Orthopedic Board Prep MCQs: Elbow & Hip Review Exam - Part 28

Key Takeaway
This page offers Part 28 of a comprehensive orthopedic board review. It features 100 high-yield, verified MCQs modeled on OITE and AAOS exams. Designed for orthopedic residents and surgeons, this interactive quiz facilitates rigorous preparation for ABOS certification with detailed explanations and two learning modes.
About This Board Review Set
This is Part 28 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 28
This module focuses heavily on: Elbow, Hip.
Sample Questions from This Set
Sample Question 1: Which of the following nutraceuticals has been associated with perioperative bleeding?...
Sample Question 2: Which of the following prognostic indicators is associated with the least favorable outcome for patients newly diagnosed with osteosarcoma?...
Sample Question 3: Which clinical finding most strongly suggests that nonsurgical care should be discontinued and surgical intervention is necessary?...
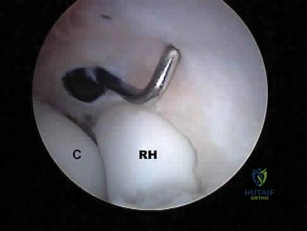
Sample Question 4: What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50? Review Topic...
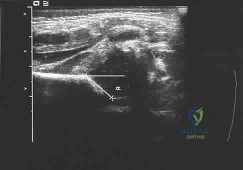
Sample Question 5: A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management? ...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following nutraceuticals has been associated with perioperative bleeding?
Explanation
REFERENCES: Rowin J, Lewis SL: Spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Neurology 1996;46:1775-1776.
Vale S: Subarachnoid hemorrhage associated with ginkgo biloba. Lancet 1998;352:36.
Bebbington A, Kulkarni R, Roberts P: Ginkgo biloba: Persistent bleeding after total hip arthroplasty caused by herbal self-medication. J Arthroplasty 2005;20:125-126.
Question 2
Which of the following prognostic indicators is associated with the least favorable outcome for patients newly diagnosed with osteosarcoma?
Explanation
REFERENCES: Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790.
Heck RK, Stacy GS, Flaherty MJ, et al: A comparison study of staging systems for bone sarcomas. Clin Orthop Relat Res 2003;415:64-71.
Kager L, Zoubeck A, Potschger U, et al: Primary metastatic osteosarcoma: Presentation and outcome of patients treated on neoadjuvant Cooperative Osteosarcoma Study Group protocols.
J Clin Oncol 2003;21:2011-2018.
Question 3
Which clinical finding most strongly suggests that nonsurgical care should be discontinued and surgical intervention is necessary?
Explanation
Epidural abscesses are potentially devastating. Nonsurgical care may be chosen for select patients. A baseline failure rate of 8.3% increases based on patient risk factors, which include a history of IV drug abuse, diabetes, age older than 65, CRP level higher than 115, WBC level higher than 12.5, and Staphylococcus aureus as the causative organism. Immunosuppression and abscess size are not significant risk factors for failure of nonsurgical care. Nonsurgical care may be regarded as "failed" if there is worsening of a patient's neurologic status. When nonsurgical care fails, delayed surgery is less successful at restoring motor function (vs early surgery).
RECOMMENDED READINGS
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 4
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50? Review Topic
Explanation
Question 5
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management? Review Topic
Explanation
not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness.
Question 6
50%
Explanation
Enneking et al. conducted both radiographic and histologic studies of sixteen massive retrieved human allografts four to sixty-five months after implantation. Analysis of the articular cartilage revealed no evidence that any chondrocytes had survived, even when the graft had been cryoprotected before it was preserved by freezing.
A 64-year-old woman with a longstanding history of rheumatoid arthritis complains of finger dysfunction for the past 6 months. Figure A displays her hand during active extension of all fingers. Figure B displays her hand maintaining her fingers extended following passive extension. What is the next most appropriate treatment for the ring finger?
Spiral oblique retinacular ligament reconstruction
Sagittal band reconstruction
Lateral band reconstruction
Central slip reconstruction
Triangular ligament and transverse retinacular ligament reconstruction
Sagittal band disruption is often associated with rheumatoid arthritis. When this patient attempts to actively extend the affected digit, the extensor tendon
subluxates ulnarly as a result of the sagittal band rupture, and is left with an extensor lag. If one passively extends the finger fully, the patient is able to maintain this position, as the tendon is intact.
Sagittal band reconstruction can be performed with Watson's technique of creating a distally based tendon graft harvested from the central third of the extensor tendon, passed deep to the intermetacarpal ligament and sutured back to itself. Illustration A depicts an intraoperative view of the tendon before reconstruction and Illustration B displays tendon following sagittal band reconstruction. Illustration C displays all of the anatomic locations
of the options listed above.
A splenectomy is performed in a 7-year-old boy following a motor vehicle accident. All of the following are recommended for long-term management EXCEPT:
Pneumococcal vaccination
Haemophilus influenza type B vaccination
Meningococcal group C vaccination
Lifelong prophylactic antibiotics
Hepatitis A vaccination
All of the responses are correct except the need for Hepatitis A vaccine. Hepatitis A is a virus with tropism for hepatocytes which causes infection from fecal-oral contaminated food/water, and shows no increased rate of either infectivity or morbidity in patients with hyposplenism.
Basic recommendations for splenectomized patients include:
All splenectomized patients and those with functional hyposplenism should receive pneumococcal immunization.
Patients not previously immunized should receive haemophilus influenza type B vaccine.
Patients not previously immunized should receive meningococcal group C conjugate vaccine.
Influenza immunization should be given.
Lifelong prophylactic antibiotics are still recommended (oral phenoxymethylpenicillin or erythromycin). This is seemingly despite lack of good data demonstrating a role for lifelong chemoprophylaxis and the acknowledgement that long-term compliance may be problematic.
Davies et al review the current level of evidence supporting these guidelines
for infection prevention in patients with hyposplenism. New to these guidelines are issues regarding occupational exposure and the use of the meningococcal group C and the seven-valent pneumococcal vaccine in non-immunized hyposplenic patients.
Gandhi et al evaluated their nonoperative management of blunt splenic injury in pediatric trauma care. They found compared to historical controls, children with blunt splenic injuries who were hemodynamically stable could be safely monitored with a protocol which required 4 days of inpatient care, 3 weeks of quiet home activities, and 3 months of light activity. This protocol seems to allow for safe return to unrestricted activity.
Incorrect Answer:
Ligaments attach to bone by both direct insertion and indirect insertion. Which of the following most accurately describes the order of the four transition zones of direct insertion?
Ligament > fibrocartilage > mineralized fibrocartilage > bone
Ligament > mineralized fibrocartilage > fibrocartilage > bone
Ligament > mineralized fibrocartilage > periosteum > bone
Ligament > Sharpey's fiber > periosteum > bone
Ligament > periosteum > fibrocartilage > bone
There are two types of tendon/ligament insertion into bone: direct and indirect insertion. The more common, indirect insertion, occurs when the superficial ligament fibers insert into the periosteum. Direct insertion of tendon/ligaments
into bone occurs through a transition of 4 distinct phases: 1) ligament, 2) fibrocartilage, 3) mineralized fibrocartilage, and 4) bone.
While flexing the elbow to perform a biceps curl, what type of muscle contraction is occuring?
Isometric
Isokinetic
Plyometric
Eccentric
Concentric
Concentric muscle contractions occur when a muscle shortens during contraction, as in the upward motion when performing a biceps curl. An eccentric contraction occurs when a muscle lengthens with contraction, as in the "negative" or lowering motion of a biceps curl. An example of an isometric (muscle contracts while maintaining constant length) contraction would be pushing against an immovable object. An example of an isokinetic (muscle has constant speed of contraction) occurs with specialized equipment like Cybex machines. Plyometric contractions occur when a muscle rapidly lengthens just prior to contraction - like during repetitive box jumping.
Woo and Buckwalter describe the mechanisms, barriers, and molecular processes involved in ligament and tendon injury and repair.
A 34-year-old laborer has her left foot crushed in a piece of farming equipment as shown in Figure A. All of the following are reasons for a poor outcome following a crush injury to the foot EXCEPT:
Workers compensation injury
Development of reflex sympathetic dystrophy (complex regional pain syndrome)
Delayed soft-tissue coverage in mangled extremities
Immediate skeletal stabilization
Ongoing litigation
This patient has a mangled extremity. Rigid skeletal stabilization is recommended to enhance soft-tissue healing.
Level 4 evidence from Myerson et al found that delayed soft-tissue coverage in mangled extremities correlated with poor outcome. Poor results also occurred
if treatment was not immediately initiated (immediate debridement shown in Illustration A), if patients subsequently had neuritis or reflex sympathetic dystrophy, or if patients were involved in ongoing workers' compensation and litigation. Neuroischemia following substantial soft-tissue injury likely plays a role in the development of chronic pain after crush injuries to the foot, either through direct trauma to the peripheral nerves or by intraneural or extraneural fibrosis. This trauma to the nerve may cause chronic neuritis, which then triggers a sympathetically mediated reflex sympathetic dystrophy (complex regional pain syndrome).
A 65-year-old man undergoes total knee replacement and is found to have deep vein thrombosis two days later. What molecule is
thought to be involved in this process when it is released during surgical dissection?
Prothrombin
RANKL
IL-1b
Thromboplastin
Factor XI Corrent answer: 4
Thromboplastin is also known more commonly as Tissue Factor (TF), which is involved in the Extrinsic Pathology of the coagulation cascade.
During surgical dissection, insults occur to the endothelial walls of blood vessels. There are three ways in which the body reacts to form a clot so that the patient does not bleed excessively. One is via vessel contraction, another is by collagen release, and a third is by tissue thromboplastin release. Thromboplastin release is part of the extrinsic coagulation pathway (see
Illustration A). Thromboplastin release activates Factor VII which activates Factor X which converts prothrombin to thrombin. Thrombin is the catalyst for converting fibrinogen to fibrin which induces clot formation. While this is useful for decreasing bleeding, it is the same mechanism by which a deep venous thrombosis (DVT) develops.
Which of the following materials has a Young's modulus of elasticity that is most similar to cortical bone
Titanium
Zirconia
Stainless steel
Ceramic (Al2O3)
Alloy (Co-Cr-Mo)
Of the materials listed Titanium has an elastic moduli closest to cortical bone. Titanium is extra-ordinarily light, strong, highly ductile, and corrosion resistant. Titanium is however very notch sensitive and has poor wear resistance.
Young Modulus of Elasticity is defined as the stiffness (ability to maintain
shape under external loading) of a material. On the stress vs. strain curve it is defined as the slope of the line in the elastic zone (see Illustration A). Young’s modulus is constant and different for each material. The relevant moduli (unit GPa) are approximated below:
Question 7
A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the clavicle distal to a line drawn vertically to the coracoid process. Management should consist of
Explanation
REFERENCES: Robinson CM, Cairns DA: Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-782.
Deafenbaugh MK, Dugdale TW, Staeheli JW, et al: Nonoperative treatment of Neer type II distal clavicle fractures: A prospective study. Contemp Orthop 1990;20:405-413.
Question 8
Figures below depict the radiographs obtained from a 53-year-old man who has had swelling in his right knee for 2 years, with minimal pain. He did not note an injury to the knee but has been unable to ambulate without crutches during this period. His past history is unremarkable, and he denies a history of diabetes or back problems. The social history reveals that he emigrated from China, and he works at a desk job. Physical examination shows a healthy man in no acute distress. Range of motion of the right knee is 5° to 120° actively and 0° to 120° passively, without pain. Sensation is decreased on the bottom of both feet, but otherwise the neurologic examination is unremarkable. Laboratory testing reveals a positive rapid plasma reagin (RPR) test. What is the best next step?
Explanation
This patient has a neuropathic knee caused by neurosyphilis, as shown by the joint destruction on the radiographs, with a lack of pain and a positive RPR test. He has a low-demand job and would be best treated with a hinged knee arthroplasty to provide stability for his knee.
Question 9
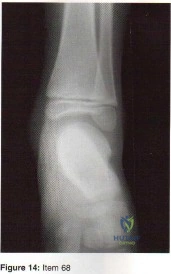
Figure 14 shows a lateral radiograph of a knee joint. The bony structure indicated by the arrow is a sesamoid bone that resides in what tendon?
Explanation
REFERENCES: Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Wilkins, 1978, pp 4-69.
Weissman BNW, Sledge CB (ed): Orthopaedic Radiology. Philadelphia, PA, WB Saunders, 1986, p 514.
Question 10
Failure of high tibial osteotomy (HTO) is most closely associated with which of the following factors?
Explanation
with HTO.
REFERENCES: Naudie D, Borne RB, Rorabeck CH, Bourne TJ: Survivorship of the high tibial valgus osteotomy: A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
Rinonapoli E, Mancini GB, Corvaglia A, Musiello S: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Coventry MB, Ilstrup DM, Wallrichs SL: Proximal tibial osteotomy: A critical long-term study of eighty-seven cases. J Bone Joint Surg Am 1993;75:196-201.
Question 11
A 10-month-old girl has the spinal deformity shown in Figures 55a and 55b with no apparent neurologic finding. The next step in evaluation should be to obtain
Explanation
REFERENCES: Beals RK, Robbins JR, Rolfe B: Anomalies associated with vertebral malformations. Spine 1993;18:1329-1332.
Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 12
A 13-year-old boy who has a history of a pituitary adenoma has an unstable unilateral slipped capital femoral epiphysis. What is the indication for prophylactic pinning of the contralateral, unslipped side? Review Topic
Explanation
Question 13
The major benefit of irrigation with a castile soap solution over irrigation with bacitracin solution for the treatment of the open fracture shown in Figure 42 can be seen in which of the following outcomes?
Explanation
REFERENCE: Anglen JO: Comparison of soap and antibiotic solutions for irrigation of lower-limb open fracture wounds: A prospective, randomized study. J Bone Joint Surg Am 2005;87:1415-1422.
Question 14
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Explanation
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 15
What is the most common pediatric soft-tissue sarcoma?
Explanation
REFERENCE: Wexler LH, Helman LJ: Pediatric soft tissue sarcomas. CA Cancer J Clin 1994;44:211-247.
Question 16
Figures 5a and 5b show the radiographs of an 11-year-old boy who felt a pop and immediate pain in his right knee as he was driving off his right leg to jam a basketball. Examination reveals that the knee is flexed, and the patient is unable to actively extend it or bear weight on that side. There is also a large effusion. Management should include
Explanation
REFERENCES: Heckman JD, Alkire CC: Distal patellar pole fractures: A proposed common mechanism of injury. Am J Sports Med 1984;12:424-428.
Tolo VT: Fractures and dislocations around the knee, in Green NE, Swiontkowski MF (eds): Skeletal Trauma in Children. Philadelphia, Pa, WB Saunders, 1994, vol 3, pp 380-382.
Question 17
A 25-year-old construction worker lands on his outstretched hand in a fall. The position of his wrist at the time of impact causes a force that leads to hyperextension, ulnar deviation, and intercarpal supination. Radiographs are shown in Figures 48a and 48b. Management should consist of
Explanation
REFERENCES: Kozin SH: Perilunate injuries: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:114-120.
Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J: Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-779.
Sotereanos DG, Mitsionis GJ, Ginnakopoulos PN, Tomaino MM, Herndon JH: Perilunate dislocation and fracture dislocation: A critical analysis of the volar-dorsal approach. J Hand Surg Am 1997;22:49-56.
Question 18
When performing hip arthroscopy, the hip should be placed in neutral to slight internal rotation to protect which of the following structures? Review Topic
Explanation
Question 19
- Which of the following factors is most likely to predispose a patient to dislocation of the patellar component following total knee arthoplasty?
Explanation
Internally rotating the femoral component produced abnormal laxity seen at 30, 60, and 90 degrees of flexion. There was no gapping noted in the neutral or externally rotated specimens.
The normal pattern for patellar tracking was a gentle curve with maximal deflection at 15 and 60 degrees of flexion. The maximal medial displacement were lowest for the externally rotated specimens.
Although contact areas could not be quantitatively measured accurately, the contact areas were more evenly distributed between the medial and lateral sides of the patella in the externally rotated specimens than they were in either the internally rotated or neutral specimens.
You have to be careful interpreting this data at least in reference to knee stability. In this study a perpendicular tibial cut was made. The normal tibia has a 30 degree varus slope and thus more bone is resected from the lateral surface. External rotation of the femoral component compensates for this.
No tests were done with lateral placement of the femoral component or medial placement of the patellar component.
Question 20
The use of knee arthroscopy following total knee arthroplasty is most effective in treating which of the following conditions?
Explanation
REFERENCES: Lucas TS, DeLuca PF, Nazarian DG, et al: Arthroscopic treatment of patellar clunk. Clin Orthop 1999;367:226-229.
Takahashi M, Miyamoto S, Nagano A: Arthroscopic treatment of soft-tissue impingement under the patella after total knee arthroplasty. Arthroscopy 2002;18:E20.
Question 21
A female cross-country runner has an insidious onset of right groin pain. Radiographs of the right hip reveal a tension-side stress fracture. History reveals that she was treated for a “foot” fracture 1 year ago. In addition to performing internal fixation of the femoral neck, which of the following should be obtained?
Explanation
REFERENCES: Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Barrow GW, Saha H: Menstrual irregularity and stress fractures in collegiate female distance runners. Am J Sports Med 1988;16:209-216.
Question 22
A 23-year-old woman reports right knee pain and fullness. The pain is worse with activity but also present at rest. Radiographs are shown in Figures 20a and 20b. What is the most likely diagnosis?
Explanation
REFERENCES: Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 175-186.
Question 23
The third plantar intrinsic muscle layer of the foot consists of which of the following structures?
Explanation
REFERENCE: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 32-33.
Question 24
Which of the following conditions is typically associated with the ankle deformity shown in figure 14?
Explanation
Question 25
- Which of the following procedures is associated with the highest risk of osteonecrosis of the metatarsal head?
Explanation
Question 26
Steroids are thought to prevent neurologic deterioration after traumatic spinal cord injury by which of the following mechanisms?
Explanation
REFERENCES: Slucky AV: Pathomechanics of spinal cord injury. Spine: State Art Rev 1999;13:409-417.
Torg JS, Thibault L, Sennett B, et al: The Nicolas Andry Award. The pathomechanics and pathophysiology of cervical spinal cord injury. Clin Orthop Relat Res 1995;321:259-269.
Question 27
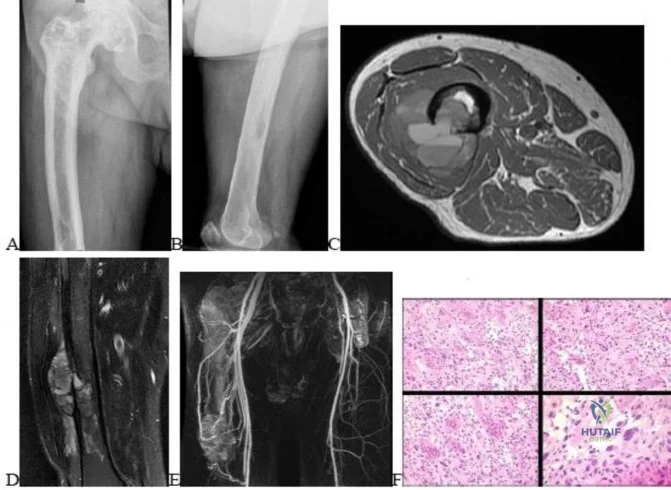
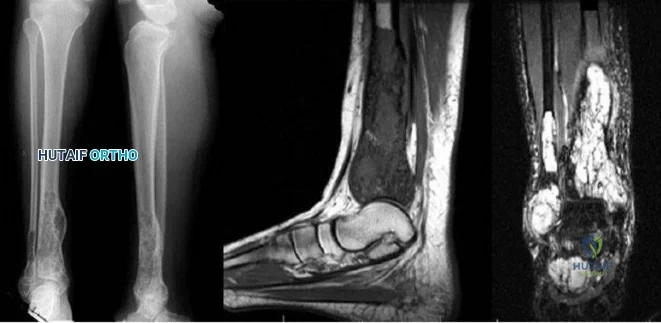
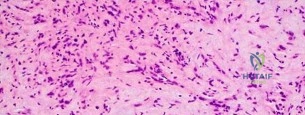
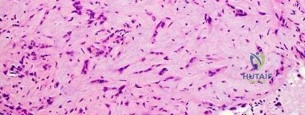
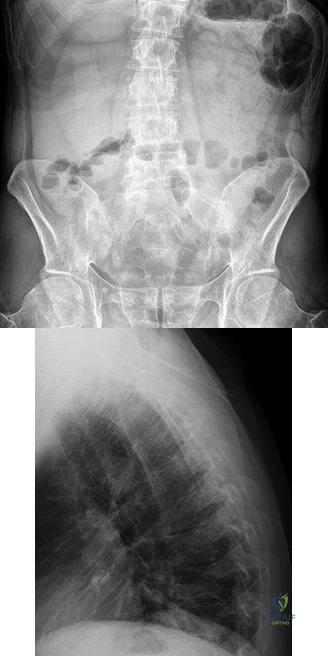
..Figures 112a and 112b are the anteroposterior and lateral radiographs of a 65-year-old man who has a significant history of tobacco abuse and a 6-week history of right thigh pain. Axial and sagittal MRI scans are seen in Figures 112c and 112d. His MR angiogram is shown in Figure 112e. A biopsy of a lesion is shown in Figure 112f. What is the most likely diagnosis?
Explanation
Figures 113a and 113b are the radiographs of a 68-year-old-man who has increasing pain in his left groin with weight-bearing activities and a Trendelenburg gait. Radiographs reveal a lytic lesion of the greater trochanter. An initial diagnosis of adenocarcinoma of the lung was made 1 year before this presentation. His lung cancer treatment consisted of partial lobectomy and postsurgical radiation therapy.


