Orthopedic Board Review MCQs: Spine, Fracture & Ligament | Part 257

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Orthopedic Board Review MCQs: Spine, Fracture & Ligament | Part 257
!
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What root is most commonly involved with a segmental root level palsy after laminoplasty?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-249.
Uematsu Y, Tokuhashi Y, Matsuzaki H: Radiculopathy after laminoplasty of the cervical spine. Spine 1998;23:2057-2062.
Question 2
Initial postoperative management after repair of an acute rotator cuff tear includes
Explanation
REFERENCES: Iannotti JP: Full-thickness rotator cuff tear: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Bigliani LU, Cordasco FA, McIlveen ST, et al: Operative repair of massive rotator cuff tears: Long-term result. J Shoulder Elbow Surg 1992;1:120-130.
Question 3
A patient with myelopathy underwent a one-level corpectomy 1 day ago and is now home. In the middle of the night he calls to report markedly increased difficulty in swallowing, diaphoresis, a change in his voice, and difficulty lying flat. What is the best course of action?
Explanation
REFERENCES: Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multilevel cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
McAfee PC, Bohlman HH, Riley LH Jr, Robinson RA, Southwick WO, Nachlas NE: The anterior retropharyngeal approach to the upper part of the cervical spine. J Bone Joint Surg Am 1987;69:1371-1383.
Question 4
Figure 12 shows an arthroscopic view from an inferolateral portal of a right knee. The asterisk indicates which structure?

Explanation
The asterisk indicates the anteromedial bundle of the anterior cruciate ligament. The anterior cruciate ligament consists of 2 functional bundles: anteromedial and posterolateral. During extension of the knee, the posterolateral bundle becomes taut. In flexion, the anteromedial bundle is tight and the posterolateral bundle relaxes. Recently, techniques for double-bundle reconstruction have been described to recreate the normal anatomic relationship of the 2 bundles.
RECOMMENDED READINGS
Chhabra A, Zelle BA, Feng MT, Fu FH. The arthroscopic appearance of a normal anterior cruciate ligament in a posterior cruciate ligament-deficient knee: the posterolateral bundle (PLB) sign. Arthroscopy. 2005 Oct;21(10):1267. PubMed PMID: 16226658. View Abstract at PubMed
Cha PS, Brucker PU, West RV, Zelle BA, Yagi M, Kurosaka M, Fu FH. Arthroscopic double-bundle anterior cruciate ligament reconstruction: an anatomic approach. Arthroscopy. 2005 Oct;21(10):1275. PubMed PMID: 16226666. View Abstract at
PubMed
Question 5
A patient with Pott's disease, tuberculosis of the spine, is more likely to have which of the following early findings? Review Topic
Explanation
Question 6
Which structure is indicated by the arrow in Figure 33?

Explanation
The posterior position of the sciatic nerve in relation to the acetabulum and the lateral peroneal division makes the peroneal division of the sciatic nerve the portion of the nerve that is most likely to be injured in a posterior traumatic hip dislocation, accounting for up to 10% of concomitant nerve injuries with posterior hip dislocation. The corona mortis is an anatomic variant that results in vascular anastomosis between the obturator and either the external iliac or inferior epigastric arteries. This variant occurs in approximately 80% of patients and varies in its position, being located 4 cm to 9 cm lateral to the symphysis pubis. The obturator vascular bundle is situated in the fat medial to the obturator internus muscle and must be mobilized to access the quadrilateral plate. Dissection may be carried out both above and below this vascular leash. The Kocher-Langenbeck approach is indicated for fractures involving the posterior wall and/or posterior column of the acetabulum and for both column fractures that require direct posterior visualization. This approach is not indicated for direct reduction of the anterior wall or column when direct visualization is required anteriorly. The L5 nerve root is located on the anterior sacrum and is indicated by the arrow.
The position of this neural structure must be considered whether the surgeon is stabilizing 31 the sacroiliac (SI) joint with percutaneous iliosacral screws or with anterior SI plating through the lateral window of the ilioinguinal approach.
RECOMMENDED READINGS
Cornwall R, Radomisli TE. Nerve injury in traumatic dislocation of the hip. Clin Orthop Relat Res. 2000 Aug;(377):84-91. Review. PubMed PMID: 10943188. View Abstract at PubMed
Darmanis S, Lewis A, Mansoor A, Bircher M. Corona mortis: an anatomical study with clinical implications in approaches to the pelvis and acetabulum. Clin Anat. 2007 May;20(4):433-9. PubMed PMID: 16944498. View Abstract at PubMed
Archdeacon MT, Kazemi N, Guy P, Sagi HC. The modified Stoppa approach for acetabular fracture. J Am Acad Orthop Surg. 2011 Mar;19(3):170-5. PubMed PMID: 21368098. View Abstract at PubMed
Rommens P. The Kocher-Langenbeck approach for the treatment of acetabular fractures. Operat Orthop Traumatol 2004; 16:59-74.
Langford JR, Burgess AR, Liporace FA, Haidukewych GJ. Pelvic fractures: part 2. Contemporary indications and techniques for definitive surgical management. J Am Acad Orthop Surg. 2013 Aug;21(8):458-68. doi: 10.5435/JAAOS-21-08-458. Review. PubMed PMID: 23908252.View Abstract at PubMed
Question 7
A year-old woman who underwent total knee replacement 18 months ago has had 3 weeks of moderate drainage from a previously healed wound. What is the most appropriate treatment?
Explanation
This situation represents a definitively and chronically infected knee replacement. Antibiotic therapy alone might suppress the infection but would not eradicate it. Debridement and polyethylene exchange would be appropriate treatment for an early postoperative infection. The treatment of choice is to perform a two-stage debridement and reconstruction. Although not among the listed choices, an aspiration or culture could be done presurgically and might help clinicians identify the best antibiotics to treat the condition. Antibiotic selection would not affect the need for the two-stage reconstruction, however.
Question 8
For a patient with an unstable pelvic fracture, the amount of blood tranfusions required in the first 24 hours has shown to be most predictive for what variable?

Explanation
According to the referenced study by Smith et al, fracture pattern and angiography/embolization were not predictive of mortality in patients with unstable pelvic injuries. The three factors they found to be predictive were: increased blood transfusions in the first 24 hours, age >60 years, and increased ISS or RTS scores. Deaths were most commonly from exsanguination (<24 hours) or multiorgan failure (>24 hours).
Incorrect Answers: Choices 1-4 are not as predictive of mortality as choice 5.
Question 9
A 43-year-old man sustained a closed, intra-articular pilon fracture. It has now been 1 year since he underwent open reduction and internal fixation. Which of the following statements most accurately describes his perceived outcome? Review Topic
Explanation
Question 10
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management? L Intensive physiotherapy
Explanation
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Question 11
Which of the following is accurate regarding low-molecular-weight heparin used for deep venous thrombosis (DVT) prophylaxis in total joint arthroplasty?
Explanation
to 18 hours. This is greater than the 1 hour half-life of unfractionated heparin.
Low-molecular-weight heparin offers an advantage over unfractionated heparin by selectively targeting Factor Xa while having a lesser effect on circulating thrombin (Factor IIa). Circulating thrombin Factor IIa is needed for local hemostasis at the site of the surgical wound. Clinical studies have shown a reduction by one third in the incidence of thrombocytopenia with the use of low-molecular-weight heparin. Low-molecular-weight heparin has been shown to demonstrate similar clinical results compared to warfarin with respect to preventing thromboembolic disease after total hip arthroplasty and complications such as bleeding.
REFERENCES: Zimlich RH, Fulbright BM, Friedman RJ: Current status of anticoagulation therapy after total hip and total knee arthroplasty. J Am Acad Orthop Surg 1996;4:54-62.
Colwell CW Jr, Spiro TE, Trowbridge AA, et al: Use of enoxaparin, a low-molecular-weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14.
Torholm C, Broeng L, Jorgensen PS, et al: Thromboprophylaxis by low-molecular-weight heparin in elective hip surgery: A placebo controlled study. J Bone Joint Surg Br 1991;73:434-438.
Question 12
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?
Explanation
REFERENCES: Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 428-429.
Question 13
In the treatment of rheumatoid arthritis, which medication is an antagonist of tumor necrosis factor-alpha?
Explanation
TNF-alpha is considered to be one of the major cytokines involved in rheumatoid arthritis pathology. As a result, many biologic agents used to treat rheumatoid arthritis (RA) are manufactured to block TNF-alpha or its receptors. This has been shown to reduce inflammation and stop disease progression. In the USA, Etanercept is approved to treat rheumatoid arthritis, juvenile rheumatoid arthritis and psoriatic arthritis, plaque psoriasis and ankylosing spondylitis. The route of administration is subcutaneous.
Bongartz et al. used a randomized control trial to asses the risk of infection and malignancy rates in RA treated with TNF-alpha antagonist. Overall, patients with RA appear to have an approximately 2-fold increased risk of serious infection compared to the general population and non-RA controls, irrespective of TNF-alpha antagonist use. The pooled odds ratio for malignancy was 3.3 (95% confidence interval [CI], 1.2-
Question 14
A 47-year-old woman underwent a bunionectomy and hallux valgus correction a few years ago. She now has the complication shown in Figures 38a and 38b. She has no pain with motion of the metatarsophalangeal or interphalangeal joints. What is the best reconstructive option in this setting?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 27-32.
Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby, 2007, pp 345-351.
Question 15
The modified Judet approach to the posterior scapula exploits the internervous interval between what two muscles?

