Orthopedic Board Review MCQs: Knee, Shoulder & Nerve | Part 82

Key Takeaway
This page offers Part 82 of a comprehensive OITE & AAOS Orthopedic Board Review. It features 100 high-yield, verified MCQs designed for orthopedic residents and surgeons preparing for board certification exams. Utilize study and exam modes with detailed explanations for optimal preparation.
About This Board Review Set
This is Part 82 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 82
This module focuses heavily on: Knee, Ligament, Nerve, Shoulder.
Sample Questions from This Set
Sample Question 1: In the anterior cruciate ligament-deficient knee, what structure provides an important secondary restraint to anterior tibial translation? Review Topic...
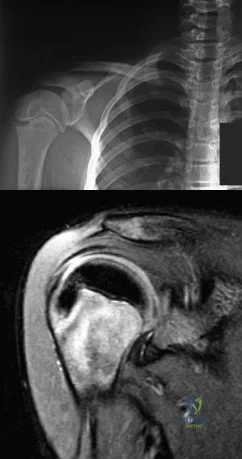
Sample Question 2: A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no ...
Sample Question 3: A patient reports changes in vocal quality after undergoing a right-sided anterior cervical approach to C6. Which of the following nerves has most likely been injured?...
Sample Question 4: A patient with a previously pain-free knee replacement now reports a sudden inability to ambulate. Radiographs of the knee are shown in Figures 33a and 33b. Management should consist of...
Sample Question 5: Which of the following statements about hoarseness due to vocal cord paralysis after anterior cervical diskectomy and fusion is most accurate?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
In the anterior cruciate ligament-deficient knee, what structure provides an important secondary restraint to anterior tibial translation? Review Topic
Explanation
Question 2
A 12-year-old boy who pitches on two “select” baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of Review Topic
Explanation
Question 3
A patient reports changes in vocal quality after undergoing a right-sided anterior cervical approach to C6. Which of the following nerves has most likely been injured?
Explanation
Question 4
A patient with a previously pain-free knee replacement now reports a sudden inability to ambulate. Radiographs of the knee are shown in Figures 33a and 33b. Management should consist of
Explanation
REFERENCES: Insall J, Salvati E: Patella position in the normal knee joint. Radiology 1971;101:101-104.
Lynch AF, Rorabeck CH, Bourne RB: Extensor mechanism complications following total knee arthroplasty. J Arthroplasty 1987;2:135-140.
Rand JA, Morrey BF, Bryan RS: Patellar tendon rupture after total knee arthroplasty. Clin Orthop 1989;244:233-238.
Question 5
Which of the following statements about hoarseness due to vocal cord paralysis after anterior cervical diskectomy and fusion is most accurate?
Explanation
REFERENCES: Beutler WJ, Sweeney CA, Connolly PJ: Recurrent laryngeal nerve injury with anterior cervical spine surgery risk with laterality of surgical approach. Spine 2001;26:1337-1342.
Kilburg C, Sullivan HG, Mathiason MA: Effect of approach side during anterior cervical discectomy and fusion on the incidence of recurrent laryngeal nerve injury. J Neurosurg Spine 2006;4:273-277.
Question 6
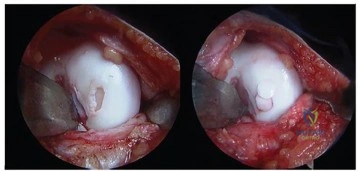
A 25-year-old patient undergoes the procedure seen in Figure A. Which of the following statements best describes the incorporation of the graft and biopsy results of the graft at one year? Review Topic
Explanation
Articular cartilage defects can be treated by a variety of methods including debridement, fixation of unstable osteochondral fragments, marrow stimulation techniques (microfracture, abrasion chondroplasty), cartilage replacement techniques (osteochondral autograft and allograft) and cellular techniques (autologous chondrocyte implantation). Osteochondral autograft transfer is performed by harvesting normal articular cartilage with underlying bone from lesser weightbearing areas (e.g. intercondylar notch) and transferring the graft to a recipient socket at the site of the chondral defect. Graft incorporation occurs by integration of the bony graft into the subchondral bone and healing of the overlying cartilage layer.
Hangody et al. reviewed the outcomes of autologous osteochondral mosaicplasty in professional athletes. They found successful outcomes similar to that of less athletic patients, despite a higher rate of preoperative osteoarthritic changes in the athletic population. The authors noted that histological evaluation revealed good graft incorporation in all 11 cases.
Alford et al. authored a two part Current Concepts article on cartilage restoration. They constructed an algorithm (Illustration A) highlighting many factors that impact treatment choice, including patient activity level and defect characteristics such as location and size. This algorithm also illustrates comorbidities (malalignment, ligament insufficiency) that warrant correction prior to addressing the chondral defect.
Figure A shows a full-thickness chondral defect (left) and subsequent osteochondral autograft transfer (right). Illustration A is a treatment algorithm for the management of chondral defects, as discussed above. Illustration B shows a microfracture procedure, a marrow stimulation technique resulting in fibrocartilage filling of the chondral defect. Illustration C shows an osteochondral allograft transplant, a cartilage replacement technique useful for large defects in which donor graft is obtained from a cadaver hemicondyle and transferred to a recipient socket at the site of the chondral defect. Illustration D shows the autologous chondrocyte implantation technique, a two-stage procedure consisting of 1. Cartilage biopsy for growth of autologous
chondrocytes, and 2. Subsequent injection of autologous chondrocytes beneath a periosteal patch.
Incorrect
Question 7
The mother of a 5-year-old child reports that he has had a fever of 103°F (39.4°C), leg swelling, and has been unwilling to bear weight on his right lower leg for the past 7 days. Examination reveals point tenderness at the distal femur. Aspiration at the metaphysis yields 10 mL of purulent fluid, and a Gram stain reveals gram-positive cocci. In addition to hospital admission, management should include
Explanation
REFERENCE: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 8
Figure 35 shows the radiograph of a 12-year-old boy who fell off a snowmobile and landed on his left shoulder. He has a closed injury. Management should consist of
Explanation
REFERENCES: Kohler R, Trillaud JM: Fracture and fracture separation of the proximal humerus in children: Report of 136 cases. J Pediatr Orthop 1983;3:326-332.
Beaty JH: Fractures of the proximal humerus and shaft in children. Instr Course Lect 1992;41:369-372.
Dobbs MB, Luhmann SL, Gordon JE, et al: Severely displaced proximal humeral epiphyseal fractures. J Pediatr Orthop 2003;23:208-215.
Beringer DC, Weiner DS, Noble JS, et al: Severely displaced proximal humeral epiphyseal fractures: A follow-up study. J Pediatr Orthop 1998;18:31-37.
Wang P Jr, Koval KJ, Lehman W, et al: Salter-Harris type III fracture-dislocation of the proximal humerus. J Pediatr Orthop B 1997;6:219-222.
Question 9
A patient who underwent a total knee arthroplasty (TKA) 4 years ago reports acute knee pain 2 days following dental surgery. Knee joint aspiration demonstrates 40000 white blood cells/µL with 90% neutrophils. An aspirate culture grows peptostreptococcus. Treatment should consist of
Explanation
This patient has an acute hematogenous infection of a TKA. Irrigation, debridement, polyethylene liner exchange, and IV antibiotics remain the treatments of choice. However, failure of this approach has been reported in 20% to 60% of cases in various series, particularly when methicillin-resistant streptococcus aureus or methicillin-resistant streptococcus epidermis is isolated.

Question 10
The transverse diameter of the pedicle is most narrow at which of the following levels?
Explanation
REFERENCES: O’Brien MF, Lenke LG, Mardjetko S, et al: Pedicle morphology in thoracic adolescent idiopathic scoliosis: Is pedicle fixation an anatomically viable technique? Spine 2000;25:2285-2293.
