OITE & ABOS Orthopedic Board Prep: Spine, Hand & Knee Arthroplasty MCQs | Part 260

Key Takeaway
This page features Part 260 of a comprehensive OITE/AAOS Orthopedic Board Review series. It provides 100 high-yield, verified MCQs for orthopedic residents and surgeons preparing for board certification exams. Questions cover Arthroplasty, Fracture, Knee, and Nerve in clinical scenarios.
About This Board Review Set
This is Part 260 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 260
This module focuses heavily on: Arthroplasty, Fracture, Knee, Nerve.
Sample Questions from This Set
Sample Question 1: An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are norm...
Sample Question 2: One year after undergoing anterior cervical decompression and fusion, what percentage of patients still have dysphagia?...
Sample Question 3: Assuming that the fracture shown in this radiograph (Figure 1) is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active...
Sample Question 4: A patient who underwent total knee arthroplasty now reports a loss of sensation in the area circled in Figure 38. This area is innervated by which of the following nerves?...
Sample Question 5: Figure 6 shows an object being held in an outstretched hand. To offset the moment created by the object (ignoring the weight of the forearm), the biceps must generate a force of...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An 18-year-old rugby player has had pain in his ring finger after missing a tackle 1 week ago. Examination reveals tenderness in the distal palm, and he is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs are normal. What is the most appropriate management?
Explanation
REFERENCES: Moiemen NS, Elliot D: Primary flexor tendon repair in zone I. J Hand Surg Br 2000;25:78-84.
Strickland JW: Flexor tendon injuries: I. Foundations of treatment. J Am Acad Orthop Surg 1995;3:44-54.
Question 2
One year after undergoing anterior cervical decompression and fusion, what percentage of patients still have dysphagia?
Explanation
Dysphagia after anterior cervical diskectomy and fusion is a common, usually transient finding after anterior cervical approaches to the spine. While it has been reported to occur in up to 70% of patients 2 weeks following surgery, in most cases the symptoms quickly resolve. There is, however, a small subset of patients for whom symptoms of dysphagia will persist. Lee and associates prospectively studied the rate of dysphagia after anterior cervical diskectomy and fusion, reporting a 15% rate of dysphagia at 12 months, and 12% at 24 months. Phillips and associates analyzed the 2-year data from the PCM FDE clinical trial and found a 12.1% incidence of dysphagia in the ACDF arm.
RECOMMENDED READINGS
Lee MJ, Bazaz R, Furey CG, Yoo J. Risk factors for dysphagia after anterior cervical spine surgery: a two-year prospective cohort study. Spine J. 2007 Mar-Apr;7(2):141-7. Epub 2007 Jan 22. PubMed PMID: 17321961. View Abstract at PubMed
Smith-Hammond CA, New KC, Pietrobon R, Curtis DJ, Scharver CH, Turner DA. Prospective analysis of incidence and risk factors of dysphagia in spine surgery patients: comparison of anterior cervical, posterior cervical, and lumbar procedures. Spine (Phila Pa 1976). 2004 Jul 1;29(13):1441-6. PubMed PMID: 15223936. View Abstract at PubMed
Edwards CC 2nd, Karpitskaya Y, Cha C, Heller JG, Lauryssen C, Yoon ST, Riew KD. Accurate identification of adverse outcomes after cervical spine surgery. J Bone Joint Surg Am. 2004 Feb;86-A(2):251-6. PubMed PMID: 14960668. View Abstract at PubMed
Phillips FM, Lee JY, Geisler FH, Cappuccino A, Chaput CD, DeVine JG, Reah C, Gilder KM, Howell KM, McAfee PC. A prospective, randomized, controlled clinical investigation comparing PCM cervical disc arthroplasty with anterior cervical discectomy and fusion. 2-year results from the US FDA IDE clinical trial. Spine (Phila Pa 1976). 2013 Jul 1;38(15):E907-18. doi: 10.1097/BRS.0b013e318296232f.
Rihn JA, Kane J, Albert TJ, Vaccaro AR, Hilibrand AS. What is the incidence and severity of dysphagia after anterior cervical surgery? Clin Orthop Relat Res. 2011 Mar;469(3):658-65. PMID: 21140251.View Abstract at PubMed
Question 3
Assuming that the fracture shown in this radiograph (Figure 1) is aligned on the anteroposterior radiograph and heals in this position, secondary to fracture malalignment, there will be loss of active

Explanation
This is a transverse proximal phalanx fracture with apex volar angulation. The fracture displaces into an apex volar angulated position under the pull of the central slip on the distal fragment and the interossei insertions at the base of proximal phalanx. Although it is possible to lose motion in flexion or extension of the MP or PIP joints, the biomechanics will not allow full extension of the PIP joint. If allowed to heal in apex palmar malunion, the predicted corresponding extensor lags are for a 10-degree lag at 16 degrees of angular deformity, a 24-degree lag at 27 degrees of deformity, and a 66-degree lag at 46 degrees of deformity. These fractures usually can be treated with closed reduction with or without percutaneous pinning. With surgical treatment, there may be loss of motion both at the MP and PIP joints.
Question 4
A patient who underwent total knee arthroplasty now reports a loss of sensation in the area circled in Figure 38. This area is innervated by which of the following nerves?
Explanation
REFERENCE: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 140-150.
Question 5
Figure 6 shows an object being held in an outstretched hand. To offset the moment created by the object (ignoring the weight of the forearm), the biceps must generate a force of
Explanation
REFERENCES: An KN, Chao ES, Kaufman KR: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 1-14.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-143.
Question 6
An otherwise healthy 35-year-old woman reports dorsal wrist pain and has trouble extending her thumb after sustaining a minimally displaced fracture of the distal radius 3 months ago. What is the next most appropriate step in management?
Explanation
REFERENCES: Christophe K: Rupture of the extensor pollicis longus tendon following Colles fracture. J Bone Joint Surg Am 1953;35:1003-1005.
Hove LM: Delayed rupture of the thumb extensor tendon: A 5-year study of 18 consecutive cases. Acta Orthop Scand 1994;65:199-203.
Question 7
A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the clavicle distal to a line drawn vertically to the coracoid process. Management should consist of
Explanation
REFERENCES: Robinson CM, Cairns DA: Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-782.
Deafenbaugh MK, Dugdale TW, Staeheli JW, et al: Nonoperative treatment of Neer type II distal clavicle fractures: A prospective study. Contemp Orthop 1990;20:405-413.
Question 8
Figures A and B show the six-month follow-up radiographs of a 62-year-old woman who sustained a hip fracture in a fall. Prior to the fall, the patient was active and had no difficulty with ambulation. The patient underwent open reduction and internal fixation with a sliding hip screw device. She has difficulty with ambulation, continues to walk with a walker, and reports startup pain. What is the most appropriate management at this time? Review Topic
Explanation
Question 9
The blood supply to the anterior cruciate ligament is primarily derived from what artery?
Explanation
REFERENCES: Arnoczky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
Arnoczky SP, Rubin RM, Marshall JL: Microvasculature of the cruciate ligaments and its response to injury. J Bone Joint Surg Am 1979;61:1221-1229.
Question 10
Figure 242 is the anteroposterior radiograph of a 28-year-old man who underwent resection and reconstruction for an Ewing sarcoma. What is the most common functional deficit encountered during rehabilitation?
Explanation

Question 11
A 34-year-old woman who is a professional skier (Figure 42)
Explanation

