Orthopedic Board Review MCQs: Spine, Shoulder & Nerve Surgery | Part 47

Key Takeaway
This page presents a professional Orthopedic Surgery Board Review MCQ quiz. Designed for orthopedic residents and surgeons, it features 100 verified, high-yield questions covering Foot, Hip, Nerve, Shoulder, and Spine. This interactive quiz rigorously prepares candidates for AAOS and ABOS board certification exams.
About This Board Review Set
This is Part 47 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 47
This module focuses heavily on: Foot, Hip, Nerve, Shoulder, Spine.
Sample Questions from This Set
Sample Question 1: A 21-year-old collegiate scholarship football player has an episode of transient quadriplegia. An MRI scan of the cervical spine reveals cord edema and severe congenital spinal stenosis. The athlete has aspirations of playing on a professio...
Sample Question 2: A 51-year-old woman with no preoperative neurologic deficit is undergoing elective anterior cervical diskectomy and fusion (ACDF) with plating and fusion for a C5-6 disk herniation with right-sided neck pain. Thirty minutes into the surgery...
Sample Question 3: A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root...
Sample Question 4: Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of...
Sample Question 5: A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 21-year-old collegiate scholarship football player has an episode of transient quadriplegia. An MRI scan of the cervical spine reveals cord edema and severe congenital spinal stenosis. The athlete has aspirations of playing on a professional level and demands that he be allowed to play. The team physician should give what recommendation to the college?
Explanation
REFERENCES: Mathias MB: The competing demands of sport and health: An essay on the history of ethics in sports medicine. Clin Sports Med 2004;23:195-214.
Bernstein J, Perlis C, Bartolozzi AR: Ethics in sports medicine. Clin Orthop 2000;378:50-60.
Question 2
A 51-year-old woman with no preoperative neurologic deficit is undergoing elective anterior cervical diskectomy and fusion (ACDF) with plating and fusion for a C5-6 disk herniation with right-sided neck pain. Thirty minutes into the surgery the neurophysiologic monitoring shows a rapid drop and then loss of amplitude in the right cortical somatosensory-evoked potential waveform. All other waveforms remained normal and unchanged, including right-sided cervical (subcortical) and peripheral (Erb’s point), and those from the left-sided upper extremity and both lower extremities. What is the most likely cause of the change?
Explanation
REFERENCES: Drummond JC, Englander RN, Gallo CJ: Cerebral ischemia as an apparent complication of anterior cervical discectomy in a patient with an incomplete circle of Willis. Anesth Analg 2006;102:896-899.
Yeh YC, Sun WZ, Lin CP, et al: Prolonged retraction on the normal common carotid artery induced lethal stroke after cervical spine surgery. Spine 2004;29:E431-E434.
Question 3
A 25-year-old athletic woman has a 16-week history of left lower-extremity radiating pain in an S1 distribution. MR images obtained by her family physician reveal a large L5-S1 paracentral disk herniation impinging on the left S1 nerve root. You suggest a left-sided L5-S1 microdiskectomy and tell her that when comparing tubular diskectomy and open procedures
Explanation
Several comparative studies have reported no difference in functional outcomes between tubular diskectomy and microsurgical lumbar diskectomy. A recent systematic review by Kamper and associates in which conventional microdiskectomy and minimally invasive approaches were compared revealed that there was no difference between the procedures in terms of clinical outcomes, complication risk, or rate of revision surgery.
RECOMMENDED READINGS
Kamper SJ, Ostelo RW, Rubinstein SM, Nellensteijn JM, Peul WC, Arts MP, van Tulder MW. Minimally invasive surgery for lumbar disc herniation: a systematic review and meta-analysis. Eur Spine J. 2014 May;23(5):1021-43. doi: 10.1007/s00586-013-3161-2. Epub 2014 Jan 18.
PubMed PMID: 24442183.View Abstract at PubMed
Dasenbrock HH, Juraschek SP, Schultz LR, Witham TF, Sciubba DM, Wolinsky JP, Gokaslan ZL, Bydon A. The efficacy of minimally invasive discectomy compared with open discectomy: a meta-analysis of prospective randomized controlled trials. J Neurosurg Spine. 2012 May;16(5):452-62. doi: 10.3171/2012.1.SPINE11404. Epub 2012 Mar 9. PubMed PMID:
Question 4
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of
Explanation
REFERENCES: Pizzutillo PD, Hummer CD III: Nonoperative treatment for painful adolescent spondylolysis or spondylolisthesis. J Pediatr Orthop 1989;9:538-540.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 5
A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals
Explanation
REFERENCES: Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Iannotti JP, Zlatkin MB, Esterhai JL, et al: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29.
Question 6
New computer scanning technology for socket design has achieved which of the following improvements in amputee care?
Explanation
Question 7
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?