Vaccaro AR, Rizzolo SJ, Allardyce TJ, et al: Placement of pedicle screws in the thoracic spine: Part I. Morphometric analysis of the thoracic vertebrae. J Bone Joint Surg Am
1995;77:1193-1199.
Question 11
A 6-year-old boy has had increasing pain and a mass in the suprapatellar region of the right femur for the past week. Examination of the mass reveals it may be firm, immobile, and tender to palpitation. The patient has no systemic symptoms. Laboratory studies show a WBC of 7000 per cubic millimeter, a hematocrit of 40%, and an erythrocyte sedimentation rate of 10 mm/hr. radiographs are normal. Figures 64a and 64b show saggital and axial T1-weighted MRI scans. Figure 64c shows frozen section pathology of the biopsy specimen. What is the most likely diagnosis?
Explanation
Question 12
In regards to a genetic disorder, which of the following is an example of "anticipation?"
Explanation
Genetic anticipation is an important concept in understanding the development and genetic implications of many heritable disorders. It is a common phenomenon in trinucleotide repeat expansion disorders. These disorders are due to unstable microsatellite trinucleotide repeats that expand beyond the normal threshold. In subsequent generations these expansions become longer and thus express disease characteristics at a younger age of onset, and often with greater severity.
Martorell et al. investigated the development of CTG trinucleotide repeats in patients with myotonic dystrophy type 1 (DM1) and their relatives. They discovered unaffected individuals carry a pre-mutation sequence which can lead to trinucleotide repeat expansion in subsequent generations and thus produce offspring with the disorder.
Kamsteeg et al. compare the characteristics of DM1 and DM2. Both are due to trinucleotide repeat expansions. However, while DM1 can present with earlier onset and increasing severity in each generation, DM2 does not exhibit this genetic anticipation.
Incorrect Answers
Question 13
An 18-year-old boy reports increasing pain with weight bearing on his right leg and at night. Examination reveals swelling around the right midcalf. Radiographs and an MRI scan are shown in Figures 13a through 13c, and a biopsy specimen is shown in Figure 13d. What is the preferred treatment?
Explanation
REFERENCES: McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 258.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
Question 14
Histologic studies of surgically resected tissue in lateral epicondylitis demonstrate which of the following findings? Review Topic
Explanation
Question 15
Figures 1 and 2 show the radiographs obtained from a 68-year-old morbidly obese man who underwent left total hip replacement 7 years ago and did well, with no symptoms prior to the current presentation. He recently rose from a seated position and felt a pop in the hip, with immediate pain and inability to bear weight. Any pressure on the left foot now produces a painful, grinding sensation with loss of left hip stability. What is the best next step?

Explanation
The modular femoral stem has fractured. Changing the liner to a constrained design is not warranted at this time based on the information provided. Revision of the acetabular implant is appropriate because of the potential for damage to the existing cup from metal debris and femoral implant contact and to convert from a metal-on-metal articulation. Nonsurgical management would not provide pain relief or improvement; revision of the total hip arthroplasty is recommended. The implant failed in a short time, and retention of the femoral stem is not recommended because of the concern for failure with only a neck exchange. A dual-mobility bearing may be a good option if the surgeon plans to retain the acetabular component. Extended trochanteric osteotomy is a useful technique for the removal of a well-fixed femoral implant. In this patient, femoral stem removal without
osteotomy would be difficult due to the fracture of the implant’s femoral neck and the inability to gain purchase for extraction.
Question 16
A 48-year-old man who is scheduled to undergo total knee replacement has an X-linked clotting disorder that leads to abnormal bleeding and recurrent, spontaneous hemarthrosis. Before undergoing surgery, he should have replacement therapy of
Explanation
Question 17
What is the main function of collagen found within articular cartilage?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Mow VC, Ratcliffe A: Structure and function of articular cartilage and meniscus, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, pp 113-177.
Question 18
40A B Figures 40a and 40b are this patient's intraoperative arthroscopic images. The abnormality seen here illustrates which of the patient's clinical findings?
Explanation
Ankle sprains are the most common musculoskeletal injury; however, most of these sprains do not progress to chronic instability. Initial injuries are treated with RICE (rest, ice, compression, elevation), range of motion, weight bearing
as tolerated, and proprioceptive therapy. Lace-up ankle braces are most effective during the subacute period after a sprain. Structured physical therapy focused on proprioception is recommended for 6 weeks. Examination findings for ankle ligament instability are unreliable because of associated subtalar joint motion. Casting is not as effective as functional rehabilitation. Stress radiographs are recommended, but a clear pathologic range of measurements is not defined. Generalized ligament laxity can result in false-positive findings of instability; therefore, contralateral stress radiographs are often necessary for comparison. The difference in anterior drawer measurement between both ankles should not exceed 5mm. Likewise, the difference in talar tilt measurement between both ankles should be 5 or fewer degrees. Patients with mechanical symptoms, a joint effusion, or continued pain may have an intra-articular pathology such as a loose body or osteochondral lesion. Ankle instability can exist without ligamentous laxity. Symptoms of chronic instability can result from osteochondral lesions of talus, peroneal tendon pathology, loose bodies, anterior ankle impingement, and fracture nonunions. Although there is not sufficient evidence to recommend arthroscopy prior to all ligament reconstructions, arthroscopy is recommended when other pathology is suspected.
RECOMMENDED READINGS
Colville MR. Surgical treatment of the unstable ankle. J Am Acad Orthop Surg. 1998 Nov-Dec;6(6):368-77. Review. PubMed PMID: 9826420. View Abstract at PubMed
DiGiovanni CW, Brodsky A. Current concepts: lateral ankle instability. Foot Ankle Int. 2006 Oct;27(10):854-66. Review. PubMed PMID: 17054892. View Abstract at PubMed
Maffulli N, Ferran NA. Management of acute and chronic ankle instability. J Am Acad Orthop Surg. 2008 Oct;16(10):608-15. Review. PubMed PMID: 18832604. View Abstract at PubMed
Question 19
What is the most common associated pathology in patients who have suprascapular nerve entrapment secondary to ganglion cysts?
Explanation
REFERENCES: Fehrman DA, Orwin JF, Jennings RM: Suprascapular nerve entrapment by ganglion cysts: A report of six cases with arthroscopic findings and review of the literature. Arthroscopy 1995;11:727-734.
Iannotti JP, Ramesey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Moore TP, Fritts HM, Quick DC, Buss DD: Suprascapular nerve entrapment caused by supraglenoid cyst compression. J Shoulder Elbow Surg 1997;6:455-462.
Question 20
A 67-year-old woman has persistent anterior thigh and knee pain after undergoing total knee arthroplasty 1 year ago. Examination and radiographs reveal no problems in the knee, mild hip flexor weakness (grade 4+), and decreased sensation over the anterior thigh including and proximal to the incision. MRI of the lumbar spine will most likely reveal which of the following findings?
Explanation
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Upper Saddle River, NJ, Prentice Hall, 1976, p 250.
Lauerman WC, Goldsmith ME: Spine, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 353-378.
Question 21
Smoking has been associated with lower fusion rates in both cervical and lumbar fusion. Which of the following statements best describes an explanation for these findings?
Explanation
have been performed to offer an explanation of the mechanism mediating this effect. Whereas all of the above have been postulated as explanations, more recent studies have demonstrated that nicotine delivered via a transdermal patch significantly enhanced posterior spinal fusion in rabbits. Thus it appears that the effects of smoking on fracture healing are multifactorial and not yet fully understood.
Question 22
Limited weight bearing usually is recommended following open reduction and internal fixation of intra-articular lower extremity fractures. A bone graft, or bone graft substitute is often placed in the metaphyseal void beneath the reduced articular fragments. Which of the following bone grafts or bone graft substitutes will most likely permit earlier weight bearing without subsidence of the articular reduction?
