Orthopedic Surgery Board Review MCQs: Spine & Wrist | Part 1

Key Takeaway
This page offers Part 1 of a comprehensive Orthopedic Surgery Board Review MCQ bank. It features 100 high-yield, verified multiple-choice questions modeled on OITE and AAOS exams, designed for orthopedic surgeons and residents. Practice in Study or Exam mode for optimal board certification preparation.
About This Board Review Set
This is Part 1 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 1
This module focuses heavily on: Spine, Wrist.
Sample Questions from This Set
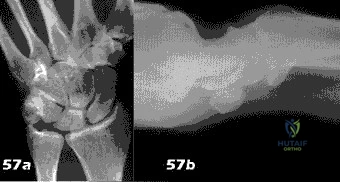
Sample Question 1: Figure 57a and 57b show the radiographs of a 57-year-old man who has pain inthe ulnar side of the wrist and hand. Examination shows tenderness at the base of the hypothenar area. Additional diagnostic testing should include...
Sample Question 2: A 10-year-old boy with an L1 myelomeningocele has a low-grade fever and a swollen thigh that is warm to touch and erythematous. AP and lateral radiographs are shown in Figures 24a and 24b. Management should consist of...
Sample Question 3: A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of...
Sample Question 4: Figure 22 reveals what anatomic variant of the lumbar spine?...
Sample Question 5: After reduction and pinning, the radial pulse is absent by both palpation and Doppler.Capillary refill in the fingers appears normal. What is the most likely explanation?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figure 57a and 57b show the radiographs of a 57-year-old man who has pain in the ulnar side of the wrist and hand. Examination shows tenderness at the base of the hypothenar area. Additional diagnostic testing should include
Explanation
Question 2
A 10-year-old boy with an L1 myelomeningocele has a low-grade fever and a swollen thigh that is warm to touch and erythematous. AP and lateral radiographs are shown in Figures 24a and 24b. Management should consist of
Explanation
REFERENCES: Lock TR, Aronson DD: Fractures in patients who have myelomeningocele. J Bone Joint Surg Am 1989;71:1153-1157.
Kumar SJ, Cowell HR, Townsend P: Physeal, metaphyseal, and diaphyseal injuries of the lower extremities in children with myelomeningocele. J Pediatr Orthop 1984;4:25-27.
Question 3
A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of
Explanation
REFERENCES: Froimson AI: Fracture of the coracoid process of the scapula. J Bone Joint Surg Am 1978;60:710-711.
Gil JF, Haydar A: Isolated injury of the coracoid process: Case report. J Trauma
1991;31:1696-1697.
Question 4
Figure 22 reveals what anatomic variant of the lumbar spine?
Explanation
REFERENCES: Brault JS, Smith J, Currier BL: Partial lumbosacral transitional vertebra resection for contralateral facetogenic pain. Spine 2001;26:226-229.
Quinlan JF, Duke D, Eustace S: Bertolotti’s syndrome: A cause of back pain in young people.
J Bone Joint Surg Br 2006;88:1183-1186.
Whelan MA, Feldman F: The variant lumbar pedicle. Neuroradiology 1982;22:235-242.
Question 5
After reduction and pinning, the radial pulse is absent by both palpation and Doppler. Capillary refill in the fingers appears normal. What is the most likely explanation?
Explanation
This is a classic extension-type supracondylar elbow fracture typically caused by a fall on an outstretched hand. The medial comminution of this fracture renders it predictably unstable and susceptible to varus malunion. Extra attention with fixation is required. In general, use of lateral-entry pins alone is effective for most supracondylar humeral fractures. The best technique for fixation with lateral-entry pins only involves maximization of pin separation at the fracture site, engaging sufficient bone in both the proximal segment and the distal fragment and using more than 2 lateral entry pins (if needed) for stability. In the presence of medial comminution, medial fixation also may be necessary.
Brachial artery spasm is the usual cause of absence of radial pulse if capillary refill is normal. Close postsurgical monitoring is warranted after reduction and pinning.
Question 6
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?
Explanation
REFERENCES: Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Posner MA: Flexor superficialis tendon transfers to the thumb: An alternative to the free tendon graft for treatment of chronic injuries within the digital sheath. J Hand Surg Am 1983;8:876-881.
Question 7
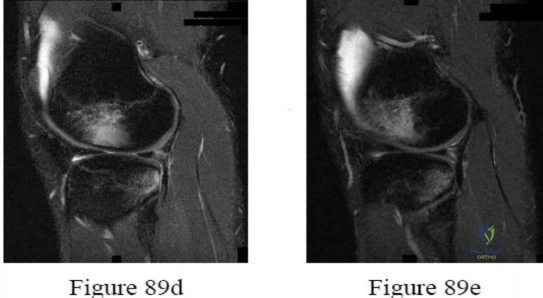
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include
Explanation
REFERENCES: Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Fisher SE, Shelbourne KD: Arthroscopic treatment of symptomatic extension block complicating anterior cruciate ligament reconstruction. Am J Sports Med 1993;4:558-564.
Question 8
Risks associated with vertebral compression fractures in the elderly population can be defined by which of the following? Review Topic
Explanation
fractures are more likely to fall and are five times more likely to sustain subsequent fractures than individuals without such a fracture. Analysis of data from Medicare patients with a vertebral fracture had an overall mortality rate that was approximately twice that of the matched controls. The survival rates following a fracture diagnosis, as estimated with the Kaplan-Meier method, were 53.9%, 30.9%, and 10.5% at 3, 5, and 7 years, respectively which were significantly lower than the rates for the controls. The mortality risk following a fracture was greater for men than for women. The mortality risk was greater when the fracture occurred at a younger age. The adjusted hazard ratio was 1.8 compared to the non-fracture group
Question 9
Os naviculare is present in which percentage of normal feet?
Explanation
Accessory navicular is found in 10% to 14% of normal feet, is generally asymptomatic, and involves 3 radiographic types. Type I represents a small ossicle embedded within the posterior tibial tendon, type II is larger with a synchondrosis, and type III is fused to the navicular tuberosity. Approximately 50% of patients with symptoms have flexible flatfoot; however, os naviculare is not directly associated with pes planovalgus deformity.
Subtalar arthroereisis describes the use of a sinus tarsi plug or implant to restrict eversion of the subtalar joint. This surgical procedure has been used in combination with tendon reconstruction for treatment of flexible flatfoot deformity. Known complications of subtalar arthroereisis include persistent sinus tarsi pain, foreign body reaction, implant failure, and osteonecrosis of the talus.
The FDL tendon travels within the same compartment adjacent to the posterior tibial tendon and is the most commonly used tendon transfer for treatment of stage II PTTD (strength characteristics are similar). The plantaris has inferior tendon strength to the FDL, and the peroneus longus travels in a different compartment than the FDL.
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Alvarez RG, Price J, Marini A, Turner NS, Kitaoka HB. Adult acquired flatfoot deformity and posterior tibial tendon dysfunction. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:215-229.
Pinney SJ, Lin SS. Current concept review: acquired adult flatfoot deformity. Foot Ankle Int. 2006 Jan;27(1):66-75. Review. PubMed PMID: 16442033. View Abstract at PubMed
Viladot R, Pons M, Alvarez F, Omaña J. Subtalar arthroereisis for posterior tibial tendon dysfunction: a preliminary report. Foot Ankle Int. 2003 Aug;24(8):600-6. PubMed PMID: 12956565. View Abstract at PubMed
Question 10
- A 30-year-old man underwent replantation of his dominant thumb at the metacarpophalangeal joint level 2 days ago. Since replantation, the temperature of the thumb has been between 87.8 F (31 C) and 93.2 F (34 C). The temperature is now 82.4 F (28 C), and there is brisk capillary refill and venous engorgement. Management at this time should include
