OITE & ABOS Orthopedic Board Exam: Spine, Trauma & Extremities | Part 46

Key Takeaway
This page presents Part 46 of a comprehensive orthopedic board review. It features 100 high-yield, verified MCQs mirroring OITE and ABOS exam formats. Authored by an expert, it's designed for orthopedic residents and surgeons preparing for certification, covering key topics like Deformity, Trauma, Elbow, Hip, Knee, and Tendon. Elevate your exam readiness.
About This Board Review Set
This is Part 46 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 46
This module focuses heavily on: Deformity, Elbow, Hip, Knee, Tendon, Trauma.
Sample Questions from This Set
Sample Question 1: An 18-year-old lacrosse player is diagnosed with infectious mononucleosis. What is the recommendation for return to play? Review Topic...
Sample Question 2: What is the most common complication after distal biceps tendon repair at the elbow?...
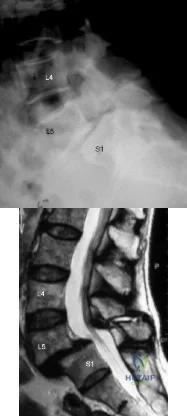
Sample Question 3: Which of the following are considered characteristic features of degeneration of a disk?...
Sample Question 4: A 68-year-old man reports a 4-week history of progressive left-sided lower back and hip pain. The pain is in the posterior buttock region with radiation to the groin and to the left anterior knee region. The pain is aggravated with walking ...
Sample Question 5: What radiographic measurement is best used to assess the adequacy of deformity correction for the patient shown in Figure 22?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An 18-year-old lacrosse player is diagnosed with infectious mononucleosis. What is the recommendation for return to play? Review Topic
Explanation
Question 2
What is the most common complication after distal biceps tendon repair at the elbow?
Explanation
Cain and associates retrospectively reviewed 198 consecutive surgical repairs of the biceps and noted a 36% overall complication rate, including 26% paresthesia of the lateral antebrachial cutaneous nerve, 6% paresthesia of the sensory branch of the radial nerve, 2% superficial infection, 4% injury to the posterior interosseous nerve, 3% symptomatic heterotopic ossification, and 2% rerupture. Grewal and associates randomized 47 patients to have single-incision repair with two suture anchors and 44 patients to have two-incision transosseous suture repair. They reported that the single-incision technique had a higher rate of transient neurapraxia to the lateral antebrachial cutaneous nerve, affecting 19 of 47 in the suture anchor group and three of 43 in the transosseous group. Also, four reruptures occurred, which appeared to be independent of the repair technique. Recordon and associates found only three complications in their series of 46 patients, 19 having endobutton repair and 27 with transosseous suture repair. They reported two injuries to the lateral antebrachial cutaneous nerve and one case of heterotopic ossification. The review by Banerjee and associates showed one rupture of repair (disengagement of the cortical button), two persistent lesions of the superficial branch of the radial nerve, and one symptomatic heterotopic ossification. Co hen remarked that rerupture of the tendon after repair is uncommon in both one-incision and two-incision techniques. Van den Bogaerde and Shin presented a case of posterior interosseous nerve
incarceration with endobutton repair.
Question 3
Which of the following are considered characteristic features of degeneration of a disk?
Explanation
REFERENCES: Happey F, Weissman A, Naylor A: Polysaccharide content of the prolapsed nucleus pulposus of the human intervertebral disc. Nature 1961;192:868.
Naylor A, Shentall R: Biomechanical aspects of intervertebral discs in aging and disease, in Jayson M (ed): The Lumbar Spine and Back Pain. New York, NY, Grune and Stratton Inc, 1976, pp 317-326.
Watkins RG, Collis JS: Lumbar Discectomy and Laminectomy. Rockville, MD, Aspen, 1987, pp 2-3.
Question 4
A 68-year-old man reports a 4-week history of progressive left-sided lower back and hip pain. The pain is in the posterior buttock region with radiation to the groin and to the left anterior knee region. The pain is aggravated with walking and improves with rest. There is no history of previous trauma. Radiographs are seen in Figures 14a and 14b, and MRI scans are seen in Figures 14c through 14e. What is the most appropriate treatment option at this time?
Explanation
REFERENCES: Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2007, pp 339-361.
Spivak JM, Connolly PJ (ed): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 43-56.
Question 5
What radiographic measurement is best used to assess the adequacy of deformity correction for the patient shown in Figure 22?
Explanation
REFERENCES: Carroll K, Coleman S, Stevens PM: Coxa vara: Surgical outcomes of valgus osteotomies. J Pediatr Orthop 1997;17:220-224.
Cordes S, Dickens DR, Cole WG: Correction of coxa vara in childhood: The use of Pauwels’ Y-shaped osteotomy. J Bone Joint Surg Br 1991;73:3-6.
Question 6
A 12-year-old boy sustained a both bone forearm fracture 10 weeks ago and underwent closed reduction and casting. Examination now reveals that the injury is healed, but he is unable to extend his little and ring fingers of the injured hand with his wrist extended. Full extension is possible with the wrist flexed. A radiograph and clinical photograph are shown in Figures 15a and 15b. The remainder of his hand and wrist examination and neurologic evaluation in the hand are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Watson PA, Blair W: Entrapment of the index flexor digitorum profundus tendon after fracture of both forearm bones in a child. Iowa Orthop J 1999;19:127-128.
Shaw BA, Murphy KM: Flexor tendon entrapment in ulnar shaft fractures. Clin Orthop 1996;330:181-184.
Kolkman KA, van Niekerk JL, Rieu PN, et al: A complicated forearm greenstick fracture: Case report. J Trauma 1992;32:116-117.
Hendel D, Aner A: Entrapment of the flexor digitorum profundus of the ring finger at the site of an ulnar fracture: A case report. Ital J Orthop Traumatol 1992;18:417-419.
Question 7
A 21-year-old hockey player who has recurrent shoulder subluxations undergoes an anterior capsulorrhaphy under general anesthesia, and an interscalene block is used to relieve postoperative pain. At the 1-week follow-up examination, he reports loss of sensation over the lateral region of the shoulder and is unable to actively contract the deltoid muscle. The remainder of the examination is normal. What is the best course of action at this time?
Explanation
REFERENCE: Ho E, Cofield RH, Balm MR, et al: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270.
Question 8
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
REFERENCES: Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L’Episcopo transfers in obstetrical palsy: A retrospective review of twenty cases. J Pediatr Orthop 1990;10:442-444.
Hoffer MM, Wickenden R, Roper S: Brachial plexus birth palsies. J Bone Joint Surgery Am 1978;60:692-695.
Question 9
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
REFERENCES: Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Mohler LR, Hanel DP: Closed fractures complicated by peripheral nerve injury. J Am Acad Orthop Surg 2006;14:32-37.
Question 10
Figure 62 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. What is the main function of the structure delineated by the black asterisks? Review Topic
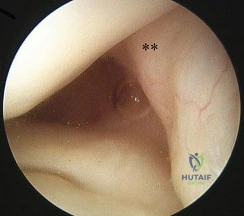
Explanation
Question 11
A 23-year-old man reports a 6-year history of recurrent instability in the right dominant shoulder. He has not undergone surgery and has essentially stopped all of his sporting activities. On examination, he has instability and apprehension in the midrange of motion (abduction of 45 to 60 degrees with external rotation) and a palpable clunk representing a transient dislocation over the anterior glenoid rim. A three-dimensional CT scan is shown in Figure 31. What is the most appropriate surgical intervention to provide him with reliable stability postoperatively?
Explanation
A bony augmentation procedure such as the Lataijet has been well-described to provide a well functioning and stable shoulder joint. A hemiarthroplasty is not indicated in the absence of arthritis. Subscapularis
advancement will not address the bone loss.
REFERENCES: Hovelius L, Sandstrom B, Sundgren K, et al: One hundred eighteen Bristow-Latarjet repairs for recurrent anterior dislocation of the shoulder prospectively followed for fifteen years: Study I— clinical results. J Shoulder Elbow Surg 2004;13:509-516.
Schroder DT, Provencher MT, Mologne TS, et al: The modified Bristow procedure for anterior shoulder instability: 26-year outcomes in Naval Academy midshipmen. Am J Sports Med 2006;34:778-786.
Itoi E, Lee SB, Berglund LJ, et al: The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: A cadaveric study. J Bone Joint Surg Am 2000;82:35-46.
Question 12
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 13
A 65-year-old woman has nausea, vomiting, and abdominal distention after undergoing total knee arthroplasty 48 hours ago. An abdominal radiograph is shown in Figure 14. Associated risk factors for this disorder include
Explanation
REFERENCES: Iorio R, Healy WL, Appleby D: The association of excessive warfarin anticoagulation and postoperative ileus after total joint replacement surgery. J Arthroplasty 2000;15:220-223.
Clarke HD, Berry DJ, Larson DR: Acute pseudo-obstruction of the colon as a postoperative complication of hip arthroplasty. J Bone Joint Surg Am 1997;79:1642-1647.
Question 14
The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?
Explanation
REFERENCES: McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Lister GD, McGregor IA Jackson IT: The groin flap in hand injuries. Injury 1973;4:229.
Question 15
An 8-month-old infant has an infection of the fingertip as shown in Figure 22. If neglected, the anticipated path of ascending infection is the fingertip, the flexor sheath, and the
Explanation
REFERENCES: Peimer CA (ed): Surgery of the Hand and Upper Extremity: Acute and Chronic Sepsis. New York, NY, Mcgraw Hill, 1996, pp 1735-1741.
Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow and Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 445-446.
Question 16
Figure 68 is the radiograph of a 33-year-old runner who recently decided to begin running barefoot on trails. Since his transition to running without shoes 3 months ago, he has been having pain in the second metatarsophalangeal (MTP) joint. He feels like he is walking on a stone, notes edema in the ball of his foot, and has started to see a deviation of the second toe. What is the most likely etiology of these symptoms and findings?

Explanation
Lesser-toe plantar plate injuries are becoming increasingly recognized. Patients typically have an increase in pain, a positive Lachman test result upon examination, and deviation of the MTP joint. On radiograph, MTP subluxation can be appreciated. Nonsurgical treatment with a metatarsal pad may be attempted. Many patients who have surgery will have a partial or full tear of the plantar plate. The repair necessitates reinsertion of the plantar plate to the base of the proximal phalanx.