Question 28
Refers to the effectiveness of various antibiotics against a particular microorganism.
Explanation
Knowledge of the basic nomenclature of antibiotic use is important to effectively treat patients and communicate with colleagues. The effectiveness of an antimicrobial against an infecting organism is measured by the MIC, which refers to the concentration needed to prevent growth of a microorganism on culture medium, and MBC, which is the smallest concentration of the antibiotic necessary to kill the microorganism in culture. Typically, an antibiotic is considered bactericidal if the MBC is no more than 4 times the MIC. The spectrum of antimicrobial coverage refers to an agent’s effectiveness against a range of bacteria. An antibiogram refers to the tabulation of prevalence of different bacteria in a specific setting or specific patient population. Antibiotic susceptibility and resistance refers to the bacteria’s ability to be affected or unaffected by a given antibiotic.

Question 29
A 19-year-old woman reports persistent neck pain for 2 years. Pain is relieved with aspirin. A bone scan shows intense uptake in the superior, posterior portion of the C3 vertebral body. A sagittal CT reconstruction is shown in Figure 5. Treatment should consist of
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
Hadjipavlou AG, Lander PH, Marchesi D, et al: Minimally invasive surgery for ablation of osteoid osteoma of the spine. Spine 2003;28:E472-E477.
Question 30
..Further imaging shows pulmonary metastases without an obvious primary tumor of origin and an incomplete fracture of the right distal femur. A decision is made to surgically treat his distal femur fracture. What is the role of establishing a preoperative histologic diagnosis for this patient?
Explanation
t(X;18)(p11.2;q11.2)
t(11;22)(q24;q12)
t(1;3)(p36.3;q25)

Question 31
A B Figures 52a and 52b are the radiographs of a patient who was involved in a motor vehicle collision. He was wearing his seat belt and is now complaining of midthoracic back pain. Radiographs in the emergency department do not reveal a fracture. What is the most appropriate next step?
Explanation
Ankylosing spinal disorders, including ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis, are conditions that make the spine rigid and at risk for 3-column unstable fractures. Spinal fractures in these patients pose high risk for complications and death and patients should be counseled and observed closely. Mortality strongly correlates with older age and increased number of comorbidities.
These spine fractures often are not seen at the time of initial evaluation, and a delay in diagnosis can occur in up to 19% of cases. This is particularly common in the setting of non- or minimally displaced fractures following minor injuries. A delayed diagnosis can lead to displacement of a previously nondisplaced fracture that can incur a high neurologic injury risk. Advanced imaging with a CT scan or MRI should be obtained for patients with ankylosing spinal disorders even when minor injuries occur. Although bracing and observation can be used, posterior multilevel spinal instrumentation is typically required to obtain adequate spinal stabilization.
The radiographs show an osteopenic ankylosed thoracic spine; the anteroposterior radiograph clearly shows fusion of the sacroiliac joints. Recognition of these radiographic findings is important when evaluating patients after an injury.
RECOMMENDED READINGS
Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. View Abstract at PubMed
Hendrix RW, Melany M, Miller F, Rogers LF. Fracture of the spine in patients with ankylosis due to diffuse skeletal hyperostosis: clinical and imaging findings. AJR Am J Roentgenol. 1994 Apr;162(4):899-904. PubMed PMID: 8141015. View Abstract at PubMed
Question 32
Figures 15a and 15b are intrasurgical photographs from the posterolateral viewing portal that were taken at the beginning and end of a right shoulder arthroscopic procedure performed on a 54-year-old man. This technique demonstrates superior results compared to traditional arthroscopic techniques when evaluating which outcome?
Explanation
The images reveal a medium-sized tear of the rotator cuff. As more clinical studies are published comparing double-row with single-row rotator cuff repair, it has become clear that the retear rate is lower with a double-row construct for small and medium-sized tears. This may be attributable to the stronger time-zero repair construct that double-row repair provides. No study to date has demonstrated a significant difference in clinical outcomes (functional and pain scores at any time) or time to healing between the 2 techniques.

CLINICAL SITUATION FOR QUESTIONS 16 THROUGH 17
Figure 16 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop," and then he needed help walking off the field. His knee is visibly swollen.
Question 33
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
Explanation
REFERENCES: Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Baker CL, Uribe JW, Whitman C: Arthroscopic evaluation of acute initial anterior shoulder dislocations. Am J Sports Med 1990;18:25-28.
Question 34
Figure 1 shows the radiograph obtained from a 67-year-old woman who has progressive wrist pain. She undergoes a salvage motion-sparing surgery that relies on the intact cartilage of the capitate head. It is necessary to preserve what structure during this procedure?
Explanation
The radioscaphocapitate ligament must be preserved in cases of proximal row carpectomy or scaphoidectomy with four-corner fusion. Failure to do so can result in ulnar translocation of the carpus. The attachment of the long radiolunate ligament to the lunate is compromised in proximal row carpectomy, although it is left intact in scaphoidectomy with four-corner fusion. Preservation of the dorsal radiocarpal ligament through a limited arthrotomy is advocated by Ozyurekoglu and Turker as a method of preserving the blood and nerve supply of the carpus, but this technique has not been proven to be required. The authors did cut through the dorsal intercarpal ligament in their exposure.
Question 35
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What factor most strongly correlates with the development of compartment syndrome after this injury?
Explanation
REFERENCES: Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
Question 36
An otherwise healthy 45-year-old man has a 3-cm subcutaneous mass on his anterior thigh that is presumed to be a lipoma. Removal of the mass is performed in the office of his primary care physician. Pathologic evaluation shows a high-grade malignant fibrous histiocytoma. Staging reveals no evidence of metastatic disease. Management at this time should consist of
Explanation
REFERENCES: Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173.
Giuliano AE, Eilber FR: The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J Clin Oncol 1985;3:1344-1348.
Lewis JJ, Leung D, Espat J, Woodruff JM, Brennan MF: Effect of resection in extremity soft tissue sarcoma. Ann Surg 2000;231:655-663.
Noria S, Davis A, Kardel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 37
An AP radiograph of the pelvis is shown in Figure 4. What muscle attaches to the avulsed fragment of bone identified by the arrow?
Explanation
REFERENCES: Woodburne RT (ed): Essentials of Human Anatomy. New York, NY, Oxford University Press, 1978, pp 542-545.
Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Question 38
Evaluation of the percent of necrosis in the resected specimen after preoperative chemotherapy is of prognostic value for what type of sarcoma?
Explanation
REFERENCES: Rosen G, Marcove RC, Caparros B, Nirenberg A, Kosloff C, Huvos AG: Primary osteogenic sarcoma: The rationale for pre-operative chemotherapy and delayed surgery. Cancer 1979,43:2163-2177.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423-431.
Wunder JS, Paulian G, Huvos AG, Heller G, Meyers PA, Healey JH: The histological response to chemotherapy as a predictor of the oncological outcome of operative treatment of Ewing sarcoma. J Bone Joint Surg Am 1998;80:1020-1033.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 39
A 57-year-old man has had right ankle pain for the past 10 months following an injury that went untreated. Radiographs are shown in Figures 30a through 30c. Management should consist of
Explanation
REFERENCES: Marti RK, Raaymakers EL, Nolte PA: Malunited ankle fractures: The late results of reconstruction. J Bone Joint Surg Br 1990;72:709-713.
Geissler W, Tsao A, Hughes J: Fractures and injuries of the ankle, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2201-2206.
Yablon IG, Leach RE: Reconstruction of malunited fractures of the lateral malleolus. J Bone Joint Surg Am 1989;71:521-527.
Question 40
-While obtaining informed consent for a lateral closing-wedge osteotomy, what complication should be discussed with the patient as exclusive to this procedure and not encountered in medial opening-wedge osteotomy?
Explanation

Figure 56 is the MRI scan of a 15-year-old girl who had left knee pain after sustaining a noncontact twisting injury while playing soccer. She reported severe pain initially that has since improved. On examination, she had a large knee effusion with lateral joint line tenderness. Range of motion is from 5 degrees of extension to 70 degrees of flexion. She wishes to return to sports at her preinjury level of activity.
Question 41
Figure 9 is the clinical photograph of a 68-year-old woman 10 days after undergoing primary total knee replacement. She is experiencing hemarthrosis, discoloration, and bruising of the soft tissue about the knee; her history includes persistent serous drainage. This clinical appearance likely is associated with
Explanation
Certain anticoagulants are associated with an increased risk for wound complications. Two studies showed an increase in postsurgical bleeding and wound drainage following use of LMWH. Other investigators have associated use of anticoagulants such as LMWH with an increased incidence of persistent wound drainage and subsequent infection. Current evidence does not support a significant difference in complication rates with and without the use of wound drains or a tourniquet. Regional anesthesia has been associated with less blood loss than general anesthesia and is not associated with a difference in wound complication incidence.