Explanation
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (<24 hours) or multiorgan failure (>24 hours).
Incorrect Answers: Choices 1-4 are not as predictive of mortality as choice 5.
Question 8
A 26-year-old man sustains a displaced bimalleolar fracture by sliding into second base while playing baseball. Following initial closed reduction and splinting of the fracture, moderate swelling is noted. What is the safest time to perform surgery?
Explanation
REFERENCES: Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119.
Hahn DM, Colton CL, Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Tile M: Fractures of the ankle, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1998, pp 523-561.
Question 9
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 179-191.
Question 10
Benign Ethnic Neutropenia is more common in males.
Explanation
Access to pediatric orthopaedic management has been well investigated. Numerous Level 4 studies have shown that orthopaedic offices in urban and rural areas prefer treating patients with private insurance over patients with Medicaid.
Iobst et al. telephoned 100 urban and rural orthopaedic outpatient offices to schedule an appointment for a 10-year-old patient with a forearm fracture. They showed that 8/100 offices would schedule an appointment within 1 week to the child with Medicaid insurance, as compared to 36/100 that gave an appointment to a child with private insurance.
Pierce et al. contacted 42 orthopaedic practices to schedule an appointment for a 14- year-old patient with an ACL injury. They showed that 38/42 offices scheduled an appointment for the child within 2 weeks with private insurance. This compared to 6/42 that scheduled an appointment for a similar child with Medicaid.
Incorrect Answers:
The perioperative use of which medication has been shown to increase the risk of post-operative infection following orthopaedic procedures in patients with rheumatoid arthritis (RA)?
Naproxen
Leflunomide
Sulfasalazine
Etanercept
Aspirin
Of the medications listed, only etanercept has been shown to increase the risk of post- operative infection following orthopaedic procedures in patients with RA.
Etanercept is a TNF-alpha antagonist with a short half-life that is administered once or twice weekly in patients with RA. Since TNF-alpha plays a central role in the pathogenesis of RA and is instrumental in causing joint destruction, the inhibition of this molecule has shown excellent results in controlling disease. The most powered study on TNF-alpha inhibitor use in the perioperative period following an orthopaedic procedures demonstrated a significant increase in
post-operative infection.
Howe et al. review the medical management of patients with RA who underwent orthopaedic procedures. They state that while there is conflicting information regarding TNF-alpha antagonists, they recommend holding them prior to major orthopaedic interventions.
Giles et al. review 91 patients with rheumatoid arthritis who underwent an orthopaedic procedure. They found TNF-alpha inhibitor therapy to be significantly associated with the development of a serious postoperative infection (p=.041)
Perhala et al. review 61 patients with RA who were treated with methotrexate during the perioperative period surrounding a total joint arthroplasty. They
failed to find a significant increase in complications in this patient group, stating the perioperative use of methotrexate does not affect wound healing or increase the likelihood of periprosthetic infection.
Illustration A shows the site of action of TNA-alpha inhibitors in the RA pathway.
Incorrect Answers:
Communication breakdown is the leading cause of which of the following?
Delayed diagnoses
Medication errors
Surgical site infections
1 and 2
All of the above
Communication failures are the leading cause of wrong side surgeries, medication errors and diagnostic delays.
Poor communication sets up environments in which medical errors can take place. Per the Joint Commission, medical errors may be the among the top 10 causes of death in the United States. Establishing open lines of communication is critical to reduce the risk of error and enhance patient safety.
Gandhi et al. designed a framework to study missed or delayed diagnoses and their causes. The most significant factors contributing to errors were poor handoffs, failures in judgment, failures in memory and failures in knowledge.
O’Daniel et al. review the importance of professional communication and collaborative team efforts. They note that patient safety is at risk when poor communication is in place. The leading cause for medication errors, treatment delays and wrong-site surgeries is communication failure.
Illustration A shows the leading causes of death in the United States. This includes “preventable errors” as a cause.
Incorrect Answers:
treatment, medication errors and wrong side surgery
Which of the following is true regarding osteoprotegerin (OPG)?
It is secreted by osteoclasts
It increases bone resorption
Binds to prostoglandin E2 before stimulating osteoclasts
Osteoprotegerin knock-out mice develop osteopetrosis
Binds to and sequesters RANKL
Osteoprotegerin is a decoy receptor for RANKL. Binding to RANKL causes decreased production of osteoclasts by inhibiting the differentiation of osteoclast precursors.
Bone resporption/remodeling is a complex process regulated by a large variety of molecules. Molecules that have shown to inhibit osteoclasts include OPG, calcitonin, estrogen, TGF-B, and IL-10. Corticosteroids have been shown to decrease production of OPG, thereby enhancing osteoclast formation and longevity. Prolia, or denosumab, is a newly approved drug used to treat osteoporosis and has a mechanism of action similar to osteoprotegerin
(inhibits binding of RANKL to RANK).
Boyle et al. review osteoclast differentiation and activation. The authors state that targeted disruption of OPG causes increased osteoclastogenesis and/or activation resulting in osteopenia.
Illustration A shows how OPG binds to RANKL inhibiting the stimulation of osteoclasts.
Incorrect Answers:
A 55-year-old woman has T-score -2.0 at the femoral neck. According to the World Health Organization Fracture Risk Assessment Tool (FRAX), she has a ten- year probability of sustaining a hip fracture of 1.5% and a ten-year probability of sustaining a major osteoporotic fracture of 8.9%. Which of the following statements is true regarding her antiresorptive therapy management?
Antiresorptive therapy should be started based on her T-score
Antiresorptive therapy should be started based on her risk of hip fracture alone
Antiresorptive therapy should be started based on her risk of major osteoporotic fracture alone
Antiresorptive therapy should not be started
Antiresorptive therapy should be started based on her risks of both hip fracture and major osteoporotic fracture
This patient has osteopenia. Assessment by FRAX shows that ten-year risk of hip fracture is less than 3% and her ten-year risk of major osteoporosis- related fracture is less than 20%. Therefore, antiresorptive therapy is not indicated at this time.
According to the 2008 National Osteoporosis Foundation guidelines, pharmacologic treatment for osteoporosis should be considered if patients are
postmenopausal women or men greater than 50 years old AND meet one of the following criteria: (1) they have a prior hip or vertebral fracture, (2) they have a T score -2.5 or less at the femoral neck or spine, (3) they have a T score between -1.0 and -2.5 at the femoral neck or spine AND a 10-year risk of hip fracture greater than 3% or 10-year risk of major osteoporosis-related fracture greater than 20%.
FRAX (World Health Organization Fracture Risk Assessment Tool) calculates
year risk of fracture based on the following variables: age, sex, race, height, weight, BMI, history of fragility fracture, parental history of hip fracture, use of oral glucocorticoids, secondary osteoporosis and alcohol use to calculate 10-year risk of fracture.
Unnanuntana et al. reviewed the assessment of fracture risk. Besides FRAX score and T-score, they discussed biochemical markers of bone formation and resorption, which are useful for monitoring the efficacy of antiresorptive / anabolic therapy, and may help identify patients at high risk for fracture.
Ekman et al. reviewed the role of the orthopaedic surgeon in minimizing mortality and morbidity associated with fragility fractures. The surgeon should consider prescribing appropriate medications, physical therapy, assessing fall risk and preventing falls and changing lifestyle factors (exercise, smoking and alcohol).
Illustration A shows the FRAX online tool (http://www.shef.ac.uk/FRAX/tool.aspx?country= =9).Illustration B shows the clinical risk factors considered in FRAX calculation.
Incorrect Answers:
A 32-year-old runner sustains a trimalleolar left ankle fracture. She undergoes open reduction and internal fixation and is kept non- weightbearing after surgery. At 2 months, what changes will occur in the articular cartilage of both her knees as a result of her current weightbearing regimen?
Cartilage thickening in the left (ipsilateral) knee and no change in cartilage thickness in the right (contralateral) knee
Cartilage thinning in both knees
Cartilage thinning in the left (ipsilateral) knee and no change in cartilage thickness in the right (contralateral) knee
Cartilage thinning in the left (ipsilateral) knee and increased cartilage thickness in the right (contralateral) knee
Increased cartilage thickness in both knees
After a period of off-loading, the off-loaded limb will experience cartilage thinning. The contralateral limb will not demonstrate any cartilage changes.
Physiologic loading of cartilage increases proteoglycan synthesis and cell proliferation and is chondroprotective. Joint immobilization leads to cartilage thinning, tissue softening, and reduced proteoglycan content, leading to cartilage erosion. Joint overuse leads to cartilage damage (in vitro only).
Hinterwimmer et al. examined cartilage atrophy after partial load bearing
using quantitative MRI. They found cartilage thinning in all knee compartments (greatest thinning, medial tibia; least thinning, patella). There was no change in cartilage morphology in the contralateral knee.
Sun reviewed the relationship between mechanical loading and cartilage degeneration. In OA, cartilage breakdown occurs at the articular surface, and is then fueled by synovial proteases and cytokines. In RA, synovial cells and macrophages are the source of degradative enzymes and incite cartilage destruction.
Milward-Sadler et al. examined mRNA levels following mechanical stimulation in normal and osteoarthritic chondrocytes. Normal chondrocytes showed increased aggrecan mRNA and decreased matrix metalloproteinase 3 (MMP-3) mRNA after stimulation. This
chondroprotective response was absent in osteoarthritic chondrocytes.
Illustration A shows pro- and anti-inflammatory mechanisms of mechanical loading on chondrocytes. Underloading and overloading induce cartilage damage through pathways involving the upregulation of MMPs and ADAMTSs (ADAMTS, a disintegrin and metalloproteinase with thrombospondin motifs, or aggrecanase). Physiological loading blocks these increases.
Incorrect Answers:
A morbidly obese 40-year-old man is scheduled to undergo hemilaminectomy for resection of an painful osteoid osteoma of the T6 lamina. He is positioned prone on a Jackson table and localization is performed with intraoperative fluoroscopy prior to the start of the case. At close to the end of the case, intraoperative frozen section reveals only normal bone fragment from the resected lamina. A probe is placed and a cross-table lateral radiograph reveals that the T7 lamina was resected instead of T6. At this point, the surgeon should
do all of the following EXCEPT
Complete the surgery
Abort the case and obtain further imaging
Apologize to the patient and family
Formally document the error in the operative report
Inform the patient and family immediately after the operation
Fluoroscopic localization of the correct thoracic vertebra can be difficult in the obese
patient. Upon detection of wrong level surgery, he should not abort the case. Rather, he should perform the desired procedure at the correct site, and advise the patient and family upon completion.
Adverse events are inevitable. The correct action following wrong-site surgery is to perform the desired procedure at the correct site followed by frank and honest communication with the patient/family. Open, honest communication favorably affects patient behavior, health outcomes, patient satisfaction, and often reduces the incidence of medical professional liability actions. The
discussion should include a disclosure of known facts and an explanation as to the likely cause, as well as ongoing treatment, follow up care, and prognosis.
The AAOS Information Statement about Wrong Site Surgery identifies 3 treatment steps following discovery of an error during surgery under general anesthesia: Return the patient to his preoperative condition, perform the correct procedure at the correct site, and advise the patient and family of what occurred and the likely consequences, if any, of the wrong- site surgery.
The AAOS Information Statement on Communicating Adverse Events states that the surgeon has an ethical and professional obligation to disclose the error to the patient and/or family. Disclosure should include what happened, why it happened, health implications, and what measures are being instituted to prevent recurrences.
Incorrect Answers:
All of the following are Standards of Professionalism relating to interactions with industry for practicing orthopaedic surgeons EXCEPT:
Decline gifts from industry with a market value over $100 (unless they are medical textbooks or patient educational materials)
Disclose to the patient any financial arrangements with industry that relates to the patient's treatment
Accept no direct financial inducements from industry for utilizing a particular implant
Disclose any relationship with industry to colleagues who may be influenced by your work
Decline to participate in industry sponsored non-CME courses or
conferences
The AAOS has adopted the Standards of Professionalism (SOP). These SOP’s establish mandatory, minimum levels of acceptable conduct for fellows and members of the AAOS to engage in relationships with industry. There are 17 standards with relation to industry. Answer choice 5 is not a SOP as surgeons are allowed to participate in or consult in meetings that are conducive to the effective exchange of information. The SOP also stipulate that tuition, travel, and modest hospitality (including meals and receptions) are allowed to attend an industry-sponsored non-CME course.
A prospective randomized trial is conducted to test the efficacy of Vitamin C versus placebo in treating patients who develop chronic regional pain syndrome (CRPS) after distal radius fractures. At first follow-up, the rates of CRPS are 1% and 9% in the study and placebo group, respectively. Which statistical test is most appropriate to determine significance?
Single factor analysis of variance
Chi-square test
Student t-test
Mann-Whitney rank sum test
Wilcoxon rank sum test
In the study provided, we need to determine whether distributions of categorical variables differ from one another. The appropriate study is the chi- square test.
Data can be classified as numerical (continuous) or categorical (proportional). Responses to such questions as "What is your major?" or Do you own a car?" are categorical because they yield data such as "biology" or "no." In contrast, responses to such questions as "How tall are you?" or "What is your G.P.A.?" are numerical. When comparing two independent means from numeric data, a t-test is performed. However, if categorical data is being compared, the chi- square test will determine if the proportions are really different.
Kocher et al. review basic clinical epidemiology and biostatistics relevant to orthopaedic surgery. Amongst other things, they describe that data can be summarized in terms of measures of central tendency, such as mean, median, and mode, and in terms of measures of dispersion, such as range, standard deviation, and percentiles.
Illustration A shows an algorithm for determining which test to use for varying data. Incorrect Answers:
distributed.
A 35-year-old patient is involved in a motor vehicle accident and sustains multiple fractures including a closed comminuted proximal meta-diaphyseal tibia fracture. The surgeon is considering bridge plating the fracture using a minimally invasive approach. Which of the following is true regarding bridge plating?
A locked plate construct (locked screws) or hybrid construct (locked and non- locked screws) is necessary.
Periosteal stripping is performed through two incisions proximal and distal to the fracture.
Bridge plating is performed following direct reduction of the fracture.
AO Type A diaphyseal fractures are best treated with this technique.
Bridge plating with a long working length creates a flexible, axially stable construct.
In bridged plating, only the most proximal and distal screw holes are filled. This creates a flexible, axially stable construct.
Bridge plating is applicable to all long-bone fractures with complex fragmentation and where intramedullary nailing or conventional plate fixation is not suitable. The construct preserves the blood supply to the fracture fragments as the fracture site is undisturbed during the operative procedure. It provides RELATIVE stability, allowing for some motion at the fracture site, leading to callus formation and secondary bone healing. The construct is FLEXIBLE because of increased distance between the 2 screws closest to the fracture (long working length), allowing for stress distribution and permitting more motion at the fracture site. The construct is also AXIALLY STABLE because the plate acts as an extramedullary splint and resists axial compression.
Livani et al. advocate using an anterior or antero-lateral approach for minimally invasive plating of the humerus. They recommend that distal access is obtained first, allowing identification of the lateral antebrachial cutaneous nerve. For distal fractures, they recommend extending the plate down to the lateral column.
Apivatthakakul et al. defined minimally-invasive plate osteosynthesis (MIPO) danger zones from the lateral epicondyle. They found the musculocutaneous nerve averaged 18- 43% of the humeral length, the danger zone for the radial nerve averaged 36-59% of the humeral length, and the most dangerous screws that penetrated or touched the radial nerve lay 47-53% of the humeral length.
Illustration A shows a distal tibia fracture. Illustration B shows radiographs 5 months after bridge plating of this fracture. There is callus formation, characteristic of indirect bone healing.
periosteal blood supply is critical.
Which of the following components of bone is most responsible for compressive strength?
Type I collagen
Osteocalcin
Proteoglycans
Osteonectin
Osteopontin
Proteoglycans, in addition to calcium hydroxyapatite [Ca10(PO4)6(OH)2], are most responsible for providing compressive strength.
Bone is composed of both organic and inorganic components. Inorganic components include calcium hydroxyapatite and osteocalcium phosphate. Organic components include collagen, proteoglycans, matrix proteins, cytokines and growth factors. While Type I collagen is responsible for providing the tensile strength of bone, proteoglycans and calcium hydroxyapatite [Ca10(PO4)6(OH)2] are most responsible for providing compressive strength. Proteoglycans contain a core protein with various
numbers of covalently attached side chains of glycosaminoglycans. In addition to providing compressive strength, they are also responsible for binding growth factors and inhibiting mineralization.
Knothe et al. review the osteocyte. They discuss that osteocytes are the most abundant
cells in bone, are actively involved in maintaining the bony matrix, and may act as mechanosensors.
Illustration A shows a proteoglycan aggregate, which can form when individual molecules link onto a chain of hyaluronic acid.
Incorrect Answers:
A prospective, randomized controlled trial of 150 patients undergoing total hip arthroplasty is performed to test whether repair of the capsule during a posterior approach reduces post-operative dislocations in the first three months. The study found no difference in dislocation rate if the capsule was repaired versus not repaired (p =
.34). Subsequently, a multicenter follow-up study of 2000 patients showed that repairing the capsule led to a decreased dislocation rate
in the first three months (p = .03). Assuming the second study reflects reality, which of the following errors occurred in the first study?
Observer bias
Type-II error
Alpha error
Type-I error
Confounding error
In this situation, the null hypothesis was accepted when it should have been rejected.
This is a type-II error.
A study can have two types of errors. Type-I errors, or alpha errors, occur when the null hypothesis is rejected when it should have been accepted. The alpha level refers to the probability of a type-I error. By convention, the alpha level of significance is set at 0.05, which means that we accept the finding of a significant association if there is less than a one in twenty chance that the observed association was due to chance alone. Type-II errors, or beta errors, occur when the null hypothesis is accepted when it should be rejected. This
often occurs when studies are underpowered. In the example above, the null hypothesis is that repair of the capsule does not reduce dislocations within the first three months. Since the first study did not show a statistically significant difference, the null hypothesis was accepted. Since a more powered study showed that repair of the capsule does reduce dislocations, the null hypothesis should have been rejected in the initial study (if it was adequately powered).
Fosgate et al. review the importance of sample size calculations when performing research. They state that sample size ensures statistical significance if the subsequent data collection is perfectly consistent with the assumptions made for the sample size calculation (assuming power was set as
50% or greater).
Illustration A shows the difference between type-I and type-II errors. Video V is a lecture discussing statistical definition review of PPV, NPV, sensitivity and specificity.
Incorrect Answers:
that properly constructed studies attempt to avoid.
Which of the following is a potential cause of fretting corrosion?
The micromotion at the femoral head-neck junction in a modular total hip replacement
A stainless-steel cerclage wire is in contact with a titanium-alloy femoral stem
Friction between polyethylene liner and femoral head leading to osteolysis
The formation of pits within a stainless-steel plate and the subsequent release of metal ions
The formation of an adherent oxide coating on titanium implants
Micromotion at the femoral head-neck junction can lead to fretting corrosion, one of the most common causes of failure of a modular implant.
Modular components give surgeons excellent intraoperative flexibility, but are susceptible to various types of corrosion. While titanium and cobalt-chrome contain a protective surface oxide layer, continued micromotion at the modular junction may disrupt the protective layer leading to fretting corrosion, defined as micromotion at contact sites under load. This may eventually lead to a painful synovitis that necessitates a revision procedure.
Srinivasan et al. review modularity in total hip arthroplasty. Amongst other things, they discuss the modularity of the femoral head/neck junction, describing the morse taper interlocking system that provides both axial and rotational stability.
Illustration A shows an example of corrosion at the head/neck junction of a total hip arthroplasty.
Incorrect Answers:
Which of the following situations is most likely to decrease sentinel event errors?
Physician and nurse training is lengthened by 20%
Resident hours are decreased to 55 hours per week
An environment is created where all members of the healthcare team feel empowered to express their concerns and beliefs
Holding individuals responsible for errors in clinical judgement
Physicians and nurses are assigned to a smaller number of patients
Creating an environment where all members of the healthcare team feel empowered to express their beliefs increases communication, the key element in decreasing sentinel events.
Research has shown that 70% of sentinel event errors are caused by improper communication. Specific ways to improve communication include effective clinical handover between shifts and breaking down the "hierarchy" so that all members of the team can discuss their expectations and concerns. Barriers to effective communication include distractions, cultural differences, power distance relationships, time pressures, and lack of organization.
Leonard et al. describe specific clinical experiences in the application of surgical briefings, properties of high reliability perinatal care, the value of critical event training and simulation, and benefits of a standardised communication process in the care of patients transferred from hospitals to skilled nursing facilities. They recommend embedding standardized tools and behaviors to bridge differences in communications styles between clinicians.
Incorrect Answers:
Which of the following side effects is most strongly associated with the use of NSAIDs?
Hepatic dysfunction
Renal impairment
Prolonged QTc
Seizures
Hematuria
All NSAIDs have the potential to cause serious renal impairment.
NSAIDs work by inhibiting the cyclooxygenase pathway (COX), which is comprised of the COX-1 and COX-2 pathways. The COX-1 pathway is involved in prostaglandin E2– mediated gastric mucosal protection and thromboxane effects on coagulation, while the COX-2 pathway is mainly involved with the modulation of pain and fever without effect on platelet function. While selective COX-2 inhibitors have a decreased side effect profile, all NSAIDS
have the potential to cause renal impairment and their use should be limited in patients with underlying renal disease.
Horlocker et al. review multimodal pain management in the perioperative setting of a total joint arthroplasty. Specifically, they note that NSAIDs should be used cautiously in patients with underlying renal dysfunction who are to undergo a procedure with major blood loss.
Griffin et al. reviewed 1,799 patients hospitalized for acute renal failure. They found that NSAIDs increased the risk of renal failure by 58% and that NSAID use resulted in 25 excess hospital admissions per 10,000 years of use.
Illustration A shows the COX pathways and their inhibition by NSAIDs. Incorrect Answers:
It is recommended that invasive dental work be completed prior to the initiation of which of the following medications?
Glucosamine
Cholecalciferol
Levothyroxine
Teriparatide
Bisphosphonates
Bisphosphonate therapy combined with invasive dental work increases the risk for development osteonecrosis of the jaw.
Bisphosphonates are a class of drugs that prevent bone mass loss by inhibiting osteoclast resorption. They are used in the treatment of vertebral compression fractures, non- vertebral fragility fractures, osteogenesis imperfecta, multiple myeloma, and avascular necrosis. Because bisphosphonates have been associated with osteonecrosis of the jaw, it is suggested that all invasive
dental work be completed prior to initiation of treatment.
Pazianas et al. (2011) review the safety profile of bisphosphonates. Specifically, they cite gastrointestinal discomfort, atypical femur fractures, osteonecrosis of the jaw, ocular inflammation, and musculoskeletal pain as common side effects. They state there is limited evidence surrounding
bisphosphonate's association with esophageal cancer and atrial fibrillation.
Pazianas et al. (2007) reviewed 11 publications that reported 26 cases of osteonecrosis of the jaw following initiation of bisphosphonate treatment. Age
>60 years, female sex, and previous invasive dental treatment were the most common characteristics of those who developed ONJ.
Illustration A shows the various bisphosphonates and their mechanisms of action. Illustration B shows an example of osteonecrosis of the jaw, a side effect that has been linked to bisphonphonate treatment.
Incorrect Answers:
Figures A and B show radiographs of a 24-year-old female with a soccer injury. A physical examination reveals an isolated, closed injury with no clinical features of neurovascular injury or compartment syndrome. She has been consented to be treated with intramedullary nail fixation. A pre-operative note by the anaesthesiology team makes reference to the patients fair skin and natural red-hair color. How will this information affect the post-operative management of this patient?
Longer duration of anticoagulation due to increased risk of DVT
Avoiding anticoagulation medications due to increased risk of bleeding
Require higher dosages of post-operative analgesia
Longer period of non-weight bearing on surgical limb
Avoiding opioids due to higher risk of unrecognized allergies
Female patients with natural red-hair may require higher dosages of post- operative analgesia compared to other hair types.
Melanocortin-1-receptor (MC1R) is one of the key proteins involved in hair color and skin tone. Mutations of the MC1R alleles can render this protein non- functional, which results in a phenotype of red-hair and fair skin. Mutations of the MC1R have shown to modulate the pain response and opioid efficacy in these patients. Women are more commonly affected and often require more anaesthetic and higher dosages of opioid to achieve comparable MAC level and pain-relief, respectively, as women with other hair types.
Liem et al. showed that a greater concentration of induction and maintenance agents (sevoflurane and desflurane, respectively) were required to sustain comparable MAC levels in red-haired patients as dark haired patients.
Fillingim et al. reviewed the affect of gender, sex and pain. They concluded there is a biopsychosocial element of pain that is perceived differently by men and women. In terms of postoperative and procedural pain, the outcome might be more severe in women than men.
Delaney et al. looked at the involvement of the melanocortin-1 receptor in acute pain in mice. They found that while the MC1R is better known as a gene involved in mammalian hair colour, it was shown to be involved in the pain pathway of inflammatory but not neuropathic origin. Mutations of MC1R showed increased tolerance to noxious pain stimulus in mice.
Figures A and B are AP and lateral radiographs of a left tibia. There is a low energy, distal third shaft fracture with no cortical apposition on the AP view.
Incorrect Answers:
Which of the following medications used for thromboprophylaxis following orthoapedic surgery is a direct inhibitor of factor Xa?
Dextran
Rivaroxaban (Xarelto)
Coumadin
Fondaparinux (Arixtra)
Aspirin
Rivaroxaban (Xarelto), an oral anticoagulant, is a direct inhibitor of factor Xa.
Rivaroxaban (Xarelto) is a member of a new class of oral, direct (antithrombin- independent) factor Xa inhibitors, which restrict thrombin generation both in vitro and in vivo. Inhibition of Factor Xa interrupts the intrinsic and extrinsic pathway of the blood coagulation cascade, inhibiting both thrombin formation and development of thrombi.
Eriksson et al. compare rivaroxaban to enoxaparin for the prevention of symptomatic venous embolism following total hip arthroplasty. Major venous thromboembolism occurred in 4 of 1686 patients (0.2%) in the rivaroxaban group and in 33 of 1678 patients (2.0%) in the enoxaparin group. Additionally, major bleeding events were similar between the two groups.
Illustration A shows the mechanisms of action of various agents used for thromboprophylaxis.
Incorrect Answers:
as Protein C and Protein S.
The origin of bovine derived grafts is particularly important to which of the following religious groups?
Christianity
Islam
Hinduism
Buddhism
Judaism
The origin of bovine-derived surgical implants should be discussed in further detail with patients ascribing to Hinduism.
Patients come from a variety of religious backgrounds. Depending on a patient’s religion, the origin of surgical implants may have implications for their use. In Hinduism, bovine animals are considered sacred. Use of cow by- products is considered purifying in nature. Subsequently, the origin of bovine derived implants should be discussed with patients ascribing to Hinduism.
Easterbrook et al. evaluated the utility of porcine and bovine surgical implants amongst those of Jewish, Muslim and Hindu faiths. Hindu religious leaders, who were surveyed, did not approve of the use of bovine surgical implants.
Enoch et al. evaluated the acceptability of biological products amongst various religious groups. The Hindu religious leaders were found to not have an objection to the use of biological implants derived from cows.
Illustration A shows a clinical photo of a fetal bovine derived dermal substitute. Incorrect Answers:
Immunological testing of anti-cyclic citrullinated peptide antibodies (anti- CCP) is most commonly used for the diagnosis and prognosis of which immunological condition?
Ankylosis spondylitis
Rheumatoid arthritis
Psoriatic arthritis
Systemic lupus erythematosus
Reiter's syndrome
Anti-cyclic citrullinated peptide antibodies (anti-CCP) are commonly used as a marker for the diagnosis and prognosis of rheumatoid arthritis (RA).
Immunological studies are commonly performed to investigate cases of suspected rheumatoid arthritis. Rheumatoid factor has historically been used as a primary marker for RA. However, in more recent years, the use of anti- CCP antibodies has shown to be as sensitive as, and more specific than, rheumatoid factor (RF) in early and fully established disease. In general, anti-
CCP assays equate to a sensitivity of 50-75% and a specificity of 90-95%. High levels of anti-CCP have been shown to be indicative of a more erosive disease process and may be detected before the onset of arthritis.
Gardner and Kadel reviewed the laboratory studies most commonly used in rhuematologic diseases. Standard ordering for clinically suspected RA include Rf, anti- CCP, ESR/CRP as well as other markers of autoimmune diseases such as antinuclear antibodies, anticardiolipin antibodies and lupus anticoagulant, HLA-B27, and uric acid levels.
Illustration A shows the sensitivity and specificity of anti-CCP vs. RF in a variety of autoimmune diseases.
Incorrect Answers:
Vitamin C has been shown to decrease the likelihood of which of the following complications following surgery on the foot and ankle in non-diabetic patients?
Nonunion
Complex Regional Pain Syndrome, type II
Malunion
Complex Regional Pain Syndrome, type I
Wound infection
Vitamin C has been shown to decrease the likelihood of developing complex regional pain syndrome (CRPS), type 1, when given post-operatively to patients undergoing foot and ankle and wrist surgery.
CRPS is a frequent post-operative complication, with rates varying from 10-
37%. Type I CRPS does not have an identifiable nerve lesion, while type II has an identifiable nerve lesion. Multiple studies have shown that vitamin C decreases rates of CRPS following distal radius fractures, and more recently, the same has been shown following foot and ankle surgery. While the exact mechanism of CRPS is unknown, vitamin C has been shown to reduce lipid peroxidation, scavenge hydroxyl radicals, protect the capillary endothelium, and inhibit vascular permeability. All of these characteristics of vitamin C may play a role in modulating the pain pathway.
Zollinger et al. perform a double-blind, prospective, multicenter trial where
416 patients with 427 wrist fractures were randomly allocated to treatment with placebo or treatment with 200, 500, or 1500 mg of vitamin C daily for fifty days. The prevalence of complex regional pain syndrome was 2.4% in the vitamin C group and 10.1% in the placebo group.
Besse et al. compare two groups of patients undergoing surgery on the foot and ankle to determine the effect of vitamin C on the development of CRPS, type I. CRPS type I occurred in 18 cases (9.6%) in the group not given vitamin C, and 4 cases (1.7%) in the group given vitamin C.
Illustration A shows an example of a limb affected by CRPS. Note the increased swelling, a common physical exam finding in patients afflicted with the disease.
Incorrect Answers:
A 25-year-old Spanish speaking male presents to the emergency department 6 hours after sustaining the injury seen in Figure A. He is grossly intoxicated and screaming in pain. Physical examination reveals a closed injury with overlying muscular compartments that are extremely firm to palpation. After sedating the patient, measurements of the intracompartmental pressures were all found to be
>75mmHg. His wife is Spanish speaking and expected to arrive to the hospital in 2-3 hours with a relative to help with translation. No medical translator is
available. You attempt to outline the risk and benefits of surgery to the patient, but the he repeatedly interrupts you and yells out ,"No surgery!". An English-Spanish speaking friend is with the patient and says that he has known the patient for over 2 years and will help with any decision making. What would be the next most appropriate step in the management of this patient?
Delay surgery to monitor the patient for impending compartment syndrome
Proceed with surgery with urgent fasciotomy after documenting the necessity of treatment without consent
Delay the surgery until the wife arrives and able to give informed consent with the aid of a translator
Proceed with surgery for urgent fasciotomy after obtaining informed consent from the patients friend
Respect the patients autonomy and reassess the patient in the morning when he demonstrates capacity to accurately comprehend the proposed treatment
This patient is presenting with compartment syndrome of the right tibia. In a situation of required surgery for limb threatening injury without available legal consent the surgeon should confirm and document the necessity of care with a fellow colleague.
Physicians are responsible for whether a patient is able to reasonably understand their medical condition and the nature of any proposed medical procedure, including the risks, benefits, and available alternatives. If the patient lacks this capacity, disclosure imposed by the doctrine of informed
consent are excused because irreparable harm that may result from the physician’s hesitation to provide treatment. Detailed documentation is also important. In addition, the attending physician should contact the Risk Management Dept at the hospital for support prior to surgical intervention or have a medical translator involved to ensure information is being translated properly.
Katz et al. reviewed the medical decision making process of Hispanic people. They showed that Hispanic people are more likely to permit their physician to take the predominant role in making health decisions compared to Non- Hispanic people.
Figure A shows a comminuted tibia and fibula fracture. Incorrect Answers
A Spanish speaking child sustained the injury seen in Figure A after a fall at school. He was casted in the emergency department without the assistance of an interpreter and advised to return to see an orthopaedic surgeon in 1 week. However, the family returns to the emergency department with the child 3 months later, still in the cast. What is the most likely reason the child did not attend the recommended orthopaedic follow-up visit.?
The child is a victim of neglect
The child had no symptoms of pain
He was allowed to return to school wearing the cast
Concerns of cost
Follow-up instructions were not effectively communicated
The most likely reason the child did not attend the recommended orthopaedic follow-up visit was a language barrier preventing effective communication of the intended follow-up instructions.
Communication skills and cultural competence is a key element in good orthopaedic care. Poor communication can often lead to devastating outcomes. In this example, poor communication resulted in this patient being lost to
follow-up. Language barriers must be accommodated and alternative methods of communication must be utilized.
Levinson et al. examined how patients present their medical issues in clinical encounters and how physicians respond to these clues in routine primary care and surgical settings. They showed that good communication relies mostly on the physicians ability to identify patient clues within the clinical encounter.
Poor communication between the physician tended to delay clinical visits, poor follow-up and unsatisfactory outcomes.
Figure A is an AP radiograph of the elbow in a skeletally immature patient. Figure B is a lateral radiograph of the elbow with a posterior fat pad sign, suggestive of an occult fracture.
Incorrect Answers:
A 25-year-old female presents to the emergency room within increasing left shoulder pain after walking into a door 5 months ago. She previously sustained a femoral fracture 2 years ago after tripping on a rug. Relevant skeletal survey radiographs and tissue biopsy results are shown in Figures A through D. Laboratory investigations show normal glomerular filtration rate and creatinine clearance. Dual energy x-ray absorptiometry (DEXA) scan shows T-score of -1.4 and
-1.2 at the hip and lumbar spine, respectively. Which of the following laboratory values in Figure E most likely reflects this patient's condition?
A
B
C
D
E
This patient has primary hyperparathyroidism. Laboratory investigations are likely to show elevated serum intact parathyroid hormone (PTH), alkaline phosphatase (ALP) and ionized serum calcium, and low serum phosphate.
Primary hyperparathyroidism is most commonly caused by a single adenoma (80-90%). Besides the signs and symptoms of hypercalcemia, patients present
with calcification of menisci and articular cartilage, erosions in hand bones, "salt and pepper skull", and brown tumors (osteoclastomas), which appear as lytic regions expanding the cortex and causing pathological fractures, so named because of hemosiderin deposition.
Singhal et al. reviewed primary hyperparathyroidism. They advocate routine serum calcium levels for patients with pathologic fractures. If this is elevated, total and ionized calcium and intact PTH levels should be obtained. They feel that surgery for orthopaedic stabilization and parathyroidectomy should be performed simultaneously for better outcome.
Mankin et al. reviewed metabolic bone disease. They suggest that patients with mild disease with normal calcium levels do not require treatment. For patients with high calcium levels, treatment should include maintenance of fluid balance, localization and removal of the adenoma, bony stabilization, and medications (calcitonin, estrogen, bisphosphonates, and calcimimetics such as cinacalcet).
Figure A is an AP radiograph showing a lytic expansile lesion with pathological fracture in metadiaphyseal region of left humerus with similar lesion in the
fifth posterior rib. Figure B is an AP radiograph showing a lytic expansile lesion in the third metacarpal of the right hand and the fifth metacarpal of the left hand. Figure C is a low power micrograph of a brown tumor demonstrating a central zone of bone resorption, and filling with fibroblastic tissue, with a peripheral rim of osteoid production. Figure D is a high power micrograph of a brown tumor. In areas of bone resorption, there are numerous osteoclast-like giant cells amidst a fibrous stroma. This is unlike a true giant cell tumor, which lacks a fibrogenic stroma.
Incorrect Answers:
and impaired 1,25-dihydroxyvitamin D production by the diseased kidneys. This patient has normal renal function. Answer 3: Elevated PTH, ALP, serum calcium and phosphate occur in tertiary hyperparathyroidism. This again occurs in chronic renal disease after prolonged chronic secondary hyperparathyroidism or after renal transplantation, where the parathyroid glands become autonomous and PTH levels do not normalize. This patient has normal renal function.
elevated.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 11
A 5-year-old girl has had a low-grade fever, right hip and buttock pain, and a right-sided limp for the past 5 days. Examination shows diffuse tenderness and extreme pain on range of motion of the hip. Laboratory studies show a peripheral WBC count of 13,500/mm 3 and an erythrocyte sedimentation rate of 55 mm/h. A radiograph is shown in Figure 46a, and an axial postgadolinium T 1 -weighted MRI scan with fat suppression and an axial T 2 -weighted fast spin echo MRI scan are shown in Figures 46b and 46c. What is the most likely diagnosis?
Explanation
REFERENCES: Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Herring JA: Tachdjian’s Pediatric Orthopaedics ed. 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 150-163.
Question 12
Figure A shows intraoperative images of a right knee in an 8-year-old boy after he sustained an injury. Which of the following is the most common indication for performing this procedure? Review Topic

