Orthopedic Board Review MCQs: Arthroplasty, Knee & Elbow Surgery | Part 253

Key Takeaway
This page offers Part 253 of a comprehensive Orthopedic Surgery Board Review series. Featuring 100 high-yield MCQs, it's designed for orthopedic residents and surgeons preparing for AAOS and ABOS board certification exams, mimicking the OITE/AAOS format. It includes interactive study and exam modes.
About This Board Review Set
This is Part 253 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 253
This module focuses heavily on: Arthroplasty, Deformity, Elbow, Infection, Knee, Revision.
Sample Questions from This Set
Sample Question 1: In either a ceramic-on-highly-cross-linked polyethylene (HXPE) or metal-on-HXPE component, increasing the ball head size leads to...
Sample Question 2: A 28-year-old woman undergoes a closing-wedge high tibial osteotomy (HTO) for medial compartmentoverload after medial meniscectomy. Postsurgically, she reports improvement in her medial pain and resumes normal activities. About 9 months aft...
Sample Question 3: Figures 36a and 36b show the radiographs of a 3-year old child who has a congenital upper extremity deformity. Which of the following features would be a major contraindication to a centralization procedure?...
Sample Question 4: A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had...
Sample Question 5: Figures 1a and 1b are the recent radiographs of an 82-year-old man with rheumatoid arthritis who underwent total knee arthroplasty (TKA) 18 years ago. These radiographs reveal osteolysis with loosening of the tibial component. Aspiration an...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
In either a ceramic-on-highly-cross-linked polyethylene (HXPE) or metal-on-HXPE component, increasing the ball head size leads to
Explanation
Increasing the size of the ball head increases the primary arc of motion prior to impingement and the jump distance prior to dislocation, assuming an acetabular component abduction of less than 90 degrees. Although HXPE has demonstrated decreases in linear wear rates even with ball head sizes larger than 28 mm, volumetric wear remains a concern. A larger ball head size does not significantly change offset, and larger metal ball heads are not associated with decreased risk for corrosion.
Question 2
A 28-year-old woman undergoes a closing-wedge high tibial osteotomy (HTO) for medial compartment overload after medial meniscectomy. Postsurgically, she reports improvement in her medial pain and resumes normal activities. About 9 months after her surgery, however, she reports burning pain in the front of her knee with running. Her examination reveals no joint line tenderness, mild pain with patellar compression, and limited patellar glides. What is the most likely cause of her symptoms?
Explanation
Question 3
Figures 36a and 36b show the radiographs of a 3-year old child who has a congenital upper extremity deformity. Which of the following features would be a major contraindication to a centralization procedure?
Explanation
REFERENCES: Green DP: Operative Hand Surgery, ed 2. New York, NY, Churchill Livingstone, 1988, pp 269-271.
Goldberg MJ, Meyn M: The radial clubhand. Orthop Clin North Am 1976;7:341-359.
Question 4
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had
Explanation
Question 5
Figures 1a and 1b are the recent radiographs of an 82-year-old man with rheumatoid arthritis who underwent total knee arthroplasty (TKA) 18 years ago. These radiographs reveal osteolysis with loosening of the tibial component. Aspiration and laboratory study findings for infection are negative. During the revision TKA, treatment of tibial bone loss should consist of
Explanation

Video 1 for reference
For severe tibial defects (Anderson Orthopaedic Research Institute [AORI] types 2 and 3), metaphyseal fixation is necessary to achieve construct fixation during revision TKA. Metaphyseal fixation may be achieved with cement, structural allograft, or conical metallic implants. The major concerns regarding structural allograft are graft resorption and mechanical failure and technical issues related to fashioning the graft and obtaining a good host-allograft interface. In a systematic review, porous metal cones were associated with a decreased loosening rate in AORI 2 and 3 defects compared to structural allografts. Metallic trabecular metal cones and metaphyseal porous coated sleeves provide a stable construct with which to support the tibial component during revision TKA. Clinical results with these devices include good metaphyseal fixation for severe tibial bone defects.
Question 6
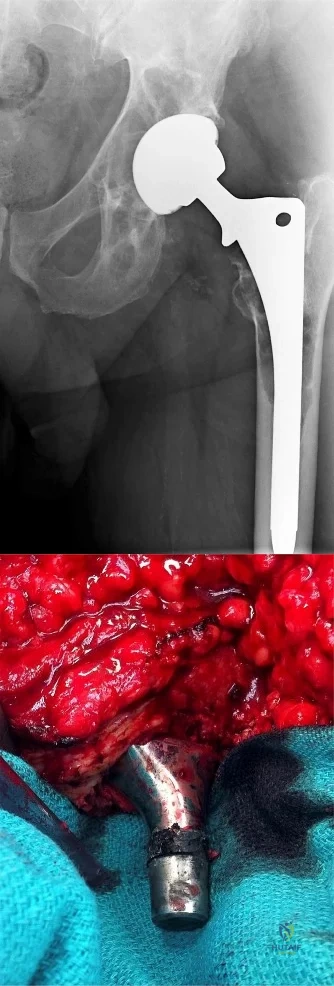
Total hip arthroplasty is most appropriate for the injury shown in Figure A for which of the following patients?

Explanation
Displaced femoral neck fractures can present a challenge to treat. In younger patients with good bone stock a closed vs. open reduction and internal fixation should be attempted. For active older patients a total hip arthroplasty is the best option, especially if there is pre-existing arthritis in the injured hip. THA provides the best function with the least pain and less need for repeat surgery (compared to hemiarthroplasty). For low-demand or debilitated patients, for patients older than age 80, or for those who can not reliably follow hip precautions a hemiarthroplasty provides the lowest risk of dislocation, and thus would be the treatment of choice.
Macaulay et al. present a prospective randomized trial of patients with femoral neck fractures treated with THA vs hemiarthroplasty. They found that functional outcomes and patient satisfaction were higher in the THA group without significant increased risk of complications. Inclusion criteria required patients to be over age 50, be a community ambulator, and were excluded for presence of dementia.
Abboud et al. retrospectively reviewed patients treated with THA for osteoarthritis and compared them to patients treated with THA for a femoral neck fracture. They found no significant difference between the two groups for outcomes or complications.
Figure A is an AP radiograph demonstrating a displaced femoral neck fracture.
Incorrect Answers:
Question 7
A 35-year-old man has numbness and tingling in the index, middle, and ring fingers. History reveals that he also has had vague wrist pain and stiffness since being injured in a motorcycle accident 1 year ago. Radiographs are shown in Figures 47a through 47c. Management should consist of
Explanation
REFERENCES: Rettig ME, Raskin KB: Long-term assessment of proximal row carpectomy for chronic perilunate dislocations. J Hand Surg Am 1999;24:1231-1236.
Howard FM, Dell PC: The unreduced carpal dislocation: A method of treatment. Clin Orthop 1986;202:112-116.
Question 8
- A 15-year-old girl has a thoracic kyphosis that causes mild pain. Examination reveals a sagittal curve measuring 55 degrees and wedging of the eighth through tenth vertebrae. The iliac apophyses are Risser 4. Management should include
Explanation
(2) with surgical fusion if >75o and Risser 3 or less, (3) with surgical fusion if >65o and Risser 4/5 if necessary or symptomatic. Posterior instrumentation, anterior release and interbody fusion is the treatment of choice for curves >75o, or those >55o on hyperextension. Other causes of kyphosis include trauma, infection, spondylitis, bone dysplasia, neoplasia, neurofibromatosis.
Question 9
As an orthopaedic surgery resident, you arrive late to a medial patellofemoral ligament reconstruction procedure in your institution's outpatient surgical center. It is standard practice in your residency program to miss the start of the first case because of didactic requirements on Tuesdays. The surgical team has your gown and gloves ready, and following scrubbing and gowning, you join the surgical team and assist the attending with the procedure. Which of the following represents a violation of standard surgical safety checklists?
Explanation
The World Health Organization and nearly every professional surgical subspecialty group advocates for safety checklists prior to operations. Although there are institutional variations to individual items on the checklists, it is important to include a system for marking the surgical site, verifying the patient's identity and procedure planned, identifying all team members in the room and agreement regarding the type of anesthesia, antibiotic prophylaxis, instrumentation used. Simply put, safety checklists have been shown to drastically reduce costly errors in other high-risk
industries, and they have been universally adopted by hospitals and surgery centers and the organizations that inspect and validate healthcare settings.
The Joint Commission Guidelines and the WHO surgical safety checklists are examples of governing bodies of healthcare implementing safety checklists in procedural settings.
Illustration A is the WHO surgical safety checklist. Incorrect Answers:
Question 10
-An absolute contraindication for closed management of a humeral shaft fracture in a fracture brace is
Explanation

Question 11
Six weeks after onset, what is the most clearly accepted indication for surgical management for lumbar disk herniation?
Explanation
REFERENCES: Rhee JM, Schaufele M, Abdu WA: Radiculopathy and the herniated lumbar disc: Controversies regarding pathophysiology and management. J Bone Joint Surg Am 2006;88:2070-2080.
Atlas SJ, Keller RB, Wu YA, et al: Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the Maine lumbar spine study. Spine 2005;30:927-935.
Question 12
An 8-year-old boy with severe hemophilia A (factor VIII) and no inhibitor is averaging eight transfusions per month for bleeding into the right ankle. Examination shows synovial hypertrophy; range of motion consists of 0° of dorsiflexion and 20° of plantar flexion. The patient’s knees, elbows, and left ankle have no restriction of motion. Standing radiographs of the right ankle are shown in Figure 18. Management should consist of
Explanation
REFERENCES: Greene WB: Synovectomy of the ankle for hemophilic arthropathy. J Bone Joint Surg Am 1994;76:812-819.
Greene WB: Chronic inflammatory arthridities and diseases related to the hematopoietic system, in Drennan JC (ed): The Child’s Foot and Ankle, New York, NY, Raven Press, 1992, pp 461-482.
Question 13
Figure 8 shows the CT scan of an 11-year-old boy who has had a 1-year history of worsening painful flatfeet. He reports pain associated with physical education at school, especially with running and jumping. Management consisting of activity restriction, anti-inflammatory drugs, and casting has failed to provide relief. Treatment should now consist of
Explanation
REFERENCES: Scranton PE Jr: Treatment of symptomatic talocalcaneal coalition. J Bone Joint Surg Am 1987;69:533-539.
Kitaoka HB, Wikenheiser MA, Schaughnessy WJ, et al: Gait abnormalities following resection of talocalcaneal coalition. J Bone Joint Surg Am 1997;79:369-374.
Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 14
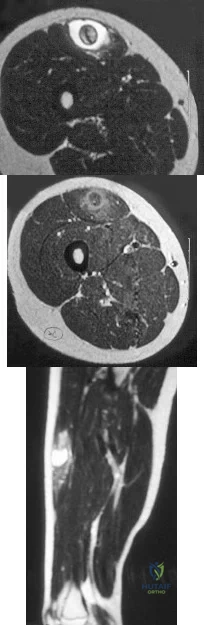
Figures 13a and 13b show the MRI scans of a 70-year-old patient who has a posterior calf mass. Examination reveals that the mass extends to the midcalf level. A biopsy specimen reveals a high-grade soft-tissue sarcoma. Metastatic work-up shows no lesions. Management should consist of
Explanation
REFERENCES: Lindberg RD, Martin RG, Romsdahl MM, et al: Conservative surgery and post-operative radiotherapy in 300 adults with soft tissue sarcoma. Cancer 1981;47:2391-2397.
Sim FT, Frassica FS, Frassica DA: Soft tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Rosenberg SA, Tepper J, Glatstein E, et al: The treatment of soft-tissue sarcomas of the extremities: Prospective randomized evaluations of (1) limb sparing surgery plus radiation therapy compared with amputation and (2) The roll of adjuvant chemotherapy. Am Surg 1982;196:305-315.
Question 15
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?
Explanation
REFERENCES: Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637.
Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Davis AM, Bell RS, Goodwin PJ: Prognostic factors in osteosarcoma: A critical review. J Clin Oncol 1994;12:423.
Question 16
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
REFERENCES: Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
D’Antonio J, Capello W, Manley M, et al: New experience with alumina-on-alumina ceramic bearings for total hip arthroplasty. J Arthroplasty 2002;17:390-397.
Question 17
- A 7-year old boy has a painless abductor limp and limited hip abduction. Radiographs show varus of the proximal femur, with a narrow upper femoral epiphysis that has the shape of an inverted "Y". Which of the following factors best predicts the risk that the deformity will become worse?
Explanation
Question 18
A 42-year-old female undergoes a subtalar bone block distraction arthrodesis as sequelae of a nonoperatively treated calcaneus fracture ten years prior. This procedure addresses which of the following issues?

