OITE & ABOS Orthopedic Board Prep: Trauma, Hand, Foot & Ankle MCQs | Part 258

Key Takeaway
This page offers Part 258 of a comprehensive Orthopedic Surgery board review. Authored by Dr. Mohammed Hutaif, it contains 100 high-yield, verified MCQs in the OITE/AAOS/ABOS format, focusing on Ankle, Fracture, and Wrist. Designed for orthopedic surgeons preparing for board certification exams.
About This Board Review Set
This is Part 258 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 258
This module focuses heavily on: Ankle, Fracture, Wrist.
Sample Questions from This Set
Sample Question 1: A 25-year-old farm worker sustained a grade III open fracture of the midshaft of the left tibia after falling from a ladder. Which of the following antibiotic regimens is best for this patient?...
Sample Question 2: Figure 24 shows an axial MRI scan of the ankle. The arrowhead is pointing to what structure?...
Sample Question 3: -A 50-year-old alcoholic man has erythema and swelling in his entire dominant upper extremity. He has a WBC of 15,000/mm3, a temp of 101 oF (38.3 oC), and a blood pressure of 90/60 mm Hg. After hemodynamic stabilization, the cellulitic fore...
Sample Question 4: An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most like...
Sample Question 5: Which of the following nonunions is appropriately treated with exchange reamed nailing without bone graft augmentation?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 25-year-old farm worker sustained a grade III open fracture of the midshaft of the left tibia after falling from a ladder. Which of the following antibiotic regimens is best for this patient?
Explanation
REFERENCES: Holton PD, Mader J, Nelson CL, Osmon DR, Patzakis MJ: Antibiotics for the practicing orthopaedic surgeon. Instr Course Lect 2000;341:36-42.
Wilkins J, Patzakis M: Choice and duration of antibiotics in open fractures. Orthop Clin North Am 1991;22:433-437.
Question 2
Figure 24 shows an axial MRI scan of the ankle. The arrowhead is pointing to what structure?
Explanation
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, pp 234-235.
Sammarco GJ: Peroneus longus tendon tears: Acute and chronic. Foot Ankle Int
1995;16:245-253.
Question 3
- A 50-year-old alcoholic man has erythema and swelling in his entire dominant upper extremity. He has a WBC of 15,000/mm3, a temp of 101 oF (38.3 oC), and a blood pressure of 90/60 mm Hg. After hemodynamic stabilization, the cellulitic forearm is longitudinally incised dorsally and volarly. The forearm muscles are normal in appearance; however, the subcutaneous fat is necrotic. A culture will most likely reveal
Explanation
Question 4
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Explanation
REFERENCES: Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
Roy S, Caine D, Singer KM: Stress changes of the distal radial epiphysis in young gymnasts: A report of twenty-one cases and a review of the literature. Am J Sports Med 1985;13:301-308.
Question 5
Which of the following nonunions is appropriately treated with exchange reamed nailing without bone graft augmentation?

Explanation
Question 6
Figure 46 shows the MRI scan of a patient who has a mass in the calf that has been fluctuating in size. Radiographs are negative. Which of the following procedures will most quickly aid in confirming the diagnosis?
Explanation
REFERENCES: Bianchi S, Abdelwahab IF, Kenan S, Zwass A, Ricci G, Palomba G: Intramuscular ganglia arising from the superior tibiofibular joint: CT and MR evaluation. Skeletal Radiol 1995;24:253-256.
Feldman F, Singson RD, Staron RB: Magnetic resonance imaging of para-articular and ectopic ganglia. Skeletal Radiol 1989;18:353-358.
Question 7
The MRI scans reveal a root tear of the medial meniscus. Studies demonstrate that this tear pattern greatly increases the tibiofemoral contact forces. These forces, and meniscal extrusion, worsen with increasing flexion. Correct answer : B 69- A 45-year-old postmenopausal smoker with a body mass index (BMI) of 22 has had severe knee pain for the past year. The pain has been progressing and the patient is now only able to perform activities of daily living. Knee radiographs reveal medial compartment osteoarthritis without any involvement of the patellofemoral joint or the lateral compartment. What is the contraindication for a high tibial osteotomy (HTO) in this patient?
Explanation
A. Healed one-level anterior cervical fusion
B. Congenital atlanto-occipital fusion
C. Cervical disk herniation previously treated nonoperatively
D. Spina bifida occulta
The one overriding principle regarding the return to any collision sport, as Torg and associates has described, is that the athlete be "neurologically intact, asymptomatic, and pain-free and have full strength and full cervical range of motion". Forces exerted on the cervical spine can be absorbed by the "elasticity of the intervertebral disk, the mobility of the spine itself, and the impact of absorbing capabilities of the cervical paravertebral musculature". The C1 and C2 levels (atlanto-occipital level) control movement of the skull and articulate the large motion movements. Specifically, partial or complete 56
congenital fusion of the atlas to the base of the occiput results in progressive cord compression by the posterior lip of the foramen magnum. It can result in sudden death.
A cervical disk herniation that was previously treated nonsurgically and is not causing cord compression in the currently asymptomatic patient is not a contraindication to return to collision sports. Spina bifida occulta is common (10-20% of healthy individuals). It is typically an incidental finding and does not result in neurologic problems. If individuals have a healed anterior, lateral or posterior disk herniation that is treated nonsurgically and they are currently asymptomatic, then there is no contraindication to participation in contact sports. If they require a diskectomy and fusion and they have a solid/healed fusion, are asymptomatic and neurologically intact with full and pain-free range of motion, then there is no contraindication to return to collision sports. An acute disk herniation, a disk herniation with associated pain or neurologic symptoms, or the presence of cord compression or loss of normal lordosis are all contraindications.
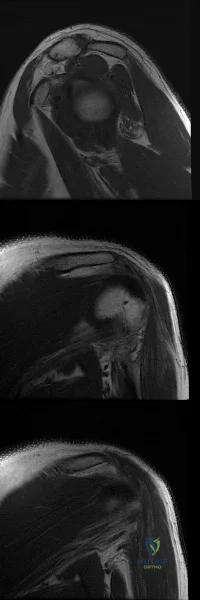
71- Based on the injury shown on the axial MRI scan of the shoulder in Figure 1, what other pathology should be closely examined for during surgery?
A. Subscapularis tear
B. Supraspinatus tear
C. Superior labral anterior- posterior (SLAP) tear
D. Bankart tear
The axial MRI scan reveals a subluxated biceps tendon. In the study by Koh and associates, 85% of patients with a biceps subluxation on MRI were found to have a subscapularis tear at the time of arthroscopy. These are not always obvious on the MRI, and close inspection of the leading edge/upper border of the subscapularis tendon at the time of arthroscopy is necessary. Although supraspinatus tears, SLAP tears, and Bankart tears can all occur in conjunction with a biceps subluxation, none have been shown to be strongly correlated with this pathology, nor as specific to this pathology.
73- Figures 1 through 4 are the MRI scans of a 24-year-old former collegiate basketball player who injured his left knee while playing recreational basketball 10 days prior to presentation. He landed from a jump awkwardly and reported that his knee gave out. He heard a pop at the time of injury and was unable to continue playing. He complains of medial and lateral knee pain and difficulty with weight bearing. On physical examination, he has a moderate effusion and his range of motion is from 10° to 80°. Ligament examination reveals a 2B Lachman, negative posterior drawer as well as negative varus and valgus stress testing. What is the diagnosis?
A. Meniscus tear
B. Anterior cruciate ligament (ACL) tear
C. ACL tear and posterior cruciate ligament (PCL) tear
D. ACL tear and medial meniscus tear
Question 8
When compared to patients with osteoarthritis, patients with ankylosing spondylitis undergoing total hip arthroplasty can expect a
Explanation
REFERENCE: Joshi A, Markovic L, Hardinge K, Murphy J: Total hip arthroplasty in ankylosing spondylitis: An analysis of 181 hips. J Arthroplasty 2002;17:427-433.
Question 9
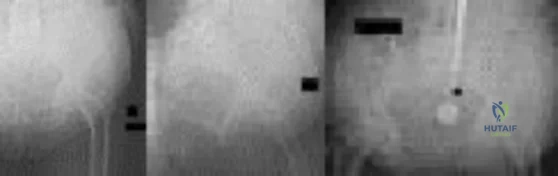
An obese (BMI = 35) 72-year-old woman with diabetes mellitus, hyptertension and a 22-pack-year smoking history is scheduled to undergo posterior spinal fusion from T10 to S1 with a pedicle subtraction osteotomy at L3 for the spinal deformity seen in Figure 1. Which of the following risk factors is most predictive of major complication following surgery Review Topic
Explanation
The surgical treatment of adult spinal deformity often requires multilevel arthrodesis with complex osteotomies including three column osteotomies such as pedicle
subtraction (PSO) and vertebral column resection (VCR). They can involve both anterior and posterior surgical approaches. Surgical time, blood loss, length of hospital stay, and length of recovery can be greater than it is for the more common degenerative conditions.
Auerbach et al. characterized the risk factors for the development of major complications in patients undergoing 3-column osteotomies for adult spinal deformity correction. They also aimed to determine whether the presence of complications affected the ultimate clinical outcome. They found age > 60 years, > or = 3 comorbid conditions and preoperative sagittal imbalance of = 40mm was associated with a major complication. However, the presence of a major complication did not affect the ultimate clinical outcomes at 2 years or more.
Daubs et al. conducted a retrospective analysis of forty-six patients = 60 years of age who underwent major spinal deformity surgery requiring a minimum 5-level arthrodesis procedure to determine the rate of complication and outcomes. The overall complication rate was 37% and the major complication rate was 20%. Increasing age was a significant factor (p<0.05) in predicting the presence of a complication, while presence of comorbidities was found to have no association.
Figure A is a standing preoperative lateral radiograph of the spine demonstrating a thoracic kyphosis of ~25° and thoracolumbar kyphosis of ~25°. Illustration A demonstrates proper sagittal balance after spinal fusion from T10 to S1 and L3 PSO.
Incorrect Answers:
Question 10
A 17-year-old boy has had elbow pain for the past 6 weeks. A radiograph, MRI scans, and biopsy specimens are shown in Figures 65a through 65e. What is the most likely diagnosis?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 87-102.
Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999,
pp 415-433.
Question 11
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
Explanation
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245.
Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Thometz JG, Gould JS: Cavus deformity, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 12
Excision of heterotopic bone about the forearm or elbow can be done with limited recurrence rates as early as which of the following after initial injury?

