Orthopedic Board Review MCQs: Trauma, Arthroplasty, Spine & Hand | Part 71

Key Takeaway
This page offers Part 71 of a comprehensive Orthopedic Surgery Board Review, featuring 100 verified, high-yield MCQs designed for orthopedic surgeons and residents preparing for OITE/AAOS certification. Engage in Study or Exam modes with detailed explanations, covering key topics like Fracture, Hip, Knee, and Nerve to optimize your exam preparation.
About This Board Review Set
This is Part 71 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 71
This module focuses heavily on: Fracture, Hip, Knee, Nerve.
Sample Questions from This Set
Sample Question 1: A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the c...
Sample Question 2: He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm3. Management s...
Sample Question 3: A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?...
Sample Question 4: A 14-year-old gymnast misses her dismount off of the uneven bars, hits the mat face first, and losesconsciousness for about 15 seconds. She is dazed and confused for several minutes. She does not complain of pain; numbness; or weakness, and...
Sample Question 5: A 65-year-old woman has severe pain and numbness in her hand. She notes frequent awakenings at nighttime and difficulty with fine tasks. She also has a history of cervical radiculopathy and notes intermittent pain in her upper arm and peris...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the clavicle distal to a line drawn vertically to the coracoid process. Management should consist of
Explanation
REFERENCES: Robinson CM, Cairns DA: Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-782.
Deafenbaugh MK, Dugdale TW, Staeheli JW, et al: Nonoperative treatment of Neer type II distal clavicle fractures: A prospective study. Contemp Orthop 1990;20:405-413.
Question 2
He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm3. Management should consist of

Explanation
has been used successfully when the duration of symptoms is 3 weeks or less. Long-term suppressive antibiotics are most commonly used when the patient’s medical condition precludes further surgery. Delayed reimplantation has been shown to be superior to immediate reimplantation in multiple studies. Little data support the use of arthroscopic irrigation and debridement.
Question 3
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
REFERENCES: Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Stuchin SA, Johanson NA, Lachiewicz PF, Mont MA: Surgical management of inflammatory arthritis of the adult hip and knee, in Zuckerman JS (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-109.
Question 4
A 14-year-old gymnast misses her dismount off of the uneven bars, hits the mat face first, and loses consciousness for about 15 seconds. She is dazed and confused for several minutes. She does not complain of pain; numbness; or weakness, and she is moving all extremities without deficit. The athlete and coach want to go back to competition that day. How should they be advised?
Explanation
symptoms with cognitive effort. They must be off of medications that could mask or alter concussion symptoms. Neurocognitive testing can be a helpful tool in determining brain function even after all symptoms of concussion have resolved. With a comparison baseline test, this evaluation, in conjunction with a physician's examination, may reduce risk for second impact syndrome. The athlete's clinical neurologic examination findings (cognitive, cranial nerve, balance testing) must return to baseline before resuming exercise. Research has shown that among youth athletes, it may take longer for tested functions to return to baseline (compared with the recovery rate in adult athletes). Brain MRI scan has no role in evaluating athletes for return to play in this situation.
Question 5
A 65-year-old woman has severe pain and numbness in her hand. She notes frequent awakenings at nighttime and difficulty with fine tasks. She also has a history of cervical radiculopathy and notes intermittent pain in her upper arm and periscapular region. An examination reveals a positive Tinel sign over the midforearm and carpal tunnel. Electrodiagnostic testing shows a median nerve sensory distal latency of 3.8 ms (normal latency is 3.5 ms). Which intervention or test would best predict if carpal tunnel release would be successful in relieving this patient's symptoms?
Explanation
This patient demonstrates several upper extremity issues including possible carpal tunnel syndrome, cervical radiculopathy, and pronator syndrome. The electrodiagnostic testing is equivocal, and a corticosteroid carpal tunnel injection should be performed prior to surgical intervention to assess its effectiveness in eliminating the patient's symptoms. Positive response (meaning improvement in symptoms), after corticosteroid injection at the carpal tunnel correlates well with symptom relief following surgery. Trigger-point injections are not indicated for carpal tunnel syndrome. Ultrasound and carpal tunnel view radiograph can provide diagnostic information but would not be helpful in determining treatment in this specific case.
Question 6
Figure 7 shows a sagittal T 1 -weighted MRI scan. What muscle/tendon is identified by the arrow?
Explanation
REFERENCES: Goutallier D, Postel JM, Gleyze P, et al: Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears.
J Shoulder Elbow Surg 2003;12:550-554.
Agur AM (ed): Grant’s Atlas of Anatomy, ed 9. Baltimore, MD, Lippincott Williams & Wilkins, 1991, p 394.
Question 7
A 26-year-old weightlifter had increasing pain in his left shoulder for 4 months. Nonsurgical treatment consisting of anti-inflammatory medication,
Explanation
Question 8
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?
Explanation
REFERENCES: Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539.
Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than
2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
Robinson CM, Court-Brown CM, McQueen MM, et al: Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am
2004;86:1359-1365.
Question 9
Figure 1 is the clinical photograph of a 22-year-old college pitcher who complains of posterior shoulder pain and feelings of shoulder weakness. He denies shoulder trauma. Evaluation should include
Explanation
Question 10
Figure 92 is the radiograph of a 45-year-old man who was thrown from his horse and now reports groin pain. Which of the following is the most common long-term sequelae of this injury?

Explanation
Question 11
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?
Explanation
REFERENCES: Gelb DE, Lenke LG, Bridwell KH, et al: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20:1351-1358.
Vedantam R, Lenke LG, Keeney JA, et al: Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine 1998;23:211-215.
Question 12
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?
Explanation
REFERENCES: Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.
Question 13
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
REFERENCES: Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393.
Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Kostuik JP, Valdevit A, Chang HG, et al: Biomechanical testing of the lumbosacral spine. Spine 1998;23:1721-1728.
Question 14
A 71-year-old woman who reports long-term use of oral steroids for asthma is referred for treatment of a distal humerus fracture. Radiographs reveal diffuse osteopenia and a severely comminuted intra-articular fracture. What is the most appropriate treatment?
Explanation
REFERENCES: Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.
Garcia JA, Mykula R, Stanley D: Complex fractures of the distal humerus in the elderly: The role of total elbow replacement as primary treatment. J Bone Joint Surg Br 2002;84:812-816.
Question 15
A nondisplaced fracture of the proximal medial femoral neck proximal to the lesser trochanter is noted at the time of insertion of a cementless tapered wedge-type femoral component in a total hip arthroplasty. Appropriate perioperative management should include which of the following?
Explanation
REFERENCES: Sharkey PF, Hozack WJ, Booth RE, et al: Intraoperative femoral fractures in cementless total hip arthroplasty. Orthop Rev 1992;21:337-342.
Sharkey PF, Wolf LR, Hume EL, et al: Insertional femoral fracture: A biomechanical study of femoral component stability. Semin Arthroplasty 1990;1:91-94.
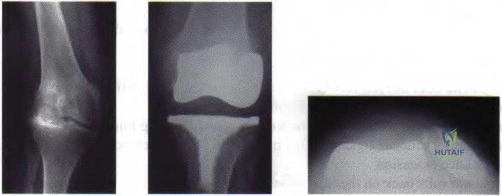
Figure 39a Figure 39b Figure 39c
Question 16
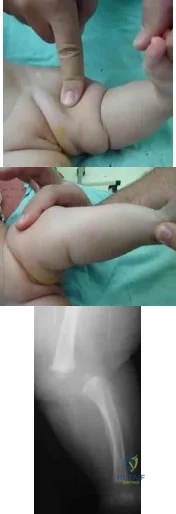
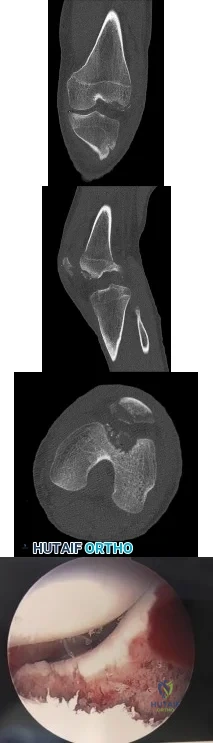
A mother brings in her 6-month-old infant with a knee deformity. The child had previously been treated with serial casting in flexion for 3 month at an outside facility. Examination reveals passive hyperextension to 25° and passive flexion to 15° as shown in Figures A and B respectively. A lateral radiograph of the knee is shown in Figure C. What is the most appropriate next step in treatment? Review Topic
Explanation
Congenital knee dislocation is rare. The etiology is thought to be quadriceps contracture. It is associated with developmental dysplasia of the hip (DDH) and clubfoot (CTEV). In newborn infant, casting or bracing with the knee in flexion
should be performed. If this fails, percutaneous or open VY quadricepsplasty, followed by above-knee casting, is indicated.
Abdelaziz et al. proposed a new grading system (Tarek CDK grading system-see Illustrations A and B) and treatment protocol as follows: (1) Serial casting for Grade 1 regardless of age and in neonates with grade 2 <1mth. If flexion to >90° is achieved within 4 weeks, then serial casting is continued; if range remains <90°, percutaneous quadriceps recession (PQR) is performed. (2) PQR is performed in Grade 2 CDK in infants >1 month of age upon presentation. (3) VY quadricepsplasty is indicated in patients with Grade 3 CDK or in recurrent cases.
Klingele et al. describe ACL shortening and reinforcement in 2 patients with congenital knee dislocation who developed ACL incompetence due to elongation. They conclude that stabilizing and reinforcing the ACL may prevent long-term anterior instability, hyperextension and recurrent deformity.
Figures A and B show the range of motion of the knee (25deg hyperextension to 15deg flexion). Figure C is a lateral radiograph showing congenital dislocation of the knee. Illustrations A and B show the Tarek grading system. Illustration C shows the different techniques of quadricepsplasty (upper row, structures divided and skin incisions used; lower row, how lengthening of the quadriceps mechanism is achieved). The most common PQR is the Roy-Crawford technique. The most common VYQ is the Curtis-Fisher technique.
Incorrect Answers:
Question 17
A 23-year-old national team rower reports pain over the radial dorsum of the forearm that is made worse with flexion and extension of the wrist during competition. His primary physician initially diagnosed de Quervain’s tenosynovitis, and a subsequent corticosteroid injection into the first dorsal compartment at the wrist provided no relief. The patient continues to report pain and audible crepitus that is noted 5 cm proximal to the wrist joint, on the radial aspect. What structures are involved in the continued pathology?
Explanation
REFERENCES: Grundberg AB, Reagan DS: Pathologic anatomy of the forearm: Intersection syndrome. J Hand Surg Am 1985; 10:299-302.
Thorson E, Szabo RM: Common tendinitis problems in the hand and forearm. Orthop Clin North Am 1992;23:65-74.
Williams JG: Surgical management of traumatic non-infective tenosynovitis of the wrist extensors. J Bone Joint Surg Br 1977;59:408-410.
Wood MB, Dobyns JH: Sports-related extraarticular wrist syndromes. Clin Orthop Relat Res 1986;202:93-102.
Question 18
Figure 38 shows the radiograph of a 40-year-old woman who reports severe groin pain and lack of motion of the right hip. History reveals that the patient underwent a femoral osteotomy for hip dysplasia approximately 30 years ago. Treatment should include
Explanation
REFERENCE: Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 789-802.
Question 19
What is the mechanism of action of an intramuscular injection of botulinum type A toxin in reducing spasticitiy?
Explanation
REFERENCES: Koman LA, Mooney JF III, Smith B, Goodman A, Mulvaney T: Management of cerebral palsy with botulinum-A toxin: Preliminary investigation. J Pediatr Orthop 1993;13:489-495.
Brin MF: Botulinum toxin: Chemistry, pharmacology, toxicity, and immunology. Muscle Nerve Suppl 1997;6:S146-168.
Question 20
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
Explanation
A. Lateral head of triceps (radial nerve) and brachialis
(musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii
(musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis
(musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis
(musculocutaneous nerve)
Question 21
A 7-year-old girl is hit by a motor vehicle and sustains the isolated ipsilateral injuries shown in Figures 16a and 16b. What is the optimal definitive method of treatment? Review Topic