Explanation
Question 19
A 7-year-old boy with spastic diplegia is a limited community ambulator. He has a moderately severe crouched gait. The parents request a treatment that will result in a permanent decrease in lower extremity muscle tone. This is best accomplished with
Explanation
REFERENCES: Arens LJ, Peacock WJ, Peter J: Selective posterior rhizotomy: A long-term follow-up study. Childs Nerv Syst 1989;5:148-152.
Koman LA, Paterson Smith B, Balkrishnan R: Spasticity associated with cerebral palsy in children: Guidelines for the use of botulinum-A toxin. Paediatr Drugs 2003;5:11-23.
Johnson MB, Goldstein L, Thomas SS, et al: Spinal deformity after selective dorsal rhizotomy in ambulator patients with cerebral palsy. J Pediatr Orthop 2004;24:529-536.
Question 20
In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
Explanation
REFERENCES: Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.
Papp SR, Athwal GS, Pichora DR: The rheumatoid wrist. J Am Acad Orthop Surg
2006;14:65-77.
Question 21
The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?
Explanation
REFERENCES: McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Lister GD, McGregor IA Jackson IT: The groin flap in hand injuries. Injury 1973;4:229.
Question 22
A 45-year-old woman has idiopathic scoliosis. Surgery is to include an anterior thoracic release through an open left thoracotomy. The thoracotomy will have what effect on the patient’s pulmonary function postoperatively?
Explanation
REFERENCES: Graham EJ, Lenke LG, Lowe TG, et al: Prospective pulmonary function evaluation following open thoracotomy for anterior spinal fusion in adolescent idiopathic scoliosis. Spine 2000;25:2319-2325.
Kishan S, Bastrom T, Betz RR, et al: Thoracoscopic scoliosis surgery affects pulmonary function less than thoracotomy at 2 years postsurgery. Spine 2007;32:453-458.
Question 23
A 25-year-old woman undergoes surgical treatment of a displaced proximal humeral fracture via a deltopectoral approach. At the first postoperative visit, she reports a tingling numbness along the anterolateral aspect of the forearm. What structure is most likely injured?
Explanation
REFERENCES: McIlveen SJ, Duralde XA, D’Alessandro DF, et al: Isolated nerve injuries about the shoulder. Clin Orthop 1994;306:54-63.
Warner JP: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg
1997;5:130-140.
Question 24
ACL rehabilitation often includes exercises with the distal end of the extremity fixed in place with axial loading and co-contracture of muscle groups to help stabilize the joint. This type of exercise is more commonly referred to as: Review Topic
Explanation
Closed chain exercises are preferred for any rehabilitation protocol that wants to minimize stress across a potentially unstable joint. After ACL reconstruction it is important to begin motion and strengthening but not stress the reconstructed ligament which may lead to loss of stability or failure.
An example of a closed chain exercise of the quadriceps is a squat or leg press in which the foot is fixed against the floor/plate and both the quadriceps and hamstrings can contract together keeping the knee joint stable and preventing excess stress across the reconstructed ACL. An example of an open chain exercise of the quadriceps is a seated leg extension in which the foot is not fixed and the quadriceps contract in isolation. This creates a strong anterior pull on the tibia which can lead to excess stress on the ACL graft.
Beynnon et al. present a review on the behavior of ACL grafts during rehabilitation. They found that exercises that produce the least amount of stress across an ACL graft are either dominated by hamstring muscle contraction, involve quadriceps muscle activity with the knee flexed at 60° or greater, or involve active knee motion between
35°
and
90°
of
flexion.
Illustration A is an example of a squat, which is a closed chain exercise. Notice the feet are fixed in place against the floor. Illustration B is an example of a seated leg extension, which is an open chain exercise. Notice the feet are not fixed in place and no axial loading or co-contracture can occur.
Incorrect
Question 25
Figures 75a and 75b are the radiographs after attempted reduction of an injury in a 9-year-old girl. Which anatomic structure is most likely to be interposed?
Explanation
The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.

CLINICAL SITUATION FOR QUESTIONS 76 THROUGH 80
Figure 76 is the clinical photograph of an infant with foot deformities.
Question 26
Which of the following complications is associated with the use of a short cephalomedullary nail for fixation of intertrochanteric hip fractures?
Explanation
REFERENCES: Robinson CM, Adams CI, Craid M, et al: Implant-related fractures of the femur following hip fracture surgery. J Bone Joint Surg Am 2002;84:1116-1122.
Valverde JA, Alonso MG, Porro JG, et al: Use of the Gamma nail in the treatment of fractures of the proximal femur. Clin Orthop Relat Res 1998;350:55-61.
Question 27
The newborn foot deformity seen in Figures 64a and 64b should initially treated with Review Topic

Explanation
Question 28
-The fracture shown in Figure 82 is scheduled to be fixed with a retrograde nail. An arthrotomy should be performed during the procedure because it
Explanation

Question 29
A 20-year-old man sustained an injury to his arm during a tug-of-war contest. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Explanation
REFERENCES: Heckman JD, Levine MI: Traumatic closed transection of the biceps brachii in the military parachutist. J Bone Joint Surg Am 1978;60:369-372.
Mellen PF: Parachute static line injury with vascular compromise. Mil Med 1989;154:364-365.
Question 30
Reverse total shoulder arthroplasty improves kinematics in the rotator cuff deficient joint by what directional change to the center of rotation? Review Topic
Explanation
Question 31
A 15-year-old boy reports a 2-day history of progressive left buttock pain and severe limping. He denies any history of trauma or radiation of the pain. He has an oral temperature of 100.4 degrees F (38 degrees C). Examination reveals that the lumbar spine and left hip have unguarded motion. The abdomen is nontender. There is moderate tenderness of the left sacroiliac region with no palpable swelling. Pain is elicited when the left lower extremity is placed in the figure-4 position (FABER test). Laboratory studies show a peripheral WBC count of 11,500/mm P 3 P (normal to 10,500/mm P 3 P ) and an erythrocyte sedimentation rate of 38 mm/h (normal up to 20 mm/h). Radiographs of the pelvis, hips, and lumbar spine are normal. A nucleotide bone scan (posterior view) is shown in Figure 44. Initial management should consist of
Explanation
Tc 99m bone scan will localize the problem in 90% of patients but may occasionally give a
false-negative result in early cases. If suspicion is high, a gallium scan or MRI scan may help confirm the diagnosis of sacroiliitis. Needle aspiration of the sacroiliac joint is difficult; therefore, antibiotic selection is usually empiric or based on blood cultures. Sacroiliitis that is the result of connective tissue inflammatory disease is usually bilateral and without fever or leukocytosis. The lack of hip irritability, spinal rigidity, and abdominal tenderness helps to rule out other causes of limping with fever, such as psoas abscess, diskitis, and septic hip.
REFERENCES: Aprin H, Turen C: Pyogenic sacroiliitis in children. Clin Orthop
1993;287:98-106.
Osman AA, Govender S: Septic sacroiliitis. Clin Orthop 1995;313:214-219.
Question 32
When obtaining grafts from a trochlear donor site during an osteochondral autograft transplantation procedure, where on the trochlea are the lowest contact pressures found? Review Topic
Explanation
Question 33
A B C What is the appropriate first step when confirming the diagnosis of a neurologically intact, 73-year-old man who has the images shown in Figures 25a through 25c?
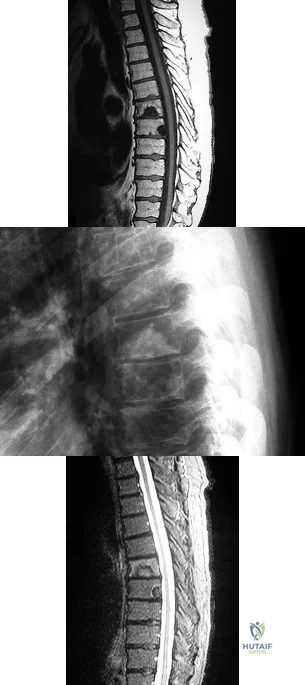
Explanation
The radiograph and MR images show an osteoblastic lesion in the T9 and T8 vertebral bodies. In an older man, this finding most likely reveals metastatic prostate cancer. The first and least invasive diagnostic step is to order a PSA level. Gleave and associates found in a retrospective review of patients with prostate cancer that isolated levels of PSA lower than 10 to 20 micrograms per liter are rarely associated with bone metastasis. Vis and associates documented that 10-year prostate cancer survival in a screened population was higher than 60%, and in an unscreened population it was 24%. In a neurologically intact patient with no evidence of neural compression or instability, surgery is not indicated. Fine-needle aspiration may be performed, but the diagnostic yield in a blastic lesion is low. A bone scan may be indicated to complete the metastatic workup, but it will not aid in the diagnosis of tissue source.
RECOMMENDED READINGS
Gleave ME, Coupland D, Drachenberg D, Cohen L, Kwong S, Goldenberg SL, Sullivan LD. Ability of serum prostate-specific antigen levels to predict normal bone scans in patients with newly diagnosed prostate cancer. Urology. 1996 May;47(5):708-12. PubMed PMID: 8650870. View Abstract at PubMed
Vis AN, Roemeling S, Reedijk AM, Otto SJ, Schröder FH. Overall survival in the intervention arm of a randomized controlled screening trial for prostate cancer compared with a clinically diagnosed cohort. Eur Urol. 2008 Jan;53(1):91-8. Epub 2007 Jun 12. PubMed PMID: 17583416. View Abstract at PubMed
Cronen GA, Emery SE. Benign and malignant lesions of the spine. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:351-366.
CLINICAL SITUATION FOR QUESTIONS 26 THROUGH 29
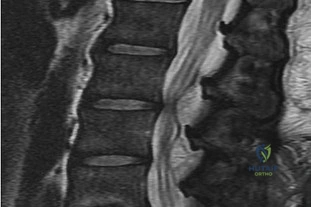

Figures 26a and 26b are the MR images with gadolinium enhancement of a 40-year-old man who arrives at the emergency department with a 4-day history of fevers and severe back pain without radiation. He is normotensive at presentation with a heart rate of 86 beats per minute. Upon examination he is neurologically intact with normal sensory and motor function. He has a history of alcohol and cocaine abuse. His white blood cell (WBC) count is 12000 (reference range [rr], 4500-11000 /µL) and his C-reactive protein (CRP) level is 100 mg/L (rr, 0.08-3.1 mg/L)
Question 34
A 20-year-old man with fascioscapulohumeral dystrophy has severe scapular winging of both shoulders. He can no longer abduct above 80 degrees, and it affects his activities of daily living. A clinical photograph is shown in Figure 26. Definitive management should consist of
Explanation
REFERENCES: Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Bunch WH, Siegel IM: Scapulothoracic arthrodesis in fascioscapulohumeral muscular dystrophy: Review of seventeen procedures with three to twenty-one-year follow-up. J Bone Joint Surg Am 1993;75:372-376.
Question 35
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of
Explanation
REFERENCES: Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Hawkins RJ, Neer CS II, Pianta RM, et al: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 36
What procedure can eliminate a sulcus sign? Review Topic
Explanation
Question 37
The parents of a 3-year-old girl who has had pain and swelling in the right ankle for the past 3 months now report that she has a limp and that the right knee and both ankles are painful and swollen. The limp and difficulty walking are most severe in the morning when the child first gets out of bed and are also more severe after extended walking. The parents deny fever, chills, weight loss, or night pain. Examination shows mild swelling and slightly restricted motion of the right knee and both ankles but is otherwise normal. In addition to initiation of treatment, the child should be referred to which of the following specialists?
Explanation
REFERENCES: Carey TP: Inflammatory arthritides: Juvenile rheumatoid arthritis, seronegative spondyloarthropathies, transient synovitis, hemophilic arthropathy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1315-1321.
Wright D: Juvenile idiopathic arthritis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 427-458.
Question 38
Figure 41 shows the MRI scan of a 38-year-old weightlifter. What does the arrow on the MRI scan indicate?
Explanation
REFERENCES: Bal GK, Basamania CJ: Pectoralis major tendon ruptures: Diagnosis and treatment. Tech Shoulder Elbow Surg 2005;6:128-134.
Aarimaa V, Rantanen J, Heikkila J, et al: Ruptures of the pectoralis major muscle. Am J Sports Med 2004;32:1256-1262.
Question 39
A patient falls off a roof and sustains the fracture shown in Figure 29. What is the most likely complication that results from injury to the structure that is located at the arrow?

