Orthopedic Surgery Board Review MCQs: Trauma, Spine & Upper Extremity | Part 235

Key Takeaway
This page offers Part 235 of a comprehensive orthopedic surgery board review quiz, specifically designed for orthopedic surgeons and residents preparing for their OITE and AAOS certification exams. It features 100 high-yield MCQs covering Ankle, Dislocation, Fracture, and Nerve topics, presented in both study and exam modes to optimize your preparation.
About This Board Review Set
This is Part 235 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 235
This module focuses heavily on: Ankle, Dislocation, Fracture, Nerve.
Sample Questions from This Set
Sample Question 1: A 24-year-old dancer reports posterior ankle pain when in the “en pointe” position. Examination reveals posteromedial tenderness, no pain reproduction with passive forced planter flexion, and pain with motion of the hallux. What is the most...
Sample Question 2: A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5...
Sample Question 3: -What is the most common nerve injury following a Monteggia fracture-dislocation of the forearm in adults?...
Sample Question 4: A 45-year-old male falls off his motorcycle and injures his arm. AP and lateral radiographs reveal an ulnar shaft fracture, 30 degrees apex anterior, and a radial head dislocation. Which direction is the radial head most likely dislocated?...
Sample Question 5: What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 24-year-old dancer reports posterior ankle pain when in the “en pointe” position. Examination reveals posteromedial tenderness, no pain reproduction with passive forced planter flexion, and pain with motion of the hallux. What is the most likely diagnosis?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 249-261.
Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
Question 2
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient?
Explanation
REFERENCES: Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 3
- What is the most common nerve injury following a Monteggia fracture-dislocation of the forearm in adults?
Explanation
Question 4
A 45-year-old male falls off his motorcycle and injures his arm. AP and lateral radiographs reveal an ulnar shaft fracture, 30 degrees apex anterior, and a radial head dislocation. Which direction is the radial head most likely dislocated?

Explanation
Question 5
What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?
Explanation
REFERENCES: Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
Steinmann SP, Linsheid RL: Pisotriquetral loose bodies. J Hand Surg 1997;22:918-921.
related link ortho mcqs bank
Question 6
Figure 17 shows the AP radiograph of a 75-year-old man with right hip pain. The femoral component is loose. The mechanism of loosening is most likely secondary to
Explanation
REFERENCES: Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-238.
Peter CL, Rivero DP, Kull LR, et al: Revision total hip arthroplasty without cement: Subsidence of proximally porous-coated femoral components. J Bone Joint Surg Am 1995;77:1217-1226.
Question 7
A 67-year-old woman has a painful, arthritic proximal interphalangeal (PIP) joint, and nonsurgical measures have failed to improve the pain. What implant and joint replacement approach combination has been demonstrated to have the lowest rate of revision surgery?
Explanation
A recent systematic review compared silicone replacement, pyrocarbon replacement, and surface replacement arthroplasty for PIP arthritis. Silicone arthroplasty through a volar approach showed the greatest gains in arc of motion and had the lowest rate of revision surgeries. The rates of revision surgeries from low to high for each type of arthroplasty were 6% for silicone volar, 10% for silicone lateral, 11%
Surface replacement arthroplasty through a volar
for silicone dorsal, 18% for surface replacement dorsal, and 37% for surface replacement volar. Revision surgeries include implant replacement (to silicone or maintaining the surface replacement), arthrodesis, explantation, amputation, and other procedures.
approach showed the highest revision rate, the worst gain in arc of motion, and the greatest extension lag. However, substantial pain relief and higher satisfaction still were reported after surface replacement arthroplasty, regardless of the complications.
Question 8
Clinical evidence suggests that grafts for replacing a torn anterior cruciate ligament often stretch after surgery. What is the most probable mechanism for this behavior?
Explanation
REFERENCES: Boorman RS, Thornton GM, Shrive NG, et al: Ligament grafts become more susceptible to creep within days after surgery. Acta Orthop Scand 2002;73:568-574.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 596-609.
Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O’Keefe RJ,
Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 9
A 57-year-old woman with diabetes mellitus has purulent drainage from a lateral incision after undergoing open reduction and internal fixation of a displaced ankle fracture 10 days ago. Examination reveals moderate erythema and a foul odor coming from the wound. Cultures are obtained. What is the next most appropriate step in management?
Explanation
REFERENCES: Carragee EJ, Csongradi JJ, Bleck EE: Early complications in the operative treatment of ankle fractures: Influence of delay before operation. J Bone Joint Surg Br 1991;73:79-82.
Blotter RH, Connolly E, Wasan A, Chapman MW: Acute complications in the operative treatment of isolated ankle fractures in patients with diabetes mellitus. Foot Ankle Int 1999;20:687-694.
Question 10
- Figure 67 shows the AP radiograph of both knees of a 26-year-old woman. A review of the patient’s medical record will most likely reveal a history of
Explanation
Question 11
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Explanation
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 12
On MRI, a nonsanguinous effusion has what appearance?
Explanation
REFERENCES: Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
White EM: Magnetic resonance imaging in synovial disorders and arthropathy of the knee. Magn Reson Imaging Clin N Am 1994;2:451-461.
Question 13
Which of the following changes in the parameters of the gait cycle occurs in the transition from normal walking to running?
Explanation
Examination of a 5-year-old child who has fibular hemimelia reveals the foot has two rays and is stiff in equinus and valgus. The level of the foot is just proximal to the midshaft of the contralateral tibia, and the knee has full active flexion and extension, but slight valgus. Treatment should include
Amputation through the midshaft of the tibia
Correction of the foot deformity and lengthening with a ring fixator
Knee disarticulation
Ankle disarticulation
Ankle disarticulation and contralateral epiphyseodesis of the proximal tibia Answer: 4
Congenital absence of the fibula, also called fibula hemimelia, has several manifestations. These range from complete absence of the fibula with missing lateral rays of the foot (i.e. terminal longitudinal deficiency) to absence of only a portion of the fibula without foot involvement (i.e. intercalary longitudinal; deficiency). Congenital fibular deficiency usually occurs sporadically without a known cause. The child with complete absence of the fibula presents clinically with an anterolateral bow of the tibia, an equinovalgus deformity of the foot, and a tarsal coalition. The talotibial joint is usually malformed, with the fused talocalcaneus having a flat upper surface that articulates with the tibia in a valgus and equinus position. The foot may be missing one or two lateral rays. There is always significant shortening of the epsilateral femur. Treatment: There is a reasonable consensus that complete fibular hemimelia is best treated by performing an ankle disarticulation in early childhood and fitting a Syme-type prosthesis. Children with lesser (<5cm) at birth may be a candidate for lengthening procedures, but the exact indications and results of these procedures have not been well defined. Children with large discrepancies (>5cm) at birth and those with major foot deformities are better managed with amputation.
Question 14
A 22-year-old man sustained a cervical fracture-dislocation of the C5-6 level in a motor vehicle accident along with an associated spinal cord injury. Six months after his injury, he has 4 out of 5 biceps on the left, with 5 out of 5 biceps on the right. Deltoid is graded at 5 out of 5 bilaterally. There is 0 strength in the triceps, wrist flexors, wrist extensors, and digital extensors. He has neurogenic bowel and bladder with absent perianal sensation and no voluntary motor in the lower extremities. The patient's neurologic deficit is best categorized as which of the following? Review Topic
Explanation
Question 15
A 35-year-old male suffers an anterior column acetabular fracture during a motor vehicle collision, and subsequently undergoes percutaneous acetabular fixation. Intraoperatively, fluoroscopy is positioned to obtain an obturator oblique-inlet view while placing a supraacetabular screw. Which of the following screw relationships is best evaluated with this view?