Explanation
Question 22
An 18-year-old man sustains an injury to the right brachial plexus after falling off his bicycle. Examination reveals no rhomboideus major or minor muscle function. This finding most likely indicates a preganglionic injury to which of the following nerve roots?
Explanation
REFERENCES: Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 23-28.
Millesi H: Brachial plexus injury in adults: Operative repair, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1285-1301.
Question 23
Decreased risk of shoulder and elbow injury in a throwing athlete has been demonstrated with which of the following? Review Topic
Explanation
Question 24
A 35-year-old man reports a 2-year history of right groin pain. The pain is made worse with hip flexion, prolonged sitting, and cycling. A radiograph and MRI scan are shown in Figures 16a and 16b. Nonsurgical management has failed to provide relief. What is the best surgical option?
Explanation
REFERENCES: Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: Preliminary results of labral refixation. J Bone Joint Surg Am 2006;88:925-935.
Parvizi J, Leunig M, Ganz R: Femoroacetabular impingement. J Am Acad Orthop Surg 2007;15:561-570. Trousdale RT: Acetabular osteotomy: Indications and results. Clin Orthop Relat Res 2004;429:182-187.
Question 25
Figures 25a and 25b show the radiograph and MRI scan of a 7 1/2-year-old boy who has been limping for 1 year. His pain has worsened over the past 2 weeks, and his parents note swelling over the dorsum of the foot for the past 4 days. Examination reveals no fever, and laboratory studies show a WBC of 6,700/mm 3 , an erythrocyte sedimentation rate of 26 mm/h, and a normal C-reactive protein level. What is the most likely diagnosis?
Explanation
REFERENCES: Wang MN, Chen WM, Lee KS, Chin LS, Lo WH: Tuberculous osteomyelitis in young children. J Pediatr Orthop 1999;19:151-155.
Watts HG, Lifeso RM: Tuberculosis of the bones and joints. J Bone Joint Surg Am 1996;78:288-298.
Question 26
What is the most common cause of the new onset of amenorrhea in a female endurance athlete who is not sexually active?
Explanation
REFERENCES: Constantini NW: Clinical consequences of amenorrhea. Sports Med 1994;17:213-223.
Bennell KL, Malcolm SA, Thomas SA, et al: Risk factors for stress fractures in track and field athletes: A twelve-month prospective study. Am J Sports Med 1996;24:810-818.
Question 27
Figures 191a and 191b are the radiographs of an 18-year-old man who had an ankle fracture requiring open reduction and internal fixation 2 years ago. He has a progressive symptomatic ankle deformity.Surgical intervention should consist of

Explanation

Question 28
making a cut toward the ball. He felt a pop and his leg gave way. During physical examination, as the knee is moved from full extension into flexion with an internal rotation and valgus force, you notice a “clunk” within the knee. What is the most likely biomechanical basis for the “clunk”?
Explanation
This patient sustained an isolated anterior cruciate ligament (ACL) injury based upon the mechanism described and examination findings. The finding that produces the “clunk” is the pivot-shift maneuver, which is positive in a knee with an incompetent ACL. With an ACL-deficient knee in full extension and internal rotation, the lateral tibial plateau subluxates anteriorly. As the knee is flexed, the lateral tibial plateau slides posteriorly into a reduced position, causing an audible clunk. Response 4 correctly describes the pathomechanics that result in the audible clunk heard during the pivot-shift maneuver. Responses 1 and 2 are incorrect because they describe the medial tibial plateau, which is not part of the pathomechanics of the pivot shift. Response 3 is incorrect because in extension, the lateral tibial plateau is subluxated, not reduced.
Question 29
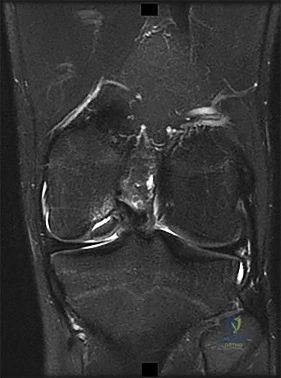
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time? Review Topic
Explanation
point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis.
(SBQ12SP.20) Amphotericin B is most appropriate for the treatment of which type of spine infection? Review Topic
Fungal osteomyelitis
Bacterial osteomyelitis with a gram-positive organism
Bacterial osteomyelitis with a gram-negative organism
Tuberculous osteomyelitis
Viral meningomyelitis
Amphotericin B would be most appropriate for the treatment of fungal infections of the spine.
Amphotericin B is a broad-spectrum anti-fungal medication. It is commonly used as the first-line agent for treatment of fungal infections of the spine. The most common fungi involving the spine include cryptococcus, candida, and aspergillus. The indications for débridement and stabilization with spinal fusion, includes resistance to antibiotic therapy, spinal instability, and/or neurologic deficits.
Kim et al. reviewed fungal infections of the spine. They comment that fungus infections are most commonly spread by hematogenous or direct spread. Access to the vascular system may include intravenous lines, during implantation of prosthetic devices, or during surgery.
Frazier et al. retrospectively reviewed 11 patients with fungal osteomyelitis of the spine. Nine of the patients were immunocompromised secondary to diabetes mellitus, corticosteroid use, chemotherapy for a tumor, or malnutrition. All were treated with anti-fungal medication. 10 of 11 patients were also treated with surgical debridement. Paralysis secondary to the spine infection developed in eight patients. After an average of 6.3 years of follow-up, the infection had resolved in all nine surviving patients.
Illustration A shows the mechanism of action of Amphotericin. Illustration B shows T1- (Image A and B) and T2-weighted (Image C) images of the lower thoracic and lumbar spine. There are hypointense signals within the T12 and L1 vertebral bodies (Images A and B) indicative of fungal osteomyelitis.
IncorrectAnswers:
Question 30
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15° of valgus, and forefoot supination can be corrected to 10° from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCE: Mann RA: Flatfoot in adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 757-784.
Question 31
A patient with myelopathy underwent a one-level corpectomy 1 day ago and is now home. In the middle of the night he calls to report markedly increased difficulty in swallowing, diaphoresis, a change in his voice, and difficulty lying flat. What is the best course of action?
Explanation
REFERENCES: Emery SE, Smith MD, Bohlman HH: Upper-airway obstruction after multilevel cervical corpectomy for myelopathy. J Bone Joint Surg Am 1991;73:544-551.
McAfee PC, Bohlman HH, Riley LH Jr, Robinson RA, Southwick WO, Nachlas NE: The anterior retropharyngeal approach to the upper part of the cervical spine. J Bone Joint Surg Am 1987;69:1371-1383.
Question 32
An axial T 1 -weighted MRI scan of the pelvis is shown in Figure 35. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, et al (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System,
ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 33
A subtrochanteric femur fracture in which the lesser trochanter is intact is associated with what deformity?
Explanation
Question 34
The incidence of osteosarcoma is highest in what age group?
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266.
Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989.
Wold L, et al: Osteogenic Sarcoma: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, p 14.
Question 35
Figures 44a and 44b show the radiographs of a 28-year-old woman who has had progressive hip pain for the past 3 months. What is the most likely diagnosis?
Explanation
REFERENCES: Scarborough M, Moreau G: Benign cartilage tumors. Orthop Clin North Am 1996;27:583-589.
Garrison R, Unni K, McLeod RA, Pritchard DJ, Dahlin DC: Chondrosarcoma arising in osteochondroma. Cancer 1982;49:1890-1897.
Question 36
An 18-year-old boy has had pain in the right knee for the past 6 months. Examination reveals some fullness behind the knee but no significant palpable soft-tissue mass. There is no effusion, and he has full knee range of motion. The remainder of the examination is unremarkable. A radiograph and MRI scans are shown in Figures 33a through 33c, and biopsy specimens are shown in Figures 33d and 33e. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 20-21.
Unni KK, Dahlin DC, Beabout JW, Ivins JC: Parosteal osteogenic sarcoma. Cancer 1976;37:2466-2475.
Question 37
What is the plasma half-life of warfarin?
Explanation
Question 38
..A 75-year-old woman sustained a 4-part fracture dislocation of the proximal humerus with a comminuted humeral head. You decide to perform a reverse total shoulder replacement because of her age and activity level. This will be your first reverse total shoulder replacement. It is common practice in your hospital for an industry representative to be present when new implants are brought into the operating room. What information are you required to disclose?
Explanation
Arthroscopic or open debridement and capsular release
Interposition arthroplasty
Ulnohumeral arthrodesis
Linked total elbow arthroplasty (TEA)
Unlinked TEA
What surgical procedure listed above is most associated with the conditions defined below?
Question 39
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management? Review Topic