Explanation
Question 23
The direct anterior (Smith-Peterson) approach to hip arthroplasty is most commonly associated with injury to what nerve?
Explanation
Some authors have reported the incidence of lateral femoral cutaneous nerve neuropraxia following hip arthroplasty with the direct anterior approach to be near 80%, but resolution of the sensory deficits has been observed in most patients over time. Femoral nerve palsy has been reported to occur in .64% to 2.3% direct lateral (Hardinge) and anterolateral (Watson-Jones) approaches, and the superior gluteal nerve may be injured with proximal extension of the abductor muscular dissection. The posterior approach has been reported to be associated with sciatic nerve injury, especially in cases of dysplasia. Pudendal nerve injury has not been reported with the anterior, anterolateral, direct lateral, or posterior approaches to hip
arthroplasty. It has been reported following hip arthroscopy and the use of a traction table, however.
Question 24
A 7-year-old girl sustains the fracture shown in Figure 29a. Casting results in uneventful healing. Ten months later, the patient has a progressive valgus deformity of the right lower extremity. A radiograph is shown in Figure 29b. Management should now consist of
Explanation
REFERENCES: Tuten HR, Keeler KA, Gabos PG, et al: Posttraumatic tibia valga in children: A long-term follow-up note. J Bone Joint Surg Am 1999;81:799-810.
McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 25
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245.
Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Thometz JG, Gould JS: Cavus deformity, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 26
An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?
Explanation
REFERENCES: Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
Modabber M, Jupiter JB: Operative management of diaphyseal fractures of the humerus: Plate versus nail. Clin Orthop 1998;347:93-104.
Question 27
Compared to metal-on-polyethylene total hip bearing surfaces, the debris particles generated by metal-on-metal articulations are
Explanation
metal-on-metal articulations in total hip arthroplasty are several orders of magnitude smaller
and may be up to 100 times more numerous than those found with metal-on-polyethylene articulations.
REFERENCES: Davies AP, Willert HG, Campbell PA, et al: An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements.
J Bone Joint Surg Am 2005;87:18-27.
Firkins PJ, Tipper JL, Saadatzadeh MR, et al: Quantitative analysis of wear and wear debris from metal-on-metal hip prostheses tested in a physiological hip joint simulator. Biomed Mater Eng 2001;11:143-157.
Question 28
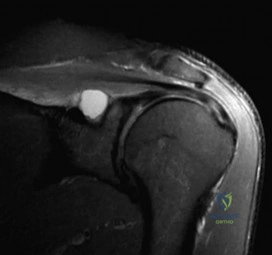
A 24-year-old avid volleyball player has noted gradual onset of shoulder fatigue and weakness limiting his game. Radiographs done by his primary care physician were normal and he has failed to improve with 6 weeks of physical therapy. Given the MRI image shown in Figure A, this patients physical exam may reveal weakness with which of the following actions? Review Topic
Explanation
Extrinsic compression or traction on the suprascapular nerve can result in suprascapular neuropathy. Compression of the nerve may occur at two distinct locations: the suprascapular notch and the spinoglenoid notch. Extrinsic compression of the suprascapular nerve by ganglion cysts can occur at the spinoglenoid notch or, less commonly, at the suprascapular notch. These cysts may originate from the transverse scapular ligament, the fibrous tissue of the scapula, or the glenohumeral joint.
Mittal et al. reviewed the literature and found that the formation of ganglionic cysts in the spinoglenoid fossa occurs with cumulative trauma and leads to entrapment neuropathy of the suprascapular nerve and denervation of the infraspinatus muscle.
Romeo et al. reported on various etiologies of suprascapular neuropathy including traction injury at the level of the transverse scapular ligament or the spinoglenoid ligament and direct trauma to the nerve. They noted that sports involving overhead motion, such as tennis, swimming, and weight lifting, may result in traction injury to the suprascapular nerve, leading to dysfunction. They also reported that the onset of weakness can be subtle and must be differentiated from cervical radiculopathy and degenerative disease of the shoulder.
Figure A depicts a T2 coronal MRI of the shoulder with a cyst easily visualized occupying the suprascapular notch. Illustration A is an algorithm for the management of suprascapular neuropathy. Illustration B is a sagittal MRI from the same patient depicting the ganglion cyst within the suprascapular notch once again leading to atrophy of both the supraspinatus and infraspinatus (asterisks).
Incorrect Answers:
Question 29
A 47-year-old landscaper presents with worsening left shoulder pain and weakness. Three years ago, he injured the left shoulder in a fall and elected for nonoperative management to minimize time off from work. Physical therapy was effective until 6 months ago when his shoulder function worsened to the point that he is now unable to work. Examination of his active range of motion reveals forward elevation 120° with pain, abduction 100°, IR at neutral to T8 and ER at neutral 5°. He has a positive ER lag sign and Hornblower's sign. Belly press and lift-off tests are normal. A recent radiograph is shown in Figures A. MRI images are shown in Figures B and C. Which of the following is the best treatment option? Review Topic
Explanation
Irreparable rotator cuff tears are marked by: (1) Superior displacement of the humeral head (AHI < 5-7mm), (2) Fatty infiltration of the rotator cuff muscles (Goutallier stage 3-4), (3) Increased duration of the tendon tear and (4) Profound external rotation weakness. These findings are predictive of poor-quality tissue and stiffness of the muscle-tendon unit, not amenable to primary repair. In this setting, a latissimus dorsi
transfer can be utilized to restore shoulder strength, function and improve pain. Relative contraindications include subscapularis deficiency, deltoid deficiency, pseudoparalysis of the shoulder and advanced glenohumeral arthritis.
Gerber et al. performed a case series analysis of 67 patients with irreparable rotator cuff tears managed with latissimus dorsi transfer. Patients with an intact subscapularis demonstrated improvement in pain, range of motion and strength postoperatively, while no improvement was noted in patients with subscapularis deficiency. The authors conclude that latissimus dorsi transfer should not be performed in the setting of poor subscapularis function.
Iannotti et al. found that better clinical results following latissimus dorsi transfer were associated with: preserved active shoulder range of motion and strength (specifically forward elevation > 90° and external rotation > 20°), synchronous firing of the transferred latissimus dorsi muscle and male gender.
Figure A is an AP radiograph of the left shoulder with superior migration of the humeral head (AHI < 5mm) and no evidence of glenohumeral arthritis. Figures B and C show a retracted posterosuperior rotator cuff tear and Goutallier stage 4 atrophy (more fat than muscle) of the supraspinatus, infraspinatus and teres minor, rendering this tear irreparable. Illustration A shows a latissimus dorsi transfer. The latissimus dorsi tendon is positioned over the top of the humeral head, covering most of the rotator cuff defect. The tendon is then secured to the subscapularis tendon edge and lesser tuberosity anteriorly, the remnant supraspinatus and infraspinatus tendons medially, and the greater tuberosity laterally.
Incorrect Answers:
Question 30
An 83-year-old woman reports pain in her left middle finger after a minor injury. Laboratory studies show a WBC count of 7,000/mm 3 , an erythrocyte sedimentation rate of 3 mm/h, a uric acid of 10.4 mg/dL, and a normal serum protein electrophoresis. Radiographs are shown in Figures 49a and 49b. A core biopsy specimen is shown is Figure 49c. In addition to treatment of the finger fracture, treatment should include
Explanation
REFERENCES: Wise CM: Crystal-associated arthritis in the elderly. Clin Geriatr Med 2005;21:491-511.
Mudgal CS: Management of tophaceous gout of the distal interphalangeal joint. J Hand Surg Br 2006;31:101-103.
Question 31
What arterial vessel is most prone to injury during posterior iliac crest bone graft harvest?
Explanation
REFERENCES: Guyer RD, Delmarter RB, Fulp T, Small SD: Complications of cervical spine surgery, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 547.
Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 330-331.
Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 297, 331-332.
Question 32
An 11-year-old boy sustained an injury to his arm in gym class. He denies prior pain in the arm. Radiographs are shown in Figures 48a and 48b. What is the next most appropriate step in the management of this lesion?
Explanation
REFERENCES: Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Deyoe L, Woodbury DF: Unicameral bone cyst with fracture. Orthopedics 1985;8:529-531.
Question 33
Figures below demonstrate the radiographs obtained from a 56-year-old man with a 3-year history of right groin pain. A comprehensive nonsurgical program has failed, and the patient would like to proceed with total hip arthroplasty. He is seen by a pain management specialist and is currently taking 40 mg of sustained-release morphine twice daily with oxycodone 10 mg 2 to 3 times a day for severe pain. What is the recommended course of action regarding his chronic narcotic use?
Explanation
Chronic opioid consumption prior to total joint arthroplasty has been associated with increased pain after surgery, increased opioid requirements, a slower recovery and longer hospital stay, and higher 90-day postoperative complications compared with patients not on chronic opioids preoperatively. Based on this information, Nguyen and associates performed a study in three patient groups that included 1) chronic opioid users who underwent no preoperative intervention, 2) chronic opioid users who were weaned down to 50% of their prior opioid regimen, and 3) patients who were not chronic opioid users. The authors found that the reduction of preoperative opioid use improved postoperative function, pain, and recovery and that the weaned group performed more like the opioid naive group than the chronic opioid user
group. Increasing opioid use prior to surgery in this patient would make it more difficult to control pain after surgery. Stopping all of his opioids just prior to surgery would place the patient at substantial risk for opioid withdrawal and is not recommended. Avoiding the use of all narcotics and using only acetaminophen postoperatively is very unlikely to provide appropriate pain relief in a chronic opioid user. The recommendation based on the provided literature is to decrease the patient's narcotic use prior to
surgery.
Question 34
A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?
Explanation
REFERENCES: Basset LW, Mirra JM, Cracchiolo A III: Ischemic necrosis of the femoral head: Correlation between magnetic resonance imaging and histologic sections. Clin Orthop 1987;223:181-187.
Sugano N: Osteonecrosis, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopedics. St Louis, MO, Mosby, 2002, pp 878-887.
Question 35
A 47-year-old woman has had medial ankle pain and swelling for the past 3 months. She recalls no specific injury, and casting and nonsteroidal anti-inflammatory drugs have failed to provide relief. Examination reveals a pes planus with heel valgus that is passively correctable. Radiographs show no evidence of arthritis. An MRI scan is shown in Figure 16. What is the most appropriate surgical procedure to alleviate her pain?
Explanation
REFERENCES: Myerson MS, Corrigan J: Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon transfer and calcaneal osteotomy. Orthopedics 1996;19:383-388.
Mosier-LaClair S, Pomeroy G, Manoli A II: Operative treatment of the difficult stage 2 adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:95-119.
Question 36
The anterior approach to total hip arthroplasty requires dissection between which of the following muscle planes?
Explanation
DISCUSSION: The anterior approach to the hip joint involves identifying the plane between the tensor fascia lata and the sartorius muscles.
REFERENCES: Berger RA, Duwelius PJ: The two-incision minimally invasive total hip arthroplasty: Technique and results. Orthop Clin North Am 2004;35:163-172.
Matta JM, Shahrdar C, Ferguson T: Single-incision anterior approach for total hip arthroplasty on an orthopaedic table. Clin Orthop Relat Res 2005;441:115-124.
28 • American Academy of Orthopaedic Surgeons
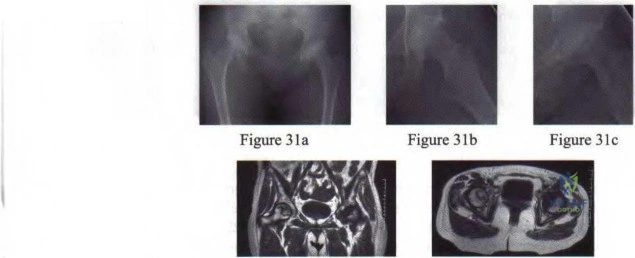
Figure 3Id Figure 31e
Question 37
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling’s test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis? Review Topic
Explanation
Question 38
A 40-year-old woman reports the atraumatic onset of severe knee pain and swelling after undergoing an uncomplicated elective cholecystectomy 1 week ago. She denies any history of diabetes mellitus or HIV but has had occasional episodes of mild knee pain and swelling that have always responded to nonsteroidal anti-inflammatory drugs. Radiographs are shown in Figures 5a and 5b. A knee aspiration yields a WBC count of 35,000/mm 3 . The aspirate should also yield which of the following findings?
Explanation
REFERENCES: Fisseler-Eckhoff A, Muller KM: Arthroscopy and chondrocalcinosis. Arthroscopy 1992;8:98-104.
Hough AJ Jr, Webber RJ: Pathology of the meniscus. Clin Orthop 1990;252:32-40.
Question 39
A 14-year-old competitive gymnast has had activity-related low back pain for the past month. Examination reveals no pain with forward flexion, but she has some discomfort when resuming an upright position. She also has pain with extension and lateral bending of the spine. The neurologic examination is normal. Popliteal angles measure 20 degrees. AP, lateral, and oblique views of the lumbar spine are negative. What is the next most appropriate step in management?
Explanation
are negative.
REFERENCES: Ciullo JV, Jackson DW: Pars interarticularis stress reaction, spondylolysis, and spondylolisthesis in gymnasts. Clin Sports Med 1985;4:95-110.
Collier BD, Johnson RP, Carrera GF, et al: Painful spondylolysis or spondylolisthesis studied by radiography and single photon emission computed tomography. Radiology 1985;154:207-211.
Jackson DW, Wiltse LL, Cirincione RT: Spondylolysis in the female gymnast. Clin Orthop 1976;117:68-73.
Ginsberg GM, Bassett GS: Back pain in children and adolescents: Evaluation and differential diagnosis. J Am Acad Orthop Surg 1997;5:67-78.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 40
Vertebral fractures are common in the thoracolumbar spine. What is the most important factor that determines the strength of the cancellous bone in the vertebral body?
Explanation
REFERENCES: Carter DR, Hayes WC: The compressive behavior of bone as a two-phase porous structure. J Bone Joint Surg Am 1977;59:954-962.
Keaveny TM: Strength of trabecular bone, in Cowin SC (ed): Bone Mechanics Handbook. Boca Raton, FL, CRC Press, 2001, pp 16-1-16-8.
Question 41
-
Explanation
Holt-Oram syndrome – Radial deficiency and cardial septal defect.
Fanconi syndrome – Severe aplastic anemia
TAR syndrome
Trisomy 17
VATER syndrome
Because of the association with severe aplastic anemia, a platelet count should be done before any surgical intervention.
Question 42
Second impact syndrome (SIS) after head injury is characterized by which of the following? Review Topic
Explanation
Question 43
A 72-year-old woman falls onto her left hip after tripping over a curb during her daily 3-mile walk. An injury radiograph is shown in Figure A. What is the best long term solution?

Explanation
The aims of surgery for FNF in elderly patients are immediate pain relief, rapid mobilization, and low complications and revision. THA has best pain relief, fewer reoperations, best survivorship and is most cost-effective but has longer operative/anesthetic time, blood loss, higher infection rate, and potential instability compared with HA.
Healy and Iorio examined the optimal treatment for elderly FNF. They compared internal fixation (120 patients) with arthroplasty (HA, 43 patients; THA, 23 patients). There was no different in reoperation or mortality rates between the 2 groups, but arthroplasty was more cost effective, had independent living, and longer interval to reoperation/death. THA had less pain, better function, and lower rates of reoperation than HA, and was most cost-effective. They concluded that THA was the best treatment.