Explanation
Question 11
What antithrombotic agent is a selective factor I0a inhibitor? Review Topic
Explanation
Question 12
A 20-year-old collegiate baseball pitcher has persistent deep shoulder pain. Examination reveals normal strength, 130 degrees of external rotation in abduction, 10 degrees of internal rotation in abduction, mild dynamic scapular winging, and equivocal findings on provocative tests for labral tears. Management should consist of
Explanation
REFERENCE: Burkhart SS, Morgan CD, Kibler WB: Shoulder injuries in overhead athletes: The “dead arm” revisited. Clin Sports Med 2000;19:125-158.
Question 13
At a minimum 2-year follow-up and compared with the metacarpophalangeal (MCP) joint, pyrolytic carbon resurfacing arthroplasties of the proximal interphalangeal (PIP) joint
Explanation
Wall and Stern published a report on MCP joint pyrolytic carbon arthroplasty for osteoarthritis and another on PIP joint pyrolytic carbon resurfacing arthroplasty for osteoarthritis. They found different outcomes, and MCP joint implants outperformed PIP joint implants. Of eleven MCP joint arthroplasties, two produced asymptomatic squeaking and clicking, whereas eleven of 31 PIP joint implants produced this problem. No dislocations were reported among the MCP joint implants, but five PIP joint dislocations were observed. Outcomes were measured by the Michigan Hand Outcomes Questionnaire in both studies and were satisfactory for the MCP joint implants, with an average score of 80. The PIP implants did not fare as well, showing a higher degree of pain along with an average score of 53. The authors noted that, in the 15 patients in the PIP study who had unilateral surgery, the uninvolved, nonsurgical hand motion was actually statistically significantly (P<0.01) better than the surgical hand. MCP joint motion increased from 62º before surgery to 76º after surgery, whereas PIP joint motion got worse after surgery, with the average motion decreasing from 57º to 31º.
Question 14
A 53-year-old patient is seen in the emergency department after sustaining a fall onto her left hip. A current radiograph is shown in Figure 40. What is the best treatment option?
Explanation
(a femoral fracture that occurs around or just distal to a loose stem, with adequate proximal bone stock). The stem is no longer fixed to proximal bone; therefore, retention of the femoral component is not recommended. Nonsurgical management is contraindicated because of the high risk of nonunion and malunion with significant component settling in the distal fragment and leg shortening. Revision femoral arthroplasty must attain distal fixation in adequate host bone, which is usually successful with a porous-coated cylindrical stem.
REFERENCES: Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Springer BD, Berry DJ, Lewallen DG: Treatment of periprosthetic femoral fractures following total hip arthroplasty with femoral component revision. J Bone Joint Surg Am 2003;85:2156-2162.
Question 15
Figures 12a and 12b show the radiographs of a 56-year-old man with diabetes mellitus who has had left foot swelling with no pain for the past several weeks. He denies any history of trauma. Examination reveals warmth, moderate swelling, no tenderness, and mild pes planus with standing. Pulses are palpable, and his sensory examination is grossly intact to light touch. Standing radiographs are shown in Figures 12c and 12d. What is the most likely diagnosis?
Explanation
REFERENCES: Brodsky JW: The diabetic foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 895-969.
Myerson MS: Diabetic neuroarthropathy, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 439-465.
Question 16
A 42 year-old-woman who underwent surgery for lumbar scoliosis 2 years ago now has fixed sagittal plane imbalance and severe back pain. Which of the following is considered a contraindication to isolated pedicle subtraction osteotomy for the treatment of iatrogenic flatback syndrome in this patient?
Explanation
REFERENCES: Potter BK, Lenke LG, Kuklo TR: Prevention and management of iatrogenic flatback deformity. J Bone Joint Surg Am 2004;86:1793-1808.
Bridwell KH, Lenke LG, Lewis SJ: Treatment of spinal stenosis and fixed sagittal imbalance. Clin Orthop 2001;384:35-44.
Question 17
An otherwise healthy 16-year-old boy who has had thoracolumbar pain with an increasingly worse deformity for the past 2 years now reports that the pain is worse at night. He responded well to nonsteroidal anti-inflammatory drugs initially, but they have become less effective. He denies any neurologic or constitutional symptoms. Examination is consistent with a mild thoracolumbar scoliosis and is otherwise normal. Laboratory studies show a normal CBC, erythrocyte sedimentation rate, and C-reactive protein. Standing radiographs show a 20 degrees left thoracolumbar scoliosis, and he has a Risser stage of 4. A bone scan shows increased uptake at L2; a CT scan through this level is shown in Figure 18. Management should now consist of
Explanation
REFERENCES: Cove JA, Taminiau AH, Obermann WR, Vanderschueren GM: Osteoid osteoma of the spine treated with percutaneous computed tomography-guided thermocoagulation. Spine 2000;25:1283-1286.
Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Pettine KA, Klassen RA: Osteoid-osteoma and osteoblastoma of the spine. J Bone Joint Surg Am 1986;68:354-361.
Question 18
Disadvantages of anterior-inferior plate fixation for acute clavicular fractures relative to superior plating include
Explanation
Question 19
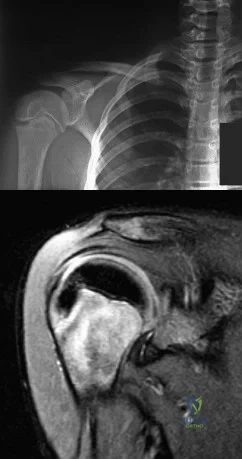
-Radiographs are shown in Figures 89a through 89c. What is the most likely diagnosis?
Explanation
Question 20
Which of the following is not a reported mode of failure for a constrained acetabular component?
Explanation
REFERENCES: Lachiewicz PF, Kelley SS: Constrained components in total hip arthroplasty. J Am Acad Orthop Surg 2002;10:233-238.
Anderson MJ, Murray WR, Skinner HB: Constrained acetabular components. J Arthroplasty 1994;9:17-23.
Fisher DA, Kiley K: Constrained acetabular cup disassembly. J Arthroplasty 1994;9:325-329.
Question 21
A 70-year-old former baseball catcher reports long-standing pain in the ring and little fingers. A gradient-echo MRI scan is shown in Figure 26. What is the most likely diagnosis?
Explanation
as indicated by the arrow. This technique suppresses the signal of the surrounding fat
and causes the stationary surrounding tissues to become intermediate in signal intensity.
The flowing blood is then easily identified with a bright signal because it does not absorb the radiofrequency pulse. Based on the findings, the diagnosis is an ulnar artery aneurysm, most likely caused by years of repetitive trauma as the result of catching baseballs. Neurolemmoma and giant cell tumor of the tendon sheath would be intermediately enhanced on this image sequence, and the continuity with the ulnar artery, demonstrated here, would not be expected. Lipomas are not enhanced using the gradient-echo technique. The chronic nature of the patient’s symptoms is not indicative of a hematoma, and the hematoma would be dark on this imaging sequence since it is stationary tissue.
REFERENCES: Koman LA, Ruch DS, Patterson Smith B, et al: Vascular disorders, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 2254-2302.
Holder LE, Merine DS, Yang A: Nuclear medicine, contrast angiography, and magnetic resonance imaging for evaluating vascular problems in the Hand: Vasospastic disorders. Hand Clin 1993;9:95-113.
Question 22
Figure 17 shows the radiograph of an 82-year-old right-hand dominant woman who fell while weeding her garden. She has severe right shoulder pain. She is neurovascularly intact. What is the most appropriate treatment? Review Topic

