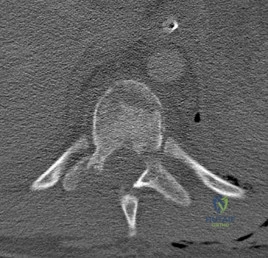
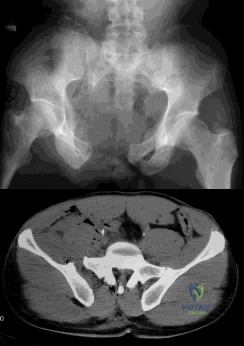
A B Figures 19a and 19b are the CT scans of an 18-year-old man who was a restrained driver in a rollover motor vehicle collision. What was the primary mechanism of injury?
Explanation
This injury pattern represents a flexion distraction injury, or a Chance fracture. The imaging hallmark of this injury is the axial split of the pedicle seen on the sagittal CT scan. This injury necessitates surgical intervention to prevent progressive deformity and pain. A rotation mechanism results in a dislocation with a rotational deformity at the level of injury. An extension force causes failure of the anterior column in tension with compression of the posterior column. An axial load force would result in a burst fracture.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Vaccaro AR, Baron EM, Sanfilippo J, Jacoby S, Steuve J, Grossman E, DiPaola M, Ranier P, Austin L, Ropiak R, Ciminello M, Okafor C, Eichenbaum M, Rapuri V, Smith E, Orozco F, Ugolini P, Fletcher M, Minnich J, Goldberg G, Wilsey J, Lee JY, Lim MR, Burns A, Marino R, DiPaola C, Zeiller L, Zeiler SC, Harrop J, Anderson DG, Albert TJ, Hilibrand AS. Reliability of a novel classification system for thoracolumbar injuries: the Thoracolumbar Injury Severity Score. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S62-9; discussion S104. PubMed PMID:16685239.View Abstract at PubMed
Question 34
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?

Explanation
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds
Question 35
What is the most common reason an individual with a malignant soft-tissue tumor in the extremities seeks medical attention?
Explanation
REFERENCES: Brouns F, Stas M, De Wever I: Delay in diagnosis of soft tissue sarcomas. Eur J Surg Oncol 2003;29:440-445.
Rougraff B: The diagnosis and management of soft tissue sarcomas of the extremities in the adult. Curr Probl Cancer 1999;23:1-50.
Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 36
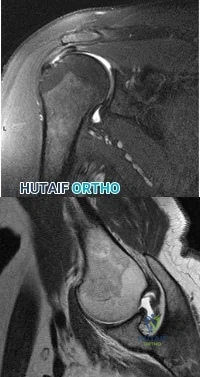
-Images from an MRI scan of this patient’s left hip are shown in Figure 30c through 30e. What is the most likely cause of his acute pain?
Explanation
This patient has cam-type femoroacetabular impingement. Decreased internal rotation and a positive impingement test (forced flexion, adduction, and internal rotation) are classic findings. The lack of pain with resisted hip flexion makes hip flexor strain unlikely, and the lack of tenderness at the greater trochanter renders trochanteric bursitis unlikely. Although athletic pubalgia can be a source of longstanding groin pain, he lacks the pain with a resisted sit-up and tenderness along the pubic ramus that is frequently noted in patients with pubalgia. His radiographs reveal a focal femoral neck prominence consistent with cam impingement, although pistol grip deformities and flattening of the lateral femoral head are often present as well. His MRI scan shows a labral tear, which is common in cam impingement.Surgical treatment for cam impingement can be effective for symptomatic patients. Even among highlevel athletes, open surgical dislocation of the hip has been shown to have good results. Most patients with cam impingement can be treated with arthroscopic osteoplasty and achieve results comparable to those realized with open surgical dislocation. The literature describes success in terms of athletes returning to sports (even professional athletes) to be approximately 90% after arthroscopic treatment.Byrd and Jones described 5 patients who developed transient neurapraxias that resolved uneventfully.The patients in his series who had concomitant microfracture had a 92% return to sports within the follow-up period. Cam impingement has long been thought to be associated with a history of a slipped capital femoral epiphysis. The capitis in these patients is displaced posteriorly, resulting in a prominent anterior femoral neck and decreased hip internal rotation. Pincer impingement is associated with a deep acetabulum, such as protrusion acetabula and acetabular retroversion. A patient who underwent a periacetabular osteotomy can develop a more retroverted acetabulum as well.
Question 37
A 12-year-old girl has had progressive left knee pain for the past 4 months. She reports that the pain is unrelated to activity, and she has no history of fever or recent infections. Examination reveals full range of motion of the knee but tenderness along the medial joint line. Plain radiographs and MRI scans are shown in Figures 39a through 39d. A biopsy specimen of the lesion is shown in Figure 39e. Treatment should include
Explanation
REFERENCE: Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 38
A 49-year-old man is seeking a second opinion for continued knee pain and swelling. He went to his primary doctor for swelling "on top of his knee," and he says his doctor drained some clear fluid. He noted that his condition improved for about 1 week before the swelling returned. He now has increasing pain and redness around his kneecap. Examination reveals significant swelling of his prepatellar bursa, with erythema over the bursa that extends to the surrounding skin. His temperature in the office is 101.7°F. What is the next step in treatment for this patient? Review Topic
Explanation
Question 39
A 40-year-old man who is a manual laborer has had 3 years of worsening medial-sided left knee pain that has inhibited his ability to work. He reports undergoing a left subtotal medial meniscectomy 10 years ago. He has been treated with nonsteroidal anti-inflammatory drugs and two different corticosteroids, with the most recent injection given 1 month ago. Each injection provided him with a few weeks of pain control. His medical history is unremarkable, and he has smoked 20 cigarettes per day for the last 15 years. His BMI is 22. On examination, he has varus alignment of the involved leg and medial joint line tenderness and no lateral or patellofemoral pain. His knee range of motion is 3° shy of full extension to 130° of flexion. He has negative Lachman and posterior drawer test results. He demonstrates no lateral thrust with ambulation. The patient is offered a VPHTO. What aspect of his history will determine the most appropriate VPHTO technique?