Question 12
- A 25-year-old patient who was wearing a seat belt in the back chair of a car involved in a head-on collision undergoes a laparotomy. During surgery, an injury to the sigmoid colon is identified and treated. Two days later the patient has back pain when sitting in a chair. What is the most likely diagnosis?
Explanation
Question 13
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of
Explanation
REFERENCES: Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Olney BW: Tarsal coalition, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 169-181.
Question 14
A 63-year-old woman had a primary total hip arthroplasty 7 years ago that included a proximally coated titanium stem, a cobalt alloy femoral head, a titanium hemispherical acetabular component, and a polyethylene liner. She did well for 4 years but has now had two dislocations and reports pain and weakness around the left hip. She denies any fevers, chills, or constitutional symptoms. On examination, the patient walks well without any signs of an antalgic or Trendelenburg gait. Her abductor mechanism demonstrates good strength. Her erythrocyte sedimentation rate and C-reactive protein level are normal. On radiographs, all components appear well fixed and in good alignment. What is the most appropriate treatment at this time?
Explanation
Trunnionosis is a recently recognized complication following total hip arthroplasty and can occur when a cobalt alloy femoral head is used on a titanium alloy or cobalt alloy femoral stem. Patients often present with pain or swelling around the hip but at times can present with instability. Certain femoral stem designs have been associated with increased reports of trunnionosis. In a patient with a cobalt alloy femoral head who presents with instability, swelling, and weakness around the hip, the potential for trunnionosis and
an adverse local tissue reaction should be considered.
Question 15
What percent of adult patients with rheumatoid arthritis test positive for rheumatoid factor?
Explanation
Question 16
During particle-induced osteolysis around implants, what cell secretes most of the interleukin-6 (IL-6)?
Explanation
REFERENCE: Bukata SV, Gelinas J, Wei X, et al: PGE2 and IL-6 production by fibroblasts in response to titanium wear debris particles is mediated through a Cox-2 dependent pathway. J Orthop Res 2004;22:6-12.
Question 17
intermittent PTH injections increase bone mass, 2) continous infusion lead to bone resorption, and 3) dosing should not continue past 2 yrs. Thus, intermittent parathyroid hormone is anabolic to bone and is used as a treatment of osteoporosis (forteo).
Explanation
a transmembrane protein that acts intracellularly to activate the G protein pathways. Myc is a proto-oncogene that encodes for a transcription factor involved in numerous cell- activation pathways, but is not directly phosphorylated by BMP receptor.
ß-catenin is an intracellular molecule that plays a key role in the Wnt signaling pathway. This pathway is also involved in osteoblastic differentiation, but differs in target proteins within the cell.
A 45-year-old previously healthy woman has experienced weakness and fatigability for 2 months. She states she feels best in the morning, but tires easily with exertion. If she sits and rests her strength improves, but she easily tires with each activity. When her fatigue is most severe, she has double vision. Physical examination is
positive for ptosis with upward gaze after 20 seconds. When she holds her arms out straight she shows good initial strength, but rapidly decreasing strength with time. What is the pathologic cause of her muscle weakness?
Ig antibodies at the neuromuscular (NM) junction
Decreased release of acetylcholine at the NM junction
Decrease in myelin sheath of axonal nerves with loss of NM junction
Absence of dystrophin with excess calcium at sarcolemma
The patient has myasthenia gravis, which has its onset in middle age and causes progressive weakness because of the loss of acetylcholine receptors secondary to autoimmune antibodies at the NM junction. Rest periods allow uptake of acetylcholine and initial strength, but easy fatigability. Treatment is aimed at immunomodulation; acetyl cholinesterase inhibitors often coupled with thymectomy can control symptoms.
Decreased release of acetylcholine at the NM junction is the effect of a nondepolarizing drug or toxin botulinum. Patients with muscular dystrophy lack dystrophin that acts at the sarcolemma to regulate calcium channels, and onset of this condition occurs at a younger age. The decrease in myelin indicates Charcot-Marie-Tooth disease and is
often seen with long axon degeneration, such as in the feet and lower legs.
You are studying a single continuous variable after administration of a defined treatment intervention. Your statistician informs you the data are not normally distributed. What is the best test to analyze the data?
Analysis of variance (ANOVA)
Regression analysis
Student t test
Mann-Whitney U test
The Mann-Whitney U test is used when data are nonparametric, meaning either not normally distributed or variances are not equal among groups. Both the Student t test and ANOVA are used with parametric, normally distributed data. A regression analysis is a
statistical model that allows for control of potentially confounding variables. It is used to assess the relationship between a dependent variable and (usually) multiple independent variables.
Which of the following is the mechanism of action of aspirin?
Inhibition of vitamin K-dependent carboxylation
Inhibition of factor Xa through antithrombin binding
Binding of cyclooxygenase (COX)-1 and COX-2
Direct thrombin inhibition
Glycoprotein IIIb agonist binding
Aspirin works by the irreversible binding of cycloxygenase (COX). This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect. In addition, there is a decrease in the level of prostaglandin production due to the COX-1 binding.
Aspirin's effects and respective mechanisms of action vary with dose:
Low doses (typically 75 to 81 mg/day) are sufficient to irreversibly acetylate serine 530 of cyclooxygenase (COX)-1. This effect inhibits platelet generation of thromboxane A2, resulting in an antithrombotic effect.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Intermediate doses (650 mg to 4 g/day) inhibit COX-1 and COX-2, blocking prostaglandin (PG) production, and have analgesic and antipyretic effects. Illustration A shows the mechanism of action of aspirin.
InCORRECT Answers: 1,2,4,5: Aspirin does not have any of these mechanisms of action.
A study is proposed in which 2 groups of patients are randomized to treatment with bisphosphonates or placebo. This is an example of what study type?
Crossover design trial
Parallel design trial
Cohort study
Case series
In a parallel design trial, participants are randomized to 2 or more groups, each of which receives a different treatment or intervention. For example, Group A receives the drug and Group B receives the placebo. This type of
design allows for comparison between groups. In a crossover design clinical trial, both groups receive both interventions over a defined time period. For example, Groups A and B both receive the drug as well as the placebo. This allows for within-participant comparisons. In a cohort study, patient groups are followed over time on the basis of having or not having received an exposure. Cohort studies are not randomized. In a case series, patients often receive a particular treatment and the outcomes are then examined.
An otherwise healthy 50-year-old man who is a smoker undergoes a posterior spine fusion with instrumentation for spondylolisthesis. What can the patient do to minimize his risk for pseudarthrosis?
Increase calcium and vitamin D intake
Avoid all nonsteroidal anti-inflammatory drugs (NSAIDs)
Maintain smoking cessation
Engage in early physical therapy to strengthen the trunk musculature
Smoking is the biggest risk factor for nonunion and should be strictly avoided. NSAIDs interfere with bone healing, but not as strongly as smoking. Early mobilization would potentially stress the construct, inducing movement that leads to nonunion. Without history of calcium and vitamin D deficiency, increasing intake would not decrease the risk of nonunion.
When making a comparison to autograft incorporation, the inflammatory process in allograft tissue anterior cruciate ligament (ACL) reconstruction
occurs earlier.
occurs later.
is prolonged.
is shortened.
Compared to similar autograft, allograft tissue demonstrates a prolonged inflammatory response, slower rate of biological incorporation and remodeling, and a higher proportion of large-diameter collagen fibrils. Native ACL inserts
into bone through a transition of 4 distinct zones: tendon, unmineralized fibrocartilage, mineralized fibrocartilage, and bone. This transition is not reproduced with tendon grafts, which instead heal with interposed fibrovascular scar at the graft-tunnel interface. The scar rapidly remodels to form perpendicular fibers resembling Sharpey fibers and, eventually, mature bone growth into the outer portion of the graft. The intra- articular portion of allograft undergoes an initial phase of necrosis followed by repopulation by host synovial cells into the acellular collagen scaffold.
Revascularization and maturation complete the ligamentization of graft tissue.
A researcher decides she wants to look at the current total number of patients who have methicillin-resistant Staphylococcus aureus (MRSA) infections in a hospital on 1 particular day. What is the researcher measuring?
Correlation coefficient of MRSA
Prevalence of MRSA
Incidence of MRSA
Relative risk of MRSA
The prevalence of a disease is a measure of the number of cases of a disease at or during a specific time point or time period. In this case, the researcher wants to know the prevalence of disease on a given day. Incidence measures new cases of a disease or event per unit of time. Correlation coefficient is a measure of how 2 things correlate with one another, while relative risk is a statistical outcome that is often used in case-control or cohort studies to provide a measure of the risk of a particular disease occurring when a certain exposure has already occurred.
A 48-year-old man who is scheduled to undergo total knee replacement has an X-linked clotting disorder that leads to abnormal bleeding and recurrent, spontaneous hemarthrosis. Before undergoing surgery, he should have replacement therapy of
protein C and S.
vitamin K.
von Willebrand factor.
factor VIII.
Hemophilia A is an X-linked recessive deficiency of factor VIII that can lead to significant bleeding problems including recurrent spontaneous hemarthroses that can lead to synovitis and joint destruction. von Willebrand disease is a lack of von Willebrand factor that leads to decreased platelet aggregation; more commonly patients have mucosal bleeding and not hemarthroses. Vitamin K deficiency is not hereditary; it is typically attributable to inadequate dietary intake, malabsorption, and loss of storage sites from hepatocellular disease. Protein C and S deficiencies are autosomal-dominant diseases that lead to thrombosis, not bleeding, as protein C and S shut off thrombin formation.
What is the recommended optimal timing of presurgical antibiotic administration to prevent infection in patients undergoing total joint replacement surgery?
Within 1 hour before incision
Within 2 hours before incision
Immediately after incision
Within 1 hour after incision
The current recommendation for antibiotic prophylaxis for major orthopaedic surgical procedures is to administer intravenous antibiotics within 1 hour of surgical incision. Redosing of antibiotics should occur 3 to 4 hours after the initial dose for procedures that extend beyond 3 to 4 hours. Little evidence supports postsurgical antibiotic use beyond 24 hours. As you move beyond 1 hour from time of administration of antibiotics, risk for infection increases and rates of bacterial cell death decline. It is not acceptable to
administer presurgical antibiotics after incision.
Bacterial resistance to antibiotics in biofilm is an example of
avoidance.
decreased susceptibility.
inactivation.
mutation. CORRECT answer: 1