Explanation
Question 23
A 24-year-old man has bilateral hip pain. An examination and imaging studies (plain radiographs and MR imaging) confirm evidence of femoroacetabular impingement (FAI) with a CAM deformity in both hips. The patient mentions that he has a 19-year-old brother who has occasional hip pain. With respect to his brother’s pain, how should you counsel the patient?
Explanation
Evidence suggests that FAI is more common in siblings of patients with FAI, particularly those with a CAM deformity. It is unlikely this patient has well-established osteoarthritis, even in the presence of FAI.

CLINICAL SITUATION FOR QUESTIONS 145 THROUGH 147
Figures 145a and 145b are the radiographs of a 56-year-old man who has had persistent pain in his right groin since undergoing primary total hip surgery 11 months ago. His erythrocyte sedimentation rate (ESR) is 38 mm/h (reference range [rr], 0-20 mm/h) and C-reactive protein (CRP) level is 28 mg/L (rr, 0.08-3.1 mg/L). A hip aspiration performed while the patient was taking antibiotics demonstrated 3200 white blood cells/µL with no growth. Treatment should consist of
Question 24
Figures 1 and 2 are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable. If present, what is the most likely complication after surgical treatment in this scenario?
Explanation
and degenerative joint disease.
Question 25
What is the most important preoperative factor predicting conversion to total hip arthroplasty after arthroscopic surgery of the hip?
Explanation
The authors cited in the references examined large databases to determine the risk factors for conversion to total hip arthroplasty after arthroscopic surgery of the hip. In the study by Kester and associates, obesity had an odds ratio (OR) of 5.6 for conversion to hip arthroplasty, whereas age over 60 years had an OR of
Question 26
A 77-year-old woman with osteoporosis who underwent cemented total hip arthroplasty 12 years ago fell down a flight of stairs. A radiograph is shown in Figure 15. What is the best option for treating this fracture?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Paprosky WG (ed): Revision Total Hip Arthroplasty. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 64-69.
Question 27
Wear particles of ultra-high molecular weight polyethylene that are generated by total hip implants are predominantly of what diameter?
Explanation
REFERENCES: Campbell P, Ma S, Yeom B, McKellop H, Schmalzried TP, Amstutz HC: Isolation of predominantly submicron-sized UHMWPE wear particles from periprosthetic tissues. J Biomed Mater Res 1995;29:127-131.
Shanbhag AS, Jacobs JJ, Glant TT, Gilbert JL, Black J, Galante JO: Composition and morphology of wear debris in failed uncemented total hip replacement. J Bone Joint Surg Br 1994;76:60-67.
Maloney WJ, Smith RL, Schmalzried TP, Chiba J, Huene D, Rubash H: Isolation and characterization of wear particles generated in patients who have had failure of a hip arthroplasty without cement. J Bone Joint Surg Am 1995;77:1301-1310.
Question 28
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain? Review Topic

Explanation
Question 29
A previously healthy 30-year-old woman has neck pain and bilateral hand and lower extremity tingling with weakness after falling down stairs. She is alert and oriented. Examination reveals incomplete quadriplegia at the C6 level that remains unchanged throughout her evaluation and initial treatment. Radiographs show a bilateral facet dislocation of C6 on C7 without fracture. Attempts at reduction with halo cervical traction up to her body weight are unsuccessful. What is the next most appropriate step?
Explanation
REFERENCES: Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217.
Fardon DF, Garfin SR, Abitbol J (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 247-262.
Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. J Bone Joint Surg Am 1991;73:1555-1560.
Cotler JM, Herbison GJ, Nasuti JF, et al: Closed reduction of traumatic cervical spine dislocation using traction weights up to 140 pounds. Spine 1993;18:386-390.
Question 30
A healthy, active 72-year-old man trips and falls, landing on his left hip 10 weeks after an uncomplicated left primary uncemented total hip replacement. A radiograph taken 6 weeks after surgery and before the fall is shown in Figure 1. A radiograph taken after the fall is shown in Figure 2. He is unable to bear weight and is brought to the emergency department. Examination reveals a slightly shortened left lower extremity and some mild ecchymosis just distal to the left greater trochanteric region, but his skin is intact, without abrasions or lacerations. What is the most appropriate treatment?