Explanation
compartment, a trial of a medial unloader brace is appropriate both diagnostically and therapeutically. If unloading the medial compartment resolves the patient’s symptoms, he would be an excellent candidate for an osteotomy. An MRI scan may be obtained to evaluate ligamentous integrity or to evaluate degenerative involvement of the lateral and patellofemoral compartment for presurgical planning of an osteotomy; however, the integrity of the medial meniscus has no clinical importance in a patient with severe medial compartment arthritis. A repeat corticosteroid injection is not indicated within 1 month of his last injection, and referral to pain management is not appropriate with other options available to help this patient. A VPHTO is the appropriate intervention considering the patient’s young age, high-functional occupation, examination, radiographic findings, and response to medial unloader bracing. A revision knee arthroscopy would be appropriate for a recurrent medial meniscus tear, but not appropriate in a patient with severe medial compartment arthritis. The patient’s young age and high functional requirements are contraindications to TKA. The presence of severe arthritis is a contraindication to medial meniscus transplant. The patient is a candidate for a VPHTO. The technical options include a medial opening-wedge or a lateral closing-wedge osteotomy. Both techniques have advantages and disadvantages; however, a medial opening-wedge osteotomy is contraindicated in a smoker because of concern for nonunion. As a result, current smoking history is the only factor listed that would influence the technique used. The history of prior arthroscopy has no relevance in the decision about which type of osteotomy is appropriate. Normal BMI is between 18.5 and 24.9, so this patient’s BMI is considered normal and would not affect the surgical technique (if this patient were obese, a lateral closing-wedge osteotomy would be considered, but this is controversial). His age of 40 years is an indication for HTO but does not influence technique.
Question 40
Figures 1 through 3 are the weight-bearing radiograph and MRI scans of a 27-year-old man who twisted his knee coming down awkwardly from a lay-up during a basketball game. He felt a sharp stabbing pain in the posterior aspect of his knee at the time of the injury. Physical examination reveals a trace effusion, full range of motion but pain with hyperflexion >90° degrees and tenderness over the affected joint line. What is the most appropriate treatment at this time?

Explanation
root tears lead to progressive degenerative changes as a result of the altered tibiofemoral contact pressures and areas. Nonsurgical treatment including injections, physical therapy, and unloader braces are more appropriate in the older patient with pre-existing advanced degenerative changes.
Question 41
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. Radiographs of the player’s right ankle confirm there are no fractures. With a lateral talar tilt test result of 19°, which additional structure is most likely damaged?
Explanation
anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
Question 42
Figure 11 shows the radiograph of a 26-year-old man with type I diabetes mellitus who was struck by a motor vehicle. What is the most common complication associated with this pelvic fracture?
Explanation
REFERENCES: Geerts WH, Code KI, Jay RM, et al: A prospective study of venous thromboembolism after major trauma. N Engl J Med 1994;331:1601-1606.
Steele N, Dodenhoff RM, Ward AJ, et al: Thromboprophylaxis in pelvic and acetabular trauma surgery: The role of early treatment with low-molecular-weight heparin. J Bone Joint Surg Br 2005;87:209-212.
Question 43
…What is the etiology of the pain associated with this lesion?
Explanation

Question 44
It has been shown that bisphosphonate-based supportive therapy (pamidronate or zoledronate) reduces skeletal events (onset or progression of osteolytic lesions) both in patients with multiple myeloma and in cancer patients with bone metastasis. The use of biphosphonate therapy has been associated with Review Topic
Explanation
Question 45
Figures 87a and 87b are the radiographs of an 18-year-old pedestrian who was struck by a car. During intramedullary nailing, it is difficult to maintain proper alignment. Poller blocking screws placed in the proximal fragment at which position(s) relative to the nail can help prevent the typical deformity?

Explanation
Question 46
During anatomic medial patellofemoral ligament (MPFL) reconstruction, the surgeon notes that the graft is becoming too tight with greater knee flexion. What is the most likely cause?
Explanation
Question 47
What is the most frequent late complication of cementless fixation in total knee arthroplasty?
Explanation
REFERENCES: Peters PC, Engh GA, Dwyer KA, Vinh TN: Osteolysis after total knee arthroplasty without cement. J Bone Joint Surg Am 1992;74:864-876.
Parks NL, Engh GA, Topoleski LDT, Emperado J: Modular tibial insert micromotion: A concern with contemporary knee implants. Clin Orthop 1998;356:10-15.
Question 48
A 54-year-old woman with idiopathic carpal tunnel syndrome undergoes open carpal tunnel release with a flexor tenosynovectomy. The pathology from the tenosynovium is likely to show
Explanation
REFERENCES: Shum C, Parisien M, Strauch RJ, et al: The role of flexor tenosynovectomy in the operative treatment of carpal tunnel syndrome. J Bone Joint Surg Am 2002;84:221-225.
Fuchs PC, Nathan PA, Myers LD: Synovial histology in carpal tunnel syndrome. J Hand Surg Am 1991;16:753-758.
Kerr CD, Sybert DR, Albarracin NS: An analysis of the flexor synovium in idiopathic carpal tunnel syndrome: Report of 625 cases. J Hand Surg Am 1992;17:1028-1030.
Question 49
A polytrauma patient underwent the following procedures: (1) statically locked intramedullary nailing for a right femoral shaft fracture; (2) open reduction with plate-and-screw fixation [ORIF] for a right simple distal fibula fracture; (3) ORIF right middle third radius and ulna fracture; and (4) ORIF left humeral shaft fracture. What is the appropriate weightbearing status for this patient? Review Topic
Explanation
Tingstad et al. examined the effect of immediate weightbearing on plated fractures of the humeral shaft. They reported that immediate weightbearing on humeral shaft fractures, treated with plating and full weightbearing, did not have any negative effect on the union or malunion rates.