Explanation
Question 40
What is the most important stabilizing mechanism in the midrange of motion of the glenohumeral joint? Review Topic
Explanation
Question 41
While performing long fusion with osteotomies for a patient with adult scoliosis and sagittal plane deformity, the neurophysiologist reports a change in motor-evoked potentials in the lower extremities. What is the most appropriate next step?
Explanation
The use of intraoperative neuromonitoring is expanding, especially in the setting of deformity surgery. Changes in monitoring are concerning for the possibility of a neurologic injury; however, several other factors can alter signals. These include hypotension, changes in anesthesia depth and medications, the use of paralytic agents, and technical issues such as leads falling out or becoming disconnected. If a change in neuromonitoring signals is noted, these factors should be checked first to rule out false-positive findings. If this does not correct the problem, the wound should be explored to ensure there is no compression on the neural elements. Finally, if the deformity has been corrected, some of the correction can be released in an attempt to improve the signals. A wake-up test is difficult to perform and does not provide specific information regarding the location of the problem or how to correct it. Steroids may be used depending on surgeon preference, but should not be used until neurologic injury is ruled out. Any neuromonitoring changes always necessitate immediate investigation.
RECOMMENDED READINGS
Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. View Abstract at PubMed
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
Review. PubMed PMID: 21102290. View Abstract at PubMed
Question 42
A 14-year-old boy with a history of cerebral palsy has a clawed hallux, cavus foot deformity, and associated pain. Examination reveals pain under the first metatarsal head and a rigid first tarsometatarsal joint. Treatment should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 79-100.
Tynan MC, Klenerman L: The modified Robert Jones tendon transfer in cases of pes cavus and clawed hallux. Foot Ankle Int 1994;15:68-71.
Question 43
A postmenopausal patient comes to your office for follow-up after a dual-energy x-ray absorptiometry (DEXA) test. The T-score is -0.7SD. The Z score is -0.4SD. By World Health Organization (WHO) criteria, these DEXA findings would merit a diagnosis of
Explanation
The WHO classifies bone density in postmenopausal women based on T-scores. Patients are classified based on the lowest T score of the spine, femoral neck, trochanter, or total hip. The classification should not be used with peripheral measurements. Z-scores are used for premenopausal women, younger men, and in children. The Z score compares a patient with age-, sex-, and race-matched norms.
Blake and Fogelman reviewed the role of central DEXA in treatment of osteoporosis, compared with quantitative CT, peripheral DEXA and quantitative ultrasound. The advantages of central DEXA include results that can be interpreted using WHO T-score definitions, ability to predict fracture risk, and effectiveness at targeting antifracture treatments.
Templeton reviewed secondary osteoporosis. In women with osteoporosis, the most common causes of secondary osteoporosis include hypercalciuria, malabsorption, hyperparathyroidism, vitamin D deficiency, and exogenous hyperthyroidism. In men with osteoporosis, the most common causes of secondary osteoporosis include hypogonadism, corticosteroid use and alcoholism.
Unnanuntana et al. reviewed the assessment of fracture risk. The FRAX (World Health Organization Fracture Risk Assessment Tool) calculates 10-year risk of fracture based on the following variables: age, sex, race, height, weight, BMI, history of fragility fracture, parental history of hip fracture, use of oral glucocorticoids, secondary osteoporosis and alcohol use to calculate 10-year risk of fracture. They also
discussed biochemical markers of bone formation and resorption, which are useful for monitoring the efficacy of antiresorptive / anabolic therapy, and may help identify patients at high risk for fracture.
Illustration A shows the WHO classification. Illustration B shows a comparison between central DEXA and other methods of BMD measurement.
Incorrect Answers:
Question 44
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Explanation
REFERENCES: Michelson JD, Magid D, Ney DR, et al, Examination of the pathologic anatomy of ankle fractures. J Trauma 1992;32:65-70.
Marsh JL, Saltzman CL: Ankle fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 2001-2090.
Question 45
Figure 35 shows the AP radiograph of a patient who underwent a previous upper tibial osteotomy (UTO). The patient may be at risk for which of the following during total knee arthroplasty (TKA)?
Explanation
REFERENCES: Parvizi J, Hanssen AD, Spangehl MJ: Total knee arthroplasty following proximal tibial osteotomy: Risk factors for failure. J Bone Joint Surg Am 2004;86:474-479.
Meding JB, Keating EM, Ritter MA, et al: Total knee arthroplasty after high tibial osteotomy: A comparison study in patients who had bilateral total knee replacement. J Bone Joint Surg Am 2000;82:1252-1259.
Question 46
A 6-year-old boy had a 4-day history of worsening atraumatic right thigh and knee pain. He was seen in the emergency department, where he had a temperature of 39.1°C. Laboratory studies reveal a white blood cell count of 15000 /µL (reference range, 4500-11000 /µL). He had a small knee effusion with range of motion 0 to 90 degrees and a swollen, painful, hot distal thigh. The knee effusion was aspirated, revealing a white blood cell (WBC) count of 2000 with negative gram stain (reference range < 2000 WBC/mL). The boy was admitted to the pediatric medical service and intravenous (IV) antibiotics were initiated. The next day, MR imaging was obtained and orthopaedics was consulted. Based on Figures 8a and 8b, what is the most appropriate description of his condition?
Explanation
The MRI scans show an advanced distal femur osteomyelitis with a substantial subperiosteal abscess. This necessitates open drainage; by definition, an abscess is avascular, so antibiotics cannot be delivered to the area without drainage.

CLINICAL SITUATION FOR QUESTIONS 9 THROUGH 12
Figures 9a and 9b are the radiographs of a 9-year-old boy who fell from the monkey bars and sustained a closed fracture of the elbow.
Question 47
A 40-year-old woman is admitted to the hospital with a history of new-onset right lower extremity weakness resulting in frequent falls. She reports that a few weeks prior to the onset of the lower extremity symptoms, she experienced an episode of acute back pain, which has since resolved. Examination reveals 1-2/5 strength in the right hip flexors, abductors, and quadriceps. There is 0-1/5 strength

Explanation
(SBQ12SP.39) Which of the following is associated with increased risk of surgical site infection following lumbar spinal decompression? Review Topic
Use of intra-wound vancomycin powder
Hair removal by clipping at the time of surgery
Use of morphine nerve paste applied to the dura after spinal decompression
Skin preparation with an alcohol-based prep solution rather than povidone iodine
Failure to use chlorhexidine gluconate wash the night prior to surgery
The use of morphine nerve paste applied to the dura after decompressive spine surgery has been used in an effort to mitigate postoperative pain but has been associated with epidemic levels of surgical site infection.
Surgical site infection risk is modulated by a myriad of factors, both host factors and perioperative factors. Perioperative strategies to reduce infection that have been shown to be effective include: 1) hair removal by clipping (not shaving) at the time of surgery, 2) use of an alcohol based skin preparation agent, 3) use of perioperative prophylactic antibiotics, 4) limiting operating room traffic from OR personnel.
Kramer et al. did a retrospective analysis of 148 patients who underwent laminectomy in order to identify risk factors for infection in the context of a sudden increase in infections. Regression analysis showed that use of morphine paste resulted in an 18-fold increase in the risk of surgical site infection. 17 of 148 had developed infection during the epidemic period, compared to 15/995. Cultures were positive in 10 of 16 cases; 7 of these involved skin flora. Histological exam showed foreign body reaction.
Devin et al. did a multi-center analysis of patients undergoing spine surgery at seven spine centers to determine whether there was a difference in infection risk based on whether or not intra-wound vancomycin was used. They analyzed 2056 patients, of whom 47% had vancomycin used in their wounds. The risk of surgical site infection was higher in those patients that did not have vancomycin (relative risk 2.5).
Incorrect answers:
Question 48
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. What is the UKA survivorship for a 55- year-old patient, compared with the survivorship for total knee arthroplasty?
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress
faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 49
Figure 29 shows the radiograph of a 55-year-old patient who has recurrent total hip dislocation. Dislocation is most likely to occur in this patient when the hip is in which of the following positions?
Explanation
REFERENCE: Paterno SA, Lachiewicz PF, Kelley SS: The influence of patient-related factors and the position of the acetabular component on the rate of dislocation after total hip replacement. J Bone Joint Surg Am 1997;79:1202-1210.
Question 50
During head-on motor vehicle collisions occurring at highway speeds, airbag-protected individuals have a decreased rate (as compared to non-airbag protected individuals) of all of the following EXCEPT:

Explanation
Question 51
Which of the following nonunions is appropriately treated with exchange reamed nailing without bone graft augmentation?

Explanation
Question 52
Two football players present with knee pain and instability after being tackled in a game. Figures A and B are injury radiographs for Player A and B, respectively. Which of the following is correct regarding the radiographic findings of these 2 players? Review Topic