Explanation
Question 40
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?
Explanation
3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness.
REFERENCES: Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Haynes RJ: Developmental dysplasia of the hip: Etiology, pathogenesis, and examination and physical findings in the newborn. Instr Course Lect 2001;50:535-540.
Question 41
An year-old obese woman has left knee pain. She had surgery 5 years ago for a patellar nonunion after total knee arthroplasty that was complicated by infection, which was treated with implant removal and patellectomy. She has not been ambulatory since then. She states she is no longer on antibiotics. She has moderate pain, but her primary problem is instability of the knee. She has a 40° extensor lag. Darkening of the skin is present distal to the incision consistent with venous stasis changes. The erythrocyte sedimentation rate is 12 mm/h (reference range 0 to 20 mm/h) and her C-reactive protein level is 0 mg/L (reference range 08 to 1 mg/L). Left knee aspiration shows a white blood cell count of 800 and 20% neutrophils. What is the best next step?
Explanation
This patient is elderly, obese, and nonambulatory and has a chronic quadriceps tendon rupture after infected total knee arthroplasty. Her potential for ambulation after revision total knee arthroplasty is very low. Primary repair of the tendon is unlikely to be successful, even with augmentation, so revision total knee arthroplasty with primary quadriceps tendon repair and two-stage revision knee arthroplasty and quadricep repair with Achilles allograft are not the best management techniques. Extensor mechanism allograft could be done but would have a high failure rate in a patient of this size. No sign of infection is seen, based on laboratory studies, so a two-stage procedure is not necessary. The best management although not optimal, would be treatment in a drop-lock brace. Arthrodesis is also an option, but would have a high complication rate, and in a patient that is nonambulatory, a fused knee would be increasingly
difficult with activities of daily living and mobility.
Question 42
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Explanation
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. These arteries arise from the popliteal artery. If this artery is not adequately mobilized, a gastrocnemius soleus flap can be devascularized.
Question 43
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?
Explanation
REFERENCES: Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Matsen FA III, Thomas SC, Rockwood CA: Anterior glenohumeral instability, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 526-622.
Question 44
When performing a cruciate-retaining total knee arthroplasty, trial components are inserted. The knee comes to full extension but is tight in flexion. The surgeon should consider
Explanation
In this scenario, the flexion gap needs to be increased. Increase in flexion gap can be accomplished by downsizing the femoral component and increasing posterior tibial slope. In posterior cruciate-retaining TKA procedures, recession or release of the posterior cruciate ligament can loosen the flexion gap, allowing for an increase in flexion. Flexing the femoral
component tightens the flexion gap, and downsizing the tibial insert thickness decreases flexion and extension gaps, while resection of the distal femur only increases the extension gap.

CLINICAL SITUATION FOR QUESTIONS 52 THROUGH 55
Figure 52 is the standing anteroposterior radiograph of a 55-year-old man who has a 5-year history of daily left knee pain with weight-bearing activities. He denies night pain or symptoms of instability. Upon examination his range of motion is 0 to 140 degrees. He has a mild, fully correctable varus deformity and a negative Lachman test result. He has failed nonsurgical treatment.
Question 45
The arthroscopic views shown in Figures 31a and 31b reveal extensive synovitis in the anterolateral corner of the ankle overlying a band of tissue sometimes implicated in soft-tissue impingement of the ankle following a chronic sprain injury. This band is a portion of the
Explanation
REFERENCES: Bassett FH III, Gates HS III, Billys JB, et al: Talar impingement by the anteroinferior tibiofibular ligament: A cause of chronic pain in the ankle after inversion sprain.
J Bone Joint Surg Am 1990;72:55-59.
DiGiovanni BF, Fraga CJ, Cohen BE, et al: Associated injuries found in chronic lateral ankle instability. Foot Ankle Int 2000;21:809-815.
Question 46
03 A 23 year old sustains an isolated right knee dislocation in an MVA. A closed reduction is performed and confirmed with radiographs. What is the next appropriate study?
Explanation
OKU Truama 2 says “the use of ABI with the blood pressure cuff and Doppler evaluation of the distal circulation has been proposed as effective in determining any occult vascular injury. A ratio > 0.9indicates a normal study.”[1] The referenced article confirms this. “Confirmation of the safety and accuracy of physical exam in the evaluation of knee dislocation for injury of the popliteal artery.” J. Trauma2002; 52: 247-252
back to this question next question
[1] OKU Trauma 2 pg 151-153
Question 47
What malignant disease most commonly develops in conjunction with chronic osteomyelitis?
Explanation
REFERENCES: Dell PC: Hand, in Simon MA, Springfield D (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 405-420.
McGrory JE, Pritchard DJ, Unni KK, Ilstrup D, Rowland CM: Malignant lesion arising in chronic osteomyelitis. Clin Orthop 1998;362:181-189.
Question 48
A 55-year-old man has had a mass in his right thigh for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 55a through 55c. What is the most likely diagnosis?
Explanation
REFERENCE: Kawaguchi S, Wada T, Nagoya S, Ikeda T, Isu K, Yamashiro K, et al: Extraskeletal myxoid chondrosarcoma. Cancer 2003;97:1285-1292.
Question 49
Which of the following clinical disorders is the result of a mutation in fibroblast growth factor recepter 3 (FGFR3)?
Explanation
REFERENCES: Wagner T, Wirth J, Meyer J, et al: Autosomal sex reversal and camptomelic dysplasia are caused by mutations in and around the SRY-related gene SOX9. Cell 1994;79:1111-1120.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 111-131.
Dietz FR, Murray JC: Update on the genetic bases of disorders with orthopaedic manifestations, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 50
A patient who underwent primary total hip arthroplasty 7 years ago that resulted in excellent pain relief and a normal gait now reports pain and a limp. Postoperative and current AP radiographs are shown in Figures 2a and 2b. What is the most likely cause of the pathology seen?
Explanation
REFERENCES: Claus MC, Hopper RH, Engh CA: Fractures of the greater trochanter induced by osteolysis with the anatomic medullary locking prosthesis. J Arthroplasty 2002;17:706-712.
Heekin RD, Engh CA, Herzwurm MF: Fractures through cystic lesions of the greater trochanter: A cause of late pain after cementless total hip arthroplasty. J Arthroplasty 1996;11:757-760.
Question 51
A 3-year-old child has bilateral genu varum and short stature. Radiographs show physeal widening and generalized osteopenia. The femora and tibiae show anterolateral bowing. Laboratory studies show low normal serum calcium values, significantly decreased serum phosphate levels, and normal parathyroid hormone (PTH), alkaline phosphatase, and vitamin-D levels. These findings are consistent with
Explanation
D-resistant rickets is the renal tubule’s inability to resorb phosphate leading to hypophosphatemia. Laboratory findings in the condition are normal or near normal serum calcium values, significantly decreased serum phosphate levels, elevated alkaline phosphatase levels, and normal PTH and vitamin-D levels. The most common form is inherited as an
X-linked dominant trait. Nutritional rickets has a normal or low serum phosphate levels, normal or low serum calcium values, and decreased levels of 25(OH) vitamin D and
1,25-dihydroxyvitamin D. Hypophosphatasia is a rare condition characterized by a deficiency of alkaline phosphatase in the serum and tissues, leading to generalized abnormal mineralization of bone. Primary hyperparathyroidism usually is caused by a parathyroid adenoma, and the child generally has abdominal problems and hypercalcemic crisis. Laboratory findings include elevated serum calcium values, alkaline phosphatase levels, and PTH levels, and decreased serum phosphate levels. Children with renal osteodystrophy tend to have genu valgum, and laboratory findings include elevated serum phosphate, alkaline phosphatase, and PTH levels, and low serum calcium values. Findings of renal disease include elevated BUN and creatinine.
REFERENCES: Herring JA: Metabolic and endocrine bone diseases, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, pp 1686-1710.
Zaleske DJ: Metabolic and endocrine abnormalities, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 181-203.
Question 52
A 6-year-old boy presents with a mass and a lucent lesion involving the tibial shaft as seen in Figure 17a. The mass is mildly tender to palpation. The bone scan is focally hot in the tibia. Biopsy specimens are shown in Figures 17b and 17c. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M, Laus M: Osteofibrous dysplasia of the tibia and fibula. J Bone Joint Surg Am 1981;63:367-375.
McCaffery M, Letts M, Carpenter B, et al: Osteofibrous dysplasia: A review of the literature and presentation of an additional 3 cases. Am J Orthop 2003;32:479-486.
Question 53
Patients with patellar clunk syndrome are best managed by which of the following methods?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 329.
Diduch DR, Scuderi GR, Scott WN, et al: The efficacy of arthroscopy following total knee replacement. Arthroscopy 1997;13:166-171.
Lucas TS, DeLuca PF, Nazarian DG, et al: Arthroscopic treatment of patellar clunk. Clin Orthop 1999;367:226-229.
Question 54
In patients undergoing elective hip or knee arthroplasty who are not at elevated risk (beyond the risk associated with the surgery) for venous thromboembolism or bleeding, using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism was assigned what grade of recommendation by the 2011 AAOS Clinical Practice Guideline, Preventing Venous Thromboembolic Disease in Patients Undergoing Elective Hip and Knee Arthroplasty?
Explanation
Using pharmacologic agents and/or mechanical compressive devices for the prevention of venous thromboembolism in patients undergoing elective hip or knee arthroplasty who are not at elevated risk beyond that of the surgery itself for venous thromboembolism or bleeding was given a moderate grade of recommendation in the 2011 AAOS Clinical Practice Guideline referenced above.
Question 55
Which of the following characteristics is seen in patients with osteochondritis dissecans of the elbow? Review Topic
Explanation
Question 56
Patient outcome after open reduction and internal fixation of tibial plateau fractures shows that patients older than 50 years of age when compared to younger patients have
Explanation
Question 57
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of
Explanation
REFERENCES: Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Jobe FW, Tibone JE, Jobe CM, Kvitne RS: The shoulder in sports, in Rockwood CA, Matsen FA (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 961-990.
Question 58
A 78-year-old athletic woman has a history of severe back pain without antecedent trauma. She was in the emergency department 2 days ago with a T12 compression fracture. A dual x-ray absorptiometry (DEXA) scan performed earlier this year revealed a T-score of -2.8. Her condition may be attributable to
Explanation
The diagnosis is severe osteoporosis because this patient's T-score is lower than -2.5 on DEXA scan and her fragility fracture involves the T12 vertebra. Osteoporosis may be associated with polymorphisms of the COL1A1 gene. EXT1 is associated with multiple hereditary exostoses, and translocation X:18 is associated with synovial sarcoma. The gene p53 is associated with Li-Fraumeni syndrome and osteosarcoma.
RECOMMENDED READINGS
Masoodi TA, Alsaif MA, Al Shammari SA, Alhamdan AA. Evaluation and identification of damaged single nucleotide polymorphisms in COL1A1 gene involved in osteoporosis. Arch Med Sci. 2013 Oct 31;9(5):899-905. doi: 10.5114/aoms.2012.28598. Epub 2012 May 13.
PubMed PMID: 24273577. ? View Abstract at PubMed
Kurt-Sirin O, Yilmaz-Aydogan H, Uyar M, Seyhan MF, Isbir T, Can A. Combined effects of collagen type I alpha1 (COL1A1) Sp1 polymorphism and osteoporosis risk factors on bone mineral density in Turkish postmenopausal women. Gene. 2014 May 1;540(2):226-31. doi: 10.1016/j.gene.2014.02.028. Epub 2014 Feb 22. PubMed PMID: 24566004. ? View Abstract at PubMed
Question 59
The photomicrograph in Figure 37 shows a repaired dural tear 4 days after surgery. The material interposed between the dural edges (D) is composed of
Explanation
REFERENCES: Cain JE Jr, Dryer RF, Barton BR: Evaluation of dural closure techniques: Suture methods, fibrin adhesive sealant, and cyanoacrylate polymer. Spine 1988;13:720-725.
Cain JE Jr, Lauerman WC, Rosenthal HG, Broom MJ, Jacobs RR: The histomorphologic sequence of dural repair: Observations in the canine model. Spine 1991;16:S319-S323.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 60
Which of the following is considered a contraindication to the use of a reverse total shoulder arthroplasty? Review Topic
Explanation
Question 61
A patient undergoes anterior spinal decompression through a left retroperitoneal approach as treatment of an L2 burst fracture. Following surgery, examination reveals the temperature of the right foot is cool when compared with the left foot. Which of the following neurologic structures has most likely been disrupted?
Explanation
Chapter 60, p. 777: “[After sympathetic denervation], at first the blood flow rises markedly because of lost vascular tone, but over a period of says to weeks the blood flow returns to almost normal because of progressive increase tone of the vascular musculature itself, thus compensating for the loss of sympathetic tone.”
Question 62
What factor is associated with a higher risk of dislocation after total hip arthroplasty?
Explanation
Dislocation after total hip arthroplasty is a multifactorial problem. Numerous risk factors may act independently or cumulatively to increase the risk of this complication. Previous hip surgery of any kind is associated with a twofold increased risk for dislocation. Other risk factors include female gender, impaired mental status, inflammatory arthritis, and older age. Numerous studies have shown a lower dislocation rate with a direct lateral approach, although surgical techniques such as capsular repair have
significantly lowered the incidence of dislocation after using the posterior approach. Metal-on-metal bearings have been associated with other complications such as adverse tissue reactions but are often used with larger-diameter bearings, which pose a lower risk of dislocation.
Question 63
The patient returns 1 year later to report curling of her toes and numbness on the plantar surface of her foot. What is the most likely cause of this condition?
Explanation
Radiographs reveal a Lisfranc fracture dislocation with fractures of the first and second metatarsals. Tenting of skin that is over a bony prominence is an orthopaedic emergency. The fracture dislocation should be reduced without delay. There is no evidence of compartment syndrome of the foot, but this may develop and monitoring is necessary. Toe deformity may develop on a delayed basis because of the subclinical presentation. Nerve irritation is not uncommon with dorsal midfoot surgical incisions. A positive Tinel test result over the midfoot in the distribution of the superficial common peroneal nerve is consistent with a stretch injury to this nerve. CRPS is usually associated with multiple nerve distributions and autonomic nerve findings such as cold hypersensitivity and hyperhidrosis.
RECOMMENDED READINGS
Benirschke SK, Meinberg EG, Anderson SA, Jones CB, Cole PA. Fractures and dislocations of the midfoot: Lisfranc and Chopart injuries. Instr Course Lect. 2013;62:79-91. PubMed PMID: 23395016. View Abstract at PubMed
Schepers T, Oprel PP, Van Lieshout EM. Influence of approach and implant on reduction accuracy and stability in lisfranc fracture-dislocation at the tarsometatarsal joint. Foot Ankle Int. 2013 May;34(5):705-10. doi: 10.1177/1071100712468581. Epub 2013 Jan 14. PubMed
PMID: 23637239. View Abstract at PubMed
Question 64
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child’s ability to walk in the future?
Explanation
REFERENCES: Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Tachdjian MO: The neuromuscular system: Cerebral palsy, in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 2, p 1621.
Question 65
Figure 109 is the radiograph of an 11-year-old boy who felt a snap in his right hip while jumping hurdles during track practice yesterday. He complains of pain to his right groin region and is walking with a limp. What physical examination test will cause the patient to experience the most discomfort?