Question 42
In children with isolated zone II lacerations of the flexor tendon, poor digital motion is best correlated with
Explanation
REFERENCE: O’Connell SJ, Moore MM, Strickland JW, Frazier GT, Dell PC: Results of zone I and zone II flexor tendon repairs in children. J Hand Surg Am 1994;19:48-52.
Question 43
A 58-year-old patient suddenly develops cardiac arrest while undergoing a routine total knee arthoplasty. He is resuscitated with 20% lipid emulsion. What was the most likely causative agent for cardiac arrest?
Explanation
Bupivacaine is a long acting local anesthetic. It acts on intracellular voltage-gated sodium channels to block sodium influx into nerve cells, which prevents depolarization. If administered systemically, bupivacaine can cause serious complications to the cardiovascular system. Side effects include hypotension, arrhythmia, bradycardia, heart block, and cardiac arrest. Treatment should involve urgent administration of intravascular lipid emulsion alongside standard ACLS protocols.
Rosenblatt et al. describe the successful use of a 20% lipid emulsion to resuscitate a patient after a presumed bupivacaine-related cardiac arrest. Resuscitation involved a lipid emulsion bolus of 1 mL/kg given immediately, which was followed by a continuous infusion until the patient stabilized.
Corman et al. evaluated the use of lipid emulsion for reversal of local anesthetic-induced toxicity. They suggest that lipid emulsion may reverse local anesthetic toxicity by extracting lipophilic local anesthetics from aqueous plasma or tissues or by counteracting local anesthetic inhibition of myocardial fatty acid oxygenation.
Illustration A shows an ECG of a patient with clinical deterioration after systemic administration of bupivicaine. The ECG shows complete heart block with multifocal ventricular beats. The patient progressed to asystole.
Inncorrect Answers:
Question 44
What does Dual Energy X-ray Absorptiometry (DEXA) testing, as a technique, measure?
Explanation
REFERENCES: Genant HK, Faulkner KG, Gluer CC: Measurement of bone mineral density: Current status. Am J Med 1991;91:49S-53S.
Genant HK, Engelke K, Fuerst T, et al: Review: Noninvasive assessment of bone mineral density and stature: State of the art. J Bone Miner Res 1996;11:707-730.
Engelke K, Gluer CC, Genant HK: Factors influencing short-term precision of dual X-ray bone absorptiometry (DXA) of spine and femur. Calcif Tissue Int 1995;56:19-25.
Question 45
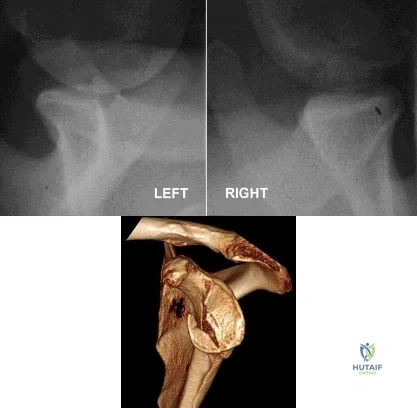
Figure A is the radiograph of an 11-year-old boy who fell directly on his left shoulder while riding a bicycle. He complained of pain in his left shoulder. An MRI scan of the injury is likely to reveal what findings? Review Topic

Explanation
Question 46
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
REFERENCES: Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
McGuire DA, Hendricks SD, Sanders HM: The relationship between anterior cruciate ligament reconstruction tibial tunnel location and the anterior aspect of the posterior cruciate ligament insertion. Arthroscopy 1997;13:465-473.
Question 47
The axis of forearm rotation occurs between what two anatomic points?
Explanation
REFERENCES: Werner FW, An KN: Biomechanics of the elbow and forearm. Hand Clin 1994;10:357-373.
Tynan MC, Fornalski S, McMahon PJ, et al: The effects of ulnar axial malalignment on supination and pronation. J Bone Joint Surg Am 2000;82:1726-1731.
Question 48
A 30-year-old man undergoes arthroscopic Bankart repair for recurrent anterior dislocation. He continues to experience instability postoperatively. Examination reveals a positive apprehension test. Radiographs of both shoulders are seen in Figure A. CT scan of his left shoulder is seen in Figure B. What is the best treatment option? Review Topic
Explanation
Patients with glenoid bone defects >20-30% have a high recurrence rate (>60%) after Bankart repair alone. Bone grafting is necessary to offer containment. Autograft options include coracoid transfer (such as the Latarjet procedure which extends the articular arc and creates a conjoined tendon sling) and iliac crest bone grafting.
Burkhart et al. addressed glenohumeral bone defects. They advise that significant bone deficits cannot be adequately addressed via arthroscopic Bankart repair alone. The Latarjet transfer creates an extra-articular platform to extend the articular arc of the glenoid.
Hantes et al. assessed Latarjet repairs using CT. They found that there is almost
complete repair of a 25% to 30% glenoid defect when using the Latarjet procedure.
Figure A comprises comparison Bernageau view glenoid profile radiographs of both shoulders. Figure B is a 3D reconstruction CT with showing glenoid bone deficiency (inverted pear deformity) with a large bony Bankart lesion. Illustration A shows the method of obtaining a Bernageau glenoid profile view. Illustration B shows the "cliff sign" of anterior glenoid bone loss. Illustration C depicts the Latarjet procedure. Illustration D depicts reduction in the articular arc with anterior glenoid loss.
Incorrect Answers:
Question 49
A concussion diagnosis is made when there is
Explanation
Neurocognitive testing is a helpful tool in the management of concussions, but testing does not independently determine if an athlete has experienced a concussion or when he or she can return to play. Neuroimaging findings typically are normal in concussive injury. Loss of consciousness occurs in fewer than 10% of patients with concussions. A concussion diagnosis is difficult to determine because of the lack of objective clinical and/or imaging findings. In general, a concussion is a disturbance in brain function caused by a direct or indirect force to the head.

RESPONSES FOR QUESTIONS 26 THROUGH 31
Plain radiographs
CT scan
MRI
Arthrogram
Which imaging method listed above is most appropriate for definitive diagnosis and management of each clinical scenario described below?
Question 50
A 45-year-old man sustained the injury seen in Figure 130a 6 weeks ago. He denies any prior injury to his shoulder. After treatment of the injury in the emergency department, he was noted to have significant weakness with empty can testing and external rotation at the side. He has full passive range of motion with forward flexion, abduction, and internal and external rotation, but has difficulty initiating abduction with his arm at his side. He has negative apprehension and relocation signs. A detailed neurologic examination shows no deficits. A coronal image from a follow-up MRI scan is seen in Figure 130b. Follow-up radiographs reveal no fractures. What is the most appropriate next step in his treatment? Review Topic
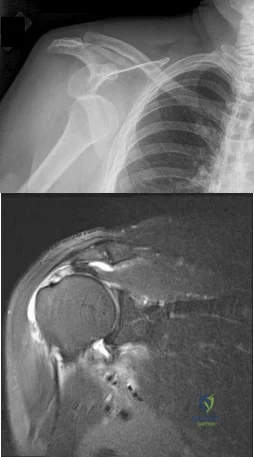
Explanation
Question 51
Figure 42 shows the sagittal T2-weighted MRI scan of a patient’s right knee. These findings are most commonly seen with a complete tear of the
Explanation
fluid in the soft tissues laterally. Additionally, there is a large bone bruise on the medial
femoral condyle. This combination indicates injury to the posterolateral complex. These injuries often have coexisting anterior and/or posterior cruciate ligament injuries. Failure to recognize the posterolateral corner injury can lead to failure of anterior or posterior cruciate ligament reconstructions.
REFERENCES: LaPrade RF, Gilbert TJ, Bollom TS, et al: The magnetic resonance imaging appearance of individual structures of the posterolateral knee: A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 2000;28:191-199.
Ross G, Chapman AW, Newberg AR, et al: Magnetic resonance imaging for the evaluation of acute posterolateral complex injuries of the knee. Am J Sports Med 1997;25:444-448.
Question 52
What is the most likely diagnosis based on the MRI findings shown in Figures 87a and 87b? Review Topic

Explanation
Question 53
Which of the following findings is considered a poor prognostic factor for postoperative neurologic recovery in patients with rheumatoid arthritis?
Explanation
REFERENCES: Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Casey AT, Crockard HA, Bland JM, et al: Predictors of outcome in the quadriparetic nonambulatory myelopathic patient with rheumatoid arthritis: A prospective study of 55 surgically treated Ranawat Class IIIb patients. J Neurosurg 1996;85:574-581.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 54
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
Robinson RP, Lovell TP, Green TM, Bailey GA: Early femoral component loosening in DF-80 total hip arthroplasty. J Arthroplasty 1989;4:55-64.
Question 55
Figures below show the radiographs obtained from a 19-year-old woman with a 3-year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?

Explanation
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 56
Figures 48a and 48b show the elbow radiographs of a 5-year-old boy who fell from a tree after dinner. Examination reveals that he is unable to extend his wrist. Management should consist of immediate
Explanation
REFERENCES: Iyengar SR, Hoffinger SA, Townsend DR: Early versus delayed reduction and pinning of type III displaced supracondylar fractures of the humerus in children: A comparative study. J Orthop Trauma 1999;13:51-55.
Leet AI, Frisancho J, Ebramzadeh E: Delayed treatment of type 3 supracondylar humerus fractures in children. J Pediatr Orthop 2002;22:203-207.
Question 57
Figures 1a and 1b show the clinical photograph and oblique radiograph of a 52-year-old man who has plantar first metatarsal pain. A felt pad in the shoe proximal to the area of pain has failed to provide relief. Management should now consist of
Explanation
REFERENCES: Mann RA, Wapner KL: Tibial sesamoid shaving for treatment of intractable plantar keratosis. Foot Ankle 1992;13:196-198.
Mann RA, Mann JA: Keratotic disorders of the plantar skin. Instr Course Lect 2004;53:287-302.
Question 58
Figure 3a is the initial radiograph of a 19-year-old man who sustained a closed clavicle fracture. Figures 3b and 3c show postoperative radiographs. If the patient had been treated nonsurgically, which of the following would most likely occur?
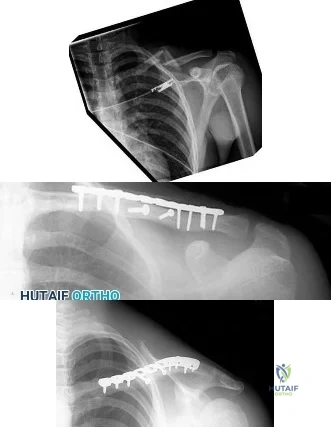
Explanation
Question 59
A 6-year-old girl is brought in for orthopaedic examination because she “walks funny” and occasionally trips. Her feet are normal in appearance. Internal rotation of her hips is 60 degrees and external rotation is 40 degrees bilaterally. The thigh-foot angle on the right is -20 degrees, and +10 degrees on the left. What is the source of her gait abnormality?
Explanation
Question 60
A 62-year-old man who underwent total knee arthroplasty 6 months ago now reports pain after falling on the anterior portion of the knee. Examination reveals weakness of knee extension but no extensor lag. Flexion that had once measured 115 degrees is now limited to 70 degrees because of pain. A radiograph is shown in Figure 25. Management should now consist of
Explanation
REFERENCES: Brown TE, Diduch DR: Fractures of the patella, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, vol 2, pp 1290-1312.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 323-337.
Question 61
With comparison to a below the knee amputation, each of the following are disadvantages of a through the knee amputation EXCEPT:

Explanation
The cohort study by MacKenzie et al prospectively followed 161 patients that were part of the Lower Extremity Assessment Project (LEAP). These patients underwent an above-the-ankle amputation at a trauma center within 3 months following the injury and followed for 2 years. This study revealed that through-the-knee amputations had significantly worse scores for the objective performance measures of self-selected walking speed, independence in transfers, walking, and stair-climbing. Through-the-knee amputees also had worse SIP scores than AKA and BKA patients. Physicians were also less satisfied with both the clinical and the cosmetic recovery of the patients with a through-the-knee amputation. It should be noted that patients with a BKA had a faster walking speed than those with an AKA. Despite the worse SIP scores for through-the-knee amputations, patients actually reported less pain than those with an AKA or BKA, though this wasn't statistically significant.
(SBQ06.2) A 21-year-old male presents to the emergency department after sustaining a gun shot wound to his back. Subsequent radiographs reveal a bullet in the L2 vertebral body. Physical exam shows no neurologic deficits. He undergoes emergent laparotomy and is found to have a small bowel laceration. What would be the preferred treatment following his exploratory laparotomy and small bowel repair?

Intravenous antibiotic coverage for Gram negative bacteria for 7 days

Surgical decompression and bullet fragment removal

Observation

Broad-spectrum oral antibiotic coverage for 7 days
Broad-spectrum intravenous antibiotic coverage for 7 days
DISCUSSION: The clinical presentation is consistent with a GSW with bowel perforation and a retained bullet in the vertebral body. Because the patient is neurologically intact broad-spectrum intravenous antibiotic coverage for 7 days is the most appropriate treatment.
Gunshot wounds to the spine present relatively little risk of infection in most cases. When there has been an injury to the small bowel, the risk of infection can be minimized with a 7-day course of broad-spectrum antibiotics. Indications for surgery include when a neurological deficit is present that correlates with imaging findings of neurological compression by the missile, or when the missile is in contact with the CSF posing a risk for metal toxicity.
Roffi et al performed a Level 4 study of 42 patients that sustained a gunshot wound that perforated the stomach or bowel and then entered the spinal column. They found that an extended regimen of broad spectrum antibiotics combined with bedrest appeared to significantly reduce the risk of spinal or paraspinal infection, whereas early bullet removal did not significantly prevent the occurrence of infection.
Velmahoos et al performed a Level 4 study including 24 patients that sustained a gunshot wound to the spine with associated colonic injury. They found that the incidence of sepsis was 8.4% (compared to 5% in non-bowel injuries) and concluded that retainment of the bullet did not increase the rate of sepsis.
Incorrect Answers:
Question 62
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time? Review Topic
Explanation
Question 63
- An otherwise healthy 65-year-old man has had chronic pain in his prosthetic knee for the past 9 months. Repeated aspirations reveal a coagulase-negative staphylococcus infection. To eradicate the infection while maintaining the best possible joint function, management should consist of
Explanation
Present recommendations are to avoid a one-stage reconstruction in a patient in whom a glycocalyx elaborating microorganism has been isolated. In one study 52% of the isolates of S. epidermidis and 28% of the isolates of S. aureus elaborated glycocalyx. The microbiology laboratory can be asked to determine if the microorganisms elaborate glycocalyx. In the present case it should be assumed that the staphylococci elaborate glycocalyx and are resistant to antibiotics. A two-stage procedure is indicated for these reasons alone.
Antibiotic therapy alone has been used for a select group of patients who could not medically tolerate either a one-stage or a two-stage arthroplasty. The patient in this case is listed as otherwise healthy.
The decision to perform a resection arthroplasty as a definitive procedure without reimplantation is based on the bacteria’s resistance to antibiotics, quality of the local soft tissues, the complexity of the reconstruction, the patient’s refusal to have another operation, the patient’s overall health, or a combination of these factors. None of which appear to be present in this case.
Question 64
A 20-year-old professional female jockey who is wearing a helmet is thrown from her horse. What is the most likely location of her injury?
Explanation
be one per 350 riding hours to one per 1,000 riding hours. Of these injuries, approximately
15% to 27% are severe enough to warrant hospital admission. Significant and serious injuries in equestrian activities are associated with recreational riders and those not wearing a helmet. Head and spine injuries are more common in recreational and nonhelmeted riders. Extremity injuries are more common in professional and helmeted riders. Professional riders are less likely to be admitted to the hospital than recreational riders, and are about half as likely to be disabled
at 6 months after injury as recreational riders.
REFERENCES: Lim J, Puttaswamy V, Gizzi M, et al: Pattern of equestrian injuries presenting to a Sydney teaching hospital. ANZ J Surg 2003;73:567-571.
Petridou E, Kediloglou S, Belechri M, et al: The mosaic of equestrian-related injuries in Greece. J Trauma 2004;56:643-647.
Question 65
The optimal method with which to diagnose component malrotation in total knee arthroplasty (TKA) is
Explanation
The epicondylar axis and tibial tubercle can be used as references on CT scans to quantitatively measure rotational alignment of the femoral and tibial components. This technique has been used to determine whether rotational malalignment is present and whether revision of 1 or both components may be indicated. Although clinical assessment is useful, malrotation can occur as a result of deformities unrelated to the arthroplasty. Similarly, an isolated radiographic skyline view of the patella may indicate a problem with patellar maltracking, but cannot quantitatively assess malrotation of the components. MR imaging proves useful for evaluating painful TKA, but it is dependent on the center’s quality and has not yet been shown to quantify component malrotation.