Explanation
The reference by Obremskey et al argues the approach "combines several important goals including: 1) exposure of all bony elements of the scapula which have adequate bone stock for internal fixation; 2) minimal trauma to the rotator cuff musculature; and 3) protection of the major neurologic structures (suprascapular nerve superiorly and axillary nerve laterally)." They believe "the main advantage of the exposure is limiting muscular dissection, which can potentially improve rehabilitation and limit morbidity of the operation."
Question 16
Which of the following best describes the resultant forces on an increased offset stem when compared with a standard offset stem?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Hurwitz DE, Andriaacchi TP: Biomechanics of the hip, in Callaghan J, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven , 1998.
Pauwels F: Biomechanics of the Normal and Diseased Hip. New York, NY, Springer-Verlag, 1976.
Question 17
A 19-year-old rugby player has severe knee pain after being injured in a game 2 weeks ago. Examination reveals a knee effusion, limited motion, and increased 3+ Lachman’s test and anterior drawer. There is also increased external rotation at 30 degrees of knee flexion when the patient is placed in the prone position. Based on these findings, which of the following actions would most likely increase the risk of anterior cruciate ligament (ACL) reconstruction failure?
Explanation
REFERENCES: Veltri DM, Warren RF: Posterolateral instability of the knee. J Bone Joint Surg Am 1994;76:460-472.
Covey DC: Injuries of the posterolateral corner of the knee. J Bone Joint Surg Am
2001;83:106-118.
Question 18
4A 4B 4C A 30-year-old man was involved in a high-speed motorcycle collision and sustained the injury shown in Figure 4a. Hypotension ensued shortly after arrival in the emergency department. Figure 4b is the initial contrast pelvic CT image with an unrecognized blush consistent with arterial bleeding. During surgical repair, the patient was noted to have active bleeding and an angiogram was obtained (Figure 4c). Which structure is the likely cause of his bleeding?
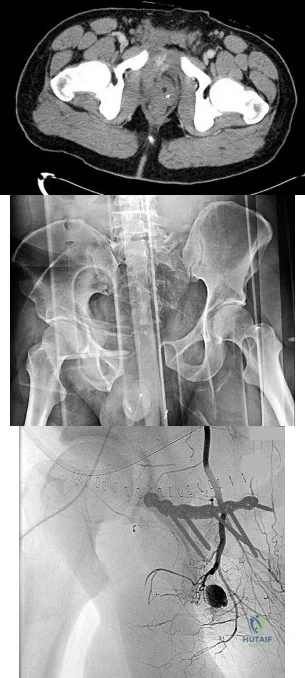
Explanation
Pelvic bleeding occurs predominantly from disruption of the posterior venous plexus and bleeding from the fractured bone. Occasionally arterial bleeding is seen, with injury to the superior gluteal artery most common. Anterior pelvic bleeding occurs from injury to the obturator artery (commonly from a pubic bone fracture laceration) and less frequently from the pudendal artery near the symphysis. The location of the bleeding on CT and angiography images does not correspond to the superior gluteal, external iliac, or femoral arteries.
RECOMMENDED READINGS
Suzuki T, Smith WR, Moore EE. Pelvic packing or angiography: competitive or complementary? Injury. 2009 Apr;40(4):343-53. Epub 2009 Mar 17. Review.PubMed PMID: 19278678. View Abstract at PubMed
Loffroy R, Yeguiayan JM, Guiu B, Cercueil JP, Krausé D. Stable fracture of the pubic rami: a rare cause of life-threatening bleeding from the inferior epigastric artery managed with transcatheter embolization. CJEM. 2008 Jul;10(4):392-5. PubMed PMID: 18652733. View Abstract at PubMed
White CE, Hsu JR, Holcomb JB. Haemodynamically unstable pelvic fractures.Injury. 2009 Oct;40(10):1023-30. Epub 2009 Apr 16. Review. PubMed PMID:19371871. View Abstract at PubMed
RESPONSES FOR QUESTIONS 5 THROUGH 8

5A

5B
- Avascular necrosis, head collapse, and screw penetration
- Fixation failure and varus collapse
- Humeral stem loosening
- Glenoid component loosening
- Hardware failure (breakage of plate or screws)
- Shoulder dislocation
Please choose from the responses to identify the most likely complication in each scenario.
Question 19
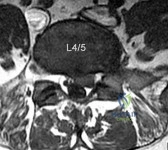
A 32-year-old male presents with left leg pain and weakness. An axial image from his MRI is shown in Figure A. Which of the following physical exam findings would be most consistent with this MRI finding. Review Topic
Explanation
radiculopathy.
While nerve root innervation shows some variability by patient, L5 is "characteristically" responsible for the sensation to the dorsal aspect of the foot, ankle dorsiflexion (tibialis anterior - along with L4), great toe extension (EHL), and hip abduction (gluteus medius).
Suri et al. reported on specific physical exam findings that significantly increased the likelihood of nerve root impingement at specific lumbar levels. They found: L2 was associated with decreased anterior thigh sensation. L3 was associated with a positive femoral stretch test. L4 was associated with a blunted patellar reflex, decreased medial ankle sensation or a positive crossed femoral stretch test. L5 was associated with was associated with decreased hip abductor strength.
Luri et al. reported 8-year follow up on the patients in the spine patient outcomes research trial who underwent surgical vs. conservative care for treatment of lumbar herniated disc. They found that patients who underwent surgical treatment had superior results that were maintained at 8 years compared to patients who underwent conservative management.
Figure A is an axial MRI at the L4/5 disc space that shows a left paracentral disc herniation compressing the descending L5 nerve root. Illustration A identifies the structures in the MRI image. Illustration B demonstrates the dermatome, reflex and motor function associated with the L4, L5 and S1 nerve root.
Incorrect Answers:
(SBQ13PE.102) An 26-year-old male presents to your office complaining of bilateral hip and low back pain. On physical examination, he has 10 degree bilateral hip flexion contractures. An AP pelvis radiograph is demonstrated in figure A. Which of the following findings is consistent with this patient's presentation? Review Topic