Explanation
A Segond fracture is commonly associated with ACL tear (75%). It is caused by internal rotation and varus load (unlike the more common cause of ACL tear, which is valgus stress). The arcuate sign is an avulsion fracture of the proximal fibula at the site of insertion of the arcuate ligament complex, and is usually associated with cruciate ligament injury (~90% of cases). The fracture fragment is attached to the LCL or biceps femoris tendon.
Dodds et al. reviewed the anatomy of the ALL in 4 cadaveric knees. They found that the ligament was isometric from 0 to 60° of flexion and slackened with the knee flexed to 90°. It passed superficial to the LCL and knee capsule. Mean length was 59 mm, mean width was 6 mm. The femoral attachment was slightly posterior to both the lateral epicondyle and the femoral attachment of the LCL. The tibial attachment just distal to the anterolateral rim of the plateau, mid-way between the head of the fibula and Gerdy’s tubercle. An arcuate complex avulsion fracture is an avulsion of the fibular styloid attachment of the arcuate complex.
Claes et al. (2014) compared the distance between the tibial ALL footprint to the center of Gerdy's tubercle (GT, in cadavers) vs the distance between GY and a Segond fracture (on CT). They found the former to be 22mm, and the latter to be
Question 53
below shows the radiograph obtained from a year-old woman who has sharp pain in her groin, thigh, and buttocks that worsens with activity. She has been dealing with this pain for more than a year but is otherwise healthy. Recently, she has begun to notice night pain. The pain no longer responds to NSAIDs. She would like to be able to dance at her daughter's wedding in 4 months and wonders how best to proceed. What is the best next step?
Explanation
The next best course of action is total hip arthroplasty. The patient is an otherwise healthy woman requesting pain relief and expresses a desire to be dancing in 4 months. She has had more than 6 months of symptoms that are classic hip osteoarthritis symptoms, with pain in the groin and thigh. Severe osteoarthritis is seen in the radiograph as well. NSAIDs are no longer working. Given the objective findings, the subjective reports, and the duration of symptoms, this patient merits surgery. Consideration for steroid injection is reasonable, but given her desire to be dancing in 4 months, an injection would increase her risk of infection if total hip arthroplasty were to be performed within 3 months of the
injection.
Question 54
A 14-year-old girl reports a 3-week history of anterior thigh pain and a palpable mass after sustaining a soccer-related injury. Examination reveals a tender, firm mass in the midportion of the rectus femoris. MRI scans are shown in Figures 39a through 39c. What is the most appropriate management? Review Topic
Explanation
Question 55
Which of the following is an advantage of unreamed nailing of the tibia compared to reamed nailing?
Explanation
REFERENCES: Larsen LB, Madsen JE, Hoiness PR, et al: Should insertion of intramedullary nails for tibial fractures be with or without reaming? A prospective, randomized study with 3.8 years’ follow-up. J Orthop Trauma 2004;18:144-149.
Blachut PA, O’Brien PJ, Meek RN, et al: Interlocking intramedullary nailing with or without reaming for the treatment of closed fractures of the tibial shaft: A prospective randomized study. J Bone Joint Surg Am 1997;79:640-646.
Question 56
Autosomal dominant
Explanation
A patient presents with a hard leg mass and pain with activity. The anteroposterior and lateral radiographs are shown in Slide 1 and Slide 2. An axial computed tomography scan is shown in Slide 3. Which of the following tumor suppressor genes is most likely involved:
Question 57
A 70-year-old man reports symptomatic medial knee pain that has become progressively worse during the past year. MRI reveals a complex, posterior horn medial meniscus tear with associated medial lateral and patellofemoral cartilage defects. Radiographs reveal medial joint space narrowing and osteophytes in the other compartments. What treatment is most likely to provide long-term, durable relief of symptoms?
Explanation
Total knee replacement is a well-established surgery for diffuse, symptomatic osteoarthritis of the knee joint, and its efficacy has been shown in many studies. According to the 2008 AAOS Clinical Practice Guideline, Treatment of Osteoarthritis of the Knee, arthroscopy in the setting of existing osteoarthritis is efficacious for relieving the signs and symptoms of a torn meniscus but not for osteoarthritis. Likewise, in young and active patients, clinical outcomes show improvement after realignment osteotomy for single- compartment osteoarthritis. Unicondylar knee replacement is not indicated for tricompartmental disease
of the knee.
Question 58
A 22-year-old man reports anterior knee pain, swelling, and is unable to perform a straight leg raise after undergoing endoscopic anterior cruciate ligament (ACL) reconstruction with a bone-patellar tendon-bone autograft 1 week ago. He is afebrile. Examination reveals a clean incision, moderate effusion, a weak isometric quadriceps contraction, active knee range of motion of 5 degrees to 45 degrees, and the patella is ballottable. Knee radiographs show postoperative changes with good femoral and tibial tunnel placements, and normal patellar height. What is the next most appropriate step in management?
Explanation
REFERENCES: Kennedy JC, Alexander IJ, Hayes KC: Nerve supply of the human knee and its functional importance. Am J Sports Med 1982;10:329-335.
Fahrer H, Rentsch HU, Gerber NJ, et al: Knee effusion and reflex inhibition of the quadriceps: A bar to effective retraining. J Bone Joint Surg Br 1988;70:635-638.
Question 59
Figure 53 shows a thoracolumbar specimen as viewed from posterior to anterior following removal of all posterior elements. Which of the following structures does the red string pass under?
Explanation
REFERENCE: Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, p 1465.
Question 60
What are the five most common tumors that metastasize to bone?
Explanation
REFERENCES: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
CA, January/February 2000, vol 50, no. 1 (Cancer Statistics).
Question 61
Preventing "missed" femoral neck fractures associated with ipsilateral femoral shaft fractures is best achieved with
Explanation
Ipsilateral femoral neck and shaft fractures occur in up to 6% of femur fractures. A femoral neck fracture is often vertical and nondisplaced. A high degree of suspicion is necessary to avoid "missed" femoral neck fractures in patients with this condition. Although an examination and dedicated hip radiographs help to avoid missed injuries, a significant decrease in missed
injuries has been described with the use of thin-cut pelvic CT images. In patients who undergo trauma, a pelvic CT scan is often performed to assess for associated injuries and is easily reviewed to examine the femoral neck. Although MRI is advocated to identify isolated occult femoral neck fractures, CT has been described as the method of choice with which to identify ipsilateral femoral neck and shaft fractures in the trauma population. Currently, no literature supports the use of MRI in this population.
RECOMMENDED READINGS
Tornetta P 3rd, Kain MS, Creevy WR. Diagnosis of femoral neck fractures in patients with a femoral shaft fracture. Improvement with a standard protocol. J Bone Joint Surg Am. 2007 Jan;89(1):39-43. PubMed PMID: 17200308.View Abstract at PubMed
Kuhn KM, Agarwal A. Femoral fractures. In: Cannada LK, ed. Orthopaedic Knowledge Update
Question 62
Which of the following is not considered to be a part of the constellation of the clinical entities known as the female athlete triad? Review Topic
Explanation
The female athlete triad was coined in 1992 by the American College of Sports Medicine as a complex disorder more prevalent in the adolescent and young female
athlete population including decreased bone mineral density (BMD), menstrual dysfunction, and low energy availability with or without a concomitant eating disorder. Treatment should involve a multidisciplinary approach, including psychological and nutritional counseling for eating behaviors and dietary management, reduction of training intensity to decrease risk of stress fractures, and initiating calcium and vitamin D supplements for osteoporosis.
Nazem et al performed a systematic review of articles containing the female athlete triad, reviewing diagnosis via screening during physical examinations as well as laboratory and imaging evaluation for menstrual dysfunction, low energy availability, and low bone mineral density. They state that potential complications including possible infertility, decreased immune function, cardiovascular disease, and irreversible loss of bone mineral density. They concluded that prevention, early recognition, and a multidisciplinary treatment team with a focus on proper nutrition and natural return of menses is vital.
Nattiv et al review the position of the American College of Sports Medicine regarding the female athlete triad, including screening for the triad at the pre-participation physical, discouragement of unhealthy weight loss practices. Essential members of the multidisciplinary treatment team include a health-care professional, a registered dietitian, and a mental health practitioner. They endorse that the first aim of treatment for any triad component is to increase energy availability by increasing energy intake and reducing exercise energy expenditure.
Question 63
An 18-year-old man sustains an injury to his lateral ankle after being kicked while playing soccer. He reports persistent pain on the lateral ankle as well as a popping sensation with attempted ankle dorsiflexion and eversion. Which of the following structures anatomically restrains the retracted structure shown in Figure 12?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 81-89.
Sarrafian S: The Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 113-158.
Question 64
A 20-year-old basketball player sustains a knee injury during a game and is seen in the orthopaedic clinic 3 days after injury. Examination reveals a positive Lachman, pivot shift, joint line tenderness, and moderate effusion. Which of the following tissue injuries is most likely causing the jointline tenderness? Review Topic
Explanation
Question 65
A patient who underwent a high tibial osteotomy (HTO) is now scheduled to undergo total knee arthroplasty (TKA). When compared with a patient undergoing primary TKA without a prior HTO, the patient should be advised to expect a higher incidence of
Explanation
REFERENCE: Mont MA, Alexander N, Krackow KA, Hungerford DS: Total knee arthroplasty after failed high tibial osteotomy. Orthop Clin North Am 1994;25:515-525.
Question 66
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 67
A 70-year-old woman with a body mass index (BMI) of 34 and a history of hypercholesterolemia has elected to undergo total hip arthroplasty. Her son recently learned he has factor V Leiden following an episode of pulmonary embolism. What are this patient's risk factors for thromboembolic disease?
Explanation
Risk stratification is one of the most critical clinical evaluations to undertake before performing total joint arthroplasty. Many factors have been identified that increase the risk for venous thromboembolism (VTE) The major factors include previous VTE, obesity, type of surgery (such as total joint arthroplasty), hypercoagulable states, myocardial infarction, congestive heart failure, family history of VTE, and hormone replacement therapy. Hypercholesterolemia is not a risk factor for thromboembolic disease.
Question 68
A polytrauma patient underwent the following procedures: (1) statically locked intramedullary nailing for a right femoral shaft fracture; (2) open reduction with plate-and-screw fixation [ORIF] for a right simple distal fibula fracture; (3) ORIF right middle third radius and ulna fracture; and (4) ORIF left humeral shaft fracture. What is the appropriate weightbearing status for this patient? Review Topic
Explanation
Tingstad et al. examined the effect of immediate weightbearing on plated fractures of the humeral shaft. They reported that immediate weightbearing on humeral shaft fractures, treated with plating and full weightbearing, did not have any negative effect on the union or malunion rates.
Brumback et al. evaluated the feasibility, safety and efficacy of immediate weightbearing after treatment of femoral shaft fractures with statically locked IM nail. Using biomechanical and clinical data, they showed that all fractures united with no loss of fixation or hardware failure.
Starkweather et al. retrospectively assessed the complications and loss of reduction in patients who bore weight in a short leg cast within 15 days after surgical repair of acute unilateral closed ankle fractures. Of the 81 ankle fracture radiographs, 80 (98.8%) showed no displacement in fracture reduction on the final follow-up examination. These results suggest early protected weightbearing may be safe.
Incorrect Answers:
Question 69
For this patient, which TKA design is most appropriate?
Explanation
TKA in the setting of valgus deformities poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when used as a rotational reference point, can lead to internal rotation of the femoral component if not recognized. This malrotation will in turn lead to patellofemoral maltracking or instability, which is a common complication associated with primary TKA. The deformity is too severe to consider a bicruciate-retaining TKA or unicompartmental arthroplasty and does not necessitate a hinged TKA.
Question 70
-What is the most common metatarsal fracture in a 3-year-old?
Explanation
Figures 77a through 77c are the preoperative and postoperative radiographs of a 13-year-old boy who had sudden worsening of left hip pain following many months of mild pain. He was unable to walk because of his pain and underwent screw fixation.
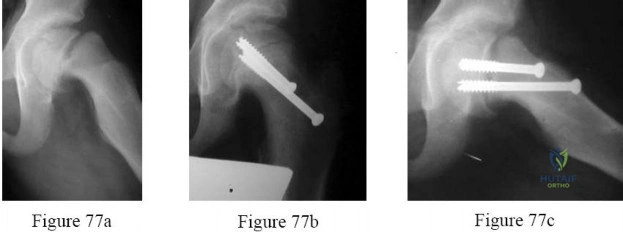
Question 71
Which clinical finding most strongly suggests that nonsurgical care should be discontinued and surgical intervention is necessary?
Explanation
Epidural abscesses are potentially devastating. Nonsurgical care may be chosen for select patients. A baseline failure rate of 8.3% increases based on patient risk factors, which include a history of IV drug abuse, diabetes, age older than 65, CRP level higher than 115, WBC level higher than 12.5, and Staphylococcus aureus as the causative organism. Immunosuppression and abscess size are not significant risk factors for failure of nonsurgical care. Nonsurgical care may be regarded as "failed" if there is worsening of a patient's neurologic status. When nonsurgical care fails, delayed surgery is less successful at restoring motor function (vs early surgery).
RECOMMENDED READINGS
Kim SD, Melikian R, Ju KL, Zurakowski D, Wood KB, Bono CM, Harris MB. Independent predictors of failure of nonoperative management of spinal epidural abscesses. Spine J. 2014 Aug 1;14(8):1673-9. doi: 10.1016/j.spinee.2013.10.011. Epub 2013 Oct 30. PubMed PMID:
Question 72
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of
Explanation
REFERENCES: Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Funasaki H, Winter RB, Lonstein JB, et al: Pathophysiology of spinal deformities in neurofibromatosis: An analysis of seventy-one patients who had curves associated with dystrophic changes. J Bone Joint Surg Am 1994;76:692-700.
Question 73
80 A B year-old with the injury pattern seen on the radiographs in Figures 80a and 80b
Explanation
Question 74
The Arg-Gly-Asp (RGD) sequence of extracellular bone proteins directly allows which of the following?
Explanation
Bone homeostasis involves molecular regulation that involves osteoblasts, osteoclasts, and bone. Osteoblasts upregulate and down regulate osteoclasts that absorb bone at the ruffled borders. Integrins, on the surface of osteoclasts bind to extracellular proteins on bone, such as vibronectin, to facilitate bone resorption at the ruffled border. The Arg-Gly-Asp (RGD) sequence plays an important roll in the binding of integrins and extraceullar proteins such as vibronectin and fibronectin. After binding, the intracellular side of these proteins binds to intracellular proteins to allow for change in the intracellular structures and function.
Bosseti et al. review the extracellular matrix interactions involved with bone induction and conduction mechanisms. They note that extracellular binding leads to intracellular protein alteration, which causes different intracellular effects depending on the specific ligand that binds.
Illustration A shows the binding of integrin and vibronectin.
Incorrect Answers:
(SBQ12SP.45) Which of the following lists these materials in order of increasing modulus of elasticity?:
Cortical bone; Titanium; Cobalt-chrome; Stainless steel; Ceramic
Titanium; Cortical bone; Ceramic; Cobalt-chrome; Stainless steel
Cortical bone; Titanium; Stainless steel; Cobalt-chrome; Ceramic
Stainless steel; Titanium; Cortical bone; Ceramic; Cobalt Chrome
Cortical bone; Stainless steel; Titanium; Cobalt-chrome; Ceramic
Cortical bone has the lowest modulus of elasticity of the materials listed, followed by titanium, stainless steel, cobalt-chrome alloy, then ceramic.
Young's modulus of elasticity is the ratio of stress to strain, and represents the stiffness of a material and its ability to resist deformation when placed under tension. Of the materials listed, titanium has the stiffness closest to cortical bone. Ceramic has the highest modulus of elasticity, making it the most stiff of the materials listed.
Illustration A (from Miller's Review) shows the relative stiffnesses of various orthopaedically relevant materials. Young's modulus is the slope of the lines shown. Illustration B (Google images) charts their Young's Modulus.
Incorrect answers:
Question 75
Genetic analysis has revealed a strong linkage between osteoarthritis in women with which of the following molecules?
Explanation
of over 400 families showed that type IX collagen is linked to development of OA in women. Mice with a type IX collagen gene deletion are also susceptible to early arthritis. Other genes, such as cartilage enzyme aggrecanase ADAMTS-5, have also been associated with OA.
Question 76
A previously healthy 30-year-old woman has neck pain and bilateral hand and lower extremity tingling with weakness after falling down stairs. She is alert and oriented. Examination reveals incomplete quadriplegia at the C6 level that remains unchanged throughout her evaluation and initial treatment. Radiographs show a bilateral facet dislocation of C6 on C7 without fracture. Attempts at reduction with halo cervical traction up to her body weight are unsuccessful. What is the next most appropriate step?
Explanation
REFERENCES: Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217.
Fardon DF, Garfin SR, Abitbol J (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 247-262.
Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. J Bone Joint Surg Am 1991;73:1555-1560.
Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 77
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?
Explanation
REFERENCES: Herring JA, Kim HT, Browne R: Legg-Calve-Perthes disease: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-2134.
Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 691-704.
Question 78
The essential lesion responsible for posterolateral rotatory instability of the elbow is disruption of the
Explanation
REFERENCES: O’Driscoll SW, Jupiter JB, King GJW, Hotchkiss RN, Morrey BF: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
Olsen BS, Sojbjerg JO, Dalstra M, Sneppen O: Kinematics of the lateral constraints of the elbow. J Shoulder Elbow Surg 1996;5:333-341.
O’Driscoll SW, Morrey BF, Korinek S, An KN: Elbow subluxations and dislocation: A spectrum of instability. Clin Orthop 1992;280:186-197.
Question 79
A 20-year-old college athlete is seen for follow-up after sustaining an injury at football practice 2 days ago. He reports that he tackled a player and felt neck pain and numbness in both arms. The numbness resolved within seconds, but his neck remains painful and stiff. He denies any history of neck pain or injury. Examination reveals limited neck motion. The neurologic examination and radiographs are normal. MRI scans of the cervical spine are shown in Figure 34. During counseling, the patient, his family, and his coach should be informed that he has an acute cervical disk herniation and cannot play
Explanation
REFERENCES: Morganti C, Sweeney CA, Albanese SA, Burak C, Hosea T, Connolly PJ: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Vaccaro AR, Watkins B, Albert TJ, Pfaff WL, Klein GR, Silber JS: Cervical spine injuries in athletes: Current return-to-play criteria. Orthopedics 2001;24:699-705.
Question 80
A 43-year-old woman is referred after excisional biopsy of a cutaneous soft-tissue mass from her left shoulder. Based on the biopsy specimens shown in Figures 44a and 44b, what is the best course of action?
Explanation
REFERENCES: Lindner NJ, Scarborough MT, Powell GJ, et al: Revision surgery in dermatofibrosarcoma protuberans of the trunk and extremities. Eur J Surg Oncol
1999;25:392-397.
Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 491-505.
Question 81
Which of the following diagnostic studies best distinguishes Ewing’s sarcoma from small cell osteosarcoma?
Explanation
REFERENCES: Perotti D, Corletto V, Giardini R, Parafioriti A, Fossati-Bellani F, Luksch R: Retrospective analysis of ploidy in primary osseous and extraosseous Ewing family tumors in children. Tumori 1998;84:493-498.
Riley RD, Burchill SA, Abrams KR, Heney D, Sutton AJ, Jones DR, et al: A systematic review of molecular and biological markers in tumours of the Ewing’s sarcoma family. Eur J Cancer 2003;39:19-30.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 11-20.
Question 82
Figure 21 is the radiograph of a 45-year-old woman who was severely injured in a motorcycle crash. Her injuries include a traumatic subarachnoid hemorrhage, bilateral pneumothoraces with pulmonary contusions and flail chest, fracture-dislocation of the left hip, and open fractures of the right distal femur and proximal tibia. Antibiotics and tetanus are administered in the emergency department. The patient is intubated and bilateral chest tubes are placed. A closed reduction is performed on the left hip. After appropriate resuscitation, what is the most appropriate initial management of the right knee injury?