Explanation
Starr et al review their initial results and technique of closed or limited open reduction and percutaneous fixation of acetabular fractures. They defined two groups of patients who may benefit from this technique; elderly patients with multiple comorbidities to facilitate early mobilization and restore hip morphology, and young patients with elementary fracture patterns and multiple associated injuries.
Starr et al describe their operative technique and outcomes for a case series of 3 patients using percutaneous acetabular fixation to augment open reduction of acetabular fractures. The authors state that, for placement of an
anterior colum ramus screw, an iliac oblique-inlet (not obturator oblique-inlet) will ensure that the screw is within the medullary canal of the ramus and does not exit anterior or posterior.
Gardner and Nork describe a technique for placement of a large femoral distractor in the supra-acetabular region to compress displaced posterior pelvic ring injuries. They note that the obturator oblique-inlet view is necessary to view the entire length of the pin as well as to ensure that pin remains in bone.
Incorrect answers:
Question 16
A 26-year-old weight lifter has had increasing pain in his left shoulder for 4 months. His symptoms do not improve with nonsurgical treatment that included activity modification, anti-inflammatory medication, and corticosteroid injections. He undergoes arthroscopic distal clavicle excision with resection of the distal 2.5 cm of clavicle. Three months after surgery, he reports persistent pain and popping in his shoulder. An examination demonstrates anterior and posterior instability of the distal clavicle without gross deformity. Radiographs are unremarkable. What is the most likely cause of distal clavicle instability after surgery?
Explanation
Overresection of the distal clavicle can result in disruption of the acromioclavicular ligamentous complex, which inserts at an average of 22.9 mm from the distal clavicle. A comparison of arthroscopic and open distal clavicle excision demonstrated less pain in the arthroscopic group, with no difference in patient satisfaction or shoulder function between groups. Injuries to the conoid and trapezoid ligaments occur with high-grade acromioclavicular separations, resulting in superior migration of the distal clavicle relative to the acromion. Release of the coracoacromial ligament typically is not performed during distal clavicle excision.

Question 17
Figures 46a through 46d are the injury radiographs and postsurgical open treatment radiographs of a 13-year-old girl who fell while on a trampoline and sustained an injury to her right-dominant elbow. The skin is closed and she has normal vascular and neurologic examination findings. Which complication most likely could occur as a result of this injury and treatment?
Explanation
This girl sustained a fracture dislocation of the elbow with a severely displaced and rotated radial neck fracture. Required treatment was open reduction and internal fixation (ORIF). Less severely displaced radial neck fractures can be treated with closed reduction, percutaneous pinning, or flexible nail manipulation. In this scenario, interposed capsular tissue and rotation of the radial head were indications for ORIF. ORIF is associated with a higher risk for poor
outcomes. Complications following ORIF of radial neck fractures in children include posterior interosseous neuropraxia, valgus angulation, premature closure of the radial head physis, AVN of the radial head, nonunion, and elbow stiffness. Stiffness is most common. Compartment syndrome, infection, and anterior interosseous nerve palsy are less common complications.

CLINICAL SITUATION FOR QUESTIONS 47 THROUGH 50
A 6-year-old boy arrives at the emergency department with forearm pain. Today he was picking up his backpack when he felt a pop in his forearm that resulted in the current injury. His history is significant for 6 other fractures treated nonsurgically. His mother states that she had 15 fractures during childhood but is healthy now. Both the boy and his mother have blue sclera. Figures 47a and 47b are the radiographs of his injured forearm.
Question 18
A 22-year-old woman reports a 4-year history of worsening low back and left lower extremity pain following a motor vehicle accident. Management consisting of physical therapy, chiropractic manipulation, and interventional pain management, including sacroiliac joint injections and epidural steroid injections, has failed to provide relief. A sagittal T 2 -weighted MRI scan is shown in Figure 8. No nerve root compression is seen on axial images. She is currently working and lives with her fiancé. She smokes half a pack of cigarettes per day and reports depression on her health history. She is being maintained on narcotic analgesics and is having increasing difficulty performing her activities of daily living secondary to pain. What is the most appropriate management at this time?
Explanation
REFERENCES: Carragee EJ, Paragioudakis SJ, Khurana S: 2000 Volvo Award winner in clinical studies: Lumbar high-intensity zone and discography in subjects without low back problems. Spine 2000;25:2987-2992.
Pneumaticos SG, Reitman CA, Lindsey RW: Diskography in the evaluation of low back pain.
J Am Acad Orthop Surg 2006;14:46-55.
Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Carragee EJ: Clinical practice: Persistent low back pain. N Engl J Med 2005;352:1891-1898.
Question 19
below show the radiographs obtained from a year-old woman with a year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?
Explanation
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 20
Which complication is most common after syndesmotic fixation?
Explanation
The injury radiographs reveal a supination external rotation IV ankle fracture with evidence of medial clear space widening exceeding 4 mm and an increase relative to the superior tibiotalar clear space. This indicates injury to the deltoid ligament and necessitates surgical reduction and fixation to restore and maintain ankle stability. Following stabilization of the fibula, an intraoperative stress examination of the syndesmosis such as an external rotation stress test under fluoroscopy or lateral pull on the fibula (the Cotton test) should be performed to determine the integrity of the syndesmosis. Radiographic evidence of tibiofibular clear space widening, medial clear space widening with external rotation, and lateral displacement of the distal fibula when pulled is consistent with syndesmotic injury. In contrast to the presurgical stress test, once the fibula has been reduced and stabilized lateral talar translation can occur only if the syndesmosis is injured in addition to the deltoid ligament. Failure of the syndesmotic screw without evidence of malalignment of the mortise and a pain-free ankle are not indications for further surgery because these patients have satisfactory outcomes when compared to those who have intact or removed screws. Hardware removal following fibula ORIF is indicated when patients have pain directly related to hardware prominence. Resolution of joint pain or stiffness is not a reliable outcome following hardware removal. Although fibular fracture can occur, this is a rare complication. Malreduction of the syndesmosis is the most common complication following ORIF of the syndesmosis and is improved with direct visualization; however, malreduction still may occur with direct visualization.
RECOMMENDED READINGS
Manjoo A, Sanders DW, Tieszer C, MacLeod MD. Functional and radiographic results of patients with syndesmotic screw fixation: implications for screw removal. J Orthop Trauma. 2010 Jan;24(1):2-6. doi: 10.1097/BOT.0b013e3181a9f7a5. PubMed PMID: 20035170. View
Abstract at PubMed
Jenkinson RJ, Sanders DW, Macleod MD, Domonkos A, Lydestadt J. Intraoperative diagnosis of syndesmosis injuries in external rotation ankle fractures. J Orthop Trauma. 2005 Oct;19(9):604-9. PubMed PMID: 16247304. View Abstract at PubMed
Stark E, Tornetta P 3rd, Creevy WR. Syndesmotic instability in Weber B ankle fractures: a clinical evaluation. J Orthop Trauma. 2007 Oct;21(9):643-6. PubMed PMID: 17921840. View Abstract at PubMed
Brown OL, Dirschl DR, Obremskey WT. Incidence of hardware-related pain and its effect on functional outcomes after open reduction and internal fixation of ankle fractures. J Orthop Trauma. 2001 May;15(4):271-4. PubMed PMID: 11371792. View Abstract at PubMed
Question 21
A 9-year-old child sustained a fracture-dislocation of C-5 and C-6 with a complete spinal cord injury. What is the likelihood that scoliosis will develop during the remaining years of his growth?
Explanation
REFERENCES: Brown JC, Swank SM, Matta J, et al: Late spinal deformity in quadriplegic children and adolescents. J Pediatr Orthop 1984;4:456-461.
Lancourt JE, Dickson JH, Carter RE: Paralytic spinal deformity following traumatic spinal-cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
Dearolf WW III, Betz RR, Vogel LC, et al: Scoliosis in pediatric spinal cord-injured patients.
J Pediatr Orthop 1990;10:214-218.
Question 22
An athletic 55-year-old man reports a painless mass in the anterior aspect of the thigh that appeared 3 weeks ago and has not changed in size. The patient denies any history of trauma. Examination reveals a firm, well-defined nontender mass in the anterior thigh and no inguinal adenopathy or cutaneous changes. Plain radiographs are unremarkable. T1- and T2-weighted MRI scans are shown in Figures 44a and 44b. What is the most likely diagnosis?
Explanation
REFERENCES: Sim FH, Frassica FJ, Frassica DA: Soft-tissue tumors: Diagnosis, evaluation and management. J Am Acad Orthop Surg 1994;2:202-211.
Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft-tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547.
Question 23
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome?
Explanation
REFERENCES: Lalonde F, Letts M, Yang JP, et al: An analysis of burst fractures of the spine in adolescents. Am J Orthop 2001;30:115-120.
Clark P, Letts M: Trauma to the thoracic and lumbar spine in the adolescent. Can J Surg 2001;44:337-345.
Been HD, Bouma GJ: Comparison of two types of surgery for thoraco-lumbar burst fractures: Combined anterior and posterior stabilization vs posterior instrumentation only. Acta Neurochir (Wien) 1999;141:349-357.
Question 24
Which of the following findings is considered a contraindication for posterior decompression (with or without fusion) for myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Malone DG, Benzel EC: Laminotomy and laminectomy for spinal stenosis causing radiculopathy or myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 817-823.
Question 25
A 26-year-old woman who noted right-sided lumbosacral pain 10 days ago while vacuuming now reports that the pain has intensified. She denies any history of back problems. No radicular component is present, and her neurologic examination is normal. The next most appropriate step in management should consist of
Explanation
REFERENCES: Bigos S, Boyer O, Braen GR, et al: Acute low back pain in adults: Clinical practice guideline No. 14. AHCPR Publication No. 95-0642. Rockville, MD, Agency for Health Care Policy and Research, Public Health Service, US Department of Health and Human Services, December, 1994.
Deyo RA: Conservative therapy for low back pain: Distinguishing useful from useless therapy. JAMA 1983;250:1057-1062.
Question 26
Which of the following factors has been shown to increase mortality in poly-trauma patients with severe head injuries?