Brumback et al. evaluated the feasibility, safety and efficacy of immediate weightbearing after treatment of femoral shaft fractures with statically locked IM nail. Using biomechanical and clinical data, they showed that all fractures united with no loss of fixation or hardware failure.
Starkweather et al. retrospectively assessed the complications and loss of reduction in patients who bore weight in a short leg cast within 15 days after surgical repair of acute unilateral closed ankle fractures. Of the 81 ankle fracture radiographs, 80 (98.8%) showed no displacement in fracture reduction on the final follow-up examination. These results suggest early protected weightbearing may be safe.
Incorrect Answers:
Question 50
Figure 54 is the lateral radiograph of a 55-year-old man who is evaluated for a 2-year history of pain and stiffness of his right metatarsophalangeal (MTP) joint. Upon examination he has dorsal bossing, severe crepitation, and pain with passive range of motion. There is pain with the "grind" test. Dorsiflexion is limited to 0 degrees. No sesamoid tenderness is present. What is the most appropriate surgical treatment?

Explanation
The radiograph reveals end-stage degenerative changes of the first MTP joint with a dorsal loose body. MTP arthritis and decreased joint dorsiflexion is referred to as hallux rigidus. A chevron bunionectomy is used to correct hallux valgus deformity without arthritis. The cheilectomy is used in lesser degrees of joint destruction. Resection of the proximal phalanx results in a floppy toe and is generally not recommended.
RECOMMENDED READINGS
McNeil DS, Baumhauer JF, Glazebrook MA. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013 Jan;34(1):15-32. doi: 10.1177/1071100712460220. Review. PubMed PMID: 23386758.
View Abstract at PubMed
Deland JT, Williams BR. Surgical management of hallux rigidus. J Am Acad Orthop Surg. 2012 Jun;20(6):347-58. doi: 10.5435/JAAOS-20-06-347. Review. PubMed PMID: 22661564.
View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 55 THROUGH 58
Figures 55a and 55b are the anteroposterior and lateral radiographs of a 57-year-old man who fell off of a ladder 10 days ago and landed on his left foot. He is now unable to weight bear on the left. He has no history of trauma to this foot, and his medical history is unremarkable. Upon examination his left foot is swollen and tender. Pulses and sensation are intact.

A B
Question 51
A 12-year-old boy with hemophilia A and no known inhibitors sustains a tibia fracture and has pain with passive motion of the deep toe flexors. Appropriate management should consist of
Explanation
REFERENCES: Dumontier C, Sautet A, Man M, Bennani M, Apoil A: Entrapment and compartment syndromes of the upper limb in haemophilia. J Hand Surg Br 1994;19:427-429.
Carr ME Jr, Loughran TP, Cardea JA, Smith WK, Kuhn JG, Dottore MV: Successful use of recombinant factor VIIa for hemostasis during total knee replacement in a severe hemophiliac with high-titer factor VIII inhibitor. Int J Hematol 2002;75:95-99.
Chuansumrit A, Isarangkura P, Angchaisuksiri P, et al: Controlling acute bleeding episodes with recombinant factor VIIa in haemophiliacs with inhibitor: Continuous infusion and bolus injection. Haemophilia 2000;6:61-65.
Question 52
1 and 2 show the radiograph and CT obtained from a year-old woman who underwent right total hip replacement in She initially did well with no pain. She was last seen 7 years ago and was having mild hip pain at that time. She was found to have a supra-acetabular cyst on radiographs. She has had severe right hip pain for the past 9 months while using a walker for ambulation. The initial blood work reveals an estimated erythrocyte sedimentation rate of 32 mm/hr, a C-reactive protein level of 5 mg/L, a serum cobalt level of 4 µg/L, and a serum chromium level of 6 µg/L. Right hip aspiration is performed, revealing a white blood cell count of 139, 52% neutrophils, and a negative leukocyte esterase test. What is the best next step?
Explanation
The hip replacement was performed in 1995, during the period when the previous generation of polyethylene was utilized. This polyethylene was subjected to irradiation in air, with subsequent oxidation and consequent osteolysis after implantation. The mechanism of osteolysis begins with the uptake of polyethylene particles by macrophages, which then initiate an inflammatory cascade and the release of osteolytic factors. This cycle continues, with eventual implant loosening and failure. The imaging shows significant osteolysis and raises concern for pelvic discontinuity and acetabular implant failure. The surgical treatment consists of acetabular reconstruction. In this patient, concern exists for discontinuity based on the substantial amount of bone loss and nonsupportive anterior and posterior columns. This scenario requires complex acetabular revision using a custom triflange device, distraction with a jumbo acetabular component, or placement of a porous metal cup/cage construct with augmentation. The laboratory values are not consistent with infection or failure due to metal debris.
Question 53
A 3-year-old boy sustains a complete paralysis following a high thoracic spinal cord injury consistent with a SCIWORA-type injury (spinal cord injury without radiographic abnormality). Subsequent progressive spinal deformity will develop in what percent of patients with this injury?
Explanation
REFERENCES: Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411.
Lancourt JE, Dickson JH, Carter RE: Paralytic spinal deformity following traumatic spinal cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
Dearolf WW III, Betz RR, Vogel LC, Levin J, Clancy M, Steel HH: Scoliosis in pediatric spinal cord injured patients. J Pediatr Orthop 1990;10:214-218.
Question 54
A 13-year-old girl who is 2 years postmenarche has been referred for management of scoliosis. She denies any history of back pain. Radiographs show a right thoracic curve of 35°. She has a Risser sign of 4 and a bone age of 15.5 years. Management should consist of
Explanation
REFERENCES: Lonstein JE, Carlson JM: The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am 1984;66:1061-1071.
Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1993, pp 447-459.
Question 55
Which of the following is an advantage of computer-assisted navigation used to place medullary nail interlocking screws compared to a freehand techinque?