Explanation
The referenced study by McAuliffe et al is a retrospective review of heterotopic ossification (HO) about the elbow followed by 100 cGY (5 fractions over 1 week) of XRT as early as 3 months post-injury. They were able to achieve an average arc of motion > 100 degrees.
The other referenced study by Beingessner et al is a review of HO excision of the forearm. They found that excision and XRT, followed by 6 weeks of indomethacin, led to an increase of forearm motion from an average of 17 degrees to 136 degrees when the excision was done at 4 months post-injury.
Question 13
Figure 10 is an anteroposterior pelvis radiograph of an 82-year-old man who had right hip pain that began 2 weeks ago but has since resolved with use of over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs). Currently he has no pain. Examination of his hip shows decreased internal rotation and minimal pain at the extremes of motion. What is the most appropriate treatment at this point?

Explanation
The radiograph shown is consistent with Paget disease of the bone. It demonstrates classic findings of widened lamellae and disorganized sclerotic and lytic areas. The cause is not clearly defined, but may be linked to a viral infection and subsequent alterations of osteoblastic and osteoclastic activity. Most patients are asymptomatic, and Paget disease is often found incidentally on radiographs. In this case, the patient’s symptoms likely were caused by hip arthritis, but Paget disease can cause diffuse bone pain in some cases. Considering the patient’s mild and short-term symptoms, observation and NSAID use is most appropriate. An MRI scan or biopsy is indicated if sarcomatous transformation is suspected, but this condition is rare and is associated with a substantial, unrelenting increase in pain. SPEP and UPEP are tests for multiple myeloma, of which the radiographs show no signs.
RECOMMENDED READINGS
Ralston SH. Pathogenesis of Paget's disease of bone. Bone. 2008 Nov;43(5):819-25. doi: 10.1016/j.bone.2008.06.015. Epub 2008 Jul 11. Review. PubMed PMID: 18672105.View Abstract at PubMed
Bonenberger E, Einhorn T. Metabolic bone diseases. In: Callaghan JJ, Rosenberg
AG, Rubash HE, eds. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams 14
& Wilkins; 2007:514-533.
Question 14
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Explanation
REFERENCES: Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Apfelbaum RI, Kriskovich MD, Haller JR: On the incidence, cause, and prevention of recurrent laryngeal nerve palsies during anterior cervical spine surgery. Spine 2000;25:2906-2912.
Question 15
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?
Explanation
REFERENCES: Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 16
Figures 20a through 20c show the radiographs of a 69-year-old woman who has severe pain in her dominant right arm after falling on the ice. History includes arthritis, hypertension, and heart disease. She is neurovascularly intact. Management should consist of
Explanation
REFERENCES: Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Morrey BF: Fractures of the distal humerus: Role of elbow replacement. Orthop Clin North Am 2001;31:145-155.
Question 17
The therapeutic effect of etanercept in the treatment of rheumatoid arthritis is primarily mediated through
Explanation
REFERENCES: Weinblatt ME, Kremer JM, Bankhurst AD, et al: A trial of etanercept, a recombinant tumor necrosis factor receptor: Fc fusion protein, in patients with rheumatoid arthritis receiving methotrexate. N Engl J Med 1999;340:253-259.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 489-530.
Question 18
When placing a percutaneous retrograde pubic rami screw for fixation of an acetabular fracture, which of the following radiographic views can best ensure that the screw does not exit the posterior aspect of the superior pubic ramus?

Explanation
Question 19
Figure below shows the radiograph obtained from a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?