Yu et al. performed a meta-analysis of randomized controlled trials to determine whether THA or hemiarthroplasty (HA) was superior. They found that THA had lower risk of reoperation (RR = 0.53), higher risk of dislocation (RR = 1.99), and
higher functional scores at 1 and 4 years. There was no difference in mortality, infection and complication rates.
Figure A shows a displaced left femoral neck fracture. Incorrect Answers:
Question 44
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?
Explanation
REFERENCES: Tan AH, Lam KS, Lee EH: The treatment outcome of trigger thumb in children. J Pediatric Orthop B 2002;11:256-259.
Slakey JB, Hennrikus WL: Acquired thumb flexion contracture in children: Congenital trigger thumb. J Bone Joint Surg Br 1996;78:481-483.
Herring JA: Disorders of the upper extremity: Thumb dysplasia, in Herring JA (ed): Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, p 445.
Question 45
What adaptations occur in the dominant shoulder of throwers compared to their nondominant shoulder? Review Topic
Explanation
Question 46
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
REFERENCES: Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 19-27.
Question 47
A 13-year-old girl has had increasing left hip pain for the past 4 months. A radiograph, bone scan, MRI scan, and photomicrograph are shown in Figures 1a through 1d. Which of the following immunohistochemistry results would confirm the most likely diagnosis?
Explanation
REFERENCES: Halliday BE, Slagel DD, Elsheikh TE, et al: Diagnostic utility of MIC-2 immunocytochemical staining in the differential diagnosis of small blue cell tumors. Diagn Cytopathol 1998;19:410-416.
Llombart-Bosch A, Navarro S: Immunohistochemical detection of EWS and FLI-1 proteins is Ewing sarcoma and primitive neuroectodermal tumors: Comparative analysis with CD99
(MIC-2) expression. Appl Immunohistochem Mol Morphol 2001;9:255-260.
Question 48
A radiograph, MRI scans, and a biopsy specimen of a 9-year-old boy with thigh pain are shown in Figures 37a through 37d. Management should consist of
Explanation
REFERENCES: Sailer SL: The role of radiation therapy in localized Ewing’ sarcoma. Semin Radiat Oncol 1997;7:225-235.
Shankar AG, Pinkerton CR, Atra A, Ashley S, Lewis I, Spooner D, et al: Local therapy and other factors influencing site of relapse in patients with localised Ewing’s sarcoma. United Kingdom Children’s Cancer Study Group (UKCCSG). Eur J Cancer 1999;35:1698-1704.
Carrie C, Mascard E, Gomez F, Habrand JL, Alapetite C, Oberlin O, et al: Nonmetastatic pelvic Ewing sarcoma: Report of the French society of pediatric oncology. Med Pediatr Oncol 1999;33:444-449.
Terek RM, Brien EW, Marcove RC, Meyers PA, Lane JM, Healey JH: Treatment of femoral Ewing’s sarcoma. Cancer 1996;78:70-78.
Question 49
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
REFERENCES: Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Mohler LR, Hanel DP: Closed fractures complicated by peripheral nerve injury. J Am Acad Orthop Surg 2006;14:32-37.
Question 50
A 35-year-old physical therapist presents with right-sided back and leg pain. For the last 4 months, he has taken anti-inflammatory medications and performed exercises on his own. While his back pain has improved slightly, his leg pain remain severe and interferes with his ability to sleep and work. Examination reveals positive ipsilateral and contralateral straight leg raise at 30 degrees. He has mildly diminished big toe dorsiflexion strength on the right side. There is a small patch of diminished sensation on the dorsum of the foot. MRI scans are shown in Figures A and B. What is the most appropriate next step in treatment? Review Topic
Explanation
For lumbar disc herniation, the first line of treatment is rest, physical therapy and oral medications (NSAIDs, gabapentin, steroids). The second line of treatment is selective nerve root corticosteroid injections. The last line in treatment is laminotomy and discectomy.
Pearson et al. determined which individuals (as opposed to groups) in the SPORT (Spine Patients Outcomes Research Trial) would benefit from surgery. They found that disc herniation patients improved more with surgery than without.
Lurie et al. reviewed the 8 year outcomes of the SPORT. In patients with HNP on imaging and leg symptoms persisting for at least 6 weeks, surgery was superior to nonoperative treatment in relieving symptoms and improving function.
Figures A and B are sagittal and axial T2-weighted MRI images showing a large L4/L5 herniated disc causing neural foramina narrowing and impinging on the right L5 root.
Incorrect Answers:
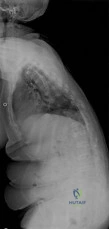
Question 51
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure 34. What is the next most appropriate step in the orthopaedic management of this patient?
Explanation
REFERENCE: Simon JA, Puopolo SM, Capla EL, et al: Accuracy of the axillary projection to determine fracture angulation of the proximal humerus. Orthopedics 2004;27:205-207.
Question 52
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
(type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive.
REFERENCES: Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Zerres K, Wirth B, Rudnik-Schoneborn S: Spinal muscular atrophy: Clinical and genetic correlations. Neuromuscul Disord 1997;7:202-207.
Question 53
A 25-year-old woman undergoes surgical treatment of a displaced proximal humeral fracture via a deltopectoral approach. At the first postoperative visit, she reports a tingling numbness along the anterolateral aspect of the forearm. What structure is most likely injured?
Explanation
REFERENCES: McIlveen SJ, Duralde XA, D’Alessandro DF, et al: Isolated nerve injuries about the shoulder. Clin Orthop 1994;306:54-63.
Warner JP: Frozen shoulder: Diagnosis and management. J Am Acad Orthop Surg
1997;5:130-140.
Question 54
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following? Review Topic
Explanation
Question 55
A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the medial collateral and anterior and posterior cruciate ligaments, as well as the posterior lateral corner. What is the most appropriate first step to rule out a vascular injury?
Explanation
REFERENCES: Miranda FE, Dennis JW, Veldenz HC, et al: Confirmation of the safety and accuracy of physical examination in the evaluation of knee dislocation for injury of the popliteal artery: A prospective study. J Trauma 2002;52:247-252.
Mills WJ, Barei DP, McNair P: The value of the ankle-brachial index for diagnosing arterial injury afterknee dislocation: A prospective study. J Trauma 2004;56:1261-1265.
Question 56
A 10-year-old boy who is active in soccer has had activity-related heel pain for the past 3 months. Examination reveals tenderness over the posterior heel and a tight Achilles tendon. Radiographs demonstrate a 2-cm cyst in the anterior body of the calcaneus. His physes have not closed. Based on these findings, what is the most appropriate management?
Explanation
REFERENCES: Ogden JA, Ganey TM, Hill JD, et al: Sever’s injury: A stress fracture of the immature calcaneal metaphysis. J Ped Orthop 2004;24:488-492.
Pogoda P, Priemel M, Linhart W, et al: Clinical relevance of calcaneal bone cysts: A study of 50 cysts in 47 patients. Clin Orthop Relat Res 2004;424:202-210.
Question 57
A 42-year-old man reports persistent arm pain after undergoing intramedullary nailing of a humeral shaft fracture 13 months ago. Physical exam shows near normal shoulder and elbow range-of-motion. Infection work-up is normal. A radiograph is shown in Figure
Explanation
Rubel et al in a combined cadaveric and clinical study comparing one versus two plate constructs for humeral nonunions found that the two plate construct was significantly stiffer, but had no difference in healing rate compared with a single plate construct; 92% of the humeral shaft nonunion patients went onto union with rigid plate fixation.
Ring et al successfully treated a cohort of osteoporotic humeral shaft nonunions with locked plating. They
report 100% union rate with locking plate fixation of these humeral shaft nonunions, with use of autograft in >50% of their cases. Subjective shoulder scores were excellent or good in 22 of 24 patients.