A positive flexion, adduction, internal rotation (FADDIR) test
A history of untreated slipped capital femoral epiphysis (SCFE)
A thrombophilia
Normal serum ESR and CRP
Positive Human Leukocyte Antigen B27 (HLA-B27)
The patient has large joint arthralgia and sacroiliac joint sclerosis on AP pelvis radiograph, which is consistent with ankylosing spondylitis. Patients with ankylosing spondylitis have positive Human Leukocyte Antigen B27 (HLA-B27).
Ankylosing spondylitis (AS) is a seronegative spondyloarthropathy that affects the axial skeleton as well as large joints including the hips and knees. The most common initial site of pain is the sacroiliac (SI) joint, and is demonstrated as sacroiliitis on pelvic radiograph. Hip involvement is common, and typically manifests as hip pain and flexion contracture. Serologic studies will be typically be negative for rheumatoid factor, but positive for HLA-B27 in 90% of patients.
Kubiak et. al. review orthopaedic management of AS. Common orthopaedic manifestations include SI joint pain, hip flexion contractures, and stiffness of the cervical and lumbar spine. They report that laboratory analysis of patients with active disease will typically demonstrate mild elevation of ESR, CRP, and WBC. Patients with chronic AS may demonstrate a normocytic anemia. If HLA-B27 is negative, a high clinical suspicion should still be maintained.
Gensler et al. review the different clinical conditions that compose of juvenile-onset spondyloarthritis. They report on the different spondyloarthritides includes ankylosing spondylitis, reactive arthritis, arthropathy associated with inflammatory bowel disease, and that associated with psoriasis. They emphasize that the appearance of sacroiliac joint and spinal disease in the form of ankylosing spondylitis usually takes 5–10 years after initial symptom presentation, and therefore, a definite diagnosis can take several years leading to a delay in diagnosis.
Figure A is an AP pelvis radiograph of a skeletally mature individual demonstrating sclerosis of the SI joint indicative of sacroiliitis. Illustration A shows a axial CT image of the patient in the stem. Sclerosis and bone erosion can be seen in the sacroiliac joint.
Incorrect Answers:
osteonecrosis Answer 3: A infarctions,
of
the
femoral
epiphysis.
thrombophilia may have
osseous manifestations such as bone
which
are
not
evident
on
this
image.
Question 20
Which of the following statements best describes the anatomic considerations of the popliteal artery posterior to the knee joint?
Explanation
90 degrees of flexion.
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 151.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-53.
Question 21
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured?
Explanation
REFERENCES: Schenck CD: Anatomy of the innervation of the upper extremity, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby-Year Book, 1991.
Hershman EB: Brachial plexus injuries. Clin Sports Med 1990;9:311-329.
Question 22
A healthy, active collegiate soccer player returns to your office approximately 10 months after returning to full play and 18 months after undergoing ACL reconstruction with bone-patellar tendon-bone (BTB) autograft. The patient reports landing awkwardly after a jumping for a ball and felt his knee give way. He presents with pain, worse with weight bearing. On physical exam, there is a mild effusion and a grade 2B Lachman. Radiographs are shown in Figure A. What is the likely underlying cause of his current diagnosis? Review Topic

Explanation
Ideal tunnel placement on the femoral side should be at the approximately 2 o'clock (for a left knee) or 10 o'clock (for a right knee) position on the lateral wall, which facilitates a more horizontal, anatomic graft. On the tibial side, the tunnel trajectory in the coronal plane should be about 60-75 degrees from the horizontal and the tunnel entrance should be approximately 10-11mm from the anterior border of the PCL.
Noyes et al. emphasize the importance of anatomic reconstruction. They recommended against using a transtibial tunnel to make the femoral tunnel because it will result in a vertical orientation. The authors summarized and recommended the use of individual drilling of each tunnel, and using a anteromedial portal to obtain the ideal femoral tunnel.
Driscoll et al. compared the rotational properties of a BTB graft placed centrally in the tibial footprint in both groups, but on the femoral side, placed in the anteromedial aspect versus central portion of the ACL femoral origin. They noted a significantly stronger resistance to rotational failure when placed centrally. Thus, noting the importance of placing the graft anatomically, within the central areas of both the tibial footprint and femoral origin.
Figure A exhibits malpositioned tunnels, both of which are too vertical. Illustration A exhibits well-placed tunnels, with the horizontality exhibited on the femoral side and approximately 75 degrees from the horizontal on the tibial side.
Incorrect answers:
Question 23
A 58-year-old woman who underwent a successful total hip replacement for degenerative arthritis 8 years ago reports groin pain for the past 6 months. A radiograph of the hip is shown in Figure 32. At revision, severe deficiency of the posterior column is noted. What reconstructive option would be most appropriate for the acetabulum?
Explanation
REFERENCES: Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Berry DJ, Muller ME: Revision arthroplasty using an anti-protrusio cage for massive acetabular bone deficiency. J Bone Joint Surg Br 1992;74:711-715.
Question 24
A patient reports pain in the hip with functional positioning. With the patient supine, pain in which of the following positions would be typical for femoral acetabular impingement? Review Topic
Explanation
(SBQ13PE.10) Which statement is true regarding discoid menisci? Review Topic
Most commonly involves the medial meniscus
Bilateral in >75% of cases
Asymptomatic discoid meniscus should undergo saucerization
Radiographs will commonly show a hyperplastic lateral intercondylar spine
Radiographs will commonly show squaring of affected condyle with cupping of tibial plateau
Radiographs of knees with discoid menisci will commonly show squaring of affected condyle (lateral>medial) with cupping of tibial plateau.
Discoid meniscus refers to the abnormal development of a hypertrophic and discoid shaped meniscus. It occurs in 3-5% of the population and it is considered the most common cause of a symptomatic clicking or clunking in a childs knee. The lateral meniscus is most commonly affected and it will occur bilaterally in 25% of affected
people. The Watanabe Classification describes the 3 types of discoid menisci. Type 1
= Incomplete, Type 2 = Complete, Type 3 = Wrisberg (lack of posterior meniscotibial attachment to tibia)
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Lee et al. retrospectively reviewed 36 patients aged less than 15 years who underwent arthroscopic procedures for torn discoid menisci. The mean patient age at the time of surgery was 9.5 years. They showed that partial meniscectomy yielded better radiologic results than subtotal/total meniscectomy for torn discoid menisci in this population.
Illustration A shows the 3 classifications of discoid menisus as originally described by Watanabe. Type 4 is a ring type discoid that was not originally described by Watanabe in his 1978 paper. Illustration B shows an AP and lateral radiograph of a discoid meniscus knee. Note squaring of affected lateral condyle in the presence of a lateral discoid meniscus. Illustration C shows 4 consecutive sagittal MRI images with meniscus continuity. It is important to note that the diagnosis of discoid menisci can be made when 3 or more 5mm sagittal images show meniscal continuity.
Incorrect Answers:
Question 25
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
Explanation
REFERENCES: Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.
Question 26
Figure 6 shows the lateral radiograph of a 22-year-old woman who has painful Scheuermanns’s kyphosis in the middle and lower thoracic spine. When planning surgical correction using instrumentation, the distal aspect of the instrumentation should ideally extend to the
Explanation
REFERENCES: Lowe TG: Scheuermann’s disease. Orthop Clin North Am 1999;30:475-487.
Lenke LG: Kyphosis of the thoracic and thoracolumbar spine in the pediatric patients: Prevention and treatment of surgical complications. Instr Course Lect 2004;53:501-510.
Question 27
Which of the following imaging modalities is most accurate in locating a toothpick in the plantar arch of the foot?
Explanation
REFERENCES: Mizel MS, Steinmetz ND, Trepman E: Detection of wooden foreign bodies in muscle tissue: Experimental comparison of computed tomography, magnetic resonance imaging, and ultrasonography. Foot Ankle Int 1994;15:437-443.
Jacobson JA, Powell A, Craig JG, et al: Wooden foreign bodies in soft tissue: Detection at US. Radiology 1998;206:45-48.
Question 28
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?
Explanation
REFERENCES: Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809.
Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Pape HC, Auf’m’Kolk M, Puffrath T, et al: Primary intramedullary femur fixation in multiple trauma patients with associated lung contusion: A cause of posttraumatic ARDS? J Trauma 1993;34:540-548.
Question 29
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?
Explanation
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Ciccotti MG, Jobe FW: Medial collateral ligament instability and ulnar neuritis in the athlete’s elbow. Instr Course Lect 1999;48:383-391.
Question 30
In the treatment of acetabular dysplasia, what type of pelvic osteotomy leaves the “teardrop” in its original position and redirects the acetabulum?
Explanation
REFERENCES: Lack W, Windhager R, Kutschera HP, Engel A: Chiari pelvic osteotomy for osteoarthritis secondary to hip dysplasia: Indications and long-term results. J Bone Joint Surg Br 1991;73:229-234.
Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Ninomija S, Tagwa H: Rotational acetabular osteotomy for the dysplastic hip. J Bone Joint Surg Am 1984;66:430.
Question 31
A young male patient underwent intramedullary nail fixation for a diaphyseal femur fracture. A post-operative CT scanogram is performed to assess rotational alignment between the surgical and non-surgical femur. Which of the following measurement(s) are considered acceptable differences in regards to femoral rotational malreduction after intramedullary nail fixation as compared to the uninjured femur?
Explanation
The maximum acceptable difference in rotational malreduction between the surgical and contralateral legs for femoral version is 15°. Therefore, answers 1 and 2 are correct.
Normal femoral neck anteversion is approximately 11-13°, with a normal range between 5-20°. The variation within the same patients can also be up to 15° difference between limbs. Current literature has shown that this 15° difference is well tolerated by patients, including when this has occured as a result of rotational malreduction following intramedullary nail fixation for a diaphyseal femur fracture.
Ayalon et al. aimed to compare the difference in femoral version (DFV) after intramedullary nailing performed by a trauma-trained and non-trauma trained surgeon. The mean post-operative DFV was 8.7° in these patients, compared to 10.7° in those treated by surgeons of other subspecialties. Post-operative version or percentage of DFV >15° did not significantly differ between these two groups.
Omar et al. studied the utility of pre-operative 'virtual reduction' of bilateral femoral fractures that were initially stabilized with external fixation. After external fixation, the mean rotational difference between both legs was 15.0°
± 10.2°. Following virtual reduction, the mean rotational difference between both legs was 2.1° ± 1.2°, after intramedullary nailing, compared to 6.1° ±
Question 32
Figure 16a shows the radiograph of a 34-year-old woman who sustained a basicervical fracture of the femoral neck. The fracture was treated with a compression screw and side plate. Seven months postoperatively, she continues to have significant hip pain and cannot bear full weight on her hip. A recent radiograph is shown in Figure 16b. Management should now consist of
Explanation
REFERENCES: Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Ballmer FT, Ballmer PM, Baumgaertel F, et al: Pauwels osteotomy for nonunions of the femoral neck. Orthop Clin North Am 1990;21:759-767.
Question 33
The MRI scans and diagnostic ultrasound shown in Figures 2a through 2c show what pathologic condition? Review Topic
Explanation
Question 34
Which of the following patients is more likely to have an overall poorer outcome following a lower extremity amputation?
Explanation
Question 35
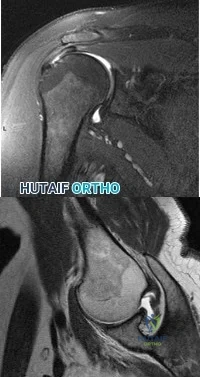
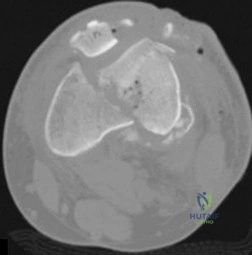
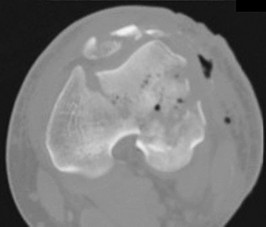
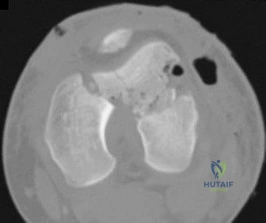
This image represents the end stage of an uncompensated rotator cuff tear.
Explanation
Axillary lateral and anteroposterior (AP) images of the right shoulder (Figures 59c and 59d) reveal osteoarthrosis of the glenohumeral joint, which typically is not associated with significant rotator cuff pathology. An examination often shows limitations in range of motion, crepitance, and pain with motion. An AP radiographic image of the right shoulder (Figure 59b) reveals proximal humeral migration, which normally correlates with rotator cuff tear size. Tears extending into the infraspinatus tendon are associated with more humeral migration than is seen with isolated supraspinatus tears. Presenting complaints are usually of pain and weakness. Examination findings include subacromial crepitance and weakness during rotator cuff testing. Rarely, this may be associated with pseudoparalysis in large uncompensated rotator cuff tears. The CT image of the right shoulder (Figure 59a) shows superior migration of the humerus with respect to the glenoid surface and end-stage
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. View Abstract at PubMed
Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
Question 36
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?
Explanation
REFERENCES: Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby Year Book, 1995, pp 165-201.
Question 37
A 30-year-old man who sustained a work-related injury 6 weeks ago reports persistent back and left-sided buttock pain that has been attributed to lumbar transverse process fractures. A pelvic radiograph and CT scans obtained 2 days ago are seen in Figures 17a through 17c. What is the best treatment for his injury?
Explanation
REFERENCES: Mears DC: Management of pelvic pseudarthroses and pelvic malunion. Orthopade 1996;25:441-448.
Matta JM, Dickson KF, Markovich GD: Surgical treatment of pelvic nonunions and malunions. Clin Orthop Relat Res 1996;329:199-206.
McLaren AC, Rorabeck CH, Halpenny J: Long-term pain and disability in relation to residual deformity after displaced pelvic ring fractures. Can J Surg 1990;33:492-494.
Question 38
Figure 1 points to the "tear drop" of the wrist. This radiographic landmark represents which anatomic portion of the wrist?