Explanation
The fracture has occurred around the stem, representing a Vancouver type B fracture, and the stem is clearly loose, making it a type B2 fracture. The appropriate treatment is removal of the loose in situ stem; ORIF of the femur using cerclage wires, cables, or a plate; and insertion of a longer revision stem such as a tapered fluted modular titanium or fully porous coated cylindrical stem to bypass the fracture. All of the other options are incorrect, because they represent inappropriate treatment options for a Vancouver type B2 fracture.
Question 20
Figures 1 and 2 show the radiographs obtained from a 56-year-old man who has been experiencing progressive wrist pain since he felt a pop while throwing a 25-pound bag over his shoulder 6 months ago. Failure to address the injury surgically might lead to progressive arthritic changes in what order?

Explanation
This patient demonstrates scapholunate dissociation with an associated dorsal intercalated segment instability deformity. Chronic scapholunate ligament tears lead to scapholunate advanced collapse (SLAC) wrist. Watson and Ballet describe SLAC wrist as having a predictable progression of arthritic changes, starting at the radial styloid, progressing to the radioscaphoid joint, and advancing to the lunocapitate joint. Some authors have described the radiolunate joint as being affected in very late-stage SLAC wrist.
Question 21
A 16-year-old football player is participating in the second session of two-a-day preseason practices. He complains of dizziness and fatigue. He is brought to the sideline by the athletic trainer where examination demonstrates confusion and disorientation. Ambient temperature is 82°F. What would be the next most appropriate step in his treatment?
Explanation
Question 22
Failure of high tibial osteotomy (HTO) is most closely associated with which of the following factors?
Explanation
with HTO.
REFERENCES: Naudie D, Borne RB, Rorabeck CH, Bourne TJ: Survivorship of the high tibial valgus osteotomy: A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
Rinonapoli E, Mancini GB, Corvaglia A, Musiello S: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Coventry MB, Ilstrup DM, Wallrichs SL: Proximal tibial osteotomy: A critical long-term study of eighty-seven cases. J Bone Joint Surg Am 1993;75:196-201.
Question 23
What type of physical therapy is most effective for chronic noninsertional Achilles tendinopathy?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 91-102.
Vora AM, Myerson MS, Oliva F, et al: Tendinopathy of the main body of the Achilles tendon.
Foot Ankle Clin 2005;10:293-308.
Question 24
A 75-year-old woman reports foot pain and states that her foot has become progressively “flatter” in the past 3 years. Custom inserts and physical therapy have failed to provide relief. Examination reveals a flexible hindfoot and mild heel cord contracture. The patient is able to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 21a through 21d. What is the most appropriate surgical management?
Explanation
REFERENCES: Toolan BC: Midfoot arthrodesis: Challenges and treatment alternatives. Foot Ankle Clin 2002;7:75-93.
Horton GA, Olney BW: Deformity correction and arthrodesis of the midfoot with a medial plate. Foot Ankle 1993;14:493-499.
Question 25
When reconstructing the anterior cruciate ligament (ACL) with autograft, what is the most common source of surgical failure?
Explanation
Question 26
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
REFERENCE: Herring JA (ed): Tachjians Pediatric Orthopedics, ed 3. Philadelphia, PA,
WB Saunders, 2002, vol 2, p 984.
Question 27
The use of nonsteroidal anti-inflammatory drugs following femoral nailing has been associated with which of the following?

Explanation
Giannoudis et al assessed factors which could affect union in 32 patients with nonunion of a fracture of the diaphysis of the femur and 67 matched patients whose fracture had united. They found that there was no relationship between the rate of union and the type of implant, mode of locking, reaming, distraction or smoking. They also concluded that there was a marked association between nonunion and the use of NSAIDs after injury and delayed healing was noted in patients who took NSAIDs and whose fractures had united.
Burd et al performed a study to determine if patients with an acetabular fracture, who received indomethacin for prophylaxis against HO, were at risk of delayed healing or nonunion of any associated fractures of long bones. The study group consisted of 112 patients who had sustained at least one concomitant fracture of a long bone; of which 36 needed no prophylaxis, 38 received focal radiation and 38 received indomethacin. When comparing patients who received indomethacin with those who did not, a significant difference was noted in the rate of long bone nonunion (26% vs 7%).
Question 28
A 68-year-old woman with metastatic breast carcinoma is seen in the emergency department. She appears lethargic, and she reports abdominal pain, nausea, and constipation. An EKG reveals a shortened QT interval. The only physical finding on examination is diffuse hyporeflexia. What is the most appropriate step in management?
Explanation
REFERENCE: Stewart AF: Clinical practice: Hypercalcemia associated with cancer. N Engl J of Med 2005;352:373-379.
Question 29
A 70-year-old golfer has pain in her dominant shoulder. She reports that initially the pain was at night but now she is unable to play. Examination reveals weakness in external rotation and shoulder abduction. Radiographs reveal the humeral head articulating with a thin acromion. Management should consist of
Explanation
REFERENCES: Bokor DJ, Hawkins RJ, Huckell GH, et al: Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
Wirth MA, Basamania C, Rockwood CA Jr: Nonoperative management of full-thickness tears of the rotator cuff. Orthop Clin North Am 1997;28:59-67.
Question 30
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
(type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive.
REFERENCES: Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Zerres K, Wirth B, Rudnik-Schoneborn S: Spinal muscular atrophy: Clinical and genetic correlations. Neuromuscul Disord 1997;7:202-207.
Question 31
A 25 year-old-male presents with the injury seen in Figure A. Which of the following would be a contraindication to closed management with a functional brace?