Explanation
Arthroscopic treatment of lateral discoid meniscus injuries has the advantages of reducing trauma, precise resection or repair of the meniscus and saucerization of the remaining discoid meniscus. Operative treatment is usually limited to patients with pain and mechanical symptoms that are undergoing partial meniscectomy or repair. Asymptomatic discoid meniscus without tears are not considered a surgical indication for routine saucerization.
Kramer et al. reviewed the diagnosis and treatment of traumatic discoid meniscal tears in children. They report that knee shape, size and skeletal maturity must be considered when determining the optimal method of repair. However, all symptomatic torn discoid menisci are best treated with saucerization and repair.
Good et al. looked at the arthroscopic techniques of discoid meniscus repair. Arthroscopic saucerization was successful in 28 of 30 knees and meniscal repair in 23 of 30 knees. At final follow-up, all patients exhibited full knee flexion beyond 135 degrees. In 3 of 30 patients there was residual knee pain, and four reported intermittent mechanical symptoms.
Figure A shows a series of arthroscopic images of the right knee lateral compartment. There is a sequential saucerization of the discoid meniscus.
Incorrect Answers:
(SBQ13PE.83) 8-year-old boy complains of intermittent painless clicking in his knee. His physical examination is normal. His family doctor orders an MRI, which reveals an incomplete lateral discoid meniscus without evidence of tear. What is the most appropriate treatment? Review Topic
Observation only
Diagnostic arthroscopy
Saucerization of meniscus
Saucerization of meniscus and microfracture
Saucerization and stabilization of the mensicus
The clinical presentation is consistent with a asymptomatic discoid meniscus. The most appropriate treatment at this time would be observation only.
MRI scans of the knee are very sensitive for identifying discoid menisci. Diagnosis is usually made when there are 3 or more 5mm sagittal MRI images showing meniscal continuity. Treatment is mostly focused on conservative modalities. Asymptomatic tears are usually treated with observation only. Saucerization is indicated for recurrent locking, swelling, persistent pain, or radiographic evidence of a meniscal tear.
Watanabe et al. described three types of discoid lateral menisci based on arthroscopic appearance. In this classification, discoid menisci with normal peripheral attachments are either type I (complete) or type II (incomplete). Type III discoid menisci, the so-called Wrisberg ligament type, are lacking posterior capsular attachments with the exception of the posterior meniscofemoral ligament.
Kramer et al. looked at the presentation of pediatric knee pain and discoid meniscus. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the meniscus.
Illustration A shows the cross-section of normal meniscus. Illustration B shows the Watanabe classification.
Incorrect Answers:
Question 13
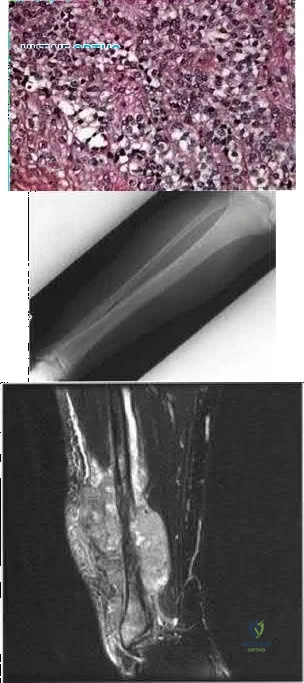
Decreased activity of which of the following proteins may be predictive of an aggressive soft-tissue sarcoma?
Explanation
REFERENCE: Benassi MS, Magagnoli G, Ponticelli F, et al: Tissue and serum loss of metalloproteinase inhibitors in high grade soft tissue sarcomas. Histol Histopathol 2003;18:1035-1040.
Question 14
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time?
Explanation
REFERENCES: Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Carragee EJ: Clinical practice: Persistent low back pain. N Engl J Med 2005;352:1891-1898.
Question 15
Contraindications to cervical laminectomy as a treatment for cervical spondylotic myelopathy include which of the following findings?
Explanation
REFERENCES: Malone DG, Benzyl EC: Laminotomy and laminectomy for spinal stenosis causing radiculopathy or myelopathy, in Clark CR (ed.): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 817-825.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 673-680.
Question 16
Which factor should most influence a patient's decision to have surgery for adult scoliosis if he or she is younger than age 50?
Explanation
In a retrospective review of 137 patients treated surgically and 153 patients treated nonsurgically for adult scoliosis, Bess and associates found that surgical treatment for patients younger than 50 years of age was driven by increased coronal plane deformity, and surgical treatment for older patients was mandated by pain and disability. They also concluded that age, comorbidities, and sagittal balance did not influence treatment decisions.
RECOMMENDED READINGS
Bess S, Boachie-Adjei O, Burton D, Cunningham M, Shaffrey C, Shelokov A, Hostin R, Schwab F, Wood K, Akbarnia B; International Spine Study Group. Pain and disability determine treatment modality for older patients with adult scoliosis, while deformity guides treatment for younger patients. Spine (Phila Pa 1976). 2009 Sep 15;34(20):2186-90. PubMed PMID: 19752704.View Abstract at PubMed
Anderson DG, Albert T, Tannoury C. Adult scoliosis. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:331-338.
Question 17
During particle-induced osteolysis around implants, what cell secretes most of the interleukin-6 (IL-6)?
Explanation
REFERENCE: Bukata SV, Gelinas J, Wei X, et al: PGE2 and IL-6 production by fibroblasts in response to titanium wear debris particles is mediated through a Cox-2 dependent pathway. J Orthop Res 2004;22:6-12.
Question 18
03 Fig 51c. What laboratory finding is most likely associated with this disease entity?
Explanation
Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Inst Course Lect 2002;51:413-428
back to this question next question
Question 19
Which of the following is considered a contraindication to cement injection techniques, such as kyphoplasty or vertebroplasty, in the treatment of osteoporotic compression fractures?
Explanation
REFERENCES: Phillips FM, Pfeifer BA, Leiberman IH, et al: Minimally invasive treatment of osteoporotic vertebral compression fractures: Vertebroplasty and kyphoplasty. Instr Course Lect 2003;52:559-567.
Truumees E, Hilibrand A, Vaccaro AR: Percutaneous vertebral augmentation. Spine J 2004;4:218-229.
Rao RD, Singrakhia MD: Painful osteoporotic vertebral fracture: Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85:2010-2022.
Question 20
A 16-year-old female with adolescent idiopathic scoliosis undergoes posterior spinal fusion with instrumentation. The thoracic pedicle screws were placed using a tap 1 mm smaller than the screw diameter and a straightforward trajectory that runs parallel to the superior endplate. This techniques allows for which of the following: Review Topic
Explanation
Contemporary segmental pedicle screw placement used in the treatment of scoliosis deformity offer significantly higher screw pullout and deformity correction than prior hook and wire constructs. Additionally, screw insertional torque has been found in numerous studies to correlate with resistance to screw pullout. Several factors have been found to increase maximum screw insertional torque, including tapping 1mm smaller than the screw diameter and using the straightforward trajectory. It is important to note that while undertapping makes for a stronger screw, there are some studies that suggest not tapping at all makes for an even stronger screw.
Lehman et al. performed a biomechanical study evaluating maximum insertional torque when tapping line to line, undertapping by 0.5mm, and undertapping by 1mm in 34 fresh frozen cadavers. They found undertapping the thoracic pedicle by 1mm increased maximum insertional torque by 47% when compared to undertapping by 0.5mm and by 93% when compared to line to line tapping.
Kuklo et al. performed a biomechanical study on thirty cadavers using the straightforward technique (sagittal trajectory of the screws parallels the superior endplate of the vertebral body) versus anatomic trajectory (22 degrees in the cephalo-caudad direction in the sagittal plane). They found maximum insertional torque to be
Question 21
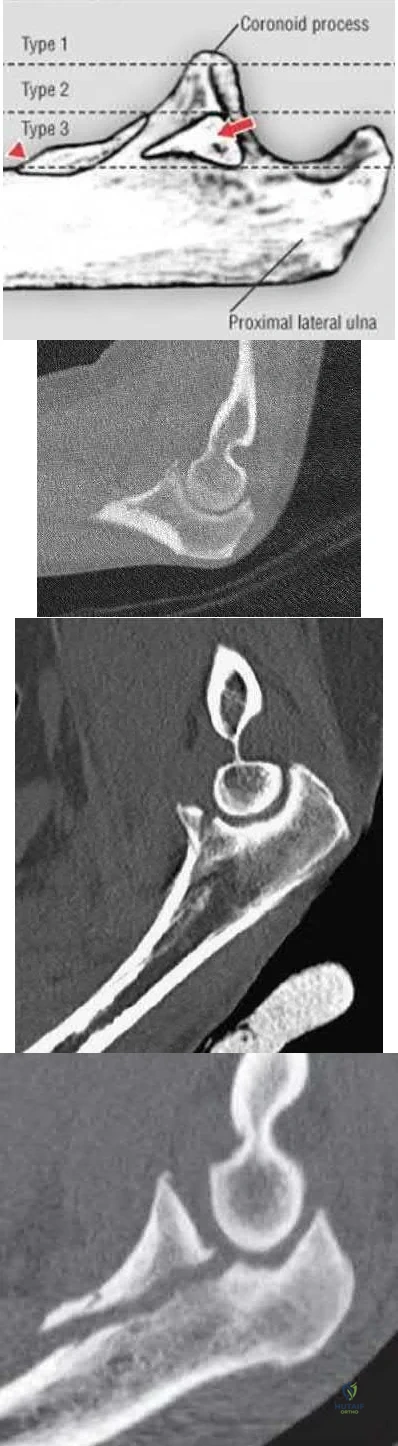
A 40-year-old man sustains a fall while mountain biking and presents with a posterior elbow fracture-dislocation. The elbow is reduced in the ER and noted to be grossly unstable with varus and valgus stress. Imaging demonstrates a two part radial head fracture involving 40% of the articular surface and a fracture involving less than 10% of the coronoid tip. He is taken to the OR for surgical reconstruction. After fixation of the radial head and repair of the LCL complex, the elbow is fluoroscopically examined and noted to be unstable with valgus stress. The elbow is ranged and dislocates at less than 45 degrees of flexion with the forearm in full supination. What is the next best step in management?
Explanation
OrthoCash 2020
Question 22
A 60-year-old woman has activity-related hip pain after undergoing arthroplasty 5 years ago. She has severe Parkinsonism and denies fevers or chills. Radiographs are shown in Figures 45a and 45b. What is the most likely cause of her pain?
Explanation
REFERENCES: Harris WH, McCarthy JC, O’Neill DA: Femoral component loosening using contemporary techniques of femoral cement fixation. J Bone Joint Surg Am 1982;64:1063-1067.
Callaghan JJ, Rosenberg AG, Rubash H (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 960, 1228-1229.
Maloney WJ, Schmalzreid T, Harris WH: Analysis of long-term cemented total hip arthroplasty retrievals. Clin Orthop Relat Res 2002;405:70-78.
Question 23
A positive straight leg raising sign is when pain radiates distal to the knee when the affected leg is passively elevated. The increased tension generally occurs between Review Topic
Explanation
Question 24
What preoperative factor correlates best with the outcome of rotator cuff repair?
Explanation
REFERENCES: Iannotti JP: Full-thickness rotator cuff tears: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Iannotti JP, Bernot MP, Kuhlman JR, Kelley MJ, Williams GR: Postoperative assessment of shoulder function: A prospective study of full-thickness rotator cuff tears. J Shoulder Elbow Surg 1996;5:449-457.
Question 25
- Which of the following advantages does the use of a vascularized fibula graft have over a nonvascularized fibula graft?
Explanation
And a vascularized graft requires greater technical skills and a larger dissection to isolate the vascular pedicle with associated increased donor site morbidity.
Question 26
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of
Explanation
REFERENCES: Cain JE Jr, Major MR, Lauerman WC, et al: The morbidity of heparin therapy after development of pulmonary embolus in patients undergoing thoracolumbar or lumbar spinal fusion. Spine 1995;20:1600-1603.
Roberts AC: Venous imaging and inferior vena cava filters. Curr Opin Radiol 1992;4:88-96.
Becker DM, Philbrick JT, Selby JB: Inferior vena cava filters. Arch Intern Med
1992;152:1985-1994.
Question 27
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of
Explanation
50 degrees) with multiple contiguous vertebral wedging and end plate irregularity, all consistent with the diagnosis of Scheuermann’s kyphosis. The patient is skeletally immature; therefore, there is the potential for progression of the kyphotic deformity. Extension bracing has shown efficacy in the treatment of Scheuermann’s kyphosis that measures 50 degrees to 74 degrees, and has actually reduced the curvature permanently in some patients. A thoracolumbosacral orthosis may be used if the apex of kyphosis is at T7 or lower. Indications for surgical treatment are controversial, but spinal fusion most likely should not be considered for a painless kyphosis measuring less than 75 degrees.
REFERENCES: Murray PM, Weinstein SL, Spratt KF: The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am 1993;75:236-248.
Wenger DR, Frick SL: Scheuermann kyphosis. Spine 1999;24:2630-2639.
Tribus CB: Scheuermann’s kyphosis in adolescents and adults: Diagnosis and management.
J Am Acad Orthop Surg 1998;6:36-43.
Question 28
A 23-year-old right-hand dominant professional baseball pitcher has right shoulder pain when releasing the ball. He has noticed his velocity has decreased over the past 2 months. Examination reveals supine abducted external rotation of 110 degrees compared to 100 degrees on the left side. His internal rotation is 30 degrees on the right compared to 70 degrees on the left side. Rotator cuff strength is normal. All other clinical tests are normal. MRI with contrast reveals no intra-articular lesions. What is the best course of treatment?
Explanation
REFERENCES: Meister K: Injuries to the shoulder in the throwing athlete. Part two: evaluation/ treatment. Am J Sports Med 2000;28:587-601.
Liu SH, Boynton E: Posterior superior impingement of the rotator cuff on the glenoid rim as a cause of shoulder pain in the overhead athlete. Arthroscopy 1993;9:697-699.
Tyler TF, Nicholas SJ, Roy T, et al: Quantification of posterior capsule tightness and motion loss in patients with shoulder impingement. Am J Sports Med 2000;28:668-673.
2010 Sports Medicine Examination Answer Book • 21
Question 29
Which of the following palpable bony landmarks is correctly matched with its corresponding vertebral level?
Explanation
REFERENCES: Smith GW, Robinson RA: The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am 1958;40:607.
An HS: Surgical Exposure and Fusion Techniques of the Spine: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and William, 1998, pp 31-62.
Question 30
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
REFERENCES: Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 31
Figure 16a shows the radiograph of a 34-year-old woman who sustained a basicervical fracture of the femoral neck. The fracture was treated with a compression screw and side plate. Seven months postoperatively, she continues to have significant hip pain and cannot bear full weight on her hip. A recent radiograph is shown in Figure 16b. Management should now consist of
Explanation
REFERENCES: Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Ballmer FT, Ballmer PM, Baumgaertel F, et al: Pauwels osteotomy for nonunions of the femoral neck. Orthop Clin North Am 1990;21:759-767.
Question 32
When an acute infection of a total elbow arthroplasty is managed with irrigation and debridement, which of the following organisms is associated with the highest risk of persistent infection?
Explanation
IV antibiotics.
REFERENCES: Yamaguchi K, Adams RA, Morrey BF: Infection after total elbow arthroplasty. J Bone Joint Surg Am 1998;80:481-491.
Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components. J Bone Joint Surg Am 1990;72:1383-1390.
Question 33
When discussing treatment options with a 35 year-old healthy male with an isolated, closed tibial shaft fracture, the surgeon should inform him that in comparison to closed treatment, the advantages of intramedullary nail fixation include all of the following EXCCEPT?