Three basic mechanisms of antibiotic resistance have been identified: avoidance, decreased susceptibility, and inactivation. Biofilm formation is a classic example of avoidance, whereby the biofilm creates a physical barrier to the antibiotic. Bacteria can decrease their susceptibility to antibiotics by mutating the antibiotic target or generating a mechanism to inactivate the antibiotic. Biofilm formation develops when a sufficient mass of bacteria forms on a surface. The cell-to-cell signaling becomes sufficient to activate transcription of genes needed for biofilm formation in a process known as quorum sensing. Once the bacteria produce a mature biofilm, they enter a greatly reduced or stationary phase of growth. Lastly, high-shear
environments seem to stimulate biofilm production.
A patient with Paget disease who is intolerant of bisphosphonates is given calcitonin. What is the mechanism of action of calcitonin?
Promotes reabsorption of phosphate in the renal tubules
Interferes with osteoclast maturation
Interferes with intestinal absorption of calcium
Upregulates osteoblast formation
Calcitonin is a hormone that reduces serum calcium concentration by directly interfering with osteoclast maturation via receptors. Calcitonin inhibits phosphate reabsorption and decreases calcium reabsorption in the kidneys. By attenuating cartilage breakdown and stimulating cartilage formation via inhibitory pathways of matrix metalloproteinases, calcitonin also has a
chondro-protective effect on articular cartilage. Calcitonin has no major effects on intestinal absorption of calcium, but may aid in small-bowel secretion of sodium, potassium, chloride, and water. Calcitonin also has no receptor effect on osteoblasts.
A cartilage water content increase is the hallmark of which
osteoarthritis stage?
Prearthritis
Early
Late
Terminal
The first stage of osteoarthritis is marked by an increase in water content secondary to disruption of the matrix framework. This is followed by an increase in chondrocyte anabolic and catabolic activity in response to tissue damage. Wnt-induced signal protein 1 increases chondrocyte protease expression. Failure to restore tissue balance ultimately leads to continued destruction and osteoarthritis. One hallmark of osteoarthritic cartilage is a reduced repair mechanism attributable to decreased chondrocyte response to growth factor stimulation (transforming growth factor-alpha and insulin-like growth factor-1).
Mitochondrial dysfunction and increased production of reactive oxygen species may promote cell senescence, a progressive slowing of cellular activity. Microscopic evidence of cartilage degeneration begins with fibrillation of the superficial and transition zones, followed by disruption of the tidemark by subchondral blood vessels and eventual subchondral bone remodeling. This process ultimately leads to cartilage degradation with decreased water content in the late and terminal phases of osteoarthritis.
What is the plasma half-life of warfarin?
1 to 2 hours
4 to 6 hours
12 to 18 hours
36 to 42 hours
Warfarin, which is dosed daily, can take 72 to 96 hours to reach therapeutic levels. It has a plasma half-life of 36 to 42 hours. Low-molecular heparins have a plasma half-life of 4 to 5 hours, and fondaparinux has a half-life of 17 to 21 hours. Warfarin will not affect the International Normalized Ratio (INR) until 2 to 3 days after it is given. Patients on chronic warfarin therapy should
have treatment stopped 3 to 5 days before elective surgery to allow the INR to normalize.
A 70-year-old woman with a body mass index (BMI) of 34 and a history of hypercholesterolemia has elected to undergo total hip arthroplasty. Her son recently learned he has Factor V Leiden following an episode of pulmonary embolism. What are this patient's risk factors for thromboembolic disease?
Type of surgery, age, and BMI
Type of surgery, hypercholesterolemia, and age
Age, BMI, and hypercholesterolemia
BMI, type of surgery, and hypercholesterolemia
Risk stratification is one of the most critical clinical evaluations before undergoing total joint arthroplasty. Many factors have been identified to increase risk for venous thromboembolism (VTE). The major factors include previous VTE, obesity, type of surgery (such as total joint arthroplasty), hypercoagulable states, myocardial infarction, congestive heart failure, family history of VTE, and hormonal replacement therapy.
Hypercholesterolemia is not a risk factor for thromboembolic disease.
DNA replication occurs during which phase of the cell cycle?
M
S
R
G1
G2
The cell cycle consists of four distinct phases: initial growth (G1), DNA replication/synthesis (S), a gap (G2), and mitosis (M) (see illustration).
The G1 and G2 phases of the cell cycle represent the “gaps” or growth phases in the cell cycle that occur between DNA synthesis and mitosis. G0 cells are in a stable state and have not entered the cell cycle. During the S phase, the DNA is synthesized and replicated. During the M phase or mitosis, all genetic material divides into two daughter cells.
The cells are diploid (2N) in the G0 and G1 phases. The cells become tetraploid (4N) at the end of S and for the entire G2 phases. There is no R phase in the cell cycle.
What antithrombotic agent is a selective factor I0a inhibitor?
Warfarin
Low-molecular-weight heparin
Rivaroxaban
Aspirin
Rivaroxaban is a selective factor I0a inhibitor. Aspirin is a cyclooxygenase inhibitor. Low-molecular-weight heparin is a nonspecific anticoagulant. Warfarin is a vitamin K antagonist and reduces production of clotting factors II, VII, IX, and X.
A 68-year-old woman had advanced right knee arthritis and total knee replacement was planned. She learned she had primary biliary cirrhosis at age 41 and now has advancing liver failure. Preoperative coagulation tests show a baseline International Normalized Ratio (INR) of 1.36. Appropriate methods to prevent thromboembolic
disease as recommended by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee
Arthroplasty, include
use of mechanical prophylaxis (eg, pneumatic calf compressors) while in the hospital.
oral warfarin with a goal INR between 2.0 and 3.0.
low-dose warfarin for 3 weeks postsurgically beginning 48 hours after surgery.
no prophylaxis because this patient already is partially anticoagulated secondary to her liver disease.
The 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty, recommends the use of mechanical prophylaxis for patients at increased risk
for bleeding (including those with liver disease or hemophilia). This recommendation is the consensus of the workgroup that established these guidelines because there was insufficient evidence to justify a stronger recommendation in this clinical scenario. The other responses use no prophylaxis or pharmacological prophylaxis. Pharmacological prophylaxis is not recommended in patients who are at increased risk for bleeding.
The pharmacokinetics of which deep venous thrombosis (DVT) prophylactic agent are affected by liver function and dietary intake?
Dalteparin
Warfarin
Fondaparinux
Enoxaparin
Warfarin is an oral vitamin K antagonist that is rapidly absorbed from the gastrointestinal tract. It accumulates in the liver, where it is metabolized and excreted. The pharmacokinetics of warfarin can be affected by certain drugs or disease states that influence liver function. Fondaparinux is a synthetic factor Xa inhibitor that is eliminated through the kidneys. Both Dalteparin and Enoxaparin are low-molecular-weight heparins that activate antithrombin and inhibit factors Xa and IIa. Like Fondaparinux, they are eliminated through the kidneys and should be used with caution in patients with kidney disease.
What infection-control measure has been shown to have the most notable impact in reducing surgical-site infections?
Intravenous antibiotic administration within 1 hour of surgical incision
Screening and decolonization of patients colonized with methicillin-resistant
<em>Staphylococcus aureus</em>
Horizontal laminar flow
Use of enclosed body exhaust suits
Timely administration of prophylactic antibiotics is the most important factor shown to decrease surgical-site infections. The use of horizontal laminar flow and body exhaust suits has not been shown to significantly affect infection rates.
The resistance to pullout of a screw in osteoporotic bone is increased by all of the following EXCEPT?
Placement parallel to the trabecular pattern
Purchase in cortical bone
Use of a fixed angle (locking screw construct)
Tapping prior to screw placement
Augmentation with polymethylmethacrylate
Of the options listed, tapping prior to screw placement is the only variable that does not increase the pullout strength of a screw in osteoporotic bone.
Cornell reviews internal fixation in osteoporotic bone. According to this article, the quality of the bone is the primary determinant of the holding power of an individual screw. Other factors that increase the pullout strength include fixation in cortical bone (cortical bone has greater mineral density and, therefore, greater resistance to screw pullout than trabecular bone), screws placed parallel to the trabecular pattern, and screw fixation augmented with PMMA. The addition of a locking plate will also increase the resistance to failure by creating a fixed angle construct. Tapping prior to placement of the screw has not been shown to increase resistance to pullout, on the contrary studies have shown
this decreases resistance to pullout.
Turner et al examined the holding strength of small and large diameter screws in healthy bovine and diseased human bone. They found the screw diameter, trabecular orientation of the bone, and mineral content of the bone all affect the holding strength. A larger diameter screw, parallel placement to the trabecular pattern, and purchase in bone with a higher density all increase the holding strength.
Gigantism affects which region of the growth plate labeled in Figure A?
A
B
C
D
E
Gigantism, like achondroplasia, affects the proliferative zone (Region C of Figure A) of the growth plate. In Figure A, Region A is the epiphysis, Region B is the resting zone, Region D is the hypertrophic zone, and Region E is the metaphysis. Illustration A is another depiction of the physis which is labeled. Gigantism is typically caused by a pituitary adenoma which over secretes growth hormone. Its effect on the proliferative zone results in bone overgrowth and excessive height and limb length. Acromegaly may also be
caused by a pituitary adenoma that over secretes growth hormone, but has its effect once the physis has closed.
Plain radiographs do not provide an accurate assessment of bone mineral density (BMD) until what percentage of mineral has been lost?
Question 18
Which of the following nerves is most commonly injured during revision surgery following a Bristow procedure?
Explanation
REFERENCES: Norris TR: Complications following anterior instability repairs, in Bigliani LU (ed): Complications of Shoulder Surgery. Baltimore, MD, Williams and Wilkins, 1993,
pp 98-116.
Flatow EL, Bigliani LU, April EW: An anatomic study of the musculocutaneous nerve and its relationship to the coracoid process. Clin Orthop 1989;244:166-171.
Question 19
Embolic material generated during total knee arthroplasty (TKA) shown in Figure 29 is composed of which of the following substances?
Explanation
REFERENCES: Markel DC, Femino JE, Farkas P, et al: Analysis of lower extremity embolic material after total knee arthroplasty in a canine model. J Arthroplasty 1999;14:227-232.
Pell AC, Christie J, Keating JF, et al: The detection of fat embolism by transoesophageal echocardiography during reamed intramedullary nailing: A study of 24 patients with femoral and tibial fractures. J Bone Joint Surg Br 1993;75:921-925.
McGrath BJ, Hsia J, Boyd A, et al: Venous embolization after deflation of lower extremity tourniquets. Anesth Analg 1994;78:349-353.
Question 20
A 12-year-old girl has had right knee pain for the past 3 months. Radiographs and a coronal T 2 -weighted MRI scan are shown in Figures 10a through 10c. A biopsy specimen is shown in Figure 10d. What is the most appropriate treatment for this lesion?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Question 21
A college basketball player is struck in the eye by a player’s hand while driving to the basket. Fluorescein evaluation reveals the injury shown in Figure 18. Management should consist of
Explanation
REFERENCES: Brucker AJ, Kozart DM, Nichols CW, et al: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby-Year Book, 1991, pp 650-670.
Zagelbaum BM: Treating corneal abrasions and lacerations. Phys Sports Med 1997;25:38-44.
Question 22
- Which of the following is considered an advantage of an unreamed intramedullary nail over a reamed intramedullary nail?
Explanation
Question 23
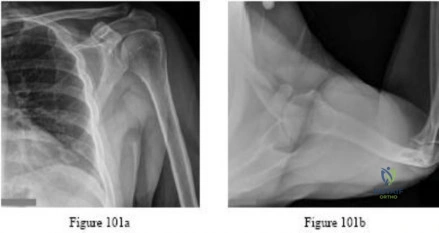
The radiographic finding in Figure 58 is indicative of what type of acetabular fracture?