Explanation
Indications for operative management of humeral shaft fractures are limited given the high rates of union and ability of adjacent joints to compensate for deformity. Intact muscular tone is necessary to effect bony apposition in closed treatment with a functional brace. The absence of neurologic and muscle function in patients with a flail extremity leads to increased rates of nonunion and malunion.
Rutgers and Ring conducted a retrospective review of patients managed with functional bracing of humeral shaft fractures at a single institution. The authors found a 90% overall union rate, with maintenance of shoulder and elbow motion. They caution though, that 29% of their proximal third fractures went on to nonunion.
Figure A demonstrates an AP radiograph of a comminuted humeral shaft fracture with varus alignment.
Incorrect Answers:
Question 32
The blood supply to the anterior cruciate ligament is primarily derived from what artery?
Explanation
REFERENCES: Arnoczky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
Arnoczky SP, Rubin RM, Marshall JL: Microvasculature of the cruciate ligaments and its response to injury. J Bone Joint Surg Am 1979;61:1221-1229.
Question 33
- A patient is in respiratory distress as a result of a high-speed motor vehicle accident. After emergent intubation, the arterial blood is poorly oxygenated, and examination shows left-sided tracheal deviation, absence of breath sounds on the right side and tympany on percussion over the right side of the chest. Management should include
Explanation
Question 34
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
REFERENCES: Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
McAuley JP, Moreau G: Sepsis: Etiology, prophylaxis, and diagnosis, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, pp 1295-1306.
Question 35
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?
Explanation
REFERENCES: Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39.
Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Relationship of disease stage, extent, and cause to natural history. J Shoulder Elbow Surg 1999;8:559-564.
Question 36
Which of the following best describes the relationship of the anterior tibial artery and dorsalis pedis artery to the extensor hallucis longus (EHL) tendon as they progress from the level of the ankle to the dorsum of the foot?
Explanation
REFERENCES: Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 37
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?
Explanation
REFERENCES: Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Warner JJ, Higgins L, Parsons IM, et al: Diagnosis and treatment of anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2001;10:37-46.
Question 38
A 38-year-old woman has a lesion on her left foot that has increased in size over the past 6 months. The clinical photograph is shown in Figure 17a, and a photomicrograph of the biopsy specimen is shown in Figure 17b. What is the most likely diagnosis?
Explanation
REFERENCES: Hughes LE, Horgan K, Taylor BA, Laidler P: Malignant melanoma of the hand and foot: Diagnosis and management. Br J Surg 1985;72:811-815.
Fortin PT, Freiberg AA: Malignant melanoma of the foot and ankle. J Bone Joint Surg Am 1995;77:1396-1403.
Question 39
Which of the following is considered a specific advantage of using COX-2 inhibitors over COX-1 inhibitors?
Explanation
REFERENCES: Lane JM: Anti-inflammatory medications: Selective COX-2 inhibitors. J Am Acad Orthop Surg 2002;10:75-78.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000.
Question 40
When using highly cross-linked ultra-high molecular weight polyethylene as an articulating surface for total knee arthroplasty, what property of the material raises concern?
Explanation
REFERENCE: Koval KJ (ed): Orthopaedic Knowlegde Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 193-199.
Question 41
A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the medial collateral ligament (MCL). Examination reveals valgus instability and ulnar nerve involvement. What recommendations should be made based on the patient’s desire to return to sport? Review Topic
Explanation
stresses during the late cocking and acceleration phase of throwing can injure the anterior band of the MCL. Clinically, the injuries may present as chronic or acute, and a pop may be noted in the latter. Associated ulnar nerve involvement is common. Valgus instability is present in about 25% of patients. Patients typically are athletes who participate in throwing and have localized medial elbow pain and tenderness along the course of a ligament that extends from the medial epicondyle of the distal humerus to the sublime tubercle of the ulna. Surgical reconstruction is the procedure of choice in an athlete desiring a return to a high level of throwing.
Question 42
Figures 23a and 23b show the radiographs of a 75-year-old woman who sustained an injury to her nondominant hand. Initial treatment should consist of
Explanation
REFERENCES: Handoll HH, Madhok R: Conservative interventions for treating distal radial fractures in adults. Cochrane Database Syst Rev 2003;2:CD000314.
Young CF, Nanu AM, Checketts RG: Seven-year outcome following Colles’ type distal radial fracture: A comparison of two treatment methods. J Hand Surg Br 2003;28:422-426.
Question 43
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals no other injuries. Radiographs are shown in Figures 35a and 35b. Initial management of this fracture should consist of
Explanation
REFERENCES: Meyers MH, McKeever FM: Fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60
Janarv PM, Westblad P, Johansson C, Hirsch G: Long-term follow-up of anterior tibial spine fractures in children. J Pediatr Orthop 1995;15:63-68.
Kuhn JE, Sailer MJ, Sterett WI, Hawkins RJ: Arthroscopic technique for the treatment of tibial spine fractures in the skeletally immature patient. J Ortho Tech 1995;3:7-12.
Question 44
-The center of rotation of the knee can be best described as
Explanation
Question 45
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
REFERENCES: Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Post M, Mayer J: Suprascapular nerve entrapment: Diagnosis and treatment. Clin Orthop 1987;223:126-136.
Question 46
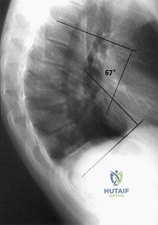
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of Review Topic
Explanation
Question 47
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the
Explanation
REFERENCES: Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235.
Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Byrd JWT: Indications and contraindications, in Byrd JWT (ed): Operative Hip Arthroscopy. New York, NY, Thieme, 1998, pp 7-24.
Question 48
Explanation
In the context of viewing a lateral cervical spine to evaluate cranial setting, multiple lines can be used to assess anatomic relationships (i.e. McRae’s Chamberlin’s, or McGregor’s) McRae’s and Chamberlin’s use the foramen magnum as one land mark. Commonly, however, the margins of the foramen magnum are difficult to precisely identify. McGregor’s line connects the posterior margin of the hard palate to the most caudal point of the occiput and is easier to use. The tip of the odontoid should not project more than 4.5 mm above this line.
Anterior subluxation of more than 10-12 mm implies destruction of the entire ligamentous complex.
An atlantoaxial distance greater than 3.5mm is considered abnormal in an adult. The subaxial cervical spine is affected through involvement of the facets, interspinous ligaments, and intervertebral discs (spondylodiscitis). The initial site of destruction has been postulated to be through synovitis of the neurocentral joints with erosion of the adjacent disc and bone causing subluxation, or through primary facetal arthritis and ligamentous laxity causing secondary chronic discovertebraltrauma and destructive hypermobile segmentsis associated with disc destruction and toward the C2-C3 and C3-C4 segments, typically lack osteophytes, and often are at multiple levels, giving a stepladder appearance.
Question 49
Which of the following is the primary mechanism of polyethylene wear in the hip?
Explanation
26-/28-mm heads (1-mm increase in size increased volumetric wear by 10%). The wear at the articulating surface was characterized by highly worn polished areas superiorly and less worn areas inferiorly separated by a ridge. Abrasion was very common, occurring after adhesion and plastic deformation of polyethylene fibrils, and abrasion secondary to third-body wear. Wear rates decreased with longer survival of components, indicating a “bedding in” phenomenon, arguing against oxidative and fatigue wear. Crevice corrosion occurs in fatigue cracks with low oxygen tension (under screw heads, etc). Oscillatory fretting consists of cyclical abrading of the outer surface from small movements. Fatigue and delamination is predominant in total knee arthroplasty where stresses are maximum just below the surface of the polyethylene component, causing fatigue over time with subsequent delamination. In contrast, hip wear occurs primarily at the surface of the polyethylene component.
REFERENCES: Jasty M, Goetz DD, Bragdon CR, et al: Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg Am 1997;79:349-358.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53.
Bell CJ, Walker PS, Abeysundera MR, et al: Effect of oxidation on delamination of
ultrahigh-molecular-weight polyethylene tibial components. J Arthroplasty 1998;13:280-290.
Sutula LC, Collier JP, Saum KA, et al: The Otto Aufranc Award: Impact of gamma sterilization on clinical performance of polyethylene in the hip. Clin Orthop 1995;319:28-40.
Question 50
This image represents the end stage of an uncompensated rotator cuff tear.
Explanation
Axillary lateral and anteroposterior (AP) images of the right shoulder (Figures 59c and 59d) reveal osteoarthrosis of the glenohumeral joint, which typically is not associated with significant rotator cuff pathology. An examination often shows limitations in range of motion, crepitance, and pain with motion. An AP radiographic image of the right shoulder (Figure 59b) reveals proximal humeral migration, which normally correlates with rotator cuff tear size. Tears extending into the infraspinatus tendon are associated with more humeral migration than is seen with isolated supraspinatus tears. Presenting complaints are usually of pain and weakness. Examination findings include subacromial crepitance and weakness during rotator cuff testing. Rarely, this may be associated with pseudoparalysis in large uncompensated rotator cuff tears. The CT image of the right shoulder (Figure 59a) shows superior migration of the humerus with respect to the glenoid surface and end-stage