Explanation
This patient has a periprosthetic femoral fracture with a loose femoral stem and normal femoral bone stock, representing a Vancouver type B2 fracture. The most appropriate treatment is fixation of the fracture, along with revision of the stem. Considering his age, bone quality, and activity level, a longer uncemented stem is most predictable. Although a cylindrical stem may also be used, the fluted stem option is the only uncemented choice listed and is the most appropriate option. A cemented stem is a poorer choice because it is difficult to keep the cement out of the fracture site, which would pose a risk for nonunion at the fracture. Also, overall poorer results have been associated with long cemented stems in healthy, active people. Surgery does not need to be delayed to allow the ecchymosis to resolve, and simple open reduction and fixation does not address the loose stem.
Question 31
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
REFERENCES: Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 47-55.
Question 32
What is the most common behavioral effect of anabolic steroid use in athletes?
Explanation
REFERENCES: Hartgens F, Kuipers H: Effects of androgenic-anabolic steroids in athletes. Sports Med 2004;34:513-554.
Blue JG, Lombardo JA: Steroids and steroid-like compounds. Clin Sports Med
1999;19:667-689.
Question 33
A 70-year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 34
A 47-year-old woman has a painful bunion of the right foot, and shoe wear modifications have failed to provide relief. Examination reveals a severe hallux valgus with dorsal subluxation of the second toe. Radiographs are shown in Figures 14a and 14b. The most appropriate management should include
Explanation
REFERENCE: Mann RA, Rudicel S, Graves SC: Repair of hallux valgus with a distal soft-tissue procedure and proximal metatarsal osteotomy: A long-term follow-up. J Bone Joint Surg Am 1992;74:124-129.
Question 35
At what age does the lateral epicondyle normally ossify in males?
Explanation
Question 36
A 24-year-old man sustains an injury to his right elbow after falling 10 feet. Radiographs are shown in Figures 41a and 41b. Treatment should consist of
Explanation
REFERENCE: Ring D, Jupiter JB, Sanders RW, et al: Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545-550.
Question 37
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?
Explanation
REFERENCES: Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167.
Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Miller TT: Magnetic resonance imaging of the knee, in Insall JN, Scott WN (eds): Surgery of the Knee, ed 4. Philadelphia, PA, Churchill Livingstone, 2006, vol 1, pp 201-224.
Question 38
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of
Explanation
REFERENCES: Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442.
Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
Tarr RR, Resnick CT, Wagner KS, Sarmiento A: Changes in tibiotalar joint contact areas following experimentally induced tibial angular deformities. Clin Orthop 1985;199:72-80.
Question 39
The safest surgical approach to the insertion of the tibial posterior cruciate ligament uses the interval between which of the following muscles?
Explanation
inlay reconstruction.
REFERENCES: Berg EE: Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy 1995;8:95-99.
Burks RT, Schaffer JJ: A simplified approach to the tibial attachment of the posterior cruciate ligament. Clin Orthop 1990;254:216-219.
Question 40
Figure 23 shows the postoperative radiograph of a patient who underwent an anterior cruciate ligament (ACL) reconstruction (with bone-patella tendon-bone autograft) that failed. He initially had loss of flexion postoperatively. What is the most likely cause of this failure?
Explanation
REFERENCES: Fu FH, Bennett CH, Latterman C, et al: Current trends in anterior cruciate ligament reconstruction: Part 1. Biology and biomechanics of reconstruction. Am J Sports Med 1999;27:821-830.
Fu FH, Bennett CH, Ma CB, et al: Current trends in anterior cruciate ligament reconstruction: Part II. Operative procedures and clinical correlations. Am J Sports Med 2000;28:124-130.
Question 41
A 14-year-old female has anal hemorrhoids. The General Surgical team has asked for a consultation in regards to her history of hand, wrist, and ankle joint pain and swelling over the past 3 years. Her physical examination reveals a swollen left wrist, right knee and left ankle. Lab work shows low hemoglobin, low albumin, elevated erythrocyte sedimentation rate (ESR), elevated antinuclear antibody (ANA) count, and a negative rheumatoid factor. Radiography of the affected joints are normal. What additional work up is required prior to her rectal surgery? Review Topic
Explanation
JIA is a persistent autoimmune inflammatory arthritis lasting more than 6 weeks in a patient younger than 16 years of age. Serologic testing for this condition will usually show elevated ESR/CRP, low hemoglobin, low albumin and an elevated anti-nuclear antibody (ANA) count, as well as negative rheumatoid factor and positive HLA-B27. Radiographs of the c-spine should be considered in patients undergoing intubation as cervical kyphosis, facet ankylosis, and atlantoaxial subluxation is associated with this condition.
Punaro et al. reviewed rheumatologic conditions in children. The typical patient with
oligoarticular JIA is a white female (5:1, F:M), with a peak onset between ages 1 and 3 years. Nearly half of patients have monoarticular involvement, with the knee and ankle being most commonly involved. Uveitis is typically chronic, bilateral, and asymptomatic.
Borchers et al. reviewed juvenile idiopathic arthritis (JIA). They state that no laboratory test can conclusively establish a rheumatic diagnosis. They state that laboratory tests will be negative for systemic inflammation and antinuclear antibody (ANA) test has no use in screening for JIA, as it has a high false positive rate.
Incorrect Answers:
Question 42
A 32-year-old male electrical worker complains of isolated left shoulder pain after a fall from 6 feet. Radiographs of the shoulder are seen in Figures A and B. The radiology technician was unable to obtain a good axillary view due to significant pain and muscle spasm. What would be the next most appropriate step in management? Review Topic
Explanation
Risk factors for posterior shoulder dislocation include epilepsy, electrocution and high-energy trauma. To make a diagnosis, standard views of the shoulder are required. These include an anteroposterior (AP) view, lateral scapular view and an axillary view. The axillary view is essential for diagnosis, but this requires the arm to be positioned in 20 - 30 degrees of abduction. If pain and muscle spasm restrict arm movement, the next most appropriate view would include a modified axially view,
such as a Velpeau view.
Robinson et al. reviewed posterior shoulder dislocations and fracture-dislocations. They state that apical oblique, Velpeau, or modified axial radiographs are preferable to other alternative axillary views, as they can be obtained with the arm in a sling. When an osseous injury is suspected, a CT scan and three-dimensional reconstruction can be useful in planning operative management.
Millet et al. wrote a JAAOS article on recurrent posterior shoulder instability. They state that 5 radiographic views, or advanced imaging, is essential to evaluate the shoulder. Characteristics to consider include, joint location, humeral head position, glenoid morphology (e.g., retroversion, hypoplasia, posterior glenoid rim), and impaction fracture of the humeral head.
Figure A and B show a normal shoulder radiograph with the shoulder positioned in internal rotation and external rotation. Illustration A shows the correct positioning of a patient to obtain a Velpeau view of the shoulder. Illustration B shows the correct positioning of a patient to obtain a Stryker notch view of the shoulder. This is used to asses for humeral head defects.
Incorrect Answers:
Question 43
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
Explanation
REFERENCES: Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337.
Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271.
Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Sneppen O, Fruensgaard S, Johannsen HV, Olsen BS, Sojbjerg JO, Anderson NH: Total shoulder replacement in rheumatoid arthritis: Proximal migration and loosening. J Shoulder Elbow Surg 1996;5:47-52.
Question 44
Which medication or supplement is recommended to promote healing of atypical subtrochanteric fractures?
Explanation
Use of teriparatide in association with fracture fixation promotes healing because these fractures are associated with delayed healing. The other responses are not associated with healing of these fractures.
RECOMMENDED READINGS
Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster D, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Koval K, Lane JM, McKiernan F, McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Sen HT, van der Meulen MC, Weinstein RS, Whyte M; American Society for Bone and Mineral Research. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010 Nov;25(11):2267-94. doi: 10.1002/jbmr.253. Erratum in: J Bone Miner Res. 2011 Aug;26(8):1987. PubMed PMID: 20842676. View Abstract at PubMed
Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, Cosman F, Curtis JR, Dell R, Dempster DW, Ebeling PR, Einhorn TA, Genant HK, Geusens P, Klaushofer K, Lane JM, McKiernan F,McKinney R, Ng A, Nieves J, O'Keefe R, Papapoulos S, Howe TS, van der Meulen MC, Weinstein RS, Whyte MP. Atypical subtrochanteric and diaphyseal femoral fractures: second report of a task force of the American society for bone and mineral research. J Bone Miner Res. 2014 Jan;29(1):1-23. doi:10.1002/jbmr.1998. Epub 2013 Oct 1. PubMed PMID: 23712442. View Abstract at PubMed
Question 45
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management? Review Topic
Explanation
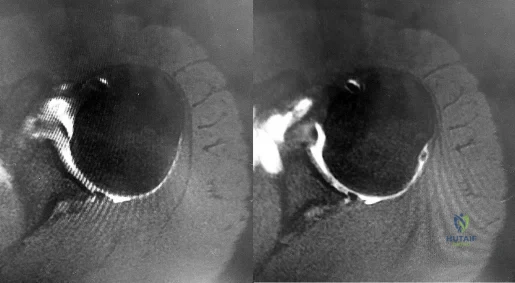
Question 46
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor. Correcr answer : C 40- A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
Explanation
A. Elbow arthroscopy with debridement
B. Immobilization and rest for 6 weeks
C. Corticosteroid injection
D. Open osteochondral autograft transfer
Osteochondritis dissecans of the capitellum is a painful condition that affects immature athletes who undergo repetitive compression of the radiocapitellar joint. Management is based primarily on the integrity of the articular cartilage surface and the stability of the lesion. Nonsurgical treatment is typically selected for patients
with early-grade, stable lesions, and it involves activity modification with cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in 3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment.
42- Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
Question 47
A 10-year-old boy has had wrist pain for the past 3 months. He denies any history of trauma. He reports mild tenderness associated with a palpable mass. A radiograph and biopsy specimens are shown in Figures 52a through 52c. What is the most likely diagnosis?
Explanation
REFERENCES: Schajowicz F: Tumors and Tumorlike Lesions of Bone: Pathology, Radiology, and Treatment, ed 2. Berlin, Springer-Verlag, 1994, pp 147-151.
Weiner SD: Enchondroma and chondrosarcoma of bone: Clinical, radiologic, and histologic differentiation. Instr Course Lect 2004;53:645-649.
Question 48
A 30 year-old male is involved in a motor vehicle collision and sustains a scapular fracture. In patients with scapular fractures, what other fracture is MOST commonly observed?
Explanation
Scapular fractures are associated with high-energy trauma, with motor vehicle collisions being a common mechanism of injury. These fractures are also associated with increased Injury Severity Scores and therefore clinicians need to be cognizant of concomitant injuries. In addition to associated orthopaedic injuries, pulmonary injuries (contusions, hemothorax, and pneumothorax) and head injuries are associated with scapular fractures. A CT chest should be considered in patients with scapula
fractures, to best visualize associated rib fractures and pulmonary injuries.
Baldwin et al. conducted a retrospective case control analysis using the US National Trauma Database that included 9,453 scapular fractures. In their study, the most commonly associated fractures were rib fractures (52.9%), followed by fractures of the spine (29.2%), clavicle (25.2%), and pelvis (15.3%). Lung and head injuries occurred in 47.1% and 39.1% of the cases, respectively.
Incorrect Answers:
(SBQ12TR.107) An 87-year-old female sustains the injury shown in Figure A after a fall from standing. At baseline, she ambulates with a walker in her home and lives with a 24-hour home health aide. She has a past medical history of stroke and mild dementia. Following medical optimization, what is the most appropriate treatment modality?