RECOMMENDED READINGS
Doty JF, Coughlin MJ, Weil L Jr, Nery C. Etiology and management of lesser toe metatarsophalangeal joint instability. Foot Ankle Clin. 2014 Sep;19(3):385-405. doi: 10.1016/j.fcl.2014.06.013. Epub 2014 Jul 10. PubMed PMID: 25129351. View Abstract at PubMed
Nery C, Coughlin MJ, Baumfeld D, Raduan FC, Mann TS, Catena F. Prospective evaluation of protocol for surgical treatment of lesser MTP joint plantar plate tears. Foot Ankle Int. 2014 Sep;35(9):876-85. doi: 10.1177/1071100714539659. Epub 2014 Jun 23. PubMed PMID:
Question 17
Which of the following is not considered to be a part of the constellation of the clinical entities known as the female athlete triad? Review Topic
Explanation
The female athlete triad was coined in 1992 by the American College of Sports Medicine as a complex disorder more prevalent in the adolescent and young female
athlete population including decreased bone mineral density (BMD), menstrual dysfunction, and low energy availability with or without a concomitant eating disorder. Treatment should involve a multidisciplinary approach, including psychological and nutritional counseling for eating behaviors and dietary management, reduction of training intensity to decrease risk of stress fractures, and initiating calcium and vitamin D supplements for osteoporosis.
Nazem et al performed a systematic review of articles containing the female athlete triad, reviewing diagnosis via screening during physical examinations as well as laboratory and imaging evaluation for menstrual dysfunction, low energy availability, and low bone mineral density. They state that potential complications including possible infertility, decreased immune function, cardiovascular disease, and irreversible loss of bone mineral density. They concluded that prevention, early recognition, and a multidisciplinary treatment team with a focus on proper nutrition and natural return of menses is vital.
Nattiv et al review the position of the American College of Sports Medicine regarding the female athlete triad, including screening for the triad at the pre-participation physical, discouragement of unhealthy weight loss practices. Essential members of the multidisciplinary treatment team include a health-care professional, a registered dietitian, and a mental health practitioner. They endorse that the first aim of treatment for any triad component is to increase energy availability by increasing energy intake and reducing exercise energy expenditure.
Question 18
An axial T 1 -weighted MRI scan of the pelvis is shown in Figure 35. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, et al (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System,
ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 19
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4°F (37.4°C), and examination reveals that abduction of the left hip is limited to 30°. Laboratory studies show a WBC of 11,000/mm 3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of
Explanation
REFERENCE: Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1993, pp 505-513.
Question 20
What structure is the primary restraint to inferior translation of the shoulder?
Explanation
REFERENCES: Harryman DTII, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53 -66.
Bigliani LU, Pollock RG, Soslowsky LJ, et al: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 21
A 10‘/2-year-old boy sustained the injury shown in Figure 72 when he fell out of a tree. This is a closed, neurologically intact injury and the patient has no head injury or loss of consciousness. He weighs 115 pounds and is otherwise healthy. What is the optimal treatment option for this injury?
Explanation
REFERENCES: Flynn JM, Schwend RM: Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-359.
Gordon JE, Swenning TA, Burd TA, et al: Proximal femoral radiographic changes after lateral transtrochanteric intramedullary nail placement in children. J Bone Joint Surg Am 2003;85:1295-1301.
Figure 71a Figure 71b Figure 71c Figure 71d
Question 22
Which set of patient characteristics has the highest risk of developing osteonecrosis after an intracapsular femoral neck fracture?
Explanation
Question 23
A 35-year-old man who is an avid weight lifter competing in local tournaments reports new onset pain and loss of motion in his dominant right shoulder. Examination reveals joint line tenderness, active elevation to 100 degrees, and external rotation to 10 degrees. His contralateral shoulder reveals 170 degrees forward elevation and 50 degrees external rotation. Radiographs are shown in Figures 46a and 46b. What is the next most appropriate step in management? Review Topic

Explanation
Question 24
- A 7-year old boy has a painless abductor limp and limited hip abduction. Radiographs show varus of the proximal femur, with a narrow upper femoral epiphysis that has the shape of an inverted "Y". Which of the following factors best predicts the risk that the deformity will become worse?
Explanation
Question 25
A 44-year-old man who sustained an elbow dislocation 3 months ago now reports pain and restricted elbow motion. Radiographs are shown in Figures 27a and 27b. Management should consist of
Explanation
REFERENCES: Jupiter J, Ring D: Treatment of unreduced elbow dislocation with hinged external fixation. J Bone Joint Surg Am 2002;84:1630-1635.
Moro JK, Werier J, MacDermid JC, et al: Arthroplasty with a metal radial head for unreconstructible fractures of the radial head. J Bone Joint Surg Am 2001;83:1201-1211.
Question 26
When do most symptomatic thromboembolic events occur after total joint arthroplasty?
Explanation
Most clinical venous thromboembolism events occur between the second and sixth weeks after surgery. It is estimated that 10% of patients are readmitted to the hospital within the first 3 months after total hip or knee arthroplasties. Most pulmonary events on the day of surgery are related to fat embolism or cardiac events.
Question 27
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient’s symptoms at this time?
Explanation
REFERENCES: Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
Mundy GR: Hypercalcemia of malignancy revisited. J Clin Invest 1988;82:1-6.
Question 28
When treating thoracolumbar spine fractures, which of the following is considered the major advantage of using a thoracolumbosacral orthosis (TLSO) when compared to a three-point fixation brace (Jewett)?
Explanation
REFERENCES: Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 347-349.
Krompinger WJ, Fredrickson BE, Mino DE, Yuan HA: Conservative treatment of fractures of the thoracic and lumbar spine. Orthop Clin North Am 1986;17:161-170.
Stauffer ES (ed): Thoracolumbar Spine Fractures without Neurological Deficit. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993.
Question 29
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely when placing a sharp retractor
Explanation
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually posterolateral to the PCL.
Question 30
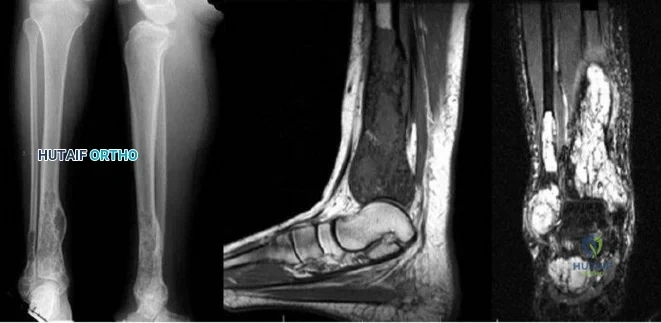
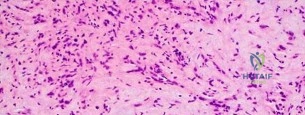
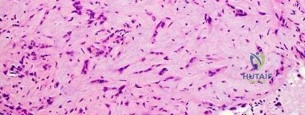
A 45-year-old man has had left thigh pain for the past 4 months. An AP radiograph, bone scan, MRI scans, and biopsy specimens are shown in Figures 6a through 6f. What is the most appropriate treatment?
Explanation
REFERENCES: Hadjipavlou AG, Gaitanis IN, Kontakis GM: Paget’s disease of the bone and its management. J Bone Joint Surg Br 2002;84:160-169.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 187-196.
Question 31
A year-old man with a body mass index of 31 had a month gradual onset of right medial knee pain. Examination revealed a small effusion, stable ligaments, a normally tracking patella, and mild medial joint line tenderness. Standing radiographs show mild medial joint space narrowing. Effective treatment at this stage of early medial compartmental osteoarthritis includes
Explanation
According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee (Nonarthroplasty), level 1 evidence confirms that weight loss and exercise benefit patients with knee osteoarthritis. The other responses have either inclusive evidence (a valgus-directing brace) or no evidence to support their use (glucosamine 1,500 mg/day and chondroitin sulfate 800 mg/day as well as
arthroscopic debridement and lavage).
Question 32
When compared with fresh-frozen bone allograft, freeze-dried bone allograft (FDBA) is characterized by
Explanation
REFERENCES: Cornu O, Libouton X, Naets B, et al: Freeze-dried irradiated bone brittleness improves compactness in an impaction bone grafting model. Acta Orthop Scand
2004;75:309-314.
Price CT, Connolly JF, Carantzas AC, et al: Comparison of bone grafts for posterior spinal fusion in adolescent idiopathic scoliosis. Spine 2003;28:793-798.
Leniz P, Ripalda P, Forriol F: The incorporation of different sorts of cancellous bone graft and the reaction of the host bone: A histomorphometric study in sheep. Int Orthop 2004;28:2-6.
Question 33
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of
Explanation
REFERENCES: Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Gerber C, et al: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 34
Figure 1 is the MR image of a 55-year-old man who sustained an acute traumatic injury to his right shoulder with loss of active range of motion. He was initially evaluated by his primary care physician and treated with physical therapy without success. He was referred to an orthopaedist for surgical consultation 8 weeks after sustaining the injury. The orthopaedic surgeon performs a successful arthroscopic repair but notes poor tendon quality at the repair site. The treating surgeon keeps the patient in a sling full time for 6 weeks without formal therapy. One year after surgery, in comparison to early therapy, this rehabilitation program will likely result in
Explanation
A. better glenoid exposure than with stemmed prostheses.
B. reliable use in four-part proximal humerus fracture reconstruction.
C. use in proximal humeral malunion without the need for an osteotomy.
D. improved long-term survivorship profile.
Question 35
Figures below show the radiographs obtained from a 75-year-old woman who underwent right total hip arthroplasty in 2009. She did well until last month, when a right posterior hip dislocation occurred after she fell from her bed to the floor. Successful closed reduction was performed. She sustained two more posterior dislocations requiring closed reduction under anesthesia. The surgical report from the index arthroplasty notes a 54-mm monoblock acetabular component with a 28-mm inner diameter compression molded polyethylene and a high offset neck cementless stem with a +8-mm length, 28-mm head. What is the best next step?
Explanation
This patient has demonstrated recurrent instability, and her current implants lack the modularity to upsize and improve the head-neck ratio and range to impingement. Given the monoblock acetabular component and a +7-mm neck length, the best option is revision to a large-diameter femoral head or dual-mobility component. Placement of a hip spica cast and resection arthroplasty are unreasonable. Revision to a longer ball length likely would not solve this recurrent instability pattern.
Question 36
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?

Explanation
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
Question 37
Figure 11 shows the radiograph of an 18-year-old soccer player who reports recurrent lateral foot pain after sustaining an inversion injury. History reveals that 6 months ago he had been treated in a non-weight-bearing cast for a fifth metatarsal fracture. Management should consist of
Explanation
REFERENCES: Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff TC, Das M: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.
DeLee JC: Fractures and dislocations of the foot, in Mann R, Coughlin M (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 1465-1503.
Question 38
Figures 1 through 4 are the wrist MR images of a 43-year-old right-hand-dominant bricklayer who reports gradually progressive left hand weakness for 4 months. He describes difficulty gripping objects, tying his shoes, and holding utensils. He denies any numbness, paresthesias, or a previous injury. An examination reveals intact sensation in a median, radial, and ulnar nerve distribution. He has atrophy of hand interossei and a positive Froment sign finding. He has no Tinel sign finding at the wrist or elbow and no exacerbation of symptoms with elbow hyperflexion. Electromyography shows signs of denervation in an ulnar nerve distribution distal to the wrist. What is the best next step?