Explanation
Question 83
Plate fixation without bone grafting
Explanation
Which of the following stress fractures most often requires internal fixation:
Question 84
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At 1-year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is
Explanation
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 85
A radiologist's report of a lateral knee radiograph comments that the height of the patella is 4 cm, and the length of the patellar tendon is 3 cm. Which of the following may lead to this measurement? Review Topic
Explanation
The measurements described allow you measure an Insall-Salvati Index (ISI). The ISI is the ratio of the patellar tendon length to the patellar height (distance from the superior pole to the inferior pole). These measurements give a ratio of 0.75 which indicates the presence of patella baja. Normal values range from 0.8 to 1.2. A lower ratio is diagnostic of patella baja, while a higher ratio is diagnostic of patella alta. The ISI as well as some other measures of the patella's position within the trochlea are important when evaluating conditions such as patellar instability or patellofemoral
pain.
Insall and Salvati present their original paper describing the anatomy of the knee with respect to patellar positioning. They note that previous methods of determining patellar positioning was either too complicated, or too subjective. They found the length of the patellar tendon and the height of the patella to be approximately equal, and saw no variations greater than 20%. Thus they proposed the ISI with "normal" values ranging from 0.8 to 1.2.
Shabshin et al. present a study making similar calculations as the ISI but done on sagittal MRI rather than lateral radiographs. They found a slightly higher degree of variation, and defined "normal" as ranging from 0.79 to 1.52. They also noted females tended to have higher ratios on average compared to males.
Aglietti et al. compared various measurements of the patellofemoral joint in a group of asymptomatic knees compared to knees with recurrent patellar subluxation. The normal knees were found to have an ISI of about 1, average congruence angle of -8, and an average Q angle of 15°. The subluxating knees had higher ISIs (average 1.23), higher congruence angles (average +16), and a higher Q angles (average 20°).
Illustration A shows how to measure and calculate the ISI. Illustration B shows measurements of the patellofemoral joint that may help identify presence of trochlear dysplasia and patellar maltracking.
Incorrect Answers:
Question 86
When balancing gaps in the coronal plane, what structure preferentially impacts the flexion space more than the extension space?
Explanation
In the setting of valgus deformities, TKA poses different challenges than those encountered when varus deformities are present. Most valgus alignment is attributable to a deformity of the distal femur rather than of the proximal tibia, as seen in varus knees. One of the major anatomical differences is a hypoplastic lateral femoral condyle which, when not recognized and used as a rotational reference point,
can lead to internal rotation of the femoral component. This malrotation in turn leads to patellofemoral maltracking or instability, which is a common complication associated with primary TKA.
Question 87
Spindled cells that are surrounded in mature osteoid that connect to other similar cells via canaliculi are best described as which of the following? Review Topic
Explanation
Question 88
A teenager had pain in the left buttock while running the hurdles. He was treated with 4 weeks of rest and crutch walking, and then started physical therapy for stretching and muscle strengthening. Nine months later he now reports pain with sitting and has not been able to resume running or sports activity. Figure 96 shows a radiograph of the pelvis. Treatment should consist of which of the following?
Explanation
REFERENCES: Fembach SK., Wilkinson RH: Avulsion injuries of the pelvis and proximal femur. AJR Am J Roentgenol 1981;137:581-584.
Watts HG: Fractures of the pelvis in children. Orthop Clin North Am 1976;7:615-624. Question 97
Congenital anomalies of the vertebral column are associated frequently with other organ system problems. In addition to radiographs of the spine, what other screening tests should be ordered?
Spinal MRI, coagulation panel
Liver enzymes, coagulation panel
Renal ultrasound, upper and lower GI
Cardiac evaluation/echocardiogram, upper and lower GI
Renal ultrasound, cardiac evaluation/echocardiogram, spinal MRI
DISCUSSION: Approximately 60% of patients with congenital anomalies of the spine have other associated findings. The spine develops around the same time as the cardiovascular system, the genitourinary system, and the musculoskeletal system. Around 20% of patients with congenital scoliosis have an associated urologic abnormality. Approximately 25% of patients with congenital scoliosis have an associated cardiac defect. Spinal cord abnormalities in one study occurred in approximately 37% of patients with congenital scoliosis.
REFERENCES: Basu PS, Elsebaie H, Noordeen MH: Congenital spinal deformity: A comprehensive assessment at presentation. Spine 2002;27:2255-2259.
Ferguson RL: Medical and congenital comorbidities associated with spinal deformities in the immature spine. J Bone Joint Surg Am 2007;89:34-41.
McMaster MJ, Ohtsuka K: The natural history of congenital scoliosis: A study of two hundred and fifty- one patients. J Bone Joint Surg Am 1982;64:1128-1147.
2010 Pediatric Orthopaedic Examination Answer Book • 81
Figure 98a Figure 98b
Question 89
Figures 51a and 51b show subluxation of the
Explanation
REFERENCES: Rowland SA: Acute traumatic subluxation of the extensor carpi ulnaris tendon at the wrist. J Hand Surg Am 1986;11:809-811.
Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1026-1027.
Question 90
A 20-year-old male military recruit reports a 5-day history of progressive deep groin pain that is made worse with weight-bearing activities and running. His initial coronal T2-weighted MRI scan is shown in Figure 75. His initial treatment should consist of which of the following? Review Topic
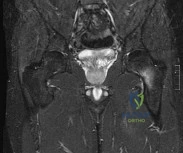
Explanation
Question 91
A 69-year-old male presents with acute on chronic neck pain. He denies trauma, fevers, or chills. He has noticed some clumsiness in his hands recently and change in his handwriting. He has had progressive deterioration of his gait. Physical exam shows a positive grip and release test, a positive Hofmann sign, and 3+ patellar reflexes. MRI image is shown in Figure A. The procedure shown in Figure B is performed. Which of the following statements is true regarding this treatment option? Review Topic