Intramedullary nail
Hemiarthroplasty
Closed reduction percutaneous pinning
Total hip arthroplasty
Sliding hip screw
At baseline, with minimal ambulatory status and dependence on a 24-hour home health aide, the best treatment choice is hemiarthroplasty.
Arthroplasty is the gold standard for displaced femoral neck fractures in the elderly. In community ambulators with relative independent lives, total hip arthroplasty (THA) is recommended. For minimal ambulator, hemiarthroplasty is recommended.
van den Bekerom et al. randomized 252 patients over 70-years-old to either THA or hemiarthroplasty for displaced femoral neck fractures. With increased blood loss, operative time and dislocation risk, they did not recommend THA unless there was good preoperative ambulatory status, and/or pre-existing osteoarthritis or rheumatoid arthritis.
Figure A exhibits a displaced femoral neck fracture Incorrect answers:
Question 49
273 In an athlete who has full, painless range of motion and a normal neurological examination, which of the following is considered an absolute contraindication to participation in a collision sport such as football?
Explanation
Thomas BE, et al. Cervical spine injuries in football players. J AM Acad Orthop Surg 1999;7:338-347
Torg JS et al: Neurapraxia of the cervical spinal with transientquadriplegia. JBJS Am 1986:68:1354-
Question 50
Figures 78a and 78b show the CT scans of a 22-year-old man with back pain after falling out of a tree. Examination reveals no palpable spinal step-offs, posterior spinal pain, and normal neurologic function in the lower extremities. Normal perineal sensation and normal rectal tone are present. What is the best management? Review Topic