CLINICAL SITUATION FOR QUESTIONS 20 THROUGH 22
Figures 20a and 20b are the radiographs of an elderly woman who underwent total knee arthroplasty (TKA) several years ago. She now states that something is not right; her knee frequently swells and is diffusely painful, especially at the end of the day. She does not trust her knee, especially while going up and down stairs or getting up from a chair.
Question 66
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?
Explanation
REFERENCES: Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Manske PR (ed): Hand Surgery Update. Rosemont, IL, American Society for Surgery of the Hand, 1994, pp 197-205.
Question 67
Figure A shows the operative technique used during arthroscopic repair of 25-year-old male patient with vague shoulder pain. The glenoid rim was prepared using the drill bit insertion angles as shown. Three suture anchors, measuring 14mm in length were inserted 4-6 mm deep to the surface. What structure is at the highest risk with this technique? Review Topic
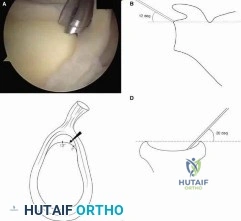
Explanation
At the scapular spine level, the suprascapular nerve is approximately 1.5-2.0 cm from the glenoid cortex. This places the nerve at risk of injury during shoulder surgery, and injuries have been described. Arthroscopic SLAP repair is known to be a safe and relatively simple procedure. However, deep drilling or anchor insertion from the anterior or anteriosuperior portal during SLAP repair can place the suprascapular nerve at risk of iatrogenic injury.
Morgan et al. performed a cadaveric study to compare the risk of injury to the suprascapular nerve during suture anchor placement in the glenoid when using an anterosuperior portal versus a rotator interval portal. Standard 3 × 14 mm suture anchors were placed in the glenoid rim (1 o’clock, 11 o’clock, and 10 o’clock positions for the right shoulder). They showed that the distance from the far-posterior anchor tip to the suprascapular nerve averaged 8 mm (range, 3.4 to 14 mm) for the anterosuperior portal and 2.1 mm (range, 0 to 5.5 mm) for the rotator interval portal (P = .001).
Koh et al. evaluated the risk of suprascapular nerve injury during the drilling and anchor insertion for anterior SLAP repair. They inserted 1 suture anchor
arthroscopically from the anterior portal at 00:30-1:00 o’clock in right shoulders (11-11:30 in left). Using a mean drill depth was 14.2 (±2.8) mm, all suture anchors perforated the glenoid wall and the tips were measured to be approx. 3.1 (±2.7) mm from the suprascapular nerve.
Figure A shows an arthroscopic view and corresponding schematic image of arthroscopic drill position for SLAP repair. Illustration A shows the close proximity of anchor tip to the suprascapular nerve, as the nerve nerve enters the supraspinatus fossa below the superior transverse scapular ligament and then enters the infraspinatus fossa between the neck of the scapula and base of the spine of the scapula.
Incorrect Answers:
(SBQ11UE.106) A 60 year-old diabetic man presents with increasing right shoulder pain and stiffness for 10 weeks. He works as a lawyer and has been treating the pain with non-steroidal anti-inflammatory drugs with little improvement. He had a previous injury to his right shoulder 15 years ago while playing hockey, but cannot recall any recent precipitants for this presentation. Physical examination shows significant reduction in right shoulder range of motion, with the greatest loss in external rotation. His MRI images are seen in Figures A-C. What would be the most appropriate treatment? Review Topic

Open supraspinatus cuff repair
Arthroscopic supraspinatus cuff repair
Reverse shoulder arthroplasty
Arthroscopic posterior capsular release
Physical therapy and medical management
The patient is presenting with right shoulder adhesive capsulitis. The most appropriate treatment at this time would be physical therapy and medical management (i.e., nonsteroidal anti-inflammatories +/- intra-articular steroid injections).
Adhesive capsulitis (aka frozen shoulder) is defined by pain and loss of both active and passive motion, especially loss of external rotation in comparison to the contralateral side. Risk factors include diabetes, thyroid disease, age, previous surgery and prolonged immobilization. Initial treatment options include NSAIDs, physical therapy, and intra-articular steroid injections. Surgical treatment is not commonly recommended, but may be used late in the course to address residual stiffness if extensive therapy has failed.
Griggs et al. prospectively reviewed seventy-five consecutive patients (seventy-seven shoulders) with adhesive capsulitis. They showed that 90 percent of the patients reported a satisfactory outcome with shoulder stretching exercises. However, male gender and diabetes mellitus were associated with worse motion at the final evaluation.
Hannafin et al. reviewed the treatment options for adhesive capsulitis. They suggest
that benign neglect, home-based and supervised physical therapy, and intra-articular corticosteroid injections should be considered in the early treatment of adhesive capsulitis. Duration of treatment should be considered for at least 3 months before more aggressive treatments are considered.
Levine et al. retrospectively reviewed the treatment and outcome of 234 patients with adhesive capsulitis. No significant difference was found for success of nonoperative treatment versus operative treatment or patient gender. With supervised treatment, most patients with adhesive capsulitis experience resolution with nonoperative measures in a relatively short period.
Figures A (Sagittal oblique T1 MRI), and Figure B (coronal oblique fat-saturated T2 MRI) show the anterior rotator cuff interval in the right shoulder demonstrate high-signal soft tissue thickening of the coracohumeral ligament (arrow). Figure C (Coronal oblique fat-saturated T2 MRI) demonstrates a thickened inferior glenohumeral ligament of the right shoulder.
Incorrect Answers:
Question 68
- A clinical trial is being conducted on a new orthopaedic device that is different from existing devices that are moderately successful, but have frequent complications when used to treat fractures in the elderly. To comply with international standards for clinical trials, the investigator must include in the study design
Explanation
Question 69
Osteoarthritic cartilage is characterized by decreased
Explanation
Chondrocytes in OA are much more metabolically active than those of normal cartilage. Studies reveal measuring the levels of utilization on sulfate and H-glucosamine informing components of cartilage matrix. The amount of DNA also rises in OA cartilage most noticeable at the articular chondrocyte.
The synthesis of hyaluronate increases. Recent data suggests 1) hyaluronate that is synthesized is abnormal and, hence, does not allow aggregation; or 2) The excess synthesis is a response to a rapid degradation of synthesized product. This is in light of the fact that synthesis increases, yet concentration of hyaluronate decreases.
The correct answer is that proteoglycan content decreases. The synthesis of proteoglycan increases in OA, but due to the increased rate of breakdown of proteoglycan there is a net result of lowered proteoglycan content.
Question 70
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of
Explanation
REFERENCES: Blazina ME, et al: Jumper’s knee. Orthop Clin North Am 1973;4:665.
Kelly DW, Carter VS, Jobe FW, Kerlan RK: Patellar and quadriceps tendon ruptures: Jumper’s knee. Am J Sports Med 1984;12:375-380.
Krums PE, Ryder B: Operative treatment of patella tendon disorders. Operative Techniques Sports Med 1994;2:303.
Rows J, et al: Patella tendinitis (jumper’s knees). Am J Sports Med 1978;6:362.
Question 71
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis? Review Topic

Explanation
Question 72
A 47-year-old man comes for evaluation of his dominant right elbow, which has been bothering him with activity for the past 3 months, especially with activities requiring wrist extension. He is an active squash player and has been unable to continue this sport. Examination shows tenderness at the common extensor origin. What is the next best step? Review Topic
Explanation
Lateral epicondylitis is a common problem with numerous non-operative treatments available. There is little scientific evidence to support any of these treatments however and the quality of most reports is low and their conclusions limited by bias and/or study design. Tennis elbow often resolves with time regardless of which conservative treatment is chosen.
Coombes et al. randomized patients with unilateral tennis elbow to receive either (1) corticosteroid injection, (2) placebo injection, (3) corticosteroid injection plus physical therapy or (4) placebo injection plus physical therapy. They found that
corticosteroid resulted in worse clinical outcome and recurrence rate compared to placebo injection. Use of physical therapy did not produce any significant differences.
Dines et al. review the diagnosis and of tennis injuries, including lateral epicondylitis. Although they acknowledge that there is "no long term benefit with regard to tendon healing," they note that steroid injection may be useful to control acute symptoms.
Boyer et al. review the myths surrounding lateral epicondylitis. They note that despite widespread use, corticosteroid injection has repeatedly been shown to have no long term benefit. They conclude based on their review of the literature that if there is any benefit to steroid injection, it is of short duration, and in patients whose symptoms have been of short duration, without any previous treatment.
Incorrect answers:
Question 73
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show
Explanation
REFERENCES: Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Question 74
Ulnohumeral distraction interposition arthroplasty is considered the most appropriate treatment for which of the following patients?
Explanation
REFERENCES: Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Mansat P: Surgical treatment of the rheumatoid elbow. Joint Bone Spine 2001;68:198-210.
Question 75
Figures below represent the radiographs obtained from a 37-year-old man with severe right knee pain. He has a history of prior tibial osteotomy for adolescent tibia vara but notes residual bowing of his legs. On examination, he is 5'8" tall and weighs 322 pounds. He has a waddling gait with a bilateral varus thrust and 20° varus deformity of both legs. His right knee range of motion is 0° to 120° with a fixed varus deformity. What is the best next step?

Explanation
This patient has severe, uncorrectable varus deformity and pain from end-stage osteoarthritis secondary to prior adolescent tibia vara. Although he is young to consider arthroplasty, this option is likely to give him the most functional limb, compared with arthrodesis with a long antegrade nail. During arthroplasty surgery, his knee will likely require extensive medial release to achieve anatomic limb alignment. Standard components in total knee arthroplasty likely would result in lateral instability, so this option is
not the best answer. The best choice is total knee arthroplasty with a constrained device, which adds constraint to the knee to provide balance.
Question 76
Long-term alendronate (Fosamax) use for osteoporosis has been associated with which of the following?
Explanation
fractures of the femur. Osteonecrosis of the jaw has been described but not in other anatomic locations. Scurvy occurs because of a lack of vitamin C and use of bisphosphonates is not associated with uterine cancer or a detached retina.
Question 77
Figure 11 shows the radiograph of a 3-year-old girl who sustained a proximal radius injury. Appropriate initial management should include
Explanation
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39.
Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Gonzalez-Herranz P, Alvarez-Romera A, Burgos J, et al: Displaced radial neck fractures in children treated by closed intramedullary pinning (Metaizeau technique). J Pediatr Orthop 1997;17:325-331.
Question 78
-is the photograph of a 2-month-old infant with a left leg deformity. The mother’s pregnancy and delivery were unremarkable, and the infant is otherwise healthy. What is the most appropriate course of action?
Explanation


Question 79
A 45-year-old man has had left thigh pain for the past 4 months. An AP radiograph, bone scan, MRI scans, and biopsy specimens are shown in Figures 6a through 6f. What is the most appropriate treatment?
Explanation
REFERENCES: Hadjipavlou AG, Gaitanis IN, Kontakis GM: Paget’s disease of the bone and its management. J Bone Joint Surg Br 2002;84:160-169.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 187-196.
Question 80
A 7-year-old male is struck by a motor vehicle while crossing the street and suffers an open tibia fracture with a crush injury of the ipsilateral foot. After multiple attempts at limb salvage, the family and treating surgeon elect to proceed with a knee disarticulation. What complication of pediatric amputations is avoided with a knee disarticulation as opposed to a transtibial amputation?

Explanation
Krajbich reviews the management of pediatric patients with lower-limb deficiences and amputations. He advocates disarticulation as opposed to transosseous amputation when possible as bone overgrowth has not been observed in bone ends covered by articular cartilage.
O'neal et al retrospectively reviewed their rates of surgical revision for bone overgrowth in pediatric and adolescent amputees. The highest rates of revision were seen with metaphyseal-level amputations (50%) and with traumatic amputations (43%).
Benevenia et al reviewed their rates of overgrowth in skeletally immature transosseous amputees using an autogenous epiphyseal transplant from the amputated limb to cap the medullary canal. They found that only 1 of 10 patients undergoing amputation with this technique had complications due to bone overgrowth, compared with 6 of 7 patients undergoing traditional transosseous amputation.
Illustration A is a clinical photo of bone overgrowth eroding through the soft tissue in a transhumeral amputee. Illustration B demonstrates the radiographic appearance of bone overgrowth in a transtibial amputation.
Incorrect Answers:
Question 81
A medial plate is best used to treat tibial plateau fractures when there is
Explanation
The patient's plain radiographs demonstrate a bicondylar tibial plateau fracture with complete separation of the diaphysis from the epiphysis, making this a Schatzker VI injury. Clinically, the patient is neurovascularly intact with symmetric palpable pulses, and ankle brachial indices are not necessary.
There is significant lateral tibial plateau displacement with the lateral femoral condyle down into the plateau defect. Considering the swelling, abrasions, and severity of the injury, a bridging external fixator is warranted followed by CT imaging.
The ligamentotaxis will provide better definition of the injury and joint fragments and allow for soft-tissue rest and subsidence of the swelling for eventual surgical intervention. Oblique views will not add as much information as CT imaging, which will show the bicondylar nature of the injury and the proximal tibia essentially split centrally with the tubercle as a separate fragment. A midline incision with medial and lateral plating has fallen out of
favor secondary to wound-healing complications. Comminution of the metaphysis or the lateral side is not an absolute indication for a medial plate. Open lateral fractures can still be managed with a laterally based plate depending on the soft-tissue injury.
RECOMMENDED READINGS
Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. doi: 10.1097/BOT.0b013e31818f8dc1. PubMed PMID: 19104303. View Abstract at PubMed Higgins TF, Klatt J, Bachus KN. Biomechanical analysis of bicondylar tibial plateau fixation: how does lateral locking plate fixation compare to dual plate fixation? J Orthop Trauma. 2007 May;21(5):301-6. PubMed PMID: 17485994. View Abstract at PubMed
Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164. View Abstract at PubMed
Barei DP, O'Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. doi:10.1097/BOT.0b013e318169ef08. PubMed PMID: 18317051.
View Abstract at PubMed
Barei DP, Nork SE, Mills WJ, Coles CP, Henley MB, Benirschke SK. Functional outcomes of severe bicondylar tibial plateau fractures treated with dual incisions and medial and lateral plates. J Bone Joint Surg Am. 2006 Aug;88(8):1713-21. PubMed PMID: 16882892. View Abstract at PubMed
Hall JA, Beuerlein MJ, McKee MD; Canadian Orthopaedic Trauma Society. Open reduction and internal fixation compared with circular fixator application for bicondylar tibial plateau fractures. Surgical technique. J Bone Joint Surg Am. 2009 Mar 1;91 Suppl 2 Pt 1:74-88. doi: 10.2106/JBJS.G.01165. PubMed PMID: 19255201. View Abstract at PubMed
Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg Am. 2011 Aug 17;93(16):1548-59. PubMed PMID: 22204013. View Abstract at PubMed
Weil YA, Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Posteromedial supine approach for reduction and fixation of medial and bicondylar tibial plateau fractures. J Orthop Trauma. 2008 May-Jun;22(5):357-62. doi: 10.1097/BOT.0b013e318168c72e. PubMed PMID:
Question 82
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain? Review Topic