Explanation
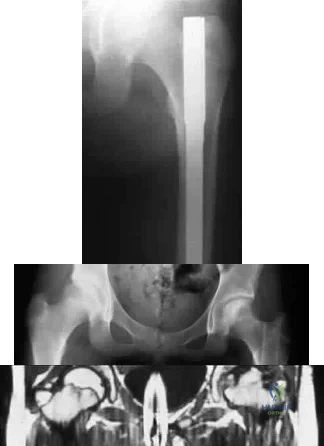
(SBQ12TR.58) A 35-year-old male was involved in a high speed motorcycle accident. He has a closed head injury, bilateral pulmonary contusions and splenic rupture. His orthopaedic injuries are shown in Figure A. He has a blood pressure of 90/50 mm Hg and a heart rate of 115, despite aggressive resuscitation. An arterial blood gas reveals that his blood lactate is 3.5 and base deficit is -6 mmol/L. Following successful closed reduction of the right hip in the operating room with a percutaneous inserted Schantz pin, what is the next most appropriate treatment for his orthopaedic injuries? Review Topic

Bilateral open reduction and internal fixation
Open reduction internal fixation on the right, reamed intramedullary nailing on the left
Temporizing external fixation on the right, open reduction and internal fixation on the left
Bilateral reamed intramedullary nailing
Bilateral temporizing external fixation
This patient presents with features of hemodynamic instability and a high injury severity score. The next most appropriate treatment would be temporizing external fixation bilaterally. This patient meets the criteria for damage control orthopaedics.
Damage control orthopaedics is an approach that contains and stabilizes orthopaedic injuries so that the patient's overall physiology does not undergo further inflammatory insult. As a result, external fixation of femoral shaft fracture and pelvic stabilization is an effective treatment under this strategy. Other indications include vascular injury and severe open fracture.
Pallister et al. reviewed the effects of surgical fracture fixation on the systemic inflammatory response to major trauma. They show that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure. However, early fracture surgery increases the post-traumatic inflammatory response, which carries a higher complication rate compared to temporary fixation.
Tisherman et al. created clinical guidelines for the endpoints of resuscitation. Level I data found that standard hemodynamic parameters do not adequately quantify the degree of physiologic derangement in trauma patients. The initial base deficit, lactate level, or gastric pH should be used to stratify patients with regard to the need for ongoing fluid resuscitation.
Pape et al. retrospectively reviewed the impact of early total care vs. damage control orthopaedics in the treatment of femoral shaft fractures in polytrauma patients. They found a significantly higher incidence of acute respiratory distress syndrome (ARDS) with intramedullary nailing (15.1%) compared to external fixation (9.1%) when DCO subgroups were compared.
Figure A is a pelvic AP radiograph showing a right hip fracture-dislocation with an ipsilateral femoral shaft fracture. On the left side there is a displaced pertrochanteric hip fracture.
Incorrect Answers:
Question 24
Anaerobic weight training has what effect in a prepubescent 10-year-old male athlete? Review Topic
Explanation
Question 25
A 24-year-old man who plays golf noted the immediate onset of pain on the ulnar side of his hand and has been unable to swing a club for the past 6 weeks after striking a tree root with his club during his golf swing. Examination reveals full motion of the wrist, diminished grip strength, and tenderness over the hypothenar region. A CT scan of the hand and wrist is shown in Figure 26. Management should consist of
Explanation
REFERENCES: Carroll RE, Lakin JF: Fracture of the hook of the hamate: Acute treatment. J Trauma 1993;34:803-805.
Whalen JL, Bishop AT, Linscheid RL: Nonoperative treatment of acute hamate hook fractures. J Hand Surg Am 1992;17:507-511.
Question 26
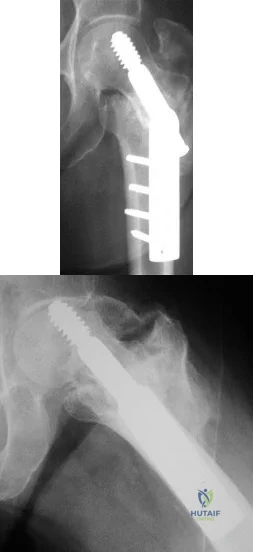
- Figure 16 shoes the AP radiograph of a 32-year-old man with a fracture cephalad to the fovea of the femoral head. A CT scan shows a single head fragment. After closed reduction of the hip, there is 5 mm of residual articular incongruity. Management should now include
Explanation
Question 27
Figures 55a through 55c are the clinical photograph and radiographs of a 5-year-old boy who fell and injured his right elbow. His radial pulse is thready. Which neurologic deficit most commonly is associated with this injury?
Explanation
This injury is a type III supracondylar humerus fracture with posterolateral displacement. The area of ecchymosis is anteromedial, corresponding to the proximal spike of the humeral metaphysis. The brachial artery is likely tented over this spike, leading to diminished perfusion. The median nerve also resides in this area, and any neurological deficit is likely in its most vulnerable fibers, those of the anterior interosseous nerve (AIN). The AIN contains no sensory fibers, and its motor function involves flexion of both the thumb IP joint and the index distal IP joint.
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.

Question 28
-In the shoulder position of 90-degree forward flexion and internal rotation, what is the most important static stabilizer of the glenohumeral joint?
Explanation
A 17-year-old high school wrestler sustains an abrasion over the posterior aspect of his right elbow during a match. During the next few days the abrasion becomes erythematous and he is placed on oral cephalexin 500 mg four times per day. The erythema extends proximally despite the antibiotic regimen. The patient is afebrile, there is no fluid collection associated with the lesion, and his elbow joint is not involved.
Question 29
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
REFERENCES: Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233.
Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526.
Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
Stanton-Hicks M, Baron R, Boas R, et al: Complex regional pain syndromes: Guidelines for therapy. Clin J Pain 1998;14:155-166.
Question 30
What anatomic site is considered at highest risk for pathologic fracture?
Explanation
REFERENCES: Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
Harrington KD, Sim FH, Enis JE, Johnston JO, Diok HM, Gristina AG: Methylmethacrylate as an adjunct in internal fixation of pathological fractures: Experience with three hundred and seventy-five cases. J Bone Joint Surg Am 1976;58:1047-1055.
Question 31
A study is proposed in which 2 groups of patients are randomized to treatment with bisphosphonates or placebo. This is an example of what study type?
Explanation
Question 32
Which of the following is a recognized predictor of mortality after hip fracture?