Explanation
In a study of 94 tibial fractures, Finkemeier reported 10 (11%) had compartment syndromes. Three of the 10 patients developed the compartment syndrome postoperatively.
In comparing IM nailing to non-op, Bone et al showed that IM nailing had a shorter time to union (mean, 18 vs 26 weeks; p = 0.02), lower non-union rate (2% vs 10%), decresed incidence of shortening (2% vs 27%), and quicker return to work (mean, 4 vs 6.5 months), but no difference in compartment syndrome (0% in both groups).
The classic article cited by Sarmiento el al. reported that closed treatment with use of a prefabricated functional below-the-knee brace was effective in a study of 1000 closed diaphyseal fractures of the tibia with an incidence of nonunion of only 1.1%. However, those authors had very strict criteria for use of the fracture-brace (exclusion criteria included intact fibular, shortening >2cm).
Question 34
- What is the primary reason for choosing a bone graft substitute rather than an autologous cancellous graft in the treatment of distal radius fractures with metaphyseal comminution and impaction?
Explanation
Question 35
Figures A and B show radiographs of a 24-year-old female with a soccer injury. A physical examination reveals an isolated, closed injury with no clinical features of neurovascular injury or compartment syndrome. She has been consented to be treated with intramedullary nail fixation. A pre-operative note by the anaesthesiology team makes reference to the patients fair skin and natural red-hair color. How will this information affect the post-operative management of this patient?

