Orthopedic Surgery Board Review MCQs: Arthroplasty, Trauma & Sports Medicine | Part 111

Key Takeaway
This page offers Part 111 of a comprehensive Orthopedic Surgery Board Review. It includes 100 high-yield, verified MCQs for orthopedic surgeons and residents preparing for OITE and AAOS certification. Leverage interactive Study and Exam Modes to master key topics such as Arthroplasty, Fracture, and Knee.
About This Board Review Set
This is Part 111 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 111
This module focuses heavily on: Arthroplasty, Fracture, Knee, Ligament, Shoulder.
Sample Questions from This Set
Sample Question 1: Second impact syndrome (SIS) after head injury is characterized by which of the following?...
Sample Question 2: Figure 21 shows the tomogram of a 26-year-old woman who sustained an axial load injury to her neck in a fall off a horse. What ligament is injured?...
Sample Question 3: An 18-year-old man was in a motor vehicle accident and sustained a closed head injury, right displaced scapular body and glenoid fractures, a right proximal humeral fracture, fractures of ribs one through three, facial fractures, and bilate...
Sample Question 4: Reverse total shoulder arthroplasty with a latissimus dorsi transfer would be the most appropriate treatment for which of the following patients? Review Topic...
Sample Question 5: A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d sho...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
REFERENCES: Cantu RC: Second-impact syndrome. Clin Sports Med 1998;17:37-44.
Saunders RL, Harbaugh RE: Second impact in catastrophic contact-sports head trauma. JAMA 1984;252:538-539.
Stevenson KL, Adelson PD: Pediatric sports-related head injuries, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, vol 1, p 781.
Question 2
Figure 21 shows the tomogram of a 26-year-old woman who sustained an axial load injury to her neck in a fall off a horse. What ligament is injured?
Explanation
REFERENCES: Levine AM, Edwards CC: Fractures of the atlas. J Bone Joint Surg Am 1991;73:680-691.
Kurz LT: Fractures of the first cervical vertebra, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 409-413.
Question 3
An 18-year-old man was in a motor vehicle accident and sustained a closed head injury, right displaced scapular body and glenoid fractures, a right proximal humeral fracture, fractures of ribs one through three, facial fractures, and bilateral pubic rami fractures with minimal displacement. He has a systolic blood pressure of 80/40 mm Hg despite fluid resuscitation. A radiograph is shown in Figure 17. Spiral CT does not identify any thoracic or abdominal injuries. What is the next most appropriate step in management?
Explanation
REFERENCES: Althausen PL, Lee MA, Finkemeier CG: Scapulothoracic dissociation: Diagnosis and treatment. Clin Orthop 2003;416:237-244.
Witz M, Korzets Z, Lehmann J: Traumatic scapulothoracic dissociation. J Cardiovasc Surg 2000;41:927-929.
Question 4
Reverse total shoulder arthroplasty with a latissimus dorsi transfer would be the most appropriate treatment for which of the following patients? Review Topic
Explanation
R-TSA has become the mainstay treatment for rotator cuff arthropathy. In the presence of severe loss of active elevation and external rotation, combined latisimus dorsi transfer and reverse total shoulder arthroplasty can restore elevation and external rotation, respectively. This may be used in the primary or revision setting.
Frankle et al. report the results of sixty patients with rotator cuff deficiency and glenohumeral arthritis who were followed for a minimum of two years. All were
treated with R-TSA. Their study showed that forward flexion increased from 55 to
105 degrees, and abduction increased from 41 to 102 degrees.
Boileau et al. followed 45 patients with severe cuff tear arthropathy and advanced atrophy/fatty infiltration of the infraspinatus or teres minor muscles. All patients were treated with R-TSA and a modified L'Episcopo procedure (latissimus dorsi and teres major transfer). Mean active elevation increased from 74 degrees preoperatively to
149 postoperatively, and external rotation increased from -21 to 13 degrees.
Illustrations A and B show the classic findings of rotator cuff arthropathy. There is significant acromial acetabularization and femoralization of humeral head. Other features include: asymmetric superior glenoid wear, osteopenia, "snowcap sign" due to subchondral sclerosis and anterosuperior escape. Illustration C shows a left shoulder after conversion from hemiarthroplasty to reverse total shoulder arthropathy.
Incorrect Answers:
Question 5
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T 1 -weighted, sagittal T 2 -weighted, axial T 1 -weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA,
WB Saunders, 2002, pp 4241-4252.
Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:1-11.
Question 6
9 degress Celsius, serum WBC is 14,000, and his C-reactive protein is elevated. He reports that he uses IV heroin. A coronal 3D CT scan of the left clavicle is shown in Figure B. Joint aspiration shows many grams stain positive organisms. Which of the following organisms is the most likely pathogen?

Explanation
Ross et al states "Staphylococcus aureus is now the major cause of
sternoclavicular septic arthritis in intravenous drug users. Pseudomonas aeruginosa infection in injection drug users declined dramatically with the end of an epidemic of pentazocine abuse in the 1980s."
The referenced article by Goldin et al is from the New England Journal of Medicine reports that all of their cases of SC joint septic arthritis were in intravenous drug abusers and that P. aeruginosa grew out of 3 patients and S. aureus grew out of 1 patient.
A more recent article by Abu Arab et al reported that Staph aureus was most common even in IV drug users. The review article by Higginbotham and Kuhn note that risk factors for SC joint septic arthritis include hemodialysis, immunocompromise, alcoholism, and HIV. Neisseria gonorrhoeae, fungal, and candida present in HIV patients.
Treatment is I&D and appropriate antibiotics, although aspiration and abx have shown some success too. CT and MRI are useful in diagnosis, and open biopsy or aspiration is recommended for definitive diagnosis.
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?
Degenerative lumbar spine changes
Ipsilateral ankle pain and stiffness
Ipsilateral hip joint degenerative changes
Contralateral hip joint degenerative changes
Ipsilateral medial knee degenerative changes Correct answer: 2
A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted
that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
A 33-year-old man sustains a femur fracture in a motorcycle accident. AP and lateral radiographs are provided in Figure A. Prior to surgery, a CT scan of the knee is ordered for preoperative planning. Which of the following additional findings is most likely to be discovered?

Tibial eminence fracture
Sagittal plane fracture of the medial femoral condyle
Schatzker I tibia plateau fracture
Coronal plane fracture of the lateral femoral condyle
Axial plane fracture through the medial femoral condyle Correct answer: 4
The "Hoffa fracture" is a coronal plane fracture of the femoral condyle that is often missed on plain radiographs of supracondylar and intercondylar femur fractures. It involves the lateral condyle more frequently than the medial.
Identification is important as it may impact operative planning and likely require screw fixation in the anteroposterior plane.
Nork et al. reviewed 202 supracondylar-intercondylar distal femoral fractures and found a 38% prevalence of associated coronal plane fractures. The authors recommend CT scan imaging of all supracondylar and intercondylar fractures.
Ostermann et al reported on 24 unicondylar fractures of the distal femur treated with open reduction internal fixation with a screw construct. Twenty-
three patients acheived satisfactory results at 5 year follow-up. Illustrations A and B are another example of a supracondylar femur fracture with an associated Hoffa fracture identified on CT scan.

A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
closed reduction and early range of motion
radial head resection and lateral collateral ligament reconstruction
radial head resection and coronoid open reduction internal fixation
radial head arthroplasty and coronoid open reduction internal fixation
radial head arthroplasty, coronoid open reduction internal fixation, and lateral collateral ligament repair
A terrible triad of the elbow includes dislocation of the elbow with associated fractures of the radial head and the coronoid process. Ring et al. stressed that these injuries are prone to complications and advised against resection of the radial head due to instability, and instead recommended a radial head replacement if too comminuted for ORIF. Coronoid fractures compromise elbow stability as well and require open reduction and internal fixation as with the lateral collateral ligament. McKee et al. showed stable elbows in 34/36 with mean Mayo elbow score of 88 when the standard protocol of coronoid ORIF, radial head repair/replacement, and LCL repair were employed.
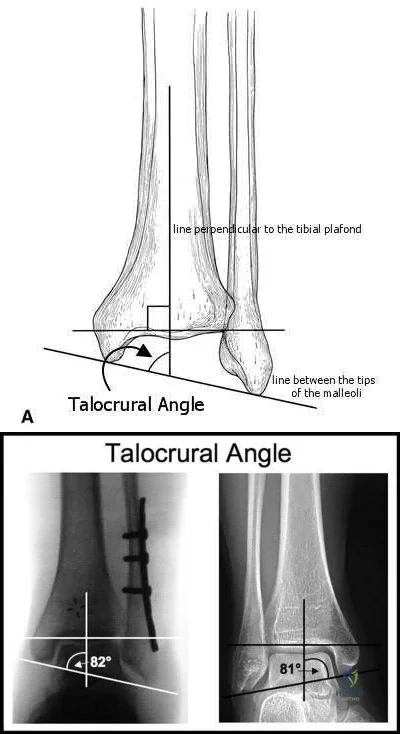
The talocrural angle of an ankle mortise x-ray is formed between a line perpendicular to the tibial plafond and a line drawn:
perpendicular to the medial clear space
parallel to the talar body
between the tips of the malleoli
perpendicular to the shaft of the fibular
parallel to the subtalar joint Correct answer: 3
The talocrural angle is formed by the intersection of a line perpendicular to the plafond with a line drawn between the malleoli (average = 83+/-4deg). When the lateral malleolus is shortened secondary to fracture, this can lead to increased talocrural angle. This malunion leads to lateral tilt of the talus.
Phillips et al looked at 138 patients with a closed grade-4 supination-external rotation or pronation-external rotation ankle fracture. Although the conclusions were limited due to poor follow up, they found the difference in the talocrural angle between the injured and normal sides was a statistically significant radiographic indicator of a good prognosis.
Pettrone et al looked at a series of 146 displaced ankle fractures, and the effect of open or closed treatment, and internal fixation of one or both malleoli. They found open reduction proved superior to closed reduction, and in bimalleolar fractures open reduction of both malleoli was better than fixing only the medial side.
Illustrations A and B are demonstrations of the talocrural angle.
A 33-year-old male sustains the injury shown in Figure A. He is initially treated with a spanning external fixator followed by definitive open reduction internal fixation of the tibia and fibula. His wounds healed without infection or other complications. Two years following surgery, which of the following parameters will most likely predict a poor clinical outcome and inability to return to work?