Explanation
Ricci et al compared two fluoroscopic navigation tracking technologies, optical and electromagnetic versus standard freehand fluoroscopic targeting, in a standardized foam block model for placement of interlocking screws. They found that fluoroscopy time (seconds) and number of fluoroscopy images were significantly less when using the computer-guided systems than for freehand-unguided insertion. Average distance of pin placement from the target in the foam blocks was significantly greater for controls than for each of the navigated systems.
Suhm et al performed a prospective controlled clinical study to compare fluoroscopic guidance with fluoroscopy-based surgical navigation for distal locking of intramedullary implants. The surgical navigation group showed increased procedure time, but equivalent precision with reduced radiation exposure. There was no significant difference in the technical reliability between both groups.
Question 56
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
REFERENCES: Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 57
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
REFERENCES: O’Driscoll SW, Morrey BF: Elbow arthroscopy, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 21-34.
Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 58
A 44-year-old patient who has had a proximal first metatarsal osteotomy has recurrent pain and difficulty wearing many types of shoes. Radiographs show a large 1-2 intermetatarsal angle (IMA).
Explanation

Question 59
Figure 31 shows the AP and lateral radiographs of the elbow of a 56-year-old man with chronic polyarticular rheumatoid arthritis. His function continues to be limited by pain with activities of daily living. Examination shows that his total arc of motion is 110 degrees. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Morrey BF, Adams RA: Capitellocondylar total elbow replacement in rheumatoid arthritis. J Bone Joint Surg Am 1992;74:479-490.
Question 60
The wear resistance of ultra-high molecular weight polyethylene can be improved by exposing the polymer to high-energy radiation (eg, gamma or electron beam), followed by a thermal treatment. What is one detrimental side effect of this process?
Explanation
REFERENCES: Collier JP, Currier BH, Kennedy FE, et al: Comparison of cross-linked polyethylene materials for orthopaedic applications. Clin Orthop 2003;414:289-304.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 203-208.
Wright TM, Maher SA: Biomaterials, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 61
…Giant-cell tumor of bone usually involves the epiphysis of long bones. What is the next most common type of tumor involving this anatomical location?
Explanation
Figures 71a through 71e are the radiographs, MRI scan, and CT scans of a 14-year-old-boy who has cyclical pain in his thigh. His symptoms began approximately 6 months ago. He complains of increased pain when he runs and also of pain that wakes him at night. This pain is relieved by nonsteroidal anti-inflammatory drugs (NSAIDs).

Question 62
Patient outcome after open reduction and internal fixation of tibial plateau fractures shows that patients older than 50 years of age when compared to younger patients have
Explanation
Question 63
Flow cytometry of tumors measures the
Explanation
Question 64
Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management should consist of
Explanation
REFERENCES: Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Pemberton PA: Pericapsular osteotomy of the ilium for the treatment of congenital subluxation and dislocation of the hip. J Bone Joint Surg Am 1965;47:65-86.
Question 65
Figure A is a pelvic radiograph of a healthy 20-month old girl with a limb leg discrepancy. A hip arthrogram under general anesthesia reveals concentric reduction of the left hip ONLY when the hip is positioned in 70 to 80 degrees of abduction. The next best step in treatment would be: Review Topic

Explanation
capsulorrhaphy, +/- femoral osteotomy +/- pelvic osteotomy
In children older than 18 months, open reduction is the preferred treatment for hip dysplasia. Open reduction is also considered when concentric closed reduction cannot be achieved or when excessive abduction (>60 degrees) is required to maintain reduction (due to increasing risk of avascular necrosis). The goal of open reduction is to remove the blocks to reduction and to increase stability by preforming soft-tissue or bone procedures.
Wenger et al. reviewed the surgical treatment of DDH. They say that the impediment to congruent reduction are the iliopsoas muscle, joint capsule, ligamentum teres, pulvinar, labrum, and transverse acetabular ligament. The most commonly used approaches are anterior and medial/anteromedial to the hip.
Gholve et al. reviewed DDH and the factors that contribute to secondary procedures. In their study, neither age nor unilateral vs bilateral dislocation had a direct influence on the outcome or the need for secondary procedures. The variable that significantly influenced the need for a secondary procedure was the concomitant use of a femoral osteotomy during initial surgical treatment. Of the 27 patients who did not have concurrent femoral osteotomy at index surgery, 19/27 (73%) required a secondary procedure (P<0.001).
Figure A shows an AP pelvic radiograph of an infant. Focusing on the left hip, there is lateral and superior subluxation of the femoral head, with the femoral head lateral to Perkin's line. The medial joint space is increased. The acetabular index is increased
>30 degrees. Shenton's line is disrupted. These are all features of DDH.
Incorrect Answers:
Question 66
Mutations of what gene are associated with subsequent development of osteosarcoma?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 4.
Scholz R, Kabisch H, Delling G, Winkler K: Homozygous deletion within the retinoblastoma gene in a native osteosarcoma specimen of a patient cured of a retinoblastoma of both eyes. Pediatr Hematol Oncol 1990;72:65.
Hovig E, Lothe R, Farrants G, et al: Chromosome thirteen alterations in osteosarcoma cell lines derived from a patient with previous retinoblastoma. Cancer Genet Cytogenet 1991;57:31-40.
Question 67
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?
Explanation
REFERENCES: Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Tewes DP, Fischer DA, Fritts HM, et al: MRI findings of acute turf toe: A case report and review of anatomy. Clin Orthop 1994;304:200-203.
Question 68
The risk of local recurrence after surgical resection of a soft-tissue sarcoma is most closely related to
Explanation
REFERENCES: Lewis JJ, Leung D, Heslin M, Woodruff JM, Brennan MF: Association of local recurrence with subsequent survival in extremity soft tissue sarcoma. J Clin Oncol 1997;15:646-652.
Meterissian SH, Reilly JA Jr, Murphy A, Romsdahl MM, Pollock RE: Soft-tissue sarcomas of the shoulder girdle: Factors influencing local recurrence. Distant metastases and survival. Ann Surg Oncol 1995;2:530-536.