Explanation
Melanocortin-1-receptor (MC1R) is one of the key proteins involved in hair color and skin tone. Mutations of the MC1R alleles can render this protein non-functional, which results in a phenotype of red-hair and fair skin. Mutations of the MC1R have shown to modulate the pain response and opioid efficacy in these patients. Women are
more commonly affected and often require more anaesthetic and higher dosages of opioid to achieve comparable MAC level and pain-relief, respectively, as women with other hair types.
Liem et al. showed that a greater concentration of induction and maintenance agents (sevoflurane and desflurane, respectively) were required to sustain comparable MAC levels in red-haired patients as dark haired patients.
Fillingim et al. reviewed the affect of gender, sex and pain. They concluded there is a biopsychosocial element of pain that is perceived differently by men and women. In terms of postoperative and procedural pain, the outcome might be more severe in women than men.
Delaney et al. looked at the involvement of the melanocortin-1 receptor in acute pain in mice. They found that while the MC1R is better known as a gene involved in mammalian hair colour, it was shown to be involved in the pain pathway of inflammatory but not neuropathic origin. Mutations of MC1R showed increased tolerance to noxious pain stimulus in mice.
Figures A and B are AP and lateral radiographs of a left tibia. There is a low energy, distal third shaft fracture with no cortical apposition on the AP view.
Incorrect Answers:
Question 36
What factor induces myofibrillar muscle protein synthesis (MPS)? Review Topic
Explanation
Question 37
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of
Explanation
REFERENCES: Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Jupiter JB, Ring D: Operative treatment of post-traumatic proximal radioulnar synostosis.
J Bone Joint Surg Am 1998;80:248-257.
Question 38
A 65-year-old woman with rheumatoid arthritis is undergoing revision total knee arthroplasty (TKA) during which the medial collateral ligament (MCL) is damaged. Suture anchors are used to attempt primary repair, and a varus-valgus constrained insert also is used. Postsurgically she experiences instability that does not respond to bracing with a 3+ opening to valgus stress (Figure 120). What is the most appropriate surgical option?
Explanation
MCL repair or reconstruction may be considered in younger, more active patients, but this intervention is technically demanding and produces variable results. Rotating-hinge TKA is associated with good results in a number of small series that include cases performed with MCL insufficiency or absence. A rotating hinge is preferable over a fixed hinge because of decreased stresses on implants imposed by fixed-hinge devices.
Question 39
A 36-year-old recreational tennis player sustains the injury shown in Figure 16. Management should consist of
Explanation
REFERENCES: Matava MJ: Patellar tendon ruptures. J Am Acad Orthop Surg 1996;4:287-296.
Marder RA, Timmerman LA: Primary repair of patellar tendon rupture without augmentation. Am J Sports Med 1999;27:304-307.
Question 40
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
REFERENCES: Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures:
A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170.
Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Cretnik A, Kosanovic M, Smrkolj V: Percutaneus versus open repair of the ruptured Achilles tendon: A comparative study. Am J Sports Med 2005;33:1369-1379.
Question 41
A 22-year-old professional baseball catcher has posterior shoulder pain and severe external rotation weakness with the arm in adduction. Radiographs are normal. MRI scans are shown in Figures 15a through 15c. Management should consist of Review Topic