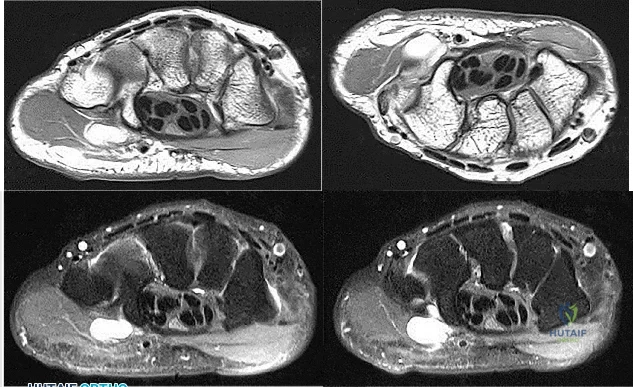
Explanation
Question 39
5 mg/dL), vitamin D 50 ng/mL (reference range, 30-100 ng/mL), and urine phosphorus 2 g/24-hour collection (reference range, 0.4-1.3 g). What effect would treatment with only Calcitriol (1,25 dihydroxy vitamin D3) have?
Explanation
which lowers plasma ionized calcium concentration and further reduces plasma calcitriol concentration (removal of hypophosphatemic stimulus). Secondary hyperparathyroidism results because of both hypocalcemia and removal of the
normal inhibitory effect of calcitriol on parathyroid hormone (PTH) synthesis. Elevated PTH levels will increase urinary phosphate excretion, defeating the aim of oral therapy.
Addition of calcitriol is necessary to increase the intestinal absorption of calcium and phosphate to prevent secondary hyperparathyroidism. Massive doses of vitamin D alone can restore normal radiographic appearances to the epiphyses, but normal growth is not restored unless phosphate replacement is adequate.
A 35-year-old woman began to train for a half marathon. After 8 weeks of increasing her mileage, what changes can you expect in her Achilles tendon?
Net decrease of type I collagen
Net increase of type I collagen
Increased diameter of collagen fibrils
Increased cross-sectional area of the tendon
Training increases turnover of type I collagen, promoting both synthesis and degradation of collagen and a net increase synthesis of type I collagen in tendon-related tissue.
Strenuous endurance training has resulted in decreased collagen cross-links, suggesting increased collagen turnover, but decreased collagen maturation. In human studies, physical training results in increased turnover of collagen. Synthesis and degradation are elevated initially when beginning an exercise program, but degradation products decrease overall. It is not known if activity levels in humans affect the diameter of collagen fibrils or the cross-sectional area of tendons.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 40
What is the advantage of percutaneous pedicle screw fixation over open instrumentation and fusion for a thoracolumbar burst fracture without neurologic deficit?
Explanation
A prospective randomized study on short-segment treatment of burst fractures with and without fusion demonstrated similar outcomes at 5 years with lower blood loss in the nonfusion group. There is by definition no fusion performed with percutaneous stabilization, so patients often develop hardware failure. Some surgeons routinely remove instrumentation following percutaneous stabilization, thus revision surgery is common. Clinical outcomes are not improved compared to open methods.
RECOMMENDED READINGS
Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. Review. PubMed PMID: 24981899. View Abstract at PubMed Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomised trial. J Bone Joint Surg Br. 2012 Aug;94(8):1101-6. doi: 10.1302/0301-620X.94B8.28311. PubMed PMID: 22844053. View Abstract at PubMed
Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone
Joint Surg Am. 2009 May;91(5):1033-41. doi: 10.2106/JBJS.H.00510. PubMed PMID:
Question 41
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include
Explanation
REFERENCE: Sabharwal S, Tredwell SJ, Beauchamp RD, Mackenzie WG, Jakubec DM, Cairns R: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 42
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time? Review Topic

Explanation
(SBQ13PE.82) A renal ultrasound should be obtained in a patient with which of the following diagnoses? Review Topic
Congenital pseudoarthrosis of the clavicle
Accessory navicular
Congenital scoliosis
Charcot-Marie-Tooth Disease
Congenital curly toe
A renal ultrasound should be obtained in a patient with congenital scoliosis.
Congenitial scoliosis has a prevalence that is estimated at 1% to 4% in general population. It is associated with systemic anomalies in up to 61% of cases. The most common anomalies are cardiac defects, genitourinary defects and spinal cord malformations. As such, additional imaging of these systems should be considered in the initial work-up of these patients.
Ruf et al. retrospectively investigated 56 consecutive operative cases of congenital scoliosis. The average age at surgery was 9.9 years (1.5–17 years). There was one wound complication, 2 hardware failures, 1 revision and no neurological complications. They concluded that one-stage posterior hemivertebra resection and instrumentation was safe in this population.
Xu et al. examined the efficacy of selective partial hemivertebra excision via posterior-only approach in 17 adolescent patients with congenital kyphoscoliosis. There were no postoperative infections and no neurological complications. They concluded that this approach may be most successful in patients aged 9 to 14 years old, with the Risser sign grades from 0–3 and Cobb angles <60°.
Illustration A from Erol et al (UPOJ, Vol 15, 2002;37-42) shows a diagram of 'types' of congenital scoliosis based on the morphology of the vertebrae.
Incorrect Answers:
Question 43
Which of the following statements correctly describes the results of gamma irradiation of musculoskeletal allograft?
Explanation
4 megarads have been shown to alter the mechanical properties of human infrapatellar tendons. Ethylene oxide, also used for allograft sterilization, has been associated with a chronic inflammatory process that resolved after graft removal.
REFERENCES: Jackson DW, Windler GE, Simon TM: Intraarticular reaction associated with the use of freeze-dried, ethylene oxide-sterilized bone-patella tendon-bone allografts in the reconstruction of the anterior cruciate ligament. Am J Sports Med 1990;18:1-10.
Conway B, Tomford W, Mankin HJ, et al: Radiosensitivity of HIV-1: Potential application to sterilization of bone allografts. AIDS 1991;5:608-609.
Rasmussen TJ, Feder SM, Butler DL, et al: The effects of 4 Mrad of gamma irradiation on the initial mechanical properties of bone-patellar tendon-bone grafts. Arthroscopy 1994;10:188-197.
Question 44
A previously healthy 35-year-old man was involved in a rollover motor vehicle accident 2 days ago. He was placed in a semi-rigid cervical orthosis. He now reports mostly axial neck pain with attempted range of motion. Examination reveals the mechanical neck pain but no obvious neurologic deficits. AP, flexion, and extension radiographs are shown in Figures 10a through 10c, and sagittal and coronal CT scans are shown in Figures 10d and 10e. What is the most appropriate management at this time?
Explanation
REFERENCES: Shilpakar S, McLaughlin MR, Haid RW Jr, et al: Management of acute odontoid fractures: Operative techniques and complication avoidance. Neurosurg Focus 2000;8:e3.
Subach BR, Morone MA, Haid RW Jr, et al: Management of acute odontoid fractures with single-screw anterior fixation. Neurosurgery 1999;45:812-819.
Fountas KN, Kapsalaki EZ, Karampelas I, et al: Results of long-term follow-up in patients undergoing anterior screw fixation for type II and rostral type III odontoid fractures. Spine 2005;30:661-669.
Question 45
A 60-year-old man who underwent left partial knee arthroplasty 6 months earlier was doing well until he experienced left knee pain and swelling for 4 weeks following a dental procedure. The left knee aspirate was bloody, with a white blood cell count of 8,000 and 70% neutrophils. Culture grew group B Streptococcus (Granulicatella adiacens), and serologies were elevated, with an erythrocyte sedimentation rate of 55 mm/h (reference range: 0 to 20 mm/h) and a C-reactive protein level of 24 mg/L (reference range: 0.08 to 3.1 mg/L). What is the best next step?
Explanation
This complication is best addressed with either a single-stage or two-stage total knee arthroplasty. A recent report suggests that a single-stage arthroplasty can be effective, although many surgeons would perform a two-stage procedure with an articulating or static spacer. Arthroscopic would be non-effective, especially given 4 weeks of symptoms. Resection arthroplasty without a spacer would leave an unstable and poorly functioning extremity. Knee fusion should be used as a salvage procedure.
belowshowtheradiographs,andtheCTobtainedfromayear-oldwomanwhounderwent
cementlesslefttotalhiparthroplasty.Ninemonthsaftersurgery,shecontinuedtohavegroinpainwhen activelyflexingherhip.Shehastroublewalkingupstairsandgettingoutofhercar.Acourseof appropriatenonsurgicaltreatmentfailed.Whatisthenextstepindefinitivetreatment?
A. Acetabularcomponentrevision
B. Femoralcomponentrevision
C. Acetabularlinerexchange
D. Trochanteric bursectomy
Submit Answer
Question 46
At the time of acetabular revision, retention of well-fixed femoral components inserted with first-generation cementing technique is most commonly associated with which of the following factors?
Explanation
Question 47
In the pediatric population, CECS most commonly presents in females involved in running sports. In this cohort, recurrence occurs at a rate of 18%. Wound complications are the next most common at a rate of 11.2%. A 15-year-old male ice hockey player is hit in the chest by a puck and immediately falls to the ground unconscious. What has been shown to predict survival in the treatment of this condition?
Explanation
against ventricular fibrillation. The velocity of the projectile (most commonly baseball, hockey puck or lacrosse ball) has also not been shown to alter survival.
Question 48
…Figure 53 is the emergency department radiograph of a 7-year-old boy who has pain and is unwilling to use his right arm after a fall on the playground. What is the most appropriate initial treatment?
Explanation

Question 49
- A 19-year-old man sustains a complete spinal cord injury at the C7 level as a result of diving into a lake. He has a blood pressure of 90/50 mm Hg, a pulse of 60/min, and respirations of 20/min. These values most likely signify
Explanation
Question 50
A 34-year-old man sustained a gunshot wound to the knee 18 months ago and was treated with bullet removal and a 10 day course of oral antibiotics. He now complains of 12 months duration of pain in the thigh and recent ulceration and drainage of the skin near the site of his gunshot wound. Physical exam is notable for a draining sinus tract, erythema and tenderness of the mid-thigh. He is afebrile. An MRI image of this patient is shown in Figure A. Which of the following is the most appropriate management?

Explanation
In the referenced article by Parsons and Strauss, the management of chronic osteomyelitis is reviewed.