Explanation
The treatment of cervical myelopathy is dictated by the number of stenotic levels, sagittal alignment of the spine, and more recently attempt to retain motion. Anterior cervical discectomy and fusion (ACDF) is used for one or two level disease with pathology localized to anterior spine. Posterior decompression and fusion is typically used for disease at more than two levels and is contraindicated with kyphosis greater than 13 degrees. Lamninoplasty and cervical disc arthroplasty are thought to be motion-preserving alternatives, although there can be unintended loss of motion with both techniques. The open door laminoplasty technique involves the use of a suture anchor or small plate to maintain the opening on one side while the french door technique involves hinges bilaterally and opening in the midline.
Emery reviewed the diagnosis and management cervical myelopathy. Surgical management is advocated for patients with functional impairment. Depending on location and extent of pathology, anterior procedures may require corpectomy and use of strut grafting.
Gerard et al. reviewed techniques of surgical management of myelopathy. They describe a minimally invasive posterior decompression using a tubular retractor system. Patients are carefully selected and should have less than 3 levels of disease, no evidence of instability, and normal lordosis.
Figure A is a T2 sagittal MRI image showing multilevel cervical stenosis. Figure B is lateral radiograph of a patient who underwent multilevel laminoplasty. Illustration A shows the open door technique.
Incorrect
Question 92
A 17-year-old high school track athlete has had progressive midfoot pain for the past 3 weeks that prevents him from running. Examination reveals pain over the tarsal navicular. Radiographs are normal, but a CT scan reveals a nondisplaced sagittally oriented fracture line. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Torg J, Pavlov H, Cooley LH, et al: Stress fractures of the tarsal navicular: A retrospective review of twenty-one cases. J Bone Joint Surg Am 1982;64:700-712.
Question 93
30%
Explanation
Initial assessment of a trauma patient should involve evaluation of airway, breathing and circulation. An average adult has approximately 5 L of circulating blood volume. Class III and IV hemorrhagic shock, approximated by loss of greater than 30% of blood volume, typically requires resuscitation with fluids and blood products. Lactate level (normal <2.5) is typically the most sensitive indicator of adequate perfusion.
According to ATLS guidelines, the emphasis of the initial assessment is to assume the worst injury and begin treatment before diagnosis. In cases of hemorrhagic shock, treatment involves aggressive resuscitation with crytalloid and/or blood products.
Illustration A is a chart showing the physiological changes associated with different levels of hemorrhagic shock
Incorrect Answers:
1: Blood loss of <15% typically leads to no changes in vital signs
2: Blood loss of 15-30% typically leads to heart rate >100 and diminished urine output
4, 5: Blood loss of greater than >40% typically leads to heart rate >140, decreased blood pressure and negligible urine output.

OrthoCash 2020
Which of the following fracture patterns would be most appropriately treated with open reduction and internal fixation with posteromedial and lateral plates via dual incisions?

The patient in Figure D has a bicondylar tibial plateau fracture with a posteromedial fracture fragment, which is an indication for lateral and posteromedial plating via dual incisions.
Bicondylar tibial plateau fractures are typically treated with open reduction internal fixation. Studies have shown that the posteromedial fragment is common in bicondylar tibial plateau fractures. Standard lateral implants do not gain adequate screw purchase in posteromedial bone. Posteromedial incisions using the interval between the semimembranosus and medial head of the gastrocnemius can be used to gain access to the fragment and provide exposure to place a posteromedial plate.
Barei et al. reviewed 57 OTA C-type bicondylar tibial plateau fractures, and found the presence of a posteromedial fragment in 74% of cases. They suggest
the use of alternate methods of fixation for the posteromedial fragment rather than lateral fixed-angle plates alone.
Higgins et al. reviewed 111 patients with bicondylar tibial plateaus that underwent CT scan evaluation. They found the incidence of a posteromedial fragment in 59% of the patients and on average accounted for 25% of the articular surface.
Barei et al. reviewed 83 patients treated with dual incisions for fixation of bicondylar tibial plateau fractures. They found deep infections in 8.4% of patients. Satisfactory articular reduction was found in 62% of patients, satisfactory coronal alignment in 91% of patients, satisfactory sagittal alignment in 72%, and satisfactory condylar width in 98%.
Figure A shows an AP and lateral radiograph of a split/depressed lateral tibial plateau fracture. Figure B shows an AP and lateral radiograph of a proximal third tibial shaft fracture with a proximal fibula fracture. Figure C shows an AP and lateral radiograph of a medial plateau fracture with articular depression. Figure D shows an AP and lateral radiograph of a bicondylar tibial plateau fracture. Figure E shows an AP and lateral radiograph of a tibial tubercle fracture in a tibia with open physes.
Incorrect Answers:
OrthoCash 2020
Figure A shows the radiographs of a 87-year-old patient after a fall from standing. He lives in a nursing home and uses a walker to transfer from bed to chair. His past medical history includes recurrent urinary tract infections, congestive heart failure, angina and diabetes. Which of the following factors is associated with the best postoperative outcome in this patient?

Immediate surgical intervention
Postoperative epidural analgesia
Postoperative antibiotics
Pre-operative medical optimization
Choosing total hip arthroplasty instead of hemiarthroplasty Corrent answer: 4
Geriatric patient with hip fractures tends to have a number of coexisting medical conditions that impact surgical risk. A successful pre-operative medical evaluation has the greatest impact on surgical outcomes in this patient population.
Patients with complex past medical histories are at great risk of complications with surgery. This helped to drive the formation of the ASA classification system as a way to score patients out of 5 based on their anesthetic and surgical risks. Patients with significant systemic disease (ASA III and IV) have shown to demonstrate poorer outcomes as compared to patients with less severe medical comorbidities (ASA I and II).
Egol et al. looked at factors that impact the outcomes of hip fractures in geriatric patients. They showed that cardiac and pulmonary complications were most frequent complications post-operatively. It was stated that early mobilization and pre-operative evaluations have the greatest impact on outcomes.
Parvizi et al. looked at the thirty-day mortality following hip arthroplasty for acute fracture. They reviewed a database of 7774 consecutive patients that underwent hip arthroplasty for the treatment of an acute fractures. The overall mortality was 2.4%. Risk factors were found to be cemented implants, female patients, elderly patients, and patients with cardiorespiratory comorbidities.
Roberts et al reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. Although pre-operative medial optimization was not mentioned in this review, there is strong evidence to support an interdisciplinary care program for patients with hip fractures.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
more than 24-48 hours and a higher 1-year mortality rate. However, In patients with with more than 3 medical comorbidities, medical optimization has a greater impact on post-operative outcomes than time to surgery.
OrthoCash 2020
A 36-year-old male sustains severe injuries as a result of a motor vehicle collision. After 5 days, the patient is stabilized and transferred to your facility for continued management. After obtaining appropriate imaging, including the images shown in Figures A, B and C the patient should be given which of the following mobility restrictions?

Touch-down weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
Weight bearing as tolerated on the left lower extremity, non-weightbearing on the right lower extremity
Non-weight bearing on the left lower extremity, non-weightbearing on the right lower extremity
Touch-down weight bearing on the left lower extremity, weight bearing as tolerated on the right lower extremity
Weight bearing as tolerated on the left lower extremity, weight bearing as tolerated on the right lower extremity
Figures B and C shows a stable, impacted lateral compression (LC) type I injury, which can be treated with immediate mobilization without restrictions. The right lower extremity has a pilon fracture, which should be treated with non-weight bearing.
LC-I injuries are stable patterns, as they involve an impaction injury to the anterior sacrum, which has some inherent stability. In addition, the posterior sacro-iliac (SI) soft tissue structures remain intact, which provides critical stability during immediate mobilization.
The reference by Tile is a review article on the principles of management of these injuries, and he reviews how the Tile classification system is important to help determine surgical need and where the stabilization is required. For the stable LC-1 type injury, no fixation is required.
Incorrect Answers:
OrthoCash 2020
A 24-year-old male sustains the fracture dislocation shown in Figure A. How is this fracture pattern best classified?
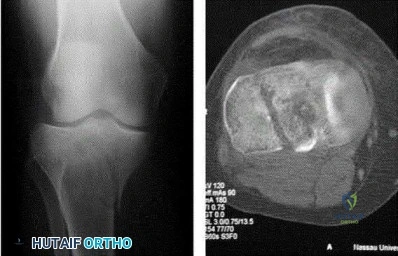
Moore I
Moore II
Schatzker III
Schatzker V
OTA type 41B3 Corrent answer: 2
Figure A shows a Moore Type II fracture. Moore type II fractures consist of fractures involving the entire tibial condyle, where the fracture line begins in the opposite compartment and extends across the tibial eminence.
A number of classification systems are used to describe tibial plateau fractures. The main classification systems that are widely used include Schatzker, AO/OTA, Hohl and Moore. The Moore classification describes high energy fracture-subluxation injuries of the knee. This is thought to have clinical implications as the type of fracture pattern can indicate an associated soft-
tissue injury.
Moore retrospectively reviewed over a 1000 proximal tibia fractures to devise a classification systems based on the characteristic of five types of tibia plateau fracture patterns. He believed this system helped to better understand knee instability and concomitant soft-tissue injury. For example, Moore Type III fractures (rim avulsion) are associated with a high rate of neurovascular injury.
Figure A shows a fracture involving the entire tibial condyle. Illustration A shows a schematic diagram of the Moore classification (I - V). Illustration B shows a table that describes the Moore classification (I - V).
Incorrect Answers:

OrthoCash 2020
A 19-year-old male football player plants and twists his right lower extremity sustaining a spiral fracture of his distal third tibial shaft. Of the following images, which is most commonly associated with distal third spiral tibial shaft fractures.

The patient has a spiral distal tibial shaft fracture. Spiral distal tibial shaft fractures are commonly associated with intraarticular fracture extension, usually in the form of a posterior malleolus fracture.
Spiral distal third tibial shaft fractures need to be evaluated for intraarticular extension prior to operative management. As this can be missed on x-rays, a CT scan of the ankle is recommended to identify this associated injury. This is important when intramedullary fixation is used for definitive management, as nail insertion can displace a previously non displaced intraarticular fracture.
Anteroposterior screw fixation prior to nailing may be useful in these cases.
Boraiah et al. found that in 62 patients with spiral distal tibial fractures, 39% (24 patients) had a posterior malleolus fracture. They recommended CT evaluation of the ankle to prevent missed intraarticular fractures.
Hou et al. found a posterior malleolus fracture in 9.7% (28 out of 288 cases) of patients with tibial shaft fractures. They recommended CT or MRI evaluation of the ankle prior to surgery.
Figure A shows an axial CT scan of a right ankle with a posterior malleolus
fracture. Figure B shows an AP radiograph of a right ankle with a vertical medial malleolus fracture. Figure C shows a coronal CT scan of a right ankle with a Tillaux fracture. Figure D shows a sagittal CT scan of a right ankle with a comminuted talus fracture. Figure E shows a lateral radiograph of a right knee showing a knee dislocation. Illustration A shows an AP radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration B shows a lateral radiograph of a left distal third spiral/oblique tibial shaft fracture. Illustration C shows a sagittal CT of a distal third spiral/oblique tibial shaft fracture with a posterior malleolus fracture.
Incorrect Answers:

OrthoCash 2020
A 67-year-old female patient presents with increasing right hip/thigh pain over the past three months, which is now recalcitrant to anti-inflammatories. There is no history of trauma or constitutional symptoms. Her past medical history consists of hypertension, coronary artery disease, osteoporosis and gastric reflux. Physical examination reveals mild pain at the extremes of range of motion of the hip and a painful right sided limp. A radiograph of the right hip is seen in Figure
What would be the most appropriate treatment for this patient at this time?

Observation only
Referral to physiotherapy
MRI spine and hip
Total hip arthroplasty
Intramedullary femoral nail Corrent answer: 5
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had
been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers

OrthoCash 2020
A right-hand dominant female sustains a right proximal humerus fracture. The patient is provided a sling, and is recommended pendulum exercises with elbow range of motion to begin in 1 to 2
weeks. Which of the following would be an indication for surgical management?