Explanation
Question 66
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
REFERENCES: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Marsh JL, Weigel DP, Dirschl DR: Tibial plafond fractures: How do these ankles function over time? J Bone Joint Surg Am 2003;85:287-295.
Question 67
A patient in the recovery room has weakness of the extensor hallucis longus and tibialis anterior muscles following a total knee replacement. Initial management should consist of
Explanation
This is a rare
complication of TKA, and when conservative nonoperative measures do not lead to sufficient improvement in nerve function, consideration may be given to operative decompression of the peroneal nerve.
Question 68
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of Review Topic
Explanation
or tumor. Brace treatment is not required for this small curve unless future progression is demonstrated.
Question 69
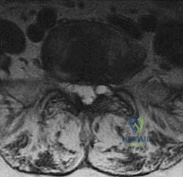
A 75-year-old man presents with worsening low back and bilateral leg pain. The pain worsens with ambulation and improves with sitting. On exam, he has strong DP and PT pulses. Straight leg raise is negative. A MRI of the lumbar spine is performed and is pictured in Figure A. On further questioning, which of the following is the patient also likely to report? Review Topic

Explanation
Lumbar spinal stenosis often results from degenerative changes of the intervertebral disc and facet joints which ultimately narrows the space available for the thecal sac and exiting nerve roots. Patients can present with neurogenic claudication, reported as worsening leg and/or back pain with ambulation and diminished walking capacity. MRI may demonstrate disc degeneration/bulging, hypertrophy of the ligamentum flavum and facet capsule, and narrowing of the central canal. Nonoperative management includes NSAIDs, PT and epidural steroid injections (ESI). Surgery is reserved for patients who have failed nonoperative measures and includes decompressive laminectomy with or without fusion depending on presence of instability.
Issack et al reviewed degenerative lumbar spinal stenosis. Unlike patients with vascular claudication, patients with neurogenic claudication are able to improve walking tolerance with postural changes, specifically with flexed-forward posture (such as leaning forward on a shopping cart). They are unable to improve their symptoms simply by cessation of walking. Patients with neurogenic claudication tend to lack the trophic changes of the skin on the legs/feet as well as diminished pulses characteristic of vascular disease.
Young et al reviewed the utilization of lumbar ESI for low back and leg pain. The authors concluded that lumbar ESI are a reasonable nonsurgical option to provide temporary symptomatic relief. Fluoroscopic guidance facilitates accurate placement of the injection into the epidural space, while its nonuse may lead to higher percentage of technical failures. Lastly, the transforaminal approach is more selective
than the interlaminar approach and can provide diagnostic information as well as symptom relief.
Figures A and B are T1 sagittal and T2 axial MR images, respectively, of the lumbar spine demonstrating significant central canal stenosis most notable at L4-L5 with broad disc protrusion, facet degeneration and infolding of the ligamentum flavum.
Incorrect
Responses:
Question 70
What is the most common physical examination finding in a patient with chronic painful spondylolysis? Review Topic
Explanation
Question 71
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Noll KH: The use of orthotic devices in adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:25-36.
Question 72
A 70-year-old man undergoes removal of an infected total hip arthroplasty (THA) and insertion of an articulating antibiotic-loaded spacer to treat a deep periprosthetic hip infection. While in a nursing home receiving intravenous antibiotics 3 weeks after surgery, the patient trips and falls. Examination reveals swelling in the mid and distal thigh, intact skin and neurovascular structures, and severe pain with knee or hip movement. Radiographs of the femur are shown in Figures 1 through 4. What is the most appropriate treatment for the fracture below the implant?
Explanation
This patient has a type C periprosthetic femoral fracture. The articulating spacer is not involved in the fracture, which is well distal to the implant. The most appropriate treatment is open reduction and internal fixation of the fracture. Traction is not appropriate for this fracture because the injury can be treated surgically despite the history of previous hip infection. Traction would also be needed for at least 5 weeks and would delay the surgical treatment of the periprosthetic fracture until the time of second-stage revision THA. The fracture is fairly distal, and revision to a longer antibiotic-loaded implant or uncemented stem is not suitable for this fracture pattern, because it extends well past the isthmus. A femoral stem in the distal fragment would provide little stability for the fracture. Removal of the articulating spacer and reimplantation using a long-stem fluted uncemented hip replacement is not appropriate, because it would be premature to reimplant the man's hip while he is still receiving treatment for a deep hip infection.
Question 73
-What do the bone scan findings represent?
Explanation
The bone scan shows no uptake of the tracer, which indicates osteonecrosis. The MRI scan of the shoulder reveals sepsis with a focus on osteomyelitis. A CT scan will not add more useful information and will delay treatment. A sequestrum is a piece of dead bone that has become separated from normal/solid bone during the osteonecrosis process. It appears as a radiopacity on plain radiograph. The involucrum is new bone formed by an elevated periosteum and can be seen on radiograph.
Heterotopic ossification appears as radiopacity within the soft tissues. Late recognition of pediatric shoulder sepsis has been reported, and damage to the joint can be extensive. Septic joints are one of the few true orthopaedic emergencies. The methodology of drainage in shoulder sepsis is controversial (aspiration vs open drainage vs arthroscopic lavage), but the joint must be drained and sterilized to prevent cartilage damage.
Question 74
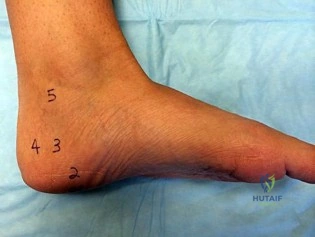
A B Figures 82a and 82b are the clinical photograph and radiograph of a 60-year-old man with a 30-year history of diabetes complicated by borderline chronic renal failure, heart failure controlled by medication, and bilateral lower extremity neuropathy. He is currently wheelchair bound because of his cardiopulmonary limitations, but uses his legs for transfers. He has had a progressive left ankle deformity that has progressed to the point at which he cannot use his leg for pivot transfers. He is adamant that something should be done to improve his living situation. Which surgical option can best achieve his goal of using the leg for transfers?