Explanation
Question 39
Internal impingement of the shoulder and posterosuperior labral pathology in throwers has been most clearly associated with which of the following? Review Topic
Explanation
Coracoacromial arch stenosis is associated with subacromial impingement and unrelated to internal impingement. Bennett's lesion refers to exostosis or calcification at the posterior capsule and while potentially associated with overhead throwing athletes who may have internal impingement, a causal link between the two has not been established and therefore posterior capsular contracture is the preferred response.
Question 40
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in
Explanation
REFERENCES: Shelton WR, Barrett GR, Dukes A: Early season anterior cruciate ligament tears: A treatment dilemma. Am J Sports Med 1997;25:656-658.
Snyder-Mackler L, Fitzgerald GK, Bartolozzi AR III, Ciccotti MG: The relationship between passive joint laxity and functional outcome after anterior cruciate ligament injury. Am J Sports Med 1997;25:191-195.
Question 41
Figure 52 shows the MRI scan of a 28-year-old baseball pitcher. Examination will most likely reveal which of the following findings?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi V: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7:223-227.
Question 42
Epithelioid sarcoma most commonly occurs in which of the following anatomic locations?
Explanation
REFERENCES: Gupta TD, Chaudhuri P (eds): Tumors of the Soft Tissues, ed 2. Stamford, CT, Appleton and Lange, 1998, p 475.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby-Year Book, 1995, p 1074.
Question 43
What structure (arrow) is shown in Figure 24?
Explanation
REFERENCES: Onibokun A, Khoo LT, Holly L: Anterior retroperitoneal approach to the lumbar spine, in Kim DH, Henn JS, Vaccaro AR, et al (eds): Surgical Anatomy and Techniques to the Spine. Philadelphia, PA, Saunders Elsevier, 2006, pp 101-105.
Netter GH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy Corporation, 1989.
Question 44
A 71-year-old woman who reports long-term use of oral steroids for asthma is referred for treatment of a distal humerus fracture. Radiographs reveal diffuse osteopenia and a severely comminuted intra-articular fracture. What is the most appropriate treatment?
Explanation
REFERENCES: Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.
Garcia JA, Mykula R, Stanley D: Complex fractures of the distal humerus in the elderly: The role of total elbow replacement as primary treatment. J Bone Joint Surg Br 2002;84:812-816.
Question 45
A 74-year-old man with ankylosing spondylitis falls off a step stool and now has a minimally displaced T10-T11 extension-type fracture. He is initially treated with percutaneous pedicle screw fixation from T8-L1 and has good pain relief. The next day, however, he experiences increased back pain and loss of strength in his lower extremities.
Explanation
Cauda equina syndrome, typically the result of severe central canal stenosis in the lower lumbar region, often is caused by a large central disk herniation. Symptoms include severe back or leg pain, perineal numbness, possible motor weakness, and initial urinary retention followed by an overflow incontinence. When bowel or bladder deficits are present, this is considered a surgical emergency because successful recovery is most likely if decompression occurs within the first 48 hours.
Ankylosing spondylitis can lead to progressive autofusion of the vertebrae and significant limitation in motion. Any sudden improvement in motion should be considered a fracture until proven otherwise. These fractures are commonly missed when using plain radiographs or even CT scan because minimal or no displacement often is noted. MR imaging can be useful to identify edema at
the fracture site. These fractures are typically very unstable and necessitate surgery to avoid displacement and potential neurologic injury.
Some fractures associated with ankylosing spondylitis can be effectively treated with percutaneous pedicle screw fixation. However, because of the highly vascular nature of some of these fractures, they pose risk for an epidural hematoma, potential neurologic deficit, and emergent decompression.
RECOMMENDED READINGS
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. Spine J. 2014 Feb 1;14(2):326-30. doi: 10.1016/j.spinee.2013.10.046. Epub 2013 Nov 12. PubMed PMID: 24231778. View Abstract at PubMed
Mathews M, Bolesta MJ. Treatment of spinal fractures in ankylosing spondylitis. Orthopedics. 2013 Sep;36(9):e1203-8. doi: 10.3928/01477447-20130821-25. PubMed PMID: 24025014.
View Abstract at PubMed
McCarthy MJ, Aylott CE, Grevitt MP, Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976). 2007 Jan 15;32(2):207-
Question 46
Which of the following choices best describes the fracture pattern shown in Figures 2a through 2c?
Explanation
REFERENCES: Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Matta J: Surgical treatment of acetabular fractures, in Browner BD, Jupiter JB, Levine AM, et al (eds): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, vol 1, pp 1009-1149.
Question 47
-An athletic 30-year-old sustained multiple injuries in a high-speed motor vehicle collision that resulted in a loss of approximately 30% of blood volume. On arrival to the emergency department, the heart rate is100 and blood pressure is 104/62. The best means with which to evaluate true hemodynamic status is
Explanation
Question 48
-If a physician elects to shorten a femur by 4 cm for traumatic bone loss treatment and places an intramedullary nail for fixation, which deformity will be created in the lower extremity?
Explanation