Age greater than 70 years.
Fracture pattern in Figure A
Significant medical comorbidities.
Fracture pattern in Figure B
Fracture pattern in Figure C
The patient has been treated with non-operative management for her proximal humerus fracture. Operative management should be considered in patients with head splitting proximal humerus fractures and in those with dislocations that cannot be reduced.
Head splitting proximal humerus fractures should be treated with operative management. Open reduction internal fixation versus hemiarthroplasty are used to treat this type of fracture. Surgical management is also considered in proximal humerus fractures in young patients, in fractures where the greater tuberosity is displaced >5 mm, and in proximal humerus fractures associated with humeral shaft fractures.
Koval et al. studied 104 patients with one-part proximal humerus fractures treated non-operatively, and found 80% with good or excellent results. They also found that 90% of patients treated non-operatively had either no or mild pain about the shoulder at follow-up.
Lefevre-Colau et al. performed a randomized prospective study on 74 patients with an impacted proximal humerus fracture. One group was treated with early mobilization of the shoulder (within 3 days after the fracture) while the other group was immobilized for 3 weeks followed by physiotherapy. They concluded that early mobilization was safe and allowed for quicker return to functional use of the affected limb.
Figure A shows an AP radiograph of a right minimally displaced greater tuberosity proximal humerus fracture. Figure B shows AP and axillary radiographs of a right head split proximal humerus fracture that is posteriorly dislocated. Figure C shows an AP radiograph of a right minimally displaced Salter Harris II proximal humerus fracture. Illustration A shows an AP radiograph of a left valgus impacted proximal humerus fracture with a greater tuberosity fragment displaced >5mm treated with ORIF.
Incorrect Answers:

OrthoCash 2020
A 37-year-old male arrives to the trauma slot following a high-speed motorcycle crash. His Glasgow Coma score is 14 and his only orthopaedic injury is exhibited in Figure A. His current vital signs are a BP of 90/60, HR 120, and a lactate of 2.5 mMol/L. Other findings include a grade 1 splenic laceration and bilateral pulmonary contusions seen on chest radiograph. Which of the following has been suggested as an indication to perform damage control orthopedic care?

HR >110
Bilateral pulmonary contusions seen on chest radiograph
SBP = 90mmHg
Unilateral femur fracture
Lactate = 2.5 mMol/L
Pulmonary contusion severe enough to be diagnosed on chest radiograph alone is an indicator that the patient may benefit from damage control orthopaedics (DCO).
Despite the patient's overall stable nature, suffering pulmonary injury severe enough to be seen on x-ray alone suggests that temporary stabilization with staged definitive fixation may avoid potential morbidity.
Pape et al. review the evolution and balance of early total care (ETC) and DCO. Summarizing the literature, the authors report several standalone indicators that would justify DCO regardless of stable status. This includes: Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with chest trauma, multiple injuries with severe pelvic/abdominal trauma/ hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs alone, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater.
Figure A exhibits a right femoral shaft fracture. Illustration A exhibits a summarized table stating the criterion used to determine the condition of a polytrauma patient. (Table from Pape et al, PMID: 19726738)
Incorrect answers:
implement DCO.

OrthoCash 2020
A 24-year-old patient presents after a fall from the balcony of a third story building in which he landed on his feet. He reports lumbar back pain and numbness in his perineum region. Radiographs of his hips and pelvis are seen in Figure A, while CT images are shown in Figures B and C. How is this fracture pattern best classified?

Young-Burgess APC Type II
Young-Burgess LC Type I
"U" Type Spinopelvic Dissociation
Denis Zone-I
Denis Zone-II
This patient has a Denis zone-III "U" Type Spinopelvic Dissociation of the sacrum.
The Denis classification system for sacral fractures is based on anatomical fracture zones. Zone-III fractures involve the spinal canal and have a high rate of associated neurologic injury. It is important to recognize bilateral sacral
fractures with a transverse component, as this often causes spinopelvic discontinuity and possible cauda equina. The lack of mechanical continuity between the spine and pelvis will most likely require reduction and fixation for initial stability. There may also be a need for sacral decompression with fixation mechanisms given the onset of neurologic symptoms.
Mehta et al. reviewed sacral fractures. They report that patients with a transverse sacral fracture involving more proximal sacral segments (S1, S2, or S3) tend to have a higher prevalence of bladder dysfunction than do those involving distal sacral segments (S4 or S5).
Schildhauer et al. report the best way to visualize Denis zone-III "U" type fractures is to obtain a lateral view of the sacrum or sagittal reformatted images with a CT scan. Standard pelvic radiographs often miss this injury.
Figure A shows an AP pelvis with suggestion of sacral irregularities. No fracture pattern can be indentified. Figures B and C show CT scan images showing a "U" Type fracture pattern with angulation and translational displacement of the cephalad and caudad parts of the sacrum. Illustration A shows examples of complex sacral Denis zone-III fractures.
Incorrect Answers:
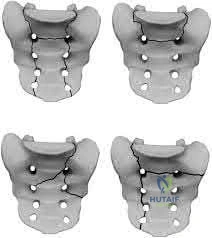
OrthoCash 2020
A 55-year-old male presents with the radiographs seen in Figures A and B after falling off his bike. Physical examination reveals an isolated, closed elbow injury. His limb is neurovascularly intact. Which complication would be most likely with surgical fixation of this injury?

Ulnar neuropathy
Posterior interosseous nerve injury
Early loss of fixation
Elbow flexion contracture
Avascular necrosis
This patient is presenting with a comminuted capitellar and trochlear fracture. If treated with open reduction internal fixation, the most likely post-operative complication would be elbow stiffness or contracture.
An axial compression force transmitted by the radial head to the capitellum with the elbow in a semiflexed position can result in a shear fracture of the anterior portion of the capitellum. AP, lateral, and radiocapitellar radiographs are recommended to identify these injuries. The lateral X-ray may reveal the “double arc” sign, which represents extension of the capitellum fracture into the trochlea. Extension of the fracture into the trochlea has important implications into the surgical approach to these injuries.
Ruchelsman et al. retrospectively reviewed the outcomes of sixteen patients with capitellar fractures treated with open reduction internal fixation. They found the presence of greater flexion contractures at the time of follow-up in elbows with Type-IV capitellar fractures. All fractures healed, and no elbows had instability or weakness with fixation.
Ring et al. retrospectively reviewed the outcomes of twenty one distal humerus articular fractures that were reduced and stabilized with implants buried beneath the articular surface. Ten patients required a second operation: (6) release of an elbow contracture; (2) treatment of ulnar neuropathy; (1) removal of hardware; (1) early loss of fixation.
Figures A and B show AP and lateral radiographs of the elbow with a comminuted fracture of the capitellum and trochlea. Note the “double arc” sign on the lateral view. Illustrations A and B show open reduction internal fixation of the fracture. Note fixation with multiple interfragmentary screws.
Incorrect Answers:

OrthoCash 2020
Figure A shows a radiograph of a 30-year-old male who underwent fixation of a left leg injury just over two years ago. He presents with persistent pain and drainage from the distal wound despite 4 months of oral antibiotics. He has no systemic symptoms. He has a past medical history of Grave's disease and Irritable Bowel Syndrome. What would be the best management at this stage?

Chronic suppressive, culture-directed, antibiotic therapy
Above knee amputation
Endocrine consultation, irrigation and debridement, removal of hardware and negative-pressure wound therapy
Irrigation and debridement, removal of hardware, over-reaming medullary canal, external fixation and culture-directed antibiotics
Irrigation and debridement, retention of hardware, acute bone grafting and culture-directed antibiotics
This is a case of fracture nonunion in the setting of chronic osteomyelitis and infected hardware. The best treatment option available would be irrigation and debridement, removal of hardware, ring external fixator and culture directed antibiotics.
The management of infected nonunion in the setting of chronic osteomyelitis is technically demanding. The aims of treatment are to eradicate the infection and obtain bone union. Non-surgical options are largely unsuccessful in patients with draining chronic osteomyeltis in the setting of infected hardware and nonunion. Surgical options involve incision and debridement of necrotic tissue followed by reconstruction of bone and possible soft tissue (to provide
healthy viable coverage). The most common techniques are ringed fixator/circular frames, staged intramedullary device with or without external fixator, free tissue transfer, or radical debridement, bone grafting, and fixation.
Motsitsi et al. reviewed the management of infected nonunion of long bones. They suggest that the Ilizarov technique is regarded as a standard treatment in infected nonunion of the tibia. When there is bone defect after debridement, the bone can be shortened or treated with bone transport.
Egol et al look at a series of patients with chronic osteomyelitis. Limb salvage should be attempted in all patients. The presence of a chronic draining sinus requires surgical debridement and culture directed antibiotics. Infected hardware should be removed. A two-stage strategy is the best and well-proven treatment option.
Figure A shows a intramedullary nail in the left tibia. There is a moderate amount of bone loss at the fracture site with mixed sclerotic bone suggestive of osteomyelitis.
Incorrect Answers:
OrthoCash 2020
A 32-year-old male sustained the injury seen in Figure A after a motor vehicle accident. Which of the following factors is most predictive of mortality with this type of injury?

Fracture classification
Number of blood transfusions in the first 24 hours
Gender
Time to operative fixation
Use of pelvic binders Corrent answer: 2
The best predictors of mortality with pelvic ring fractures include older age and hemodynamic shock at presentation. The amount of blood transfused indicates the severity of hemodynamic instability.
Pelvic ring fractures are typically high energy, blunt injuries. The leading cause of mortality with these injuries is hemorrhage and hemodynamic instability.
The most common source of hemorrhage include venous injury (80%), which is usually caused by a shearing injury of posterior thin walled venous plexus and bleeding cancellous bone. Other sources of hemorrhage include arterial injury (10-20%) from the superior gluteal artery (posterior ring injury, anterior posterior compression [APC] pattern), internal pudendal artery (anterior ring injury, lateral compression [LC] pattern) and obturator artery.
Smith et al. found fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased Injury Severity Scores (ISS) scores. Deaths were most commonly from exsanguination (<24 hours) or multiorgan failure (>24 hours).
Starr et al. demonstrated that age and shock on presentation were most predictive of mortality after pelvic ring injury.
Figure A shows a APC III pelvic fracture. Illustration A shows a table describing the Young-Burgress classification of pelvic ring fractures.
Incorrect Answers:
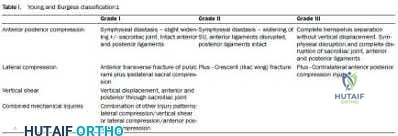
OrthoCash 2020
Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?

Early range of motion
Hinged elbow brace for 4 weeks
Repair lateral collateral ligament
Remove and upsize implant
Remove and downsize implant Corrent answer: 5
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intra-operatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by
>or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
OrthoCash 2020
Aside from improving the intramedullary nail starting point in Figure A, the use of blocking screws could have been used at the time of fixation to prevent this post-operative deformity. What would have been the correct orientation of these screw(s) in the proximal fragment?

Medial only
Lateral only
Anterior and medial
Posterior and medial
Posterior and lateral Corrent answer: 5
The clinical presentation is consistent with a malunion of a proximal one-third tibia fracture with a valgus and procurvatum deformity. The correct orientation of Poller blocking screws to help prevent this malalignment would be in the posterior and lateral aspects of the metaphyseal fragment.
Insertion of the blocking screw lateral to the nail prevents valgus deformity, and insertion of the blocking screw posterior to the nail prevents apex anterior deformity. A more lateral starting point for nail insertion can also help to
prevent valgus deformity. The semiextended position of the knee for nail insertion also helps to eliminate the tendency for the fracture to flex, due to the avoidance of excessive knee flexion during the reduction.
Stedtfeld et al. describes the mechanical model for blocking screws. They state that two or more blocking screws can be placed in each plane (AP and lateral) alongside the nail to create a narrow canal for the nail. This allows for multiple points of fixation and realignment of the bone as the nail is passed.
Lindvall et al looked at a series of 56 extra-articular proximal tibial fractures treated with intramedullary nailing or percutaneous locked plating. Neither nailing or plating these fractures showed a distinct advantage in the overall outcomes. Apex anterior malreduction however was the most prevalent form of malreduction in both groups.
Lang et al. looked at a series of proximal third tibia fracture treated with intramedullary nailing. They reported that posterior tibial comminution will also contribute to apex anterior angulation. They states this occurs when the fracture hinges on the intact cortex anteriorly during nail insertion.
Figure A shows a proximal one third tibia fracture treated with an intramedullary nail. There is malreduction of the fracture with valgus and procurvatum deformity.
Incorrect Answers:
OrthoCash 2020
When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
A fracture of the radial head requiring ORIF
A highly comminuted radial head fracture requiring radial head arthroplasty or resection
An MCL injury requiring repair
A type I avulsion fracture of the coronoid
An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture.
Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:

OrthoCash 2020
A 26-year-old female presented to the emergency department with the injury seen in Figure A after an awkward fall while intoxicated. She undergoes closed reduction and repeat radiographs are seen in Figure B. After a normal physical examination, including ranging the hip from 0-90 degrees, which of the following options would be the next most appropriate step in management?