Explanation
Question 83
What is the most commonly reported complication following elbow arthroscopy?
Explanation
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of elbow arthroscopy.
J Bone Joint Surg Am 2001;83:25-34.
Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 84
A 7-year-old girl reports foot pain and has difficulty ambulating. History reveals that she fell off a scooter 1 week ago, and there is possible exposure to a tick bite. A radiograph is shown in Figure 29. What is the best course of action?
Explanation
REFERENCES: Borges JL, Guille JT, Bowen JR: Kohler’s bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-598.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 65-78.
Question 85
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
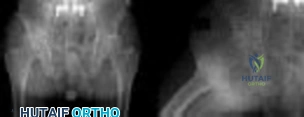
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to surgery.
Question 86
A 68-year-old woman underwent a successful total right hip arthroplasty with a metal-on-metal articulation and cementless porous-coated components. Three months later, she underwent identical surgery on the left hip. Three months after surgery on the left hip, she reports groin pain on ambulation. Examination reveals significant groin discomfort with passive hip motion, particularly at the extremes of motion. Radiographs are shown in Figures 21a and 21b. Laboratory studies show an erythrocyte sedimentation rate of 35 mm/h and a C-reactive protein of 0.9. Aspiration yields scant growth of Staphylococcus epidermidis in the broth only, with no evidence of loosening on arthrography. A second aspiration yields scant growth of Staphylococcus epidermidis in the broth only. What is the most likely cause of the patient’s pain?
Explanation
REFERENCES: White RE: Evaluation of the painful total hip arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998,
vol 2, pp 1377-1385.
Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
Question 87
Figure 24 shows the arthroscopic view of a patient with ankle impingement syndrome. This is commonly seen after high ankle sprains and represents fibrotic granulation thickening of what structure?
Explanation
REFERENCES: Hopkinson WJ, St Pierre P, Ryan JB, Wheeler JH: Syndesmosis sprains of the ankle. Foot Ankle 1990;10:325-330.
Amendola A: Controversies in diagnosis and management of syndesmosis injuries of the ankle. Foot Ankle 1992;13:44-50.
Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
Pfeffer GB (ed): Chronic Ankle Pain in the Athlete. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 11.
Question 88
Figure 1 depicts an intraoperative photograph obtained following proximal row carpectomy. The black dot denotes the capitate. The top of the figure is radial and the bottom of the figure is ulnar. Surgical disruption of the structure identified by the forceps would result in
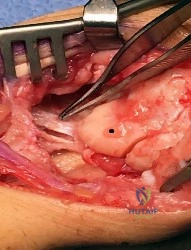
Explanation
The structure identified by the forceps is the radioscaphocapitate ligament. During a proximal row carpectomy, it is very important to identify and protect this ligament. Compromise of the ligament would result in ulnar translocation of the carpus and early failure of the proximal row carpectomy procedure. If the ligament is injured during surgery, immediate repair should be performed. Green and associates discuss the importance of the radioscaphocapitate ligament in stabilizing the carpus after this procedure is performed. Nakamura and associates compared 3-mm, 6-mm, and 10-mm radial styloidectomies, and only the 3-mm styloidectomy subsequently preserved carpal stability. Compromise of the radioscaphocapitate ligament occurred when larger portions of the radial styloid were excised. Distal radioulnar joint instability would result only from the disruption of the distal radioulnar joint stabilizers. Avascular necrosis would not occur, because the capitate receives its blood supply mainly from the palmar vessels. Finally, loss of active thumb IP flexion would not occur, because the flexor pollicis longus tendon would remain intact even if ligament compromise were to occur.
Question 89
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?
Explanation
REFERENCES: Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.
Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Question 90
9 degress Celsius, serum WBC is 14,000, and his C-reactive protein is elevated. He reports that he uses IV heroin. A coronal 3D CT scan of the left clavicle is shown in Figure B. Joint aspiration shows many grams stain positive organisms. Which of the following organisms is the most likely pathogen?

Explanation
Ross et al states "Staphylococcus aureus is now the major cause of
sternoclavicular septic arthritis in intravenous drug users. Pseudomonas aeruginosa infection in injection drug users declined dramatically with the end of an epidemic of pentazocine abuse in the 1980s."
The referenced article by Goldin et al is from the New England Journal of Medicine reports that all of their cases of SC joint septic arthritis were in intravenous drug abusers and that P. aeruginosa grew out of 3 patients and S. aureus grew out of 1 patient.
A more recent article by Abu Arab et al reported that Staph aureus was most common even in IV drug users. The review article by Higginbotham and Kuhn note that risk factors for SC joint septic arthritis include hemodialysis, immunocompromise, alcoholism, and HIV. Neisseria gonorrhoeae, fungal, and candida present in HIV patients.
Treatment is I&D and appropriate antibiotics, although aspiration and abx have shown some success too. CT and MRI are useful in diagnosis, and open biopsy or aspiration is recommended for definitive diagnosis.
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?
Degenerative lumbar spine changes
Ipsilateral ankle pain and stiffness
Ipsilateral hip joint degenerative changes
Contralateral hip joint degenerative changes
Ipsilateral medial knee degenerative changes Correct answer: 2
A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted
that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
A 33-year-old man sustains a femur fracture in a motorcycle accident. AP and lateral radiographs are provided in Figure A. Prior to surgery, a CT scan of the knee is ordered for preoperative planning. Which of the following additional findings is most likely to be discovered?

Tibial eminence fracture
Sagittal plane fracture of the medial femoral condyle
Schatzker I tibia plateau fracture
Coronal plane fracture of the lateral femoral condyle
Axial plane fracture through the medial femoral condyle Correct answer: 4
The "Hoffa fracture" is a coronal plane fracture of the femoral condyle that is often missed on plain radiographs of supracondylar and intercondylar femur fractures. It involves the lateral condyle more frequently than the medial.
Identification is important as it may impact operative planning and likely require screw fixation in the anteroposterior plane.
Nork et al. reviewed 202 supracondylar-intercondylar distal femoral fractures and found a 38% prevalence of associated coronal plane fractures. The authors recommend CT scan imaging of all supracondylar and intercondylar fractures.
Ostermann et al reported on 24 unicondylar fractures of the distal femur treated with open reduction internal fixation with a screw construct. Twenty-
three patients acheived satisfactory results at 5 year follow-up. Illustrations A and B are another example of a supracondylar femur fracture with an associated Hoffa fracture identified on CT scan.

A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
closed reduction and early range of motion
radial head resection and lateral collateral ligament reconstruction
radial head resection and coronoid open reduction internal fixation
radial head arthroplasty and coronoid open reduction internal fixation
radial head arthroplasty, coronoid open reduction internal fixation, and lateral collateral ligament repair
A terrible triad of the elbow includes dislocation of the elbow with associated fractures of the radial head and the coronoid process. Ring et al. stressed that these injuries are prone to complications and advised against resection of the radial head due to instability, and instead recommended a radial head replacement if too comminuted for ORIF. Coronoid fractures compromise elbow stability as well and require open reduction and internal fixation as with the lateral collateral ligament. McKee et al. showed stable elbows in 34/36 with mean Mayo elbow score of 88 when the standard protocol of coronoid ORIF, radial head repair/replacement, and LCL repair were employed.
The talocrural angle of an ankle mortise x-ray is formed between a line perpendicular to the tibial plafond and a line drawn:
perpendicular to the medial clear space
parallel to the talar body
between the tips of the malleoli
perpendicular to the shaft of the fibular
parallel to the subtalar joint Correct answer: 3
The talocrural angle is formed by the intersection of a line perpendicular to the plafond with a line drawn between the malleoli (average = 83+/-4deg). When the lateral malleolus is shortened secondary to fracture, this can lead to increased talocrural angle. This malunion leads to lateral tilt of the talus.
Phillips et al looked at 138 patients with a closed grade-4 supination-external rotation or pronation-external rotation ankle fracture. Although the conclusions were limited due to poor follow up, they found the difference in the talocrural angle between the injured and normal sides was a statistically significant radiographic indicator of a good prognosis.
Pettrone et al looked at a series of 146 displaced ankle fractures, and the effect of open or closed treatment, and internal fixation of one or both malleoli. They found open reduction proved superior to closed reduction, and in bimalleolar fractures open reduction of both malleoli was better than fixing only the medial side.
Illustrations A and B are demonstrations of the talocrural angle.
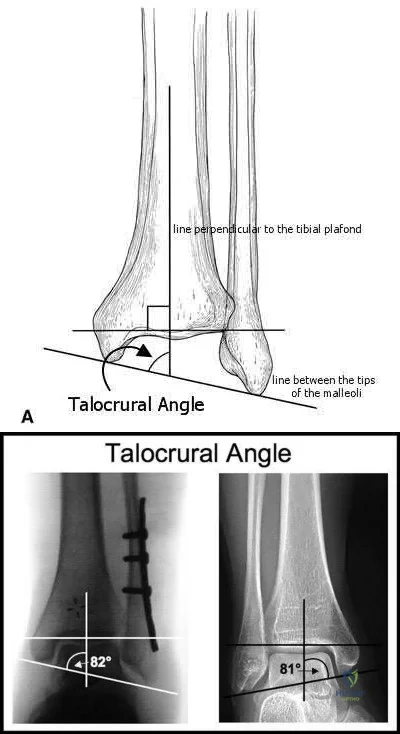
A 33-year-old male sustains the injury shown in Figure A. He is initially treated with a spanning external fixator followed by definitive open reduction internal fixation of the tibia and fibula. His wounds healed without infection or other complications. Two years following surgery, which of the following parameters will most likely predict a poor clinical outcome and inability to return to work?

Joint line restoration
Degree of fracture displacement
Time before definitive ORIF
Open fracture
Lower level of education Correct answer: 5
Lower level of education is the parameter that correlated most closely with a poor clinical outcome and inability to return to work.
To determine what fracture- and patient-specific variables affect outcome, Williams et al evaluated 29 patients with 32 tibial plafond fractures at a minimum of 2 years from the time of injury. Outcome was assessed by four independent measures: a radiographic arthrosis score, a subjective ankle score, the Short Form-36 (SF-36), and the patient’s ability to return to work. The four outcome measures did not correlate with each other. Radiographic arthrosis was predicted best by severity of injury and accuracy of reduction. However, these variables did not show any significant relationship to the clinical ankle score, the SF-36, or return to work. These outcome measures were more influenced by patient-specific socioeconomic factors. Higher ankle
scores were seen in patients with college degrees and lower scores were seen in patients with a work-related injury. The ability to return to work was affected by the patient’s level of education.
Pollak et al performed a retrospective cohort analysis of pilon fractures. Patient, injury, and treatment characteristics were recorded. The primary outcomes that were measured included general health, walking ability, limitation of range of motion, pain, and stair-climbing ability. A secondary outcome measure was employment status. Multivariate analyses revealed that presence of two or more comorbidities, being married, having an annual personal income of less than $25,000, not having attained a high-school diploma, and having been treated with external fixation with or without limited internal fixation were significantly related to poorer results as reflected by at least two of the five primary outcome measures.
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?
Irrigation and local wound care in the emergency department
Emergent irrigation and debridement in the operating room with vacuum-assisted wound closure
Emergent irrigation and debridement in the operating room with 7 days of intravenous antibiotics
Wound closure in the emergency department with follow-up wound check in 1 week
Exploration and removal of all bullet fragments in the emergency department and 10 day course of oral antibiotics
The question refers to appropriate management of a gunshot wound to the forearm. The first question that must be answered when evaluating gunshot injuries is whether the gunshot is low velocity or high velocity. Low-velocity wounds are less severe, are more common in the civilian population, and are typically attributed to bullets with muzzle velocities below 1,000 to 2,000 feet per second. Tissue damage is usually more substantial with higher-velocity (greater than 2,000 to 3,000 fps) military and hunting weapons. In this question, a muzzle velocity of 1,000 ft/sec is provided. Low velocity injuries with stable, non-operative fractures can be treated with local wound care.
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds.
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?
pulselessness
pallor
paresthesia
paralysis
increasing analgesia requirement Correct answer: 5
Although pain, pallor, paresthesia, paralysis, and pulselessness are all possible signs and symptoms of compartment syndrome in children with fractures, studies have shown increasing analgesia requirement is more sensitive.
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of
compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
A 45-year-old man sustains the injury seen in Figures A and B following a motor vehicle accident. Postoperative radiographs are seen in Figures C and D. Which of the following is the most accurate when comparing outcomes between intramedullary nailing (IMN) and open reduction internal fixation (ORIF) for this injury?

Union rates at one year are higher with ORIF
Infection rates are higher with IMN
Functional shoulder outcomes at one year are equivalent with IMN and ORIF
Iatrogenic radial nerve injury rate is higher with ORIF
Shoulder stiffness rates at one year are equivalent with IMN and ORIF Correct answer: 3
Although shoulder pain and stiffness is increased following IMN compared to ORIF, functional outcome scores at one year have been shown to be equivalent
in both treatment groups.
Diaphyseal humeral shaft fractures outcomes following IMN and ORIF are under further investigation. Diaphyseal humeral shaft fractures have historically been treated with ORIF, however proponents for IMN cite benefits of less periosteal stripping and soft tissue dissection. Recent investigations have shown outcomes with regard to nonunion, infection, re-operation, and nerve palsy appear equivalent between both groups. Rates of shoulder stiffness and shoulder pain have been demonstrated to be higher in IMN compared to ORIF. American Shoulder and Elbow Scores (ASES) have shown no difference at one year post-operatively.
Bhandari et al. performed a meta-anaylsis of 3 prospective randomized trials. They found lower rates of re-operation and shoulder impingement with ORIF of humeral shaft fractures.
Wali et al. performed a prospective randomized study of IMN or ORIF on 50 patients with mid-diaphyseal humeral shaft fractures. They found IMN had shorter operative time, shorter hospital stay, and lower blood loss. They found no difference in union rates, complication, or shoulder functional outcomes scores. They conclude IMN to be an effective option for treating mid-diaphyseal humeral shaft fractures.
Heineman et al. have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF. The authors found no significant difference between the two treatment modalities for the secondary outcomes (nonunion, infection, nerve palsy, re-operation).
Figures A and B show a diaphyseal humeral shaft fracture. Figure C and D show postoperative radiographs following intramedullary nailing of a humeral shaft fracture.
Incorrect Answers:
A 25-year-old female presents complaining of progressive anteromedial pain in her left ankle. She underwent operative fixation 5 months prior at an outside hospital. The operative report indicated that, due to anterior fracture blisters, a direct medial incision was utilized, centered over the posterior colliculus of the medial malleolus, without violation of the deltoid ligament. A radiograph and computed tomographic scan of her initial injury are shown in Figures A and B, respectively. On exam, she has well-healed incisions, exhibits no tenderness to palpation over her hardware, but does endorse pain with deep palpation along the anteromedial joint line. Figure C shows an anteroposterior left ankle radiograph taken today. Labs are obtained and reveal a white blood cell count of 9.0 k/uL (reference range 4.5-11.0 k/uL) and a C-reactive protein value of 0.8 mg/dL (<0.9 mg/dL). What is the next best step in managing her problem?