degenerative changes at the glenohumeral joint. These changes are classified as rotator cuff arthropathy. Pain and weakness are common, as is the presence of pseudoparalysis and limited range of motion.
RECOMMENDED READINGS
Kelly JD Jr, Norris TR. Decision making in glenohumeral arthroplasty. J Arthroplasty. 2003 Jan;18(1):75-82. Review. PubMed PMID: 12555187. View Abstract at PubMed
Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009 Jun;91(6):1405-13. doi: 10.2106/JBJS.H.00854. PubMed PMID:
Question 51
The vessel seen in the clinical photographs shown in Figures 50a and 50b (1,2 intercompartmental supraretinacular artery) is being dissected to be used as a source of vascularized bone graft for a patient who is scheduled to undergo internal fixation of a scaphoid nonunion. This vessel is a branch of what artery?
Explanation
REFERENCES: Sheetz KK, Bishop AT, Berger RA: The arterial blood supply of the distal radius and ulna and its potential use in vascularized pedicled bone grafts. J Hand Surg 1995;20:902-914.
Steinmann SP, Bishop AT, Berger RA: Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg
2002;27:391-401.
Question 52
At the time of revision knee arthroplasty, a surgeon performs a rectus snip to gain exposure to the knee. When compared with a standard parapatellar approach, what is the expected outcome?
Explanation
Rectus snip during total knee arthroplasty has no effect on motion or strength at long-term follow-up. It has not been associated with extensor mechanism lag.
Question 53
When performing the exposure for an anterior approach to the cervical spine, excessive retraction of the trachea and esophagus should be avoided to prevent injury of the
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD,
Williams and Wilkins, 1998, chapter 2.
Flynn TB: Neurologic complication of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 54
Figures below show the radiographs obtained from an 86-year-old-woman who has had chronic left hip pain for several years. She now uses a walker and a wheelchair for ambulation. She is medically healthy. What is the most appropriate surgical intervention?
Explanation
This 86-year-old woman has poor bone quality and osteoarthritis of the left hip. Her lateral radiograph confirms Dorr type C bone quality. A hybrid left THA with a cemented femoral stem would be the treatment of choice.
Question 55
A 56-year-old woman presents with left hip pain and diminishing range of motion. Examination reveals pain with range of motion of the hip. Radiographs reveal multiple calcific lesions within the hip and well-preserved joint space. MRI scan shows thickened synovium nodular loose bodies with decreased signal on T1 and T2. What is the best next step?
Explanation
Question 56
..Figures 83a and 83b are the radiographs of a 53-year-old otherwise healthy homemaker who had a syncopal episode and sustained a ground-level fall and injury to her right elbow. She presently admits to right elbow pain, swelling, and an inability to bend her elbow. What is the best initial treatment for this injury?
Explanation
Figure 84 is the glenoid CT scan of a 20-year-old man who dislocated his shoulder anteriorly while playing football. He had persistent instability 2 months after the injury, but he did not have a sulcus sign or posterior instability. He underwent an arthroscopic Bankart repair with 4 bioabsorbable anchors with simple sutures through the labrum and capsule.
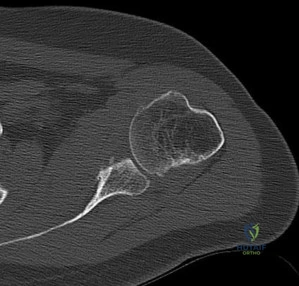
He did not have an engaging Hill-Sachs lesion, the rotator cuff was unremarkable, and the capsule was not torn from the humerus. After surgery, he did well for 6 months until he jumped into a lake and again dislocated his shoulder anteriorly. He says his shoulder no longer felt stable after his reduction.
Question 57
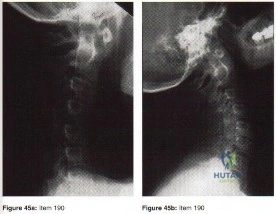
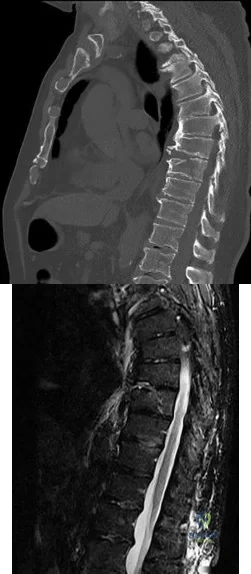
A B Figures 45a and 45b are the CT and MR spine images of an 82-year-old man who has a history of ankylosing spondylitis falls onto his back. He has no neurologic deficits upon examination in the emergency department. What is the most appropriate next step?
Explanation
Spinal fractures in patients with ankylosing spondylitis are unstable and generally necessitate surgical intervention. In a patient with a spinal fracture in the setting of ankylosing spondylitis, posterior instrumented fusion is an appropriate surgical procedure. Treatment with a thoracolumbar orthosis is not an option for patients with extension distraction injuries in the setting of an ankylosed spine because of risk for displacement. Similarly, simply checking upright radiographs is generally not advocated. Laminectomy alone is inappropriate for this patient because there is no cord compression and neurologic symptoms are absent. Stabilization is the treatment goal.
RECOMMENDED READINGS
Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007 Apr 21;369(9570):1379-90. Review. PubMed PMID: 17448825.View Abstract at PubMed
Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64. doi: 10.1097/BRS.0b013e3181cc764f. PubMed PMID: 20421858. View Abstract at PubMed Finkelstein JA, Chapman JR, Mirza S. Occult vertebral fractures in ankylosing spondylitis. Spinal Cord. 1999 Jun;37(6):444-7. PubMed PMID: 10432265. View Abstract at PubMed Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002 Sep;97(2 Suppl):218-22. PubMed PMID: 12296682. View Abstract at PubMed
Question 58
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5° of angulation. When the MCP joint is flexed 30°, a radially directed stress produces 45° of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
REFERENCES: Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Heyman P: Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint.
J Am Acad Orthop Surg 1997;5:224-229.
Question 59
A 14-year-old female has anal hemorrhoids. The General Surgical team has asked for a consultation in regards to her history of hand, wrist, and ankle joint pain and swelling over the past 3 years. Her physical examination reveals a swollen left wrist, right knee and left ankle. Lab work shows low hemoglobin, low albumin, elevated erythrocyte sedimentation rate (ESR), elevated antinuclear antibody (ANA) count, and a negative rheumatoid factor. Radiography of the affected joints are normal. What additional work up is required prior to her rectal surgery? Review Topic
Explanation
JIA is a persistent autoimmune inflammatory arthritis lasting more than 6 weeks in a patient younger than 16 years of age. Serologic testing for this condition will usually show elevated ESR/CRP, low hemoglobin, low albumin and an elevated anti-nuclear antibody (ANA) count, as well as negative rheumatoid factor and positive HLA-B27. Radiographs of the c-spine should be considered in patients undergoing intubation as cervical kyphosis, facet ankylosis, and atlantoaxial subluxation is associated with this condition.
Punaro et al. reviewed rheumatologic conditions in children. The typical patient with
oligoarticular JIA is a white female (5:1, F:M), with a peak onset between ages 1 and 3 years. Nearly half of patients have monoarticular involvement, with the knee and ankle being most commonly involved. Uveitis is typically chronic, bilateral, and asymptomatic.
Borchers et al. reviewed juvenile idiopathic arthritis (JIA). They state that no laboratory test can conclusively establish a rheumatic diagnosis. They state that laboratory tests will be negative for systemic inflammation and antinuclear antibody (ANA) test has no use in screening for JIA, as it has a high false positive rate.
Incorrect Answers:
Question 60
Figures A-C are images of a 37-year-old man who presents with isolated muscle atrophy due to a compressed nerve. Which of the following sequences correctly describes the pathway of this nerve through the brachial plexus, before it innervates the affected muscles?
Explanation
Quadrilateral space syndrome is a condition defined by axillary nerve, +/- posterior humeral circumflex artery compression in the quadrilateral space. It most commonly affects the dominant shoulder in overhead movement athletes (e.g. basketball players) or other throwing athletes. Physical examination may reveal weakness with the arm positioned in abduction and external rotation. In situations of long-standing compression, there may also be atrophy of the teres minor and deltoid muscle.
Chafik et al. dissected thirty-one cadaveric human shoulders to describe the neuromuscular anatomy of teres minor. They showed that the primary nerve branch to teres minor travelled in a fascial sling 44 mm medial to the muscular insertion. This
area may be the potential site of greatest compression and tethering of this nerve in patients with isolated teres minor atrophy.
Friend et al. performed a cadaveric dissection of nine shoulder specimens to look at the anatomical variability in course, length and branching pattern of both the teres minor nerve and the axillary nerve. These were compared to a case-based study of these two male patients with isolated atrophy of teres minor. They concluded that there is no good anatomical predictor of nerve compression outside the quadrilateral space as there is considerable anatomical variation in its origin and course, as well as potential site of compression.
Figure A-C are MRI images that show atrophy of the teres minor muscle and possibly deltoid muscle. The rotator cuff muscles are labeled in Illustration A. The teres minor muscle is labeled in Illustration B. Illustration C shows a diagram of the brachial plexus.
Incorrect
1:
This
describes
the
musculocutaneous
nerve.
3:
This
describes
the
suprascapular
nerve.
4:
This
describes
the
long thoracic
nerve.
Question 61
What is the primary intracellular signaling mediator for bone morphogenetic protein (BMP) activity?
Explanation
REFERENCES: Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Zuscik MJ, Drissi MH, Reynolds PR, et al: Molecular and cell biology in orthopaedics, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 62
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?
Explanation
REFERENCES: Gelb DE, Lenke LG, Bridwell KH, et al: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20:1351-1358.
Vedantam R, Lenke LG, Keeney JA, et al: Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine 1998;23:211-215.
Question 63
In infantile idiopathic scoliosis, which of the following factors suggests progression?
Explanation
REFERENCES: Mehta MH: The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J Bone Joint Surg Br 1972;54:230-243.
Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 697.
Question 64
Following operative repair of lower extremity long bone and periarticular fractures, what is the time frame for patients to return to normal automobile braking time?