Joint line restoration
Degree of fracture displacement
Time before definitive ORIF
Open fracture
Lower level of education Correct answer: 5
Lower level of education is the parameter that correlated most closely with a poor clinical outcome and inability to return to work.
To determine what fracture- and patient-specific variables affect outcome, Williams et al evaluated 29 patients with 32 tibial plafond fractures at a minimum of 2 years from the time of injury. Outcome was assessed by four independent measures: a radiographic arthrosis score, a subjective ankle score, the Short Form-36 (SF-36), and the patient’s ability to return to work. The four outcome measures did not correlate with each other. Radiographic arthrosis was predicted best by severity of injury and accuracy of reduction. However, these variables did not show any significant relationship to the clinical ankle score, the SF-36, or return to work. These outcome measures were more influenced by patient-specific socioeconomic factors. Higher ankle
scores were seen in patients with college degrees and lower scores were seen in patients with a work-related injury. The ability to return to work was affected by the patient’s level of education.
Pollak et al performed a retrospective cohort analysis of pilon fractures. Patient, injury, and treatment characteristics were recorded. The primary outcomes that were measured included general health, walking ability, limitation of range of motion, pain, and stair-climbing ability. A secondary outcome measure was employment status. Multivariate analyses revealed that presence of two or more comorbidities, being married, having an annual personal income of less than $25,000, not having attained a high-school diploma, and having been treated with external fixation with or without limited internal fixation were significantly related to poorer results as reflected by at least two of the five primary outcome measures.
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?
Irrigation and local wound care in the emergency department
Emergent irrigation and debridement in the operating room with vacuum-assisted wound closure
Emergent irrigation and debridement in the operating room with 7 days of intravenous antibiotics
Wound closure in the emergency department with follow-up wound check in 1 week
Exploration and removal of all bullet fragments in the emergency department and 10 day course of oral antibiotics
The question refers to appropriate management of a gunshot wound to the forearm. The first question that must be answered when evaluating gunshot injuries is whether the gunshot is low velocity or high velocity. Low-velocity wounds are less severe, are more common in the civilian population, and are typically attributed to bullets with muzzle velocities below 1,000 to 2,000 feet per second. Tissue damage is usually more substantial with higher-velocity (greater than 2,000 to 3,000 fps) military and hunting weapons. In this question, a muzzle velocity of 1,000 ft/sec is provided. Low velocity injuries with stable, non-operative fractures can be treated with local wound care.
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds.
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?
pulselessness
pallor
paresthesia
paralysis
increasing analgesia requirement Correct answer: 5
Although pain, pallor, paresthesia, paralysis, and pulselessness are all possible signs and symptoms of compartment syndrome in children with fractures, studies have shown increasing analgesia requirement is more sensitive.
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of
compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
A 45-year-old man sustains the injury seen in Figures A and B following a motor vehicle accident. Postoperative radiographs are seen in Figures C and D. Which of the following is the most accurate when comparing outcomes between intramedullary nailing (IMN) and open reduction internal fixation (ORIF) for this injury?

Union rates at one year are higher with ORIF
Infection rates are higher with IMN
Functional shoulder outcomes at one year are equivalent with IMN and ORIF
Iatrogenic radial nerve injury rate is higher with ORIF
Shoulder stiffness rates at one year are equivalent with IMN and ORIF Correct answer: 3
Although shoulder pain and stiffness is increased following IMN compared to ORIF, functional outcome scores at one year have been shown to be equivalent
in both treatment groups.
Diaphyseal humeral shaft fractures outcomes following IMN and ORIF are under further investigation. Diaphyseal humeral shaft fractures have historically been treated with ORIF, however proponents for IMN cite benefits of less periosteal stripping and soft tissue dissection. Recent investigations have shown outcomes with regard to nonunion, infection, re-operation, and nerve palsy appear equivalent between both groups. Rates of shoulder stiffness and shoulder pain have been demonstrated to be higher in IMN compared to ORIF. American Shoulder and Elbow Scores (ASES) have shown no difference at one year post-operatively.
Bhandari et al. performed a meta-anaylsis of 3 prospective randomized trials. They found lower rates of re-operation and shoulder impingement with ORIF of humeral shaft fractures.
Wali et al. performed a prospective randomized study of IMN or ORIF on 50 patients with mid-diaphyseal humeral shaft fractures. They found IMN had shorter operative time, shorter hospital stay, and lower blood loss. They found no difference in union rates, complication, or shoulder functional outcomes scores. They conclude IMN to be an effective option for treating mid-diaphyseal humeral shaft fractures.
Heineman et al. have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF. The authors found no significant difference between the two treatment modalities for the secondary outcomes (nonunion, infection, nerve palsy, re-operation).
Figures A and B show a diaphyseal humeral shaft fracture. Figure C and D show postoperative radiographs following intramedullary nailing of a humeral shaft fracture.
Incorrect Answers:
A 25-year-old female presents complaining of progressive anteromedial pain in her left ankle. She underwent operative fixation 5 months prior at an outside hospital. The operative report indicated that, due to anterior fracture blisters, a direct medial incision was utilized, centered over the posterior colliculus of the medial malleolus, without violation of the deltoid ligament. A radiograph and computed tomographic scan of her initial injury are shown in Figures A and B, respectively. On exam, she has well-healed incisions, exhibits no tenderness to palpation over her hardware, but does endorse pain with deep palpation along the anteromedial joint line. Figure C shows an anteroposterior left ankle radiograph taken today. Labs are obtained and reveal a white blood cell count of 9.0 k/uL (reference range 4.5-11.0 k/uL) and a C-reactive protein value of 0.8 mg/dL (<0.9 mg/dL). What is the next best step in managing her problem?

Syndesmotic fixation
Intra-articular corticosteroid injection
Referral to physical therapy
Surgical correction of malunion
Removal of hardware Correct answer: 4
This patient sustained a supination-adduction (SAD) injury with a vertical shear fracture of her medial malleolus and a fibular avulsion fracture. She sustained a medial plafond articular impaction injury that was not addressed at the time of surgery.
In SAD injuries, supination of the foot is combined with inward rotation at the ankle, adduction of the hindfoot, and inversion of the forefoot. This results in the following sequence of events: 1. Talofibular sprain or distal fibular avulsion (equivalent to Weber A). 2. Vertical medial malleolus fracture as the talus strikes the tibia. Associated injuries may include osteochondral damage to the talus and marginal impaction of the medial plafond. It is important to evaluate the medial plafond for articular impaction. When present, an arthrotomy must be performed, typically utilizing an anteromedial incision, with direct visualization of the articular surface to restore the joint line appropriately.
Weber et al. provided a review article on corrective osteotomies for malleolar fracture malunions. They stress that malunions can lead to ankle instability, abnormal load transfer, and post-traumatic arthritis. They conclude that corrective osteotomies that restore anatomical alignment show good results in long-term follow-up.
Perera et al. provided additional commentary on the surgical reconstruction of malunited ankle fractures. The authors emphasize the link between malunion and poor outcomes. They state that successful salvage procedures involve a clear understanding of the deformity, careful preoperative planning, and a solid understanding of reconstructive techniques. They provide several instructive case examples in their review.
McConnell et al. provided a discussion on SAD ankle fractures at their institution and emphasized the importance of recognizing marginal impaction of the tibial plafond when treating these injuries. Of 800 ankle fractures identified over a 5-year period, 44 were SAD injuries, 19 of the 44 displayed a vertical shear fracture of the medial malleolus, and 8 of the 19 demonstrated marginal impaction of the tibial plafond. These 8 impaction injuries were treated with open reduction internal fixation with elevation of the articular impaction; all had good to excellent outcomes without arthritic changes at last
follow-up.
Figure A is an anteroposterior left ankle radiograph demonstrating a SAD injury with a vertical shear fracture of the medial malleolus, a fibular avulsion fracture, and articular impaction of the medial tibial plafond. Figure B is a coronal CT demonstrating articular impaction of the medial plafond. Illustration A is an intra-operative photograph with the medial malleolus retracted allowing inspection of the articular surface; mild anteromedial plafond impaction is present.
Incorrect Answers:

A 90-year-old female slips and falls at home. She is a community ambulator and has no medical problems. She reports right hip pain at this time. Injury radiographs are shown in Figures A & B. Delay of more than 48 hours may result in:

Increased intraoperative time
Increased 30-day mortality
No impact on the rate of postoperative pneumonia
Higher rates of blood transfusion
Increased risk of post-operative infection Correct answer: 2
Figures A & B demonstrate a right, unstable intertrochanteric femur fracture. Surgical stabilization within 48 hours improves short-term and 30-day mortality.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:

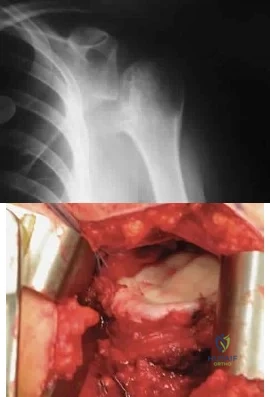
A 22-year-old healthy left hand dominant male presents to the ED with left shoulder pain after falling from an ATV. Figure A is the radiograph of his left clavicle. He is neurovascularly intact and there is no evidence of skin tenting or open fracture. Which of the following most predisposes this patient to nonunion?

Diaphyseal fracture
Fracture displacement
Age
Male Gender
Injury involving the dominant extremity Correct answer: 2
Displaced clavicle fractures are associated with higher rates of nonunion.
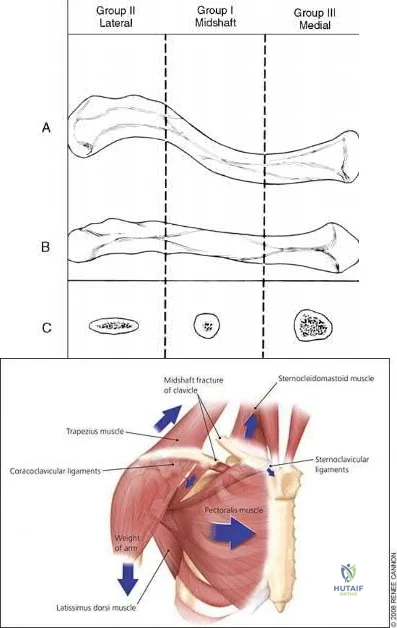
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
A 24-year-old male presents with ankle pain after being involved in a motor vehicle accident. His injury radiograph is shown in Figure A. Which of the following has been shown to contribute to the development of post-traumatic arthritis in this injury pattern?