Question 69
Figures 1 and 2 show the intraoperative photographs obtained from a man who is undergoing open reduction and internal fixation of a fifth carpometacarpal joint fracture dislocation. If the structure marked with an arrow in Figure 2 is cut, the patient can expect to experience
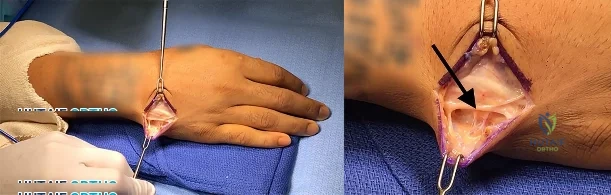
Explanation
The arrow in Figure 2 marks the dorsal sensory branch of the ulnar nerve. Injury to this nerve results in sensory loss of the dorsal ulnar palm and the dorsal small and ring finger digits. The dorsal sensory branch of the ulnar nerve exits the main ulnar nerve at an average distance of 8.3 cm from the proximal border of the pisiform. It becomes subcutaneous on the ulnar aspect of the forearm at an average distance of 5
cm from the proximal edge of the pisiform. It then travels dorsal to the extensor carpi ulnaris tendon to innervate the dorsal ulnar hand and the dorsal ring and small digits. Injuries to this nerve can occur from open and arthroscopic procedures (such as triangular fibrocartilage complex repair) as well as from procedures requiring percutaneous pinning. Care must be taken to identify and protect this nerve to avoid the complications of numbness and possible neuroma formation. The inability to extend the small finger would be caused by an injury to the extensor tendon(s) in this area, and the inability to abduct the small finger would require an injury to the abductor digiti minimi muscle/tendon unit or the ulnar nerve motor branch, which is located on the volar aspect of the proximal palm. Clawing of the small and ring fingers would be caused by absent intrinsic function due to an injury to the ulnar motor nerve branch located on the volar proximal palm.
Question 70
- A 55 year-old man has multiple lytic lesions in the humeri, clavicles, and scapulae. Which of the following diagnostic studies best confirms a diagnosis of multiple myeloma?
Explanation
Question 71
A 53-year-old man reports acute, severe left shoulder pain after undergoing abdominal surgery 10 days ago. Initial management, consisting of anti-inflammatory drugs, physical therapy, and a subacromial injection of corticosteroid, fails to provide relief. Reexamination of the shoulder 2 months after the onset of symptoms reveals atrophy of the infraspinous and supraspinous fossa and profound weakness of active abduction and external rotation. His neck is supple with a full range of motion. Plain radiographs and an MRI scan of the shoulder are normal. What diagnostic study should be performed next in the evaluation of this patient?
Explanation
In this patient, the injury is most likely caused by traction or compression of the nerve in the suprascapular notch as the result of positioning during abdominal surgery; therefore, the studies of choice are electromyography and nerve conduction velocity studies. While MRI of the cervical spine may be of some value in ruling out a radiculopathy, the clinical history does not support such a cause for this condition.
REFERENCES: Rengachary SS, Neff JP, Singer PA, Brackett CE: Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 1: Clinical study. Neurosurgery 1979;5:441-446.
Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H: Suprascapular entrapment neuropathy: A clinical, anatomical and comparative study. Part 2: Anatomical study. Neurosurgery 1979;5:447-451.
Bigliani LU, Dalsey RM, McCann PD, April EW: An anatomical study of the suprascapular nerve. Arthoscopy 1990;6:301-305.
Question 72
Figure 3 is the clinical photograph of a 20-year-old college soccer player who has a 7-day history of worsening left ankle pain and swelling after being slide-tackled in a game. Radiograph findings of his ankle and foot are normal. He complains of malaise. His history includes a severe ankle sprain 3 months ago. The sprain caused him to miss half the season, but he was able to play in the last 2 games. What is the most appropriate treatment? Review Topic

Explanation
Question 73
A 67-year-old woman has a painful, arthritic proximal interphalangeal (PIP) joint, and nonsurgical measures have failed to improve the pain. What implant and joint replacement approach combination has been demonstrated to have the lowest rate of revision surgery?
Explanation
A recent systematic review compared silicone replacement, pyrocarbon replacement, and surface replacement arthroplasty for PIP arthritis. Silicone arthroplasty through a volar approach showed the greatest gains in arc of motion and had the lowest rate of revision surgeries. The rates of revision surgeries from low to high for each type of arthroplasty were 6% for silicone volar, 10% for silicone lateral, 11%
Surface replacement arthroplasty through a volar
for silicone dorsal, 18% for surface replacement dorsal, and 37% for surface replacement volar. Revision surgeries include implant replacement (to silicone or maintaining the surface replacement), arthrodesis, explantation, amputation, and other procedures.
approach showed the highest revision rate, the worst gain in arc of motion, and the greatest extension lag. However, substantial pain relief and higher satisfaction still were reported after surface replacement arthroplasty, regardless of the complications.
Question 74
A 45-year-old woman has severe anterior knee pain. Her radiographs indicate end-stage patellofemoral compartment osteoarthritis. The tibiofemoral compartments are preserved. Extensive nonsurgical treatment has failed to provide relief, and she is offered patellofemoral arthroplasty (PFA). What is the most common long-term mode of failure for PFA using an implant with an onlay prosthesis design?
Explanation
Contemporary onlay-design trochlear prostheses in PFA replace the entire anterior trochlear surface. Previous inlay designs were inset within the native trochlea and carried a higher risk of catching and patellar instability, particularly in patients with trochlear dysplasia; they also generally have higher failure rates. The current most common mode of failure is progression of arthritis throughout the knee, in some series as high as 25% at 15 years. Aseptic loosening, particularly of cemented implants, is less common. Infection is an uncommon long-term complication. Patients considering PFA should be advised of the risk of arthritis progression. Many authors routinely obtain a preoperative MRI to assess the status of the tibiofemoral compartments.