Explanation
The indications for surgery in a Charcot joint are an unbraceable deformity or recurrent ulceration despite use of adequate bracing. Any significant varus/valgus deformity of the ankle or hindfoot (as in this patient) is unbraceable, whereas midfoot Charcot deformities usually can be treated nonsurgically. The goal of surgery is to provide a stable aligned foot and ankle to permit activities and reduce risk for recurrent ulceration. This does not mean that there has to be a radiographic fusion because many patients with diabetes achieve a stable nonunion without pain. The only surgical construct that will provide long-term inherent stability and alignment in this situation is use of a hindfoot fusion rod. It provides better stability and purchase than screw fixation and can be left in indefinitely (unlike an external fixator).
RECOMMENDED READINGS
Dalla Paola L, Volpe A, Varotto D, Postorino A, Brocco E, Senesi A, Merico M, De Vido D, Da Ros R, Assaloni R. Use of a retrograde nail for ankle arthrodesis in Charcot neuroarthropathy: a limb salvage procedure. Foot Ankle Int. 2007 Sep;28(9):967-70. PubMed PMID: 17880869. View Abstract at PubMed
Pinzur MS. Benchmark analysis of diabetic patients with neuropathic (Charcot) foot deformity. Foot Ankle Int. 1999 Sep;20(9):564-7. PubMed PMID: 10509683. View Abstract at PubMed Pinzur M. Surgical versus accommodative treatment for Charcot arthropathy of the midfoot. Foot Ankle Int. 2004 Aug;25(8):545-9. PubMed PMID: 15363375. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 83 THROUGH 87

Figures 83a and 83b are the clinical photographs of a 42-year-old woman with a BMI of 31 who has had a 1-year history of right heel pain.
A
B
Question 75
A 15-year-old boy has a fracture of the proximal tibia extending from the apophysis of the tubercle up through the posterior part of the proximal tibial epiphysis and into the joint. What is the most likely mechanism of injury?
Explanation
Question 76
What are the five most common tumors that metastasize to bone?
Explanation
REFERENCES: Frassica FJ, Gitelis S, Sim FH: Metastatic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
CA, January/February 2000, vol 50, no. 1 (Cancer Statistics).
Question 77
Which of the following plain radiographic views of the shoulder best reveals a Hill-Sachs lesion of the humeral head?
Explanation

Question 78
Figures A through C are the radiograph and CT scans of a 42-year-old man who sustained an injury to both of his ankles and underwent surgical repair 2 weeks prior to presentation to your office. One ankle is healing well. On the contralateral side, he reports pain and restricted ankle range of motion. Management should consist of
Explanation
Question 79
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of
Explanation
REFERENCE: Simon MA, Springfield DA: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, ch 29.
Question 80
An 8-year-old boy with severe hemophilia A (factor VIII) and no inhibitor is averaging eight transfusions per month for bleeding into the right ankle. Examination shows synovial hypertrophy; range of motion consists of 0° of dorsiflexion and 20° of plantar flexion. The patient’s knees, elbows, and left ankle have no restriction of motion. Standing radiographs of the right ankle are shown in Figure 18. Management should consist of
Explanation
REFERENCES: Greene WB: Synovectomy of the ankle for hemophilic arthropathy. J Bone Joint Surg Am 1994;76:812-819.
Greene WB: Chronic inflammatory arthridities and diseases related to the hematopoietic system, in Drennan JC (ed): The Child’s Foot and Ankle, New York, NY, Raven Press, 1992, pp 461-482.
Question 81
Figures 13a and 13b show the MRI scans of a 70-year-old patient who has a posterior calf mass. Examination reveals that the mass extends to the midcalf level. A biopsy specimen reveals a high-grade soft-tissue sarcoma. Metastatic work-up shows no lesions. Management should consist of
Explanation
REFERENCES: Lindberg RD, Martin RG, Romsdahl MM, et al: Conservative surgery and post-operative radiotherapy in 300 adults with soft tissue sarcoma. Cancer 1981;47:2391-2397.
Sim FT, Frassica FS, Frassica DA: Soft tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Rosenberg SA, Tepper J, Glatstein E, et al: The treatment of soft-tissue sarcomas of the extremities: Prospective randomized evaluations of (1) limb sparing surgery plus radiation therapy compared with amputation and (2) The roll of adjuvant chemotherapy. Am Surg 1982;196:305-315.
Question 82
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Explanation
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. These arteries arise from the popliteal artery. If this artery is not adequately mobilized, a gastrocnemius soleus flap can be devascularized.
Question 83
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
REFERENCES: Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 84
A 52-year-old woman slips in her bathroom and strikes her right hand on a cabinet. She notes swelling, ecchymosis, and pain with attempted motion. There are no open wounds. Radiographs are shown in Figures 5a through 5c. What is the most appropriate treatment?
Explanation
REFERENCES: Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Kozin SH, Thoder JJ, Lieberman G: Operative treatment of metacarpal and phalangeal shaft fractures. J Am Acad Orthop Surg 2000;8:111-121.
Question 85
83A B year-old with the injury pattern seen on the left lower extremity in CT images in Figures 83a and 83b
Explanation
In Figures 79a through 79c, CT images show a Schatzker IV medial tibial plateau fracture. This fracture is best treated with a medial incision and posteromedial plate, which will function as an antiglide or buttress plate. Percutaneous screw fixation is insufficient for this injury. Lateral fixation is not needed, and in many instances will not capture the medial fragment even with locking fixation. ?
In Figures 80a and 80b, the patient has a fairly well-aligned bicondylar tibial plateau fracture. The lateral joint is significantly depressed, necessitating open reduction and elevation with stabilization. The posteromedial fragment is often missed with single lateral locked plating and is best treated with a posteromedial plate. Percutaneous fixation does not address the joint depression.
In Figure 81, the patient has a classic split depression lateral tibial plateau fracture (Schatzker II). The joint must be reduced from a lateral approach and then supported and stabilized. Definitive ORIF with a lateral plate can be performed when appropriate.
In Figures 82a and 82b, the radiographs show a Schatzker I nondisplaced tibial plateau fracture that is amenable to percutaneous screw fixation if surgical intervention is required. The fracture pattern can be treated surgically, although, considering the comminution at the inferior aspect, late displacement could occur. The other surgical approaches mentioned are not required for this injury.
In Figures 83a and 83b, a lateral split depression tibial plateau fracture is noted (similar to the fracture seen in Figure 81). The same logic applies.
RECOMMENDED READINGS
Higgins TF, Kemper D, Klatt J. Incidence and morphology of the posteromedial fragment in bicondylar tibial plateau fractures. J Orthop Trauma. 2009 Jan;23(1):45-51. doi: 10.1097/BOT.0b013e31818f8dc1. PubMed PMID: 19104303. View Abstract at PubMed Berkson EM, Virkus WW. High-energy tibial plateau fractures. J Am Acad Orthop Surg. 2006 Jan;14(1):20-31. Review. PubMed PMID: 16394164. View Abstract at PubMed
Barei DP, O'Mara TJ, Taitsman LA, Dunbar RP, Nork SE. Frequency and fracture morphology of the posteromedial fragment in bicondylar tibial plateau fracture patterns. J Orthop Trauma. 2008 Mar;22(3):176-82. doi: 10.1097/BOT.0b013e318169ef08. PubMed PMID: 18317051.
View Abstract at PubMed
Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg Am. 2011 Aug 17;93(16):1548-59. PubMed PMID: 22204013. View Abstract at PubMed
Weil YA, Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Posteromedial supine approach for reduction and fixation of medial and bicondylar tibial plateau fractures. J Orthop Trauma. 2008 May-Jun;22(5):357-62. doi: 10.1097/BOT.0b013e318168c72e. PubMed PMID:
Question 86
What is the dominant component of articular cartilage extracellular matrix by weight?
Explanation
REFERENCES: Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Inst Course Lect 1998;47:487-504.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 3-18.
Question 87
A 32-year-old recreational basketball player underwent a successful anterior cruciate ligament (ACL) reconstruction using hamstring autograft approximately 15 months ago. His chart notes that he has good functional knee outcome scores as tested by his physical therapist. However, he has not returned to play despite being cleared by his physician 3 months ago. After successful ACL reconstruction, which of the following factors has shown to contribute the greatest influence on a player's decision to return to sport? Review Topic
Explanation
The return to their preinjury level of sport is frequently expected within 1 year after anterior cruciate ligament (ACL) reconstruction, yet many athletes do not achieve this milestone. Having a previous ACL reconstruction to either knee, poorer hop-test symmetry and subjective knee function, and more negative psychological responses were associated with not returning to the preinjury level sport. Fear of reinjury is considered one of the most common reasons cited for a postoperative reduction in or
cessation of sports participation.
Tjong et al. conducted a qualitative study of 31 patients, aged 18 to 40 years, to understand the factors influencing a patient's decision to return to his or her preinjury level of sport after ACL reconstruction. They found 3 overarching factors what largely influenced their decision to return to the preinjury sport: fear, lifestyle changes, and innate personality traits. This highlighted the importance of recognizing and addressing the psychological factors and lifestyle changes that significantly contribute to a patient's postoperative decision to return to sport.
Ardern et al. investigated the return-to-sport rates at 2 years after ACL reconstruction in athletes. At 2 years after surgery, 66% were playing sport, with 41% playing their preinjury level of sport and 25% playing a lower level of sport. Demographics, physical function, and psychological factors were supported as the most important influencing factors for the return to their preinjury level of sport.
Incorrect Answers:
Question 88
- Which of the following acetabular/femoral head components would be expected to show an optimal combination of linear and volumetric wear?
Explanation
Question 89
A 2-year-old child has been referred for management of congenital kyphosis. Neurologic examination is normal, and radiographs show a type I congenital kyphosis. Which of the following anomalies is seen in the MRI scan shown in Figure 6?
Explanation
REFERENCES: Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Mimaston MJ: Occult intraspinal anomalies and congenital scoliosis. J Bone Joint Surg Am 1984;66:588-601.
Question 90
Figures 1 through 4 are the CT scans and intraoperative image of a 17-year-old boy who sustained a gunshot wound to his knee. What is the most appropriate definitive surgical management for his articular cartilage defect?
Explanation
Question 91
Why is tendon considered an anisotropic material?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Lu L, Kaufman KR, Yaszemski MJ: Biomechanics, in Einhorn TA, O’Keefe RJ,
Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, in press.
Question 92
A 15-year-old girl has left knee pain and an enlarging mass in the distal thigh. AP and lateral radiographs are shown in Figures 52a and 52b, and a biopsy specimen is shown in Figure 52c. What is the most likely diagnosis?
Explanation
REFERENCES: Unni KK: Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 93
A 48-year-old man who is scheduled to undergo total knee replacement has an X-linked clotting disorder that leads to abnormal bleeding and recurrent, spontaneous hemarthrosis. Before undergoing surgery, he should have replacement therapy of
Explanation
Question 94
A 55-year-old woman has slowly increasing pain at the distal end of her little finger that is exacerbated by cold temperatures. She denies any history of trauma to her hands and is employed as a school teacher. The histology of the resected specimen is shown in Figure 71. What is the most likely diagnosis?
Explanation
REFERENCES: Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
McDermott EM, Weiss AP: Glomus tumors. J Hand Surg Am 2006;31:1397-1400.
Question 95
Decreased activity of which of the following proteins may be predictive of an aggressive soft-tissue sarcoma?
Explanation
REFERENCE: Benassi MS, Magagnoli G, Ponticelli F, et al: Tissue and serum loss of metalloproteinase inhibitors in high grade soft tissue sarcomas. Histol Histopathol 2003;18:1035-1040.
Question 96
Progressive paralysis is most likely to be seen in association with what type of congenital vertebral abnormality?
Explanation
REFERENCES: McMaster MJ, Singh H: Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-1383.
Dubousset J: Congenital kyphosis and lordosis, in Weinstein SL (ed): The Pediatric Spine: Principles and Practice, ed 1. New York, NY, Raven Press, 1994, pp 245-258.
Question 97
Figures 28a and 28b show the sagittal and axial lumbar MRI scans of a 72-year-old man who reports dull aching back pain that spreads to his legs, calves, and buttocks. He has had the pain for several years and it is precipitated by standing and walking and relieved by sitting. His symptoms have been worsening over the past year and he notes that he is leaning forward while walking to help relieve his symptoms. He has had no treatment to date. What is his prognosis if he chooses to pursue nonsurgical management for this condition?
Explanation
REFERENCES: Amundsen T, Weber H, Nordal HJ, et al: Lumbar spinal stenosis: Conservative or surgical management? A prospective 10-year study. Spine 2000;25:1424-1435.
Hilibrand AS, Rand N: Degenerative lumbar stenosis: Diagnosis and management. J Am Acad Orthop Surg 1999;7:239-249.
Tadokoro K, Miyamoto H, Sumi M, et al: The prognosis of conservative treatments for lumbar spinal stenosis: Analysis of patients over 70 years of age. Spine 2005;30:2458-2463.
Question 98
During a posterior approach to the right Achilles tendon, the surgeon encounters a nerve running with the small saphenous vein as shown in Figure 22. This nerve innervates what part of the foot?
Explanation
REFERENCES: Aktan Ikiz ZA, Ucerler H, Bilge O: The anatomic features of the sural nerve with an emphasis on its clinical importance. Foot Ankle Int 2005;26:560-567.
Lawrence SJ, Botte MJ: The sural nerve in the foot and ankle: An anatomic study with clinical and surgical implications. Foot Ankle Int 1994;15:490-494.
Question 99
9 degress Celsius, serum WBC is 14,000, and his C-reactive protein is elevated. He reports that he uses IV heroin. A coronal 3D CT scan of the left clavicle is shown in Figure B. Joint aspiration shows many grams stain positive organisms. Which of the following organisms is the most likely pathogen?