Brinker and O'Connor analyzed the current available evidence for exchange nailing of nonunions and could not recommend this treatment for humeral shaft nonunions.
OrthoCash 2020
Question 58
Which of the following ligaments is most commonly involved in posterolateral rotatory instability of the elbow?
Explanation
REFERENCES: Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
O’Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 59
An 18-month-old boy has 45 degrees of kyphosis in the thoracolumbar spine secondary to type I congenital kyphosis. Examination reveals that he is neurologically intact, and an MRI scan shows no evidence of intraspinal pathology. Management should consist of
Explanation
REFERENCES: Winter RB: Congenital Deformities of the Spine. New York, NY, Thieme-Stratton, 1983, pp 229-261.
Winter RB, Moe JH: The results of spinal arthrodesis for congenital spinal deformity in patients younger than five years old. J Bone Joint Surg Am 1982;64:419-432.
Question 60
An adult patient has an 8- x 4- x 10-cm soft-tissue mass located within the adductor compartment of the thigh. Staging studies should consist of
Explanation
REFERENCES: Demetri GD, Pollock R, Baker L, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
Pollock R, Brennan M, Lawrence W Jr: Society of Surgical Oncology practice guidelines: Soft-tissue sarcoma surgical practice guidelines. Oncology (Huntingt) 1997;11:1327-1332.
Question 61
What is the advantage of percutaneous pedicle screw fixation over open instrumentation and fusion for a thoracolumbar burst fracture without neurologic deficit?
Explanation
A prospective randomized study on short-segment treatment of burst fractures with and without fusion demonstrated similar outcomes at 5 years with lower blood loss in the nonfusion group. There is by definition no fusion performed with percutaneous stabilization, so patients often develop hardware failure. Some surgeons routinely remove instrumentation following percutaneous stabilization, thus revision surgery is common. Clinical outcomes are not improved compared to open methods.
RECOMMENDED READINGS
Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar and lumbar spine trauma. Neurosurg Focus. 2014;37(1):E11. doi: 10.3171/2014.5.FOCUS1494. Review. PubMed PMID: 24981899. View Abstract at PubMed Jindal N, Sankhala SS, Bachhal V. The role of fusion in the management of burst fractures of the thoracolumbar spine treated by short segment pedicle screw fixation: a prospective randomised trial. J Bone Joint Surg Br. 2012 Aug;94(8):1101-6. doi: 10.1302/0301-620X.94B8.28311. PubMed PMID: 22844053. View Abstract at PubMed
Dai LY, Jiang LS, Jiang SD. Posterior short-segment fixation with or without fusion for thoracolumbar burst fractures. a five to seven-year prospective randomized study. J Bone
Joint Surg Am. 2009 May;91(5):1033-41. doi: 10.2106/JBJS.H.00510. PubMed PMID:
Question 62
A 38-year-old man is three quarters of the way through the Hawaiian Ironman events run in a temperature of 60 degrees F. He is sweating profusely and suddenly collapses. Prior to this he had been drinking large amounts of bottled water at every water stop. What is the most likely diagnosis? Review Topic
Explanation
Question 63
Surgical restoration of sagittal balance of an adult spinal deformity will have which effect on outcome?
Explanation
The influence of sagittal balance on outcomes following fusion-based procedures for degenerative conditions of the lumbar spine has only recently been appreciated. Restoration of sagittal spinal balance improves low-back-pain outcomes and quality of life. Sagittal spinal balance has not been shown to relieve neurogenic claudication attributable to spinal stenosis.
RECOMMENDED READINGS
Li Y, Hresko MT. Radiographic analysis of spondylolisthesis and sagittal spinopelvic deformity. J Am Acad Orthop Surg. 2012 Apr;20(4):194-205. doi: 10.5435/JAAOS-20-04-194. Review. PubMed PMID: 22474089. View Abstract at PubMed
Korovessis P, Repantis T, Papazisis Z, Iliopoulos P. Effect of sagittal spinal balance, levels of posterior instrumentation, and length of follow-up on low back pain in patients undergoing posterior decompression and instrumented fusion for degenerative lumbar spine disease: a multifactorial analysis. Spine (Phila Pa 1976). 2010 Apr 15;35(8):898-905. doi: 10.1097/BRS.0b013e3181d51e84. PubMed PMID: 20354466. View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 99 AND 100
Figures 99a and 99b are MR images of a 59-year-old man with a history of intravenous (IV) drug abuse who arrives at the emergency department with malaise and fever. Upon admission, the patient's temperature is 38.9°C, his white blood cell count is 17000/µL (reference range [rr], 4500-11000/µL), his erythrocyte sedimentation rate is 98 mm/h (rr, 0-20 mm/h), and his C-reactive protein level is 45 mg/L (rr, 0.08-3.1 mg/L). He is admitted to the medical service to evaluate the source of his fevers. On hospital day 1, the patient reports weakness in his left arm and leg. Blood cultures are positive for methicillin-resistant Staphylococcus aureus.
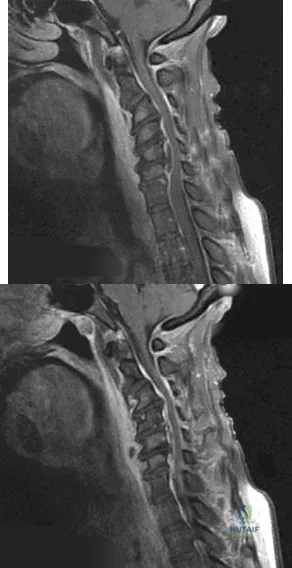
A B
Question 64
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Noll KH: The use of orthotic devices in adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:25-36.
Question 65
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
REFERENCES: Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Helfgott SM: Sensible approach to low back pain. Bull Rheum Dis 2001;3:50.
Question 66
What is the mechanism of action of an intramuscular injection of botulinum type A toxin in reducing spasticitiy?
Explanation
REFERENCES: Koman LA, Mooney JF III, Smith B, Goodman A, Mulvaney T: Management of cerebral palsy with botulinum-A toxin: Preliminary investigation. J Pediatr Orthop 1993;13:489-495.
Brin MF: Botulinum toxin: Chemistry, pharmacology, toxicity, and immunology. Muscle Nerve Suppl 1997;6:S146-168.
Question 67
Figure 100 is the MR image of a 19-year-old man who sustains recurrent anterior shoulder dislocations. The lesion shown occupies approximately 10% of the articular surface. What is the most appropriate treatment?
Explanation
The MR image shows a bony Bankart lesion involving less than 20% of the glenoid joint surface. One series reported high success rates after arthroscopic treatment when the defect was incorporated into the repair. Anterior bony deficiencies occupying more than 25% to 30% of the glenoid joint surface treated with soft-tissue repair only are associated with high
recurrence rates. In these patients, an open or arthroscopic coracoid transfer or distal tibial allograft reconstruction should be considered. ORIF has been reported for treatment of large acute glenoid rim fractures, but is not recommended for recurrent anterior shoulder instability in the setting of a 10% glenoid rim fracture.
Question 68
A 38-year-old woman who tripped and fell on her outstretched arm reports pain with movement. Examination reveals swelling. AP and lateral radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
REFERENCES: Mehdian H, McKee M: Management of proximal and distal humerus fractures. Orthop Clin North Am 2000;31:115-127.
Ring D, Jupiter J, Gulotta L: Articular fractures of the distal part of the humerus. J Bone Joint Surg Am 2003;85:232-238.
Question 69
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of Review Topic

Explanation
Question 70
What is the most prevalent adverse event associated with allogeneic blood transfusion?
Explanation
REFERENCES: Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.
Popovsky MA, Whitaker B, Arnold NL: Severe outcomes of allogeneic and autologous blood donation: Frequency and characterization. Transfusion 1995;35:734-737.