Explanation
The study by Richmond et al looked at 836 patients treated for a hip fracture and found that this injury is not associated with significant excess mortality amongst patients older than age 85. However, in younger patients, those with ASA classifications of 3 or 4 have significant excess mortality following hip fracture that persists up to 2 years after injury.
Question 33
When reconstructing the anterior cruciate ligament (ACL), what is the most common source of potential autograft failure? Review Topic
Explanation
Question 34
Which of the following factors increases the risk of sciatic nerve injury in primary total hip arthroplasty (THA)?
Explanation
REFERENCES: DeHart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.
Anas P, Felix B: Evaluation and prevention of postoperative complications, in Neurologic Injury in Revision THA. New York, NY, Springer Verlag, 1999, pp 361-371.
Question 35
A patient undergoes an arthroscopic debridement for lateral epicondylitis. Postoperatively she reports pain and a sense of clicking of the elbow. Examination reveals apprehension to supination, load, and extension. What structure has been injured resulting in the clinical presentation?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 318.
O’ Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 36
Which of the following nerves is most commonly injured during arthroscopy of the ankle?
Explanation
Question 37
Figure 3 shows the clinical photograph of a wrestler who has an acute mass in his ear. He does not wear protective headgear. The area is mildly tender and without erythema. Management should consist of
Explanation
REFERENCES: Kaufman BR, Heckler FR: Sports-related facial injuries. Clin Sports Med 1997;16:543-562.
Griffin CS: Wrestler’s ear: Pathophysiology and treatment. Ann Plastic Surg 1992;28:131-139.
Question 38
A patient who was involved in a motor vehicle accident 2 days ago now reports neck pain. He denies any other symptoms. Radiographs reveal a type II odontoid fracture that is 2 mm anteriorly displaced. Management consists of halo vest immobilization in extension, and repeat radiographs reveal that the fracture is completely reduced. The patient is discharged to home, but later that evening he notes difficulty swallowing while trying to eat dinner. What is the most likely cause of this difficulty?
Explanation
REFERENCES: Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
Glaser JA, Whitehill R, Stamp WG, Jane JA: Complications associated with the halo-vest: A review of 245 cases. J Neurosurg 1986;65:762-769.
Question 39
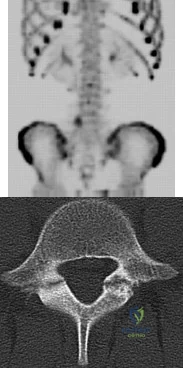
A 13-year-old girl presents with back pain for 6 months. Figures A and B are SPECT scan and CT images taken at the time of presentation. What is the most likely diagnosis? Review Topic
Explanation
patient
has
spondylolysis.
Spondylolysis is a common cause of back pain in children/adolescents. It is common in sports with repetitive hyperextension (gymnasts, weightlifters, football linemen). It is best seen on lateral and oblique radiographs, CT (best study to diagnose and delineate anatomy), and SPECT.
Saifuddin et al. reviewed the orientation of the pars fracture. They found that only 32% of defects were oriented within 15° of the 45° lateral oblique plane and would be
visible on oblique radiographs. They thus recommend CT scans for spondylolysis.
Cheung et al. reviewed spondylolysis and spondylolisthesis. They advocate pars repair for symptomatic spondylolysis and low-grade, mobile spondylolisthesis with pars defects cephalad to L5 and for those with multiple-level defects.
Figure A is a 99mTc-MDP SPECT scan showing increased uptake at the right L5 pars interarticularis. Figure B is an axial helical CT image showing bilateral spondylolysis at L5. Illustration A is a corresponding sagittal reconstruction image demonstrating right pars fracture into the right L5 superior facet. Illustration B shows the appearance of osteoblastic metastasis (green arrow). Illustration C shows the options for pars repair.
Incorrect
Question 40
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient’s neurologic recovery can be best determined by
Explanation
REFERENCES: Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1185-1194.
Question 41
Figures 28a through 28c show the MRI scans of a 30-year-old woman who weighs 290 lb and has low back and left leg pain. She also reports frequent urinary dribbling, which her gynecologist has advised her may be related to obesity. Examination will most likely reveal
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Appleton, WI, Century-Crofts, 1976.
Hollinshead WH (ed): Anatomy for Surgeons: The Back and the Limbs, ed 3. Philadelphia, PA, Harper & Rowe, 1982.
Question 42
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
REFERENCE: Ebraheim NA, Haman SP, Xu R, Stanescu S, Yeasting RA: The lumbosacral nerves in relation to dorsal SI screw placement and their locations on plain radiographs. Orthopedics 2000;23:245-247.
Question 43
Figures 26a and 26b show the radiograph and MRI scan of a 22-year-old man with knee pain. What is the most likely diagnosis?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 44
A 65-year-old woman sustained an axial load on the arm followed by an abduction injury after falling on ice. Treatment in the emergency department consisted of reduction of an anterior dislocation. She now has a positive drop arm sign and a positive lift-off test. An MRI scan is shown in Figure 9. Based on these findings, management should consist of
Explanation
REFERENCES: Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes.
J Am Acad Orthop Surg 1999;7:300-310.
Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654.
Walch G, Boileau P: Subluxations and dislocations of the tendon of the long head of the biceps. J Shoulder Elbow Surg 1998;7:100-108.
Question 45
What phase of overhead throwing puts the rotator cuff at most risk of injury from internal impingement?
Explanation
and symptoms.
Question 46
A 56-year-old man with poorly controlled diabetes mellitus has rapidly developing and advancing erythema, warmth and swelling with bullae formation on the left lower extremity. These findings appear to be advancing proximally several millimeters per hour. Culture results are most likely to reveal
Explanation
the diagnosis is confirmed and an extensive debridement should be performed. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score can be utilized to risk stratify people who have signs of cellulitis and determine the likelihood of necrotizing fasciitis being present. It uses six serologic measures, including C-reactive protein, total white blood cell count, hemoglobin, sodium, creatinine and glucose.
Polymicrobial synergistic infection was the most common cause of necrotizing fasciitis (48 patients; 53.9%) with streptococci and enterobacteriaceae being the most common isolates. Group-A streptococcus was the most common cause of monomicrobial necrotizing fasciitis. The most common associated comorbidity was diabetes mellitus (63 patients; 70.8%).
Question 47
A 56-year-old woman sustains a type IIIB open tibial shaft fracture. She undergoes irrigation and debridement and intramedullary nailing with flap coverage 24 hours later. Cultures are taken pre-debridement and post-debridement. She develops a surgical site infection at 6 weeks, which requires removing the hardware and placing show Commented [1]: an external fixator. Deep cultures are most likely to pathogens found in
Explanation
In another study, before any interventions were performed, initial aerobic and anaerobic cultures of the wounds of 117 consecutive open extremity fractures grades I through III were obtained. The results of these cultures were correlated with the development of a wound infection. If an infection occurred, the organism grown from the infected wound was compared with any organism grown from the primary wound cultures. Of the initial cultures, 76% (89/117) did not demonstrate any growth, while the other 24% (28/117) only grew skin flora. There were only 7 (6%) wound infections, and 71% (5/7) initially did not grow any organisms. Of the isolates that grew from the initial cultures, none were the organisms that eventually led to
Question 48
During spinal deformity surgery, which of the following is the most specific early indicator of an intraoperative injury to the spinal cord? Review Topic
Explanation
Question 49
What mechanism of injury is most likely to cause a fracture of the anteromedial facet of the coronoid?
Explanation
(SBQ12TR.86) Figure A shows intraoperative radiographs of a 45-year-old patient with a left elbow injury. What would be the next most appropriate step in this patients care?

Early range of motion
Hinged elbow brace for 4 weeks
Repair lateral collateral ligament
Remove and upsize implant
Remove and downsize implant
The intraoperative images are consistent with overstuffing of the ulnohumeral joint during a radial head replacement. The most appropriate next step would be removing and downsizing the implant.
Overstuffing the radiohumeral joint by >2.5 mm can significantly alter elbow kinematics. It has also shown to lead to pain and early joint disease. The most sensitive method to assess for overstuffing of the joint is by direct visualisation intraoperatively. This can be performed by visualising the lateral aspect of the ulnohumeral joint when the radial head is resected and comparing this to when the trial radial head is reduced in place. In comparison, radiographic asymmetry of the medial ulnohumeral joint has been shown to be less sensitive. Radiographic findings of incongruity of ulnohumeral joint only occurs when significant overlengthening of the radius occurs.
Frank et al. examined the effect of radial head thickness in seven cadaver specimens. They found that incongruity of the medial ulnohumeral joint would only become apparent radiographically after overlengthening of the radius by >or=6 mm.
Doornberg et al. examined seventeen computed tomography scans of the elbow to investigate the height of the radial head relative to the lateral edge and central ridge of the coronoid process. They found that the radial head was on average only 0.9 mm more proximal than the lateral edge of the coronoid process.
Figure A shows intraoperative radiographs of a patient that has undergone a radial head arthroplasty. There is significant widening of the medial ulnohumeral joint on an AP radiograph as well as widening of the ulnohumeral joint on the lateral radiograph,
Incorrect Answers:
Question 50
A 34-year-old male arrives intubated with a closed head injury to the trauma bay after a motor vehicle accident. After initial hospital workup and resuscitation, he is transferred to the intensive care unit. In addition to multiple systemic injuries, he sustained the closed injury shown in Figure A. Intracompartmental pressure monitoring of the limb measure in a range from 28-30 mm Hg. Which of the following sustained blood pressure measurements would support the treatment of limb fasciotomy? Review Topic 1 110/60 mmHg 2 115/55 mmHg 3 92/64 mmHg