Question 75
Figures 48a and 48b are the initial radiograph and clinical photograph of a 21-year-old woman who sustained a severe mangling injury to her left foot in a rollover ATV crash. After multiple dTbridements, she underwent definitive transmetatarsal amputation with split-thickness skin graft. She did have intact plantar sensation. Figure 48c shows the clinical photograph 10 days after amputation. Her wounds healed without infection and she did not require further surgery. At 2 years after injury, which of these factors is most likely to be associated with improved level of satisfaction? Review Topic

Explanation
and education level do not predict patient satisfaction. Instead, the most important predictors of patient satisfaction at 2 years after injury include the ability to return to work, absence of depression, faster walking speed, and decreased pain.
(SBQ12TR.26) A 44-year-old male presents after being struck by a car. He is hypotensive, and has an obvious open tibia and a closed femoral shaft fracture. A pelvic radiograph is obtained and shown in Figure A. A representative CT scan image in shown in Figure B. The patient is placed in a pelvic binder, and his blood pressure normalizes with crystalloid and a blood transfusion. He then undergoes pelvic angiography, and his internal iliac artery is embolized. Which of the following definitive treatment options is most appropriate in this case? Review Topic
Anterior pelvic external fixation with pins placed in the AIIS and a posterior sacroiliac screw
Open reduction and internal fixation of the pubic symphysis with a two hole plate and posterior fixation with a iliosacral screw
Open reduction and internal fixation of the pubic symphysis with a non-locking multi-hole plate and posterior fixation with a iliosacral screw
Anterior pelvic external fixation and posterior triangular osteosynthesis
Open reduction and internal fixation of the pubic symphysis with a locked multi-hole plate and posterior sacral plate fixation
The radiographs and CT scan show a fracture pattern consistent with an APC-III injury. This is most appropriately treated with pubic symphysis ORIF with a multi-hole plate and posterior iliosacral screw fixation.
APC-III pelvic ring injuries are associated with with disruption of the anterior and posterior SI ligaments (SI dislocation) as well as disruption of sacrospinous and sacrotuberous ligaments. They are commonly associated with vascular injury and retroperitoneal bleeding.
Sagi et al studied the radiographic and clinical outcome of symphyseal plating techniques, specifically comparing two hole (THP) vs multi-hole plating (MHP). Retrospective review of charts and radiographs immediately after the index procedure to latest follow-up was performed. When comparing the 2 different methods of anterior fixation, they found that the rate of fixation failure was greater in group THP (33%) than group MHP (12%). When evaluating the presence of a malunion as a result of these 2 treatment methods, there were more present in the THP group (57%) than in the MHP group (15%). On the basis of these findings, the authors recommended multi-hole plating of unstable pubic symphyseal disruptions.
Grimshaw et al performed a biomechanical study to determine the failure risk and potential benefit to use of locked fixation constructs in simulated pelvic ring injuries. The authors used a six-hole 3.5-mm plate specifically designed for the symphysis pubis with the capability of fixation in locked or unlocked mode, six pelves were fixed with locked screws and six pelves were fixed standard unlocked bicortical screws. Biomechanical testing was performed, and no abrupt failures were noted. However, locked plating of the pubic symphysis did not appear to offer any advantage over the standard unlocked technique
Illustrations A, B, and C show the AP, outlet, and inlet postoperative radiographs. Incorrect Answers:
1,4-Anterior pelvic fixation is typically not used as definitive treatment of these
injuries unless performed in a damage-control setting. The patient in this case is stable.
2-Multi-hole plate fixation of the pubic symphysis is preferred over 2-hole plate fixation.
5-Posterior sacral plating is not indicated in this fracture pattern, as there is no significant sacral comminution of vertical shear component. Furthermore, no distinct advantage has been found with locked symphyseal plating.
Question 76
Among the options listed below, what is the best treatment for the complication shown in Figure 10c?
Explanation
Proximal femur fractures can be treated using a variety of implants including intramedullary nails, blade plates, and locking plates (now precontoured proximal femur plates). The comminution and lack of medial cortical support may predispose these fractures to nonunion.
The recent popularity of locking plates for proximal femur treatment has increased their use for this fracture; however, a disproportionately high rate of failure of these plates, including early implant failure with plate and screw breakage, cut out with varus collapse, and nonunion have been reported.?
Malreduction predisposes these fractures to failure. The initial postoperative radiographs do not reveal a varus malreduction because the tip of the greater trochanter is below the center of the femoral head.
Once failure occurs, the best fixation method among the options detailed is an intramedullary nail (second generation with screws into the femoral head) and restoration of alignment. THA is usually not recommended for treatment of subtrochanteric femur fractures in young patients.
RECOMMENDED READINGS
Wirtz C, Abbassi F, Evangelopoulos DS, Kohl S, Siebenrock KA, Krüger A. High failure rate of trochanteric fracture osteosynthesis with proximal femoral locking compression plate.
Injury. 2013 Jun;44(6):751-6. doi: 10.1016/j.injury.2013.02.020. Epub 2013 Mar 21. PubMed PMID: 23522837. View Abstract at PubMed
Floyd JC, O'Toole RV, Stall A, Forward DP, Nabili M, Shillingburg D, Hsieh A, Nascone JW. Biomechanical comparison of proximal locking plates and blade plates for the treatment of comminuted subtrochanteric femoral fractures. J Orthop Trauma. 2009 Oct;23(9):628-33. doi: 10.1097/BOT.0b013e3181b04835. PubMed PMID: 19897983. View Abstract at PubMed Glassner PJ, Tejwani NC. Failure of proximal femoral locking compression plate: a case series. J Orthop Trauma. 2011 Feb;25(2):76-83. doi: 10.1097/BOT.0b013e3181e31ccc.
PubMed PMID: 21245709. View Abstract at PubMed
Question 77
- A right-handed 35-year old man who underwent a Putti-Platt repair for recurrent anterior instability 20 years ago now has increasing shoulder pain and stiffness. Examination of the shoulder reveals internal rotation to the posterior superior iliac spine and external rotation to 10 degrees with the shoulder adducted. The supraspinatus and infraspinatus are moderately atrophied. What is the most likely diagnosis?