Explanation
Question 51
An 85-year-old obese woman has left knee pain. She had surgery 5 years ago for a patellar nonunion after total knee arthroplasty that was complicated by infection, which was treated with implant removal and patellectomy. She has not been ambulatory since then. She states she is no longer on antibiotics. She has moderate pain, but her primary problem is instability of the knee. She has a 40° extensor lag. Darkening of the skin is present distal to the incision consistent with venous stasis changes. The erythrocyte sedimentation rate is 12 mm/h (reference range 0 to 20 mm/h) and her C-reactive protein level is 1.0 mg/L (reference range 0.08 to 3.1 mg/L). Left knee aspiration shows a white blood cell count of 800 and 20% neutrophils. What is the best next step?
Explanation
This patient is elderly, obese, and nonambulatory and has a chronic quadriceps tendon rupture after infected total knee arthroplasty. Her potential for ambulation after revision total knee arthroplasty is very low. Primary repair of the tendon is unlikely to be successful, even with augmentation, so revision total knee arthroplasty with primary quadriceps tendon repair and two-stage revision knee arthroplasty and quadricep repair with Achilles allograft are not the best management techniques. Extensor mechanism allograft could be done but would have a high failure rate in a patient of this size. No sign of infection is seen, based on laboratory studies, so a two-stage procedure is not necessary. The best management although not optimal, would be treatment in a drop-lock brace. Arthrodesis is also an option, but would have a high complication rate, and in a patient that is nonambulatory, a fused knee would be increasingly difficult with activities of daily living and mobility.
Question 52
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of
Explanation
REFERENCES: Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Moor TJ: Functional outcome following surgical excision of heterotopic ossification in patients with traumatic brain injury. J Orthop Trauma 1993;7:11-14.
Question 53
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and

Explanation
Question 54
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has
been shown to be successful in the treatment of traumatic instability.
REFERENCES: Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002.
Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
Kim SH, Ha KI, Park JH, et al: Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am 2003;85:1479-1487.
Question 55
CLINICAL SITUATION Figures 1 through 3 are the radiographs of a 25-year-old man who is brought to the emergency department after a motorcycle collision. He is complaining of isolated knee pain. Examination reveals swelling, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. Initial surgical management should consist of

Explanation
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Supine positioning is preferred for definitive fixation, but surgical approaches vary. Attempting to stabilize a medial partial articular pattern in the supine position from a lateral utility approach is fraught with difficulties. Lateral locked plating is not designed for this indication. The lateral utility approach allows for visualization of the centrolateral impaction and lateral meniscal peripheral capsular avulsion repair,
but when used alone leads to biomechanically unsound implant placement. The primary plate should be on the medial side of the tibia rather than the intact lateral column.
Question 56
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
REFERENCES: Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186.
Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Riester JN, Baker BE, Mosher JF, Lowe D: A review of scaphoid fracture healing in competitive athletes. Am J Sports Med 1985;13:159-161.
Question 57
The parents of a 14-year-old female soccer player are concerned about any future injury. They have been advised that she has the potential to play for the US Olympic team. They are especially concerned about the anterior cruciate ligament (ACL). What should you advise them? Review Topic
Explanation
Question 58
A 60-year-old right hand-dominant women fell on her outstretched arm and sustained an anterior shoulder dislocation. The shoulder is reduced in the emergency department and she is seen for follow-up 1 week later wearing a sling. Examination reveals that she has significant difficulty raising her arm in forward elevation and has excessive external rotation compared to the contralateral shoulder. What is the next most appropriate step in management? Review Topic
Explanation
in management should be MRI. If the findings are negative, suspicion of nerve injury should lead to electromyography.
Question 59
Figure 18a shows the clinical photograph of a 31-year-old man who has a slowly growing nodule on his right middle finger. It is minimally tender, and there is no erythema on examination. A biopsy specimen is shown in Figure 18b. What is the most likely diagnosis?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 1074.
Halling AC, Wollan PC, Pritchard DJ, et al: Epithelioid sarcoma: A clinicopathologic review of 55 cases. Mayo Clin Proc 1996;71:636-642.
Question 60
Figure 31 shows the radiograph of an 8-year-old boy who has a swollen forearm after falling out of a tree. Examination reveals that all three nerves are functionally intact, and there is no evidence of circulatory embarrassment. Management should consist of
Explanation
REFERENCES: Gibson WK, Timperlake RW: Operative treatment of a type IV Monteggia fracture-dislocation in a child. J Bone Joint Surg Br 1992;74:780-781.
Stanley EA, DeLaGarza JF: Part IV: Monteggia fracture. Dislocations in children, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 576-577.
Question 61
The patient experiences little improvement with activity modification and more physical therapy. An intra-articular corticosteroid injection provides excellent relief, but relief only lasts for 1 month. The player requests further treatment for his hip and is counseled regarding surgical intervention. Hip arthroscopy is performed. Intrasurgically, a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. Which treatment is most appropriate considering these findings?
Explanation

Video 67 for reference
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown.
The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. An ultrasound may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasound is not commonly used to diagnose labral pathology.
Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has important functions for hip stability and maintenance of the suction seal of the joint.
Question 62
An active 36-year-old woman with rheumatoid arthritis has continued forefoot discomfort despite the use of orthotics and shoe wear modifications. A radiograph and a clinical photograph are shown in Figures 26a and 26b. Treatment at this point should consist of
Explanation
REFERENCES: Ouzounian T: Rheumatoid arthritis of the foot & ankle, in Myerson MS (ed): Foot & Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 2, pp 1189-1204.
Mann RA, Thompson FM: Arthrodesis of the first metatarsophalangeal joint for hallux valgus in rheumatoid arthritis. J Bone Joint Surg Am 1984;66:687-692.
Coughlin MJ: Rheumatoid forefoot reconstruction: A long-term followup study. J Bone Joint Surg Am 2000;82:322-341.
Question 63
In a patient with rheumatoid arthritis of the wrist, which of the following extensor tendons is most at risk of rupture?
Explanation
REFERENCES: Vaughan-Jackson OJ: Rupture of extensor tendons by attrition at the inferior radioulnar joint: A report of two cases. J Bone Joint Surg Br 1948;30:528-530.
Papp SR, Athwal GS, Pichora DR: The rheumatoid wrist. J Am Acad Orthop Surg
2006;14:65-77.
Question 64
A 23-year-old woman with recurrent anterior instability undergoes an open Bankart procedure. Six months after surgery the patient reports shoulder

Explanation
Question 65
Two years after undergoing a total shoulder arthroplasty, a patient reports increasing pain, stiffness, and swelling, and has an increased white blood cell count. Radiographs show lucencies around the glenoid and humeral components. You suspect infection. Which of the following is the most likely responsible organism? Review Topic
Explanation
Question 66
A 6-year-old girl sustains an ankle injury after falling on roller blades. An AP radiograph is shown in Figure 68. Treatment should consist of which of the following?
Explanation
REFERENCES: Cass JR, Peterson HA: Salter-Harris type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070. Barmada A, Gaynor T, Mubarak SJ: Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-739.
Question 67
A 13-year-old boy was evaluated for leg length difference. His pelvis balanced when a 1-inch (2.54 cm) block was placed under his left foot. History revealed he had a left distal femur physeal fracture treated with casting at age 10. Radiographs show normal limb alignment, but his left distal femoral physis is closed and his left femur is 2.5 cm shorter than the right. All other physes are open. His bone age is equal to his chronologic age. What surgical treatments will best equalize his discrepancy? Review Topic
Explanation
Question 68
What imaging study should be obtained next to further evaluate this patient? Review Topic