Question 49
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
Explanation
REFERENCES: Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337.
Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271.
Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Sneppen O, Fruensgaard S, Johannsen HV, Olsen BS, Sojbjerg JO, Anderson NH: Total shoulder replacement in rheumatoid arthritis: Proximal migration and loosening. J Shoulder Elbow Surg 1996;5:47-52.
Question 50
A 36-year-old man was injured in a motorcycle collision and sustained the injury shown in Figure 70. He has a blood pressure (BP) of 70/40 mm Hg, pulse of 148 beats per minute (bpm), and Glasgow Coma Scale score of 6 (scores lower than 8 indicate severe brain injury), and there is negligible urine output. His airway is secure and intravenous (IV) access is obtained. Two liters of warm crystalloid solution are given; repeated vital signs reveal the same BP and a pulse of 142 bpm. What is the best next step?

Explanation
This patient has an anteroposterior compression pelvic fracture associated with shock. In patients with closed pelvic fractures and hypotension, mortality rises to approximately 1 in 4 (10%-42%) and hemorrhage is the major reversible contributing factor. Initial management of a major pelvic disruption associated with hemorrhage requires hemorrhage control and rapid fluid resuscitation. A pelvic binder should be placed to reduce pelvic volume. The patient has signs and symptoms of class IV hemorrhage, which include marked tachycardia exceeding 140, a significant decrease in BP, and a very narrow pulse pressure. Urinary output is negligible, and mental status is markedly depressed. The skin is cold and pale. The degree of exsanguination with class IV hemorrhage is immediately life threatening, and rapid transfusion and immediate surgical intervention are necessary. Nonresponse to fluid administration indicates persistent blood loss. Blood preparation should be emergency blood release. Type and cross-match of blood can be used for additional resuscitation in transient responders.
RECOMMENDED READINGS
Olson SA, Reilly MC, eds. Acetabular and Pelvic Fractures. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2007:15-42.
Advanced Trauma Life Support for Doctors, ed 8. Chicago, IL, American College of Surgeons, 2008.
RESPONSES FOR QUESTIONS 71 THROUGH 74
- Retrograde intramedullary (IM) nailing
- Open reduction and internal fixation (ORIF) with screws alone
- Locking condylar plate
- Circular external fixation
- Lateral and medial plates
Which treatment option listed is best for each patient described?
71A

B
C
D
A 54-year-old healthy man with the condition seen in Figures 71a through 71d
- Retrograde intramedullary (IM) nailing
- Open reduction and internal fixation (ORIF) with screws alone
- Locking condylar plate
- Circular external fixation
- Lateral and medial plates
Question 51
Which of the following are considered characteristic features of degeneration of a disk?
Explanation
REFERENCES: Happey F, Weissman A, Naylor A: Polysaccharide content of the prolapsed nucleus pulposus of the human intervertebral disc. Nature 1961;192:868.
Naylor A, Shentall R: Biomechanical aspects of intervertebral discs in aging and disease, in Jayson M (ed): The Lumbar Spine and Back Pain. New York, NY, Grune and Stratton Inc, 1976, pp 317-326.
Watkins RG, Collis JS: Lumbar Discectomy and Laminectomy. Rockville, MD, Aspen, 1987, pp 2-3.
Question 52
An 11-year-old child has Ewing’s sarcoma of the femoral diaphysis with a small soft-tissue mass. Staging studies show no evidence of metastases. Treatment should consist of
Explanation
REFERENCES: Toni A, Neff JR, Sudanese A, et al: The role of surgical therapy in patients with non-metastatic Ewing’s sarcoma of the limbs. Clin Orthop 1991;286:225.
Picci P, Rougraff BT, Bacci G, et al: Prognostic significance of histopathologic response to chemotherapy in non-metastatic Ewing’s sarcoma of the extremities. J Clin Oncol 1993;11:1763.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant Bone Tumors. Instr Course Lect 2002;51:413-428.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 53
Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?
Explanation
REFERENCE: Flatow EL, Duralde XA, Nicholson GP, Pollock RG, Bigliani LU: Arthroscopic resection of the distal clavicle with a superior approach. J Shoulder Elbow Surg 1995;4:41-50.
Question 54
A 45-year-old man reports right shoulder pain with overhead activities only. Figures 47a through 47d show the radiographs, bone scan, and MRI scan of a lesion of the proximal shoulder. What is the most appropriate treatment?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Question 55
Lumbar disk replacement has been shown to offer which of the following results?
Explanation
REFERENCES: Geisler FH, Blumenthal SL, Guyer RD, et al: Neurological complications of lumbar artificial disc replacement and comparison of clinical results with those related to lumbar arthrodesis in the literature. J Neurosurg Spine 2004;1:143-154.
Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 56
Which of the following treatments for osteoporosis is a direct inhibitor of RANK ligand (RANK-L)?
Explanation
RANKL (Receptor activator of nuclear factor kappa-B ligand) is a key molecule for osteoclast differentiation and activation. Inhibition of RANKL activity with anti-RANKL antibody reduces osteoclastogenesis, resulting in inhibition of bone resorption.
Capozzi et al. author a review article on denosumab. They state the medication confers improved bone mineral density and prevents new fragility fractures similar to alendronate. However, denosumab presents less risk of atypical femoral fractures and
osteonecrosis of the jaw.
Yasuda et al. present a review that details the creation of three elegant animal models to mimic metabolic bone disease and how the animal models can create a template to help cure human metabolic bone disease. These enable modeling of osteoporosis, hypercalcemia, and osteopetrosis by treating normal mice with soluble RANKL (sRANKL), adenovirus expressing sRANKL, and anti-mouse RANKL neutralizing antibody, respectively. They report that these animal models can be established in about 14 days using normal mice.
Illustration A demonstrates the mechanism of action of bisphosphonates and denosumab.
Incorrect Answers:
1: Romosozumab is the first humanized anti-sclerostin monoclonal antibody that has been demonstrated to increase bone formation. 2: Zoledronic acid (Reclast) is a nitrogen containing bisphosphonates that inhibits osteoclast resorption by inhibiting the enzyme farnesyl diphosphate synthase. 4: Teriparatide (Forteo) comprises the first 34 amino acids of the 84 amino acid parathyroid hormone (PTH) and can reproduce the primary effects of PTH by activating adenyl cyclase. 5: Blosozumab is an investigational monoclonal anti-sclerostin antibody showing osteoanabolic properties with the potential to improve clinical outcomes in patients with osteoporosis.
Question 57
This condition is most prevalent in people of which ancestry?
Explanation
The radiograph of the lateral lumbosacral spine reveals an isthmic spondylolysis with a Meyerding grade 1 spondylolisthesis. The incidence of spondylolysis in the general population is around 5%, and grade 1 or 2 slips are present in the majority of children with a spondylolysis. Many cases of spondylolysis are painless and discovered incidentally, but, when painful, hyperextension of the lumbar spine may stress the area of the pars defect and exacerbate a patient’s symptoms. A diagnosis can usually be determined with a lateral radiograph of the lumbar spine. Although oblique lumbar radiographs are frequently ordered, several studies have shown that they do not increase diagnostic or prognostic accuracy. Progression of an isthmic spondylolysis, with or without a grade 1 or 2 listhesis, to a serious slip that might
necessitate surgical intervention is rare and occurs in fewer than 5% of patients. Chance for progression diminishes with age, with patients at highest risk prior to the adolescent growth spurt. Spondylolysis may have a genetic component; an increased prevalence has been found in some families and in some ethnic groups, especially among the Native American population.