Syndesmotic fixation
Intra-articular corticosteroid injection
Referral to physical therapy
Surgical correction of malunion
Removal of hardware Correct answer: 4
This patient sustained a supination-adduction (SAD) injury with a vertical shear fracture of her medial malleolus and a fibular avulsion fracture. She sustained a medial plafond articular impaction injury that was not addressed at the time of surgery.
In SAD injuries, supination of the foot is combined with inward rotation at the ankle, adduction of the hindfoot, and inversion of the forefoot. This results in the following sequence of events: 1. Talofibular sprain or distal fibular avulsion (equivalent to Weber A). 2. Vertical medial malleolus fracture as the talus strikes the tibia. Associated injuries may include osteochondral damage to the talus and marginal impaction of the medial plafond. It is important to evaluate the medial plafond for articular impaction. When present, an arthrotomy must be performed, typically utilizing an anteromedial incision, with direct visualization of the articular surface to restore the joint line appropriately.
Weber et al. provided a review article on corrective osteotomies for malleolar fracture malunions. They stress that malunions can lead to ankle instability, abnormal load transfer, and post-traumatic arthritis. They conclude that corrective osteotomies that restore anatomical alignment show good results in long-term follow-up.
Perera et al. provided additional commentary on the surgical reconstruction of malunited ankle fractures. The authors emphasize the link between malunion and poor outcomes. They state that successful salvage procedures involve a clear understanding of the deformity, careful preoperative planning, and a solid understanding of reconstructive techniques. They provide several instructive case examples in their review.
McConnell et al. provided a discussion on SAD ankle fractures at their institution and emphasized the importance of recognizing marginal impaction of the tibial plafond when treating these injuries. Of 800 ankle fractures identified over a 5-year period, 44 were SAD injuries, 19 of the 44 displayed a vertical shear fracture of the medial malleolus, and 8 of the 19 demonstrated marginal impaction of the tibial plafond. These 8 impaction injuries were treated with open reduction internal fixation with elevation of the articular impaction; all had good to excellent outcomes without arthritic changes at last
follow-up.
Figure A is an anteroposterior left ankle radiograph demonstrating a SAD injury with a vertical shear fracture of the medial malleolus, a fibular avulsion fracture, and articular impaction of the medial tibial plafond. Figure B is a coronal CT demonstrating articular impaction of the medial plafond. Illustration A is an intra-operative photograph with the medial malleolus retracted allowing inspection of the articular surface; mild anteromedial plafond impaction is present.
Incorrect Answers:

A 90-year-old female slips and falls at home. She is a community ambulator and has no medical problems. She reports right hip pain at this time. Injury radiographs are shown in Figures A & B. Delay of more than 48 hours may result in:

Increased intraoperative time
Increased 30-day mortality
No impact on the rate of postoperative pneumonia
Higher rates of blood transfusion
Increased risk of post-operative infection Correct answer: 2
Figures A & B demonstrate a right, unstable intertrochanteric femur fracture. Surgical stabilization within 48 hours improves short-term and 30-day mortality.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:

A 22-year-old healthy left hand dominant male presents to the ED with left shoulder pain after falling from an ATV. Figure A is the radiograph of his left clavicle. He is neurovascularly intact and there is no evidence of skin tenting or open fracture. Which of the following most predisposes this patient to nonunion?

Diaphyseal fracture
Fracture displacement
Age
Male Gender
Injury involving the dominant extremity Correct answer: 2
Displaced clavicle fractures are associated with higher rates of nonunion.
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
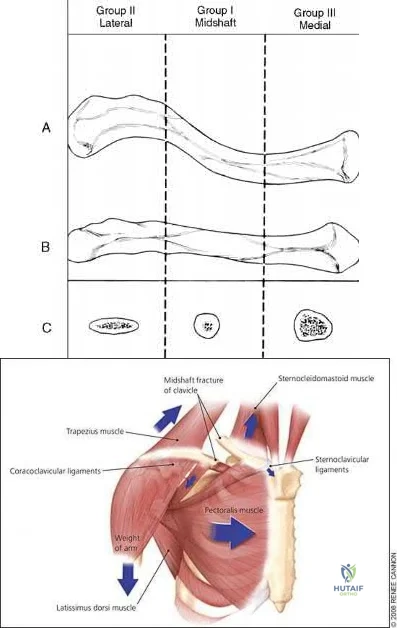
A 24-year-old male presents with ankle pain after being involved in a motor vehicle accident. His injury radiograph is shown in Figure A. Which of the following has been shown to contribute to the development of post-traumatic arthritis in this injury pattern?

Initial superficial zone cartilage cell death via apoptosis at the fracture margins
Initial superficial zone cartilage cell death via apoptosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis at the fracture margins
Delayed superficial zone cartilage cell death via necrosis at the fracture margins
Figure A demonstrates a tibial plafond fracture. Initial superficial zone cartilage cell death via necrosis at the fracture margins has been shown to contribute to post-traumatic arthritis.
Post-traumatic osteoarthritis typically occurs after an intra-articular fracture. Impacted chondrocytes die by either necrosis or apoptosis, which have both been implicated in post-traumatic osteoarthritis. Initial cell death in the superficial cartilage zones at the fracture margins occurs by necrosis. Apoptosis occurs in a delayed fashion and is mitigated by several bioactive agents.
Apoptosis also affects the superficial cartilage zones near the fracture margins. Deep cartilaginous zones and areas away from the fracture margins do not seem to be involved in these processes.
McKinley et al. performed a review of the basic science of intra-articular fractures and posttraumatic osteoarthritis. They report that initial damage to the cartilage in combination with the ensuing pathomechanical and pathobiologic response of the cartilage after a fracture contribute to posttraumatic arthritis. Chronic abnormal joint loading is also thought to contribute to this process as well. They conclude that the relative contribution of each is unknown.
Tochigi et al. performed a study to determine the distribution and progression of chondrocyte damage after intra-articular ankle fractures. They harvested 7 normal human ankles and subjected them to impaction. They found that immediate superficial zone chondrocyte death was greater in fracture-edge regions than on-fracture regions. Subsequent cell death over the next 48 hours was significantly higher in fracture-edge regions as well. They conclude that cartilage damage in intra-articular fractures was characterized by chondrocyte death at fracture margins.
Figure A is an ankle mortise radiograph demonstrating an intra-articular tibial plafond fracture.
Incorrect Answers:
A 35-year-old male presents with left knee pain after sustaining the injury seen in Figure A. He is neurovascularly intact and can perform a straight leg raise, but has pain with passive range of motion. Figures B and C show an anteroposterior and lateral radiograph of the left knee, respectively. 175 cc of saline is injected into the superolateral quadrant with no egress of fluid from the inferolateral
laceration. What percentage of traumatic arthrotomies would be detected with this test?

Question 91
1 and 2 demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 92
The MRI scans and diagnostic ultrasound shown in Figures 2a through 2c show what pathologic condition? Review Topic
Explanation
Question 93
Plate fixation without bone grafting
Explanation
Which of the following stress fractures most often requires internal fixation:
Question 94
Figures 62a and 62b show the radiographs of a 50-year-old man who has a long-standing history of wrist pain. What is the most likely cause of pain?
Explanation
Question 95
A 65-year-old woman undergoes a lumbar laminectomy for spinal stenosis at the L3-L4 level. The surgery and postsurgical course are uncomplicated. Eight weeks after surgery she has severe left anterior thigh, groin, and knee pain with ambulation and standing. Which condition is the most likely cause of her symptoms?
Explanation
Disorders of the hip can mimic and/or coexist with lumbar spine disorders. The prevalence of hip pain lasting longer than 1 month in patients ages 65 to 74 years is 19%. There is often overlap between their respective signs and symptoms. In a patient with failed back surgery syndrome, hip pathology may have been present before back surgery and not recognized. Osteoarthritis of
the hip typically causes groin and anterior thigh pain. Meralgia paraesthetica is more likely to manifest immediately after surgery. Trochanteric bursitis usually affects the proximal lateral thigh and often can radiate to the distal thigh. Facet joint pain causes low-back pain that can be referred to the gluteal region. Epidural hematoma 6 weeks after surgery is highly unlikely.
RECOMMENDED READINGS
Bolt PM, Wahl MM, Schofferman J: The roles of the hip, spine, sacroiliac joint, and other structures in patients with persistent pain after back surgery. Seminars in Spine surgery 2008;20:14-19.
Brown MD, Gomez-Marin O, Brookfield KF, Li PS. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res. 2004 Feb;(419):280-4. PubMed PMID: 15021166. View Abstract at PubMed
Question 96
A 55-year-old active left-hand-dominant woman sustains a minimally displaced (less than 2 mm displaced) left proximal humerus fracture that involves fractures of the greater tuberosity and surgical neck. Her activities include tennis and golf. What is the best treatment for this patient?
Explanation
Literature guiding indications for surgical vs nonsurgical treatment of proximal humerus fractures is not definitive. Many of the recommendations are based on older, nonrandomized series. Newer data suggest that surgical and nonsurgical treatment provide comparable results. Although surgical treatment is preferred for treatment of displaced fractures, fractures with minimal displacement are best managed without surgery.
RECOMMENDED READINGS
Hauschild O, Konrad G, Audige L, de Boer P, Lambert SM, Hertel R, Südkamp NP. Operative versus non-operative treatment for two-part surgical neck fractures of the proximal humerus. Arch Orthop Trauma Surg. 2013 Oct;133(10):1385-93. doi:10.1007/s00402-013-1798-2. Epub 2013 Jul 3. PubMed PMID: 23820852.View Abstract at PubMed
Bell J-R, Cadel ER. Shoulder trauma: Bone. In: Cannada LK, ed. Orthopaedic Knowledge Update 11. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2014:319-337.
Question 97
A 52-year-old man has had groin and deep buttock pain for the past 2 months. Examination reveals that hip range of motion is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 28. Management should consist of
Explanation
REFERENCES: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Urbanski SR, de Lange EE, Eschenroeder HC Jr: Magnetic resonance imaging of transient osteoporosis of the hip:. A case report. J Bone Joint Surg Am 1991;73:451-455.
Question 98
5cm. Recent radiographs are seen in Figures A and B. What is the most appropriate treatment plan?

Explanation
Subtrochanteric fractures can be treated with cephalomedullary nailing or fixed angle plates. Nailing of these fractures is technically challenging because the fracture must be reduced prior to nail passage. Failure to do so leads to varus and procurvatum malreduction.
Bellabarba et al. reviewed plating of femoral nonunions after intramedullary nailing. Of 23 nonunions, 21 healed at an average of 12 weeks. The remaining 2 cases required repeat plating (at 2 and 8 weeks) for hardware breakage because of noncompliance with weightbearing restrictions. They advocate plating because it allows for correction of malalignment and provides a biomechanically superior tension band construct.
Incorrect Answers:
OrthoCash 2020
A 38-year-old male was struck by a truck and sustained the injury seen in figure A. Treating this injury with an intramedullary nail with a larger radius of curvature can lead to what complication?

Posterior perforation of the distal femur
Varus malreduction
Comminution of the fracture site
Iatrogenic femoral neck fracture
Anterior perforation of the distal femur Corrent answer: 5
According to the study by Egol et al, the average femoral anterior radius of curvature was 120 cm (+/- 36 cm), and currently available femoral nails have a greater radius of curvature (i.e. more straight). This mismatch has been shown to lead to an increased risk of perforation of the anterior distal femur as the nail is impacted into the canal.
The referenced study by Tencer et al noted an increased risk of iatrogenic femoral fracture with anterior starting point >6mm from the anatomic axis.
They recommend starting in line with the femoral axis, or just a few millimeters anterior in order to minimize this risk.
Illustration A depicts anterior femoral cortex penetration secondary to nail/femur radius of curvature mismatch.

OrthoCash 2020
A 60-year-old woman is undergoing closed reduction and percutaneous pinning of a proximal humerus fracture. What structure is at greatest risk for injury from the pin marked by the red arrow in Figure A?
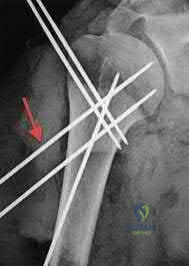
Anterior branch of the axillary nerve
Posterior humeral circumflex artery
Long head of the biceps tendon
Cephalic vein
Musculocutaneous nerve
Certain anatomic structures are at risk with percutaneous pinning of proximal humerus fractures. The red arrow in Figure A marks a proximal lateral pin that would place the anterior branch of the axillary nerve at risk.
Rowles and McGrory performed an anatomic study of the structures at risk with closed reduction and percuatneous pinning of the proximal humerus and found that proximal lateral pins were a mean of 3mm from the anterior branch of the axillary nerve. Pins placed through the anterior cortex and directed into the humeral head fragment were a mean of 2mm from the long head of the biceps tendon and greater tuberosity pins were found to be 8mm from the posterior humeral circumflex and 10mm from the main trunk of the axillary nerve as they penetrated the medial cortex of the humerus.
Jaberg et al retrospectively reviewed the clinical and radiographic results of 48 patients at an average of 3 years after undergoing closed reduction and percutaneous pinning of a proximal humerus fracture. 70% good to excellent results with their described technique, and the authors caution that radiographic malunion did not correlate with patient function.
Incorrect Answers
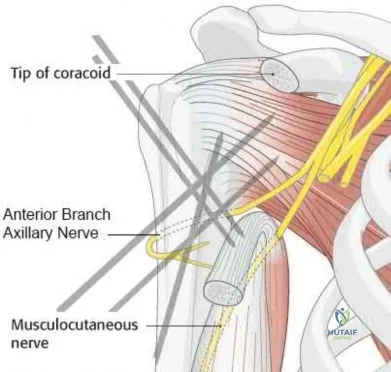
OrthoCash 2020
A 42-year-old female sustains the injury seen in the computed tomography images seen in Figures A and B. According to the Letournel classification, what is the injury pattern shown?

Posterior wall
Transverse
Anterior wall
Posterior column
Both column
The axial CT cut and Judet radiographic view shown reveals a transverse fracture pattern according to the Letournel classification system. This can be determined by the fact that the articular surface of the acetabulum is attached to the intact portion of the ilium, which is connected to the axial skeleton posteriorly through the sacroiliac joint. This differs from a both-column fracture, in which the articular surface of the acetabulum has no attachments to the axial skeleton due to fracture line(s). The axial CT scan also shows a vertical fracture line which is typical of a transverse fracture pattern.
Durkee et al review the classification schemes for these injuries, as well as comment on the importance of quality images (Judet views, CT, etc).
Figures A and B show a transverse acetabular fracture with mild displacement.
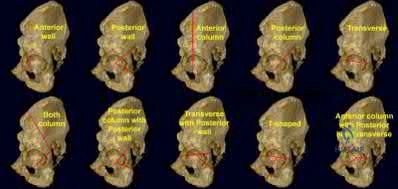
OrthoCash 2020
Which of the following is true regarding plating of humeral shaft fractures compared to intramedullary nailing?
worse functional results
higher need for subsequent surgeries
higher incidence of radial nerve injury
lower complication rates
decreased nonunion rates Corrent answer: 4
Controversy exists regarding nailing compared with plating of humeral shaft fractures, but the most recent and highest level evidence indicates decreased complication rates with open reduction and internal fixation of these injuries.
Lin et al found less blood loss with intramedullary nailing than plating, but nailing was also associated with increased shoulder surgery, likely due to disruption of the rotator cuff tendon during insertion.
Meekers et al found a higher union rate, better functional results and a lower reoperation rate after plate and screw fixation versus nailing. They concluded that plating was superior in most cases of humeral shaft fracture, however more recent studies have challenged these findings.
Heineman et al. (2012) have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF. The authors found no significant difference between the two treatment modalities for the secondary outcomes (nonunion, infection, nerve palsy, re-operation)
Incorrect Answers:
OrthoCash 2020
A 35-year-old male sustains the fracture seen in Figures A and B. Which of the following substances has been shown to result in the least radiographic subsidence when combined with open reduction and internal fixation?