Explanation
The second reference by Egol studied only operatively treated ankle fractures and found that time to appropriate braking returns at 9 weeks postoperatively. Interestingly, no significant association was found between the functional scores and normalization of total braking time.
Question 65
Figure 22 reveals what anatomic variant of the lumbar spine?
Explanation
REFERENCES: Brault JS, Smith J, Currier BL: Partial lumbosacral transitional vertebra resection for contralateral facetogenic pain. Spine 2001;26:226-229.
Quinlan JF, Duke D, Eustace S: Bertolotti’s syndrome: A cause of back pain in young people.
J Bone Joint Surg Br 2006;88:1183-1186.
Whelan MA, Feldman F: The variant lumbar pedicle. Neuroradiology 1982;22:235-242.
Question 66
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?
Explanation
REFERENCES: Calvert E, Younger A, Penner M: Post talus neck fracture reconstruction.
Foot Ankle Clin 2007;12:137-151.
Migues A, Solari G, Carrasco NM, et al: Repair of talar neck nonunion with indirect corticocancellous graft technique: A case report and review of the literature. Foot Ankle Int 1996;17:690-694.
Question 67
In a patient with a major head injury and a femoral shaft fracture, intraoperative hypotension during femoral fixation has been associated with which of the following?

Explanation
Question 68
All of the following indicators of resuscitation may be within normal limits for a trauma patient that is in "compensated" shock EXCEPT:

Explanation
Question 69
The palmar cutaneous branch of the median nerve (PCBMN) originates from the
Explanation
REFERENCES: Hobbs RA, Magnussen PA, Tonkin MA: Palmar cutaneous branch of the median nerve. J Hand Surg Am 1990;15:38-43.
Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System: Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8,
p 52.
Question 70
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. What is the most likely area of injury?
Explanation
Question 71
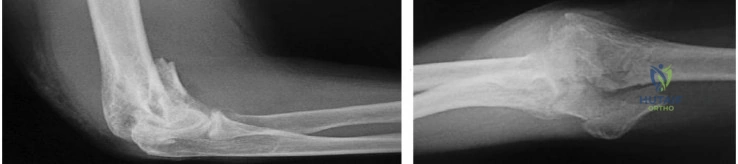
A 72-year-old woman presents for follow-up after elbow surgery. Her radiographs are shown in Figures A and B. Which of the following pre-operative diagnoses is a relative contraindication to the use of this prosthesis design? Review Topic
Explanation
Unconstrained (unlinked or resurfacing prosthesis) TEA depend on intact bony and ligamentous constraints for stability. These are appropriate for humeroulnar conditions with intact collateral ligaments and radiocapitellar articulation e.g. osteoarthritis, post-traumatic arthritis, intra-articular distal humerus fracture, and malunion of the distal humerus. Conditions with increased risk of instability (ligamentous injury, rheumatoid arthritis) will benefit from a linked or semiconstrained prosthesis.
Mansat et al. reviewed the Coonrad-Morrey linked (semi-constrained) TEA implant in 70 patients after 5 years. They found that patients with inflammatory arthritis had higher function than those with traumatic conditions (fractures, nonunions and posttraumatic arthritis). Survival rate was 98% and 91% at 5 and 10 years, respectively. They concluded that this implant provided satisfactory treatment for different indications although radiolucent lines and bushing wear were a concern.
Hildebrand et al. reviewed the functional outcome of the Coonrad-Moorey prosthesis in 51 elbows after 50 months. The inflammatory arthritis group had higher performance scores than the traumatic/post-traumatic conditions group. Isometric extensor torque was found to be less than the nonoperated side. Radiolucency was noted in 11 elbows.
Figures A and B show an unconstrained TEA with radial head replacement. Illustration A shows more examples of unconstrained TEA. Illustration B shows a semiconstrained TEA. The arrow points to the anterior flange. Illustration C shows radiolucent lines around the stems. Illustration D shows severe bushing wear leading to locking mechanism failure. Illustration E is a table comparing linked and unlinked implants.
Incorrect Answers:
Question 72
A 22-year-old man sustained a shoulder dislocation while playing collegiate football at age 18. Since that time, he has dislocated the shoulder three more times despite physical therapy. His last dislocation occurred 4 weeks ago while sleeping. What is the most appropriate management for this patient? Review Topic
Explanation
Question 73
A 79-year-old woman with a massive rotator cuff tear presents to the emergency department with pain and difficulty moving her arm 7 weeks after undergoing reverse TSA for a displaced 4-part proximal humerus fracture.
Explanation
The complication rate is high after surgical treatment of proximal humerus fractures, particularly in elderly patients with osteoporotic bone. In patients treated with ORIF, common complications include varus malunion (16%), avascular necrosis (10%), screw penetration (8%), and infection (4%). In cases involving a dislocation of the humeral head, avascular necrosis is more common. In patients treated with hemiarthroplasty or TSA, complications include component loosening, infection, and dislocation. TSA is associated with
glenoid loosening in patients with rotator cuff incompetence and should be avoided in these patients. Reverse TSA is a potential solution for this population. Dislocation and postoperative infection are potential complications after reverse TSA.
RECOMMENDED READINGS
Krappinger D, Bizzotto N, Riedmann S, Kammerlander C, Hengg C, Kralinger FS. Predicting failure after surgical fixation of proximal humerus fractures. Injury. 2011 Nov;42(11):1283-
Question 74
A 54-year-old man undergoes total shoulder arthroplasty for osteoarthritis. Despite compliance with an early passive range-of-motion exercise program, he does not regain more than 90 degrees of elevation, 10 degrees of external rotation, and has internal rotation to the fifth lumbar vertebra. At 6 months, his motion fails to improve. Radiographs are shown in Figures 18a and 18b. What is the best course of action?
Explanation
REFERENCES: Cuomo F, Checroun A: Avoiding pitfalls and complication in total shoulder arthroplasty. Orthop Clin North Am 1998;29:507-518.
Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 75
A 32-year-old man presents to the emergency department with a humeral shaft fracture. He has wrist drop as well as impaired finger and thumb extension. Which motor function would be expected to recover last?