Explanation
Question 42
Which of the following patients is considered the most appropriate candidate for selective dorsal rhizotomy?
Explanation
REFERENCES: Peacock WJ, Arens LJ, Berman B: Cerebral palsy spasticity: Selective posterior rhizotomy. Pediatr Neurosci 1987;13:61-66.
Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
Mooney JF III, Millis MB: Spinal deformity after selective dorsal rhizotomy in patients with cerebral palsy. Clin Orthop 1999;364:48-52.
Question 43
A 78-year-old man has a history of worsening bilateral calf pain with activity. MRI scans are shown in Figures 31a through 31d. His symptoms are not improved with forward flexion of the lumbar spine. His lower extremity pain is relieved when he sits or ceases activity. Which of the following tests would be most helpful in establishing a diagnosis? Review Topic
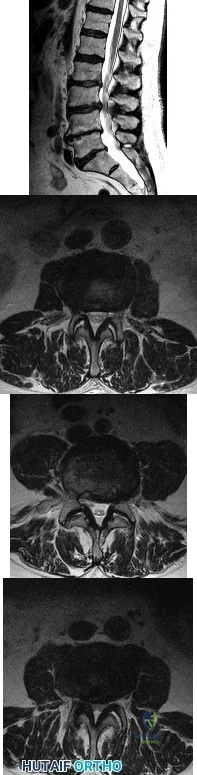
Explanation
Decreased range of motion and hip joint pain, especially in internal rotation and abduction, are common findings in patients with degenerative arthritis of the hip. While post-myelography CT has been found superior to MRI as a single study for the preoperative planning of decompression for lumbar spinal stenosis, it will not assist in differentiating vascular from neurogenic claudication.
Question 44
When using a two-incision approach for open reduction and internal fixation of a Hawkins III talar fracture-dislocation involving the talar neck and body, what anatomic structure must be preserved to optimize outcome?
Explanation
REFERENCES: Mulfinger GL, Trueta J: The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-167.
Vallier HA, Nork SE, Barei DP, et al: Talar neck fractures: Results and outcomes. J Bone Joint Surg Am 2004;86:1616-1624.
Question 45
Figure 83a shows an axillary radiograph and Figures 83b and 83c show axial MR arthrograms of a 20-year-old collegiate offensive lineman who has shoulder pain while pass-blocking. He sustained a shoulder injury 3 months earlier when he "jammed it." Prior to this injury, he denies any pain or instability in either shoulder. Despite undergoing rehabilitation with a physical therapist and trainer and abstaining from playing for 6 weeks, he is currently unable to play because of his symptoms. Examination reveals full active range of motion, a positive jerk test which reproduces his symptoms, and a grade 2 posterior translation of the humeral head with load and shift testing which also reproduces his symptoms. What is the best management option to allow him to return to his pre-injury function next season? Review Topic
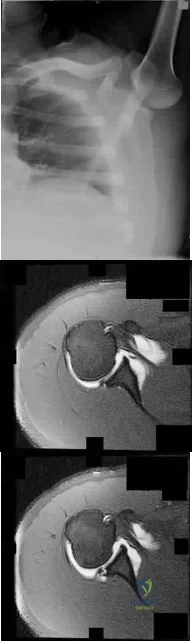
Explanation
Question 46
Which of the following have been found to affect the rate of perioperative infections or wound complication rates in foot and ankle surgery?
Explanation
REFERENCES: Bibbo C, Anderson RB, Davis WH, et al: The influence of rheumatoid chemotherapy, age, and presence of rheumatoid nodules on postoperative complications in rheumatoid foot and ankle surgery: Analysis of 725 procedures in 104 patients. Foot Ankle Int 2003;24:40-44.
Bibbo C, Goldberg JW: Infections and healing complications after elective orthopaedic foot and ankle surgery during tumor necrosis factor-alpha inhibition therapy. Foot Ankle Int
2004;25:331-335.
Sorensen LT, Karlsmark T, Gottrup F: Abstinence from smoking reduces incisional wound infection: A randomized controlled trial. Ann Surg 2003;238:1-5.
Question 47
A 30-year-old man has had a 3-day history of severe, incapacitating lower back pain without radiation. He reports improvement with rest. He denies any history of trauma, has no constitutional symptoms, and his neurologic examination is normal. What is the best course of action?
Explanation
REFERENCE: Deyo RA, Diehl AK, Rosenthal M: How many days of bed rest for acute low back pain? A randomized clinical trial. N Engl J Med 1986;315:1064-1070.
Question 48
A 58-year-old woman with a history of severe asthma and long-term prednisone use reports a progression of chronic shoulder pain for the past 6 months. Radiographs and MRI scans are shown in Figures 30a through 30d. What is the most likely diagnosis?
Explanation
REFERENCES: Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 871-874.
Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
Question 49
What is the most important muscle adaptation resulting from endurance training? Review Topic
Explanation
Question 50
- A 12 month old infant has congenital complete absence of the tibia. Examination reveals that the femur in the abnormal limb is 3 cm short, with a normal ipsilateral hip. The patient has an intact fibula, an equinovarus foot with four rays, and moderate popliteal skin webbing. Management should consist of
Explanation
Question 51
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals a lumbar paraspinal spasm and a positive straight leg raising test. The deep tendon reflexes, motor strength, and sensation in the lower extremeties are normal. The radiographs are normal. If symptoms persist for more than a few weeks, management should consist of
Explanation
REFERENCES: Epstein JA, Epstein NE, Marc J, Rosenthal AD, Lavine LS: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Hashimoto K, Fujita K, Kojimoto H, Shimomura Y: Lumbar disc herniation in children. J Pediatr Orthop 1990;10:394-396.
Question 52
A 56-year-old woman underwent a total knee arthroplasty 2 years ago and now has pain and swelling. Radiographs of her knee are unremarkable. Her C-reactive protein (CRP) level is 3.0 (reference range [rr], 0.08–3.1 mg/L), and her erythrocyte sedimentation rate (ESR) is 18 mm/h (rr, 0-20 mm/h). Aspiration of the knee reveals a white blood cell (WBC) count of 1200/mm3 with a differential of 30% neutrophils and 70% monocytes. Cultures will not be available for several days, and the patient has not been taking antibiotics. Based on these findings, the most appropriate next step is
Explanation
ESR and CRP level are recommended as starting points in the workup for the diagnosis or exclusion of periprosthetic joint infection (PJI). When both the ESR and CRP findings are within defined limits, PJI is unlikely. When both test findings are positive, PJI must be considered and further investigation is warranted. Clinicians need to be aware of other inflammatory conditions such as rheumatoid arthritis that can lead to elevation of inflammatory markers.
A high likelihood of infection is noted when the knee aspirate contains more than 2500 WBCs per high-powered field (HPF) with a differential count exceeding 60% neutrophils. Using these criteria, Mason demonstrated a sensitivity of 98% and a specificity of 95% for infection diagnosis.
For this patient, the inflammatory markers are within normal limits. The aspiration result is below 2500 WBC/HPF with a low percentage of neutrophils. The likelihood of infection is remote, and further nonsurgical treatment should not include antibiotics. There is no indication for surgery based upon the information presented.

Question 53
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient’s neurologic recovery can be best determined by
Explanation
REFERENCES: Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1185-1194.
Question 54
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?
Explanation
Question 55
- Chronic flatfoot deformity is most commonly associated with a contracture of the
Explanation
Deltoid ligament, plantar fascia, or intrinsic tendon contracture would not cause this deformity.
Question 56
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70° of the right knee. The active arc of motion is from 70° to 90°, and the opposite knee has a flexion contracture of 10°. Both hips are dislocated with flexion contractures of 10°, passive hip motion is from 10° to 90° of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
REFERENCES: Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469.
DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Sells JM, Jaffe KM, Hall JG: Amyoplasia, the most common type of arthrogryposis: The potential for good outcome. Pediatrics 1996;97:225-231.
Question 57
This condition is most prevalent in people of which ancestry?
Explanation
The radiograph of the lateral lumbosacral spine reveals an isthmic spondylolysis with a Meyerding grade 1 spondylolisthesis. The incidence of spondylolysis in the general population is around 5%, and grade 1 or 2 slips are present in the majority of children with a spondylolysis. Many cases of spondylolysis are painless and discovered incidentally, but, when painful, hyperextension of the lumbar spine may stress the area of the pars defect and exacerbate a patient’s symptoms. A diagnosis can usually be determined with a lateral radiograph of the lumbar spine. Although oblique lumbar radiographs are frequently ordered, several studies have shown that they do not increase diagnostic or prognostic accuracy. Progression of an isthmic spondylolysis, with or without a grade 1 or 2 listhesis, to a serious slip that might
necessitate surgical intervention is rare and occurs in fewer than 5% of patients. Chance for progression diminishes with age, with patients at highest risk prior to the adolescent growth spurt. Spondylolysis may have a genetic component; an increased prevalence has been found in some families and in some ethnic groups, especially among the Native American population.

Question 58
Figure below depicts the radiograph obtained from a 30-year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of Figure below reveals

Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 59
Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?
Explanation
REFERENCES: Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 145-150, 324.
Anderson JE (ed): Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Williams & Wilkins, 1978, plate 4-46.
Question 60
Figures 1 through 3 demonstrate the radiographs obtained from a 45-year-old construction worker who has wrist pain, loss of motion, and loss of strength. Nonsurgical measures have failed, and the patient requests surgery. What is the best surgical option for this patient?

Explanation
This patient has a physically demanding occupation. His radiographs show a long-standing nonunion with avascular necrosis and collapse of the proximal pole. This condition is referred to as a scaphoid nonunion advanced collapse wrist (SNAC). He has advanced arthritis of the capitolunate joint, but the radiolunate joint is preserved. The best option for him would be scaphoid excision with four-corner fusion. Proximal row carpectomy, would be incorrect because of the advanced arthritis of the capitolunate joint. This procedure relies on normal cartilage/joint articulation of the capitate as well as of the lunate fossa of the distal radius. Proximal pole scaphoid excision alone would not address the advanced arthritis of the capitolunate joint. Scaphoid fixation with bone grafting would not address the midcarpal arthritis and advanced proximal pole collapse.
Question 61
Which of the following treatments of polyethylene results in the highest amount of oxidative degradation?
Explanation
REFERENCES: Sanford WM, Saum KA: Accelerated oxidative aging testing of UHMWPE. Trans Orthop Res Soc 1995;20:119.
Sun DC, Schmidig G. Stark C, et al: On the origins of a subsurface oxidation maximum and its relationship to the performance of UHMWPE implants. Trans Soc Biomater 1995;18:362.
Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 35-41.
McKellup HA: Bearing surfaces in total hip replacement: State of the art and future developments. Instr Course Lect 2001;50:165-179.
Question 62
A 51-year-old woman with shoulder pain responds transiently to a subacromial injection and physical therapy exercise program. When her symptoms recur, an arthroscopic subacromial decompression is recommended. During the surgery, a partial-thickness articular-sided supraspinatus tear is noted. The supraspinatus footprint is exposed for 3 mm from the articular margin. The remaining intra-articular structures are normal. Inspection from the bursal surface reveals the tendon to be intact. What is the most appropriate course of management? Review Topic
Explanation
Question 63
Following total knee arthroplasty, a patient is noted to have asymmetrical absent pulses and poor capillary refill. What is the next most appropriate step in management?
Explanation
perform an
DISCUSSION: An assessment of the location of the vascular compromise is necessary prior to surgical exploration. Vascular repair will most likely require a separate surgical exposure. Vascular reperfusion may be accomplished at the time of an arteriogram with the use of a stent in certain situations. Return to the operating room with vascular surgical consultation and intraoperative arteriogram is appropriate.
An immediate postoperative compartment syndrome is unlikely. Magnetic resonance angiogram is not appropriate because of the potential for a delay in diagnosis.
REFERENCE: Smith DE, McGraw RW, Taylor DC, et al: Arterial complications and total knee arthroplasty. J Am Acad Orthop Surg 2001 ;9;253-257.
Question 64
A 58-year-old man has a painful right hip 3 years after undergoing a large head metal-on-metal total hip arthroplasty (THA) in which the components are well positioned. MR imaging confirms a cystic mass around the hip and metal ion levels show a marked increase in cobalt compared to chromium levels. The erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level are within defined limits. What is the most likely cause for his discomfort?
Explanation
This patient presents with a pseudotumor likely attributable to local tissue reaction resulting from either articular metal wear debris and/or corrosion and fretting of the trunnion. The trunnion is a more likely source of the problem for a number of reasons: good position of metal articulation, increased trunnion corrosion and fretting associated with large-head THA, and markedly increased cobalt levels compared to chromium levels. Infection is very unlikely
in the setting of normal ESR and CRP findings. MR imaging findings are consistent with pseudotumor and not iliopsoas tendonitis or trochanteric bursitis.