OrthoCash 2020
Question 51
A 45-year-old man reports severe discomfort following a twisting injury to his right ankle and foot. Plain radiographs are negative; however, the CT scans shown in Figures 39a and 39b reveal a fracture. Management should consist of
Explanation
REFERENCES: Heckman JD: Fractures and dislocations in the foot, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2267-2405.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 52
A 14-year-old boy with a history of cerebral palsy has a clawed hallux, cavus foot deformity, and associated pain. Examination reveals pain under the first metatarsal head and a rigid first tarsometatarsal joint. Treatment should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 79-100.
Tynan MC, Klenerman L: The modified Robert Jones tendon transfer in cases of pes cavus and clawed hallux. Foot Ankle Int 1994;15:68-71.
Question 53
A 10-year-old boy sustained an injury to the left knee. The radiographic findings shown in Figure 19 are most commonly associated with injury to which of the following structures?
Explanation
REFERENCES: Baxter MP, Wiley JJ: Fractures of the tibial spine in children: An evaluation of knee stability. J Bone Joint Surg Br 1988;70:228-230.
Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 406-432.
Question 54
..Further imaging shows pulmonary metastases without an obvious primary tumor of origin and an incomplete fracture of the right distal femur. A decision is made to surgically treat his distal femur fracture. What is the role of establishing a preoperative histologic diagnosis for this patient?
Explanation
t(X;18)(p11.2;q11.2)
t(11;22)(q24;q12)
t(1;3)(p36.3;q25)

Question 55
A 74-year-old man has had worsening left shoulder pain for the past 3 years. Extensive nonsurgical management has provided only minimal relief. Examination reveals limitations in motion due to pain but good rotator cuff strength. Radiographs are shown in Figures 53a and 53b. What surgical procedure is most appropriate?
Explanation
REFERENCES: Bryant D, Litchfield R, Sandow M, et al: A comparison of pain, strength, range of motion, and functional outcomes after hemiarthroplasty and total shoulder arthroplasty in patients with osteoarthritis of the shoulder: A systemic review and meta-analysis. J Bone Joint Surg Am 2005;87:1947-1956.
Edwards TB, Kadakia NR, Boulahia A, et al: A comparison of hemiarthroplasty and total shoulder arthroplasty in the treatment of primary glenohumeral osteoarthritis: Results of a multicenter study. J Shoulder Elbow Surg 2003;12:207-213.
Gartsman GM, Roddey TS, Hammerman SM: Shoulder arthroplasty with or without resurfacing of the glenoid in patients who have osteoarthritis. J Bone Joint Surg Am 2000;82:26-34.
Question 56
A 40-year-old man fell 10 feet from a tree and sustained the closed isolated injury shown in Figures 35a and 35b. Management consists of splinting. At his 2-week follow-up visit, he clinically passes the wrinkle test. He agrees to open reduction and internal fixation. What is the best surgical approach to obtain anatomic reduction and limit wound dehiscence?
Explanation
REFERENCES: Borrelli J Jr, Lashgari C: Vascularity of the lateral calcaneal flap: A cadaveric injection study. J Orthop Trauma 1999;13:73-77.
Freeman BJC, Duff S, Allen PE, et al: The extended lateral approach to the hindfoot: An anatomical basis and surgical implications. J Bone Joint Surg Br 1998;80:139-142.
Zwipp H, Tscherne H, Wulker N: Osteosynthesis of dislocated intra-articular calcaneus fractures. Unfallchirurg 1988;91:507-515.
Question 57
- Which of the following rehabilitation methods should be used for the first 24 hours following a blunt injury to the quadriceps musculature to avoid short-term stiffness?
Explanation
In the past immobilization in full extension was recommended, but it was noticed that the lack of flexion prolonged disability. Flexion of the knee during the first 24 hours also aids in limiting the extent of intramuscular hematoma.
Myositis ossificans is higher in any patient presenting after a quad contusion and has active knee ROM of less than 120 degrees and delay in treatment greater than 3 days.
Question 58
3 degrees Celsius and heart rate of 105 bpm. A clinical photograph, results of synovial fluid analysis, and a polarizing microscopy image are seen in Figures A through C. Synovial fluid gram stain and cultures are pending. What is the most appropriate next step in management?
Explanation
While the incidence of superimposed gout and septic arthritis is low (~1.5%),
it is reported. In the presence of crystals on aspiration, one should not rule out the possibility of septic arthritis. If there are other risk factors for infection, or the synovial WBC count is high (greater than 50,000), then empiric antibiotics should be initiated immediately after cultures are obtained. If the patient has other evidence supporting septic arthritis (positive Gram stain, purulence), emergent I&D is indicated. Even if the initial suspicion is lower, if they have
not respond to antibiotics after 24-48 hours they should undergo I&D.
Shah et al. investigated 265 crystal-positive joint aspirates in a 7-year retrospective study. They found the incidence of concomitant septic arthritis and crystal disease was 1.5% (4 cases including 2 knees, 1 hip, 1 ankle). All 4 patients that had superimposed infection had a WBC of > 50,000. They concluded that the presence of crystals in the synovial fluid cannot
conclusively rule out a septic joint.
Schuind et al. described a case report of concomitant septic arthritis and gout of the wrist. They found that cultures were positive for Staphylococcus aureus while pathological examination revealed aggregated crystals of monosodium urate.
Figure A shows tense, erythematous swelling of the right knee. Figure B is a table showing synovial fluid analysis with elevated WBC and PMN cell count characteristic of septic arthritis. Figure C shows needle-shaped negatively birefringent crystals on polarizing microscopy. Illustration A shows the synovial fluid characteristics in different disease conditions.
Incorrect Answers:
An 82-year-old osteoporotic woman undergoes total hip arthroplasty for osteoarthritis. During implant trialing, a crack is heard. Intraoperative fluoroscopy reveals a long, spiral fracture of the distal femur. The fracture is reduced and fixed with an anatomic locking plate. The rest of the total hip arthroplasty proceeds uneventfully. Following surgery the surgeon has a meeting with the family and apologizes and provides full disclosure, accepts responsibility, provides a detailed explanation as to what happened, and gives reassurance that steps will be taken to prevent recurrences. This communication approach will most likely
Lead to lower patient satisfaction rates
Lead to higher patient satisfaction rates
Lead to higher likelihood the patient will take legal action against surgeon
Lead to higher likelihood the patient will change physicians
Prevent any legal action
The surgeon has provided all the elements of good communication with the patient and family. His actions will lead to improved patient satisfaction, compared to nondisclosure and attempting to push or shirk responsibility.
In the event of a medical error or adverse event, effective communication with the patient and family is necessary. Effective communication should comprise:
an apology, full disclosure (an explanation of what happened), accepting responsibility, and corrective steps that will be taken to prevent recurrence.While accepting responsibility is integral to the explanation process, it is different from accepting blame.
Mazor et al. found patients would more likely change physicians and seek legal advice in situations with a life-threatening outcome where physicians chose
non-disclosure. They recommend full disclosure, acceptance of responsibility, an apology, detailed explanations, and assurances that steps will be taken to prevent recurrences will result in positive outcomes in terms of patient satisfaction, trust, and emotional response.
MacDonald et al. addressed medical errors in an editorial. Besides full disclosure, they feel that an apology is necessary. This includes an acknowledgement of the event and one’s role in the event, and a genuine expression of regret. Apology laws exist to to reduce concerns about legal implications of disclosure and apology.
Incorrect Answers:
The acquired immune response mediated by the interaction between the T cell receptor and major histocompatibility complex requires which of the following first steps?
Antigen phagocytosis by T cells
Antigen processing and presentation to T cells
Antigen recognition by natural killer T cells
Antigen proliferation by polymerase chain reaction
T cell disulfide bond cleavage and enzymatic processing
The process of antigen processing and presentation is the first step of the acquired immune response. This is performed by the so called antigen presentation cells (APC) of which B cells and dentritic cells are two examples. The APC breaks down the protein antigen in a multitude of enzymatic reactions and presents key peptide sequences via the major histocompatibility complex
(MHC) receptors. Once presented on the surface of the APC, the T-cell receptor recognizes the MHC/antigen complex leading to T-cell activation. At no point in this process are antigens phagocytosed by T cells. Natural killer T cells are involved in this sequence, but not for antigen processing and presentation. Polymerase chain reaction is a laboratory tool used to amplify nucleic acid. Finally, disulfide bond cleavage is a step involved in the APCs antigen processing reaction and does not occur in T cells.
All of the following are true regarding a physician responding to a formal written complaint by a patient EXCEPT:
Complaint should be taken seriously
Written response by the physician is required
Physician mandated to retain an attorney to address the formal complaint
Patient should be supplied with contact information for the institution's patient representative department
Law mandates that the physician respond to the formal complaint
It is important for the surgeon to know how to manage a formal complaint. An attorney is not required to assist on behalf of the physician when addressing a formal complaint. All complaints must be taken seriously and the physician is required by law to respond to all formal complaints in writing. Verbal
responses to formal, written complaints are not sufficient. If a patient is filing a formal complaint it is advisable that the patient be supplied with contact information for the institution's patient representative department.
What laboratory findings would you expect to find in a patient newly diagnosed with renal osteodystrophy?
Decreased PTH secretion, hypophosphatemia, and hypocalcemia
Increased PTH secretion, hyperphosphatemia, and hypocalcemia
Decreased PTH secretion, hypophosphatemia, and hypercalcemia
Increased PTH secretion, hyperphosphatemia, and hypercalcemia
Hypophosphatemia and hypocalcemia
Renal osteodystrophy is characterized by bone mineralization deficiency due to the electrolyte and endocrine abnormalities associated with chronic kidney disease. The pathogenesis of renal osteodystrophy is multifactorial. Hypocalcemia occurs due to the inability of the damaged kidney to convert vitamin D3 into its active form, calcitriol. The hypocalcemia and lack of phosphate excretion by the damaged kidney causes hyperparathyroidism and secondary hyperphosphatemia.
Loss of function in the 25(OH) vitamin D1-alpha hydroxylase gene causes which of the following diseases?
Hyperphosphatemia
Vitamin D resistant rickets
Hereditary Vitamin D dependant rickets type I
Hereditary Vitamin D dependant rickets type II
Hypophosphatemic rickets
Loss of function mutations in the 25 (OH) vitamin D hydroxylase gene cause hereditary vitamin D dependant rickets type I. Hereditary vitamin D dependant rickets type II is caused by a defect in intracellular receptor for 1,25-(OH)2- vitamin D3. Both forms of
hereditary vitamin D dependent rickets show decreased serum calcium/phosphorous, elevated alkaline phosphatase/PTH,
but type I has a decrease in the 1,25(OH)2 vitamin D and type II shows a increase in 1,25(OH)2 vitamin D. Vitamin D resistant rickets (Familial Hypophosphatemic Rickets) is caused by a large deletion in the PHEX gene and results in low serum phosphorous, elevated alkaline phosphatase, and normal calcium. Hyperphosphatemia can be caused by mutation in the GALNT3 gene and results in elevated serum phosphate and decreased PTH/calcium.