Explanation
Chesnut et al demonstrated that hypotension (SBP <90mmHg) was profoundly detrimental, occurring in 35% of these patients and associated with 150% increase in mortality.
Pietropaoli et al reviewed 53 patients with severe head injuries and required early surgical intervention (surgery within 72 hours of injury). All patients were initially normotensive on arrival. There were 17 patients (32%) who developed intra-operative hypotension and 36 (68%) who remained normotensive throughout surgery. The mortality rate was 82% in the IH group and 25% in the normotensive group.
Question 27
A 34-year-old man presents to clinic with 4 months of right elbow pain. He began going to the gym and playing squash about 3 months ago. On exam, he is tender over the lateral aspect of the elbow and has pain with resisted wrist extension. Which of the following choices lists the correct compartment of the muscle typically involved in this disease and then lists its antagonist muscle? Review Topic
Explanation
Lateral epicondylitis is an overuse injury, typically secondary to repetitive pronation and supination motion in extension, that leads to inflammation of the ECRB origin at the elbow. Histological analysis typically shows vascular hyperplasia and disorganized collagen. Clinically, patients will have pain over the lateral elbow exacerbated by resisted wrist extension. ECRB, the most commonly involved muscle origin, is innervated by the deep branch of the radial nerve and inserts on the base of the 3rd metacarpal. As it is radial wrist extensor, its antagonist is the ulnar sided wrist flexor.
Brummel et al. reviewed the clinical presentation and management options for lateral epicondylitis. They report acute symptoms in younger patients and chronic symptoms in older patients. NSAIDs, extensor stretching and activity modification are the mainstay of nonsurgical treatment.
Bunata et al. studies 85 cadavar elbows to determine anatomic factors contributing to tennis elbow. They found that the ECRB undersurface rubs against the lateral capitellium in elbow extension leading to tendinosis.
Illustration A is cross-sectional diagram of the forearm with muscle bellies labeled. Notice the location of ECRB in the mobile wad. Illustration B is a coronal T2 MRI showing fluid signal and undersurface tearing near the extensor origin as can be seen in lateral epicondylitis.
Incorrect Answers:
1-4: The ECRB is in the mobile wad and its antagonist is flexor carpi ulnaris. All other answers are incorrect.
Question 28
Joint contact pressure in normal or artificial joints can best be minimized by what mechanism?
Explanation
(eg, a walking aid) will decrease the stress. Similarly, any mechanism that increases the area over which the load is distributed (eg, using a more conforming set of articular surfaces in a knee joint arthroplasty) will also decrease the stress. Other mechanisms that influence joint contact pressure include the elastic modulus of the materials (cartilage in the case of natural joints and polyethylene in joint arthroplasty) and the thickness of the structures through which the joint loads pass.
REFERENCES: Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in UHMWPE components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 265-274.
Question 29
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
Explanation
REFERENCES: Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337.
Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271.
Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Sneppen O, Fruensgaard S, Johannsen HV, Olsen BS, Sojbjerg JO, Anderson NH: Total shoulder replacement in rheumatoid arthritis: Proximal migration and loosening. J Shoulder Elbow Surg 1996;5:47-52.
Question 30
The knee arthroplasty type associated with the highest 5-year revision rate is
Explanation
Revision rates for UKA at 10 years are lower than 5% at specialty centers. However, the 10-year revision rate associated with UKA in registries such as the National Joint Registry for England and Wales is 2 to 3 times that of TKA. Among partial knee replacements, patellofemoral arthroplasty is associated with the highest revision rate at every time interval.

CLINICAL SITUATION QUESTIONS 167 THROUGH 169
Figures 167a and 167b are the radiographs of a middle-age man. He is a noncompliant patient who has severe insulin-dependent diabetes and a below-knee amputation on the right side. He is usually in a wheelchair, does not use a prosthesis, transfers using a walker, and resides in an institution. He had an infection in the left leg years ago, which was treated successfully with intravenous antibiotics (the details are unknown). His left knee is mildly painful, swollen but not warm, has limited range of motion (40-140 degrees), and is grossly unstable.
Question 31
A 40-year-old woman sustains a flexion injury to her neck. Physical examination is normal. A lateral radiograph of the cervical spine is shown in Figure 57a. MRI scans of the cervical spine are shown in Figures 57b and 57c. Treatment should include
Explanation
REFERENCES: Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1120-1128.
Coe JD, Warden KE, Sutterlin CE, et al: Biomechanical evaluation of cervical spinal stabilization methods in a human cadaveric model. Spine 1989;14:1122-1131.
Question 32
A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Chan KW, McAdams TR: Central screw placement in percutaneous screw scaphoid fixation: A cadaveric comparison of proximal and distal techniques. J Hand Surg Am 2004;29:74-79.
Bedi A, Jebson PJ, Hayden RJ, et al: Internal fixation of acute non-displaced scaphoid waist fractures via a limited dorsal approach: An assessment or radiographic and functional outcomes. J Hand Surg Am 2007;32:326-333.
McCallister WV, Knight J, Kaliappan R, et al: Central placement of the screw in simulated fractures of the scaphoid waist: A biomechanical study. J Bone Joint Surg Am 2003;85:72-77.
Question 33
A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of
Explanation
REFERENCES: Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Krakauer JD, Stern PJ: Hinged device for fractures involving the proximal interphalangeal joint. Clin Orthop 1996;327:29-37.
Question 34
Figures 132a and 132b are the lateral and anteroposterior radiographs of a 15-year-old boy with a 6-month history of recurrent, activity-related posterior elbow pain when pitching. Two separate 6-week periods of rest have failed to provide relief. What is the next best step to enable him to return to play? Review Topic

Explanation
cessation from throwing followed by appropriate physiotherapy, surgical management with cannulated screw fixation is appropriate and has been demonstrated to have favorable success rates. Hinged-elbow bracing will not facilitate healing or return to play. Long-arm casting is likely to result in stiffness and would not be unreasonable for a short duration at the onset of symptoms, but is less likely to be helpful at this point. Plate fixation is not indicated for treatment of this injury.
Question 35
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following? Review Topic
Explanation
the restraints to medial translations of the biceps have been disrupted. Attempts at recentering the biceps have not been successful, and clinical results appear to be improved when tenodesis or tenotomy is employed in the treatment of the unstable biceps associated with subscapularis tears.
Question 36
Your 25-year-old patient complains of anterior knee pain after retrograde femoral nailing for a diaphyseal fracture and asks you why you didn’t perform antegrade nailing as he has seen on the internet. You tell him that retrograde nailing is your preferred technique over antergrade nailing for diaphyseal femoral fractures because it has been shown to have?