Explanation
Question 78
What percent of adult patients with rheumatoid arthritis test positive for rheumatoid factor?
Explanation
Question 79
The MRI scans and diagnostic ultrasound shown in Figures 2a through 2c show what pathologic condition? Review Topic
Explanation
Question 80
Figures 24a and 24b are the radiographs of a 7-year-old boy who fell off the monkey bars and has a closed injury. His hand appears warm and well perfused with an absent radial pulse. What is the best initial treatment?
Explanation
In displaced extension-type supracondylar fractures, the neurovascular structures get kinked anteriorly or anteromedially related to the displacement. In almost all cases, there is a spontaneous resolution of this kink following closed fracture reduction.
Question 81
A 13-year-old gymnast presents with ongoing knee pain for the past few months. She tried conservative measures including kinesiotaping, physical therapy and rest. On physical exam, she has normal valgus alignment, negative patellar tilt and discomfort with resisted open chain knee extension. A representative radiographs are shown in Figure A-C. What is the most likely clinical diagnosis? Review Topic

Explanation
Evaluation of a patient with patellofemoral pain requires a physical examination and plain radiographs. Appropriate examination of all structures around the knee is critical to rule out other diagnoses. An MRI is useful for evaluating intra-articular or intra-osseous lesions, if clinical suspicion is suggestive of this. Treatment is predominantly conservative, with focus on low impact exercises that maximize aerobic conditioning.
Earl et al. review the epidemiology, etiology and management of patellofemoral syndrome. They note that there is no clear cause of this issue, although issues related to the quadriceps and dynamic malalignment may be contributory.
Outerbridge et al. describe overuse injuries in the young athletic patient. They provide an overview of diagnosis and management specific to this patient population.
Figures A, B and C show AP, lateral and merchant radiographs of a normal knee in a skeletally immature individual. No osseous abnormalities are identified.
Incorrect
Question 82
Figures 12a and 12b show the radiographs of a 56-year-old man with diabetes mellitus who has had left foot swelling with no pain for the past several weeks. He denies any history of trauma. Examination reveals warmth, moderate swelling, no tenderness, and mild pes planus with standing. Pulses are palpable, and his sensory examination is grossly intact to light touch. Standing radiographs are shown in Figures 12c and 12d. What is the most likely diagnosis?
Explanation
REFERENCES: Brodsky JW: The diabetic foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 895-969.
Myerson MS: Diabetic neuroarthropathy, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 439-465.
Question 83
Which of the following best describes heat stroke? Review Topic
Explanation
Question 84
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Explanation
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Question 85
When performing a long fusion to the sacrum in an osteopenic patient in whom optimal sagittal balance is restored, which of the following is a benefit of extending the distal fixation to the pelvis, rather than the sacrum alone? Review Topic
Explanation
Question 86
The mother of a 2-year-old boy reports that he had pain in the right hip all night and refuses to walk on the leg this morning. He is afebrile. Examination reveals pain on hip extension and adduction, but he is able to internally and externally rotate the hip approximately 20 degrees in each direction without pain. Laboratory studies reveal a WBC count of 7,400/mm 3 , with 62% polymorphonuclear neutrophil leukocytes. The AP radiograph shown in Figure 15 reveals a left teardrop distance of 8 mm, while the right side measures 10 mm. Which of the following diagnostic studies will best help confirm the diagnosis?
Explanation
REFERENCE: Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990, pp 1415-1435.
Question 87
A 22-year-old javelin thrower reports that he has had increasing discomfort in his right elbow and loss of distance from his throws for the past 3 months. Examination reveals tenderness over the medial elbow. Application of valgus torque to the elbow through a passive range of motion elicits pain from 70 degrees to 120 degrees of flexion, with no pain at the limits of extension. What structure is primarily responsible for the patient's symptoms? Review Topic
Explanation
is a secondary stabilizer at 30 degrees of flexion, and not susceptible to valgus load when the anterior bundle is intact. The annular ligament and triceps insertion are not involved with medial instability of the elbow. Olecranon osteophytes likely cause pain in terminal extension of the elbow.
Question 88
A 12-year-old girl with juvenile rheumatoid arthritis (JRA) has had chronic pain and synovitis about the knee that is now well-controlled medically. Examination reveals 20° of valgus at the knee. Knee range of motion shows 10° to 90° of flexion. Treatment should consist of
Explanation
REFERENCE: Rydholm U, Brattstrom H, Bylander B, Lidgren L: Stapling of the knee in juvenile chronic arthritis. J Pediatr Orthop 1987;7:63-68.
Question 89
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. What is the most likely area of injury?
Explanation
Question 90
Osteophyte formation at the posteromedial olecranon and olecranon articulation in high-caliber throwing athletes is most often the result of underlying
Explanation
REFERENCES: Conway JE, Jobe FW, Glousman RE, Pink M: Medial instability of the elbow in throwing athletes: Treatment by repair or reconstruction of the ulnar collateral ligament. J Bone Joint Surg Am 1992;74:67-83.
Wilson FD, Andrews, JR, Blackburn TA, McCluskey G: Valgus extension overload in the pitching elbow. Am J Sports Med 1983;11:83-88.
Question 91
An 8-year-old boy with moderate factor VIII hemophilia played kickball earlier in the day and now reports progressively severe groin pain and is unable to walk. Examination reveals marked paresthesias over the medial aspect of the distal tibia. What is the most likely diagnosis?
Explanation
REFERENCES: Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 379-426.
Gilbert MS, Radomisli TE: Therapeutic options in the management of hemophilic synovitis. Clin Orthop 1997;343:88-92.