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. A clinical assessment is the diagnostic cornerstone of acute compartment syndrome. However, the intracompartmental pressure measurement has been advocated to help confirm the diagnosis in patients where there remains uncertainty after clinical exam - especially with intubated patients. An absolute compartment pressure >30 mm Hg or a difference in diastolic pressure and compartments pressure (delta p) <30 mm Hg may help to confirm the necessity for fasciotomy.
McQueen et al. prospectively reviewed 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Olson et al. provide a review of compartment syndrome for the lower extremity. They discuss a variety of injuries and medical conditions that may initiate acute compartment syndrome, including fractures, bleeding disorders, and other trauma. Although the diagnosis is primarily a clinical one, they also recommend supplementation with compartment pressure measurements in equivocal cases.
Figure A shows a closed comminuted tibial shaft fracture. Incorrect Answers:
Question 51
A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient? Review Topic
Explanation
Question 52
When treating a proximal tibia fracture, the surgeon decides to (1) use blocking screws in the proximal fragment, and (2) pick the intramedullary nail based on the location of the Herzog curve. Which of the following combinations will best prevent the classic deformity associated with this fracture?
Explanation
Up to 58% of proximal tibial fractures are malaligned. Malalignment arises because the nail fits loosely in the wide metaphyses and cannot control alignment. Without close fit of the nail at the fracture site, the nail will not align the fracture independent of a stable reduction and careful nail path. Blocking screws serve to reduce the size of the proximal metaphyseal canal and guide final nail passage.
Stinner et al. discuss strategies in proximal tibial fracture nailing. They describe an accurate starting point (using the twin peaks AP view or fibular bisector AP view, and flat plateau lateral view). They emphasize fracture reduction prior to reaming and implant placement.
Hiesterman reviewed nailing of extra-articular proximal tibial fractures. Techniques described include blocking screws, unicortical plating, using a universal distractor, nailing in flexion/locking in extension, semiextended nailing (including percutaneous suprapatellar quads-splitting approaches), multiple proximal interlocking screws (>=3).
Illustration A shows placement of a coronal blocking screw. Illustration B shows placement of a sagittal blocking screw. Illustration C shows the effect of the Herzog curve. A more distal Herzog curve leads to a "wedge" effect and fracture displacement whereas a proximal Herzog curve contains the fracture. The "wedge" effect occurs as the nail is seated and impinges on the posterior cortex of the distal segment accentuating an apex anterior deformity because of the effective widening of the nail above the bend and posterior force on the distal segment to match the nail shape.
Incorrect Answers:
Question 53
A 26-year-old ballet dancer reports posterolateral ankle pain, especially with maximal plantar flexion. Examination reveals maximal tenderness just posterior to the lateral malleolus, and symptoms are heightened with forced passive plantar flexion. Radiographs are shown in Figures 42a and 42b. What is the most likely cause of the patient’s symptoms?
Explanation
REFERENCES: Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Hamilton WG: Foot and ankle injuries in dancers, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1241-1276.
Question 54
A 72-year-old woman who sustained a cerebrovascular accident 9 months ago now has a fixed elbow flexion contracture of 80 degrees. Management should consist of
Explanation
REFERENCE: Waters RL, Keenan ME: Surgical treatment of the upper extremity after stroke, in Chapman MW (ed): Operative Orthopedics. Philadelphia, PA, JB Lippincott, 1988, vol 2,
pp 1449-1450.
Question 55
A 20-year-old woman sustained the closed injury shown in Figures 49a and 49b in a motor vehicle accident. Examination reveals that this is an isolated injury; however, she has a complete radial nerve palsy. Management should consist of
Explanation
REFERENCES: Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am 2004;29:144-147.
Foster RJ, Swiontkowski MF, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
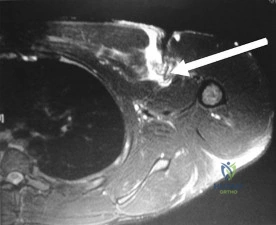
Question 56
Figure 41 shows the MRI scan of a 38-year-old weightlifter. What does the arrow on the MRI scan indicate? Review Topic
Explanation
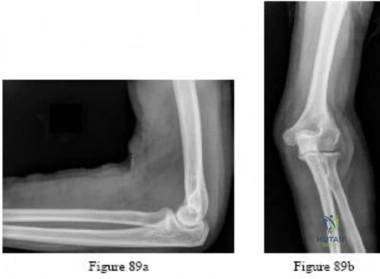
Question 57
.Figures 89a and 89b are the radiographs of an 18-year-old woman who has had elbow pain after falling on an outstretched hand. She is evaluated 5 days after the injury. Examination reveals the wrist is normal and her elbow has a limited arc of motion of 30 to 90 degrees of flexion/extension and 20 to 20 degrees of pronation and supination, with tenderness isolated to the lateral side of the elbow. What is the most appropriate treatment option?
Explanation
Question 58
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling’s test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis? Review Topic
Explanation
Question 59
Examination of a 28-year-old woman reveals a moderate hallux valgus deformity and a prominence of the medial eminence. She reports that she can participate in all activities, wear 3-inch heels with minimal discomfort, and walk in a 1-inch heel with no pain. However, she is concerned that the deformity will get worse and requests recommendations regarding surgical correction. What is the best course of action?
Explanation
REFERENCES: Donley BG, Tisdel CL, Sferra JJ, Hall JO: Diagnosing and treating hallux valgus: A conservative approach for a common problem. Cleve Clin J Med 1997;64:469-474.
Teitz CC, Hu SS, Arendt EA: The female athlete: Evaluation and treatment of sports-related problems. J Am Acad Orthop Surg 1997;5:87-96.
Question 60
Figures below show the radiographs obtained from a 79-year-old woman who has been experiencing increasing tibial pain 10 years after undergoing revision total knee arthroplasty. No evidence of infection is seen. What is the most appropriate treatment?

Explanation
Stems are available for cemented and press-fit implantation. To be effective, press-fit stems should engage the diaphysis, as shown in Figures 3 and 4. They also assist in obtaining correct limb alignment. Short metaphyseal-engaging stems are associated with failure rates that range between 16% and 29%. Cemented stems may be shorter than press-fit stems, because they do not have to engage the diaphysis. Short, fully cemented stems offer the advantage of metaphyseal fixation. Hybrid stem fixation makes use of the metaphysis for cement fixation with metaphyseal cones or sleeves and diaphyseal-engaging press-fit stems.
Question 61
A 52-year-old man has pain in the sternal area after landing on his right shoulder in a fall from his bicycle. In addition, he reports that he had difficulty swallowing and breathing immediately after the fall, but the symptoms resolved. A CT scan reveals a posterior sternoclavicular dislocation. Initial management should include
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont IL, American Academy of Orthopaedic Surgeons, 1999, pp 287-297.
Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, vol 2, pp 1010-1017.
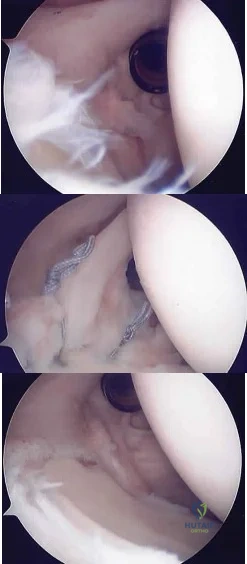
Question 62
A 20-year-old man has activity-related deep-seated shoulder pain in his dominant right shoulder. He has taken 3 months off training as a college javelin thrower, and management consisting of physical therapy has failed to provide relief. Shoulder arthroscopic views are shown in Figures 16a through 16c. What is the underlying association with this condition? Review Topic
Explanation
Question 63
A 63-year-old man with type I diabetes mellitus who underwent open forefoot amputation now has a high fever, and an elevated WBC count and blood glucose levels. Repeat laboratory studies the day after surgery show a WBC count of 9,500/mm 3 , a serum albumin level of 1.9 g/dL, and a total lymphocyte count of 1,900/mm 3 . Examination reveals that he is afebrile, and his blood glucose level is now normal. An ultrasound Doppler of the dorsalis pedis artery shows an ankle-brachial index of 0.6. A transcutaneous partial pressure measurement of oxygen at the ankle joint shows a level of 38 mm Hg. What is the best course of action?
Explanation
REFERENCE: Pinzur MS, Stuck RM, Sage R, et al: Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am 2003;85:1667-1672.
Question 64
The CT scan reveals a nondisplaced greater trochanteric fracture. The patient is now experiencing severe pain. What is the most appropriate treatment at this time?
Explanation
This patient presents with significant polyethylene wear, which can lead to both osteolysis and synovitis. However, synovitis usually manifests as a mild to moderate chronic ache, which should explain the discomfort. Although infection should always be ruled out with new-onset pain, no clinical parameters suggest acute hematogenous infection. Similarly, without any mention of back pain or neuropathy, radicular pain from the spine is unlikely. If this patient has a nondisplaced greater trochanteric fracture noted on MR imaging, the optimal immediate mode of treatment is to not rush into surgery despite the mild osteolysis. The patient’s severe pain is likely attributable to the nondisplaced greater trochanteric fracture rather than wear-induced synovitis, which typically presents as a mild to moderate ache. It is recommended to
allow the fracture to heal to avoid fracture displacement. Once the fracture is healed, a revision surgery with liner exchange can be recommended. Based on this clinical scenario, the acetabular component is within what is largely considered the “safe-zone” in THA. Despite this patient’s dislocations, the preferred treatment modality is to revise to a constrained liner. This patient had a well-functioning hip for longer than 15 years. Therefore, conversion to a constrained liner is the best treatment.
Question 65
A 38-year-old woman fell from a ladder onto her right hip. The radiographs and CT scan are shown in Figures 52a through 52d. What is the best surgical approach for this fracture?
Explanation
REFERENCES: Letournel E: The treatment of acetabular fractures through the ilioinguinal approach. Clin Orthop Relat Res 1993;292:62-76.
Matta JM: Operative treatment of acetabular fractures through the ilioinguinal approach:
A 10-year perspective. Clin Orthop Relat Res 1994;305:10-19.
Question 66
An 82-year-old woman fell on her right shoulder 2 days ago. She is alert, oriented, and in mild discomfort. Prior to falling, she lived alone and functioned independently. Examination reveals extensive ecchymosis extending to the midhumeral region. Her neurovascular examination is normal. Radiographs are shown in Figures 41a and 41b. What is the most appropriate management?
Explanation
REFERENCES: Neer CS II: Displaced proximal humeral fractures: I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-1089.
Bigliani LU, Flatow EL, Pollock RG: Fractures of the proximal humerus, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA,
WB Saunders, 1998, pp 352-354.
Question 67
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor. Correcr answer : C
Explanation
Figure 1 is the radiograph of a 12-year-old baseball player who has posterolateral elbow pain with throwing. The area of interest is designated by the black arrow. His range of motion and strength are full. No previous treatment has been provided. What is the most appropriate initial treatment?
Elbow arthroscopy with debridement
Immobilization and rest for 6 weeks
Corticosteroid injection
Open osteochondral autograft transfer
Osteochondritis dissecans of the capitellum is a painful condition that affects immature athletes who undergo repetitive compression of the radiocapitellar joint. Management is based primarily on the integrity of the articular cartilage surface and the stability of the lesion. Nonsurgical treatment is typically selected for patients
with early-grade, stable lesions, and it involves activity modification with cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in 3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment.
Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
Question 68
What portion of the pitching phase creates forces approaching the tensile limit of the medial collateral ligament?
Explanation
REFERENCES: Fleisig GS, Andrews JR, Dillman CJ, et al: Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med 1995;23:233-239.
Lynch JR, Waitayawinyu T, Hanel DP, et al: Medial collateral ligament injury in the overhand-throwing athlete. J Hand Surg 2008;33:430-437.