Explanation
Abrams et al detailed the order of innervation of the radial nerve and found the following order (proximal to distal): brachioradialis, extensor carpi radialis longus, supinator, extensor carpi radialis brevis, extensor digitorum communis, extensor carpi ulnaris, extensor digiti quinti, abductor policis longus, extensor policis longus, extensor policis brevis, and extensor indicis proprius.
Branovacki et al found a slightly different pattern: brachioradialis, extensor carpi radialis longus, superficial sensory, extensor carpi radialis brevis, supinator, extensor digitorum/extensor carpi ulnaris, extensor digiti minimi, abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus and extensor indicis proprius.
While both extensor digitorum and extensor indicis proprius extend the index finger MCP joint, only extensor indicis proprius hyperextends the index finger past neutral
Question 76
What is the most likely cause of the lesion shown in Figures 35a and 35b?
Explanation
REFERENCES: Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Jarvinen TA, Jarvinen TL, Kaariainen M, et al: Muscle injuries: Biology and treatment. Am J Sports Med 2005;33:745-764.
Question 77
Which nerve root contributes to both the sciatic and femoral nerves?
Explanation
The lumbosacral plexus is formed from the lumbar and sacral roots that are redistributed into the obturator, femoral, and sciatic nerves. The obturator nerve is composed of the L1, L2, and L3 roots. The femoral nerve has contributions from the L3 and L4 roots. The sciatic nerve contains the L4, L5, S1, and lower sacral roots. Therefore, only the L4 root contributes to the femoral and sciatic (via the lumbosacral trunk) nerves, which allows it to innervate the quadriceps and the anterior tibialis muscles.
RECOMMENDED READINGS
Question 78
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?
Explanation
REFERENCES: Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Posner MA: Flexor superficialis tendon transfers to the thumb: An alternative to the free tendon graft for treatment of chronic injuries within the digital sheath. J Hand Surg Am 1983;8:876-881.
Question 79
To preserve blood supply to the fractured bone seen in Figures 12a and 12b, care should be taken when exposing which of the following areas?
Explanation
REFERENCE: Yamaguchi K, Sweet FA, Bindra R, et al: The extraosseous and intraosseous arterial anatomy of the adult elbow. J Bone Joint Surg Am 1997;79:1653-1662.
Question 80
What is the most common complication following total disk arthroplasty in the lumbar spine?
Explanation
REFERENCE: Tropiano P, Huang RC, Girardi FP, et al: Lumbar total disc replacement: Seven to eleven-year follow-up. J Bone Joint Surg Am 2005;87:490-496.
Question 81
A positive straight leg raising sign is when pain radiates distal to the knee when the affected leg is passively elevated. The increased tension generally occurs between Review Topic
Explanation
Question 82
Figure 16 shows an axial MRI scan through the knee joint. What structure is identified by the arrow?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 675-699.
Fitzgerald SW, Remer EM, Friedman H, Rogers LF, Hendrix RW, Schafer MF: MR evaluation of the anterior cruciate ligament: Value of supplementing sagittal images with coronal and axial images. Am J Roentgenol 1993;160:1233-1237.
Question 83
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include “onion bulb” formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?
Explanation
REFERENCES: Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422.
Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Miller GM, Hsu JD, Hoffer MM, Rentfro R: Posterior tibial tendon transfer: A review of the literature and analysis of 74 procedures. J Pediatr Orthop 1982;2:363-370.
Question 84
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of
Explanation
REFERENCES: Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Gerber C, et al: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 85
A 62-year-old patient with rheumatoid arthritis has had pain and instability of the elbow following total elbow replacement 2 years ago. A complete work-up, including aspiration and cultures, is negative. Figures 9a and 9b show the AP and lateral radiographs. Treatment should consist of
Explanation
REFERENCES: Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Morrey BF, King GJ: Revision of failed total elbow arthroplasty, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Question 86
Figure 30 shows the radiograph of a 38-year-old man who reports persistent pain laterally and plantarly about the fifth metatarsal head. Examination reveals calluses dorsolaterally and plantarly about the fifth metatarsal head. Nonsurgical management has failed to provide relief. Surgical treatment should include
Explanation
REFERENCES: Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Moran MM, Claridge RJ: Chevron osteotomy for bunionette. Foot Ankle Int 1994;15:684-688.
Question 87
Figures 1 through 3 are the MRI scans of a 26-year-old man who injured his knee wrestling one day prior. He has a moderate effusion, medial knee pain and an inability to extend his knee actively or passively. What is the most appropriate definitive treatment option?
Explanation
Question 88
A patient who underwent a high tibial osteotomy (HTO) is now scheduled to undergo total knee arthroplasty (TKA). When compared with a patient undergoing primary TKA without a prior HTO, the patient should be advised to expect a higher incidence of
Explanation
REFERENCE: Mont MA, Alexander N, Krackow KA, Hungerford DS: Total knee arthroplasty after failed high tibial osteotomy. Orthop Clin North Am 1994;25:515-525.
Question 89
A 13-year-old boy sustains a valgus stress injury to the knee while playing football, and he is unable to bear weight after the injury. Examination reveals tenderness medially superior to the joint line. The knee is held in flexion, and he has a large effusion and localized medial swelling. Plain radiographs show no obvious fracture. What is the next diagnostic step?
Explanation
REFERENCES: Smith L: Concealed injury to the knee. J Bone Joint Surg Am 1962;44:1659-1660.
Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 90
Which of the following best describes heat stroke?
Explanation
[41 degrees C]), central nervous system dysfunction, and cessation of sweating with hot, dry skin. It is a medical emergency that results from failure of the thermoregulatory mechanisms of the body. It has a high death rate and requires rapid reduction in body core temperature. Heat syncope is characterized by a transient loss of consciousness with peripheral vasodilation and decreased cardiac output with normal body temperature. Heat cramps involve painful contractions of large muscle groups because of decreased hydration and a decrease of serum sodium and chloride. Heat exhaustion is distinguished by a core temperature of less than
Question 91
In patients with suspected hepatitis C, which of the following tests is commonly used to confirm the diagnosis after a positive ELISA screening test?
Explanation
REFERENCES: de Medina M, Schiff ER: Hepatitis C: Diagnostic assays. Semin Liver Dis 1995;15:33-40.
McGrory BJ, Kilby AE: Hepatitis C virus infection: Review and implications for the orthopedic surgeon. Am J Orthop 2000;29:261-266.
Question 92
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Explanation
REFERENCES: Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Simpson NS, Jupiter JB: Clavicular nonunion and malunion: Evaluation and surgical management. J Am Acad Orthop Surg 1996;4:1-8.
Question 93
What is the best initial screening test for a patient with a limb-length discrepancy?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 1041-1045.
Schoenecker PL, Rich MM: The lower extremity, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1120-1122.
Stanitski DF: Limb-length inequality: Assessment and treatment options. J Am Acad Orthop Surg 1999;7:143-153.
Aaron A, Weinstein D, Thickman D, Eilert R: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Question 94
A 7 5-year-old man who sustained an intertrochanteric hip fracture underwent open reduction and internal fixation with a sliding hip screw. Six months after the procedure, the patient has shortening and external rotation of the extremity and progressively severe groin pain with ambulation. Radiographs are shown in Figures 5a and 5b. What is the most appropriate management?
Explanation
REFERENCE: Said GZ, Farouk O, El-Sayed A, et al: Salvage of failed dynamic hip screw fixation of intertrochanteric fractures. Injury 2006;37:194-202.
Question 95
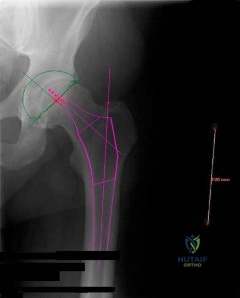
Figure below depicts the radiograph obtained from a 30-year-old woman who began having more right than left hip pain during a recent pregnancy. Physical examination reveals increased range of motion with positive flexion abduction and external rotation and flexion adduction and internal rotation as well as pain with external logroll. Assessment of Figure below reveals