Explanation
Ross et al states "Staphylococcus aureus is now the major cause of
sternoclavicular septic arthritis in intravenous drug users. Pseudomonas aeruginosa infection in injection drug users declined dramatically with the end of an epidemic of pentazocine abuse in the 1980s."
The referenced article by Goldin et al is from the New England Journal of Medicine reports that all of their cases of SC joint septic arthritis were in intravenous drug abusers and that P. aeruginosa grew out of 3 patients and S. aureus grew out of 1 patient.
A more recent article by Abu Arab et al reported that Staph aureus was most common even in IV drug users. The review article by Higginbotham and Kuhn note that risk factors for SC joint septic arthritis include hemodialysis, immunocompromise, alcoholism, and HIV. Neisseria gonorrhoeae, fungal, and candida present in HIV patients.
Treatment is I&D and appropriate antibiotics, although aspiration and abx have shown some success too. CT and MRI are useful in diagnosis, and open biopsy or aspiration is recommended for definitive diagnosis.
A 30-year-old man presents with a distal third tibia fracture that has healed in 25 degrees of varus alignment. The patient is at greatest risk of developing which of the following conditions as a result of this malunion?
Degenerative lumbar spine changes
Ipsilateral ankle pain and stiffness
Ipsilateral hip joint degenerative changes
Contralateral hip joint degenerative changes
Ipsilateral medial knee degenerative changes Correct answer: 2
A significant malunion of the distal tibia has important consequences for patient outcome, including pain, gait changes, and cosmesis.
The first referenced article by Milner et al looked at long-term outcomes of tibial malunions and noted that varus malunion led to increased ankle/subtalar stiffness and pain regardless of the amount of radiographic degenerative changes.
The second referenced article by Puno et al reinforced the concept of decreased functional outcomes of the ankle with tibial malunions, and noted
that other lower extremity joints (ipsilateral and contralateral) do not have increased rates of degeneration from such a malunion.
A 33-year-old man sustains a femur fracture in a motorcycle accident. AP and lateral radiographs are provided in Figure A. Prior to surgery, a CT scan of the knee is ordered for preoperative planning. Which of the following additional findings is most likely to be discovered?

Tibial eminence fracture
Sagittal plane fracture of the medial femoral condyle
Schatzker I tibia plateau fracture
Coronal plane fracture of the lateral femoral condyle
Axial plane fracture through the medial femoral condyle Correct answer: 4
The "Hoffa fracture" is a coronal plane fracture of the femoral condyle that is often missed on plain radiographs of supracondylar and intercondylar femur fractures. It involves the lateral condyle more frequently than the medial.
Identification is important as it may impact operative planning and likely require screw fixation in the anteroposterior plane.
Nork et al. reviewed 202 supracondylar-intercondylar distal femoral fractures and found a 38% prevalence of associated coronal plane fractures. The authors recommend CT scan imaging of all supracondylar and intercondylar fractures.
Ostermann et al reported on 24 unicondylar fractures of the distal femur treated with open reduction internal fixation with a screw construct. Twenty-
three patients acheived satisfactory results at 5 year follow-up. Illustrations A and B are another example of a supracondylar femur fracture with an associated Hoffa fracture identified on CT scan.