Figure 5a Figure 5b
Question 69
Venous thromboembolism may occur after total joint arthroplasty. The risk of this complication is elevated in patients with
Explanation
Obesity, a prior history of venous thromboembolism, and metabolic syndrome have all been associated with an increased risk of thromboembolism. A recent meta-analysis showed that diabetes had no significant relationship with venous thromboembolism following hip or knee arthroplasty. Tranexamic acid is an antifibrinolytic agent that has been shown to reduce blood loss substantially following hip and knee arthroplasty. It has also been shown to be safe in patients with severe medial comorbidities and a prior history of venous thromboembolism.
Question 70
A 16-year-old swimmer has right shoulder pain with activity. She describes the continued sensation that her shoulder is “loose.” She has been in physical therapy for 7 months to work on strengthening the muscles around her shoulder and scapula. She denies being able to voluntarily dislocate her shoulder. Upon examination, you can feel the humeral head slide over the glenoid rim both anteriorly and posteriorly with the load and shift test. She has a grade III sulcus sign. What is the most appropriate next step?
Explanation
Nonsurgical treatment with activity modification and physical therapy is generally considered the first-line approach for young athletes with multidirectional instability (MDI) of the shoulder. Physical therapy focuses on exercises to strengthen the scapular stabilizers and rotator cuff muscles and restore scapulohumeral rhythm. Although a definitive length of time
to assess physical therapy failure is not known, many surgeons believe that a patient with MDI should undergo at least 6 months of physical therapy and activity modification before considering surgery. Although an open inferior capsular shift has historically been considered the gold standard for surgical treatment for MDI, studies have shown good success rates for arthroscopic capsulorrhaphy. Arthroscopy can allow a surgeon to assess all intra-articular structures and address a patient’s particular problem based on arthroscopic findings.

CLINICAL SITUATION FOR QUESTIONS 21 THROUGH 25
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow.
Question 71
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?
Explanation
REFERENCES: Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Csizy M, Buckley R, Tough S, et al: Displaced intra-articular calcaneal fractures: Variables predicting late subtalar fusion. J Orthop Trauma 2003;17:106-112.
Question 72
The comparative outcomes of needle aponeurotomy (NA) and collagenase Clostridium histolyticum (CCH) use in the treatment of Dupuytren contracture indicate that patients treated with CCH have
Explanation
A. Proximal row carpectomy
B. Vascularized bone graft
C. Radial shortening osteotomy
D. Capitate shortening osteotomy
Osteonecrosis of the capitate is a rare condition that presents with an insidious onset of dorsal wrist pain. When nonsurgical treatment fails to alleviate symptoms, surgical intervention is appropriate. When collapse of the capitate is present, partial excision of the capitate with interposition, partial wrist arthrodesis, or wrist denervation can be considered. In the absence of collapse, capitate-preserving options are available. Vascularized grafting is a mainstay of treatment. Grafting with distal radius vascularized grafts based on the 1,2 intercompartmental supraretinacular artery or the 4 + 5 extensor compartment artery and second metacarpal graft based on the first dorsal metacarpal artery have been described.
Question 73
What is the most common foot and ankle deformity in patients with arthrogryposis?
Explanation
REFERENCES: Guidera KJ, Drennan JC: Foot and ankle deformities in arthrogryposis multiplex congenita. Clin Orthop 1985;194:93-98.
Handelsman JE, Badalamente MA: Neuromuscular studies in clubfoot. J Pediatr Orthop 1981;1:23-32.
Dias LS, Stern LS: Talectomy in the treatment of resistant talipes equinovarus deformity in myelomeningocele and arthrogryposis. J Pediatr Orthop 1987;7:39-41.
Question 74
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty?
Explanation
REFERENCES: Visotsky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.
Zuckerman JD, Scott AJ, Gallagher MA: Hemiarthroplasty for cuff tear arthropathy. J Shoulder Elbow Surg 2000;9:169-172.
Question 75
Which of the following factors is most critical to the success of a meniscal allograft transplantation?
Explanation
cryopreservation of the graft to ensure cell viability is not necessary. There is a limited immune response to musculoskeletal allografts; therefore, immunosuppression, as is required for visceral organ transplantation, is not indicated.
Question 76
A 40-year-old woman has local back pain and intense burning pain in her perianal region after being shot twice in the back. Motor and sensory examination of her lower extremities reveals no apparent deficit. She has present but decreased sensation in her perianal region, an intact anal wink, good rectal tone, and an intact bulbocavernosus reflex. Radiographs and CT scans are shown in Figures 3a through 3d. What is the next most appropriate step in management?
Explanation
REFERENCES: Bracken MB, Shepard MJ, Holford TR: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. JAMA 1997;277:1597-1604.
Waters RL, Adkins RH: The effects of removal of bullet fragments retained in the spinal canal: A collaborative study by the National Spinal Cord Injury Model Systems. Spine
1991;16:934-939.
Stauffer ES, Wood RW, Kelly EG: Gunshot wounds of the spine: The effects of laminectomy.
J Bone Joint Surg Am 1979;61:389-392.
Question 77
The condition seen in Figure 60 is attributable to

Explanation
Cephallomedullary implants for treatment of proximal femur fractures have gained in popularity over the last decade. Although these implants have improved outcomes for certain fracture types, multiple complications are associated with this implant. Failure may occur secondary to implant design (for example, mismatch of curvature of the nail to the femur, which can result in distal anterior cortical perforation).
RECOMMENDED READINGS
Bazylewicz DB, Egol KA, Koval KJ. Cortical encroachment after cephalomedullary nailing of the proximal femur: evaluation of a more anatomic radius of curvature. J Orthop Trauma. 2013 Jun;27(6):303-7. doi: 10.1097/BOT.0b013e318283f24f. PubMed PMID: 23287752.
View Abstract at PubMed
Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults. Cochrane Database Syst Rev. 2008 Jul 16;(3):CD000093. doi: 10.1002/14651858.CD000093.pub4. Review. Update
in: Cochrane Database Syst Rev. 2010;(9):CD000093. PubMed PMID: 18646058. View Abstract at PubMed
Question 78
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?
Explanation
REFERENCE: Ruedi T, Murphy WM (eds): AO Principles of Fracture Management. New York, NY, Thieme, 2000, p 221.
Question 79
A 12-year-old girl is seen after tripping and twisting her ankle earlier in the morning. She had immediate pain and swelling and was unable to bear weight. Radiographs are shown in Figures 80a through 80c. Appropriate treatment should consist of which of the following? Review Topic