Cancellous allograft bone chips
Autograft iliac crest
Femoral intramedullary reamings
Calcium phosphate cement
Calcium sulfate cement Corrent answer: 4
Figures A and B show a plateau fracture with a lateral split and depression of the articular surface. In treating tibial plateau fractures, calcium phosphate has been shown to have the least amount of articular subsidence on follow-up examinations due to its high compressive strength.
The study by Lobenhoffer et al noted improved radiographic outcomes and earlier weightbearing with usage of calcium phosphate cement. Welch and Zhang reproduced tibial plateau fractures in goats and compared cancellous autograft to calcium phosphate cement augmentation. At 24 hours, four of five specimens treated with autograft had subsidence of the fragment. Only two specimens from limbs treated with cement showed minimal subsidence; the remaining were congruent.
Yetkinler’s study compared cement to no cement treatment in a model of depressed plateau fractures. Calcium phosphate cement of high compressive
strength provided equivalent or better stability than conventional open reduction
and internal fixation with either auto/allograft bone which had both a lower compressive strength and reduced mechanical stability.
OrthoCash 2020
The modified Judet approach to the posterior scapula exploits the internervous interval between what two muscles?
Supraspinatus and infraspinatus
Supraspinatus and subscapularis
Infraspinatus and teres minor
Teres minor and teres major
Teres major and lattisimus Corrent answer: 3
The posterior or modified Judet approach to the scapula is typically used for internal fixation of scapular fractures. This approach utilizes a transverse incision over the scapular spine with detachment of the posterior deltoid. The interval between the infraspinatus (suprascapular n.) and teres minor (axillary n.) is identified and used to gain access to the posterior aspect of the scapula and glenoid.
The reference by Obremskey et al argues the approach "combines several important goals including: 1) exposure of all bony elements of the scapula which have adequate bone stock for internal fixation; 2) minimal trauma to the rotator cuff musculature; and 3) protection of the major neurologic structures (suprascapular nerve superiorly and axillary nerve laterally)." They believe "the main advantage of the exposure is limiting muscular dissection, which can potentially improve rehabilitation and limit morbidity of the operation."
OrthoCash 2020
An 82-year-old female sustains an intertrochanteric hip fracture and is treated with a sliding hip screw. What is the most appropriate definitive step in treating the failure seen in figure A?

Non-weight bearing
Valgus proximal femoral osteotomy
Total hip arthroplasty
Revision open reduction and internal fixation
Proximal femoral resection Corrent answer: 3
Figure A shows superior cutout of the lag screw from the sliding hip screw as well as the superior cannulated screw used for an "antirotation" device.
In the referenced review article by Haidukewych and Berry, salvage of failed treatment of hip fractures in the elderly is limited by bone quality and comorbidities. They recommend total hip arthroplasty in this instance to restore function, decrease pain, and limit periods of immobilization. They mention that the major challenges for arthroplasty are: assessing the need for acetabular resurfacing, selecting the femoral implant, and managing the greater trochanter.
OrthoCash 2020
A 13-year-old boy falls out of a tree and sustains the injury seen in Figures A and B. He is taken to the OR for fixation of his fracture.
The next morning, the patient’s blood pressure is 185/105 mm Hg and pulse rate is 130. He complains of pain that is not improved with opiates. On physical exam, the foot is firm. The decision is made to obtain compartment pressures to rule out compartment syndrome of the foot. Which of the following paths in Figure C marks the
appropriate location to measure the central compartment, and what would be considered abnormal values?

Path A, absolute value of 30-45 mmHg or delta p > 30mmHg
Path B, absolute value of 30-45 mmHg or delta p > 30mmHg
Path B, absolute value of 30-45 mmHg or delta p < 30mmHg
Path C, absolute value of 30-45 mmHg or delta p > 30mmHg
Path C, absolute value of 30-45 mmHg or delta p < 30mmHg Corrent answer: 3
The correct approach to measure pressures in the central compartment of the foot is by directing the needle lateral and plantar through the abductor hallicus, just under the base of the first metatarsal. Abnormal values indicating the need for decompression are an absolute value of 30-45 mmHg or a Δp < 30mmHg (the difference between the patient's diastolic blood pressure and compartment pressures).
The most common symptom of compartment syndrome in the extremities is intense pain. However, compartment syndrome can be difficult to diagnose in children and patients who are comatose, nonverbal, and/or mentally compromised because they may not be able to properly express their level of pain. Additionally, in compartment syndrome of the foot, pain on passive extension of the toes may or may not be present, and swelling and absence of the dorsalis pedis pulse may be expected findings with extensive trauma to the foot, making the clinical diagnosis even more difficult. Thus, for patients with equivocal findings on physical exam, foot compartment pressures should be measured in order to confirm the diagnosis. There are 8 compartments in the foot: lateral, medial, central, and 4 interosseous. The lateral compartment
contains the abductor digiti minimi and flexor digiti minimi brevis, and is measured by directing the needle 1cm medial and plantar under the midshaft of the 5th metatarsal. The medial compartment contains the abductor hallicus and flexor hallicus brevis, and is measured by directing the needle lateral and plantar under the base of the first metatarsal. The central compartment contains the oblique head of the adductor hallucis, and is measured through the same approach as the medial compartment after advancing the needle more deeply. The 4 interosseous compartments entail the 2nd, 3rd, and 4th web spaces, and can be measured by directing the needle plantar into each respective dorsal webspace.
Ojika et al. performed a systematic review on foot compartment syndrome. They found that the most common cause of foot compartment syndrome was crush injury to the foot, and that diagnosis was mostly made through a combination of clinical findings and compartment pressure measurements.
Badhe et al. reported 4 cases where competent sensate patients developed compartment syndromes without any significant pain. They found that pain is not a reliable clinical indicator for underlying compartment syndrome, so in a competent sensate patient, the absence of pain does not exclude compartment syndrome. They concluded that a high index of clinical suspicion must prevail in association with either continuous compartment pressure monitoring or frequent repeated documented clinical examination with a low threshold for pressure measurement.
Flynn et al. looked at the diagnosis and outcome of acute traumatic compartment syndrome of the leg in children. They found that a delay in diagnosis may occur because acute traumatic compartment syndrome manifests itself more slowly in children or because the diagnosis is harder to establish in this age group. They state that the results of the present study should raise awareness of late presentation and the importance of vigilance for developing compartment syndrome in the early days after injury.
Figures A and B are lateral and Harris radiographs of the foot demonstrating a calcaneus fracture. Figure C is a cross-sectional image of the foot. Illustration A is an image depicting the compartments of the foot.
Incorrect Answers:
compartment. Additionally, a Δp < 30mmHg (not > 30mmHg) is considered abnormal.
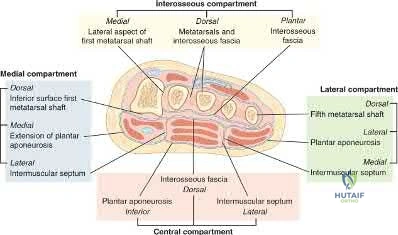
OrthoCash 2020
A 35-year-old female presents to the emergency room after a motor vehicle collision where her leg was pinned under the car for over 30 minutes. A clinical photo and radiographs are shown. Which of the following is the most accurate way to diagnose compartment syndrome?

surgeon's palpation of the leg compartments
paresthesias in her foot
diastolic blood pressure minus intra-compartmental pressure is less than 30 mmHg
diastolic blood pressure minus intra-compartmental pressure is greater than 30 mmHg
intra-compartmental pressure measurement of 25 mmHg Corrent answer: 3
The clinical picture is consistent with compartment syndrome. The most accurate way to make the diagnosis is to measure the difference between the diastolic blood pressure and intracompartmental pressure (delta p).
In a prospective study of 116 patients with tibial diaphyseal fractures, McQueen et al found that the use of a differential pressure of 30 mmHg as a threshold for fasciotomy led to no missed cases of acute compartment syndrome. They recommended that a fasciotomy should be performed if the differential pressure level drops to under 30 mmHg.
The cited study by Kakar et al found the intraoperative DBP is significantly lower than the preoperative DBP in patient undergoing IM nailing for tibia shaft
fractures. Therefore, they emphasize that the surgeon should recognize that intraoperative DeltaP may be lower than DeltaP once the patient is awakened in deciding whether to perform a fasciotomy versus awaken the patient and perform serial examinations and or compartment pressure measurements.
An absolute intra-compartmental value greater than 30 to 45mmHg can also be used to make the diagnosis of compartment syndrome, but is more controversial than the delta p according to Kakar and Amendola.
OrthoCash 2020
What is the most common mode of failure of the lateral ulnar collateral ligament associated with an elbow dislocation?
ligament avulsion off the humeral origin
ligament avulsion off the ulnar insertion
midsubstance rupture
bony avulsion of the humeral origin
combined proximal and distal ligament avulsions Corrent answer: 1
The lateral ulnar collateral ligament (LUCL) is often injured with elbow dislocations, and is most commonly injured at the proximal origin.
McKee noted that in 62 consecutive operative elbow dislocations and fracture/dislocations, the LUCL was ruptured in all of the patients, proximally in 32, bony avulsion proximally in 5, midsubstance rupture in 18, ulnar detachment in 3, ulnar bony avulsion in only 1, and combined patterns in 3.
Pugh et al established a standard protocol to treat elbow fracture dislocations (terrible triad) which includes coronoid repair, radial head repair/replacement, LUCL repair, and MCL and/or external fixation as needed.
OrthoCash 2020
A 24-year-old male sustains the injury seen in Figure A after being thrown from a motorcycle at a high speed. Which of the following fixation methods has been shown to be the most stable fixation construct for this injury?

Posterior bridge plating and anterior ring external fixation
Percutaneous iliosacral screw and anterior ring external fixation
Percutaneous iliosacral screw and anterior ring internal fixation
Transiliac screw
Two percutaneous iliosacral screws Corrent answer: 3
Figure A shows an APC III injury, which is a rotationally and vertically unstable injury, with damage to the anterior ring, pelvic floor, and posterior ligamentous stabilizing structures.
The referenced study by Sagi et al found that biomechanically, a percutaneous iliosacral screw and anterior ring internal fixation was the most stable construct. In addition, he found no biomechanical support for addition of a second iliosacral screw.
OrthoCash 2020
A 33-year-old male patient presents with a comminuted open tibia fracture after involvement in a motor vehicle crash. He has a history of smoking but is otherwise healthy. He is given antibiotics, and taken immediately for irrigation and debridement, followed by an un-reamed stainless steel intramedullary nail. Due to bone loss there is a non-circumferential cortical defect measuring 12 mm at the fracture site. All of the following factors in this patient's history and presentation increase his risk for adverse outcome EXCEPT:
High-energy mechanism of injury
Use of un-reamed nail
Implant material
Fracture gap
History of smoking Corrent answer: 2
Of the factors listed only the use of an un-reamed intramedullary nail for an open tibia fracture has not been shown to increase the risk of adverse outcome or need for reoperation.
The treatment of open tibia fractures with intramedullary nailing can be complicated by many factors. High energy mechanism of injury, use of a stainless steel nail, residual fracture gap greater than 1 cm, and a history of smoking have all been shown to increase the risk of adverse outcome. The use of reamed and un-reamed nails for open tibia fractures have been studied, and no significant difference in outcome has been found.
Schemitsch et al. present data from a prospective randomized trial of tibia fractures treated with reamed or unreamed intrameduallry nails. They found no difference in risk of adverse outcome between reamed and un-reamed nails in open tibia fractures. They did, however, find an increased risk of adverse outcomes in high-energy mechanisms, use of stainless steel (versus titanium) rods, and a residual fracture gap of greater than 1 cm. They comment that their data did not show a significant increase in risk due to history of smoking, but cite other studies that have demonstrated such a relationship.
Bhandari et al. present data from a prospective randomized study of patients with tibia fractures randomized to reamed or un-reamed tibial nails. For closed fractures they found a lower rate of primary events (most commonly need for dynamization) in the reamed group. However, they found no difference in outcomes for either technique in open fractures.
Incorrect answers:
OrthoCash 2020
Following antegrade intramedullary nailing of a femoral shaft fracture, the complication shown in Figure A occurs. Which of the following errors most likely resulted in this complication?
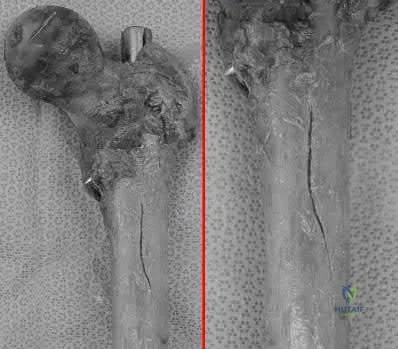
Applying external rotation torque on the proximal femur after placing proximal interlocking screws
Excessive interfragmentary compression of the fracture site prior to placing proximal interlocking screws
Using too anterior a starting point for a piriformis-entry point nail
Inserting a trochanteric-entry point nail through the piriformis fossa
Inserting a right femoral nail into the left femur Corrent answer: 3
Using a piriformis nail, a starting point that is too anterior will result in iatrogenic fracture ("bursting") of the proximal femur.
Antegrade nailing achieves fixation via 3-point fixation. In the sagittal plane, because of anterior sagittal bow, this is achieved at distal anterior cortex, middle posterior cortex (apex of curvature) and proximal anterior cortex. In the coronal plane, because of the lateral bow, this is achieved at the lateral distal femur, middle medial femur (apex of curvature), and proximal lateral femur (greater trochanter). Piriformis nails have a single sagittal bow.
Trochanteric nails are bowed in 2 planes, necessitating a twisting motion during insertion to negotiate both bows.
Papadakis et al. performed an experimental study on 18 cadaveric femora. Anterior bursting was found in 56% of nails placed too anteriorly. Bursting was not seen in nails placed through a more posterior entry point. They emphasize the location of the entry point when performing antegrade nailing.
Johnson et al. reviewed the biomechanical factors affecting fracture stability
and femoral bursting. They found that position of the starting hole was most important. Anterior displacement by >6mm led to high hoop stresses and bursting of the anterior cortex. This is important as an eccentrically reamed cortex may be difficult to recover from. They recommend either selecting a smaller diameter nail or overreaming by 1-2mm as a solution.
Figure A shows a fracture split of the proximal femur (left, without magnification; right, close-up). Illustration A shows anterior cortex pressures exceeding 100kPa for too-anterior entry points.
Incorrect Answers:
Wrong-side placement of a trochanteric entry nail would lead to varus malalignment at the fracture site, more so than placing a piriformis nail through the greater trochanter.
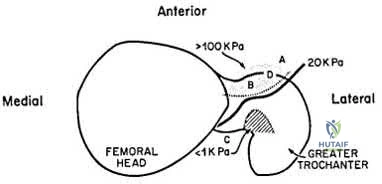
OrthoCash 2020
A 30-year-old male sustains a brachial plexus injury as the result of a motor vehicle collision. Palsy of which of the following muscles would not be expected with this injury if the injury was postganglionic in nature?
Rhomboid major
Extensor carpi radialis longus
Biceps brachii
Deltoid
Brachioradialis
A brachial plexus injury would involve all of the upper extremity muscles as well as most of the periscapular muscles. Complete plexus palsies are rare, and are often associated with scapulothoracic dissociation or other high-energy injuries.
Preganglionic injuries often involve the cervical paraspinal musculature as well as a complete plexus injury. EMG evidence of intact signals in the serratus anterior (long thoracic nerve) and rhomboids (dorsal scapular nerve) are suggestive of a postganglionic lesion/injury.
Tubbs et al. reported on the surgical anatomy of the dorsal scapular nerve in a cadaver study. They found that the nerve came off the C5 nerve root in 95%, ran 2.5cm medial to the spinal accessory nerve as it traveled on the anterior border of the trapezius muscle, and was intertwined with the dorsal scapular artery in all specimens.
Balakrishnan et al reported on the comparison of clinical exam and EMG in predicting site of lesions in brachial plexus injuries. The combination of EMG and exam localized the nerve injury in 80%, while the paraspinal EMG was the most sensitive solitary examination method (67%).
Illustration A shows a diagram of the brachial plexus. Incorrect Answers:
5: These muscles are all innervated by nerves that come from the brachial
plexus, and would be affected with a postganglionic injury.
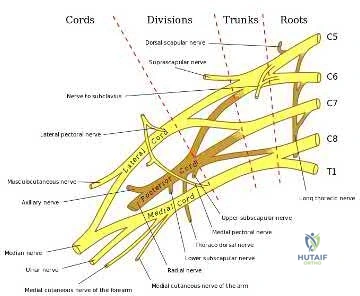
OrthoCash 2020
A 40-year-old male sustains a fall from a height. He sustains the isolated injury shown in the radiograph and CT images seen in Figures A through C. Surgery is planned. Which of the following constructs is the most appropriate definitive fixation for this injury?