Question 58
A 75-year-old man has persistent radial sided hand and wrist pain. Radiographs demonstrate severe scaphotrapezial trapezoidal arthritis. His basal joint is unaffected. His pain has failed to improve with bracing, activity modification, and image-guided corticosteroid injection. He has elected surgical treatment. What longterm complication can arise from a distal scaphoid resection?
Explanation
Resection of the distal pole of the scaphoid eliminates the arthritic contact at the scaphotrapeziotrapezoid joint; however, it functionally shortens the scaphoid. Theoretically, the lunate is at equilibrium between the extension moment of the capitate and the triquetrum and the flexion moment of the scaphoid. Shortening the scaphoid allows the extension moment of the triquetrum to predominate, pulling the lunate into extension and creating a DISI deformity. Concomitant capsulodesis or interposition is recommended by some authors to prevent this complication.
Question 59
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What factor most strongly correlates with the development of compartment syndrome after this injury?
Explanation
REFERENCES: Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
Question 60
The Coleman block test is used to evaluate the cavovarus foot. What is the most important information obtained from this test?
Explanation
REFERENCES: Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 61
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
Explanation
REFERENCE: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 62
Disadvantages of anterior-inferior plate fixation for acute clavicular fractures relative to superior plating include
Explanation
Question 63
Figures 86a through 86c are the radiographs and biopsy specimen of a 14-year-old boy who has had left knee pain for 4 weeks. What is the most likely diagnosis?
Explanation
Question 64
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?
Explanation
3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness.
REFERENCES: Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 65
Currently, what is the most common clinical study type in the orthopaedic literature?
Explanation
Question 66
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T 1 - and T 2 -weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?
Explanation
REFERENCES: Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Kausch T, Rutt J: Subcutaneous rupture of the tibialis anterior tendon: Review of the literature and case report. Arch Orthop Traum Surg 1998;117:290-293.
Question 67
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?
Explanation
Question 68
A 33-year-old woman reports a 3-month history of pain in both feet while running. Examination reveals bilateral point tenderness over the plantar fascia at its origin, and the pain is accentuated when the ankle is dorsiflexed. Management should consist of
Explanation
The most common site for heel pain is where the plantar fascia and intrinsic muscles arise from the medial calcaneal tuberosity on the anteromedial aspect of the heel.
First line treatment is NSAID’s, Physical therapy involving heel cord stretching and an orthosis. Second line therapy after these treatments are unsuccessful involve steroid injection and plaster immobilization. Surgical intervention should be the very last choice in the options given.
Question 69
Figure 42 shows the sagittal T2-weighted MRI scan of a patient’s right knee. These findings are most commonly seen with a complete tear of the
Explanation
fluid in the soft tissues laterally. Additionally, there is a large bone bruise on the medial
femoral condyle. This combination indicates injury to the posterolateral complex. These injuries often have coexisting anterior and/or posterior cruciate ligament injuries. Failure to recognize the posterolateral corner injury can lead to failure of anterior or posterior cruciate ligament reconstructions.
REFERENCES: LaPrade RF, Gilbert TJ, Bollom TS, et al: The magnetic resonance imaging appearance of individual structures of the posterolateral knee: A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 2000;28:191-199.
Ross G, Chapman AW, Newberg AR, et al: Magnetic resonance imaging for the evaluation of acute posterolateral complex injuries of the knee. Am J Sports Med 1997;25:444-448.
Question 70
A young male patient underwent intramedullary nail fixation for a diaphyseal femur fracture. A post-operative CT scanogram is performed to assess rotational alignment between the surgical and non-surgical femur. Which of the following measurement(s) are considered acceptable differences in regards to femoral rotational malreduction after intramedullary nail fixation as compared to the uninjured femur?
Explanation
The maximum acceptable difference in rotational malreduction between the surgical and contralateral legs for femoral version is 15°. Therefore, answers 1 and 2 are correct.
Normal femoral neck anteversion is approximately 11-13°, with a normal range between 5-20°. The variation within the same patients can also be up to 15° difference between limbs. Current literature has shown that this 15° difference is well tolerated by patients, including when this has occured as a result of rotational malreduction following intramedullary nail fixation for a diaphyseal femur fracture.
Ayalon et al. aimed to compare the difference in femoral version (DFV) after intramedullary nailing performed by a trauma-trained and non-trauma trained surgeon. The mean post-operative DFV was 8.7° in these patients, compared to 10.7° in those treated by surgeons of other subspecialties. Post-operative version or percentage of DFV >15° did not significantly differ between these two groups.
Omar et al. studied the utility of pre-operative 'virtual reduction' of bilateral femoral fractures that were initially stabilized with external fixation. After external fixation, the mean rotational difference between both legs was 15.0°
± 10.2°. Following virtual reduction, the mean rotational difference between both legs was 2.1° ± 1.2°, after intramedullary nailing, compared to 6.1° ±
Question 71
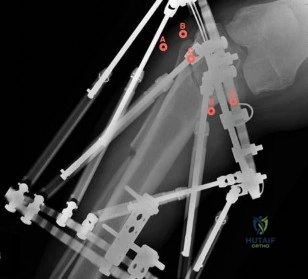
A patient has a vertically and rotationally unstable hemipelvis following a motor vehicle accident. An indication for application of an anterior resuscitative pelvic external fixator is made. Two options with regard to pin insertion location are considered as seen in Figure 20. When compared to pins in position A, the pins in position B may be more advantageous because
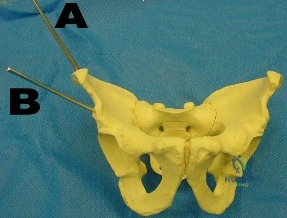
Explanation
Question 72
Figure 65 is the lumbar spine MR image of a 63-year-old woman who has a 3-year history of increasingly bothersome back pain and bilateral buttock and leg pain. She has performed 6 weeks of physical therapy, received epidural injections, and experienced some good short-term results, but her leg pain continues to worsen. What is the most appropriate course of treatment?