CLINICAL SITUATION FOR QUESTIONS 42 THROUGH 45
Figures 42a through 42e are the radiographs, MR image, and MR arthrogram of a 25-year-old collegiate soccer player who has new-onset left groin pain. He played competitive soccer from a young age and has either competed or practiced 5 to 6 times per week since the age of
Question 65
In revision total hip arthroplasty, an acetabular reconstruction cage is best indicated for which of the following patterns of bone loss?
Explanation
REFERENCES: Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 66
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of
Explanation
REFERENCES: Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
Brumback RJ, Ellison TS, Poka A, et al: Intramedullary nailing of femoral shaft fractures: Part III. Long-term effects of static interlocking fixation. J Bone Joint Surg Am 1992;74:106-112.
Question 67
Figure 1 is the MR image of a high school soccer player who sustained a right knee injury during a game while making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a "clunk" within the knee. What is the most likely biomechanical basis for the "clunk"?

Explanation
Question 68
Figure 61 is the radiograph of a 34-year-old woman who was involved in a rollover motor vehicle accident. On arrival at the trauma center she is hypotensive and tachycardic. An abdominal CT scan reveals a spleen laceration. The patient remains hypotensive despite resuscitation and is taken to surgery for an emergent laparotomy and splenectomy. After surgery her delta base is -9 mmol/L. What is the most appropriate management of her pelvic ring injury? Review Topic

Explanation
(SBQ12TR.80) A 37-year-old male arrives to the trauma slot following a high-speed motorcycle crash. His Glasgow Coma score is 14 and his only orthopaedic injury is exhibited in Figure A. His current vital signs are a BP of 90/60, HR 120, and a lactate of 2.5 mMol/L. Other findings include a grade 1 splenic laceration and bilateral pulmonary contusions seen on chest radiograph. Which of the following has been suggested as an indication to perform damage control orthopedic care?

1 HR >110
Bilateral pulmonary contusions seen on chest radiograph
SBP = 90mmHg
Unilateral femur fracture
Lactate = 2.5 mMol/L
Pulmonary contusion severe enough to be diagnosed on chest radiograph alone is an indicator that the patient may benefit from damage control orthopaedics (DCO).
Despite the patient's overall stable nature, suffering pulmonary injury severe enough to be seen on x-ray alone suggests that temporary stabilization with staged definitive fixation may avoid potential morbidity.
Pape et al. review the evolution and balance of early total care (ETC) and DCO. Summarizing the literature, the authors report several standalone indicators that would justify DCO regardless of stable status. This includes: Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with chest trauma, multiple injuries with severe pelvic/abdominal trauma/ hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs alone, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater.
Figure A exhibits a right femoral shaft fracture. Illustration A exhibits a summarized table stating the criterion used to determine the condition of a polytrauma patient. (Table from Pape et al, PMID: 19726738)
Incorrect answers:
Question 69
Corticosteroids inhibit the formation of effectors of the inflammatory pathway via inhibition of
Explanation
Question 70
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?
Explanation
REFERENCES: Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815.
Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Moro JK, Werier J, MacDermid JC, et al: Arthroplasty with a metal radial head for unreconstructable fractures of the radial head. J Bone Joint Surg Am 2001;83:1201-1211.
Question 71
Figure 17 shows the radiograph of an 82-year-old right-hand dominant woman who fell while weeding her garden. She has severe right shoulder pain. She is neurovascularly intact. What is the most appropriate treatment? Review Topic

Explanation
Question 72
Which of the following structures is the most important restraint to posterior subluxation of the glenohumeral joint when positioned in 90 degrees of flexion and internal rotation?
Explanation
REFERENCES: Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML: Posterior glenohumeral subluxation: Active and passive stabilization in a biomechanical model. J Bone Joint Surg Am 1997;79:433-440.
Flatow EL, Warner JI: Instability of the shoulder: Complex problems and failed repairs: Part I. Relevant biomechanics, multidirectional instability, and severe glenoid loss. Instr Course Lect 1998;47:97-112.
Question 73
A well-developed college football player reports swelling and a heaviness in the arm after lifting weights. Examination reveals that distal pulses are normal and equal in both arms. A venogram is shown in Figure 13. What is the most likely cause of this condition?
Explanation
REFERENCES: Angle N, Gelabert HA, Farooq MM, et al: Safety and efficacy of early surgical decompression of the thoracic outlet for Paget-Schroetter syndrome. Ann Vasc Surg 2001;15:37-42.
Azakie A, McElhinney DB, Thompson RW, et al: Surgical management of subclavian-vein effort thrombosis as a result of thoracic outlet compression. J Vasc Surg 1998;28:777-786.
Question 74
A 37-year-old man has left shoulder pain and weakness. Coronal T1- and axial T2-weighted MRI scans are shown in Figures 17a and 17b. The biopsy specimen is shown in Figure 17c. What is the most likely diagnosis?
Explanation
REFERENCES: Ferrick MR, Marzo JM: Suprascapular entrapment neuropathy and ganglion cysts about the shoulder. Orthopedics 1999;22:430-434.
Post M: Diagnosis and treatment of suprascapular nerve entrapment. Clin Orthop 1999;368:92-100.
Question 75
Figure 1 shows a patient with an open tibia fracture who presents to the emergency department after a propeller injury in brackish water (river water and sea water). What is the most appropriate antibiotic coverage for this patient?

Explanation
soil-borne pathogens (clostridial species). Vancomycin is not indicated for coverage in marine environments, rather it is more commonly used for populations with a high prevalence of nosocomial infections. Sulfamethoxazole-trimethoprim is not used for open fracture coverage.
Question 76
- Radiographs of the cervical spine of a 73-year-old man who fell down stairs reveal cervical spondylosis without evidence of fracture or dislocation. MRI and CT scans are consistent with the plain radiographs. After 72 hours, neurologic evaluation reveals intact sensation; however, weakness of the upper extremities is greater than that of the lower extremities. What is the most likely diagnosis?
Explanation
extremity deep pressure and proprioceptive preserved. 3-Posterior cord syndrome is rare with loss of deep pressure, deep pain, and proprioception. 4-Brown-Sequard syndrome-Uncommon-Ipsilateral motor deficit, contralateral pain and temperature deficit. 5-Cervical nerve root injury- functional impairment of the cervical spine. Symptoms are often acute and severe, dependent on the level of the lesion. An infraforaminal protrusion may compress only the spinal root ganglion resulting in severe brachialgia with paresthesia and numbness but with little or no motor involvement.
Question 77
A 72-year-old woman is evaluated for sacrococcygeal pain sustained after a twisting injury. Radiographic and MRI evaluation confirms the presence of a nondisplaced fracture at the sacrococcygeal junction. Over a 3-week period, the pain has gotten significantly better. No additional lesions or injuries are noted. Laboratory studies show a serum calcium level of 8.8 mg/dL (normal 8.6-10.3 mg/dL) and a 25-OH Vitamin D level of 14 ng/mL (normal 30-80 ng/mL). What is the most appropriate treatment for this patient?
Explanation
Question 78
What is the neoplastic cell of origin for this tumor?
Explanation
Tenosynovial giant-cell tumors are widely known as pigmented villonodular synovitis (PVNS), although this term is misleading because this tumor type is a clonal neoplasm and does not involve an inflammatory process. It often is shown to have a t(1:2)(p13q37) karyotype resulting in CSF1-COL6A3 gene fusion. There are various amounts of mononuclear cells, osteoclastlike giant cells, foamy histiocytes, hemosiderophages, and chronic inflammatory cells. Local recurrences are common, but CSF1R inhibitors are being investigated in studies involving local control improvement and disease regression.
Targeted therapy trials to assist in control of the diffuse-type tenosynovial giant-cell tumor (formerly called PVNS) involve the use of monoclonal antibodies that inhibit CSF1R activation. CSF1R-expressing mononuclear phagocytes are affected by these monoclonal antibodies.
Infantile fibrosarcoma is associated with the t(12;15)(p13;q25) karyotype and ETV6-NTRK3 gene fusion product. Nodular fasciitis is associated with the t(17;22)(p13;q13.1) karyotype and MYH9-USP6 gene fusion product. Inflammatory myofibroblastic tumor is associated with translocations involving 2p23 resulting in multiple fusion products of ALK with TPM4 (19p13.1), TPM3 (1q21), CLTC (17q23), RANBP2 (2q13), ATIC (2q35), SEC31A (4q21), and CARS (11p15). No
nonpreferred response has a histologic appearance that includes hemosiderin, foamy histiocytes, and osteoclastlike giant cells.
A conformation-specific inhibitor of the juxtamembrane region of CSF1R is a synthetic molecule that is designed to access the autoinhibited state of the receptor through direct interactions with the juxtamembrane residues embedded in the adenosine 5’-triphosphate-binding pocket. It is designed to bind in the regulatory a-helix of the N-terminal lobe of the kinase domain in neoplastic cells of tenosynovial giant-cell tumor that have expression of the CSF1 gene. There is a structural plasticity of the domain of the CSF1R that allows the molecule to directly bind the autoinhibited state of CSF1R.
Another approach involves the development of the anti-CSF1R antibody, emactuzumab, which targets tumor-associated macrophages. A lower percentage of volume reduction has been reported with imatinib, a tyrosine kinase inhibitor. Alkylating agents have not been used in this benign neoplasm.
Tenosynovial giant-cell tumor is characterized by an overexpression of CSF1. CSF1R activation leads to recruitment of CSF1R-expressing cells of the mononuclear phagocyte lineage.
RECOMMENDED READINGS
Cassier PA, Gelderblom H, Stacchiotti S, Thomas D, Maki RG, Kroep JR, van der Graaf WT, Italiano A, Seddon B, Dômont J, Bompas E, Wagner AJ, Blay JY. Efficacy of imatinib mesylate for the treatment of locally advanced and/or metastatic tenosynovial giant cell tumor/pigmented villonodular synovitis. Cancer. 2012 Mar 15;118(6):1649-55. doi: 10.1002/cncr.26409. Epub 2011 Aug 5. PubMed PMID: 21823110. View Abstract at PubMed
Ladanyi M, Fletcher JA, Dal Cin P. Cytogenetic and molecular genetic pathology of soft tissue tumors. In: Goldblum JR, Folpe AL, Weis SW, eds. Enzinger & Weiss’s Soft Tissue Tumors. 6th ed. Philadelphia, PA: Elsevier Saunders; 2014:76-109.
Staals EL, Ferrari S, Donati DM, Palmerini E. Diffuse-type tenosynovial giant cell tumour: Current treatment concepts and future perspectives. Eur J Cancer. 2016 Aug;63:34-40. doi: 10.1016/j.ejca.2016.04.022. Epub 2016 Jun 5. Review. View Abstract at PubMed
Tap WD, Wainberg ZA, Anthony SP, Ibrahim PN, Zhang C, Healey JH, Chmielowski B, Staddon AP, Cohn AL, Shapiro GI, Keedy VL, Singh AS, Puzanov I, Kwak EL, Wagner AJ, Von Hoff DD, Weiss GJ, Ramanathan RK, Zhang J, Habets G, Zhang Y, Burton EA, Visor G, Sanftner L, Severson P, Nguyen H, Kim MJ, Marimuthu A, Tsang G, Shellooe R, Gee C, West BL, Hirth P, Nolop K, van de Rijn M, Hsu HH, Peterfy C, Lin PS, Tong-Starksen S, Bollag G. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N Engl J Med. 2015 Jul 30;373(5):428-37. doi:10.1056/NEJMoa1411366. PubMed PMID: 26222558. View Abstract at PubMed
Ries CH, Cannarile MA, Hoves S, Benz J, Wartha K, Runza V, Rey-Giraud F, Pradel LP, Feuerhake F, Klaman I, Jones T, Jucknischke U, Scheiblich S, Kaluza K, Gorr IH, Walz A, Abiraj K, Cassier PA, Sica A, Gomez-Roca C, de Visser KE, Italiano A, Le Tourneau C, Delord JP, Levitsky H, Blay JY, Rüttinger D. Targeting tumor-associated macrophages with anti-CSF-1R antibody reveals a strategy for cancer therapy. Cancer Cell. 2014 Jun 16;25(6):846-59. doi: 10.1016/j.ccr.2014.05.016. Epub 2014 Jun 2. PubMed PMID: 24898549.View Abstract at PubMed
Question 79
Lymphangioma
Explanation
Question 80
A 12-year-old girl has progressive development of cavus feet. Examination reveals slightly diminished vibratory sensation on the bottom of the foot. Reflexes are 1+ at the knees and ankles. Motor examination shows that all muscles are 5/5 in the foot, except the peroneal and anterior tibial muscles are rated as 4+/5. Which of the following studies is considered most diagnostic?
Explanation
REFERENCES: Chance PF: Molecular genetics of hereditary neuropathies. J Child Neurol 1999;14:43-52.
Bell C, Haites N: Genetic aspects of Charcot-Marie-Tooth disease. Arch Dis Child 1998;78:296-300.
Question 81
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?
Explanation
REFERENCES: Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Sanders R: Displaced intraarticular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Sanders R, Fortin P, DiPasquale T, et al: Operative treatment in 120 displaced intra-articular calcaneal fractures: Results using a prognostic computed tomography scan classification. Clin Orthop Relat Res 1993;290:87-95.
Question 82
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?
Explanation
REFERENCES: Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Sharkey PF, Hozack WJ, Dorr LD, Maloney WJ, Berry D: The bearing surface in total hip arthroplasty: Evolution or revolution, in Price CT (ed): Instructional Course Lectures 49. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 41-56.
Question 83
A 46-year-old man with a sacral chordoma is treated with sacrectomy.
Explanation
Complications frequently occur following treatment for spinal disorders. Postsurgical morbidity may range from minor complications such as urinary tract infection to death. Wound infections are among the most commonly encountered complications following any surgical intervention; however, their incidence after spine surgery has been reported to be in the range of only 1% to 6%. Meanwhile, risk for adjacent segment degeneration, particularly following a fusion procedure performed with an interbody device, has been documented as high as 30%. Pressure ulcers can occur when spinal injuries are treated with rigid orthoses, especially in individuals who are immobile. Risk for pressure sores and decubiti is further elevated in patients who are obtunded and cannot communicate regarding pain levels and their need to mobilize. Hardware failure may occur following any instrumented spine procedure, but risk for this complication is elevated in the event of pseudarthrosis or in settings in which no fusion is performed.
In the recent work of Lee and associates, hardware failure was the only complication encountered among patients who were treated with percutaneous stabilization without fusion for thoracolumbar burst fractures. Similarly, iatrogenic neurologic injury may transpire in the setting of any spinal intervention (its incidence is rare). For example, in a large cohort of
more than 10000 patients undergoing surgical treatment for spondylolisthesis, acute neurologic injury was reported in only 0.8% of cases. Postsurgical wound infection, although relatively rare in cases of elective spine surgery, is common following large tumor resection such as sacrectomy performed for treatment of chordomas.
RECOMMENDED READINGS
Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. View Abstract at PubMed
Bransford RJ, Morgan RA. Thoracolumbar trauma. In: Schmidt AH, Teague DC, eds. Orthopaedic Knowledge Update: Trauma 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2010:373-385.
Lee JK, Jang JW, Kim TW, Kim TS, Kim SH, Moon SJ. Percutaneous short-segment pedicle screw placement without fusion in the treatment of thoracolumbar burst fractures: is it effective? comparative study with open short-segment pedicle screw fixation with posterolateral fusion. Acta Neurochir (Wien). 2013 Dec;155(12):2305-12; discussion 2312. doi: 10.1007/s00701-013-1859-x. Epub 2013 Sep 10. PubMed PMID: 24018981. View
Abstract at PubMed
Schoenfeld AJ, Carey PA, Cleveland AW 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: a prognostic study based on 5,887 patients. Spine J. 2013 Oct;13(10):1171-9. doi: 10.1016/j.spinee.2013.02.071. Epub 2013 Apr 9. PubMed PMID:
Question 84
Figure 38 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. To minimize additional trauma to the medial soft tissues, the elbow should be reduced in
Explanation
REFERENCES: O’Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 414.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 85
A 10-year-old boy reports heel pain with sporting activities. An examination demonstrates gastrocnemius contracture and tenderness at the calcaneal apophysis. Radiographs are unremarkable. What is the best next step?
Explanation
Sever disease, or calcaneal apophysitis, is best treated with activity modification that includes rest, restriction from sports and running, and Achilles tendon stretching exercises. The diagnosis is clinical (rendering MRI study unnecessary) and the course is usually self-limited, obviating the need for surgery. Occasionally, children with severe symptoms may benefit from a short period of cast or fracture brace immobilization.
RECOMMENDED READINGS
Sullivan RJ. Adolescent foot and ankle conditions. In: Pinzur MD, ED. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:47-55.
Feldman DS. Osteochondrosis. In: Spivak JM, Di Cesare PE, Feldman Ds, et al, eds. Orthopaedic: A Study Guide. New York, NY: McGraw-Hill; 1999:765-766.
Question 86
Figures 38a and 38b
Explanation
Inversion of the ankle can cause various injuries about the foot and ankle, all via the same mechanism. Fifth metatarsal base avulsion (Figure 35) fractures can be treated with use of a walking boot until pain subsides. Jones fractures (Figure 36) can be treated with surgical or nonsurgical treatment, although young, active patients are perhaps better treated with ORIF, which can decrease disability time. Treatment of an anterior process calcaneus fracture (Figure 37) is similar to that for a fifth metatarsal base avulsion fracture. Figures 38a and 38b show a calcaneal fracture-dislocation, which necessitates ORIF.
RECOMMENDED READINGS
Schepers T, Backes M, Schep NW, Carel Goslings J, Luitse JS. Functional outcome following a locked fracture-dislocation of the calcaneus. Int Orthop. 2013 Sep;37(9):1833-8. PubMed PMID: 23959223. View Abstract at PubMed
Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012 Oct;43(10):1626-32. doi: 10.1016/j.injury.2012.03.010. Epub 2012 Mar 30. Review. PubMed PMID: 22465516. View Abstract at PubMed
Roche AJ, Calder JD. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2013 Jun;21(6):1307-15. doi: 10.1007/s00167-012-2138-8. Epub 2012 Sep 6. Review. PubMed PMID: 22956165. View Abstract at PubMed
Berkowitz MJ, Kim DH. Process and tubercle fractures of the hindfoot. J Am Acad Orthop Surg. 2005 Dec;13(8):492-502. Review. PubMed PMID: 16330511. View Abstract at PubMed
Question 87
Which component is most common to both simple and complex elbow dislocations?