Lateral locked plating
Medial bridge plating
Medial buttress plate
Medial lag screw with washers
External fixation
This patient has a medial tibial plateau fracture. Medial buttress plating (MBP) is indicated.
Medial tibial plateau fractures (Schatzker IV, Hohl and Moore II) may represent fracture dislocations of the knee. Neurovascular injuries must be excluded. In these instances, the medial fragment represents the stable fragment, and the rest of the tibia is the fractured fragment, with the entire leg acting as the lever arm.
Berkson et al. reviewed high energy tibial plateau fractures. Medial fractures may be treated with a medial plate or external fixation. Open reduction may be necessary because of fracture line obliquity and propensity of the medial plateau to shorten and rotate in the sagittal plane. Meniscal injuries should be repaired and avulsed cruciates fixed early. Collateral ligaments should be reconstructed after obtaining bone healing and range of motion.
Ratcliff et al. compared the stability of lateral locked plates and medial buttress plates in a cadaver model. They found that the medial buttress plate had greater fixation strength/failure force (4136N) compared with the lateral locking plate (2895N), although maximum cyclic displacement and residual displacement results were not different. They concluded that for vertically
orientated medial tibial plateau fractures, medial buttress plates were more stable.
Figure A is a radiograph showing a medial tibial plateau fracture extending across the tibial eminence. This is also classified as a Hohl and Moore Type II fracture. Figures B and C are coronal and axial CT scan images confirming the medial tibial plateau fracture and excluding a bicondylar fracture. Illustration A shows a medial tibial plateau fracture fixed with a medial buttress plate (cadaveric model with fibula removed). Illustration B shows the Hohl and Moore Type II fracture involving the entire condyle.
Incorrect Answers:
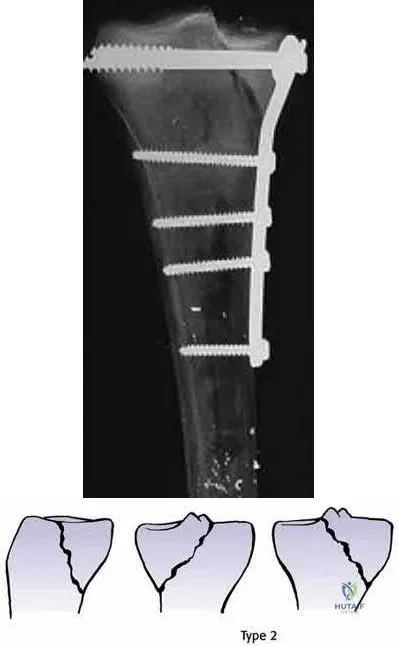
OrthoCash 2020
A 39-year-old female presents with the following motor vehicle crash with the injury seen in Figure A (immobilized in a pelvic binder). The iatrogenic neurologic injury most commonly caused by placement of the anterior construct for this injury, as shown in Figure B, would cause which of the following?
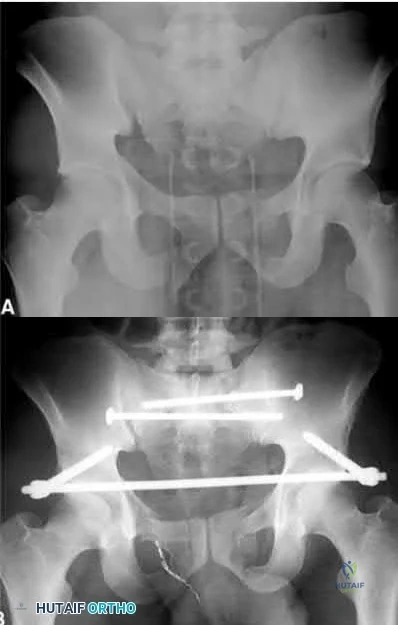
Weakness of hip flexion
Weakness of ankle dorsiflexion
Numbness of the medial thigh
Numbness of the lateral thigh
Numbness of the perineum Corrent answer: 4
This patient was treated with posterior stabilization, and an anterior subcutaneous internal fixator (ASIF). The most common neurologic injury seen following placement of the ASIF construct is irritation of the lateral femoral cutaneous nerve (LFCN), causing numbness and/or pain of the lateral thigh.
Unstable pelvic fractures can be treated in a multitude of ways. The ASIF construct is typically created by placing long pelvic screws or polyaxial pedicle screws in the supraacetabular region, similar to the supraacetabular pins for an
anterior external fixator. Then a curved bar is placed subcutaneously and connected to the supraacetabular screws. They are typically removed after 3-4 months when fracture healing is complete.
Vaidya et al. present a retrospective review of the use of ASIF as definitive treatment of unstable pelvic fractures. All patients in the study tolerated the construct well. LFCN irritation was seen in 30% of patients, and resolved in all but one patient.
Müller et al. present a retrospective review of the use of posterior stabilization and ASIF. They report an acceptably low complication rate, and good to excellent outcomes in 64.5% of patients.
Figure A is a radiograph demonstrating a right APC3 and left APC2 pelvic injury, imaged in a pelvic binder. Figure B is a postoperative radiograph following posterior stabilization and ASIF.
Incorrect answers:
OrthoCash 2020
What would be the most appropriate surgical indication for transferring fascicles of the ulnar nerve to the motor nerve of the biceps and fascicles of the median nerve to the motor nerve of the brachialis?
C8 - T1 nerve root avulsion 3 months ago
C5 - C6 nerve root avulsion 2 months ago
Upper brachial plexus palsy 22 months ago
Medial and posterior cord injury from gunshot wound 2 months ago
C6 ASIA A spinal cord injury Corrent answer: 2
Transfer of fascicles from (1) ulnar nerve to the nerve to the biceps and (2) median nerve to the motor nerve of the brachialis would be appropriate in the
treatment of an acute (<3-6 months) upper brachial plexus palsy.
Upper trunk injury (C5, C6) often results from the avulsion of both the C5 and C6 nerve roots. Injuries of this nature usually result from a downward force on the shoulder with lateral bending of the cervical spine in the opposite direction. This results in what is commonly called an Erb-Duchenne palsy. Patients often present with a flail shoulder and loss of elbow flexion. Other common treatments for C5 and C6 root avulsion include neurotization of the musculocutaneous (MSC) nerve by the spinal accessory (SA) or intercostal nerve, and neurotization of the supra-scapular nerve by the SA.
Liverneaux et al. looked at short term results of (1) ulnar nerve fascicle transfer to the nerve to the biceps and (2) fascicle of the median nerve to the motor branch to the brachialis in 15 patients with acute C5 - C6 nerve root avulsion injuries. Grade 4 elbow flexion was restored in each of the 10 patients. There was no secondary deficit in grip strength or sensation.They concluded that this double nerve transfer technique will likely reduce the need for secondary procedures to augment elbow flexion.
Teboul et al. reviewed thirty-two patients with an upper nerve-root brachial plexus injury that underwent ulnar nerve fascicle transfer to the nerve of biceps to restore elbow flexion. After the nerve transfer, twenty-four patients achieved grade 3 elbow flexion strength or better. They note that this procedure will spare the C5 nerve root and other nerves for grafting or transfer elsewhere.
Illustration A shows harvesting of an ulnar nerve fascicle for transfer. Illustration B shows transfer of the fascicle of the ulnar nerve to the motor nerve of the biceps.
Incorrect Answers:
sensory quadriplegia. Nerve transfers using the ulnar nerve (C8-T1) would also be redundant as this nerve would be non-functional in this patient.
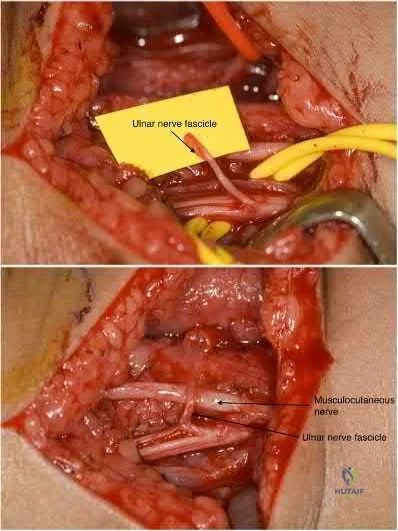
OrthoCash 2020
A 31-year-old female presents to the trauma bay following a motorcycle crash. Her blood pressure is 95/70 mmHg, heart rate is 115 bpm. Lactate measured in the trauma bay is 10 mmol/L. She has multiple rib fractures, pulmonary contusions, and a positive FAST exam requiring immediate exploratory laparotomy. After laparotomy her lacate remains unchanged. She has a closed right femur fracture and an open right tibia fracture as seen in Figures A and B. Besides antibiotics and thorough irrigation and debridement, which of the following would be an appropriate step in the immediate management of her fractures?

Reamed intramedullary nailing of the tibia and femur
Un-reamed intramedullary nailing of the tibia, and reamed intramedullary nailing of the femur
Reamed intramedullary nail of the tibia, and un-reamed intramedullary nail
of the femur
Posterior slab splint of the tibia, and 10 lbs skeletal traction of the femur
External fixation of the tibia and femur Corrent answer: 5
This patient is suffering from multiple injuries and has evidence of chest injury and incomplete resuscitation. The immediate treatment of her fractures should be external fixation for both the tibia and the femur.
For polytraumatized patients with multiple injuries including extremity fractures, damage control orthopaedics dictates that long bone fractures should be temporarily stabilized. Either inadequate stabilization, or early total care, such as a reamed or unreamed nails, can exacerbate the patient's condition and increase the risk of a second-hit phenomenon. For this patient with pulmonary contusions and continued elevation of lactate indicating end-organ hypoperfusion her extremities should have staged treatment according to damage control principles.
Morshed et al. present a retrospective review of polytraumatized patients with femur fractures and compared outcomes based on the time frame in which their fractures were definitively treated. They found delaying treatment at least 12 hours to allow appropriate resuscitation and treatment of other traumatic injuries led to a decrease in mortality of 50%. Patients with intra-abdominal injuries benefited most from staged treatment of the extremities.
Figure A is a radiograph showing a closed right femur fracture. Figure B is a radiograph of an open right tibia fracture.
Incorrect answers:
OrthoCash 2020
A 68-year-old woman undergoes a hemiarthroplasty for a proximal humerus fracture through a deltopectoral approach. What
range of motion exercise should not be utilized in the immediate postoperative period due to concerns about lesser tuberosity fixation?
Pendulums
Passive internal rotation of the shoulder to the plane of the body
Active forearm supination
Passive external rotation of the shoulder past 30 degrees
Passive forward flexin of the shoulder to 90 degrees Corrent answer: 4
Frankle et al found that passive external rotation of the shoulder placed the most stress on the lesser tuberosity fixation. The subscapularis tendon inserts on the lesser tuberosity and is the deforming force when placed under tension during external rotation. They also found that non-anatomic tuberosity reduction of 4-part proximal humerus fractures treated with hemiarthroplasty increased torque and impaired external rotation kinematics.
OrthoCash 2020
A 72-year-old female sustains a displaced intracapsular femoral neck fracture. Which of the following is TRUE regarding the long term differences between possible treatment options for this injury?
Patients undergoing total hip arthroplasty are more likely to experience persistent pain than those undergoing internal fixation
Patients undergoing total hip arthroplasty are less likely to require reoperation than those undergoing internal fixation
There is no difference in functional outcome scores between internal fixation and total hip arthroplasty
Patients undergoing internal fixation perform activities of daily living better than those undergoing total hip arthroplasty
Mortality rates are higher following total hip arthroplasty than internal fixation
Elderly patients with femoral neck fractures (FNF) undergoing total hip arthroplasty (THA) are less likely to require reoperation than those undergoing internal fixation.
Intracapsular FNF are common in elderly patients after a fall from standing height. Treatment depends on physiological age and displacement (Garden's classification). For displaced fractures, physiologically young patients are treated with internal fixation while physiologically old patients are treated with
either hemiarthroplasty (debilitated, less active patients) or THA (more active patients, those with acetabular disease or preexisting inflammatory arthritis).
Chammout et al. retrospectively compared the long term (17 years) results of THA (cemented both component) and ORIF (2 cannulated screws) in elderly patients (>65 years). They found no difference in mortality. But hip scores were higher and pain was better in the THA group, while reoperation rates were higher in the ORIF group. Walking speed was initially faster in the THA group, but later did not differ between groups. They recommend THA for elderly patients with displaced FNF.
Rogmark et al. prospectively compared closed reduction and internal fixation (CRIF) with arthroplasty (combining hemiarthroplasty and THA) at 2 years in elderly patients (>70 years). Failure rates were higher, pain was worse, and walking was more impaired after CRIF. They recommend arthroplasty for patients >70 with FNF.
Incorrect Answers:
OrthoCash 2020
A polytrauma patient underwent the following procedures: (1) statically locked intramedullary nailing for a right femoral shaft fracture; (2) open reduction with plate-and-screw fixation [ORIF] for a right simple distal fibula fracture; (3) ORIF right middle third radius and ulna fracture; and (4) ORIF left humeral shaft fracture. What is the appropriate weightbearing status for this patient?
Weight bearing as tolerated in all extremities
Early protected weight bearing right lower extremity in walking cast, weight bearing as tolerated left upper extremity, non-weight bearing right forearm
Weight bearing as tolerated in bilateral lower extremities and right upper extremity, non-weight bearing left upper extremity
Non-weight bearing bilateral upper extremities and right lower extremity
Non-weight bearing right upper and lower extremities, weight bearing as tolerated left upper and lower extremities without walking cast
The standard postoperative weightbearing for locked medullary nailing for femoral shaft fractures and humeral shaft fractures is weight bearing as tolerated (WBAT). Simple ORIF ankle fractures may be managed with early protected weight bearing. ORIF right middle third radius and ulna fracture should be managed with a period of non-weight bearing due to risk of secondary displacement of the fracture.
Tingstad et al. examined the effect of immediate weightbearing on plated fractures of the humeral shaft. They reported that immediate weightbearing on humeral shaft fractures, treated with plating and full weightbearing, did not have any negative effect on the union or malunion rates.
Brumback et al. evaluated the feasibility, safety and efficacy of immediate weightbearing after treatment of femoral shaft fractures with statically locked IM nail. Using biomechanical and clinical data, they showed that all fractures united with no loss of fixation or hardware failure.
Starkweather et al. retrospectively assessed the complications and loss of reduction in patients who bore weight in a short leg cast within 15 days after surgical repair of acute unilateral closed ankle fractures. Of the 81 ankle fracture radiographs, 80 (98.8%) showed no displacement in fracture reduction on the final follow-up examination. These results suggest early protected weightbearing may be safe.
Incorrect Answers:
OrthoCash 2020
A 22-year-old female falls off the back of a motorcycle and sustains the injury in Figure A. She is hemodynamically unstable and massive transfusion protocol is activated. What is the correct ratio of transfusion of packed red blood cells, platelets and plasma?

Question 99
You have been waiting to enroll a patient into your recent institutional review board (IRB)-approved clinical research protocol. A patient is admitted who, upon initial screening, meets all inclusion criteria. However, he has late-stage dementia, and you are told by your research coordinator that this condition is an exclusionary criterion. This scenario demonstrates the need for which aspect of proper informed consent?
Explanation
Question 100
Histologic studies of surgically resected tissue in lateral epicondylitis demonstrate which of the following findings? Review Topic
Explanation