Kato et al. describe the molecular physiology of vitamin D metabolism and the recognized gene mutations associated with various clinical manifestations of mutations in vitamin D homeostasis.
Figure A is a radiograph taken after an open reduction and internal fixation of a periprosthetic distal femur fracture. With this type of hybrid locked plate fixation, what is the difference between screw A and screw B?
Screw A can assist in fracture reduction while screw B provides a fixed angle support
Screw A provides improved axial stiffness while screw B provides a fixed angle support
Screw A can be used to reduce the plate to bone while screw B can be used to lag fracture fragments together
Screw A provides a fixed angle support while screw B can be used to reduce the plate to the bone
Screw A can be used to lag fracture fragments together and screw B increases the plate bone frictional stability
Locking screws provide a fixed angle support and can improve fixation in osteoporotic bone while nonlocking screws can be used to reduce the plate to the bone, lag fracture fragments together and increase the plate bone frictional stability. "Hybrid" locked plate fixation utilizes both screw types in order to assist with difficult fracture fixation such as when there is a short metaphyseal segment and osteoporotic bone.
Zura et al discusses the biomechanical and biological advantages offered by locked plate fixation.
Using levels of evidence in research studies, which of the following represents a level II study?
Retrospective case control study
Prospective cohort study
Case report of 3 patients with the same disease
High-quality randomized prospective clinical trial
The opinion of a review panel at the annual AAOS meeting
Level II Evidence includes prospective cohort studies. There are 5 levels of evidence in clinical research. Level I includes randomized clinical trials. Level II includes prospective cohort studies. Level III includes case control studies AND retrospective cohort studies. Level IV includes case series. Level V evidence includes expert opinion, case reports, and personal observation. The cited reference by Bernstein et al is an excellent review of Evidence Based Medicine (EBM) and describes the 5 step process of making medical decisions based on the available, and often limited, evidence. These steps include: 1) Formulate answerable questions. 2) Gather the evidence. 3) Appraise the evidence. 4) Implement the evidence. 5) Evaluate the process. The reference by Spindler et al is another review article that discusses the different levels of evidence for different study types.
All of the following are true regarding the assessment of bone mineral density EXCEPT?
Bone mineral density loss is not apparent on standard radiographs until 30% to 40% of mineral is lost
Dual energy x-ray absorbtiometry (DEXA) is only able to measure mineralization of the axial skeleton
Single photon absorbtiometry allows for the analysis of bone mineralization in the appendicular skeleton alone
Quantitative computed tomography (QCT) is associated with 10 times the radiation of a DEXA scan
MRI allows for accurate discrimination of normal bone from osteopenic bones
without exposing the patient to ionizing radiation
Dual energy x-ray absorbtiometry (DEXA) scans allow for accurate assessment of bone mineralization in both the axial and appendicular skeleton.
Over the last decade, DEXA has become a safe, cost-effective and reliable method to quantify bone mineral density. The World Health Organization (WHO) has adopted DEXA derived BMD measurements to define normal bone, osteopenia, and osteoporosis in the adult and paediatric population. The typical DEXA analysis therefore reports a Z-score, which is the number of standard deviations (SDs) that a patient's BMD is above or below the mean value for persons of the patient's age and sex. The T score is the number of SDs the patient's BMD is either above or below the mean value for young patients of the same gender.
Tortolani et al. provide an overview of the techniques used to assess bone mineral density, the pathophysiology of osteopenia, and the evaluation and treatment options for the general pediatric population as well as for patients with specific pediatric disorders. The authors encouraged orthopaedic surgeons to understand the problems of osteopenia in both otherwise healthy children and children with chronic disorders.
Binkovitz & Henwood provide a review of DEXA technique and interpretation with emphasis on the considerations unique to pediatrics. They found that changes in bone size over time, as occurs in normal pediatric development, confound DXA interpretation. This is one of the major limitations in the use of pediatric DXA. However, attempts to correct for or to circumvent this limitation have been proposed and show promise in improving DXA interpretation and
our understanding of bone physiology.
T-score according to the World Health Organization (WHO): A T- score of -1.0 or above is normal bone density.
A T-score between -1.0 and -2.5 means you have low bone density or osteopenia.
A T-score of -2.5 or below is a diagnosis of osteoporosis.
Incorrect Answers:
A mother brings her 4-year-old daughter to your clinic for evaluation of knocked knees and short stature. On exam, the patient ambulates with a circumduction gait pattern and frequently falls. Plain radiographs are displayed in Figure A. Laboratory data is obtained and notable for calcium 9.1 mg/dL (RR 8.5-
Question 59
A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. Management should consist of
Explanation
REFERENCES: Kozin SH: Perilunate injuries: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:114-120.
Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
Sotereanos DG, Mitsionis GJ, Ginnakopoulos PN, Tomaino MM, Herndon JH: Perilunate dislocation and fracture dislocation: A critical analysis of the volar-dorsal approach. J Hand Surg Am 1997;22:49-56.
Question 60
A 60-year-old woman has activity-related hip pain after undergoing arthroplasty 5 years ago. She has severe Parkinsonism and denies fevers or chills. Radiographs are shown in Figures 45a and 45b. What is the most likely cause of her pain?
Explanation
REFERENCES: Harris WH, McCarthy JC, O’Neill DA: Femoral component loosening using contemporary techniques of femoral cement fixation. J Bone Joint Surg Am 1982;64:1063-1067.
Callaghan JJ, Rosenberg AG, Rubash H (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 960, 1228-1229.
Maloney WJ, Schmalzreid T, Harris WH: Analysis of long-term cemented total hip arthroplasty retrievals. Clin Orthop Relat Res 2002;405:70-78.
Question 61
A B
Explanation
The radiographs reveal a tibial pilon fracture with an extruded and rotated anterior tibial fragment that lies deep to the anterior compartment neurovascular bundle, which contains the deep peroneal nerve. This nerve innervates the anterior compartment muscles and the extensor digitorum brevis and extensor hallucis brevis muscles and provides sensation to the dorsal aspect of the first interspace. An injury to the deep peroneal nerve at this level will only affect the innervation to the extensor digitorum brevis and extensor hallucis brevis muscles and the innervation of the first interspace. The superficial peroneal nerve innervates
the lateral compartment muscles above the level of this injury and innervates the dorsum of the foot. The medial forefoot is innervated by the saphenous nerve and the posterior tibial nerve innervates the posterior compartment muscles above the level of the injury. The sural nerve innervates the lateral foot and has no motor component, and the superficial peroneal nerve innervates the peroneus longus, which plantar flexes the first metatarsal above the level of the injury.
RECOMMENDED READINGS
Agur AM, Dalley AF, eds. Grant’s Atlas of Anatomy. 13th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2013:362-370.
Hoppenfeld S, de Boer P, Buckley R, eds. Surgical Exposures in Orthopaedics: The Anatomic Approach. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:625-673.
Question 62
Figure 1 is an MRI scan of the right hip of a 19-year-old woman with a 6-month history of right groin pain. She was diagnosed with a stress fracture and was treated with 3 months of limited weight bearing. Figure 2 is a repeat MRI scan in which the edema pattern changed minimally but the pain worsened. Ibuprofen alleviates most of her pain. What is the best next step?
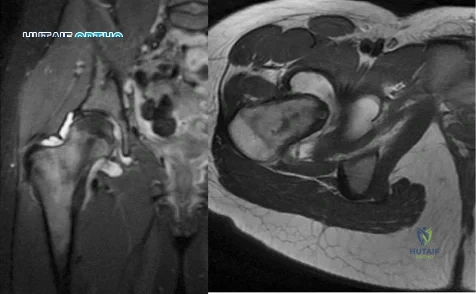
Explanation
cells, forms the nidus of the tumor, which is easily identified on CT scans.
Question 63
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in Review Topic
Explanation
Question 64
Figures 2a and 2b show the radiograph and MRI scan of a 56-year-old woman who has low back pain and right leg pain. She has grade 3/5 toe and ankle dorsiflexion strength on the right side. Nonsurgical management has failed to provide relief; therefore, surgery should include Review Topic
Explanation
Question 65
The primary function of structure “A” in Figure 29 is to limit
Explanation
REFERENCES: Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
Veltri DM, Deng XH, Torzilla PA, et al: The role of the cruciate and posterolateral ligaments in stability of the knee: A biomechanical study. Am J Sports Med 1995;23:436-443.
Question 66
A 62-year-old man who underwent total knee arthroplasty 6 months ago now reports pain after falling on the anterior portion of the knee. Examination reveals weakness of knee extension but no extensor lag. Flexion that had once measured 115 degrees is now limited to 70 degrees because of pain. A radiograph is shown in Figure 25. Management should now consist of
Explanation
REFERENCES: Brown TE, Diduch DR: Fractures of the patella, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1290-1312.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 323-337.
Question 67
Figure 12 shows the radiograph of an 80-year-old woman who has had an 8-month history of back pain after a fall. What is the most likely diagnosis based on the radiographic findings at the fractured vertebrae?
Explanation
REFERENCES: Murakami H, Kawahara N, Gabata T, et al: Vertebral body osteonecrosis without vertebral collapse. Spine 2003;28:E323-E328.
Jang JS, Kim DY, Lee SH: Efficacy of percutaneous vertebroplasty in the treatment of intravertebral pseudarthrosis associated with noninfected avascular necrosis of the vertebral body. Spine 2003;28:1588-1592.
Question 68
A 32-year-old male sustains an APC-III pelvic ring disruption after a motor vehicle collision. Which of the following imaging techniques best describes the correct utilization of intraoperative flouroscopy for percutaneous iliosacral screw placement across S1?

Explanation
view and an inlet pelvis view would best guide anterior-posterior screw orientation.
Routt et al did a review of percutaneous techniques of pelvic surgery. Although anterior pelvic external fixation remains the most common form of percutaneous pelvic fixation, iliosacral screws have the advantage of stabilizing pelvic disruptions directly while diminishing operative blood loss and operative time. They stress importance of a thorough knowledge of pelvic osseous anatomy, injury patterns, deformities, and their fluoroscopic correlations for surgical success.
Routt et al also looked at the complications that can result from percutaneous iliosacral screw placement. Complications ranged from inability for adequate imaging due to patient obesity, L5 nerve root injuries, fixation failure, and sacral nonunions. They support quality triplanar fluoroscopic imaging during iliosacral screw insertions to help accurately reduce injured posterior pelvic rings.
Illustration A shows the radiographic technique used to shoot an outlet pelvis view and illustration of the pelvic view. Illustration B is an example of an outlet view image status post anterior pelvic ring plating and percutaneous iliosacral screw. This outlet view allows superior S1 neural foramen visualization to help guide screw placement and avoid nerve injury.