A 35-year-old woman presents with an elbow injury which includes a coronoid fracture involving more than 50%, a comminuted
radial head fracture, and an elbow dislocation. What is the most appropriate treatment?
closed reduction and early range of motion
radial head resection and lateral collateral ligament reconstruction
radial head resection and coronoid open reduction internal fixation
radial head arthroplasty and coronoid open reduction internal fixation
radial head arthroplasty, coronoid open reduction internal fixation, and lateral collateral ligament repair
A terrible triad of the elbow includes dislocation of the elbow with associated fractures of the radial head and the coronoid process. Ring et al. stressed that these injuries are prone to complications and advised against resection of the radial head due to instability, and instead recommended a radial head replacement if too comminuted for ORIF. Coronoid fractures compromise elbow stability as well and require open reduction and internal fixation as with the lateral collateral ligament. McKee et al. showed stable elbows in 34/36 with mean Mayo elbow score of 88 when the standard protocol of coronoid ORIF, radial head repair/replacement, and LCL repair were employed.
The talocrural angle of an ankle mortise x-ray is formed between a line perpendicular to the tibial plafond and a line drawn:
perpendicular to the medial clear space
parallel to the talar body
between the tips of the malleoli
perpendicular to the shaft of the fibular
parallel to the subtalar joint Correct answer: 3
The talocrural angle is formed by the intersection of a line perpendicular to the plafond with a line drawn between the malleoli (average = 83+/-4deg). When the lateral malleolus is shortened secondary to fracture, this can lead to increased talocrural angle. This malunion leads to lateral tilt of the talus.
Phillips et al looked at 138 patients with a closed grade-4 supination-external rotation or pronation-external rotation ankle fracture. Although the conclusions were limited due to poor follow up, they found the difference in the talocrural angle between the injured and normal sides was a statistically significant radiographic indicator of a good prognosis.
Pettrone et al looked at a series of 146 displaced ankle fractures, and the effect of open or closed treatment, and internal fixation of one or both malleoli. They found open reduction proved superior to closed reduction, and in bimalleolar fractures open reduction of both malleoli was better than fixing only the medial side.
Illustrations A and B are demonstrations of the talocrural angle.
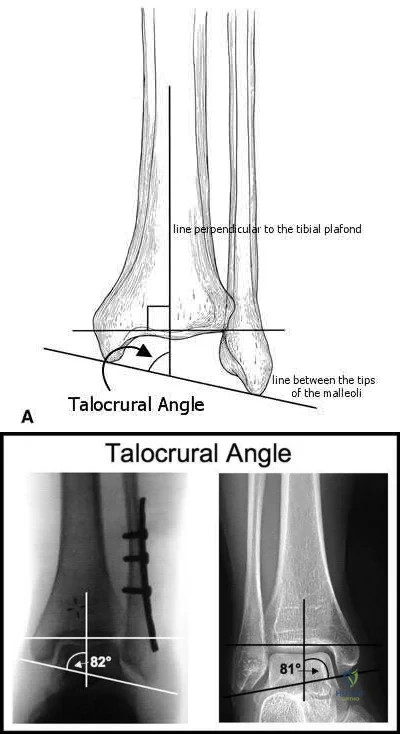
A 33-year-old male sustains the injury shown in Figure A. He is initially treated with a spanning external fixator followed by definitive open reduction internal fixation of the tibia and fibula. His wounds healed without infection or other complications. Two years following surgery, which of the following parameters will most likely predict a poor clinical outcome and inability to return to work?

Joint line restoration
Degree of fracture displacement
Time before definitive ORIF
Open fracture
Lower level of education Correct answer: 5
Lower level of education is the parameter that correlated most closely with a poor clinical outcome and inability to return to work.
To determine what fracture- and patient-specific variables affect outcome, Williams et al evaluated 29 patients with 32 tibial plafond fractures at a minimum of 2 years from the time of injury. Outcome was assessed by four independent measures: a radiographic arthrosis score, a subjective ankle score, the Short Form-36 (SF-36), and the patient’s ability to return to work. The four outcome measures did not correlate with each other. Radiographic arthrosis was predicted best by severity of injury and accuracy of reduction. However, these variables did not show any significant relationship to the clinical ankle score, the SF-36, or return to work. These outcome measures were more influenced by patient-specific socioeconomic factors. Higher ankle
scores were seen in patients with college degrees and lower scores were seen in patients with a work-related injury. The ability to return to work was affected by the patient’s level of education.
Pollak et al performed a retrospective cohort analysis of pilon fractures. Patient, injury, and treatment characteristics were recorded. The primary outcomes that were measured included general health, walking ability, limitation of range of motion, pain, and stair-climbing ability. A secondary outcome measure was employment status. Multivariate analyses revealed that presence of two or more comorbidities, being married, having an annual personal income of less than $25,000, not having attained a high-school diploma, and having been treated with external fixation with or without limited internal fixation were significantly related to poorer results as reflected by at least two of the five primary outcome measures.
What is the most appropriate treatment for a 17-year-old boy who sustained a gunshot wound to his forearm from a handgun with a muzzle-velocity of 1000 feet/second if he is neurovascularly intact and radiographs reveal no fracture?
Irrigation and local wound care in the emergency department
Emergent irrigation and debridement in the operating room with vacuum-assisted wound closure
Emergent irrigation and debridement in the operating room with 7 days of intravenous antibiotics
Wound closure in the emergency department with follow-up wound check in 1 week
Exploration and removal of all bullet fragments in the emergency department and 10 day course of oral antibiotics
The question refers to appropriate management of a gunshot wound to the forearm. The first question that must be answered when evaluating gunshot injuries is whether the gunshot is low velocity or high velocity. Low-velocity wounds are less severe, are more common in the civilian population, and are typically attributed to bullets with muzzle velocities below 1,000 to 2,000 feet per second. Tissue damage is usually more substantial with higher-velocity (greater than 2,000 to 3,000 fps) military and hunting weapons. In this question, a muzzle velocity of 1,000 ft/sec is provided. Low velocity injuries with stable, non-operative fractures can be treated with local wound care.
The two referenced articles offer guidance for treating low-velocity gunshot injuries with stable, non-operative fracture patterns. The first article by Geissler et al is a retrospective study comparing 25 patients that prospectively received local irrigation and debridement, tetanus prophylaxis and a long acting cephalosporin intramuscularly to a random retrospective sample of 25 patients with similar ballistic-induced fractures and wounds managed by local debridement and 48h of intravenous antibiotics. One infection occurred in each group, requiring further therapy. It was concluded that patients with low-velocity gunshot induced fractures can be managed without the use of short-term intravenous antibiotics with no increased risk of infection.
In the second study, Dickey et al evaluated the efficacy of an outpatient management protocol for patients with a gunshot-induced fracture with a stable, non-operative configuration. 41 patients with a grade I or II open, nonoperative fracture secondary to a low-velocity bullet were treated with 1gm of cefazolin administered in the emergency room and a 7-day course of oral cephalexin. No patient developed a deep infection. Thus, local I&D, tetanus, and oral antibiotics for 2-3 days is adequate for low velocity gunshot wounds.
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?
pulselessness
pallor
paresthesia
paralysis
increasing analgesia requirement Correct answer: 5
Although pain, pallor, paresthesia, paralysis, and pulselessness are all possible signs and symptoms of compartment syndrome in children with fractures, studies have shown increasing analgesia requirement is more sensitive.
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of
compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
A 45-year-old man sustains the injury seen in Figures A and B following a motor vehicle accident. Postoperative radiographs are seen in Figures C and D. Which of the following is the most accurate when comparing outcomes between intramedullary nailing (IMN) and open reduction internal fixation (ORIF) for this injury?

Union rates at one year are higher with ORIF
Infection rates are higher with IMN
Functional shoulder outcomes at one year are equivalent with IMN and ORIF
Iatrogenic radial nerve injury rate is higher with ORIF
Shoulder stiffness rates at one year are equivalent with IMN and ORIF Correct answer: 3
Although shoulder pain and stiffness is increased following IMN compared to ORIF, functional outcome scores at one year have been shown to be equivalent
in both treatment groups.
Diaphyseal humeral shaft fractures outcomes following IMN and ORIF are under further investigation. Diaphyseal humeral shaft fractures have historically been treated with ORIF, however proponents for IMN cite benefits of less periosteal stripping and soft tissue dissection. Recent investigations have shown outcomes with regard to nonunion, infection, re-operation, and nerve palsy appear equivalent between both groups. Rates of shoulder stiffness and shoulder pain have been demonstrated to be higher in IMN compared to ORIF. American Shoulder and Elbow Scores (ASES) have shown no difference at one year post-operatively.
Bhandari et al. performed a meta-anaylsis of 3 prospective randomized trials. They found lower rates of re-operation and shoulder impingement with ORIF of humeral shaft fractures.
Wali et al. performed a prospective randomized study of IMN or ORIF on 50 patients with mid-diaphyseal humeral shaft fractures. They found IMN had shorter operative time, shorter hospital stay, and lower blood loss. They found no difference in union rates, complication, or shoulder functional outcomes scores. They conclude IMN to be an effective option for treating mid-diaphyseal humeral shaft fractures.
Heineman et al. have recently conducted an update on their meta-analysis to include more recent randomized studies. With the inclusion of newer studies the author found a statistically significant increase in total complication rate with the use of IM nailing compared with ORIF. The authors found no significant difference between the two treatment modalities for the secondary outcomes (nonunion, infection, nerve palsy, re-operation).
Figures A and B show a diaphyseal humeral shaft fracture. Figure C and D show postoperative radiographs following intramedullary nailing of a humeral shaft fracture.
Incorrect Answers:
A 25-year-old female presents complaining of progressive anteromedial pain in her left ankle. She underwent operative fixation 5 months prior at an outside hospital. The operative report indicated that, due to anterior fracture blisters, a direct medial incision was utilized, centered over the posterior colliculus of the medial malleolus, without violation of the deltoid ligament. A radiograph and computed tomographic scan of her initial injury are shown in Figures A and B, respectively. On exam, she has well-healed incisions, exhibits no tenderness to palpation over her hardware, but does endorse pain with deep palpation along the anteromedial joint line. Figure C shows an anteroposterior left ankle radiograph taken today. Labs are obtained and reveal a white blood cell count of 9.0 k/uL (reference range 4.5-11.0 k/uL) and a C-reactive protein value of 0.8 mg/dL (<0.9 mg/dL). What is the next best step in managing her problem?