Question 71
An obese (BMI = 35) 72-year-old woman with diabetes mellitus, hyptertension and a 22-pack-year smoking history is scheduled to undergo posterior spinal fusion from T10 to S1 with a pedicle subtraction osteotomy at L3 for the spinal deformity seen in Figure 1. Which of the following risk factors is most predictive of major complication following surgery Review Topic
Explanation
The surgical treatment of adult spinal deformity often requires multilevel arthrodesis with complex osteotomies including three column osteotomies such as pedicle
subtraction (PSO) and vertebral column resection (VCR). They can involve both anterior and posterior surgical approaches. Surgical time, blood loss, length of hospital stay, and length of recovery can be greater than it is for the more common degenerative conditions.
Auerbach et al. characterized the risk factors for the development of major complications in patients undergoing 3-column osteotomies for adult spinal deformity correction. They also aimed to determine whether the presence of complications affected the ultimate clinical outcome. They found age > 60 years, > or = 3 comorbid conditions and preoperative sagittal imbalance of = 40mm was associated with a major complication. However, the presence of a major complication did not affect the ultimate clinical outcomes at 2 years or more.
Daubs et al. conducted a retrospective analysis of forty-six patients = 60 years of age who underwent major spinal deformity surgery requiring a minimum 5-level arthrodesis procedure to determine the rate of complication and outcomes. The overall complication rate was 37% and the major complication rate was 20%. Increasing age was a significant factor (p<0.05) in predicting the presence of a complication, while presence of comorbidities was found to have no association.
Figure A is a standing preoperative lateral radiograph of the spine demonstrating a thoracic kyphosis of ~25° and thoracolumbar kyphosis of ~25°. Illustration A demonstrates proper sagittal balance after spinal fusion from T10 to S1 and L3 PSO.
Incorrect Answers:
Question 72
Which of the following nonunions is appropriately treated with exchange reamed nailing without bone graft augmentation?

Explanation
Question 73
Design factors that enhance the long-term survival of proximally coated cementless hip implants include both initial stability and
Explanation
REFERENCES: Mont MA, Hungerford DS: Proximally coated ingrowth prostheses: A review. Clin Orthop 1997;344:139-149.
Engh CA, Hooten JP Jr, Zettl-Schaffer KF, Ghaffarpour M, McGovern TF, Bobyn JD: Evaluation of bone ingrowth in proximally and extensively porous-coated anatomic medullary locking prostheses retrieved at autopsy. J Bone Joint Surg Am 1995;77:903-910.
Urban RM, Jacobs JJ, Sumner DR, Peters CL, Voss FR, Galante JO: The bone-implant interface of femoral stems with non-circumferential porous coating. J Bone Joint Surg Am 1996;78:1068-1081.
Question 74
An 11-year-old girl is struck in the leg by a loaded sled while sledding and is seen in the emergency department; she is reporting severe knee pain. Radiographs are read as normal. Examination reveals that she is exquisitely tender over the proximal tibial physis. The neurovascular examination is normal. What is the next step in management?
Explanation
REFERENCES: McGuigan JA, O’Reilly MJ, Nixon JR: Popliteal arterial thrombosis resulting from disruption of the upper tibial epiphysis. Injury 1984;16:49-50.
Burkhart SS, Peterson HA: Fractures of the proximal tibial epiphysis. J Bone Joint Surg Am
1979;61:996- 1002.
Question 75
A 23-year-old woman with a history of bilateral recurrent ankle sprains, progressive cavovarus feet, and a family history of high arches and foot deformities is seen for evaluation. Management consisting of bracing and physical therapy has been poorly tolerated. Heel varus is partially corrected with a Coleman block. There are thick calluses under the first metatarsal heads. Sensation to touch and
Explanation
Question 76
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. Knee range of motion is between 0° and 70°. What is the most appropriate treatment option?

Explanation
The MR image shows bone bruises (“kissing contusions”) consistent with an ACL tear. During the ACL subluxation event, the posterolateral tibial plateau subluxes anteriorly, making contact with the mid portion of the lateral femoral condyle and resulting in this characteristic bone bruise pattern on MRI. Randomized clinical trials comparing early accelerated versus nonaccelerated rehabilitation programs have demonstrated no significant differences in long-term results with regard to function, reinjury, and successful return to play. These studies did not address timing of return to play with an early accelerated rehabilitation program. At 2 and 3 years postsurgically, there are no differences in laxity, number of graft failures, or KOOS scores.
Question 77
A 40-year-old male who sustained an open pilon fracture 2 weeks ago is scheduled for a below-the-knee amputation (BKA). What laboratory value is the best predictor for wound healing?

Explanation
Question 78
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include
Explanation
REFERENCES: Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Hawkins RJ, Murnaghan JP: The shoulder, in Gruess RL, Ronnie WRJ (eds): Adult Orthopaedics. New York, NY, Churchill Livingstone, 1984, pp 945-1054.
Question 79
A 77-year-old man who underwent right total knee replacement surgery 2 and a half years ago has had knee pain since surgery. The pain is diffuse, constant, and made worse with activity. He notes warmth and swelling in his knee. Examination shows a well-healed incision, no erythema, moderate warmth, synovitis, and an effusion. The knee is stable, and has an arc of flexion between 3° and 120°. Radiographs show well-fixed and well-aligned implants. What is the most appropriate initial treatment?
Explanation
This patient's history and physical findings are concerning for deep infection. Inflammatory markers, including ESR and CRP, should be obtained first. If the levels are elevated, knee aspiration should be performed for the synovial cell count and culture. A bone scan is not indicated in an initial investigation for deep infection; it is rarely helpful and is not cost effective. CT to assess implant rotation is an appropriate investigation for knee pain when the clinical scenario is not suspicious for a deep infection and when infection has been excluded.
Question 80
What is the most appropriate treatment for a chordoma involving the sacrum?
Explanation
REFERENCES: Fardin DF, Garfin SR, Abitbol J, et al (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 123-133.
Stener B, Gunterberg B: High amputation of the sacrum for extirpation of tumors: Principles and technique. Spine 1978;3:351-366.
Stener B: Resection of the sacrum for tumors. Chir Organi Mov 1990;75:S108-S110.
Question 81
A 4-year-old child sustains a spiral fracture to the tibia in an unwitnessed fall. History reveals three other fractures to long bones, and the parents are vague about the etiology of each. There is no family history of bone disease. The parents ask if the child has osteogenesis imperfecta (OI); however, there are no clinical or radiographic indications of this diagnosis. In addition to fracture care, management should include
Explanation
REFERENCES: Rockwood CA, Wilkins KE, King RE (eds): Fractures in Children. Philadelphia, PA, JB Lippincott, 1984, vol 3, pp 173-175.
Kempe CH, Silverman FN, Stelle BF, Droegemueller W, Silver HK: The battered-child syndrome. JAMA 1962;181:17-24.
Akbarnia BA, Akbarnia NO: The role of the orthopedist in child abuse and neglect. Orthop Clin North Am 1976;7:733-742.
Question 82
A college athlete has a knee injury requiring surgery. He has acne, gynecomastia, and well-developed muscles related to the use of anabolic steroids. What association with steroid use is concerning for surgery and anesthesia? Review Topic
Explanation
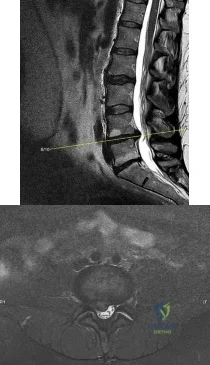
Question 83
Figure 35 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?
Explanation
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-a, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-ß, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
RECOMMENDED READINGS
Kim HT, Yoon ST, Jarrett C. Articular cartilage and intervertebral disk. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:23-33.