Question 69
A 2-year-old child has refused to bear weight on his leg for the past 2 days. His parents report that he will crawl, has no fever, and has painless full range of motion of his hip and knee. Examination reveals no deformity or bruising, but there is mild swelling and tenderness over the anterior tibia. C-reactive protein, WBC count, and erythrocyte sedimentation rate studies are normal. Radiographs are negative. What is the best course of action?
Explanation
REFERENCES: Halsey MF, Finzel KC, Carrion WV, Haralabatos SS, et al: Toddler’s fracture: Presumptive diagnosis and treatment. J Pediatr Orthop 2001;21:152-156.
Oudjihane K, Newman B, Oh KS, et al: Occult fractures in preschool children. Trauma 1988;28:858-860.
Question 70
A 38-year-old woman has persistent elbow pain but is unable to recall a specific traumatic event. Examination reveals that the patient exhibits apprehension when the elbow is placed in valgus with forearm supination and axial loading. Because of chronicity and failure to respond to nonsurgical management, what is the most appropriate treatment? Review Topic
Explanation
Question 71
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?
Explanation
REFERENCES: Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Meister K: Injuries to the shoulder in the throwing athlete. Part one: Biomechanics, pathophysiology, classification of injury. Am J Sports Med 2000;28:265-275.
Question 72
A researcher experimenting with limb patterning removes some tissue from 1 part of the limb bud (which we shall call Site A) and transplants it along the anteroposterior (AP) axis to create a mirror-hand duplication. Which of the following is true?
Explanation
The ZPA controls AP (radioulnar) growth. The signaling molecule is Shh, which is dose dependent. Higher Shh doses lead to posterior (ulnar) digits ulnar sided polydactyly. The extent of duplication is dose dependent (higher dose = more replication). Reduced Shh leads to loss of digits. Posterior elements (little finger/ulna) are formed EARLY prior to anterior elements which are formed LATE (radius/thumb). Disruption of AP patterning will result in loss of later forming elements (radius/thumb).
Al-Qattan et al. reviewed embryology of the upper limb. They summarized that embryology of the upper limb can be viewed in 2 distinct ways: the steps of limb development and the way that the limb is patterned along its 3 spatial axes. Cell signaling plays a major role in regulating growth and patterning of the vertebrate limbs. Signaling cell dysfunction results in congenital differences according to the affected signaling axis.
Illustration A shows an experiment to create ulnar dimelia by adding ZPA tissue to the anterior limb bud. The video shows development of the limb.
Incorrect Answers:
Question 73
Poor pre-injury cognitive function has been proven to increase mortality for which of the following injuries?

Explanation
Question 74
Radiographs of the femur are unremarkable. A radionuclide bone scan demonstrates abnormal uptake in the mid-femur. A radionuclide bone marrow scan demonstrates decreased uptake within the marrow. Which of the following is the best step in management?
Explanation
Skaggs et al reviewed 79 cases of acute extremity pain in sickle cell patients. Radionuclide bone marrow and bone scan was used to differentiate osteomyelitis from bone infarct. Four cases of infection were diagnosed by normal uptake on the bone marrow scan and abnormal uptake on the bone scan. These cases were confirmed osteomyelitis by positive culture. Seventy cases were diagnosed as bone infarct by decreased uptake on the bone marrow scan and abnormal uptake bone scan.
Chambers et al reviewed the charts of 2000 known sickle cell patients. Fourteen patients had an episode of osteomyelitis or septic arthritis. Radiographs and bone scans were not helpful in differentiating infection from an acute bone infarct. Salmonella was the most frequent organism cultured from the osteomyelitis cases. The authors recommend bone aspiration or biopsy in an sickle cell patient with extremity pain, swelling, and a fever greater than 38.2 degrees C.
An otherwise healthy, 65-year-old male undergoes a right total knee arthroplasty without complications. Which of the following statements is recommended by the American Academy of Orthopaedic Surgeons Clinical Practice Guidelines for preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty?
Administer aspirin one week pre-operatively
Use elastic compressive stockings for 10 days pre-operatively
Obtain a post-operative duplex ultrasound of the patient for screening purposes
Administer Coumadin to maintain the patient’s INR between 1.5 and 2.5 during the post-perative period
Use mechanical compressive devices in the postoperative period
Use of mechanical compressive devices and aspirin during the postoperative period is
recommended by the American Academy of Orthopaedic Surgeons Clinical Practice Guidelines.
In 2011, the American Academy of Orthopaedic Surgeons published their Clinical Practice Guidelines for preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. A summary of those guidelines provide general recommendations for venous thromboembolic disease in patients with and without bleeding disorders. These recommendations range from strong (recommending against the use of routine post-operative duplex ultrasonography), to moderate (using mechanical compressive devices or a pharmacologic agent for prophylaxis in the post- operative period), to inconclusive (they are unable to recommend for or against specific pharmacologic prophylaxis agents). Additionally, there are recommendations based on consensus agreement of the authors (the recommendation of early mobilization in the post-operative period).
These guidelines are now much closer to in agreement with the American College of Chest Surgeons (ACCS) 2012 guidelines for VTE prophylaxis. One of the differences between the guidelines is that the AAOS guidelines do not state a specific amount of time that a pharmacologic agent should be given post- operatively while the ACCS recommends such agents for a minimum of 10-14 days.
Incorrect answers:
The definition of effect size is best described as which of the following?
Likelihood that a statistically significant difference would be found between 2 groups given that a difference truly did exist
Estimated magnitude of the difference in the means between two groups
Average of the squares of each value's deviation from the mean
Range within which it is probable that the true value lies for the whole population of patients
Probability of obtaining a result equal to or more extreme than what was actually observed assuming the null hypothesis is true
The effect size is best defined as the magnitude of the difference in the means of the control and experimental groups in a study with respect to the pooled standard deviation. Effect sizes are normally used for continuous variables in contrast to relative risk reduction which is used for dichotomous variables. Power (1), variance (3), confidence interval (4), and P value (5) are the other options provided.
Which of the following patients are at greatest risk of having a future vertebral fragility fracture?
Elderly female with prior hip fragility fracture
Elderly female with prior distal radius fragility fracture
Elderly female with prior T6 compression fragility fracture
Elderly female with a T-score of -3.0
Elderly female currently on hormone replacement therapy
History of a prior vertebral fragility fracture is the strongest predictor of a future fragility fracture. A meta-analysis by Klotzbuecher et al examined risk factors for fragility fractures and found an association between prior and subsequent fragility fractures. The strongest associations were observed between prior and subsequent vertebral fractures. They found women with preexisting vertebral fractures had an approximately 4 times greater risk of subsequent vertebral fractures than those without prior fractures. They also found this risk increases with the number of prior vertebral fractures. Other combinations of prior and future fracture sites, such as the hip or wrist, were also strongly associated, but none so high as vertebral fractures.
A 79-year-old female falls onto her right hip at home and sustains the injury shown in Figure A. She undergoes an uncemented unipolar hemiarthroplasty. During insertion of the stem into the femoral canal, the patient becomes hypotensive and hypoxic. Which of the following has most likely occurred?
Femoral shaft fracture
Inadequate fluid resuscitation during surgery
Acute myocardial infarction
Pulmonary embolism caused by dislodging of deep venous thrombosis during hip exposure
Intramedullary fat and marrow embolization
During insertion of the femoral stem, the intramedullary pressures are increased. Fat and marrow elements can become embolized into the bloodstream at this point resulting in ventilation perfusion mismatch in the lungs.
Kim et al prospectively followed 156 total hip arthroplasties including bilateral and unilateral procedures as well as cemented and uncemented procedures. They found no difference in fat embolization amongst any of the groups. However, they did find that if patients had evidence of bone marrow cells in the right atrium on the first postoperative day, they developed diffuse encephalopathy with confusion and agitation that lasted for about twenty-four hours.
Which of the following investigative studies is most useful in the definitive diagnosis of Amyotrophic Lateral Sclerosis (ALS)?
Genetic testing
MRI brain and spinal cord
Muscle biopsy
Serum protein electrophoresis and immunoelectrophoresis
Electrodiagnostic studies
The diagnosis of ALS requires a period of clinical observation to document the progressive loss of upper and lower motor function. Electrodiagnositic studies are required to make a definitive diagnosis.
Amyotrophic lateral sclerosis (ALS) is the most common degenerative disease of the motor neuron system. Nerve conduction studies and needle electromyography (EMG) are useful for confirming the diagnosis of ALS and for excluding peripheral conditions that resemble ALS. Hallmark findings in the electrodiagnosis of ALS are abnormal motor nerve conduction studies, with normal sensory nerve conduction studies. UMN signs are mild weakness, spasticity, and abnormally brisk reflexes; LMN signs are progressive weakness, wasting, and loss of reflexes and muscle tone.
Brooks et al. developed a diagnostic algorithm for the diagnosis of ALS. The algorithm is based on the degree of certainty of diagnosis, which is increased by the number of body segments that demonstrate upper motor neuron (UMN) and lower motor neuron (LMN) abnormalities. Clinical and electrophysiologic findings in 3 or more body segments is definitive of the diagnosis.
Incorrect Answers:
Radiographic changes suggestive of osteopetrosis in children are a known complication of which of the following types of medications?
TNF-alpha inhibitors
Bone morphogenic proteins
Bisphosphonates
Fluoroquinolones
RANKL antibiodies
Radiographic changes suggestive of osteopetrosis (marble bone disease) are a known complication of bisphosphonate usage. The common cellular pathway in this process is the osteoclast. Bisphosphonates target and inhibit the osteoclast, and these cells are not functioning in patients with osteopetrosis.
Whyte et al describe a case report of a 12-year-old child with idiopathic hyperphosphatasia treated with bisphosphonates who developed osteopetrosis.
Falk et al report on their small case series which showed the beneficial effects and known complications in the treatment of osteogenesis imperfecta with bisphosphonate therapy.
Marini presents a perspective article describing the off-label use of bisphosphonates in children.
What function does computerized physician order entry have on medication monitoring?
Reduces the rate of medication errors
Improves physician satisfaction
Decreases narcotic requirements by patients
Increases rates of allergy related medication errors
Improves physician knowledge about the drugs they are prescribing
Computerized physician order entry has greatest impact on reducing medication errors.
Bobb et al. studied medication errors averted by pharmacists at a 700-bed academic center and concluded that 65% of them would likely have been prevented with computerized physician order entry.
Upperman et al. reviewed medication errors at a pediatric hospital before and after implementation of a computerized physician order entry system. They found a significant decrease in adverse drug events following establishment of the computerized system.
Incorrect Answers:
2: Physician satisfaction has not been correlated with computer entry for medications.
3: Narcotic requirements are related to injury or patient characteristics, not computerized entry.
4: Allergy-related errors are decreased with use of computerized entry.