Initial superficial zone cartilage cell death via apoptosis at the fracture margins
Initial superficial zone cartilage cell death via apoptosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis at the fracture margins
Delayed superficial zone cartilage cell death via necrosis at the fracture margins
Figure A demonstrates a tibial plafond fracture. Initial superficial zone cartilage cell death via necrosis at the fracture margins has been shown to contribute to post-traumatic arthritis.
Post-traumatic osteoarthritis typically occurs after an intra-articular fracture. Impacted chondrocytes die by either necrosis or apoptosis, which have both been implicated in post-traumatic osteoarthritis. Initial cell death in the superficial cartilage zones at the fracture margins occurs by necrosis. Apoptosis occurs in a delayed fashion and is mitigated by several bioactive agents.
Apoptosis also affects the superficial cartilage zones near the fracture margins. Deep cartilaginous zones and areas away from the fracture margins do not seem to be involved in these processes.
McKinley et al. performed a review of the basic science of intra-articular fractures and posttraumatic osteoarthritis. They report that initial damage to the cartilage in combination with the ensuing pathomechanical and pathobiologic response of the cartilage after a fracture contribute to posttraumatic arthritis. Chronic abnormal joint loading is also thought to contribute to this process as well. They conclude that the relative contribution of each is unknown.
Tochigi et al. performed a study to determine the distribution and progression of chondrocyte damage after intra-articular ankle fractures. They harvested 7 normal human ankles and subjected them to impaction. They found that immediate superficial zone chondrocyte death was greater in fracture-edge regions than on-fracture regions. Subsequent cell death over the next 48 hours was significantly higher in fracture-edge regions as well. They conclude that cartilage damage in intra-articular fractures was characterized by chondrocyte death at fracture margins.
Figure A is an ankle mortise radiograph demonstrating an intra-articular tibial plafond fracture.
Incorrect Answers:
A 35-year-old male presents with left knee pain after sustaining the injury seen in Figure A. He is neurovascularly intact and can perform a straight leg raise, but has pain with passive range of motion. Figures B and C show an anteroposterior and lateral radiograph of the left knee, respectively. 175 cc of saline is injected into the superolateral quadrant with no egress of fluid from the inferolateral
laceration. What percentage of traumatic arthrotomies would be detected with this test?

Question 7
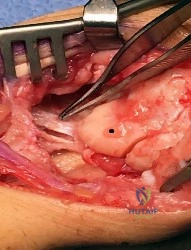
Figure 1 depicts an intraoperative photograph obtained following proximal row carpectomy. The black dot denotes the capitate. The top of the figure is radial and the bottom of the figure is ulnar. Surgical disruption of the structure identified by the forceps would result in
Explanation
The structure identified by the forceps is the radioscaphocapitate ligament. During a proximal row carpectomy, it is very important to identify and protect this ligament. Compromise of the ligament would result in ulnar translocation of the carpus and early failure of the proximal row carpectomy procedure. If the ligament is injured during surgery, immediate repair should be performed. Green and associates discuss the importance of the radioscaphocapitate ligament in stabilizing the carpus after this procedure is performed. Nakamura and associates compared 3-mm, 6-mm, and 10-mm radial styloidectomies, and only the 3-mm styloidectomy subsequently preserved carpal stability. Compromise of the radioscaphocapitate ligament occurred when larger portions of the radial styloid were excised. Distal radioulnar joint instability would result only from the disruption of the distal radioulnar joint stabilizers. Avascular necrosis would not occur, because the capitate receives its blood supply mainly from the palmar vessels. Finally, loss of active thumb IP flexion would not occur, because the flexor pollicis longus tendon would remain intact even if ligament compromise were to occur.
Question 8
03 A 28-year-old man underwent surgical fixation for an intra-articular distal humeral fracture 8 weeks ago now reports progressively restricted elbow motion. Radiographs at the time of union are shown in Figures 13a and 13b. Management should now consist of
Explanation
delayed until the heterotopic ossification was “mature”. This was signified by a cold bone scan and normal serum alk phos, as well as a mature appearance on xray. It was thought that by waiting until the HO was mature, recurrence would be avoided. However, in the cited reference, out of the widely read Journal of Hand Surgery, the authors obtained good results with increased range of motion, resolution of cubital tunnel syndrome and no recurrence of contractures or loss of motion with excision of ectopic bone and elbow release that was performed once bony union of fracture was obtained. They also used a 5 day course of indomethacin post-op.
back to this question next question
Question 9
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function? Review Topic
Explanation
Question 10
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What test should be performed to aid in this diagnosis?
Explanation
Question 11
In hybrid arthroplasty, the use of a polymethylmethacrylate (PMMA) precoated femoral component has been shown to result in
Explanation
REFERENCES: Sporer SM, Callaghan JJ, Olejniczak JP, Goetz DD, Johnston RC: The effects of surface roughness and polymethylmethacrylate precoating on the radiographic and clinical results of the Iowa hip prosthesis: A study of patients less than fifty years old. J Bone Joint Surg Am 1999;81:481-492.
Schulte KR, Callaghan JJ, Kelley SS, Johnston RC: The outcome of Charnley total hip arthroplasty with cement after a minimum twenty-year follow-up: The results of one surgeon. J Bone Joint Surg Am 1993;75:961-975.
Question 12
A 20-year-old basketball player reports a 6-month history of right groin pain that radiates into his testicles with activities of daily living. He denies any history of trauma. Examination reveals tenderness about the groin, and he has full hip range of motion. The abdomen is soft. Radiographs are normal. Nonsurgical management has consisted of rest and physical therapy, but he continues to have pain. What is the next step in management?
Explanation
REFERENCES: Kluin J, den Hoed PT, van Linschoten R, et al: Endoscopic evaluation and treatment of groin pain in the athlete. Am J Sports Med 2004;32:944-949.
Genitsaris M, Goulimaris I, Sikas N: Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238-1242.
Meyers WC, Foley DP, Garrett WE, et al: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Question 13
Five weeks after the patient completes a 6-week course of antibiotics, his ESR is 24 mm/h and CRP level is 10 mg/L, which is similar to the levels at 6 weeks. What is the most appropriate treatment at this time?
Explanation
This patient has both serologic and synovial fluid findings that are concerning for indolent infection. He was taking antibiotics at the time of aspiration. The AAOS clinical practice guideline, The Diagnosis of Periprosthetic Joint Infections of the Hip and Knee, suggests that patients discontinue antibiotics for a minimum of 2 weeks and that a repeat aspiration should be performed in cases of contradictory findings. In this situation, the cell count is elevated
along with an elevated ESR and CRP level. As a result, the appropriate treatment at this time is to reaspirate his hip.
This patient has a periprosthetic joint infection with a draining sinus tract. He has had symptoms for several months and, as a result, irrigation and debridement are not indicated. A single-stage surgery may be performed in some centers for healthy patients with susceptible organisms. However, single-stage reconstructions are generally performed with cemented implants in patients without a draining sinus tract. A 2-stage procedure with an antibiotic spacer is the surgical treatment modality most likely to eradicate this infection.
Serologic findings have significantly improved since the time of the prior surgical procedure. Surgical intervention does not need to be delayed until these values have completely normalized.
Question 14
Figure 1 is the radiograph of a 50-year old woman with lateral-sided left knee pain. She noticed the pain over the last few months and has had no new injury. She had a microfracture performed of her lateral femoral condyle 5 years ago. What is the likely cause of the finding noted on her radiograph?

Explanation
Question 15
A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a
Explanation
REFERENCES: Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Mink JH, Deutsch AL: The knee, in MRI of the Musculoskeletal System, ed 1. New York, NY, Raven Press, 1990, pp 251-387.
Question 16
A 35-year-old female runner reports progressive vague aching pain involving her midfoot. Her pain is most notable when running. She denies specific injury. Examination reveals minimal swelling and localized tenderness over the dorsal medial midfoot and navicular. Radiographs and an MRI scan are shown in Figures 37a through 37c. What is the most appropriate management?
Explanation
REFERENCES: Lee A, Anderson R: Stress fractures of the tarsal navicular. Foot Ankle Clin 2004;9:85-104.
Coughlin M: Tarsal navicular stress fractures. Tech Foot Ankle Surg 2002;1:112-122.
Question 17
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
REFERENCES: Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186.
Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
Question 18
Surgical arthroscopy performed 1 week after injury presents increased risk for
Explanation
The MR images show injuries to the ACL, PCL, and PLC consistent with a knee dislocation. The optimal timing of surgery after multiligament knee injury remains unclear. Two systematic reviews demonstrated superior clinical outcome scores after early treatment, including higher mean Lysholm scores and a higher percentage of good/excellent International
Knee Documentation Committee scores. Early treatment was associated with increased residual anterior knee instability but no difference in posterior instability, varus laxity, or valgus laxity. Although numbers were limited, the average range of motion and rate of extension loss of at least 5 degrees was similar between groups. More patients in the early-treatment group demonstrated a higher rate of flexion loss of 10 or more degrees and an increased need to undergo a second procedure to address arthrofibrosis, including manipulation under anesthesia and arthrolysis. Return to work did not significantly differ between groups, but return to sports was lower in the early-treatment group. Evidence demonstrates a higher rate of low-energy mechanisms resulting in multiligament knee injury and an increased odds ratio for complications among obese (= 30 degrees kg/m2 patients, including wound complications and neurovascular injury. The complication rate increased 9.2% for every 1-point increase in body mass index. There is no association between complication rate and age, injury mechanism, or timing of surgery. Orthopaedic surgeons performing arthroscopy during the early postinjury period must be mindful of the extensive soft-tissue damage present in these patients, including potential capsular defects. Use of high-pressure irrigation can lead to substantial fluid extravasation into the thigh or lower leg compartments, placing patients at increased risk for compartment syndrome. In addition to avoiding high-pressure irrigation, some orthopaedic surgeons have advocated the creation of generous capsular incisions during portal establishment to allow for ready egress of irrigation fluid from the portal sites rather than into soft tissues.
RESPONSES FOR QUESTIONS 85 THROUGH 88
Excessive medial placement of coracoid autograft
Excessive lateral placement of coracoid autograft
Excessive inferior dissection during the procedure
Excessive retraction and dissection of the medial portion of the conjoint tendon
A 20-year-old right-hand-dominant football player sustained a traumatic shoulder dislocation during a tackle. He has had multiple recurrent dislocations, and radiographs reveal anterior glenoid bone loss. He underwent a Latarjet procedure. Match the most likely complication described below with the surgical error listed above.
Question 19
During spinal deformity surgery, which of the following is the most specific early indicator of an intraoperative injury to the spinal cord? Review Topic
Explanation
Question 20
- A 40-year old man has limited, painful motion in dorsiflexion at the metatarsophalangeal (MTP) joint of the right great toe, despite nonsurgical treatment. Radiographs show dorsal and medial osteophytes and minimal narrowing of the articular space. Treatment should consist of
Explanation
Question 21
Which of the following statements best describes the kinematic behavior of the knee during motion from full extension to flexion?
Explanation
greater in the anterior-posterior direction (translates), resulting in more lateral translation, rollback, and medial pivoting.
REFERENCE: Churchill DL, Incavo SJ, Johnson CC, et al: The transepicondylar axis approximates the optimal flexion axis of the knee. Clin Orthop Relat Res 1998;356:111-118.
Figure 98c Question 98
A 71-year-old businessman reports medial knee pain recalcitrant to nonsurgical management.
Examination reveals that his body mass index (BMI) is 28 and he has a mild varus deformity with a range of
motion from 5 degrees to 130 degrees of flexion. Anterior drawer and Lachman’s test are negative. Radiographs are shown in Figures 98a through 98c. For cultural and religious reasons, he is concerned about maintaining his range of motion and kneeling ability. Which of the following options is best?
High tibial osteotomy
Unicompartmental knee arthroplasty
Cruciate-retaining total knee arthroplasty with a fixed bearing design
Posterior stabilized total knee arthroplasty with a fixed bearing design
Cruciate-sacrificing total knee arthroplasty with a rotating platform design PREFERRED RESPONSE: 2
DISCUSSION: Unicompartmental arthroplasty of the knee is associated with better range of motion than either total knee arthroplasty or high tibial osteotomy. In a prospective randomized trial of unicompartmental and total knee arthroplasty for patients with medial compartment osteoarthritis, patients with the unicompartmental prosthesis had better range of motion. The literature that compares range of motion in cruciate-retaining as opposed to posterior stabilized and fixed bearing as opposed to mobile- bearing total knees suggests relatively equivalent range of motion between these designs.
REFERENCES: Newman JH, Ackroyd CE, Shah NE: Unicompartmental or total knee replacement? Five- year results of a prospective randomized trial of 102 osteoarthritic knees with unicompartmental arthritis.
J Bone Joint Surg Br 1998;80:862-865.
Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 59-69.
Question 22
A 24-year-old dancer sustains the injury shown in Figure 28. Management should consist of
Explanation
REFERENCES: O’Malley MJ, Hamilton WG, Munyak J: Fractures of the distal shaft of the fifth metatarsal: “Dancer’s Fracture.” Am J Sports Med 1996;24:240-243.
DeLee JC: Fractures and dislocations of the foot, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1465-1703.
Hamilton WG: Foot and ankle injuries in dancers, in Yokum L (ed): Sports Clinics of North America. Philadelphia, PA, Williams and Wilkins, 1988.
Question 23
Based on the radiograph shown in Figure 4, the innervation of what muscle is most at risk with total hip arthroplasty?
Explanation
REFERENCES: Eggli S, Hankemayer S, Muller ME: Nerve palsy after leg lengthening in total replacement arthroplasty for developmental dysplasia of the hip. J Bone Joint Surg Br 1999;81:843-845.
Schmalzried TP, Amstutz HC, Dorey FJ: Nerve palsy associated with total hip replacement:
Risk factors and prognosis. J Bone Joint Surg Am 1991;73:1074-1080.
Question 24
- A 14-year-old girl has idiopathic scoliosis with a 52-degree right thoracic curve and a 36-degree left lumbar curve. The rotation of the apical vertebra appears greater in the thoracic curve. A sagittal view radiograph shows the spine to be virtually straight. The iliac apophyses are Risser 2. Treatment should consist of
Explanation
Question 25
The clinical photograph in Figure 27 shows a palsy of what nerve/associated muscle? Review Topic