Explanation
Question 88
Which of the following clinical scenarios represents an appropriate indication for convex hemiepiphysiodesis/hemiarthrodesis in the treatment of a child with a congenital spinal deformity?
Explanation
REFERENCE: Winter RB, Lonstein JE, Denis F, Sta-Ana de la Rosa H: Convex growth arrest for progressive congenital scoliosis due to hemivertebrae. J Pediatr Orthop 1988;8:633-638.
Question 89
Which of the following findings best describes the effects of increasing conformity of a fixed tibial bearing component and femoral component in total knee arthroplasty?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 265-274.
Bartel DL, Rawlinson JJ, Burstein AH, Ranawat CS, Flynn WF Jr: Stresses in polyethylene components of contemporary total knee replacements. Clin Orthop 1995;317:76-82.
Question 90
The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced
Explanation
REFERENCES: Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036.
Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U: Operative versus nonoperative treatment of Achilles tendon rupture: A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-799.
Nistor L: Surgical and non-surgical treatment of Achilles tendon rupture. J Bone Joint Surg Am 1981;63:394-399.
Question 91
A 14-year-old patient has anterior knee pain. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 6a through 6e. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea & Febiger, 1989, vol 2, ch 18.
Question 92
A 35-year-old male sustains a closed tibial shaft fracture after falling from 12 feet. Which of the following measurements would be concerning for an evolving compartment syndrome?

Explanation
Given the poor outcomes associated with missed compartment syndromes, it is important to obtain both clinical and objective data when determining if a patient needs fasciotomies. Determining if a patient needs fasciotomies in the operating room while a patient is under anesthesia is complicated by the fact that obtaining a clinical exam is impossible, and that the diastolic blood pressure may be falsely decreased compared to normal pre- or postoperative measurements. Currently, it is recommended that intraoperative compartment pressures be compared to preoperative diastolic blood pressures, with delta p < 30 indicating the need for fasciotomies.
Kakar et al. review the preoperative, intraoperative, and postoperative diastolic blood pressure (DBP) in 242 patients with a tibia fracture treated operatively. They found the mean DBP was 18 points lower in the operating room compared to the preoperative measurement. In addition, they found the difference between preoperative and postoperative diastolic blood pressures to be within 2 points, indicating the decrease seen intraoperatively is likely a spurious value induced by anesthetic.
McQueen and Court-Brown prospectively review 116 patients with tibia fractures that had continuous monitoring of their anterior compartment for 24 hours. They found that using an absolute pressure of 30 mmHg would have resulted in 50 patients (43%) treated with unnecessary fasciotomies. They conclude using a differential pressure of
30 mmHg is a more reliable indicator of compartment syndrome.
Incorrect Answers:
Question 93
- When taken concomitantly with which of the following, erythromycin can cause an increase in the blood level of
Explanation
Question 94
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?
Explanation
REFERENCES: Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Eckman MH, Greenfield S, Mackey WC, et al: Foot infections in diabetic patients: Decision and cost-effectiveness analyses. JAMA 1995;273:712-720.
Question 95
Following a fall from a height of 5 feet, a patient reports pain along the lateral border of the foot. The CT scan shown in Figure 54 indicates what pathology?
Explanation
REFERENCE: Robbins MI, Wilson MG, Sella EJ: MR imaging of anterosuperior calcaneal process fractures. Am J Roentgenol 1999;172:475-479.
Question 96
Figures 20a and 20b show the radiographs of an obese 15-year-old boy who has severe left groin pain and is unable to bear weight following a minor injury. Treatment should consist of
Explanation
REFERENCES: Aronson DD, Loder RT: Treatment of the unstable (acute) slipped capital femoral epiphysis. Clin Orthop 1996;322:99-110.
Karol LA, Doane RM, Cornicelli SF, Zak PA, Haut RC, Manoli A II: Single versus double screw fixation for treatment of slipped capital femoral epiphysis: A biomechanical analysis. J Pediatr Orthop 1992;12:741-745.
Stanitski CL: Acute slipped capital femoral epiphysis: Treatment alternatives. J Am Acad Orthop Surg 1994;2:96-106.
Question 97
Regarding the role of the orthopaedic surgeon in addressing domestic and family violence, all of the following statements are true EXCEPT:

Explanation
state. The AAOS Advisory statement gives information to assist in meeting the ethical and legal obligations on Domestic and Family Violence and Abuse.
Domestic and family violence affects over 10% of the US population (approximately 32 million Americans). Child abuse and neglect contributed to 1,400 fatalities in 2002 and there was 565,747 reports of suspected elder abuse.
Reporting of suspected child abuse is required in all states. The orthopaedic surgeon should hospitalize elderly victims who are in immediate danger and help develop a plan to insure their safety.
Question 98
A 27-year-old man has had pain in the right index finger for the past 9 months. The pain is completely relieved with ibuprofen. An AP radiograph and CT scan are shown in Figures 80a and 80b. What is the most likely diagnosis?
Explanation
radiolucent nidus. A small area of calcification may be present within the center of the nidus. The radiolucent nidus is surrounded by a thick rim of sclerotic bone. These diagnostic
features are frequently better seen on CT. An increase in cyclooxygenase activity has been demonstrated within osteoid osteomas, which may explain why aspirin and other nonsteroidal anti-inflammatory drugs classically relieve the pain associated with these lesions.
REFERENCES: Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 121-130.
Question 99
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.
Question 100
A 27-year-old man has recurrent right shoulder instability. He first dislocated his shoulder in college while playing rugby and was treated nonsurgically. Since then, he has sustained nearly 1 dozen dislocations and says that his shoulder always feels “loose.” The shoulder recently dislocated in his sleep and while he was putting on clothes. Which factor is a contraindication to an arthroscopic soft-tissue repair?
Explanation
There is much debate in the literature regarding optimal techniques for treatment of shoulder instability. Although some studies suggest that open stabilization may result in lower recurrence rates in contact athletes, this approach is now under scrutiny. Extensive labral involvement (posterior labral involvement in this scenario) is likely more accessible via arthroscopic methods. Although HAGL lesions may be more easily accessible via an open approach (particularly for inexperienced arthroscopists), numerous authors describe successful repair via arthroscopic techniques. Among these responses, the strongest indication for an open approach, including possible bony transfer, is high-grade glenoid bone loss. Although the critical amount of bone loss is a topic of debate, most surgeons and authors suggest a cutoff of 20% to 25%.

CLINICAL SITUATION FOR QUESTIONS 90 THROUGH 92
Figure 90 is the radiograph of a 14-year-old pitcher who plays in a year-round baseball program and has vague pain in his dominant shoulder. The pain occurs with throwing, and it has been worsening for 2 months. Pain typically occurs during the late cocking phase of throwing. He has no tenderness of the rotator cuff and 5/5 rotator cuff strength. His arc of motion is symmetric between his dominant and nondominant arms. The sulcus sign is negative.