Explanation
Question 69
A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of Review Topic
Explanation
Question 70
What is the most commonly reported complication following elbow arthroscopy?
Explanation
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of elbow arthroscopy.
J Bone Joint Surg Am 2001;83:25-34.
Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 71
Figures 4a through 4c show the radiographs, CT scans, and T1-weighted MRI scan of a 19-year old man who has had increasing right hip pain and decreasing range of motion for the past several years. He also reports intermittent “locking” of the hip. What is the most likely diagnosis?
Explanation
REFERENCES: Crotty JM, Monu JU, Pope TL Jr: Synovial osteochondromatosis. Radiol Clin North Am 1996;34:327-342.
Frassica F: Orthopaedic pathology, in Miller M (ed): Review of Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1996, pp 292-335.
Question 72
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?
Explanation
REFERENCES: Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.
Question 73
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
REFERENCES: Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Question 74
You are asked to evaluate the patient whose current clinical photographs are shown in Figures 46a and 46b following aortic valve replacement 9 days ago. He is currently taking anticoagulation medication. He has no systemic signs of sepsis. What is the best management?
Explanation
REFERENCES: Bowker JH, Pfeiffer MA (eds): The Diabetic Foot. St Louis, MO, Mosby, 2001,
pp 219-260.
Coughlin MJ, Mann RA: Soft tissue disorders of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1373-1397.
Question 75
An 83-year-old man has a painful mass of the great toe. Radiographs and a biopsy specimen are seen in Figures 22a and 22b. What is the most likely diagnosis?
Explanation
REFERENCES: Hamilton W, Breedman KB, Haupt HM, Lackman R: Knee pain in a 40-year-old man. Clin Orthop 2001;383:282-285,290-292.
Mizel M, Miller R, Scioli M (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 301-302.
Question 76
A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of
Explanation
REFERENCES: Cooney WP, Linscheid RL, Dobyns JH, Wood MB: Scaphoid nonunion: Role of anterior interpositional bone grafts. J Hand Surg Am 1988;13:635-650.
Fernandez DL: A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-737.
Stark HH, Rickard TA, Zemel NP, Ashworth CR: Treatment of ununited fractures of the scaphoid by illiac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am
1988;70:982-991.
Feldman MD, Manske PR, Welch RL, Szerzinski JM: Evaluation of Herbert screw fixation for the treatment of displaced scaphoid nonunions. Orthopedics 1997;20:325-328.
Question 77
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T 1 - and T 2 -weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?
Explanation
REFERENCES: Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Kausch T, Rutt J: Subcutaneous rupture of the tibialis anterior tendon: Review of the literature and case report. Arch Orthop Traum Surg 1998;117:290-293.
Question 78
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Explanation
REFERENCES: Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 79
Figures 18a and 18b show the radiographs of a 13-year-old baseball player who sustained a patellar dislocation with an associated lateral femoral condyle fracture. What ligament is attached to this fragment?
Explanation
REFERENCES: Jobe CM, Wright M: Anatomy of the knee, in Fu FH, Harner CD, Vince KG (eds): Knee Surgery. Baltimore, MD, Williams & Wilkins, 1994, pp 1-54.
Moore KL, Dalley AF: Lower limb, in Moore KL, Dalley AF (eds): Clinically Oriented Anatomy, ed 4. Philadelphia, PA, Lippincott, Williams & Wilkins, 1999, pp 503-664.
Question 80
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
Explanation
REFERENCES: Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Pape HC, Auf’m’Kolk M, Puffrath T, et al: Primary intramedullary femur fixation in multiple trauma patients with associated lung contusion: A cause of posttraumatic ARDS? J Trauma 1993;34:540-548.
Question 81
Figures 39a through 39c show a clinical photograph and the radiographs of a 32-year-old woman who has been unable to actively extend her dominant ring and small finger for the past two weeks. She has no history of trauma and has minimal pain. Examination reveals full passive range of motion (ROM) of the fingers. Active ROM of the wrist is extension of 40 degrees and flexion of 35 degrees. Active forearm pronation is 45 degrees, and supination is 50 degrees. Treatment should consist of
Explanation
“like a buzzsaw” on the overlying tendons. This is called a Vaughan-Jackson lesion when extensor tendons are ruptured at the distal radial-ulnar joint. Of the dorsal/extensor compartments, typically the digiti minimi is involved first and further ruptures progress radially as the hand ulnarly deviates and the other tendons sublux and are brought within range of the “buzzsaw.” The cited articles state that after a dorsal exposure the hypertrophic tenosynovium is removed from each tendon sytematically, and the wrist joint then evaluated. Any bony spicules which may further damage tendons are removed, and the distal ulna is excised. Tendon transfers, grafts, or repairs are then performed. Surgical results tend to be better with single or double tendon ruptures than with multiple tendon ruptures.
Question 82
What nerve is most likely to develop a traumatic neuroma following open reducation and internal fixation of a talar neck fracture via a posterolateral approach?
Explanation
REFERENCES: Swanson TV, Bray TJ, Holmes GB Jr: Fractures of the talar neck: A mechanical study of fixation. J Bone Joint Surg Am 1992;74:544-551.
Lawrence S, Botte M: The sural nerve of the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 83
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?
Explanation
REFERENCES: Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539.
Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than
2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
Robinson CM, Court-Brown CM, McQueen MM, et al: Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am
2004;86:1359-1365.
Question 84
A 7-month-old girl has had a severe flatfoot deformity since birth. The talar head is prominent in the medial plantar arch of the foot. No other deformities of the spine or extremities are present. Motor and sensory examinations of the extremities are normal. Figures 37a through 37c show simulated weight-bearing AP and lateral radiographs and a planter flexion lateral view. What is the most likely diagnosis?
Explanation
REFERENCES: Kodros SA, Dias LS: Single-stage surgical correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Stricker SJ, Rosen E: Early one-stage reconstruction of congenital vertical talus. Foot Ankle Int 1997;18:535-543.
Question 85
Patients in compensated shock (normal vital signs) are thought to be at risk for which of the following?
Explanation
REFERENCES: Schulman AM, Claridge JA, Carr G, et al: Predictors of patients who will develop prolonged occult hypoperfusion following blunt trauma. J Trauma 2004;57:795-800.
Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: Endpoints of resuscitation. J Trauma 2004;57:898-912.
Question 86
Figures 20a and 20b show the sagittal and coronal T1-weighted MRI scans of a patient’s left knee. Abnormal findings include
Explanation
REFERENCES: Ahn JH, Shim JS, Hwang CH, et al: Discoid lateral meniscus in children: Clinical manifestations and morphology. J Pediatr Orthop 2001;21:812-816.
Andrish JT: Meniscal injuries in children and adolescents: Diagnosis and management.
J Am Acad Orthop Surg 1996;4:231-237.
Question 87
In children with isolated zone II lacerations of the flexor tendon, poor digital motion is best correlated with
Explanation
REFERENCE: O’Connell SJ, Moore MM, Strickland JW, Frazier GT, Dell PC: Results of zone I and zone II flexor tendon repairs in children. J Hand Surg Am 1994;19:48-52.
Question 88
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?
Explanation
REFERENCES: Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
Martinez A, Sarmiento A, Latta LL: Closed fractures of the proximal tibia treated with a functional brace. Clin Orthop 2003;417:293-302.
Question 89
What is the most likely complication following treatment of the humeral shaft fracture shown in Figure 6?
Explanation
REFERENCES: Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
McCormack RG, Brien D, Buckley RE, et al: Fixation of fractures of the shaft of the humerus by dynamic compression plate or intramedullary nail: A prospective, randomised trial. J Bone Joint Surg Br 2000;82:336-339.
Question 90
Figure 21 shows the tomogram of a 26-year-old woman who sustained an axial load injury to her neck in a fall off a horse. What ligament is injured?
Explanation
REFERENCES: Levine AM, Edwards CC: Fractures of the atlas. J Bone Joint Surg Am 1991;73:680-691.
Kurz LT: Fractures of the first cervical vertebra, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 409-413.
Question 91
A 51-year-old woman who underwent a total knee arthroplasty 14 months ago for severe degenerative arthritis now reports progressive pain, swelling, and buckling of the knee. She must use crutches and is unable to negotiate stairs. Laboratory testing reveals a normal erythrocyte sedimentation rate and C-reactive protein. Radiographs of the patient are shown in Figures 17a through 17c. What is the most important test to further evaluate this problem?
Explanation
REFERENCES: Stiehl JB: Patellar instability in total knee arthroplasty. J Knee Surg 2003;16:229-235. Berger RA, Crossett LS, Jacobs JJ, et al: Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res 1998;356:144-153.
Question 92
Which of the following is most important to acheive a good outcome following a Syme amputation?