Explanation
such as Parsonage-Turner syndrome. The nerve is easily injured in surgical dissection of the axilla, and is predisposed to injury due to its relatively long course, it is small in diameter, and it has little surrounding connective tissue. If rehabilitation and time are unsuccessful, both nerve and muscle transfers have been described with mixed results.
Question 26
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral
Explanation
REFERENCES: Schepsis AA, Grafe MW, Jones HP, et al: Rupture of the pectoralis major muscle: Outcome or repair of acute and chronic injuries: Am J Sports Med 2000;28:9-15.
Petilon J, Carr DR, Sekiya JK, et al: Pectoralis major muscle injuries: Evaluation and management. J Am Acad Orthop Surg 2005;13:59-68.
Question 27
A 34-year- woman has pain at the base of the thumb that worsens é pinching activities. Nonsurgical treatment has failed to provide relief. Examination reveals that the basilar joint is hypermobile, tender and painful when stressed. A radiograph of the trapeziometacarpal joint shows normal contour with widening when compared with the opposite side. Management should consist of
Explanation
Question 28
The mechanism for the osseous destruction is attributable to
Explanation
This scenario is a classic example of the development of Charcot foot. A red, swollen, deformed foot without ulceration suggests neuroarthropathy. Normal inflammatory marker findings, no history of fever or chills, and radiographs demonstrating bone loss support the diagnosis. Limb elevation with dramatic reduction in erythema is also characteristic of this disease process and does not occur with infection. Total-contact casting is the cornerstone of treatment for acute Charcot disease. Hemoglobin A1C is an indicator of glucose averaged over a 3-month period, providing the most reliable indication of a patient's ongoing glucose control. The pathophysiology of bone destruction is believed to be hypervascularity of bone. Infection and Charcot disease may develop simultaneously, but the combination is rare.
RECOMMENDED READINGS
Kaynak G, Birsel O, Güven MF, Ogüt T. An overview of the Charcot foot pathophysiology. Diabet Foot Ankle. 2013 Aug 2;4. doi: 10.3402/dfa.v4i0.21117.Print 2013. PubMed PMID: 23919113.View Abstract at PubMed
Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006 May;27(5):324-9. PubMed PMID: 16701052. View Abstract at PubMed
Question 29
A woman with a neck and chest tumor has weakness in the biceps and paresthesias in the thumb. Brachioradialis and infraspinatus function are normal. The lesion is affecting which of the following structures?
Explanation
REFERENCE: Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995, p 334.
Question 30
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include
Explanation
REFERENCES: Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Wenger DR, Ditkoff TJ, Herring JA, Mauldin DM: Protrusio acetabuli in Marfan’s syndrome. Clin Orthop 1980;147:134-138.
Question 31
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
REFERENCES: Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 544-545.
Question 32
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?
Explanation
REFERENCE: Leffert RD: Anatomy of the Brachial Plexus in Brachial Plexus Injuries. Churchill Livingstone, New York, NY, 1985.
Question 33
What arterial vessel is most prone to injury during posterior iliac crest bone graft harvest?
Explanation
REFERENCES: Guyer RD, Delmarter RB, Fulp T, Small SD: Complications of cervical spine surgery, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 547.
Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 330-331.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 297, 331-332.
Question 34
What muscle is most often encountered during surgical approaches to C5-6?
Explanation
REFERENCES: Chang U, Lee MC, Kim DH: Anterior approach to the midcervical spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 45-56.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 35
Calcitonin acts as an antiresorptive agent by
Explanation
REFERENCE: Lane JM, Nydick M: Osteoporosis: Current modes of prevention and treatment. J Am Acad Orthop Surg 1999;7:19-31.
Question 36
A 77-year-old man with diabetes mellitus has had a nonhealing Wagner grade I ulcer under the medial sesamoid for the past 3 months. He smokes tobacco regularly. He has undergone several debridements and total contact casting. Examination reveals no palpable pulses. He has no erythema or purulence, and he is afebrile. Radiographs reveal no abnormalities. What is the best initial diagnostic test to help determine why the ulcer has failed to heal?
Explanation
REFERENCE: Brodsky JW: Evaluation of the diabetic foot. Instr Course Lect 1999;48:289-303.
Question 37
A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle?
Explanation
REFERENCES: Hansen ST: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott, Williams & Wilkins, 2000, pp 433-435.
Vienne P, Schoniger R, Helmy N, et al: Hindfoot instability in cavovarus deformity: Static and dynamic balancing. Foot Ankle Int 2007;28:96-102.
Question 38
Figures 63a and 63b show the radiographs of a 38-year-old man who reports low back and bilateral lower extremity pain. The spondylolisthesis is best classified as which of the following? Review Topic

Explanation
Question 39
Figures 174a and 174b are the radiograph and clinical photograph of a 64-year-old obese woman (body mass index [BMI] of 48) who has controlled diabetes and hypertension. She has failed nonsurgical treatment and a weight loss program. She is considering total knee arthroplasty (TKA). What is the most significant postsurgical risk for this patient?
Explanation
The literature has demonstrated increased risk for complications among obese patients undergoing TKA (10%-30%). An evaluation of TKA among obese patients revealed 3- to 9-fold higher incidence of wound complications and deep-seated infection. Belmont and associates demonstrated that patients with a BMI higher than 40 are at higher risk for overall complications than patients with a BMI lower than 25, with a particularly high risk for developing local wound complications and infection. An increased risk for thromboembolic complications was not shown among obese patients undergoing TKA. Patient-reported outcome scores among obese patients undergoing TKA are equivalent to those of nonobese
patients. There are conflicting data regarding the outcome and survivorship following TKA for obese patients. Although some studies show a difference in patient-reported outcomes at differing postsurgical intervals, most obese patients undergoing TKA are satisfied with the procedure.
Question 40
A 63-year-woman has an elbow flexion contracture. History reveals that she underwent three previous surgeries to remove a malignant fibrous histiocytoma of the forearm. An MRI scan reveals a locally recurrent tumor at the site of the previous surgery. Which of the following is considered the most predictive factor for local recurrence?
Explanation
REFERENCES: Bell RS, O’Sullivan B, Liu FF, et al: The surgical margin in soft-tissue sarcoma. J Bone Joint Surg Am 1989;71:370-375.
Sadoski C, Suit HD, Rosenberg A, Mankin H, Efird J: Preoperative radiation, surgical margins, and local control of extremity sarcomas of soft tissues. J Surg Oncol 1993;52:223-230.
Wilson AN, Davis A, Bell RS, et al: Local control of soft tissue sarcoma of the extremity: The experience of a multidisciplinary sarcoma group with definitive surgery and radiotherapy. Eur J Cancer 1994;30:746-751.
Question 41
A 66-year-old male undergoes the procedure shown in figures A and B. After 4 years, he develops progressive pain and limitations in his daily function that is refractory to conservative measures. He is indicated for conversion to a total knee replacement with almost complete relief of his symptoms postoperatively. What preoperative factor likely led to the subsequent failure?
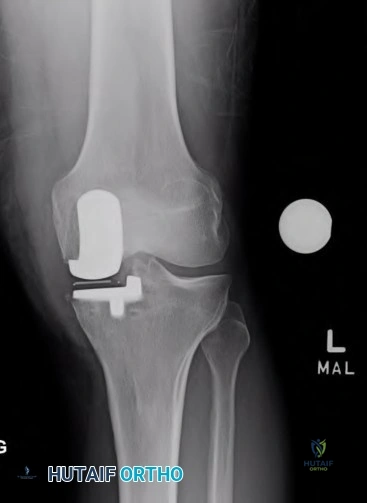
Explanation