Explanation
Question 37
A 22-year-old man who sustained a Gustilo-Anderson grade IIIC open fracture of the right tibia and fibula was treated with an immediate open transtibial amputation. After two serial debridements, he underwent wound closure with a posterior myocutaneous soft-tissue flap. What is the preferred method of early rehabilitation?
Explanation
REFERENCES: Burgess EM, Romano RL, Zettl JH: The Management of Lower Extremity Amputations. Washington, DC, US Government Printing Office, 1969, also at: www.prs-research.org.
Smith DG, McFarland LV, Sangeorzan BJ, et al: Postoperative dressing and management strategies for transtibial amputations: A critical review. J Rehabil Res Dev 2003;40:213-224.
Question 38
-An otherwise healthy 15-year-old wrestler has a 6-cm cutaneous lesion on the posterior aspect of his right elbow that he reports as a spider bite. What is the most likely diagnosis?
Explanation
Figure 44 is the MRI scan of a 14-year-old soccer player who injured his right knee during a game.He describes feeling a “pop” and he needed help walking off the field. His knee is visibly swollen. A Lachman test demonstrates asymmetry with no endpoint.
Question 39
Figures 1 and 2 are the radiographs of a 24-year-old male wrestler who underwent surgery for recurrent shoulder dislocations using coracoid autograft. At his first postoperative visit, the patient complains of decreased sensation on the lateral aspect of his forearm. The patient’s symptoms are most likely due to injury of the
Explanation
Question 40
Figures 157a and 157b are the radiographs of a 22-year-old laborer who has progressively increasing lateral knee pain that is unresponsive to nonsurgical treatment. What is the most appropriate treatment at this time?
Explanation
Distal femoral osteotomy is the preferred surgical treatment for this young patient. A varus-producing proximal tibial osteotomy is not indicated with valgus deformity and lateral femoral hypoplasia. Osteotomy on the tibial side would result in obliquity of the joint line and improper loading. Lateral unicompartmental arthroplasty or TKA are both less appropriate for this patient, who will be placing high demands on his knee; these demands will pose high risk for premature failure of an artificial knee implant and could necessitate revision surgery.
Question 41
The carpal tunnel canal is narrowest (smallest cross-sectional area) at what level?
Explanation
REFERENCES: Cobb TK, Dalley BK, Posteraro RH, et al: Anatomy of the flexor retinaculum. J Hand Surg Am 1993;18:91-99.
Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow and Shoulder. Rosemont, IL, American Society of Surgery of the Hand, 2003, p 300.
Question 42
below show the clinical photograph and radiograph obtained from a year-old man who has deformity and pain 1 year after primary total hip arthroplasty. What is the reason for the observed deformity?
Explanation
Figure 1 reveals an external rotation deformity of the right lower extremity. This deformity can have numerous causes, including extra-articular deformity. Figure 2 reveals a loose, subsided femoral component. Femoral stems typically subside into retroversion due to proximal femoral biomechanics, which cause a compensatory external rotation deformity. The combined findings from both images suggest an external rotation deformity most likely related to subsidence into retroversion.
Question 43
Which of the following prognostic indicators is associated with the least favorable outcome for patients newly diagnosed with osteosarcoma?
Explanation
REFERENCES: Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790.
Heck RK, Stacy GS, Flaherty MJ, et al: A comparison study of staging systems for bone sarcomas. Clin Orthop Relat Res 2003;415:64-71.
Kager L, Zoubeck A, Potschger U, et al: Primary metastatic osteosarcoma: Presentation and outcome of patients treated on neoadjuvant Cooperative Osteosarcoma Study Group protocols.
J Clin Oncol 2003;21:2011-2018.
Question 44
A collegiate division I football player ruptures his anterior cruciate ligament (ACL). After counseling him, you agree to perform a double-bundle ACL reconstruction. Which of the following is a correct statement for this technique? Review Topic
Explanation
Question 45
A 55-year-old man reports increasing weakness in his arms that has progressed to his lower limbs, resulting in frequent tripping and falling. Examination reveals weakness in shoulder abduction and external and internal rotation bilaterally. Fasciculation is noted. He also has weakness in elbow flexion and extension bilaterally, and his grip strength is diminished. An electromyogram and nerve conduction velocity studies show decreased amplitude of compound motor action potential, slightly slowed motor conduction velocity, and denervation signs with decreased recruitment in all extremities. The sensory study is normal. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: de Carvalho M, Johnsen B, Fuglsang-Frederiksen A: Medical technology assessment: Electrodiagnosis in motor neuron diseases and amyotrophic lateral sclerosis. Neurophysiol Clin 2001;31:341-348.
Daube JR: Electrodiagnostic studies in amyotrophic lateral sclerosis and other motor neuron disorders. Muscle Nerve 2000;23:1488-1502.
Troger M, Dengler R: The role of electromyography (EMG) in the diagnosis of ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1:S33-S40.
Question 46
Increased hip intracapusular pressures can lead to diminished femoral head perfusion. What leg position has been shown to create the lowest intracapsular hip pressures after femoral neck fracture?

Explanation
Question 47
A 21-year-old man has had posterior neck discomfort for the past 6 months. Radiographs, an MRI scan, and a photomicrograph of the biopsy specimen are shown in Figures 17a through 17d. What is the most likely diagnosis?
Explanation
REFERENCES: Bridwell KH, Ogilvie JW: Primary tumors of the spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery. Philadelphia, PA, JB Lippincott, 1991,
vol 2, pp 1143-1174.
Enneking WF: Musculoskeletal Tumor Surgery. New York, NY, Churchill Livingstone, 1983, pp 1043-1053.
Question 48
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of
Explanation
REFERENCES: Jakob RP, Miniaci A, Anson PS, et al: Four-part valgus impacted fractures of the proximal humerus. J Bone Joint Surg Br 1991;73:295-298.
Resch H, Povacz P, Frohlich R, et al: Percutaneous fixation of three- and four-part fractures of the proximal humerus. J Bone Joint Surg Br 1997;79:295-300.
Question 49
Nutritional rickets is associated with which of the following changes in chemical blood level?
Explanation
and low to normal serologic levels of calcium. To boost serum calcium levels, there is a compensatory increase in PTH and bone resorption, leading to increased alkaline
phosphatase levels.
REFERENCES: Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
Pettifor J: Nutritional and drug-induced rickets and osteomalacia, in Farrus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 399-466.
Einhorn TA: Metabolic bone disease, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 50
Which of the following pelvic injury types has the highest reported mortality rate?
Explanation

OrthoCash 2020
Question 51
After performing a total hip arthroplasty through a posterolateral approach, an orthopaedic surgeon is unable to adequately externally rotate the leg and subsequently exposes the anterior capsule. When releasing the inferior aspect of the anterior capsule, pulsatile bleeding is encountered. A branch of which artery is most likely lacerated?
Explanation
Branches of the lateral femoral circumflex artery arise from the inferior aspect of the anterior hip capsule. They can be injured when removing the anterior capsule from any approach. The inferior gluteal artery supplies the gluteus maximus. The medial femoral circumflex artery enters the hip joint along the path of the obturator externus tendon. The femoral artery crosses the anterior hip joint in the superior-to-inferior direction and is located just medial to the hip joint.