Explanation
Question 80
An 18-year-old man underwent open reduction and internal fixation of a tibial spine avulsion and a posterolateral corner repair. Two years later, he underwent lateral collateral ligament (LCL) and posterolateral corner reconstruction because of instability. Examination reveals a pronounced lateral varus knee thrust when ambulating. Varus stress in 30 degrees of flexion produces a 10-mm opening that is eliminated in extension. The Lachman’s test is 2 mm with a firm end point, and the posterior drawer test is negative. Standing radiographs show widening of the lateral joint space and a 5-degree mechanical varus alignment. What is the most effective course of treatment?
Explanation
REFERENCES: Naudie DD, Amendola A, Fowler PJ: Opening wedge high tibial osteotomy for symptomatic hyperextension-varus thrust. Am J Sports Med 2004;32:60-70.
Covey DC: Injuries of the posterolateral corner of the knee. J Bone Joint Surg Am
2001;83:106-118.
Question 81
Figures 35a through 35c show the clinical photograph and radiographs of a 15-year-old boy who stubbed his toe 1 day ago while walking barefoot in the yard. Management should consist of
Explanation
REFERENCES: Kensinger DR, Guille JT, Horn BD, et al: The stubbed great toe: Importance of early recognition and treatment of open fractures of the distal phalanx. J Pediatr Orthop 2001;21:31-34.
Pinckney LE, Currarino G, Kennedy LA: The stubbed great toe: A cause of occult compound fracture and infection. Radiology 1981;138:375-377.
Seymour N: Juxta-epiphysial fracture of the terminal phalanx of the finger. J Bone Joint Surg Br 1966;48:347-349.
Question 82
Patient-specific instrumentation (PSI) reliably demonstrates which benefit over conventional intramedullary guidance systems?
Explanation
Cost is usually increased with PSI because the theoretical decreased number of surgical trays and shortened surgical time do not offset cost of presurgical imaging and extra cost associated with the necessary jigs. Studies do not demonstrate a reliable improvement in functional outcomes or coronal alignment when PSI is compared to standard instrumentation. Evidence reveals that PSI necessitates fewer trays than standard instrumentation.
Question 83
A 55-year-old woman with type I diabetes mellitus has a chronic ulcer over the dorsum of her right foot and reports forefoot pain. Examination reveals 1- x 2-cm nondraining ulcer over the dorsum of the foot. The patient has 1-2+ pain with compression of the foot and ankle. She has a weakly palpable posterior tibial pulse and an absent dorsalis pedis pulse. There is no erythema, cellulitis, or drainage. Radiographs are normal. Which of the following diagnostic studies should be obtained?
Explanation
REFERENCES: Wagner FW Jr: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981;2:64-122.
Apelqvist J, Castenfors J, Larson J, Stenstrom A, Agardh CD: Prognostic value of systolic ankle and toe blood pressure levels in outcome of diabetic foot ulcer. Diabetes Care 1989;12:373-378.
Question 84
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
REFERENCES: Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
D’Antonio J, Capello W, Manley M, et al: New experience with alumina-on-alumina ceramic bearings for total hip arthroplasty. J Arthroplasty 2002;17:390-397.
Question 85
Based on the findings shown in Figures 22a and 22b, corrective surgery to obtain maximal safe correction and optimal instrumentation fixation should be performed at which of the following locations?
Explanation
REFERENCES: Shufflebarger HL, Clark CE: Thoracolumbar osteotomy for postsurgical sagittal imbalance. Spine 1992;17:S287-S290.
Murrey DB, Brigham CD, Kiebzak GM, et al: Transpedicular decompression and pedicle subtraction osteotomy (eggshell procedure): A retrospective review of 59 patients. Spine 2002;27:2338-2345.
Question 86
A 78-year-old man with ankylosing spondylitis sustains a minor fall. Shortly afterward he experiences sudden worsening of his chronic back pain and is brought to the emergency department by his caregiver. Radiographs and a CT scan of the spine do not show a clear fracture. What is the most appropriate next step?
Explanation
Patients with ankylosing spondylitis are at high risk for occult fractures after low-energy injuries. Although radiographs and a CT scan do not demonstrate a spinal fracture in this patient, high risk for an unstable occult fracture necessitates further imaging with MRI to ensure that no fractures are missed. Although a CT scan is typically the primary imaging modality for workup of spine injuries in similar patients, CT and MRI complement each other and each detects fractures that are missed using the other modality. A CT myelogram might detect cord or root compression but would not aid in the diagnosis of an occult fracture. Nonsteroidal anti-inflammatory drugs are first-line treatment for idiopathic low-back pain. In a patient with ankylosing spondylitis at high risk for fracture, further workup is needed to rule out an occult fracture. Flexion and extension radiographs of the spine are inferior to MRI for evaluating occult fractures and ligamentous injuries. The primary concern for this patient remains an unstable spinal fracture, which necessitates an MRI of the spine before initiating a workup for other possible causes of his back pain.
RECOMMENDED READINGS
Duane TM, Cross J, Scarcella N, Wolfe LG, Mayglothling J, Aboutanos MB, Whelan JF, Malhotra AK, Ivatury RR. Flexion-extension cervical spine plain films compared with MRI in the diagnosis of ligamentous injury. Am Surg. 2010 Jun;76(6):595-8. PubMed PMID: 20583514. View Abstract at PubMed
Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002 Sep;97(2 Suppl):218-22. PubMed PMID: 12296682. View Abstract at PubMed
Koivikko MP, Koskinen SK. MRI of cervical spine injuries complicating ankylosing spondylitis. Skeletal Radiol. 2008 Sep;37(9):813-9. doi: 10.1007/s00256-008-0484-x. Epub 2008 Apr
Question 87
- A high school distance runner reports a 3-week history of heel pain while running. Examination elicits no pain with dorsiflexion or with palpitation of the plantar fascia; however, pain is evident with palpitation over the muscular origin of the abductor hallucis. What is the most likely etiology of the pain?
Explanation
Question 88
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?
Explanation
REFERENCES: Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Callaghan JJ, Salvati EA, Pellicci PM, Wilson PD Jr, Ranawat CS: Results of revision for mechanical failure after cemented total hip replacement, 1979 to 1982: A two- to five-year follow-up. J Bone Joint Surg Am 1985;67:1074-1085.
Question 89
During primary total knee arthroplasty, what is the maximum distance the joint line can be raised or lowered before poor motion, joint instability, and increased chance of revision occur?
Explanation
REFERENCE: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365.
Question 90
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
REFERENCES: Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Norris T (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 433-442.
Question 91
Treatment of an atrophic nonunion of the radial diaphysis should include which of the following?

Explanation
Question 92
What complication is more likely following excessive medial retraction of the anterior covering structures during the anterolateral (Watson-Jones) approach to the hip?
Explanation
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, p 325.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-17, 4-18.
Question 93
Figures 27a through 27c show the AP radiograph, MRI scan, and biopsy specimen of an otherwise healthy man who has a painful wrist. Serum chemistry studies are normal. What is the most likely diagnosis?
Explanation
REFERENCE: Vander Griend RA, Funderburk CH: The treatment of giant-cell tumors of the distal part of the radius. J Bone Joint Surg Am 1993;75:899-908.
Question 94
03 Which of the following findings is one of the diagnostic criteria for diffuse idiopathic skeletal hyperostosis?
Explanation
Diffuse idiopathic skeletal hyperostosis is a common disease, most prevalent in those over 50 years of age. The usual presentation is a middle-aged or older patient with chronic mild pain in the middle to lower back, spinal stiffness, and typical radiographic changes in the thoracic spine. Diffuse idiopathic skeletal hyperostosis is predominantly a radiographic diagnosis with 3 major diagnostic criteria. 1. Flowing ossification along the anterolateral aspect of at least four contiguous vertebrae. 2. Preservation of disk height in the involved vertebral segment; the relative absence of significant degenterative changes, such as marginal sclerosis in vertebral bodies or vacuum phenomenon. 3.
Absence of facet-joint ankylosis; absence of sacroiliac erosion, sclerosis, or intra-articular osseous fusion. Treatment is typically non-operative, with anti-inflammatories, activity modification and PT.
back to this question next question
Question 95
A 13-year-old girl is diagnosed with a stage IIB osteosarcoma of the proximal tibia. Following neoadjuvant chemotherapy, local control should consist of
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue. Philadelphia, PA, Lippincott Raven, 1998, p 274.
Wold LA, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 14-15.
Question 96
A 25-year-old volleyball player reports pain and clicking in his dominant shoulder during overhand serving. Three months of physical therapy fail to provide relief. Radiographs are normal, and an MRI scan is shown in figures 18a and 18b. Atrophy and weakness are most likely to be localized to which of the following muscles?

Explanation
Question 97
A 15-year-old girl sustained the injury shown in Figures 70a and 70b when she jumped from the back of a moving truck. She is seen in the emergency department 2 hours after her injury. She has no other injuries. Her foot is warm and she has a normal motor and sensory examination. Pulses are only evident on Doppler. What is the most appropriate management? Review Topic

Explanation
Question 98
What is the most likely complication after surgical treatment in this scenario?
Explanation
Posterior shoulder instability is a rare form of instability that often presents with pain rather than feelings of instability. It often occurs in young athletes during activities that put the shoulder in an “at-risk position” (flexion, adduction, and internal rotation). Repetitive microtrauma can lead to posterior shoulder instability such as seen in football linemen. Swinging a bat or golf club places the lead arm in a flexed, adducted, and internally rotated position, which can lead to posterior translation of the humeral head that is forcibly reduced in follow-through as seen in this patient.
The glenohumeral joint relies on static and dynamic stabilizers. Static stabilizers help prevent instability at the end ranges of motion when the ligaments are taut. Dynamic stabilizers work to prevent subluxation at midranges of motion at which the ligaments are lax. The rotator cuff is integral as a dynamic stabilizer of the shoulder. It works through a process called concavity compression. The 4 muscles of the rotator cuff compress the humeral head into the concavity of the glenoid-labrum. This prevents the humeral head from subluxing during the midranges of motion. Of the 4 rotator cuff muscles, the subscapularis is most important at preventing posterior subluxation.
This patient has posterior instability, and various surgical techniques may be indicated depending on findings. Arthroscopic labral repair is indicated for anterior instability. Arthroscopic posterior labral repair is indicated for this patient because he has a posterior labral tear and posterior instability. If a patient has ligamentous laxity (not seen in this scenario because sulcus and Brighton sign findings would be negative), a posterior capsular shift with rotator interval closure is indicated. If a patient has excessive glenoid retroversion, a posterior opening-wedge osteotomy is appropriate.
The most common complication seen after arthroscopic posterior labral repair is stiffness, followed by recurrent instability and degenerative joint disease.
Question 99
A 75-year-old woman has had severe shoulder pain for the past month. Her medical history includes hypertension and a total nephrectomy for renal cell carcinoma 7 years ago. Radiographs and sagittal MRI scans are shown in Figures 36a through 36d. A bone scan reveals this to be an isolated lesion. Biopsy findings are consistent with metastatic renal cell carcinoma. What is the most appropriate treatment for this patient?
Explanation
REFERENCES: Fuchs B, Trousdale RT, Rock MG: Solitary bony metastasis from renal cell carcinoma: Significance of surgical treatment. Clin Orthop Relat Res 2005;431:187-192.
Jung ST, Ghert MA, Harrelson JM, et al: Treatment of osseous metastases in patients with renal cell carcinoma. Clin Orthop Relat Res 2003;409:223-231.
Question 100
In the treatment of intra-articular calcaneal fractures, surgical reduction and fixation has been shown to have improved outcomes over nonoperative treatment in all of the following patient groups EXCEPT:

Explanation