Syndesmotic fixation
Intra-articular corticosteroid injection
Referral to physical therapy
Surgical correction of malunion
Removal of hardware Correct answer: 4
This patient sustained a supination-adduction (SAD) injury with a vertical shear fracture of her medial malleolus and a fibular avulsion fracture. She sustained a medial plafond articular impaction injury that was not addressed at the time of surgery.
In SAD injuries, supination of the foot is combined with inward rotation at the ankle, adduction of the hindfoot, and inversion of the forefoot. This results in the following sequence of events: 1. Talofibular sprain or distal fibular avulsion (equivalent to Weber A). 2. Vertical medial malleolus fracture as the talus strikes the tibia. Associated injuries may include osteochondral damage to the talus and marginal impaction of the medial plafond. It is important to evaluate the medial plafond for articular impaction. When present, an arthrotomy must be performed, typically utilizing an anteromedial incision, with direct visualization of the articular surface to restore the joint line appropriately.
Weber et al. provided a review article on corrective osteotomies for malleolar fracture malunions. They stress that malunions can lead to ankle instability, abnormal load transfer, and post-traumatic arthritis. They conclude that corrective osteotomies that restore anatomical alignment show good results in long-term follow-up.
Perera et al. provided additional commentary on the surgical reconstruction of malunited ankle fractures. The authors emphasize the link between malunion and poor outcomes. They state that successful salvage procedures involve a clear understanding of the deformity, careful preoperative planning, and a solid understanding of reconstructive techniques. They provide several instructive case examples in their review.
McConnell et al. provided a discussion on SAD ankle fractures at their institution and emphasized the importance of recognizing marginal impaction of the tibial plafond when treating these injuries. Of 800 ankle fractures identified over a 5-year period, 44 were SAD injuries, 19 of the 44 displayed a vertical shear fracture of the medial malleolus, and 8 of the 19 demonstrated marginal impaction of the tibial plafond. These 8 impaction injuries were treated with open reduction internal fixation with elevation of the articular impaction; all had good to excellent outcomes without arthritic changes at last
follow-up.
Figure A is an anteroposterior left ankle radiograph demonstrating a SAD injury with a vertical shear fracture of the medial malleolus, a fibular avulsion fracture, and articular impaction of the medial tibial plafond. Figure B is a coronal CT demonstrating articular impaction of the medial plafond. Illustration A is an intra-operative photograph with the medial malleolus retracted allowing inspection of the articular surface; mild anteromedial plafond impaction is present.
Incorrect Answers:

A 90-year-old female slips and falls at home. She is a community ambulator and has no medical problems. She reports right hip pain at this time. Injury radiographs are shown in Figures A & B. Delay of more than 48 hours may result in:

Increased intraoperative time
Increased 30-day mortality
No impact on the rate of postoperative pneumonia
Higher rates of blood transfusion
Increased risk of post-operative infection Correct answer: 2
Figures A & B demonstrate a right, unstable intertrochanteric femur fracture. Surgical stabilization within 48 hours improves short-term and 30-day mortality.
Hip fractures are common and mortality rates vary. In the elderly, mortality rates may reach 10% at 1-month, 20% at 4-months, and 30% at 1-year. Time to surgery has found to be a decisive factor. A pre-operative delay may lead to an increase in mortality and adversely influence other clinical outcomes.
Clinical guidelines recommend immediate operative stabilization, given the patient is medically fit for surgery.
Nyholm et al. performed a retrospective study of the Danish Fracture Database to investigate whether a surgical delay increases 30-day and 90-day mortality rates for patients with proximal femoral fractures. The 30-day and 90-day mortalities were 10.8% and 17.4%, respectively. The risk of 30-day mortality increased with increasing time intervals of more than 12 hours, 24 hours, and more than 48 hours. 90-day mortality increased with a surgical delay of more than 24 hours. They conclude that rapid surgical treatment should be performed by attending orthopaedic surgeons.
Moja et al. performed a meta-analysis and meta-regression to assess the relationship between surgical delay and mortality in elderly patients with a hip fracture. They analyzed 35 independent studies with 191,873 patients and 34,448 deaths. The majority of studies had a cut-off of 48 hours. They report that early hip surgery was associated with a lower risk of death and pressure sores. They conclude that early hip fracture surgery appears to provide a survival benefit compared to later intervention.
Rodriguez-Fernandez et al. performed a study examining 2 groups with hip fractures. The first group was studied retrospectively and had an average delay of surgical treatment of more than 1-week while the second group was studied prospectively, and had surgical treatment within 48 hours. They found a larger number of complications in the group with a delay in surgical treatment. They conclude that elderly patients with hip fractures should be treated as soon as their medical condition permits.
Figures A and B are the AP and lateral radiographs demonstrating a right, unstable intertrochanteric femur fracture. Illustration A is an intertrochanteric femur fracture, stabilized with a cephalomedullary nail.
Incorrect Answers:

A 22-year-old healthy left hand dominant male presents to the ED with left shoulder pain after falling from an ATV. Figure A is the radiograph of his left clavicle. He is neurovascularly intact and there is no evidence of skin tenting or open fracture. Which of the following most predisposes this patient to nonunion?

Diaphyseal fracture
Fracture displacement
Age
Male Gender
Injury involving the dominant extremity Correct answer: 2
Displaced clavicle fractures are associated with higher rates of nonunion.
Nonunion occurs in roughly 5-6% of clavicle fractures and can result in slower functional return, poor cosmesis and muscle fatigability. Clavicle fractures can be sub-classified using the Allman classification into medial, diaphyseal, and lateral injuries (Illustration A). The Neer classification for diaphyseal injuries describes fractures as "nondisplaced" (less than 100% displacement) and "displaced" (greater than 100% displacement).
Robinson et al. performed a prospective cohort study to identify risk factors for nonunion after nonoperative management of clavicle fractures. The overall nonunion rate was 6.2% and was highest in lateral third fractures (11.5%).
Diaphyseal fractures had the lowest nonunion rate (4.5%). Additionally, the authors found that the risk for nonunion was increased by advancing age, female gender, fracture displacement, and comminution.
Jorgensen et al. performed a systemic review of the literature looking for predictors of non-union and malunion in mid shaft clavicle fractures treated non-operatively. They found fracture comminution, displacement, older age, female gender, and the presence of smoking to be his factors for non-union. Of these, displacement was the most likely factor that can be used to predict nonunion.
Figure A demonstrates a displaced left clavicle diaphyseal fracture. Note that the medial fragment is displaced superiorly by the deforming force of the sternocleidomastoid. Illustration A represents the Allman classification.
Illustration B demonstrates the deforming forces acting on the clavicle.
Incorrect Answers:
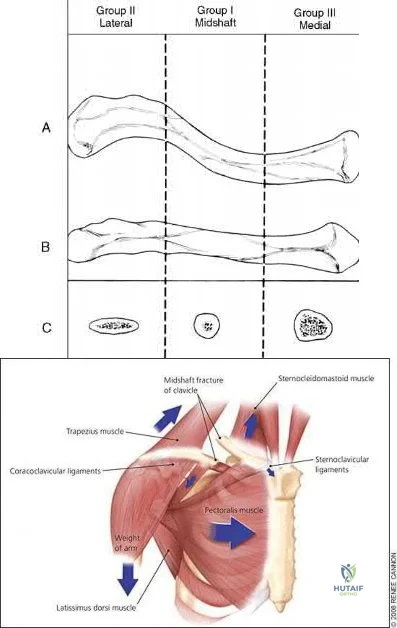
A 24-year-old male presents with ankle pain after being involved in a motor vehicle accident. His injury radiograph is shown in Figure A. Which of the following has been shown to contribute to the development of post-traumatic arthritis in this injury pattern?

Initial superficial zone cartilage cell death via apoptosis at the fracture margins
Initial superficial zone cartilage cell death via apoptosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis remote from the fracture margins
Initial superficial zone cartilage cell death via necrosis at the fracture margins
Delayed superficial zone cartilage cell death via necrosis at the fracture margins
Figure A demonstrates a tibial plafond fracture. Initial superficial zone cartilage cell death via necrosis at the fracture margins has been shown to contribute to post-traumatic arthritis.
Post-traumatic osteoarthritis typically occurs after an intra-articular fracture. Impacted chondrocytes die by either necrosis or apoptosis, which have both been implicated in post-traumatic osteoarthritis. Initial cell death in the superficial cartilage zones at the fracture margins occurs by necrosis. Apoptosis occurs in a delayed fashion and is mitigated by several bioactive agents.
Apoptosis also affects the superficial cartilage zones near the fracture margins. Deep cartilaginous zones and areas away from the fracture margins do not seem to be involved in these processes.
McKinley et al. performed a review of the basic science of intra-articular fractures and posttraumatic osteoarthritis. They report that initial damage to the cartilage in combination with the ensuing pathomechanical and pathobiologic response of the cartilage after a fracture contribute to posttraumatic arthritis. Chronic abnormal joint loading is also thought to contribute to this process as well. They conclude that the relative contribution of each is unknown.
Tochigi et al. performed a study to determine the distribution and progression of chondrocyte damage after intra-articular ankle fractures. They harvested 7 normal human ankles and subjected them to impaction. They found that immediate superficial zone chondrocyte death was greater in fracture-edge regions than on-fracture regions. Subsequent cell death over the next 48 hours was significantly higher in fracture-edge regions as well. They conclude that cartilage damage in intra-articular fractures was characterized by chondrocyte death at fracture margins.
Figure A is an ankle mortise radiograph demonstrating an intra-articular tibial plafond fracture.
Incorrect Answers:
A 35-year-old male presents with left knee pain after sustaining the injury seen in Figure A. He is neurovascularly intact and can perform a straight leg raise, but has pain with passive range of motion. Figures B and C show an anteroposterior and lateral radiograph of the left knee, respectively. 175 cc of saline is injected into the superolateral quadrant with no egress of fluid from the inferolateral
laceration. What percentage of traumatic arthrotomies would be detected with this test?

Question 100
below depict the AP and lateral radiographs obtained from a year-old man with long-standing right knee osteoarthritis and pain that is unresponsive to nonsurgical treatment. The patient undergoes navigated cruciate-retaining right total knee arthroplasty. After surgery, this patient continues to experience pain and swelling of the knee with recurrent effusions. He returns to the office reporting continued pain 2 years after surgery. He describes instability, particularly when descending stairs. On examination, range of motion of 0° to 120° is observed, with no extensor lag. Slope of the tibial component is 7°. The knee is stable to varus and valgus stress in extension, but flexion instability is present in both the anterior-posterior direction and the varus-valgus direction. Bracing leads to a slight decrease in symptoms but is not well tolerated. Isokinetic testing demonstrates decreased knee extension velocity at mid push. Radiographs demonstrate well-aligned and fixed knee implants. An infection work-up is negative. What is the most appropriate surgical intervention at this time?
Explanation
The patient’s symptoms at follow-up—pain, swelling, and difficulty descending stairs—suggest knee flexion instability. Considering his history, an incompetent PCL must be considered. Revision of the knee to a posterior stabilized or nonlinked constrained condylar implant (depending on the condition of the ligaments) likely is needed to address his symptoms. The difference in extension stability and flexion stability makes polyethylene exchange a poor option. A constrained rotating hinge design is not necessary. Repeat use of a PCL-retaining insert is not recommended. Tibial and femoral revision both are required. Correction of excessive slope will be attained with tibial revision, femoral component revision is required to convert to a PCL-substituting design. There is also an opportunity to increase posterior condylar offset if needed.