Question 52
When treating thoracic disk herniations, which of the following surgical approaches has the highest reported rate of neurologic complications?
Explanation
REFERENCES: Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
Benjamin V: Diagnosis and management of thoracic disc disease. Clin Neurosurg
1983;30:577-605.
Russell T: Thoracic intervertebral disc protrusion: Experience of 67 cases and review of the literature. Br J Neurosurg 1989;3:153-160.
Fessler RG, Sturgill M: Review: Complications of surgery for thoracic disc disease. Surg Neurol 1998;49:609-618.
Question 53
Serum phosphate levels are high. Tumoral calcinosis is a heritable condition that is characterized by periarticular metastatic calcification. Most patients are black, and the inheritance is usually autosomal recessive. Metastatic calcifications occur around joints and in the skin, marrow, teeth, and blood vessels. The periarticular masses may grow quite large and are attached to the fascia, but they are extra-articular. The masses may occur at the shoulder, hip, and elbow. Radiographically: The masses are composed of heavy, amorphous calcification in nodules. Laboratory:
Explanation
Question 54
- Which of the following rehabilitation methods should be used for the first 24 hours following a blunt injury to the quadriceps musculature to avoid short-term stiffness?
Explanation
In the past immobilization in full extension was recommended, but it was noticed that the lack of flexion prolonged disability. Flexion of the knee during the first 24 hours also aids in limiting the extent of intramuscular hematoma.
Myositis ossificans is higher in any patient presenting after a quad contusion and has active knee ROM of less than 120 degrees and delay in treatment greater than 3 days.
Question 55
A 45-year-old construction worker sees a surgeon 23 days after sustaining an eccentric injury to his dominant right elbow. An MRI demonstrates a distal biceps tendon rupture with 5 cm of proximal retraction. In the operating room, the surgeon encounters good tissue quality but finds that primary repair can only be performed with the elbow hyperflexed to 70°. What is the best next step?
Explanation
strength. Isolated debridement of the distal tendon would not be an appropriate treatment.
Question 56
What condition favors pollicization in hypoplasia of the thumb?
Explanation
The decision to ablate and pollicize vs preserve and reconstruct is based on the stability of the carpometacarpal joint. A stable thumb is more easily used in prehension activities of grasping and pinching. All other responses are associated with surgical options for reconstruction of the thumb. The carpometacarpal joint is the “keystone” for thumb-to-hand attachment. Without a stable carpometacarpal joint, pollicization may be required. No other response necessitates pollicization.
RECOMMENDED READINGS
McCarroll HR. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000 Nov;25(6):1007-37. Review. PubMed PMID: 11119659. View Abstract at PubMed
Manske PR, Goldfarb CA. Congenital failure of formation of the upper limb. Hand Clin. 2009 May;25(2):157-70. doi: 10.1016/j.hcl.2008.10.005. Review. PubMed PMID: 19380058.View Abstract at PubMed
Question 57
A 73-year-old man is scheduled to have mature heterotopic bone resected from around his left total hip arthroplasty. The optimal management for prophylaxis against the return of heterotopic bone postoperatively is radiation therapy that consists of
Explanation
REFERENCES: Healy WL, Lo TC, DeSimone AA, Rask B, Pfeifer BA: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595.
Pelligrini VD Jr, Gregoritch SJ: Preoperative irradiation for the prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;78:870-881.
Pelligrini VD Jr, Konski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Question 58
An 18-year-old man was in a motor vehicle accident and sustained a closed head injury, right displaced scapular body and glenoid fractures, a right proximal humeral fracture, fractures of ribs one through three, facial fractures, and bilateral pubic rami fractures with minimal displacement. He has a systolic blood pressure of 80/40 mm Hg despite fluid resuscitation. A radiograph is shown in Figure 17. Spiral CT does not identify any thoracic or abdominal injuries. What is the next most appropriate step in management?
Explanation
REFERENCES: Althausen PL, Lee MA, Finkemeier CG: Scapulothoracic dissociation: Diagnosis and treatment. Clin Orthop 2003;416:237-244.
Witz M, Korzets Z, Lehmann J: Traumatic scapulothoracic dissociation. J Cardiovasc Surg 2000;41:927-929.
Question 59
The majority of severe cervical spine injuries occurring in contact sports evolve during axial loading and flexion of the cervical spine. At what minimum degree of flexion does axial loading place the cervical spine at risk during contact sports?
Explanation
REFERENCES: Thomas BE, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Torg JS, Truex R Jr, Quedenfeld TC, Burstein A, Spealman A, Nichols C III: The National Football Head and Neck Injury Registry: Report and conclusions 1978. JAMA 1979;241:1477-1479.
Question 60
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
REFERENCE: Talan DA, Citron DM, Abrahamian FM, et al: Bacteriologic analysis of infected dog and cat bites. Emergency Medicine Animal Bite Infection Study Group. N Engl J Med 1999;340:85-92.
Question 61
A 51-year-old woman has had progressively increasing right knee pain for the past 6 months. She has a history of metastatic renal cell carcinoma to the lung and the skeletal system. Radiographs are seen in Figures 18a and 18b. The next step in management of the right distal femur lesion should consist of
Explanation
REFERENCES: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Sim FH: Metastatic bone disease of the pelvis and femur. Instr Course Lect 1992;41:317-327.
Question 62
Compact bone, titanium, stainless steel, cobalt-chrome
Explanation
In a patient with a previous compression hip screw in place at the time of total hip arthroplasty, what precautionary measures should be undertaken after hardware removal to prevent a periprosthetic fracture:
Question 63
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18° of valgus compared with 3° of valgus on the opposite side. Management should now include
Explanation
REFERENCES: Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 64
Which of the following statements is true regarding the superomedial fragment of an intra-articular calcaneus fracture?

Explanation
Question 65
An open biopsy specimen of a radiodense distal clavicle lesion in a 12-year-old girl shows chronic polyclonal inflammatory cells without granuloma formation. Laboratory studies show that bacterial, fungal, and acid-fast bacillus cultures are negative. Subsequently, a similar lesion is noted in the fibula. The next most appropriate step in management should consist of
Explanation
REFERENCE: Carr AJ, Cole WG, Roberton DM, Chow CW: Chronic multifocal osteomyelitis. J Bone Joint Surg Br 1993;75:582-591.
Question 66
Figure 49 shows an acute axial MRI scan of a right knee. What is the most likely diagnosis? Review Topic
Explanation
Question 67
A 55-year-old patient with rheumatoid arthritis reports increasing elbow pain and swelling for the past 2 months. She underwent a cemented, semiconstrained elbow arthroplasty 8 years ago. Laboratory studies show a normal peripheral white blood cell count; however, the erythrocyte sedimentation rate and C-reactive protein level are elevated. Radiographs are shown in Figures 48a and 48b. Which of the following organisms is most difficult to eradicate? Review Topic