5: Physician knowledge is not necessarily increased with computerized entry.
What is the cellular mechanism of action for non-nitrogen containing bisphosphonates (such as clodronate and etidronate) to induce osteoclast apoptosis?
Inhibiting caspase
Inhibiting matrix metalloprotease
Inhibiting reverse transcriptase
Targeting of farnesyl diphosphate synthase
Creating toxic analog of adenosine triphosphate that targets mitochondria
Bisphosphonates work by one of two mechanisms. Non-nitrogren containing bisphosphonates (such as etidronate and clodronate) work by creating a toxic analog of ATP which inhibits ATP and leads to osteoclast apoptosis. Nitrogen containing bisphosphonates (such as alendronate, risedronate, and zoledronate) inhibit the enzyme farnesyl diphosphate synthase which prevents protein geranylgeranylation and prevents osteoclastic bone resorption.
Reska et. al. specifically discuss the difference between the two pathways. Non-nitrogen containing compounds inhibit ATP production and cause osteoclast apoptosis. Nitrogen containing bisphophonates inhibit protein synthesis by interrupting the cholesterol biosynthetic pathway, which prevents osteoclastic resorption.
Which class of antibiotics inhibit early fracture healing through toxic effects on chondrocytes?
cephalosporins
quinolones
penicillins
macrolides
sulfonamides
Animal models have shown that quinolones inhibit early fracture healing through a toxic effect on chondrocytes. The study by Perry et al demonstrated that fracture calluses in the animals treated with quinolones showed a lower histologic grade as compared with control animals representing a less mature callus with the presence of more cartilage and less woven bone. The study by Huddleston et al demonstrated fracture calluses in the animals treated with ciprofloxacin showed abnormalities in cartilage morphology and endochondral bone formation and a significant decrease in the number of chondrocytes compared with the controls. None of the other antibiotics listed are known to have toxic effects on chondrocytes.
A mutation of the retinoblastoma gene RB-1 leads to the development of malignancies such as retinoblastoma and osteosarcoma. Which term best characterizes the RB-1 gene?
growth factor
retro-oncogene
proto-oncogene
oncogene
tumor suppressor
A tumor suppressor is a gene whose presence normally prevents neoplasia and whose absence leads to unregulated cell growth. Two well-studied tumor suppressor genes include p53 and RB-1. P53 normally suppresses cell division by blocking the cell cycle if genetic damage is present. If it is absent or mutated, the p53 suppressing effect no longer regulates cell growth and neoplasm results. In a similar fashion, a mutation in RB-1, or the retinoblastoma gene, may leads to retinoblastoma and osteosarcoma.
Youarecounseling ayoungfemalepatientabout herfuturerisk of osteoporosis. Which of the following regarding peak bone mass (PBM) is true?
PBM is consistently attained by the end of the second decade of life in both men and women.
PBM is independent from environmental factors.
PBM correlates strongly with post-menopausal bone mineral density
Timing of PBM varies based on anatomic site.
Women attain PBM prior to men, regardless of anatomic site. Corrent answer: 4
The timing and magnitude of PBM varies based on anatomic site. PBM is often reached in the appendicular skeleton earlier than in the axial skeleton.
PBM is defined as the greatest amount of bone an individual will attain in his or her lifetime. Controversy has surrounded the timing of PBM due to significant anatomical variations as well as strong gender-based, genetic, geographic, environmental, and mechanical influences. While women may reach PBM
earlier than men in the hip, the converse has been found to be true of the spine. Furthermore, the age at which each is obtained varies widely. Though the PBM of the hip is most often achieved by the end of the second decade of life, PBM of the spine may not occur until the third or fourth decade of life. Interestingly, PBM has been found to correlate poorly with post-menopausal bone mineral density, likely a result of these strong confounding influences.
Bonjour et al. reviewed the controversy behind peak bone mass. The authors note that the gender-based difference in bone mass becomes expressed during puberty and that there is a large variability in normal values of bone mineral density between anatomic sites.
They conclude that bone mass accumulation can be completed by the end of the second decade at both the lumbar spine and femoral neck, but that this may be significantly influenced by a number of variables during growth such as genetics, diet, endocrine and mechanical factors.
Berger et al. more recently evaluated trends in peak bone mass from longitudinal data in the Canadian Multicentre Osteoporosis Study (CaMos). The authors found that peak bone mass was highly variable between the axial and appendicular skeleton. Specifically, lumbar spine PBM was reached in women
at 33-40 years, but much earlier in men at 19-33 years. Conversely, hip PBM was reached earlier in women at 16-19 years and later in men at 19-21 years. Furthermore, there was a lack of concordance between PBM and BMD over age
Question 75
A 3-year-old boy is referred to you because of "abnormal radiographs". The child's radiographs are shown in Figures A and B. This patient is at increased risk for all of following conditions EXCEPT: Review Topic
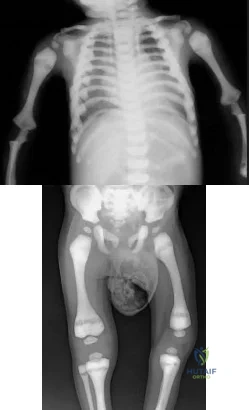
Explanation
Osteopetrosis is caused by genetic mutations affecting acidification of Howship’s lacuna. Proton pump mutations are most common (60%), followed by mutations in the chloride channel CLCN7 (12%) and mutations in carbonic anhydrase II (<5%). The difference mutations drive the clinical phenotype and lead to the three different types of osteopetrosis including: malignant infantile (AR), intermediate (AR) and benign type II (AD).
Landa et al. reviewed surgical management of osteopetrosis. For fractures, they recommend pre-drilling pin and screw holes, and using nails instead of plates. For arthroplasty, they recommend opening the medullary canal with drill bits of increasing diameter, and short femoral stems (THA).
Dietz et al. reviewed genetic disorders with orthopaedic manifestations. The gene for autosomal recessive osteopetrosis is found on 1p21-13.
Figure A is an AP radiograph of the chest and upper extremities demonstrating marked generalized bone sclerosis. Figure B is an AP radiograph of the pelvis and lower extremities showing Erlenmeyer flask femora and incidental inguinal hernia. Illustration A shows endobone (bone-within-bone) formation. Illustration B shows sandwich vertebrae (rugger jersey spine).
Incorrect Answers:
Question 76
What vessel is marked with an asterisk in Figure 44?
Explanation
REFERENCES: Agur AM, Dalley AF (eds): Grant’s Atlas of Anatomy, ed 12. Philadelphia, PA, Lippincott Williams and Wilkins, 2008.
Uflacker R: Atlas of Vascular Anatomy: An Angiographic Approach, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006.
Question 77
In a hypothetical study, an investigator uses pedometers to determine that the 20 women in his activity study averaged 2.1 million steps per year, whereas the 20 men averaged 1.8 million. The p-value for this difference was 0.09. Which of the following is a correct interpretation of the outcome of this study?
Explanation
Question 78
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
REFERENCES: Zlowodzki M, Williamson S, Cole PA, et al: Biomechanical evaluation of the less invasive stabilization system, angled blade plate, and retrograde intramedullary nail for the internal fixation of distal femur fractures. J Orthop Trauma 2004;18:494-502.
Comparison of the AO Locking Plate with the Standard Limited-Contact Dynamic Compression Plate (LC-DCP) for Fixation of Osteoporotic Humeral Shaft Fractures. David J. Hak, MD, MBA; Scott J. Hazelwood, PhD. OTA Book of Abstracts 2003.
Question 79
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 80
Overgrowth of a limb in a patient with neurofibromatosis type 1 (NF1) is most likely associated with the presence of
Explanation
REFERENCES: Alman BA, Goldberg MJ: Syndromes of orthopaedic importance, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 287-338.
Greene WB: Neurofibromatosis type I, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1584-1588.
Question 81
The patient returns 4 days after surgery and says he has noticed a red, swollen knee since yesterday. He reports a fever of 38.0°C since last evening and denies traumatic injury. He has an erythematous knee with a large, tense effusion; his range of motion is limited; and the surgical incisions are not draining. Radiographs taken in the office show no change from the immediate postsurgical images. Aspiration in the office returns 50 cc of cloudy, blood-tinged synovial fluid, and analysis of the fluid reveals a white blood cell count of 92000 (reference range 4500-11000 /µL). Which bacteria is most commonly responsible for this clinical scenario?
Explanation
This patient has a history of failed primary and revision ACL reconstructions, both times with medial meniscus repairs. The clinical scenario suggests a recurrent ACL injury with a recurrent medial meniscus tear that is now locked. The most critical risk factor for ACL reconstruction is age younger than 20 years. The meniscal repair success rate using an all-inside device is between 80% and 90%. Traditionally, it was believed that healing rates were
higher in ACL reconstruction, but current literature demonstrates a similar rate of healing associated with ACL reconstruction and no reconstruction of stable knees.
The images show a vertical femoral tunnel resulting from this patient’s prior reconstruction and revision. The MR images reveal a locked bucket-handle tear of the medial meniscus, and the examination shows a positive Lachman test finding attributable to ACL graft failure. In the setting of a young individual who has failed 2 meniscal repairs, a third repair is not indicated. In addition to a revision ACL reconstruction to stabilize the knee, a partial medial meniscectomy is indicated. An attempt at revision medial meniscus repair would be indicated if the technique were poor in the first attempt, but a failed repair otherwise should indicate the need for partial meniscectomy. The postsurgical images reveal a much more anatomic position of the femoral tunnel that should provide better rotational control of the knee, thereby improving the pivot shift (compared to the vertical femoral tunnel).
This patient has an obvious postsurgical infection based on the timing, examination, and results of the aspiration. In multiple studies of septic arthritis following ACL reconstruction, the most common pathogen was coagulase-negative staph (Staphylococcus epidermidis), followed by S. aureus. If S. aureus is the causative pathogen, the rate of necessary graft removal is higher because of the aggressive nature of this specific bacteria.
Question 82
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of
Explanation
REFERENCES: Pizzutillo PD, Hummer CD III: Nonoperative treatment for painful adolescent spondylolysis or spondylolisthesis. J Pediatr Orthop 1989;9:538-540.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 83
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?
Explanation
REFERENCES: Gusmer PB, Potter HG, Schatz JA, et al: Labral injuries: Accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-524.
Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Williams MM, Snyder SJ, Buford D Jr: The Buford complex: The “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex. A normal anatomic capsulolabral variant. Arthroscopy 1994;10:241-247.
Question 84
You have been waiting to enroll a patient into your recent institutional review board (IRB)-approved clinical research protocol. A patient is admitted who, upon initial screening, meets all inclusion criteria. However, he has late-stage dementia, and you are told by your research coordinator that this condition is an exclusionary criterion. This scenario demonstrates the need for which aspect of proper informed consent?