OrthoCash 2020
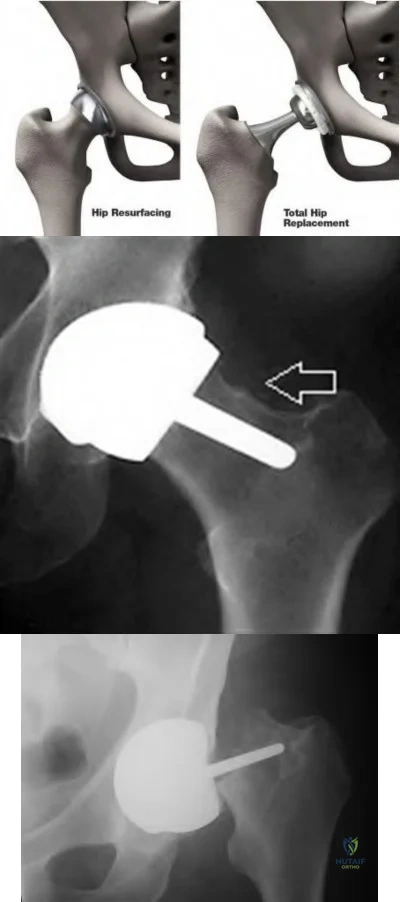
Which of the following is the most common cause of early revision surgery (<20 weeks) following a hip resurfacing arthroplasty?
Periprosthetic fracture
Rupture of abductors
Dislocation
Heterotopic ossification
Post-operative stiffness
Periprosthetic fracture, specifically femoral neck fracture, is the most common cause of early revision less than 20 weeks following surgery.
The rate of femoral neck fractures following hip resurfacing varies, but most literature reports a rate of 1%. A majority of these fractures happen in the early post-operative period and are the most frequent cause of revision surgery within several months following surgery. The cause is usually multifactorial, but placing the femoral implant in varus, osteonecrosis, and notching have been proven risk factors for fracture.
Little el al. report on 377 patients undergoing hip resurfacing. 13 required revision including 8 for fracture of the femoral neck and 3 for loosening of a component. Evidence of osteonecrosis was seen in two of these cases, leading the authors to believe it may contributed to fracture.
Illustration A shows a comparison of a typical total hip replacement and a hip resurfacing arthroplasty. Illustration B shows notching of the femoral neck, a known cause of femoral neck fracture following hip resurfacing. Illustration C shows a femoral neck fracture in a patient with a hip resurfacing.
OrthoCash 2020
A 55-year-old male undergoes a revision total knee arthroplasty of an implant that is only 3 years old. At the time of surgery, the tibial polyethylene liner shows catastrophic delamination and cracking. What is the most likely cause of this extensive, accelerated wear of the polyethylene liner?
Sterilization in ethylene oxide
Gamma irradiation of the polyethylene liner in the presence of air
Gamma irradiation of the polyethylene liner with vacuum packaging
Gamma irradiation of the polyethylene liner in nitrogen
Gamma irradiation of the polyethylene liner in argon Corrent answer: 2
Irradiation of polyethylene in air (i.e. oxygen present) has been shown to be a risk factor for catastrophic failure after total knee replacement.
Free radicals are generated when polyethylene is irradiated in the presence of air. Initially, these free radicals result in cross-linking. However, if the polyethylene is exposed to these free radicals for an extended period of time, delamination, cracking, and catastrophic failure may ensue. The industry has completely abandoned this method of sterilization as a result. Currently, the standard of care is irradiation of polyethylene in an inert gas (e.g. argon, nitrogen or vacuum packaging). The amount of oxidative products when polyethylene is sterilized in the absence of oxygen is much less and does not lead to catastrophic failure.
Sterilization without irradiation is another option (ethylene oxide). When this occurs, there is no cross-linking and thus the increased wear properties are lost. However, since there is no oxidization, you do not have the risk of catastrophic failure as seen in those liners irradiated in the presence of oxygen.
The cited reference by McNulty et al. from Orthopedics discusses the influence of sterilization methods on wear performance. They found that gamma irradiation and storage of the polyethylene components in an essentially oxygen-free environment imparted by gamma irradiation in a vacuum foil pouch (GVF) protects the components from oxidization.
Illustration A shows a polyethylene liner that has undergone catastrophic wear as a result of irradiation in the presence of oxygen.
Incorrect Answers:
catastrophic wear, although wear properties are less than gamma irradiation in the absence of air.

OrthoCash 2020
Which of the following interventions reduces osteolysis around distal portion of the femoral stem when performing a total hip arthroplasty?
Use of an extended offset femoral neck component
Use of a proximal circumferentially coated ingrowth stem
Use of a collared stem
Use of a long femoral stem
Ensuring that the stem fills the diaphysis of the femur Corrent answer: 2
Osteolysis of the femur is caused by activation of macrophages by microscopic polyethylene particles within the "effective joint space", defined as any area where joint fluid can come into contact with bone. This can occur above the acetabular cup, through screw holes, and down the femoral shaft around the prosthetic stem. Ideally, with a cementless stem, both the proximal and metaphyseal femur are well filled by the prosthesis. Collared stems are used to augment poor calcar bone quality or bone loss.
Sinha et al showed in a retrospective review of 101 hips with cementless circumferentially coated femoral stems no distal femur osteolysis occurred, but 82% showed “evidence of proximal femur stress shielding”, though only 38% showed proximal femoral osteolysis.
OrthoCash 2020
During a minimally invasive approach to total hip arthroplasty a femoral periprosthetic fracture occurs. Which of the following steps is crucial to properly treat this complication?
Transitioning to an extensile approach to adequately visualize and reduce the fracture
Limiting post-operative weight bearing
Switching to a cemented femoral stem to avoid the stresses created during press-fit fixation
Delaying the arthroplasty until the fracture has healed
Supplementing the fracture with autograft Corrent answer: 1
Proper treatment of an intraoperative femoral fracture during total hip arthroplasty involves adequate exposure, anatomic reduction, and bypassing the fracture site by 2 cortical diameters of the femur with a long stem. This may involve repositioning the patient on the table if the arthroplasty is performed in the supine position. Minimally invasive surgical techniques have been developed to insert the components through smaller exposures and less soft tissue dissection. The purported advantages include faster rehabilitation, less blood loss, shorter hospital stays, and better cosmesis. However, complications an arise if the surgeon sacrifices surgical exposure and visualization.
Fehring et al review 3 cases of total hip arthroplasty performed through minimally invasive techniques with catastrophic outcomes. Intra-operative fracture, chronic instability, and death were all identified.
OrthoCash 2020
A 70-year-old man underwent total hip arthroplasty 4 months ago and has experienced 3 dislocations. Radiographs reveal no failure of the hardware and an acetabular component that has an abduction
angle of 40 degrees and a version of 10 degrees retroverted. What is the most appropriate treatment for the recurrent dislocations?
hip abduction brace
revision of the acetabular liner to a constrained type
revision of the entire acetabular component
revision of the femoral head to a larger size
revision to an extended offset prosthesis Corrent answer: 3
Per Dorr et al: post-operative hip instability can be caused by several factors: soft tissue imbalance, component malposition, or position. Component malposition, as in this case, should be treated with revision of the offending component. In this case the acetabulum was placed in retroversion when it should have been 15-20 degrees anteverted. None of the other options addresses the cause of the instability. According to Morrey, the most signficant risk factors to instability are prior hip surgery, trochanteric nonunion, and posterior surgical approach. He wrote that the most reliable way to correct instability is to reorient a retroverted acetabular cup.
OrthoCash 2020
In patients with sickle cell disease and asymptomatic osteonecrosis of the femoral head identified with magnetic resonance imaging, what percentage will eventually go on to femoral head collapse?
Question 42
What is the most common behavioral effect of anabolic steroid use in athletes? Review Topic
Explanation
Question 43
What is the standard interval for placement of an anterolateral portal in ankle arthroscopy?
Explanation
Question 44
A patient has a C6-7 herniated nucleus pulposus. What is the most likely distribution of symptoms? Review Topic
Explanation
(SBQ12SP.27) A 24-year-old male sustains the injury shown in Figure A. What was the most likely mechanism of injury? Review Topic

Hyperextension
Flexion-distraction
Flexion-compression
Rotational
Pure axial load
Figure A shows a quadrangular fracture pattern of C5. These injuries are observed with flexion-compression loads.
Quadrangular fractures of the cervical spine are considered flexion teardrop fractures. However, they present with a larger anterior lip fragment compared to the classic teardrop fracture pattern. The radiographic findings include a quadrangular-shaped fragment from the anterior one-third of the vertebral body with significant posterior vertebral subluxation, angular kyphosis, and an increased interspinous space with facet subluxation due to disruption of the posterior elements. These are unstable fractures, and almost always require anterior and posterior stabilization.
Moore et al. studied the reliability of Cervical Spine Injury Severity Score to measure stability after cervical spine trauma. The classification system is based on morphologic descriptions and, secondly, on stability based on a quantifiable value. They showed that the Cervical Spine Injury Severity Score had excellent reliability with intra-observer intraclass correlation coefficients (ICC) >0.97 and inter-observer ICC >0.88.
Vaccaro et al. published the subaxial cervical spine injury classification system (SLIC). This systems involves 3 main categories (injury morphology, disco-ligamentous complex, and neurologic status). The overall injury severity score is obtained by summing the scores from each category. They propose that SLIC < 4 can be treated non-operatively.
Allen et al. published a classification system of cervical spine injuries which breaks injuries of the subaxial spine into six phylogenic groups based on mechanism of injury. These include: 1) flexion-compression 2) vertical-compression 3) flexion-
distraction 4) extension-compression 5) extension-distraction 6) lateral flexion. Facet
dislocation
is
caused
by
flexion-distraction
force.
Figure A shows a lateral radiograph of the cervical spine demonstrating a typical flexion-compression fracture with anteriorly displaced quadrangular fragment. Illustration A shows a flexion-compression injury. Illustration B shows the mechanism of injury for a quadrangular fracture of the cervical spine. This unstable fracture pattern is characterized by anterior column failure in flexion/compression and posterior column failure in tension. Illustration C shows an illustration of the fracture morphology according to the Allen and Ferguson classification.
Incorrect Answer 1:
Hyperextension injuries
Flexion-distraction injuries usually result in facet dislocations.
Question 45
Figure 53 shows the MRI scan of a 53-year-old carnival worker who has pain and swelling in the left shoulder as a result of attempting to stop a roller coaster car with his arm. Examination reveals decreased ROM, apprehension, and inability to move the dorsum of his hand away from his back. Treatment should consist of
Explanation
Question 46
Figure 1 is the MR image of a high school soccer player who sustained a right knee injury during a game while making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a "clunk" within the knee. What is the most likely biomechanical basis for the "clunk"?