Explanation
Question 68
A 25-year-old patient undergoes the procedure seen in Figure A. Which of the following statements best describes the incorporation of the graft and biopsy results of the graft at one year? Review Topic
Explanation
Articular cartilage defects can be treated by a variety of methods including debridement, fixation of unstable osteochondral fragments, marrow stimulation techniques (microfracture, abrasion chondroplasty), cartilage replacement techniques (osteochondral autograft and allograft) and cellular techniques (autologous chondrocyte implantation). Osteochondral autograft transfer is performed by harvesting normal articular cartilage with underlying bone from lesser weightbearing areas (e.g. intercondylar notch) and transferring the graft to a recipient socket at the site of the chondral defect. Graft incorporation occurs by integration of the bony graft into the subchondral bone and healing of the overlying cartilage layer.
Hangody et al. reviewed the outcomes of autologous osteochondral mosaicplasty in professional athletes. They found successful outcomes similar to that of less athletic patients, despite a higher rate of preoperative osteoarthritic changes in the athletic population. The authors noted that histological evaluation revealed good graft incorporation in all 11 cases.
Alford et al. authored a two part Current Concepts article on cartilage restoration. They constructed an algorithm (Illustration A) highlighting many factors that impact treatment choice, including patient activity level and defect characteristics such as location and size. This algorithm also illustrates comorbidities (malalignment, ligament insufficiency) that warrant correction prior to addressing the chondral defect.
Figure A shows a full-thickness chondral defect (left) and subsequent osteochondral autograft transfer (right). Illustration A is a treatment algorithm for the management of chondral defects, as discussed above. Illustration B shows a microfracture procedure, a marrow stimulation technique resulting in fibrocartilage filling of the chondral defect. Illustration C shows an osteochondral allograft transplant, a cartilage replacement technique useful for large defects in which donor graft is obtained from a cadaver hemicondyle and transferred to a recipient socket at the site of the chondral defect. Illustration D shows the autologous chondrocyte implantation technique, a two-stage procedure consisting of 1. Cartilage biopsy for growth of autologous
chondrocytes, and 2. Subsequent injection of autologous chondrocytes beneath a periosteal patch.
Incorrect
Question 69
A 23-year-old man who was the restrained driver in a car involved in a high-speed motor vehicle accident sustained the closed injury shown in Figures 32a through 32c. Which of the following factors has the greatest impact on the risk of osteonecrosis?
Explanation
REFERENCES: Lindvall E, Haidukewych G, Dipasquale T, et al: Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am 2004;86:2229-2234.
Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.
Question 70
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus?
Explanation
REFERENCES: Harryman DT II, Sidles JA, Harris SL, et al: The role of the rotator interval capsule in passive motion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53-66.
Wang VM, Flatow EL: Pathomechanics of acquired shoulder instability: A basic science perspective. J Shoulder Elbow Surg 2005;14:2S-11S.
Question 71
Which of the following is considered a contraindication to cement injection techniques, such as kyphoplasty or vertebroplasty, in the treatment of osteoporotic compression fractures?
Explanation
REFERENCES: Phillips FM, Pfeifer BA, Leiberman IH, et al: Minimally invasive treatment of osteoporotic vertebral compression fractures: Vertebroplasty and kyphoplasty. Instr Course Lect 2003;52:559-567.
Truumees E, Hilibrand A, Vaccaro AR: Percutaneous vertebral augmentation. Spine J 2004;4:218-229.
Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 72
A 72-year-old woman is scheduled to undergo right total hip arthroplasty. Her preoperative radiograph is shown in Figure below. To avoid increasing this patient’s combined offset while maintaining her leg length, what is the most appropriate surgical plan?
Explanation
The management of patients with proximal femoral deformity can be difficult. Appropriate implant selection and preoperative templating are critical. In this patient, it would be difficult to avoid increasing the combined offset by too much, which could contribute to the overtensioning of the soft tissues and trochanteric pain. By medializing the acetabular component (decreasing the combined offset), using a low offset femoral component or a cemented component placed more valgus (decreasing the combined offset), and making a longer neck cut (to avoid shortening of the lower extremity), restoration of the patient’s native offset and leg length can be achieved.
Question 73
An 18-year-old collegiate football player injures his right shoulder during a tackle. He reports pain and numbness in the shoulder and numbness radiating to his fingers. His symptoms improve within 15 minutes and he has no residual symptoms. This condition is best known as
Explanation
REFERENCES: Safran MR: Nerve injury about the shoulder in athletes. Part 2: Long thoracic nerve, spinal accessory nerve, burners/stingers, thoracic outlet syndrome. Am J Sports Med 2004;32:1063-1076. Aval SM, Durand P Jr, Shankwiler JA: Neurovascular injuries to the athlete’s shoulder: Part I. J Am Acad Orthop Surg 2007;15:249-256.
Question 74
Which of the following treatments for osteoporosis is a direct inhibitor of RANK ligand (RANK-L)?
Explanation
RANKL (Receptor activator of nuclear factor kappa-B ligand) is a key molecule for osteoclast differentiation and activation. Inhibition of RANKL activity with anti-RANKL antibody reduces osteoclastogenesis, resulting in inhibition of bone resorption.
Capozzi et al. author a review article on denosumab. They state the medication confers improved bone mineral density and prevents new fragility fractures similar to alendronate. However, denosumab presents less risk of atypical femoral fractures and
osteonecrosis of the jaw.
Yasuda et al. present a review that details the creation of three elegant animal models to mimic metabolic bone disease and how the animal models can create a template to help cure human metabolic bone disease. These enable modeling of osteoporosis, hypercalcemia, and osteopetrosis by treating normal mice with soluble RANKL (sRANKL), adenovirus expressing sRANKL, and anti-mouse RANKL neutralizing antibody, respectively. They report that these animal models can be established in about 14 days using normal mice.
Illustration A demonstrates the mechanism of action of bisphosphonates and denosumab.
Incorrect Answers:
1: Romosozumab is the first humanized anti-sclerostin monoclonal antibody that has been demonstrated to increase bone formation. 2: Zoledronic acid (Reclast) is a nitrogen containing bisphosphonates that inhibits osteoclast resorption by inhibiting the enzyme farnesyl diphosphate synthase. 4: Teriparatide (Forteo) comprises the first 34 amino acids of the 84 amino acid parathyroid hormone (PTH) and can reproduce the primary effects of PTH by activating adenyl cyclase. 5: Blosozumab is an investigational monoclonal anti-sclerostin antibody showing osteoanabolic properties with the potential to improve clinical outcomes in patients with osteoporosis.
Question 75
A 62-year-old active man returns for routine follow-up 16 years after hip replacement. He has no hip pain. Radiographs reveal a well-circumscribed osteolytic lesion around a single acetabular screw. All hip components are perfectly positioned. Comparison radiographs obtained 6 months later show an increase in the size of the osteolytic lesion. CT depicts a well-described lesion that is 3 cm at its largest diameter and is localized around one screw hole with an eccentric femoral head. What treatment is appropriate, assuming that well-fixed cementless total hip components are in place?
Explanation
Given a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected from liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings arise during revision surgery. Here, complete cup revision is not warranted, considering the appropriate implant position. Beaulé and associates reviewed 83 consecutive patients (90 hips) in whom a well-fixed acetabular component was retained in a clinical scenario such as the one described. No hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, acetabular component revision may be indicated.
Question 76
A 26-year-old weightlifter has increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication, corticosteroid injections, and rest fails to alleviate his symptoms. He undergoes an arthroscopic distal clavicle resection with excision of the distal 8 mm of clavicle (Mumford procedure). Three months after surgery, he reports mild pain and popping by his clavicle. His clavicle demonstrates mild posterior instability on examination without any obvious deformity on his radiographs. What structures were compromised during his excision?
Explanation
Question 77
A 22-year-old man reports that he initially dislocated his shoulder while playing basketball 2 years ago and was subsequently treated with an arthroscopic Bankart repair. Despite appropriate rehabilitation, the patient continues to report recurrent instability. An axillary view radiograph and CT scan are shown in Figures 57a and 57b. What is the most appropriate management at this time? Review Topic

Explanation
Question 78
Figures 91a through 91c are the radiographs of a 10-year-old boy who has a 6-month history of progressive heel pain. The patient is a year-round soccer player and now experiences pain with most every step. What is the most appropriate management?

Explanation
Question 79
A 28-year-old male sustains a fall on icy ground and fractures his ankle. An intraoperative fluoroscopy image is shown in Figure A. This fixation suggests that the mechanism of injury was one of

Explanation
A vertical fracture of the medial malleolus is characteristic of a Lauge-Hansen SA fracture. Bimalleolar SA fractures will also demonstrate a distal fibular avulsion. Another characteristic is impaction of anteromedial distal tibia by the talar dome. An anteromedial surgical approach allows visualization of this region, elevation of impaction, and bone grafting of the defect if necessary.
Dumigan et al. analyzed 4 different methods of treating vertical shear fractures with polyurethane models. They found that fixation with a 4 hole 1/3 tubular plate with 2 screws in the distal fragment was stiffer than fixation with the same plate with 1 screw in the distal fragment (3 in the proximal), fixation with two 3.5mm cortical screws with washers, and fixation with two 4mm cortical screws with washers. They recommend plating over screw-alone constructs.
McConnell et al. reported 8 cases of anteromedial marginal impaction in SA fractures. They note that 44 fractures were SA type. Following reduction and fixation, all 8 patients had excellent outcome and no arthritis. They recommend an anteromedial approach to the medial malleolus for visualization.
Figure A is a lateral radiograph showing fixation of both malleoli with reconstruction plates. Illustration A is an postoperative AP fluoroscopy image. Illustration B is an injury film demonstrating the same SA ankle fracture. Illustration C shows articular impaction at the medial shoulder of the ankle joint typical of SA injuries. Illustration D shows marginal impaction in SA fractures.
Incorrect Answers
(SBQ12TR.76) A 24-year-old male sustains the fracture dislocation shown in Figure
A. How is this fracture pattern best classified?