Hoyland JA, Le Maitre C, Freemont AJ. Investigation of the role of IL-1 and TNF in matrix degradation in the intervertebral disc. Rheumatology (Oxford). 2008 Jun;47(6):809-14. doi: 10.1093/rheumatology/ken056. Epub 2008 Apr 8. PubMed PMID: 18397957. View Abstract at PubMed
Gruber HE, Ingram JA, Hanley EN Jr. Immunolocalization of MMP-19 in the human intervertebral disc: implications for disc aging and degeneration. Biotech Histochem. 2005 May-Aug;80(3-4):157-62. PubMed PMID: 16298901. View Abstract at PubMed
Question 84
A 44-year-old woman has bilateral knee pain, and history reveals bilateral hip replacements. Radiographs are seen in Figure 28a, and histopathologic specimens from the total hip replacement are shown in Figures 28b and 28c. Laboratory studies reveal anemia. What is the most likely diagnosis?
Explanation
REFERENCE: Dutkowsky J: Miscellaneous non traumatic disorders, in Crenshaw A (ed): Campbell’s Operative Orthopaedics. St Louis, MO, Mosby, 1992, pp 2007-2012.
Question 85
What is the predominant type of collagen in the tissue resulting from the surgical procedure shown in Figures 40a through 40c?
Explanation
REFERENCES: Magnussen RA, Dunn WR, Carey JL, et al: Treatment of focal articular cartilage defects in the knee: A systematic review. Clin Orthop Relat Res 2008;466:952-962.
Williams RJ III, Hamly HW: Microfracture: Indications, technique, and results. Instr Course Lect 2007;56:419-428.
Mithoefer K, Williams RJ III, Warren RF, et al: Chondral resurfacing of articular cartilage defects in the knee with the microfracture technique: Surgical technique. J Bone Joint Surg Am 2006;88:294-304.
Question 86
A 30-year-old accountant and recreational softball player, who is seen at the end of his baseball season, reports a several month history of pain along the medial side of his dominant elbow. He cannot identify a specific injury and notes it only hurts when he throws the ball in from the outfield. Besides the pain, he remarks that his speed and distance while throwing have diminished considerably. Examination reveals tenderness along the medial elbow but no weakness or gross instability is found. Radiographs are normal. Based on the history, what is the most likely diagnosis? Review Topic
Explanation
the forearm during resisted forearm pronation and is not associated with the throwing motion in particular. Valgus extension overload may mimic medial collateral ligament injury, not varus extension injuries. Medial epicondylitis may be confused with ligament insufficiency but the examination and a history of pain only while throwing make this an unlikely diagnosis.
Question 87
A patient who is an observant Jehovah’s Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use? Review Topic
Explanation
Question 88
A 2-year-old girl has had a swollen right knee for the past 7 weeks. There is no history of significant trauma, and she has not had a fever or been ill. Her parents report that she is stiff in the morning but otherwise does not report pain. A CBC count and erythrocyte sedimentation rate are normal. Treatment with naproxen at appropriate doses for the past 2 weeks has resulted in some improvement. Radiographs show only soft-tissue swelling. Examination reveals a healthy-appearing child with a warm and swollen right knee that is only slightly tender but lacks full extension by 20 degrees. What is the next most appropriate step in management?
Explanation
REFERENCES: Wolf MD, Lichter PR, Ragsdale CG: Prognostic factors in the uveitis of juvenile rheumatoid arthritis. Ophthalmology 1987;94:1242.
Cassidy JT, Petty RE: Textbook of Pediatric Rheumatology. Philadelphia, PA, WB Saunders, 2001, p 220.
Chalom ED, Goldsmith DP, Koehler MA, et al: Prevalence and outcome of uveitis in a regional cohort of patients with juvenile rheumatoid arthritis. J Rheumatol 1997;24:2031-2034.
Question 89
A 24-year-old dancer reports posterior ankle pain when in the “en pointe” position. Examination reveals posteromedial tenderness, no pain reproduction with passive forced planter flexion, and pain with motion of the hallux. What is the most likely diagnosis?
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 249-261.
Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
Question 90
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?
Explanation
REFERENCES: Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129.
Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Thompson JE: Anatomical methods of approach in operations on the long bones of the extremities. Ann Surg 1918;68:309-316.
Question 91
A 26-year-old man with chronic lateral ankle instability underwent a modified Broström procedure 8 months ago. He reports persistent pain and swelling of the lateral ankle. Examination reveals lateral ankle tenderness and swelling and a negative anterior drawer test. Laboratory studies show a WBC count of 6,500/mm 3 and an erythrocyte sedimentation rate of 15 mm/h. Radiographs of the ankle are normal. What is the most likely cause of this problem?
Explanation
REFERENCES: Bonnin M, Tavernier T, Bouysset M: Split lesions of the peroneus brevis tendon in chronic ankle laxity. Am J Sports Med 1997;25:699-703.
Sobel M, Geppert MJ, Warren RF: Chronic ankle instability as a cause of peroneal tendon injury. Clin Orthop Relat Res 1993;296:187-191.
Question 92
The view from an anterosuperior portal of the right shoulder shown in Figure 12 reveals which of the following findings?
Explanation
REFERENCES: Wolf EM, Cheng JC, Dickson K: Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy 1995;11:600-607.
Bigliani LU, Pollack RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Warner JJ, Beim GM: Combined Bankart and HAGL lesion associated with anterior shoulder instability. Arthroscopy 1997;13:749-752.
Question 93
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?
Explanation
REFERENCES: Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment.
J Am Acad Orthop Surg 2001;9:268-278.
Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Duchesneau S, Fallat LM: The Tillaux fracture. J Foot Ankle Surg 1996;35:127-133.
Question 94
In the United States, groups at risk for community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) within the pediatric and adolescent populations include
Explanation
CA-MRSA is a growing problem in the United States. Groups at risk for CA-MRSA include athletes in contact sports and children in daycare. Tennis players, golfers, and runners are at lowest risk because their sports do not require close contact with teammates or competitors. Outbreaks have been noted in Alaskan native, Native American, and Pacific Islander minority populations.

CLINICAL SITUATION FOR QUESTIONS 64 THROUGH 68
Figures 64a through 64d are the radiographs of an 11-year-old boy with a prolonged history of activity-related ankle pain. An examination is notable for restricted subtalar motion and moderate pes planovalgus.
Question 95
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 1, pp 532-533.
Severin E: Contribution to the knowledge of congenital dislocation of the hip joint.
Acta Chir Scand 1941;84:1.
Question 96
Figure 12 shows the radiograph of an 80-year-old woman who has had an 8-month history of back pain after a fall. What is the most likely diagnosis based on the radiographic findings at the fractured vertebrae?
Explanation
REFERENCES: Murakami H, Kawahara N, Gabata T, et al: Vertebral body osteonecrosis without vertebral collapse. Spine 2003;28:E323-E328.
Jang JS, Kim DY, Lee SH: Efficacy of percutaneous vertebroplasty in the treatment of intravertebral pseudarthrosis associated with noninfected avascular necrosis of the vertebral body. Spine 2003;28:1588-1592.
Question 97
A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?
Explanation
REFERENCES: Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96.
Templeman DC, Schmidt AH, Sems AS, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Tile M: Management, in Tile M: Fractures of the Pelvis and Acetabulum, ed 2. Philadelphia, PA, Williams and Wilkins, 1995, pp 108-134.
Question 98
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern? Review Topic
Explanation
Question 99
What is the most common malignant bone tumor seen in patients with multiple hereditary exostosis?
Explanation
REFERENCES: Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 1660-1669.
Simon MA, Springfield DS, et al: Common Malignant Bone Tumors: Chondrosarcoma. Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 275-286.
Question 100
Which of the following 50-year-old patients with an irreparable rotator cuff tendon is the best candidate for an isolated latissimus dorsi muscle transfer? Review Topic
Explanation