Explanation
Question 47
In patients without spondylolisthesis or scoliosis undergoing laminectomy for lumbar spinal stenosis, spinal fusion is generally recommended if
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 299-409.
Fischgrund JS, Mackay M, Herkowitz HN, et al: 1997 Volvo Award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 48
A 32-year-old man notes increasing back pain and progressive paraparesis over the past few weeks. He is febrile, and laboratory studies show a WBC of 12,500/mm3. MRI scans are shown in Figures 6a and 6b. Management should consist of
Explanation
REFERENCES: Emery SE, Chan DP, Woodward HR: Treatment of hematogenous pyogenic vertebral osteomyelitis with anterior debridement and primary bone grafting. Spine 1989;14:284-291.
Lifeso RM: Pyogenic spinal sepsis in adults. Spine 1990;15:1265-1271.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 49
The diagnosis of an infection after total knee arthroplasty is most reliably proven based on what single study?
Explanation
REFERENCES: Windsor RE, Bono JV: Infected total knee replacements. J Am Acad Orthop Surg 1994;2:44-53.
Windsor RE, Insall JN, Urs WK, et al: Two-stage reimplantation for the salvage of total knee arthroplasty complicated by infection: Further follow-up and refinement of indications. J Bone Joint Surg Am 1990;72:272-278.
Question 50
A patient undergoing joint arthroplasty is put on a drug that competitively inhibits the activation of an enzyme that breaks down Factor Ia. The drug is
Explanation
Tranexamic acid competitively inhibits the activation of plasminogen to plasmin by binding to specific sites on both plasminogen and plasmin. Tranexamic acid has roughly eight times the antifibrinolytic activity of an older analogue, e-aminocaproic acid. It is used during joint replacement surgery to reduce blood loss and the need for transfusion.
Watts et al. review strategies for minimizing blood loss and transfusion. They recommend 1g of TXA prior to incision, and 1g at wound closure. They also recommend giving fluids for symptoms of anemia, rather than transfusion, as even high risk patients do well with sufficient intravascular volume even with low hemoglobin levels.
Imai et al. evaluated TXA in 107 patients undergoing THA. They found that intraoperative blood loss after preoperative TXA administration was lower than both control and postoperative TXA administration groups. They recommend using 1 g of TXA 10 minutes before surgery and 6 hours after the first administration to best reduce blood loss during THA.
Gillette et al. retrospectively reviewed 2046 patients receiving TXA for THA or TKA together with either aspirin, warfarin or dalteparin. They found that the rates of symptomatic DVT (0.35%, 0.15%, and 0.52%, respectively) and nonfatal PE were similar (0.17%, 0.43%, and 0.26%, respectively) for the 3 drugs respectively. They recommend TXA to decrease blood loss and transfusion.
Illustration A shows the role of tranexamic acid in the fibrinolytic cycle and the
clotting cascade.
Incorrect Answers:
Question 51
A female cross-country runner has an insidious onset of right groin pain. Radiographs of the right hip reveal a tension-side stress fracture. History reveals that she was treated for a “foot” fracture 1 year ago. In addition to performing internal fixation of the femoral neck, which of the following should be obtained?
Explanation
REFERENCES: Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Barrow GW, Saha H: Menstrual irregularity and stress fractures in collegiate female distance runners. Am J Sports Med 1988;16:209-216.
Question 52
A 20-year-old man is brought to the emergency department after a high-speed motor vehicle accident. His initial blood pressure is 70/40 mm Hg. He is currently receiving intravenous fluids as well as blood. His Focused Assessment with Sonography for Trauma examination did not show any free fluid in his abdomen and his chest radiograph is unremarkable. An AP pelvis radiograph is shown in Figure 15. What is the next most appropriate step in the management of his pelvic injury?
Explanation
REFERENCES: Kreig JC, Mohr M, Ellis TJ, et al: Emergent stabilization of pelvic ring injuries by controlled circumferential compression: A clinical trial. J Trauma 2005;59:659-664.
Croce MA, Magnotti LJ, Savage SA, et al: Emergent pelvic fixation in patients with exsanguinating pelvic fractures. J Am Coll Surg 2007;204:935-942.
Routt ML Jr, Falicov A, Woodhouse E, et al: Circumferential pelvic antishock sheeting:
A temporary resuscitation aid. J Orthop Trauma 2002;16:45-48.
Question 53
Radiographs shown in Figures 1 through 3 show two different prosthetic design variations of the same knee implant. When compared with the design of right knee prosthesis, the left can be expected to have a
Explanation
Question 54
Figure 1 is the MRI scan of a 15-year-old boy who has had knee pain with running for 5 months. Radiographs show an osteochondritis dissecans (OCD) lesion of the medial femoral condyle. What is the most appropriate treatment?

Explanation
Question 55
A 27-year-old professional football player complains of acute onset neck and radiating left arm pain after making a tackle. For approximately 1 week after injury his left deltoid strength was 4/5. An MRI is performed, which demonstrates a C4-5 disc herniation without evidence of cord compression. He was treated with a brief course of oral steroids followed by aggressive physical therapy. At this time he is asymptomatic and his neurologic exam is normal. If the patient returns to professional football play, what is his increased risk of sustaining a catastrophic spinal cord injury? Review Topic
Explanation
A C5 radiculopathy from an acute disc herniation can manifest as pain in the neck and affected arm, as well as weakness in the affected myotome. The natural history of this pathology is symptomatic improvement over time. In professional athletes, there are few studies to guide treatment, but oral methylprednisolone has been shown to improve symptoms and expedite return to play. The risk of sustaining catastrophic spinal cord injury after return to play is considered low, and has been reported to be 0%.
Wong et. al. performed a systematic review of the literature identifying the natural history, clinical course, and prognostic factors of symptomatic cervical disc herniations with radiculopathy. They found substantial symptomatic improvement within the first 4-6 months after onset, with maintained improvements for 2-3 years. No patients in their review developed progressive neurological deficits or myelopathy
at
any
point
during
follow
up.
Meredith et. al. performed a retrospective chart review of 16 professional football players with cervical disc herniations. The authors recommended surgery if patients had MRI with cord compression and signal change within the cord, but otherwise encouraged nonoperative treatment with return to sports after symptoms improved and repeat MRI demonstrated no cord compression. Symptoms generally improved with a course of anti-inflammatory medications including NSAIDs, oral methylprednisolone, and epidural steroid injections. Nine of the 16 patients were able to return to play, and at one year after return to play there were no catastrophic spinal cord injuries among the group.
Incorrect
Question 56
A 12½-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full range of motion without effusion. Radiographs reveal an osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. MRI scans are shown in Figures 14a and 14b. Initial treatment should consist of Review Topic
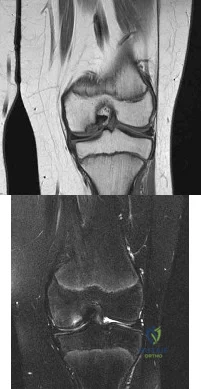
Explanation
Cessation of sport activities for 4 to 6 months may allow healing of the lesion. Surgical treatment of juvenile OCD lesions is reserved for unstable lesions, patients
who have not shown radiographic evidence of healing and are still symptomatic after
6 months of nonsurgical management, or patients who are approaching skeletal maturity. Good results with stable in situ lesions that have failed to respond to nonsurgical management have been reported with both transarticular and retroarticular drilling. Results after excision alone are poor at 5-year follow-up, and it is unclear if microfracture will improve the long-term outcome. Mosaicplasty may be the next best option for patients who remain or become symptomatic after excision of the fragment and microfracture.
Wall et al. reviewed juvenile OCD. They state that JOCD has better potential for healing than adult OCD, but several series have shown up to a 50% failure to heal with nonsurgical techniques. The presence of a loose body is an indication for surgical fixation, drilling or regenerative procedures, depending on the presence/extent of subchondral bone sclerosis and the surgeon's experience.
Figure A and B are coronal MRI images showing a stable appearing JOCD lesion of the medial femoral condyle.
Incorrect
in the first
(SBQ13PE.9) A 6-year-old boy complains of a 'clunking' sensation in his left knee. He has no associated pain and denies trauma. He can elicit the sensation when moving his knee from flexion into full extension. He is otherwise healthy, with no birth or developmental issues. On examination, there is a palpable clunk felt over the anterior knee through range of motion. There is no obvious instability or tenderness and he had normal patellar tracking. An AP radiograph of the knee is shown in Figure A. What would be the most likely diagnosis? Review Topic

Agenesis of the anterior cruciate ligament
Thickened medial plica
Grade IV chondral flap
Pigmented villonodular synovitis
Abnormal meniscal morphology
This child presents with an asymptomatic click in the knee. It is associated with widening of the lateral joint space of the knee on X-ray. These features are highly suggestive of a discoid lateral meniscus in this age category.
The principal diagnostic feature of a discoid meniscus is the complaint of snapping or clicking in the knee. Children are usually asymptomatic. Although, less frequently, children may present with pain that is largely secondary to an underlying meniscal tear. MRI scans of the knee have show to have the greatest sensitivity for identifying discoid menisci. The presence of a contiguous central meniscus on three consecutive slices is usually indicative of the diagnosis. Treatment is mostly focused on conservative modalities. Surgical intervention is reserved for symptomatic cases with recurrent locking, swelling or persistent pain is present in older children.
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Figure A shows an AP radiograph of a pediatric knee. There is an increased lateral joint space suggestive of a discoid meniscus.
Illustrations A-C show an MRI of the knee with 3 consecutive coronal cuts showing an abnormal appearing discoid meniscus.
Incorrect Answers:
Question 57
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At 1-year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is
Explanation
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 58
Which of the following enzymes is used to resorb bone by mature osteoclasts?
Explanation
Question 59
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 60
While performing a total shoulder arthroplasty, excessive retraction is placed on the "strap muscles" (short head of biceps and coracobrachialis). Neurovascular examination would reveal weakness of which of the following? Review Topic
Explanation
this area. Excessive traction on the musculocutaneous nerve could lead to a neurapraxia with resultant weakness of elbow flexion and forearm supinaton because of the loss of biceps function.
Question 61
Treatment should include
Explanation
The MR images show a tear through a discoid lateral meniscus. A discoid meniscus is caused by a failure of apoptosis during development in utero and is considered a congenital abnormality. Discoid menisci are prone to tearing and can be caused by minimal trauma. There is no known genetic cause for this condition. Radiographic findings that may be present in the setting of a discoid meniscus include lateral joint space widening, squaring of the lateral femoral condyle, and cupping of the lateral tibial plateau. Contralateral discoid menisci are noted in 20% of patients. There are no other known associated conditions. Treatment of a symptomatic discoid meniscus should include partial meniscectomy and saucerization or repair.

Question 62
Creatine is currently being used by athletes as a dietary supplement in an attempt to enhance performance. What is the physiologic basis for its use?
Explanation
REFERENCES: Greenhaff PL: Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5:S100-S110.
Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E: Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci 1993;84:565-571.
Trump ME, Heigenhauser GJ, Putman CT, Spriet LL: Importance of muscle phosphocreatine during intermittent maximal cycling. J Appl Physiol 1996;80:1574-1580.
Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL: Muscle creatine loading in men. J Appl Physiol 1996;81:232-237.
Question 63
Figure 30 shows the radiograph of a 38-year-old man who reports persistent pain laterally and plantarly about the fifth metatarsal head. Examination reveals calluses dorsolaterally and plantarly about the fifth metatarsal head. Nonsurgical management has failed to provide relief. Surgical treatment should include
Explanation
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Moran MM, Claridge RJ: Chevron osteotomy for bunionette. Foot Ankle Int 1994;15:684-688.
Question 64
An open biopsy specimen of a radiodense distal clavicle lesion in a 12-year-old girl shows chronic polyclonal inflammatory cells without granuloma formation. Laboratory studies show that bacterial, fungal, and acid-fast bacillus cultures are negative. Subsequently, a similar lesion is noted in the fibula. The next most appropriate step in management should consist of
Explanation
REFERENCE: Carr AJ, Cole WG, Roberton DM, Chow CW: Chronic multifocal osteomyelitis. J Bone Joint Surg Br 1993;75:582-591.
Question 65
What is the typical axial plane transverse angulation of the thoracic pedicles?
Explanation
starting point is more lateral. T2 angles about 15 degrees, and then the pedicles average about
5 to 7 degrees down to T10. At T11 and 12, the angulation is minimal.
REFERENCES: Weinstein L: Pediatric Spine Principles and Practice. New York, NY, Raven Press, 1994, pp 1659-1681.
Lenke LG, Orchowski J: Segmental posterior spinal instrumentation: Thoracic spine to sacrum, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 537-552.
Question 66
Which sterilization method is expected to produce the most degradation of an allograft used for anterior cruciate ligament reconstruction?
Explanation
A biomechanical study compared unprocessed, irradiated (2.0 Mrad-2.8 Mrad), and supercritical CO2-treated soft-tissue allografts and demonstrated a 27% to 36% decrease in stiffness of the supercritical CO2-treated grafts. No significant difference was found between the irradiated and untreated soft-tissue allografts. Low-dose (1.0 Mrad-1.2 Mrad) gamma irradiation of bone-patellar-tendon-allograft has been shown to produce a 20% decrease in graft stiffness. Deep freezing or cleansing with 4% chlorhexidine gluconate does not appear to adversely affect the biomechanical properties of the allograft tissue.