Moore I
Moore II
Schatzker III
Schatzker V
OTA type 41B3
Figure A shows a Moore Type II fracture. Moore type II fractures consist of fractures involving the entire tibial condyle, where the fracture line begins in the opposite compartment and extends across the tibial eminence.
A number of classification systems are used to describe tibial plateau fractures. The main classification systems that are widely used include Schatzker, AO/OTA, Hohl and Moore. The Moore classification describes high energy fracture-subluxation injuries of the knee. This is thought to have clinical implications as the type of fracture pattern can indicate an associated soft-tissue injury.
Moore retrospectively reviewed over a 1000 proximal tibia fractures to devise a classification systems based on the characteristic of five types of tibia plateau fracture patterns. He believed this system helped to better understand knee instability and concomitant soft-tissue injury. For example, Moore Type III fractures (rim avulsion) are associated with a high rate of neurovascular injury.
Figure A shows a fracture involving the entire tibial condyle. Illustration A shows a schematic diagram of the Moore classification (I - V). Illustration B shows a table that
describes the Moore classification (I - V).
Incorrect Answers:
Question 80
A 32-year-old male sustains a posterior wall acetabulum fracture as the result of a high-speed motor vehicle collision. Improved patient-reported outcomes after surgical treatment are associated with which of the following variables?

Explanation
The reference by Borrelli et al evaluated muscle strength and outcomes after acetabular surgery via an anterior approach. They report that hip extension strength was affected least(6%), whereas abduction, adduction, and flexion strength was affected to a greater degree. They note that hip muscle strength after operative treatment of a displaced acetabular fracture directly influences patient outcome.
The reference by Engsberg et al is a review of patients that underwent ORIF of acetabular fractures through anterior or posterior approaches. They report that maximizing hip muscle strength may improve gait, and improvement in hip muscle strength and gait is likely to improve functional outcome. Worsening functional outcomes were correlated with decreased gait kinematics and stride length.
Question 81
Which structure is the primary stabilizer of the lesser metatarsophalangeal (MTP) joint?
Explanation
Synovitis of the second MTP occurs in association with instability of the joint. This can be idiopathic or secondary to an external deforming force (such as a hallux valgus or shoe wear causing a claw toe). The primary stabilizer of the MTP joint for translation in the vertical plane is the plantar plate. The flexor digitorum brevis flexes the MTP joint, and the flexor digitorum longus flexes
all joints of the toe. The collateral ligaments are primary stabilizers in the transverse plane and secondary stabilizers in the sagittal plane.
RECOMMENDED READINGS
Deland JT, Sung IH. The medial crosssover toe: a cadaveric dissection. Foot Ankle Int. 2000 May;21(5):375-8. PubMed PMID: 10830654.View Abstract at PubMed
Suero EM, Meyers KN, Bohne WH. Stability of the metatarsophalangeal joint of the lesser toes: a cadaveric study. J Orthop Res. 2012 Dec;30(12):1995-8. doi: 10.1002/jor.22173. Epub 2012 Jun 13. PubMed PMID: 22696467. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 91 THROUGH 95
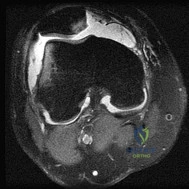
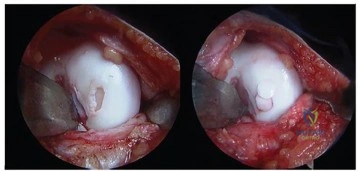
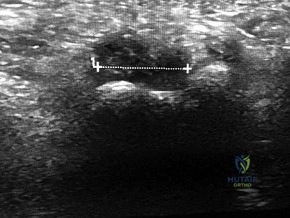
Figure 91a is the sagittal plane ultrasound of the second web space of a 48-year-old woman who has noted burning pain in the ball of her right foot for 2 years. The pain intermittently radiates into her second and the third toes. Figure 91b shows the surgical procedure and Figure 91c is the pathologic specimen.
A
B

C

Question 82
Figure 28 shows the postoperative radiograph of a 36-year-old patient. The cerclage cable was placed for a minimal medial calcar fracture seen during femoral preparation. In the immediate postoperative period, what is the highest level of activity that would be safely permitted?
Explanation
REFERENCES: Berend KR, Lombardi AV Jr, Mallory TH, et al: Cerclage wires or cables for the management of intraoperative fracture associated with a cementless, tapered femoral prosthesis: Results at 2 to 16 years. J Arthroplasty 2004;19:17-21.
Schmidt AH, Kyle RF: Periprosthetic fractures of the femur. Orthop Clin North Am 2002;33:143-152.
Greidanus NV, Mitchell PA, Masri BA, et al: Principles of management and results of treating the fractured femur during and after total hip arthroplasty. Instr Course Lect 2003;52:309-322.
Question 83
In total knee arthroplasty, in vitro testing has shown that cross-linking can diminish the rate of polyethylene wear by 30% to 80%. What other change in material properties is possible when polyethylene is highly cross-linked?
Explanation
The most important concern regarding highly cross-linked polyethylene relates to decreased mechanical properties. Cross-linking results in reduced ductility, tensile strength, and fatigue crack propagation resistance. These problems have not been shown to cause implant failure in the most recent clinical trials, but they remain the most important mechanical issues associated with current material processing methods.
Question 84
Figures 35a and 35b show the radiographs of a 7-year-old patient who has progressive deformity of the right thigh accompanied by a dull persistent pain radiating to the knee. Examination reveals an obvious bulge in the right thigh, with flexion of the hip beyond 50° only if the hip is allowed to externally rotate. Management should consist of
Explanation
REFERENCES: Zionts LE, Ebramzadeh E, Stott NS: Complications in the use of the Bailey-Dubow extensible nail. Clin Orthop 1998;348:186-195.
Luhmann SJ, Sheridan JJ, Capelli AM, Schoenecker PL: Management of lower-extremity deformities in osteogenesis imperfecta with extensible intramedullary rod technique: A 20-year experience. J Pediatr Orthop 1998;18:88-94.
Glorieux FH, Bishop NJ, Plotkin H, Chabot G, Lanoue G, Travers R: Cyclic administration of pamidronate in children with severe osteogenesis imperfecta. N Engl J Med 1988;339:947-952.
Question 85
A 22-year-old college baseball pitcher reports the recent onset of anterior and posterosuperior shoulder pain in his throwing shoulder. Examination shows a 15-degree loss of internal rotation, tenderness over the coracoid, and a positive relocation test. Radiographs are normal, and an MRI scan without contrast shows no definitive lesions. A rehabilitation program is prescribed. Which of the following regimens should be initially employed? Review Topic
Explanation
Question 86
A 15-year-old boy reports feeling a pop and notes sudden giving way of the left knee while playing basketball. He has immediate pain and swelling in the knee. An AP radiograph is shown in Figure 32. A small avulsion fragment from the lateral tibial margin is the only finding. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Larson RL, Tailon M: Anterior cruciate ligament insufficiency: Principles of treatment. J Am Acad Orthop Surg 1994;2:26-35.
Question 87
below show the radiograph and the MRI scan obtained from a year-old woman with a month history of left hip pain. Which presurgical factor is most commonly associated with a poor outcome after a hip joint salvage procedure?
Explanation
MRI reveals an anterior labral tear, and the radiograph shows minimal arthritis with possible dysplasia. The most common location of pain in patients with a labral tear is the groin, and the most common physical finding is a positive impingement test result. Pain during sitting, clicking, and buttock pain are frequently described by patients with a labral tear, but these symptoms are less common than groin pain. A positive posterior impingement test finding is more common in patients with a posterior labral tear. Although age over 40 years and a body mass index higher than 30 can adversely affect clinical outcomes after joint preservation procedures such as PAO, hip arthroscopy, and femoral acetabular impingement surgery, the presence of hip arthritis on presurgical radiographs is the most commonly mentioned cause of failed hip joint preservation surgery. Tönnis grade is a radiographic measure of hip arthritis. A higher Outerbridge score is associated with more frequent poor outcomes after hip arthroscopy; however, the
Outerbridge cartilage score is determined by direct visualization at the time of surgery. The Outerbridge
score cannot be determined presurgically.
Question 88
below shows the radiograph obtained from a year-old woman who returns status post total hip arthroplasty 14 years earlier. She denies pain and has no discomfort on examination. She then undergoes revision total hip arthroplasty with head and liner exchange and bone grafting. After a physical therapy session two days after surgical intervention, she develops inability to dorsiflex the foot while she is sitting in a chair. The initial treatment should consist of
Explanation
Gamma irradiation produces free radicals. Although these free radicals can form cross-links with other polyethylene chains, the free radicals can also form a bond with oxygen, resulting in early oxidation. Gamma irradiation in air produces the highest risk for oxidized polyethylene, resulting in the highest risk for wear, delamination, and subsequent osteolysis. This patient demonstrates severe periarticular osteolysis. When she is asymptomatic, this suggests the acetabular and femoral components remain well fixed to the bone. Consequently, she can be treated by removing the wear generator (polyethylene exchange), along with bone grafting of the osteolytic defect. Considering the extensive amount of osteolysis indefinite observation would not be appropriate. A foot drop develops 2 days after surgery. As a result, it can be assumed that the nerve was not injured directly during the surgical procedure. Although MRI or CT may be indicated to identify an evolving hematoma, the immediate concern is to minimize pressure on the sciatic nerve. Tension on the nerve can be reduced by flexing the surgical knee and positioning the bed flat.
Question 89
What do the T2-weighted, fat-saturated MRI scans shown in Figures 1 through 4 reveal?