Question 92
The parents of a 14-year-old female soccer player are concerned about any future injury. They have been advised that she has the potential to play for the US Olympic team. They are especially concerned about the anterior cruciate ligament (ACL). What should you advise them? Review Topic
Explanation
Question 93
An acute posterolateral disk herniation at the L4-5 level will most likely affect what nerve root? Review Topic
Explanation
Question 94
Figures 80a and 80b are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test result, trace effusion, and range of motion from 0 to 85 degrees of knee flexion. Which factor is most contributory to his examination findings?
Explanation
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario.
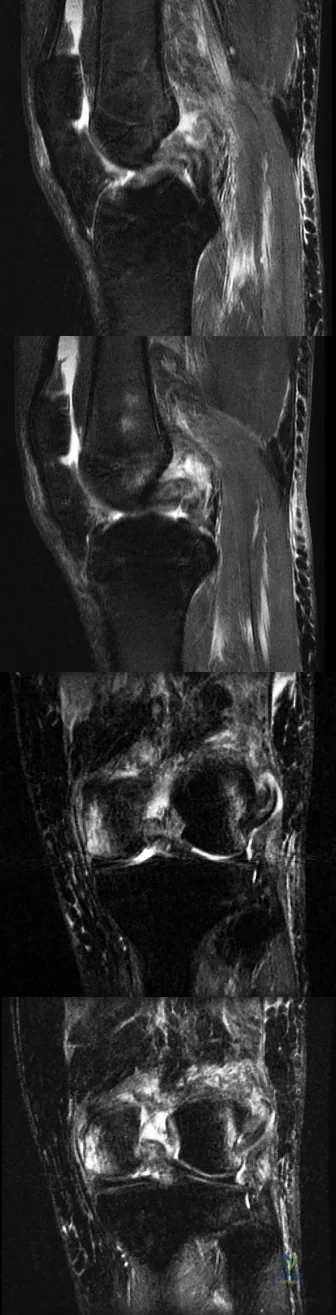
CLINICAL SITUATION FOR QUESTIONS 81 THROUGH 84
Figures 81a through 81d are the MR images of a 25-year-old man with left knee pain after a motorcycle collision. He has palpable pedal pulses with an ankle-brachial index of 0.95. Neurologic examination findings of the injured extremity are normal.
Question 95
A 21-year-old woman has a nontraumatic rupture of the Achilles tendon. Which of the following commonly prescribed medications has been associated with this condition?
Explanation
REFERENCES: van der Linden PD, van de Lei J, Nab HW, et al: Achilles tendinitis associated with fluoroquinolones. Br J Clin Pharmacol 1999;48:433-437.
Bernard-Beaubois K, Hecquet C, Hayem G, et al: In vitro study of cytotoxicity of quinolones on rabbit tenocytes. Cell Biol Toxicol 1998;14:283-292.
Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Question 96
A 20-year-old woman with spastic hemiplegia is evaluated for function and hygiene issues with her right wrist. Her wrist has a resting posture of 90° of flexion and can be passively extended to 65° of flexion. Her fingers are flexed into her palm but can be passively extended with the wrist at 95°. What treatment is likely to provide the most durable result for improved hygiene, function, and cosmesis?
Explanation
The patient has a static deformity of the wrist with a fixed flexion deformity of more than 45°. Soft-tissue procedures such as those referenced in options A and B would not be sufficient to address the degree of contracture. Additionally, Botulinum toxin injections would not provide relief for capsular contractures. Wrist arthrodesis combined with a proximal row carpectomy has been shown to provide a functional and cosmetic alternative for patients with severe wrist flexion contractures.
Question 97
03 An 18 month old child has bilateral “corner fractures” of the distal femoral metaphyses of unknown origin. Following a skeletal survey, the first step in management should consist of
Explanation
back to this question next question
Question 98
The clinical factors shown to most significantly predict the long-term outcome of Perthes disease of the hip include which of the following? Review Topic
Explanation
(SBQ13PE.87) A 4-week-old child is suspected to have classic arthrogryposis, also known as amyoplasia. Clinical examination and hip ultrasound reveal a unilateral, non-reducible, hip dislocation. What do you recommend to reduce the hip? Review Topic
Pavlik harness application
Semi-rigid abduction brace application
Skeletal traction
Early closed reduction and spica casting
Delayed open reduction with or without pelvic and femoral osteotomy
Delayed open reduction with or without pelvic and femoral osteotomy is recommended in the management of unilateral hip deformities associated with amyoplassia. This procedure should be performed at 6-9 months of age. In order to proceed with reduction, there must be a reasonable arc of flexion/extension and active movement of the lower limbs.
Amyoplasia is the most common recognizable form of arthrogryposis. It most commonly occurs as a sporadic symmetric contracture syndrome that is characterized by symmetrical limb involvement, normal to above-average intelligence, and often a midline facial hemangioma. Approximately 80% of children with amyoplasia will have involvement of the hip ranging from soft tissue contractures to unilateral or bilateral hip dislocations.
Bevan et al. reviewed arthrogryposis. They state that open hip reduction is recommended for the management of unilateral dislocation. There is more controversy with regard to the treatment of bilateral hip dislocations. Open reduction can be performed by a medial or anterolateral approach, with or without pelvic and
femoral osteotomy. This procedure is generally delayed for 6-9 months to facilitate the procedure.
Bernstein et al. also reviewed arthrogryposis. They state that the term 'arthrogryposis' encompasses a broad spectrum of diseases, all with the common phenotype of multiple congenital contractures.
Illustration A shows the characteristic features of an infant with severe arthrogryposis. Note the internal rotation of the shoulders, elbow and knee hyperextension, flexed and ulnarly deviated wrists, flexed finger, external rotation of hips and bilateral clubfeet.
Incorrect answers:
Question 99
Of all the pelvic ring injury types, anteroposterior compression type III pelvic ring injuries have the highest rate of which of the following?

Explanation
Question 100
Kinematic testing of patellofemoral motion demonstrates that malalignment that produces increased Q angle causes a shift of the patella laterally in the trochlear groove and is most pronounced during what phase of the flexion arc? Review Topic
Explanation