Explanation
This patient has symptoms consistent with neurogenic claudication secondary to lumbar spinal stenosis and degenerative spondylolisthesis. Her symptoms are chronic and she has undergone an appropriate course of nonsurgical care. Nevertheless, her symptoms are worsening and surgical intervention is a
reasonable consideration. Studies have shown that patients with lumbar spinal stenosis with associated degenerative spondylolisthesis benefit most from decompression of the neural elements that are stenotic and subsequent fusion across the degenerative slip. Anterior lumbar interbody fusion likely will not address stenosis at the level of the slip and may not result in adequate neurologic decompression. Partial laminotomy and diskectomy likely will not provide adequate neural decompression because these procedures would only address unilateral compression and this patient has bilateral issues. Lumbar laminectomy without fusion could be performed but has been associated with results inferior to lumbar laminectomy with fusion when addressing stenosis with spondylolisthesis.
RECOMMENDED READINGS
Weinstein JN, Lurie JD, Tosteson TD, Zhao W, Blood EA, Tosteson AN, Birkmeyer N, Herkowitz H, Longley M, Lenke L, Emery S, Hu SS. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J Bone Joint Surg Am. 2009 Jun;91(6):1295-304. PubMed PMID: 19487505. View Abstract at PubMed
Herkowitz HN, Kurz LT. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991 Jul;73(6):802-8. PubMed PMID: 2071615. View Abstract at PubMed
Lombardi JS, Wiltse LL, Reynolds J, Widell EH, Spencer C 3rd. Treatment of degenerative spondylolisthesis. Spine (Phila Pa 1976). 1985 Nov;10(9):821-7. PubMed PMID: 4089657. View Abstract at PubMed
RESPONSES FOR QUESTIONS 66 THROUGH 69
Deep surgical-site infection
Adjacent segment degeneration
Pressure ulcers
Iatrogenic neurologic injury
Incidental durotomy
Hardware failure
Match the frequently encountered complication listed above with the appropriate clinical scenario below.
Question 73
Resuscitation of a trauma patient who has been in hypovolemic shock is complete when which of the following has occurred?
Explanation
REFERENCES: Tisherman SA, Barie P, Bokhari F, et al: Clinical practice guideline: End point of resuscitation. J Trauma 2004;57:898-912.
Moore FA, McKinley BA, Moore EE, et al: Inflammation and the Host Response to Injury, a large-scale collaborative project: Patient-oriented research core--standard operating procedures for clinical care. III. Guidelines for shock resuscitation. J Trauma 2006;61:82-89.
Englehart MS, Schreiber MA: Measurement of acid-base resuscitation end points: Lactate, base deficit, bicarbonate or what? Curr Opin Crit Care 2006;12:569-574.
Question 74
Halo treatment for preadolescent children typically requires the use of which of the following? Review Topic
Explanation
Question 75
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of
Explanation
REFERENCES: Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265.
Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Question 76
Spontaneous entrapment of the posterior interosseous nerve most commonly occurs in which of the following locations?
Explanation
REFERENCE: Spinner RJ, Spinner M: Nerve entrapment syndromes, in Morrey BF: The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 839-862.
Question 77
A 32-year-old runner has pain in the medial arch that radiates into the medial three toes. He reports the presence of pain only when running. Examination reveals normal hindfoot alignment. There is a weakly positive Tinel’s sign over the posterior tibial nerve. Tenderness is noted with palpation over the plantar medial area in the vicinity of the navicular tuberosity. What is the most likely diagnosis?
Explanation
REFERENCES: Rask MR: Medial plantar neurapraxia (jogger’s foot): Report of three cases. Clin Orthop 1978;134:193-195.
Murphy PC, Baxter DE: Nerve entrapment of the foot and ankle in runners. Clin Sports Med 1985;4:753-763.
Lutter LD: Surgical decisions in athletes’ subcalcaneal pain. Am J Sports Med 1986;14:481-485.
Question 78
Which of the following is considered a risk factor for the development of low back pain?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 627-643.
Question 79
Which of the following statements best describes labral tears in the hip?
Explanation
The most common associated lesions are chondral injuries. They can occur with or without abnormal bone morphology. The etiology for labral tears can be from traumatic and degenerative causes, structural abnormalities from femoroacetabular impingement, developmental abnormalities, and hip instability.
REFERENCES: Beck M, Kalhor M, Leunig M, et al: Hip morphology influences the pattern of damage to the acetabular cartilage: Femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br 2005;87:1012-1018.
Ito K, Leunig M, Ganz R: Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin Orthop Relat Res 2004;429:262-271.
Crawford MJ, Dy CJ, Alexander JW, et al: The 2007 Frank Stinchfield Award. The biomechanics of the hip labrum and the stability of the hip. Clin Orthop Relat Res 2007;465:16-22.
Question 80
Which of the following is considered an advantage of the tibial inlay fixation compared to transtibial tunnel technique when used in posterior cruciate ligament reconstruction? Review Topic
Explanation
Question 81
An 11-year-old boy sustained an injury to his arm in gym class. He denies prior pain in the arm. Radiographs are shown in Figures 48a and 48b. What is the next most appropriate step in the management of this lesion?
Explanation
REFERENCES: Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Deyoe L, Woodbury DF: Unicameral bone cyst with fracture. Orthopedics 1985;8:529-531.
Question 82
A patient who underwent a L4-L5 hemilaminotomy and partial diskectomy for radiculopathy 8 weeks ago now reports increasing low back pain without neurologic symptoms. A sagittal T2-weighted MRI scan is shown in Figure 13a, and a contrast enhanced T1-weighted MRI scan is shown in Figure 13b. What is the most appropriate management for the patient’s symptoms? Review Topic
Explanation
pseudomeningocele is not present. A revision diskectomy is useful for recurrent radiculopathy but would not be helpful for degenerative low back pain.
(SBQ12SP.29) A 17-year-old female is undergoing posterior instrumented fusion from T5-T12 for adolescent idiopathic scoliosis. At the time of the correction maneuver, the neurophysiologist notifies you of a 60% decrease in somatosensory evoked potential (SSEP) amplitude throughout bilateral lower extremities. Which of the following is an acceptable approach to manage this finding? Review Topic
Immediate wake-up test with examination for clonus
Drop the mean arterial pressure (MAP) to ~60mmHg
Discontinue instrumentation and optimize MAP to 85mmHg or greater
Immediate infusion of intravenous corticosteroids
Modification of the anesthesia plan to include inhalational agents only followed by repeated SSEP testing
The patient has a significant drop in SSEP amplitudes at the completion of the corrective maneuver. The most appropriate response is to raise the MAP to 85 mmHg or greater, discontinue the instrumentation, re-evaluate the SSEPs, and if there is no improvement, to consider reversing the reduction of the deformity.
Intra-operative neurophysiologic monitoring is an effective method to monitor insults to the spinal cord and its exiting roots during spinal instrumentation. The common measurements include SSEPs, which monitor sensory potentials transmitted through the dorsal column system, and motor-evoked potentials (MEPs), which monitor motor response to a trans-cranial stimulus. Decreases in amplitude and latency of the circuits are recorded, however diminished signal amplitudes are more sensitive for neurologic injury, and decreases of of >50-60% being highly concerning. The wake-up test involves reversal of anesthesia so that an intra-operative neurologic examination can be performed.
Devlin et al. reviewed the basic science and practice of neurophysiologic monitoring in spine surgery. They proposed an algorithmic approach to managing intraoperative alerts which include discontinuation of inhalational anesthetics, increasing the MAP to >90 mmHg, discontinuing instrumentation, and performing a wake-up test if neurologic signals fail to normalize.
Herdmann et al. reviewed the practice of neurophysiologic monitoring and the effects of anesthesia upon signal transduction. They report that anesthesia affecting a neuron's intrinsic excitability can alter the results of monitoring. Inhalational anesthetics and decreased MAPs can be responsible for decreased amplitudes.
Vitale et. al. developed a consensus-based intraoperative checklist for management of lost neuromonitoring signals. In this checklist, the first steps across the surgical and anesthetic teams should include: stop the case and announce signal losses to the room, optimize the mean arterial pressure, discuss the status of anesthetic agents, and discuss reversible surgical actions just prior to signal loss.
Incorrect
Question 83
A patient with a grade 2 L5-S1 isthmic spondylolisthesis reports low back pain and bilateral lower extremity pain. Nonsurgical management has failed to provide relief, and the patient is now a candidate for surgical intervention. The
Explanation
Question 84
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include
Explanation
REFERENCES: Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Wenger DR, Ditkoff TJ, Herring JA, Mauldin DM: Protrusio acetabuli in Marfan’s syndrome. Clin Orthop 1980;147:134-138.
Question 85
A 56-year-old woman undergoes an arthroscopic rotator cuff repair for a two-tendon retracted tear (supraspinatus and infraspinatus), requiring the use of four suture anchors placed in a double row technique. At her 1 month follow-up visit, what is the appropriate recommendation for her continued rehabilitation program? Review Topic
Explanation
Question 86
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of
Explanation
REFERENCES: Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Myerson M, Quill GE Jr: Late complications of fractures of the calcaneus. J Bone Joint Surg Am 1993;75:331.
Question 87
A surgeon decides to report outcomes for a new surgical procedure that he has performed on 10 patients who have a rare type of arthritis. He provides data on the functional and subjective patient outcomes. This type of study design is best described as a
Explanation
Question 88
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
REFERENCES: Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
McAuley JP, Moreau G: Sepsis: Etiology, prophylaxis, and diagnosis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 1295-1306.
Question 89
- The radiographs shown in Figures 71a through 71c, and the CT scan shown in Figure 71d reveal an acetabular fracture that should be classified as
Explanation
Note the classic “Spur Sign” seen in these radiographs. This is pathognomonic of a both-column fracture of the acetabulum.
The other defining feature of the both column fx (as evident by these films) is that there is no intact acetabulum connected to the bone fragment which is connected to the ipsilateral SI joint.
Question 90
A 25-year-old man sustained an L1 compression fracture in a fall from his roof. He is neurologically intact and has no other injuries. Radiographs reveal a 25% loss of height anteriorly and 5 degrees of kyphosis at the fracture site. A CT scan reveals no compromise of the posterior column. Management should consist of
Explanation
REFERENCES: Cantor JB, Lebwohl NH, Garvey T, Eismont FJ: Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993;18:971-976.
Rechtine GR II, Cahill D, Chrin AM: Treatment of thoracolumbar trauma: Comparison of complications of operative versus nonoperative treatment. J Spinal Disord 1999;12:406-409.
Question 91
Which of the following zones of articular cartilage has the highest concentration of proteoglycans?
Explanation
Question 92
Figure A shows intraoperative images of a right knee in an 8-year-old boy after he sustained an injury. Which of the following is the most common indication for performing this procedure? Review Topic