Explanation
disruption of the ACL. The medial meniscus images show a disruption of normal meniscus morphology consistent with a bucket handle medial meniscus tear. Note the appearance on the sagittal MRI scan of what appears to be a second soft-tissue density in line with the PCL. This "double PCL" sign is highly indicative of a displaced medial meniscus tear rather than a displaced lateral meniscus tear.
Question 90
A 14-year-old boy with a history of cerebral palsy has a clawed hallux, cavus foot deformity, and associated pain. Examination reveals pain under the first metatarsal head and a rigid first tarsometatarsal joint. Treatment should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 79-100.
Tynan MC, Klenerman L: The modified Robert Jones tendon transfer in cases of pes cavus and clawed hallux. Foot Ankle Int 1994;15:68-71.
Question 91
Which of the following hip fracture patterns is at increased risk of proximal fragment flexion malreduction with dynamic hip screw fixation?

Explanation
Mohan et al conducted a study to assess the effect of clockwise rotational torque onto the fracture configuration in unstable and stable intertrochanteric fractures fixed with a dynamic hip screw construct. They found that 11 out of 30 unstable fractures showed an anterior spike (flexion malreduction) in left-sided fixations due to clockwise torque. This malreduction was not present in right-sided or stable fractures.
Question 92
A characteristic genetic translocation has been noted in which of the following tumors?
Explanation
REFERENCES: Brockstein BE, Peabody TD, Simon MA: Soft tissue sarcomas, in Vokes EE Golomb HM (eds): Oncologic Therapies. New York, NY, Springer-Verlag, 1999, pp 925-952.
Simon MA, Springfield DS, et al: Management of Surgical Specimens: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 67-75.
Question 93
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course of action?
Explanation
REFERENCES: Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16.
Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27.
Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546.
Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Cohn BT, Brahms MA, Cohn M: Injury to the eleventh cranial nerve in a high school wrestler. Orthop Rev 1986;15:59-64.
Question 94
Figure 56 is the radiograph of a 62-year-old noninsulin-dependent woman with diabetes who twisted her ankle while walking and felt a pop. At the emergency department she describes heel pain. What is the best course of action?

Explanation
The radiograph reveals a displaced calcaneal tuberosity fracture. Displacement of a large tuberosity fragment necessitates urgent fracture reduction and stabilization. Delayed reduction results in compromise of the skin and soft tissues at the posterior heel. This injury occurs frequently in patients with diabetes. Protected weight-bearing activity does not address the displaced fragment or the threatened skin. Closed reduction, if possible, will not maintain the tuberosity fragment in a reduced position and will likely result in redisplacement. The fragment is large enough that it may be fixed and not excised. The Achilles tendon inserts on the displaced tuberosity fragment, so tuberosity reduction and fixation is necessary to achieve proper Achilles function.
RECOMMENDED READINGS
Beavis RC, Rourke K, Court-Brown C. Avulsion fracture of the calcaneal tuberosity: a case report and literature review. Foot Ankle Int. 2008 Aug;29(8):863-6. Review. PubMed PMID: 18752789.View Abstract at PubMed
Gardner MJ, Nork SE, Barei DP, Kramer PA, Sangeorzan BJ, Benirschke SK. Secondary soft tissue compromise in tongue-type calcaneus fractures. J Orthop Trauma. 2008 Aug;22(7):439-45. PubMed PMID: 18670282. View Abstract at PubMed
RESPONSES FOR QUESTIONS 57 THROUGH 59
- High strain
- Low strain
For each fracture detailed, select the appropriate description.
A simple fracture pattern that is anatomically reduced and compressed and treated with an 8-hole conventional plate with 4 bicortical conventional screws placed on each side of the fracture
- High strain
- Low strain
Question 95
An active 66-year-old man who underwent total shoulder arthroplasty 3 years ago now reports pain. Laboratory studies reveal an elevated erythrocyte sedimentation rate and C-reactive protein. Intraoperative frozen section reveals greater than 10 white blood cells per high power field on two slides and the Gram stain reveals gram-positive cocci in clusters. What is the most appropriate surgical treatment to eradicate the infection and maintain function? Review Topic
Explanation
Question 96
All of the following techniques can help to prevent valgus angulation during intramedullary nailing of proximal one-third tibia fractures EXCEPT:

Explanation
A final technical trick is the usage of blocking (Poller) screws - the referenced article by Ricci et al had 100% correction and maintenance of reduction with usage of blocking screws without other adjunct techniques. These should be placed in the lateral aspect of the proximal and distal fragments when needed.
The referenced study by Krettek et al is a biomechanical evaluation of blocking screws in a tibial model that showed significantly increased strength when they were utilized.
Question 97
An 8-year-old boy sustains nondisplaced midshaft fractures of the tibia and fibula after being struck by a car while he was riding his bicycle. No other injuries are noted, but the patient reports pain with passive motion of his toes. His neurovascular examination is otherwise normal. What is the best course of action?
Explanation
REFERENCES: Mubarak SJ, Owen CA, Hargens AR, et al: Acute compartment syndromes: Diagnosis and treatment with the aid of the wick catheter. J Bone Joint Surg Am
1978;60:1091-1095.
Matsen FA III, Veith RG: Compartmental syndromes in children. J Pediatr Orthop
1981;1:33-41.
Question 98
A 12-year-old girl who plays softball has chronic lateral hindfoot aching pain that is aggravated by weight-bearing activity. She reports that the pain has recurred after initial improvement with cast immobilization, and it continues to limit her overall level of activity. Radiographs are seen in Figures 40a through 40c. What is the most appropriate surgical treatment?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765.
Lemley F, Berlet G, Hill K, et al: Current concepts review: Tarsal coalition. Foot Ankle Int 2006;27:1163-1169.
Question 99
below demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. A further work-up reveals elevations in serum cobalt and chromium levels and fluid collections surrounding the hip on MRI with MARS. Revision THA is recommended. The most common complication following revision of a failed metal-on- metal hip arthroplasty is
Explanation
Question 100
A patient who underwent total knee arthroplasty 6 years ago now reports knee pain for the past 3 days following dental surgery. Cultures of the aspirate are positive for Staphylococcus epidermidis. Management should consist of
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 323-337.
Goldman RT, Scuderi GR, Insall JN: 2-stage reimplantation for infected total knee replacement. Clin Orthop 1996;331:118-124.