Explanation
Question 85
Which of the following statements is true regarding the superomedial fragment of an intra-articular calcaneus fracture?

Explanation
Question 86
What is the most important genetic element that distinguishes community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) from hospital-acquired MRSA? Review Topic
Explanation
encodes a penicillin-binding protein with a very low affinity for beta-lactam antibiotics, resulting in methicillin resistance. SCCmec mobile genetic units carry the mecA gene with additional genetic elements that together yield the multidrug-resistant strains found in healthcare environments. SCCmec type IV is specific to CA-MRSA and lacks these additional genetic elements, resulting in less multidrug resistance.
Question 87
-The patient has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they “want to get the therapy over with as fast as possible” to expedite his return to sports,and the surgeon and rehabilitation team consider their request. Compared to nonaccelerated rehabilitation,patients who follow an early accelerated rehabilitation protocol experience
Explanation
The Lachman test is the most sensitive examination for acute ACL injuries. ACL injury rates are higher in women than in men. This likely is attributable to anatomic differences (smaller notches, smaller ligaments, and different landing biomechanics). Lateral meniscal tears are more common than medial tears. The anterior drawer test is accentuated with 30 degrees of external rotation of the tibia. The MRI scan shows bone bruises consistent with an ACL tear. It is also always necessary to examine other structures of the knee in patients with ACL tears. All ligaments of the affected knee should be assessed.Lateral meniscal tears are frequently associated with ACL tears. Medial meniscal tears and posterolateral corner deficiency are also possible. Randomized clinical trials comparing an early accelerated vs nonaccelerated rehabilitation have demonstrated no significant differences in long-term results. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 88
A 78-year-old woman undergoes an uneventful semiconstrained total elbow arthroplasty through a Bryan-Morrey approach. Her immediate postoperative management should include which of the following? Review Topic
Explanation
Question 89
Figure 1 is the MR image of a 36-year-old athlete who is tackled from behind and falls forward onto his left knee. He has pain, swelling, and stiffness. Examination includes a moderate effusion, positive quadriceps active test, and normal Lachman test finding. The injured structure is composed of an

Explanation
Numerous strategies have been described to reduce the risk, including use of a posteromedial accessory incision to allow finger retraction of the popliteal neurovascular bundle, oscillating drills to prevent excessive soft-tissue entanglement, and tapered (rather than square) drill bits that may minimize cut-out of sharp edges as drilling reaches the posterior tibial cortex. Knee extension lessens, rather than increases, the distance between the posterior tibia and the neurovascular bundle and increases, not lessens, risk for vascular injury.
Question 90
What type of nerve palsy is most common following elbow arthroscopy?
Explanation
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of elbow arthroscopy.
J Bone Joint Surg Am 2001;83:25-34.
Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 91
Figure 53 shows the arteriogram of a 45-year-old man who has severe vasculitis. What do the findings show?
Explanation
REFERENCE: Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadephia, PA, Mosby-Year Book, 1998, p 110.
Question 92
A 32-year-old volleyball player has dull posterior shoulder pain. An examination reveals moderate external rotation weakness with his arm at his side, but normal strength on supraspinatus isolation. Deltoid and supraspinatus bulk appear normal, although there appears to be mild infraspinatus atrophy. Sensation is normal throughout the shoulder and shoulder girdle. What is the most likely diagnosis?
Explanation
This clinical scenario describes a patient with an isolated injury affecting the infraspinatus muscle. The anatomic location of such a lesion would be at the spinoglenoid notch, at which the suprascapular nerve may be compressed distal to its innervation of the supraspinatus but proximal to the infraspinatus innervation. A calcified transverse scapular ligament would also affect the suprascapular nerve but is proximal to the innervation of both muscles. Quadrilateral space syndrome would affect innervation of the deltoid (and teres minor). Parsonage-Turner syndrome is a more diffuse, and often severely painful, brachial plexus neuropathy.
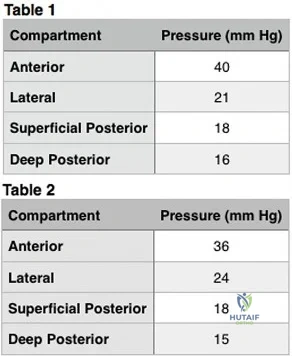
Question 93
A 66-year-old male sustains an open crush injury to his right lower leg with significant skin loss. His history is significant for COPD, diabetes controlled with an insluin pump, and testicular cancer treated with bleomycin twenty years ago. A radiograph of the chest shows a pneumothorax which is treated with a thoracostomy tube. Which of the following is not a contraindication to hyperbaric oxygen treatment for this patient?

Explanation
Hyperbaric oxygen therapy potentially can provide enhanced oxygen delivery to peripheral tissues affected by vascular disruption, cytogenic and vasogenic edema, and cellular hypoxia caused by extremity trauma. The idea behind HBO is to provide enhanced oxygen delivery to peripheral tissues affected by vascular disruption, cytogenic and vasogenic edema, and cellular hypoxia caused by extremity trauma.
Greensmith et al provide a review of HBO therapy and discuss the relative and absolute contraindications and indications for this treatment. They report in patients with crush injury or early compartment syndrome, hyperbaric oxygen therapy may reduce the penumbra of cells at risk for delayed necrosis and secondary ischemia. They report that both animal studies and prospective human clinical trials suggest the benefits of such therapy.
Buettner et al found that based on clinical evidence and cost analysis, medical institutions that treat open fractures and crush injuries are justified in incorporating HBO theray as a standard of care.
Illustration A shows an example of a hyperbaric oxygen(HBO) chamber. Incorrect Answers:
Question 94
Figure 1 is the MRI scan of a patient with recurrent knee instability, which persists after a period of nonsurgical treatment. Anatomic reconstruction of the torn ligament is recommended. What radiographic finding is the most important independent predictor of recurrent instability following surgery?
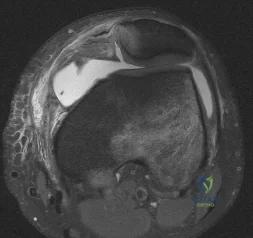
Explanation
Question 95
A 68-year-old woman with serologically proven rheumatoid arthritis underwent an open synovectomy and radial head resection 10 years ago. She now has severe pain that has failed to respond to nonsurgical management. Examination reveals a flexion arc of greater than 90 degrees. Radiographs are shown in Figures 15a and 15b. What is the most appropriate management?
Explanation
REFERENCES: Whaley A, Morrey BF, Adams R: Total elbow arthroplasty after previous resection of the radial head and synovectomy. J Bone Joint Surg Br 2005;87:47-53.
Maenpaa HM, Kuusela PP, Kaarela KK, et al: Reoperation rate after elbow synovectomy in rheumatoid arthritis. J Shoulder Elbow Surg 2003;12:480-483.
Schemitsch EH, Ewald FC, Thornhill TS: Results of total elbow arthroplasty after excision of the radial head and synovectomy in patients who had rheumatoid arthritis. J Bone Joint Surg Am 1996;78:1541-1547.
Question 96
A 4-month-old infant is unable to flex her elbow as a result of an obstetrical brachial plexus palsy. This most likely illustrates a predominate injury to what structure?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 28-29.
Wolock B, Millesi H: Brachial plexus-applied anatomy and operative exposure, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991,
pp 1255-1272.
Zancolli E: Reconstructive surgery in brachial plexus sequelae, in Gupta A, Kay S, Scheker L (eds): The Growing Hand. London, England, Mosby, 1999, p 807.
Question 97
A 10-year-old boy with a history of retinoblastoma now reports right knee pain. AP and lateral radiographs are shown in Figures 3a and 3b. What is the most likely diagnosis?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Chauveinc L, Mosseri V, Quintana E, Desjardins L, Schlienger P, Doz F, Dutrillaux B: Osteosarcoma following retinoblastoma: Age at onset and latency period. Ophthalmic Genet 2001;22:77-88.
Question 98
A 37-year-old man has had isolated chronic knee swelling for the past 6 months. He denies any history of specific trauma. Examination reveals a large effusion with a stable knee, but the remainder of the examination is normal. Plain radiographs are unremarkable. An MRI scan reveals a large effusion without meniscal injury. An arthroscopic image of the suprapatellar pouch is shown in Figure 23. What is the most likely diagnosis?
Explanation
REFERENCES: Flandry FC, Hughston JC, Jacobson KE, Barrack RL, McCann SB, Kurtz DM: Surgical treatment of diffuse pigmented villonodular synovitis of the knee. Clin Orthop 1994;300:183-192.
Zvijac JE, Lau AC, Hechtman KS, Uribe JW, Tjin-A-Tsoi EW: Arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 1999;15:613-617.
Question 99
Figure 21 is the intraoperative fluoroscopic image of a 40-year-old man who felt a pop during a twisting injury to his right ankle. He underwent open reduction and internal fixation (ORIF) of a bimalleolar ankle fracture. During the surgery the medial and lateral malleoli fractures were reduced and rigidly was internally fixed. Following fracture fixation, which additional test is recommended to ensure mortise stability?

Explanation
Following ORIF of a known osseous injury, stress testing of the syndesmosis is recommended, especially for pronation-external rotation injuries. The Cotton test applies a laterally directed force to the fibula to assess for widening of the distal tibiofibular joint space. A positive Cotton test result indicates that syndesmotic stabilization is indicated. The Thompson test is used to determine Achilles tendon integrity. The squeeze test is a clinical, not intraoperative, assessment of syndesmotic injury. The anterior drawer test assesses the integrity of the anterior talofibular ligament.
RECOMMENDED READINGS
Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg. 2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882. View Abstract at PubMed
Pakarinen H, Flinkkilä T, Ohtonen P, Hyvönen P, Lakovaara M, Leppilahti J, Ristiniemi J. Intraoperative assessment of the stability of the distal tibiofibular joint in supination-external rotation injuries of the ankle: sensitivity, specificity, and reliability of two clinical tests. J Bone Joint Surg Am. 2011 Nov 16;93(22):2057-61. doi: 10.2106/JBJS.J.01287. PubMed PMID:
Question 100
A 77-year-old man has had increasing right knee pain for the past 3 months. A radiograph and coronal T 1 -weighted MRI scan are shown in Figures 19a and 19b. A biopsy specimen is shown in Figure 19c. What is the most likely diagnosis?
Explanation
REFERENCES: Mitchell AD, Ayoub K, Mangham DC, et al: Experience in the treatment of dedifferentiated chondrosarcoma. J Bone Joint Surg Br 2000;82:55-61.
Frassica FJ, Unni KK, Beabout JW, Sim FH: Dedifferentiated chondrosarcoma: A report of the clinicopathological features and treatment of seventy-eight cases. J Bone Joint Surg Am 1986;68:1197-1205.