Explanation
Arthroscopic treatment of lateral discoid meniscus injuries has the advantages of reducing trauma, precise resection or repair of the meniscus and saucerization of the remaining discoid meniscus. Operative treatment is usually limited to patients with pain and mechanical symptoms that are undergoing partial meniscectomy or repair. Asymptomatic discoid meniscus without tears are not considered a surgical indication for routine saucerization.
Kramer et al. reviewed the diagnosis and treatment of traumatic discoid meniscal tears in children. They report that knee shape, size and skeletal maturity must be considered when determining the optimal method of repair. However, all symptomatic torn discoid menisci are best treated with saucerization and repair.
Good et al. looked at the arthroscopic techniques of discoid meniscus repair. Arthroscopic saucerization was successful in 28 of 30 knees and meniscal repair in 23 of 30 knees. At final follow-up, all patients exhibited full knee flexion beyond 135 degrees. In 3 of 30 patients there was residual knee pain, and four reported intermittent mechanical symptoms.
Figure A shows a series of arthroscopic images of the right knee lateral compartment. There is a sequential saucerization of the discoid meniscus.
Incorrect Answers:
(SBQ13PE.83) 8-year-old boy complains of intermittent painless clicking in his knee. His physical examination is normal. His family doctor orders an MRI, which reveals an incomplete lateral discoid meniscus without evidence of tear. What is the most appropriate treatment? Review Topic
Observation only
Diagnostic arthroscopy
Saucerization of meniscus
Saucerization of meniscus and microfracture
Saucerization and stabilization of the mensicus
The clinical presentation is consistent with a asymptomatic discoid meniscus. The most appropriate treatment at this time would be observation only.
MRI scans of the knee are very sensitive for identifying discoid menisci. Diagnosis is usually made when there are 3 or more 5mm sagittal MRI images showing meniscal continuity. Treatment is mostly focused on conservative modalities. Asymptomatic tears are usually treated with observation only. Saucerization is indicated for recurrent locking, swelling, persistent pain, or radiographic evidence of a meniscal tear.
Watanabe et al. described three types of discoid lateral menisci based on arthroscopic appearance. In this classification, discoid menisci with normal peripheral attachments are either type I (complete) or type II (incomplete). Type III discoid menisci, the so-called Wrisberg ligament type, are lacking posterior capsular attachments with the exception of the posterior meniscofemoral ligament.
Kramer et al. looked at the presentation of pediatric knee pain and discoid meniscus. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the meniscus.
Illustration A shows the cross-section of normal meniscus. Illustration B shows the Watanabe classification.
Incorrect Answers:
Question 93
What type of muscle contraction occurs while the muscle is lengthening?
Explanation
REFERENCES: Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000,
pp 12-13.
Lieber RL: Form and function of skeletal muscle, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 94
Figures 52a and 52b show the radiographs of a left proximal femoral lesion noted serendipitously following minor trauma to the left hip. The patient has no thigh pain and is fully active without limitation. What is the most likely diagnosis of this bony lesion?
Explanation
REFERENCE: Parsons TW: Benign bone tumors, in Fitzgerald R Jr, Kaufer H, Malkani A (eds): Orthopaedics. Philadelphia, PA, Mosby International, 2002, pp 1027-1035.
Question 95
A 68-year-old woman underwent a successful total right hip arthroplasty with a metal-on-metal articulation and cementless porous-coated components. Three months later, she underwent identical surgery on the left hip. Three months after surgery on the left hip, she reports groin pain on ambulation. Examination reveals significant groin discomfort with passive hip motion, particularly at the extremes of motion. Radiographs are shown in Figures 21a and 21b. Laboratory studies show an erythrocyte sedimentation rate of 35 mm/h and a C-reactive protein of 0.9. Aspiration yields scant growth of Staphylococcus epidermidis in the broth only, with no evidence of loosening on arthrography. A second aspiration yields scant growth of Staphylococcus epidermidis in the broth only. What is the most likely cause of the patient’s pain?
Explanation
REFERENCES: White RE: Evaluation of the painful total hip arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998,
vol 2, pp 1377-1385.
Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
Question 96
A 25-year-old man is involved in a motor vehicle accident and brought to the emergency department at 4 am on Sunday morning. He has a closed distal third femoral shaft fracture. His leg is initially pulseless but after applying inline traction, a distal pulse can be palpated and the limb appears to be viable. The pulse in the injured limb “feels” different than the pulse in the uninjured limb. What is the next step in assessing the vascular status of this limb?
Explanation
REFERENCES: Levy BA, Zlowodzki MP, Graves M, et al: Screening for extremity arterial injury with the arterial pressure index. Am J Emerg Med 2005;23:689-695.
Abou-Sayed H, Berger DL: Blunt lower-extremity trauma and politeal artery injuries: Revisiting the case for selective arteriography. Arch Surg 2002;137:585-589.
Mills WJ, Barei DP, McNair P: The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: A prospective study. J Trauma 2004;56:1261-1265.
Question 97
A 35-year-old man sustained a 10% compression fracture of the C5 vertebra in a diving accident. Radiographs show good alignment, and examination reveals no neurologic compromise. An MRI scan reveals no significant soft-tissue disruption posteriorly. Management should consist of
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 457-464.
Allen GL, Ferguson RL, Lehmann TR, O’Brien RP: A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7:1-27.
Question 98
What structure is located at the tip of the arrow in Figure 18?
Explanation
REFERENCE: An H: Diagnostic imaging of the spine, in Principles and Techniques of Spine Surgery. Baltimore, MD, Lippincott Williams & Wilkins, 1998, pp 102-125.
Question 99
Recurrence of this deformity after initial treatment should be treated with
Explanation
Single nuclear polymorphism (SNP) on chromosome 12q24.31, an intergenic SNP, is the PITX1-TBX4 transcriptional pathway that codes for hindfoot formation and is associated with clubfoot. The COLIA-1 gene is related to osteoporosis. Mutations in EXT genes that control formation of tumors cause multiple hereditary exostosis. Mutations in the COL5A or COL3A genes are associated with Ehlers-Danlos syndrome. All idiopathic clubfeet involve abnormalities of or around the talus.
The classic Ponseti technique is associated with a low recurrence rate when followed precisely. The most common reason for recurrence is noncompliance with postsurgical bracing. The initial treatment for recurrence after Ponseti casting is recasting.
NCOA2 fusion transcripts has been noted in mesenchymal chondrosarcoma. Ring chromosomes with CDK4 and MDM2 amplification may be identified with low-grade central osteosarcoma or parosteal osteosarcoma. Fusion transcripts of CDH11-USP6 have been observed in aneurysmal bone cysts.

Video 85
CLINICAL SITUATION FOR QUESTIONS 82 THROUGH 85
Figures 82a and 82b are the radiographs of a 10-year-old girl who was an unrestrained back seat passenger in a motor vehicle collision. Her sole injury is to her left leg. She has a deformed valgus knee with lateral swelling and bruising, and no wound is visible. Upon examination, she has symmetric pulses to her right leg but diminished sensation on the dorsum of the foot and in the first web space. She cannot dorsiflex her left foot or toes but can plantar flex and invert them. Weak ankle eversion is present. Sensation to the plantar foot, medial ankle, and lateral ankle is intact. She likely will reach skeletal maturity at age 14.
Question 100
What effect does deep freezing have on allograft tissue?
Explanation
REFERENCES: Shelton WR, Treacy SH, Dukes AD, Bomboy AL: Use of allografts in
knee reconstruction: I. Basic science aspects and current status. J Am Acad Orthop Surg 1998;6:165-168.
Caspari RB, Botherfield S, Horwitz RL, et al: HIV transmission via allograft organs and tissues. Sports Med Arthroscopy Rev 1993;1:42-46.