Femoral skeletal traction
CT scan
Hip spica cast application
Observation only
Serial neurovascular examinations Corrent answer: 2
This patient has presented with a posterior left hip dislocation. The next most appropriate step would be performing a post-reduction CT scan to assess for joint reduction and congruity, associated fractures, or loose bodies.
Hip dislocations occur most commonly in young patients with high energy trauma. They are usually classified as simple or complex, with complex dislocations being those with associated fractures of the acetabulum or proximal femur. Urgent close reduction should occur within 6 hours from the time of injury. Post reduction CT scans must be performed for all traumatic hip dislocations to look for fractures or impacted areas of the femoral head or acetabulum, as well as incongruent reductions and free intra-articular joint fragments.
Calkins et al. looked at measurements of the posterior acetabulum on CT scans (the Acetabular Fracture Index) after hip dislocations to evaluate for hip stability. Hips were found to be unstable if less than 34% of the remaining posterior acetabulum was present after dislocation. Hips with greater than 55% were stable. In between 34 and 55% were indeterminate.
Moed et al. found that posterior wall fractures involving less than 20% of the posterior wall were considered stable. Fractures involving more than 40%-50% were unstable, leaving a wide range of posterior wall fractures classified as indeterminate.
Figure A shows a left posterior hip dislocation. Figure B shows a reduced left hip with no obvious fracture. Illustration A shows an axial CT scan image of the left hip. There is no acetabular fracture identified.
Incorrect Answers:

OrthoCash 2020
A 40-year-old male sustained the injury seen in Figure A, and subsequently underwent the procedure shown in Figure B. One hour post-operatively he starts to complain of pain in the operative leg, and the pain is unchanged with active or passive stretch. The external dressing is released with little resolution of symptoms. His blood pressure is 115/78 mm Hg with compartment pressures in the leg measuring 31 to 35 mm Hg. His ABI index is 1.1 in the leg. What would be the next step in management?

MRI angiography of leg
Four-compartment fasciotomy
Follow-up examination the following day
Continued monitoring and serial examinations
EMG study
The patient is at risk for developing compartment syndrome of the leg. The next most appropriate step would be to support his systemic blood pressure and monitor compartment pressures.
A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy. However, the treatment of early compartment syndrome should be to initially improve the limbs perfusion pressure gradient. This can be done by treating underlying factors such as hypotension, coagulopathy, or vascular compromise due to either a true vascular injury or artificially by external compression. Frequent reassessment is then critical to effectively manage these patients. If clinical
diagnosis persists despite these efforts, urgent fasciotomy would be considered.
McQueen looked at 116 patients with tibial diaphyseal fractures who had continuous monitoring of anterior compartment pressure for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of 30 mmHg is a more reliable indicator of compartment syndrome.
White et al. looked at 101 patients with tibial fractures with satisfactory Delta P measurements. THey found that patients with elevated intramuscular pressures >30 mm Hg after tibial fracture do not have a greater incidence of complications than those with low pressures, so long that Delta P <30 mm Hg.
Figure A shows a Shatzker V tibial plateau fracture. Figure B shows fixation of fracture seen in Figure A.
Incorrect Answers:
OrthoCash 2020
A 10-year-old girl suffers a displaced tibia fracture. Initial numbness over the dorsum of the the foot resolved following an anatomic closed reduction and placement in a long leg cast performed in the emergency room. The cast was placed with the the ankle dorsiflexed just above neutral to prevent equinus contracture and then the cast and padding was adequately bivalved. Overnight, the patient began experiencing recurrent numbness and paresthesias in her exposed toes and a slight increase in her pain at the fracture site. Your next best step would be:
Repeat closed reduction under conscious sedation
Selective compartment fasciotomies
External fixation and compartment monitoring
compartment fasciotomies with fracture fixation done emergently
Modify the cast to reposition the ankle into slight plantarflexion Corrent answer: 5
Circumferential casting with the ankle dorsiflexed can cause increased intracompartmental pressures in the leg. However, this patient's cast has been adequately bivalved during initial cast placement. Therefore, the next best step is cast modification to allow the ankle to assume an angle between neutral and 30 degrees of plantar flexion and further reducing the compartment pressure.
Tibia fractures are one of many common underlying etiologies for the development of compartment syndrome in the leg. Fracture reduction as well as eliminating circumferential dressings are important early preventative steps to take. Bivalving casts - including splitting the cast padding - is often indicated in fractures of long bones that are treated with initial casting. While casting patients in a plantigrade or dorsiflexed position reduces the risk of equinus contractures and holds the ankle mortise reduced, dorsiflexing the ankle has been shown to increase the intracompartmental pressures throughout the leg compartments.
Weiner et al. placed pressure monitors into the anterior and deep posterior compartments in healthy volunteers to measure the effects of casting on compartment pressures. They found that the intramuscular pressures were lowest with the ankle positioned between plantigrade and a resting plantar flexion position (0-37 degrees), and that bivalving the cast reduced the pressures 33-47%.
Illustration A shows the needle trajectories for compartment pressure monitoring in the leg. This should be performed within 5 cm of the fracture to get accurate peak pressures.
Incorrect Answers:
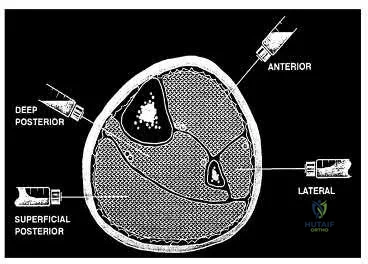
OrthoCash 2020
A 35-year-old male horseback rider was bucked into the air and then landed forcefully with his perineum on the saddlehorn of the saddle. At a one year follow-up, the only long term sequela of his injuries is erectile dysfunction. Which radiographic injury seen in Figures A-E is most commonly associated with this complication?

This patient has sustained a saddle-horn injury to the pelvis. An anterior posterior compression (APC) injury is the most common pelvic injury associated with this mechanism.
Saddle-horn injury to the pelvis occurs when a horseback rider is bucked into the air and then lands forcefully with his or her perineum on the saddlehorn of the saddle. The bony injury to the pelvis usually consists of a diastasis of the pubic symphysis with/without subsequent widening of the sacroiliac joints. The
majority of patients are able to return close to their pre-injury level of employment and activity after these injuries. However, sexual dysfunction is a common complication with this injury. Sexual dysfunction can be due to urethral, vascular, neurologic, and psychogenic injuries.
Collinge et al. looked at a series of male patients with injuries to the perineum after coming into contact with the saddle or saddle horn on a horse. Eighteen of the twenty patients were found to have sexual dysfunction at the time of the latest follow-up. A multi-disciplinary approach to these patients is needed when treating pelvic injuries.
Cannada et al. surveyed 71 women of childbearing age who had a pelvic fracture. She found that half the patients reported physical genitourinary complaints with 38 percent of women noting new onset pain with intercourse. In terms of psychological impact, they showed that 45 percent of patients answered affirmatively to decreased interest in intercourse and decreased orgasm frequency after the injury.
van Nieuwenhoven et al. describe three equestrians who suffered from straddle injuries with symphysis diastasis and rupture of sacroiliac ligaments after falls or kicks from horses. They show that these presumed low-energy injuries can cause extremely severe injuries to the pelvis itself and to the adjacent organs.
Figure A shows a Burgess APC Type II pelvic fracture. Figure B shows left ASIS avulsion fracture. Figure C shows a left hip dislocation. No pelvic fracture is identified. Figure D shows a subacute superior/inferior pubic rami fracture.
Figure E shows a right femoral neck fracture.
Incorrect Answers:
OrthoCash 2020
A 31-year-old male driver was involved in a high-speed motor vehicle accident. His injuries include a left subdural hematoma (Abbreviated Injury Score [AIS]=4), left segmental femur fracture (AIS=3), ruptured spleen (AIS=4), nasal fracture (AIS=2), fractured left ribs 4 to 7 (AIS=2), and a closed pelvic ring fracture (AIS=3). What is his Injury Severity Score (ISS)?
Question 94
A 55-year-old woman develops posttraumatic arthritis in the elbow following a distal humerus fracture. What is the most likely mid-term (5-10 years after surgery) complication following semiconstrained total elbow arthroplasty (TEA)?
Explanation
intermediate-term follow-up.
Question 95
What property of titanium alloys accounts for their high corrosion resistance in vivo?
Explanation
REFERENCES: Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott, 2003, vol 1, pp 269-278.
Lemons JE: Metallic alloys, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 19-27.
Question 96
What is the treatment recommendation for an American Joint Committee on Cancer stage IIB (Enneking stage IIB) malignant fibrous histiocytoma of bone?
Explanation
Question 97
A 4-year-old child sustains a spiral fracture to the tibia in an unwitnessed fall. History reveals three other fractures to long bones, and the parents are vague about the etiology of each. There is no family history of bone disease. The parents ask if the child has osteogenesis imperfecta (OI); however, there are no clinical or radiographic indications of this diagnosis. In addition to fracture care, management should include
Explanation
REFERENCES: Rockwood CA, Wilkins KE, King RE (eds): Fractures in Children. Philadelphia, PA, JB Lippincott, 1984, vol 3, pp 173-175.
Kempe CH, Silverman FN, Stelle BF, Droegemueller W, Silver HK: The battered-child syndrome. JAMA 1962;181:17-24.
Akbarnia BA, Akbarnia NO: The role of the orthopedist in child abuse and neglect. Orthop Clin North Am 1976;7:733-742.
Question 98
Figures 11a and 11b show the T2-weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a? Review Topic
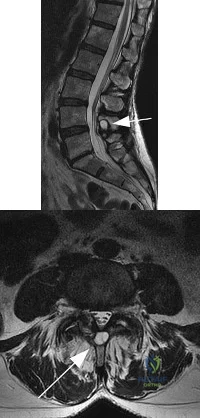
Explanation
Question 99
A 40-year-old man is thrown off his motorcycle and sustains an open Type IIIA fracture shown in Figure A. He is taken to the operating room for debridement and reamed intramedullary nailing with a 10mm diameter nail. He returns at 10 months with persistent pain at the fracture site with ambulation. Examination reveals healed wounds with no erythema, warmth or tenderness. Erythrocyte sedimentation rate and C-reactive protein levels are within normal limits. Radiographs taken at that time are shown in Figure B. What is the next best treatment step?

Explanation
Tibial delayed union can be defined as lack of union from 20-26 weeks post-injury, while nonunion is defined as lack of healing at >9mths post-injury, or absence of progressive signs of healing on radiographs for 3 consecutive months. Persistent pain is a symptom of nonunion. ESR and CRP are performed to rule out infection.
Bhandari et al. performed a blinded, multicenter trial on 622 reamed tibial nails and 604 unreamed tibial nails. In closed fractures, patients in the unreamed nail group were at greater risk of primary events than the reamed nail group. There was no difference in groups for open fractures. Primary events were defined as bone-grafting, implant exchange/removal, dynamization, and debridement.
Hak reviewed aseptic tibial nonunion. They discuss exchanged reamed nailing for diaphyseal nonunion, adjunctive plate fixation for metaphyseal nonunion, and nail removal and plating for metadiaphyseal nonunion, external fixation for infected nonunion and distraction osteogenesis of defects.
Figure A shows a mid-diaphyseal tibial fracture Figure B shows nonunion following
IM nailing of the fracture. Illustration A shows union following exchange nailing with a larger 12mm diameter nail.
Incorrect Answers:
Question 100
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of
Explanation
REFERENCES: Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
Brumback RJ, Ellison TS, Poka A, et al: Intramedullary nailing of femoral shaft fractures: Part III. Long-term effects of static interlocking fixation. J Bone Joint Surg Am 1992;74:106-112.