Explanation
Question 93
The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?
Explanation
REFERENCES: McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Lister GD, McGregor IA Jackson IT: The groin flap in hand injuries. Injury 1973;4:229.
Question 94
What is the most appropriate next step in the work-up of a patient with the asymptomatic lesion shown in Figure 23?
Explanation
REFERENCES: Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377-393.
Bullough PG, Walley J: Fibrous cortical defect and non-ossifying fibroma. Postgrad Med J 1965;41:672-676.
Skrede O: Non-osteogenic fibroma of bone. Acta Orthop Scand 1970;41:362-380.
Question 95
Epithelioid sarcoma most commonly occurs in which of the following anatomic locations?
Explanation
REFERENCES: Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 475.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby-Year Book, 1995, p 1074.
Question 96
A 32-year-old woman has an isolated left posterior wall acetabular fracture in which about 25% of the wall surface is involved. Which of the following criteria would indicate the need for surgical reduction and fixation?
Explanation
REFERENCES: Tornetta P III: Non-operative management of acetabular fractures: The use of dynamic stress views. J Bone Joint Surg Br 1999;81:67-70.
Keith JE Jr, Brashear HR Jr, Guilford WB: Stability of posterior fracture-dislocations of the hip: Quantitative assessment using computed tomography. J Bone Joint Surg Am 1988;70:711-714.
Question 97
A 3-year-old boy with severe cerebral palsy is unable to sit independently and does not crawl. Examination reveals a 40-degree hip flexion contracture by the Thomas test and 25 degrees of passive abduction. A radiograph of the pelvis shows subluxation of both hips, with a migration index of 30%. Management should consist of
Explanation
REFERENCES: Miller F, Cardoso Dias R, Dabney KW, et al: Soft-tissue release for spastic hip subluxation in cerebral palsy. J Pediatr Orthop 1997;17:571-584.
Cornell MS, Hatrick NC, Boyd R, et al: The hip in children with cerebral palsy: Predicting the outcome of soft tissue surgery. Clin Orthop 1997;340:165-171.
Question 98
A year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. What is the most appropriate management of this condition?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross- sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 99
Figures 9a and 9b are the radiographs of a 19-year-old woman with a painful juvenile bunion. The pathologic findings associated with this deformity include a

Explanation
The radiographs show a hallux valgus deformity with a laterally deviated distal metatarsal articular surface, a large intermetatarsal angle with medial deviation at the first metatarsocuneiform joint, an elongated medial collateral ligament, and a contracted lateral collateral ligament. There is no distal 1-2 transverse intermetatarsal ligament. The distal transverse ligament in the first interspace extends from the second metatarsal to the lateral (fibular) sesamoid, remains intact, and keeps the sesamoids in a lateral position as the first metatarsal head migrates medially.
RECOMMENDED READINGS
Coughlin MJ. Roger A. Mann Award. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int. 1995 Nov;16(11):682-97. PubMed PMID: 8589807.
View Abstract at PubMed
Coughlin MJ, Mann RA. Hallux valgus. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. 8th ed. Philadelphia, PA: Mosby Elsevier; 2007:183-226.
Question 100
Figures 48a and 48b are the axial and sagittal T1-weighted MR images of the L4-5 disc level of a 38-year-old man. He is symptomatic from the pathology shown. A surgeon would expect the neurological findings to include

Explanation
The pathology shown in the MR images is a right-sided far lateral herniated nucleus pulposus at L4-5, which, if symptomatic, would cause a radiculopathy of the exiting root, L4. A more common posterolateral herniation at L4-5 would cause irritation of the traversing root, L5. The L4 root has a sensory distribution over the anterior thigh that extends along the anterior shin but does not tend to reach the toes. The motor distribution is to the quadriceps and anterior tibialis muscles, with the predominant reflex effect being the patella reflex. The L5 root has a sensory distribution to the first dorsal web space of the foot, motor distribution to the EHL, and no specific reflex.
RECOMMENDED READINGS
Standaert CJ, Herring SA, Sinclair JD. The patient history and physical examination: Cervical, thoracic, and lumbar. In: Herkowitz HN, Garfin SR, Eismont FJ, Bell GR, Balderston RA, eds. Rothman-Simeone The Spine. Vol 1. 5th ed. Philadelphia, PA: Saunders Elsevier; 2006:171-186.
Bono CM, Wisneski R, Garfin SR: Lumbar disc herniations. In: Herkowitz HN, Garfin SR, Eismont FJ, Bell GR, Balderston RA, eds. Rothman-Simeone The Spine. Vol 1. 5th ed. Philadelphia, PA: Saunders Elsevier; 2006:967-991.