CLINICAL SITUATION FOR QUESTIONS 43 THROUGH 46
Figures 43a and 43b are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable.
Question 67
The relocation test is most reliable for diagnosing anterior subluxation of the glenohumeral joint when
Explanation
REFERENCE: Speer KP, Hannafin JA, Altchek DW, Warren RF: An evaluation of the shoulder relocation test. Am J Sports Med 1994;22:177-183.
Question 68
An 19-year-old male presents to the emergency room following an motor vehicle accident as an unrestrained driver. Examination reveals unilateral jugular vein engorgement. Chest and special view radiographs are seen in Figures A and B respectively. Following CT scan of the chest, the next step in management is Review Topic
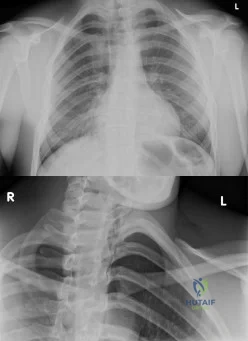
Explanation
The SC joint can dislocate anteriorly or posteriorly. Posterior dislocations are first treated with closed reduction. If closed reduction fails, open reduction is indicated. Early complications of posterior SC dislocation include pneumothorax, laceration/erosion/occlusion of great vessels, esophageal rupture and brachial plexus compression. Late complications include tracheoesophageal fistula, stridor and dysphagia.
Groh et al. reviewed traumatic SC injuries. Reduction maneuvers in posterior SC dislocation include: (1) traction on the arm and slowly bringing it into extension, (2) traction with the arm in adduction and posterior pressure applied to the shoulder, and
(3) pulling anteriorly on a towel clip encircling the medial clavicle. Chronic instability after posterior SC dislocations can be managed with figure-of-8 semitendinosus graft or medial clavicle resection and reattachment of the clavicle to the first rib with dacron tape.
Glass et al. performed a systematic review on SC dislocations. They found mediastinal compression occurred 30% of the time with posterior dislocations.
Figures A and B are radiographs demonstrating asymmetry of the SC joints, characteristic of a right posterior SC dislocation (Figure B is not a serendipity view). Illustration A demonstrates how in POSTERIOR dislocation, the clavicle appears INFERIOR, and in ANTERIOR dislocation, the clavicle appears SUPERIOR on a serendipity view radiograph respectively. Illustration B shows the imaging technique for a serendipity view radiograph. Illustration C is a reconstructed CT image of the patient showing left posterior SC dislocation.
Incorrect Answers:
Question 69
A 45-year-old man underwent unipolar hemiarthroplasty reconstruction using cementless fixation for nontraumatic osteonecrosis of the femoral head 5 years ago. He now reports buttock and groin pain that is associated with loading activities. What is the most likely cause of his pain?
Explanation
REFERENCES: Steinberg ME, Corces A, Fallon M: Acetabular involvement in osteonecrosis of the femoral head. J Bone Joint Surg Am 1999;81:60-65.
Dalldorf PG, Banas MP, Hicks DG, Pelligrini VD Jr: Rate of degeneration of human acetabular cartilage after hemiarthroplasty. J Bone Joint Surg Am 1995;77:877-882.
Question 70
A 25-year-old male polytrauma patient undergoes initial temporary external fixation for a femoral shaft fracture. He is converted to a femoral nail at 7 days. This management can be expected to result in
Explanation
REFERENCES: Harwood PJ, Giannoudis PV, Probst C, et al: The risk of local infective complications after damage control procedures for femoral shaft fracture. J Orthop Trauma 2006;20:181-189.
Roberts CS, Pape HC, Jones AL, et al: Damage control orthopaedics: Evolving concepts in the treatment of patients who have sustained orthopaedic trauma. Instr Course Lect
2005;54:447-462.
Question 71
After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office with continued pain 2 years after surgery. He describes instability, particularly when descending stairs. Upon examination, there is range of motion from 0 to 120 degrees with no extensor lag. The knee is stable to varus and valgus stress in extension, but there is flexion instability in both the anterior-posterior direction and in the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection workup is negative. What is the most appropriate surgical intervention at this time?
Explanation

Video 99 for reference
This patient has valgus knee alignment, and, after undergoing appropriate bone resections and soft-tissue balancing, has demonstrated a tight PCL on trial reduction as evidenced by lift-off of the trial insert as described by Scott and Chmell. The appropriate maneuver is PCL recession with partial release of tight (usually anterolateral) PCL fibers. However, for this patient, instability resulted in increased anterior translation. At this stage, the options are to convert to either a deeper-dish insert with increased sagittal conformity or a posterior stabilized insert. The only appropriate choice among the responses is use of an insert with increased sagittal conformity to prevent excessive anterior translation. Increasing the polyethylene could improve stability in flexion, but, considering there is good stability in extension, this likely would lead to an inability to achieve full extension. The patient’s valgus deformity, flexion contracture, correction with release of the iliotibial band, and posterolateral capsule predispose him to increased risk for peroneal nerve palsy. His symptoms at follow-up suggest knee flexion
instability with pain, swelling, and difficulty descending stairs. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant depending on the condition of the ligaments likely is needed to address his symptoms. The difference in extension vs flexion stability makes polyethylene exchange a poor option. There is no reason to believe a constrained rotating hinge design is necessary. Repeat use of a PCL-retaining insert is not recommended.
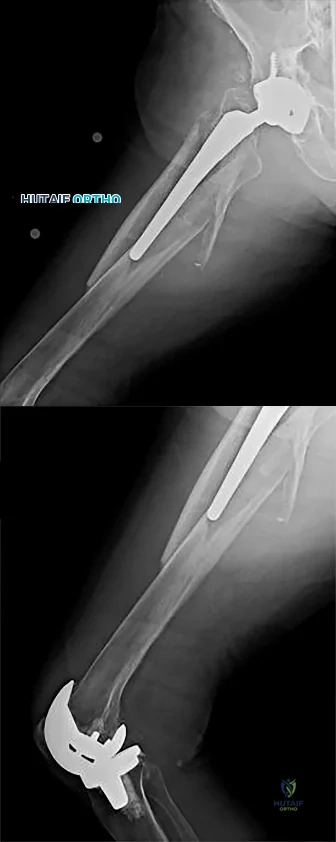
Question 72
A 32-year-old football coach has had a 4-month history of increasing right wrist pain, particularly during blocking exercises, and he reports significant pain with range of motion and gripping activities. He denies any history of trauma. Examination reveals dorsal wrist tenderness and boggy fullness over the dorsum of the wrist. No erythema is noted. Grip strength is 60% compared with the opposite side. Radiographs are shown in Figures 5a and 5b. What is the most likely diagnosis?
Explanation
REFERENCES: Green DP, Hotchkiss RN, Pederson WC: Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, pp 837-848.
Gerwin M, Weiland AJ: Avascular necrosis of the carpals. Hand Clin 1993, p 761.
Question 73
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
REFERENCES: Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JS (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 74
Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the best treatment?
Explanation
REFERENCES: McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective.
Am J Orthop 1999;28:21-26.
Taylor MS: Cold weather injuries during peacetime military training. Milit Med 1992;157:602-604.
Question 75
A 44-year-old man sustains the injury shown in Figures 1 through 3. What is the most appropriate treatment?

Explanation
Reduction, either open or closed, with internal fixation (pinning) is the recommended treatment for the majority of these injuries. Closed reduction with pinning is most often performed for acute injuries. Open reduction with pinning is performed for those injuries that cannot be reduced by closed means or those with a delayed presentation. Four cases of successful closed reduction and splinting, all performed upon presentation in the emergency department, have been described by Storken and associates, but the authors note that their review of three prior reports uncovered cases of secondary dislocation, which required surgical stabilization. One of the dislocations occurred 4 months after the reduction. They assert that an indication for primary ORIF is a CMC dislocation associated with major fractures. Primary arthrodesis can be considered in cases with severe intra-articular comminution, but this procedure substantially limits the ability of the hand to increase and decrease the transverse metacarpal arch, which is an important functional movement. It can also lead to osteoarthritis of the triquetrohamate joint. Suspension arthroplasty has been described for old fracture-dislocations of the fifth CMC joint, using a partial slip of the extensor carpi ulnaris.








Question 76
Figure 56 is the MR image of a 20-year-old Division I baseball pitcher who has a 1-month history of medial elbow pain in his throwing arm. He also notes a decrease in both control and pitching velocity. An examination reveals tenderness at the medial epicondyle that is exacerbated with valgus elbow stress. The strongest indication for ulnar collateral ligament (UCL) reconstruction is
Explanation
All responses represent findings that may be associated with chronic UCL insufficiency. Responses 1 and 3 reflect injury to the UCL itself. In most patients, particularly young patients, UCL reconstruction should not be considered until an appropriate trial of nonsurgical measures has failed. This trial should include, at a minimum, 6 weeks of throwing abstinence followed by rehabilitation to address pitching mechanics and shoulder motion deficits and core strengthening. Although the decision to enter the MLB draft may influence surgical decision making, a pitcher with a 1-month history of elbow symptoms should attempt nonsurgical therapy before making a surgical decision that is not based on clinical data.
Question 77
A 30-year-old woman who runs approximately 30 miles a week has had right hip and groin pain for the past 3 weeks. Examination reveals an antalgic gait, limited motion of the right hip, and pain, especially with internal and external rotation. Plain radiographs are normal, and an MRI scan is shown in Figure 21. Management should consist of
Explanation
REFERENCES: Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 239-253.
Fullerton LR Jr, Snowdy HA: Femoral neck stress fractures. Am J Sports Med
1988;16:365-377.
Question 78
With the arm abducted 90 degrees and fully externally rotated, which of the following glenohumeral ligaments resists anterior translation of the humerus? Review Topic
Explanation
Question 79
Which of the following nerves is most commonly injured during revision surgery following a Bristow procedure?
Explanation
REFERENCES: Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993,
pp 98-116.
Flatow EL, Bigliani LU, April EW: An anatomic study of the musculocutaneous nerve and its relationship to the coracoid process. Clin Orthop 1989;244:166-171.
Question 80
A 75-year-old man who is right-hand dominant has had a painful right shoulder for the past 6 months, with no improvement with nonsurgical management. Examination reveals an active motion of 60 degrees of forward flexion and abduction, with severe crepitus and pain. Radiographs reveal a high-riding humeral head with severe glenohumeral arthritic changes. What is the most appropriate treatment? Review Topic
Explanation
Question 81
Limited weight bearing usually is recommended following open reduction and internal fixation of intra-articular lower extremity fractures. A bone graft, or bone graft substitute is often placed in the metaphyseal void beneath the reduced articular fragments. Which of the following bone grafts or bone graft substitutes will most likely permit earlier weight bearing without subsidence of the articular reduction?
Explanation
Question 82
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
Question 83
A 46-year-old woman had an ankle fracture and ORIF 6 years ago. She had subsequent removal of some of the hardware, but her pain has persisted (Figures 44a and 44b).