Explanation
Studies have demonstrated that pelvic inclination can dramatically affect the interpretation of radiographs in the dysplastic hip, with 9° of increased pelvic inclination leading to the presence of crossover signs and posterior wall signs. A distance of 30 mm to 50 mm from the sacrococcygeal junction to the pubis is often used to assess the adequacy of pelvic inclination on radiographs, although Siebenrock and associates determined the mean difference to be 32 mm in men and 47 mm in women. In this patient, the pelvic inclination is dramatically increased, leading to overestimation of acetabular retroversion.
Question 96
A complication associated with using the Morrey approach (triceps reflecting) to implant a semiconstrained total elbow arthroplasty is
Explanation
used for elbow arthroplasty.
Question 97
A 5-year-old boy reports intermittent left elbow pain. History reveals that he injured his elbow 4 months ago, but had no treatment. He is now using his arm normally but reports pain almost daily. Examination reveals tenderness over the lateral epicondyle and a prominence is evident. Range of motion is from -5 degrees to

Explanation
(SBQ13PE.40) Immediate spica casting is most appropriate for which of the following?: Review Topic
2-month-old girl with a displaced spiral mid-diaphyseal femur fracture
A 26-month-old boy with a displaced spiral mid-diaphyseal femur fracture with <2 centimeters of shortening
3-day-old with teratologic right hip dislocation
9-year-old boy with a displaced spiral mid-diaphyseal femur fracture
12-year-old girl weighing 90 pounds with a displaced spiral mid-diaphyseal femur fracture
Children older than 6 months and up to 6 years with diaphyseal femur fractures may be treated with spica casting.
Children younger than 6 months may only require a Pavlik harness. Immediate spica casting is indicated in children 6 months to 6 years with less than 2 cm of shortening. Each additional cm of shortening at presentation doubles the risk of loss of reduction (1 cm: 12%, 2 cm: 24%, 3 cm; 50%).
Kocher et al. provide the AAOS Clinical Practice Guideline for the treatment of pediatric diaphyseal femur fractures. Their recommendation for diaphyseal femur fractures with <2 cm shortening in children 6 months to 5 years is Grade B, based on Level II evidence (two level II and one level I study). They recommend early spica or traction with delayed spica. They suggest early spica, as this is more convenient than traction.
In an earlier article, Flynn et al. review the management of pediatric femoral shaft fractures. They recommend early spica casting for the child between 1 and 6 years in
low-energy femoral fractures with up to 2 cm shortening. Illustration A shows several styles of lower extremity spica casts.
Incorrect answers:
Question 98
A high school football player asks you about an oral supplement that increases body mass and improves sprint times. He would like to use it to improve performance. What is the most likely agent?
Explanation
REFERENCES: McGuine TA, Sullivan JC, Bernhardt DT: Creatine supplementation in high school football players. Clin J Sports Med 2001 ;11:247-253.
Rawson ES, Gunn B, Clarkson PM: The effects of creatine supplementation on exercise-induced muscle damage. J Strength Cond Res 2001; 15:178-184.
Branch JD: Effect of creatine supplementation on body composition and performance: A meta-analysis.
Int J Sport Nutr Exerc Metab 2003;13:198-226.
Question 99
A year-old man with insulin-dependent diabetes mellitus underwent primary total knee arthroplasty (TKA). A full-thickness skin slough measuring 3 cm by 4 cm developed, with postsurgical exposure of the patellar tendon. No change is observed in the appearance of the wound after 2 weeks of wet-to-dry dressing changes. What is the best next treatment step for the soft-tissue defect?
Explanation
If wound healing does not occur and deep soft tissues such as the patellar tendon are exposed following TKA, local rotational flap is the procedure of choice. The procedure should be performed relatively early after the recognition of a soft-tissue wound-healing problem. In the setting of TKA, the gastrocnemius muscle is an excellent source of flaps for wound coverage of the proximal tibia.
Question 100
An 18-year-old boy has had pain in the right knee for the past 6 months. Examination reveals some fullness behind the knee but no significant palpable soft-tissue mass. There is no effusion, and he has full knee range of motion. The remainder of the examination is unremarkable. A radiograph and MRI scans are shown in Figures 33a through 33c, and biopsy specimens are shown in Figures 33d and 33e. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 20-21.
Unni KK, Dahlin DC, Beabout JW, Ivins JC: Parosteal osteogenic sarcoma. Cancer 1976;37:2466-2475.