Explanation
Patients younger than 40 years of age who have ankle arthritis pose an ongoing clinical challenge. Nonsurgical treatment should be maximized, although distraction arthroplasty can be used in an effort to delay the need for fusion.
One of the strongest indications for ankle arthroplasty is a preexisting hindfoot fusion with a goal to retain some ankle/hindfoot motion. Ankle fusion is perhaps the most predictable surgical treatment for a relatively young, active patient with ankle arthritis. Moreover, there are concerns regarding implant loosening when performing TAA in active patients.
Outcome after syndesmosis ORIF has been linked to the quality of the reduction at the index procedure. Syndesmotic malreduction that is severe necessitates osteotomy and revision ORIF.
RECOMMENDED READINGS
Sagi HC, Shah AR, Sanders RW. The functional consequence of syndesmotic joint malreduction at a minimum 2-year follow-up. J Orthop Trauma. 2012 Jul;26(7):439-43. doi: 10.1097/BOT.0b013e31822a526a. PubMed PMID: 22357084. View Abstract at PubMed
Smith NC, Beaman D, Rozbruch SR, Glazebrook MA. Evidence-based indications for distraction ankle arthroplasty. Foot Ankle Int. 2012 Aug;33(8):632-6. Review. View Abstract at PubMed
Kim BS, Knupp M, Zwicky L, Lee JW, Hintermann B. Total ankle replacement in association with hindfoot fusion: Outcome and complications. J Bone Joint Surg Br. 2010 Nov;92(11):1540-7. doi: 10.1302/0301-620X.92B11.24452. PubMed PMID: 21037349. View Abstract at PubMed
Daniels TR, Younger AS, Penner M, Wing K, Dryden PJ, Wong H, Glazebrook M. Intermediate-term results of total ankle replacement and ankle arthrodesis: a COFAS multicenter study. J Bone Joint Surg Am. 2014 Jan 15;96(2):135-42. doi: 10.2106/JBJS.L.01597. View Abstract at PubMed
Question 84
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
REFERENCE: Sarrafian SK: Anatomy of the Foot and Ankle, Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, p 364.
Question 85
At revision, the stem is retained and a new head with a polyethylene bearing is selected. The best option for the head is
Explanation
Ceramic-on-ceramic is a controversial bearing surface typically reserved for younger patients such as this one. Some studies have suggested that the bearing is more expensive and does not really prolong the service life of the implant, although a recent meta-analysis of high-quality trials showed that there is a decreased revision rate with ceramic-on-ceramic, so its use may be justified. Complications of intraoperative bearing fracture and squeaking are more common than with conventional bearings, but pain and function scores are equivalent. Stripe wear associated with a vertical cup and morbid obesity are related to an increased risk for liner fracture. Concerns about head fractures with a new ceramic head and a damaged trunnion have led investigators to conclude that using a harder bearing than the initial bearing surface with a built-in titanium sleeve is probably the best solution when a stem is retained during revision surgery.

Question 86
A 35-year-old male sustains a closed tibial shaft fracture after falling from 12 feet. Which of the following measurements would be concerning for an evolving compartment syndrome?

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. Determining if a patient needs fasciotomies in the operating room while a patient is under anesthesia is complicated by the fact that obtaining a clinical exam is impossible, and that the diastolic blood pressure may be falsely decreased compared to normal pre- or postoperative measurements. Currently, it is recommended that intraoperative compartment pressures be compared to preoperative diastolic blood pressures, with delta p < 30 indicating the need for fasciotomies.
Kakar et al. review the preoperative, intraoperative, and postoperative diastolic blood pressure (DBP) in 242 patients with a tibia fracture treated operatively. They found the mean DBP was 18 points lower in the operating room compared to the preoperative measurement. In addition, they found the difference between preoperative and postoperative diastolic blood pressures to be within 2 points, indicating the decrease seen intraoperatively is likely a spurious value induced by anesthetic.
McQueen and Court-Brown prospectively review 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Incorrect Answers:
Question 87
Five weeks after undergoing a successful L4-L5 diskectomy, with complete relief of his preoperative sciatica, a 36-year-old man has severe, relentless back and buttock pain. Examination and laboratory studies are unremarkable with the exception of an erythrocyte sedimentation rate (ESR) of 90 mm/h. What is the next most appropriate step in management?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Beatty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 713-721.
Question 88
Cortical bone demonstrates viscoelastic behavior as its mechanical properties are sensitive to strain rate and duration of applied load. Regarding longitudinal strain in cortical bone, which of the following statements regarding this characteristic is true?
Explanation
For LOW strain rates typical of normal activity (physiological strain rates of <0.1/s), bone is ELASTIC and DUCTILE (increasing ultimate strain with increasing strain rate). There is a ductile-to-brittle transition with increasing strain rate from normal to
supranormal rates. For EXTREMELY HIGH supranormal strain rates (>0.1/s, high impact trauma), bone is VISCOELASTIC and BRITTLE (low ultimate strain with increasing strain rate). Bone also becomes stronger and stiffer (higher modulus, steeper slope of stress-strain plot) as strain rate increases. This viscoelastic property helps in damping muscle contracture.
Natali and Meroi reviewed studies examining mechanical properties of bone. Mechanical properties are correlated with moisture, deformation rate, density and region of bone. Mechanical adaptation of bone is affected by strain rate (rate at which bone is deformed), strain mode (tension, compression, shear), strain direction (direction of strain relative to bone surface), strain frequency (cycles/second), stimulus duration (period over which deformation cycles are applied), strain distribution (pattern of strain magnitude across bone section) and strain energy (energy stored during deformation).
Illustration A shows the mechanical properties of bone with increasing strain rates. Incorrect Answers:
increase. During normal activity, as strain rate increases, bone is more ductile. With high impact trauma, bone is more brittle.
Question 89
In patients with neurofibromatosis, what is the most important sign of impending rapid progression of a spinal deformity?
Explanation
REFERENCES: Crawford AH, Schorry EK: Neurofibromatosis in children: The role of the orthopaedist. J Am Acad Orthop Surg 1999;7:217-230.
Durrani AA, Crawford AH, Chouhdry SN, Saifuddin A, Morley TR: Modulation of spinal deformities in patients with neurofibromatosis type 1. Spine 2000;25:69-75.
Question 90
A 6-year-old boy is being treated for acute hematogeneous osteomyelitis of the distal femur with intravenous antibiotics. The best method to determine the success or failure of initial treatment is by serial evaluations of which of the following studies? Review Topic
Explanation
Question 91
A 16-year-old high school football player sustains an injury to the left hip. The avulsed fragment identified by the arrow in Figure 34 represents the origin of which of the following structures?
Explanation
REFERENCES: Metzmaker JN, Pappas AM: Avulsion fractures of the pelvis. Am J Sports Med 1985;13:349-358.
Mader TJ: Avulsion of the rectus femoris tendon: An unusual type of pelvic fracture. Pediatr Emerg Care 1990;6:198-199.
Question 92
A 19-year-old running back lands directly on his anterior knee after being tackled. He has mild anterior knee pain, a trace effusion, a 2+ posterior drawer, a grade 1+ stable Lachman, no valgus laxity, and negative dial tests at 30° and 90°. What is the best treatment strategy at this time?
Explanation
Question 93
Radiotherapy for palliative pain control as the risk for pathological fracture is very small
Explanation
some centers, this procedure may contaminate the entire bone with tumor and make limb salvage nearly impossible if this is a sarcoma. If the incisional biopsy shows carcinoma, then intramedullary nailing with adjuvant radiotherapy would be completely appropriate.
Question 94
Which of the following growth factors binds and activates the lipoprotein receptor-related protein 5/6 (LRP5/6) during bone development? Review Topic
Explanation
Question 95
What is the most common type of malalignment after intramedullary nailing of distal 1/3 tibia fractures?

Explanation
McKee et al randomized 85 patients undergoing intramedullary tibial nailing using manual traction with the leg draped free versus standard fracture table positioning and traction. They found that manual traction is an effective technique that can save a significant amount of time without sacrificing the quality of reduction or fixation of tibial shaft fractures.
Question 96
A hockey player had a puck hit his foot. Radiographs taken immediately after the game were negative. He still has persistent pain 5 days after the injury and difficulty weight bearing. What is the best next step?
Explanation
Question 97
Figure 69 is the radiograph of a 9-year-old who has posterior hindfoot pain while running. What is the most likely diagnosis?

Explanation
Sever disease is a traction apophysitis at the Achilles tendon insertion on the calcaneus. Plain radiographs may be unremarkable for this condition. Other osteochondroses of the foot include Kohler disease (tarsal navicular), Freiberg infraction (lesser metatarsal head), and Thiemann disease (great toe phalanx).
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
Schantz K, Rasmussen F. Thiemann's finger or toe disease. Follow-up of seven cases. Acta Orthop Scand. 1986 Feb;57(1):91-3. PubMed PMID: 3962642. View Abstract at PubMed
Question 98
Figures 18a and 18b show the radiographs of a patient who has pain with walking. On careful questioning, it is determined that the discomfort occurs at push-off, or when the patient attempts to climb stairs. What nonsurgical option is most likely to ameliorate the symptoms?
Explanation
REFERENCES: Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 58-63.
Question 99
A 47-year-old woman has an asymptomatic pelvic mass that was discovered on routine gynecologic examination. A radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 7a through 7d. Metastatic work-up is negative. Treatment should consist of
Explanation
REFERENCES: Springfield DS, Gebhardt MS, Mcguire MH: Chondrosarcoma: A review. J Bone Joint Surg Am 1996;78:141-149.
Marco RA, Gitelis S, Brebach GT, Healey JH: Cartilage tumors: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:292-304.
Question 100
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 1, pp 532-533.
Severin E: Contribution to the knowledge of congenital dislocation of the hip joint.
Acta Chir Scand 1941;84:1.
